Il ruolo della viremia nel management del paziente HIV. Carlo Federico Perno
|
|
|
- Mervin Copeland
- 6 years ago
- Views:
Transcription




1 Il ruolo della viremia nel management del paziente HIV Carlo Federico Perno 18 giugno 2014

 in order to")

2 All the current guidelines agree that the primary goal of antiretroviral therapy is to suppress HIV RNA maximally (<20 75 copies/ml, depending on the assay used) in order to preserve immunologic function and increase disease-free survival July 2012 October 2013 May, 2014

3 Science 1996 Viral load monitoring and CD4 monitoring should be used together to monitor disease progression, response to therapy, and guide opportunistic infection prophylaxis. Highlight from the XI International AIDS Conference Vancouver July 7 12, 1996.
4 Plasma HIV-1 RNA (Viral Load) Monitoring Pre-treatment viral load level is also an important factor in the selection of an initial ARV regimen because several currently approved ARV drugs or regimens have been associated with poorer responses in patients with high baseline viral load. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents May 2014
5 Plasma HIV-1 RNA (Viral Load) Monitoring Pre-treatment viral load level is also an important factor in the selection of an initial ARV regimen because several currently approved ARV drugs or regimens have been associated with poorer responses in patients with high baseline viral load. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents May 2014 La viremia pre-terapia ha un ruolo importante nel raggiungimento della soppressione virologica. In presenza di valori di viremie pre-terapia particolarmente elevati, il raggiungimento della soppressione virologica può richiedere un tempo più lungo (a volte superiore alle 24 settimane attese), e/o è meno frequente. Linee Guida Italiane sull utilizzo dei farmaci antiretrovirali e sulla gestione diagnostico-clinica delle persone con infezione da HIV-1 Novembre 2013
 to achieve VS (weeks) Probability of VS at 48 weeks >500K 135 23 (21-25) 83% 300K - 500K 102 22 (21-24) 93% 100K - 300K 273 18 (17-20) 93% 30K - 100K 229 15 (14-16) 98% <30K 235")
6 The time to achieve virological undectability and the rate of success at 48 weeks are pre-haart viremia dependent Pre-HAART viremia ranges (copies/ml) No. Median Time (95% CI) to achieve VS (weeks) Probability of VS at 48 weeks >500K (21-25) 83% 300K - 500K (21-24) 93% 100K - 300K (17-20) 93% 30K - 100K (14-16) 98% <30K (9-11) 99% Time (weeks) Santoro MM. Antiv Ther 2013
7 Probability to reach virological rebound Patients having pre-haart viremia >500K copies/ml showed the highest probability of virological rebound (VL>50 copies/ml) by 4 years from the achievement of virological suppression Rebound as the first of 2 consecutive HIV-RNA >50 copies/ml 29% P< Viremia Ranks (cps/ml) Time (years from first date of VL<50 cps/ml) 0-100K K K >500K No. at risk Armenia et al., V ICAR 2013

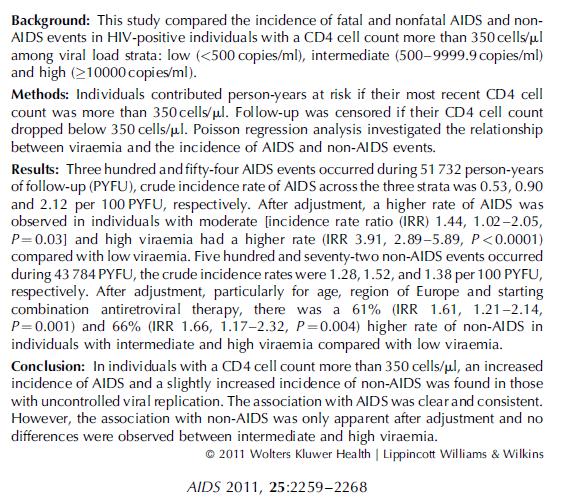
8 Reekie et al., AIDS 2011
9 Adjusted incidence rate ratios for AIDS and non- AIDS events by viral load strata stratified by current CD4 cell count. J Reekie et al., AIDS 2011

10 CROI 2014, abstr # 558
11 Adjusted hazard ratios for the effect of initiation vs. deferring ART on time from seroconversion (SC) to AIDS/death by a) viremia copy years pooling CD4 stratum, b) viremia copy years with CD4<350 cells/mm 3 and c) viremia copy years with CD4 350 cells/mm 3 Pooling CD4 strata, hazard ratios for the effect of initiating ART on time from seroconversion to AIDS/death decreased as VCYyear increased, with a 63% reduced risk of AIDS/death for those initiating ART when VCY exceeded 100,000. At CD4<350 cells/mm 3, there was an overall reduction in the risk of AIDS/death in all VCY groups (all HR < 1) for those initiating vs. deferring ART with no evidence that this benefit varied by VCY (p=0.78). At CD4 350 there was a trend for increasing benefit of initiation vs. deferral with increasing VCY, with the largest benefit seen in the VCY 100,000 c/ml group (HR, 95% CI= 0.56, , p(heterogeneity) = 0.16). Results were qualitatively similar for CD4 strata 500 cells/mm 3. CROI 2014, abstr # 558
12 CID 2011;53:
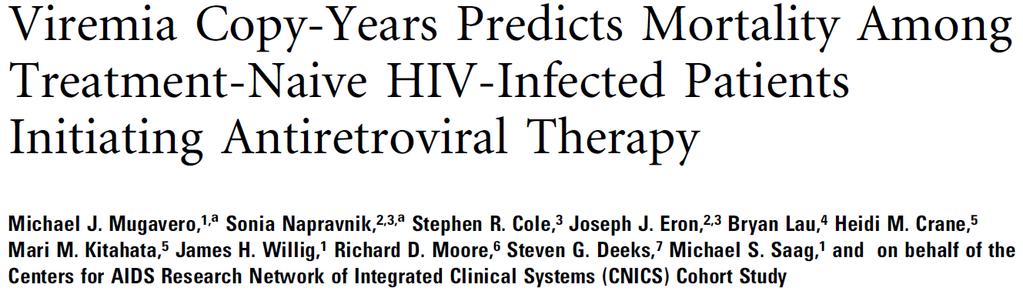
 Mugavero et al.")
13 Cumulative plasma HIV burden, demonstrated prognostic value for allcause mortality among 2027 HIV-infected patients following ART (viral load values prior to 24 weeks of ART initiation were excluded) Mugavero et al., CID 2011;53:

14 CROI 2014, abstr # 291
15 Higher average VL is associated with a higher risk of clinical AIDS/death. SC: seroconversion CROI 2014, abstr # 291
16 Transient low level viremias, with plasma HIV-1 RNA levels in the range of 50 to 400 copies/ml, have been reported to occur in 25 to 40% of adults in whom viral replication appeared to have been suppressed by HAART Greub, G., A. et al. Intermittent and sustained low-level HIV viral rebound in patients receiving potent antiretroviral therapy. AIDS 2002 Havlir, D. V., et al. Prevalence and predictive value of intermittent viremia with combination HIV therapy. JAMA 2001 Sklar, et al. Prevalence and clinical correlates of HIV viremia ( blips ) in patients with previous suppression below the limits of quantification. AIDS 2002
17 Residual viremia reflects the size of the viral reservoir (CD4-associated HIV DNA) during suppressive HAART Relationship between residual plasma viremia and cell-associated HIV DNA Frequencies of CD4 + T cells carrying HIV proviral DNA based on plasma viremia Chun T et al. J Infect Dis. 2011
, especially between 50 and 200 copies/ml, the best management and clinical consequences remain unknown.")
