Huntington s & Parkinson s Diseases: Neurologic & Psychiatric Issues. Burton Scott PhD, MD Duke Movement Disorders Center Durham, NC
|
|
|
- Maude Nelson
- 5 years ago
- Views:
Transcription

1 Huntington s & Parkinson s Diseases: Neurologic & Psychiatric Issues Burton Scott PhD, MD Duke Movement Disorders Center Durham, NC

2 Huntington s Disease Typically adult-onset, autosomal dominant disorder characterized by involuntary movements (chorea), dementia, and behavioral changes 25,000 affected w/ HD in USA Loss of medium spiny neurons from caudate/putamen Chm 4p16.3 CAG repeats George Huntington Huntington G. On chorea. Med Surg Report 1872; 26:320
3 Triad of Symptoms of HD
4 Basal Ganglia Huntington s disease (loss of medium spiny neurons in striatum:

5 Epidemiology of Huntington s Disease

6 Cause of Huntington s disease: The HD gene

7 Early Huntington s Disease 28 yrs old 1 yr h/o falls, dropping things 6 month h/o mild chorea

8 Huntington s Disease 5 yrs later Age 33 6 yrs after sx onset
9 Prodromal Issues in HD Impaired perception of time. Frequently late, mis-estimate time needed to complete tasks Slowing of processing speed. Ordinary mental tasks more tiring and take longer. Impaired determination of emotion from facial expression or verbal intonation Impaired smell identification, but detection ok. Paulsen JS; Curr Neuro Neurosci Rep (2011) 11:474-83
10 Cognitive Difficulty in HD Can occur decades before motor symptoms appear. Difficulty learning new things and retrieving previously learned information Implicit memory (i.e. skills required to ride a bike, play an instrument, drive a car, perform a task) more compromised than explicit memory (i.e. names, dates) Attention deficits Impaired executive function Impaired communication due to dysarticulation, impaired initiation & comprehension of discourse. Can have impairment of one s own actions & feelings Paulsen JS; Curr Neuro Neurosci Rep (2011) 11:474-83
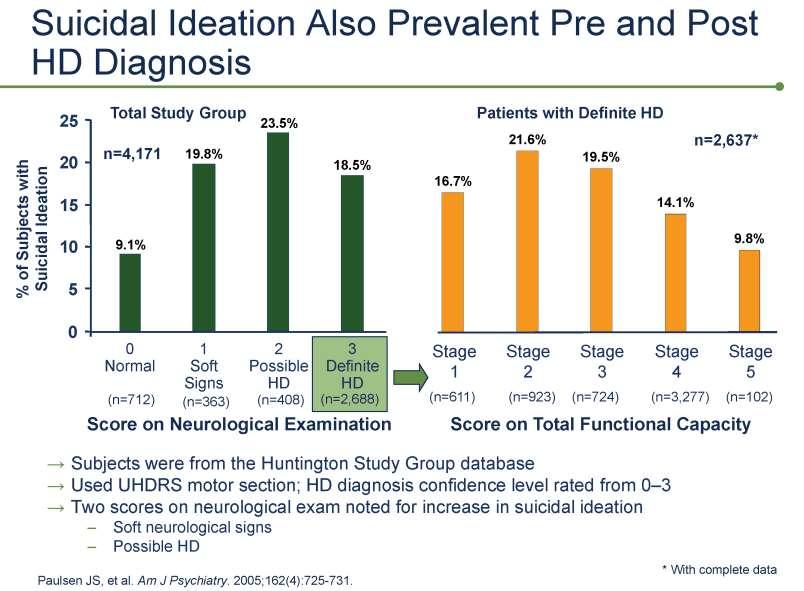
11 Mood-Related Symptoms Common in HD Presymptomatic carriers of HTT mutation: higher psychologic stress, irritability, hostility Predict-HD study found depression, hostility,obsessive-compulsiveness, anxiety, interpersonal sensitivity, phobic anxiety, psychoticism in HTT mutation carriers 10 yrs before predicted onset of motor sx. Depression common; 19% w/ MDD; increased risk of attempted/completed suicide Acta Psychiatr Scand 105(2002):224-30; Biol Psychiatry 62(2007):1341-6;J Neurol Neurosurg Psychiatry 71(2001):310-4; Neurodegener Dis 8(2011): ; J Med Genet 30(1993):293-5.

