INTRODUCTION. It is our hope you will find this book an essential addition to your professional reference library.
|
|
|
- rajeshwwari raji
- 5 years ago
- Views:
Transcription
1 ITRODUCTIO Introduction Pages: - Interventional radiology procedural coding is recognized as one of the most complex areas of CPT coding. The use of component coding to describe these diagnostic and therapeutic percutaneous procedures allows for thousands of code combinations, depending on how and what procedures are performed. dd in the new trend to create all-inclusive comprehensive codes, keeping the coding rules straight becomes even more difficult. The physician, clinician, or coding professional must have a strong knowledge of both vascular and non-vascular interventional radiology coding rules. Each of these sets of rules by themselves are challenging to master. This compounds the complexity and the scope of knowledge required for accurate and compliant billing of interventional radiology procedures. This book has been written with several key objectives in mind: to provide physicians, technologists, nurses, and coding professionals with the most comprehensive resource dealing with the issues of coding interventional radiology procedures; to simplify access to the necessary information needed to successfully manage the coding process for interventional radiology procedures; and to provide an extensive full color pictorial review of the procedures and anatomy associated with interventional radiology procedures to assist in knowledge building and understanding. It is our hope you will find this book an essential addition to your professional reference library. BILLIG FOR PROFESSIOL SERVICES There are two types of bills used for medical procedure billing that we address: Uniform Billing Form (UB-) used for hospital billing and Uniform Billing Form used for physician billing. The two billing forms are very different, and the coding rules for the two may vary. When the rules for hospitals vary from the rules for physician billing, the difference in the two is explained. PROVIDER PYMET Provider payment is made based on the procedure codes assigned for the procedures performed. The Healthcare Common Procedure Coding System (HCPCS) is used, which has two levels of active codes: HCPCS Level I and HCPCS Level II. HCPCS Level I codes are the merican Medical ssociation's (M's) Current Procedural Terminology (CPT). CPT is further divided into three types of codes. Category I CPT codes describe procedures that are consistent with contemporary medical practice and are being performed by many physicians in clinical practice in multiple locations. Category II CPT codes describe clinical components that may be
2 included in an evaluation and management (E&M) service. They do not describe separately billable services, but are used for performance monitoring. Category III CPT codes describe procedures that are emerging technology that do not have the frequency of performance needed to be a Category I CPT code. They are for tracking purposes and may or may not be reimbursed. Category III CPT codes are usually active for up to five years, when the code is either dropped or a Category I CPT code is developed as a replacement code. Expiration dates are listed for all Category III codes in the CPT Codebook. The majority of procedures will be reported with Category I CPT codes. These codes are used to report the procedures performed and, in most instances, have payment based on the CPT code submitted. HCPCS Level II codes created by the Centers for Medicare and Medicaid Services (CMS) are alphanumeric codes that are used most often by physicians to bill for supplies. There are a few HCPCS Level II codes that describe physician procedures, while hospitals use HCPCS Level II codes for many procedures and supplies. The HCPCS coding system will be further discussed in Chapter 2. PYMET SYSTEMS Physician and hospital services are paid in a variety of ways. By far, the most common payment methodology for physicians is fee schedule based. Under fee schedule based payment, each procedure has a predetermined amount of payment established. Both the type of procedure and the frequency performed affect physician payment. Medicare uses this type of reimbursement schema for physicians and a hybrid form of this payment type for hospitals. However, hospital payment is advancing towards a system that pays by encounter instead of by the individual procedures performed. Payment for procedures that are considered device-dependent (over % of the payment is for the medical device, stent, generator, etc. utilized) has moved to an encounter-based payment for hospital outpatient services. nother payment method is a negotiated structure where the provider becomes a preferred provider organization (PPO). preferred provider agrees to accept discounted fees in exchange for the plan's enrollees being encouraged to seek the services of the provider. The enrollee pays a higher co-pay for services if a provider other than the preferred provider is seen. This is the method many commercial insurance companies employ. payment method that is seen mostly in some of the Medicaid programs is a case rate. ll services performed are bundled into the most intensive procedure (as defined by CPT coding), which is paid based on a fee schedule. The surgical CPT codes are grouped into categories for payment based on the type of procedure and resources utilized. They are normally grouped into nine or more payment categories. ll services, to include ancillary procedures, are grouped into the highest paying CPT code on the bill. These are termed mbulatory Surgery Center (SC) or mbulatory Payment Group (PG) procedures. There are other modes of payment; however, these three are the most prevalent. UDERSTDIG THE MEDICRE BILLIG PROCESS
3 Medicare rules and regulations are used as the source of information in this manual. While there are other payers besides Medicare, Medicare usually sets the rules that the other payers soon follow. In addition, Medicare has the most severe penalties for non-compliance. Understanding the methodology of Medicare payment provides a basis for understanding the rules and regulations related to coding. MEDICRE PYMET FOR PROVIDER SERVICES There are two types of Medicare coverage: Part covering hospital inpatient services and Part B covering hospital outpatient services and all physician services. Providers do not send bills for services performed on Medicare patients directly to CMS for reimbursement since CMS does not pay claims directly. Rather, CMS contracts with other insurance companies to manage the payment of claims, called Medicare dministrative Contractors (MCs). MCs are responsible for paying both Part and Part B claims in a region. Medicare coverage decisions come from two sources. CMS makes some coverage decisions and releases them as ational Coverage Decisions (CDs). Certain services such as routine care, cosmetic-only procedures, investigational procedures, and other procedures not meeting medical necessity are nationally non-covered. However, CMS leaves approximately 9% of coverage decisions up to the discretion of the MCs. The MCs often create Local Coverage Determinations (LCDs), defining coverage policy by specific procedure. Since there are different MCs in different regions of the country, the policies can vary from one area to another. Providers cannot assume that because one MC covers and pays for a service one way that other MCs will do the same. There has been a recent trend for different MCs to adopt the same LCD, so more consistency in coverage across the nation is occurring. MEDICRE COMPLICE Compliance with Medicare rules and regulations is crucial to having a successful practice. ll services that can be coded and billed separately must be identified for financial health. However, procedures that are not performed, not sufficiently documented, or are inherent in other procedures performed in the same setting cannot be coded. The penalties for non-compliance are severe and can result in catastrophic sanctions placed on the practice. This book focuses on information crucial to compliant coding for interventional radiology procedures. 2-2 ZHealth Publishing. ll rights reserved. CPT Only 27 merican Medical ssociation. ll rights reserved.
4 2 Coding Basics Pages: 7- Coding Instructions CODIG BSICS For payment to be accurate, coding must be accurate The basic building blocks of a bill are codes. Every procedure performed must be translated into a numeric or alphanumeric format. There are codes that indicate demographic information such as patient status, date of birth, medical record number, etc. ll procedures performed are converted into codes that are key to appropriate reimbursement. Three codes that are especially important to coders are: Diagnosis codes Procedure codes Modifiers Diagnosis information is translated into International Classification of Disease, th Revision, Clinical Modification (ICD--CM) codes. Without the appropriate code, payment will not be made. With an inappropriate code, the provider may be improperly reimbursed. The Medicare Contractor's Local Coverage Determinations (LCDs) should be frequently reviewed to determine covered diagnoses. Diagnosis coding is beyond the scope of this reference. PROCEDURE CODIG The procedure coding process currently in use began in 9, when the merican Medical ssociation (M) created the Current Procedural Terminology (CPT ) coding system for tracking statistics on procedures performed by physicians. When the Centers for Medicare and Medicaid Services (CMS) established a physician payment system based on coding, it contracted with the M to utilize the CPT coding system instead of creating its own. CMS, however, has little to no control of the CPT coding system. The M continues to hold the copyright. CMS holds one seat on the seventeen member CPT Editorial Panel that is responsible for updating the CPT coding system. However, CMS has the ability to determine how CPT codes can be used independent of the M. CMS can, and does, establish different coding guidelines from those promoted by the M. The M has changed code descriptions based on CMS interpretation. In addition, the M is now replacing the historical system of component codes with comprehensive codes that include all aspects of a procedure (e.g., surgical procedure, supervision and interpretation) in response to CMS requiring bundling of procedure codes that are reported together 7% of the time. The component coding system is slowly being phased out. Since CPT codes are for procedures performed by physicians, they do not cover the scope of services provided in a hospital setting. To meet this need, CMS created the Healthcare Common Procedure Coding System (HCPCS). HCPCS is currently comprised of two levels. Level I codes are equivalent to the M's CPT codes. Since CPT codes only describe physician services, a method was needed for providers to report procedures and items that are not covered by the CPT coding system. HCPCS Level II was created to solve this problem. HCPCS Level II codes are alphanumeric codes created by CMS for the billing of items not covered by CPT codes, such as dental procedures, supplies, drugs, mobile services, etc. They were also created for
5 procedures that CMS wants to separately track or pay for in a different manner. Iliac angiography at the time of cardiac catheterization (G27), sacroiliac joint injections (G29, G2), and closure device placement (G29) are a few commonly used examples. CODIG COVETIOS There are certain facts regarding coding and reimbursement that are important to understand. Fact umber : Just because a code exists doesn't mean it can be used. Because the CPT Codebook is not written by CMS, there are procedures and services that have codes that CMS does not recognize. These codes are assigned a status indicator (SI) in the physician and Hospital Outpatient Prospective Payment System (HOPPS) fee schedules, which indicates they are non-reportable. (Status indicator codes are discussed in detail in chapters and.) Fact umber 2: The CPT code submitted for a procedure must exactly match the service provided. If a code that accurately describes the procedure performed cannot be found, an unlisted CPT code must be used. Please refer to the following table for a limited list of unlisted CPT codes used for interventional radiology procedures. TBLE - COMMO ULISTED PROCEDURE CODES ULISTED DESCRIPTIO CODE 999 Unlisted procedure, breast 2999 Unlisted procedure, musculoskeletal system, general 2299 Unlisted procedure, spine 2999 Unlisted procedure, lungs and pleura 999 Unlisted procedure, cardiac surgery 299 Unlisted procedure, vascular injection 7799 Unlisted procedure, vascular procedure 799 Unlisted procedure, liver 7999 Unlisted procedure, biliary tract 9999 Unlisted procedure, abdomen, peritoneum and omentum 99 Unlisted procedure, urinary system 999 Unlisted procedure, nervous system PC TOTL RVU
6 79 Unlisted fluoroscopy procedure Unlisted CT procedure Unlisted magnetic resonance procedure Unlisted diagnostic radiology procedure Unlisted ultrasound procedure (eg, diagnostic, interventional) Unlisted cardiovascular service or procedure Unlisted non-invasive vascular diagnostic study. Fact umber : The most comprehensive procedure to describe the services provided must be reported. When multiple procedures are performed, and a CPT code describes all the components of the service, that code must be used instead of multiple component codes. For example, if a bilateral lower extremity angiogram is performed, you are not allowed to bill two unilateral procedures (77 x 2) since there is a bilateral description that is comprehensive of the two studies (77). When an abdominal aortogram (72) is performed, followed by selective visceral angiography (772), code 72 must not be billed, as the CPT description for 772 states "with or without aortography". The aortography is a bundled component of 772. Just because there is not a ational Correct Coding Initiative (CCI) edit between two codes, does not mean that it is appropriate to bill both. Close attention to the description of the code is critical to accurate coding. Fact umber : ew CPT codes are effective January unless notified elsewise. Every year the CPT Codebook is updated. The book is usually released in September preceeding the effective year. ew CPT codes are not reportable when released. CMS will notify providers the effective date for new codes. It is usually January. If the CMS contractors have not fully implemented software updates, payment of claims involving new codes is delayed until the software changes are finalized. CPT Level III codes are implemented twice a year, usually on January and July. CMS will communicate the implementation date. If CMS has not received the next year's CPT code changes early enough to perform rate-setting, the new codes will not be reportable. G-codes will be established to replace deleted codes in this instance. Fact umber : If a CPT code is reportable, that doesn't mean everyone can use it. CMS has definitive rules for some CPT codes including competancy standards and clinical efficacy monitoring. For example, code 72 (cervical carotid artery stent placement) can only be reported when performed in facilities that have been credentialed for it. To become credentialed, the physician and facility must meet specific criteria. Fact umber : Just because a CPT code has payment assigned in the fee schedule, doesn't guarantee it will be reimbursed. Coverage is not guaranteed for any code. Medical necessity must be met. The medical necessity criteria for a specific procedure can vary by region based on the
7 region's MC. In addition, site-of-service can affect whether a code is reimbursed. nd, in some cases, sex and age affect coverage. Fact umber 7: HCPCS Level II code does not always supercede a CPT (HCPCS Level I) code. Close attention to communication from CMS and the status indicators assigned to procedure codes is important. Some HCPCS Level II codes are only for hospital use and some are for other providers such as home health, durable medical equipment suppliers, imaging services for nursing homes, etc. Translating the CPT Codebook The most valuable characteristic of the CPT Codebook is that the codes are usually grouped by type of procedure. However, the M has run out of new codes in some ranges, and has started assigning them out of sequence. Codes that are out of sequence are identified in ppendix of the CPT Codebook. To assist in navigating the CPT Codebook, there is also an alphabetical index in the back that allows you to look up a procedure by name, which cross-walks to the procedure code(s). lways fully read the procedure code description and any explanations that accompany the code before utilizing any code. ever code just from the index. The book is laid out as follows: CODE RGE TYPE OF PROCEDURE nesthesia Integumentary SystemSurgery Musculoskeletal SystemSurgery Respiratory SystemSurgery Cardiovascular SystemSurgery Lymphatic SystemSurgery Mediastinum and Diaphragm Surgery Digestive System Surgery Genitourinary SystemSurgery - 99 Endocrine SystemSurgery ervous SystemSurgery Ocular SystemSurgery 999 Operating Microscope Radiology - 7U Laboratory and Pathology Medicine Evaluation & Management (Visits) 2T - T Category IIITemporary Codes The radiology section is further divided into Diagnostic RadiologyCTMRI (7-799), Ultrasound (7-7999), Radiologic Guidance ( ), Breast Procedures (77-777), BoneJoint Studies (777-77), Radiation Therapy ( ), and uclear Medicine ( ). Category III codes are for emerging technology, and new codes are released on January and July every year. They are implemented by Medicare six months later. The new codes can only be accessed on the M website, as they are not included in the CPT Codebook until the year after implementation. SYMBOLS
8 The CPT Codebook has guides to help quickly identify important items in the book. These guides should be used when the new book is received to assist in identifying what has changed from the previous year. There are symbols to indicate both a new code and a revised description to an existing code. ew Code Revised Code There are other symbols in the book that have specific indications. The + symbol indicates an add-on procedure. These procedures are not stand-alone procedures, but are always performed after something else. Code 777, ngiography, selective, each additional vessel studied after basic examination, radiological supervision and interpretation (List separately in addition to code for primary procedure), is an add-on procedure. This CPT code cannot be used until the basic exam it relates to has been performed. Many add-on codes have "each additional" in their description. The symbol is used to indicate modifier - should not be appended to the CPT code. Modifier - is used for physician billing to indicate additional procedures performed that are subject to multiple procedure discounting. PPEDIX B nother important resource when a new CPT Codebook is received is ppendix B. ppendix B lists all changes to the book to include additions, deletions, and description changes. For additions, you will still need to refer to the code section of the book since the ppendix does not provide the description of new codes. Revised codes show what has changed in the description, which is often very helpful in determining if its application has changed. The ppendix is the only quick way to identify codes that have been deleted. IDETED DESCRIPTIOS While reading CPT code descriptions, it is important to note descriptions that are indented from their respective code. The descriptions for these codes are comprised not only of the listed description, but also must include a portion of the description from the prior un-indented code. ll the verbiage that is listed to the left of the semicolon in the prior description must also be used in addition to the indented code. For example, when you see the following description: 7 Endovascular repair of descending thoracic aorta (e.g., aneurysm, pseudoaneurysm,
9 9 dissection, penetrating ulcer, intramural hematoma, or traumatic disruption); involving coverage of left subclavian artery origin, initial endoprosthesis plus descending thoracic aortic extension(s), if required, to level of celiac artery origin, radiological supervision and interpretation not involving coverage of left subclavian artery origin, initial endoprosthesis plus descending thoracic aortic extension(s), if required, to level of celiac artery origin, radiological supervision and interpretation The complete description for 797 is Endovascular repair of descending thoracic aorta (e.g., aneurysm, pseudoaneurysm, dissection, penetrating ulcer, intramural hematoma, or traumatic disruption); not involving coverage of left subclavian artery origin, initial endoprosthesis plus descending thoracic aortic extension(s), if required, to level of celiac artery origin, radiological supervision and interpretation. It is important to read and understand the complete description of the code before placing it on any bill. WITH OR WITHOUT ny code whose description indicates that it is "with or without" a particular procedure or service can be used in both instances. good example is CPT code 79, Venous sampling by catheter, with or without angiography, per organ sampled, radiological supervision and interpretation (RS&I). If you do venography and sampling, you report only code 79 for the RS&I. If you only perform sampling, you still report the same code (79). Venography is not reported separately with this terminology. SEPRTE PROCEDURE The narrative for many CPT codes includes a parenthetical statement that the procedure represents a "separate procedure". The inclusion of this statement indicates that the procedure, while possible to perform separately, is generally included in a more comprehensive procedure. The service is not to be billed when a related, more comprehensive service is performed. The "separate procedure" designation is used with codes in the surgery (-9999), radiology ( ), and medicine (9-9999) sections of the CPT Codebook. When a related procedure from the same section, subsection, category, or subcategory is performed, a code with the designation of "separate procedure" is not to be billed with the primary procedure. n example is fluoroscopy, code 7. n interventional RS&I procedure cannot be performed without fluoroscopy, so it is considered inherent in the RS&I procedure. Fluoroscopy is not to be coded and billed separately if performed with an RS&I procedure. On occasion, fluoroscopy is performed as a stand-alone radiology procedure, such as fluoroscopy used to reposition a central venous access catheter. In this instance it would be coded and billed separately. CODIG GUIDELIES
10 One of the best sources for understanding the use of each CPT code is the CPT ssistant newsletter, published by the M. CPT ssistant is published monthly and highlights a particular type of procedure and the proper coding. There is also a useful Q& section at the end of the newsletter that addresses specific coding questions. The Professional Edition of the CPT Codebook is annotated with CPT ssistant articles that have been published regarding each CPT code. There are two sources for reference regarding the use of HCPCS Level II codes. One is the CMS. When a Level II code is released, its announcement is usually accompanied by an explanation of why it was created. This may be communicated in a bulletin from the CMS or may be buried in the Federal Register. The CMS has appointed the merican Hospital ssociation (H) as the source hospitals should use for HCPCS coding advice. The H publishes a Coding Clinic for HCPCS newsletter dedicated to outpatient coding. Similar to CPT ssistant, it has articles followed by Q&s. Modifiers - The Second Key Component of HCPCS Coding The use of all the correct CPT codes and listing them appropriately on the bill is not always the end of the task. Often, the submitted bill will be returned or will contain line item denials. Sometimes denials are due to improperly using modifiers or, more likely, not including modifiers, which can be essential to accurate coding and reimbursement. modifier is a two-character code that is appended to a CPT code to either provide additional information or to indicate the procedure was performed under an unusual circumstance. Many modifiers have no effect on payment. There are key modifiers, however, that have a very significant effect on coding accuracy and payment. Please refer to the inside cover of the CPT Codebook for a list of all modifiers reportable for physician services and hospital outpatient services. Interventional Radiology Coding Reference will focus only on those modifiers most typically used with interventional radiology procedures and will detail their impact on coding and reimbursement. When reporting, the modifier that affects payment (the functional modifier) should be placed in the first modifier field. Informational modifiers should be placed in the subsequent modifier fields. For example, if a physician billed a CPT code with both the -22 (unusual procedural service) and the -LT (left) modifier, the -22 would be placed in the first modifier field and the -LT would be placed in the second modifier field. Please see the following table for a list of relevant modifiers. TBLE - COMMO MODIFIERS M O D I F I E R DESCRIPTIO USGE 2 Unusual Procedural Used when the service 2 Services provided is greater than what EFFECT O MEDICRE PYMET Individual consideration is given for additional payment,
11 2 2 2 Unrelated Evaluation and Management Service by the Same Physician During a Postoperative Period Significant, Separately Identifiable Evaluation and Management Service by the Same Physician on the Same Day of the Procedure or Other Service Professional Component is usually required for the listed procedure. This modifier is not reportable by hospitals for facility billing. Used to indicate that an evaluation and management service was performed during a post-operative period for a reason unrelated to the original procedure. This modifier only applies to billing for physician professional services. Used to indicate that on the day a procedure or service identified by a CPT code was performed, the patient's condition required a significant, separately identifiable E&M service above and beyond the usual preoperative and post-operative care associated with the procedure that was performed. This modifier is utilized by hospitals for clinic and emergency room visits that are accompanied by diagnostic procedures. Used to indicate that only the professional component of the procedure was performed. Used when a procedure is not performed in the physician office (e.g., performed in a hospital setting), so another provider is billing for the technical component. This modifier only applies to billing for physician professional services. Used for procedures Bilateral Procedure performed on paired organsanatomical sites. so a copy of the medical record will need to be provided to Medicare. llows payment for the E&M service when it would otherwise be bundled into the operative procedure that was previously performed. llows payment for an E&M service that would otherwise be bundled into the procedure payment. Payment is made for the professional component of the procedure instead of global payment. Physician payment varies based on the indicator in the Bilateral Surgery column of the ational Physician Fee Schedule Relative Value File (Physician RVU File). Hospital
12 2 Multiple Procedure Discounted Reduced Services Discontinued Procedure Surgical Care Only Postoperative Management Only Used to indicate separate procedures subject to discounting performed on the same patient at the same operative session or on the same day. It is not applicable to all CPT codes. This modifier is not reportable by hospitals for facility billing. Used only for a limited service that is not described by another CPT code. For hospitals, this modifier is also used to indicate a cancelled or reduced radiology procedure that did not require anesthesia. Used to indicate that a procedure could not be completed due to a medical reason. This modifier is not reportable by hospitals for facility billing. Used to indicate that the intraoperative portion and post-operative work while the patient was in the hospital was the only portion of the global package service provided by the physician. This modifier only applies to billing for physician professional services. Used to indicate that only the post-operative portion of the global package that is provided in the office after discharge from the hospital was provided by the physician. This modifier only applies to billing for physician professional services. payment is the same as if billing the two separately (may be subject to discounting or packaging depending on the status indicator assigned). For the procedures it applies to the st procedure (without modifier - appended) is paid at % and the 2 nd through th (with modifier - appended) at % of the Medicare fee schedule amount. % reduction in payment. Individual consideration is given for payment, so a copy of the medical record will need to be provided to Medicare. Payment varies based on the percentage of the global package indicated in the Intraoperative column of the Physician RVU File. Payment varies based on the percentage of the global package indicated in the Postoperative column of the Physician RVU File. Preoperative Used to indicate that only the Payment varies based on the
13 Management Only preoperative portion of the global package was provided by the physician. This modifier only applies to billing for physician professional services. 7 9 X E X P X S Decision for Surgery Staged or Related Procedure or Service by the Same Physician During the Postoperative Period Distinct Procedure Separate Encounter Separate Practitioner Separate Structure n E&M service that resulted in the initial decision to perform the surgery may be identified by adding modifier -7 to the E&M CPT code. This modifier only applies to billing for physician professional services. Used to indicate that the performance of a procedure or service during the post-operative period was (a) planned prospectively at the time of the original procedure; (b) more extensive than the original procedure; or (c) for therapy following a diagnostic surgical procedure. Since hospitals' global surgical period is only the day of the procedure, this modifier would typically not need to be reported by a hospital. Used to identify separate procedures performed that should not be subject to bundling. Used to identify a service that is distinct because it occurred during a separate encounter. This modifier is a subset of modifier -9. Used to identify a service that is distinct because it was performed by a different practitioner. This modifier is a subset of modifier -9. Used to identify a service that is distinct because it was performed on a separate organstructure. This modifier is a subset of modifier -9. percentage of the global package indicated in the Preoperative column of the Physician RVU File. llows separate payment for the E&M service on the day prior to or the day of major surgery. llows payment for a procedure that would otherwise be denied or payment reduced as being performed in the global surgery period. llows payment on a procedure that would otherwise be bundled. Effect on payment varies. Effect on payment varies. Effect on payment varies.
14 X U Unusual on-overlapping Service 2 Co-Surgeons Procedure Performed on Infants (Less than kg) Surgical Team Discontinued Outpatient Procedure Pre nesthesia Discontinued Outpatient Procedure Post nesthesia Repeat Procedure by Same Physician Used to identify a service that is distinct because it does not overlap usual components of the main service. This modifier is a subset of modifier -9. n example is a true diagnostic study performed in the same setting as an intervention. Used to indicate that a surgical procedure required two surgeons from different specialties. This modifier only applies to billing for physician professional services. Created for use with CPT codes to report the increased work involved with taking care of such small infants. This modifier only applies to billing for physician professional services. Used to indicate a single operative procedure that requires the skills of more than two surgeons from different specialties. This modifier only applies to billing for physician professional services. Used when the patient is present and procedure is cancelled due to medical reason(s) prior to administration of anesthesia. (Hospital OPPS reporting only) Used when the procedure is cancelled due to medical reason(s) after anesthesia has been administered or after the procedure has started. This modifier is also used to indicate that a procedure utilizing anesthesia was performed in a limited manner. (Hospital OPPS reporting only) Used when a patient has a procedure repeated by the Effect on payment varies. Payment for each physician is 2.% of the fee schedule amount allowed for the procedure. dd-on payment of up to 2% of the fee schedule amount for the procedure. Payment varies based on the indicator in the Team Surgery column of the Physician RVU File. Reimbursed at % of the procedure's PC rate. Reimbursed at % of the procedure's PC rate. llows payment for a duplicate submission of a CPT
15 Repeat Procedure by nother (Different) Physician Return to the Operating Room for a Related Procedure During the Postoperative Period Unrelated Procedure or Service by the Same Physician During the Postoperative Period ssistant Surgeon Minimum ssistant Surgeon ssistant Surgeon (When qualified resident surgeon not available) same physician that performed the first procedure that same day. It is only used when an identical CPT code is repeated. Used when a patient has a procedure repeated by a different physician from the one that performed the first procedure. It is only used when an identical CPT code is reported. Used to indicate the performance of another surgical procedure during the post-operative period that was related to the initial surgery. Used to indicate that the performance of a procedure during the post-operative period was unrelated to the initial surgery. Used to indicate that the physician was providing full assistance to the primary surgeon. This modifier only applies to billing for physician professional services. Used to indicate that the physician was providing minimum assistance to the primary surgeon. This modifier only applies to billing for physician professional services. This modifier is reported when there is no qualified resident surgeon available or when the services are performed in a teaching hospital that does not have an approved training program related to the medical code which might otherwise have been denied. llows payment on a procedure that would otherwise be considered a duplicate bill and not paid. The allowance will be reduced, since pre and post-operative care is included in the allowance for the prior surgical procedure. Since a hospital's global surgery period is only the day of the procedure, this modifier would rarely need to be reported by a hospital. Procedure is paid and a new global surgical period begins. Since a hospital's global surgery period is only the day of the procedure, this modifier would rarely need to be reported by a hospital. Payment varies based on the indicator in the ssistant at Surgery column of the Physician RVU File. Payment varies based on the indicator in the ssistant at Surgery column of the Physician RVU File. Payment varies based on the indicator in the ssistant at Surgery column of the Physician RVU File.
16 S 9 9 L T R T F X F Y G G X Physician ssistant (P), Clinical urse Specialist (CS), or urse Practitioner (P) Services for ssistant-at-surgery Multiple Modifiers Left Side Used Right Side Used X-ray Taken Using Film X-ray Taken Using Computed Radiography Technology Cassette-based Imaging otice of Liability Statement Issued as Required by Payer Policy otice of Liability Issued Voluntarily specialty required for the surgical procedure. This modifier only applies to physician professional services. Used to indicate the assistant was one of the designated providers instead of a physician. This modifier is not reportable by hospitals, unless they are billing for professional services (not the technical component). Used to indicate that there are more than four () modifiers to append to a CPT code on a billing form. This modifier only applies to billing for physician professional services. when only the left of a pair of organsanatomical sites is studied or treated. when only the right of a pair of organsanatomical sites is studied or treated. ppended to any procedure code describing an x-ray procedure when the image is captured on film instead of direct digital capture. ppended to any procedure code describing an x-ray procedure when the image is captured on a digital cassette-based imaging system. Used to indicate that an dvance Beneficiary otification (B) signed by the beneficiary was obtained because it is a payer requirement. Used to indicate that it is expected that Medicare will deny a service as not reasonable and necessary and an dvance Beneficiary otification (B) signed by Payment varies based on the indicator in the ssistant at Surgery column of the Physician RVU File. The effect on payment varies based on which modifier(s) would have been left off if only the four modifier fields on the claim form have been used. Effect on payment varies. Effect on payment varies. There is a 2% reduction in payment under HOPPS and a 2% reduction in the technical component of the physician fee schedule payment. There is a 7% reduction in payment under HOPPS and a 7% reduction in the technical component of the physician fee schedule payment. The beneficiary becomes responsible for payment for the service. The beneficiary is responsible for payment for the service.
17 G Y G Z K X S C P P B P C P P O Item or Service Statutorily Excluded or Does ot Meet the Definition of ny Medicare Benefit Item or Service Expected to Be Denied as ot Reasonable and ecessary Requirements Specified in the Medical Policy Have Been Met Medically ecessary Service or Supply Surgical or Other Invasive Procedure on Wrong Body Part Surgical or Other Invasive Procedure on Wrong Patient Wrong Surgery or Other Invasive Procedure on Patient on-excepted Service Provided at an Off-campus, Outpatient, Provider-based Department of a Hospital Excepted Service Provided at an Off-campus, Outpatient, the beneficiary is on file, even though not required for the type of procedure performed. Used to indicate that the item or service is statutorily non-covered or is not a Medicare benefit. Used to indicate that it is expected that Medicare will deny an item or service as not reasonable and necessary and an B signed by the beneficiary is not on file. Used when Medicare policy requires the provider to attest that there is documentation that the requirements of the Medicare coverage policy have been met. Used when Medicare requires documentation that the procedure meets medical necessity. Used when a procedure is performed on the wrong body part. Used when a procedure is performed on the wrong patient. Used when the wrong procedure is performed on a patient. ppend to procedure codes when billing the technical component of visits and procedures performed in an off-campus provider-based department of a hospital that was OT billing for covered outpatient provider department (OPD) services furnished prior to ovember 2, 2. ppend to procedure codes when billing the technical component of visits and The beneficiary is responsible for payment for the service. There is no payment, and the beneficiary may not be billed for the service. If not used when required, payment for the service will be denied for lack of medical necessity. Informational only. There will be no payment. There will be no payment. There will be no payment. Payment is made using the OPPS fee schedule with additional discounting to align the payment with that for the same service when reimbursed under the physician fee schedule. o effect on payment.
18 Q Q Provider-based Department of a Hospital Investigational Clinical Service Provided in a Clinical Research Study that is in an pproved Clinical Research Study Routine Clinical Service Provided in an pproved Clinical Research Study procedures performed in an off-campus provider-based department of a hospital that WS billing for covered outpatient provider department (OPD) services furnished prior to ovember 2, 2. Used for those items and services that are being investigated as an object within the study. Used for those items and services that are not part of the study, but are used for direct patient management within the study (e.g., blood tests, administration of chemotherapy). Payment for a service that would be non-covered, as it is considered investigational. Payment for a service that may otherwise be non-covered. The physician table of Relative Value Units (RVUs) provides information regarding modifier usage by CPT code for modifiers that affect reimbursement. There are several columns with codes that specify how a particular modifier appended to a code will be processed. The following is an example of the modifier section of the RVU file. It will be referenced in the following discussion on modifiers. 2 RVU File: H C P CS M O D DESCRIPTIO GLO B DYS PR E OP IT R OP Thoracic aortic graft 9.9. Endovasc taa repr incl subcl Insert endovasc prosth, taa Endovasc prosth, taa, add-on Place catheter in aorta Place catheter in artery ZZZ PO ST OP MUL T PRO C BILT SURG SST SUR G CO- SU RG TE M SUR G
19 Place catheter in artery Place catheter in artery Vascular surgery procedure Upper GI endoscopy with tube Transect artery, sinus XXX.. ZZZ.. YYY.... ZZZ.. Contrast x-ray of hip XXX T C Contrast x-ray of hip XXX... 2 Contrast x-ray of hip XXX... T C 2 T C 2 Ct angio abdominal arteries Ct angio abdominal arteries Ct angio abdominal arteries rtery x-rays, armleg rtery x-rays, armleg rtery x-rays, armleg rtery x-rays, armslegs XXX.. XXX.. XXX.. XXX.. XXX.. XXX.. XXX T rtery x-rays, XXX... 2
20 7 7 7 C armslegs 2 rtery x-rays, armslegs XXX... 2 MODIFIER 22 - UUSUL PROCEDURL SERVICES Modifier -22 is applicable only to those procedures codes for which the global surgery concept applies, whether the procedure code is surgical in nature or not. Supportive documentation (e.g., operative reports, progress notes, order sheets, pathology reports, etc.) must be submitted with the claim for the MC to determine if additional payment will be made. Modifier -22 will be removed by the MC when reported with procedures that do not have a global surgery period of,, or 9 days indicated in the "Global Days" column of the Physician RVU file. For example, radiologic S&I codes have XXX in the "Global Days" column, so modifier -22 cannot be appended to them. MODIFIER - BILTERL Modifier - represents that the procedure was performed bilaterally. To report bilateral services, bill the code with modifier - appended and a unit of one () in the daysunits fields. The billed charge should reflect a bilateral procedure amount. If a modifier - is appended to a procedure that is not eligible for bilateral payment, only one procedure will be reimbursed. It is important to know when its use is appropriate. Procedures that a - modifier may be appended to are identified in the Physician RVU file under the column titled "BILT SURG", with the following indicators: = % payment adjustment for bilateral procedures does not apply. If the procedure is reported with modifier - or with modifiers -RT and -LT, the payment for the two sides is the lower of: (a) the total actual charge for both sides, or (b) % of the fee schedule amount for a single code. Example: The physician fee schedule amount for code 2 is $2. The physician reports code 2-LT with an actual charge of $ and 2-RT with an actual charge of $. Payment will be based on the fee schedule amount ($2) since it is lower than the total actual charges for the left and right sides ($2). The bilateral adjustment is inappropriate for codes in this category because of: (a) physiology or anatomy, or (b) the code description specifically states that it is a unilateral procedure and there is an existing code for the bilateral procedure. = % payment adjustment for bilateral procedures applies. If the code is billed with the bilateral modifier or is reported twice on the same day by any other means (e.g., with -RT and -LT modifiers, or with a 2 in the units field), the payment is the lower of: (a) the total actual charge for both sides, or (b) % of the fee schedule amount for a single code. If the code is reported as a bilateral procedure and is reported with other procedure codes on the same day, the bilateral adjustment applies before application of any multiple procedure rules. 2 = % payment adjustment does not apply. RVUs are already based on the procedure being performed as a bilateral procedure. If the procedure is reported with modifier - or is reported twice on the same day by any other means (e.g.,
21 with -RT and -LT modifiers, or with a 2 in the units field), the payment is the lower of: (a) the total actual charge by the physician for both sides, or (b) % of the fee schedule for a single code. Example: The physician fee schedule amount for code 77 is $2. The physician reports code 77-LT with an actual charge of $ and 77-RT with an actual charge of $ or 77- with a $2 charge. Payment will be based on the fee schedule amount ($2) since it is lower than the total actual charges for the left and right sides ($2). The RVUs are based on a bilateral procedure because: (a) the code descriptor specifically states that the procedure is bilateral, (b) the code descriptor states that the procedure may be performed either unilaterally or bilaterally, or (c) the procedure is usually performed as a bilateral procedure. = The usual payment adjustment for bilateral procedures does not apply. If the procedure is reported with modifier - or is reported for both sides on the same day by any other means (e.g., with -RT and -LT modifiers, or with a 2 in the units field), the payment for each side or organ or site of a paired organ is the lower of: (a) the actual charge for each side, or (b) % of the fee schedule amount for each side. If the procedure is reported as a bilateral procedure and with other procedure codes on the same day, the fee schedule amount for a bilateral procedure will be calculated before applying any multiple procedure rules. Services in this category are generally radiology procedures or other diagnostic tests that are not subject to the special payment rules for other bilateral surgeries. 9 = Concept does not apply. Modifier - must not be used for: Procedures identified by their terminology as bilateral, such as 77 (bilateral extremity angiogram). Procedures identified by their terminology as unilateral or bilateral. There are currently no codes used in interventional radiology that have this terminology. Procedures assigned a 2 in the "BILT SURG" column of the physician RVU file. MODIFIER - MULTIPLE PROCEDURES Medicare recognizes a reduction in the cost and work effort for a procedure when it is an additional procedure performed during an operative session. system of discounting has been developed for these procedures to reflect the decreased cost. The - modifier is applied to the additional procedures to indicate they were performed in the same session and are subject to discounting. The definition of multiple surgeries is separate procedures performed by a single physician or physicians in the same group practice on the same patient during the same operative session or on the same day for which separate payment may be allowed. The surgery with the highest reimbursement is reported on line one without a - modifier and will be reimbursed at % of the fee schedule amount. The 2 nd to the th procedures are listed on subsequent lines with modifier - appended and will be reimbursed at % of the fee schedule amount. If the number of procedures exceeds five, an operative report of the entire session is required to be submitted to the MC for review and payment determination.
22 ote: While the MCs have been instructed by CMS to assign the multiple procedure modifier if appropriate based on the services billed, the provider should append modifier - when billing Medicare. Some of the other payers, however, do not want the provider to report modifier - on the claim form. Review your payer's guidelines to determine if it should be reported. ot all procedures are subject to multiple procedure discounting. Procedures that are indicated as add-on procedures, such as code 727, Transcatheter placement of an intravascular stent(s) (except lower extremity artery(s) for occlusive disease, cervical carotid, extracranial vertebral or intrathoracic carotid, intracranial, or coronary), open or percutaneous, including radiological supervision and interpretation and including all angioplasty within the same vessel, when performed; each additional artery (List separately in addition to code for primary procedure), are already discounted in the physician fee schedule and therefore are not subject to the multiple procedure discounting. Procedures subject to the - modifier and discounting are indicated on the Physician RVU File in column titled "MULT PROC". The indicator assigned to each code will be one of the following: = o payment adjustment rules for multiple procedures apply. If a procedure is reported on the same day as another procedure, the payment is based on the lower of: (a) the actual charge, or (b) the fee schedule amount for the procedure. = Standard payment adjustment rules in effect before January, 99 for multiple procedures apply. If procedure is reported on the same day as another procedure that has an indicator of, 2, or, the procedures are ranked by fee schedule amount, and the appropriate reduction is applied to this code (%, %, 2%, 2%, 2%, and by report). The payment is based on the lower of: (a) the actual charge, or (b) the fee schedule amount reduced by the appropriate percentage. 2 = Standard payment adjustment rules for multiple procedures apply. If a procedure is reported on the same day as another procedure with an indicator of, 2, or, the procedures are ranked by fee schedule amount, and the appropriate reduction is applied to this code (%, %, %, %, %, and by report). The payment is based on the lower of: (a) the actual charge, or (b) the fee schedule amount reduced by the appropriate percentage. = Special rules for multiple endoscopic procedures apply if procedure is billed with another endoscopy in the same family (e.g., another endoscopy that has the same base procedure). The base procedure for each code with this indicator is identified in the Endobase field of the file. The multiple endoscopy discount rules apply to a family before ranking the family with the other procedures performed on the same day (for example, if multiple endoscopies in the same family are reported on the same day as endoscopies in another family or on the same day as a non-endoscopic procedure). If an endoscopic procedure with intervention is reported with its base procedure, the base procedure is not paid separately. Payment for the base procedure is included in the payment for the other endoscopy. = Special rules for the technical and professional components of diagnostic imaging procedures apply if procedure is billed with another diagnostic imaging procedure in the same family. If procedure is reported in the same session on the same day as another procedure with the same family indicator, the procedures are ranked by fee schedule amount. For the technical component, % is paid for the highest priced procedure and % for each subsequent procedure. The payment for subsequent
23 procedures is based on the lower of: (a) the actual charge, or (b) the fee schedule amount reduced by the appropriate percentage. The professional component is paid at % for the first procedure and 7% for each subsequent procedure. = Special rules for the technical components of cardiovascular procedures apply if a procedure is billed with another cardiovascular procedure in the same family. 9 = Concept does not apply. MODIFIER 2 - REDUCED SERVICES For physician billing, use modifier -2 to identify that a service or procedure was partially reduced or eliminated at the physician's election. If a lesser procedure has been performed, bill the lesser procedure instead of using the modifier -2. If there is no procedure code that describes what was performed, append modifier -2 to the CPT code for the procedure that was attempted or planned. Claims with modifier -2 need to include documentation in the electronic notepad or Item 9 of the claim form explaining what services were rendered. Modifier -2 results in a % discount of the fee schedule amount for the procedure. For hospital billing, modifier -2 is used to indicate partial reduction or discontinuation of radiology procedures and other services that do not require anesthesia. For purposes of billing for services furnished in the hospital outpatient department, anesthesia is defined to include local, regional block(s), moderate sedationanalgesia ("conscious sedation"), deep sedationanalgesia, and general anesthesia. The elective cancellation of a procedure should not be reported. Modifier -2 is not utilized by hospitals with codes describing procedures that utilize anesthesia. Modifier -7 is used instead. Modifiers -7 and -7 are used by hospitals to indicate discontinued surgical and certain diagnostic procedures only. They are not used to indicate discontinued radiology procedures not requiring anesthesia. MODIFIER - DISCOTIUED PROCEDURE Under certain circumstances, the physician may elect to terminate a surgical or diagnostic procedure. Due to extenuating circumstances or those that threaten the well-being of the patient, it may be necessary to indicate that a surgical or diagnostic procedure was started, but discontinued. This modifier is not used to report the elective cancellation of a service prior to the patient's anesthesia induction andor surgical preparation in the operating suite. HCPCS codes with modifier - will be considered for payment if they are one of the following types of services: Physician services Surgery Radiation therapy nesthesia Hospitals cannot use modifier -. For hospital billing, use modifier -7. MODIFIERS & - SURGICL OR POST-OPERTIVE CRE OLY The surgical package includes the preoperative, surgical, and post-operative service. Specific billing guidelines must be followed when the surgical procedure and the post-operative care are split between different physicians for procedures that have a
24 or 9-day post-operative period. Modifiers - and - are used to indicate that the surgical care and post-operative management services are being rendered by two different physicians. The physician who is rendering the one-day preoperative care, the intraoperative services, and any in-hospital visits bills hisher services with the date of the surgery, the procedure code for the surgery, and a - modifier to indicate that the bill is reflective only of the surgical care. The physician rendering the post-operative, out-of-hospital care associated with a given surgical procedure should bill for hisher services with the date of the surgery, the procedure code for the surgery, and a - modifier. If the surgeon also cares for the patient for some period following discharge, the surgeon should bill the surgery with a - modifier and indicate the portion of the post-operative care provided in addition to the surgery by billing the surgical code with a - modifier appended. In those cases where the post-operative care is "split" between physicians, the billing for the post-operative care should be reported as follows: Report the date of service using the date of the surgical procedure. Report the procedure code for the surgical procedure, followed by modifier -. Report the range of dates that you provided the post-operative care in the procedure description (narrative) field on electronic claims and block 9 on the claim form. Each date does not need to be reported, only the range of dates. Both the surgeon and the physician(s) providing the post-operative care must keep a copy of the written transfer agreement in the beneficiary's medical records. Where the physicians agree on the transfer of care during the global period, the following modifiers are used:» - for surgical care only, or» - for post-operative management only. Both the bill for the surgical care only and the bill for the post-operative care only, will contain the same date of service and the same surgical procedure code, with the services distinguished by the use of the appropriate modifier. Providers need not specify on the claim that care has been transferred. However, the date on which care was relinquished or assumed, as applicable, must be shown on the claim. This should be indicated in the remarks fieldfree text segment on the claim formformat. Where a transfer of post-operative care occurs, the receiving physician cannot bill for any part of the global services until heshe has provided at least one service. Once the physician has seen the patient, that physician may bill for the period beginning with the date on which heshe assumes care of the patient. MODIFIER - STGED PROCEDURE BY THE SME PHYSICI DURIG THE POSTOPERTIVE PERIOD The physician may need to indicate that the performance of a procedure or service during the post-operative period was: (a) planned prospectively (staged) at the time of the original procedure, (b) more extensive than the original procedure, or (c) for therapy following a diagnostic surgery procedure. These circumstances may be reported by adding modifier - to the staged procedure. new post-operative period begins when the next procedure in the series is billed.
25 n example of when to use modifier - would be if a patient had a removal of a breast lesion (92) followed in less than 9 days by the simple removal of the entire breast. Code 9- would be used to report the mastectomy. This modifier is not used to report the treatment of an unexpected complication that requires a return to the operating room. (See modifier -7.) It would not be appropriate to report this modifier for codes that indicate in their terminology "one or more sessions", as the relative value units assigned to "one or more sessions" procedures represent the work for the total number of sessions necessary for completion of the procedure. Therefore, subsequent sessions performed within the global period of the initial surgery are included in the global fee. MODIFIER 9 - DISTICT PROCEDURE Modifier -9 is an important modifier, but one that requires careful use. It should be used when an otherwise bundled procedure was performed as a separate service. For example, when performing an aorto iliofemoral run-off angiogram (7) and a bilateral upper extremity angiogram (77), modifier -9 must be appended to code 77. Thebilateral extremity angiogram (77) is an CCI edit with 7, as a bilateral lower extremity angiogram is included in code 7. Since an upper extremity angiogram is separate and distinct, the use of modifier -9, or one of its subcategory modifiers, ensures the appropriate reimbursement for the upper extremity angiogram. This code and modifier combination should not be used if the legs instead of the arms were imaged. Modifier -9 is not intended to replace existing modifiers that indicate a separate site or session. The following modifiers indicate a separate site or session and will allow the service to be paid when used with the code for the lesser service: E - E (eyelids), F - F9 (fingers), F (left thumb), T (left great toe), T - T9 (toes), LT, RT, 2,, 7, 7, 79, LC, LD, RC, RI, LM. There are modifiers that are considered subcategories of modifier -9. Modifiers -XE, -XP, -XS, and XU are used to designate specific situations when an CCI edit should be bypassed. There has been very little information regarding the use of these modifiers other than what their titles relay (see specific section regarding these modifiers). Do not append both modifier -9 and one of the sub-modifiers to a code. sub-modifier replaces modifier -9. Modifier -9 should only be used if no other listed modifier is appropriate; however, some combinations will not be effective. Example: comprehensive code is reported with bilateral modifier -, and the component code is reported with an -RT or -LT modifier. The two modifiers will be regarded as contradictory statements, and the component code will bundle into the comprehensive code. Do not use modifier -9 to: Receive reimbursement on a bundled procedure such as an abdominal aortogramperformed with renal angiography. The aortogram is included in the renal angiography, and modifier -9 should not be appended to it to receive separate payment. Receive reimbursement for additional imaging that is follow-up to most interventions, such as routine leg imaging following femoral angioplasty.
