Diagnosis of MDR TB Neha Shah, MD, MPH
|
|
|
- Conrad Powers
- 5 years ago
- Views:
Transcription
1 TB Nurse Case Management Lisle, Illinois April 27-28, Diagnosis of MDR TB Neha Shah, MD, MPH April 27, 2010 Drug Resistant TB Neha Shah MD MPH Centers for Disease Control and Prevention Division of Tuberculosis Elimination Chicago Department of Health "The findings and conclusions in this presentation are those of the author(s) and do not necessarily represent the views of the Centers for Disease Control and Prevention/the Agency for Toxic Substances and Disease Registry." 1



2 Multi-drug Resistant TB MDR 3 MDR TB is a manmade problem.. It is costly, deadly, debilitating, and the biggest threat to our current TB control strategies. 2


3 Drug-Resistant TB Primary Resistance Secondary Resistance Caused by person-to-person transmission of drug-resistant organisms Develops during TB treatment: Patient was not given appropriate treatment regimen OR Patient did not follow treatment regimen as prescribed 6 3
 TB")
4 Drug Resistant TB Multi-drug resistant TB (MDR) Resistant to INH AND Rifampin Pre-XDR TB Resistant to INH and Rifampin AND EITHER Resistance to any fluroquinolone OR Resistant to one of the 2nd line injectables 7 Extensively Drug Resistant (XDR) TB 8 4
5 Epidemiology Outline Pathogenesis Laboratory Resources Management and Treatment Infection control Case studies 9 Epidemiology 10 5

6 Distribution of proportion of MDR- TB among new TB cases, Argentina Armenia Azerbaijan Australia Bangladesh Botswana Brazil Canada Chile Czech Rep. Ecuador Countries with XDR-TB confirmed cases as of June 2008 Italy Japan Latvia Lesotho Lithuania Mexico Moldova Mozambique Namibia China, Hong Kong SAR Netherlands Nepal Russian Fed. Slovenia The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the WHO co oncerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimita ation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. WHO All rights reserved Estonia France Georgia Germany Ireland India Norway Peru Philippines Poland Portugal Rep of Korea South Africa Spain Swaziland Sweden Thailand UK Islamic Rep. of Iran USA Ukraine Israel Romania Vietnam Based on information provided to WHO Stop TB Department - June
7 Primary Anti-TB Drug Resistance United States, * 10 % Resistant Isoniazid MDR TB *Updated as of May 20, Note: Based on initial isolates from persons with no prior history of TB. No. of Cases Primary MDR TB United States, * Percentage No. of Cases Percentage *Updated as of May 20, Note: Based on initial isolates from persons with no prior history of TB. 7


8 Have germs, will travel Migrating populations in the 1990s Compared 4 x to increase , in volume four-fold as increase compared in to migration Source: Population Action International Primary Isoniazid Resistance in U.S.-born vs. Foreign-born Persons, United States, * % Resistant U.S.-born Foreign-born *Updated as of May 20, Note: Based on initial isolates from persons with no prior history of TB. 8
9 Primary MDR TB in U.S.-born vs. Foreignborn Persons, United States, * 3 % Resistant U.S.-born Foreign-born *Updated as of May 20, Note: Based on initial isolates from persons with no prior history of TB XDR TB Case Count defined on Initial DST by Year, * Case Count Year of Diagnosis Drug susceptibility test. *Reported incident cases as of May 20,
10 XDR TB counted cases, * XDR TB Cases (Initial DST) by Race/Ethnicity XDR TB Cases (Initial DST) in U.S.- born vs. Foreign-born Persons Black, 21% Asian, 21% Unknown, 2% White, 21% Hispanic, 35% U.S.-born 17 (65%) Foreign-born 9 (35%) + Two cases of unknown origin (25%) 15 (75%) 19 XDR TB Cases in the United States (Initial DST), * NYC 16 New Jersey * Preliminary data- not for distribution 20 10
11 Number of TB drug resistant cases, Chicago Total Cases INH R (RIF S) RIF R (INH S) 15 (4.9%) 16 (4.9%) 18 (6.3%) 19 (7.3%) 17 (7.9%) 19 (9.4%) (0%) (0%) (0%) (0.8%) (0.5%) (1%) MDR 2 (0.6%) 0 (0%) 0 (0%) 1 (0.4%) 1 (0.5%) 1 (0.5%) 21 Pathogenesis of drugresistant TB 22 11
12 Pathogenesis TB drug resistance Spontaneous mutations occur naturally Occur by chance alone Do not necessarily depend on prior drug exposure Are present in wild type TB isolates 23 Spontaneous mutations develop as bacilli proliferate to >10 8 Drug Mutation Rate Rifampin 10-8 Isoniazid 10-6 Pyrazinamide
13 Drug-resistant mutants in large bacterial population Multidrug therapy: No bacteria resistant to all 3 drugs INH RIF PZA Monotherapy: INH-resistant bacteria proliferate INH 25 INH resistant bacteria multiply l to large numbers INH Spontaneous mutations develop as bacilli proliferate to >10 8 INH RIF INH mono-resist. mutants killed, RIF-resist. mutants proliferate MDR TB 26 13
14 Low Rifabutin Drug Levels Associated with Rifampin Resistance Pharmokinetic evaluation of HIV+ patients with rifabutin (Rifabutin 300mg/INH 300mg daily Patients with treatment failure or relapse with acquired rifamycin resistance had significantly lower rifabutin levels measured by area under curve Patients also had significantly lower INH levels Acquired Rifamycin Resistance USPHS 23 INH + rifabutin twice weekly in continuation 169 patients enrolled 3 treatment failures + 6 relapses; 9/169 (5.3%) 8/9 (89%) acquired rifamycin resistance Risk factors for ARR: Twice weekly RX during first 2 months Low CD4 CD4 < 100: 9/73 (12%) CD4 > 100: 0/65 (0%)» Burman. Am J Respir Crit Care Med
15 What Situations Contribute to Drug Resistant TB? Individual level Treatment errors Missed opportunities for treatment of contacts Public health policy TB in immigrants, refugees, foreign born visitors and students Poor infection control (especially developing countries) Lack of policies to deal with untreatable patients Causes of Inadequate TB Treatment WHO 2006 Drug Resistant TB 15
16 Who is at risk for MDR TB? Foreign-born HIV+/IVDU History of previous TB treatment History of exposure to MDR-TB case TB treatment failures or interruptions 31 Diagnosis of MDR TB 32 16
17 Role of the Laboratory Detect drug resistance to enable clinician to design effective multidrug regimen Initial M. tuberculosis isolate tested against primary drugs INH, RIF, PZA, EMB For Rif-R isolates, test secondary drugs as needed 33 FQ, AMI, KAN, CAP Reasons for Discordant DST Results Differential growth kinetics Different inoculation methods Different methods or media Cross-contamination Transcription, labeling li errors Problem strains and drugs 34 17
 *CDC unpublished data. J. Ridderhof, P.")
