Utility of PPD or IGRA to answer the age old question of "TB or not TB
|
|
|
- William Reeves
- 5 years ago
- Views:
Transcription
1 Utility of PPD or IGRA to answer the age old question of "TB or not TB Thomas S. Alexander, Ph.D., D(ABMLI) Immunologist Summa Health
2 Yes, The reservation is in the name of Dr. Alexander. May I ask, is that an actual medical degree, or merely a Ph.D.? Adapted from The New Yorker, 1987
3 Acknowledgements and Disclosure I thank Qiagen for providing some of the slides and references I thank Dr. Anthony Catanzaro for helpful discussions in preparing the talk No conflicts to disclose
4 Talk Outline Quick TB review TB Skin Test (TST) Problems with the TST Difficulties in developing in vitro TB assays Development of IGRAs Quantiferon iterations Performance of Quantiferon Plus T-Spot Assay Performance of T-Spot Some recent literature Use of IGRAs prior to starting anti TNF agents Current Recommendations
 Other organs - Extra-pulmonary TB Infection may be: Active (with symptoms, highly contagious) Latent")
5 What Is Tuberculosis? Tuberculosis (TB) overview Infectious communicable disease Caused by Mycobacterium tuberculosis complex organisms M. tuberculosis M. bovis M. africanum M. canetti M. microti Affects different parts of the body: Lungs - Pulmonary TB (> 70% of all TB cases) Other organs - Extra-pulmonary TB Infection may be: Active (with symptoms, highly contagious) Latent (asymptomatic, not contagious) Photo courtesy of WHO Stop TB initiative. Website: FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 5

6 What Is Tuberculosis? Outcomes of transmission of TB infection No infection Majority of these people eradicate the infection and never develop active disease Some of these people become ill from TB within weeks to months and develop Active TB Individual with infectious tuberculosis TB Infection Some of these people remain asymptomatically infected for years with Latent TB infection Outcome depends partially on the person s immune status FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 6
7 What Is Tuberculosis? From latent to active TB People with LTBI have a lifetime risk of developing TB of 10% 1 The greatest risk occurs within the first 2 years after infection Some groups of people are at even higher risk of TB: Risk group TB risk, times HIV/AIDS TNF-α therapy Diabetes Healthcare workers Corticosteroid therapy > 5 4 LTBI treatment can prevent later development of TB 1 World Health Organization 2 Winthrop KL et al. Arthritis Rheum 2005, Gardam MA et al. Lancet infect Dis Baussano I et al. Emerg Infect Dis Cisneros JR at al. Ann Pharmacother 1996 FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 7
8 No. of Cases Cases per 100,000 Population Reported Tuberculosis (TB) Cases and Rates United States, ,000 25,000 20,000 15,000 10,000 5, Year No. of Cases Incidence Rate
9 TB Case Rates,* United States, 2017 NY C DC *Cases per 100,000 DC, District of Columbia; NYC, New York City (excluded from New York state) 2.8 (2017 national average) >2.8
10 Cases per 100,000 Population TB Cases and Rates Among U.S.-Born versus Non-U.S. Born Persons, United States, No. of cases 30,000 25,000 20,000 15,000 U.S.-born Cases Non-U.S. born Cases U.S.-born Rate Non-U.S. born Rate ,000 5, Year
11 Coinfection (%) Estimated HIV Coinfection Among Persons Reported with TB, United States, * All ages Ages yrs Year * Minimum estimates are based on reported HIV-positive status among all TB patients in the age group.
12 Diagnosis And Treatment: LTBI Current practices There is no gold standard to determine if a person has LTBI Currently there are two classes of diagnostic test for LTBI: Interferon-gamma release assays (IGRAs) Tuberculin skin test No test can discriminate between old and new infection LTBI testing is usually only performed on those: At increased risk of being infected: - Healthcare workers, contacts of active TB cases, etc. At risk of developing active TB: Immunosuppressed Enrolled in schools FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 12
13 Diagnosis And Treatment: LTBI Tuberculin Skin Test (TST) The TST (also known as the Mantoux or a PPD test ) was originally developed as a diagnostic test for active TB Many people without active TB were positive to the test and significant proportion of these later developed active TB Led to the term latent TB infection (LTBI) to describe people who presumably were infected, but had no symptoms LTBI was (crudely) defined on the basis of a positive TST However, the TST employs tuberculin PPD, a poorly defined, complex mixture of antigens which is non-specific for TB since many of its proteins are found in different mycobacterial species This is just one of the many limitations of the TST FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 13
 response to M.")
 Erythema (redness) Requires two visits: to have the test administered")
14 Diagnosis And Treatment: LTBI Tuberculin Skin Test (TST) First used in 1906 as a diagnostic for TB Measures a person s cell mediated immune (CMI) response to M. tuberculosis Tuberculin Purified Protein Derivative (PPD) is injected intra-dermally into the forearm and hours later the size of the resultant reaction is measured: Induration (firm area) Erythema (redness) Requires two visits: to have the test administered and read FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 14
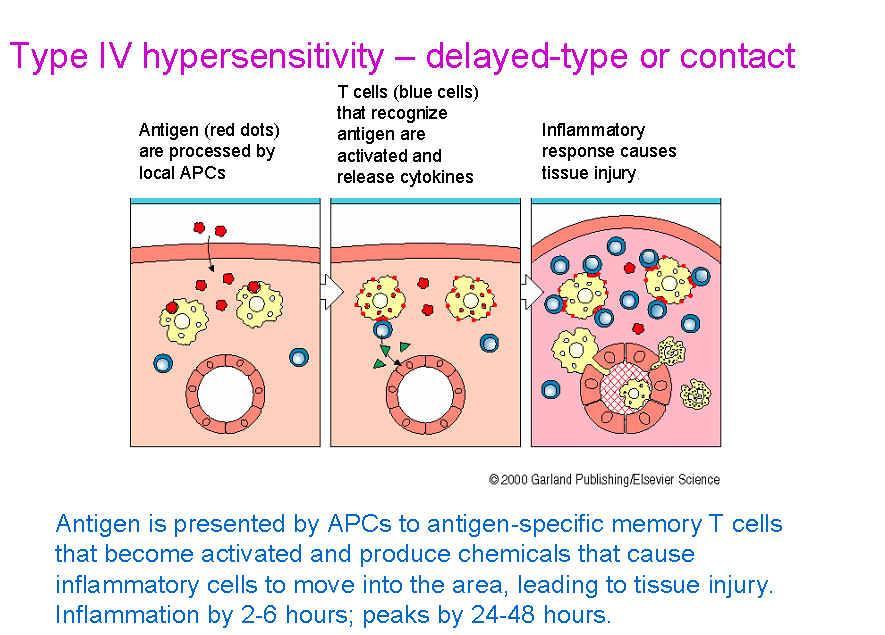
15 The TST detects a delayed type hypersensitivity reaction T cells, antigen presenting cells and cytokines are involved Reaction is localized at the site of antigen presence Redness (erythema) due to inflammation and induration (swelling) due to cellular influx will occur With respect to the TST, only induration is measured Inexperienced or poorly trained readers may measure erythema leading to false positive results

16 PPD Skin test
17

18 TST erythema and induration

19 Measure Induration Only
20 Interpretation of PPD High-risk patients (>5X5 mm= positive). Patients infected with HIV Those who have had close recent contact with a person who has active TB Those who have symptoms or a chest X-ray that shows TB. Patients taking immunosuppressive medications Moderate-risk patients. (>10 X 10 mm= positive) TB; People who have recently moved from or traveled in a country with a high rate of IV Drug users Nursing home residents and staff Hospital workers Those in schools, and prisons Children younger than 4 years old; Children (ages 4 to 18) who are exposed to high-risk adults Homeless people. Those who are 10% or more below their ideal body weight People with renal failure, diabetes, leukemia, cancer, or hose who have had part of their stomach removed (gastrectomy). Low-risk group >15 X 15 mm = positive) groups. people who do not have any likely exposure to TB or are listed in the other risk

21 1950s TB Testing in School One of my earliest memories!