18 Background. The current goal of antiretroviral therapy (ART) is to maintain a suppressed human immunodeficiency virus (HIV) viral load below limits of assay detection. When viral loads remain in low-level viremia (LLV), especially between 50 and 200 copies/ml, the best management and clinical consequences remain unknown. Our objective was to study the long-term impact of persistent LLV on the subsequent risk of virologic failure in a cohort of people living with HIV in Montreal, Canada. Methods. We compared the cumulative incidence of subsequent virologic failure (defined as an HIV RNA viral load of >1000 copies/ml) in patients receiving ART for at least 12 months by following 4 persistence categories (<50, , , and copies/ml) for 6, 9, or 12 months, using Kaplan-Meier analysis. The association between subsequent virologic failure and persistence status were estimated using a Cox proportional hazards model. Results. The cumulative incidence of virologic failure 1 year after having maintained a LLV for 6 months was 22.7% (95% confidence interval [CI], ) for copies/ml, 24.2% (95% CI, ) for copies/ml, and 58.9% (95% CI, ) for copies/ml, compared with 6.6% (95% CI, ) for an undetectable HIV RNA viral load. Even after adjustment for potential confounders, a persistent LLV of copies/ ml for 6 months doubled the risk of virologic failure (hazard ratio, 2.22; 95% CI, ), compared with undetectable viral loads for the same duration. Similar results have been found for persistent LLV of 9 or 12 months. Conclusions. In this cohort, all categories of persistent LLV between 50 and 999 copies/ml were associated with an increased risk of virologic failure. The results shed new light for the management of patients with LLV, especially with regard to LLV of copies/ml. Laprise et al, CID 2013
19 The cumulative incidences of subsequent virologic failure (ie, > 1000 copies/ml) over 5 years, following persistence of LLV was significantly higher for all LLV strata compared to who maintained undetectable HIV load. Laprise et al, CID 2013

20 PNAS 2104
 compartment, particularly in the lymph node.")
 from the LN, ileum, and rectum were performed.")
21 Compared with concentrations in PBMCs, the IC concentration of TFV-DB, FTC-TP, ATV, DRV and EFV was lower in the lymphatic tissue (LT) compartment, particularly in the lymph node. 714 determinations of ARV drug concentrations in plasma and 592 analyte determinations for IC drug concentrations in PBMCs and in mononuclear cells (MNCs) from the LN, ileum, and rectum were performed. Fletcher et al., PNAS 2104

22 2012


23 Resistance to NRTI, NNRTI or PI/r classes in samples collected from January 2008 to December 2012 stratified for plasma viremia ranges Santoro MM et al., CID 2014
24 Jan-11 Feb-11 Mar-11 Mar-11 Apr-11 Jun-11 Aug-11 Oct-11 Nov-11 Jan-12 Feb-12 Apr-12 Jun-12 Jul-12 Oct-12 Feb-13 Jun-13 Sep-13 Jan-14 Apr-14 Clinical Case: ID Patient infected with HIV-1 B subtype Age: 34 Sex: F Risk Factor: Heterosexual 1 ST Seropositivity: November 2010 CDC stage: B2 CD4 cell count (cells/ul) in out GRT JANUARY 2011 VL: 18,391 cps/ml; CD4: 360 cells/µl PR: L63P RT: NONE > cps/ml Other pol mutations PR: K14T L19T RT: K49R K122E D123N I135T I142T T165I D177E, I202V A272P K277R L283I I293V S322A Undetectability threshold Viremia (log copies/ml) February 2011 January 2014 TDF/FTC (TRUVADA) + DRV800/r
25 Nov-09 Dec-09 Feb-10 Jul-10 Sep-10 Dec-10 Apr-11 May-11 Aug-11 Dec-11 Apr-12 Jul-12 Oct-12 Feb-12 Sep-13 Jan-14 Clinical Case: ID 9964 Patient infected with HIV-1 B subtype Age: 41 Sex: M Risk Factor: MSM 1 ST Seropositivity: December 2007 CDC stage: A CD4 cell count (cells/ul) 1100 in out in out in out in out in out 1050 GRT 1000 NOVEMBER GRT NOVEMBER 2009 GRT 2009 GRT SEPTEMBER GRT DECEMBER 2011 PR: 950 L63P PR: L63P PR: PR: L63P L63P PR: L63P 900 > cps/ml RT: 850 NONE RT: NONE RT: NONE RT: NONE RT: NONE Other 800 pol mutations Other pol mutations Other Other pol mutations pol mutations Other pol mutations 750 PR: 700 K14R I15V PR: K14R E35D I15V K70E E35D PR: K70E K14R PR: K14R I15V I15V E35D E35D K70E K70E PR: K14R I15V E35D K70E RT: 650 K49R D123E RT: K49R I135T D123E I135T RT: K49R RT: K49R D123E D123E I135T I135T RT: E29AEG K49R G51W E169D 600 Q207E E169D R211K Q207E F214L R211K E169D F214L E169D Q207E Q207E R211K R211K F214L F214L D123E I135T Q145HQ A324AV 550 I329V A324AV I329V I293IV I293IV I329V I329V E169D Q207E R211K F214L 500 I329L Undetectability threshold , Viremia (log copies/ml) NOV 09 JAN 10 TDF+FTC LPV/r FEB. 10 APR 12 TDF+FTC+EFV(ATRIPLA) MAY 12 JAN 14 TDF+FTC(TRUVADA) DRV/r
26 Nov-07 Dec-07 Dec-07 Apr-08 May-08 Jul-08 Sep-08 Nov-08 May-09 Aug-09 Mar-10 Jun-10 Sep-10 Oct-10 Jan-11 Apr-11 Jul-11 Sept-11 Jan-12 May-12 Aug-12 Jan-13 Jun-13 Nov-13 May-14 CD4 cell count (cells/ul) Clinical Case ID 7036 : Patient infected with HIV-1 B subtype Age: 52 Sex: M Risk Factor: Heterosexual 1 st seropositivity: October in out GRT from plasma 09/11/2007 VL: > cps/ml; CD4: 11 cells/µl PR: L63A V77I RT: L100I > K103N copies/ml T215D IN: No resistance mutations GP-41: No resistance mutations Other pol mutations PR: I13V G16E N37C/S I62V RT: V35I/L V60I V90I A98S D121H K122E T139K V179I Q197E I202I/V I293V P294Q E297R I329V IN: I72V A91D L1010I G106A K111G S119R T124N V176L V201I K211K/R Y227Y/F N254R S255G C280S V281M GP-41: T18T/A L44M L54M E137E/K Undectability threshold in out GRT from CSF 09/11/2007 VL: 192 cps/ml PR: L63A V77I RT: L100I K103N T215D IN: No resistance mutations GP-41: Not amplified Other pol mutations PR: I13V G16E N37C/S I62V RT: V35I V60I V90I A98S D121H K122E T139K V179I Q197E I202I/V I293V P294Q E297R I329V IN: I72V A91D L1010I G106A K111G S119R T124N V176L V201I K211K/R Y227Y/F N254R S255G C280S V281M GP-41: Not amplified Viremia (copies/ml) Nov 07- Mar 08 TDF/FTC LPV/r T20 Apr 08- Sep 10 TDF/FTC LPV/r Oct 10- May 14 TDF/FTC ATV/r
