ENCEPHALITIS. Diana Montoya Melo
|
|
|
- Kathryn Allen
- 5 years ago
- Views:
Transcription
1 ENCEPHALITIS Diana Montoya Melo
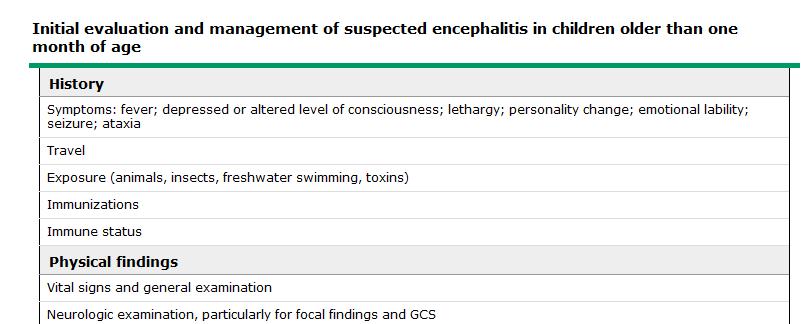
2 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated with decreased activity level and 1 day history of lethargy. Mom has been treating the fever at home, and the last dose of Tylenol was given 1 hour ago.
3 On arrival, VS: T: 37.9, PR: 135/min, RR: 26, BP: 87/59. O2 Sat 100%. Patient is obtunded, tolerates RA, Moist mucous membranes, nasal congestion, pink TM bilaterally, tonsillar erythema, no exudates, oropharynx with few small pustules. LCTAB. Abd:soft, ND, NT. Skin: cap refill prolonged. Small pustules over palms and soles. Neuro: appears obtunded but arouses with painful stimuli. Neurologic exam reveals no focal findings. No neck stiffness, neg meningeal signs PMH: unremarkable Immunizations UTD
4 PARTIAL VS FULL SEPSIS WORKUP?
5 Besides getting a full sepsis workup, what other diagnostic tools should be included: a) Brain imaging B) CMP C) Coags C) EEG E) all of the above
6 Besides getting a full sepsis workup, what other diagnostic tools should be included: a) Brain imaging B) CMP C) Coags C) EEG E) all of the above
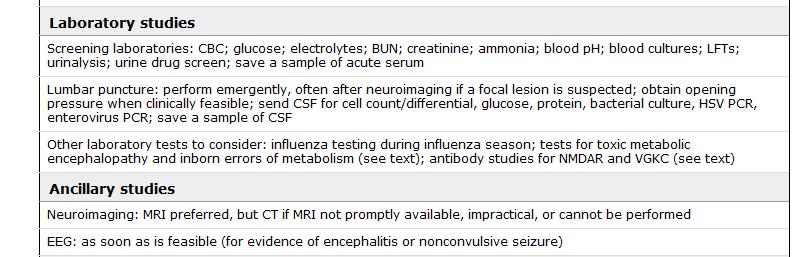
7 WHAT ELSE CAN BE INCLUDED AS PART OF THE WORKUP?
8
9
10
11 CSF results are back, which of the following would you expect to find in this patient? A) WBC: 328, L: 18% N: 82%, RBC:0, prot: 250, Glucose: 38 B) WBC: 128, L: 78% N: 22, RBC:0, prot: 140, Glucose: 68 C) WBC: 328, L: 88% N: 12, RBC:0, prot: 300, Glucose: 10 D) none of the above
12 CSF results are back, which of the following would you expect to find in this patient? A) WBC: 328, L: 18% N: 82%, RBC:0, prot: 250, Glucose: 38 B) WBC: 128, L: 78% N: 22, RBC:0, prot: 140, Glucose: 68 C) WBC: 328, L: 88% N: 12, RBC:0, prot: 300, Glucose: 10 D) none of the above
13
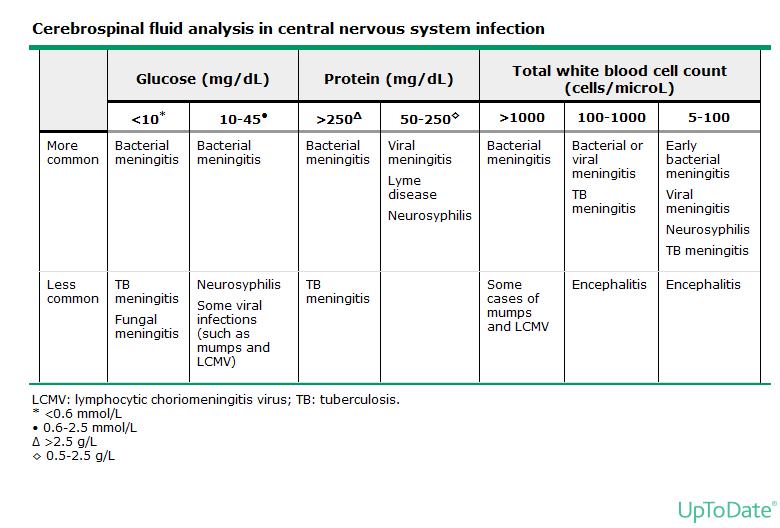
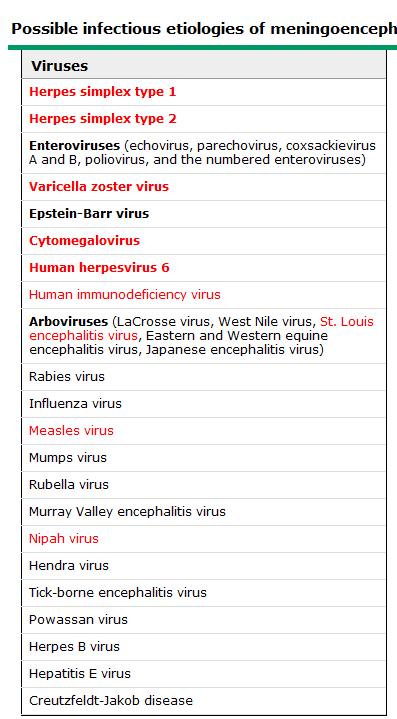
14 CSF AND VIRAL ENCEPHALITIES The CSF indices in viral encephalitis are similar to those in viral meningitis and meningoencephalitis and may overlap with those of bacterial meningitis 3 to 5%, CSF findings are completely normal CSF findings in viral encephalitis are as follows: CSF pleocytosis. WBC typically ranges from 0 to 500 cells/microl with a lymphocytic predominance; however, a predominance of neutrophils can be seen during the first 24 to 48 hours of infection. RBC are usually absent (except in traumatic tap), but their presence can indicate HSV encephalitis, La Crosse virus encephalitis, or other necrotizing encephalitides (eg, Eastern equine encephalitis, amebic encephalitis) Protein is usually slightly elevated (generally <150 mg/dl) Glucose is usually normal and >50 percent of blood value