22 Two Step PPD Algorithm
23 Diagnosis And Treatment: LTBI People without TB may be falsely positive due to many reasons, including: BCG vaccination MAC Exposure Immune reactivity to non-tuberculous mycobacteria (NTM) - In US-born individuals, up to 50% of TST responses can be due to NTM infections (1) People with TB may be falsely negative Difficulty in proper intradermal injection of PPD The need read the test 2-3 days after PPD injection People may not return for reading Subjective: Two different readers, two answers Different cut-offs for different situations ( 5mm, 10mm, 15mm) Boosting: as PPD antigen is injected into the person, this can lead to the boosting of a subsequent test and a false-positive result, especially in those BCG vaccinated. Limitations of the TST 1. von Reyn CF, Horsburgh CR, Olivier KN, et al. Skin test reactions to Mycobacterium tuberculosis purified protein derivative and Mycobacterium avium sensitin among health care workers and medical students in the United States. Int J Tuberc Lung Dis 2001; 5 (12): FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 23
24 SUMMARIZING THE PROBLEM TB is a highly contagious disease, with great morbidity and mortality and is difficult to eliminate from an infected individual. Identifying and treating individuals with current or latent TB infections is important from a public health standpoint. Toward this end, TB testing has long been required by schools and health care related work environments. TB testing has classically been performed by the tuberculin skin test (TST), an intradermal injection of protein (PPD), inducing a cell mediated immune (CMI) response in those previously or currently infected, or exposed to M. tuberculosis. The patient must return to have the test evaluated. Results are determined subjectively and reader inexperience may lead to errors in interpretation. PPD cross reacts with non TB mycobacteria. False positive and false negative results do occur.
25 Why Was There Not a Laboratory Test for TB for Many Years? Many in vitro clinical assay techniques exist for detecting organism specific antibody Anti M. tuberculosis antibody is not useful for diagnosis An in vitro assay measuring cell mediated immunity to M. tb would be useful In vitro CMI assays are difficult to develop due to MHC Restriction
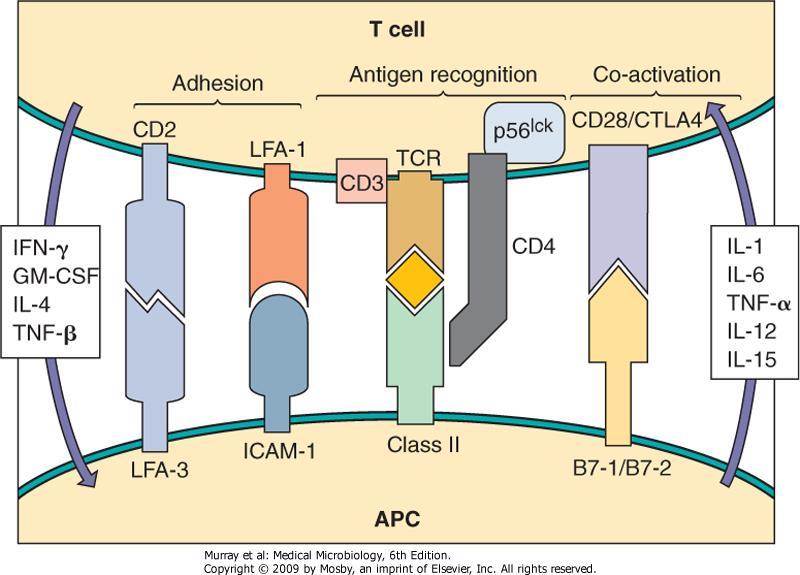
26 MHC Restriction? What the &%^^ is that? Antibodies react directly with their antigenic targets T cells recognize antigen only when a portion of the antigen is bound to a major histocompatability complex molecule (MHC or, in the human, HLA) T cells only recognize antigen bound to self MHC molecules on antigen presenting cells Thus, it is difficult to develop a single system to measure CMI in all patients.
27

28 Interferon Gamma Release

 Both IGRAs measure the secretion of the cytokine interferon-gamma (IFN-γ) by lymphocytes stimulated in vitro with")
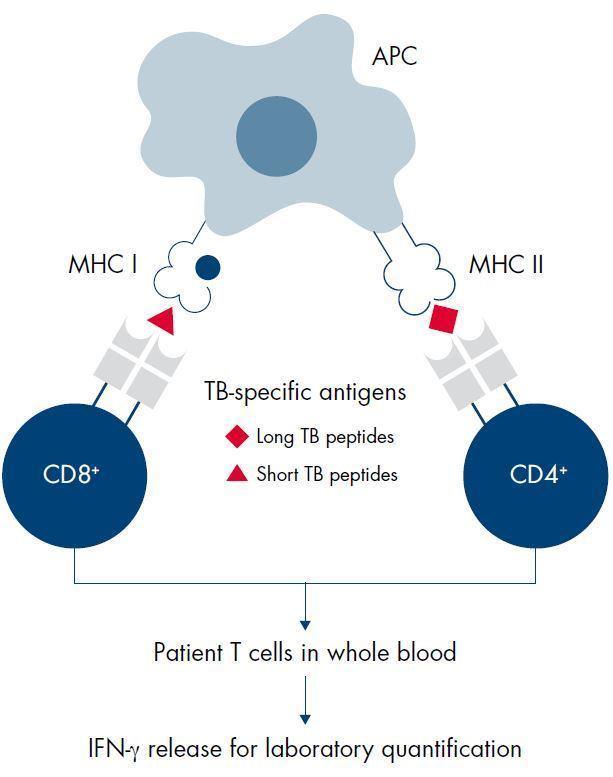
29 Diagnosis And Treatment: LTBI Interferon-gamma release assays (IGRAs) In response to the limitations of the TST, IGRAs have been developed and have become available over the last decade More specific and sensitive than TST for diagnosis of LTBI Two IGRAs commercially available: QuantiFERON -TB Gold (QFT ) in tube Plus and T-Spot.TB (Elispot-based IGRA) Both IGRAs measure the secretion of the cytokine interferon-gamma (IFN-γ) by lymphocytes stimulated in vitro with TB-specific antigens FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 29
30 Immunological Basis for IGRAs In normal circumstances, there is little Interferon Gamma (IFN- ) within the blood. T-cells activate and secrete IFN-γ. In the presence of the TB specific antigens, T cells of infected persons are stimulated to produce IFN- In the QFT and T-spot tests whole blood is exposed to TB specific antigens T cells of infected persons are activated and secrete IFN- Measurement of IFN- using an ELISA assay is the basis for the QFT test Measurement of IFN-gamma using an ELISPOT assay is the basis for the T-spot test FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 30v
31 IGRAs are not affected by BCG vaccination (1) Tuberculosis Complex QFT TB-Specific Antigens ESAT -6 TST Antigens CFP-10 TB 7.7 PPD Environmental strains QFT TB-Specific Antigens TST Antigens ESAT-6 CFP-10 TB 7.7 PPD M. tuberculosis M. africanum M. bovis BCG Sub- Substrain QFT TB-Specific Antigens ESAT -6 TST Antigens CFP-10 TB 7.7 PPD Gothenberg Moreau Tice Tokyo Danish Glaxo Montréal Pasteur M. abcessus M. avium M. branderi M. celatum M. chelonae M. fortuitum M. gordonii M. intracellulare M. kansasii M. malmoense M. marinum M. oenavense M. scrofulaceum M. smegmatis M. szulgai M. terra M. vaccae M. xenopi QuantiFERON-TB Gold Package Insert, July 2011 /2. Matulis G et al Ann Rhuem Dis 2008; 67(1): FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 31
 Contains TB antigens optimized to stimulate both CD4 and CD8 T cells Mitogen (purple cap) Positive control May indicate: Decreased patient")
32 QuantiFERON-TB Gold Plus Blood Collection Tubes Nil (grey cap) Negative control Adjusts for background noise or non-specific IFN- in blood samples TB1 Antigen (green cap) Contains TB antigens that primarily stimulate CD4 T cells TB2 Antigen (yellow cap) Contains TB antigens optimized to stimulate both CD4 and CD8 T cells Mitogen (purple cap) Positive control May indicate: Decreased patient immune status Incorrect blood handling & incubation Nil TB 1 TB 2 Mitogen 32
33
34 Data Sheet
35 Result Interpretation
36 Data Interpretation Guide Although TB-Nil values >0.35 are positive, values <1.0 may repeat negative Interpret all, but primarily low, values within clinical context Results are reported as positive, negative or Indeterminate Positive values are reported with the TB-Nil value Indeterminate values indicate low mitogen response and do not mean the patient has a borderline TB result Immune suppression Collection or processing error
37 Indeterminate
