The Most Widely Misunderstood Test of All
|
|
|
- Belinda Kelley
- 5 years ago
- Views:
Transcription


1 The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute
2
3
4 History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons with latent Mycobacterium tuberculosis infection to prevent active disease has been an essential component of TB control in the US. History of Treatment of Latent Tuberculosis Infection 1965: First recommended for use in the US for previously untreated TB, PPD converters, and all children <3 years with a positive tuberculin test 1967: Recommendations broadened to include all PPD + (>10 mm) and close contacts History of Treatment of Latent Tuberculosis Infection 1970: 2 deaths and 19 developed liver disease out of 2000 contacts exposed to an infectious case on Capitol Hill 1974: Development of guidelines regarding pretreatment screening and monitoring to minimize risk for hepatitis and exclusion of low-risk persons older than 35 as candidates for treatment
5 History of Treatment of Latent Tuberculosis Infection 1983: Guidelines further revised to recommend routine clinical and laboratory monitoring for persons older than 35 or with increased risk for hepatotoxicity 1998: 2 months of RIF + PZA recommended for HIV+, subsequently HIV- 2000: 9 months Isoniazid decreed better than 6 2RZ decreed equal to 9 Isoniazid 2001: 2RZ deemphasized due to liver toxicity in favor of 9 month Isoniazid 2004: 4R suggested as effective advantageous regimen U.S. Guidelines for FDA-Approved IGRAs Recent FDA Approvals Oct 2007 Quantiferon -TB Gold-In-Tube (QFT-GIT) July 2008 T-Spot.TB test (T-spot) Targeted Tuberculin Testing and Treatment of Latent TB Infection As the rate of active TB in the United States has decreased, identification and treatment of persons with latent infection who are at high risk for active TB have become essential components of the TB elimination strategy.
6 Change in Nomenclature To focus on groups at the highest risk for TB, the term targeted tuberculin testing is used to encourage directed program activities Treatment of latent TB infection (LTBI) rather than preventive therapy or chemoprophylaxis to promote greater understanding of the concept for both patients and providers resulting in better implementation of this TB control strategy Targeted Testing Targeted testing identifies persons at high risk for TB who would benefit by treatment of LTBI Screening of low-risk persons should be replaced by targeted testing Purpose of Targeted Testing Find persons with LTBI who would benefit from treatment Find persons with TB disease who would benefit from treatment Groups that are not high risk for TB should NOT be tested routinely
7 Incidence of Active TB in Persons with Selected Risk Factors Risk Factor TB cases/1,000 person-years Recent TB infection Infection <1 yr past 12.9 Infection 1-7 yr past 1.6 HIV Infection Injection Drug Use HIV seropositive 76.0 HIV seronegative or unknown 10.0 Silicosis 68 Radiographic findings consistent with prior TB Weight deviation from standard Underweight by > 15% Underweight by 10 14% Underweight within 5% of standard Groups at Risk / Risk Factors for Infection -1 Persons or groups with presumed recent MTB infection Close contacts to infectious TB Skin test or IGRA conversion within 2 years Immigrant from endemic countries (within 5 years of arrival) Children <5 years with + TST or + IGRA Groups at Risk / Risk Factors for Infection -2 Clinical conditions associated with progression to active TB HIV infection Prior, untreated TB, with fibrotic lesions on CXR Underweight, malnourished persons

8 Groups at Risk / Risk Factors for Infection -3 Other medical conditions Silicosis Diabetes mellitus Chronic renal failure/hemodialysis Solid organ transplantation (heart, kidney) Carcinoma of head/neck Gastrectomy/jejunoilial bypass Chest Radiograph Abnormalities often seen in apical or posterior segments of upper lobe or superior segments of lower lobe May have unusual appearance in HIV-positive persons Cannot confirm diagnosis of TB Has NO role in screening for LTBI or TB disease


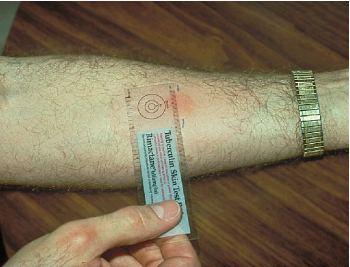
9 Administering the Tuberculin Skin Test Inject intradermally 0.1 ml of 5 TU PPD tuberculin Produce wheal 6mm to 10mm in diameter Do not recap, bend, or break needles, or remove needles from syringes Follow universal precautions for infection control



10 PHRENOLOGY The study of the mind and character from the shape of the skull Dorlands Illustrated Medical Dictionary 26th Edition 1985, Philadelphia: WG Saunders Reading the Tuberculin Skin Test Read reaction hours after injection Measure only induration Record reaction in millimeters

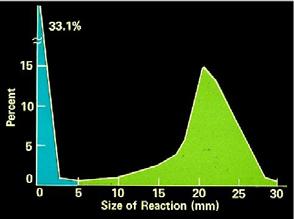
11 Determining a Cut Point Reichman


12 Determining a Cut Point - 2 Concentric-Circle Approach to Contact Tracing Home Environment Casual Close Leisure Environment Index Case Work/School Environment Adapted from Etkind S., Veen J., In Reichman-Hershfield: Tuberculosis: A Comprehensive International Approach, 2000 Criteria for TST Positivity by Risk Group - 1 Induration 5mm or more HIV+ Close contacts Chest radiograph consistent with prior untreated TB Patients with organ transplants and other immunosuppressed patients (i.e. prednisone 15 mg/d x 1 mo.)