 650 600 550 500 450 400 350 300 250 200 150 100 50 0 in out GRT December 2011 PR: >500000 K20R, cps/ml M36I, On December 2011 L63P, L89I, I93L RT: NONE Other pol mutations PR: I13V,")
27 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 Clinical Case: ID Patient infected with HIV-1 CRF01_AE Age 43 Sex F Risk Factor Heterosex I Seropositivity December 2011 CDC stage C3 CD4 cell count (cells/ul) in out GRT December 2011 PR: > K20R, cps/ml M36I, On December 2011 L63P, L89I, I93L RT: NONE Other pol mutations PR: I13V, Q18H/Q, E35D, N37D, R41K, K43R, H69K RT: E6D, V35T, T39K, K43E, D121D/H, I142V, S162A, K173I, Q174K, D177E, G196EG, I202IV, Q207A, R211S, V245E, A272P, V276IV, T286A, E291D, V292I, I293V, Viremia: 624,734 copies/ml CD4 cell count: 19 cells/µl H69K Undetectability threshold E312T, I326V in out GRT April 2012 PR: K20R, M36I, L63P, L89I, I93L RT: K103N, Y188H/Y Other pol mutations PR: T12I/T, I13V, E35D, N37D, R41K, K43R, RT: E6D, V35T, T39K, K43E, F61F/L, D121H, K122E, I142V, S162A, K173I, Q174K, D177E, Q207A, R211S, V245E, A272P, V276I, T286A, E291D, V292I, I293V, E312T, I326V, Q334R, G335D Viremia (log copies/ml) DECEMBER 2011 APRIL 2012 TDF+FTC+EFV
28 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Apr-11 Jun-11 Aug-11 Dec-11 Jan-12 Apr-12 Clinical Case: ID 6784 Patient infected with HIV-1 B subtype Age 33 Sex M Risk Factor MSM I Seropositivity January 2001 CDC stage B2 CD4 cell count (cells/ul) in out GRT AUGUST 2010 PR: L10I, L63T, I93L RT: V118I, G333E > cps/ml Other pol mutations PR: I15V, R57K, E65D RT: V35L, P55A, V60I, K64KR, D121H, K122E, S134C, I135T, T139R, D177E, T200AT, R211K, F214L, V245E, D250E, A272P, K281R, I293V, E297R, L301I, Q334K in Undetectability threshold out GRT JANUARY 2012 PR: L10I, M36IM, L63T, I93L RT: V118I, G333E Other pol mutations PR: T12PT, I15V, R57K, E65D RT: V35L, P55A, V60IV, K64R, D121H, K122E, S134C, I135T, T139R, D177E, I195IL, R211K, F214L, V245E, D250E, A272P, K281R, I293V, E297R, L301I, Q334K Viremia (log copies/ml) SEPT 10 - JAN 12 TDF+FTC, DRV (800)/r FEB 12 - APR 12 TDF+FTC, DRV(600X2)/r
29 Conclusions (I) The construction of antiretroviral therapy must be designed taking into account the long-term strategy, and not the mere control of short term viral replication. Viremia remains today a key marker of efficacy of antiviral therapy High viral load (including cumulative one) at baseline is consistently associated with higher risk of virological failure and clinical outcome. nevertheless. persistent low viremia is also associated with an increased risk of virological failure, of development of resistance, and of progression of the disease, compared to patients with stable undetectable viral load
30 Conclusions (II) Resistance tests need to be used in clinical practice (also at low level viremia!) soon when virological failure is defined Genetic barrier still represents a key factor to be considered in a therapeutic strategy aimed at controlling the virus for long period of time, by maintaining viremia stably below the level of detection
Clinical Case. Prof.ssa Cristina Mussini
 Clinical Case Prof.ssa Cristina Mussini Clinical history Male, born in Ivory Coast in 1968. HIV positive since dal 1998 Risk factor: heterosexual contacts He started antiretroviral therapy in 2001 with
Clinical Case Prof.ssa Cristina Mussini Clinical history Male, born in Ivory Coast in 1968. HIV positive since dal 1998 Risk factor: heterosexual contacts He started antiretroviral therapy in 2001 with
Antiretroviral Treatment Strategies: Clinical Case Presentation
 Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Professor Anna Maria Geretti
 THIRD JOINT CONFERENCE OF BHIVA AND BASHH 2014 Professor Anna Maria Geretti Institute of Infection & Global Health, University of Liverpool 1-4 April 2014, Arena and Convention Centre Liverpool THIRD JOINT
THIRD JOINT CONFERENCE OF BHIVA AND BASHH 2014 Professor Anna Maria Geretti Institute of Infection & Global Health, University of Liverpool 1-4 April 2014, Arena and Convention Centre Liverpool THIRD JOINT
Round table discussion Patients with multiresistant virus : A limited number, but a remarkable deal Introduction
 Disclosure statement: Dr. Santoro reports personal fees from ViiV Healthcare, Gilead and JANSSEN Cilag Round table discussion Patients with multiresistant virus : A limited number, but a remarkable deal
Disclosure statement: Dr. Santoro reports personal fees from ViiV Healthcare, Gilead and JANSSEN Cilag Round table discussion Patients with multiresistant virus : A limited number, but a remarkable deal
Virological failure to Protease inhibitors in Monotherapy is linked to the presence of signature mutations in Gag without changes in HIV-1 replication
 Virological failure to Protease inhibitors in Monotherapy is linked to the presence of signature mutations in Gag without changes in HIV-1 replication Oscar Blanch-Lombarte Rome, 7-9 June, 2017 European
Virological failure to Protease inhibitors in Monotherapy is linked to the presence of signature mutations in Gag without changes in HIV-1 replication Oscar Blanch-Lombarte Rome, 7-9 June, 2017 European
14 TH EUROPEAN HIV & HEPATITIS MEETING Abst#_O_06
 14 TH EUROPEAN HIV & HEPATITIS MEETING 2016 Abst#_O_06 Patients with pre-existent NRTI- and NNRTI-resistance have a higher risk to lose virological suppression under tenofovir/emtricitabine/rilpivirine
14 TH EUROPEAN HIV & HEPATITIS MEETING 2016 Abst#_O_06 Patients with pre-existent NRTI- and NNRTI-resistance have a higher risk to lose virological suppression under tenofovir/emtricitabine/rilpivirine
Rajesh T. Gandhi, M.D.
 HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
The role of cohorts studies in current treatment guidelines development: the Italian experience. Andrea Antinori INMI L Spallanzani IRCCS, Roma
 The role of cohorts studies in current treatment guidelines development: the Italian experience Andrea Antinori INMI L Spallanzani IRCCS, Roma INITIATING THERAPY When to start ART? 2012-2013 Guidelines
The role of cohorts studies in current treatment guidelines development: the Italian experience Andrea Antinori INMI L Spallanzani IRCCS, Roma INITIATING THERAPY When to start ART? 2012-2013 Guidelines
Low-Level Viremia in HIV
 Mountain West AIDS Education and Training Center Low-Level Viremia in HIV Brian R. Wood, MD Medical Director, Mountain West AETC ECHO Telehealth Program Assistant Professor of Medicine, University of Washington
Mountain West AIDS Education and Training Center Low-Level Viremia in HIV Brian R. Wood, MD Medical Director, Mountain West AETC ECHO Telehealth Program Assistant Professor of Medicine, University of Washington
Virological suppression and PIs. Diego Ripamonti Malattie Infettive - Bergamo
 Virological suppression and PIs Diego Ripamonti Malattie Infettive - Bergamo Ritonavir-boosted PIs Boosted PIs: 3 drugs in one The intrinsic antiretroviral activity Viral suppression and high baseline
Virological suppression and PIs Diego Ripamonti Malattie Infettive - Bergamo Ritonavir-boosted PIs Boosted PIs: 3 drugs in one The intrinsic antiretroviral activity Viral suppression and high baseline
HIV-1 Subtypes: An Overview. Anna Maria Geretti Royal Free Hospital
 HIV-1 Subtypes: An Overview Anna Maria Geretti Royal Free Hospital Group M Subtypes A (1, 2, 3) B C D F (1, 2) G H J K Mechanisms of HIV-1 genetic diversification Point mutations RT error rate: ~1 per
HIV-1 Subtypes: An Overview Anna Maria Geretti Royal Free Hospital Group M Subtypes A (1, 2, 3) B C D F (1, 2) G H J K Mechanisms of HIV-1 genetic diversification Point mutations RT error rate: ~1 per
Switching strategies and ARV treatment costs
 February 2014 Switching strategies and ARV treatment costs Josep M Llibre/Bonaventura Clotet Fundació Lluita contra la SIDA Hosp Univ Germans Trias i Pujol Badalona Rationale. Spain is under a huge economic
February 2014 Switching strategies and ARV treatment costs Josep M Llibre/Bonaventura Clotet Fundació Lluita contra la SIDA Hosp Univ Germans Trias i Pujol Badalona Rationale. Spain is under a huge economic
Dr Carole Wallis, PhD Medical Director, BARC-SA Head of the Specialty Molecular Division, Lancet Laboratories, South Africa
 Dr Carole Wallis, PhD Medical Director, BARC-SA Head of the Specialty Molecular Division, Lancet Laboratories, South Africa Transmitted drug resistance Resistance patterns in first-line failures in adults
Dr Carole Wallis, PhD Medical Director, BARC-SA Head of the Specialty Molecular Division, Lancet Laboratories, South Africa Transmitted drug resistance Resistance patterns in first-line failures in adults
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
Somnuek Sungkanuparph, M.D.
 HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
Prevalence of Transmitted Drug Resistance Mutations among Naive HIV-infected patients ( ) in Northwest Spain
 in Northwest Spain") Prevalence of Transmitted Drug Resistance Mutations among Naive HIV-infected patients (2014-2016) in Northwest Spain Berta Pernas 1, Andrés Tabernilla 1, Marta Grandal 1, Angelina Cañizares 2, Sofía Ortún
Prevalence of Transmitted Drug Resistance Mutations among Naive HIV-infected patients (2014-2016) in Northwest Spain Berta Pernas 1, Andrés Tabernilla 1, Marta Grandal 1, Angelina Cañizares 2, Sofía Ortún
Tools to Monitor HIV Infection in 2013 and Beyond.
 Tools to Monitor HIV Infection in 2013 and Beyond. Federico García, fegarcia@ugr.es Servicio de Microbiología Univ. Hospital San Cecilio Granada, Spain Outline Address clinical questions: Ultra sensitive
Tools to Monitor HIV Infection in 2013 and Beyond. Federico García, fegarcia@ugr.es Servicio de Microbiología Univ. Hospital San Cecilio Granada, Spain Outline Address clinical questions: Ultra sensitive
HIV viral load testing in the era of ART. Christian Noah Labor Lademannbogen, Hamburg
 HIV viral load testing in the era of ART Christian Noah Labor Lademannbogen, Hamburg 1 Life expectancy of patients on ART Data from the UK Collaborative HIV Cohort (UK CHIC) Requirements: Early diagnosis
HIV viral load testing in the era of ART Christian Noah Labor Lademannbogen, Hamburg 1 Life expectancy of patients on ART Data from the UK Collaborative HIV Cohort (UK CHIC) Requirements: Early diagnosis
APACC 2016 HIV drug resistance. Shinichi Oka, MD, PhD. AIDS Clinical Center (ACC) National Center for Global Health and Medicine (NCGM)
 National Center for Global Health and Medicine (NCGM)") APACC 2016 HIV drug resistance Shinichi Oka, MD, PhD. AIDS Clinical Center (ACC) National Center for Global Health and Medicine (NCGM) HIV drug resistance 1. Current situation of ART and TDR in Japan 2.
APACC 2016 HIV drug resistance Shinichi Oka, MD, PhD. AIDS Clinical Center (ACC) National Center for Global Health and Medicine (NCGM) HIV drug resistance 1. Current situation of ART and TDR in Japan 2.
Starting ART in Western Europe. Andrea Antinori National Institute for Infectious Diseases Lazzaro Spallanzani IRCCS, Rome, Italy
 Starting ART in Western Europe Andrea Antinori National Institute for Infectious Diseases Lazzaro Spallanzani IRCCS, Rome, Italy CD4 count (cells/mm 3 ) Benefits and disadvantages of cart 1995 2005 2013
Starting ART in Western Europe Andrea Antinori National Institute for Infectious Diseases Lazzaro Spallanzani IRCCS, Rome, Italy CD4 count (cells/mm 3 ) Benefits and disadvantages of cart 1995 2005 2013
How to best manage HIV patient?