26 MODIFIER XE - SEPRTE ECOUTER, SERVICE THT IS DISTICT BECUSE IT OCCURRED DURIG SEPRTE ECOUTER Modifier -XE is a subset of modifier -9. It is used to indicate a procedure should be reported separately with another procedure that it would typically bundle into because it was performed in a separate encounter. Modifier -7 is used if the same procedure code is reported. Modifier -XE is used when a procedure is performed that is an CCI edit with a procedure performed in a different session (a different CPT code). MODIFIER XP - SEPRTE PRCTITIOER, SERVICE THT IS DISTICT BECUSE IT WS PERFORMED BY DIFFERET PRCTITIOER Modifier -XP is a subset of modifier -9. It is used to indicate a procedure should be reported separately with another procedure that it would typically bundle into because it was performed by a different practitioner (physician, nurse practitioner, etc.). One MC (WPS) has stated that this modifier is used when two physicians with the same specialty in the same group practice perform procedures subject to CCI edits. MODIFIER XS - SEPRTE STRUCTURE, SERVICE THT IS DISTICT BECUSE IT WS PERFORMED O SEPRTE ORGSTRUCTURE Modifier -XS is a subset of modifier -9. It is used to indicate a procedure should be reported separately with another procedure that it would typically bundle into because it was performed on a separate site. It may be used to bypass CCI edits for procedures such as selective catheter placements in different vascular families, angioplasty in one vessel and stent placement in another vessel, intracranial angiography on one side and cervical carotid angiography on the other side, etc. Modifiers -LT and -RT may also explain the relationship between the codes and bypass an edit. MODIFIER XU - UUSUL O-OVERLPPIG SERVICE THT IS DISTICT BECUSE IT DOES OT OVERLP USUL COMPOETS OF THE MI SERVICE Modifier -XU is a subset of modifier -9. It can be used to indicate a diagnostic procedure was distinct from an interventional procedure on the same date of service, if it is not a repeat or guiding study. MODIFIER 2 - CO-SURGEOS Under some circumstances, the individual skills of two surgeons are required to perform surgery on the same patient during the same operative session. This may be required because of the complex nature of the procedure(s) andor the patient's condition. In these cases, the additional physician is not acting as an assistant-at surgery. Co-surgery refers to a single surgical procedure that requires the skill of two surgeons of different specialties performing parts of the same procedure simultaneously (e.g., heart transplant or endovascular aortic aneurysm repair). It is not always co-surgery when two doctors perform surgery on the same patient during the same operative session. Co-surgery has been performed if the procedure(s)
27 performed is (are) part of and would be billed under the same surgical code [e.g., placement of an aortic aneurysm stent graft (CPT code 7) by a vascular surgeon and an interventional radiologist]. In this case, each physician reports code 7 with the -2 modifier (two surgeons). Payment for each surgeon is 2.% of the Medicare fee schedule amount. Procedures that a -2 modifier may be appended to are identified in the Physician RVU file under the column titled "CO-SURG", with the following indicators: = Co-surgeons not permitted for this procedure. = Co-surgeons could be paid, though supporting documentation is required to establish the medical necessity of two surgeons for the procedure. 2 = Co-surgeons permitted and no documentation required if the two-specialty requirement is met. 9 = Concept does not apply. MODIFIER - PROCEDURE PERFORMED O IFTS Modifier - was created to describe the significant increase in physician work and complexity related to invasive surgery on neonates and infants up to a present body weight of kg (. pounds). There is more work and complexity due to temperature control, obtaining IV access, maintenance of hemostasis, etc. Modifier - is not intended to be used with the following CPT sections: Evaluation and Management, nesthesia, Radiology, PathologyLaboratory, or the Medicine section. ppendix F of the CPT Codebook contains a list of additional CPT codes to which modifier - cannot be appended. Modifier - is administered in the same manner as modifier -22. Documentation that supports the use of the modifier will be required, and if supported, there will be additional reimbursement of 2% to the maximum allowed. Multiple procedure reductions apply. Both modifiers - and -22 will not be valid for the same procedure code. MODIFIER - SURGICL TEM Team surgery also applies to a single procedure; however, it requires the skills of more than two surgeons of different specialties, working together to carry out various portions of a complicated surgical procedure. For example, a kidney transplant could involve the services of a transplant surgeon, urologist, and vascular surgeon to remove the diseased kidney, implant the donated kidney, and transplant the ureter. Each surgeon should bill using the procedure code for the procedure the team performed together, using modifier - attached to the procedure code. Payment for codes defined as eligible for team surgery will be reimbursed on an individual consideration basis. The reimbursement is % of the fee schedule for each procedure. Procedures that a - modifier may be appended to are identified in the Physician RVU file under the column titled "TEM SURG", with the following indicators: = Team surgeons not permitted for this procedure. = Team surgeons could be paid, though supporting documentation required to establish medical necessity of a team; pay by report. 2 = Team surgeons permitted; pay by report. 9 = Concept does not apply.
28 MODIFIER 7 - DISCOTIUED OUTPTIET PROCEDURE PRIOR TO ESTHESI DMIISTRTIO Modifier -7 is used when an outpatient procedure has been terminated after a patient has been prepared for surgery (including sedation when provided) and taken to the room where the procedure is to be performed, but before the induction of anesthesia (e.g., local, regional block(s), or general anesthesia). The procedure must be discontinued for medical reasons not for the convenience of the patient or the provider. This modifier is for hospital outpatient use only. It cannot be used for physician billing. It is used by hospitals in place of modifier -. When this modifier is used, CMS will remove the amount of the PC payment attributable to the medical device, if it is a device-intensive procedure. The remainder of payment will then be reduced by %. MODIFIER 7 - DISCOTIUEDLIMITED OUTPTIET PROCEDURE FTER ESTHESI DMIISTRTIO Modifier -7 is used when an outpatient procedure has been terminated or reduced after the induction of anesthesia (e.g., local, regional block(s), or general anesthesia) or after the procedure was started (e.g., incision made, catheter inserted, biopsy pass attempted). The procedure must be discontinued for medical reasons not for the convenience of the patient or the provider. Modifier -7 is also used to indicate a procedure is performed in a limited manner. This modifier is for hospital outpatient use only. It cannot be used for physician billing. It is used by hospitals in place of modifier -2. Payment will be at % of the PC rate when this modifier is used. If a lesser procedure has been performed, report the lesser procedure instead of the planned procedure. MODIFIER 7 - REPET PROCEDURE OR SERVICE BY SME PHYSICI OR OTHER QULIFIED HELTH CRE PROFESSIOL Modifier -7 has changed usage over the last few years, and different instructions have been published by different MCs. Many of the Part B MCs have stated that modifier -7 is used when the same procedure code is reported more than once during the same session when the procedure cannot be "quantity billed" (billed on one line item with multiple units of service). Some Medicare Contractors publish a list of codes that can be quantity billed on their websites. Knowledge of the Medically Unlikely Edits (MUEs) is also necessary in determining the ability to quantity bill, as the lists of codes that can be quantity billed on the MC websites do not take into consideration the MUE assigned to each. The first procedure code is billed without modifier -7. The additional instances of the code are reported on one line item with modifier -7 appended to the code and the units of service equal to the number of times the procedure described by the code was repeated. It may also be necessary to indicate, in Loop 22 TE segment for electronic claims or in item 9 of the CMS claim form, the number of services performed that day to still avoid "duplicate denials". Modifier -7 is not used in place of bilateral or -RT and -LT modifiers when these anatomical modifiers can be used to explain why a procedure code was repeated. ote that non-medicare payers and some Part B MCs may not want modifier -7 used when the procedures are performed in the same session.
29 They may follow the initial intent of modifier -7 which is to use when a procedure is repeated in a separate session. In addition, the M states that modifier -7 is used only when a procedure is repeated on the same date of service. Some non-medicare payers have extended that to within 2 hours of the first procedure. Hospitals have not been instructed to use a -7 modifier for duplicate codes in the same session. -7 modifier does not bypass an CCI edit, so do not use it when edits are involved. Modifier -7 does not change reimbursement. Multiple procedure discounting is in effect when a -7 modifier is appended when the code is subject to multiple procedure discounting. MODIFIER 77 - REPET PROCEDURE OR SERVICE BY OTHER PHYSICI OR OTHER QULIFIED HELTH CRE PROFESSIOL Modifier -77 is similar to modifier -7, as it indicates a procedure code was repeated on the same date of service. It indicates that a different physician than the one that performed the initial procedure repeated the procedure. Physicians in the same group practice with the same specialty are considered the same physician when reporting repeat procedures. MODIFIER 7 - RELTED PROCEDURE PERFORMED DURIG POST-OPERTIVE PERIOD The physician may need to indicate that another procedure was performed during the post-operative period from an initial procedure. When the subsequent procedure is related to the first and requires the use of the operating room, it may be reported by adding the -7 modifier to the related procedure. When treatment for complications requires a return trip to the operating room, physicians must bill the CPT code that describes the procedure(s) performed during the return trip. n operating room for this purpose is defined as a place of service specifically equipped and staffed for the sole purpose of performing procedures. The term includes a cardiac catheterization suite, a laser suite, and an endoscopy suite. It does not include a patient's room, minor treatment room, recovery room, or intensive care unit (unless the patient's condition was so critical there would be insufficient time for transportation to an operating room). Example of appropriate use of modifier -7: Patient has an endovascular repair of an using an aorto-uni-iliac endograft (7). Within the 9-day global period, surveillance reveals a type I endoleak at the left iliac attachment site. The patient is readmitted and has an extension prosthesis placed at the endoleak site. This procedure would be reported with code 7-7. Modifier -7 should not be used for services outside the global surgery period. Modifier -7 should not be used when a more extensive procedure is performed. Modifier - should be utilized when a more complex procedure is performed in the post-operative period of a less complex procedure. Modifier -7 is utilized when the disease process progresses and a related procedure is required. The payment is reduced when a -7 modifier is used to reflect the inclusion of the preoperative and post-operative activities in the global surgery package for the initial procedure.
30 Modifier -7 is not applied to any procedures with XXX as their global surgery indicator. It is applied to procedures with,, 9, YYY, or ZZZ global surgery indicators. MODIFIER 79 - URELTED PROCEDURE BY THE SME PHYSICI DURIG THE POSTOPERTIVE PERIOD The physician may need to indicate that the performance of a procedure or service during the post-operative period was unrelated to the original procedure. This circumstance may be reported by using modifier -79. new post-operative global surgery period will begin with this procedure. Example of appropriate use of modifier -79: Patient has an endovascular repair of an using an aorto-uni-iliac endograft (7). Within the 9-day global period, the patient develops deep vein thrombosis (DVT), and an IVC filter is placed. This procedure should be reported with Modifier -79 should not be used for services outside the global surgery period. It is not appended to codes assigned an XXX global surgery indicator. The payment for the procedure will not be reduced, as it is unrelated to the initial procedure. MODIFIERS,, 2, & S - SSISTT SURGEO Medicare will make payment for an assistant-at-surgery when the procedure is covered for an assistant and either of the following situations exists: The person reporting the service is a physician, or The person bears the designation of physician assistant (P), nurse practitioner (P), nurse midwife (M), or clinical nurse specialist (CS). o one else can receive Medicare reimbursement. If the person who assists at surgery is a surgical technician, first surgical assistant, scrub nurse, or bears any title other than those listed, Medicare will not reimburse for the assistant, and the provider may not bill the patient. Procedures that are covered for assistant-at-surgery are identified in the Physician RVU file under the column titled "SST SURG", with the following indicators: = Payment restriction for assistants-at-surgery applies to this procedure unless supporting documentation is submitted to establish medical necessity. = Statutory payment restriction for assistants-at-surgery applies to this procedure. ssistant-at-surgery may not be paid. 2 = Payment restriction for assistants-at-surgery does not apply to this procedure. ssistant-at-surgery may be paid. 9 = Concept does not apply. When paid, the payment for a physician assistant is % of the physician fee schedule. Payment for a P, M, or CS assistant is % of the % of the physician fee schedule (.%). MODIFIERS LT D RT - LEFT SIDE & RIGHT SIDE The -LT and -RT modifiers apply to codes that can be performed on paired organs or paired anatomical sites whenever only one side is performed. Do not use -LT and -RT when surgical procedures involving both organs or sides are performed; use modifier - instead. Modifiers -LT and -RT may affect payment. However, if appended to
31 catheter placements above the diaphragm, an -XS or -9 modifier still needs to be appended to the lesser selective code. For example, if left common carotid and right common carotid arteries were catheterized, they may be reported with 2-RT and 2-9LT (the -LT and -RT modifiers do not have an effect, as these CPT codes are not considered unilateral codes; modifier -XS will most likely replace modifier -9 in this scenario). The claim form allows up to four modifiers per HCPCS code. lways append the modifier that affects payment first, followed by informational modifiers. Payers may vary state to state and insurance company to insurance company, so check local policies when applying modifiers. Some payers do not want the -LT or -RT modifiers on their claims. MODIFIER FX - X-RY TKE USIG FILM Modifier -FX must be appended to any CPT code that includes the technical component of an x-ray procedure when film is used to capture the images. This includes outpatient hospital billing of all x-rays and physician billing of the global and technical (modifier -TC) components. It does not apply to physician billing for the interpretation of the x-ray procedure. Medicare will reduce the payment for the technical component by 2% when modifier -FX is appended. MODIFIER FY - X-RY TKE USIG COMPUTED RDIOGRPHY TECHOLOGYCSSETTE-BSED IMGIG Modifier -FY is new in 2 and must be appended to any CPT code that includes the technical component of an x-ray procedure when computed radiography is used to capture the images ("cassette-based imaging, which utilizes an imaging plate to create the image involved"). This includes outpatient hospital billing of all x-rays and physician billing of the global and technical (modifier -TC) components. It does not apply to physician billing for the interpretation of the x-ray procedure. Payment will be reduced 7% in calendar years 2 through 222 and % in 22. MODIFIER G - OTICE OF LIBILITY OBTIED S REQUIRED BY PYER Modifier -G should be used to report that a required dvanced Beneficiary otice (B) was issued for a service. n B is required when the procedure is expected to be denied for reasons other than statutory non-coverage (e.g., the service will not meet the reasonable and necessary standard). Charges should be listed as covered on the claim. The Medicare system may deny payment for codes appended with modifier -G and make the patient responsible for payment (rather than subjecting them to possible medical review). The patient has the right to appeal this determination. MODIFIER GX - OTICE OF LIBILITY OBTIED VOLUTRILY Modifier -GX should be used to report that a voluntary B was issued for a service. Procedures that are statutorily non-covered (i.e., cosmetic-only procedures, most screening procedures, etc.) are automatically the patient's responsibility to pay. The provider is not required to notify the patient that the procedure is not a benefit as the patient is expected to know the scope of their Medicare coverage. However, many providers want to notify the patient that they will be expected to pay and have the patient sign an B agreeing to pay. The -GX modifier is used to notify Medicare
32 that a notice of liability regarding services excluded from Medicare coverage by statute was voluntarily provided to, and signed by, the patient. The -GX modifier must be submitted with non-covered charges only. Medicare will automatically deny the claim as a patient liability. MODIFIER GY - ITEM OR SERVICE STTUTORILY EXCLUDED OR DOES OT MEET THE DEFIITIO OF Y MEDICRE BEEFIT The -GY modifier must be used to indicate that the item or service being billed is statutorily non-covered or is not a Medicare benefit. The -GY modifier is used: When it is expected a claim will be denied because it is not a Medicare benefit or because Medicare law specifically excludes it. When it is expected a claim will be denied because the service does not meet all the requirements of the definition of a benefit in Medicare law. To obtain a denied Medicare claim for secondary payer purposes. The MC may "auto-deny" claims with the -GY modifier. This action may be quicker than if a -GY modifier is not used. The beneficiary will be liable for all charges, whether personally or through other insurance. If Medicare pays the claim, the -GY modifier is irrelevant. The -GY modifier applies to the so-called "statutory exclusions" or "categorical exclusions" and the "technical denials". For example: Routine physicals, laboratory tests in absence of signs or symptoms, hearing aids, air conditioners, services in a foreign country, services to a family member. Surgery performed by a physician not licensed to perform surgery in that state. There are no B requirements for statutory exclusions. MODIFIER GZ - ITEM OR SERVICE EXPECTED TO BE DEIED S OT RESOBLE D ECESSRY The -GZ modifier should be used to indicate that Medicare is expected to deny an item or service as not reasonable and necessary and the patient has not signed an B. The -GZ modifier is used: When a service is expected to be denied because it does not meet Medicare program standards for medically necessary care and a signed B was not obtained from the beneficiary. When an B was given to a patient who refused to sign the B and, nevertheless, the services were furnished. When an B would have been given to a patient but could not because of an emergency care situation (e.g., in an EMTL covered situation in an emergency room or in an ambulance transport). When a patient was not personally present at the lab and could not be reached to timely sign an B (e.g., before a specimen is tested). When it is realized too late, only after furnishing a service, that the patient should have been given an B.
33 The claim will be reviewed by Medicare like any other claim and may or may not be denied. The MC will not use the presence of the -GZ modifier to influence its determination of Medicare coverage and payment of the service. If Medicare pays the claim, the -GZ modifier is irrelevant. If the claim is denied, the beneficiary generally will not be liable to pay the provider for the service. However, even though the beneficiary is found not liable, if the provider is also found not liable with respect to an unassigned claim or an assigned claim denied for one of the Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) technical denial reasons specified, the provider may be allowed to collect from the beneficiary. Medicare may or may not hold the provider liable depending whether or not the provider knew that payment would be denied when they furnished the service. In cases where the provider gave an B to the patient (or attempted to) but could not obtain a beneficiary signature, Medicare will most likely hold the provider liable and unable to collect from the beneficiary. MODIFIER KX - REQUIREMETS SPECIFIED I THE MEDICL POLICY HVE BEE MET When performing procedures that may or may not be covered based on how they are done or the documentation that the provider has to indicate to Medicare that the requirements have been met for coverage, the -KX modifier is appended to the procedure. For example, MRI is not covered when performed on a patient with a pacemaker, unless the pacemaker is approved for use in an MRI environment. Medicare may automatically deny the MRI charge when the diagnosis code for presence of cardiac pacemaker (Z9.) is on the claim. ppending the -KX modifier to the MRI procedure codes indicates that the pacemaker is approved for use in an MRI environment. MODIFIER SC - MEDICLLY ECESSRY SERVICE OR SUPPLY Modifier -SC is rarely used and should not be appended unless the service meets coverage criteria. For specialty procedure billing, at this time, only one MC has given instructions to use modifier -SC, and it is when reporting pacemaker procedures. Single and dual chamber pacemakers are only covered for two indications:. Documented non-reversible symptomatic bradycardia due to sinus node dysfunction, and 2. Documented non-reversible symptomatic bradycardia due to second degree andor third degree atrioventricular block. Hospitals are required to append modifier -KX to the pacemaker procedure codes to attest that the patient has one of these conditions. There are instances, however, when the pacemaker codes may be used and the patient doesn't meet one of these criteria (e.g., a generator and lead replacement or implantation of a biventricular device). oridian Healthcare Solutions has instructed that its providers should append an -SC modifier when the procedure should be covered but doesn't meet the above criteria. Examples provided for its use in the oridian article are cardiac resynchronization therapy; obstructive hypertrophic cardiomyopathy; pacing in children, adolescents, and patients with congenital heart disease; pacemaker or
34 generator replacements; and sustained pause-dependent ventricular tachycardia, with or without QT prolongation. MODIFIER P - SURGICL OR OTHER IVSIVE PROCEDURE O WROG BODY PRT Medicare does not reimburse a surgical or other invasive procedure when the procedure is performed on the wrong body part. Medicare will also not cover hospitalizations and other services related to this non-covered procedure. However, related services do not include performance of the correct procedure. The following are CMS guidelines regarding wrong body part procedure errors: ll services provided in the operating room when an error occurs are considered related and therefore not covered. ll providers in the operating room when the error occurs, who could bill individually for their services, are not eligible for payment. ll related services provided during the same hospitalization in which the error occurred are not covered. Following hospital discharge, any reasonable and necessary services are covered, regardless of whether they are or are not related to the surgical error. This policy includes all procedures described by the codes in the surgery section of CPT and other invasive procedures such as percutaneous transluminal angioplasty and cardiac catheterization. It includes minimally invasive procedures involving biopsies or placement of probes or catheters requiring the entry into a body cavity through a needle or trocar. It does not include use of instruments such as otoscopes for examinations or very minor procedures such as drawing blood. surgical or other invasive procedures is considered to have been performed on the wrong body part if it is not consistent with the correctly documented informed consent for that patient including surgery on the right body part, but on the wrong location on the body; for example, left versus right (appendages andor organs), or at the wrong level (spine). OTE: Emergent situations that occur in the course of surgery andor whose exigency precludes obtaining informed consent are not considered erroneous under this policy. lso, the policy is not intended to capture changes in the plan upon surgical entry into the patient due to the discovery of pathology in close proximity to the intended site when the risk of a second surgery outweighs the benefit of patient consultation; or the discovery of an unusual physical configuration (e.g., adhesions, spine levelextra vertebrae). MODIFIER PB - SURGICL OR OTHER IVSIVE PROCEDURE O WROG PTIET Medicare does not reimburse a surgical or other invasive procedure when the procedure is performed on the wrong patient. Medicare will also not cover hospitalizations and other services related to this non-covered procedure. The following are CMS guidelines regarding wrong patient procedure errors: ll services provided in the operating room when an error occurs are considered related and therefore not covered. ll providers in the operating room when the error occurs, who could bill individually for their services, are not eligible for payment.
35 ll related services provided during the same hospitalization in which the error occurred are not covered. Following hospital discharge, any reasonable and necessary services are covered, regardless of whether they are or are not related to the surgical error. This policy includes all procedures described by the codes in the surgery section of the CPT Codebook and other invasive procedures such as percutaneous transluminal angioplasty and cardiac catheterization. It includes minimally invasive procedures involving biopsies or placement of probes or catheters requiring the entry into a body cavity through a needle or trocar. It does not include use of instruments such as otoscopes for examinations or very minor procedures such as drawing blood. surgical or other invasive procedure is considered to have been performed on the wrong patient if that procedure is not consistent with the correctly documented informed consent for that patient. MODIFIER PC - WROG SURGERY OR OTHER IVSIVE PROCEDURE O PTIET Medicare does not reimburse a surgical or other invasive procedure when the wrong procedure is performed. Medicare will also not cover hospitalizations and other services related to this non-covered procedure. The following are CMS guidelines regarding wrong procedure errors: ll services provided in the operating room when an error occurs are considered related and therefore not covered. ll providers in the operating room when the error occurs, who could bill individually for their services, are not eligible for payment. ll related services provided during the same hospitalization in which the error occurred are not covered. Following hospital discharge, any reasonable and necessary services are covered, regardless of whether they are or are not related to the surgical error. This policy includes all procedures described by the codes in the surgery section of the CPT Codebook and other invasive procedures such as percutaneous transluminal angioplasty and cardiac catheterization. It includes minimally invasive procedures involving biopsies or placement of probes or catheters requiring the entry into a body cavity through a needle or trocar. It does not include use of instruments such as otoscopes for examinations or very minor procedures such as drawing blood. surgical or other invasive procedure is considered to be the wrong procedure if it is not consistent with the correctly document informed consent for that patient. MODIFIER P - O-EXCEPTED SERVICE PROVIDED T OFF-CMPUS, OUTPTIET, PROVIDER-BSED DEPRTMET OF HOSPITL Modifier -P is appended to the code for the technical component of non-excepted services and procedures performed in an off-campus provider-based department of a hospital. on-excepted services include all services except those performed at hospital remote locations, satellite facilities, and emergency departments. Excepted services are items and services furnished after January, 27: By a dedicated emergency department;
36 By an off-campus PBD that was billing for covered outpatient provider department (OPD) services furnished prior to ovember 2, 2, [i.e., the date of enactment of section of the Bipartisan Budget ct of 2 (Section )] that has not impermissibly relocated or changed ownership (see modifier -PO); By an off-campus PBD that qualifies for an exception under section or 2 of the 2st Century Cures ct*; or In a PBD that is "on the campus", or within 2 yards, of the hospital or a remote location of the hospital. Payment for services reported with a -P modifier will result in a new payment methodology for the technical component. The new fee schedule combines some of the bundling concepts of the OPPS with the payment to physicians for procedures performed in a non-facility (office) setting. In 2, the technical payment is made at % of the OPPS payment amount that would be paid for outpatient from hospital procedures. The professional component will be paid under the existing physician fee schedule. MODIFIER PO - SERVICES, PROCEDURES, DOR SURGERIES PROVIDED T OFF-CMPUS PROVIDER-BSED OUTPTIET DEPRTMETS Modifier -PO is used, instead of modifier -P, for off-campus provider-based outpatient departments that submitted attestations to Medicare of their creation prior to December 2, 2. They are excepted and continue to be paid under the HOPPS payment methodology. The same services are excepted from the use of the -PO modifier as are excepted from the -P modifier: By a dedicated emergency department; By an off-campus PBD that was billing for covered outpatient provider department (OPD) services furnished prior to ovember 2, 2, [i.e., the date of enactment of section of the Bipartisan Budget ct of 2 (Section )] that has not impermissibly relocated or changed ownership; or In a PBD that is "on the campus", or within 2 yards, of the hospital or a remote location of the hospital. The -PO modifier is never reported by a dedicated hospital emergency room. Both the -PO and -P modifiers would never be reported on the same claim line. However, if services reported on a claim reflect items and services furnished from both an excepted and a nonexcepted off-campus PBD of the hospital, the -PO modifier should be used for the excepted department claim lines, and the -P modifier should be used for the non-excepted department claim lines. MODIFIER Q - IVESTIGTIOL CLIICL SERVICE PROVIDED I CLIICL RESERCH STUDY THT IS PPROVED CLIICL RESERCH STUDY Investigational clinical services are defined as those items and services that are being investigated as an object within the study. Investigational clinical services may include items or services that are approved, unapproved, or otherwise covered (or non-covered under Medicare). Modifier -Q should be appended to procedures that are investigational but part of a clinical study, such as implantation of a
37 cardio-defibrillator for prevention of sudden death. If the patient is not enrolled in a clinical study, the procedure is non-covered by Medicare, and the -Q modifier should not be appended. Data should be submitted to the data collection agency prior to billing Medicare. MODIFIER Q - ROUTIE CLIICL SERVICE PROVIDED I CLIICL RESERCH STUDY THT IS PPROVED CLIICL RESERCH STUDY Routine clinical services are defined as those items and services that are covered for Medicare beneficiaries outside of the clinical research study; are used for the direct patient management within the study; and, do not meet the definition of investigational clinical services. Routine clinical services may include items or services required solely for the provision of the investigational clinical services (e.g., administration of a chemotherapeutic agent); clinically appropriate monitoring, whether or not required by the investigational clinical service (e.g., blood tests to measure tumor markers); and items or services required for the prevention, diagnosis, or treatment of research related adverse events (e.g., blood levels of various parameters to measure kidney function). Edits While the procedures performed and additional services provided are described by codes, the assignment and billing of the codes doesn't assure appropriate payment or any payment at all. There are coding rules in effect that must be followed, as well as edits to assure many of the rules are followed. The ational Correct Coding Initiative (CCI) edits are encountered when billing Medicare and other payers and can result in line item or total claim denial. TIOL CORRECT CODIG IITITIVE (CCI) The CCI is a system of billing edits created by CMS. The CCI was developed "to promote national correct coding methodologies and to control improper coding that leads to inappropriate payment of Part B (physician and hospital outpatient) claims. The coding policies are based on coding conventions defined in the merican Medical ssociation's Current Procedural Terminology (CPT) Manual, national and local Medicare policies and edits, coding guidelines developed by national societies, standard medical and surgical practice, andor current coding practice." The CCI continues to expand and now includes three types of edits: Procedure-to-Procedure edits, Medically Unlikely Edits, and dd-on Code Edits. It is important to be aware of CCI edits, as it is necessary for a bill to pass the edits in order to be paid correctly and in a timely manner. Return of the claim for revision delays payment and affects the provider's cash flow. The edits are updated on a quarterly basis, so they should be checked at the start of each calendar quarter. PROCEDURE-TO-PROCEDURE EDITS Procedure-to-procedure (PTP) edits were the first type of edits developed and are often referred to by the comprehensive term CCI or CCI edits. The PTP edit file consists of code pairs that may be inappropriate to report together. PTP edits are to prevent unbundling and the reporting of codes that are mutually exclusive based on their code description. The PTP edit file is presented in columns. The Column code is the comprehensive procedure. It is typically the procedure that utilizes the most resources; though, it is the procedure utilizing lesser resources for mutually exclusive
38 procedure codes. The Column 2 code is typically the lesser code and is considered bundled into the Column code under usual circumstances. n example of this is code 722 (femoralpopliteal atherectomy and angioplasty, if performed) and 722 (femoralpopliteal angioplasty). Code 722 is the Column code and is considered to include the work that is described by 722. When billed together, code 722 (the Column 2 code) will not be paid. If femoral angioplasty is performed on the right leg, and femoral atherectomy is performed on the left leg, a modifier must be appended to denote the distinct sites, as it is appropriate to bill the two procedures separately. This can usually be accomplished through -RT and -LT modifiers. In some instances, an -XS or -9 modifier may be necessary. MEDICLLY ULIKELY EDITS Medically unlikely edits (MUEs) were created to limit the number of times a specific CPT or HCPCS code can be reported. They do not apply to all codes. For the codes that they do apply to, a numerical limitation is assigned. When units of service exceed the limitation, the line item is denied. There are two types of MUEs: line item and date of service. Date of service edits are further differentiated as to whether they may be appealed. Line item MUEs are processed by Medicare on a line-by-line basis. If the same code is on more than one line it is evaluated separately. For example, code 77 (unilateral extremity arteriogram) is assigned a line item MUE of. If code 77 is reported with two units of service for unilateral upper and lower extremity imaging, it will be denied, as it exceeds the edit. If an upper extremity unilateral arteriogram and a lower extremity unilateral arteriogram are both performed, code 77 needs to be listed on two line items with appropriate modifier(s) appended to pass the edit. Each line item has one unit of service, so the edit is satisfied. Date of service MUEs are processed by Medicare on a date of service basis. ll units of service for the code on the same date of service are combined and evaluated against the MUE. If the MUE is exceeded, the extra units of service will be denied. For example, code 79 (IVC filter placement) is assigned a date of service MUE of. If it is billed more than once on the same date of service, even if on different claim lines (e.g., 79, 79-9), only one unit of service will be allowed. If billed on one claim line with two units of service, it will result in denial of the line item. Date of service MUEs are further differentiated as to whether there is the ability to appeal the denial by an MUE djudication Indictor (MI). The MI is a numerical classification with 2 denoting it cannot be appealed and denoting it can be appealed. If a denial is received for an MI edit and, after further review, the provider determines the units of service were correct, the denial can be appealed. Code 79, discussed above, is an MI edit. If it is denied and the provider determines it should have been reported more than once because the procedure was repeated in a separate session, the denial can be appealed. Code 72 (arterial thrombolysis, initial day) is an MI2 edit. denial based on the edit cannot be appealed. DD-O CODE EDITS dd-on code edits define what procedure each add-on code can be reported with. dd-on codes are preceded by a + sign in the CPT Codebook. Many of these add-on
39 codes have footnotes below them stating what procedures the add-on code is reported with. CMS uses these footnotes to create edits. The add-on code cannot be reported unless one of the base codes listed is also on the claim. For example, the footnote to code 72 (IVUS each additional vessel) states: "(Use 72 in conjunction with 722)." If code 72 is on the claim without code 722, it will be denied. It cannot be reported without its base code. Moderate (Conscious) Sedation Moderate sedation may be reported separately by physicians and facilities. To accurately bill for moderate sedation, there must be specific information documented to include: Preservice work; Intraservice work; and Postservice work. The activities required for each are found in the CPT Codebook introductory section for the moderate sedation codes (99-997). There should be documentation in either the physician report, the nursing documentation, or the room log that these activities have been performed. There must be a trained observer to perform patient monitoring that is supervised by the physician. The trained observer should not be involved in any other activities that would prevent monitoring the patient and responding to changes in the patient's condition. Moderate sedation codes are determined based on the face-to-face time the physician has with the patient during the sedation (this time is only calculated based on the "intraservice work" time). The physician must be present when the sedation is administered, which is the start time for tracking the time. The sedation time ends when the physician is no longer required to have face-to-face time with the patient - the patient is stable enough to move on to recovery. If the physician interrupts the face-to-face time with the patient, conscious sedation time is ended. In the procedure report, the physician should document at a minimum the use of an independent, trained observer and the amount of face-to-face time spent with the patient. Many of the monitoring activities (i.e., blood pressure, pulse oximetry measurement, etc.) may be documented in the room log, nursing notes, or anesthesia record. Moderate sedation is reported in -minute increments, with a specific code for the initial minutes based on patient age and whether the physician performing the procedure also supervised the moderate sedation or if it was performed by a different physician. The each additional -minute code is specific to which physician performed the moderate sedation. There must be at least minutes of moderate sedation to report a code for minutes. PROCEDURE DESCRIPTIO Moderate sedation services provided by the same physician or other qualified health care professional performing the diagnostic or therapeutic service that PR OC CO DE 99 P C TO T L RV U. 7
40 the sedation supports, requiring the presence of an independent trained observer to assist in the monitoring of the patient's level of consciousness and physiological status; initial minutes of intraservice time, patient younger than years of age Moderate sedation services provided by the same physician or other qualified health care professional performing the diagnostic or therapeutic service that the sedation supports, requiring the presence of an independent trained observer to assist in the monitoring of the patient's level of consciousness and physiological status; initial minutes of intraservice time, patient age years or older Moderate sedation services provided by the same physician or other qualified health care professional performing the diagnostic or therapeutic service that the sedation supports, requiring the presence of an independent trained observer to assist in the monitoring of the patient's level of consciousness and physiological status; each additional minutes intraservice time (List separately in addition to code for primary service) Moderate sedation services provided by a physician or other qualified health care professional other than the physician or other qualified health care professional performing the diagnostic or therapeutic service that the sedation supports; initial minutes of intraservice time, patient younger than years of age Moderate sedation services provided by a physician or other qualified health care professional other than the physician or other qualified health care professional performing the diagnostic or therapeutic service that the sedation supports; initial minutes of intraservice time, patient age years or older Moderate sedation services provided by a physician or other qualified health care professional other than the physician or other qualified health care professional performing the diagnostic or therapeutic service that the sedation supports; each additional minutes intraservice time (List separately in addition to code for primary service) dd-on Code CODIG ISTRUCTIOS:. Moderate sedation is reported separately whenever performed and documented appropriately (see the CPT Codebook introductory section to codes for required elements). 2. n "independent trained observer" is required when the physician performing the procedure oversees the moderate sedation. This individual
41 monitors the patient throughout the procedure and should not have other duties that interfere with this responsibility.. The codes are differentiated by age, as well as whether the moderate sedation is provided by the same physician (or other qualified healthcare professional) who is performing the procedure or by someone different. The codes are also broken down into initial versus additional time.. For a patient under years of age, report code 99 for the initial minutes of moderate sedation provided by the physician performing the procedure.. For a patient years of age or older, report code 992 for the initial minutes of moderate sedation provided by the physician performing the procedure.. Report code 99 for each additional minutes of moderate sedation provided by the physician performing the procedure, regardless of age. It is reported in addition to code 99 or 992 (for facility billing). 7. Physicians will not be reimbursed by Medicare for code 99 when overseeing moderate sedation in a facility (hospital) setting. CMS has designated code 99 as a technical component only code for physician billing. It will only be reimbursed by Medicare when performed in the non-facility (e.g., office, IDTF) setting.. For a patient under years of age, report code 99 for the initial minutes of moderate sedation provided by a different physician than the one performing the procedure. 9. For a patient years of age or older, report code 99 for the initial minutes of moderate sedation provided by a different physician than the one performing the procedure.. Report code 997 for each additional minutes of moderate sedation provided by a different physician than the one performing the procedure, regardless of age. It is reported in addition to code 99 or 99.. Report initial procedure codes 99, 992, 99, and 99 only one time per session. 2. Do not report moderate sedation (99, 992, 99, or 99) separately if less than minutes of sedation is performed.. Do not report an additional minutes of moderate sedation until a total of 2 minutes of sedation has been performed. The second additional -minute charge would be applied after a total of minutes of sedation time. To report an additional -minute code, at least additional minutes of sedation must have occurred after achieving the previous -minute block of time.. When determining face-to-face time, the timed sequence begins when the sedating agents are administered and ends when the procedure is completed and the patient is stable for recovery. The physician face-to-face time is the determining factor for reporting time. The documentation must clearly support this direct and continuous physician face-to-face time with the patient during moderate sedation.. Do not include pre-procedure activities (i.e., assessment of the patient, explanation of the procedure and informed consent, record review, etc.)
42 CODE when calculating sedation time; the sedation must be administered to begin counting time.. Do not include post-procedure activities (i.e., monitoring vital signs, discharging patient, documentation of sedation, family explanation, additional face-to-face time after sedation monitoring has ended, etc.) when calculating sedation time. 7. Do not report the services of patient monitoring separately. Pulse oximetry, rhythm strips, blood pressure monitoring, etc. are included in the moderate sedation codes.. Do not report minor sedation (anxiolysis) with the moderate sedation codes. Moderate sedation codes describe a "drug-induced depression of consciousness during which patients respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation". 9. For hospitals billing under HOPPS, moderate sedation is reported separately, but Medicare does not reimburse it separately. 2. ZHealth Publishing recommends the physician document face-to-face time in the report, as well as the drugs utilized, and that an independent trained observer was present during the procedure. 2. The physician should be well versed in the requirements outlined in the CPT Codebook section on moderate sedation. 2-2 ZHealth Publishing. ll rights reserved. CPT Only 27 merican Medical ssociation. ll rights reserved. Physician Payment Basics To assign CPT codes for Medicare billing, it is useful to understand Medicare payment. This includes how to determine coverage and specific rules for physician billing. Status Codes Each code is assigned a status code in the physician fee schedule. Status codes indicate whether the code can be reported and if it can receive payment. The following is a sample of the RVU schedule showing the status codes that are discussed below: M O D DESCRIPTIO G29 Injection procedure for sacroiliac joint; arthrography E G29 Place vascular closure device B Collection of venous blood by venipuncture X 9 72 Contrast injection(s) for radiologic evaluation of existing central venous access device, including fluoroscopy, image documentation and report Transcatheter placement of intravascular stent(s), cervical carotid artery, open or percutaneous, including angioplasty, when performed, and radiological supervision and interpretation; with distal embolic protection 72 Transcatheter placement of intravascular stent(s), STTUS CODE T R
43 cervical carotid artery, open or percutaneous, including angioplasty, when performed, and radiological supervision and interpretation; without distal embolic protection 2 Transcatheter permanent occlusion or embolization (eg, for tumor destruction, to achieve hemostasis, to occlude a vascular malformation), percutaneous, any method; non-central nervous system, head or neck (extracranial, brachiocephalic branch) Balloon angioplasty, intracranial (eg, atherosclerotic stenosis), percutaneous R 7 Consultation on x-ray examination made elsewhere, written report I 97 on-invasive ear or pulse oximetry for oxygen saturation; single determination T 7T Transcatheter placement of extracranial vertebral artery stent(s), including radiologic supervision and interpretation, open or percutaneous; initial vessel C There are currently nine active physician status indicator (SI) codes of importance:, B, C, E, I,, R, T, and X. STTUS IDICTOR - CTIVE CODE These codes are paid separately under the physician fee schedule, if covered. There will be RVUs for codes with this status. The presence of an status indicator does not mean that Medicare has made a national coverage determination regarding the service and that payment is guaranteed. In most instances, the Medicare Contractors remain responsible for coverage decisions. STTUS IDICTOR B - BUDLED CODE Payment for the service, when covered, is always bundled into payment for other services. There will be no RVUs or payment amount for these codes, and no separate payment is made. When these services are covered, payment for them is included in the payment for the services to which they are incident. For example, the receipt of a telephone call from a hospital nurse regarding patient status is bundled into the payment for the inpatient visit. In our sample schedule, placement of a vascular closure device (G29) is bundled and not paid separately. STTUS IDICTOR C - CRRIERS PRICE THE CODE Medicare Contractors will establish RVUs and payment amounts for these services, generally on an individual case basis following review of documentation, such as an operative report. CPT Category III codes 7T, Transcatheter placement of extracranial vertebral artery stent(s), including radiologic supervision and interpretation, open or percutaneous; initial vessel, and 7T, Transcatheter placement of extracranial vertebral artery stent(s), including radiologic supervision and interpretation, open or percutaneous; each additional vessel (List separately in addition to code for primary procedure),are status indicator C codes.