18 Difficult Strains Strains sent to >100 laboratories for analysis Resistant t Strains Agree Disagree Rifampin (n=19) 16 3 Isoniazid (n=40) Strain INH-R RIF-R 1 31/88 (35%) 106/ /112 74/117 (62%) *CDC unpublished data. J. Ridderhof, P. Angra 35 Drug Susceptibility Testing Every confirmed case gets susceptibility testing Tests should be repeated if: Patient has positive culture after 3 Drug susceptibility testing on solid media months of treatment OR Patient does not get better 36 18
19 Treatment and Management 37 Principles of Drug Resistant Tuberculosis Standard of care always exclude active tuberculosis before treating LTBI Avoid use of a single TB drug Standard of care start with 4 drugs INH resistance common ~ 7 8% PZA does not protect rifampin Ethambutol will protect rifampin if INH resistance 19
20 Why is MDR so challenging? Treatment of case Less effective, toxicity and side effects <80% cure Higher relapse rates (30 40%) Unclear prophylaxis for contacts Prolonged infectiousness Costly 39 Principles INH resistant treatment Active cases Rifampin, EMB, PZA Low level INH resistant can be given INH No data on clinical significance 6 9 months Add fluroquinolone if extensive disease or immunosuppression Contacts: Rifampin 40 20
21 Principles of Rifampin resistant treatment Rifmapin most important drug in regimen Poor outcomes Need as much attention as MDR cases Treatment options INH, EMB, PZA, Levofloxacin x 12 months; +/- Injectable x 2 months At least months 41 Protecting Rifampin Rifampin single most important TB drug If INH resistant, EMB will protect Rifampin PZA Not active in cavities and rapidly growing lesions Does not protect Rifampin Prevent relapse Shortens therapy duration Mostly for dormant bugs 42 21
22 MDR TB drug options Injectables Streptomycin Amikacin Kanamycin Capreomycin Fluoroquinolones Levofloxacin Moxifloxacin Oral meds PAS Cycloserine Ethionamide Third line Linezolid Imipenem Agumentin Macrolides 43 Principles for MDR treatment Seek consultation with MDR-TB expert Use at least 3 previously unused drugs Proven or suspected to be sensitive to Any first lines with proven susceptibility 44 22
23 Principles for MDR treatment Initially, one drug should be bactericidal injectable Continue injectable 6-12 months after culture conversion Duration: months after conversion of culture Monitor closely for side effects (of which there are many) 45 Principles for MDR treatment NEVER add a single drug to a failing regimen If culture still positive, add 2 more drugs Daily DOT REQUIRED throughout entire treatment course 46 23
24 Building a MDR treatment regimen Step 1 Begin with first-line agents to which isolate susceptible ADD Fluoroquinolone AND Use any One of One of available PLUS these PLUS these First-line drugs Fluoroquinolones Injectable agents Amikacin Pyrazinamide Gatifloxacin Capreomycin Ethambutol Levofloxacin Streptomycin Moxifloxacin Kanamycin Injectable based on susceptibilities Principals of Treatment and Management of MDR TB Levofloxin or Moxifloxin Both highly hl bactericidal id Both well absorbed Avoid calcium and magnesium containing antacids and supplements, multivitamins, iron, enteral supplements, sucralfate Good penetration to all tissue sites No need to decrease dose of moxifloxin in renal insufficiency 24
25 Principals of Treatment and Management of MDR TB Which fluoroquinolone? Levofloxin: 750mg/day Extensive experience with long term use and pushing drug levels to mg/day Peak level at 12 Moxifloxin: 400mg/day Early bactericidal activity rivals rifampin, potentially greater than levofloxin Peak level at 4 Prolonged half life Principals of Treatment and Management of MDR TB Which injectable? All are bactericidal Streptomycin: document susceptibility, more auditory toxicity, less renal Amikacin: easy to get drug levels Capreomycin: smaller volume if IM injection planned Toxicity depends on total dose 15mg/kg 5 x/week first 4-6 months 15mg/kg 3 x/week next 6 8 months Attempt to reach peak serum level of 25 Dual injectable therapy? (Capreomycin and Amikacin) When extensive drug resistance and extensive disease 25
26 Building a MDR Treatment Regimen Step 2 Add second-line drugs until you have 4-6 drugs the isolate is susceptible to (and preferably which have not been used to treat the patient previously) Pick one or more of these Oral second-line drugs Cycloserine Ethionamide PAS Building a MDR Treatment Regimen Step 3 If there are not 4-6 drugs available in the above categories, consider thirdline drugs in consultation with an MDR-TB expert Consider use of these Clofazimine Linezolid Amoxicillin/ clavulanate Third-line drugs Imipenem Macrolides High-dose Isoniazid 26
27 When to start treatment? Wait to identify enough drugs to constitute an appropriate regimen VS Empirically start enough drugs to cover for unsuspected additional resistance 53 When to start treatment? Consider how sick patient is HIV positive patients should be started on treatment immediately Are others still exposed? At all costs avoid creating a more resistant bug 54 27