13 Criteria for TST Positivity by Risk Group - 2 Induration 10 mm or greater Recent immigrants (within the past 5 years) from high prevalence countries Injection drug users Resident and employees of the high-risk congregate settings (prisons, nursing homes, hospitals, shelters, residential facilities for AIDS patients) Criteria for TST Positivity by Risk Group - 3 Induration 10 mm or greater Mycobacteriology lab personnel Persons with clinical conditions (silicosis, diabetes, chronic renal failure, malignancies and hematologic disorders, malnutrition) Children < 4yrs, infants, children, and adolescents exposed to adults at high risk Criteria for TST Positivity by Risk Group - 4 Positive skin test result 15 mm Persons with no known risk factors for TB may be considered Targeted skin testing programs should only be conducted among high risk groups
14 Occupation Exposure to TB Appropriate cutoff depends on Individual risk factors for TB Prevalence of TB in the facility Factors that May Cause False-Positive and False-Negative Reactions to the Tuberculin Skin Test Type of Reaction False-positive False-negative Possible Cause Nontuberculous mycobacteria BCG vaccination Anergy Recent TB infection Very young age: < 8 mos. old Live-virus vaccination Overwhelming TB disease Poor TST technique BCG Fantasy and Fact FANTASY BCG protects against getting TB infection BCG provides lifetime protection against developing active TB BCG causes the tuberculin skin test (TST) to be positive for life In a BCG-vaccinated person, a positive TST is most likely due to BCG A positive TST in a person of any age from any country is most likely due to BCG, not TB infection There is no need for a BCG-vaccinated person with a positive TST to be treated FACT BCG will not protect against becoming infected with TB BCG protects against severe complications of TB disease in young children, but provides little or no protection in adolescents and adults BCG causes the TST to be positive for a few years and then the TST reaction becomes much weaker. Generally, no reaction is present after 5 years. There is no way to tell whether a positive TST is due to BCG or to TB infection A positive TST in an adolescent or adult from a TB high-burden country is almost always due to TB infection, not BCG Persons with a positive TST from TB highburden countries are at high risk of developing active TB and should be treated
15 Boosting Some people with LTBI may have negative skin test reaction when tested years after infection Initial skin test may stimulate (boost) ability to react to tuberculin Positive reactions to subsequent tests may be misinterpreted as a new infection Two Step Testing Use two step testing for initial skin testing of adults who will be retested periodically If first test positive, consider the person infected If first test negative, give second test 1-3 weeks later If second test positive, consider person infected If second test negative, consider person uninfected Tuberculin Testing True Infection vs Booster Effect (mm induration) Time 0 1 week 1 year Situation A B C
16 Anergy Testing I am constantly astounded by the faith that clinicians have in this procedure Under the best of circumstances these tests are worthless, and under the worst of circumstances they re delusional. RE Chaisson, Clinical Infectious Diseases, 1996; 22:668 The Folly of Anergy Testing 60 % Anergic Patients Becoming Non-Anergic > 599 Baseline CD4+ Cell Count (cells/μl) Chin, et al, AJRCCM,1996;153: Interferon Gamma Release Assays Quantiferon -TB GOLD TB Spot TB Approved by FDA Uses antigens not found in BCG or MAC (ESAT-6 CFP-10) More specific, no cross reactors CDC Guidelines, 2005: Use in place of TST for all indications
17 Comparison of IGRAs and TST IGRAs In vitro test Specific antigens No boosting 1 patient visit Minimal inter-reader variability Results possible in 1 day Requires phlebotomy TST In vivo test Single antigen Boosting 2 patient visits Inter-reader variability Results in 2-3 days TB Infection Prevalence By Test and Clinic Type, San Francisco TST ( ) 2003) QFT-1 (11/03-2/05) QFT-G (3/05-11/08) QFT-IT (4/08-11/08) Homeless TB Clinic Methadone Immigrant 26% ~50% 10% 37% 17 % n= % n= % n= % n= % n= % n= % n=346 4 % n= % n= % n= Decline in positive rate from TST 73% >54% 60% 62% Updated 12/09/08 Courtesy, Masae Kawamura QFT Gold for Predicting Active Tuberculosis 601 contacts to active TB screened with TST and QFT Gold 40% (243) + TST all offered treatment for } LTBI, many declined 11% (66) + QFT Gold All patients followed for 2 years 6 people developed TB disease all QFT+ who had declined treatment QFT predictive value of developing TB disease 15% TST predictive value of developing TB disease 2.3% - Diel R et al, Am J Respir Crit Care Med, 2008