44 STTUS IDICTOR E - EXCLUDED FROM THE PHYSICI FEE SCHEDULE BY REGULTIO These codes are for items andor service that CMS has chosen to exclude from the physician fee schedule payment by regulation. o RVUs or payment amounts are shown, and no payment may be made under the physician fee schedule for these codes. HCPCS Level II codes G29, Injection procedure for sacroiliac joint; arthrography,and G2, Injection procedure for sacroiliac joint; provision of anesthetic, steroid andor other therapeutic agent, with or without arthrography, are status indicator E codes. These procedures were created for hospitals to recognize the differing cost based on the substance injected. Since the hospital, not the physician, purchases the drug, the physician payment is the same for the injection procedure under the CPT code describing sacroiliac joint injection. The physician would report these procedures with code 279, Injection procedure for sacroiliac joint, arthrography andor anestheticsteroid, with image guidance (fluoroscopy or CT), including arthrography when performed, which is a status indicator E procedure. STTUS IDICTOR I - OT VLID FOR MEDICRE PURPOSES Medicare uses another code for reporting of, and payment for, these services. Status indicator I is a commonly used indicator. It is most often used on HCPCS Level II codes describing supply items. It is also assigned to all the CPT Category II codes, as they are for performance monitoring and not payment. Code 7 is assigned status indicator I. STTUS IDICTOR - OCOVERED SERVICES These services are noncovered by Medicare. Code 72, Transcatheter placement of intravascular stent(s), cervical carotid artery, open or percutaneous, including angioplasty, when performed, and radiological supervision and interpretation; without distal embolic protection, is status indicator. Medicare only covers cervical carotid stent placement when embolization protection is used. When status indicator procedures are performed, an B should be signed by the patient and the code billed with a -G modifier appended. The patient may then be held liable for payment of the procedure. STTUS IDICTOR R - RESTRICTED COVERGE Special coverage instructions apply. The majority of codes to which this status indicator will be assigned are the alpha-numeric dental codes which begin with "D;" however, codes 72 (carotid stent placement with embolic protection device) and (intracranial balloon angioplasty) are assigned status indicator R. If the service is covered, it is Contractor priced. STTUS IDICTOR T - PID S OLY SERVICE There are RVUs and payment amounts for these services, but they are only paid if there are no other services payable under the physician fee schedule billed on the same date by the same provider. If any other services payable under the physician fee schedule are billed on the same date by the same provider, these services are bundled into the physician services for which payment is made. Code 9, Contrast injection(s) for radiologic evaluation of existing central venous access device,
45 including fluoroscopy, image documentation and report, is a status indicator T procedure. STTUS IDICTOR X - STTUTORY EXCLUSIO These codes represent an item or service that is not in the statutory definition of "physician services" for physician fee schedule payment purposes. o RVUs or payment amounts are shown for these codes, and no payment will be made under the physician fee schedule. Examples are ambulance services and clinical diagnostic laboratory services. Calculation of Physician Fees The calculation of physician fees is a complex formula. It is based on an RVU system that takes into consideration the amount of physician work (Work RVU), the malpractice risk associated with the procedure (Malpractice RVU), and the cost of maintaining an office attributable to the procedure (Practice Expense RVU). Each of these RVUs is assigned a cost index for calculating procedure reimbursement in a geographical area. The calculation is performed by the Medicare Contractor, but it is important to understand the components, especially for forecasting purposes. The elements used to calculate the fee schedule amounts are as follows: Resource Based Relative Value Units (RBRVU)-This factor takes into consideration the physician work required for the service, practice expenses, and the malpractice insurance premium. RBRVUs are established at a national level and do not vary among Medicare Contractors. There are three RBRVU values that make up the payment formula (work, practice expense, and malpractice). Geographic Practice Cost Index (GPCI)-This factor represents the variations in practice costs, which exist in different geographic areas. Connecticut comprises a single geographical area (locality); Florida is comprised of three () localities. The GPCI is established for each RBRVU component (work, practice expense, and malpractice). Conversion Factor (CF)-This factor is a single number set at a national level and is used by all Contractors in calculating the final fee schedule amounts. In 2 the conversion factor is $.999. For each procedure, there are three RBRVUs: relative value unit for physician work (RVUw); relative value unit for practice expense (RVUpe); and relative value unit for malpractice (RVUm). ote: For certain services, there are different practice expense RVUs depending on the place of service - facility or non-facility. Facility expense recognizes the reduced cost of performing a service in a hospital, SC, or skilled nursing facility versus the physician setting. For each payment locality, there are three GPCIs: GPCI for physician work (GPCIw), GPCI for practice expense (GPCIpe), and GPCI for malpractice (GPCIm). The formula for calculating the payment allowance for a given service under the fee schedule is:
46 Fee Schedule mount = [(RVUw x GPCIw) + (RVUpe x GPCIpe) + (RVUm x GPCIm)] x CF (CF is the conversion factor currently in place) The RBRVUs, the GPCIs, and the conversion factor are published in a Final Rule in the Federal Register, generally on or near ovember of each year. These calculations do not take into account any reduction based on fee schedule payment policies (e.g., pre, post, and intraoperative percentages, professional and technical components, multiple surgery, bilateral surgery, assistant-at-surgery, co-surgery, team surgery, sequestration, or facility pricing rules). Following is a sample of the RVUs in the 2 physician fee schedule: CPT HC PCS M O D ST TUS DESCRIPTIO PHYSICI WORK RVUs O-FCIL ITY PE RVUs FCILI TY PE RVUs MLPRC TICE RVUs scending aortic graft Transverse aortic arch graft Thoracic aortic graft Thoracoabdominal graft Endovasc taa repr incl subcl ThrmbcFS dialysis circuit Revision of circulation rtery x-rays, armleg T C rtery x-rays, armleg rtery x-rays, armleg rtery x-rays, armslegs T C rtery x-rays, armslegs rtery x-rays, armslegs Following is a sample of the GPCIs for 2: WOR PE COTR LOC LOCLITY ME K GPC CTOR LITY GPCI I MP GPC I ew Orleans, L Rest of Louisiana
47 Los ngeles-long Beach-naheim (Los ngeles County), C San Francisco-Oakland-Hayward (lamedacontra Costa County), C San Jose-Sunnyvale-Santa Clara (Santa Clara County), C Oxnard-Thousand Oaks-Ventura, C.2 To demonstrate how physician fees are calculated, we will calculate and compare the payment for a percutaneous V dialysis circuit thrombectomy procedure (CPT code 9) performed in lexandria, Louisiana and Los ngeles, California, in the hospital site of service. CPT CODE 9 LEXDRI LOS GELES RVUw RVUpe (facility setting) RVUm.. GPCIw.977. GPCIpe.7.77 GPCIm.99.9 RVUw x GPCIw RVUpe x GPCIpe.9 2. RVUm x GPCIm Total of rows above..22 Conversion factor Procedure payment $.2 $. In this example, while the malpractice expense is higher in lexandria, the wages and office expenses are significantly higher in Los ngeles, resulting in a physician in Los ngeles, California receiving higher reimbursement than the same procedure performed in lexandria, Louisiana. Discounting of Cardiovascular Procedures The technical component of additional procedures is discounted when multiple cardiovascular procedures are performed on the same day by the same physician or physicians in a group practice (billing with same PI number). When multiple procedures are performed, the procedure with the highest reimbursement is reimbursed at % of the physician fee schedule amount for the technical component. The other procedures are reimbursed at 7% of the technical fee. t this time there is no discounting of the professional component as there is with the imaging family of codes. The following procedure codes are included in the cardiovascular family of codes subject to discounting: PROC CODE TOTL RVU DESCRIPTOR 7.9 Contrast x-ray exam of aorta 7. Contrast x-ray exam of aorta 72.9 Contrast x-ray exam of aorta 7 2. X-ray aorta leg arteries 77.2 rtery x-rays spine rtery x-rays armleg
48 rtery x-rays armslegs rtery x-rays abdomen 77. rtery x-rays adrenal gland 77. rtery x-rays adrenals 77. rtery x-rays pelvis rtery x-rays lung rtery x-rays lungs 77. rtery x-rays lung 77.2 rtery x-rays chest 79. onvascular shunt x-ray Vein x-ray armleg 722. Vein x-ray armslegs 72.9 Vein x-ray trunk 727. Vein x-ray chest 7.7 Vein x-ray kidney Vein x-ray kidneys 7. Vein x-ray adrenal gland Vein x-ray adrenal glands 7.9 Vein x-ray neck 77. Vein x-ray skull 772. Vein x-ray skull 7. Vein x-ray eye socket 7.9 Vein x-ray liver 77.9 Vein x-ray liver 79. Vein x-ray liver 79.7 Vein x-ray liver Venous sampling by catheter 72.7 Cardiac shunt imaging 7.7 Vascular flow imaging 7.9 Ht muscle image spect sing Ht muscle image spect mult 7. Ht muscle image planar sing 7.9 Ht musc image planar mult 7. cute venous thrombus image 77.7 Venous thrombosis imaging 7.2 Ven thrombosis images bilat 7. Heart infarct image 7. Heart infarct image (EF) 79.2 Heart infarct image (D) Gated heart planar single Gated heart multiple 7. Heart first pass single Heart first pass multiple 79. Heart image spect 9. Electrocardiogram complete 9.2 Electrocardiogram tracing Cardiovascular stress test
49 97.97 Cardiovascular stress test 92.2 Cardiac drug stress test 92. Microvolt T-wave assess 9. Rhythm ECG with report 9. Rhythm ECG tracing 9.2 rt pressure waveform analys ECG monitreprt up to hrs ECG monitreprt up to hrs ECG monitreprt up to hrs Remote day ECG tech supp 92.2 Prgrmg dev eval impltbl sys 92.7 Interrogate subq defib 92. ECG recordreview Remote day ECG revreport 927. ECGmonitoring and analysis 927. ECGsignal-averaged PM device progr eval sngl 92.9 PM device progr eval dual PM device progr eval multi Prgrmg eval implantable DFB 92. ICD device progr eval dual ICD device progr eval mult 92.7 ILR device eval progr 92. Peri-px pacemaker device EVL 927. Peri-px device eval & prgr 92. PM device eval in person 929. Interrog device eval heart ICM device eval ILR device interrogate WCD device interrogate 9. Echo transthoracic 9. Echo transthoracic 9 2. TTE w Doppler complete 97.2 TTE wo Doppler complete 9.7 TTE f-up or lmtd 92. Echo transesophageal 9 2. Echo transesophageal Echo transesophageal intraop Stress TTE only Stress TTE complete 97.9 Bioimpedance CV analysis 972. BIS xtracell fluid analysis nalyze pacemaker system 97.2 mbulatory BP monitoring 97. mbulatory BP recording 97. mbulatory BP analysis 9. Extracranial study
50 92.72 Extracranial study 9. Intracranial study 9.7 Intracranial study 99. Tcd vasoreactivity study Tcd emboli detect wo inj 99.7 Tcd emboli detect winj 99. Carotid intima atheroma eval Uprl xtremity art 2 levels 992. Uprlxtr art stdy + lvls Lwr xtr vasc stdy bilat 992. Lower extremity study Lower extremity study 99. Upper extremity study 99.7 Upper extremity study Extremity study 997. Extremity study 997. Vascular study 997. Vascular study 997. Vascular study Vascular study 99.7 Penile vascular study 99.2 Penile vascular study Doppler flow testing Global Surgical Package When surgical procedures are performed on Medicare patients, the procedure payment includes a standard package of preoperative, intraoperative, and postoperative services. The preoperative period included in the global fee for major surgery is day. The postoperative period for major surgery is 9 days. The postoperative period for minor surgery is either or days, depending on the procedure. For endoscopic procedures (except procedures requiring an incision), there is no postoperative period. The following services are included in the global surgical package and are not separately reimbursed when furnished by the physician who performed the surgery: SERVICE Preoperative Visits 9-DY GLOBL SURGERY PCKGE Visits after the decision is made to operate beginning with the day before the day of surgery Intraoperative Services ll ll Complications Following Surgery Treatment of complications unless the patient returns to surgery OR -DY GLOBL SURGERY PCKGE Visits after the decision is made to operate beginning the day of surgery Treatment of complications during the -day global period unless the patient returns to surgery. Payment for procedures with global days
51 Postoperative Visits Follow-up visits that are related to recovery from the surgery Postsurgical Pain Management By the surgeon By the surgeon Supplies Related to the surgery Miscellaneous Services (dressing changes; local incisional care; removal of operative pack, removal of cutaneous sutures and staples, lines, wires, tubes, drains, casts and splints; insertion, irrigation and removal of urinary catheters, routine peripheral intravenous lines, nasogastric and rectal tubes; and changes and removal of tracheostomy tubes). Included includes treatment of complications the day of surgery unless the patient returns to surgery. Follow-up visits that are related to recovery from the surgery Related to the surgery Included The following services are not included in the global surgery package: The initial evaluation of the problem by the surgeon to determine the need for surgery. If the visit that results in the decision to perform a major surgery is the day before or the day of the surgery, append modifier -7 to the E&M code for the visit. The -7 modifier is not used with minor surgeries, as the global period for minor surgeries does not include the day prior to surgery. In addition, where the decision to perform the minor procedure is typically done immediately before the service, it is considered a routine preoperative service, and a visit is not billed in addition to the procedure. Services of other physicians except where the surgeon and the other physician(s) agree on the transfer of care. This agreement may be in the form of a letter or an annotation in the discharge summary, hospital record, or SC record. Visits unrelated to the diagnosis for which the surgical procedure is performed, unless the visits occur due to complication of the surgery. Modifier -79 is appended to a procedure code when the physician needs to indicate that the performance of a procedure or service during a postoperative period was unrelated to the original procedure. Modifier -2 is appended to an E&M code when a visit is unrelated to the original surgical procedure. In addition, modifier -2 may be appropriate if the physician needs to indicate that on the day a procedure or service was performed, the patient's condition required a significant, separately identifiable evaluation and management service above and beyond the usual preoperative and postoperative care associated with
52 the procedure or service that was performed. Treatment for the underlying condition or an added course of treatment which is not part of the normal recovery from surgery. Diagnostic tests and procedures, including diagnostic radiological procedures. Clearly distinct surgical procedures during the postoperative period which are not re-operations or treatment for complications (a new postoperative period begins with the subsequent procedures). This includes procedures done in two or more parts for which the decision to stage the procedures is made prospectively or at the time of the first procedure. Modifier - is used to indicate a staged procedure or service by the same physician during the postoperative period. Treatment for postoperative complications that require a return trip to the operating room. n operating room for this purpose is defined as a place of service specifically equipped and staffed for the sole purpose of performing procedures. The term includes a cardiac catheterization suite, a laser suite, and an endoscopy suite. It does not include a patient's room, a minor treatment room, a recovery room, or an intensive care unit (unless the patient's condition is so critical there would be insufficient time for transportation to an operating room). These services would be reported with modifier -7 appended. If a less extensive procedure fails, and a more extensive procedure is required on a subsequent date, the second procedure is separately payable. Immunotherapy management for organ transplants. Critical care services unrelated to the surgery where a seriously injured or burned patient is critically ill and requires constant attendance of the physician. In order for these services to be paid, two reporting requirements must be met:. Codes and modifier -2 (for preoperative care) or modifier -2 (for postoperative care) must be used.. Documentation that the critical care was unrelated to the specific anatomic injury or general surgical procedure performed must be submitted. n ICD--CM code in the range of S through T (except T-) that clearly indicates the critical care was unrelated to the surgery is acceptable documentation. dditional documentation may be requested if it is needed to process the claim. For minor surgeries and endoscopies, the Medicare program will not pay separately for an Evaluation & Management service on the same day as a minor surgery or
53 endoscopy, unless a significant, separately identifiable service is also performed (e.g., an initial new patient visit). CMS has developed modifiers to bill for eligible services rendered in the pre and postoperative periods of a surgery. These modifiers are explained in detail in Chapter 2. CMS has assigned global periods of "ZZZ" to many procedures. These procedures are add-on codes that are always billed with another procedure. There is no postoperative work included in the fee schedule amount for "ZZZ" procedures. However, when billed independent of another qualifying service, "ZZZ" procedures will be denied since they, by definition, are not stand-alone procedures. When billed in conjunction with a primary surgical procedure or qualifying service, both the primary and add-on code will be paid. The global surgery rules will be applied to the primary procedure. KEEP TRCK OF THE DTE CMS revises physician payment annually. s such, make sure you have the appropriate information based on the date of service when trying to predict payment. The key dates or time-frames for important updates to be aware of include: Physician Payment Rates - January each year CPT Category I Codes - Effective January each year CPT Category III Codes - Effective January and July each year HCPCS Level II Codes - Can change at any time, but there are usually revisions on a quarterly basis Modifiers - Can change at any time CCI Edits - Each quarter 2-2 ZHealth Publishing. ll rights reserved. CPT Only 27 merican Medical ssociation. ll rights reserved. Hospital Outpatient Prospective Payment System Hospital Outpatient Prospective Payment System Pages: 7- Most hospitals, but not all, are reimbursed by Medicare for outpatient procedures under the Hospital Outpatient Prospective Payment System (HOPPS). Under the HOPPS payment, most procedures (codes) are assigned to ambulatory payment classifications (PCs). The PC the procedure is assigned to determines the methodology of payment and the reimbursement amount for each procedure. When outpatient claims are submitted to Medicare, they are passed through the Outpatient Code Editor (OCE). This is software that screens the claim for missing data, claims not meeting date of service requirements (such as an outpatient claim overlapping an inpatient claim), matches sex of patient with procedure performed (cannot bill a hysterectomy on a male), as well as other key elements. For hospital billing, the Outpatient Code Editor is used to process claims and currently manages over fifty types of edits to include ational Correct Coding Initiative (CCI) edits. HOW REIMBURSEMET IS DETERMIED
54 ll CPT codes are not created equal. The HOPPS reimbursement system has a system of bundling and discounting. Many procedures, such as surgical procedures, are determined to have reduced costs when more than one procedure is done in one session. s a result, reimbursement may be reduced for subsequent procedures. For example, if two breast biopsies are done at the same setting, the second biopsy is reimbursed less, since the first biopsy includes the patient preparation, the room set-up, and sterile instruments. These actionsitems are not required to be repeated for the second procedure. nother factor deals with procedures that are always considered secondary to another procedure. When analyzed historically, these procedures were always billed secondary to another procedure and, therefore, would never be a stand-alone procedure. For instance, a selective catheter placement in the artery is not done unless a percutaneous selective vascular procedure is performed. Essentially, you cannot do one without the other. s a result of these and other factors, PCs are assigned into categories based on how they are paid. The categorization system is described by status indicators. The most important status indicators are listed below. ll services reported on the claim, even if performed on different dates, are considered performed on the same date for Medicare bundling. The explanations of status indicators apply to all procedures on a claim, regardless of the date of service. SIXTEE STTUS IDICTORS HVE IMPCT O ITERVETIOL RDIOLOGY PYMET There are sixteen status indicators that impact interventional radiology coding. These include status indicators B, C, E, E2, H, J, J2, K,, Q, Q2, Q, S, T, U, and V. Each will be discussed briefly. Status Indicator B Procedures that are assigned to status indicator B are codes that can not be reported to Medicare by hospitals paid under HOPPS. It is used on codes that describe procedures that are considered experimental or CPT codes that CMS has developed a HCPCS Level II code to replace, such as 279, Injection procedure for sacroiliac joint, arthrography andor anestheticsteroid, with image guidance (fluoroscopy or CT), including arthrography when performed, which was replaced with Level II codes G29 and G2, as well as codes that are physician-only services, such as interpretation of an EKG (9). When a code is assigned status indicator B, look for a HCPCS Level II code or another CPT code (if the service is broken out into technical and professional components) to replace it. If there is no other code describing the service, it may not be billable to Medicare. Status Indicator C Procedures that are assigned to status indicator C are procedures that must be done on an inpatient basis. When these types of procedures are performed and coded on an outpatient, the facility will receive no payment from Medicare. Most of the procedures assigned to a status indicator C are not normally performed on an outpatient basis due to their complexity or the severity of the patient's condition (e.g., for repair of descending thoracic aorta with initial endoprosthesis). In this case, the payment is only based on reimbursement under the Diagnosis Related Group (DRG) payment system, and not under HOPPS. Status indicators may change
55 over time, so check every year for an updated list. Status indicator C codes pertinent to interventional radiology are listed in ppendix C. Do not perform these procedures on an outpatient basis when Medicare is the payer. Status Indicators E and E2 Status indicators E and E2 identify items, codes, and services that are non-covered by Medicare. This is different from status indicator B, as the code is recognized, just not covered. Status indicator E indicates the procedure is non-covered due to statue, not part of a Medicare benefit, or not reasonably necessary. Status indicator E2 indicates the procedure is non-covered as a result of pricing information and claims data not being available. n example of a status indicator E procedure is code 7, Review of film performed elsewhere. Status Indicator H Some medical devices and therapeutic radiopharmaceutical agents are assigned to status indicator H and are reimbursed by the following two methods: a) separate cost-based Pass-Through device payment or b) separate cost-based on-pass-through radiopharmaceutical payment. For procedures that are considered "device-dependent" (the cost of the device implanted or the device utilized to perform the procedure is % or more of the PC payment amount), payment is essentially bundled into a single payment for all services on that date of service [except procedures paid under other coverage criteria, such as mammography, certain screening procedures, pass through devices, and drugs (status indicators F, G, H, L, U)]. Status Indicator J Status indicator J indicates outpatient department services paid through a comprehensive PC (C-PC). Procedures assigned status indicator J include defibrillator insertions, pacemaker insertions, event recorder insertions, neurostimulator implantations, electrode implantations, atherectomies, vascular embolizations, vascular angioplasties, vascular stent placements, electrophysiology procedures, infusion pump implantations, and other procedures outside the scope of this manual. The comprehensive PC bundles all services reported on a single claim into the payment for the highest weighted comprehensive PC reported. ncillary procedures are bundled and are assigned to status indicator (unconditionally packaged) or Q (packaged when provided with a service assigned a status indicator of J, J2, S, T, or V). When more than one procedure assigned status indicator J is on the claim, in most cases only the highest paid procedure will be reimbursed. ll other status indicator J procedures will be packaged. There is a complexity adjustment that may be applied when certain combinations of procedures are reported on the same claim. For example, certain additional codes reported in addition to the main C-PC code may trigger higher payment due to the complexity adjustment; however, not all additional procedure codes will be considered. The following table lists all the code combinations that will result in a complexity adjustment. When the two procedures in a row are billed together, the PC in the right-hand column will be paid. It pays significantly more than just one of the procedures. These are the only combinations of procedures that result in higher payment. PRI PRIMR P PRIM SECOD SECOD SE SECO COMPLEXI COMPLEX
56 MR Y HCP CS COD E Y SHORT DESCRIP TOR Drainag e of hemato mafluid Deb bone 2 sq cm< Deb bone 2 sq cm< Deb bone 2 sq cm< Exc tr-ext b9+mar g >. cm Exc tr-ext b9+mar g >. cm Exc tr-ext b9+mar g >. cm Exc tr-ext b9+mar g >. cm Exc tr-ext mal+ma rg > cm Exc tr-ext RI M R Y SI RY PC SSIG ME T RY J OR DD-O HCPCS CODE J 72 J 72 J J J 72 J 72 J J 72 2 J 72 J 72 RY SHORT DESCRIP TOR Drainag e of hemato mafluid Deb bone 2 sq cm< mputa tion of toe Partial amputat ion of toe Exc tr-ext b9+mar g.- cm Exc tr-ext b9+mar g >. cm Exc h-f-nk-s p b9+mar g.-2 Exc h-f-nk-s p b9+mar g.- Exc tr-ext b9+mar g >. cm Exc tr-ext CO D RY SI DRY PC SSIG ME T TY DJUSTED HCPCS SSIGME T J 72 X 7 J 72 D 7 J 2 D 7 J 2 D 7 J 72 G 7 J 72 G 7 J 72 G 7 J 72 G 7 J 72 G 7 ITY DJUSTED PC SSIGM ET J 72 G 7
57 2 2 2 mal+ma rg > cm Exc tr-ext mal+ma rg > cm Exc tr-ext mal+ma rg > cm Exc tr-ext mal+ma rg > cm Exc tr-ext mal+ma rg > cm Exc snhf g mal+mr g 2.- Exc snhf g mal+mr g.- Exc snhf g mal+mr g.- Exc feen l mal+mr g 2.- Exc feen l mal+mr J 72 2 J 72 2 J 72 J 72 J 72 2 J 72 2 J 72 J 72 J 72 mal+ma rg > cm Exc snhf g mal+mr g 2.- Exc snhf g mal+mr g.- Exc feen l mal+mr g 2.- Exc feen l mal+mr g.- Exc snhf g mal+mr g 2.- Exc snhf g mal+mr g 2.- Exc feen l mal+mr g.- Exc feen l mal+mr g 2.- Exc feen l mal+mr J 72 G 7 J 72 G 7 J 72 G 7 J 72 G 7 J 72 2C 7 J 72 2D 7 J 72 2D 7 J 72 C 7 J 72 D 7
58 g.- g 2.- Exc Exc feen feen l J 72 l mal+mr mal+mr g.- g.- Bx breast st lesion strtctc Bx breast st lesion strtctc Bx breast st lesion strtctc Bx breast st lesion us imag Bx breast st lesion us imag Bx breast st lesion mr imag Bx breast st lesion mr imag Bone biopsy trocarn eedle Bone biopsy J 72 9 J 72 9 J 72 J 72 9 J 72 J 72 9 J 72 9 J J Bx breast st lesion strtctc Bx breast st lesion us imag eedle biopsy lymph nodes Bx breast st lesion us imag eedle biopsy lymph nodes Bx breast st lesion us imag Bx breast st lesion mr imag eedle biopsy muscle eedle biopsy J 72 D 7 J J J J 72 9C 7 J 72 9C 7 J 72 9E 7 J 72 9E 7 J X 7 J E 7
59 trocarn eedle Bone biopsy trocarn eedle Bone biopsy trocarn eedle Exc back les sc cm> Exc forearm les sc cm> Percut bx lungme diastinu m Percut bx lungme diastinu m Tempor al artery procedu re Dx bone marrow biopsies Dx bone marrow biopsies Dx bone marrow biopsies Dx bone marrow biopsies J J 72 2 J J J J 72 J J J J 72 2 J muscle Bone biopsy trocarn eedle Percut bx lungme diastinu m Exc back les sc cm> Exc forearm les sc cm> Bone biopsy trocarn eedle eedle biopsy lymph nodes Tempor al artery procedu re eedle biopsy muscle Bone biopsy trocarn eedle Percut bx lungme diastinu m Dx bone marrow biopsies J E 7 J E 7 J J J 72 2E 7 J 72 2E 7 J 72 7S 7 J J J J
60 Dx bone marrow biopsies Dx bone marrow biopsies Dx bone marrow biopsies eedle biopsy of liver Biopsy abdomi nal mass Image cath fluid colxn visc Image cath fluid periret ro Image cath fluid periret ro Renal biopsy perq Partial mastect omy Partial mastect omy J 72 J 72 9 J 72 2 J 72 2 J 72 2 J 72 9 J 72 9 J 72 9 J 72 2 J 9 92 J 9 9 eedle biopsy lymph nodes Biopsy abdomi nal mass Renal biopsy perq eedle biopsy pancrea s Percut bx lungme diastinu m Image cath fluid colxn visc Biopsy abdomi nal mass Image cath fluid periret ro Percut bx lungme diastinu m Excision breast lesion Partial mastect omy J J J J 72 7X 7 J 72 9X 7 J 72 9E 7 J 72 9G 7 J 72 9G 7 J 72 2X 7 J J Partial J 9 Biopsyr J
61 mastect omy Partial mastect omy Mast subq Surgery of breast capsule Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes J 9 J 9 9 J 9 97 J 9 J 9 2 J 9 2 J 9 J 9 J 9 92 J 9 emoval lymph nodes Biopsyr emoval lymph nodes Mast subq Surgery of breast capsule Exc tr-ext mal+ma rg > cm Exc snhf g mal+mr g 2.- Exc snhf g mal+mr g > cm Exc feen l mal+mr g.- Exc feen l mal+mr g > cm Excision breast lesion Biopsyr emoval lymph nodes J J 9 9D 92 J 9 97X 92 J 72 X 92 J 72 X 92 J 7 X 92 J 72 X 92 J 7 X 92 J 9 X 92 J 9 X 92 Biopsyr J 9 2 Partial J X 92
62 emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes J 9 J 9 2 J 9 2 J 9 2 J 9 J 9 J 9 J 9 2 J 9 removal of vulva Exc tr-ext mal+ma rg > cm Exc snhf g mal+mr g 2.- Exc snhf g mal+mr g.- Exc snhf g mal+mr g > cm Exc feen l mal+mr g 2.- Exc feen l mal+mr g.- Exc feen l mal+mr g > cm Resect facesca lp tum 2 cm> Laryngo scopy wbx & op scope J 72 X 92 J 72 X 92 J 72 X 92 J 7 X 92 J 72 X 92 J 72 X 92 J 7 X 92 J 7 X 92 J X 92
63 Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph J 9 J 9 J 9 9 J 9 J 9 J 9 2 J 9 92 J 9 9 J 9 9 J 9 27 J 9 27 Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Remove external ear partial Exc tr-ext b9+mar g >. cm Exc tr-ext mal+ma rg > cm Exc snhf g mal+mr g > cm Excision breast lesion Partial mastect omy Mast subq Exc armelb ow les sc cm> Exc forearm les sc J 9 X 92 J 9 X 92 J 7 X 92 J 72 2E 92 J 72 2E 92 J 7 2E 92 J 9 2E 92 J 9 2E 92 J 9 2E 92 J 7 2E 92 J 72 2E 92
64 nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes P-maste ctomy wln removal Mast mod rad Immedi ate breast prosthe sis Treat shoulde r dislocati on Incision of tendon sheath Remove wrist J 9 27 J 9 29 J 9 J 9 J 9 2 J 92 9 J 92 9 J 92 9 J 2 2 J 2 2 J 2 2 cm> Resect forarm wrist tum cm> mputa tion of fingert humb Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Biopsyr emoval lymph nodes Reducti on of large breast Immedi ate breast prosthe sis Mast simple complet e Treat shoulde r dislocati on Remove tendon sheath lesion Remove tendon J 7 2E 92 J 2E 92 J 9 2E 92 J 9 2E 92 J 9 2E 92 J 92 9B 9 J 92 9Q 9 J 92 9X 9 J 2 2E J 2 2X J 2 2
65 tendon lesion Excise wrist tendon sheath Repair hand tendon Repair finger tendon Realign ment of tendons Incision of finger tendon Release finger contract ure Treat hip dislocati on Remova l of foot lesion Remova l of toe lesions Partial removal of toe Incision of foot tendon mputa tion of toe mputa tion of toe mputa tion of toe J 2 2 J 2 2 J 2 2 J 2 27 J 2 2 J 2 22 J J 2 2 J 2 2 J 2 22 J 2 22 J J 2 22 J 2 22 sheath lesion Excise wrist tendon sheath Repair hand tendon Repair finger tendon Realign ment of tendons Incision of finger tendon Release finger contract ure Treat hip dislocati on Remova l of foot lesion Remova l of toe lesions Partial removal of toe Incision of foot tendon Incision of toe tendon mputa tion of toe Partial amputat ion of J 2 2R J 2 2X J 2 2R J 2 2Q J 2 2E J 2 22E J 2 272G J 2 2X J 2 2R J 2 22D J 2 22D J 2 22X J 2 22X J 2 22X
66 Partial amputat ion of toe Partial amputat ion of toe Wrist endosco pysurg ery Wrist endosco pysurg ery Wrist endosco pysurg ery Wrist endosco pysurg ery Wrist endosco pysurg ery Wrist endosco pysurg ery Wrist endosco pysurg ery Perq cervicot horacic inject Perq lumbosa cral injectio n J J 2 22 J 2 2 J 2 2 J 2 2 J 2 2 J 2 2 J 2 2 J 2 29 J 222 J 222 toe Incision of toe tendon J 2 22E Partial amputat ion of toe J 2 22E Incision of tendon J 2 29R sheath Remove wrist tendon J 2 29R lesion Remove wristfo rearm J 2 29R lesion Incise finger tendon J 2 29R sheath Tendon excision palmfin J 2 29R ger Remove tendon sheath J 2 29R lesion Wrist endosco pysurg J 2 29R ery Vertebr oplasty addl 22X inject Vertebr oplasty addl inject 22 2 Repair J 2 Fusion J 2Q
67 7 wrist joints Repair wrist joints Revise knuckle joint Revise finger joint Treat metacar pal fracture Repair achilles tendon Repair achilles tendon Repair achilles tendon Repair achilles tendon Revision of calf tendon Remova l of heel bone Remova l of heel spur Repair of foot tendon Correcti on hallux J 7 J 2 J 2 J 2 J 277 J 2 J 29 J 22 J 22 J 277 J 277 J 2 J 227 of finger joint Revise ulnar nerve at elbow Revise knuckle joint Revise finger joint Treat metacar pal fracture Revision of calf tendon Remova l of heel bone Remova l of heel spur Part removal of ankleh eel Repair of hammer toe Revision of calf tendon Revision of calf tendon Incision of metatar sal Release of foot contract J 2Q J 2X J 2E J 2E J 27X J 27X J 27X J 27X J 27Q J 2R J 2S J 22X J 229G
68 valgus Correcti on hallux valgus Correcti on hallux valgus Correcti on hallux valgus Correcti on hallux valgus Correcti on hallux valgus Correcti on hallux valgus Correcti on hallux valgus Correcti on hallux valgus Correcti on hallux valgus Correcti on hallux valgus Correcti on hallux valgus J 22 J 229 J 2292 J 229 J 2 J 2 J 2 J 2 J 227 J 22 J 2299 ure Repair of hammer toe Corrj halux rigdus wo implt Correcti on hallux valgus Correcti on hallux valgus Incision of metatar sal Repair deformi ty of toe Repair toe dislocati on Part removal of metatar sal Release of foot contract ure Repair of hammer toe Correcti on hallux valgus J 229G J 229G J 229G J 229G J 229G J 229G J 229G J 229S J 229S J 229S J 229S
69 Correcti on hallux valgus Correcti on hallux valgus Incision of metatar sal Incision of metatar sal Incision of metatar sal Incision of metatar sal Incision of metatar sal Revision of big toe Repair toe dislocati on Repair toe dislocati on mputa tion thru metatar sal J 2 J 2 J 277 J 229 J 2292 J 2 J 2 J 229 J 2 J 2 J 277 Incision of metatar sal Repair deformi ty of toe Revision of calf tendon Corrj halux rigdus wo implt Correcti on hallux valgus Incision of metatar sal Repair deformi ty of toe Correcti on hallux valgus Incision of metatar sal Repair toe dislocati on Revision of calf tendon J 229S J 229S J 2R J 2R J 2R J 2R J 2R J 2X J 2E J 2E J 2E 292 Shoulde J 22 Partial J 292B
70 2 r arthrosc opysur gery Shoulde r arthrosc opysur gery Shoulde r arthrosc opysur gery Shoulde r arthrosc opysur gery Elbow arthrosc opysur gery Knee arthrosc opysur gery Remove sympat hetic nerves pply bone fixation device blate bone tumor(s ) perq Perq vertebra l augmen tation J 22 J 299 J 292 J 29 J 2979 J 22 J 27 J 22 J 22 removal collar bone Partial removal collar bone Shoulde r arthrosc opysur gery Shoulde r arthrosc opysur gery Elbow arthrosc opysur gery Knee arthrosc opysur gery Remove sympat hetic nerves Treatme nt of ankle fracture Perq lumbosa cral injectio n Open bone biopsy Perq vertebra J 292 blate bone J 292C J 292C J 292C J 29R J 29B J 2 J 2 29X J 29B J 22C J 22C
71 l augmen tation Perq vertebra l augmen tation Perq vertebra l augmen tation Perq vertebra l augmen tation Perq vertebra l augmen tation Perq vertebra l augmen tation Perq vertebra l augmen tation Perq vertebra l augmen tation Perq vertebra l augmen tation Perq vertebra l augmen J 22 J 22 J 22 J 22 J 292 J 22 J 22 J 22 J tumor(s ) perq Perq cervicot horacic inject Perq lumbosa cral injectio n Perq vertebra l augmen tation Perq vertebra l augmen tation blate bone tumor(s ) perq Perq cervicot horacic inject Perq lumbosa cral injectio n Perq vertebra l augmen tation Low back disk surgery J 22C J 22C J 22C 22C J 22D J 22D J 22D 22D J 22D
72 tation Perq vertebra l augmen tation Treat clavicle fracture Treat ulnar fracture Treat fx rad extra-ar ticul Treat fx rad intra-art icul Treat fx rad intra-art icul Treat fx radial + frag Treat fx radial + frag Treat fx radial + frag Revise knuckle with implant Revisei mplant finger joint Treatme nt of ankle fracture J 7 J 2 J 2 J 2 J 2 J 2 J 2 J 2 J 29 J 2 J 2 J 277 Remove spine lamina lmbr Treat clavicle dislocati on Treat radius fracture Treat fracture of ulna Treat fracture of ulna Treat fracture radiusu lna Treat fracture of ulna Treat fracture radiusu lna Treat fx radial + frag Revise knuckle with implant Revisei mplant finger joint Optx medial ankle fx J 22D J 2E J 2E J 2Q J 2R J 2 2R J 2S J 2 2S J 2S J 2 J 2G J 2779B
73 Treatme nt of ankle fracture Correcti on hallux valgus Correcti on hallux valgus Correcti on hallux valgus Incision of heel bone Incision of heel bone Incision of heel bone Fusion of foot bones Fusion of foot bones Fusion of foot bones Fusion of foot bones Fusion of foot bones J 27 J 229 J 2 J 2 J 279 J 279 J 2 J 292 J 279 J 2297 J 229 J 2 Treatme nt of ankle fracture Correcti on hallux valgus Incision of heel bone Incision of metatar sal Repair of ankle ligamen t Repair of ankle ligamen t Incision of midfoot bones Remova l of bone for graft Revise lower leg tendon Correcti on hallux valgus Correcti on hallux valgus Incision of heel bone J 2 272B J 229Q J 229Q J 229Q J 2X J 2X J 2X J 27X J 27X J 27X J 27X J 27X
74 Fusion of foot bones Fusion of foot bones Fusion of foot bones Fusion of foot bones Fusion of foot bones Fusion of big toe joint Fusion of big toe joint Fusion of big toe joint Fusion of big toe joint Fusion of big toe joint Fusion of big toe joint Fusion of big toe joint Shoulde r J 2 J 2 J 27 J 27 J 22 J 292 J 229 J 2 J 29 J 2 J 27 J 22 J 2927 Incision of metatar sal Treat metatar sal fracture Fusion of foot bones Fusion of big toe joint Dx bone marrow aspirati ons Remova l of bone for graft Correcti on hallux valgus Incision of metatar sal Incision of metatar sals Repair toe dislocati on Fusion of big toe joint Dx bone marrow aspirati ons rthrosc op J 27X J 27X J 27X J 27X J 72 27X J 27X J 27X J 27X J 27X J 27X J 27X J 72 27X J 29G
75 arthrosc opysur gery Tibial arthrosc opysur gery Knee arthrosc opysur gery Hip arthro wlabral repair Remove spine lamina lmbr Revision of knee joint Revision of knee joint asalsi nus endosco py surg asalsi nus endosco py surg Dx laryngos copy excl nb Dx laryngos copy woper scope Dx broncho scopela vage J 279 J 292 J 299 J 22 J 27 J 27 J 27 J 2 J 22 J 22 J 2 rotator cuff repr Treatme nt of thigh fracture Knee arthrosc opysur gery Hip arthro acetabu loplasty pply spine prosth device Remove knee joint lining Revision of knee joint asalsi nus endosco py surg asalsi nus endosco py surg Dx broncho scopew ash Dx broncho scopew ash Dx broncho scopela vage J 29E J 29R J 299G Q J 27G J 27G J 2R J 2R J 2E J 2G J 2D
76 2 2 2 Broncho scopy wbiops y(s) Broncho scopy wbiops y(s) Broncho scopy wbiops y(s) Laryngo scopy wbiops y Broncho scopy dilatefx repr Broncho scopy dilatefx repr Broncho scopy treat blockag e Bronch ebus samplng > node Bronch ebus samplng > node Bronch ebus samplng > node J 2 J 2 J J 2 J 2 J J 2 J 2 J 29 J Dx broncho scopeb rush Dx broncho scopela vage Broncho scopy wfb removal Egd place gastrost omy tube Broncho scopylu ng bx each Broncho scopy treat blockag e Bronch ebus samplng 2 node Broncho scopylu ng bx each Broncho scopyn eedle bx each Broncho scopy treat blockag e J 2E J 2E J 2E J 2 E J X J X J J C J C J C 2 Remove J 2 Remove J 2
77 exostosi s mandibl e Remova l of intranas al lesion Repair of nasal septum Repair of nasal septum Repair of nasal septum Repair of nasal septum Repair of nasal septum Repair of nasal septum Repair of nasal septum Explorat ion maxillar y sinus Explorat ion maxillar y sinus Remova l of ethmoid sinus J 2 J J J J 27 J 2 J 2 J 22 J 2 J 2 J 2 exostosi s mandibl e asalsi nus endosco py surg Excise inferior turbinat e Resect inferior turbinat e Repair nasal septum defect asalsi nus endosco py surg asalsi nus endosco py surg asalsi nus endosco py surg Remova l of tonsils Repair of nasal septum Explorat ion maxillar y sinus Remova l of ethmoid sinus J Q J 2X J 2X J 2X J 2X J 2X J 2X J 2X J 2X J 2X J 2
78 Repair tooth socket Remova l of tonsils Right heart cath Coronar y artery angio s&i Coronar y artgrft angio s&i Coronar y artgrft angio s&i R hrt coronar y artery angio R hrt coronar y artery angio R hrt artgrft angio L hrt arteryv entricle angio L hrt arteryv entricle angio J 7 J 9 J 9 9 J J J 9 97 J J 9 97 J 9 97 J J 9 9 Repair tooth socket Esophag oscopy rigid trnso dx Right heart cath Endolu minl ivus oct c st Endolu minl ivus oct c st Heart flow reserve measur e Endolu minl ivus oct c st Heart flow reserve measur e Heart flow reserve measur e Endolu minl ivus oct c st Coronar y artery angio s&i J 7D J 2 22G J D 92 9E 92 9E 92 9G 92 9G 92 9Q 92 9R 92 J 9 9R 92 9 L hrt J 9 9 L hrt J 9 9R 92
79 arteryv entricle angio L hrt arteryv entricle angio L hrt artgrft angio L hrt artgrft angio L hrt artgrft angio R&l hrt artvent ricle angio R&l hrt artvent ricle angio R&l hrt artvent ricle angio Prim art m-thrm bc st vsl Fempo pl revas wtla Fempo pl revas wtla J 9 97 J J 9 9 J 9 97 J J 9 97 J 9 97 J J J arteryv entricle angio Heart flow reserve measur e Endolu minl ivus oct c st Coronar y artgrft angio s&i Heart flow reserve measur e Endolu minl ivus oct c st Heart flow reserve measur e Heart flow reserve measur e Fempo pl revas wtla Iliac revasc Fempo pl revas wtla 9R 92 9S 92 J 9 9S 92 9S 92 9X 92 9X J 92 7D 9 J D 9 J D Fempo J 92 9 L hrt J 9 722D 9
80 pl revas wtla Prq cardiac angiopla st art Revision of aortic valve Revision of aortic valve Iliac revasc wstent Iliac revasc wstent Fempo pl revas wather Fempo pl revas wather Fempo pl revas wather Fempo pl revas wather Fempo pl revas wather Fempo pl revas wather Fempo pl revas wather J J 92 9 J 92 9 J 9 7 J 9 C9 J 9 7 J J J J J J 9 72 arteryv entricle angio Prq cardiac angiopla st art R&l hrt cath wventr iclgrphy R&l hrt artvent ricle angio Prim art m-thrm bc st vsl Perc drug-el cor stent sing Prim art m-thrm bc st vsl Iliac revasc Iliac revasc wstent Fempo pl revas wather Fempo pl revasc wstent Tibper revasc wtla Openp erq place J X 9 J 9 929G 9 J 9 929G 9 J J J E 9 J E 9 J 9 722E 9 J 9 722E 9 J 9 722E 9 J 9 722E 9 J 9 722E 9
81 Fempo pl revasc wstent Fempo pl revasc wstent Fempo pl revasc wstent Openp erq place stent same Openp erq place stent same Vasc emboliz eocclu de artery Vasc emboliz eocclu de artery Vasc emboliz eocclu de organ Vasc emboliz eocclu de organ Prq card angioat J 9 7 J J 9 C9 J 9 77 J 9 72 J J 9 72 J 9 72 J 9 72 J 9 C9 stent st Prim art m-thrm bc st vsl Iliac revasc wstent Perc drug-el cor stent sing Venous mech thromb ectomy Openp erq place stent same Iliac revasc wstent Vasc emboliz eocclu de organ Vasc emboliz eocclu de organ Percut ablate liver rf Perc drug-el J G 9 J 9 722G 9 J 9 722G 9 J 92 72R 9 J 9 72R 9 J 9 72B 9 J 9 72B 9 J 9 72C 9 J 72C 9 J D 9
82 C9 C9 C9 C hrect art Perc drug-el cor stent sing Perc drug-el cor stent sing Perc drug-el cor stent sing Perc d-e cor revasc t cabg s Electrop hysiolog y evaluati on Implant pat-acti ve ht record Implant pat-acti ve ht record Insert heart pm atrial Insert heart pm ventricu lar J 9 2 J 9 2 J 9 22 J 9 C9 J 22 9 J J J J cor stent sing Insrt heart pm atrial & vent Insert electrd pm cath sngl Implant pat-acti ve ht record Perc drug-el cor stent sing blate heart dysrhyt hm focus R&l hrt artvent ricle angio Electrop hysiolog y evaluati on L ventric pacing lead add-on L ventric pacing lead add-on J 22 C9X 9 J 222 C9X 9 J 222 C9X 9 J 9 C9D 9 J 22 92X 2 J 9 2B 22 J 22 2B 22 2G 22 2Q 22 2 Insrt J L ventric 2R 22
83 heart pm atrial & vent Insrt heart pm atrial & vent Insrt heart pm atrial & vent Upgrad e of pacema ker system Remv&r eplc pm gen dual lead Insert cath pleura wo image Esophag oscopy rigid trnso dx Esophag oscopy rigid trnso dx Esophag oscopy balloon <mm Egd us fine needle bxaspir Egd us fine J 22 9 J 22 9 J J J 2 2 J 2 2 J 2 22 J 2 2 J 2 2 J 2 2 pacing lead add-on R&l hrt artvent ricle angio blate heart dysrhyt hm focus L ventric pacing lead add-on L ventric pacing lead add-on Insert cath pleura wo image Dx laryngos copy excl nb Dx broncho scopew ash Esoph scope wsubm ucous inj Egd remove lesion snare Egd dilate J 9 2R 22 J 22 2R 22 2D 22 22R 22 J 2 2G J 9 J 9 J 2 22X J 2 2R J 2 2B
84 needle bxaspir Egd us fine needle bxaspir Egd us fine needle bxaspir Egd place gastrost omy tube Esoph egd dilation < mm Egd endo mucosal resectio n Egd endo mucosal resectio n Egd endo mucosal resectio n Egd endo mucosal resectio n Egd endo mucosal resectio n Egd endo mucosal J 2 29 J 2 2 J 2 2 J 2 22 J 2 27 J 2 2 J 2 22 J 2 2 J 2 2 J 2 29 stricture Esoph egd dilation < mm Egd remove lesion snare Egd place gastrost omy tube Dx broncho scopew ash Endosco pic us exam esoph Egd us fine needle bxaspir Egd us fine needle bxaspir Egd remove lesion snare Egd control bleedin g any Egd us exam duoden J 2 2B J 2 2B J 2 2G J 2S J 2 2D J 2 2D J 2 2D J 2 2D J 2 2D J 2 2D
85 resectio n Egd control bleedin g any Egd lesion ablation Egd lesion ablation Egd lesion ablation Egd lesion ablation Exchang e drainag e catheter Exchang e drainag e catheter Place gastrost omy tube perc Egd wthrml txmnt gerd Endo cholangi opancre J 2 2 J 2 27 J 2 22 J 2 2 J 2 29 J 2 9 J 2 92 J 2 9 J 22 J 22 umjeju num Egd control bleedin g any Endosco pic us exam esoph Egd us fine needle bxaspir Egd endo mucosal resectio n Egd us exam duoden umjeju num Image cath fluid periret ro Exchang e drainag e catheter Change g-tube to g-j perc Egd optical endomi croscop y Egd us fine needle J 2 2E J 2 27X J 2 27X J 2 27X J 2 27X J 72 92C J 2 92C J 2 9X J 2Q J 2 2B
86 atograp h Plmt biliary drainag e cath Biliary endosco py thru skin Prp ihern init reduc > yr Prp ihern init reduc > yr Prp ihern init block > yr Prp ihern init block > yr Prp ihern init block > yr Prp ihern init block > yr Prp ihern init block > yr Rerepair ing J 7 J 7 J 9 J 2 J 9 J 97 J 9 J 97 J 2 J 9 bxaspir Exchang e biliary drg cath Exchang e biliary drg cath Prp ihern init reduc > yr Remova l of testis Prp ihern init reduc > yr Prp ihern init block > yr Rpr umbil hern reduc > yr Rpr umbil hern block > yr Remova l of testis Prp ihern J 7D J 7E J 9E J 7 9E J 9Q J 9Q J 9Q J 9Q J 7 9Q J 92X
87 hernia reduce Rerepair ing hernia reduce Rerepair ing hernia reduce Rerepair ing hernia reduce Rerepair ing hernia blocked Repair ing hernia sliding Repair ing hernia sliding Rpr ventral hern init reduc Rpr ventral hern init reduc Rpr ventral hern init reduc Rpr ventral J 92 J 9 J 2 J 92 J 9 J 9 J J 9 J 97 J 92 init reduc > yr Rerepair ing hernia reduce Rpr umbil hern reduc > yr Remova l of testis Rerepair ing hernia blocked Prp ihern init reduc > yr Rpr umbil hern reduc > yr Exc tr-ext b9+mar g >. cm Prp ihern init reduc > yr Prp ihern init block > yr Rerepair ing J 92X J 92X J 7 92X J 92 J 92E J 92E J 72 9X J 9X J 9X J 9X
88 hern init reduc Rpr ventral hern init reduc Rpr ventral hern init reduc Rpr ventral hern init reduc Rpr ventral hern init block Rpr ventral hern init block Rpr ventral hern init block Rpr umbil hern block > yr Laparos copy lymph node biop Laparos copy append ectomy Percut ablate liver rf J 9 J 9 J 97 J 9 J 97 J 9 J 9 J J J 7 hernia reduce Rpr ventral hern init reduc Rpr ventral hern init block Rpr umbil hern block > yr Prp ihern init reduc > yr Prp ihern init block > yr Rpr ventral hern init block Prp ihern init reduc > yr Laparos copy remove adnexa Laparos copy remove adnexa eedle biopsy of liver J 9X J 9X J 9X J 9 J 9 J 9 J 9Q J 7X 2 J 97X 2 J 72 7B 2 7 Perq J 7 Perq J 7R 2
89 plmt bile duct stent plmt bile duct stent Endo Laparos cholangi 7 copic J 22 opancre 2 cholecys atograp tectomy h J 7B 2 Laparos Ercp 7 copic remove J 2 2 cholecys duct J 7B 2 tectomy calculi Ercp Laparos duct 7 copic J 27 stent 2 cholecys placeme tectomy nt J 7B 2 Endo Laparo cholangi 7 cholecys J 22 opancre tectomy atograp graph h J 7C 2 Laparo Ercp 7 cholecys remove J 2 tectomy duct J 7C 2 graph calculi Ercp Laparo duct 7 cholecys J 27 stent tectomy placeme graph nt J 7C 2 Laparo Lap proc 9 ventab J 929 abdmp 2 d hernia erome repair nt J 9B 2 Prp Lap ihern 9 ventab J 9 init 2 d hernia reduc > repair yr J 9B 2 Lap Lap 9 ventab ventab J 92 2 d hernia d hernia J 9B 2 repair repair 9 Lap J Laparos J 9B 2
90 2 ventab d hernia repair Lap ventab d hern proc comp Lap ventab d hern proc comp Laparos copy remove adnexa Laparos copy remove adnexa Laparos copy remove adnexa Laparos copy remove adnexa Change stent via transure th Change stent via transure th Plmt nephros tomy catheter Plmt nephros tomy catheter J 929 J 9 J 22 J 72 J 72 J 2 J 7 J 7 2 J 7 2 J 7 copy remove adnexa Laparo proc abdmp erome nt Lap ventab d hern proc comp Cystosc opy and treatme nt nterior colporrh aphy Repair bladder defect Vaginal hysterec tomy Change stent via transure th Cystosc opy & ureter catheter Plmt nephros tomy catheter Exchang e nephros tomy cath J 9C 2 J 9C 2 J 7 2 J 2 J 2 J 2 J 7 E 7 J 7 E 7 J 7 B 7 J 7 B 7 Plmt J 7 2 Cystosc J 7 B 7
91 2 nephros tomy catheter Plmt nephros tomy catheter Plmt nephrou reteral catheter Plmt nephrou reteral catheter Plmt nephrou reteral catheter Convert nephros tomy catheter Convert nephros tomy catheter Incise & drain bladder Drain bl wcath insertio n Cystosc opy & ureter catheter Cystosc opy & ureter catheter Cystosc opy J 7 2 J 7 2 J 7 J 7 J 7 J 7 J 7 22 J 7 22 J 7 2 J 7 7 J 7 2 opy & ureter catheter Cystosc opy and treatme nt Plmt nephros tomy catheter Plmt nephrou reteral catheter Exchang e nephros tomy cath Convert nephros tomy catheter Exchang e nephros tomy cath Cystosc opy and treatme nt Cystosc opy and treatme nt Drain bl wcath insertio n Biopsy of prostate Drain bl wcath J 7 B 7 J 7 C 7 J 7 C 7 J 7 C 7 J 7 D 7 J 7 D 7 J 7 X 7 J 7 B 7 J 7 2E 7 J 7 2E 7 J 7 22D 7
92 wbiops y(s) Cystosc opy wbiops y(s) Cystosc opy wbiops y(s) Cystosc opy wbiops y(s) Cystosc opy and treatme nt Cystosc opy and treatme nt Cystosc opy and treatme nt Cystosc opy and treatme nt Cystosc opy and treatme nt Cystosc opy and treatme nt Cystosc opy and treatme nt J 7 2 J 7 7 J 7 C97 J 7 22 J J J 7 7 J 7 C97 J J insertio n Cystosc opy & ureter catheter Biopsy of prostate Blue light cysto imag agent Cystosc opy wbiops y(s) Cystosc opy and treatme nt Cystosc opy chemod enervati on Biopsy of prostate Blue light cysto imag agent Cystosc opy and treatme nt Cystosc opy chemod enervati on J 7 22D 7 J 7 22D 7 22D 7 J 7 22D 7 J 7 22D 7 J 7 22D 7 J 7 22D 7 22D 7 J 7 222D 7 J 7 222D Cystosc J 7 7 Biopsy J 7 222D 7
93 opy and treatme nt Cystosc opy and treatme nt Cystosc opy and treatme nt Cystosc opy and treatme nt Cystosc opy and treatme nt Cystosc opy and treatme nt Cystosc opy and treatme nt Cystosc opy and treatme nt Cystosc opy chemod enervati on Cystosc opy chemod enervati on Cystosc opy chemod enervati on J 7 C97 J 7 J 7 2 J 7 22 J 7 J 7 7 J J 7 J 7 2 J 7 2 of prostate Blue light cysto imag agent Incise & drain bladder Drain bl wcath insertio n Cystosc opy wbiops y(s) Circum 2 days or older Biopsy of prostate Cystosc opy and treatme nt Incise & drain bladder Drain bl wcath insertio n Cystosc opy & ureter catheter 222D 7 J 7 227G 7 J 7 227G 7 J 7 227G 7 J 7 227G 7 J 7 227G 7 J 7 22C 7 J 7 22Q 7 J 7 22Q 7 J 7 22Q 7
94 Cystosc opy chemod enervati on Cystosc opy chemod enervati on Cystosc opy chemod enervati on Cystour etero & or pyelosc ope Cystour etero & or pyelosc ope Cystour etero & or pyelosc ope Cystour etero & or pyelosc ope Circum 2 days or older Circum 2 days or older Circum 2 days or older Remove epididy J 7 22 J 7 22 J J 7 2 J 7 22 J 7 22 J J 7 22 J 7 J 7 7 J 7 Cystosc opy wbiops y(s) Cystosc opy and treatme nt Cystosc opy and treatme nt Plmt nephros tomy catheter Cystosc opy wbiops y(s) Cystosc opy and treatme nt Cystosc opy and treatme nt Cystosc opy and treatme nt Biopsy of penis Biopsy of prostate Repair of J 7 22Q 7 J 7 22Q 7 J 7 22Q 7 J J J J J 7 7 J 72 7 J 7 7 J 7 X 7
95 mis lesion Biopsy of prostate Cystosc opy and treatme nt Cystosc opy and treatme nt Prostate ctomy (turp) Insert uteri tandem ovoids Vaginal hysterec tomy Vag hyst includin g to Vag hyst wto & vag repair Vag hyst wto & vag repair Vag hyst wenter ocele repair Decomp ression of tibia nerve J 7 2 J 7 2 J 7 2 J 7 9 J 7 J 72 J 72 J 72 J 72 J 72 J 7 hydroce le Cystosc opy and treatme nt Plmt nephros tomy catheter Plmt nephros tomy catheter Prp ihern init reduc > yr Insert uteri tandem ovoids Repair bladder defect Repair bladder defect Cmbn ap colprhy wntrcl rpr Repair bladder defect Repair bladder defect Revise handfo ot nerve J 7 7X 7 J 7 2B 7 J 7 22X 7 J 2 7 J 7E J 2X J 2B J 2C J 2C J 27X J 2E 2 7 Revise J 2 Decomp J 7R 2
96 armleg nerve Revise armleg nerve Revise armleg nerve Glauco ma surgery Repair retinal detach cplx Revise eye muscle Revision of eyelid Correcti on eyelid wimpla nt Correcti on eyelid wimpla nt Correcti on eyelid wimpla nt Correcti on eyelid wimpla nt Revision of eyelid J 7 J 7 J 9 9 J J 7 J 7 J 79 J 792 J 797 J 79 J 79 ression of tibia nerve Revise armleg nerve Revise ulnar nerve at elbow Cataract surg wiol stage Cataract surgery complex Revise eye muscle Revision of eyelid Repair brow defect Correcti on eyelid wimpla nt Repair eyelid defect Revision of eyelid Revision of eyelid J 7R 2 J 7R 2 J 9 X 92 J 9 7C 9 J 7D J 7X J 79B J 79B J 79B J 79B J 79X
97 Revision of eyelid Reconst ruction of eyelid Reconst ruction of eyelid Remove eyelid lining lesion Intro cath dialysis circuit Intro cath dialysis circuit Thrmbc nfs dialysis circuit Thrmbc nfs dialysis circuit J 79 J 79 J 79 J J 92 9 J 9 9 J 92 9 J 9 9 Revision of eyelid Revision of eyelid Revision of eyelid Remove eyelid lining lesion Stent plmt ctr dialysis seg Stent plmt ctr dialysis seg Stent plmt ctr dialysis seg Stent plmt ctr dialysis seg J 79X J 797 J 797 J X 9B 9 9C 9 9D 9 9E 9 Status Indicator J2 Status indicator J2 describes a second type of comprehensive PC. It is specific to observation billing and follows the following logic. Status indicator J2 will be paid instead of other status indicatorscodes on the bill, except those excluded by law, in the following situation: The claim does not contain a procedure assigned status indicator T on the same date of service or the previous day; The claim contains eight or more units of service of HCPCS code G7, Observation services per hour; The claim does not contain services described by a code assigned status indicator J; and
98 The claim contains one of the following on the same date of service or the previous day:» Code G79, Direct Referral of patient for hospital observation care, provided on the same date of service as G7;» ny emergency department visit code ( or G-G);» CPT code 9929, Critical care, evaluation and management of the critically ill or critically injured patient - first -7 minutes; or» HCPCS code G, Hospital outpatient clinic visit for assessment and management of a patient, provided on the same date of service or the previous day with G7. When these criteria are met, a single payment will be made based on C-PC (comprehensive observation services). If there is a procedure code assigned status indicator T on the claim on the same date of service or the previous day, that procedure code will be reimbursed instead of the C-PC. If there is a procedure code assigned status indicator J on the claim, that procedure will be paid and other services bundled following the status indicator J logic. Status Indicator K on-pass-through drugs, non-implantable biologicals, and therapeutic radiopharmaceuticals are assigned to status indicator K and are reimbursed under the HOPPS with a separate PC payment. Status indicator K includes brachytherapy sources. Status Indicator Procedure codes that are assigned to status indicator are procedures that are not performed alone. Examples of this areselective catheter placements, which are only done with another procedure, all radiological guidance codes, and all add-on codes. Since they are incidental to another procedure, their reimbursement has been included in the other procedure, and there is no separate reimbursement by Medicare. It is still important to properly code these procedures in spite of the fact that there is no payment. One other idiosyncrasy of status codes is that they cannot be billed alone. Status Indicators Q and Q2 Status indicators Q and Q2 designate procedures that are conditionally bundled. In contrast to status indicator, procedure codes assigned Q and Q2 may be reimbursed separately. It all depends on what other procedures are reported on the same claim. Status indicator Q results in packaging reimbursement (not paying separately) for the procedure it is assigned to if there is another procedure on the claim that is assigned status indicator J, J2, S, T, or V. The procedure assigned the Q status indicator is bundled into these other procedures. If there is no other procedure on the bill with a status indicator of J, J2, S, T, or V, the Q status indicator procedure is reimbursed. If there is more than one status indicator Q procedure on the bill, only the one assigned the highest reimbursed PC will be reimbursed. The others will be packaged. Status indicator Q2 is similar to Q; it is conditionally packaged, but only with status indicator J, J2, and T procedures. Status indicators S and V do not result in packaging the payment for the Q2 procedures. If there are procedures assigned
99 status indicators Q and Q2 on the claim, only one will be reimbursed. The other will be packaged. Status Indicator Q Status indicator Q designates procedures that are part of a composite PC. composite PC is a single payment that is made when certain combinations of procedures are reported on the same claim. The individual procedures are not reimbursed; there is a flat payment for all procedures. Most complex imaging procedures [ultrasound (US), computed tomography (CT), and magnetic resonance imaging (MRI)] are included in composite PCs. When multiple CT procedures are reported on a single claim, each procedure is not reimbursed separately; a single payment is made for two or more procedures. Status Indicator S Procedures assigned to status indicator S are procedures that are not subject to multiple procedure discounting. When multiple status indicator S procedures are performed, each procedure will be reimbursed at % of the PC amount for the procedure. Status Indicator T Procedures that are assigned to status indicator T are surgery codes that are subject to discounting when multiple status indicator T procedures are performed in the same session. The first status indicator T code is paid at % of the PC payment rate. Each additional status indicator T code is paid at % of the PC payment rate. CPT codes 7-7 (venous sclerotherapy) are status indicator T codes and are subject to discounting. If bilateral venous sclerotherapy is performed on an outpatient Medicare patient, the payment would be % of the PC amount for one leg and % of the PC amount for the other leg. Status Indicator U Brachytherapy sources are assigned status indicator U. They have separate HOPPS payment. Code C2 (Y-9) is used for liver chemoembolization. Status indicator U sources do not bundle into the J status indicator; they are paid separately. Status Indicator V Status indicator V is assigned to emergency room and other clinic room charges. It denotes a medical visit. Evaluation and Management (EM) CPT codes are assigned status indicator V. The significance of status indicator V to interventional radiology is that when a procedure assigned status indicator V, such as an emergency room visit, is billed on the same date as CPT codes assigned status indicator Q (S, T, V, or X packaged), the procedure(s) assigned status indicator Q will not be paid separately. MEDICL DEVICES PROVIDED T DISCOUT FROM THE VEDOR Medicare has a classification of procedures called "device-intensive". These are procedures that have over % of the PC payment attributed to the cost of the device used (stent, catheter, generator, lead, etc.). When these devices are provided by the vendor at no cost or at a % or more reduction in cost to the hospital, the hospital must enter the exact amount of the discount received on the UB- claim form. value code has been created, "FD" (Credit Received from the Manufacturer for a Replaced Medical Device), that is used to indicate there was a discount. The exact amount of the discount is included in the field next to the value code field. The PC payment will be reduced by the actual amount of the discount with one
100 exception. If the discount is more than the established amount CMS has determined to be the actual device component of the PC (the device offset amount), the reduction in PC payment will be at the offset amount instead of the amount the hospital saved. Example : femoral artery stent placement is performed with a stent that is provided to the hospital at a % discount. The stent cost is normally $,. The hospital is rebated % of the stent cost. Value code FD would be put in the appropriate field (9,, or ) on the UB- with 2. in its associated dollar field. The national PC payment for the femoral artery stent placement (722) is $,9.72. The device offset for code 722 is 7.%. The amount of the offset (7.% of $,9.72) is $,99.2. Since the rebate was less than the device offset amount, payment will be reduced by $2, (the discounted amount). Example 2: tunneled central venous catheter is placed using a catheter that is provided to the hospital at no cost. The catheter would normally cost $, but is provided to the hospital for free. Value code FD would be put in the appropriate field on the UB- with. in its associated dollar field. The national PC payment for code is $2,92.7. The device offset for code is.99%. The amount of the offset (.99% of $2,92.7) is $,.. Since the offset amount is less than the actual amount the hospital saved, the payment will be reduced by the offset amount of $,.. Refer to ddendum P of Hospital Outpatient Prospective Payment - Final Rule with Comment and Final CY2 Payment Rates (published by CMS) for a list of procedures that are designated as device-intensive and subject to reporting the FD value code when a % or greater discount or rebate of the cost of the device is received. LL PC RTES RE OT CRETED EQUL While CMS publishes a table of PC payment rates each year, these published rates are not what you are actually reimbursed from Medicare when that code is billed. While equipment and supply costs are relatively consistent across the nation, labor costs vary greatly by city and state. To recognize the difference in the cost of labor, the PC national rate is subject to a wage index adjustment based on your specific location. The wage index is published each year and is implemented on October for inpatient payment (DRGs) and on the following January st for outpatient procedures. Since wages only affect part of the cost of doing a procedure, the wage index is only applied to % of the PC payment rate, with the remaining % paid standard to all facilities. DEVICE EDITS Medicare has implemented code edits for some procedure codes. s long as a C-code for any device that was previously involved in any edit is on the claim with the device-dependent procedure, the edit is satisfied. Hospitals have enough experience with the specific device edits that CMS believes they will report the devices correctly. See ppendix D for the device codes that are in place as of October, 27. ote that not all device codes will satisfy the device code edit. Only a certain subset has been included in the edits.