12 Depression is common in HD

13 Depression symptoms occur early in HD
14
15 Cognitive & Behavioral Changes Place the greatest burden on HD families Most highly associated with functional decline Can be predictive of NH placement Can be present >15 yrs before motor dx. Are highly related to disease specific MRI volume loss Paulsen JS; Curr Neuro Neurosci Rep (2011) 11:474-83
16 Medical Treatment of HD Motor (chorea): Tetrabenazine, deutetrabenazine Behavioral: antidepressants (sertraline & others), antipsychotics (risperidone, aripiprazole & others), anxiolytics (clonazepam) Dementia: consider acetylcholinesterase inhibitors off-label such as donepezil, rivastigmine; and also memantine
17 Summary for HD Cognitive (dementia) and Behavioral decline (irritability, compulsiveness, apathy, poor judgement)d are generally more disabling in Huntington s disease than the motor signs and symptoms Decline of motor control leads to morbidity due to falls, in addition to weight loss from dysphagia and resulting aspiration and resulting infection. HD depletes family resources financially and emotionally

18 Parkinson s Disease Dr James Parkinson English physician Published An Essay on the Shaking Palsy in 1817 Description of 6 patients me-jaa.com

19 Parkinson s Disease: Clinical Features Chronic neurodegenerative illness caused by loss of dopamine-containing neurons in substantia nigra Cardinal signs: Rigidity, bradykinesia, tremor at rest, postural instability Other features: Hypomimia, drooling, hypophonia, micrographia, stooped posture, shuffling gait, retropulsion, festination Often asymmetric onset Control Parkinson s disease
20 Basal Ganglia Clinical Correlation Parkinson s disease (loss of dopaminergic neurons in substantia nigra)
21

22 Parkinson s Disease
23 Symptomatic Treatment of Parkinson s Disease Dopamine releaser Amantadine Symmetrel mg Anticholinergics Trihexyphenidyl Artane 2-10 mg Benztropine Cogentin mg MAO-B inhibition Selegiline Eldepryl, Zelopar 5-10 mg, mg Rasagiline Azilect mg Dopamine agonists Bromocriptine Parlodel mg (Pergolide) (Permax) ( mg) Pramipexole Mirapex mg Ropinirole Requip 2-24 mg (Rotigotine) (Neupro) (2-6 mg/24hrs)
24 Symptomatic Treatment of PD Dopamine precursor carbidopa/levodopa Sinemet regular 10/100, 25/100, 25/250 Sinemet ext rel CR25/100, CR50/200 COMT Inhibitor entacapone Comtan tolcapone Tasmar rarely used Peripheral Decarboxylase Inhibitor carbidopa Lodosyn mg Combination carbidopa/levodopa/entacapone Stalevo 12.5/50/200, 25/100/ /150/200
25 Non-Motor Symptoms in PD Depression Dementia Hallucinations Sleep difficulty include: Impulse dyscontrol manifested as: pathologic gambling hypersexuality, and other compulsive behaviors.
26 Neuropsychiatric Symptoms in Early, Untreated PD Depression 33% Alexithymia 20% Anxiety 20% Impulsivity 10% Poletti et al. J Neuropsych Clinc Neurosci 2012; 24:E22-E23.
27 ICDs in early, untreated PD Minnesota Impulsive Disorder Interview and South Oaks Gambling Scale At least 1 ICD 18.5 % Binge eating 7.1 % Hobbyism 5.4 % Punding 4.8 % Hypersexuality 4.2 % Buying 3.0 % Gambling 1.2 % Walkabout 0.6 % Weintraub et al, Neur, 2013; 80:
28 Impulse Control Disorders in Parkinson s Disease Compulsive gambling, buying, sexual behaviors, eating, punding Failure to resist an impulse, drive, or temptation to perform an act that is harmful to the person or to others (DSM-IV-TR)
29 Possible ICDs Change in personality or behavior Increased secrecy Increased time at hobbies or work Decreased need for sleep, or increased insomnia Increased medication intake Hoarding medications Stacy (2009). Medicine Reports 1:29
30 Risk Factors for ICD PD dx before age 50 Dx > 5 yrs Male Hx/o depression, anxiety, bipolar d/o Prior drug/etoh abuse, gambling, other addiction FHx of mental illness, drug/etoh addiction Dyskinesias Levodopa or equivalent > 1000 mg/day Dopamine agonist use Stacy (2009). Medicine Reports 1:20
 Mov Disord")
31 Cerebral Blood Flow in ICD vs non-icd Parkinson s Disease Pts Rao et al (2010) Mov Disord 25:
32 Impulse Control Disorder: Cross Dressing 82 yo WM with PD. Onset age 70 with decreased dexterity at L hand when typing. FHx: Sister with schizophrenia. Mom (d) suicide when pt was age 2. Two children. SHx: Flew jets in the military. Married for 55 yrs. 73: Urge to cross dress since prostate surgery, w/ incr urges since starting PD meds. Ropin 9 mg, selegiline 5 mg, l-dopa 200 mg 73.6: Sees psych for recurr depression. Awakes w/ urge to cross dress. 74.1: Psych: urge to wear woman s clothes,? rel to mother leaving him (suicide) and having 3 step-mothers as child. Stays active to fight cross dressing urges Age 82: Still has urges to wear women s undergarments. On l-dopa 900, ropinirole 4, olanzapine 10 (after hospital n for psychosis, later tapered off), ritalin 10
33 ICD Case: Compulsive Fishing 49 yo WM. Onset PD age 40 w/ sl hand tr, decr L hand dexterity typing. FHx: sister bipolar; brother w/ tremor SHx: Heavy etoh in college; Navy grad; Married w/2 kids. Executive Dxd PD age 41, started pramipexole 45: Fishes compulsively about 1 hr daily, but says, I don t have to every day. Not a problem. On L-dopa , pram 3; clonaz 2 46: Fishing compulsively. Trip to Brazil to fish. 47: Eats compulsively. Daytime sleepiness. Rollover MVA, (? sleep driving). Inj knee jumping out of boat. Personality changes. Wife tearful & near to leaving him. Insomnia. Fixates on a topic. Intense. Pressured speech. Decreased insight. Thinks about fishing daily. L- dopa 1200, pram 2, amant 100, rasag 1 mg, modaf 100, amitrip 50
34 ICD: Fishing 48: Compuls eating. No filter : Says whatever he thinks. Argues, agitated. Fishes compulsively, out 8 PM to 5 AM. Online poker. Easily distracted. Unable to multitask. Wild dreams. L-dopa , entac 1200, pram 2, amant 100, rasag 1. May double meds. Then: Wife discovered he spent $100 s at a strip club when supposedly out all night fishing. Frequented strip clubs in past, now much more often. Wanted to change, reduce PD meds. 48.5: Deep Brain Stim (DBS) surgery By age 49: Behavior stabilized. No problems with compulsive urges. Exercising. Doing yard work. Taking L-dopa 500 to 600, amantadine 200 Age 49.5: No compulsive behaviors. Home life stable.