28 Ensure Toxicity Monitoring Ethionamide and PAS TSH (baseline, Q 2-3 monthly); monthly LFTs Severe nausea and vomiting Better tolerated if slowly ramped up May require premed with anti-emetic Non-caffeinated carbonated beverage and soda crackers may help PAS check serum electrolytes and CBC must give Paser granules with acidic food/drink Ensure Toxicity Monitoring Fluoroquinolones (levofloxacin, moxifloxacin) No specific laboratory tests Monitor for signs of acute tendon rupture QT prolongation can occur; consider obtaining baseline EKG Linezolid CBC (weekly initially then monthly if stable) Monitor for c/o optic and/or peripheral neuropathy 28
29 Ensure Toxicity Monitoring Aminoglycosides and polypeptides Monthly assess: Hearing (Audiogram) Vestibular function (Rhomberg, past-to-point) Serum electrolytes (including Ca+ and Mg++) Serum creatinine Cycloserine Weekly depression monitoring Serum drug level to ensure within therapeutic range Monitor Clinical Response Bacteriology 3 sputa prior to treatment initiation Weekly sputum until smear negative Monthly throughout treatment; at Rx completion TB Symptoms Weekly, noting improvements/worsening of symptoms (cough, weight, fever, etc.) Radiology Every 3 6 months throughout treatment and at completion of treatment 29
30 Cost of MDR Treatment Capreomycin 1gm IV TIW x6 months 2500 Levofloxacin 740mg po daily x 2 years Ethionamide 500mg po daily x 2 years 5500 Cycloserine 500mg po daily x 2 years 8200 PAS 4gm BID x 2 years 6500 Ehtambutol 800mg daily x 2 years 5000 Vit B6 50mg daily x 2 years 40 $39,340 Ranges from $28,217 - $1,278, Address Other Medical Issues If patient has HIV, coordinate management Optimize nutrition consider nutritional consultation in patients with substantial weight loss, diabetes or substance abuse history Assess for potential drug-drug interactions Dose adjustments may be required in patients with compromised renal function Pregnancy discuss options based on stage of pregnancy; teratogenicity of drugs must be considered 30
31 Address Other Social Issues Cultural and language barriers Substance abuse Incarceration Homelessness Unemployment and migration for work Post-Treatment Monitoring Monitor for a minimum of 2 years following treatment Clinical evaluation quarterly during year 1 Then every 6 months during year 2 31
32 Outcomes 63 Culture conversion California ( ) XDR: 46.7%, 195 days MDR: 87.3%, 98.5 days Germany ( ) XDR: 80% MDR: 87.2% Lativia (2000) MDR 77%, 60 days South Korea ( ) XDR 66% MDR 67% 64 32
33 Fighting TB and HIV We can t fight AIDS unless we do much more to fight TB. Nelson Mandela, International AIDS Conference, Thailand 14 July, Nelson Mandela at 2004 International AIDS Conference Image source: BBC News Online ( Extensively Drug Resistant (XDR) TB Recent Outbreak in Kwazulu Natal, SA 1500 patients evaluated 544 (35%) with TB 995 (65%) without TB 221(41%) MDRTB 323 (59%) Susceptible * Moll A et al, (10%) XDRTB 52 died, All HIV+ died Time to death=16 d 33
34 Factors associated with good treatment outcomes HIV negative Younger age No cavitary lesions Sensitivity to ofloxacin No prior therapy with ofloxacin Few resistant drugs Appropriate therapy Primary disease? Surgery Culture conversion by 3 months 67 Contacts 68 34
35 Management of Contacts End of infectious period when CULTURE negative Few guidelines for contacts of MDR CDC contact guidelines:..estimating risk after exposure to a person with pulmonary TB without lung cavities includes a cut-off of 120 hours of exposure per month This is for non-cavitary disease No recommendations or guidelines for cavitary disease 69 Treatment of MDR Contacts Sparse data on treatment regimens Choose 2 drugs source case is sensitive to Treat for 6 months or observe without treatment HIV and immunocompromised should be strongly gyencouraged to take treatment HIV patients should be treated for 12 months Follow for 2 years with CXR and clinical evaluation 70 35
36 Treatment Outcomes of MDR Contacts Schaaf et al followed 119 children who were contacts to active cases of MDR TB. Sixty-one children were infected (51%) and 14 (12%) had active disease. Two (5%) of 41 children who received preventive therapy developed TB, compared to 13 (20%) who did not (OR 4.97). Schaaf et al. Pediatrics : Treatment Outcomes of MDR Contacts Conover study, during two years of follow-up no further cases of MDR-TB were identified. Preventive regimens were determined by the treating physician and were typically a combination of two of the following EMB PZA Ofloxacin All medications were given by DOT. Conover et al IJTLD 5(1):
37 Case Presentation 73 History of Present Illness On 11/09: 20 year old female presented to OSH with dry cough for 4 months ROS: 15 pound weight loss Occasional hemoptysis No fever or SOB 74 37
38 Additional History Family History: no one previously sick No recent travel Immigrated from Kyrgystan 6/2008 Social History quit smoking 3 months ago No IVDU or EtOH use 75 Additional History Past Medical History: h/o BCG vaccine Work History Working in small, not well ventilated Kabob house Was symptomatic while working there Taking English as Second Language (ESL) classes on weekend 76 38





39 Hospital Admission #1 PE: nontib contributory t HIV: negative CXR: cavitary lesion RUL