101 TRDITIOL PSS-THOUGH PYMETS On occasion there are medical devices and drugs that will receive separate payment under HOPPS. These are new devices and new drugs that have costs that weren't considered when rate-setting was performed for the PCs. These items are paid at cost to the facility, using the hospital's cost-to-charge ratio. The additional payment will be allowed until the device or drug cost is phased into the procedure reimbursement. The device or drug will then change to a bundled status. There are some drugs that are not considered pass-through drugs, but are paid separately due to other Medicare policies or laws. These include drugs for immunotherapy, chemotherapy, and infusion therapy. These drugs are reported with HCPCS codes starting with an or J and are paid on a fee schedule basis. KEEP TRCK OF THE DTE CMS revises PC payment rates and wage indexes annually. s such, make sure you have the appropriate information based on the date of service when trying to predict payment. The key dates or time-frames for important updates to be aware of include the following: Wage Indexes - October for inpatient (DRGs), January for outpatient (PCs) PC Payment Rates - January CPT Codes - January for Category I CPT codes, January and July for Category III CPT codes HCPCS Level II Codes - Can change at any time, but there are usually revisions on a quarterly basis Modifiers - Can change at any time OCE (CCI Edits) - Each quarter 2-2 ZHealth Publishing. ll rights reserved. CPT Only 27 merican Medical ssociation. ll rights reserved. Basic Interventional Radiology Coding Rules Basic Interventional Radiology Coding Rules Pages: -92 Interventional radiology procedures explained in this manual are those imaging procedures that involve placing a catheter, needle, tube, wire, or other device into the body to inject contrast material or to perform a therapeutic procedure. They are done under sterile conditions and are usually performed by a physician. They are typically performed in the endovascular suite, the radiology department, the cardiac catheterization lab, the operating room, the pain clinic, or the nephrology lab. These procedures span a wide spectrum of complexity from performing a simple biopsy to placing an aortic stent graft. WHT ROLE DOES DOCUMETTIO PLY I BEIG PID PPROPRITELY? manual on interventional radiology cannot be considered complete without referencing physician documentation. If a procedure is not sufficiently documented
102 in the physician's report, it is not considered reimbursable by Medicare or other insurance companies. Therefore, it is essential that complete and accurate documentation be a priority. Documentation must be in written format. Having archived images is not documentation in this context. There are typically two components to an interventional radiology procedure: the imaging procedure and the surgical procedure or intervention performed. It is important that the physician fully document each of these components. Each additional procedure performed must also be documented. There should be chronological order to the report since the timing of when one procedure is performed compared to another may determine whether or not it can be separately coded. While there is not a standard format for interventional radiology reports, the following components must be included: ngiography Clinical indications, medical necessity, and history Prior diagnostic CT, MR, or catheter-based angiography; reason for repeat diagnostic catheter-based angiography (if done) ccess site(s) Route of catheter(s) with ending position of catheter tip Injection sites for imaging natomy imaged with documented interpretation (the I of S&I), with documentation of exact location, % stenoses, and presence of occlusions Site of and type of interventions performed along with any complications and subsequent interventions Method of hemostasis at access site Clinical findings on-vascular Interventions Clinical indications, medical necessity, and history Site of intervention Type of device used (fine needle, catheter, etc.) Type of intervention performed Injection sites natomy imaged Final disposition (was the catheter removed or left in place) Clinical findings Physician documentation is an important building block in establishing a strong foundation for accurate coding and Medicare compliance. THERE RE SOMETIMES TWO DISTICT COMPOETS TO ITERVETIOL RDIOLOGY PROCEDURES Interventional radiology coding is different from other procedure coding in that there are usually two distinct components to an interventional procedure. The interventional radiology coding system is comprised of imaging (radiological S&I) codes from the 7 section of the CPT Codebook and codes from the surgical section of the CPT Codebook (-9999) (with a few Level II HCPCS and CPT Category III code exceptions). The imaging codes describe the work of taking x-rays,
103 performing image guidance, and the processing and interpreting of images. The surgical codes describe the work of actually performing the intervention, such as inserting catheters or needles, inflating balloons, deploying stents, etc. The surgical procedure codes describe what the physician does. There is a technical component of payment assigned to them for hospitals, as they consume hospital resources such as personnel and supplies. The rules for the two components are very different. Some codes have been created that bundle both components into a single code. Examples include gastrointestinal tubes, urologic intervention, TIPS, lower extremity endovascular revascularization, diagnostic renal angiography, vena cava filters, diagnostic cervicocerebral angiography, chest drainage procedures, vascular embolizations, vascular stent placement, abscess drainage procedures, breast interventions, and many spine interventions (e.g., kyphoplasty). ITERVETIOL RDIOLOGY PROCEDURE CODIG RULES Interventional radiology procedures are subject to complex coding rules. Some of the time there is a one-to-one correlation between the surgical code and the imaging code, as seen with therapeutic procedures such as venous angioplasty, renal angioplasty, etc. In other cases, there is no correlation (e.g., catheter placements). In addition, the rules of application for the two sets of codes are very different. Therefore, the two sets of codes will be discussed separately. Imaging codes are the least complex of the two. Imaging codes are based on the vessel or vascular system imaged. There must be images taken and dictation regarding the findings to support coding the procedure. The imaging procedure must have contributed to the study and not be incidental, such as performing a left vertebral angiogram from a subclavian injection and then commenting on the internal mammary artery which was incidentally seen and described without a clinical justification. Codes cannot be submitted for re-filming performed as a result of inadequate imaging or for oblique imaging from the same catheter position. If, however, the catheter is moved more selectively to better image a more distal vessel after an initial complete study was performed, then it may be coded separately. In most other instances, if an area is imaged intentionally with medical necessity and findings discussed, an imaging code can be submitted. The most recent trend by the M is to create "all-inclusive" CPT codes that bundle all of the component codes into one code. Examples are lower extremity revascularization, selective renal and cervicocerebral arteriography, and IVC filter placement. Close attention must be paid to the CPT code description to determine what services are bundled. Example(s): catheter is placed in the right femoral artery. It is advanced to the ascending aorta (2). Contrast is injected, and imaging of the descending thoracic aorta (7) is performed. The catheter is pulled down to the L2 level. Contrast is injected, and imaging of the abdominal aorta is performed (72). The catheter is removed. In the example above, two areas are imaged and separately coded. However, there is only one catheter placement. Movement of the catheter in a vessel does not allow additional catheter placement coding. In most cases, the catheter does not need to be selectively positioned in the vessel imaged to code for the imaging of that vessel. There are, however, several codes that are specifically described as requiring selective catheter placement before they can be coded. In order to use one of these
104 codes, the catheter tip must be placed within that vessel or one of its branches. See the following table for a list of arterial and venous selective-only codes. detailed discussion of the use of the imaging codes for vascular procedures can be found in Chapters and 7. TBLE - IMGIG PROCEDURES THT MUST BE DOCUMETED S SELECTIVELY PERFORMED CP T C O D E DESCRIPTIO Selective catheter placement, common carotid or innominate artery, unilateral, any approach, with angiography of the ipsilateral extracranial carotid circulation and all associated radiological supervision and interpretation, includes angiography of the cervicocerebral arch, when performed Selective catheter placement, common carotid or innominate artery, unilateral, any approach, with angiography of the ipsilateral intracranial carotid circulation and all associated radiological supervision and interpretation, includes angiography of the extracranial carotid and cervicocerebral arch, when performed Selective catheter placement, internal carotid artery, unilateral, with angiography of the ipsilateral intracranial carotid circulation and all associated radiological supervision and interpretation, includes angiography of the extracranial carotid and cervicocerebral arch, when performed Selective catheter placement, subclavian or innominate artery, unilateral, with angiography of the ipsilateral vertebral circulation and all associated radiological supervision and interpretation, includes angiography of the cervicocerebral arch, when performed Selective catheter placement, vertebral artery, unilateral, with angiography of the ipsilateral vertebral circulation and all associated radiological supervision and interpretation, includes angiography of the cervicocerebral arch, when performed Selective catheter placement, external carotid artery, unilateral, with angiography of the ipsilateral external carotid circulation and all associated radiological supervision and interpretation (List separately in addition to code for primary procedure) Selective catheter placement, each intracranial branch of the internal carotid or vertebral arteries, unilateral, with angiography of the selected vessel circulation and all associated radiological supervision and interpretation (eg, middle cerebral artery, posterior inferior cerebellar artery) (List separately in addition to code for primary procedure) Selective catheter placement (first-order), main renal artery and any accessory renal artery(s) for renal angiography, including arterial puncture and catheter placement(s), fluoroscopy, contrast injection(s), image postprocessing, permanent recording of images, and radiological supervision and interpretation, P C TO T L RV U
105 including pressure gradient measurements when performed, and flush aortogram when performed; unilateral Selective catheter placement (first-order), main renal artery and any accessory renal artery(s) for renal angiography, including arterial puncture and catheter placement(s), fluoroscopy, contrast injection(s), image postprocessing, permanent recording of images, and radiological supervision and interpretation, including pressure gradient measurements when performed, and flush aortogram when performed; bilateral Superselective catheter placement (one or more second order or higher renal artery branches) renal artery and any accessory renal artery(s) for renal angiography, including arterial puncture, catheterization, fluoroscopy, contrast injection(s), image postprocessing, permanent recording of images, and radiological supervision and interpretation, including pressure gradient measurements when performed, and flush aortogram when performed; unilateral Superselective catheter placement (one or more second order or higher renal artery branches) renal artery and any accessory renal artery(s) for renal angiography, including arterial puncture, catheterization, fluoroscopy, contrast injection(s), image postprocessing, permanent recording of images, and radiological supervision and interpretation, including pressure gradient measurements when performed, and flush aortogram when performed; bilateral ngiography, spinal, selective, radiological supervision and interpretation ngiography, visceral, selective or supraselective, (with or without flush aortogram), radiological supervision and interpretation ngiography, adrenal, unilateral, selective, radiological supervision and interpretation ngiography, adrenal, bilateral, selective, radiological supervision and interpretation ngiography, pelvic, selective or supraselective, radiological supervision and interpretation ngiography, pulmonary, unilateral, selective, radiological supervision and interpretation 7 ngiography, pulmonary, bilateral, selective, radiological supervision and
106 interpretation ngiography, selective, each additional vessel studied after basic examination, radiological supervision and interpretation (List separately in addition to code for primary procedure) Venography, renal, unilateral, selective, radiological supervision and interpretation Venography, renal, bilateral, selective, radiological supervision and interpretation Venography, adrenal, unilateral, selective, radiological supervision and interpretation Venography, adrenal, bilateral, selective, radiological supervision and interpretation For the surgical procedure portion of interventional vascular procedures, there are four different systems: arterial (most complex), venous, pulmonary, and portal. The arterial system is the most complex. Catheter Placements There are two separate kinds of catheter placements: non-selective and selective. non-selective placement is when the catheter stays in the vessel entered or only advances to the aorta or vena cava. Selective catheter placement codes are used when the catheter advances from the vessel entered or from the aorta or vena cava into a branch vessel. Regardless of the approach (from the arm or leg) once the aorta or vena cava is entered and a branch is selected, a selective catheter placement code must be used and the non-selective catheter position is included. The selective catheter placement codes follow a logical hierarchy. Selective catheter placements are assigned by vascular family. vascular family is a vessel that arises from the vessel entered, the vena cava, or the aorta and includes all of the branches of that branch vessel. For example, if you approach the great vessels through the aorta, there are normally three vascular families: the brachiocephalic, the left carotid, and the left subclavian. Each vascular family is coded independently. s the selective vessel begins to branch, the codes become more selective. The initial segment of the vessel is considered a first order, the second distinct segment or branch is considered a second order, and the third branch is considered a third order. ny branch higher than a third order is also coded as a third order or additional second or third order. If you had to go through a section of a vessel to get to a more selective vessel, the catheter placement in the initial vessel is included in the higher order selection. s a rule of thumb, a second order includes all first order
107 placements and any non-selective placements along the path. third order includes all first, second, and non-selective placements along the path. RTERIL SYSTEM CTHETER PLCEMETS See the following table for a list of non-selective arterial catheter placements: CPT CODE DESCRIPTIO Introduction of catheter, right heart or main pulmonary artery Introduction of needle or intracatheter, carotid or vertebral artery Introduction of needle or intracatheter, upper or lower extremity artery Introduction of needle or intracatheter, aortic, translumbar 2 Introduction of catheter, aorta The arterial selective catheter placement codes are further differentiated between vessels above the diaphragm and vessels below the diaphragm. CPT codes 2-2 describe placements above the diaphragm and 2-2 describe placements below the diaphragm. See the following table for a list of selective arterial catheter placements: CP T C O DE DESCRIPTIO Selective catheter placement, arterial system; each first order thoracic or brachiocephalic branch, within a vascular family Selective catheter placement, arterial system; initial second order thoracic or brachiocephalic branch, within a vascular family Selective catheter placement, arterial system; initial third order or more selective thoracic or brachiocephalic branch, within a vascular family Selective catheter placement, arterial system; additional second order, third order, and beyond, thoracic or brachiocephalic branch, within a vascular family P C Selective catheter placement, arterial system; each first order abdominal, pelvic, or lower extremity artery branch, within a vascular family TOTL RVU P C TO T L RV U
108 Selective catheter placement, arterial system; initial second order abdominal, 2 pelvic, or lower extremity artery branch, within a vascular family Selective catheter placement, arterial system; initial third order or more selective abdominal, pelvic, or lower extremity artery branch, within a vascular family Selective catheter placement, arterial system; additional second order, third order, and beyond, abdominal, pelvic, or lower extremity artery branch, within a vascular family If a second access site is used, the coding starts over again from that access site following the same rules. DO'S D DOT'S WHE CODIG RTERIL CTHETER PLCEMETS:. Do code to where the tip of the catheter is.. Do code each individual vascular family separately with the same rules using modifiers as necessary. 7. Do use codes 2-2 for selections above the diaphragm and 2-2 for selections below the diaphragm, unless selective catheter placements are for diagnostic renal or cervicocerebral angiography, carotidvertebral stent placements, or lower extremity endovascular revascularization. (n exception is that code 2 can be used with codes 22 and 22 in certain circumstances.). Do code each approach from a different access site separately. 9. Do code the aorta placement (2) instead of other non-selective codes if the aorta has been entered.. Do use code 2-2 for unilateral or bilateral selective or superselective renal angiography. These codes include catheter placements, renal S&I, accessory renal catheter placements and S&I, non-selective abdominal aortography, D reconstructions, and pressure gradient if obtained.. Do use codes for selective or superselective cervicocerebral angiography. These codes include catheter placements; cervical carotid, cerebral carotid, vertebral, intracranial, and external carotid supervision and interpretation, as well as non-selective arch aortography. Catheter placements may be used to describe additional vessels selected arising off the subclavian arteries at the same session as 22 or Do not use code for pullback of the catheter from the aorta or contralateral iliac into the ipsilateral iliac for extremity imaging of the ipsilateral leg
109 . Do not code imaging codes for injecting small amounts of contrast to localize a vessel for subsequent selection.. Do not code for reforming catheters.. Do not include a non-selective catheter placement code once a vessel coming off of the non-selective vessel has been selected, as it is included.. Do not code for non-selective catheter placement used for embolization codes Do not code the access site separately once a catheter through the sheath has reached the aorta or selected another vessel.. If there are three vascular families selected above the diaphragm, there should only be three initial vessel codes (2, 2, or 27), no matter how many vessels in those vascular families are selected. The other additionally selected vessels would be 2 codes. 9. Do add -9 modifier to any above diaphragm catheter placement equal to or below the most selective catheter placement code. 2. Do not use - modifier on above diaphragm catheter placement codes. 2. Some procedures bundle catheter placements (e.g., TIPS, carotid stent placement, femoralpopliteal angioplasty). Example(s): ) catheter is placed in the right femoral artery. It is advanced to the abdominal aorta (2). Contrast is injected, and imaging of the abdominal aorta is performed (72). The catheter is advanced into the left common iliac artery (add 2, delete 2) and images taken of the entire left lower extremity to the foot (77). The catheter is then advanced into the left superficial femoral artery (add 27, delete 2), and additional images are obtained to further evaluate the tibial vessels (777). Catheter placement codes: 27 (left superficial femoral artery) (final placement includes lesser first order selection 2 and non-selective 2) Imaging codes: 72 (abdominal aorta), 77 (unilateral extremity), 777 (for the additional selective imaging of the tibial vessels) ote: In the example above the catheter placement in the aorta and in the left iliac artery are included in the catheter placement in the superficial femoral artery, since they both had to be traversed to get to the superficial femoral artery. 2) sheath and guidewire are placed in the right femoral artery (-9). The guidewire will not advance to the aorta. n injection of the right femoral artery through the sheath is performed showing occlusion of the right common iliac. Right
110 leg runoff angio is then completed. The right side is abandoned and access is gained through the left femoral artery. The catheter is advanced into the abdominal aorta at the L2 level (2). Contrast is injected, and imaging of the abdominal aorta is performed (72). The catheter is pulled down to L and left leg runoff done (77). Catheter placement codes: -9 (right-sided access), 2 (left-sided access) Imaging codes: 72 (abdominal aorta), 77 (bilateral runoff, one leg at a time) ote: In the above example both access sites are coded separately. If the right side access had resulted in advancement of the catheter to the aorta, it would also be assigned code 2-9. CODIG OF DDITIOL SECOD D THIRD ORDER SELECTIVE PLCEMETS There are two codes that describe the coding of each additional second order, third order, and beyond selective catheter placement in the same vascular family: 2 and 2. s vessels are traversed to get more selective, each lower level of selectivity vessel that is passed through is included in the final destination. Some vessels can only be selected by pulling the catheter back and going a different route in the same vascular family. This is where additional second or higher selective catheter position codes 2 and 2 apply. When there is additional work to get to a branch vessel after a second or third order selection has been performed, the "each additional" code should be used. Example(s): catheter is placed in the right femoral artery. It is advanced to the high abdominal aorta, and an aortogram is performed (2, 72). The catheter is placed in the celiac artery with contrast injection and imaging of the celiac distribution (add 2, 772; delete 2, 72). The catheter is advanced into the common hepatic artery for additional selective imaging (add 2, 777; delete 2). The catheter is withdrawn from the common hepatic artery and placed in the splenic artery for additional selective imaging (2, 777). Catheter placement codes: 2 (common hepatic), 2 (splenic) Imaging codes: 772 (celiac), 777 (common hepatic), 777 (splenic) ote: In the example above, both selections are in the same vascular family. One vessel selected (common hepatic) is coded with the specific code for that level of selectivity, and the other vessel (splenic) is coded with the "each additional" code. These vessels were the same level of selectivity, so either one can be the initial code. When the levels of selectivity are different, always code to the highest level of selectivity in a given vascular family regardless of the order that the vessels were selected. VEOUS SYSTEM CTHETER PLCEMETS
111 There are two main differences between coding catheter placements in the venous system and coding catheter placements in the arterial system: The vena cava takes the role of the aorta as the major non-selective vessel. There are only two selective codes instead of eight. See the following table for a list of the venous catheter placement codes: CPT CO DESCRIPTIO DE 2 Injection procedure for extremity venography (including introduction of needle or intracatheter) Introduction of catheter, superior or inferior vena cava Selective catheter placement, venous system; first order branch (eg, renal vein, jugular vein) Selective catheter placement, venous system; second order, or more selective, branch (eg, left adrenal vein, petrosal sinus) The venous system follows the same coding conventions as the arterial system. Once you enter the vena cava it takes precedence over any other non-selective vessel codes. Example(s): ) catheter is placed in the right femoral vein. It is advanced to the inferior vena cava (). Contrast is injected, and imaging of the inferior vena cava is performed (72). The catheter is advanced into the superior vena cava (no change). Contrast is injected, and imaging of the superior vena cava is performed (727). Catheter placement code: (vena cava) P C TOT L RVU.... Imaging codes: 727 (superior vena cavagram), 72 (inferior vena cavagram) ote: In the example above (as in the arterial system), this is considered one catheter placement, regardless of how many times the catheter is repositioned in the vena cava. The highest order selection that can be coded in the venous system is a second order, and it is designated as second order or higher. ny higher selective placements are also reported with the second order code (2). In addition, code 2 takes the place of the each additional second order or higher selective placement that is available for arterial coding. Each additional 2 would require a -9 modifier. 2) catheter is placed in the right femoral vein. It is advanced to the inferior vena cava. Contrast is injected, and imaging of the inferior vena cava is performed (, 72). The catheter is advanced into the left renal vein with contrast injection and imaging (add, 7; delete ). The catheter is advanced into the left ovarian vein with contrast injection and imaging (add 2, delete ). The
112 catheter is retracted and advanced into the left adrenal vein (add 2-9, 7) with contrast injection and imaging. Catheter placement codes: 2 (left ovarian vein), 2-9 (left adrenal vein) Imaging codes: 72 (inferior vena cavagram), 7 (selective unilateral renal), 7 (selective unilateral adrenal) ote: The left adrenal and left ovarian are second order vessels and are reported with code 2. The catheter placement into the vena cava and main renal vein are bundled into the more selective 2 code. PULMORY CTHETER PLCEMETS Catheter placement in the pulmonary system is reported with three codes. See the following table for a list of codes describing pulmonary catheter placement: CPT CODE DESCRIPTIO Introduction of catheter, right heart or main pulmonary artery Selective catheter placement, left or right pulmonary artery Selective catheter placement, segmental or subsegmental pulmonary artery Pulmonary angiography performed non-selectively via the main pulmonary artery is reported with code. When performed selectively via the left or right pulmonary arteries, it is reported with code. When performed sub-selectively, each segmentalsubsegmental artery catheterized is reported separately with code. s in the other systems, the non-selective and lower selective codes are included in the higher selective codes. [Pulmonary arteries selected and imaged during a cardiac catheterization are described by a single cardiac code (9). Do not use codes - or during a cardiac catheterization procedure (9-9).] Example(s): catheter is placed in the right femoral vein. It is advanced through the inferior vena cava and into the right pulmonary artery (). Contrast is injected, and imaging is performed (77). The catheter is advanced into the upper segmental right pulmonary artery (add, delete ) with contrast injection and imaging (777). Catheter placement code: (right upper segmental artery) P C TOTL RVU..7.9 Imaging codes: 77 (unilateral pulmonary angiogram), 777 (for the additional selective imaging of the upper segmental right pulmonary artery)
113 ote: In the example above the right pulmonary artery catheter placement is not reported separately, as it is included in the more selective catheter placement of the segmental right upper lobe pulmonary artery. PORTL SYSTEM CTHETER PLCEMETS There is one code for catheter placement in the portal system: CPT CODE DESCRIPTIO Percutaneous portal vein catheterization by any method Code is used for all methods of access to the portal system. Once entered, any selective venous injections are coded with the previously described venous protocols (e.g.,, 2 for mesenteric venous selections). CODE THE FOUR VSCULR SYSTEMS SEPRTELY s previously described, there are four vascular systems: arterial, venous, pulmonary, and portal. Each of these systems is coded separately. For example, if an inferior vena cavagram is performed (-9, 72), followed by bilateral selective pulmonary angiography (-, 77), all four codes are submitted because they represent procedures performed in separate vascular systems. Even though the inferior vena cava was traversed on the way to the selective catheter placement in the pulmonary arteries, it is coded separately in this example. It is not coded separately if an inferior vena cava study was not performed. If a filter were deployed, code 79 would be used (codes -9 and 72 would be deleted, as code 79 bundles catheter placement and imaging for vena cava filter placement). In that case, only code would be submitted for the catheter placement(s). The same rule applies when crossing over from the venous system to the portal system. Even though the venous system was on the route to the portal system, each system is coded individually when imaging is done in both. If work is performed in each system, both sets of catheter codes may be used; however, if the one vascular system is used as an "approach" to another, only code for the system that is intentionally and purposefully evaluated (e.g., only code for access to the portal vein in a patient with a patent TIPS shunt; do not code for the peripheral venous access to the hepatic veinshunt, as no imaging was done in this region). CODE FOR CLOSURE DEVICE PLCEMET The CMS created HCPCS Level II codes G29 to describe the use of a closure device to assist in hemostasis for percutaneous vascular diagnostic and interventional studies. Many procedures now bundle closure device placement. Code G29 includes any angiography performed for evaluation of the vascular access site (to determine suitability of the vessel for device placement). partial list of currently available devices qualifying for use of code G29 includes ngio-seal, Boomerang, Closer S, Duett, EVS vascular stapling system, Exoseal, MPatch, Mynx, Perclose, ProGel, Prostar, Starclose, SuperStitch, and Vasoseal. dditional devices will certainly P C TOTL RVU 9.7
114 become available as technology continues to change. Skin or puncture site bandages and externally applied pressure devices do not qualify for use of code G29. Code G29 is typically not utilized for physician billing since there is no separate payment. 2-2 ZHealth Publishing. ll rights reserved. CPT Only 27 merican Medical ssociation. ll rights reserved. Diagnostic ngiography Coding Cervicocerebral ngiography Diagnostic ngiography Coding Cervicocerebral ngiography Cervicocerebral rch ngiography Pages: 99-2 Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: Cervicocerebral arch angiography involves placement of a catheter into the ascending aorta with imaging of the origin of the "great vessels" (right brachiocephalic, left carotid, and left subclavian) of the aorta at this level. This also includes complete imaging of the cervical and cerebral carotids and vertebrals if done. CLIICL IDICTIOS: For evaluation of the origins of vessels supplying the head, neck, and upper extremities. Cervicocerebral arch angiography may be performed on patients with atherosclerosis, stroke, TI, hemorrhage, neoplasm, or trauma. The arch may also be evaluated to determine the size and integrity of the ascending and transverse aorta and may be done in combination with the descending thoracic and abdominal aorta to evaluate aneurysm and dissection.
115 CODES: PROCEDURE DESCRIPTIO on-selective catheter placement, thoracic aorta, with angiography of the extracranial carotid, vertebral, andor intracranial vessels, unilateral or bilateral, and all associated radiological supervision and interpretation, includes angiography of the cervicocerebral arch, when performed PR OC CO DE 22 P C TO T L RV U. S &I C O D E CODIG ISTRUCTIOS: 22. To assist planning for cervical carotid stent placement, a classification was created to describe the amount of tortuosity (elongation) of the aortic arch and, subsequently, the degree of difficulty a physician may encounter during stent placement. The arch usually elongates over time in patients with hypertension and advanced age. Type I, II, III, and IV arches in this classification describe increasing amounts of tortuosity and subsequent complexity expected when performing carotid intervention. These descriptions of the arch do not change the coding for selective catheter placements for intervention (those that don't bundle catheter placement) or comprehensive codes Cervicocerebral arch angiography (22) is often performed in conjunction with procedure codes 222 (cervical carotid, unilateral), 22 (cervical and cerebral carotid, unilateral), 22 (selective internal carotid catheter placement with cerebral imaging, unilateral), and 2222 (vertebral angiography with catheter tip in the subclavianbrachiocephalic or the vertebral artery, respectively, unilateral). This procedure additionally serves as a guide for safe catheterization of vessels supplying the arms, neck, and face, and may show evidence of eccentric calcified plaque, proximal stenoses, aneurysm, and dissection. If performed with any of the procedures described by codes , it is bundled. Do not report code 22 when selective cervicocerebral or vertebral imaging procedures are also performed. 2. Code 22 is separately reported if cervicocerebral arch angiography is performed with upper extremity imaging procedures (77 and 77) (unless a procedure described by codes is additionally performed, which bundles code 22). 2. If more selective catheterization is performed from the same access site [e.g., right or left carotid from a femoral access site (222-22)], non-selective arch code 22 is deleted, as it is considered bundled with the selective procedure code. procedure performed via a second access site is coded separately and may require a modifier; however, if arch angiogram (22) is the additional procedure via a separate access, it is still bundled with codes lthough both the cervicocerebral arch and the descending thoracic aorta are in the thoracic cavity, physican documentation and verbiage may cause
116 confusion. The physician may call a cervicocerebral arch exam a "thoracic" aortogram (7) when evaluation of the arch and the origins of the great vessels was actually performed and documented. If this is the case, discuss the terminology and documentation with your physician and use code Code 22 is used to describe imaging related to evaluation of the origins and proximal portions of the blood supply to the head and neck (common carotid, brachiocephalic, subclavian, and vertebral arteries) and the ascending, transverse, and proximal descending portions of the thoracic aorta (the cervicocerebral cerebral arch). Imaging of the neck (carotid bifurcation) or head (intracranial vessels) performed via the same injectioncatheter position in the aorta is also bundled in code 22. Only if selective work is also performed does the coding change. 2. "ormal arch anatomy with patent common carotids, proximal subclavians with antegrade flow up both vertebrals, left side dominant" is typical documentation for an isolated diagnostic cervicocerebral arch exam (22). Do not code separately for carotid cervicals, subclavians, or vertebrals from this injection. 29. rch angiography (22) may be separately reported when performed at the time of a cervical carotid stent placement. The study must be a complete study and be diagnostic in nature (not just a "guiding" shot). Selective imaging of the ipsilateral carotid (222, 22, 22) is bundled with carotid stent placement and should not be separately billed. The contralateral carotid imaging can be billed with the appropriate modifier during carotid stent placement.. Variant anatomy is common in the aortic arch. This may affect subsequent selective catheter placement codes for neurointervention. natomic variants include a common origin of the right brachiocephalic and left common carotid artery, bovine arch (where the left common carotid artery arises from the right brachiocephalic artery as a branch vessel), aberrant right subclavian artery, direct origin of the left or right vertebral arteries off the arch, as well as various combinations of these.. Diagnostic cervicocerebral imaging procedures (22-22) include the catheter placement related to these procedures. 2. Cervicocerebral arch angiography is different from the cardiac "aortic root" evaluation (coded 97). ortic root injection and imaging is performed during cardiac catheterization for evaluation of the ascending thoracic aorta and "root", as well as aortic valvular disease. ortic root injection to evaluate the origins of the native coronary arteries or saphenous vein bypass graft origins is considered inherent to coronary angiography, and therefore code 97 is not submitted when aortic root injection is performed solely for this indication.. If, during a cardiac catheterization, the physician injects the aortic root to evaluate for aortic vascular disease, but also mentions the arch vessels (without medical necessity), do not report code 22, as the findings are incidental. There must be medical necessity to perform and charge for separate cervicocerebral arch diagnostic angiography. Use code 97 in this case.
117 EXMPLE(S): ) Patient presents with searing back pain and a possible aortic dissection. Via the transfemoral approach, the catheter is advanced to the ascending aorta (bundled). Contrast is injected with imaging of the arch (22), the descending thoracic aorta (7), and the abdominal aorta (72). This shows a type II aortic dissection. ote:catheter placement code 2 is bundled with code 22. 2) 2-year-old with Marfan's syndrome and chest pain. From a left radial approach, a French catheter is placed into the proximal ascending aorta (bundled) with contrast injection performed. Imaging of the aortic arch (22) and the descending thoracic aorta (7) shows a 7 cm aneurysm of the ascending aorta. The proximal great vessels appear uninvolved. The descending thoracic aorta is of normal size. ) Patient with gunshot wound to the upper chest and decreased left upper extremity pulses. From a transfemoral approach, a catheter is advanced into the proximal ascending aorta with injection and imaging of the cervicocerebral arch in multiple views (22). Questionable left subclavian narrowing is seen. The other proximal great vessels and arch itself appear unaffected. The left subclavian artery is selected, and diagnostic left upper extremity angiography is performed (2, 77-9). This demonstrates a cm pseudoaneurysm that compresses the native lumen of the left subclavian artery. wire is advanced across the lesion, followed by covered stent graft deployment (72). Follow-up angiography (bundled) demonstrates complete exclusion of pseudoaneurysm with resolution of the native subclavian lumen to a normal size. Upper extremity pulses return to normal.
 region. This includes the carotid bifurcation, where most atheromatous disease occurs.")
118 Diagnostic ngiography Coding Cervicocerebral ngiography Carotid Cervical ngiography Pages: - Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: Carotid cervical angiography involves imaging of the carotid vasculature in the cervical (or neck) region. This includes the carotid bifurcation, where most atheromatous disease occurs. This imaging may be performed selectively after placing catheters and injecting contrast into each common carotid artery or non-selectively after injection is made from a catheter in the ascending aortic arch. The imaging procedure may be unilateral or bilateral. Codes 222, 22, and
119 22 all include selective unilateral cervical carotid imaging. Selective cervical carotid imaging only (222, unilateral) includes catheter placement in the innominate or common carotid artery as well as images of the cervical portions of the common, external, and internal carotid arteries on one side to the level of the skull base. Images of the intracranial vessels are not included with code 222. CLIICL IDICTIOS: For evaluation of atherosclerotic carotid artery stenosis (primary or recurrent), stroke, TI, fibromuscular dysplasia (FMD), aneurysm, arteritis, dissection, and trauma. CODES: PROCEDURE DESCRIPTIO Selective catheter placement, common carotid or innominate artery, unilateral, any approach, with angiography of the ipsilateral extracranial carotid circulation and all associated radiological supervision and interpretation, includes angiography of the cervicocerebral arch, when performed PR OC CO DE 22 2 P C TO T L RV U. 2 S &I C O D E CODIG ISTRUCTIOS:. Code 222 is unilateral and includes selective catheter placement in the common carotid or innominate artery, as well as S&I of the cervical carotid.. Since there is not a bilateral code, use modifier - with code 222 for bilateral selective cervical carotid imaging (without cerebral imaging).. selective or non-selective approach may be taken. Bilateral cervical carotid imaging may be performed after selective catheter placements in the right brachiocephalic andor right and left common carotid arteries (222-) or from an arch injection with imaging of the neck (22). 7. Variant anatomy bovine arch changes selective transfemoral right and left common carotid catheter placement codes from 2-92 to 272 when coding for neurointervention only (without diagnostic imaging) from a femoral access. If for diagnostic imaging only or diagnostic imaging with neurointervention, the catheter placements are bundled, and variant anatomy does not affect the coding.. Use a -9 or -XS modifier for less selective catheter placements in separate and distinct vascular families when neurointervention is performed. 9. Do not append a - modifier to above diaphragm catheter placement codes 2, 2, 27, and 2.. Some neurointerventional procedures bundle the ipsilateral carotid or vertebral catheter placements. These include procedures described by codes 7T, 7T, 72, 72, 727, 72, 2,,,,, 2,,, and. Imaging of the ipsilateral cervical
120 and cerebral vessels is bundled with these procedures. (Exceptions to this include codes 2,,, and 2. For further details, see the "eurovascular Interventional Procedures" section.). Direct carotid punctures are rarely performed. When done, the catheter is usually advanced selectively (e.g., for patients with occluded common carotid requiring selective intracranial catheterization for complex cerebral VM embolization). Use code 727 for retrograde common carotid or brachiocephalic stent placement via open ipsilateral cervical carotid access. Code 727 bundles ipsilateral catheter placement and imaging. Common carotid stent placement is usually done via this open access at the time of an ipsilateral carotid endarterectomy (separately reported). 2. Description of the internal carotid artery is included in the selective unilateral "cervical" angiography code (222). Do not code cerebral angiography (22) for findings limited to the internal carotid artery. Code 22 requires imaging of the intracranial arteries.. ny above diaphragm selective catheter placement code (2, 2, or 27) equal to or less than the highest level of selectivity achieved by a catheter placement code in a separate vascular family requires a -9 or -XS modifier. (This only applies to carotidcerebral neurointervention not at the time of diagnostic cervicocerebral angiography.) EXMPLE(S): ) patient with carotid stenosis evident on Doppler has diagnostic angiography performed from a right femoral approach with catheter placement in the right common carotid artery and left common carotid artery with imaging of both carotid bifurcations (222-). The intracranial vessels are not evaluated. 2) Same patient, however, access is from the right brachial approach in patient with bovine arch. The injection is from the innominate artery with imaging of both cervical carotids (222-). ) Same patient, however, the imaging of the cervical carotids bilaterally is performed by an aortic arch injection (22), rather than selectively (any approach). ) Same patient with bovine arch, however, imaging of the cervical carotids is performed bilaterally after selecting the right common carotid and left common carotid arteries selectively from the right brachial approach (222-). ) Same patient with bovine arch, however, imaging of the cervical carotids is performed bilaterally after selecting the right common carotid and left common carotid arteries selectively from the left brachial approach (222-). ) Patient with symptomatic right internal carotid stenosis (high risk for carotid endarterectomy) on ultrasound presents for possible carotid stent. Diagnostic imaging via an arch injection (22) shows normal anatomy without proximal stenoses. This is followed by bilateral selective common carotid injections from a right femoral approach (add 222-, delete 22) with imaging of the carotid bifurcations showing 9% right proximal internal carotid artery stenosis and 2% left proximal internal carotid artery plaque. Based on these findings, the decision is made to place a stent. Right carotid stent is placed after embolic protection device deployment (add 72, delete modifier - from 222).