35 ICD Case: Gambling etc. 62 yo WM with PD > 10 yrs. Age 54: Rotigotine 13.5 mg patch. Some drowsiness when driving without falling asleep. Age 55: Drowsy, not falling asleep driving. Rotigotine 18 mg patch, selegiline 10 mg
36 Case: Pathologic Gambling Age 56.2: Enjoyed recreational gambling with losses of $ On PD meds, addiction to video poker. Losses of $1-2K over hrs. $ K over yrs, mostly video poker. Made excuses for being late so he could gamble. Read about pathologic gambling & DA use while seeing gambling counselor. He noted increased interest in gambling after starting selegiline. H/o cross dressing 2-3/ yr since age 6-7. Not previously interfering with his life. Urges to cross dress became overwhelming since fighting the gambling addiction. Pt & wife separated because she was unable to tolerate his behavior.
37 Case: Gambling etc. Moved into appt. Cross dressed daily after work. Obsessive cleaning. Punding: takes apart lawnmower, cleans it, and puts it back together. Compelled to mow his small yard daily. Emotionally labile. SI, no SA or plan. On selegiline, more aggressive betting. On L-dopa 500 mg, rotigotine 18 mg, selegiline 10 mg. Age 56.6: Reunited with his wife of 36 yrs who finds his behavior improved & he is more like he was years ago. No punding. Can concentrate. Still working. Wife working to help w/ debts. Some marital strain due to finances. No cross dressing except briefly a few wkends. No compul gambling since stopped rotigot. L-dopa 400 Age 59.3: Wife retired. Both home. Financially okay. Reconciled. No ICD. L-dopa 700, amant 200
38 Impulse Control Disorder (ICD) Treatment Recognition of the problem! Taper off of stimulants, dopamine agonists Treatment with amantadine, antipsychotics DBS may permit further reduction of dopaminergic therapy and hence better control of ICD.
39 Summary for PD Both Motor and Non-Motor symptoms are problematic in PD Motor symptoms including rigidity, bradykinesias, resting tremor, postural instability Non-Motor symptoms include depression, dementia, hallucination, sleep difficulty, and impulse dyscontrol manifested as pathologic gambling, hypersexuality, and other compulsive behaviors.
Huntington s & Parkinson s Diseases: Neurologic & Psychiatric Issues. Huntington s Disease
 Huntington s & Parkinson s Diseases: Neurologic & Psychiatric Issues Burton Scott PhD, MD Duke Movement Disorders Center Durham, NC Huntington s Disease Typically adult-onset, autosomal dominant disorder
Huntington s & Parkinson s Diseases: Neurologic & Psychiatric Issues Burton Scott PhD, MD Duke Movement Disorders Center Durham, NC Huntington s Disease Typically adult-onset, autosomal dominant disorder
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Associate Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Assistant Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
Best Medical Treatments for Parkinson s disease
 Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
Parkinson s Disease Update. Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015
 Parkinson s Disease Update Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015 Parkinson s Disease Progressive, chronic, neurodegenerative disease Slow,
Parkinson s Disease Update Colleen Peach, RN, MSN, FNP Movement Disorders Clinic Emory University School of Medicine March 7, 2015 Parkinson s Disease Progressive, chronic, neurodegenerative disease Slow,
Alison Charleston 1 st September 2016
 Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1)
") 475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
475 GERIATRIC PSYCHOPHARMACOLOGY (p.1) I. General Information? Use lower doses? Start low and go slow? Expect prolonged elimination ½ lives? Expect sedative-hypnotics to be dementing, to impair cognitive
PARKINSON S MEDICATION
 PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
PARKINSON S MEDICATION History 1940 50 s Neurosurgeons operated on basal ganglia. Improved symptoms. 12% mortality 1960 s: Researchers identified low levels of dopamine caused Parkinson s leading to development
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Objectives. Emerging Treatments in Parkinson s s Disease. Pathology. As Parkinson s progresses it eventually affects large portions of the brain.