18 Boosting of IGRAs after TST Antigen specific response in IGRA+ & IGRA - subjects are influenced by result of TST Boosting evident by day 7 but not day 3 3 days is safe window to perform IGRA after TST - Van Zyl-Smit et al, AJRCCM, 2009, 180 Provisional Recommendations - 1 TST or IGRAs (QFT-G; QFT-GIT; T-Spot) used as aids to diagnose infection with M. tuberculosis IGRAs should be performed and interpreted according to established protocols using FDA approved test formats, in compliance with Clinical Laboratory Improvement Amendment (CLIA) standards Both standard qualitative interpretation and quantitative assay measurements should be reported Arrangement for IGRA testing should be made prior to blood collection to assure that blood is collected in proper tubes and testing performed within the required timeframe on viable blood cells As with the TST, IGRAs should not be used for testing persons with low risk of infection and low risk of disease due to M. tuberculosis (noted exception for those likely to be at increased risk in the future) - CDC, 2009 Provisional Recommendations - 2 Selection of the most suitable test or combination of tests for detection of M. tuberculosis infection based on rationale and context for testing, test availability, and overall cost effectiveness of testing IGRAs may be used in place of (not in addition to) TST in all situations in which CDC recommends tuberculin skin testing as an aid to diagnose M. tuberculosis infection with noted preferences and special considerations - CDC, 2009
19 Provisional Recommendations - 3 IGRA is preferred for testing persons from groups that historically have poor rates of return for TST reading IGRA is preferred for testing persons who have received BCG (as a vaccine or for cancer therapy) TST is preferred for testing children younger than 5 years of age - CDC, 2009 Provisional Recommendations - 4 IGRAs may be used in place of TST (without preference) to test recent contacts of persons with infectious tuberculosis with special considerations for follow-up testing Negative results prior to 8 wks typically should be confirmed by repeating the test 8 10 weeks after the end of exposure Repeating same test minimizes misclassification due to test discordance IGRAs may be used in place of TST (without preference) for periodic screening to address occupational exposure to TB with special considerations regarding conversions and reversions - CDC, 2009 Provisional Recommendations - 5 Both TST & IGRA may be useful if the initial test is negative and: risk of infection, risk of progression, and risk of poor outcomes are high (e.g., persons with HIV infection, children < 5 years exposed to persons with infectious TB) clinical suspicion for active tuberculosis (persons with symptoms, signs, and/or radiographic evidence suggestive of active tuberculosis) and confirmation of M. tuberculosis infection is desired - CDC, 2009
20 Provisional Recommendations - 6 Both TST & IGRA may be useful if the initial test is positive and: additional evidence of infection is required to encourage compliance (such as in foreign-born healthcare workers who believe their positive TST is due to BCG) healthy persons who have a low risk of both infection and progression Repeating an IGRA or performing a TST may be useful when the initial IGRA result is indeterminate, borderline, or invalid, and reason for testing persists Each institution and TB control program should evaluate availability, overall cost effectiveness, and benefits of IGRAs in their setting - CDC, 2009 Provisional Recommendations - 7 Diagnosis of M. tuberculosis infection, and decisions about medical or public health management should include epidemiological, historical, and other clinical information when using IGRA or TST results Persons with a positive TST or IGRA result should be evaluated for likelihood of M. tuberculosis infection, for risks of disease progression if infected, and for symptoms and signs of tuberculosis disease With these risks, symptoms, or signs, additional evaluation is indicated and should include a chest radiograph and possibly testing of sputum or other clinical samples for the presence of M. tuberculosis Diagnosis of LTBI requires that tuberculosis disease be excluded by medical evaluation - CDC, 2009 Provisional Recommendations - 8 Persons with symptoms, signs, or radiographic evidence of TB disease, and in those at high risk of disease progression if infected, a positive result with either an IGRA or TST may be taken as evidence of M. tuberculosis infection However, negative IGRA or TST results are not sufficient to exclude infection in these persons Healthy persons with low likelihood both of M. tuberculosis infection and of progression to TB disease if infected, a single positive IGRA or TST result should not be taken as reliable evidence of M. tuberculosis infection Reevaluation to confirm lack of risk and consider repeat testing on a caseby-case basis; or alternatively, assume, without additional testing, that the initial result is falsely positive - CDC, 2009
21 Provisional Recommendations - 9 Persons with discordant test results (one positive and the other negative) decisions about medical or public health management requires individualized judgment to assess quality of each test & magnitude of each result, probability of infection, risk of disease if infected, and risk of a poor outcome if disease occurs - CDC, 2009 Provisional Recommendations - 10 Further studies should focus on determining the value and limitations of IGRAs in situations critical to TB control Are IGRAs better at predicting subsequent tuberculosis disease than TST? Do IGRAs perform differently in children as compared to adults? Why do simultaneously performed TST, QFT-GIT, QFT-G, and T- Spot results differ? - CDC, 2009 IGRAs are best utilized in: General Advice Non-adherent populations (results with one visit) BCG vaccinated populations (higher TB specificity) Confirming positive TST results in individuals without risk for TB Confirming questionable TST results Other reasons: immediate hypersensitivity to PPD, convincing high risk patient with strongly positive TST to take LTBI treatment
22 IGRA Summary IGRAs are a significant advance because of its high specificity and operational advantages to the TST Like the TST, it is not a perfect test. Cases will be missed if relying exclusively on an IGRA result IGRAs are powerful epidemiologic and clinical tools Provider and patient misconceptions need to be met with widespread education and access to consultation Training, Q/A and maintaining IGRA proficiency of laboratory are feasible, achievable, and preferable over maintaining TST proficiency of thousands of clinic personnel Is there still a role for the tuberculin skin test in this era of new science and new technological breakthroughs? Perhaps just as there is still a role for the horse in our era of the modern car. Like horses, the tuberculin skin test has a long relationship with mankind. We feel comfortable with it. But also like horses, it is slower, less focused, its actions are often unpredictable, and occasionally it can leave a mess at the end but it is less expensive. - John Sbarbaro: Second Global Symposium on Interferon Gamma Assays, Dubrovnik, 2009 In reality, the tuberculin test will always remain subject to variation in all of its phases: the test material, the individual response, and the application and reader interpretation. The tuberculin test can only serve as a diagnostic aide. - John Sbarbaro: Second Global Symposium on Interferon Gamma Assays, Dubrovnik, 2009
23 All testing activities should be accompanied by a plan for follow-up care LTBI Treatment for TST (+) Contacts 120 Recommended Started Completed All TST+ Substance Abusers HIV+ Children <6 Foreign Born n = 1725 n = 58 n = 11 n = 132 n = 721 Marks, Taylor, Qualls, et al: Outcomes of TB Contact Investigations, AJRCCM, Dec Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection - 1 Isoniazid for 6-12 months has been the mainstay of treatment for LTBI in the United States for more than 30 years The application of isoniazid for LTBI has been limited because of poor adherence due to the relatively long duration of treatment required and because of concerns about toxicity There has been interest in the development of shorter, rifampin-based regimens as alternative to isoniazid for the treatment of LTBI