15
16 What would be the best empiric therapy in this case: A) Vancomycin B) Acyclovir C) Vancomycin + Ceftriaxone D) Doxycycline E) Bactrim
17 What would be the best empiric therapy in this case: A) Vancomycin B) Acyclovir C) Vancomycin + Ceftriaxone D) Doxycycline E) Bactrim
18 EMPIRIC THERAPY OF VIRAL ENCEPHALITIS Empiric acyclovir prompt initiation of intravenous (IV) acyclovir for children (beyond the neonatal period) and adolescents with suspected encephalitis Dose >28 days to <3 months 20 mg/kg per dose every eight hours 3 months to <12 years 10 to 15 mg/kg per dose every eight hours 12 years 10 mg/kg per dose every eight hours Duration If HSV is confirmed or probable, should be continued for 21 days LP should be performed near the end of acyclovir treatment to ensure that HSV PCR is negative; acyclovir therapy should be continued if CSF HSV PCR remains positive. The decision to continue acyclovir therapy for patients in whom HSV PCR is negative must be individualized. HSV PCR in the CSF can be negative during the first few days of the illness
19 EMPIRIC THERAPY OF VIRAL ENCEPHALITIS 2012 shortage of IV acyclovir in agreement with the AAP Committee on ID IV ganciclovir 6 mg/kg every 12 hours for patients 90 days of age and 5 mg/kg every 12 hours for patients >90 days of age If ganciclovir cannot be given, IV foscarnet 60 mg/kg every 12 hours Empiric antibiotics If clinically and/or epidemiologically indicated, empiric treatment should be provided for bacterial meningitis, rickettsial infection, and ehrlichiosis, pending the results of cultures and other diagnostic studies
20
21
22 REFERENCES Acute viral encephalitis in children and adolescents: Clinical manifestations and diagnosis. edited by Denise S. Basow, published by UpToDate in Waltham, MA. Acute viral encephalitis in children and adolescents: Treatment and prevention. edited by Denise S. Basow, published by UpToDate in Waltham, MA.
ID Emergencies. BGSMC Internal Medicine Edwin Yu
 ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies. BUMC-P Internal Medicine Edwin Yu
 ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
 1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Dilemmas in the Management of Meningitis & Encephalitis HEADACHE AND FEVER. What is the best initial approach for fever, headache, meningisums?
 Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
PEDIATRIC INFECTIOUS DISEASES UPDATE. Neonatal HSV. Recognition, Diagnosis, and Management Coleen Cunningham MD
 Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
CNS INFECTIONS MENINGITIS
 CNS INFECTIONS MENINGITIS Learning Objectives: 1. Describe patient risk factors,signs and symptoms that may indicate meningitis 2. Identify tests and significant laboratory values used to diagnose meningitis
CNS INFECTIONS MENINGITIS Learning Objectives: 1. Describe patient risk factors,signs and symptoms that may indicate meningitis 2. Identify tests and significant laboratory values used to diagnose meningitis
4/14/2010. Theoretical purpose of fever? Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010
 Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Emergency Neurological Life Support Meningitis and Encephalitis
 Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants
 Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
Managing meningitis not just antibiotics. Helena White December 2013
 Managing meningitis not just antibiotics Helena White December 2013 Case history 43 year old British-born Asian lady Legal advisor Married with a three year old child (on Amoxicillin for recent ear infection)
Managing meningitis not just antibiotics Helena White December 2013 Case history 43 year old British-born Asian lady Legal advisor Married with a three year old child (on Amoxicillin for recent ear infection)
Infectious Neurology. Alison Ruiz PA-C
 Infectious Neurology Alison Ruiz PA-C Case Presentation 48 y/o F presents to the ER with c/o headache and fever for the past two days. tates started with head pain and then patient developed fever max
Infectious Neurology Alison Ruiz PA-C Case Presentation 48 y/o F presents to the ER with c/o headache and fever for the past two days. tates started with head pain and then patient developed fever max
Septic Shock. Kathryn Sims, PGY I
 Septic Shock Kathryn Sims, PGY I A 6 y.o. previously healthy boy presents to the ED with 7 days of fever accompanied by chills. Further history reveals the patient has also been experiencing dysuria for
Septic Shock Kathryn Sims, PGY I A 6 y.o. previously healthy boy presents to the ED with 7 days of fever accompanied by chills. Further history reveals the patient has also been experiencing dysuria for
Management of Complex Febrile Seizures
 Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
An Intriguing Case of Meningitis. Tiffany Mylius MLS (ASCP)
") An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report
 Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
Hot Hot Tot:! The Hot Tot. Fever in KIds <90 Days 5/26/10
 Hot Hot Tot:! Fever in KIds
Hot Hot Tot:! Fever in KIds
VIRAL ENCEPHALITIS EASY TO MISS
 TAMORISH KOLE MBBS MRCS(EDIN) FRSM(UK) SENIOR CONSULTANT & HEAD, EMERGENCY MEDICINE, MAX HEALTHCARE, NEW DELHI, INDIA ADJUNCT ASSISTANT PROFESSOR, EMERGENCY MEDICINE, GEORGE WASHINGTON UNIVERSITY, WASHINGTON
TAMORISH KOLE MBBS MRCS(EDIN) FRSM(UK) SENIOR CONSULTANT & HEAD, EMERGENCY MEDICINE, MAX HEALTHCARE, NEW DELHI, INDIA ADJUNCT ASSISTANT PROFESSOR, EMERGENCY MEDICINE, GEORGE WASHINGTON UNIVERSITY, WASHINGTON
The Febrile Infant. SJRH ED Rounds Dec By: Robin Clouston
 1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
A Neurologist s Approach to Altered Mental Status
 A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
Rational Evaluation of the Febrile Infant
 Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN
 MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN OVERVIEW 1980s: dramatically improved by aciclovir HSV encephalitis in adults Delays treatment(> 48h after hospital admission): associated with a
MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN OVERVIEW 1980s: dramatically improved by aciclovir HSV encephalitis in adults Delays treatment(> 48h after hospital admission): associated with a
Case Report. Herpes simplex virus encephalitis presenting as frontal lobe hemorrhage
 1 Case Report Herpes simplex virus encephalitis presenting as frontal lobe hemorrhage Authors: Shila, MD, *Jessica Erfan, MPAS, PA-C, Ray Bogitch, MD, Jefferson T. Miley, MD Department of Neurology, Dell
1 Case Report Herpes simplex virus encephalitis presenting as frontal lobe hemorrhage Authors: Shila, MD, *Jessica Erfan, MPAS, PA-C, Ray Bogitch, MD, Jefferson T. Miley, MD Department of Neurology, Dell
Fever in Babies. Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases
 Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
Meningitis. Matthew Grant MD
 Meningitis Matthew Grant MD Objectives Understand the diagnostic accuracy of clinical findings Appreciate the differential diagnosis of aseptic meningitis syndrome, and indications for hospitalization
Meningitis Matthew Grant MD Objectives Understand the diagnostic accuracy of clinical findings Appreciate the differential diagnosis of aseptic meningitis syndrome, and indications for hospitalization
Fever in the Newborn Period
 Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS
 ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
Clinical Information on West Nile Virus (WNV) Infection
 Infection") Clinical Information on West Nile Virus (WNV) Infection Introduction In 1999, West Nile Virus (WNV), an Old World flavivirus, producing a spectrum of disease including severe meningoencephalitis, appeared
Clinical Information on West Nile Virus (WNV) Infection Introduction In 1999, West Nile Virus (WNV), an Old World flavivirus, producing a spectrum of disease including severe meningoencephalitis, appeared
CNS Infections. Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London. Hammersmith Acute Medicine 2011
 CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
Mommy, my head hurts : Pediatric Neurologic Emergencies. Craig S. LaRusso MA, BSN, RN, C-NPT
 Mommy, my head hurts : Pediatric Neurologic Emergencies Craig S. LaRusso MA, BSN, RN, C-NPT 6 yr old boy with altered LOC 6 yr old boy with no past medical history 12 days ago fever x 4days up to 103 with
Mommy, my head hurts : Pediatric Neurologic Emergencies Craig S. LaRusso MA, BSN, RN, C-NPT 6 yr old boy with altered LOC 6 yr old boy with no past medical history 12 days ago fever x 4days up to 103 with
FILMARRAY: CAN IT MAKE A DIFFERENCE FOR CSF TESTING L O U I S E O S U L L I V A N, M M U H O S U L L I V A N M A T E R. I E
 FILMARRAY: CAN IT MAKE A DIFFERENCE FOR CSF TESTING L O U I S E O S U L L I V A N, M M U H O S U L L I V A N L @ M A T E R. I E Level 4 teaching hospital based in Dublin s north inner city Over 600 in-patient
FILMARRAY: CAN IT MAKE A DIFFERENCE FOR CSF TESTING L O U I S E O S U L L I V A N, M M U H O S U L L I V A N L @ M A T E R. I E Level 4 teaching hospital based in Dublin s north inner city Over 600 in-patient
Lumbar puncture. Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: ml Replenished: 4-6 h Routine LP (3-5 ml): <1h
: <1h") Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
URIs and Pneumonia. Elena Bissell, MD 10/16/2013
 URIs and Pneumonia Elena Bissell, MD 10/16/2013 Objectives Recognize and treat community acquired PNA in children/adults Discern between inpatient and outpatient treatment of PNA Recognize special populations/cases
URIs and Pneumonia Elena Bissell, MD 10/16/2013 Objectives Recognize and treat community acquired PNA in children/adults Discern between inpatient and outpatient treatment of PNA Recognize special populations/cases
When the drugs don t work- a case of HSV encephalitis.
 When the drugs don t work- a case of HSV encephalitis. Nicky Price Consultant Virologist Public Health Wales 67 year old Caucasian Female Presenting complaint 2 day history of: Confusion Shivering Headache
When the drugs don t work- a case of HSV encephalitis. Nicky Price Consultant Virologist Public Health Wales 67 year old Caucasian Female Presenting complaint 2 day history of: Confusion Shivering Headache
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
AMSER Case of the Month July 2018 Complicated Headache with Fever
 AMSER Case of the Month July 2018 Complicated Headache with Fever Benjamin Park, MS IV Dr. Karen Xie Department of Radiology University of Illinois College of Medicine at Chicago Patient Presentation CC:
AMSER Case of the Month July 2018 Complicated Headache with Fever Benjamin Park, MS IV Dr. Karen Xie Department of Radiology University of Illinois College of Medicine at Chicago Patient Presentation CC:
Critical Review Form Clinical Prediction or Decision Rule
 Critical Review Form Clinical Prediction or Decision Rule Development and Validation of a Multivariable Predictive Model to Distinguish Bacterial from Aseptic Meningitis in Children, Pediatrics 2002; 110:
Critical Review Form Clinical Prediction or Decision Rule Development and Validation of a Multivariable Predictive Model to Distinguish Bacterial from Aseptic Meningitis in Children, Pediatrics 2002; 110:
Neurologic Emergencies
 Neurologic Emergencies S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology Director, Neurohospitalist
Neurologic Emergencies S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology Director, Neurohospitalist
Neurologic Emergencies Case #1
 Neurologic Emergencies Case #1 S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chairman, Department of Neurology Director,
Neurologic Emergencies Case #1 S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chairman, Department of Neurology Director,
The gold standard? A 4-year-old boy with somnolence and focal weakness
 The gold standard? A 4-year-old boy with somnolence and focal weakness Alex Florence, MD, PGY-3, UNC Children s Hospital Disclosures I have no conflicts of interest or financial obligations to disclose.
The gold standard? A 4-year-old boy with somnolence and focal weakness Alex Florence, MD, PGY-3, UNC Children s Hospital Disclosures I have no conflicts of interest or financial obligations to disclose.
Aseptic meningitis: inflammation of meninges with sterile CSF (without any causative organisms which can be grown on culture media).