 Objectives Emerging Treatments in Parkinson s s Disease 1) Describe recent developments in the therapies for Parkinson s Disease Jeff Kraakevik MD Assistant Professor OHSU/Portland VAMC Parkinson s Center
Objectives Emerging Treatments in Parkinson s s Disease 1) Describe recent developments in the therapies for Parkinson s Disease Jeff Kraakevik MD Assistant Professor OHSU/Portland VAMC Parkinson s Center
Cardinal Features of Parkinson s. Management of Parkinson s Disease. Drug Induced Parkinson s. Other Parkinson s Symptoms.
 Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Cardinal Features of Parkinson s Management of Parkinson s Disease Kristin S. Meyer, PharmD, CGP, FASHP Assistant Professor of Pharmacy Practice Drake University & Iowa Veterans Home Spring 2009 Tremor
Parkinson s Disease Medications: Professionals Edition
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
8/28/2017. Behind the Scenes of Parkinson s Disease
 BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
PD ExpertBriefing: Impulsive and Compulsive Behaviors in Parkinson s Disease
 PD ExpertBriefing: Impulsive and Compulsive Behaviors in Parkinson s Disease Presented By: Daniel Weintraub, M.D. Associate Professor of Psychiatry, University of Pennsylvania; Parkinson s Disease and
PD ExpertBriefing: Impulsive and Compulsive Behaviors in Parkinson s Disease Presented By: Daniel Weintraub, M.D. Associate Professor of Psychiatry, University of Pennsylvania; Parkinson s Disease and
Key Concepts and Issues in Parkinson s Disease in 2016
 Key Concepts and Issues in Parkinson s Disease in 2016 Michael Rezak, M.D., Ph.D. Section Chief, Neurosciences Institute Director, Movement Disorders and Neurodegenerative Diseases Center Northwestern
Key Concepts and Issues in Parkinson s Disease in 2016 Michael Rezak, M.D., Ph.D. Section Chief, Neurosciences Institute Director, Movement Disorders and Neurodegenerative Diseases Center Northwestern
Medications used to treat Parkinson s disease
 Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
Medications used to treat Parkinson s disease Edwin B. George, M.D., Ph.D. Director of Wayne State University Movement Disorder Clinic University Health Center Neurology Clinic University Health The John
Treatment of Parkinson s Disease and of Spasticity. Satpal Singh Pharmacology and Toxicology 3223 JSMBS
 Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
PARKINSON S DISEASE. Nigrostriatal Dopaminergic Neurons 5/11/16 CARDINAL FEATURES OF PARKINSON S DISEASE. Parkinson s disease
 5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Parkinson s disease Therapeutic strategies. Surat Tanprawate, MD Division of Neurology University of Chiang Mai
 Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
How to Effectively Manage the Motor Symptoms of HD
 How to Effectively Manage the Motor Symptoms of HD Yvette Bordelon, MD, PhD Associate Clinical Professor of Neurology David Geffen School of Medicine at UCLA The information provided by speakers in workshops,
How to Effectively Manage the Motor Symptoms of HD Yvette Bordelon, MD, PhD Associate Clinical Professor of Neurology David Geffen School of Medicine at UCLA The information provided by speakers in workshops,
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University
 Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to
 parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
parts of the gastrointenstinal tract. At the end of April 2008, it was temporarily withdrawn from the US Market because of problems related to crystallization of the drug, which caused unreliable drug
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging. Dr. Olav E. Krigolson Lecture 5: PARKINSONS DISEASE
 ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
Parkinson s Disease Update
 Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
Parkinson s Disease Update Elise Anderson MD Providence Center for Parkinson s Disease October 26, 2017 11/6/2017 1 Disclosures GE Speaker, DaTSCAN 11/6/2017 2 Outline PD diagnosis Motor and nonmotor symptoms
What is Parkinson s Disease?