24 Contacts to Smear Positive TB Cases Contact count Contacts per case Contacts evaluated for TB Contacts with TB disease Contacts with LTBI Started treatment for LTBI Completed treatment for LTBI 73, % 1% 26% 73% 59% Objectives 95% 85% -K. Castro Dear Colleague letter, April 6, 2006 Treatment of Latent TB Infection 2 The isoniazid daily regimen for 9 months is recommended because prospective, randomized trials in HIV-negative persons indicate that 12 months of treatment is more effective than 6 months. However in subgroup analysis of several trials the maximal beneficial effect of isoniazid is likely achieved by 9 months, and minimal additional benefit is gained by extending therapy to 12 months Both the 9-month and 6-month isoniazid regimens may be given intermittently (only as directly observed therapy - DOT) Treatment of Latent TB Infection 3 Rifampin given daily for 4 months is recommended on the basis of the efficacy of a similar regimen in a prospective randomized trial of tuberculin-positive persons with silicosis and a non-randomized trial in persons exposed to persons with isoniazid-resistant TB In situations where rifampin cannot be used (e.g., HIVinfected persons receiving protease inhibitors), rifabutin may be substituted Before beginning treatment of LTBI, active TB must be ruled out by history, physical examination, chest radiography, and, when indicated, bacteriologic studies
25 Rifampin in Treatment of Latent Tuberculosis Infection 1 We argue that 4R is an effective, relatively nontoxic, affordable strategy that clinicians and program managers should consider for more widespread use in selected populations and settings to effectively and efficiently treat LTBI, thereby accelerating the decline of TB in their communities. AJRCCM 170; , 2004 Rifampin in Treatment of Latent Tuberculosis Infection 2 Study in County Chest Clinic 474 Patients 2000 Predominately 9 months Isoniazid (9H) 2003 Predominately 4 months Rifampin (4R) Treatment completion 9H 53% 4R 80.5% } P < Treatment completion predicted by regimen (OR 5.1; 95% CI 3.3, 8.1) -Lardizabal, A. CHEST, Vol.130, p , Dec Rifampin in Treatment of Latent Tuberculosis Infection 3 Comparison of Regimen Features: 9H and 4R Regimen Feature 9H 4R High efficacy X * Lower hepatotoxicity X Lower overall cost X Higher adherence X More effective against INH-resistant strains X (e.g., among foreign-born persons) Shorter duration X Fewer drug-drug interactions X * Good evidence that 3R is at least as efficacious as 6H. Inferential reasoning from other evidence suggests that efficacy of 4R may approach that of 9H. AJRCCM 170; , 2004


26 INFORMATION LINE TB DOCS ( )
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Latent TB Infection (LTBI)
") Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
The Role of Rifampin for the Treatment of Latent TB Infection. Introduction. Introduction
 The Role of Rifampin for the Treatment of Latent TB Infection March 26, 2008 Alfred A. Lardizabal, MD Associate Professor of Medicine New Jersey Medical School Global Tuberculosis institute Treatment of
The Role of Rifampin for the Treatment of Latent TB Infection March 26, 2008 Alfred A. Lardizabal, MD Associate Professor of Medicine New Jersey Medical School Global Tuberculosis institute Treatment of
Peggy Leslie-Smith, RN
 Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Advanced Concepts in Pediatric Tuberculosis
 Advanced Concepts in Pediatric Tuberculosis: Nizar F. Maraqa, MD, FPIDS Division of Pediatric Infectious Diseases & Immunology University of Florida College of Medicine - Jacksonville Advanced Concepts
Advanced Concepts in Pediatric Tuberculosis: Nizar F. Maraqa, MD, FPIDS Division of Pediatric Infectious Diseases & Immunology University of Florida College of Medicine - Jacksonville Advanced Concepts
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Diagnosis and Medical Case Management of Latent TB. Bryan Rock, MD April 27, 2010
 TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis and Medical Case Management of Latent TB Infection Bryan Rock, MD April 27, 2010 DIAGNOSIS AND MANAGEMENT OF LATENT TUBERCULOSIS
TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis and Medical Case Management of Latent TB Infection Bryan Rock, MD April 27, 2010 DIAGNOSIS AND MANAGEMENT OF LATENT TUBERCULOSIS
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
Therapy for Latent Tuberculosis Infection
 Screening and Treatment of LTBI in TB Control in the US Margarita Elsa Villarino MD MPH Division of TB Elimination, CDC April 14, 2004 TB Prevention and Control in the United States The fundamental strategies
Screening and Treatment of LTBI in TB Control in the US Margarita Elsa Villarino MD MPH Division of TB Elimination, CDC April 14, 2004 TB Prevention and Control in the United States The fundamental strategies
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Tuberculosis: Where Are We Now?
 Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Community pharmacy-based tuberculosis skin testing
 Community pharmacy-based tuberculosis skin testing Shanna K. O Connor, PharmD ISU KDHS Spring CE Seminar 2018 In support of improving patient care, Idaho State University Kasiska Division of Health Sciences
Community pharmacy-based tuberculosis skin testing Shanna K. O Connor, PharmD ISU KDHS Spring CE Seminar 2018 In support of improving patient care, Idaho State University Kasiska Division of Health Sciences
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Screening for Tuberculosis Infection. Harlingen, TX. Linda Dooley, MD has the following disclosures to make:
 TB Infection Diagnosis Recommendations Talk Developed by Lisa Y. Armitige, MD, PhD Medical Consultant, Heartland National TB Center Associate Professor Internal Medicine/Pediatrics/Infectious Disease UT
TB Infection Diagnosis Recommendations Talk Developed by Lisa Y. Armitige, MD, PhD Medical Consultant, Heartland National TB Center Associate Professor Internal Medicine/Pediatrics/Infectious Disease UT
TB Intensive Tyler, Texas December 2-4, 2008
 TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
LTBI: Who to Test & When to Treat
 LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI)
") Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014
 TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011 Douglas Hornick, MD has the following disclosures to
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of Latent TB Infection Douglas Hornick, MD September 27, 2011 Douglas Hornick, MD has the following disclosures to
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Using Interferon Gamma Release Assays for Diagnosis of TB Infection
 Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents
 New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
Advanced Concepts in Pediatric TB: Latent TB Infection
 Welcome to the second of eight sessions on Advanced Concepts in Pediatric TB, sponsored by the Southeastern National Tuberculosis Center. Today we present the in Pediatric TB. Today s presenter is Dr.
Welcome to the second of eight sessions on Advanced Concepts in Pediatric TB, sponsored by the Southeastern National Tuberculosis Center. Today we present the in Pediatric TB. Today s presenter is Dr.
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
American Thoracic Society
 Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection THIS OFFICIAL STATEMENT OF THE AMERICAN THORACIC SOCIETY WAS ADOPTED BY THE ATS BOARD OF DIRECTORS, JULY 1999. THIS IS A JOINT
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection THIS OFFICIAL STATEMENT OF THE AMERICAN THORACIC SOCIETY WAS ADOPTED BY THE ATS BOARD OF DIRECTORS, JULY 1999. THIS IS A JOINT
Tuberculin Skin Testing
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 Testing to TB Infection Using the TST Presented by Debra Howenstine, MD for Debbie Onofre, RN October 5, 2010 Tuberculin
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 Testing to TB Infection Using the TST Presented by Debra Howenstine, MD for Debbie Onofre, RN October 5, 2010 Tuberculin
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines
 Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
2016 OPAM Mid-Year Educational Conference, Sponsored by AOCOPM Sunday, March 13, 2016
 Learning Objectives Tuberculosis Case Discussions: Evaluation for Tuberculosis Infection Melissa C. Overman, DO, MPH, CHES, FAOCOPM Describe appropriate technique for TST placement, reading and interpretation
Learning Objectives Tuberculosis Case Discussions: Evaluation for Tuberculosis Infection Melissa C. Overman, DO, MPH, CHES, FAOCOPM Describe appropriate technique for TST placement, reading and interpretation
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Table 9. Policy for Tuberculosis Surveillance and Screening
 Policy for Tuberculosis Surveillance and Screening Purpose: to identify active cases of tuberculosis or latent TB among residents and staff of the nursing home in order to prevent transmission in this
Policy for Tuberculosis Surveillance and Screening Purpose: to identify active cases of tuberculosis or latent TB among residents and staff of the nursing home in order to prevent transmission in this
Interpretation of TST & IGRA results. Objectives
 Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Tuberculosis Education for the Medical Professional
 Tuberculosis Education for the Medical Professional North Dakota Diagnosis and Medical Management of Latent TB Infection Dawn Farrell, RN, BSN, PHN Maria Robles, BSN July 10, 2007 Tuberculosis Education
Tuberculosis Education for the Medical Professional North Dakota Diagnosis and Medical Management of Latent TB Infection Dawn Farrell, RN, BSN, PHN Maria Robles, BSN July 10, 2007 Tuberculosis Education
Detecting latent tuberculosis using interferon gamma release assays (IGRA)
") Detecting latent tuberculosis using interferon gamma release assays (IGRA) American Society for Microbiology June 2017 Edward Desmond, Ph.D., D (ABMM) San Lorenzo, CA Edward Desmond has no financial connections