40 Hospital Course #1 Sputum: smear negative, culture pending Started on RIPE 11/27/2009 Discharged to follow-up with CDPH 79 Laboratory Results IDPH notifies CDPH of drug susceptibility results 1/8/2010 from OSH specimen INH, Rifampin and PZA resistant Specimen sent to CDC for 2 nd line testing Rapid PCR: sensitive to floroquinolone and injectables Final sensitivities: sensitive all 2 nd line EMB resistant 80 40
41 What would you do? 81 Treatment Management EMB monotherapy for 2 months Consulted with Heartland Stop all medications and wait for 2 nd line results Monitor pt monthly Pt minimal symptoms Feeling better Sputums continue to be positive 82 41


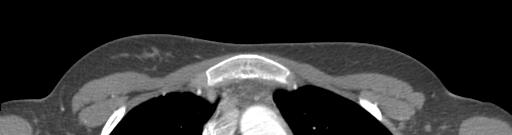
42 Laboratory Results 1/21: rapid PCR testing showed no resistance to quinolone and injectables 2/4: IDPH reports EMB resistance on different specimen using PCR 2/16: Resistance: INH (high level), RIF, EMB, STR, PZA, and rifabutin Sensitive: Kan, AMik, Cap, ethionamide, PAS, and FQ 83 Hospitalization #2 Admitted to Stroger 2/22/2010 Repeat CXR and CT 84 42




43 85 Hospitalization #2 2/23: PAS, Ethionamide, Moxifloxacin, Amikacin, Cycloserine 2/23: sputum positive Tolerating meds well 86 43
44 Contacts 3 roommates 2 TST positive All 3 QFN-gold negative 1 boyfriend: currently QFN-gold and symptom negative 2 nd screening pending culture conversion 87 Institutional Investigation ESL class Restaurant 88 44


45 Patient feeling better Sputums 3/15 rare 3/17 negative 3/31 rare Still not able to return to school or work yet CXR improving Current Status 89 Other concerns Incentives Apartment subsidized Medications free from Stroger No fly list Concern of flying Contagious Patient non-complaint No good way to get off list Parents: Concerned daughter getting appropriate care and support Turmoil in home country 90 45
46 Challenges Almost all contacts foreign born with BCG No great treatment option for contacts Small concern flight risk No treatment for 2 months Side effects of medications Multiple jurisdictions 91 Summary MDR and XDR is here Can be treated and cured BUT consult experts first Requires longer duration and more medications with higher side effect profile No great options for contacts Never add 1 medication to a failing regimen! 92 46
47 Acknowledgements Slides modified from following presentations: ti Dr. Barbara J Seaworth Dr. Karen Lewis Dr. Sundari Mase Multidrug-Resistant Tuberculosis (MDR TB) and Extensively-Drug Resistant (XDR) TB: A Web-Based Seminar 93 Thanks Questions
Drug resistance TB in People Living with HIV: research questions and priorities.
 Drug resistance TB in People Living with HIV: research questions and priorities. Haileyesus Getahun, MD, PhD. Stop TB Department World Health Organisation Geneva, Switzerland Outline of presentation Definition
Drug resistance TB in People Living with HIV: research questions and priorities. Haileyesus Getahun, MD, PhD. Stop TB Department World Health Organisation Geneva, Switzerland Outline of presentation Definition
XDR-TB Extensively Drug-Resistant Tuberculosis. What, Where, How and Action Steps
 XDR-TB Extensively Drug-Resistant Tuberculosis What, Where, How and Action Steps The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever
XDR-TB Extensively Drug-Resistant Tuberculosis What, Where, How and Action Steps The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
What can be done against XDR-TB?
 What can be done against XDR-TB? Dr Matteo Zignol Stop TB Dep. World Health Organization Geneva 16 th Swiss Symposium on tuberculosis Münchenwiler, 22 March 2007 XDR-TB Extensive Drug Resistance XDR =
What can be done against XDR-TB? Dr Matteo Zignol Stop TB Dep. World Health Organization Geneva 16 th Swiss Symposium on tuberculosis Münchenwiler, 22 March 2007 XDR-TB Extensive Drug Resistance XDR =
XDR and MDR TB Urgent Research Priorities. Gerald Friedland MD Yale School of Medicine Nelson R Mandela School of Medicine
 XDR and MDR TB Urgent Research Priorities Gerald Friedland MD Yale School of Medicine Nelson R Mandela School of Medicine The Year of MDR XDR TB CDC, WHO report on global XDR TB XDR TB defined Global distribution
XDR and MDR TB Urgent Research Priorities Gerald Friedland MD Yale School of Medicine Nelson R Mandela School of Medicine The Year of MDR XDR TB CDC, WHO report on global XDR TB XDR TB defined Global distribution
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
4/25/2012. The information on patterns of infection and disease can assist in: Assessing current and evolving trends in TB
 Sindy M. Paul, MD, MPH, FACPM May 1, 2012 The information on patterns of infection and disease can assist in: Assessing current and evolving trends in TB morbidity, including resistance Identifying people
Sindy M. Paul, MD, MPH, FACPM May 1, 2012 The information on patterns of infection and disease can assist in: Assessing current and evolving trends in TB morbidity, including resistance Identifying people
MULTIDRUG- RESISTANT TUBERCULOSIS. Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic
 MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist, NH GEISELMED.DARTMOUTH.EDU GEISELMED.DARTMOUTH.