 2018 Update in Parkinson s Disease: Treatments and Future Plans Arita McCoy, MSN, CRNP Johns Hopkins Parkinson s Disease and Movement Disorder Center A National Parkinson Foundation Center of Excellence
2018 Update in Parkinson s Disease: Treatments and Future Plans Arita McCoy, MSN, CRNP Johns Hopkins Parkinson s Disease and Movement Disorder Center A National Parkinson Foundation Center of Excellence
Non-Motor Symptoms of Parkinson s Disease
 Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Psychiatric aspects of Parkinson s disease an update
 Psychiatric aspects of Parkinson s disease an update Dr Chris Collins 027 2787593 chris.collins@cdhb.health.nz Disclosures: none Non-motor aspects physical Sensory anosmia, visual symptoms Speech and
Psychiatric aspects of Parkinson s disease an update Dr Chris Collins 027 2787593 chris.collins@cdhb.health.nz Disclosures: none Non-motor aspects physical Sensory anosmia, visual symptoms Speech and
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
PD: Key Treatment Considerations
 PD: Key Treatment Considerations 2018 Management of Neurologic and Neurosurgical Disorders in Daily Practice Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 11/27/2018 1 Outline Treatment
PD: Key Treatment Considerations 2018 Management of Neurologic and Neurosurgical Disorders in Daily Practice Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 11/27/2018 1 Outline Treatment
Communicating About OFF Episodes With Your Doctor
 Communicating About OFF Episodes With Your Doctor Early in Parkinson s disease (PD), treatment with levodopa and other anti-pd drugs provides continuous benefit. As the disease progresses, however, symptom
Communicating About OFF Episodes With Your Doctor Early in Parkinson s disease (PD), treatment with levodopa and other anti-pd drugs provides continuous benefit. As the disease progresses, however, symptom
The Fresco Institute for Parkinson's and Movement Disorders
 The Fresco Institute for Parkinson's and Movement Disorders Follow Up Patient Questionnaire Name: Date: Accompanied by: Do you smoke? CURRENT PAST NEVER Which neurological symptom bothers you most right
The Fresco Institute for Parkinson's and Movement Disorders Follow Up Patient Questionnaire Name: Date: Accompanied by: Do you smoke? CURRENT PAST NEVER Which neurological symptom bothers you most right
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Advances in Parkinson s Disease Treatment. Ryan J. Uitti, M.D. Professor of Neurology Mayo Clinic, Jacksonville, FL
 Advances in Parkinson s Disease Treatment Ryan J. Uitti, M.D. Professor of Neurology Mayo Clinic, Jacksonville, FL Uitti.ryan@mayo.edu Ryan J. Uitti, MD Disclosure receives research support from NIH/NINDS,
Advances in Parkinson s Disease Treatment Ryan J. Uitti, M.D. Professor of Neurology Mayo Clinic, Jacksonville, FL Uitti.ryan@mayo.edu Ryan J. Uitti, MD Disclosure receives research support from NIH/NINDS,
Drug Therapy of Parkinsonism. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N.
 PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
PD ExpertBriefings: Parkinson s Medications: Today and Tomorrow Led By: Cynthia L. Comella, M.D., F.A.A.N. To hear the session live on: Tuesday, April 17, 2012 at 1:00 PM ET. DIAL: 1 (888) 272-8710 and
Parkinson s Disease. Medications
 Parkinson s Disease Medications By David Houghton, MD, MPH, Howard Hurtig, MD, and Sharon Metz, RN, MPH, with guest authors Monique Giroux, MD, Giselle Petzinger, MD, Beth Fisher, PT, PhD, Lauren Hawthorne,
Parkinson s Disease Medications By David Houghton, MD, MPH, Howard Hurtig, MD, and Sharon Metz, RN, MPH, with guest authors Monique Giroux, MD, Giselle Petzinger, MD, Beth Fisher, PT, PhD, Lauren Hawthorne,
9/26/18. Objectives. Disclosures. Parkinson s Disease Update Clinical and Operational Considerations
 Parkinson s Disease Update Clinical and Operational Considerations Dana Saffel, PharmD, BCGP, CPh, FASCP President, CEO PharmaCare Strategies, Inc. September 2018 Objectives Describe epidemiology and pathophysiology
Parkinson s Disease Update Clinical and Operational Considerations Dana Saffel, PharmD, BCGP, CPh, FASCP President, CEO PharmaCare Strategies, Inc. September 2018 Objectives Describe epidemiology and pathophysiology
History Parkinson`s disease. Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson
 Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinson s Disease. Gillian Sare
 Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
Parkinson s Disease Gillian Sare Outline Reminder about PD Parkinson s disease in the inpatient Surgical patients with PD Patients who cannot swallow End of life care Parkinson s disease PD is the second
The symptoms of the Parkinson s disease may vary from person to person. The symptoms might include the following:
 1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Faculty. Joseph Friedman, MD
 Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Parkinson s Disease Foundation. PD ExpertBriefing: Managing the Motor Symptoms in PD
 Parkinson s Disease Foundation PD ExpertBriefing: Managing the Motor Symptoms in PD Led By: Sotirios A. Parashos, M.D. Minneapolis Clinic of Neurology and Struthers Parkinson's Center This session was
Parkinson s Disease Foundation PD ExpertBriefing: Managing the Motor Symptoms in PD Led By: Sotirios A. Parashos, M.D. Minneapolis Clinic of Neurology and Struthers Parkinson's Center This session was
With Time, The Pathology of PD Spreads Throughout the Brain
 With Time, The Pathology of PD Spreads Throughout the Brain Braak s staging of Parkinson s disease pathology dm co sn mc hc fc 1 Hubert H. Fernandez, MD, FAAN Professor of Medicine (Neurology) Cleveland
With Time, The Pathology of PD Spreads Throughout the Brain Braak s staging of Parkinson s disease pathology dm co sn mc hc fc 1 Hubert H. Fernandez, MD, FAAN Professor of Medicine (Neurology) Cleveland
Commonly encountered medications and their side effects - what the generalist needs to know
 Commonly encountered medications and their side effects - what the generalist needs to know Jeremy Cosgrove Consultant Neurologist Leeds Teaching Hospitals NHS Trust Outline: Parkinson s medications and
Commonly encountered medications and their side effects - what the generalist needs to know Jeremy Cosgrove Consultant Neurologist Leeds Teaching Hospitals NHS Trust Outline: Parkinson s medications and
What s new for diagnosing and treating Parkinson s Disease?