.") You have to refer to the slides, since I have included the extra information only. Slide #1: Both illnesses aseptic meningitis and encephalitis can be caused by the same viruses; that viruses which cause
You have to refer to the slides, since I have included the extra information only. Slide #1: Both illnesses aseptic meningitis and encephalitis can be caused by the same viruses; that viruses which cause
COPYRIGHT 2012 THE TRANSVERSE MYELITIS ASSOCIATION. ALL RIGHTS RESERVED
 The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
Neonatal HSV SARA SAPORTA-KEATING 3/1/17
 Neonatal HSV SARA SAPORTA-KEATING 3/1/17 Pt Sx onset Presentation Clinical Presentation HSV risk factor(s) HSV results CSF WBC 1 DOL 7 DOL 8 Vesicular rash FOC with active cold sore (DOL2), C/S 2 DOL 7
Neonatal HSV SARA SAPORTA-KEATING 3/1/17 Pt Sx onset Presentation Clinical Presentation HSV risk factor(s) HSV results CSF WBC 1 DOL 7 DOL 8 Vesicular rash FOC with active cold sore (DOL2), C/S 2 DOL 7
Oh SCH It s a neonatal emergency
 trekk.ca 1 1 Oh SCH It s a neonatal emergency Emma Burns, MD, FRCPC IWK Health Centre 2 1 Objectives Critically ill neonate approach and tips Stay on time! Thanks to: Shannon MacPhee, Mike Young, Jon Cherry,
trekk.ca 1 1 Oh SCH It s a neonatal emergency Emma Burns, MD, FRCPC IWK Health Centre 2 1 Objectives Critically ill neonate approach and tips Stay on time! Thanks to: Shannon MacPhee, Mike Young, Jon Cherry,
5/23/14. Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments
 Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments Andi Marmor, MD, MSEd Associate Professor, Pediatrics University of California,
Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments Andi Marmor, MD, MSEd Associate Professor, Pediatrics University of California,
Initial Management of Suspected Encephalitis. Dr Ruth Palmer Consultant Microbiologist
 Initial Management of Suspected Encephalitis Dr Ruth Palmer Consultant Microbiologist CNS infections are urgent and important Mortality is significant recovery is slow and and post infection deficits occur
Initial Management of Suspected Encephalitis Dr Ruth Palmer Consultant Microbiologist CNS infections are urgent and important Mortality is significant recovery is slow and and post infection deficits occur
Real Cases: Bad Outcomes
 Real Cases: Bad Outcomes Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Real Cases: Bad Outcomes Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
SHASTA COUNTY Health and Human Services Agency
 FROM: 530 229 8447 TO: 15302293984 08/06/14 12:30 Pg 1 of 5 especially SHASTA COUNTY Health and Human Services Agency Public Health 2650RreslauerWay Redding, CA 96001-4297 (530) 229-8484 FAX (530) 225-3743
FROM: 530 229 8447 TO: 15302293984 08/06/14 12:30 Pg 1 of 5 especially SHASTA COUNTY Health and Human Services Agency Public Health 2650RreslauerWay Redding, CA 96001-4297 (530) 229-8484 FAX (530) 225-3743
EPG Clinical Guidelines
 Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Neurological Emergencies
 Neurological Emergencies S. Andrew Josephson MD C. Castro-Franceschi and G. Mitchell Endowed Chair Vice Chairman, Parnassus Programs Director, Neurohospitalist Program Medical Director, Inpatient Neurology
Neurological Emergencies S. Andrew Josephson MD C. Castro-Franceschi and G. Mitchell Endowed Chair Vice Chairman, Parnassus Programs Director, Neurohospitalist Program Medical Director, Inpatient Neurology
Fevers and Seizures in Infants and Young Children
 Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Human Herpes Virus-6 Limbic Encephalitis
 Case Studies [1] March 19, 2013 Case history: A 32-year-old Caucasian female with newly diagnosed acute myeloid leukemia (AML) was treated with induction chemotherapy and attained complete remission. She
Case Studies [1] March 19, 2013 Case history: A 32-year-old Caucasian female with newly diagnosed acute myeloid leukemia (AML) was treated with induction chemotherapy and attained complete remission. She
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 3/12/2011 Radiology Quiz of the Week # 11 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 3/12/2011 Radiology Quiz of the Week # 11 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
11/9/2012. Group B Streptococcal Infections: Consensus and Controversies. Prevention of Early-Onset GBS Disease in the USA.
 Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Evidence-based Management of Fever in Infants and Young Children
 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Symptoms of meningism and raised numbers of cells in the CSF with a sterile bacterial culture.