38 Are Shaking, Blood Volume and Incubation Times Limiting Factors? (Gaur, et al., JCM, 2013) Vigorous shaking increased nil and TB IFN levels in 33 uninfected individuals compared to gentle shaking TB values went from 0.12 (gentle) to 0.24 (vigorous), p= Nil values went from , p<0.001 Blood Volume did not show differences in uninfected controls but a lower blood volume (0.8 ml) had a lower number of false negative results compared to 1.0 (p=0.2) and 1.2 ml (p=0.05) draws Incubation times of 16, 20 and 24 hours did not affect results.
39 Bad Lot of Tubes Slater, JCM, 2012 (Stanford) Sudden Increase in Positivity from 10-31% Compared different lot numbers and found different rates Confirmed at ARUP (Couterier, et al., JCM, 2013) Summa Health Issues We had the bad lots and found increased positive and indeterminate rates Indeterminate rate is now a QA monitor (<6%)
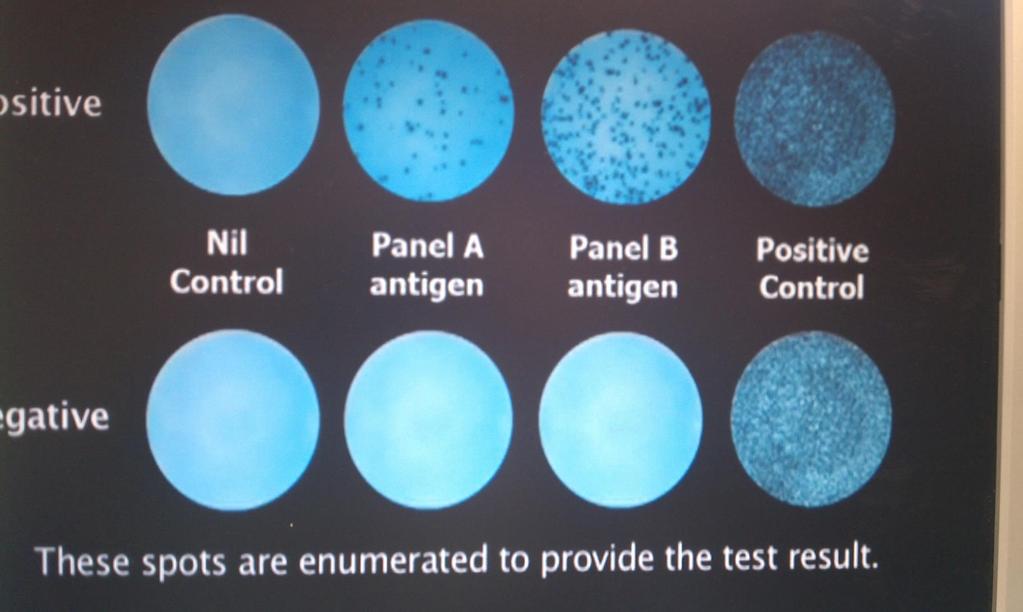
40 T-Spot IGRA Assay 1-2 Heparin Tubes required Simpler collection protocol than Quantiferon Separate mononuclear cells prior to incubating with TB antigens Allows standardization of antigen:cell concentration Postulated to increase sensitivity in immunosuppressed individuals Overnight incubation in plates followed by ELISA type stain for cells producing gamma interferon Cell colonies producing interferon are enumerated
41 T-Spot
42 T-Spot Result Interpretation Mitogen-Nil >8 spots- Valid Assay Mitogen-Nil <8 spots- Indeterminate Panel A and/or Panel B-Nil Spots <5- Negative 5-7- Borderline >8- Positive
43 Our T-Spot Experience Two small evaluations No difference between T-spot and Quantiferon in HIV positive patients More up front processing time, not conducive to automation or handling large volumes of specimens Subjective interpretation, although magnifier provided by the company was helpful
44 Current T-Spot Availability Few clinical laboratories perform the test due to upfront processing time Oxford, the manufacturer, has set up their own laboratory to receive and process specimens collected at clinics, hospitals or physician offices Specimens must be received in the testing facility within 32 hours of collection
45 Characteristic Tuberculin skin test (TST) IGRA Single patient visit NO YES Use of positive and negative controls NO YES Objective results NO YES Unaffected by BCG vaccination NO YES Unaffected by most environmental nontuberculosis mycobacteria Set interpretation criteria NO NO YES YES Cost Low High
46 T Spot vs Quantiferon In Tube From Oxford BioTech Standard blood collection tubes are used Blood collection tube is filled using standard phlebotomy practices Phlebotomist gently inverts blood tube after drawing specimen, consistent with standard phlebotomoy practices Butterfly needles may be used without the need for a purge tube A borderline zone is used, consistent with the recommendations of the 2010 CDC Guidelines Specimens can be maintained at room temperature for up to 32 hours T-SPOT.TB Test Yes Yes Yes Yes Yes Yes In-Tube No; requires three specialized tubes drawn in specific order. No; specialized tubes must be filled between 0.8mL and 1.2mL or within the black mark on the side of the tube label.³ Over or underfilling of the tubes outside the range may lead to erroneous results. 4 No; once filled, each tube must be mixed by shaking 10 times.³ Over-energetic shaking should be avoided to minimize erroneous results due to gel dislodgement.³ No; when a butterfly needle is used, a purge tube should be used to fill the tubing with blood prior to filling the Nil tube.³ No; Although not included in FDA-approved interpretation criteria for QFT-GIT an appropriate borderline category for QFT-GIT might increase its accuracy 5 No; tubes must be transferred to an incubator as soon as possible but within 16 hours.³
47 Quantiferon Goes After T-Spot s Single tube Collection From Qiagen, except for last sentence Experience the benefits of QFT-Plus single tube blood collection Geographic expansion Inventory control Centralized tube handling Up to 53 hours from sample collection at the draw site to sample incubation at your testing laboratory No need to supply specialized blood collection tubes to draw site blood is drawn to a single lithiumheparin tube Increase efficiency and consistency with centralized sample processing Additional Laboratory Staff may be required
48 T spot vs Quantiferon QTF is more sensitive to collection technique QTF must be processed within 16 hours for four tube collection; 53 hours for single tube collection; T spot within 32 hours. T spot is more labor intensive and less amenable to automation Some data suggest T-spot is more sensitive in immune suppressed individuals. Quantiferon is read objectively; T spot is read subjectively with an optical aid CDC study showed conversions from negative to positive in 2767 health care workers were 6.1% for Quantiferon and 8.3% for T spot (Catanzaro and Daley, 2013) High number (unspecified) of conversions reverted to and remained negative upon retesting

49 Is the IGRA cutoff Point Appropriate? Fong, et al., (CCF), Chest, 2012 Do not treat positive Quantiferon results <1.0 Daley, et al., Inf. Ctl.Hosp. Epid., 2013 Meeting report concerning variable results around the cutoff point of IGRAs Recommends caution in interpreting low positive values but does not recommend changing the cutoff point Raising the cutoff point reduces sensitivity Individuals with values <1 should have retesting considered Esmail, BMC Infect. Dis /22 HIV patients seroconverted on QTF in tube They had higher baseline TB-nil values than non converters Suggest lowering QTF cutoff in this population 49
50 Are IGRAs Bad Assays? Gamsky, et al., Ann Am thoracic Soc., 2016 Retrospective evaluation of results from serial screening of a cohort from /557 TST negative individuals were positive on the IGRA in that timeframe. 10 individuals remained positive when the test was repeated the following year 9/10 were IGRA negative within 3 years Authors recommend against using the Quantiferon Assay as a screening test in low risk populations.