 The image part with relationship ID rid2 was not found in the file. MDR TB Management Review of the Evolution (or Revolution?) Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist,
The image part with relationship ID rid2 was not found in the file. MDR TB Management Review of the Evolution (or Revolution?) Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist,
Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer
 Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Treatment of Tuberculosis
 Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Global epidemiology of drug-resistant tuberculosis. Factors contributing to the epidemic of MDR/XDR-TB. CHIANG Chen-Yuan MD, MPH, DrPhilos
 Global epidemiology of drug-resistant tuberculosis Factors contributing to the epidemic of MDR/XDR-TB CHIANG Chen-Yuan MD, MPH, DrPhilos By the end of this presentation, participants would be able to describe
Global epidemiology of drug-resistant tuberculosis Factors contributing to the epidemic of MDR/XDR-TB CHIANG Chen-Yuan MD, MPH, DrPhilos By the end of this presentation, participants would be able to describe
6/8/2018 TB TREATMENT. Bijan Ghassemieh, MD Seattle TB Clinical Intensive Disclosures. None
 TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
Management of Multidrug- Resistant TB in Children. Jennifer Furin, MD., PhD. Sentinel Project, Director of Capacity Building
 Management of Multidrug- Resistant TB in Children Jennifer Furin, MD., PhD. Sentinel Project, Director of Capacity Building Objectives To review data on best practices for diagnosis, treatment and prevention
Management of Multidrug- Resistant TB in Children Jennifer Furin, MD., PhD. Sentinel Project, Director of Capacity Building Objectives To review data on best practices for diagnosis, treatment and prevention
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Management of MDR TB. Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore
 Management of MDR TB Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore Outline Global epidemiology of Tuberculosis Epidemiology of Tuberculosis
Management of MDR TB Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore Outline Global epidemiology of Tuberculosis Epidemiology of Tuberculosis
3.1 PHASE 2 OF THE GLOBAL PROJECT
 RESULTS CHAPTER 3 3.1 PHASE 2 OF THE GLOBAL PROJECT (1996 1999) This new report of the Global Project provides data on anti-tuberculosis drug resistance from 58 geographical settings. Of these, 28 provided
RESULTS CHAPTER 3 3.1 PHASE 2 OF THE GLOBAL PROJECT (1996 1999) This new report of the Global Project provides data on anti-tuberculosis drug resistance from 58 geographical settings. Of these, 28 provided
Marcos Burgos, MD has the following disclosures to make:
 Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Laboratory Diagnosis for MDR TB
 Laboratory Diagnosis for MDR TB Neha Shah MD MPH Centers for Disease Control and Prevention Division of Tuberculosis Elimination California Department of Public Health Guam March 07 Objectives Describe
Laboratory Diagnosis for MDR TB Neha Shah MD MPH Centers for Disease Control and Prevention Division of Tuberculosis Elimination California Department of Public Health Guam March 07 Objectives Describe
How Is TB Transmitted? Sébastien Gagneux, PhD 20 th March, 2008
 How Is TB Transmitted? Sébastien Gagneux, PhD 20 th March, 2008 Today s Outline 1) Global spread of Mtb Comparative genomics Phylogeny 2) Transmission of drug-resistant Mtb Fitness assays Molecular epidemiology
How Is TB Transmitted? Sébastien Gagneux, PhD 20 th March, 2008 Today s Outline 1) Global spread of Mtb Comparative genomics Phylogeny 2) Transmission of drug-resistant Mtb Fitness assays Molecular epidemiology
Treatment of Tuberculosis
 TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
Treatment: First Line Drugs TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS TREATMENT: GENERAL PRINCIPLES MECHANISM OF ACTION MID 27
 TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
Research in Tuberculosis: Translation into Practice
 Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Short Course Treatment for MDR TB
 Objectives Short Course Treatment for MDR TB Barbara J Seaworth M.D. Medical Director Heartland National TB Center Professor of Medicine, University of Texas Health Northeast Participants will utilize
Objectives Short Course Treatment for MDR TB Barbara J Seaworth M.D. Medical Director Heartland National TB Center Professor of Medicine, University of Texas Health Northeast Participants will utilize
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
New Drugs, New Treatments, Shorter Regimens
 New Drugs, New Treatments, Shorter Regimens Sarah K. Brode, MD MPH FRCP(C) West Park Healthcare Centre, University Health Network, University of Toronto TB Elimination: Back to Basics November 16, 2016
New Drugs, New Treatments, Shorter Regimens Sarah K. Brode, MD MPH FRCP(C) West Park Healthcare Centre, University Health Network, University of Toronto TB Elimination: Back to Basics November 16, 2016
Global, National, Regional
 Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Management of Drug-resistant Tuberculosis (DR-TB)
") Management of Drug-resistant Tuberculosis (DR-TB) Nitipatana Chierakul Division of Respiratory Disease & Tuberculosis Department of Medicine Faculty of Medicine Siriraj Hospital October 14 th, 2008 Tropical
Management of Drug-resistant Tuberculosis (DR-TB) Nitipatana Chierakul Division of Respiratory Disease & Tuberculosis Department of Medicine Faculty of Medicine Siriraj Hospital October 14 th, 2008 Tropical
Global, National, Regional
 Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
Treatment of Tuberculosis
 Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
The WHO Global Project on anti-tb drug resistance surveillance: background, objectives, achievements, challenges, next steps