 What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
What s new for diagnosing and treating Parkinson s Disease? Erika Driver-Dunckley, MD Associate Professor of Neurology Program Director Movement Disorders Fellowship Assistant Program Director Neurology
Chapter 20. Media Directory. Amyotrophic Lateral Sclerosis. Alzheimer s Disease. Huntington s Chorea. Multiple Sclerosis
 Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Enhanced Primary Care Pathway: Parkinson s Disease
 Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Parkinson's Disease KP Update
 Parkinson's Disease KP Update Andrew Imbus, PA-C Neurology, Movement Disorders Kaiser Permanente, Los Angeles Medical Center No disclosures "I often say now I don't have any choice whether or not I have
Parkinson's Disease KP Update Andrew Imbus, PA-C Neurology, Movement Disorders Kaiser Permanente, Los Angeles Medical Center No disclosures "I often say now I don't have any choice whether or not I have
The Role of Pharmacists in Treating & Managing Parkinson s Disease Author: Mary Jo Carden, RPh, JD Principal, Carden Associates
 The Role of Pharmacists in Treating & Managing Parkinson s Disease Author: Mary Jo Carden, RPh, JD Principal, Carden Associates Editor: Marsha K. Millonig, MBA, RPh President/CEO Catalyst Enterprises,
The Role of Pharmacists in Treating & Managing Parkinson s Disease Author: Mary Jo Carden, RPh, JD Principal, Carden Associates Editor: Marsha K. Millonig, MBA, RPh President/CEO Catalyst Enterprises,
Medication Management & Strategies When the levodopa honeymoon is over
 Medication Management & Strategies When the levodopa honeymoon is over Eric J Pappert, MD Parkinson s Disease & Movement Disorders Center Neurology Associates Medication Options in Parkinson s Carbidopa/Levodopa
Medication Management & Strategies When the levodopa honeymoon is over Eric J Pappert, MD Parkinson s Disease & Movement Disorders Center Neurology Associates Medication Options in Parkinson s Carbidopa/Levodopa
Behavioral Aspects of Parkinson s Disease
 Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Program Highlights. Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone Medical Center New York, New York
 Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Parkinsons Disease update. Sindhu R Srivatsal MD MPH Virginia Mason Medical Center
 Parkinsons Disease update Sindhu R Srivatsal MD MPH Virginia Mason Medical Center PARKINSONISM Vs PARKINSON S Parkinsonism Bradykinesia: slowness of movements (essential feature) PLUS one of Tremor: resting
Parkinsons Disease update Sindhu R Srivatsal MD MPH Virginia Mason Medical Center PARKINSONISM Vs PARKINSON S Parkinsonism Bradykinesia: slowness of movements (essential feature) PLUS one of Tremor: resting
Parkinson s disease. Information for patients and carers. The Leeds Teaching Hospitals NHS Trust
 n The Leeds Teaching Hospitals NHS Trust Parkinson s disease Information for patients and carers in partnership with Leeds Community Healthcare NHS Trust The symptoms of Parkinson s appear when the levels
n The Leeds Teaching Hospitals NHS Trust Parkinson s disease Information for patients and carers in partnership with Leeds Community Healthcare NHS Trust The symptoms of Parkinson s appear when the levels
Margo J Nell Dept Pharmacology
 Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease Duncan Gerry. 5/12/12 All drugs are poison
 Parkinson s Disease Duncan Gerry 5/12/12 All drugs are poison Order of the Day Current and future of PD service in Hillingdon Case history highlighting the complexity of management, presentation and some
Parkinson s Disease Duncan Gerry 5/12/12 All drugs are poison Order of the Day Current and future of PD service in Hillingdon Case history highlighting the complexity of management, presentation and some
Managing Challenging Behaviors
 Managing Challenging Behaviors Barbara J. Kocsis, MD Psychiatry Resident, HDSA Center of Excellence UC Davis School of Medicine & Lorin M. Scher, MD Attending Psychiatrist, HDSA Center of Excellence UC
Managing Challenging Behaviors Barbara J. Kocsis, MD Psychiatry Resident, HDSA Center of Excellence UC Davis School of Medicine & Lorin M. Scher, MD Attending Psychiatrist, HDSA Center of Excellence UC
Parkinson s Pharmacology
 PHPP 517 (IT-III) Fall 2011 JACOBS Wed 10/12 8:00 8:50 AM 1 Learning objectives 1. Describe the direct and indirect pathways of the extrapyramidal system and its modulation by ACh and DA. 2. Contrast the
PHPP 517 (IT-III) Fall 2011 JACOBS Wed 10/12 8:00 8:50 AM 1 Learning objectives 1. Describe the direct and indirect pathways of the extrapyramidal system and its modulation by ACh and DA. 2. Contrast the
Parkinson s Disease. Graham A. Glass, MD. Assistant Professor of Neurology University of California San Francisco
 Parkinson s Disease Graham A. Glass, MD Assistant Professor of Neurology University of California San Francisco San Francisco VA Medical Center Parkinson s Disease Research, Education and Clinical Center
Parkinson s Disease Graham A. Glass, MD Assistant Professor of Neurology University of California San Francisco San Francisco VA Medical Center Parkinson s Disease Research, Education and Clinical Center
Welcome and Introductions