51 Recently Published Data Ruhwald, et al., Lancet Resp. Med., 2017 C-Tb skin test Uses CFP-6 and ESAT 10 Same antigens as the IGRAs Compared C-Tb, TST and IGRA (n=979) C-Tb skin test had induration the same as TST C-Tb had same specificity as IGRA Study funded and reported by company that makes C-Tb Knierer, J. Occup Med Toxicol, 2017 QFT-Plus; new generation QFT Uses separate CD4 and CD8 Tb analysis tubes 95.1% agreement with QFT in tube Conversion and reversion rates slightly higher in Plus
52 Recently Published Data, 2 Abubaker, et al., Lancet Infection, Oct 2018 UK study comparing TST, T-Spot and QFT in tube N= 9610 ; 4861 contacts 4749 migrants 97 developed active TB NPV was % for all tests PPV 3.3% for QFT 4.2% for T-spot 2.2% for TST-5 2.7% for TST % for tst-15 Overall conclusion- no real difference among tests
53 Abubakar, et al., lancet infection, Oct, 2018
54 Australian National Tuberculosis Advisory Committee Position Statement Bastian, et al., nsf/content/cdi Reviewed three meta alalyses IGRAs and TST have similar (but poor) ability to identify patients with LTBI at risk of developing active disease The Committee recommends either test for LTBI The Committee recommends neither test for active TB investigation
55 And there s more.. Nemes, et al., Clin Infect Dis Jan 21. doi: /cid/ciz034. [Epub ahead of print] South African Study ESAT-6 TB vaccines are being developed ESAT-6 is in the Quantiferon and t-spot tests Developed ESAT-6 free IGRA and tested it vs Quantiferon 91% concordance between the assays Positivity rates were 43% for ESAT-6 free and 45% for QFT Recommended the ESAT-6 free test for vaccine effectiveness studies T-spot panel B does not have ESAT-6
56 IGRA TESTING PRIOR TO STARTING ANTI TUMOR NECROSIS FACTOR ALPHA THERAPY
57 Increased risk of active TB Tuberculosis (TB) exists as active disease or latent infection TNF-a inhibitor therapies can increase the risk of LTBI progressing to active TB (1,2) Compared to the general population, patients on TNF- inhibitor therapy are at 4- to 8-fold increased relative risk of developing active TB (1,2) Knowing the LTBI risk before tumor necrosis factor alpha (TNF- ) inhibitor therapy is vital References: 1. Winthrop KL et al. Arthritis Rheum 2005; 52: Gardam MA et al. Lancet Infect Dis 2003; 3: FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 57


58 TB Refresher reactivation of latent TB Treatment of RA with TNF- inhibitors may predispose to significant increase in TB risk TNF- plays a central part in the host response against tuberculosis including granuloma formation and containment of disease. with TNF- inhibitors Granuloma formation and maintenance No granuloma no containment Reference: Keane et al NEJM 2001 FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background
59 LTBI testing in patients receiving TNF- inhibitors Limitations of the TST Most patients awaiting TNF- inhibitor therapy are already treated with immunosuppressive DMARD therapy which impacts on the reliability of the TST (1) Limitations of the TST in inflammatory rheumatic patients: Lack of positive and negative controls: It is impossible to decide whether a negative TST result is a true or false negative. Negative TST results are clearly more common in inflammatory rheumatic patients compared to healthy people, suggesting a high rate of false negative TST results in patients. Negative TST results may give false security and expose patients to a higher risk of developing active TB upon initiation of TNF- inhibitor therapy (2) Reduced sensitivity in patients with immune-mediated diseases with or without immunosuppression (3-7) Insufficient antigen specificity for TB-causing pathogens BCG vaccination or previous infection with non-tuberculosis mycobacteria can cause false positive TST results (8-13) 1. Ledingham j. et al, Rhuematol 20005; 44(10): Gomez-Reino J.J. et al, Arthritis Rheum 2003; 48(8): Inanc, N et al, J Rhuematol 2009; 36(12): ) 4. Belard E et al Inflam Bowel Dies 2011; 17(11): Ponce de Leon D et al J Rhuematol 2008; 35(5): Mow, WS et al Gastroenterol Hepatol 2004; 2(4): Ponce de Leon D et al, Ann Rheum Dis 2005; 64(9): Chiu H-Y et al BR J Dermatol 2011; 164(3); Kwakernak AJ et al Clin Rheumatol 2011; 30(4): Diel R et al Chest 2010; 137(4): Matulis G et al Ann Rhuem Dis 2008; 67(1): Chang B et al Clin Rheumatol Mazurek GH et al JAMA 2001; 286(14): FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 59

 patients being considered for")
60 IGRAs in the Guidelines International and US guidelines and recommendations indicate IGRAs for screening patients on TNF-a inhibitors for LTBI 2010 CDC guidelines* provide recommendations for test selection in the diagnosis of M. tuberculosis infection IGRA may be substituted for TST in all situations as an aid in the diagnosis of M. tuberculosis infection IGRA is preferred over TST in patients who have received BCG as a vaccine or for cancer therapy Both an IGRA and TST may be considered if either initial test is negative and risk for infection, risk for progression and risk for a poor outcome are increased ** Updated 2012 ACR guidelines recommend TB screening in all rheumatoid arthritis (RA) patients being considered for therapy with biological agents regardless of presence of risk factors for TB infection *Guidance for immune-suppressed patients; no specific guidance for TNF- inhibitor therapy ** Situation 1 page 11 TST or IGRA can be performed as an initial test in all such RA patients and annual testing is recommended in patients who live, travel, or work in situations where TB exposure is likely IGRA is preferred over TST in patients who previously received BCG vaccination due to high-false positive rates associated with TST In immunosuppressed RA patients with high risk of TB exposure, a repeat test can be considered 1-3 weeks after initial negative result IGRAs are an aid to the diagnosis of mycobacterium tuberculosis infection and should be used in conjunction with detailed medical history and chest x-ray Skin test reagents currently have limited availability FOR INTERNAL USE ONLY QuantiFERON-TB Gold Product Training Tuberculosis background QM A 60
:e1-e33. doi:10.1093/cid/ciw694 Date of download: 2/6/2017 The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America.")