 How to best manage HIV patient? 1 2 Treatment Treatment Failure success HIV therapy = a long life therapy Why do we want to change a suppressive ART? Side effect Comorbidities Reduce drug burden How to
How to best manage HIV patient? 1 2 Treatment Treatment Failure success HIV therapy = a long life therapy Why do we want to change a suppressive ART? Side effect Comorbidities Reduce drug burden How to
MDR HIV and Total Therapeutic Failure. Douglas G. Fish, MD Albany Medical College Albany, New York Cali, Colombia March 30, 2007
 MDR HIV and Total Therapeutic Failure Douglas G. Fish, MD Albany Medical College Albany, New York Cali, Colombia March 30, 2007 Objectives Case study Definitions Fitness Pathogenesis of resistant virus
MDR HIV and Total Therapeutic Failure Douglas G. Fish, MD Albany Medical College Albany, New York Cali, Colombia March 30, 2007 Objectives Case study Definitions Fitness Pathogenesis of resistant virus
HIV Treatment: New and Veteran Drugs Classes
 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
Antiretroviral Prophylaxis and HIV Drug Resistance. John Mellors University of Pittsburgh
 Antiretroviral Prophylaxis and HIV Drug Resistance John Mellors University of Pittsburgh MTN Annual 2008 Outline Two minutes on terminology Origins of HIV drug resistance Lessons learned from ART Do these
Antiretroviral Prophylaxis and HIV Drug Resistance John Mellors University of Pittsburgh MTN Annual 2008 Outline Two minutes on terminology Origins of HIV drug resistance Lessons learned from ART Do these
Resistance Workshop. 3rd European HIV Drug
 3rd European HIV Drug Resistance Workshop March 30-April 1 st, 2005 Christine Hughes, PharmD Clinical Associate Professor Faculty of Pharmacy & Pharmaceutical Sciences University of Alberta Tenofovir resistance
3rd European HIV Drug Resistance Workshop March 30-April 1 st, 2005 Christine Hughes, PharmD Clinical Associate Professor Faculty of Pharmacy & Pharmaceutical Sciences University of Alberta Tenofovir resistance
ID Week 2016: HIV Update
 Mountain West AIDS Education and Training Center ID Week 2016: HIV Update Robert Harrington, M.D. This presentation is intended for educational use only, and does not in any way constitute medical consultation
Mountain West AIDS Education and Training Center ID Week 2016: HIV Update Robert Harrington, M.D. This presentation is intended for educational use only, and does not in any way constitute medical consultation
History (August 2010) Therapy for Experienced Patients. History (September 2010) History (November 2010) 12/2/11
 Therapy for Experienced Patients. History (September 2010) History (November 2010) 12/2/11") (August 2010) Therapy for Experienced Patients Hiroyu Hatano, MD, MHS Assistant Professor of Medicine University of California San Francisco Medical Management of AIDS December 2011 42M HIV (CD4=450, VL=6250,
(August 2010) Therapy for Experienced Patients Hiroyu Hatano, MD, MHS Assistant Professor of Medicine University of California San Francisco Medical Management of AIDS December 2011 42M HIV (CD4=450, VL=6250,
Resistance Characteristics of Integrase Inhibitors
 Resistance Characteristics of Integrase Inhibitors Madrid, November 2016 Jonathan M Schapiro, MD National Hemophilia Center, Israel Stanford University School of Medicine, USA Disclaimer Presentation includes
Resistance Characteristics of Integrase Inhibitors Madrid, November 2016 Jonathan M Schapiro, MD National Hemophilia Center, Israel Stanford University School of Medicine, USA Disclaimer Presentation includes
Socio-Demographic Factors associated with Success of Antiretroviral Treatment among HIV Patients in Tanzania
 Socio-Demographic Factors associated with Success of Antiretroviral Treatment among HIV Patients in Tanzania Dr. Fausta Franklin Mosha (MD, MSc, MSc, PHD) Ministry of Health and Social Welfare 22 nd October
Socio-Demographic Factors associated with Success of Antiretroviral Treatment among HIV Patients in Tanzania Dr. Fausta Franklin Mosha (MD, MSc, MSc, PHD) Ministry of Health and Social Welfare 22 nd October
Treatment of HIV-1 in Adults and Adolescents: Part 2
 Treatment of HIV-1 in Adults and Adolescents: Part 2 Heather E. Vezina, Pharm.D. University of Minnesota Laboratory Medicine & Pathology Experimental & Clinical Pharmacology wynnx004@umn.edu Management
Treatment of HIV-1 in Adults and Adolescents: Part 2 Heather E. Vezina, Pharm.D. University of Minnesota Laboratory Medicine & Pathology Experimental & Clinical Pharmacology wynnx004@umn.edu Management
DRUGS IN PIPELINE. Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015
 DRUGS IN PIPELINE Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015 N(t)RTI The Development of TAF TAF Delivers the High Potency of TDF While Minimizing Off- Target Kidney and Bone Side Effects
DRUGS IN PIPELINE Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015 N(t)RTI The Development of TAF TAF Delivers the High Potency of TDF While Minimizing Off- Target Kidney and Bone Side Effects
HIV Drug Resistance among Adolescents and Young Adults Failing HIV Therapy in Zimbabwe
 HIV Drug Resistance among Adolescents and Young Adults Failing HIV Therapy in Zimbabwe V Kouamou 1, J Manasa 1, D Katzenstein 1, A McGregor 1, CE Ndhlovu 1 & AT Makadzange 1. 1 University of Zimbabwe Introduction
HIV Drug Resistance among Adolescents and Young Adults Failing HIV Therapy in Zimbabwe V Kouamou 1, J Manasa 1, D Katzenstein 1, A McGregor 1, CE Ndhlovu 1 & AT Makadzange 1. 1 University of Zimbabwe Introduction
Cases from the Clinic(ians): Case-Based Panel Discussion
: Case-Based Panel Discussion") Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
BHIVA Workshop: When to Start. Dr Chloe Orkin Dr Laura Waters
 BHIVA Workshop: When to Start Dr Chloe Orkin Dr Laura Waters Aims To use cases to: Review new BHIVA guidance Explore current data around when to start To discuss: Medical decisions, pros and cons Luigi
BHIVA Workshop: When to Start Dr Chloe Orkin Dr Laura Waters Aims To use cases to: Review new BHIVA guidance Explore current data around when to start To discuss: Medical decisions, pros and cons Luigi
Efficacy and Safety of Doravirine 100mg QD vs Efavirenz 600mg QD with TDF/FTC in ART-Naive HIV-Infected Patients: Week 24 Results
 Efficacy and Safety of Doravirine 1mg QD vs Efavirenz 6mg QD with TDF/FTC in ART-Naive HIV-Infected Patients: Week 24 Results Jose M. Gatell, Francois Raffi, Andreas Plettenberg, Don Smith, Joaquin Portilla,
Efficacy and Safety of Doravirine 1mg QD vs Efavirenz 6mg QD with TDF/FTC in ART-Naive HIV-Infected Patients: Week 24 Results Jose M. Gatell, Francois Raffi, Andreas Plettenberg, Don Smith, Joaquin Portilla,
Is HIV management moving towards personalized medicine? Carlo Federico Perno
 Is HIV management moving towards personalized medicine? Carlo Federico Perno .15188 Icona patients.. Proportion of patients with a VL
Is HIV management moving towards personalized medicine? Carlo Federico Perno .15188 Icona patients.. Proportion of patients with a VL
Treatment strategies for the developing world
 David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia First line standard of care First line in the developing world First line failure
David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia First line standard of care First line in the developing world First line failure
Does Resistance Still Matter? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School
 Does Resistance Still Matter? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosure The speaker serves as a consultant to, and has received
Does Resistance Still Matter? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosure The speaker serves as a consultant to, and has received
Clinical skills building - HIV drug resistance
 Clinical skills building - HIV drug resistance Richard Lessells Clinical case 44-year old HIV-positive male HIV diagnosis 2010 Pre-treatment CD4+ count not known Initiated first-line ART (TDF/FTC/EFV)
Clinical skills building - HIV drug resistance Richard Lessells Clinical case 44-year old HIV-positive male HIV diagnosis 2010 Pre-treatment CD4+ count not known Initiated first-line ART (TDF/FTC/EFV)