 Table 1. Definitions. Meningism Meningitis Sepsis Severe sepsis Septic shock Meningococcal sepsis Invasive meningococcal disease (IMD) Encephalitis Meningoencephalitis Aseptic Meningitis Symptoms associated
Table 1. Definitions. Meningism Meningitis Sepsis Severe sepsis Septic shock Meningococcal sepsis Invasive meningococcal disease (IMD) Encephalitis Meningoencephalitis Aseptic Meningitis Symptoms associated
Neonatal Herpes Infection: Case Report and Discussion
 BRIEF REPORT Neonatal Herpes Infection: Case Report and Discussion Jordan C. White, MD, and Susanna R. Magee, MD, MPH Neonatal herpes simplex virus (HSV) infections are often life-threatening. Although
BRIEF REPORT Neonatal Herpes Infection: Case Report and Discussion Jordan C. White, MD, and Susanna R. Magee, MD, MPH Neonatal herpes simplex virus (HSV) infections are often life-threatening. Although
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
Burrowing Bugs in a 5 week-old that Mite be Difficult to Diagnosis
 Burrowing Bugs in a 5 week-old that Mite be Difficult to Diagnosis Farbod Bahadori-Esfahani,MD Pediatrics LSU Health Shreveport Louisiana Chapter AAP Red Stick Potpourri Disclosure I have nothing to disclose
Burrowing Bugs in a 5 week-old that Mite be Difficult to Diagnosis Farbod Bahadori-Esfahani,MD Pediatrics LSU Health Shreveport Louisiana Chapter AAP Red Stick Potpourri Disclosure I have nothing to disclose
Your first patient of the day
 Your first patient of the day 1 month old male with 2 days of fussiness Decreased stool output for 3 days Poor latch during breastfeeding noted at 3AM on day of arrival to the ED Started spitting up later
Your first patient of the day 1 month old male with 2 days of fussiness Decreased stool output for 3 days Poor latch during breastfeeding noted at 3AM on day of arrival to the ED Started spitting up later
CHILD IN NON - TRAUMATIC COMA
 May / 2018 PELC / SLCP 1 CHILD IN NON - TRAUMATIC COMA PELS May / 2018 PELC / SLCP 2 Objectives Recognize depressed mental status Know the causes of depressed mental status in children Assessment and workup
May / 2018 PELC / SLCP 1 CHILD IN NON - TRAUMATIC COMA PELS May / 2018 PELC / SLCP 2 Objectives Recognize depressed mental status Know the causes of depressed mental status in children Assessment and workup
CNS INFECTIONS 1 Acute meningitis
 Definition CNS INFECTIONS 1 Acute meningitis DR. BADRI PAUDEL Bacterial meningitis is a medical emergency. Meningitis is an acute infection within the subarachnoid space. usually secondary bacteremia or
Definition CNS INFECTIONS 1 Acute meningitis DR. BADRI PAUDEL Bacterial meningitis is a medical emergency. Meningitis is an acute infection within the subarachnoid space. usually secondary bacteremia or
Case 3: what grew? BA Gram stain morphology Mucoid colonies on BA
 Case 3: what grew? BA Gram stain morphology Mucoid colonies on BA 43 Case 3: probability split! Gram variable, grows on BA, MAC, barely on CHOC Oxidase positive Vitek: probability split, Acinetobacter
Case 3: what grew? BA Gram stain morphology Mucoid colonies on BA 43 Case 3: probability split! Gram variable, grows on BA, MAC, barely on CHOC Oxidase positive Vitek: probability split, Acinetobacter
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS. All children with suspected or confirmed meningitis
 GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
Neutropenic Fever. CID 2011; 52 (4):e56-e93
:e56-e93") Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Cerebrospinal Fluid Glucose and Protein in Disposition and Treatment Decisions
 298 BRIEF REPORTS Givens et al. CSF GLUCOSE AND PROTEIN Cerebrospinal Fluid Glucose and Protein in Disposition and Treatment Decisions Routine laboratory analysis performed when bacterial meningitis is
298 BRIEF REPORTS Givens et al. CSF GLUCOSE AND PROTEIN Cerebrospinal Fluid Glucose and Protein in Disposition and Treatment Decisions Routine laboratory analysis performed when bacterial meningitis is
RESEARCH ARTICLE IS LUMBAR PUNCTURE ALWAYS NECESSARY IN THE FEBRILE CHILD WITH CONVULSION?
 RESEARCH ARTICLE IS LUMBAR PUNCTURE ALWAYS NECESSARY IN THE FEBRILE CHILD WITH CONVULSION? MR. Salehi Omrani MD¹, MR. Edraki MD 2, M. Alizadeh MD 3 Abstract: Objective Febrile convulsion is the most common
RESEARCH ARTICLE IS LUMBAR PUNCTURE ALWAYS NECESSARY IN THE FEBRILE CHILD WITH CONVULSION? MR. Salehi Omrani MD¹, MR. Edraki MD 2, M. Alizadeh MD 3 Abstract: Objective Febrile convulsion is the most common
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
From. The Department of Pediatrics Dr. Mehtas Hospital
 From The Department of Pediatrics Dr. Mehtas Hospital Case history A 12 yr old girl : Fever 5 days Redness of eyes & erythematous rashes over the body for 2 days Past: Febrile fits at 9 mo. Of age Afebrile
From The Department of Pediatrics Dr. Mehtas Hospital Case history A 12 yr old girl : Fever 5 days Redness of eyes & erythematous rashes over the body for 2 days Past: Febrile fits at 9 mo. Of age Afebrile
Rebecca T Slagle, MN, APRN, NNP-BC. Speak up!!
 Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Practical Approaches to Medical Necessity
 Practical Approaches to Medical Necessity CAROLYN AVERY, CPC, CEMC CAROLYN AVERY & ASSOCIATES, PC ROBERT OSSOFF DMD, MD, CHC ASSISTANT VICE CHANCELLOR FOR COMPLIANCE &CORPORATE INTEGRITY VANDERBILT MEDICAL
Practical Approaches to Medical Necessity CAROLYN AVERY, CPC, CEMC CAROLYN AVERY & ASSOCIATES, PC ROBERT OSSOFF DMD, MD, CHC ASSISTANT VICE CHANCELLOR FOR COMPLIANCE &CORPORATE INTEGRITY VANDERBILT MEDICAL
Fever in Young Infants 7 90 days of age
 Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
Fever in children aged less than 5 years
 Fever in children aged less than 5 years A fever is defined as a temperature greater than 38 degrees celsius Height and duration of fever do not identify serious illness. However fever in children younger
Fever in children aged less than 5 years A fever is defined as a temperature greater than 38 degrees celsius Height and duration of fever do not identify serious illness. However fever in children younger
PRESENTATION OF INFECTIONS COEXISTENCE IN AN HIV+ PATIENT
 PRESENTATION OF INFECTIONS COEXISTENCE IN AN HIV+ PATIENT Piddubna Anna Sumy State University Department of Infectious Diseases and Epidemiology Sumy Ukraine Patient history Complaints Patient Sex Male
PRESENTATION OF INFECTIONS COEXISTENCE IN AN HIV+ PATIENT Piddubna Anna Sumy State University Department of Infectious Diseases and Epidemiology Sumy Ukraine Patient history Complaints Patient Sex Male
A39-year-old man presented to the emergency
 CLINICAL CASE OF THE MONTH A 39-Year-Old Man with Acute Mental Status Changes Emily D. Billingsley, MD; Allison Hovland, BS; Demetrio Agcaoili, MD; David Long, MD; and David Borne, MD Article Editor: Fred
CLINICAL CASE OF THE MONTH A 39-Year-Old Man with Acute Mental Status Changes Emily D. Billingsley, MD; Allison Hovland, BS; Demetrio Agcaoili, MD; David Long, MD; and David Borne, MD Article Editor: Fred
FEVER. What is fever?
 FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
Mousa Suboh. Zaid Emad. Anas Abu -Humaidan
 1 Mousa Suboh Zaid Emad 1 P a g e Anas Abu -Humaidan In this lecture we will talk about the microbiology of the central nervous system The central nervous system is supposedly sterile, so there is no micro
1 Mousa Suboh Zaid Emad 1 P a g e Anas Abu -Humaidan In this lecture we will talk about the microbiology of the central nervous system The central nervous system is supposedly sterile, so there is no micro
Hot Stuff: The Febrile Child
 Hot Stuff: The Febrile Child Dr. Shannon MacPhee, Department of Emergency Medicine, Division Head Pediatric Emergency Medicine. IWK Health Centre. Dalhousie University November 2017 Know when to suspect
Hot Stuff: The Febrile Child Dr. Shannon MacPhee, Department of Emergency Medicine, Division Head Pediatric Emergency Medicine. IWK Health Centre. Dalhousie University November 2017 Know when to suspect
SEMINAR ON ACUTE BACTERIAL MENINGITIS AND ANTI MICROBIALS IN NEURO SURGERY. Presented By : DR. ROHIT K GOEL
 SEMINAR ON ACUTE BACTERIAL MENINGITIS AND ANTI MICROBIALS IN NEURO SURGERY. Presented By : DR. ROHIT K GOEL ACUTE BACTERIAL MENINGITIS ABM is acute purulent infection in the subarachnoid space It is associated
SEMINAR ON ACUTE BACTERIAL MENINGITIS AND ANTI MICROBIALS IN NEURO SURGERY. Presented By : DR. ROHIT K GOEL ACUTE BACTERIAL MENINGITIS ABM is acute purulent infection in the subarachnoid space It is associated
Approach to the critically ill patient with advanced HIV in low resource settings. Sebastian Albus, MD MSF, Operational Center Bruxelles
 Approach to the critically ill patient with advanced HIV in low resource settings Sebastian Albus, MD MSF, Operational Center Bruxelles why You should be this guy. instead of that guy ME USFR, Guinea-Conakry
Approach to the critically ill patient with advanced HIV in low resource settings Sebastian Albus, MD MSF, Operational Center Bruxelles why You should be this guy. instead of that guy ME USFR, Guinea-Conakry
Bacteria: Scarlet fever, Staph infection (sepsis, 4S,toxic shock syndrome), Meningococcemia, typhoid Mycoplasma Rickettsial infection
, Meningococcemia, typhoid Mycoplasma Rickettsial infection") Exanthematous Fever objectives FEVER WITH RASH 1 Determine the feature of skin rashes 2 Enumerate the most common causes of skin rashes in children (measles, chicken pox, rubella,erythema infectiosum,
Exanthematous Fever objectives FEVER WITH RASH 1 Determine the feature of skin rashes 2 Enumerate the most common causes of skin rashes in children (measles, chicken pox, rubella,erythema infectiosum,
! Other health care professionals working with pa,ents and their families may also find this program of interest.