61 From: Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children Clin Infect Dis. 2016;64(2):e1-e33. doi: /cid/ciw694 Date of download: 2/6/2017 The Author Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions,
:e1-e33. doi:10.1093/cid/ciw694 Date of download: 2/6/2017 The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America.")
62 From: Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children Clin Infect Dis. 2016;64(2):e1-e33. doi: /cid/ciw694 Date of download: 2/6/2017 The Author Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions,
63 Take Home Points Most, but not all, studies suggest that IGRAs are more specific with equal or better sensitivity when compared to the TST IGRAs are more convenient for patients Low level positive IGRA results must be interpreted in light of the patient s clinical history and presentation Indeterminate IGRA results suggest a collection/processing error or poor immune capabilities. Conversion to positive and reversion to negative IGRA results will occur and may be related to the patient s immune capabilities or exposure status. IGRAs provide more accurate TB and immune status information than TSTs for patients about to receive TNF alpha inhibitor therapy
64 Professor, May I please be excused? My brain is full! Adapted from The Far Side, Gary Larson, 1985
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA)
 and Interferon-gamma Release Assays (IGRA)") Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2019 Bob Belknap M.D. Director, Denver Metro TB Program Disclosures No relevant financial relationships Objectives Be able to
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2019 Bob Belknap M.D. Director, Denver Metro TB Program Disclosures No relevant financial relationships Objectives Be able to
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA)
 and Interferon-gamma Release Assays (IGRA)") Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2018 Bob Belknap M.D. Director, Denver Metro TB Program No Disclosures Objectives be able to describe: 1. Who should get tested
Tuberculin Skin Test (TST) and Interferon-gamma Release Assays (IGRA) April 2018 Bob Belknap M.D. Director, Denver Metro TB Program No Disclosures Objectives be able to describe: 1. Who should get tested
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB Intensive Tyler, Texas December 2-4, 2008
 TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Technical Bulletin No. 172
 CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Peggy Leslie-Smith, RN
 Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Detecting latent tuberculosis using interferon gamma release assays (IGRA)
") Detecting latent tuberculosis using interferon gamma release assays (IGRA) American Society for Microbiology June 2017 Edward Desmond, Ph.D., D (ABMM) San Lorenzo, CA Edward Desmond has no financial connections
Detecting latent tuberculosis using interferon gamma release assays (IGRA) American Society for Microbiology June 2017 Edward Desmond, Ph.D., D (ABMM) San Lorenzo, CA Edward Desmond has no financial connections
Testing for TB. Bart Van Berckelaer Territory Manager Benelux. Subtitle
 Testing for TB Bart Van Berckelaer Territory Manager Benelux Subtitle Agenda TB infection pathway TB immunisation Testing options Pre lab considerations of the whole blood ELISA test The T-SPOT.TB test
Testing for TB Bart Van Berckelaer Territory Manager Benelux Subtitle Agenda TB infection pathway TB immunisation Testing options Pre lab considerations of the whole blood ELISA test The T-SPOT.TB test
Transmission and Pathogenesis of Tuberculosis
 Transmission and Pathogenesis of Tuberculosis 2011 John Bernardo, M.D. Pulmonary Center Boston University School of Medicine Massachusetts Department of Public Health Division of TB Prevention and Control
Transmission and Pathogenesis of Tuberculosis 2011 John Bernardo, M.D. Pulmonary Center Boston University School of Medicine Massachusetts Department of Public Health Division of TB Prevention and Control
Conflict of Interest Disclosures:
 Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
Using Interferon Gamma Release Assays for Diagnosis of TB Infection
 Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Identifying TB co-infection : new approaches?
 Identifying TB co-infection : new approaches? Charoen Chuchottaworn MD. Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH Primary tuberculosis Natural history
Identifying TB co-infection : new approaches? Charoen Chuchottaworn MD. Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH Primary tuberculosis Natural history
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Diagnosis and Medical Management of LTBI
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Diagnosis and Medical Management of LTBI Barbara Seaworth, MD December 8, 2009 CLINICAL DIAGNOSIS AND MANAGEMENT OF LATENT TB INFECTION Barbara
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Diagnosis and Medical Management of LTBI Barbara Seaworth, MD December 8, 2009 CLINICAL DIAGNOSIS AND MANAGEMENT OF LATENT TB INFECTION Barbara
Interpretation of TST & IGRA results. Objectives
 Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines
 Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Screening for Tuberculosis Infection. Harlingen, TX. Linda Dooley, MD has the following disclosures to make:
 TB Infection Diagnosis Recommendations Talk Developed by Lisa Y. Armitige, MD, PhD Medical Consultant, Heartland National TB Center Associate Professor Internal Medicine/Pediatrics/Infectious Disease UT
TB Infection Diagnosis Recommendations Talk Developed by Lisa Y. Armitige, MD, PhD Medical Consultant, Heartland National TB Center Associate Professor Internal Medicine/Pediatrics/Infectious Disease UT
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
A Clinician s Perspective: Improving Rheumatology Patient Care Using the T-SPOT.TB Test
 A Clinician s Perspective: Improving Rheumatology Patient Care Using the T-SPOT.TB Test Solomon Forouzesh, MD, FACD, FACR Medical Director Arthritis Care & Treatment Center Clinical Associate Professor
A Clinician s Perspective: Improving Rheumatology Patient Care Using the T-SPOT.TB Test Solomon Forouzesh, MD, FACD, FACR Medical Director Arthritis Care & Treatment Center Clinical Associate Professor
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 TB Partial Update Appendix 1 - Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial
TB Partial Update Appendix 1 - Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial
2016 OPAM Mid-Year Educational Conference, Sponsored by AOCOPM Sunday, March 13, 2016
 Learning Objectives Tuberculosis Case Discussions: Evaluation for Tuberculosis Infection Melissa C. Overman, DO, MPH, CHES, FAOCOPM Describe appropriate technique for TST placement, reading and interpretation
Learning Objectives Tuberculosis Case Discussions: Evaluation for Tuberculosis Infection Melissa C. Overman, DO, MPH, CHES, FAOCOPM Describe appropriate technique for TST placement, reading and interpretation
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial update) 1.1 Short title Tuberculosis
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Tuberculosis: interferon gamma tests for the diagnosis of latent tuberculosis (partial update) 1.1 Short title Tuberculosis
QuantiFERON-TB Gold Plus
 QuantiFERON-TB Gold Plus A New Interferon-γ Release Assay (IGRA) for the Indirect Detection of Mycobacterium tuberculosis HOT TOPIC / 2018 Presenter: Elitza S. Theel, PhD, D(ABMM) Director of Infectious
QuantiFERON-TB Gold Plus A New Interferon-γ Release Assay (IGRA) for the Indirect Detection of Mycobacterium tuberculosis HOT TOPIC / 2018 Presenter: Elitza S. Theel, PhD, D(ABMM) Director of Infectious
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Testing & Treatment for TB Infection: Blood Tests, Skin Tests, Who to Screen & Who to Treat?