121 ote: The ipsilateral catheter placement and imaging are bundled on the side with stent placement. Code 222 is submitted for the evaluation of the non-stented left cervical carotid. Code 22 is bundled with selective left carotid imaging (222). If a diagnostic arch is performed without selective imaging with carotid or vertebral stent placement and it is diagnostic in nature, use code 22. 7) Via femoral approach, selective right common carotid catheter placement and cervical carotid imaging are performed (222). The left common carotid is unable to be selected due to origin plaque, so the left cervical carotid is imaged via a cervicocerebral arch injection (no additional code, as the right-sided selective code 222 includes an arch, even though the arch imaging also includes the left carotid). Carotid cerebral angiography
122 Diagnostic ngiography Coding Cervicocerebral ngiography Carotid Cerebral ngiography Pages: -9 Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: Carotid cerebral angiography involves imaging of cerebral vasculature supplied by the carotid arteries. This is a non-selective imaging procedure code, but is usually performed selectively by injection of the common carotid artery (CC) or internal carotid artery (IC). This procedure may be unilateral or bilateral, and may or may not be done with arch and carotid cervical imaging. CLIICL IDICTIOS: For evaluation of stroke, TI, aneurysm, V malformation, neoplasm, fistula, vasculitis, intracerebral or subarachnoid hemorrhage. CODES: PROCEDURE DESCRIPTIO Selective catheter placement, common carotid or innominate artery, unilateral, any approach, with angiography of the ipsilateral intracranial carotid circulation and all associated radiological supervision and interpretation, includes angiography of the extracranial carotid and cervicocerebral arch, when performed Selective catheter placement, internal carotid artery, unilateral, with angiography of the ipsilateral intracranial carotid circulation and all associated radiological supervision and interpretation, includes angiography of the extracranial carotid and cervicocerebral arch, when performed PR OC CO DE P C TO T L RV U S &I C O D E
123 Selective catheter placement, each intracranial branch of the internal carotid or vertebral arteries, unilateral, with angiography of the selected vessel circulation and all associated radiological supervision and interpretation (eg, middle cerebral artery, posterior inferior cerebellar artery) (List separately in addition to code for primary procedure) dd-on Code CODIG ISTRUCTIOS:. Diagnostic selective cerebral angiography codes 22 and 22 are unilateral procedure codes. They describe imaging of the intracranial vessels and include the selective catheter placements.. Use modifier - for bilateral procedures (22- or 22-).. rch angiography (22), bilateral selective carotid cervical angiography (222-), and bilateral selective vertebral (22-) angiography are commonly performed at the same time as carotid cerebral angiography (22- or 22-). (Please refer to guidelines below, as only one code from and one code from can be submitted per side per encounter, and code 22 is bundled with codes ) 7. Because the diagnostic carotid and cerebral codes are built on a hierarchy, only one code from can be submitted per side (22 > 22 > 222 > 22).. The arch is not always performed. Codes include an arch study if performed. These codes can be submitted even if an arch exam is not performed or not documented. 9. Documentation may discuss the intracerebral vasculature, the intracranial vessels, or the anterior and middle cerebral arteries as verification that carotidcerebral angiography was performed. "ormal" is a diagnostic finding. Complete studies often include capillary phase imaging and venous phase imaging of the draining cerebral veins and sinuses. There is no additional code for including these descriptions.. Carotid cerebral angiography may not be used for the evaluation of the "internal carotid" artery. Rather, it is intended for the evaluation of the intracranial branches of the internal carotid artery. The "internal carotid" is part of "carotid cervical" code Unilateral cerebral angiography (22 or 22) may be performed as part of an intracranial aneurysm follow-up exam (often performed three to six months following embolization). 2. The right and left common carotid arteries arise from the same vascular family when there is a bovine arch. The right carotid selection is a third order selective catheter placement, and the left carotid selection becomes a
124 second order selective catheter placement. When both are selected from a transfemoral approach, codes 27 (third order or higher) and 2 (additional second, third order, or higher) are used. This pertains to neurointervention without diagnostic imaging.. Do not code cerebral angiography for commenting on "asymmetric flow into the intracranial vessels" or "carotid run-off is normal". This does not qualify as a diagnostic cerebral angiogram. Diagnostic cerebral angiography usually includes venous phase imaging.. Do not use code (direct carotid puncture) when the selective catheter placement for neurointervention is performed from a femoral or brachial access. The procedure described by code is rarely performed; it is appropriate only when a catheter or needle is placed directly through the skin of the neck into the carotid artery for local intervention. If the physician places the catheter directly into the cervical carotid and then selects the aorta, use code 2 to describe the most selective catheter position obtained via that access. Remember that stent placement codes 72, 72, 727, 72, 7T, and 7T bundle catheter placements (including ). If the physician has open access to the cervical carotid artery (usually associated with an endarterectomy), places a catheter into the thoracic aorta, and then places a common carotid or brachiocephalic artery stent, code 727 includes the catheter placement to perform the procedure (e.g., or 2 is bundled). If the physician accesses the cervical carotid artery directly () and then selects an intracranial branch for intervention (usually embolization) from this access, use the appropriate above diaphragm selective codes (2, 2, 27, 2) to describe these more selective catheter placements (and delete ).. dditional intracranial catheter placements and imaging are described by code 22, which can be reported up to two times per side for a maximum of four times total. Code 22 can be used once for selection and imaging of the middle cerebral artery and all of its branches and once for selection and imaging of the anterior cerebral artery and all of its branches. Other selective IC branches that qualify for code 22 include the opthalmic, posterior communicating, and meningohypophyseal trunk arteries. Code 22 also applies to branches of the vertebral andor basilar arteries (e.g., opthalmic artery, MC, C, meningohypophyseal trunk, IC, PIC, superior cerebellar artery, posterior cerebral artery, posterior communicating artery).. Do not use above diaphragm selective catheter placement codes 2-2 when selective diagnostic cervicocerebral angiography is performed (as catheter placements are bundled with codes 22-22) unless the catheter placements are in vessels used to image the non-cervicocerebral vascular distribution (e.g., right brachial artery for upper extremity imaging, 27), for bronchialintercostal artery selection off the descending thoracic aorta (e.g., 2, 2), or for selection of vessels off the subclavian artery to further image the shoulder and neck. Code 2 is an add-on code to 22 and 22 used for selection of these branches off the subclavian artery and include the thyrocervical trunk, costocervical trunk,
125 and their branches. dditional selective imaging code 777 is also submitted for selective imaging of these branches. 7. Submit selective catheter placement codes 2-2 as appropriate for neurointerventional procedures performed not at the time of diagnostic studies. This excludes neurointerventional procedures that bundle ipsilateral catheter placement codes (7T, 7T, 72, 72, 727, 72, 2,,,,, 2,,, and ).. Code 22 is an add-on code to selective common and internal carotid codes for cerebral imaging (22, 22) and selective vertebral imaging codes (22, 22). 9. If different levels of catheter selection or imaging are performed on the right and left sides, use a modifier on the lower level code [e.g., use codes 22-9 (or -XS) and 22 to describe right CC catheter placement with cerebral imaging and left IC catheter placement with cerebral imaging]. EXMPLE(S): ) -year-old patient with carotid stenosis on ultrasound. Via the right brachial approach, a catheter is advanced into the aorta, then selectively into the right and left common carotid arteries with injection of contrast and imaging of the intracranial vasculature and the cervical carotid bifurcations (22-). ote: rch (22) is not performed in this example. If performed, it is bundled with code 22 and is not separately reported. 2) 7-year-old male, status-post coil embolization of right middle cerebral artery aneurysm one year ago. Recurrent symptoms of headache. Via the left femoral approach, a catheter is advanced to the right common carotid artery, and unilateral carotid cervical angiography shows % proximal IC stenosis (222). Catheter is advanced into the right internal carotid artery, and unilateral carotid cerebral angiography (add 22, delete 222) shows recanalization of the aneurysm. s treating physician, the neurointerventionalist performing this procedure does angiography with D reformatting on an independent workstation to fully evaluate the aneurysm (777). Patient will return in two weeks for repeat embolization. Diagnostic ngiography Coding Cervicocerebral ngiography Vertebral ngiography Pages: - Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: The right and left vertebral arteries unite to form the basilar artery that supplies the posterior fossa (back of brain, cerebellum, and brainstem). They usually arise from the subclavian arteries. Five percent of the time, variant anatomy consists of the left vertebral artery arising directly off the aorta, between the left subclavian and left common carotid artery. The procedure codes are non-selective (22) or selective
126 (22 or 22). Imaging is usually done by selective catheter injection of the subclavian or vertebral arteries. The vessels may be imaged unilaterally or bilaterally. One code includes imaging of both the cervical and cerebellar areas when done. The codes for selective vertebral imaging are unilateral. These codes must be repeated and modified (e.g., -, -9, -LT-RT, -XS as appropriate) if complete bilateral vertebral artery imaging is performed. CLIICL IDICTIOS: For evaluation of stroke, TI, aneurysm, V malformation, and vertebrobasilar insufficiency related to vertebral steal and subsequent "drop attacks". The vertebral vessels may enlarge and represent the dominant flow to the entire brain in patients with carotid occlusive disease. CODES: PROCEDURE DESCRIPTIO on-selective catheter placement, thoracic aorta, with angiography of the extracranial carotid, vertebral, andor intracranial vessels, unilateral or bilateral, and all associated radiological supervision and interpretation, includes angiography of the cervicocerebral arch, when performed Selective catheter placement, subclavian or innominate artery, unilateral, with angiography of the ipsilateral vertebral circulation and all associated radiological supervision and interpretation, includes angiography of the cervicocerebral arch, when performed Selective catheter placement, vertebral artery, unilateral, with angiography of the ipsilateral vertebral circulation and all associated radiological supervision and interpretation, includes angiography of the cervicocerebral arch, when performed PR O C C O D E P C T O T L R V U S & I C O D E P C T O T L R V U Selective catheter placement, each intracranial branch of the internal carotid or vertebral arteries, unilateral, with angiography of the selected vessel circulation and all associated radiological supervision and interpretation (eg, middle cerebral artery, posterior inferior cerebellar artery) (List separately in addition to code for primary procedure) Selective catheter placement, arterial system; additional second order, third order, and beyond, thoracic or brachiocephalic branch, within a vascular family (List in addition to code for initial second or third order vessel as appropriate).. 9
127 dd-on Code CODIG ISTRUCTIOS:. Codes 22 and 22 include imaging of the cervical andor cerebral portions of the vertebral artery. This differs from the carotid system, where the cervical and cerebral imaging portions may impact coding (e.g., 222 vs. 22). The cerebral portion of the vertebral artery includes imaging of the distal vertebral artery, the posterior inferior cerebellar artery (PIC), and the basilar artery and its branches. Selective catheter placement and additional imaging of the branches of the vertebral (PIC) or basilar artery (IC, superior cerebellar, posterior cerebral) can be reported with add-on code 22 (up to two times in this territory).. There are three territories of the brain: right cerebral, left cerebral, and posterior fossa. The vertebral arteries supply the posterior fossa. 2. Do not report code 777 if additional selective catheter placement and imaging of the carotid or vertebral arteries are performed after a basic cervicocerebral or vertebral angiogram is completed. Code 777 can be used to describe additional selective imaging of subclavian branches (e.g., thyrocervical trunk, costocervical trunk) that supply head, neck, and extremity structures after these basic angiographic procedures (77, 77, 22, 22).. dditional intracranial catheter placements and imaging are described by code 22 (which can be coded up to two times per side for a maximum of four times total). Code 22 can be used once for selection and imaging of the middle cerebral artery and all of its branches and once for selection and imaging of the anterior cerebral artery and all of its branches. Other IC branches include the opthalmic, posterior communicating, and meningohypophyseal trunk arteries. Code 22 also applies to branches of the vertebral andor basilar arteries (e.g., IC, PIC, superior cerebellar, posterior cerebral).. Code 22 is an add-on code to selective common and internal carotid codes for cerebral imaging (22, 22) and selective vertebral imaging codes (22, 22).. If the vertebral is imaged (22 or 22) and the catheter is advanced further out the arm or one of its branches for additional selective imaging of the neck or shoulder, add the appropriate catheter placement code (2) and imaging code (77, 77, 777) based on documentation.
128 . If both the cervical and cerebral portions of the vertebral are selectively imaged unilaterally, use code 22 or 22 only once. 7. Imaging codes 22 and 22 are per side imaged. If both sides are imaged from the same level of catheter selectivity, use modifier -.. If one side is imaged selectively with the catheter in the subclavian or innominate, and the other side is imaged selectively with the catheter in the vertebral artery, use codes 22-9 and If imaging of one vertebral is via an arch injection, and the other vertebral is imaged via selective vertebral injection, use code 22 only once, as arch injection and imaging of the non-selected vertebral are bundled with code Do not code vertebral angiography if vessel origins or antegrade flow are described from a cervicocerebral arch evaluation. The arch exam (22) includes the proximal subclavians, proximal or complete vertebrals, brachiocephalic, common carotids, and cerebral carotids if evaluated. 7. Do not report code 77 (unilateral extremity angiography) if proximal subclavian imaging is performed for the purpose of determining if it is safe to selectively catheterize the vertebral artery origin. This is a guiding shot and is part of the selective vertebral codes 22 and Report code 77 (unilateral extremity angiography) if imaging shows occlusion of the vertebral artery and evaluation of the subclavian artery is described. If the imaging is for evaluation of the vertebral, use code 22 instead. 7. Report code 22 if delayed images from subclavian injection shows reconstitution of the ipsilateral cervical vertebral from collaterals off the thyrocervical and costocervical arteries and vertebral imaging is the intent of the imaging procedure. 7. Do not code bilateral vertebral angiography for "reflux" of contrast down the non-injected opposite vertebral artery to see the contralateral posterior inferior cerebellar artery (PIC). These vessels are part of the cerebral evaluation bundled with the unilateral cervicalcerebralvertebral angiography. If unilateral selective vertebral angiography also includes complete evaluation of the entire opposite cervical vertebral artery to the level of the opposite subclavian artery, still only code for one unilateral vertebral angiography (22), as only one selective catheter placement was performed. This may occur with "subclavian steal" phenomena associated with contralateral proximal subclavian artery stenosis or occlusion. EXMPLE(S): ) 2-year-old female with subarachnoid hemorrhage. Via a right transfemoral approach, selective catheter placement, injection, and imaging of the brain via the right and left internal carotid arteries (22-) is performed, followed by selective right vertebral and left vertebral (22-) catheter placement and imaging. posterior communicating aneurysm is seen. 2) -year-old with vertebrobasilar insufficiency symptoms. Via a right transfemoral approach, a pigtail catheter is placed in the ascending aorta and arch exam is performed (22). Due to ostial stenoses of the great vessels, selective
129 catheterization is not done. rch injection is then performed with imaging over the neck and head. 7% bilateral proximal internal carotid stenoses (included) with normal intracranial vessels (included) are noted. right vertebral occlusion with reconstruction via thyrocervical collaterals (included) and an % proximal left vertebral stenosis (included) is also seen. The basilar artery is patent (included as part of vertebral cerebral imaging). ) Same patient as #2 except vertebral findings are "vertebral origins are patent, left side dominant". (This limited imaging is considered part of the basic arch exam and is included in code 22.) ) Same patient as #2, however, the left vertebral artery is selected with a "Head hunter" catheter, and imaging of the left vertebral and basilar artery is performed (add 22, delete 22). ) Same patient as #. Following this diagnostic angiography, a drug-eluting stent is placed across the vertebral stenosis (7T) and deployed (add 22 for initial diagnostic non-selective cervicocerebral arch imaging of contralateral vertebral and carotids; delete 22, as ipsilateral vertebral catheter placement and imaging are bundled with 7T). ) Same patient as #, however, the left thyrocervical trunk (2, 777) and left costocervical trunk (2, 777) are additionally selected and imaged to evaluate the head and neck region. 7) Same patient as #, however, the posterior cerebral arteries are selected and imaged bilaterally using a microcatheter to evaluate flow to the occipital cortex (add 22 x 2). Diagnostic ngiography Coding Cervicocerebral ngiography External Carotid ngiography Pages: -7 Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: External carotid angiography requires placement of a catheter into the right or left external carotid artery or their branches with imaging of these vessels. The external carotid must be selectively catheterized in order to code external carotid angiography. This vessel arises from the common carotid artery and supplies blood flow to the face, nose, neck, scalp, and meninges of the brain. The main branches include the lingual, facial, occipital, internal maxillary, ascending pharyngeal,
130 superficial temporal, middle meningeal, sphenopalatine, superior thyroidal, and posterior auricular arteries. CLIICL IDICTIOS: Meningioma, facial tumor, trauma, arteriovenous malformation or nosebleed (epistaxis) evaluation, andor treatment with embolotherapy. Occasionally these vessels are selected to evaluate collateral flow for possible bypass surgery to the brain in cases of severe carotid occlusive disease. CODES: PROCEDURE DESCRIPTIO P R O C C O D E P C T O T L R V U S & I C O D E P C T O T L R V U Selective catheter placement, external carotid artery, unilateral, with angiography of the ipsilateral external carotid circulation and all associated radiological supervision and interpretation (unilateral) Selective catheter placement, external carotid artery, unilateral, with angiography of the ipsilateral external carotid circulation and all associated radiological supervision and interpretation (bilateral) dditional vessel, selective, after basic exam (for use when additional branches of the subclavian artery are selected and imaged, with imaging of the neck andor shoulder)
131 dditional vessel, selective, after basic exam (for use when branches of the external carotid artery are selected and imaged after the initial external carotid angiography) 7 7 B u n dl ed B u n dl e d dd-on Code CODIG ISTRUCTIOS: 7. The catheter must be selectively placed in the external carotid artery or one of its branches to use procedure code If additional superselective catheter placement and diagnostic imaging is performed of branches of the external carotid artery, do not use code 777, as all additional imaging and selections of branches of the external carotid artery are included in add-on code Unilateral selective external carotid (227) and bilateral selective external carotid angiography (227-) may be performed. 7. Since a single selective code (227) exists, use modifier - when bilateral procedures are performed. 79. Do not report code 227 when physician describes external carotid imaging findings from a common carotid injection. These findings, since performed with a catheter not selectively in the external carotid artery, are included in the cervical carotid imaging codes External carotid angiography code 227 is an add-on code to Do not report code 227 unless cervical or cerebral angiography is also performed. Consider either using an unlisted code (7799) for diagnostic imaging or a catheter placement (27) for intervention.. If an embolization is carried out from this vessel, use the appropriate 2X embolization code based on the location of the pathology being treated [e.g., intracranial meningioma treated via the middle meningeal artery is 2 (CS) and nosebleed (epistaxis) treated via the sphenopalatine artery is 2 (head and neck)]. Do not use codes for selective CS or head and neck embolizations. Use code 72 for non-selective, direct access venous embolization procedures for head and neck pathologies (e.g., cystic hygroma, lymphangioma, venous malformation). 2. Selection and imaging of selective or superselective branches of the subclavian artery to further evaluate andor treat abnormalities of the neck and shoulder girdle are described by codes 2 and 777, respectively, when vertebral evaluation (22 or 22) has also been performed on the same side.
132 . Branch vessel names include the ascending pharyngeal, lingual, facial, internal maxillary, occipital, middle meningeal, sphenopalatine, superficial temporal, superior thyroidal, and posterior auricular.. The external carotid arteries are rarely selected and imaged by non-neuro specialists. EXMPLE(S): ) Bilateral selective common carotid, bilateral selective internal carotid, and bilateral selective external carotid catheter placements with injection and imaging of the carotid bifurcation (222-), cerebral vasculature (add 22-, delete 222-), and external carotid supply (227-) showing a meningioma supplied by both the right and left middle meningeal arteries. The middle meningeal arteries are additionally selected and imaged bilaterally (bundled). The catheter is removed. ote: The external carotid artery catheter placement is included in the diagnostic selective procedure code 227. Superselective external carotid branch catheterization and imaging are also included in code ) 7-year-old patient with epistaxis. Via transfemoral approach, a catheter is used to perform cervicocerebral arch angiography (22), followed by bilateral cervical carotid angiography (add 222-, delete 22). o significant stenoses are seen. Selective catheter placement into both external carotid arteries with imaging (227-) shows extravasation on the right and hypervascularity on the left side of the nose. Microcatheters are advanced (bundled) into the sphenopalatine arteries, and additional imaging is performed (bundled), showing extravasation bilaterally (after removal of the nares packing) and no intracranial communication. Bilateral embolization with particles (2, 79) is performed until stasis of flow. Follow-up angiography bilaterally via the common carotid arteries (79) shows excellent result. ote: lthough two vessels were embolized, this is one surgical site, so code 2 is billed only once. Only report code 79 once for completion angiography post-embolization for head and neck (non-cs) embolizations. ) 7-year-old with left thyroid malignancy. Bilateral selective cervical carotid angiography (222-), bilateral selective external carotid angiography (227-), selective left superior thyroid injection and imaging (no code), superselective left vertebral angiography (22) and subsequent selection of the thyrocervical trunk with imaging (2, 777), and inferior thyroid selection and imaging (777) are performed. Chemoembolization is performed (2, 79). Follow-up angiography (79) shows stasis of flow to this head and neck tumor.

133 Diagnostic ngiography Coding Cervicocerebral ngiography Cervicocerebral Variations Page: Variations in Coding Related to pproach The variations only affect the catheter placement codes for neurointerventional procedures performed at a session separate from the diagnostic angiography, as catheter placements are bundled with diagnostic cervicocerebral codes (other than code 2, which can be submitted with codes 22 and 22 in certain circumstances). For diagnostic imaging, variant anatomy and access site will not impact CPT coding. RIGHT BRCHIL OR RDIL RTERY PPROCH The right vertebral and right common carotid and left common carotid arteries are separate first order selective placements (2).
134 The left vertebral is a second order selective placement (2). LEFT BRCHIL OR RDIL RTERY PPROCH The catheter placement code for the left common carotid remains a first order selective placement (2). The right common carotid artery is a second order selective placement (2). The right vertebral is a third order selective placement (27). The left vertebral is a first order selective placement (2). ote: If the right common carotid and right vertebral arteries are both selected from a left brachial approach, the right vertebral remains a third order selective placement and the right common carotid is an additional second or third order selective catheter placement (2). If there is a bovine arch, the left common carotid catheter placement becomes an additional second or third order selective catheter placement (2) as well. TRSLUMBR ORTIC PPROCH Same as femoral approach. BILTERL DIRECT PUCTURE COMMO CROTID PPROCH (RRE) The common carotid catheter placements using a direct puncture technique are reported with code -. If the catheter is advanced into either the internal or external carotid artery, the catheter placement codes are first order (2, 2-9) bilaterally. Code 2 is not reported with a - modifier due to its designation in the physician fee schedule as not being a procedure that is unilateral. If direct carotid puncture after open surgical access is done to perform open intrathoracic common carotid or right brachiocephalic stent placement (727), the selective catheter placement code is bundled and not separately billable. Direct carotid puncture (code ) is rarely performed today and, if seen on a bill, should be questioned. 2-2 ZHealth Publishing. ll rights reserved. CPT Only 27 merican Medical ssociation. ll rights reserved. natomic variation

135

136

137

138 Diagnostic ngiography Coding Descending Thoracic orta ngiography Pages: 2- Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: Descending thoracic aorta angiography involves non-selective catheter placement into the aorta within the chest, usually at a level just below the origin of the left subclavian artery; however, evaluation can also be performed from the ascending aortic or cervicocerebral arch level. This angiography is usually performed by
139 obtaining two views at 9 degree angles (bi-plane technique) to evaluate the aorta. Images obtained depict the descending thoracic aorta below the take off of the left subclavian artery to the level of the diaphragm. CLIICL IDICTIOS: To evaluate dissectiontear of the aorta, aortic transection, aortic aneurysms, patent ductus arteriosus, or coarctation of the aorta (congenital anomalies). Dissection may be hypertensive or post traumatic in nature. neurysm may be atherosclerotic, mycotic, or congenital (connective tissue disorder such as Marfan's syndrome or Ehlers-Danlos syndrome) in nature. Pseudoaneurysms may be the result of trauma, including gunshot, stabbing, or an MV. Thoracic aortic stent grafting is a common treatment for these aneurysms. CODES: PROCEDURE DESCRIPTIO Introduction of catheter, aorta (non-selective) S&I Codes ortography, thoracic, without serialography, radiological supervision and interpretation ortography, thoracic, by serialography, radiological supervision and interpretation PROC CODE ote: If selective catheter placement is subsequently performed and coded, the non-selective code 2 is bundled by the selective catheter position code and should not be coded. Code 2 is bundled and not separately billable with a cardiac catheterization, as heart catheterization procedures include aortic catheter placement. P C TOT L RVU..9. CODIG ISTRUCTIOS:. Descending thoracic aorta angiography is often coded in association with cervicocerebral arch angiography (22) and abdominal aortography (72). Look for these associated procedure descriptions in the report. s cervicocerebral arch angiography bundles catheter placement, do not report code 2 when arch imaging is additionally performed.
140 . Code 7 is not intended for routine use with cardiac catheterization injectionsprocedures, but may be used if specific indications are met and a full and complete study is performed (e.g., coarctation of the aorta, descending aortic dissection, or aneurysm). (See code 97 for ascending aortic injection and imaging procedure during cardiac catheterization.) 7. Due to CCI edits, codes 7 and 7 should be closely reviewed for medical necessity if submitted during a cardiac catheterization procedure.. Code 7 is often coded mistakenly when arch angiography (22) is actually performed. Carefully review the imaging findings to see which portion of the aorta is being evaluated. 9. Physicians may call the arch exam (22) a "thoracic" aortogram (7) when evaluation of the arch and the origins of the great vessels is actually performed and documented. In this case, use code 22. Both of these codes describe a portion of the aorta that resides in the thoracic cavity. 9. Code 7 is almost never appropriate, as imaging by "single shot" technique is rarely performed. If code 7 is seen on a bill, it should be questioned for appropriateness and corrected based on review of physician documentation. 9. Do not report code 22, 7, 7, or 97 with PD occlusion (92) or thoracic stent graft (TEVR) procedures, as these diagnostic imaging codes are bundled in the CPT code descriptions for the above mentioned interventional procedures. EXMPLE(S): ) Patient presents with severe back pain and hypotension. Dissection of the aorta is suspected. From a transfemoral route, the catheter is placed non-selectively into the ascending aorta with arch injection (22), followed by repositioning of the catheter and injection and bi-plane imaging of the descending thoracic aorta (7); the catheter is repositioned, and an abdominal aortic injection with imaging (72) is performed. The catheter is repositioned, and oblique views of the pelvis and proximal thighs are performed (add 7, delete 72). The catheter is removed. There is no evidence of dissection. bdominal aneurysm is noted. The iliofemoral vessels are widely patent. 2) -year-old patient presents with leg weakness after exercise and decreased pulses in the feet. Via a left radial approach, a French pigtail catheter is advanced up the arm into the aorta (2). Contrast injection with imaging of the descending thoracic aorta (7) demonstrates coarctation of the aorta with a 7% narrowing and a mm systolic gradient across the stenosis. Balloon dilation with a mm balloon (72) shows significant residual stenosis requiring placement of an 2 mm balloon expandable stent (add 72, delete 72 - stent placement bundles any associated angioplasty in the same vessel), which results in a widely patent thoracic aorta without evidence of complication.
")
141 Diagnostic ngiography Coding Descending Thoracic orta ngiography Spinal ngiography Pages: 2-29 Procedure Clinical Indications Codes Coding Instructions Example(s) References
142 PROCEDURE: Spinal angiography involves catheter placement into paired spinal arteries (intercostal above and lumbar below the diaphragm) with injection of contrast and imaging of the blood flow to the spine or spinal cord. This may also include bilateral catheter selection and injection of contrast with imaging of the supreme intercostal, subclavian, thyrocervical, vertebral, internal iliac, median sacral, and internal iliac arteries. CLIICL IDICTIOS: Evaluation for subarachnoid hemorrhage related to possible spinal arteriovenous malformation or abnormal MRI suggesting spinal VM. Evaluation of blood supply to primary or metastatic tumors of the vertebral bodies. bnormal findings may be followed by an embolization procedure. CODES: PROCEDURE DESCRIPTIO Selective catheter placement, arterial system; each first order thoracic or brachiocephalic branch, within a vascular family Selective catheter placement, arterial system; initial second order thoracic or brachiocephalic branch, within a vascular family Selective catheter placement, arterial system; initial third order or more selective thoracic or brachiocephalic branch, within a vascular family PR OC CO DE P C TO T L RV U Selective catheter placement, arterial system; additional second order, third order, and beyond, thoracic or brachiocephalic branch, within a vascular family (List in addition to code for initial second or third order vessel as appropriate) Selective catheter placement, arterial system; each first order abdominal, pelvic, or lower extremity artery branch, within a vascular family Selective catheter placement, arterial system; initial second order abdominal, pelvic, or lower extremity artery branch, within a vascular family S&I Codes Spinal angiography, per vessel (selective), if supplying spinal structure
143 Spinal angiography, per vessel (selective), if supplying bronchial structure Internal iliac angiography (selective), if supplying spinal structure (for S-S) Median sacral angiography (selective), if supplying spinal structure (for S-S2) Median sacral angiography (selective), if supplying pelvic structure Subclavian angiography Costovertebral trunk angiography (following subclavian) (additional vessel, selective, after basic exam) Supreme intercostal angiography (after selective catheter placement into the vessel), if supplying spinal structure Supreme intercostal angiography (after selective catheter placement into the vessel), if supplying bronchial structure Thyrocervical trunk angiography (following subclavian) (additional vessel, selective, after basic exam) Internal mammary angiography
144 7 2 dd-on Code CODIG ISTRUCTIOS: 92. Spinal angiography (77) requires selective catheter placement into the vessel to use this code. 9. Spinal angiography (77) has an MUE of ot all spinal (intercostal, lumbar) arteries are injected, as there may be collateralization to adjacent levels present. Detailed review of the documentation is necessary. 9. Embolization via a "spinal" artery may be performed for treatment of spinal cord lesions (2) or vertebral body lesions (e.g., VM-722, tumors-72, hemorrhage-72). 9. There may be a combined bronchial-intercostal trunk off the thoracic aorta on the right side. The ascending cervical artery to the spinal cord arises off the right bronchial artery, requiring more selective catheterization for imaging and embolization. This imaging is reported with code 77, as it is a spinal angiogram. If performed, the initial bronchial angiography is reported with code 772. Visceral angiography bundles descending thoracic aortography, so do not report code 7 with Code 77 is a unilateral code. Use this code twice if procedure is done bilaterally (77 and 77-9). (Payers may require a -7 modifier for repeat code instead of a -9 modifier.) This code may be used 2- times appropriately when a comprehensive spinal angiogram is performed. Physician documentation must support selective catheter placement, imaging, and interpretation of the images. Do not expect payment for every one of these imaging procedures when the number of repeated codes is this high. The updated MUE for code 77 is Do not use a combination -9 modifier for multiple above diaphragm bilateral catheter placements (e.g., 2). Bill the codes with multiple service units and an appropriate modifier, or as required by your particular payer. 99. The supreme (superior or "highest") intercostal artery is a third order selective branch off the costocervical trunk (which originates as the third branch directed in a cephalad direction off both the right and left subclavian arteries, transfemoral approach).. If intent is to image for spinal abnormality, use code 77 when injecting the intercostal artery. If intent is to image for bronchial bleeding or other bronchial abnormality, use code 772 when injecting the intercostal artery. Closely review physician documentation for the indication and purpose of this angiography.
145 . The middle or median sacral artery is considered a spinal artery (77) if injected to evaluate the sacrum (S and S2 bilaterally) for neurologic abnormalities. If injected to image a pelvic mass (e.g., bladder tumor), use code The internal iliac artery is considered a spinal artery (77) if injected to evaluate the sacrum (S-S bilaterally) for neurologic abnormalities. If injected to image a pelvic mass (e.g., bladder tumor), use code 77.. Internal mammary angiography (77) cannot be billed during cardiac catheterization procedures due to CCI edits (zero edit). EXMPLE(S): ) Patient presents with subarachnoid hemorrhage and abnormal MRI suggesting spinal cord arteriovenous malformation. Thoracic (7) and abdominal (72) aortograms are performed, followed by selective catheterization and imaging of T-T2 intercostal arteries bilaterally (2-9 x, 77, 77-9 x ), L-L spinal arteries bilaterally (2-9 x, 77-9 x ), both subclavian arteries (77), both internal mammary arteries (77, 77-9), both supreme intercostals (77-9 x 2), the median sacral (2-9, 77-9), and both internal iliac arteries (2-9, 2, 77-9 x 2). The patient requires embolization of two vessels (2, 79, note: this is one surgical site), and two post embolization follow-up exams (79, 79-9). (The catheter placement codes for the work related to imaging from the subclavian, internal mammary, and supreme intercostal arteries are 27 and 2 on the left and 27-9, 2 on the right.) ote: The case detailed above is likely one of the more complicated cases you will code - CPT codes during one session! Due to implementation of MUEs, there is limitation of the number of accepted codes by Medicare. You should discuss with your payer. The MUE for code 79 is a date of service MUE that has a limit of two (at the time of this writing). The MUE for code 77 is 2. Do not necessarily expect payment for all these codes; however, all described catheter placements and imaging are appropriate to code and charge. This should be discussed with your payer to ensure accurate reimbursement. Use a -9 or -7 modifier, as needed, to distinguish separate and distinct procedures (particularly for codes 77, 77, 77, and catheter placements). Do not use a - modifier on code 2, 2, or 27. Diagnostic ngiography Coding Descending Thoracic orta ngiography Internal Mammary ngiography Pages: - Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE:
146 Internal mammary angiography involves placement of a catheter into the rightor left internal mammary artery, injection of contrast, and imaging over the shoulder, neck, or chest area. The internal mammary artery (IM) usually arises as the first branch off the inferior aspect of each proximal subclavian artery. CLIICL IDICTIOS: For Radiology: Evaluation for adequacy of vascular pedicle for reconstructive surgery performed by plastic surgeons (TRM flap) and for collateralization to the lower extremities in patients with severe peripheral vascular disease. ccessory blood supply to lung lesions (granulomatous, neoplastic, cystic fibrosis) in patients with hemoptysis. Evaluation of blood supply to the head and neck in cases of severe vascular disease, VMs, tumors, and, occasionally, cases of trauma. For Cardiology: To evaluate an established internal mammary artery arterial conduit (CBG) or to determine if the internal mammary artery is a usable vessel for future coronary bypass surgery. For evaluation of systemic to pulmonary arterial collaterals in cases of congenital heart disease. CODES: PROCEDURE DESCRIPTIO Right internal mammary artery via left brachial artery Left internal mammary artery via left brachial artery Right internal mammary artery via right brachial artery Left internal mammary artery via right brachial artery PROC CODE Right internal mammary artery via femoral artery 27 Left internal mammary artery via femoral artery 2 P C TOTL RVU S&I CODE P C TOTL RVU
147 CODIG ISTRUCTIOS:. Use radiology codes for radiology indication (e.g., 2, 77).. Use cardiology codes for cardiac indication when IM is selected and injected during cardiac catheterization (e.g., included with 9, 97, 99, 9, 9).. Code 77 is a non-selective radiology code, so the imaging can be done via an aortic, subclavian, or internal mammary injection. 7. Code 77 is a unilateral code. If bilateral evaluation is performed, use code 77 twice with appropriate modifier for your payer.. Do not confuse this IM (internal mammary arteriogram) with the inferior mesenteric arteriogram (772), which is an imaging procedure of a visceral artery supplying the left colon. 9. Do not use the radiology internal mammary artery code (77) during cardiac cases. This is a significant compliance risk. Pediatric cardiology procedures (e.g., coarctation of the aorta or arterial-pulmonary collaterals) may appear to require use of code 77 for the "non" cardiac related IM procedures. These procedures are more peripheral in nature than cardiac; however, code 77 still should not be billed if a diagnostic pediatric cardiac catheterization is performed at the same setting. (ote: Many pediatric cardiac patients are on Medicaid. Most Medicaid payers use the same rules as Medicare.) Code 9 is an add-on code to congenital heart catheterizations describing IM injection when done to evaluate for arterial to coronary artery bypass. We do not recommend congenital code 9 when the IM is injected to evaluate aorto-pulmonary collaterals. EXMPLE(S): ) -year-old patient with need for a TRM flap (plastic surgery) from the abdomen. Via a transfemoral approach, selective bilateral internal mammary angiography is performed to evaluate the blood supply and viability of this planned surgical procedure (27, 2-9, 77, 77-9). 2) 2-year-old HIV positive patient with cavitary tuberculosis presents with left-sided bronchoscopically documented hemoptysis. Via a right femoral approach, selective catheter placement into the left bronchial artery (arising directly off the aorta) (2-9), left IM (2), left T, T, and T intercostal arteries (2-9 x ) with imaging of all sites (772, 77, x ) to evaluate bronchial bleeding. ctive hemorrhage from the left IM injection is documented, so two coils are placed (72) in a distal, third order branch of the IM (add 27, delete 2). Follow-up angiography (bundled) shows cessation of bleeding and occlusion of the vessel supplying the lung abnormality. REFERECES: CPT ssistant, Fall 9:, ug 9:, pr 99:7 (Topic, Topic 2), Oct : CPT Changes: n Insider's View 2 SIR Interventional Radiology Coding Users' Guide 29, pages -2 2
148 2-2 ZHealth Publishing. ll rights reserved. CPT Only 27 merican Medical ssociation. ll rights reserved. Diagnostic ngiography Coding Descending Thoracic orta ngiography Bronchial ngiography Pages: 2- Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: Bronchial angiography involves catheter placement and imaging of the thoracic aorta, the subclavian arteries and branches, the bronchial arteries bilaterally, and often several intercostal arteries. CLIICL IDICTIOS: Hemoptysis, usually uncontrolled and massive, related to neoplasm, granulomatous processes (including tuberculosis), cystic fibrosis, and other inflammatory lung diseases. CODES: PROCEDURE DESCRIPTIO Selective catheter placement, arterial system; each first order thoracic or brachiocephalic branch, within a vascular family Selective catheter placement, arterial system; initial second order thoracic or brachiocephalic branch, within a vascular family Selective catheter placement, arterial system; initial third order or more selective thoracic or brachiocephalic branch, within a vascular family PR OC CO DE P C TO T L RV U
149 Selective catheter placement, arterial system; additional second order, third order, and beyond, thoracic or brachiocephalic branch, within a vascular family (List in addition to code for initial second or third order vessel as appropriate) S&I Codes Selective bronchial angiography (viscera of the chest) with or without aortography (this includes thoracic aortography) Intercostal angiography (selective), if supplying spinal structure Intercostal angiography (selective), if supplying bronchial structure Esophageal, mediastinal, and pericardial branch arteries Upper extremity angiography, unilateral Upper extremity angiography, bilateral Internal mammary angiography, unilateral Supreme intercostal angiography (selective), if supplying spinal structure Supreme intercostal angiography (selective), if supplying bronchial structure
150 Costo-vertebral trunk angiography (additional selective vessel after basic exam to see the supreme intercostal) dd-on Code CODIG ISTRUCTIOS:. Bronchial arteries arise from the anterolateral aspect of the thoracic aorta and supply the "viscera" of the chest. Imaging of the "viscera" is described by code Do not code for thoracic aortography (7) when done with selective bronchial angiography (772). The aortography is bundled into the "visceral" angiography code (772). 2. This procedure is almost always done with the intent to perform embolization. The embolization code for treatment of bronchial bleeding is 72, which is reported per surgical field treated (e.g., per lung treated for hemorrhage).. The supreme intercostal artery (also called "the highest intercostal" artery) arises from the costocervical artery off the subclavian (a third order selective catheter placement bilaterally when performed from a transfemoral approach).. Use code 772 when an intercostal artery is injected and selectively imaged to evaluate the lungs for hemoptysis. Use code 77 when selective intercostal artery imaging is used for spinal cord evaluation.. The bronchial arterial anatomy is quite varied. There may be one or two right or left bronchial arteries that arise directly off the aorta. There may also be a single "common bronchial trunk" that bifurcates into the left and right bronchial arteries. Code separately for each vascular family selected off the aorta.. The anterior cervical artery, supplying the upper thoracic and cervical portions of the spinal cord, usually arises as the first branch oriented in a cephalad direction off the right bronchial artery. 7. Less commonly selected visceral arteries include esophageal, mediastinal, and pericardial branches. EXMPLE(S): ) -year-old patient with cystic fibrosis and active hemoptysis from the right lung at bronchoscopy. n arch (22) and thoracic aortogram (7) show enlarged vessels supplying the right lung from the bronchial artery and numerous collaterals.
151 The right subclavian artery (77), right internal mammary artery (77), right costocervical trunk (777), right bronchialintercostal trunk (772; visceral angiography withwithout aortogram, must delete 7), and right T-T intercostals (772, x 2) are selected, injected, and imaged with embolization performed (72) in all six selective and superselective branch vessels. Post embolization filming from all six sites is performed (bundled) with cessation of bleeding documented. [The selective catheterizations performed are 27 (right internal mammary artery), 2 (right costocervical trunk to see the supreme intercostal), 2-9 (right bronchial, advanced past the ascending cervical spinal artery), and 2-9 x (T-T right intercostal arteries). The right subclavian artery catheter placement is included in the more selective catheterizations of this vascular tree.] ote: Use an appropriate modifier, as needed, to distinguish separate and distinct procedures. Code 772 was used to describe the visceral imaging performed of the chest from the right T- intercostal artery injections. The MUE for code 772 is three..