Resistance to Integrase Strand Transfer Inhibitors
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Resistance to Integrase Strand Transfer Inhibitors David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Resistance to Integrase Strand Transfer Inhibitors David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases
DNA Genotyping in HIV Infection
 Frontier AIDS Education and Training Center DNA Genotyping in HIV Infection Steven C. Johnson M.D. Director, University of Colorado HIV/AIDS Clinical Program; Professor of Medicine, Division of Infectious
Frontier AIDS Education and Training Center DNA Genotyping in HIV Infection Steven C. Johnson M.D. Director, University of Colorado HIV/AIDS Clinical Program; Professor of Medicine, Division of Infectious
Professor Jonathan Weber
 HIV/AIDS at 30: Back to the Future BHIVA / Wellcome Trust Multidisciplinary Event to mark World AIDS Day 2011 British HIV Association (BHIVA) 2011 HIV/AIDS at 30: Back to the Future BHIVA / Wellcome Trust
HIV/AIDS at 30: Back to the Future BHIVA / Wellcome Trust Multidisciplinary Event to mark World AIDS Day 2011 British HIV Association (BHIVA) 2011 HIV/AIDS at 30: Back to the Future BHIVA / Wellcome Trust
Dr Marta Boffito Chelsea and Westminster Hospital, London
 Dr Marta Boffito Chelsea and Westminster Hospital, London Speaker Name Statement Dr Marta Boffito has received travel and research grants from and has been an advisor for Janssen, Roche, Pfizer, ViiV,
Dr Marta Boffito Chelsea and Westminster Hospital, London Speaker Name Statement Dr Marta Boffito has received travel and research grants from and has been an advisor for Janssen, Roche, Pfizer, ViiV,
Transmission of integrase resistance HIV
 Transmission of integrase resistance HIV Charles Boucher, MD, PhD Clinical Virology, Dept. Viroscience, Erasmus Medical Center, Erasmus Universiy, The Netherlands Major resistance mutations (Stanford)
Transmission of integrase resistance HIV Charles Boucher, MD, PhD Clinical Virology, Dept. Viroscience, Erasmus Medical Center, Erasmus Universiy, The Netherlands Major resistance mutations (Stanford)
1. Africa Centre for Health and Population Studies 2. London School of Hygiene and Tropical Medicine 3. University College London
 A systematic review of the effects of interrupted antiretroviral interventions for prevention of mother-to-child transmission of HIV on maternal disease progression and survival Naidu KK 1, Mori R 2, Newell
A systematic review of the effects of interrupted antiretroviral interventions for prevention of mother-to-child transmission of HIV on maternal disease progression and survival Naidu KK 1, Mori R 2, Newell
Improving PI drug resistance scores. Jens Verheyen, MD Institute of Virology University Duisburg-Essen
 Improving PI drug resistance scores Jens Verheyen, MD Institute of Virology University Duisburg-Essen Overview Why can all PI drug resistance scores be improved? Do we still need to improve PI drug resistance
Improving PI drug resistance scores Jens Verheyen, MD Institute of Virology University Duisburg-Essen Overview Why can all PI drug resistance scores be improved? Do we still need to improve PI drug resistance
Disclosures. Introduction to ARV Drug Resistance New Clinicians Workshop. Introduction. ARS Question 12/6/2017
 Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
IAS 2013 Towards an HIV Cure Symposium
 In chronically HIV-1-infected patients long-term antiretroviral therapy initiated above 500 CD4/mm 3 achieves better HIV-1 reservoirs' depletion and T-cell count restoration IAS 2013 Towards an HIV Cure
In chronically HIV-1-infected patients long-term antiretroviral therapy initiated above 500 CD4/mm 3 achieves better HIV-1 reservoirs' depletion and T-cell count restoration IAS 2013 Towards an HIV Cure
Costo-efficacia del monitoraggio immunologico standard. Enrico Girardi UOC Epidemiologia Clinica INMI L. Spallanzani, Roma
 Costo-efficacia del monitoraggio immunologico standard Enrico Girardi UOC Epidemiologia Clinica INMI L. Spallanzani, Roma Beneficio clinico del monitoraggio della conta CD4 Studi in Paesi ricchi There
Costo-efficacia del monitoraggio immunologico standard Enrico Girardi UOC Epidemiologia Clinica INMI L. Spallanzani, Roma Beneficio clinico del monitoraggio della conta CD4 Studi in Paesi ricchi There
HIV 101. Applications of Antiretroviral Therapy
 HIV 101. Applications of Antiretroviral Therapy Michael S. Saag, MD Professor of Medicine Associate Dean for Global Health Jim Straley Chair in AIDS Research University of Alabama at Birmingham Birmingham,
HIV 101. Applications of Antiretroviral Therapy Michael S. Saag, MD Professor of Medicine Associate Dean for Global Health Jim Straley Chair in AIDS Research University of Alabama at Birmingham Birmingham,
Individual Study Table Referring to the Dossier SYNOPSIS. Final Clinical Study Report for Study AI424138
 Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Reyataz Name of Active Ingredient: Atazanavir () Individual Study Table Referring to the Dossier (For National Authority Use Only)
Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Reyataz Name of Active Ingredient: Atazanavir () Individual Study Table Referring to the Dossier (For National Authority Use Only)
Hepatitis B Case Studies
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Hepatitis B Case Studies Nina Kim, MD MSc Associate Professor of Medicine University of Washington Harborview Madison Clinic and Hepatitis & Liver Clinic No
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Hepatitis B Case Studies Nina Kim, MD MSc Associate Professor of Medicine University of Washington Harborview Madison Clinic and Hepatitis & Liver Clinic No
Clinical cases: HIV/HCV coinfection
 Clinical cases: HIV/HCV coinfection José Vicente Fernández-Montero Hospital Carlos III, Madrid Case #1 General considerations about antiviral therapy CASE # 1 43 year-old, male patient Former IDU No prior
Clinical cases: HIV/HCV coinfection José Vicente Fernández-Montero Hospital Carlos III, Madrid Case #1 General considerations about antiviral therapy CASE # 1 43 year-old, male patient Former IDU No prior
0% 0% 0% Parasite. 2. RNA-virus. RNA-virus
 HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
2 nd Line Treatment and Resistance. Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012
 2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
A case, and some pharmacological considerations. from the perspective of a virologist. Anna Maria Geretti University of Liverpool, United Kingdom
 A case, and some pharmacological considerations. from the perspective of a virologist Anna Maria Geretti University of Liverpool, United Kingdom 1 Case History: Mr RS 53-year-old male Diagnosed HIV positive
A case, and some pharmacological considerations. from the perspective of a virologist Anna Maria Geretti University of Liverpool, United Kingdom 1 Case History: Mr RS 53-year-old male Diagnosed HIV positive
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
Second and third line paediatric ART strategies
 Second and third line paediatric ART strategies Dr. Marape Marape Assistant Professor Ohio University School of Health Professions Gaborone, Botswana Marape Marape MB, BCh, BAO, MPH, PhD Assistant Professor
Second and third line paediatric ART strategies Dr. Marape Marape Assistant Professor Ohio University School of Health Professions Gaborone, Botswana Marape Marape MB, BCh, BAO, MPH, PhD Assistant Professor
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
When to start: guidelines comparison
 The editorial staff When to start: guidelines comparison The optimal time to begin antiretroviral therapy remains a critical question for the HIV field, and consensus about the appropriate CD4+ cell count
The editorial staff When to start: guidelines comparison The optimal time to begin antiretroviral therapy remains a critical question for the HIV field, and consensus about the appropriate CD4+ cell count
Supervised Treatment Interruption (STI) in an Urban HIV Clinical Practice: A Prospective Analysis.