 The WHO Global Project on anti-tb drug resistance surveillance: background, objectives, achievements, challenges, next steps Matteo Zignol STOP TB Department World Health Organization TB surveillance and
The WHO Global Project on anti-tb drug resistance surveillance: background, objectives, achievements, challenges, next steps Matteo Zignol STOP TB Department World Health Organization TB surveillance and
Controlling TB in the era of HIV
 Controlling TB in the era of HIV Christy Hanson, PhD, MPH TB Research Advisor Amy Bloom, MD TB/HIV Advisor TB Incidence rates highest in Africa Estimated new TB cases (all forms) per 100 000 population
Controlling TB in the era of HIV Christy Hanson, PhD, MPH TB Research Advisor Amy Bloom, MD TB/HIV Advisor TB Incidence rates highest in Africa Estimated new TB cases (all forms) per 100 000 population
Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health
 Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health C. Robert Horsburgh, Jr. Boston University School of Public Health Background Outline Why does drug resistance threaten
Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health C. Robert Horsburgh, Jr. Boston University School of Public Health Background Outline Why does drug resistance threaten
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
TB Intensive Minneapolis, Minnesota September 23-26, 2008
 TB Intensive Minneapolis, Minnesota September 23-26, 2008 TB in the Foreign-Born Population: Background and Demographic Overview Marge Higgins, LSW September 24, 2008 TB in the Foreign-Born Population
TB Intensive Minneapolis, Minnesota September 23-26, 2008 TB in the Foreign-Born Population: Background and Demographic Overview Marge Higgins, LSW September 24, 2008 TB in the Foreign-Born Population
Pediatric TB Intensive San Antonio, Texas October 14, 2013
 Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
TB in Foreign Born and High Risk Populations
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Updates on the global TB Global TB burden Policy response Treatment approaches
 Ernesto Updates on the global TB Global TB burden Policy response Treatment approaches Ernesto Jaramillo WHO Global TB Programmme World Health Organization, Geneva, Tuberculosis is the leading infectious
Ernesto Updates on the global TB Global TB burden Policy response Treatment approaches Ernesto Jaramillo WHO Global TB Programmme World Health Organization, Geneva, Tuberculosis is the leading infectious
XDR TUBERCULOSIS IN EUROPE EPIDEMIOLOGICAL ASPECTS. Enrico Girardi Unità di Epidemiologia Clinica INMI Spallanzani, Roma. Pag. 1
 XDR TUBERCULOSIS IN EUROPE EPIDEMIOLOGICAL ASPECTS Enrico Girardi Unità di Epidemiologia Clinica INMI Spallanzani, Roma Pag. 1 TB estimated incidence in EUR, 2004 Russian Fed. 12 th among the 22 TB high-burden
XDR TUBERCULOSIS IN EUROPE EPIDEMIOLOGICAL ASPECTS Enrico Girardi Unità di Epidemiologia Clinica INMI Spallanzani, Roma Pag. 1 TB estimated incidence in EUR, 2004 Russian Fed. 12 th among the 22 TB high-burden
Drug Side Effects and Toxicity
 Drug Side Effects and Toxicity Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Toxicity Nausea and vomiting Any Drug Can Cause
Drug Side Effects and Toxicity Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Toxicity Nausea and vomiting Any Drug Can Cause
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Anti Tuberculosis Medications: Side Effects & adverse Events
 Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN,
Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN,
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Tuberculosis Intensive November 17 20, 2015 San Antonio, TX
 Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Tuberculosis in Chicago 2007
 City of Chicago Communicable Disease Information Department of Public Health Richard M. Daley, Mayor May 2008 Terry Mason, MD, FACS, Commissioner www.cityofchicago.org/health/ West Side Center For Disease
City of Chicago Communicable Disease Information Department of Public Health Richard M. Daley, Mayor May 2008 Terry Mason, MD, FACS, Commissioner www.cityofchicago.org/health/ West Side Center For Disease
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
The epidemiology of tuberculosis
 The epidemiology of tuberculosis Tuberculosis Workshop Shanghai, 12-22 May 28 Philippe Glaziou World Health Organization Outline Epidemiology refresher Estimates of tuberculosis disease burden Notifications
The epidemiology of tuberculosis Tuberculosis Workshop Shanghai, 12-22 May 28 Philippe Glaziou World Health Organization Outline Epidemiology refresher Estimates of tuberculosis disease burden Notifications
Diagnosis of drug resistant TB
 Diagnosis of drug resistant TB Megan Murray, MD, ScD Harvard School of Public Health Brigham and Women s Hospital Harvard Medical School Broad Institute Global burden of TB 9 million new cases year 2 million
Diagnosis of drug resistant TB Megan Murray, MD, ScD Harvard School of Public Health Brigham and Women s Hospital Harvard Medical School Broad Institute Global burden of TB 9 million new cases year 2 million
2016 Annual Tuberculosis Report For Fresno County
 206 Annual Tuberculosis Report For Fresno County Cases Rate per 00,000 people 206 Tuberculosis Annual Report Fresno County Department of Public Health (FCDPH) Tuberculosis Control Program Tuberculosis
206 Annual Tuberculosis Report For Fresno County Cases Rate per 00,000 people 206 Tuberculosis Annual Report Fresno County Department of Public Health (FCDPH) Tuberculosis Control Program Tuberculosis
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)
") Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012
 TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
Tuberculosis: The Big Picture And Challenge of Drug-resistance
 5 th APHL National Conference on Laboratory Aspects of Tuberculosis August 11-13, 2008 San Diego, California Tuberculosis: The Big Picture And Challenge of Drug-resistance RADM Kenneth G. Castro, M.D.