Detecting latent tuberculosis using interferon gamma release assays (IGRA) American Society for Microbiology June 2017 Edward Desmond, Ph.D., D (ABMM) San Lorenzo, CA Edward Desmond has no financial connections
11/1/2017. Disclosures. Update In Tuberculosis, Indiana Outline/Objectives. Pathogenesis of M.tb Global/U.S. TB Burden, 2016
 Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
Core Curriculum on Tuberculosis: What the Clinician Should Know
 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Conflict of Interest Disclosures:
 Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Tuberculosis. WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED
 Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
Tuberculosis WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments COL Paul Keiser LTC James E. Moon LTC Jaime Mancuso LTC Anjali Kunz MAJ Kristopher Paolino MAJ Leyi
Why need to havetb Clearance. To Control and Prevent Tuberculosis
 Why need to havetb Clearance To Control and Prevent Tuberculosis How to ID Tuberculosis There are two kinds of tests that are used to determine if a person has been infected with TB bacteria: the tuberculin
Why need to havetb Clearance To Control and Prevent Tuberculosis How to ID Tuberculosis There are two kinds of tests that are used to determine if a person has been infected with TB bacteria: the tuberculin
Technical Bulletin No. 172
 CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
LATENT TUBERCULOSIS SCREENING AND TREATMENT:
 LATENT TUBERCULOSIS SCREENING AND TREATMENT: TB or not TB Christopher Kwong, MD and William Rifkin, MD Week 14 Educational Objectives: 1. Understand who should be screened for latent TB infection and why
LATENT TUBERCULOSIS SCREENING AND TREATMENT: TB or not TB Christopher Kwong, MD and William Rifkin, MD Week 14 Educational Objectives: 1. Understand who should be screened for latent TB infection and why
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis Infection in the US Military
 Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
Tuberculosis Infection in the US Military Edward Munch. The Sick Child. (1885) Anjali Kunz, MAJ (P), MC Pediatric Infectious Disease, Chief, JBLM Courtesy of : Paul B. Keiser, Feb 2014 Walter Reed Army
The Challenges and Pitfalls in Diagnosing or Misdiagnosing Tuberculosis: Are the Days of TB Skin Tests Over?
 The Challenges and Pitfalls in Diagnosing or Misdiagnosing Tuberculosis: Are the Days of TB Skin Tests Over? ROY F. CHEMALY, MD, MPH, FIDSA, FACP PROFESSOR OF MEDICINE DIRECTOR, INFECTION CONTROL SECTION
The Challenges and Pitfalls in Diagnosing or Misdiagnosing Tuberculosis: Are the Days of TB Skin Tests Over? ROY F. CHEMALY, MD, MPH, FIDSA, FACP PROFESSOR OF MEDICINE DIRECTOR, INFECTION CONTROL SECTION
INDEX CASE INFORMATION
 Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
PEDIA MANOR POLICY AND PROCEDURE MANUAL
 REVISED: REVIEWED: PAGE: 1 of 5 POLICY: A tuberculin skin test (TST) will be performed using the tuberculin PPD by intradermal injection. The PPD will be administered per the Centers for Disease Control
REVISED: REVIEWED: PAGE: 1 of 5 POLICY: A tuberculin skin test (TST) will be performed using the tuberculin PPD by intradermal injection. The PPD will be administered per the Centers for Disease Control
ATS/CDC Guidelines for Treating Latent TB Infection
 TB Intensive Tyler, Texas June 2-4, 2010 ATS/CDC Guidelines for Treating Latent TB Infection Timothy R. Aksamit, MD June 2, 2010 ATS/CDC Guidelines for Treating LTBI Tuberculosis Intensive University of
TB Intensive Tyler, Texas June 2-4, 2010 ATS/CDC Guidelines for Treating Latent TB Infection Timothy R. Aksamit, MD June 2, 2010 ATS/CDC Guidelines for Treating LTBI Tuberculosis Intensive University of
Tuberculosis Screening and Targeted Testing of College and University Students: Developing a Best Practice Approach:
 Tuberculosis Screening and Targeted Testing of College and University Students: Developing a Best Practice Approach: Lori A. Soos MA, BSN, RN, Niagara University Deborah Penoyer, MS, RN, SUNY Geneseo Learning
Tuberculosis Screening and Targeted Testing of College and University Students: Developing a Best Practice Approach: Lori A. Soos MA, BSN, RN, Niagara University Deborah Penoyer, MS, RN, SUNY Geneseo Learning
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
Michael J. Huey, MD. NYSCHA Annual Meeting WE-2, October 19, 2016
 Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine Emory University School of Medicine President-elect
Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine Emory University School of Medicine President-elect
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lynn Horvath, MD November 11, 2014 Lynn Horvath, MD has the following disclosures to
TB Intensive San Antonio, Texas November 11 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lynn Horvath, MD November 11, 2014 Lynn Horvath, MD has the following disclosures to
These recommendations will remain in effect until the national shortage of PPD solution has abated.