 NECHA 11/4/2016 Testing & Treatment for TB Infection: Blood Tests, Skin Tests, Who to Screen & Who to Treat? E. Jane Carter, M.D. Immediate Past President International Union Against TB and Lung Disease
NECHA 11/4/2016 Testing & Treatment for TB Infection: Blood Tests, Skin Tests, Who to Screen & Who to Treat? E. Jane Carter, M.D. Immediate Past President International Union Against TB and Lung Disease
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
Table 9. Policy for Tuberculosis Surveillance and Screening
 Policy for Tuberculosis Surveillance and Screening Purpose: to identify active cases of tuberculosis or latent TB among residents and staff of the nursing home in order to prevent transmission in this
Policy for Tuberculosis Surveillance and Screening Purpose: to identify active cases of tuberculosis or latent TB among residents and staff of the nursing home in order to prevent transmission in this
Diagnosis and Medical Case Management of Latent TB. Bryan Rock, MD April 27, 2010
 TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis and Medical Case Management of Latent TB Infection Bryan Rock, MD April 27, 2010 DIAGNOSIS AND MANAGEMENT OF LATENT TUBERCULOSIS
TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis and Medical Case Management of Latent TB Infection Bryan Rock, MD April 27, 2010 DIAGNOSIS AND MANAGEMENT OF LATENT TUBERCULOSIS
Investigation of false-positive results by the QuantiFERON-TB Gold In-Tube assay
 JCM Accepts, published online ahead of print on 11 July 2012 J. Clin. Microbiol. doi:10.1128/jcm.00730-12 Copyright 2012, American Society for Microbiology. All Rights Reserved. 1 2 Investigation of false-positive
JCM Accepts, published online ahead of print on 11 July 2012 J. Clin. Microbiol. doi:10.1128/jcm.00730-12 Copyright 2012, American Society for Microbiology. All Rights Reserved. 1 2 Investigation of false-positive
Effect of prolonged incubation time on the results of the QuantiFERON TB Gold In-Tube assay for the diagnosis of latent tuberculosis infection
 CVI Accepts, published online ahead of print on 3 July 2013 Clin. Vaccine Immunol. doi:10.1128/cvi.00290-13 Copyright 2013, American Society for Microbiology. All Rights Reserved. 1 2 3 Effect of prolonged
CVI Accepts, published online ahead of print on 3 July 2013 Clin. Vaccine Immunol. doi:10.1128/cvi.00290-13 Copyright 2013, American Society for Microbiology. All Rights Reserved. 1 2 3 Effect of prolonged
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Tuberculosis and Biologic Therapies: Risk and Prevention
 Tuberculosis and Biologic Therapies: Risk and Prevention Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health & Science
Tuberculosis and Biologic Therapies: Risk and Prevention Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health & Science
TB Nurse Case Management San Antonio, Texas March 7 9, Clinical Diagnosis and
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Clinical Diagnosis and Management of LTBI Lynn Horvath, MD March 7, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Clinical Diagnosis and Management of LTBI Lynn Horvath, MD March 7, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Dimitrios Vassilopoulos,* Stamatoula Tsikrika, Chrisoula Hatzara, Varvara Podia, Anna Kandili, Nikolaos Stamoulis, and Emilia Hadziyannis
 CLINICAL AND VACCINE IMMUNOLOGY, Dec. 2011, p. 2102 2108 Vol. 18, No. 12 1556-6811/11/$12.00 doi:10.1128/cvi.05299-11 Copyright 2011, American Society for Microbiology. All Rights Reserved. Comparison
CLINICAL AND VACCINE IMMUNOLOGY, Dec. 2011, p. 2102 2108 Vol. 18, No. 12 1556-6811/11/$12.00 doi:10.1128/cvi.05299-11 Copyright 2011, American Society for Microbiology. All Rights Reserved. Comparison
Latent TB Infection (LTBI)
") Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lynn Horvath, MD November 11, 2014 Lynn Horvath, MD has the following disclosures to
TB Intensive San Antonio, Texas November 11 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lynn Horvath, MD November 11, 2014 Lynn Horvath, MD has the following disclosures to
Tuberculin Skin Testing
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 Testing to TB Infection Using the TST Presented by Debra Howenstine, MD for Debbie Onofre, RN October 5, 2010 Tuberculin
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 Testing to TB Infection Using the TST Presented by Debra Howenstine, MD for Debbie Onofre, RN October 5, 2010 Tuberculin
Therapy for Latent Tuberculosis Infection
 Screening and Treatment of LTBI in TB Control in the US Margarita Elsa Villarino MD MPH Division of TB Elimination, CDC April 14, 2004 TB Prevention and Control in the United States The fundamental strategies
Screening and Treatment of LTBI in TB Control in the US Margarita Elsa Villarino MD MPH Division of TB Elimination, CDC April 14, 2004 TB Prevention and Control in the United States The fundamental strategies
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis Pathogenesis and Treatment f Latent TB Infection Lynn Horvath, MD October 15, 2013 Lynn Horvath, MD has the following disclosures to make: No
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis Pathogenesis and Treatment f Latent TB Infection Lynn Horvath, MD October 15, 2013 Lynn Horvath, MD has the following disclosures to make: No
Thorax Online First, published on December 8, 2009 as /thx
 Thorax Online First, published on December 8, 2009 as 10.1136/thx.2009.119677 Title Page Cost effectiveness of the NICE guidelines for screening for latent tuberculosis infection: the Quantiferon-TB gold
Thorax Online First, published on December 8, 2009 as 10.1136/thx.2009.119677 Title Page Cost effectiveness of the NICE guidelines for screening for latent tuberculosis infection: the Quantiferon-TB gold
LTBI: Who to Test & When to Treat
 LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
These recommendations will remain in effect until the national shortage of PPD solution has abated.