 Parkinson s Disease Spotlight on Treatment Advances Tuesday, January 26, 2016 Welcome and Introductions Stephanie Paul Vice President Development and Marketing American Parkinson Disease Association 1
Parkinson s Disease Spotlight on Treatment Advances Tuesday, January 26, 2016 Welcome and Introductions Stephanie Paul Vice President Development and Marketing American Parkinson Disease Association 1
2/20/18. History of Parkinson s. What is happening in the brain? DOPAMINE! Epidemiology. Parkinson s Disease. It s much more than tremor
 Parkinson s Disease History of Parkinson s It s much more than tremor Laura Dixon, DNP, MPA, APRN, FNP-BC University of Louisville Department of Neurology Movement Disorders Division Parkinson s Disease
Parkinson s Disease History of Parkinson s It s much more than tremor Laura Dixon, DNP, MPA, APRN, FNP-BC University of Louisville Department of Neurology Movement Disorders Division Parkinson s Disease
05-Nov-15. Impact of Parkinson s Disease in Australia. The Nature of Parkinson s disease 21st Century
 Peter Silburn Professor Clinical Neuroscience University of Queensland Queensland Brain Institute Neurosciences Queensland Impact of in Australia Second most common neurodegenerative disorder Up to 64,000
Peter Silburn Professor Clinical Neuroscience University of Queensland Queensland Brain Institute Neurosciences Queensland Impact of in Australia Second most common neurodegenerative disorder Up to 64,000
HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D.
 HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D. Professor of Psychiatry, Neurology, and Pediatrics University of Iowa, Iowa City, Iowa The information provided
HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D. Professor of Psychiatry, Neurology, and Pediatrics University of Iowa, Iowa City, Iowa The information provided
Drugs Affecting the Central Nervous System
 Asst Prof Inam S Arif isamalhaj@yahoo.com Drugs Affecting the Central Nervous System Ass Efferent neurons in ANS Neurodegenerative Diseases Parkinson s Disease Multiple Sclerosis Alzheimer s Disease
Asst Prof Inam S Arif isamalhaj@yahoo.com Drugs Affecting the Central Nervous System Ass Efferent neurons in ANS Neurodegenerative Diseases Parkinson s Disease Multiple Sclerosis Alzheimer s Disease
2-The age at onset of PD is variable, usually between 50 and 80 years, with a mean onset of 55 years (1).
.") Parkinson Disease 1-Parkinson disease (PD) is a chronic, progressive movement disorder resulting from loss of dopamine from the nigrostriatal tracts in the brain, and is characterized by rigidity, bradykinesia,
Parkinson Disease 1-Parkinson disease (PD) is a chronic, progressive movement disorder resulting from loss of dopamine from the nigrostriatal tracts in the brain, and is characterized by rigidity, bradykinesia,
Anticholinergics. COMT* Inhibitors. Dopaminergic Agents. Dopamine Agonists. Combination Product
 Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review:
Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Class Update: Parkinson s Drugs Month/Year of Review:
Date of Referral: Enhanced Primary Care Pathway: Parkinson s Disease
 Specialist LINK Linking Physicians CALGARY AND AREA Patient Name: Date of Birth: Calgary RHRN: PHN / ULI: Date of Referral: Referring MD: Fax: Today s Date: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS:
Specialist LINK Linking Physicians CALGARY AND AREA Patient Name: Date of Birth: Calgary RHRN: PHN / ULI: Date of Referral: Referring MD: Fax: Today s Date: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS:
Managing Challenging Behaviors
 Managing Challenging Behaviors Barbara J. Kocsis, MD Psychiatry Resident, HDSA Center of Excellence UC Davis School of Medicine In partnership with Drs. Lorin Scher, MD and Vicki Wheelock, MD 1 Our Goal
Managing Challenging Behaviors Barbara J. Kocsis, MD Psychiatry Resident, HDSA Center of Excellence UC Davis School of Medicine In partnership with Drs. Lorin Scher, MD and Vicki Wheelock, MD 1 Our Goal
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019
 WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
Faculty Information 2/15/2013
 Timothy Reilly, PharmD, BCPS, CGP, FASCP Clinical Assistant Professor Ernest Mario School of Pharmacy Rutgers, The State University of New Jersey tjreilly@pharmacy.rutgers.edu Faculty Information Presenter:
Timothy Reilly, PharmD, BCPS, CGP, FASCP Clinical Assistant Professor Ernest Mario School of Pharmacy Rutgers, The State University of New Jersey tjreilly@pharmacy.rutgers.edu Faculty Information Presenter:
Clinical Features and Treatment of Parkinson s Disease
 Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy"
 Parkinson's Disease First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy" Parkinson s disease (PD) is a neurological disorder characterized by a progressive
Parkinson's Disease First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy" Parkinson s disease (PD) is a neurological disorder characterized by a progressive
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
ZELAPAR (selegiline hydrochloride) orally disintegrating tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Movement Disorders. Eric Kraus, MD! Neurology!