5 th APHL National Conference on Laboratory Aspects of Tuberculosis August 11-13, 2008 San Diego, California Tuberculosis: The Big Picture And Challenge of Drug-resistance RADM Kenneth G. Castro, M.D.
Global Perspective on Transmission: Value in Genotype Mapping of Disease Transmission Dynamics
 Global Perspective on Transmission: Value in Genotype Mapping of Disease Transmission Dynamics Neel R. Gandhi, MD Emory Rollins School of Public Health January 17, 2013 Medical Research Council BMJ 1948
Global Perspective on Transmission: Value in Genotype Mapping of Disease Transmission Dynamics Neel R. Gandhi, MD Emory Rollins School of Public Health January 17, 2013 Medical Research Council BMJ 1948
Debbie Onofre, RN, BSN March 18, TB Nurse Case Management March 17 19, 2015 San Antonio, Texas
 Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
International Standards for Tuberculosis Care Barbara J. Seaworth, MD August 22, 2007
 TB Along the US/Mexico Border El Paso, Texas August 22-23, 2007 International Standards for Tuberculosis Care Barbara J. Seaworth, MD August 22, 2007 Barbara J Seaworth MD Medical Director Heartland National
TB Along the US/Mexico Border El Paso, Texas August 22-23, 2007 International Standards for Tuberculosis Care Barbara J. Seaworth, MD August 22, 2007 Barbara J Seaworth MD Medical Director Heartland National
DNA FINGERPRINTING. Barry N. Kreiswirth, PhD Director, PHRI TB Center
 DNA FINGERPRINTING Barry N. Kreiswirth, PhD Director, PHRI TB Center Molecular Epidemiology Local Epidemiology Are M. tuberculosis isolates recovered from localized cases of disease the same or different
DNA FINGERPRINTING Barry N. Kreiswirth, PhD Director, PHRI TB Center Molecular Epidemiology Local Epidemiology Are M. tuberculosis isolates recovered from localized cases of disease the same or different
DRUG SIDE EFFECTS AND TOXICITY
 DRUG SIDE EFFECTS AND TOXICITY Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Objectives After participating in this lecture,
DRUG SIDE EFFECTS AND TOXICITY Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Objectives After participating in this lecture,
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Failure to Implement the Plan to Eliminate TB in the US: Implications in the Era of Declining Resources
 Failure to Implement the Plan to Eliminate TB in the US: Implications in the Era of Declining Resources Sustaining Public Health Capacity in an Age of Austerity Forum on Microbial Threats Board on Global
Failure to Implement the Plan to Eliminate TB in the US: Implications in the Era of Declining Resources Sustaining Public Health Capacity in an Age of Austerity Forum on Microbial Threats Board on Global
Update on Management of
 Update on Management of DR TB Definitions Presumptive MDR-TB A patient suspected of drug-resistant TB, based on RNTCP criteria for submission of specimens for drug-susceptibility testing MDR-TB Case A
Update on Management of DR TB Definitions Presumptive MDR-TB A patient suspected of drug-resistant TB, based on RNTCP criteria for submission of specimens for drug-susceptibility testing MDR-TB Case A
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
Sirturo: a new treatment against multidrug resistant tuberculosis
 Sirturo: a new treatment against multidrug resistant tuberculosis TB is an on-going problem WHO estimated incidence of new TB cases 2009 Global Tuberculosis Control: WHO report 2010. Available at: http://www.who.int/tb/publications/global_report/2010/en/index.html
Sirturo: a new treatment against multidrug resistant tuberculosis TB is an on-going problem WHO estimated incidence of new TB cases 2009 Global Tuberculosis Control: WHO report 2010. Available at: http://www.who.int/tb/publications/global_report/2010/en/index.html
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
TB Nurse Case Management. March 7-9, Diagnosis of TB: Ken Jost Wednesday March 7, 2012
 TB Nurse Case Management San Antonio, Texas March 7-9, 2012 Diagnosis of TB: Laboratory Ken Jost Wednesday March 7, 2012 Ken Jost has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 7-9, 2012 Diagnosis of TB: Laboratory Ken Jost Wednesday March 7, 2012 Ken Jost has the following disclosures to make: No conflict of interests No relevant
Surgery for MDR/XDR Tuberculosis
 Surgery for MDR/XDR Tuberculosis John D. Mitchell, M.D. Davis Endowed Chair in Thoracic Surgery Professor and Chief, General Thoracic Surgery Department of Surgery University of Colorado School of Medicine
Surgery for MDR/XDR Tuberculosis John D. Mitchell, M.D. Davis Endowed Chair in Thoracic Surgery Professor and Chief, General Thoracic Surgery Department of Surgery University of Colorado School of Medicine
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
Utilizing All the Tools in the TB Toolbox
 Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Multidrug-resistant Tuberculosis - World, Europe, Switzerland
 Multidrug-resistant Tuberculosis - World, Europe, Switzerland Magglingen March 23, 2017 peter.helbling@bag.admin.ch Topics Definitions Epidemiology of TB and MDR-TB worldwide Treatment outcome results
Multidrug-resistant Tuberculosis - World, Europe, Switzerland Magglingen March 23, 2017 peter.helbling@bag.admin.ch Topics Definitions Epidemiology of TB and MDR-TB worldwide Treatment outcome results