 Maryland Recommendations Regarding the National Shortage of Purified Protein Derivative (PPD) Solution; Attachment to Health Officer Memorandum National Shortages of Tubersol and Aplisol for TB Skin Testing;
Maryland Recommendations Regarding the National Shortage of Purified Protein Derivative (PPD) Solution; Attachment to Health Officer Memorandum National Shortages of Tubersol and Aplisol for TB Skin Testing;
IGRAs for Diagnosis of Tuberculosis: 2010 Update
 IGRAs for Diagnosis of Tuberculosis: 2010 Update Nira Pollock, M.D., Ph.D. Division of Infectious Diseases Beth Israel Deaconess Medical Center Boston, MA May 1, 2010 Problems with the PPD False positives
IGRAs for Diagnosis of Tuberculosis: 2010 Update Nira Pollock, M.D., Ph.D. Division of Infectious Diseases Beth Israel Deaconess Medical Center Boston, MA May 1, 2010 Problems with the PPD False positives
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Role of the Laboratory in TB Diagnosis and Management
 Role of the Laboratory in TB Diagnosis and Management Michael Pentella, Ph.D., D(ABMM), CIC Associate Director University Hygienic Lab Clinical Associate Professor, College of Public Health, University
Role of the Laboratory in TB Diagnosis and Management Michael Pentella, Ph.D., D(ABMM), CIC Associate Director University Hygienic Lab Clinical Associate Professor, College of Public Health, University
CUSOM Student Health Immunization Requirements
 CUSOM Student Health Immunization Requirements Regulatory and legislative authorities require that students demonstrate immunization, immunity and/or protection from multiple contagious diseases before
CUSOM Student Health Immunization Requirements Regulatory and legislative authorities require that students demonstrate immunization, immunity and/or protection from multiple contagious diseases before
Use of an Interferon- Release Assay To Diagnose Latent Tuberculosis Infection in Foreign-Born Patients*
 Original Research MYCOBACTERIAL DISEASE Use of an Interferon- Release Assay To Diagnose Latent Tuberculosis Infection in Foreign-Born Patients* Daniel Brodie, MD; David J. Lederer, MD, MS; Jade S. Gallardo,
Original Research MYCOBACTERIAL DISEASE Use of an Interferon- Release Assay To Diagnose Latent Tuberculosis Infection in Foreign-Born Patients* Daniel Brodie, MD; David J. Lederer, MD, MS; Jade S. Gallardo,
The Challenges and Pitfalls in Diagnosing or Misdiagnosing Tuberculosis: Are the Days of TB Skin Tests Over?
 The Challenges and Pitfalls in Diagnosing or Misdiagnosing Tuberculosis: Are the Days of TB Skin Tests Over? ROY F. CHEMALY, MD, MPH, FIDSA, FACP PROFESSOR OF MEDICINE DIRECTOR, INFECTION CONTROL SECTION
The Challenges and Pitfalls in Diagnosing or Misdiagnosing Tuberculosis: Are the Days of TB Skin Tests Over? ROY F. CHEMALY, MD, MPH, FIDSA, FACP PROFESSOR OF MEDICINE DIRECTOR, INFECTION CONTROL SECTION
The Most Widely Misunderstood Test of All
 The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons
The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons
Community pharmacy-based tuberculosis skin testing
 Community pharmacy-based tuberculosis skin testing Shanna K. O Connor, PharmD ISU KDHS Spring CE Seminar 2018 In support of improving patient care, Idaho State University Kasiska Division of Health Sciences
Community pharmacy-based tuberculosis skin testing Shanna K. O Connor, PharmD ISU KDHS Spring CE Seminar 2018 In support of improving patient care, Idaho State University Kasiska Division of Health Sciences
ORIGINAL ARTICLE. Clinical evaluation of QuantiFERON TB-2G test for immunocompromised patients
 ERJ Express. Published on July 25, 2007 as doi: 10.1183/09031936.00040007 ORIGINAL ARTICLE Clinical evaluation of QuantiFERON TB-2G test for immunocompromised patients Yoshihiro Kobashi, Keiji Mouri, Yasushi
ERJ Express. Published on July 25, 2007 as doi: 10.1183/09031936.00040007 ORIGINAL ARTICLE Clinical evaluation of QuantiFERON TB-2G test for immunocompromised patients Yoshihiro Kobashi, Keiji Mouri, Yasushi
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014
 TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
QuantiFERON -TB Gold Plus (QFT -Plus) Package Insert
 Package Insert") QuantiFERON -TB Gold Plus (QFT -Plus) Package Insert July 2018 2 x 96 (cat. no. 622130) 20 x 96 (cat. no. 622832) The Whole Blood IFN-γ test measuring responses to ESAT-6 and CFP-10 peptide antigens For
QuantiFERON -TB Gold Plus (QFT -Plus) Package Insert July 2018 2 x 96 (cat. no. 622130) 20 x 96 (cat. no. 622832) The Whole Blood IFN-γ test measuring responses to ESAT-6 and CFP-10 peptide antigens For
The Whole Blood IFN-gamma Test Measuring Responses to ESAT-6, CFP-10 & TB7.7 Peptide Antigens PACKAGE INSERT. For In Vitro Diagnostic Use
 The Whole Blood IFN-gamma Test Measuring Responses to ESAT-6, CFP-10 & TB7.7 Peptide Antigens PACKAGE INSERT For In Vitro Diagnostic Use index 1. INTENDED USE 2 2. SUMMARY AND EXPLANATION OF THE TEST 2
The Whole Blood IFN-gamma Test Measuring Responses to ESAT-6, CFP-10 & TB7.7 Peptide Antigens PACKAGE INSERT For In Vitro Diagnostic Use index 1. INTENDED USE 2 2. SUMMARY AND EXPLANATION OF THE TEST 2
Screening of HIV-Infected Patients with IGRAs for LTBI. Background. Tuberculosis is the most prevalent in the world.
 Screening of HIV-Infected Patients with IGRAs for LTBI Kentaro Sakashita, Akira Fujita, Shuji Hatakeyma Stay strong, Japan! Tokyo Metropolitan Tama Medical Center Department of Pulmonary Medicine Background
Screening of HIV-Infected Patients with IGRAs for LTBI Kentaro Sakashita, Akira Fujita, Shuji Hatakeyma Stay strong, Japan! Tokyo Metropolitan Tama Medical Center Department of Pulmonary Medicine Background
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Student Health Requirements Master of Arts, Biomedical Sciences Program
 Student Health Requirements Master of Arts, Biomedical Sciences Program All students in medically related programs, just as physicians in practice, are required to be current with required immunizations
Student Health Requirements Master of Arts, Biomedical Sciences Program All students in medically related programs, just as physicians in practice, are required to be current with required immunizations
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 LTBI: Screening & Testing Anna M. Mandalakas, MD, MS Epi, FAAP Global Tuberculosis Program Director The Tuberculosis Initiative Texas Children s Hospital
Pediatric TB Intensive Houston, Texas October 14, 2013 LTBI: Screening & Testing Anna M. Mandalakas, MD, MS Epi, FAAP Global Tuberculosis Program Director The Tuberculosis Initiative Texas Children s Hospital
Variation in T-SPOT.TB spot interpretation between independent observers of different laboratories
 8 Variation in T-SPOT.TB spot interpretation between independent observers of different laboratories Willeke P.J. Franken 1, Steven Thijsen 2, Ron Wolterbeek 3, John J.M. Bouwman 2, Hanane el Bannoudi
8 Variation in T-SPOT.TB spot interpretation between independent observers of different laboratories Willeke P.J. Franken 1, Steven Thijsen 2, Ron Wolterbeek 3, John J.M. Bouwman 2, Hanane el Bannoudi