152
153 Diagnostic ngiography Coding Visceral ngiography Pages: - Procedure Clinical Indications Codes Coding Instructions PROCEDURE: Visceral angiography involves evaluation of the blood vessels supplying the visceral or body cavity organs. These vessels arise from the anterior aspect of the abdominal aorta. Vessels included in this category are the celiac, superior mesenteric, and inferior mesenteric arteries. The inferior phrenic arteries arise off the aorta laterally or off branches of the celiac artery and supply the diaphragm. The renal and adrenal
154 arteries arise posterolaterally off the abdominal aorta and are considered to supply the retroperitoneal structures and have their own organ specific codes. Congenital variations that affect the selective catheterization codes are common. Familiarity with these variations of anatomy is required for accurate coding. CLIICL IDICTIOS: Gastrointestinal bleeding, tumor evaluation, portal hypertension, systemic hypertension, trauma with evidence of abdominal hemorrhage, and visceral ischemia. Interventional procedures involving these vessels include embolization, angioplasty, atherectomy, stent placement, thrombolytic infusions, and thrombectomy. CODES: PROCEDURE DESCRIPTIO bdominal aortogram Celiac, with or without aorta, selective Superior mesenteric, with or without aorta, selective P C T O T L R V U. S&I COD E Inferior mesenteric, with or without aorta, selective. 77. P R O C C O D E P C T O T L R V U
155 Inferior phrenic (for evaluation of the diaphragm), selective, arising off aorta Inferior phrenic (for evaluation of the viscera), with or without aorta, selective, arising off aorta Inferior phrenic with or without aorta, selective, arising as branch off celiac or left gastric drenal unilateral (may be multiple), selective drenal bilateral (may be multiple), selective or or 2 2 or vs
156 Pelvic (internal iliac) unilateral, selective (ipsilateral) Pelvic (internal iliac) unilateral, selective (contralateral) dditional vessel, selective, after basic exam Gonadal (ovariantesticular) unilateral, selective Median (middle) sacral, selective, to evaluate for pelvic structures Median (middle) sacral, selective, to evaluate for spinal structure Selective catheter placement (first-order), main renal artery and any accessory renal artery(s) for renal angiography, including arterial puncture and catheter placement(s), fluoroscopy, contrast injection(s), image postprocessing, permanent recording of images, and radiological supervision and interpretation, including pressure gradient measurements when performed, and flush aortogram when performed; unilateral Selective catheter placement (first-order), main renal artery and any accessory renal artery(s) for renal angiography, including arterial puncture and catheter placement(s), fluoroscopy, contrast injection(s), image postprocessing, permanent recording of images, and radiological supervision and interpretation, including pressure gradient measurements when performed, and flush aortogram when performed; bilateral 2 X 77 7 Superselective catheter placement (one or more second order or
157 higher renal artery branches) renal artery and any accessory renal artery(s) for renal angiography, including arterial puncture, catheterization, fluoroscopy, contrast injection(s), image postprocessing, permanent recording of images, and radiological supervision and interpretation, including pressure gradient measurements when performed, and flush aortogram when performed; unilateral Superselective catheter placement (one or more second order or higher renal artery branches) renal artery and any accessory renal artery(s) for renal angiography, including arterial puncture, catheterization, fluoroscopy, contrast injection(s), image postprocessing, permanent recording of images, and radiological supervision and interpretation, including pressure gradient measurements when performed, and flush aortogram when performed; bilateral dd-on Code CODIG ISTRUCTIOS:. Code 772 (visceral angiography of abdominal structures) includes preliminary or follow-up abdominal aortography (72). "flush" aortogram is the same as an aortogram. Do not report code 72 when a selective abdominal visceral angiogram is performed. 9. Codes 7 and 72 may not be charged separately once a selective visceral angiogram has been performed in the thoracic or abdominal aortic regions respectively. ortography is bundled with selective visceral and renal angiography. 2. fter a complete basic exam, code 777 (additional selective catheter placement and imaging) can be used to describe additional vascular imaging beyond the basic exam. This would be most applicable when more selective hepatic or splenic injections are performed after a basic celiac exam or when additional selective jejunal or ileal branch injections are performed after a basic superior mesenteric angiogram. 2. Use of code 777 requires that additional imaging beyond a basic exam is performed after an additional level of catheter selectivity is documented. Do not use code 777 merely for additional lateral or oblique views from the same catheter position. 22. Extensive collateralization between the visceral vessels can develop in occlusive disease. This includes additional vessels called the "arc of Riolan" and the "arc of Bühler", which create SMIM collateralization. 2. The internal iliac arteries supply blood to the pelvic viscera and are reported with S&I code 77 and must be performed selectively by placing a catheter into the internal iliac, one of its branches, the median sacral artery, or any other branch vessel supplying pelvic structures. Use code 77 if the
158 internal iliac or median sacral are injected to image the sacrum instead of the pelvis. 2. Do not report code 777 for additional visceral vessels selected and imaged off the aorta (e.g., celiac, SM, IM). Use code 772 to describe the initial imaging of a visceral vessel that arises from a separate vascular family off the aorta. Code 772 is often used three times during visceral angiography (e.g., during GI bleeding study where selective injections and imaging of the celiac trunk, the SM, and the IM are performed). 2. The inferior phrenic artery supplies blood to the diaphragm. This is not a visceral structure. The inferior phrenic artery may be selected during hypervascular hepatic tumor embolization procedures. This imaging would be a visceral angiogram. If the inferior phrenic artery arises as a branch off the left gastric artery and is the first vessel injected (no preliminary celiac angiography), consider code 772. If a visceral angiogram (celiac or left gastric) has already been performed, use code 777 to describe the additional selective imaging of the inferior phrenic. When the inferior phrenic arises directly off the aorta, use code 2 for catheter placement and unlisted code 79 to describe the imaging of the diaphragm and code 772 for imaging of the liver or spleen. 2. Gonadal arteries arise anterolaterally from the abdominal aorta just below the renal artery level. They are first order selective vessels that supply blood to the ovaries or testicles. These are considered pelvic structures (77). 27. Use code 77 or 77 for unilateral or bilateral selective adrenal arterial imaging codes. If additional adrenal arteries (beyond the basic one adrenal artery on each side) are imaged, use code 777 and any additional selective catheter positioning codes. There can be up to three adrenal arteries per side. 2. Do not use code 777 for selective imaging of accessory renal arteries after the main renal artery on that side has been selected and imaged. Codes 2-2 include all catheter placements and imaging of the main renal arteries, branches, and accessory renal arteries and include abdominal aortography if performed. 29. Less common visceral arteries include esophageal, mediastinal, and pericardial branches. Diagnostic ngiography Coding Visceral ngiography Celiac rtery ngiography Pages: - Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE:
159 The celiac artery is the first of the abdominal visceral arteries to arise anteriorly off the aorta. It arises at the T-2 level and supplies the stomach, proximal duodenum, distal esophagus, spleen, and liver. The celiac artery normally trifurcates into the left gastric, splenic, and common hepatic arteries. The left gastric artery courses superiorly, the splenic artery towards the left, and the common hepatic artery towards the right. The common hepatic artery divides into the proper hepatic artery (supplying the liver) and the gastroduodenal artery (GD), which supplies the lower portion of the stomach, duodenum, and pancreatic head. The GD gives rise to the pancreaticoduodenal arcade, which provides collateralization to the superior mesenteric artery (SM). The GD may be used as an arterial conduit for right coronary artery bypass grafting. The splenic artery supplies the spleen (via splenic artery branches) and pancreas (via the pancreatic magna and dorsal pancreatic branches). The left gastric artery supplies the proximal stomach, distal esophagus, and occasionally the left lobe of the liver. The inferior phrenic artery can arise from the left gastric artery. There are numerous ways that blood can be re-routed to the visceral organs when one channel is interrupted. This allows embolization procedures to be performed safely and allows collateral flow in patients with arterial occlusive disease. Congenital variations are very common in the visceral vasculature, so close attention to physician documentation is necessary when coding these exams. CLIICL IDICTIOS: The celiac artery is often evaluated in cases of GI bleeding (gastric or duodenal ulcer, Mallory-Weiss tear of the distal esophagus), abdominal trauma, pancreatitis, hepatic or pancreatic neoplasm, thromboembolism, and portal hypertension. THE DEGREE OF CTHETER SELECTIVITY FOR "ORML" TOMY IS S FOLLOWS: RTERY CODE P C TOTL RVU Celiac 2.9 Left gastric 2 7. Splenic 2 7. Pancreatica magna 27. Dorsal pancreatic 27. Common hepatic 2 7. Proper hepatic 27.
160 Right hepatic 27. Left hepatic 27. Right gastric 27. Right gastroepiploic 27. Gastroduodenal 27. If the vessels selected arise from the same vascular trunk, only the highest order selective catheterization is coded and 2 is used for the selective catheterization of the other branches. CODES: PROCEDURE DESCRIPTIO Celiac angiogram (selective) with or without aortogram ny selective branch as the initial exam ny selective branch if additional imaging is done after the basic celiac exam PRO C COD E 2 2, 2 7 2, 2 7, or 2 P C TOT L RVU S&I COD E P C TOT L RVU dd-on Code
161 CODIG ISTRUCTIOS:. Celiac artery angiography is often performed at the same time as evaluations of the superior mesenteric and inferior mesenteric arteries.. Report code 777 if additional selective catheter placement and imaging is performed after a basic celiac angiogram has been performed. 2. lways consider the many anatomic variations that exist when coding the visceral vasculature.. Hepatic branches are named for segments of the liver as seen on a CT scan. They are labeled segments -, with subsegments labeled "a" or "b". These are commonly described during TCE (chemoembolization) and Y-9 (radioembolization) procedures. ll branches selected are selective catheter placements described by code 27 for the farthest selection and by code 2 for each additional selective catheter placement documented.. replaced right hepatic artery arising as a second order selective vessel off the SM, a direct origin of the left gastric artery off the aorta, a left hepatic artery arising off the left gastric artery, and a common or single trunk off the aorta supplying the celiac and superior mesenteric arteries are all common anatomical variants of the visceral arteries.. Do not code the non-selective aortogram (72) when performed in conjunction with a selective visceral angiogram (772).. Do not report the non-selective catheter placement code 2 when a selective catheter placement has been performed (2, 2, or 27) via the same access site. 7. Do not report code 772 unless the catheter has been selectively placed in the celiac artery or one of its branches. Code 772 is a selective imaging code.. If the GD is selected and imaged to evaluate for use as an arterial conduit for coronary artery bypass surgery (or to evaluate an existing bypass graft) during a cardiac catheterization, use the appropriate cardiac catheterization code 9, 97, 99, 9, or Code 772 has an MUE of three. EXMPLE(S): ) -year-old male with liver metastasis for possible embolization. Diagnostic angiography is performed to determine if the patient is a candidate for embolization. Via a right transfemoral approach, the celiac artery is selected and imaged (772), demonstrating normal anatomy without stenoses. The splenic artery is selected and imaged for portal venous perfusion evaluation. This shows normal splenic arterial anatomy and a widely patent splenic and portal vein (2, 77). The left gastric artery is selected and imaged, showing no collateral flow to the left lobe of the liver (2, 777). The gastroduodenal artery is selected and imaged with normal findings (27, 777). This vessel can be coil embolized prior to hepatic chemo-infusion or chemo-embolization. The right hepatic (2, 777) and left hepatic (2, 777) arteries are also selected and imaged, showing normal anatomy and a tumor in the right lobe. The cystic artery to the gallbladder is present and must be avoided during embolization.
162 ote: The celiac selective catheter placement code is included in the more selective catheter placements in the left and right hepatic arteries. To code for S&I codes, images must be obtained with purpose (medical necessity) and must be described and documented in the permanent medical record. 2) Patient with upper gastrointestinal bleeding after vomiting. Via a transfemoral approach, the celiac artery is selected and imaged (772). The gastroduodenal artery is selected and imaged (27, 777). o bleeding is seen in the duodenum. The left gastric is not seen off the celiac. ortogram is performed (no code), showing the left gastric arising as a separate vessel off the aorta. This is selected and imaged (2-9, 772-9), showing a hypervascular region with active bleeding at the gastroesophageal junction due to a Mallory-Weiss tear. This is embolized with gel-foam (72). Follow-up angiography (bundled) shows cessation of bleeding. ) Patient with bleeding duodenal ulcer at endoscopy. Via a transfemoral route, a catheter is placed in the celiac artery (2) and SM (2-9) with imaging performed (772, 772-9). ctive bleeding is seen in the region of the duodenum. Catheter is advanced into the anterior and posterior superior pancreatico-duodenal arteries of the celiac artery (add 27, 2; delete 2), and embolization with coils is performed (72). ext, the anterior and posterior divisions of the inferior pancreatico-duodenal arteries arising off the SM are selected and embolized [add 27-9 and 2 (embolization is included, as one surgical site), delete 2-9]. Follow-up angiography from all four vessels shows resolution of bleeding (bundled).
 arises anteriorly from the aorta at the L level and supplies the small bowel and colon.")
163 Diagnostic ngiography Coding Visceral ngiography Superior Mesenteric rtery ngiography Pages: - Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: The superior mesenteric artery (SM) arises anteriorly from the aorta at the L level and supplies the small bowel and colon. There is collateral supply via the gastroduodenal artery and the inferior pancreaticoduodenal arcade arteries to the
164 celiac arterial distribution and via the "arc of Bühler" and the "arc of Riolan" to the inferior mesenteric arterial distribution. The most common variant anatomy is a replaced right hepatic artery, which supplies a portion of the right lobe of the liver exclusively and arises as the first branch towards the right off the SM. CLIICL IDICTIOS: The most common indication for evaluation of the SM is GI bleeding. Other indications include portal hypertension, acute and chronic visceral ischemia, aneurysm, neoplasm, and trauma. Proximal visceral arterial stenoses are now treated successfully with angioplasty andor stent placement. Percutaneous thrombectomy may also be used in cases of acute thromboticembolic visceral ischemia. Distal coil embolization is a common treatment for bleeding sites. This vessel may be accessed to embolize the IM in patients with endoleak of an aortic stent graft. CODES: PROCEDURE DESCRIPTIO Superior mesenteric angiography, selective (with or without aorta) Replaced right hepatic angiography off the superior mesenteric artery, selective Right colic angiography, selective PRO C COD E P C TOT L RVU S&I COD E vs vs. 777 P C TOT L RVU
165 Ileocolic angiography, selective Jejunal or ileal branch angiography, selective vs vs dd-on Code CODIG ISTRUCTIOS:. Do not code a non-selective aortogram (72) when performed in conjunction with a selective visceral angiogram (772), as the code description of 772 states "with or without aortography".. SM angiography is often performed at the same time as evaluations of the celiac and inferior mesenteric arteries. 2. Use code 777 if additional selective catheter placement and imaging is performed after a basic selective superior mesenteric angiogram has been performed.. lways consider the many anatomic variations that exist when coding the visceral vasculature.. replaced right hepatic artery arising as a second order selective vessel off the SM, a direct origin of the left gastric artery off the aorta, a left hepatic artery arising off the left gastric artery, and a common or single trunk off the aorta supplying the celiac and superior mesenteric arteries are all common anatomical variants of the visceral arteries.. Do not use code 772 unless the catheter has been selectively placed in the superior mesenteric artery or in one of its branches. This is a selective code.. When the inferior mesenteric artery is not accessible due to presence of an abdominal aortic stent graft, and a catheter is advanced via the SM (after initial imaging with 772) via collaterals to the IM, any additional selective imaging would be reported with code 777, not 772 again.
166 EXMPLE(S): ) 7-year-old with small bowel bleeding on nuclear GI bleeding study. Via a right transfemoral route, a catheter is placed in the aorta and aortogram performed (2, 72). ormal anatomy is seen. The superior mesenteric artery is selected and completely imaged (add 2, 772; delete 2, 72, as they are included in SM catheter selection and visceral S&I codes). There is suggestion of vascular abnormality in the jejunum, requiring further selective imaging. The ileocolic and three jejunal branches are selected and imaged (add 2, 2, 2, 2, 777, 777, 777, 777; delete 2, as it is included in 2), showing an V malformation in the jejunum supplied by all three jejunal branches. The patient is sent to surgery for resection of this vascular lesion. 2) -year-old with recent aortic stent graft placement and documented endoleak. Via a transfemoral approach, a pigtail catheter is placed in the suprarenal aorta. ortogram shows no proximal anastomotic leak. The SM is selected with imaging (772 - includes initial abdominal aortography) showing the IM in a retrograde fashion. microcatheter is advanced via the middle colic artery to the left colic (27), and additional imaging of the IM is performed to delineate any leak (777). This shows an endoleak at the origin of the IM. The catheter is advanced to this level, and multiple coils are placed (722). Follow-up imaging (bundled) shows non-filling of the prior aortic endoleak. ote: If a second endoleak with coil embolization is treated via the iliolumbar artery, add a catheter placement and imaging code. However, since the aortic aneurysm is one surgical site, no additional embolization is coded. ) Patient with severe abdominal pain and acute visceral ischemia. Via a right brachial approach, a catheter is placed in the aorta, and aortography is performed (2, 72). SM and complete diagnostic angiography is performed (add 2, 772; delete 2, 72), showing embolus with clot in the SM and two jejunal branches. Primary thrombectomy of the SM (7) and the two branches (add 2, 2, 7; delete 2) is performed with an ngiojet device. Follow-up imaging (bundled) shows residual clot in the SM. Catheter-directed continuous infusion thrombolysis for four hours (72-9) with tp shows clinical improvement. Follow-up imaging (bundled) shows complete clearing of thrombus. Catheters are removed..
 arises anterolaterally towards the left at the level of the third lumbar vertebra just above the level where the aorta bifurcates into the iliac arteries.")
167 Diagnostic ngiography Coding Visceral ngiography Inferior Mesenteric rtery ngiography Pages: 7-9 Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: The inferior mesenteric artery (IM) arises anterolaterally towards the left at the level of the third lumbar vertebra just above the level where the aorta bifurcates into the iliac arteries. CLIICL IDICTIOS: The inferior mesenteric artery is often evaluated in cases of GI bleeding or visceral ischemia. The inferior mesenteric artery collateralizes to the median sacral artery
168 (recto-sigmoid region) and the superior mesenteric artery (in the splenic flexure region of the colon). The inferior mesenteric artery is a small vessel that may dramatically enlarge in cases of superior mesenteric artery occlusion to supply collateral flow to the SM and celiac distribution. The proximal inferior mesenteric artery may be embolized prior to or after aortic aneurysm endovascular therapy to prevent backflow into the residual aneurysm sac. CODES: PROCEDURE DESCRIPTIO Selective catheter placement, arterial system; each first order abdominal, pelvic, or lower extremity artery branch, within a vascular family Selective catheter placement, arterial system; initial second order abdominal, pelvic, or lower extremity artery branch, within a vascular family Selective catheter placement, arterial system; initial third order or more selective abdominal, pelvic, or lower extremity artery branch, within a vascular family PR O C C O DE P C T O T L R V U S &I C O DE vs vs P C T O T L R V U
169 dd-on Code CODIG ISTRUCTIOS: 7. Inferior mesenteric artery angiography is often performed at the same time as evaluation of the celiac and superior mesenteric arteries.. Use code 777 if additional selective catheter placement and imaging is performed after a basic inferior mesenteric angiogram has been performed. 9. lways consider the many anatomic variations that exist when coding the visceral vasculature, as well as the extensive collateral network between the celiac, SM, and IM vessels.. Do not code the non-selective aortogram (72) when performed in conjunction with a selective visceral angiogram (772). This is a bundled component of the visceral angiography.. Do not use code 772 unless the catheter has been selectively placed in the inferior mesenteric artery or in one of its branches. This is a selective code. 2. The IM is quite often visualized from a non-selective aortic injection with a pigtail catheter. This is not selective and is coded as an aortogram (72). The aortogram (72) cannot be coded if another visceral or renal artery is selectively injected, as codes 772 and 2-2 include aortography (72).. The IM is often embolized prior to or during an EVR (endovascular aortic repair) as a "non-target vessel" embolization. Use code 722 for this type of arterial embolization, along with the selective catheter placement. Imaging of the aorta and its branches is bundled with EVR cases.. Code 772 has an MUE of three.. Do not confuse "IM", as it can refer to either internal mammary angiography or inferior mesenteric angiography. EXMPLE(S): ) 79-year-old female with lower GI bleed. Both superior mesenteric and inferior mesenteric arteries are selected and imaged (2, 2-9, 772, 772-9) after an initial aortogram [no codes, as the aortogram imaging (72) and catheter placement (2) are included in the selective procedure]. Diverticular bleeding in the left colon is seen. n infusion catheter is placed into the IM and continuous infusion of vasopressin started (no existing CPT code for this procedure; consider unlisted code 7799). One hour follow-up angiography shows continued bleeding, so superselective embolization with a microcoil is done (72) with occlusion of the bleeding branch of the IM. ote: Vasopressin infusion therapy is rarely performed, with embolization more likely to be used as a definitive treatment for arterial bleeding in the gastrointestinal tract.
, celiac (2-9, 772-9), and selective right and left main renal arteriograms (22) are performed with normal findings. o active hemorrhage.")
170 2) Trauma patient. bdominal aortogram (bundled) was initially performed with normal findings. Selective SM (2-9, 772), celiac (2-9, 772-9), and selective right and left main renal arteriograms (22) are performed with normal findings. o active hemorrhage. Due to an infrarenal abdominal aortic aneurysm, the IM cannot be selected, so a pigtail catheter is placed near the IM origin with contrast injections and imaging performed [no codes, as aortogram (72) is bundled into 772; the IM imaging was not performed selectively]. The IM and its distal distribution are normal without extravasation of contrast. Diagnostic ngiography Coding Visceral ngiography Renal ngiography Pages: - Procedure Clinical Indications Codes Coding Instructions Example(s) References
171 PROCEDURE: The renal arteries arise posterolaterally from the aorta and supply the kidneys, which are retroperitoneal structures. The main renal arteries arise at the L-L2 level on each side of the aorta. Usually there is one artery to each kidney; however, there may be several on each side. More than one renal artery per side is common. The renal artery may also arise from the iliac artery (rare). Renal transplants, however, do have their arterial supply arise from the iliac artery, as the surgeon usually places the transplant kidney in the pelvis. nother variant anatomy is the horseshoe kidney. This variant consists of both kidneys conjoined across the midline anteriorly with multiple vessels arising from the mid-abdominal aorta supplying this kidney. CLIICL IDICTIOS: Evaluation of the renal arteries is performed for hypertension, stenosis, renal insufficiency, trauma, neoplasm, aneurysm, and polyarteritis nodosum work-up. Stenosis of these vessels may be found at the origin of the vessel (related to aortic plaque) or in the vessel itself. The cause of stenosis may be atherosclerotic or fibromuscular dysplastic in origin. CODES: PROCEDURE DESCRIPTIO Selective catheter placement (first-order), main renal artery and any accessory renal artery(s) for renal angiography, including arterial puncture and catheter placement(s), fluoroscopy, contrast injection(s), image postprocessing, permanent recording of images, and radiological supervision and interpretation, including pressure gradient measurements when performed, and flush aortogram when performed; unilateral Selective catheter placement (first-order), main renal artery and any accessory renal artery(s) for renal angiography, including arterial puncture and catheter placement(s), fluoroscopy, contrast injection(s), image postprocessing, permanent recording of images, and radiological supervision and interpretation, including pressure gradient measurements when performed, and flush aortogram when performed; bilateral P R O C C O D E P C T O T L R V U S & I C O D E P C T O T L R V U
172 Superselective catheter placement (one or more second order or higher renal artery branches) renal artery and any accessory renal artery(s) for renal angiography, including arterial puncture, catheterization, fluoroscopy, contrast injection(s), image postprocessing, permanent recording of images, and radiological supervision and interpretation, including pressure gradient measurements when performed, and flush aortogram when performed; unilateral Superselective catheter placement (one or more second order or higher renal artery branches) renal artery and any accessory renal artery(s) for renal angiography, including arterial puncture, catheterization, fluoroscopy, contrast injection(s), image postprocessing, permanent recording of images, and radiological supervision and interpretation, including pressure gradient measurements when performed, and flush aortogram when performed; bilateral Introduction of catheter, aorta (with abdominal aortogram) CODIG ISTRUCTIOS:. Codes 2-2 describe selective diagnostic renal angiography. 7. Do not use code 777 if additional selective catheter placement and imaging is performed after a basic renal angiogram is completed. dditional catheter placements and imaging of accessory or branch renal arteries are included in codes Most renal interventions involve angioplasty, stenting, or embolization. 9. Imaging may be done with CO 2 or gadolinium in patients with renal insufficiency. The imaging codes are the same.. Do not use code 2 for selective catheterization of renal artery origins selected off the aorta (or iliac, if a transplant kidney), as the catheter placements are bundled with diagnostic renal angiography codes Do not use codes 2-2 unless the catheter has been selectively or superselectively placed in the renal artery or one of its branches. These codes are defined as selective or superselective. 2. Do code for selective catheterization of renal arteries (2-2) when performed for intervention only (without diagnostic renal imaging). This may occur when stent placement is performed based on recent CT, MR, or catheter-based angiography.. Do not code for aortogram (72) when performed in conjunction with a selective renal angiogram (2-2). The aortogram is bundled into the renal code description.
173 . Do not use a -9 modifier with the abdominal aortogram code (72) when done with renal angiography (2-2). This would be considered inappropriate unbundling.. There may be multiple accessory renal arteries arising off the aorta. These are bundled into codes Placing a catheter "at" the renal artery is not the same as "in" the renal artery. "t" implies the catheter is still in the aorta (e.g., use code 72). Engaging the orifice of a vessel with a catheter is considered a selective catheter placement. 7. "Selective" renal angiography is unlikely if performed with a pigtail catheter. "Selective" refers to the catheter placement, not to the imaging performed.. Use of a "selective" catheter does not guarantee that it has been placed selectively in the vessel. Be sure documentation supports placement of the catheter tip selectively into the artery (which includes the orifice of the vessel). 9. "Selective" renal angiograms performed at the time of cardiac catheterizations must meet requirements of medical necessity. Please refer to strict guidelines from your payer. 7. Selective renal angiography codes are based on selective (first order catheter selection) and superselective (second order or higher catheter selection) catheterization. 7. on-selective renal angiography is described by code 72 if complete aortography done. 72. bdominal aortography (if done) is included in codes ccessory renal angiography (catheterization and imaging) is included in codes Codes 2-2 include selection and imaging of one or more accessory renal arteries. 7. Codes 2-2 include vascular access, selective or superselective catheter placement, imaging of the renal artery (or arteries), D reconstruction, pressure gradients across the stenosis, aortography (if performed), and vascular closure of the access site. 7. Do not code separately for D reconstructions (do not use code 77 or 777), as this is bundled with codes Codes 2 and 2 are unilateral renal codes. 7. Codes 22 and 2 are bilateral renal codes. 79. Codes 2 and 2 include superselective catheter placements and imaging of one or more second order or higher renal artery branches. These codes also include selection and imaging of one or more accessory renal arteries.. Consider unlisted code 7799 for renal intravascular Doppler (FFR) without angiography of the renal arteries. Pressure measurements are included in codes Use code 722 for initial vessel diagnostic renal artery intravascular ultrasound (IVUS) when performed. Use add-on code 72 if an additional vessel IVUS is performed.
174 2. Diagnostic renal angiography, catheter placements, and pressures are bundled with transcatheter renal denervation codes T and 9T.. Do not report codes 2-2 or 72 with codes T and 9T. EXMPLE(S): ) Patient presents with severe hypertension, despite current three-drug regimen of anti-hypertensives. bnormal renal Doppler. Via a transfemoral route, non-selective aortogram shows two right and one left renal artery with % ostial stenosis of the left renal artery. First order selective catheterization and imaging of all three vessels is performed (22). Primary stent placement is performed (72) with follow-up imaging (included in the stent placement procedure) showing no residual stenosis. ote: If the renal angiography was not diagnostic (e.g., guiding shots for planned intervention), change code 22 to 2 (for catheter placement related to unilateral stent placement) as appropriate. 2) Patient presents with blunt trauma and hematuria. Via a left brachial approach, a pigtail catheter is advanced into the abdominal aorta for aortogram (bundled with selective renal angiogram). The right renal artery is normal as seen from aorta. Three left renal arteries are seen. Each left renal artery is separately selected and imaged (2). Compression of the kidney due to hematoma is present, but no active bleeding is seen from any of the three vessels imaged. o embolization is performed. ) Patient with heart disease, drug-resistant hypertension, and hip claudication undergoes diagnostic native coronary angiography (9) and pull-back angiography of the abdominal aorta and iliofemoral arteries (7-9) via pigtail catheter injection at the level of the renals and then, after repositioning, at the aortic bifurcation. The renal, iliac, and coronary arteries are patent without significant stenosis. The abdominal aorta is non-aneurysmal. ) Patient with known % right renal artery stenosis due to fibromuscular disease (FMD) seen on recent heart catheterization. From a right femoral approach, a guiding catheter is placed in the right renal artery (2), and imaging is performed (not coded, as done for sizing and guidance and patient had a recent diagnostic renal arteriogram), confirming FMD. Balloon angioplasty with a mm balloon x seconds at TM is performed (72). Follow-up imaging shows dissection leading to acute vascular occlusion. With guidewire in place, a mm stent is placed, resolving the dissection (add 72, delete 72) and restoring flow.

175
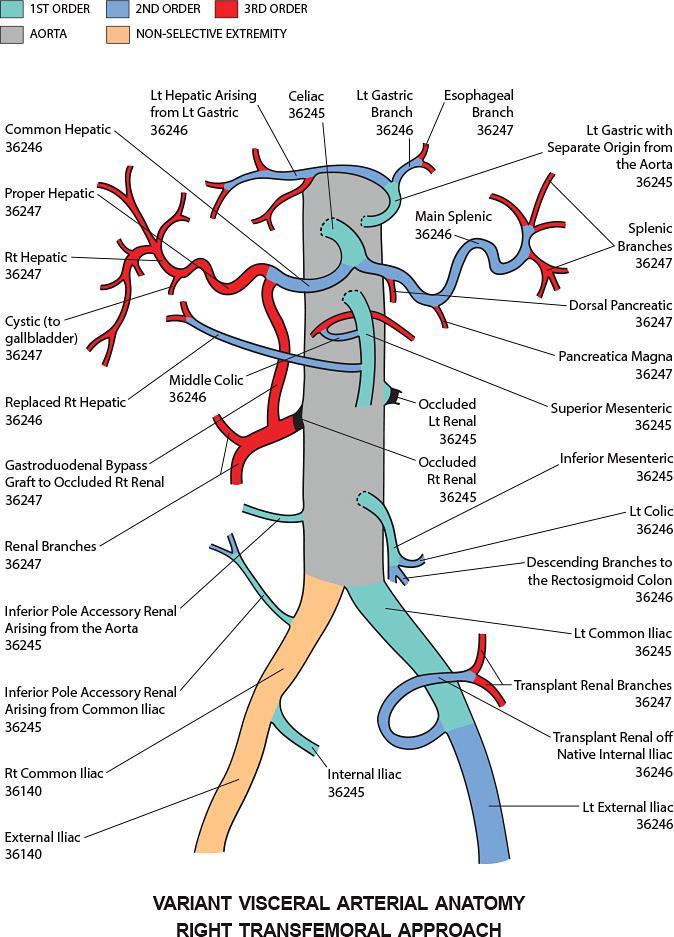
176
177 Diagnostic ngiography Coding Visceral ngiography Other Visceral Vasculature Pages: - Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: fter an abdominal aortogram, the adrenal arteries, inferior phrenic arteries, and gonadal arteries may be catheterized and imaged to evaluate blood flow to these regions. The inferior phrenic vessels supply the diaphragm. The gonadal arteries
178 supply the ovaries and testicles and are considered pelvic structures. The middle or median sacral artery supplies the sacrum, but may be parasitized to supply pelvic masses. Other visceral vessels in the chest include pericardial, mediastinal, and esophageal branches. CLIICL IDICTIOS: Diaphragmatic trauma and hemorrhage, adrenal or gonadal neoplasm, and collateral supply to other pelvic neoplasm. These vessels may require embolization in cases of trauma and neoplasm. CODES: PROCEDURE DESCRIPTIO PROC CODE Unilateral inferior phrenic angiogram 2 Bilateral inferior phrenic angiogram 2- P C T O T L R V U S&I CODE 79 vs vs. 772 x 2 Inferior epigastric angiogram (additional vessel, selective, after basic extremity angiogram): 2.. P C 2 2 T O T L R V U
179 Ipsilateral femoral approach Contralateral femoral approach Gonadal (ovarian, testicular) angiogram drenal angiogram, unilateral (may be multiple) drenal angiogram, bilateral (may be multiple) 2 2 or 2 2 or dditional vessel, selective, after basic exam 2X (may be st, 2 nd, rd, or additional 2 nd or rd order selective). 9 Median sacral or dd-on Code
180 CODIG ISTRUCTIOS:. Use code 79 (unlisted) for inferior phrenic angiography to evaluate the diaphragm. If the inferior phrenic artery supplies a visceral structure (e.g., liver tumor), use code 772 or 777 as appropriate instead.. Use the appropriate S&I code that describes the area imaged (e.g., use code 77 for median sacral angiography for angiography describing collateralization to a pelvic mass and code 77 when angiography describes collateralization to a spinal mass or VM).. The inferior phrenic artery may arise from the aorta, superior adrenal, or left gastric artery. EXMPLE(S): ) To evaluate a left diaphragmatic mesothelioma, the left inferior phrenic (2-9, 79), left gastric (2, 772-9), and left adrenal (arising off the left renal) (2-9, 77) arteries are injected and imaged. o significant blood flow to the tumor is seen on these injections. 2) Patient with pelvic trauma and bleeding. From a brachial approach, aortography (bundled with 772), inferior mesenteric (2-9, 772), bilateral ovarian (2-9 x 2, 77, 77-9), and bilateral internal iliac (2, 2-9, 77-9 x 2) angiography is performed after selectively catheterizing these vessels. ctive extravasation of contrast from the left obturator artery is identified. This is selected (add 27, delete 2) and embolized (72) with coils. Follow-up angiography shows cessation of bleeding (bundled). ote: Code 772 has an MUE of three. Code 77 has an MUE of two.
")
181 Diagnostic ngiography Coding Upper Extremity ngiography Pages: 9- Procedure Clinical Indications Codes Coding Instructions Example(s) References
182 PROCEDURE: Upper extremity angiography can be performed from a femoral or a retrograde brachial approach. CLIICL IDICTIOS: Indications include ischemia related to proximal large vessel atherosclerotic vascular disease or ischemia related to small vessel disease as seen in Raynaud's disease, trauma, or upper extremity arteriovenous shunt inflow evaluation. rteriovenous malformations in the shoulder may involve branches of these vessels. Gunshots, stab wounds, and iatrogenic injuries may result in vascular disruption and pseudoaneurysm requiring embolization or stent grafting. Stenotic disease may require angioplasty or stenting. CODES: PROCEDURE DESCRIPTIO Introduction of needle or intracatheter, upper or lower extremity artery Selective catheter placement, arterial system; each first order thoracic or brachiocephalic branch, within a vascular family Selective catheter placement, arterial system; initial second order thoracic or brachiocephalic branch, within a vascular family Selective catheter placement, arterial system; initial third order or more selective thoracic or brachiocephalic branch, within a vascular family Selective catheter placement, arterial system; additional second order, third order, and beyond, thoracic or brachiocephalic branch, within a vascular family (List in addition to code for initial second or third order vessel as appropriate) PR OC CO DE P C TO T L RV U
183 S&I Codes ngiography, extremity, unilateral, radiological supervision and interpretation ngiography, extremity, bilateral, radiological supervision and interpretation Costo-vertebral trunk angiography (additional selective vessel after basic exam to see the supreme intercostal) dd-on Code CODIG ISTRUCTIOS: 7. Codes 2 and 7 are deleted in 2 and replaced with existing codes and 77 respectively.. If extremity angiography from a remote access is done to evaluate the necessary inflow of an V fistulagraft, and the venous follow-through to evaluate the graft and outflow veins of a shunt, use code 9-2 (or -7 for hospital billing) to describe the imaging procedure performed. Selective catheter placement may be separately reported. lso use code 9-2 (or -7 for hospital billing) for the same imaging if performed via a pre-existing catheter or sheath in the graftfistula. 9. Use code 77 if only the subclavian artery is imaged. If imaging of the rest of the arm is performed, even if the catheter is moved, only add the selective catheter placement code (e.g., 27), but do not use code 777, as you are merely completing the exam. 9. Use code 777 if additional selective catheter placement and injection after the basic exam is performed. Remember a "complete" upper extremity angiogram (77) must be done first, then additional selective (777) imaging may be coded to further evaluate an area of concern after the catheter is advanced to a higher level of selectivity. Code 777 may also be used to describe selective imaging of branches arising off the subclavian
184 artery or other upper extremity branches after initial extremity (77) or vertebral imaging (22, 22). 9. Extremity angiography may be done with or without an arch exam. Use codes 22 and 77 if arch and unilateral extremity angiography are performed. 92. Variant anatomy of brachial, radial, and ulnar arteries exists, with high take-off of the radial artery the most common. 9. If the catheter is introduced via a brachial artery access and the catheter reaches the aorta, the catheter placement code changes from to 2. The S&I code remains the same (77). 9. If a catheter is introduced via an V fistulagraft and imaging is performed (9), then catheter is advanced into the native upper extremity arterial system centrally, additionally report code 2 for catheter placement. If the catheter is further advanced into the aorta from this position, keep code 2. Do not change to 2. Report code 77 for the additional upper extremity arterial evaluation. 9. Code 77 describes ipsilateral upper extremity imaging when subclavian occlusion prevents catheter movement into the aorta. Use code for the catheter placement if via the radialbrachial artery approach. 9. Do not use code 77 for routine imaging of a radial artery access (usually for cardiac catheterization). This is a normal component of the procedure via this access. If complete occlusion is seen centrally, necessitating a different access for the heart catheterization, consider codes 77 and. 97. Code 77 is a non-selective imaging code and does not require the catheter to be placed in that vessel. 9. Retrograde brachial arteriography is an upper extremity angiogram that involves catheter placement in the brachial artery directed toward the chest with injection and imaging of that arm. Use code 77 to describe this upper extremity imaging. If performed only to image the vertebral, use code 22 and delete codes 77 and. 99. The distinction between second and third order selectivity in the left upper extremity from a transfemoral approach is the origin of the profunda brachialis artery per SIR. M ppendix L considers the entire left brachial artery as second order selective with the ulnar, radial, and interosseous as third order vessels. 2. There is no code for injection of Priscoline or nitroglycerin used to vasodilate distal arterial branches for diagnostic work-up. It is included as part of the exam, as are duplicate images with the arms repositioned in abduction and adduction. 2. Do not use code 77 when subclavian artery injection is performed to image and evaluate the vertebral artery. Use code 22. This includes the selective catheter placement in the subclavian or innominate arteries. 22. Use code 77 when subclavian artery imaging shows occlusion of the vertebral artery and only the subclavian is evaluated. Do not code for subclavian imaging that only confirms the "absence" of the left vertebral artery off the subclavian due to its direct origin off the arch. Use code 22 instead of 77 when left subclavian injection is performed in patient with
185 occluded vertebral origin when delayed images show reconstitution of the vertebral artery in the neck via collaterals. This bundles the catheter placement. 2. Do not use code 77 for imaging of the vertebral artery origin prior to catheter placement selectively in the vertebral. This is part of the vertebral artery evaluation and is considered a "guiding shot". The selective vertebral imaging code is 22 and bundles the catheter placement. 2. Use codes 2 and 777 for selection of subclavian branches to further evaluate the neck and shoulder after vertebral imaging (22, 22). 2. Do not use code 77 for imaging of all necessary native arterial inflow of an V fistulagraft. This is considered a routine portion of a shuntogram (9). If medically necessary and a full and complete study of the upper extremity arterial system separate from the V fistulagraft is performed along with a separate V fistula study, consider adding code 77. If V fistulagraft evaluation is performed via a pre-existing catheter in the shunt or via a remote catheter, code 9-2 (or -7 for hospital billing) may be used to describe all imaging necessary to evaluate the V fistulagraft. 2. Codes 77 and 77 require a -9 modifier if true diagnostic angiography is performed at the same setting as a subclavian arterial angioplasty or stent placement. 27. Code 77 is a unilateral code. If both upper (or lower) extremities are evaluated, use the bilateral code 77. Do not use code 77 twice, unless one arm and one leg are evaluated. EXMPLE(S): ) Patient with cold fingers. Via a right transfemoral approach, catheter is advanced to the arch. rch aortogram (22) is followed by selective left subclavian angiography (2, 77). The exam is repeated (no additional codes) with arms abducted. Priscoline is given, and repeat images are obtained (no additional codes). The catheter is advanced to the brachial artery, and imaging is performed to complete the upper extremity angiogram (add 27, delete 2, no additional imaging codes). The study is repeated after micrograms intra-arterial nitroglycerin injection (no codes). The catheter is removed. 2) -year-old with ischemic fingers and decreased left arm pressure. Via a left brachial artery approach, a catheter is advanced to the mid-axillary level and contrast injected with imaging of the left arm and subclavian region showing a 9% axillary stenosis (, 77-XU). mm stent is placed (72) with resolution of the stenosis. ) -year-old female with newly documented left vertebral steal and poorly functioning left V shunt in the forearm and decreased brachial artery pulse. Puncture and sheath placement in the graft with angiographic evaluation of the arterial inflow, graft, and venous outflow to the right atrium shows no evidence of stenoses (9). catheter is advanced across the arterial anastomosis centrally to the level of the subclavian artery. Injection and imaging shows 9% stenosis of the proximal left subclavian artery (2, 77-9). This is treated with a 7 mm balloon expandable stent (72). To deploy this safely, the catheter is advanced into

186 the aorta (no catheter code change). Follow-up imaging shows widely patent vessels (no code). Diagnostic ngiography Coding bdominal ortography and Lower Extremity ngiography bdominal ortography and Run-off Pages: -7
187 Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: bdominal aortography and run-off can be performed a variety of ways, but typically involves catheter placement in the aorta with imaging of the aorta and lower extremities. Examples given below show the many varied techniques currently used. CLIICL IDICTIOS: Most commonly this study is performed to evaluate peripheral vascular disease and symptoms of claudication or ischemia of the lower extremities. The exam may also be used to evaluate aneurysms, pseudoaneurysms, vasculitis, prior surgery, tumors, VMs, and trauma. CODES: PROCEDURE DESCRIPTIO PROC CODE P C TOTL RVU S&I CODE PC TOTL RVU ortogram
188 orto-iliofemoral run-off 2. 7 Unilateral lower extremity run-off Varies 77 Bilateral lower extremity run-off Varies dditional selective imaging after basic exam Varies dd-on Code CODIG ISTRUCTIOS: 2. Use code 777 for additional imaging after a basic exam is completed and a more selective catheter placement has been performed. 29. Do not use code 777 for images obtained to "complete" a run-off exam, even if a more selective catheter placement has been done. Do code for the more selective catheter placement in this situation. 2. Discuss accuracy of documentation with the individual physician performing the procedure, as this greatly affects the appropriate coding. Most importantly, if a catheter placement or repositioning is not clearly described, a lesser exam may need to be coded. 2. Do not use code 77 for oblique views of the pelvis. Code 77 requires placing the catheter in a selective pelvic artery (e.g., the internal iliac artery or one of its branches, not the common or external iliac artery). Code 77 is used to image pelvic structures (e.g., the uterus or bladder). 22. Do not use code 777 for additional lateral, oblique, or rotational views without additional selective catheter movement. 2. Use code 7 for aorto-pelvic angiography performed for work-up, despite any catheter movement between the aortic and the pelvic oblique study. This includes imaging of the abdominal aorta and bilateral oblique views of the pelvis. If initial imaging is done at the time of EVR, even if a diagnostic study has not been done previously, it is bundled and not reported. 2. Use code 7 if complete angiogram and run-off performed from a single catheter position or if the documentation does not support separate complete studies from two catheter positions.
189 2. Use codes 72 and 77 if full and complete aortogram and a separate run-off study are performed from high and low catheter positions in the aorta. 2. Code 7 requires imaging of the abdominal aorta, not just the distal most aspect of the aorta. This distal most portion of the aorta is incidentally and routinely seen when a pigtail catheter is injected at the level of the aortic bifurcation for the purpose of bilateral lower extremity angiography and is part of code If lower extremity endovascular revascularization is performed at the same setting as a diagnostic lower extremity study, the catheter placement in the interventional target vessel is bundled, unless the intervention is performed via a separate access [e.g., right femoral access for diagnostic run-off with catheter placement into the contralateral left SF for additional imaging prior to intervention, followed by left popliteal access for stent placement into the left SF; the diagnostic catheter placement (27) is billable, and the popliteal access catheter placement for stent placement is bundled]. EXMPLE(S): ) ortogram and complete bilateral run-off from one catheter position (2, 7). 2) ortogram and unilateral run-off from one catheter position in the aorta (2, 7). ) ortogram and complete bilateral run-off beyond the pelvis from two catheter positions (high and low aortic catheter positions) (2, 72, 77). ) ortogram and pelvis from one catheter position (2, 7). ) ortogram and pelvis from one catheter position using CO 2 as contrast agent (2, 7). ) ortogram and pelvis (iliac and femoral arteries) from high and low aortic catheter positions (2, 7). ote: This is typically performed during aortic aneurysm work-up. Code 7 is used despite the catheter movement. 7) Contralateral unilateral left leg run-off via separate stations (catheter placed at the left common iliac, left common femoral, and left popliteal with injections performed) using CO 2 as contrast agent (27, 77). ) Same patient as #7, however, popliteal angioplasty is then performed (add 722, delete 27). 9) ortogram from high aortic catheter position, run-off by selective catheter placement in each common iliac (via femoral approach: 2, 72, 77; via brachial approach: 2-, 72, 77). ) ortogram and complete run-off from high and low aortic catheter position with additional imaging by selective catheter placement in the contralateral external iliac artery (2, 72, 77, 777). ) ortogram and complete run-off from high and low catheter positions (via femoral approach) with selective catheter placement and additional imaging from the contralateral common femoral artery with pull back into the ipsilateral iliac and additional images of the ipsilateral leg (2, 72, 77, 777).
190 ote: Do not use a second 777, as the ipsilateral iliac is additionallynon-selective instead of additionally selective, as required by the description of code ) Via transbrachial approach, aortogram and complete lower extremity run-off from high and low catheter positions with selective catheter placement into both superficial femoral arteries for additional imaging (27-, 72, 77, 777 x 2). ) ortogram from high aortic catheter position, unilateral run-off from low catheter position (2, 72, 77). ) Patient with bilateral hip claudication. ortogram from high aortic catheter position, repositioning of the catheter for bilateral pelvis obliques for iliacs and proximal femoral arteries bilaterally, followed by selective unilateral lower extremity angiography from catheter position in the contralateral common femoral artery (2, 72, 77) to complete the study. ) Same as example #, but left hip claudication. Via right transfemoral approach, aortogram from high aortic catheter position, repositioning of the catheter for bilateral pelvis obliques to evaluate the "left" iliac and proximal femoral artery followed by selective unilateral left lower extremity angiography from catheter position in the contralateral common femoral artery (2, 72, 77). ote: Right iliac imaging is considered incidental in this case and not medically necessary. If the physician states why the right-sided imaging was necessary, change code 77 to 77. ) ortogram from high catheter position. Contralateral unilateral run-off from low aortic position. Ipsilateral run-off via the sheath (2, 72, 77). 7) ortogram via brachial artery approach with catheter low in aorta, lower extremity run-off via collaterals after catheter pulled back into the mid-thoracic aorta (2, 72, 77). ) ortogram and run-off via translumbar approach, one catheter position in the aorta (, 7). 9) ortogram and run-off via translumbar approach with high and low aortic catheter positions (, 72, 77). 2) ortogram and run-off via translumbar approach with catheter positioned in the aorta and repositioned into both common iliac arteries (2-, 72, 77). 2) ortogram and run-off from high and low catheter positions with selective unilateral renal angiography (2, 77). 22) ortogram and run-off from one catheter position with selective bilateral renal angiography (22, 77). 2) ortogram and pelvis from one catheter position with selective visceral (celiac) angiography (2, 772, 77). ote: In this case, the pelvic (iliofemoral portion) of the study is reported with code 77. The aortogram is bundled into code ) Lower extremity angiography with catheter position in the low abdominal aorta, findings describe iliacs and run-off only (2, 77). 2) Lower extremity angiography with catheter position in the low abdominal aorta, findings describe a significant portion of the distal aorta (including one or more visceral or renal arteries or a description of disease in the aorta itself), iliacs, and run-off (2, 7).