New TB Medications. National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention New TB Medications Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention New TB Medications Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers
Case presentation. Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD
 Case presentation Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD History of presenting illness 20 Year old woman from Nigeria who came to study at Montgomery in August 2013 About 2 weeks after arriving,
Case presentation Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD History of presenting illness 20 Year old woman from Nigeria who came to study at Montgomery in August 2013 About 2 weeks after arriving,
MDR-TB and HIV co-infection in Eastern Europe. Francis Drobniewski MBBS PhD Professor of Global Health and Tuberculosis
 MDR-TB and HIV co-infection in Eastern Europe Francis Drobniewski MBBS PhD Professor of Global Health and Tuberculosis f.drobniewski@imperial.ac.uk Conflict of interest In the last year I have been a consultant
MDR-TB and HIV co-infection in Eastern Europe Francis Drobniewski MBBS PhD Professor of Global Health and Tuberculosis f.drobniewski@imperial.ac.uk Conflict of interest In the last year I have been a consultant
Antimycobacterial drugs. Dr.Naza M.Ali lec Dec 2018
 Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Substance Abuse and Tuberculosis Springfield, IL April 27, 2011
 5/6/2011 Substance Abuse and Tuberculosis Springfield, IL April 27, 2011 Epidemiology of Substance Abuse and Tuberculosis: Where is the Problem? Debra Stephens, RN, BSN, MPH April 27, 2011 Debra Stephens,
5/6/2011 Substance Abuse and Tuberculosis Springfield, IL April 27, 2011 Epidemiology of Substance Abuse and Tuberculosis: Where is the Problem? Debra Stephens, RN, BSN, MPH April 27, 2011 Debra Stephens,
The Public Health Impact of TB in the Correctional System. Sarah Bur, RN, MPH Federal Bureau of Prisons Infection Prevention and Control Officer
 The Public Health Impact of TB in the Correctional System Sarah Bur, RN, MPH Federal Bureau of Prisons Infection Prevention and Control Officer The Public Health Impact of TB in the Correctional System
The Public Health Impact of TB in the Correctional System Sarah Bur, RN, MPH Federal Bureau of Prisons Infection Prevention and Control Officer The Public Health Impact of TB in the Correctional System
TB Clinical Guidelines: Revision Highlights March 2014
 TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
When Can Isolation Be Discontinued?
 When Can Isolation Be Discontinued? - It Depends on the Patient and the Setting. Masae Kawamura M.D. and Barbara Seaworth M.D. Texas: (800) TEX-LUNG New Jersey: 973-972-3270? HNTC Consultation Line California:
When Can Isolation Be Discontinued? - It Depends on the Patient and the Setting. Masae Kawamura M.D. and Barbara Seaworth M.D. Texas: (800) TEX-LUNG New Jersey: 973-972-3270? HNTC Consultation Line California:
2014 Annual Report Tuberculosis in Fresno County. Department of Public Health
 214 Annual Report Tuberculosis in Fresno County Department of Public Health www.fcdph.org Tuberculosis (TB) is a common communicable disease caused by the bacterium Mycobacterium tuberculosis and occasionally
214 Annual Report Tuberculosis in Fresno County Department of Public Health www.fcdph.org Tuberculosis (TB) is a common communicable disease caused by the bacterium Mycobacterium tuberculosis and occasionally
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Patient History 1. Patient History 2. Social History. The Role of Surgery in the Management of TB. Reynard McDonald, MD & Paul Bolanowski, MD
 Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
The authors assessed drug susceptibility patterns
 Drug Resistance Among Tuberculosis Patients, 1991 and 1992 New York City, CYNTHIA R. DRIVER, RN, MPH THOMAS R. FRIEDEN, MD, MPH ALAN B. BLOCH, MD, MPH IDA M. ONORATO, MD All the authors are with the Division
Drug Resistance Among Tuberculosis Patients, 1991 and 1992 New York City, CYNTHIA R. DRIVER, RN, MPH THOMAS R. FRIEDEN, MD, MPH ALAN B. BLOCH, MD, MPH IDA M. ONORATO, MD All the authors are with the Division
Undetectable = Untransmittable. Mariah Wilberg Communications Specialist
 Undetectable = Untransmittable Mariah Wilberg Communications Specialist Undetectable=Untransmittable PLWH who get and stay undetectable have effectively no risk of transmitting HIV to their sex partners
Undetectable = Untransmittable Mariah Wilberg Communications Specialist Undetectable=Untransmittable PLWH who get and stay undetectable have effectively no risk of transmitting HIV to their sex partners
Responding to a TB Event Bismarck, North Dakota June 24-25, 2008
 Responding to a TB Event Bismarck, North Dakota June 24-25, 2008 TB Epidemiology: Global and State Lynelle Phillips, RN, MPH June 24, 2008 TB Epidemiology Global and State Lynelle Phillips RN MPH Nurse
Responding to a TB Event Bismarck, North Dakota June 24-25, 2008 TB Epidemiology: Global and State Lynelle Phillips, RN, MPH June 24, 2008 TB Epidemiology Global and State Lynelle Phillips RN MPH Nurse
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.