Literature Overview. Health Economics. Experience with QuantiFERON -TB Gold. Cellestis Clinical Guide series
 Literature Overview Experience with QuantiFERON -TB Gold Health Economics Cellestis Clinical Guide series 2008 www.cellestis.com This literature overview is intended to provide healthcare professionals
Literature Overview Experience with QuantiFERON -TB Gold Health Economics Cellestis Clinical Guide series 2008 www.cellestis.com This literature overview is intended to provide healthcare professionals
DEPARTMENT OF THE ARMY OFFICE OF THE SURGEON GENERAL 5109 LEESBURG PIKE FALLS CHURCH, VA
 DEPARTMENT OF THE ARMY OFFICE OF THE SURGEON GENERAL 5109 LEESBURG PIKE FALLS CHURCH, VA 22041-3258 DASG-PPM-NC r% 5 SEP 2008 MEMORANDUM FOR SEE DISTRIBUTION SUBJECT: Supplemental guidance for the Army
DEPARTMENT OF THE ARMY OFFICE OF THE SURGEON GENERAL 5109 LEESBURG PIKE FALLS CHURCH, VA 22041-3258 DASG-PPM-NC r% 5 SEP 2008 MEMORANDUM FOR SEE DISTRIBUTION SUBJECT: Supplemental guidance for the Army
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
LTBI conception definitions and relevance for diagnostic products
 LTBI conception definitions and relevance for diagnostic products Frank Cobelens Amsterdam Institute for Global Health and Development Amsterdam, Netherlands KNCV Tuberculosis Foundation The Hague, Netherlands
LTBI conception definitions and relevance for diagnostic products Frank Cobelens Amsterdam Institute for Global Health and Development Amsterdam, Netherlands KNCV Tuberculosis Foundation The Hague, Netherlands
Evaluation of an In Vitro Assay for Gamma Interferon Production in Response to Mycobacterium tuberculosis Infections
 CLINICAL AND DIAGNOSTIC LABORATORY IMMUNOLOGY, Nov. 2004, p. 1089 1093 Vol. 11, No. 6 1071-412X/04/$08.00 0 DOI: 10.1128/CDLI.11.6.1089 1093.2004 Copyright 2004, American Society for Microbiology. All
CLINICAL AND DIAGNOSTIC LABORATORY IMMUNOLOGY, Nov. 2004, p. 1089 1093 Vol. 11, No. 6 1071-412X/04/$08.00 0 DOI: 10.1128/CDLI.11.6.1089 1093.2004 Copyright 2004, American Society for Microbiology. All
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Jeffrey R. Starke, M.D. has the following disclosures to make:
 AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Title: Role of Interferon-gamma Release Assays in the Diagnosis of Pulmonary Tuberculosis in Patients with Advanced HIV infection
 Author's response to reviews Title: Role of Interferon-gamma Release Assays in the Diagnosis of Pulmonary Tuberculosis in Patients with Advanced HIV infection Authors: Adithya Cattamanchi (acattamanchi@medsfgh.ucsf.edu)
Author's response to reviews Title: Role of Interferon-gamma Release Assays in the Diagnosis of Pulmonary Tuberculosis in Patients with Advanced HIV infection Authors: Adithya Cattamanchi (acattamanchi@medsfgh.ucsf.edu)
Diagnosis of tuberculosis
 Diagnosis of tuberculosis Madhukar Pai, MD, PhD Assistant Professor, Epidemiology McGill University, Montreal, Canada madhukar.pai@mcgill.ca Global TB Case Detection A major concern 2.6 million new smear
Diagnosis of tuberculosis Madhukar Pai, MD, PhD Assistant Professor, Epidemiology McGill University, Montreal, Canada madhukar.pai@mcgill.ca Global TB Case Detection A major concern 2.6 million new smear
Latent Tuberculosis in Adults: From Testing TO Treatment
 Latent Tuberculosis in Adults: From Testing TO Treatment Sergio M. Borgia, MD, MSc., FRCP(C) Infectious Diseases Consultant, WOHS Medical Director, WOHS Tuberculosis Clinic Assistant Clinical Professor,
Latent Tuberculosis in Adults: From Testing TO Treatment Sergio M. Borgia, MD, MSc., FRCP(C) Infectious Diseases Consultant, WOHS Medical Director, WOHS Tuberculosis Clinic Assistant Clinical Professor,
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents
 New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
Tuberculosis and TNF Inhibitors
 Tuberculosis and TNF Inhibitors Sundari Mase MD, MPH Medical Team Lead CDC/DTBE/FSEB January 18, 2011 Objectives Discuss the association between and epidemiology of TNF inhibitors and TB Discuss the challenges
Tuberculosis and TNF Inhibitors Sundari Mase MD, MPH Medical Team Lead CDC/DTBE/FSEB January 18, 2011 Objectives Discuss the association between and epidemiology of TNF inhibitors and TB Discuss the challenges
The evolving concept of LTBI diagnosis tests for incipient TB and tests for persistent infection
 The evolving concept of LTBI diagnosis tests for incipient TB and tests for persistent infection Frank Cobelens f.cobelens@aighd.org KNCV Tuberculosis Foundation The Hague, Netherlands Amsterdam Institute
The evolving concept of LTBI diagnosis tests for incipient TB and tests for persistent infection Frank Cobelens f.cobelens@aighd.org KNCV Tuberculosis Foundation The Hague, Netherlands Amsterdam Institute
Author's response to reviews
 Author's response to reviews Title: Contribution of Interferon Gamma Release Assays testing to the Diagnosis of Latent Tuberculosis Infection in HIV-Infected Patients: A comparison of QuantiFERON Gold
Author's response to reviews Title: Contribution of Interferon Gamma Release Assays testing to the Diagnosis of Latent Tuberculosis Infection in HIV-Infected Patients: A comparison of QuantiFERON Gold
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI)
") Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Use of Interferon-γ Release Assays (IGRAs) in TB control in low and middle-income settings - EXPERT GROUP MEETING -
 in TB control in low and middle-income settings - EXPERT GROUP MEETING -") Use of Interferon-γ Release Assays (IGRAs) in TB control in low and middle-income settings - EXPERT GROUP MEETING - Date and time: 20-21 July 2010, 09:00 18:00 Venue: Salle B, WHO-HQ, Geneva, Switzerland
Use of Interferon-γ Release Assays (IGRAs) in TB control in low and middle-income settings - EXPERT GROUP MEETING - Date and time: 20-21 July 2010, 09:00 18:00 Venue: Salle B, WHO-HQ, Geneva, Switzerland
(In-Tube Method) The Whole Blood IFN-gamma Test Measuring Responses to ESAT-6, CFP-10 & TB7.7(p.4) Peptide Antigens PACKAGE INSERT
 The Whole Blood IFN-gamma Test Measuring Responses to ESAT-6, CFP-10 & TB7.7(p.4) Peptide Antigens PACKAGE INSERT") (In-Tube Method) The Whole Blood IFN-gamma Test Measuring Responses to ESAT-6, CFP-10 & TB7.7(p.4) Peptide Antigens PACKAGE INSERT For In Vitro Diagnostic Use BlanK Page INDEX 1. INTENDED USE 2 2. SUMMARY
(In-Tube Method) The Whole Blood IFN-gamma Test Measuring Responses to ESAT-6, CFP-10 & TB7.7(p.4) Peptide Antigens PACKAGE INSERT For In Vitro Diagnostic Use BlanK Page INDEX 1. INTENDED USE 2 2. SUMMARY
Identification of latent tuberculosis infection in rheumatic patients under consideration for treatment with anti-tnf-α agents
 Clinical research Identification of latent tuberculosis infection in rheumatic patients under consideration for treatment with anti-tnf-α agents Jolanta Paluch-Oleś 1, Agnieszka Magryś 1, Maria Kozioł-Montewka
Clinical research Identification of latent tuberculosis infection in rheumatic patients under consideration for treatment with anti-tnf-α agents Jolanta Paluch-Oleś 1, Agnieszka Magryś 1, Maria Kozioł-Montewka