 ! This presenta,on will take approximately one hour to complete.! This program is designed for primary care physicians.! Other health care professionals working with pa,ents and their families may also
! This presenta,on will take approximately one hour to complete.! This program is designed for primary care physicians.! Other health care professionals working with pa,ents and their families may also
SELECTED INFECTIONS ACQUIRED DURING TRAVELLING IN NORTH AMERICA. Lin Li, MD August, 2012
 SELECTED INFECTIONS ACQUIRED DURING TRAVELLING IN NORTH AMERICA Lin Li, MD August, 2012 Case 1 32 year old male working in Arizona; on leave back in Singapore Presented to hospital A for fever x (7-10)
SELECTED INFECTIONS ACQUIRED DURING TRAVELLING IN NORTH AMERICA Lin Li, MD August, 2012 Case 1 32 year old male working in Arizona; on leave back in Singapore Presented to hospital A for fever x (7-10)
Panel Discussion: What s New with DRGs and ICD?
 Panel Discussion: What s New with DRGs and ICD? Moderator: Angie Comfort, RHIA, CDIP, CCS, CCS-P Thilo Koepfer, MD Wilbur Lo, MD, CDIP, CCA Objectives Get updated on the current status of ICD- 11 IR-DRG
Panel Discussion: What s New with DRGs and ICD? Moderator: Angie Comfort, RHIA, CDIP, CCS, CCS-P Thilo Koepfer, MD Wilbur Lo, MD, CDIP, CCA Objectives Get updated on the current status of ICD- 11 IR-DRG
Periodic and Rhythmic Patterns. Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina
 Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Neonatal Meningoencephalitis caused by Herpes Simplex Virus Type 2
 Case Report Korean J Pediatr Infect Dis 2014;21:150-156 DOI: http://dx.doi.org/10.14776/kjpid.2014.21.2.150 ISSN 1226-3923 (print) ISSN 2289-0343 (online) Neonatal Meningoencephalitis caused by Herpes
Case Report Korean J Pediatr Infect Dis 2014;21:150-156 DOI: http://dx.doi.org/10.14776/kjpid.2014.21.2.150 ISSN 1226-3923 (print) ISSN 2289-0343 (online) Neonatal Meningoencephalitis caused by Herpes
Narong Auervitchayapat,MD MD., Assist Prof Department of Pediatrics Faculty of Medicine KKU
 Narong Auervitchayapat,MD MD., Assist Prof Department of Pediatrics Faculty of Medicine KKU 5 common diseases:- 1. Bacterial meningitis 2. Tuberculous meningitis 3. Aseptic meningitis 4. Viral encephalitis
Narong Auervitchayapat,MD MD., Assist Prof Department of Pediatrics Faculty of Medicine KKU 5 common diseases:- 1. Bacterial meningitis 2. Tuberculous meningitis 3. Aseptic meningitis 4. Viral encephalitis
PAEDIATRIC ACUTE CARE GUIDELINE. Herpes Stomatitis
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Herpes Stomatitis Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Herpes Stomatitis Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read
Pet Pigs and Pyrexia
 Pet Pigs and Pyrexia 7 th Annual SHM Iowa Chapter Conference Dianna Edwards, MD Hospitalist UnityPoint Health- St. Luke s Cedar Rapids No disclosures 10/29/2016 HPI: 6/2016 45 yo male with OSH ED with
Pet Pigs and Pyrexia 7 th Annual SHM Iowa Chapter Conference Dianna Edwards, MD Hospitalist UnityPoint Health- St. Luke s Cedar Rapids No disclosures 10/29/2016 HPI: 6/2016 45 yo male with OSH ED with
Laboratory Diagnosis of Central Nervous System Infections in Children
 Laboratory Diagnosis of Central Nervous System Infections in Children R. Selvarangan. BVSc, PhD, D(ABMM). Professor, UMKC-SOM Director, Microbiology Laboratory Children's Mercy Hospital Kansas City, MO
Laboratory Diagnosis of Central Nervous System Infections in Children R. Selvarangan. BVSc, PhD, D(ABMM). Professor, UMKC-SOM Director, Microbiology Laboratory Children's Mercy Hospital Kansas City, MO
Central Nervous System Infection
 Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
BODY FLUID ANALYSIS. Synovial Fluid. Synovial Fluid Classification. CLS 426 Urinalysis and Body Fluid Analysis Body Fluid Lecture Session 1
 BODY FLUID ANALYSIS Synovial Fluid Serous fluids the 3 P s Peritoneal Pleural Pericardial Cerebrospinal Fluid Karen Keller, MT(ASCP), SH Synovial Fluid Lubricant and sole nutrient source of joint. Normal
BODY FLUID ANALYSIS Synovial Fluid Serous fluids the 3 P s Peritoneal Pleural Pericardial Cerebrospinal Fluid Karen Keller, MT(ASCP), SH Synovial Fluid Lubricant and sole nutrient source of joint. Normal
Nottingham Children s Hospital
 Meningitis and Encephalitis Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Guideline for the assessment
Meningitis and Encephalitis Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Guideline for the assessment
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital
 Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Disclaimer. This is a broad survey and cannot cover all differential diagnoses or each condition in thorough detail
 Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do