 Maryland Recommendations Regarding the National Shortage of Purified Protein Derivative (PPD) Solution; Attachment to Health Officer Memorandum National Shortages of Tubersol and Aplisol for TB Skin Testing;
Maryland Recommendations Regarding the National Shortage of Purified Protein Derivative (PPD) Solution; Attachment to Health Officer Memorandum National Shortages of Tubersol and Aplisol for TB Skin Testing;
TB Screening and Diagnosis
 TB Screening and Diagnosis Douglas B. Hornick, MD Pulmonologist w/ Infectious Attitude Division of Pulm/Crit Care/Occ Med UI Carver College of Medicine Disclosures: None Objectives Rural (US) TB epidemiology
TB Screening and Diagnosis Douglas B. Hornick, MD Pulmonologist w/ Infectious Attitude Division of Pulm/Crit Care/Occ Med UI Carver College of Medicine Disclosures: None Objectives Rural (US) TB epidemiology
Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges
 Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges David Karol, MD, MA Bureau of Prisons, FMC Butner Duke University Medical Center June 26, 2013 No Disclosures
Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges David Karol, MD, MA Bureau of Prisons, FMC Butner Duke University Medical Center June 26, 2013 No Disclosures
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA)
 and Interferon-gamma Release Assays (IGRA)") Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2019 Bob Belknap M.D. Director, Denver Metro TB Program Disclosures No relevant financial relationships Objectives Be able to
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2019 Bob Belknap M.D. Director, Denver Metro TB Program Disclosures No relevant financial relationships Objectives Be able to
Nguyen Van Hung (NTP, Viet Nam)
") Technical Consultation Meeting on the Programmatic Management of Latent Tuberculosis Infection 31 August-1 September 2017, Seoul, Republic Korea Adopting new LTBI diagnostics at country level: perspective
Technical Consultation Meeting on the Programmatic Management of Latent Tuberculosis Infection 31 August-1 September 2017, Seoul, Republic Korea Adopting new LTBI diagnostics at country level: perspective
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
Thorax Online First, published on December 8, 2009 as /thx
 Thorax Online First, published on December 8, 2009 as 10.1136/thx.2009.119677 Title Page Cost effectiveness of the NICE guidelines for screening for latent tuberculosis infection: the Quantiferon-TB gold
Thorax Online First, published on December 8, 2009 as 10.1136/thx.2009.119677 Title Page Cost effectiveness of the NICE guidelines for screening for latent tuberculosis infection: the Quantiferon-TB gold
Revised Technical Instructions for Civil Surgeons. October 9, 2018
 Revised Technical Instructions for Civil Surgeons October 9, 2018 Speakers Joanna Regan Centers for Disease Control and Prevention Shereen Katrak California Department of Public Health Pennan Barry California
Revised Technical Instructions for Civil Surgeons October 9, 2018 Speakers Joanna Regan Centers for Disease Control and Prevention Shereen Katrak California Department of Public Health Pennan Barry California
FLORIDA DEPARTMENT OF JUVENILE JUSTICE DETENTION SERVICES FACILITY MEDICAL POLICIES
 FLORIDA DEPARTMENT OF JUVENILE JUSTICE DETENTION SERVICES FACILITY MEDICAL POLICIES Superintendent Signature Designated Health Authority Signature Effective Date: November 1, 2016 Subject: TUBERCULOSIS
FLORIDA DEPARTMENT OF JUVENILE JUSTICE DETENTION SERVICES FACILITY MEDICAL POLICIES Superintendent Signature Designated Health Authority Signature Effective Date: November 1, 2016 Subject: TUBERCULOSIS
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any