191 2) on-selective renal angiography, including aortogram, followed by low catheter positions and complete bilateral lower extremity angiography at the time of a selective native coronary angiogram (9, 72-9, 77-9). ote: on-selective aortic catheter placement (code 2) is bundled with the heart catheterization and not separately billed. For code 77-9, the bilateral run-off study should be as complete an exam as if performed at a time separate from a cardiac catheterization procedure. For code 72-9, the aortography study should be as complete an exam as if performed at a time separate from a cardiac catheterization procedure. 27) Complete aortography with attention to the renals (72-9) and pelvic oblique non-selective iliac angiography (add 7-9, delete 72-9) at the time of a left heart catheterization procedure with selective coronary artery injections, imaging, and left ventriculography (9). 2) bdominal aortogram (72-9) for abdominal aortic aneurysm work-up and complete bilateral lower extremity run-off (77-9) for claudication at time of native coronary angiography (9). ote: The aortogram and peripheral run-off studies must be as complete an exam as if performed at a time separate from the cardiac catheterization. 29) Right femoral puncture with right leg run-off via the sheath. Left femoral puncture with left leg run-off also via the sheath (patient had bilateral common iliac occlusion). ortogram is performed at the renal level using brachial approach (2, -9, 72, 77). ) Same as example #29. Right femoral puncture with right leg run-off via the sheath. Left femoral puncture with left leg run-off also via the sheath (patient had right common liiac occlusion). The left femoral catheter is advanced to the L-2 level and aortogram done (2, -9, 72, 77). ) xillo-femoral bypass graft is accessed with a sheath along the chest wall. catheter is advanced into the subclavian, then the aorta to the level of the renals. ortogram is performed (2, 72). The catheter is removed, and bilateral lower extremity arteriogram (patient also has a fem-fem cross-over graft) is performed via the sheath (77) in the axillo-femoral bypass graft. 2) Left common femoral to right common femoral cross-over graft is accessed from the right towards the left. Right leg angio is performed. The catheter is advanced to the left iliac and left leg run-off is done (77). The catheter is advanced up through the left iliac to the renals and aortogram performed (72, 2 for catheter position in the aorta). ) Same patient as #2, however, the catheter is advanced from the fem-fem cross-over graft into the left superficial femoral artery (2), and diagnostic left leg angiography is performed. Diagnostic right leg angiography is performed through the sheath (77-9). n angioplasty followed by stent placement across a left mid-superficial femoral artery % stenosis (add 722, delete 2) with excellent results. ) Patient with bilateral axillary femoral bypass grafts. Each graft is accessed at the abdominal level. Sheaths are placed. Each side is injected, and imaging of the legs is performed separately (-9, 77). catheter via the left sheath is advanced to the aorta, and cervicocerebral arch angiography is performed (22) to fully evaluate the cervicocerebral arch and proximal brachiocephalic vessels. Each
192 subclavian artery is selected (add 2-9, 2), and complete imaging of the bilateral subclavian, axillary, and brachial arteries (including the bilateral ax-fem anastomoses) is performed due to digital ischemia of the hands (77-9). ) Patient with left axillary-femoral and femoral-femoral artery bypass graft. The left axillary-femoral graft is accessed antegrade with a sheath. Left lower extremity angiography is performed via the sheath. catheter is advanced into the fem-fem graft (2), and right lower extremity angiography (77-9) is performed. This is exchanged for a mm balloon, which is advanced over a wire across a 9% right popliteal stenosis (delete 2, bundled with angioplasty) and angioplasty performed (722) with excellent results. ote: If drug-eluting balloons are utilized in the procedure, hospitals should bill code C22 for each balloon. ) Same patient as #, however, a stent or stent graft is placed in the popliteal stenosis for treatment of occlusive disease (722). 7) Same patient as #, however, treatment with a stent or stent graft is for popliteal aneurysm (not occlusive disease) (27, 72). ) Right femoral puncture with catheter placement at the level of the renals for aortogram and complete run-off to the feet from this catheter position (2, 7). This is followed by selective catheter placement to the left common femoral (add 2, delete 2) for additional images of disease at the popliteal level (777). The catheter is then further advanced into the popliteal artery (add 27, delete 2), and additional images of the trifurcation (777) show much worse distal disease than initially thought. 9) The patient is placed prone. Via a right popliteal puncture, the catheter is advanced across an SF occlusion to the level of the renals. ortogram is done (2, 72). The catheter is pulled back into the common iliac artery, and right leg angiography is done (77-9). The mid superficial femoral artery occlusion is treated with laser atherectomy followed by stent placement (add 7227, delete 2). Follow-up angiography (no code) shows patency. ote: If an existing bypass graft is being intervened on, code the intervention, imaging, andor catheter placement based on the vessel the graft is replacing. For example, if a femoral-popliteal insitu saphenous vein bypass graft is in place, and contralateral selection (bundled with lower extremity revascularization codes) and angioplasty (722) are performed, use codes that describe the arterial intervention, not a venous intervention. ) bdominal aortogram, selective SM, celiac, and non-selective bilateral iliofemoral angiography are performed during EVR procedure [2-9 x 2, 7X (depending on EVR type)]. ote: Only code the selective catheter placements 2-9 x 2, as non-selective catheter placements and imaging of the aorta and its branches are bundled with the new 2 EVR procedure codes (7-7). Do not report code 772, 7, or 77 in this example, as the imaging is at the same setting as the endovascular repair of the abdominal aortic aneurysm. ) From a posterior tibial approach, a catheter is advanced across a known tibialperoneal trunk occlusion. This required a "Quick-Cross" catheter. therectomy with a Diamondback Orbital device followed by cryo-balloon angioplasty (7229) shows excellent results.
193 ote: Do not bill extremity angiography, as the patient had a "known" lesion and the imaging was used for guidance, localization, sizing, etc. The catheter placement is bundled with lower extremity revascularization. There is no S&I code with ) Patient has left leg run-off via catheter placement in the aorta (2, 77) due to LLE emboli. Left iliac aneurysm is present. This is treated with ilio-iliac tube endograft placement (add 77, delete 2 and 77, as diagnostic imaging and non-selective catheter placement are bundled). Follow-up to evaluate for distal embolization (bundled) shows patent vessels. ote: Iliac aneurysm repair with endograft is an inpatient-only procedure (status indicator C) for Medicare recipients. ) Via right common femoral approach, pigtail catheter is advanced for abdominal aortogram (bundled), followed by catheter exchange and selective celiac (2-9, 772), selective SM (2-9, 772-9), and superselective upper, mid, and lower pole left renal artery angiography with selection and imaging of two left accessory renal arteries off the aorta (all renal superselections and imaging bundled with 2). The catheter then selects the left common iliac (2-9) with left leg run-off and is pulled back to the right common iliac (bundled) for right leg run-off (77). 9% right common iliac artery stenosis is treated with a balloon deployable stent (722; catheter placements are unchanged). ) Recent CT (coded and billed with 7) shows bilateral external iliac and left popliteal 9% stenoses. Via right femoral approach, a catheter is placed in the aorta. Complete aorta-iliofemoral angiography confirms these stenoses. ngioplasty is performed at all three sites (722-, 722). ote: Do not use code 7, as the "complete study" was confirmatory only and did not change planned therapy. ) Same patient as #, however, there is change in clinical symptomalogy prior to the procedure with acute ischemia of the left leg (7), necessitating a new diagnostic study. Significant thrombus is seen in the left popliteal, which is treated with thrombectomy (7) and angioplasty of all three sites (722-, 722). ote: Code 7 is reported here, as there is "new or changed medical necessity since prior diagnostic CT".
194
195
196
197 Diagnostic ngiography Coding bdominal ortography and Lower Extremity ngiography Pelvic Vasculature Pages: 7-7 Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: Most pelvic vessels arise from the internal iliac artery. This vessel divides into two main vessels: the anterior division of the internal iliac artery (including the uterine, obturator, superior and inferior vesical, inferior gluteal, and internal pudendal arteries as well as collateral branches to the inferior mesenteric artery) and the posterior division of the internal iliac (including the superior gluteal and iliolumbar
198 arteries). Code 77 requires selective catheter placement into the internal iliac artery or one of its branches (or of a vessel arising from the aorta or iliac arteries that supplies the pelvis including the ovarian, testicular, and median sacral arteries). Variant anatomy of the internal iliac arterial branches is common. Prostatic artery embolization for treatment of benign prostatic hyperplasia (BPH), iatrogenic vascular injury, or neoplastic hemorrhage is occasionally performed. CLIICL IDICTIOS: This study may be performed for evaluation of pelvic trauma, VM, aneurysm, dysfunctional uterine bleeding, and uterine fibroids. The pelvic vasculature is also imaged when aortic stent graft endoleak is found, as there may be collateral flow to the aneurysm sac via iliolumbar artery collaterals. Impotence may be related to internal pudenal artery stenoses. CODES: PROCEDURE DESCRIPTIO PROC CODE S&I CODE Pelvic angiography selective, unilateral 2X 77 Pelvic angiography selective, bilateral 2X x 2 77, 77-9 P C TOTL RVU.. dditional vessel, selective, after basic exam 2X dd-on Code CODIG ISTRUCTIOS: 2. Catheter selectivity codes are based on the approach used. 29. The uterine and prostatic arteries are third order selective catheter placements from any approach.
199 22. Use code 77 once if the internal iliac artery is injected selectively to image sacral branches unilaterally during spinal angiography. 22. Use code 777 if additional selective catheter placement and imaging are performed after a basic pelvic angiogram has been completed Use codes 77 and 77-9 when reporting bilateral internal iliac imaging, as code 77 is a unilateral procedure code. There is no bilateral selective pelvic imaging code available. 22. Do not use code 77 unless the catheter has been selectively placed in the internal iliac artery, in one of its branches, or in a branch arising from the aorta or iliac artery supplying the pelvis. This is a selective imaging code. 22. Do not use code 77 for "obliques of the pelvis" performed from the aorta. Use code 77 for obliques with imaging of the iliacfemoral run-off vessels. Use code G27 for obliques of pelvis with imaging of the iliac arteries non-selectively at the time of cardiac catheterization. 22. Uterine fibroid embolization (72) allows separate coding for catheter placement in the internal iliac and ovarian arteries (and any other vessels supplying the fibroid uterus); however, any selective pelvic, selective ovarian, abdominal aortic, and any other angiography to evaluate the supply to and treat the fibroid uterus is for guidance and is not coded. Do not use code 77 with this procedure. When uterine artery embolization is performed for reasons other than fibroids (placental hemorrhage, uterine trauma), the imaging may be separately coded as appropriate, along with a different embolization code (722 for VM, 72 for hemorrhage). 22. Use code 77 x 2 for diagnostic bilateral selective pelvic angiography (i.e., internal iliac) prior to placement of temporary occlusion balloons (for use during high risk pelvic surgery), along with catheter placements (e.g., 2-). If the temporary balloons are inflated for prevention of bleeding, delete 77 x 2 and add code (or -7 for hospital billing). If inflated for treatment of active bleeding, use code 72-2 (or -7 for hospital billing). If coils are deployed, no modifiers are necessary Code 77 has an MUE of two. 22. The prostatic artery may be selected for embolization to treat BPH (72) or prostatic hemorrhage (72). The prostatic artery has great variation of anatomy, with the most common origins arising from the internal pudendal, superior or inferior vesical, gluteal, or obturator arteries. Many other less common anatomical variations exist. The prostate embolization is performed to decrease the size or volume of the prostate, similar to partial embolization of the spleen to treat hypersplenism. This embolization shrinks the overall size of prostate in men with urinary retention symptoms secondary to BPH. We recommend use of embolization code 72 for BPH treatment. If for hemorrhage, use code 72. EXMPLE(S): ) Patient with pelvic trauma presents for evaluation. Via a right transfemoral route, a catheter is placed selectively in each internal iliac artery with contrast injection and imaging (2-9, 2, 77, 77-9). o bleeding is seen.

200

201
202 Diagnostic ngiography Coding Diagnostic Dialysis Circuit Imaging Pages: 79-
203 Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: Dialysis circuits are created as vascular access sites required for hemodialysis. Dialysis circuits may be constructed in a variety of ways and at various locations. Most commonly these are located in the arm or forearm, and are V fistulae (direct artery to vein anastomosis) or V grafts (prosthetic material in a loop or straight configuration anastomosed to an artery proximally and a vein distally). Medicare has encouraged a shift from grafts to fistulae, as there is less infection and stenosis with the native vessel surgery. V fistulae may require weeks or months to mature for use in dialysis, thus requiring non-tunneled or tunneled central venous catheter placement for immediate temporary dialysis. Dialysis circuits may be placed in the upper arm, forearm, thigh, or chest. Shuntograms (angiograms of the shunt or fistula) allow for the diagnosis of stenoses and planning for interventions. CLIICL IDICTIOS: Thrombosis or poor flow with inadequate dialysis. The most common etiology of these problems are venous anastomotic strictures, but can also be caused by outflow vein or central vein stenosis, intra-shunt stenosis, or inflow arterial stenosis. Other problems may relate to difficulty obtaining access of the graft, failure of the V fistula to mature, peripheral extremity ischemia, pseudoaneurysm, infection, and occlusion. Occasionally collateral, competing vessels in V fistulae require embolization or surgical ligation to allow the primary venous outflow to mature and enlarge enough to support dialysis. CODES: PROCEDURE DESCRIPTIO PRO T S T
204 Introduction of needle(s) andor catheter(s), dialysis circuit, with diagnostic angiography of the dialysis circuit, including all direct puncture(s) and catheter placement(s), injection(s) of contrast, all necessary imaging from the arterial anastomosis and adjacent artery through entire venous outflow including the inferior or superior vena cava, fluoroscopic guidance, radiological supervision and interpretation and image documentation and report; Diagnostic angiography of the dialysis circuit performed via remote or existing access Introduction of needle or intracatheter, upper or lower extremity artery Selective catheter placement, arterial system; each first order thoracic or brachiocephalic branch, within a vascular family Selective catheter placement, arterial system; each first order abdominal, pelvic, or lower extremity artery branch, within a vascular family Selective catheter placement, venous system; first order branch (eg, renal vein, jugular vein) C COD E (or -7) 2 2 P C O T L R V U & I C O D E P C O T L R V U CODIG ISTRUCTIOS: 229. Code 9 is a complete code describing the initial access to an V fistula or graft (dialysis circuit) and includes the injection of contrast and all necessary imaging to complete the evaluation of the dialysis circuit. This includes imaging of the entire dialysis circuit, including the adjacent inflow artery (peri-anastomotic region), arterial anastomosis, shunt, and venous outflow up to and including the complete superior or inferior vena cava. 2. Code 9 includes advancement of the catheter across the arterial inflow vessel for arterial inflow evaluation. It does not include advancement of the catheter centrally in the upper extremity arterial vessels (additionally report codes 2 and 77) for evaluation of central arterial inflow.
205 2. When diagnostic angiography of the dialysis circuit is performed via a remote or existing access, report code 9-2 (or -7 for hospital billing). lso report selective catheter placement codes as appropriate when imaging is performed from a remote access. 22. Code 9-2 (or -7 for hospital billing) includes evaluation of the entire V shunt, extremity outflow veins, and central veins all the way to the right atrium performed via a pre-existing catheter in the fistulagraft or via a remote catheter. Central veins include the subclavian, brachiocephalic veins, and superior vena cava for arm shunts and the iliofemoral veins and inferior vena cava for leg shunts. Repeat injections with graft occlusive pressure (or use of occlusion balloon) to reflux contrast and visualize the arterial anastomosis and adjacent peri-anastomotic arterial inflow segment are also included. This combination of vessels is called the "dialysis circuit". 2. Report conventional catheterization codes (2, 2, 27) if percutaneous arterial access is established remotely from the shunt (e.g., transfemoral arterial catheter placement for subsequent diagnostic study or intervention), along with code 9-2 (or -7 for hospital billing). 2. Use code for direct brachial artery puncture done to evaluate a radiocephalic (V) fistula. Code 9-2 (or -7 for hospital billing) is used for the S&I. 2. ll access sites into the dialysis circuit for diagnostic shuntogram andor intervention are bundled with codes Code 9 includes the advancement of the catheter centrally into the SVC, IVC, or right atrium. It does not include selective vein branch procedures (e.g., for branch embolization use add-on code 99, which includes all selective venous catheter placements, embolization, S&I, and follow-up imaging). 27. dditionally report code 2 if, after shunt access and evaluation (9), selective catheterization of the upper extremity artery more centrally is necessary to evaluate proximal arterial inflow stenoses substantially away from the peri-anastomotic region (e.g., axillary or subclavian artery). Code 2 includes advancement of the catheter centrally into the aorta or distally into the wrist or hand. Imaging code 77-9 may also be reported for extremity angiography when done. 2. If venous collaterals or branches are selected and embolized, report add-on code 99, which includes all selective venous catheter placements related to the embolization. 29. Report conventional catheterization code 2 if percutaneous venous access is established remotely from the shunt (e.g., transfemoral venous access with placement of a catheter for subsequent diagnostic study or intervention of an upper extremity shunt), along with code 9-2 (or -7 for hospital billing). 2. Code 9 includes all additional separate accesses to an V fistula or graft (dialysis circuit) for the purpose of further imaging. If a therapeutic intervention (venoplasty, stent placement, thrombectomy, etc.) is performed, use the appropriate code from code range These codes include all catheter placements via the dialysis circuit access.
206 2. Only one code from code range 9-9 is submitted per session. These codes are built on a progressive hierarchy with the highest level intervention being billed. 22. There are no additional imaging codes to be added for angiography during or after completion of the shunt intervention (e.g., angioplasty, stent placement, thrombectomy). Dialysis circuit evaluation is included with codes 92-9, if done. If a diagnostic study is not performed, you can still submit codes 92-9 without a modifier. 2. Do not report code 9 more than once for access and evaluation of an V graft or shunt. ccess into the shunt may be single or multiple, but this code may only be used once to describe access and imaging for a diagnostic study. Code 9 and any additional direct access sites into an V graft or shunt for intervention are bundled with the intervention (92-9). 2. Do not report code 72, 727, or 72 when unilateral extremity venography of the same extremity or cavography is described during shuntogram. Codes 727 and 72 are considered bundled with arm shunt evaluation code 9. If venography of a different extremity is performed, add code 72 with an appropriate modifier. 2. Do not report code 77 for routine imaging of the immediate arterial inflow (peri-anastomotic segment) of an V fistula or shunt. This is clearly described as being included in code 9. This code includes "all necessary imaging from the arterial anastomosis and adjacent artery through the entire venous outflow". 2. Report code 77 if further imaging of the upper (or lower) extremity arterial system is medically necessary (e.g., onset of ischemic changes in the hand, distal to the arterial anastomosis; suspected arterial stenosis central to the peri-anastomotic arterial segment). (Catheter placement code 2 is additionally reported here, and code 9 is unchanged.) 27. If upper extremity angiography (77) is performed for separate medical necessity unrelated to the shunt and incidental imaging of a shunt is noted, these findings would be considered part of the normal venous outflow and code 9-2 (or -7 for hospital billing) would not be reported. If the shunt evaluation is necessary and fully evaluated via this remote access, the catheter placement code and 9-2 (or -7 for hospital billing) would be reported. 2. If imaging is via remote access [catheter placement in brachial artery via femoral approach- 27, 9-2 (or -7 for hospital billing)], and then a separate access to the graft is performed for intervention (venoplasty), delete code 9-2 (or -7 for hospital billing) and add the appropriate code(s) for the intervention (92-99). 29. If a graft study via direct access is performed (9), followed by selection of two branch veins for embolization, the embolization procedure, and follow-up angiography, report add-on code 99 with Ultrasound guidance for vascular access (797) may be additionally coded if necessary to obtain safe access into the V graftfistula (new or poorly developed fistulae, pseudoaneurysms, slow flow, or failing grafts), as long as
207 necessary documentation (per CPT Codebook) is in the physician's dictated report. 2. Do not code for "routine surveillance" shuntograms. These do not meet medical necessity. Findings or symptoms of shunt failure should be documented prior to performing an invasive procedure. 22. Stenoses must be accurately measured and documented with percent stenosis. Only hemodynamically significant stenoses (e.g., % or greater diameter stenosis) meet medical necessity for intervention (per recent DOJ settlements). 2. Prophylactic venoplasty is not considered medically necessary and should not be coded. Terms such as mild, moderate, and severe should be avoided in favor of percent stenosis. EXMPLE(S): ) ccess to a left forearm loop PTFE graft is performed after sterile preparation (9). Wire, sheath, and catheter are inserted and contrast is injected, visualizing the V graft and the venous outflow (bundled). nother injection to reflux the arterial anastomosis (using occlusion balloon technique) is also performed (no additional codes). The graft, cephalic vein, subclavian vein, innominate vein, and superior vena cava are all visualized (no additional codes). Imaging reveals a stenosis at the venous anastomosis and in the subclavian vein. 2) ccess to left brachial artery with a 22 gauge ngiocath is performed (). Contrast injection for V brachialbasilic fistula study shows the arterial inflow, arterial anastomosis, and venous outflow to the right atrium [9-2 (or -7 for hospital billing)] (including the subclavian vein, innominate vein, and superior vena cava). o stenosis is seen. ote: If angioplasty of the dialysis circuit is performed via the native brachial artery access, change the circuit study with intervention to code 92-2 (or -7) and change the catheter placement to code 2. ) The brachial artery of an upper arm V fistula is accessed with a French sheath (), and V fistulogram is performed, showing a patent fistula and central venous outflow [9-2 (or -7 for hospital billing)]. 9% stenosis of the cephalic vein is seen. separate puncture of the fistula is performed (delete modifier-2-7 from code 9) along with 7 mm balloon venoplasty (add 92, delete 9), which gives excellent results. Injection via the native brachial artery access shows a widely patent arterial anastomosis with good arterial inflow, but there is slow flow distally into the hand. Complete evaluation of the arterial vessels distal to the anastomosis, including the palmar arch and digital vessels, shows a filling defect consistent with an embolus in the distal radial artery (77). There is poor flow into the digital arteries of the hand. catheter is advanced from the brachial artery approach into the radial artery (add 2, delete ), and suction thrombectomy is done (7). Follow-up angiography shows good flow into the hand (no code). ) Puncture of the V graft with dialysis circuit imaging shows slow flow but patency of the system from the peri-anastomotic arterial segment through the venous system to the right atrium (9). catheter is advanced into the native arterial system, beyond the peri-anastomotic segment centrally to the subclavian artery, with
208 imaging showing a 9% subclavian artery stenosis (2, 77-9). ngioplasty with a 7 mm balloon (72) shows significant recoil. For this reason, a stent is placed (add 72, delete 72) with improved flow noted. Diagnostic ngiography Coding Diagnostic Dialysis Circuit Imaging Pages: 79- Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: Dialysis circuits are created as vascular access sites required for hemodialysis. Dialysis circuits may be constructed in a variety of ways and at various locations. Most commonly these are located in the arm or forearm, and are V fistulae (direct artery to vein anastomosis) or V grafts (prosthetic material in a loop or straight configuration anastomosed to an artery proximally and a vein distally). Medicare has encouraged a shift from grafts to fistulae, as there is less infection and stenosis with the native vessel surgery. V fistulae may require weeks or months to mature for use in dialysis, thus requiring non-tunneled or tunneled central venous catheter placement for immediate temporary dialysis. Dialysis circuits may be placed in the upper arm, forearm, thigh, or chest. Shuntograms (angiograms of the shunt or fistula) allow for the diagnosis of stenoses and planning for interventions. CLIICL IDICTIOS: Thrombosis or poor flow with inadequate dialysis. The most common etiology of these problems are venous anastomotic strictures, but can also be caused by outflow vein or central vein stenosis, intra-shunt stenosis, or inflow arterial stenosis. Other problems may relate to difficulty obtaining access of the graft, failure of the V fistula to mature, peripheral extremity ischemia, pseudoaneurysm, infection, and occlusion. Occasionally collateral, competing vessels in V fistulae require embolization or surgical ligation to allow the primary venous outflow to mature and enlarge enough to support dialysis.
209 CODES: PROCEDURE DESCRIPTIO Introduction of needle(s) andor catheter(s), dialysis circuit, with diagnostic angiography of the dialysis circuit, including all direct puncture(s) and catheter placement(s), injection(s) of contrast, all necessary imaging from the arterial anastomosis and adjacent artery through entire venous outflow including the inferior or superior vena cava, fluoroscopic guidance, radiological supervision and interpretation and image documentation and report; Diagnostic angiography of the dialysis circuit performed via remote or existing access Introduction of needle or intracatheter, upper or lower extremity artery Selective catheter placement, arterial system; each first order thoracic or brachiocephalic branch, within a vascular family Selective catheter placement, arterial system; each first order abdominal, pelvic, or lower extremity artery branch, within a vascular family Selective catheter placement, venous system; first order branch (eg, renal vein, jugular vein) PRO C COD E (or -7) 2 2 P C T O T L R V U S & I C O D E P C T O T L R V U CODIG ISTRUCTIOS: 2. Code 9 is a complete code describing the initial access to an V fistula or graft (dialysis circuit) and includes the injection of contrast and all necessary imaging to complete the evaluation of the dialysis circuit. This
210 includes imaging of the entire dialysis circuit, including the adjacent inflow artery (peri-anastomotic region), arterial anastomosis, shunt, and venous outflow up to and including the complete superior or inferior vena cava. 2. Code 9 includes advancement of the catheter across the arterial inflow vessel for arterial inflow evaluation. It does not include advancement of the catheter centrally in the upper extremity arterial vessels (additionally report codes 2 and 77) for evaluation of central arterial inflow. 2. When diagnostic angiography of the dialysis circuit is performed via a remote or existing access, report code 9-2 (or -7 for hospital billing). lso report selective catheter placement codes as appropriate when imaging is performed from a remote access. 27. Code 9-2 (or -7 for hospital billing) includes evaluation of the entire V shunt, extremity outflow veins, and central veins all the way to the right atrium performed via a pre-existing catheter in the fistulagraft or via a remote catheter. Central veins include the subclavian, brachiocephalic veins, and superior vena cava for arm shunts and the iliofemoral veins and inferior vena cava for leg shunts. Repeat injections with graft occlusive pressure (or use of occlusion balloon) to reflux contrast and visualize the arterial anastomosis and adjacent peri-anastomotic arterial inflow segment are also included. This combination of vessels is called the "dialysis circuit". 2. Report conventional catheterization codes (2, 2, 27) if percutaneous arterial access is established remotely from the shunt (e.g., transfemoral arterial catheter placement for subsequent diagnostic study or intervention), along with code 9-2 (or -7 for hospital billing). 29. Use code for direct brachial artery puncture done to evaluate a radiocephalic (V) fistula. Code 9-2 (or -7 for hospital billing) is used for the S&I. 2. ll access sites into the dialysis circuit for diagnostic shuntogram andor intervention are bundled with codes Code 9 includes the advancement of the catheter centrally into the SVC, IVC, or right atrium. It does not include selective vein branch procedures (e.g., for branch embolization use add-on code 99, which includes all selective venous catheter placements, embolization, S&I, and follow-up imaging). 22. dditionally report code 2 if, after shunt access and evaluation (9), selective catheterization of the upper extremity artery more centrally is necessary to evaluate proximal arterial inflow stenoses substantially away from the peri-anastomotic region (e.g., axillary or subclavian artery). Code 2 includes advancement of the catheter centrally into the aorta or distally into the wrist or hand. Imaging code 77-9 may also be reported for extremity angiography when done. 2. If venous collaterals or branches are selected and embolized, report add-on code 99, which includes all selective venous catheter placements related to the embolization. 2. Report conventional catheterization code 2 if percutaneous venous access is established remotely from the shunt (e.g., transfemoral venous access with placement of a catheter for subsequent diagnostic study or
211 intervention of an upper extremity shunt), along with code 9-2 (or -7 for hospital billing). 2. Code 9 includes all additional separate accesses to an V fistula or graft (dialysis circuit) for the purpose of further imaging. If a therapeutic intervention (venoplasty, stent placement, thrombectomy, etc.) is performed, use the appropriate code from code range These codes include all catheter placements via the dialysis circuit access. 2. Only one code from code range 9-9 is submitted per session. These codes are built on a progressive hierarchy with the highest level intervention being billed. 27. There are no additional imaging codes to be added for angiography during or after completion of the shunt intervention (e.g., angioplasty, stent placement, thrombectomy). Dialysis circuit evaluation is included with codes 92-9, if done. If a diagnostic study is not performed, you can still submit codes 92-9 without a modifier. 2. Do not report code 9 more than once for access and evaluation of an V graft or shunt. ccess into the shunt may be single or multiple, but this code may only be used once to describe access and imaging for a diagnostic study. Code 9 and any additional direct access sites into an V graft or shunt for intervention are bundled with the intervention (92-9). 29. Do not report code 72, 727, or 72 when unilateral extremity venography of the same extremity or cavography is described during shuntogram. Codes 727 and 72 are considered bundled with arm shunt evaluation code 9. If venography of a different extremity is performed, add code 72 with an appropriate modifier. 27. Do not report code 77 for routine imaging of the immediate arterial inflow (peri-anastomotic segment) of an V fistula or shunt. This is clearly described as being included in code 9. This code includes "all necessary imaging from the arterial anastomosis and adjacent artery through the entire venous outflow". 27. Report code 77 if further imaging of the upper (or lower) extremity arterial system is medically necessary (e.g., onset of ischemic changes in the hand, distal to the arterial anastomosis; suspected arterial stenosis central to the peri-anastomotic arterial segment). (Catheter placement code 2 is additionally reported here, and code 9 is unchanged.) 272. If upper extremity angiography (77) is performed for separate medical necessity unrelated to the shunt and incidental imaging of a shunt is noted, these findings would be considered part of the normal venous outflow and code 9-2 (or -7 for hospital billing) would not be reported. If the shunt evaluation is necessary and fully evaluated via this remote access, the catheter placement code and 9-2 (or -7 for hospital billing) would be reported. 27. If imaging is via remote access [catheter placement in brachial artery via femoral approach- 27, 9-2 (or -7 for hospital billing)], and then a separate access to the graft is performed for intervention (venoplasty), delete code 9-2
212 (or -7 for hospital billing) and add the appropriate code(s) for the intervention (92-99). 27. If a graft study via direct access is performed (9), followed by selection of two branch veins for embolization, the embolization procedure, and follow-up angiography, report add-on code 99 with Ultrasound guidance for vascular access (797) may be additionally coded if necessary to obtain safe access into the V graftfistula (new or poorly developed fistulae, pseudoaneurysms, slow flow, or failing grafts), as long as necessary documentation (per CPT Codebook) is in the physician's dictated report. 27. Do not code for "routine surveillance" shuntograms. These do not meet medical necessity. Findings or symptoms of shunt failure should be documented prior to performing an invasive procedure Stenoses must be accurately measured and documented with percent stenosis. Only hemodynamically significant stenoses (e.g., % or greater diameter stenosis) meet medical necessity for intervention (per recent DOJ settlements). 27. Prophylactic venoplasty is not considered medically necessary and should not be coded. Terms such as mild, moderate, and severe should be avoided in favor of percent stenosis. EXMPLE(S): ) ccess to a left forearm loop PTFE graft is performed after sterile preparation (9). Wire, sheath, and catheter are inserted and contrast is injected, visualizing the V graft and the venous outflow (bundled). nother injection to reflux the arterial anastomosis (using occlusion balloon technique) is also performed (no additional codes). The graft, cephalic vein, subclavian vein, innominate vein, and superior vena cava are all visualized (no additional codes). Imaging reveals a stenosis at the venous anastomosis and in the subclavian vein. 2) ccess to left brachial artery with a 22 gauge ngiocath is performed (). Contrast injection for V brachialbasilic fistula study shows the arterial inflow, arterial anastomosis, and venous outflow to the right atrium [9-2 (or -7 for hospital billing)] (including the subclavian vein, innominate vein, and superior vena cava). o stenosis is seen. ote: If angioplasty of the dialysis circuit is performed via the native brachial artery access, change the circuit study with intervention to code 92-2 (or -7) and change the catheter placement to code 2. ) The brachial artery of an upper arm V fistula is accessed with a French sheath (), and V fistulogram is performed, showing a patent fistula and central venous outflow [9-2 (or -7 for hospital billing)]. 9% stenosis of the cephalic vein is seen. separate puncture of the fistula is performed (delete modifier-2-7 from code 9) along with 7 mm balloon venoplasty (add 92, delete 9), which gives excellent results. Injection via the native brachial artery access shows a widely patent arterial anastomosis with good arterial inflow, but there is slow flow distally into the hand. Complete evaluation of the arterial vessels distal to the anastomosis, including the palmar arch and digital vessels, shows a filling defect consistent with an embolus in the distal radial artery (77). There is poor flow into
213 the digital arteries of the hand. catheter is advanced from the brachial artery approach into the radial artery (add 2, delete ), and suction thrombectomy is done (7). Follow-up angiography shows good flow into the hand (no code). ) Puncture of the V graft with dialysis circuit imaging shows slow flow but patency of the system from the peri-anastomotic arterial segment through the venous system to the right atrium (9). catheter is advanced into the native arterial system, beyond the peri-anastomotic segment centrally to the subclavian artery, with imaging showing a 9% subclavian artery stenosis (2, 77-9). ngioplasty with a 7 mm balloon (72) shows significant recoil. For this reason, a stent is placed (add 72, delete 72) with improved flow noted.
 References")
214 Diagnostic ngiography Coding Venography Central Venous Coding - Vena Cava Pages: - Procedure Clinical Indications Codes Coding Instructions Example(s) References
215 PROCEDURE: Vena cava angiography can be performed from a peripheral injection at the time of extremity venography () or by placing the catheter centrally into the vena cava (). CLIICL IDICTIOS: Upper and lower extremity swelling, superior vena cava syndrome, non-functioning central venous catheter, congenital anomalies, and intravascular tumor. CODES: PROCEDURE DESCRIPTIO Introduction of catheter, superior or inferior vena cava (inferior vena cavagram) Introduction of catheter, superior or inferior vena cava (superior vena cavagram) Unlisted injection code for imaging of venous structure other than extremity when catheter is not placed in the cava (not via central venous catheter), non-selective Fluoroscopic imaging for catheter check without documentation of complete venography (includes fluoroscopy and contrast injection) PR O C C O D E P C 9 T O T L R V U.... S & I C O D E P C T O T L R V U. 9. CODIG ISTRUCTIOS: 279. Imaging of the vena cava (72) is not a component of selective renal venous imaging (7), so it can be separately coded. This differs from the arterial coding rules, which bundle aortography (72) into selective renal angiography (2-2). 2. Code for a separate diagnostic cavagram when performed with pulmonary angiography (unless an IVC filter is placed at the same session). 2. Do not code for an inferior vena cavagram (72) when performed with vena cava filter placement (79), repositioning (792), or retrieval (79), as imaging guidance and all radiological supervision and
216 interpretation are included with these procedures. Catheter placements (e.g.,, ) and ultrasound guidance (722, 72, 797) are also bundled with codes Do not code a cavagram if performed to measure the caval size, locate the renal veins, or evaluate for variant anatomy or thrombus in the cava at the time of cava filter procedures. These evaluations are considered guiding shots and are not separately coded. The cavagram (SVC or IVC) is bundled with cava filter interventions. 2. Do not include separate S&I codes for cavagram when imaged as part of a dialysis fistulogram. The cavagram (72 or 727) is considered part of the central venous evaluation and is included in code Do not include a separate S&I code for cavagram when imaged as part of a venous sampling study. The cavagram, as well a selective venography of the sampled organ, is included in code If the findings only describe a fibrin sheath or patency of the catheter with flow into or through the cava, do not use code 72 (inferior vena cavagram) or 727 (superior vena cavagram) for imaging at the time of lower or upper extremity dialysis catheter check respectively. The cavagram must be a full and complete diagnostic study to use code 72 or 727. Use code 9 to describe this limited imaging. If mechanical removal of obstructive material from the catheter is subsequently done (9 or 9), do not report code 9 either, as it is bundled with codes 979 and Consider code 299 for the non-selective injection code for imaging of a venous structure, other than an extremity, when the catheter is not placed in the vena cava (e.g., catheter placement in the jugular vein via jugular vein access). Use code 9 if injection is done through a central venous access device or catheter to evaluate the device and venous outflow. If a full and complete superior vena cava study is indicated, performed, and documented, use code 727 instead of 9. EXMPLE(S): ) Patient with shortness of breath and suspected pulmonary embolus undergoes selective bilateral pulmonary angiography (-, 77). Because of clot in the left lower lobe, the catheter is placed in the IVC, and inferior vena cavagram is performed (bundled with filter placement). This shows the vena cava to be patent (no clot) and of normal size, so a temporary vena cava filter is placed (79). 2) Patient with neck, head, and arm swelling. Bilateral catheter placements in the basillic veins with injection of contrast simultaneously for imaging of both upper extremity venous systems and the superior vena cava. This shows severe stenosis of the SVC due to compression by a lung mass. rm veins are patent with collaterals noted in the mediastinum (-, 722, 727). ) Chest port is accessed using sterile technique and a Huber needle. Contrast injection shows the tip of the catheter in the right atrium without obstruction (9). ) Chest port is accessed with a Huber needle. Contrast injection shows a patent catheter. Further complete imaging of the SVC is performed due to bilateral arm
217 swelling. There is 9% stenosis and adherent clot in the SVC (727-9). Overnight infusion of thrombolytic agent (722) is started. Continued thrombolytic infusion into the morning with follow-up angiography (72) shows clearing of clot, but residual stenosis of %. The port is removed (9). From a femoral vein approach, a catheter is placed into the SVC (), and venoplasty with a mm balloon is performed (72) for seconds. Follow-up shows recoil with % residual. For this reason, a 2 mm self-expanding stent is successfully deployed (add 72, delete 72).
218 Diagnostic ngiography Coding Venography Extremity Venous Coding Pages: 9-9 Procedure Clinical Indications References Codes Coding Instructions
219 PROCEDURE: Extremity venography is a rather simple exam, which includes injecting a peripheral vein(s) and imaging of the unilateral or bilateral venous structures of the upper or lower extremities. Venography can also be done selectively with catheters from a femoral or brachial approach. Popliteal approach is often used when lower extremity DVT thrombectomy and thrombolysis is anticipated. CLIICL IDICTIOS: Extremity swelling, deep vein thrombosis (DVT), venous insufficiency, venous reflux, or venous malformation evaluation, as in Klippel Trenaunay syndrome. CODES: PROCEDURE DESCRIPTIO PROC TOT
220 Injection procedure for extremity venography (including introduction of needle or intracatheter) (non-selective unilateral) Injection procedure for extremity venography (including introduction of needle or intracatheter) (non-selective bilateral) Selective catheter placement, venous system; first order branch (eg, renal vein, jugular vein) Selective catheter placement, venous system; second order, or more selective, branch (eg, left adrenal vein, petrosal sinus) S&I Codes Venography, extremity, unilateral, radiological supervision and interpretation (upper or lower) Venography, extremity, bilateral, radiological supervision and interpretation (upper or lower) CODE, P C 2 L RV U CODIG ISTRUCTIOS: 27. Code is specific for injection of contrast to image extremity veins. 2. Do not code extremity venography (72) when imaging the venous outflow during a dialysis shuntogram. It is included in the ipsilateral shuntogram code (9). 29. Do not code extremity venography (72) or catheter placement () with lower extremity venous insufficiency therapies (e.g., procedures described by codes -). 29. Extremity venography to evaluate for patency prior to pacemakerdefibrillator placement is not coded. It is considered a guidance procedure for lead placement. If the pacemaker procedure is cancelled, or the lead access has to be changed to a different site due to unexpected central venous occlusion, consider codes This is an infrequent occurrence. 29. Do not code a unilateral venogram (72) twice, as a bilateral code exists (722). n exception would be made if both unilateral upper and unilateral lower extremity venography is performed Do not use a - modifier with code 72, as a bilateral code exists (722). 29. Use code 72 for imaging of unilateral pelvic veins and code 722 for imaging of bilateral pelvic veins. This would include imaging of the legs if performed. The entire upper or lower extremity venous system does not
221 have to be imaged to use 72 or 722. Use code 72 if only the iliofemoral or subclavianbrachiocephalic central veins are imaged. Do not use a -2 modifier.
222 Diagnostic ngiography Coding Venography Visceral Venous Coding Pages: 92-9 Procedure Clinical Indications Codes Coding Instructions Example(s) Grey Zone Discussion References PROCEDURE: Visceral venous coding requires selective catheter placement into a vein supplying a visceral organ from a peripheral access (brachial, jugular, or femoral). CLIICL IDICTIOS: Diagnostic work-up for portal hypertension, neoplasm, or infertility. CODES: PROCEDURE DESCRIPTIO PROC CODE Unilateral selective renal venography Bilateral selective renal venography dditional selective renal venography after the basic procedure - 2 Left testicular venography (without renal) 2 Right testicular venography (without renal) Bilateral testicular venography (without renal) -9 2 P C TOT L RVU S&I COD E P C 2 TOT L RVU Left ovarian (with or without renal) venography
223 Right ovarian venography Bilateral ovarian venography Unilateral selective adrenal venography: Right Left Bilateral selective adrenal venography Hepatic venography with hemodynamics Hepatic venography without hemodynamics or 2 or 2 Unilateral selective venous sampling Pulmonary venography during congenital heart catheterization.
224 9 dd-on Code CODIG ISTRUCTIOS: 29. If the procedure is done for venous sampling, the selective catheter placement is included in code and the imaging S&I code is included in code 79. Do not bill diagnostic venography separately. Do not bill selective catheter placements separately. 29. For hospitals, code 79 is paid if no other payable interventional codes are on the facility bill. If venography is inappropriately billed, the lower paying venogram will be paid instead of code Use codes and 79 once per organ sampled, not per vessel sampled. Multiple renal veins (upper, mid, lower) may be sampled at the same setting. Do not code catheter placement(s) during selective organ sampling procedures, as imaging and catheter placement are bundled If the pituitary gland is sampled from a bilateral approach (also called petrosal vein sampling), use codes and 79 twice. 29. Selective codes and 2 require placement of the catheter into a first and second order vessel respectively n inferior vena cavagram can be coded separately when performed in conjunction with a renal venogram. This is contrary to coding rules in the arterial system, where abdominal aortography is included in selective renal angiography.. Use code 7 for unilateral left renalgonadal venography when performed to evaluate for reflux into the gonadal vein or to identify collaterals that contribute to ovarian vein congestion syndrome or varicocele. This includes selective gonadal venography. Bilateral selective iliac (pelvic) venography (or imaging of pelvic veins by bilateral gonadal vein injections) is reported with code specific code does not exist for selective right gonadal venography. This vessel usually arises directly off the cava and is a first order selective vessel (). There is no corresponding S&I code. Consider code 79 (or 7 if the right gonadal arises as a variant off the right renal vein). 2. Bilateral testicular vein embolization (for varicoceles) is coded as two separate embolizations (72, 72-9). These are considered two surgical fields and require two surgical approaches. This procedure is usually performed unilaterally on the left.. Ovarian vein embolization procedures for pelvic venous congestion syndrome are based on whether the central ovarian veins are embolized (unilateral or bilateral) andor the pelvic region veins (internal iliacs) are embolized as a second surgical site (unilateral or bilateral). If both central and pelvic veins are embolized, use codes 72 and If only bilateral pelvic veins are embolized, use code 72 once.
225 . Do not code for coronary sinus venography.. Diagnostic pulmonary venography during congenital heart catheterization is reported as pulmonary angiography with add-on code 9. Do not use code 9 for localization of pulmonary vein ostia during pulmonary vein isolation study (atrial fibrillation ablation described by codes 9 and 97).. Do not use code 777 for additional selective venous exams beyond the basic venography. Consider use of code 79 for these additional selective images. Discuss with your payer. 7. If hepatic "wedge" venography is performed with a diagnostic imaging catheter, the catheter placement is "wedged" in a peripheral hepatic vein branch. This is at least a second order selective vein (2). If occlusion balloon technique is used, the selectivity may be first or second order or higher. Be sure to discuss accurate catheter position documentation with your physician, otherwise default to first order () when using an occlusion balloon.. Evaluation of a Rex shunt (SMV graft to left portal vein in patient with central portal vein occlusion) may require selection of the left, middle, and right hepatic veins with hepatic venography and wedged portal vein imaging. Report the three catheter placements (e.g., 2 x ) and wedged hepatic venography with pressures (79 x ). EXMPLE(S): ) Male patient with infertility presents for varicocele evaluation. Via a transjugular route, a catheter is placed into the left renal vein with imaging showing an enlarged gonadal vein with reflux. The catheter is advanced down the enlarged left gonadal vein (2, 7). Varicocele is identified and collaterals noted. Embolization with boiling contrast and coils is performed (72). Follow-up venogram (bundled) shows no residual abnormality. (If bilateral varicoceles are treated, add codes -9 and 72-9 for the right side.) GREY ZOE DISCUSSIO: Consider use of code 79 for additional selective angiography of the right gonadal vein. Discuss with your payer.

226 Diagnostic ngiography Coding Venography Head and eck Venous Coding Pages: 9-9 Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: Cerebral venous imaging requires complex catheterization and imaging, usually from a femoral access. Jugular imaging can be selective or by direct puncture. CLIICL IDICTIOS:
227 Evaluations of cavernous carotid (CC) fistula, intracranial or jugular venous thrombosis, central venous access, as part of a petrosal vein sampling study or a venous malformation embolization procedure. ll head and neck venous structures are second order or greater selectivity (2) from a transfemoral approach. CODES: PROCEDURE DESCRIPTIO Jugular venography (unilateral) PROC CODE on-selective, jugular vein (direct puncture) 299 Selective catheterization, jugular vein, via femoral vein Superior sagittal sinus (transverse sinus) venography Epidural venography Orbital venography 2 2 dditional vessel, selective, after basic exam 2 P C TOTL RVU.... S&I CODE P C 2 TOTL RVU CODIG ISTRUCTIOS: 9. Consider code 299 to report the injection procedure for direct puncture and code 7 for imaging of the jugular vein. If the catheter is advanced centrally into the SVC, change code 299 to. If SVC imaging is done, add code 727. If a central venous access catheter is then placed, delete
 is rarely performed as a separate diagnostic study.")
228 codes, 7, and 727, as catheter placements and imaging along the route and via the same access as the eventual CVC are bundled.. Epidural venography (772) is rarely performed as a separate diagnostic study. Code 772 is not coded when performed as a "guidance" or "confirmation of needle tip location" procedure during pain management procedures. Code 772 is bundled with vertebroplasty and kyphoplasty procedures and should not be billed separately with codes Consider code 79 for additional selective venous imaging. Discuss with payer. EXMPLE(S): ) -year-old with superior sagittal sinus thrombosis presents for venography. Via a transfemoral route, a microcatheter is advanced to the right transverse sinus (2). Contrast is injected and images obtained of the transverse sinus (77-9) and jugular vein (7-9). This shows stenosis of the sigmoid sinus on the right. Reflux of contrast into thrombus in the superior sagittal sinus is noted. Mechanical venous thrombectomy is performed (77), which opens a channel; however, this clots off quickly. Infusion microcatheter is then advanced and three-hour tp thrombolysis infusion is performed in this vessel (722). Follow-up angiography (bundled) shows clearing of clot with 7% stenosis of the sigmoid sinus. Balloon venoplasty to mm is performed (72) with 2% residual. The patient is heparinized after catheter removal.
229 Diagnostic ngiography Coding Pulmonary ngiography Pages: Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: The pulmonary arterial system is one of four separate and distinct vascular systems and the only system with arteries that carry "venous" blood. There are specific codes for selective catheter placement in these vessels. The pulmonary arteries bring un-oxygenated blood from the venous system to the lungs, where it returns oxygenated via the pulmonary veins to the left atrium. To access these vessels, the physician must access the peripheral venous system first, then pass a catheter through the heart into the pulmonary artery. The S&I codes consist of unilateral and bilateral selective or non-selective imaging. If the physician does a basic exam, followed by selective or superselective imaging of other pulmonary arterial branches, report the basic exam code and additional selective imaging code 777, along with selective catheter placement code. lways code to the highest degree of selectivity. CLIICL IDICTIOS: To evaluate for pulmonary embolism, pulmonary hypertension, or vascular malformations (such as VMs or V fistulae related to Osler-Weber-Rendu syndrome). These patients may present with paradoxical stroke. Interventions may include thrombectomy and thrombolysis of clot or pulmonary arterial embolization of fistulae and VMs. Stenoses may require angioplasty or stent placement. Foreign body retrievals of central venous catheter fragments are also performed in these vessels. CODES: PROCEDURE DESCRIPTIO PR O C C O D E P C T O T L R V U S & I C O D E P C T O T L R V U
230 Selective catheter placement, left or right pulmonary artery (unilateral) Selective catheter placement, left or right pulmonary artery (bilateral) Introduction of catheter, right heart or main pulmonary artery (non-selective) dditional selective imaging after basic pulmonary angiogram is completed Injection procedure during cardiac catheterization including imaging supervision, interpretation, and report; for pulmonary angiography (List separately in addition to code for primary procedure) 9. CODIG ISTRUCTIOS: 2. If clinically indicated, imaging of the inferior vena cava (72) prior to or after a pulmonary angiogram may be reported, as well as the catheter placement code (). Do not use code 72 or if IVC filter placement is anticipated and placed (use code 79).. Do not code for catheter placement in the cava () when the cava is merely traversed to gain access to the pulmonary arteries.. Code is to be used for non-selective pulmonary angiography by injection at the level of the right atrium, right ventricle, or main pulmonary artery.. If the exam consists of selective catheter placement and imaging in both of the upper and lower pulmonary arteries without first performing a
231 pulmonary angiogram, do not use code 777. bilateral complete pulmonary angiogram (77) was performed one quarter at a time.. Use code777 if additional selective or superselective imaging and catheter placement is performed after the basic exam (bilateral pulmonary angiogram) has been completed. This is common with multiple pulmonary V fistulae evaluation and embolization. 7. Do not use radiology codes when pulmonary angiogram is performed during a cardiac catheterization. Use the appropriate cardiac code (9). Code 9 includes the catheter placement(s) and all imaging of one or more pulmonary arteries. This includes pediatric cardiac intervention performed on multiple pulmonary arteries if performed at the time of a pediatric cardiac catheterization. EXMPLE(S): ) Patient with shortness of breath presents for evaluation for pulmonary embolism. Via a transfemoral venous access, a catheter is placed in the left and right pulmonary arteries with injection of contrast and imaging (77). catheter is advanced into both lower lobe pulmonary arteries with additional imaging (-, 777 x 2). Clot is seen, so the catheter is retracted into the inferior vena cava, and imaging of the inferior vena cava is done (cavagram and catheter placement in the IVC are not billed, as these components are bundled with IVC filter placement). There is no thrombus in the cava. vena cava filter is placed without difficulty (79). ote: The catheter placements in both central pulmonary arteries (-) are bundled into the more selective bilateral lower lobe pulmonary artery catheter placements (-).