 in an Urban HIV Clinical Practice: A Prospective Analysis.") Supervised Treatment Interruption (STI) in an Urban HIV Clinical Practice: A Prospective Analysis. J.L. YOZVIAK 1, P. KOUVATSOS 2, R.E. DOERFLER 3, W.C. WOODWARD 3 1 Philadelphia College of Osteopathic
Supervised Treatment Interruption (STI) in an Urban HIV Clinical Practice: A Prospective Analysis. J.L. YOZVIAK 1, P. KOUVATSOS 2, R.E. DOERFLER 3, W.C. WOODWARD 3 1 Philadelphia College of Osteopathic
SEXUAL TRANSMISSION. SEXUAL TRANSMISSION under ART: Biological Considerations
 SEXUAL TRANSMISSION under ART: Biological Considerations Dr Steve Taylor, MB ChB, FRCP, PhD Consultant Physician, HIV/GU Medicine, Lead Consultant HIV Services, Directorate of Sexual Medicine and HIV Birmingham
SEXUAL TRANSMISSION under ART: Biological Considerations Dr Steve Taylor, MB ChB, FRCP, PhD Consultant Physician, HIV/GU Medicine, Lead Consultant HIV Services, Directorate of Sexual Medicine and HIV Birmingham
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies. Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine
 Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
Clinical support for reduced drug regimens. David A Cooper The University of New South Wales Sydney, Australia
 Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
Disclosures. Introduction to ARV Drug Resistance New Clinicians Workshop 12/9/16. Introduction. ARS Question
 Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
Disclosures Introduction to ARV Drug Resistance New Clinicians Workshop I have no disclosures Susa Coffey, MD Division of HIV, ID and Global Medicine ARS Question Which resistance test do you order for
Management of ART Failure. EACS Advanced HIV Course 2015 Dr Nicky Mackie
 Management of ART Failure EACS Advanced HIV Course 2015 Dr Nicky Mackie Outline Defining treatment success Defining treatment failure Reasons for ART failure Management of ART failure Choice of second
Management of ART Failure EACS Advanced HIV Course 2015 Dr Nicky Mackie Outline Defining treatment success Defining treatment failure Reasons for ART failure Management of ART failure Choice of second
What s New in Acute HIV Infection?
 3 4 Disclosure I have received research grants awarded to my institution from Gilead Sciences, Inc. ntiretroviral medications have been provided by Gilead Sciences, Inc. Susan Little, M.D. Professor of
3 4 Disclosure I have received research grants awarded to my institution from Gilead Sciences, Inc. ntiretroviral medications have been provided by Gilead Sciences, Inc. Susan Little, M.D. Professor of
New HIV EACS and Italian Guidelines
 Original Article HIV correlated pathologies and other infections Marco Borderi New HIV EACS and Italian Guidelines Infectious Disease Unit - S. Orsola-Hospital - University of Bologna Corresponding author:
Original Article HIV correlated pathologies and other infections Marco Borderi New HIV EACS and Italian Guidelines Infectious Disease Unit - S. Orsola-Hospital - University of Bologna Corresponding author:
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
Pediatric Antiretroviral Resistance Challenges
 Pediatric Antiretroviral Resistance Challenges Thanyawee Puthanakit, MD The HIVNAT, Thai Red Cross AIDS research Center The Research Institute for Health Science, Chiang Mai University Outline The burden
Pediatric Antiretroviral Resistance Challenges Thanyawee Puthanakit, MD The HIVNAT, Thai Red Cross AIDS research Center The Research Institute for Health Science, Chiang Mai University Outline The burden
Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary?
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
What are the most promising opportunities for dose optimisation?
 What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
ICAAC/IDSA DC, Oct. 26, 2008
 Tenofovir (TDF)- or Abacavir (ABC)-selected Minority Subpopulations in Viremic Subjects Detected by Ultra-deep Sequencing R. T. D Aquila 1, E. Rouse 2, J. Horton 2, A. Kheshti 1,3, S. Raffanti 1,3, K.
Tenofovir (TDF)- or Abacavir (ABC)-selected Minority Subpopulations in Viremic Subjects Detected by Ultra-deep Sequencing R. T. D Aquila 1, E. Rouse 2, J. Horton 2, A. Kheshti 1,3, S. Raffanti 1,3, K.
Clinical use of HIV-DNA quantity and resistance testing
 Clinical use of HIV-DNA quantity and resistance testing Personal fees and travel grants Abbott Molecular Gilead Sciences Janssen-Cilag Merck Sharp and Dohme ViiV Healthcare Research and educational grants
Clinical use of HIV-DNA quantity and resistance testing Personal fees and travel grants Abbott Molecular Gilead Sciences Janssen-Cilag Merck Sharp and Dohme ViiV Healthcare Research and educational grants
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Didactic Series. Archive Genotype Resistance Testing in the Setting of Regimen Switching
 Didactic Series Archive Genotype Resistance Testing in the Setting of Regimen Switching Craig Ballard, Pharm.D., AAHIVP UCSD Medical Center Owen Clinic June 11, 2015 ACCREDITATION STATEMENT: University
Didactic Series Archive Genotype Resistance Testing in the Setting of Regimen Switching Craig Ballard, Pharm.D., AAHIVP UCSD Medical Center Owen Clinic June 11, 2015 ACCREDITATION STATEMENT: University
BHIVA Best of CROI Feedback Meetings. London Birmingham North West England Cardiff Gateshead Edinburgh
 BHIVA Best of CROI Feedback Meetings London Birmingham North West England Cardiff Gateshead Edinburgh BHIVA Best of CROI Feedback Meetings 2010 ANTIRETROVIRAL TREATMENT STRATEGIES AND NEW DRUGS A5202:
BHIVA Best of CROI Feedback Meetings London Birmingham North West England Cardiff Gateshead Edinburgh BHIVA Best of CROI Feedback Meetings 2010 ANTIRETROVIRAL TREATMENT STRATEGIES AND NEW DRUGS A5202:
Integrase Inhibitor Based Antiretroviral Therapy in Botswana; a Case Report
 Detection of Four-Class Resistant HIV-1C in a patient on Integrase Inhibitor Based Antiretroviral Therapy in Botswana; a Case Report Kaelo K. Seatla MPhil / PhD Student Supervisors: Dr. Simani Gaseitsiwe
Detection of Four-Class Resistant HIV-1C in a patient on Integrase Inhibitor Based Antiretroviral Therapy in Botswana; a Case Report Kaelo K. Seatla MPhil / PhD Student Supervisors: Dr. Simani Gaseitsiwe
PROSPECTS FOR HIV CURE IN ADULTS. Nov 11 th 2013 John Frater
 PROSPECTS FOR HIV CURE IN ADULTS FIS 2013 Nov 11 th 2013 John Frater April 29 th 2013; Telegraph online THE COMPONENTS OF A CURE. What is cure? Issues to consider: Post treatment control the benefit of
PROSPECTS FOR HIV CURE IN ADULTS FIS 2013 Nov 11 th 2013 John Frater April 29 th 2013; Telegraph online THE COMPONENTS OF A CURE. What is cure? Issues to consider: Post treatment control the benefit of
Clinical Development of ABX464, drug candidate for HIV Functional Cure. Chief Medical Officer ABIVAX
 Clinical Development of ABX464, drug candidate for HIV Functional Cure Jean-Marc Steens, MD Chief Medical Officer ABIVAX 1 DECLARATION OF CONFLICT OF INTEREST GSK ABIVAX 2 ABX464: Mechanism of Action ABX464
Clinical Development of ABX464, drug candidate for HIV Functional Cure Jean-Marc Steens, MD Chief Medical Officer ABIVAX 1 DECLARATION OF CONFLICT OF INTEREST GSK ABIVAX 2 ABX464: Mechanism of Action ABX464
Professor José Arribas
 19 th Annual Conference of the British HIV Association (BHIVA) Professor José Arribas Hospital La Paz, Madrid, Spain 16-19 April 2013, Manchester Central Convention Complex Can we live without nucleosides?
19 th Annual Conference of the British HIV Association (BHIVA) Professor José Arribas Hospital La Paz, Madrid, Spain 16-19 April 2013, Manchester Central Convention Complex Can we live without nucleosides?