 Movement Disorders Eric Kraus, MD! Neurology! Classify Bradykinesia! Tic! Myoclonus! Tremor! Dystonia! Athetosis! Chorea! Ballismus! Case 1 This 64 year-old female has had progression of a tremor over
Movement Disorders Eric Kraus, MD! Neurology! Classify Bradykinesia! Tic! Myoclonus! Tremor! Dystonia! Athetosis! Chorea! Ballismus! Case 1 This 64 year-old female has had progression of a tremor over
Parkinson s Disease and Treatment Options for the Younger Adult
 Parkinson s Disease and Treatment Options for the Younger Adult David E. Riley, M.D. Chair, Medical Education InMotion April 22, 2016 Case Presentation - 1 A 57-year-old woman had Tremor of her right hand
Parkinson s Disease and Treatment Options for the Younger Adult David E. Riley, M.D. Chair, Medical Education InMotion April 22, 2016 Case Presentation - 1 A 57-year-old woman had Tremor of her right hand
Depression & Anxiety. What can I do? What are other possible treatments? What is this? Why does this happen? KEY POINTS
 Depression & Anxiety One set of important protectors from depression is friends and family as much as you can, keep yourself active and engaged with others. Exercise, particularly while outside, may help.
Depression & Anxiety One set of important protectors from depression is friends and family as much as you can, keep yourself active and engaged with others. Exercise, particularly while outside, may help.
Parkinson s Disease and Treatment Options for the Younger Adult
 The Way CME Should Be Parkinson s Disease and Treatment Options for the Younger Adult David E. Riley, M.D. Chair, Medical Education InMotion April 22, 2016 Case Presentation - 1 A 57-year-old woman had
The Way CME Should Be Parkinson s Disease and Treatment Options for the Younger Adult David E. Riley, M.D. Chair, Medical Education InMotion April 22, 2016 Case Presentation - 1 A 57-year-old woman had
Elements for a public summary
 VI.2 VI.2.1 Elements for a public summary Overview of disease epidemiology Parkinson s disease affects individuals globally (WHO 2006). It is the most common serious movement disorder, including speech
VI.2 VI.2.1 Elements for a public summary Overview of disease epidemiology Parkinson s disease affects individuals globally (WHO 2006). It is the most common serious movement disorder, including speech
CE on SUNDAY Newark, NJ October 18, 2009
 CE on SUNDAY Newark, NJ October 18, 2009 Date: Sunday, October 18, 2009 Time: 10:30 AM 11:45 AM Location: Sheraton Newark Airport Hotel Title: Speaker(s): Treating Parkinson s Disease: A Pharmacist s Overview
CE on SUNDAY Newark, NJ October 18, 2009 Date: Sunday, October 18, 2009 Time: 10:30 AM 11:45 AM Location: Sheraton Newark Airport Hotel Title: Speaker(s): Treating Parkinson s Disease: A Pharmacist s Overview
Parkinson's Disease and how you can make a difference with medication
 Parkinson's Disease and how you can make a difference with medication Alyson Franks Parkinson's and Movement Disorder Nurse Specialist Royal Hallamshire Hospital No treatment all Complementary Therapy
Parkinson's Disease and how you can make a difference with medication Alyson Franks Parkinson's and Movement Disorder Nurse Specialist Royal Hallamshire Hospital No treatment all Complementary Therapy
Moving fast or moving slow: an overview of Movement Disorders
 Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Making Every Little Bit Count: Parkinson s Disease. SHP Neurobiology of Development and Disease
 Making Every Little Bit Count: Parkinson s Disease SHP Neurobiology of Development and Disease Parkinson s Disease Initially described symptomatically by Dr. James Parkinson in 1817 in An Essay on the
Making Every Little Bit Count: Parkinson s Disease SHP Neurobiology of Development and Disease Parkinson s Disease Initially described symptomatically by Dr. James Parkinson in 1817 in An Essay on the
Subthalamic Nucleus Deep Brain Stimulation (STN-DBS)
") Subthalamic Nucleus Deep Brain Stimulation (STN-DBS) A Neurosurgical Treatment for Parkinson s Disease Parkinson s Disease Parkinson s disease is a common neurodegenerative disorder that affects about
Subthalamic Nucleus Deep Brain Stimulation (STN-DBS) A Neurosurgical Treatment for Parkinson s Disease Parkinson s Disease Parkinson s disease is a common neurodegenerative disorder that affects about
Parkinson s Disease in 60 minutes. Dr. Claire Hinnell Movement Disorder Neurologist Director Movement Disorder Clinic JPOCSC
 Parkinson s Disease in 60 minutes Dr. Claire Hinnell Movement Disorder Neurologist Director Movement Disorder Clinic JPOCSC S Plan of attack S What causes Parkinson s disease brief S Symptoms/Diagnostic
Parkinson s Disease in 60 minutes Dr. Claire Hinnell Movement Disorder Neurologist Director Movement Disorder Clinic JPOCSC S Plan of attack S What causes Parkinson s disease brief S Symptoms/Diagnostic