232 Diagnostic ngiography Coding The Portal System Pages: 2-2 Procedure Clinical Indications Codes Coding Instructions Example(s) References PROCEDURE: The portal system is similar to the pulmonary system, as it is a completely separate vascular system with its own selective catheterization codes. This system is the site for venous return of the abdominal viscera (specifically the spleen, pancreas, stomach, small and large bowel). ll the blood from these organs returns to the liver via the portal system where it is "processed" in the liver and returned to the systemic venous system via the hepatic veins. The evaluation of this system has become increasingly important with the advent of interventional techniques to help treat diseases affecting the liver and these venous structures (TIPS procedure).
2018 Cerebrovascular Reimbursement Coding Fact Sheet
 The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft
 MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
Diagnostic and interventional venous procedures (lower extremity)
") 2017 Coding and Medicare payment guide Diagnostic and interventional venous procedures (lower extremity) All coding, coverage, billing and payment information provided herein by Philips Volcano is gathered
2017 Coding and Medicare payment guide Diagnostic and interventional venous procedures (lower extremity) All coding, coverage, billing and payment information provided herein by Philips Volcano is gathered
Coronary intravascular ultrasound (IVUS)
") 2017 Coding and Medicare payment guide Coronary intravascular ultrasound (IVUS) All coding, coverage, billing and payment information provided herein by Philips Volcano is gathered from third-party sources
2017 Coding and Medicare payment guide Coronary intravascular ultrasound (IVUS) All coding, coverage, billing and payment information provided herein by Philips Volcano is gathered from third-party sources
Lumify. Lumify reimbursement guide {D DOCX / 1
 Lumify Lumify reimbursement guide {D0672917.DOCX / 1 {D0672917.DOCX / 1 } Contents Overview 4 How claims are paid 4 Documentation requirements 5 Billing codes for ultrasound: Non-hospital setting 6 Billing
Lumify Lumify reimbursement guide {D0672917.DOCX / 1 {D0672917.DOCX / 1 } Contents Overview 4 How claims are paid 4 Documentation requirements 5 Billing codes for ultrasound: Non-hospital setting 6 Billing
Diagnostic and interventional venous procedures (lower extremity)
") Coding and Medicare national payment guide 2018 Diagnostic and interventional venous procedures (lower extremity) All coding, coverage, billing and payment information provided herein by Philips is gathered
Coding and Medicare national payment guide 2018 Diagnostic and interventional venous procedures (lower extremity) All coding, coverage, billing and payment information provided herein by Philips is gathered
2018 Endovascular Reimbursement Coding Fact Sheet
 The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
Reimbursement Information for Diagnostic Ultrasound and Ultrasound-guided Vascular Procedures 1
 GE Healthcare Reimbursement Information for Diagnostic Ultrasound and Ultrasound-guided Vascular Procedures 1 January, 2013 www.gehealthcare.com/reimbursement This overview addresses coding, coverage,
GE Healthcare Reimbursement Information for Diagnostic Ultrasound and Ultrasound-guided Vascular Procedures 1 January, 2013 www.gehealthcare.com/reimbursement This overview addresses coding, coverage,
Diagnostic and interventional arterial procedures (lower extremity)
") 2017 Coding and Medicare payment guide Diagnostic and interventional arterial procedures (lower extremity) Page 2 All coding, coverage, billing and payment information provided herein by Philips Volcano
2017 Coding and Medicare payment guide Diagnostic and interventional arterial procedures (lower extremity) Page 2 All coding, coverage, billing and payment information provided herein by Philips Volcano
Sample page. For the Physical Therapist An essential coding, billing and reimbursement resource for the physical therapist CODING & PAYMENT GUIDE
 CODING & PAYMENT GUIDE 2019 For the Physical Therapist An essential coding, billing and reimbursement resource for the physical therapist Power up your coding optum360coding.com Contents Getting Started
CODING & PAYMENT GUIDE 2019 For the Physical Therapist An essential coding, billing and reimbursement resource for the physical therapist Power up your coding optum360coding.com Contents Getting Started
Fractional Flow Reserve (FFR) and instant wave-free Ratio (The ifr modality)
 and instant wave-free Ratio (The ifr modality)") 2017 Coding and Medicare payment guide Fractional Flow Reserve (FFR) and instant wave-free Ratio (The ifr modality) All coding, coverage, billing and payment information provided herein by Philips Volcano
2017 Coding and Medicare payment guide Fractional Flow Reserve (FFR) and instant wave-free Ratio (The ifr modality) All coding, coverage, billing and payment information provided herein by Philips Volcano
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Vascular Plug Procedures 2014 CODING AND PAYMENT REFERENCE GUIDE ST. JUDE MEDICAL - CARDIOVASCULAR DIVISION
 Vascular Plug Procedures 2014 CODING AND PAYMENT REFERENCE GUIDE ST. JUDE MEDICAL - CARDIOVASCULAR DIVISION IMPORTANT: St. Jude Medical provides this reference guide for general information purposes only
Vascular Plug Procedures 2014 CODING AND PAYMENT REFERENCE GUIDE ST. JUDE MEDICAL - CARDIOVASCULAR DIVISION IMPORTANT: St. Jude Medical provides this reference guide for general information purposes only
Physician s Compliance Guide
 Physician s Compliance Guide Updates to this guide will be posted on the Optum website and can be found at: http://www.optumcoding.com/product/updates/2013pcg/pcg13 Please use the following password to
Physician s Compliance Guide Updates to this guide will be posted on the Optum website and can be found at: http://www.optumcoding.com/product/updates/2013pcg/pcg13 Please use the following password to
2015 Facility and Physician Billing Guide Heart Valve Technologies
 2015 Facility and Physician Billing Guide Heart Valve Technologies PHYSICIAN BILLING CODES Clinicians use Current Procedural Terminology (CPT 1 ) codes to bill for procedures and services. Each CPT code
2015 Facility and Physician Billing Guide Heart Valve Technologies PHYSICIAN BILLING CODES Clinicians use Current Procedural Terminology (CPT 1 ) codes to bill for procedures and services. Each CPT code
Assistant Surgeon Payments
 Assistant Surgeon Payments January 18, 2018 We are seeing payers ask for payment back when we use Modifier 80 for assistant surgeon. Is there a reason why they would take the payment back? We are seeing
Assistant Surgeon Payments January 18, 2018 We are seeing payers ask for payment back when we use Modifier 80 for assistant surgeon. Is there a reason why they would take the payment back? We are seeing
2013 Coding Changes. Diagnostic Radiology. Nuclear Medicine
 2013 Coding Changes The principal coding changes affecting Radiologists in 2013 occur in the Interventional Radiology Section of the AMA/CPT Manual. As in the past, we continue to see the Relative Update
2013 Coding Changes The principal coding changes affecting Radiologists in 2013 occur in the Interventional Radiology Section of the AMA/CPT Manual. As in the past, we continue to see the Relative Update
CPT Code Details
 CPT Code 93572 Details Code Descriptor Intravascular Doppler velocity and/or pressure derived coronary flow reserve measurement (coronary vessel or graft) during coronary angiography including pharmacologically
CPT Code 93572 Details Code Descriptor Intravascular Doppler velocity and/or pressure derived coronary flow reserve measurement (coronary vessel or graft) during coronary angiography including pharmacologically
Reimbursement Information for Diagnostic Musculoskeletal Ultrasound and Ultrasound-guided Procedures 1
 GE Healthcare Reimbursement Information for Diagnostic Musculoskeletal Ultrasound and Ultrasound-guided Procedures 1 January, 2013 www.gehealthcare.com/reimbursement This overview addresses coding, coverage,
GE Healthcare Reimbursement Information for Diagnostic Musculoskeletal Ultrasound and Ultrasound-guided Procedures 1 January, 2013 www.gehealthcare.com/reimbursement This overview addresses coding, coverage,
Detailed Summary of the Proposed Rule for the Hospital Outpatient Prospective Payment System
 Detailed Summary of the Proposed Rule for the Hospital Outpatient Prospective Payment System The Centers for Medicare and Medicaid Services (CMS) released its proposed rule for calendar year (CY) 2017
Detailed Summary of the Proposed Rule for the Hospital Outpatient Prospective Payment System The Centers for Medicare and Medicaid Services (CMS) released its proposed rule for calendar year (CY) 2017
2 016 HF10 THERAPY HOSPITAL OUTPATIENT DEPARTMENT AND AMBULATORY SURGERY CENTER REIMBURSEMENT REFERENCE GUIDE
 HF10 therapy, delivered by the Nevro Senza System, is a new high-frequency spinal cord stimulation technology designed to aid in the management of chronic intractable pain of the trunk/limbs, including
HF10 therapy, delivered by the Nevro Senza System, is a new high-frequency spinal cord stimulation technology designed to aid in the management of chronic intractable pain of the trunk/limbs, including
Reimbursement Information for Diagnostic Ultrasound and Ultrasound-guided Procedures 1 Performed by Emergency Medicine Physicians
 GE Healthcare Reimbursement Information for Diagnostic Ultrasound and Ultrasound-guided Procedures 1 Performed by Emergency Medicine Physicians January, 2013 www.gehealthcare.com/reimbursement This overview
GE Healthcare Reimbursement Information for Diagnostic Ultrasound and Ultrasound-guided Procedures 1 Performed by Emergency Medicine Physicians January, 2013 www.gehealthcare.com/reimbursement This overview
2011 CPT Code Update. Diagnostic Radiology. Computed Tomography (CT), Abdomen and Pelvis. Deletion of Xeroradiography and Subtraction Codes
, Abdomen and Pelvis. Deletion of Xeroradiography and Subtraction Codes") 2011 CPT Code Update [The Health Insurance Portability and Accountability Act [HIPAA] transaction and code set rules require the use of the medical code set that is valid at the time a service is provided.
2011 CPT Code Update [The Health Insurance Portability and Accountability Act [HIPAA] transaction and code set rules require the use of the medical code set that is valid at the time a service is provided.
Sample page. Contents
 CODING COMPANION 2018 Cardiology/ Cardiothoracic/ Vascular Surgery A illustrated guide to coding and reimbursement POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
CODING COMPANION 2018 Cardiology/ Cardiothoracic/ Vascular Surgery A illustrated guide to coding and reimbursement POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
H F 1 0 T H E R A P Y R E I M B U R S E M E N T R E F E R E N C E G U I D E
 HF10 therapy, delivered by the Nevro Senza System, is the high-frequency spinal cord stimulation technology designed to aid in the management of chronic intractable pain of the trunk/limbs without paresthesia.
HF10 therapy, delivered by the Nevro Senza System, is the high-frequency spinal cord stimulation technology designed to aid in the management of chronic intractable pain of the trunk/limbs without paresthesia.
Routine Venipuncture and/or Collection of Specimens
 Manual: Policy Title: Reimbursement Policy Routine Venipuncture and/or Collection of Specimens Section: Laboratory & Pathology Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM012 Last Updated:
Manual: Policy Title: Reimbursement Policy Routine Venipuncture and/or Collection of Specimens Section: Laboratory & Pathology Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM012 Last Updated:
CY2015 Hospital Outpatient: Endovascular Procedure APCs and Complexity Adjustments
 CY2015 Hospital Outpatient: Endovascular Procedure APCs Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) CMS finalized the implementation of 25 Comprehensive APC to further
CY2015 Hospital Outpatient: Endovascular Procedure APCs Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) CMS finalized the implementation of 25 Comprehensive APC to further
Question: Are you using the KX modifier correctly on PT/OT claims?
 KX Modifiers February 15, 2018 Are you using the KX modifier correctly on PT/OT claims? One Medicare carrier has concerns that the KX modifier if not being used appropriately. National Government Services
KX Modifiers February 15, 2018 Are you using the KX modifier correctly on PT/OT claims? One Medicare carrier has concerns that the KX modifier if not being used appropriately. National Government Services
REPORTING POSTOPERATIVE PAIN PROCEDURES IN CONJUNCTION WITH ANESTHESIA
 Committee of Origin: Economics (Approved by the ASA House of Delegates on October 17, 2007 and last updated on September 2, 2008) ASA has recently received reports of payers inappropriately bundling the
Committee of Origin: Economics (Approved by the ASA House of Delegates on October 17, 2007 and last updated on September 2, 2008) ASA has recently received reports of payers inappropriately bundling the
Ultrasound Reimbursement Information for Anesthesiology 1
 GE Healthcare Ultrasound Reimbursement Information for Anesthesiology 1 January, 2009 www.gehealthcare.com/reimbursement This overview addresses coding, coverage, and for ultrasound guidance with continuous
GE Healthcare Ultrasound Reimbursement Information for Anesthesiology 1 January, 2009 www.gehealthcare.com/reimbursement This overview addresses coding, coverage, and for ultrasound guidance with continuous
Defining Non-Compounded Sclerotherapy
 Defining Non-Compounded Sclerotherapy December 14, 2017 I m not sure I understand the new vein surgery codes in the 2018 CPT manual. Can you explain what non- compounded means? The new 2018 coded, 36465,
Defining Non-Compounded Sclerotherapy December 14, 2017 I m not sure I understand the new vein surgery codes in the 2018 CPT manual. Can you explain what non- compounded means? The new 2018 coded, 36465,
Anesthesia Reimbursement
 This drafted policy is open for a two-week public comment period. This box is not part of the drafted policy language itself, and is intended for use only during the comment period as a means to provide
This drafted policy is open for a two-week public comment period. This box is not part of the drafted policy language itself, and is intended for use only during the comment period as a means to provide
CPT Code Details
 CPT Code 93572 Details Code Descriptor Intravascular Doppler velocity and/or pressure derived flow reserve measurement ( vessel or graft) during angiography pharmacologically induced stress; each additional
CPT Code 93572 Details Code Descriptor Intravascular Doppler velocity and/or pressure derived flow reserve measurement ( vessel or graft) during angiography pharmacologically induced stress; each additional
2016 HF10 THERAPY REIMBURSEMENT REFERENCE GUIDE
 206 HF0 THERAPY REIMBURSEMENT REFERENCE GUIDE HF0 therapy, delivered by the Nevro Senza System, is a new high-frequency spinal cord stimulation technology designed to aid in the management of chronic intractable
206 HF0 THERAPY REIMBURSEMENT REFERENCE GUIDE HF0 therapy, delivered by the Nevro Senza System, is a new high-frequency spinal cord stimulation technology designed to aid in the management of chronic intractable
OIG Work Plan for Orthotics
 OIG Work Plan for Orthotics February 1, 2018 We recently heard that the government will be focusing audits on off the shelf orthotics. We have tried to find information but have not been successful. Are
OIG Work Plan for Orthotics February 1, 2018 We recently heard that the government will be focusing audits on off the shelf orthotics. We have tried to find information but have not been successful. Are
Coding Companion for Podiatry. A comprehensive illustrated guide to coding and reimbursement
 Coding Companion for Podiatry comprehensive illustrated guide to coding and reimbursement 2016 Contents Contents Foot and Toes 28043-28045 [28039, 28041] 28043 28039 28045 28041 Excision, tumor, soft tissue
Coding Companion for Podiatry comprehensive illustrated guide to coding and reimbursement 2016 Contents Contents Foot and Toes 28043-28045 [28039, 28041] 28043 28039 28045 28041 Excision, tumor, soft tissue
Moderate (Conscious) Sedation
 Sedation") Manual: Policy Title: Reimbursement Policy Moderate (Conscious) Sedation Section: Medicine Subsection: None Date of Origin: 12/16/2016 Policy Number: RPM048 Last Updated: 10/27/2017 Last Reviewed: 11/8/2017
Manual: Policy Title: Reimbursement Policy Moderate (Conscious) Sedation Section: Medicine Subsection: None Date of Origin: 12/16/2016 Policy Number: RPM048 Last Updated: 10/27/2017 Last Reviewed: 11/8/2017
2019 ABBOTT REIMBURSEMENT GUIDE CMS Physician Fee Schedule
 ABBOTT REIMBURSEMENT GUIDE CMS Physician Fee Schedule This document and the information contained herein is for general information purposes only and is not intended and does not constitute legal, reimbursement,
ABBOTT REIMBURSEMENT GUIDE CMS Physician Fee Schedule This document and the information contained herein is for general information purposes only and is not intended and does not constitute legal, reimbursement,
Final MPFS 2014 Summary SIR
 Final MPFS 2014 Summary SIR The CY 2014 PFS CF is $27.2006 (p531) Impact Tables (p1285) Refinement Panel Recommendations (p183) Table 23 presents information on the work RVUs for the codes considered by
Final MPFS 2014 Summary SIR The CY 2014 PFS CF is $27.2006 (p531) Impact Tables (p1285) Refinement Panel Recommendations (p183) Table 23 presents information on the work RVUs for the codes considered by
Final Rule CMS-1676-F was released on November 2, 2017 and finalized policies first proposed
 November 8, 2017 Subject: (CMS 1676 F) Summary of the Centers for Medicare and Medicaid Services Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2018
November 8, 2017 Subject: (CMS 1676 F) Summary of the Centers for Medicare and Medicaid Services Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2018
HF10 THERAPY 2018 Ambulatory Surgery Center Reimbursement and Coding Reference Guide
 HF10 therapy, delivered by the Nevro Senza System, is the high-frequency spinal cord stimulation technology operated at 10,000 Hz designed to aid in the management of chronic intractable pain of the trunk
HF10 therapy, delivered by the Nevro Senza System, is the high-frequency spinal cord stimulation technology operated at 10,000 Hz designed to aid in the management of chronic intractable pain of the trunk
How Many Sections Is The Cpt Manual Divided Into
 How Many Sections Is The Cpt Manual Divided Into Vocabulary words for This is a review students can take as many times as they would like. 6. The CPT manual is divided into how many sections? Medicine
How Many Sections Is The Cpt Manual Divided Into Vocabulary words for This is a review students can take as many times as they would like. 6. The CPT manual is divided into how many sections? Medicine
Claim Submission. Agenda 1/31/2013. Payment Basics
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 Payment Basics Agenda 2013 PT / OT / SP Codes Deleted Codes New Codes Significant
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 Payment Basics Agenda 2013 PT / OT / SP Codes Deleted Codes New Codes Significant
Nevro Reimbursement Support
 HF10 therapy, delivered by the Nevro Senza System, is the high-frequency spinal cord stimulation technology operated at 10,000 Hz designed to aid in the management of chronic intractable pain of the trunk
HF10 therapy, delivered by the Nevro Senza System, is the high-frequency spinal cord stimulation technology operated at 10,000 Hz designed to aid in the management of chronic intractable pain of the trunk
b. To facilitate the management decision of a patient with an equivocal stress test.
 National Imaging Associates, Inc. Clinical guidelines EBCT HEART CT & HEART CT CONGENITAL CCTA CPT4 Codes: 75571 EBCT 75572, 75573 Heart CT & Heart CT Congenital 75574 - CCTA LCD ID Number: L33559 J K
National Imaging Associates, Inc. Clinical guidelines EBCT HEART CT & HEART CT CONGENITAL CCTA CPT4 Codes: 75571 EBCT 75572, 75573 Heart CT & Heart CT Congenital 75574 - CCTA LCD ID Number: L33559 J K
Advanced Anesthesia. Presented by: Shelly Cronin, CPC, CPMA, CANPC, CGSC, CGIC. Agenda
 Advanced Anesthesia Presented by: Shelly Cronin, CPC, CPMA, CANPC, CGSC, CGIC 1 Agenda Understanding key terms Review coding concepts & modifiers Documentation standards How to avoid coding pitfalls New
Advanced Anesthesia Presented by: Shelly Cronin, CPC, CPMA, CANPC, CGSC, CGIC 1 Agenda Understanding key terms Review coding concepts & modifiers Documentation standards How to avoid coding pitfalls New
National Imaging Associates, Inc. Clinical guidelines CARDIAC CATHETERIZATION -LEFT HEART CATHETERIZATION. Original Date: October 2015 Page 1 of 5
 National Imaging Associates, Inc. Clinical guidelines CARDIAC CATHETERIZATION -LEFT HEART CATHETERIZATION CPT Codes: 93451, 93452, 93453, 93454, 93455, 93456, 93457, 93458, 93459, 93460, 93461 LCD ID Number:
National Imaging Associates, Inc. Clinical guidelines CARDIAC CATHETERIZATION -LEFT HEART CATHETERIZATION CPT Codes: 93451, 93452, 93453, 93454, 93455, 93456, 93457, 93458, 93459, 93460, 93461 LCD ID Number:
Ultrasound and Fluoroscopic Paravertebral Facet Joint Injections
 Policy Number FAC06222011RP Ultrasound and Fluoroscopic Approved By UnitedHealthcare Medicare Committee Current Approval Date 06/25/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable
Policy Number FAC06222011RP Ultrasound and Fluoroscopic Approved By UnitedHealthcare Medicare Committee Current Approval Date 06/25/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable
Sample page. Primary Care, Pediatrics/ Emergency Medicine. A comprehensive illustrated guide to coding and reimbursement CODING COMPANION
 CODING COMPANION 2018 Primary Care, Pediatrics/ Emergency Medicine A comprehensive illustrated guide to coding and reimbursement POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
CODING COMPANION 2018 Primary Care, Pediatrics/ Emergency Medicine A comprehensive illustrated guide to coding and reimbursement POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
Arterial Map of the Thorax, Abdomen and Pelvis 2017 Edition
 Arterial Map of the Thorax, Abdomen and Pelvis Angiography 75605 (-26) Aortography, thoracic 75625 (-26) Aortography, abdominal by serialography 75630 (-26) Aortography, abdominal + bilat iliofemoral 75705
Arterial Map of the Thorax, Abdomen and Pelvis Angiography 75605 (-26) Aortography, thoracic 75625 (-26) Aortography, abdominal by serialography 75630 (-26) Aortography, abdominal + bilat iliofemoral 75705
Intro: Slide 1. Slide 2. Slide 3. Basic understanding of interventional radiology. Gain knowledge of key terms and phrases
 Slide 1 Intro: PRESENTED BY: Selena M. Moore, AAS, CCS, CPC HIMS Physician Liaison Coder This is a modified/updated presentation that was originally written by: Rosemary Waligorski, RHIT, CCS, RCC and
Slide 1 Intro: PRESENTED BY: Selena M. Moore, AAS, CCS, CPC HIMS Physician Liaison Coder This is a modified/updated presentation that was originally written by: Rosemary Waligorski, RHIT, CCS, RCC and
Policy Specific Section:
 Payment Policy Anesthesia Services Type: Payment Policy Policy Specific Section: Payment Original Policy Date: Effective Date: October 1, 2010 06-16-2014 Description Anesthesia services consist of the
Payment Policy Anesthesia Services Type: Payment Policy Policy Specific Section: Payment Original Policy Date: Effective Date: October 1, 2010 06-16-2014 Description Anesthesia services consist of the
Transcatheter therapy, venous infusion for thrombolysis, any method, including radiological supervision and interpretation, initial treatment day
 Potential CPT Codes 1 CPT CPT Description Physician Work RVU Total RVU (In-Facility) 2018 National Avg. Medicare Physician Payment (In-Facility) Mechanical Thrombectomy 37187 37188 Percutaneous transluminal
Potential CPT Codes 1 CPT CPT Description Physician Work RVU Total RVU (In-Facility) 2018 National Avg. Medicare Physician Payment (In-Facility) Mechanical Thrombectomy 37187 37188 Percutaneous transluminal
The Third-Party Reimbursement Process for Orthotics
 The Third-Party Reimbursement Process for Orthotics When the foot hits the ground, everything changes. We know that over 90% of the population suffers with overpronation of their feet. Implementing Foot
The Third-Party Reimbursement Process for Orthotics When the foot hits the ground, everything changes. We know that over 90% of the population suffers with overpronation of their feet. Implementing Foot
Professional CGM Reimbursement Guide
 Professional CGM Reimbursement Guide 2015 TABLE OF CONTENTS Coding, Coverage and Payment...2 Coding and Billing...2 CPT Code 95250...3 CPT Code 95251...3 Incident to Billing for Physicians..............................................
Professional CGM Reimbursement Guide 2015 TABLE OF CONTENTS Coding, Coverage and Payment...2 Coding and Billing...2 CPT Code 95250...3 CPT Code 95251...3 Incident to Billing for Physicians..............................................
2017 Reimbursement Information for Mammography, CAD and Digital Breast Tomosynthesis 1
 GE Healthcare 2017 Reimbursement Information for Mammography, CAD and Digital Breast Tomosynthesis 1 February 2017 www.gehealthcare.com/reimbursement This advisory addresses Medicare coding, coverage and
GE Healthcare 2017 Reimbursement Information for Mammography, CAD and Digital Breast Tomosynthesis 1 February 2017 www.gehealthcare.com/reimbursement This advisory addresses Medicare coding, coverage and
General Surgery Getting to the Core. Disclaimer
 General Surgery Getting to the Core AAPC Regional Conference Nashville, Tennessee September 2011 1 Disclaimer The information in this presentation was current at the time the presentation was complied
General Surgery Getting to the Core AAPC Regional Conference Nashville, Tennessee September 2011 1 Disclaimer The information in this presentation was current at the time the presentation was complied
2019 MITRACLIP CODING AND PAYMENT GUIDE
 CLAIM 2019 MITRACLIP AND PAYMENT GUIDE MitraClip Transcatheter Mitral Valve Repair Hospital Rates: Effective October 1, 2018 Physician Rates: Effective January 1, 2019 References and Brief Summary 1 CLAIM
CLAIM 2019 MITRACLIP AND PAYMENT GUIDE MitraClip Transcatheter Mitral Valve Repair Hospital Rates: Effective October 1, 2018 Physician Rates: Effective January 1, 2019 References and Brief Summary 1 CLAIM
CODING SHEETS CHRONIC INTRACTABLE PAIN MANAGEMENT. Effective January 1, 2009 CODMAN 3000 NEUROMODULATION AND ONCOLOGY REIMBURSEMENT HOTLINE
 CODING SHEETS CHRONIC INTRACTABLE PAIN MANAGEMENT Effective January 1, 2009 CODMAN 3000 NEUROMODULATION AND ONCOLOGY REIMBURSEMENT HOTLINE Phone: 800-609-1108 Email: codmanpump@aol.com Fax: 303-703-1572
CODING SHEETS CHRONIC INTRACTABLE PAIN MANAGEMENT Effective January 1, 2009 CODMAN 3000 NEUROMODULATION AND ONCOLOGY REIMBURSEMENT HOTLINE Phone: 800-609-1108 Email: codmanpump@aol.com Fax: 303-703-1572
Modifier 62 - Co-surgery (Two Surgeons)
") Manual: Policy Title: Reimbursement Policy Modifier 62 - Co-surgery (Two Surgeons) Section: Modifiers Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM035 Last Updated: 7/5/2017 Last Reviewed:
Manual: Policy Title: Reimbursement Policy Modifier 62 - Co-surgery (Two Surgeons) Section: Modifiers Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM035 Last Updated: 7/5/2017 Last Reviewed:
POLICY AND PROCEDURE
 PAGE: Page 1 of 8 SCOPE: This policy applies to any provider furnishing services represented by Category III CPT codes. PURPOSE & IMPORTANT REMINDER: This policy is current at the time of publication.
PAGE: Page 1 of 8 SCOPE: This policy applies to any provider furnishing services represented by Category III CPT codes. PURPOSE & IMPORTANT REMINDER: This policy is current at the time of publication.
AHLA. UU. Diagnostic Imaging Services. Thomas W. Greeson Reed Smith LLP Falls Church, VA
 AHLA UU. Diagnostic Imaging Services Thomas W. Greeson Reed Smith LLP Falls Church, VA Institute on Medicare and Medicaid Payment Issues March 25-27, 2015 AHLA Institute on Medicare and Medicaid Payment
AHLA UU. Diagnostic Imaging Services Thomas W. Greeson Reed Smith LLP Falls Church, VA Institute on Medicare and Medicaid Payment Issues March 25-27, 2015 AHLA Institute on Medicare and Medicaid Payment
CODING SHEET HYDROCEPHALUS REIMBURSEMENT. All Medicare information is current as of the time of printing.
 CODING SHEET HYDROCEPHALUS REIMBURSEMENT All Medicare information is current as of the January 2014 Hydrocephalus ing Coding Options Commonly Billed Codes for Physicians, Hospitals, and Ambulatory Surgery
CODING SHEET HYDROCEPHALUS REIMBURSEMENT All Medicare information is current as of the January 2014 Hydrocephalus ing Coding Options Commonly Billed Codes for Physicians, Hospitals, and Ambulatory Surgery
2015 Reimbursement Information for Mammography, CAD and Digital Breast Tomosynthesis 1
 GE Healthcare 2015 Reimbursement Information for Mammography, CAD and Digital Breast Tomosynthesis 1 April, 2015 www.gehealthcare.com/reimbursement This advisory addresses Medicare coding, coverage and
GE Healthcare 2015 Reimbursement Information for Mammography, CAD and Digital Breast Tomosynthesis 1 April, 2015 www.gehealthcare.com/reimbursement This advisory addresses Medicare coding, coverage and
2018 Reimbursement Information for Mammography, CAD and Digital Breast Tomosynthesis 1
 GE Healthcare 2018 Reimbursement Information for Mammography, CAD and Digital Breast Tomosynthesis 1 May 2018 www.gehealthcare.com/reimbursement This advisory addresses Medicare coding, coverage and payment
GE Healthcare 2018 Reimbursement Information for Mammography, CAD and Digital Breast Tomosynthesis 1 May 2018 www.gehealthcare.com/reimbursement This advisory addresses Medicare coding, coverage and payment
Anesthesia. Chapter 16. CPT copyright 2010 American Medical Association. All rights reserved.
 Anesthesia Chapter 16 1 CPT Copyright CPT copyright 2010 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned
Anesthesia Chapter 16 1 CPT Copyright CPT copyright 2010 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned
CPT 2015: Prepare Your Coding Practice For New Codes As Technology Makes An Advance
 2015 Radiology Coding Survival Guide Section X : 2015 Coding Updates CPT 2015: Prepare Your Coding Practice For New Codes As Technology Makes An Advance Watch for changes in Vertebral fracture assessment,
2015 Radiology Coding Survival Guide Section X : 2015 Coding Updates CPT 2015: Prepare Your Coding Practice For New Codes As Technology Makes An Advance Watch for changes in Vertebral fracture assessment,
2018 HEMODIALYSIS CATHETERS CODING AND REIMBURSEMENT GUIDE
 2018 HEMODIALYSIS CATHETERS CODING AND REIMBURSEMENT GUIDE Contents Overview of Central Venous Access s for Hemodialysis 2 Procedures Using Hemodialysis s 2 Physician Reimbursement for Hemodialysis s 3
2018 HEMODIALYSIS CATHETERS CODING AND REIMBURSEMENT GUIDE Contents Overview of Central Venous Access s for Hemodialysis 2 Procedures Using Hemodialysis s 2 Physician Reimbursement for Hemodialysis s 3
Reimbursement Information for Automated Breast Ultrasound Screening
 GE Healthcare Reimbursement Information for Automated Breast Ultrasound Screening January 2015 www.gehealthcare.com/reimbursement The Invenia ABUS is indicated as an adjunct to mammography for breast cancer
GE Healthcare Reimbursement Information for Automated Breast Ultrasound Screening January 2015 www.gehealthcare.com/reimbursement The Invenia ABUS is indicated as an adjunct to mammography for breast cancer
Reimbursement Information for Ultrasound-guided Procedures Performed by Anesthesiologists 1
 GE Healthcare Information for Ultrasound-guided Procedures Performed by Anesthesiologists 1 January, 2013 www.gehealthcare.com/reimbursement This overview addresses coding, coverage, and payment for ultrasound
GE Healthcare Information for Ultrasound-guided Procedures Performed by Anesthesiologists 1 January, 2013 www.gehealthcare.com/reimbursement This overview addresses coding, coverage, and payment for ultrasound
CPT Category III Codes
 CPT Category III Codes Most recent changes to the CPT Category III Codes document Addition of 20 new Category III codes (0543T-0562T) and one revised Category III code (0402T) and guidelines accepted by
CPT Category III Codes Most recent changes to the CPT Category III Codes document Addition of 20 new Category III codes (0543T-0562T) and one revised Category III code (0402T) and guidelines accepted by
Sample page Orthopaedics: Spine & Above. A comprehensive illustrated guide to coding and reimbursement CODING COMPANION
 CODING COMPNION 2018 Orthopaedics: Spine & bove illustrated guide to coding and reimbursement POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com. Contents
CODING COMPNION 2018 Orthopaedics: Spine & bove illustrated guide to coding and reimbursement POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com. Contents
Primary to non-coronary IVUS
 codes 2018 2018 codes Primary to non-coronary IVUS Page 2 All coding, coverage, billing and payment information provided herein by Philips is gathered from third-party sources and is subject to change.
codes 2018 2018 codes Primary to non-coronary IVUS Page 2 All coding, coverage, billing and payment information provided herein by Philips is gathered from third-party sources and is subject to change.
REIMBURSEMENT GUIDE. Sovereign. Spinal System
 REIMBURSEMENT GUIDE Sovereign Spinal System REIMBURSEMENT GUIDE The Sovereign Spinal System is indicated for use with autogenous bone graft in patients with degenerative disc disease The Sovereign Spinal
REIMBURSEMENT GUIDE Sovereign Spinal System REIMBURSEMENT GUIDE The Sovereign Spinal System is indicated for use with autogenous bone graft in patients with degenerative disc disease The Sovereign Spinal
Coding of Procedures in Interventional Nephrology Produced in collaboration with:
 Coding of Procedures in Interventional Nephrology 2013 Produced in collaboration with: Introduction Proper coding of interventional procedures is a difficult and daunting, but essential task. Each procedure
Coding of Procedures in Interventional Nephrology 2013 Produced in collaboration with: Introduction Proper coding of interventional procedures is a difficult and daunting, but essential task. Each procedure
RADIATION THERAPY SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL
 RADIATION THERAPY SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL APRIL 2018 CSHCN PROVIDER PROCEDURES MANUAL APRIL 2018 RADIATION THERAPY SERVICES Table of Contents 34.1 Enrollment......................................................................
RADIATION THERAPY SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL APRIL 2018 CSHCN PROVIDER PROCEDURES MANUAL APRIL 2018 RADIATION THERAPY SERVICES Table of Contents 34.1 Enrollment......................................................................
2017 Final MFS Summary of Key IR Items SIR
 2017 Final MFS Summary of Key IR Items SIR On Wednesday, November 2, 2016, the Centers for Medicare & Medicaid Services (CMS) issued a final rule that updates payment policies and payment rates for services
2017 Final MFS Summary of Key IR Items SIR On Wednesday, November 2, 2016, the Centers for Medicare & Medicaid Services (CMS) issued a final rule that updates payment policies and payment rates for services
Six Major Section Of The Cpt Manual
 Six Major Section Of The Cpt Manual What section of the CPT manual would you find the code for a superficial abscess of the skin of the penis? What are the major sections of the CPT manual? 1. A discussion
Six Major Section Of The Cpt Manual What section of the CPT manual would you find the code for a superficial abscess of the skin of the penis? What are the major sections of the CPT manual? 1. A discussion
Working Smarter. Coding For Orthopaedic Trauma; Receiving Correct Reimbursement for Complex Cases
 Coding For Orthopaedic Trauma; Receiving Correct Reimbursement for Complex Cases 1 Presenting the claims for appropriate payment Unless the documentation is clear Coders cannot properly code No basis of
Coding For Orthopaedic Trauma; Receiving Correct Reimbursement for Complex Cases 1 Presenting the claims for appropriate payment Unless the documentation is clear Coders cannot properly code No basis of
Local Coverage Article for Chiropractic Services (A47798) Contractor Information. Article Information. Contractor Name. Contractor Numbers
 Contractor Information. Article Information. Contractor Name. Contractor Numbers") Local Coverage Article for Chiropractic Services (A47798) Print Contractor Information Contractor Name Novitas Solutions, Inc. Contractor Numbers 12501, 12502, 12101, 12102, 12201, 12202, 12301, 12302,
Local Coverage Article for Chiropractic Services (A47798) Print Contractor Information Contractor Name Novitas Solutions, Inc. Contractor Numbers 12501, 12502, 12101, 12102, 12201, 12202, 12301, 12302,
Radiation Therapy Services
 Radiation Therapy Services Chapter.1 Enrollment..................................................................... -2.2 Benefits, Limitations, and Authorization Requirements...........................
Radiation Therapy Services Chapter.1 Enrollment..................................................................... -2.2 Benefits, Limitations, and Authorization Requirements...........................
CPT 2018 Radiology Code Changes
 CPT 2018 Radiology Code Changes CPT 2018 Radiology Code Changes The following is a listing of new Current Procedural Terminology (CPT ) codes and their descriptors as described in the CPT 2018 codebook.
CPT 2018 Radiology Code Changes CPT 2018 Radiology Code Changes The following is a listing of new Current Procedural Terminology (CPT ) codes and their descriptors as described in the CPT 2018 codebook.
Schedule of Medical and Hospital Fees Adopted December 22, Effective January 1, 2010 Updated March 3, Marcia Davis Administrator
 Schedule of Medical and Hospital Fees Adopted December 22, 2009 Effective January 1, 2010 Updated March 3, 2010 Marcia Davis Administrator NOTICE The five character codes included in the Schedule of Medical
Schedule of Medical and Hospital Fees Adopted December 22, 2009 Effective January 1, 2010 Updated March 3, 2010 Marcia Davis Administrator NOTICE The five character codes included in the Schedule of Medical
ADDITIONS. The following codes have been added.
 ADDITIONS The following codes have been added. 99446 Interprofessional telephone/internet assessment and management service provided by treating/requesting physician or other qualified health care professional;
ADDITIONS The following codes have been added. 99446 Interprofessional telephone/internet assessment and management service provided by treating/requesting physician or other qualified health care professional;
SAMPLE. Behavioral Health Services
 Coding and Payment Guide www.optumcoding.com Behavioral Health Services An essential coding, billing, and reimbursement resource for psychiatrists, psychologists, and clinical social workers 2017 a ICD-10
Coding and Payment Guide www.optumcoding.com Behavioral Health Services An essential coding, billing, and reimbursement resource for psychiatrists, psychologists, and clinical social workers 2017 a ICD-10
CD Horizon Spire. CD Horizon Spire Z PHYSICIAN REIMBURSEMENT REIMBURSEMENT GUIDE. Spinal System and. Spinal System
 REIMBURSEMENT GUIDE CD Horizon Spire Spinal System and CD Horizon Spire Z Spinal System The CD Horizon Spire Plate is a posterior, single level, non-pedicle supplemental fixation device intended for use
REIMBURSEMENT GUIDE CD Horizon Spire Spinal System and CD Horizon Spire Z Spinal System The CD Horizon Spire Plate is a posterior, single level, non-pedicle supplemental fixation device intended for use
Re: CMS-1676-P Medicare Program; Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2018
 September 11, 2017 The Honorable Seema Verma Administrator Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services Attention: CMS-1676 P P.O. Box 8016 Baltimore, MD 21244-1850
September 11, 2017 The Honorable Seema Verma Administrator Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services Attention: CMS-1676 P P.O. Box 8016 Baltimore, MD 21244-1850
Reimbursement Information for Diagnostic Ultrasound and Ultrasound-guided Procedures Commonly Performed by Otolaryngologists
 GE Healthcare Reimbursement Information for Diagnostic Ultrasound and Ultrasound-guided Procedures Commonly Performed by Otolaryngologists 1 January, 2013 www.gehealthcare.com/reimbursement imagination
GE Healthcare Reimbursement Information for Diagnostic Ultrasound and Ultrasound-guided Procedures Commonly Performed by Otolaryngologists 1 January, 2013 www.gehealthcare.com/reimbursement imagination
Foundational funding sources allow BCCHP to screen and diagnose women outside of the CDC guidelines under specific circumstances in Washington State.
 Program Description The Breast, Cervical and Colon Health Program (BCCHP) screens qualifying clients for breast cancer. The program is funded through a grant from the Centers for Disease Control and Prevention
Program Description The Breast, Cervical and Colon Health Program (BCCHP) screens qualifying clients for breast cancer. The program is funded through a grant from the Centers for Disease Control and Prevention
2009 Pain Coding Update and Pain Industry Business Trends
 2009 Pain Coding Update and Pain Industry Business Trends Linda Van Horn, MBA June 13, 2009 2009 Pain Coding Update and Pain Industry Trends Agenda 2009 CPT Coding Updates Pay For Incentives ICD-10 American
2009 Pain Coding Update and Pain Industry Business Trends Linda Van Horn, MBA June 13, 2009 2009 Pain Coding Update and Pain Industry Trends Agenda 2009 CPT Coding Updates Pay For Incentives ICD-10 American
Medicare Updates Part 2. Tracy Cole, D.C.
 Medicare Updates Part 2 Tracy Cole, D.C. tcoledc@gmail.com Tracy Cole, D.C., Bio u u u u CCA representative to Noridian Contractor Advisory Committee for California Member, ACA Medicare Committee Member,
Medicare Updates Part 2 Tracy Cole, D.C. tcoledc@gmail.com Tracy Cole, D.C., Bio u u u u CCA representative to Noridian Contractor Advisory Committee for California Member, ACA Medicare Committee Member,
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. Rehabilitative Therapy Services
 Fee-for-Service Provider Manual Rehabilitative Therapy Services Updated 12.2015 PART II (PHYSICAL THERAPY, OCCUPATIONAL THERAPY, SPEECH/LANGUAGE PATHOLOGY) Introduction Section BILLING INSTRUCTIONS Page
Fee-for-Service Provider Manual Rehabilitative Therapy Services Updated 12.2015 PART II (PHYSICAL THERAPY, OCCUPATIONAL THERAPY, SPEECH/LANGUAGE PATHOLOGY) Introduction Section BILLING INSTRUCTIONS Page
Coding and Legislative Update. Sean P. Roddy, MD Professor of Surgery Albany Medical College Albany, NY
 Coding and Legislative Update Sean P. Roddy, MD Professor of Surgery Albany Medical College Albany, NY DISCLOSURES Sean Roddy, MD No relevant financial relationship reported Medicare Conversion Factor
Coding and Legislative Update Sean P. Roddy, MD Professor of Surgery Albany Medical College Albany, NY DISCLOSURES Sean Roddy, MD No relevant financial relationship reported Medicare Conversion Factor
The Endocrine Section Of The Cpt Manual Contains Codes For 6 Endocrine Glands
 The Endocrine Section Of The Cpt Manual Contains Codes For 6 Endocrine Glands The Endocrine subsection of the CPT manual contains codes for endocrine glands.. 3 b. 4 c. 5 d. 6. B. 4. there are nine glands
The Endocrine Section Of The Cpt Manual Contains Codes For 6 Endocrine Glands The Endocrine subsection of the CPT manual contains codes for endocrine glands.. 3 b. 4 c. 5 d. 6. B. 4. there are nine glands
Physical Medicine & Rehabilitation: Maximum Combined Frequency per Day Policy
 Policy Number Physical Medicine & Rehabilitation: Maximum Combined Frequency per Day Policy 2017R0101E Annual Approval Date 7/13/2016 Approved By Payment Policy Oversight Committee IMPORTANT NOTE ABOUT
Policy Number Physical Medicine & Rehabilitation: Maximum Combined Frequency per Day Policy 2017R0101E Annual Approval Date 7/13/2016 Approved By Payment Policy Oversight Committee IMPORTANT NOTE ABOUT
For more information, please contact your Molina Healthcare of New Mexico, Inc. Provider Service Representative toll free at (800)
") December 2012 Dear Practitioner/Provider, Effective January 1, 2013, there will be major changes to CPT-4 codes for behavioral health nationwide. These changes impact all practitioner/provider types (e.g.,
December 2012 Dear Practitioner/Provider, Effective January 1, 2013, there will be major changes to CPT-4 codes for behavioral health nationwide. These changes impact all practitioner/provider types (e.g.,
CPT Code Changes for 2013 Frequently Asked Questions Last Updated 12/2/2012
 1. Why are CPT codes changing? CPT Code Changes for 2013 Frequently Asked Questions Last Updated 12/2/2012 CPT code changes occur every year. The Current Procedural Terminology, or CPT, code set is maintained
1. Why are CPT codes changing? CPT Code Changes for 2013 Frequently Asked Questions Last Updated 12/2/2012 CPT code changes occur every year. The Current Procedural Terminology, or CPT, code set is maintained
Cervicocerebral Angiography Codes CPT Code Shortened Descriptor RUC Rec RVU CMS Interim RVU
 AMERICAN ASSOCIATION OF NEUROLOGICAL SURGEONS THOMAS A. MARSHALL, Executive Director 5550 Meadowbrook Drive Rolling Meadows, IL 60008 Phone: 888-566-AANS Fax: 847-378-0600 info@aans.org President MITCHEL
AMERICAN ASSOCIATION OF NEUROLOGICAL SURGEONS THOMAS A. MARSHALL, Executive Director 5550 Meadowbrook Drive Rolling Meadows, IL 60008 Phone: 888-566-AANS Fax: 847-378-0600 info@aans.org President MITCHEL
Ultrasound Reimbursement Guide 2015: BioJet Fusion
 Ultrasound Reimbursement Guide 2015: BioJet Fusion Diagnosis codes explain the rationale for a given service and are a key factor in a payer s evaluation of medical necessity and coverage determination
Ultrasound Reimbursement Guide 2015: BioJet Fusion Diagnosis codes explain the rationale for a given service and are a key factor in a payer s evaluation of medical necessity and coverage determination
Coding Terminology Getting Back To The Basics. Financial Interest. Getting Back To The Basics. Rose & Associates
 Coding Terminology Getting Back To The Basics ASCRS ASOA Symposium & Congress Administrator Program Boston, Massachusetts April 25-29, 2014 Presented by: Patricia Kennedy, COMT, CPC, COE Financial Interest
Coding Terminology Getting Back To The Basics ASCRS ASOA Symposium & Congress Administrator Program Boston, Massachusetts April 25-29, 2014 Presented by: Patricia Kennedy, COMT, CPC, COE Financial Interest