Changes in cellular HIV DNA levels during the MONET trial: 144 Weeks of darunavir/ritonavir monotherapy versus DRV/r + 2NRTIs
 Changes in cellular HIV DNA levels during the MONET trial: 144 Weeks of darunavir/ritonavir monotherapy versus DRV/r + 2NRTIs Anna Maria Geretti, Jose R Arribas, Johan Vingerhoets, Geraldine Foster, Sabine
Changes in cellular HIV DNA levels during the MONET trial: 144 Weeks of darunavir/ritonavir monotherapy versus DRV/r + 2NRTIs Anna Maria Geretti, Jose R Arribas, Johan Vingerhoets, Geraldine Foster, Sabine
Advances in HIV science and treatment. Report on the global AIDS epidemic,
 HIV biomolecular advances and treatment updates David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia UNAIDS: global l HIV infections
HIV biomolecular advances and treatment updates David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia UNAIDS: global l HIV infections
OPPORTUNISTIC INFECTIONS. Institute of Infectious Diseases, Pune India
 OPPORTUNISTIC INFECTIONS Institute of Infectious Diseases, Pune India DISCLOSURES Nothing to declare Outline The problem Bacterial Fungal Protozoal Viral Decline in OI prevalence in HAART era: USA CROI
OPPORTUNISTIC INFECTIONS Institute of Infectious Diseases, Pune India DISCLOSURES Nothing to declare Outline The problem Bacterial Fungal Protozoal Viral Decline in OI prevalence in HAART era: USA CROI
This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts
 1 2 This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts decreased. This period of acute infection or serocnversion
1 2 This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts decreased. This period of acute infection or serocnversion
Dolutegravir used in real-life provides high rates of virological response in conjunction with a rare emergence of integrase resistance.
 Dolutegravir used in real-life provides high rates of virological response in conjunction with a rare emergence of integrase resistance. D. Armenia 1, V. Borghi 2, F Forbici 3, C. Gori 3, A. Bertoli 1,
Dolutegravir used in real-life provides high rates of virological response in conjunction with a rare emergence of integrase resistance. D. Armenia 1, V. Borghi 2, F Forbici 3, C. Gori 3, A. Bertoli 1,
The injectables: a new silver bullet?
 The injectables: a new silver bullet? Geneva October 6 Francois Venter Wits Reproductive Health and HIV Institute Thanks Clinical Care Options, Helen Rees, Joe Eron, Wits RHI sex worker team Disclosures
The injectables: a new silver bullet? Geneva October 6 Francois Venter Wits Reproductive Health and HIV Institute Thanks Clinical Care Options, Helen Rees, Joe Eron, Wits RHI sex worker team Disclosures
Innovative diagnostics for HIV, HBV and HCV
 Innovative diagnostics for HIV, HBV and HCV Dan Otelea National Institute for Infectious Diseases Bucharest, Romania Disclaimer No conflicts of interest Innovative diagnostics for HIV, HBV and HCV - is
Innovative diagnostics for HIV, HBV and HCV Dan Otelea National Institute for Infectious Diseases Bucharest, Romania Disclaimer No conflicts of interest Innovative diagnostics for HIV, HBV and HCV - is
Didactic Series. CROI New Antiretroviral Therapies. Daniel Lee, MD Clinical Professor of Medicine UCSD Medical Center Owen Clinic July 14, 2016
 Didactic Series CROI 2016 - New Antiretroviral Therapies Daniel Lee, MD Clinical Professor of Medicine UCSD Medical Center Owen Clinic July 14, 2016 This project is supported by the Health Resources and
Didactic Series CROI 2016 - New Antiretroviral Therapies Daniel Lee, MD Clinical Professor of Medicine UCSD Medical Center Owen Clinic July 14, 2016 This project is supported by the Health Resources and
Pediatric Antiretroviral Therapy
 Update on Pediatric Antiretroviral Therapy Lynne M. Mofenson, M.D. Pediatric, Adolescent and Maternal AIDS Branch National Institute of Child Health and Human Development National Institutes of Health
Update on Pediatric Antiretroviral Therapy Lynne M. Mofenson, M.D. Pediatric, Adolescent and Maternal AIDS Branch National Institute of Child Health and Human Development National Institutes of Health
HIGH VIRAL LOAD AND TREATMENT RESPONSE
 16 th Annual Resistance and Antiviral Dr Bonaventura Clotet Hospital Germans Trias i Pujol, Barcelona, Spain Thursday 20 September 2012, Wellcome Collection Conference Centre, London HIGH VIRAL LOAD AND
16 th Annual Resistance and Antiviral Dr Bonaventura Clotet Hospital Germans Trias i Pujol, Barcelona, Spain Thursday 20 September 2012, Wellcome Collection Conference Centre, London HIGH VIRAL LOAD AND
Potential Issues in Treating HIV/HCV co-infection with new HCV antivirals
 State of the Art in Hepatitis C Virus Infection in HIV/HCV-Coinfected Patients FORMATTED: 11/17/15 David L. Wyles, MD Associate Professor of Medicine University of California San Diego San Diego, California
State of the Art in Hepatitis C Virus Infection in HIV/HCV-Coinfected Patients FORMATTED: 11/17/15 David L. Wyles, MD Associate Professor of Medicine University of California San Diego San Diego, California
ART Treatment. ART Treatment
 Naïve Experienced Strategies ARV in pregnancy ART Treatment Naïve studies: ART Treatment Abstract 37 Atazanavir/r vs Lopinavir/r: Castle study Abstract 774 Kivexa vs Truvada: HEAT study Abstract 775 Lopinavir/r
Naïve Experienced Strategies ARV in pregnancy ART Treatment Naïve studies: ART Treatment Abstract 37 Atazanavir/r vs Lopinavir/r: Castle study Abstract 774 Kivexa vs Truvada: HEAT study Abstract 775 Lopinavir/r
The BATAR Study Boosted Atazanavir Truvada vs. Atazanavir Raltegravir
 The BATAR Study Boosted Atazanavir Truvada vs. Atazanavir Raltegravir A Pilot Study of the Novel Antiretroviral Combination of Atazanavir and Raltegravir in HIV-1 Infected Subjects with Virologic Suppression
The BATAR Study Boosted Atazanavir Truvada vs. Atazanavir Raltegravir A Pilot Study of the Novel Antiretroviral Combination of Atazanavir and Raltegravir in HIV-1 Infected Subjects with Virologic Suppression
ART for HIV Prevention:
 ART for HIV Prevention: KENNETH H. MAYER, M.D. Brown University/The Fenway Institute August 22, 2009 APPROACHES TO PREVENT HIV TRANSMISSION DECREASE SOURCE OF INFECTION Barrier Protection Treat STI Antiretroviral
ART for HIV Prevention: KENNETH H. MAYER, M.D. Brown University/The Fenway Institute August 22, 2009 APPROACHES TO PREVENT HIV TRANSMISSION DECREASE SOURCE OF INFECTION Barrier Protection Treat STI Antiretroviral
Didactic Series. CROI 2014 Update. March 27, 2014
 Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Update on HIV Drug Resistance. Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School
 Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Infertility Treatment and HIV
 Infertility Treatment and HIV Infertility Treatment by IVF Or Intra-cytoplasmic Sperm Injections (ICSC) In Chronic HIV-1 Sero- discordant Couples (Poster 670) Retrospective study of outcome of IVF or ICSC
Infertility Treatment and HIV Infertility Treatment by IVF Or Intra-cytoplasmic Sperm Injections (ICSC) In Chronic HIV-1 Sero- discordant Couples (Poster 670) Retrospective study of outcome of IVF or ICSC