Antiretroviral Treatment: What's in the Pipeline
|
|
|
- Amy Grant
- 6 years ago
- Views:
Transcription


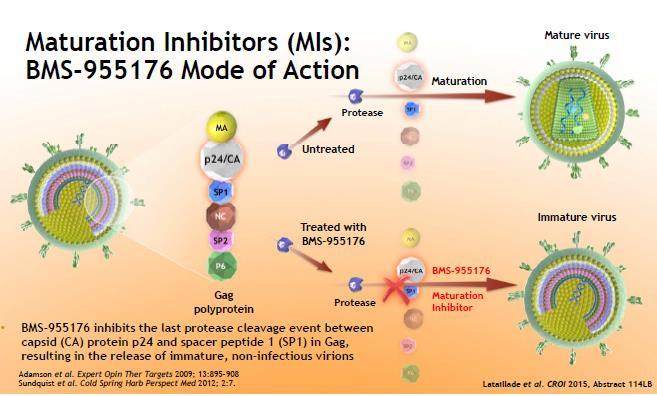
1 Antiretroviral Treatment: What's in the Pipeline Joseph P. McGowan, MD, FACP, FIDSA Professor of Medicine Hofstra North Shore-LIJ School of Medicine October 14, 2015 Which describes best how HIV Maturation Inhibitors Work? A. Block of release of budding viral progeny from CD4 cell surface B. Block integration of HIV DNA from forming stable pro-virus C. Inhibits protease cleavage step of viral polypeptide D. Engages virus in endless video game play 44% 29% 25% 2% Block of release of buddi.. Block integration of HIV... Inhibits protease cleavag... Engages virus in endless... 1
2 Session Objectives -To describe the need for new antiretroviral treatment options - To describe promising investigational agents in existing ARV classes - To review the landscape of emerging novel targets for antiretroviral therapy development Why do we need new ARV therapies? HIV/AIDS remains a global health threat despite current treatment options HIV management requires life-long treatment with combination therapy which must be safe and tolerable ARV options for treatment experienced patients may be limited due to cross class resistance, DDIs, adverse effects, chronic medical conditions, complexity Novel therapies would need to target different steps of the viral life cycle, have unique resistance profiles, be tolerable and have few DDIs. 2
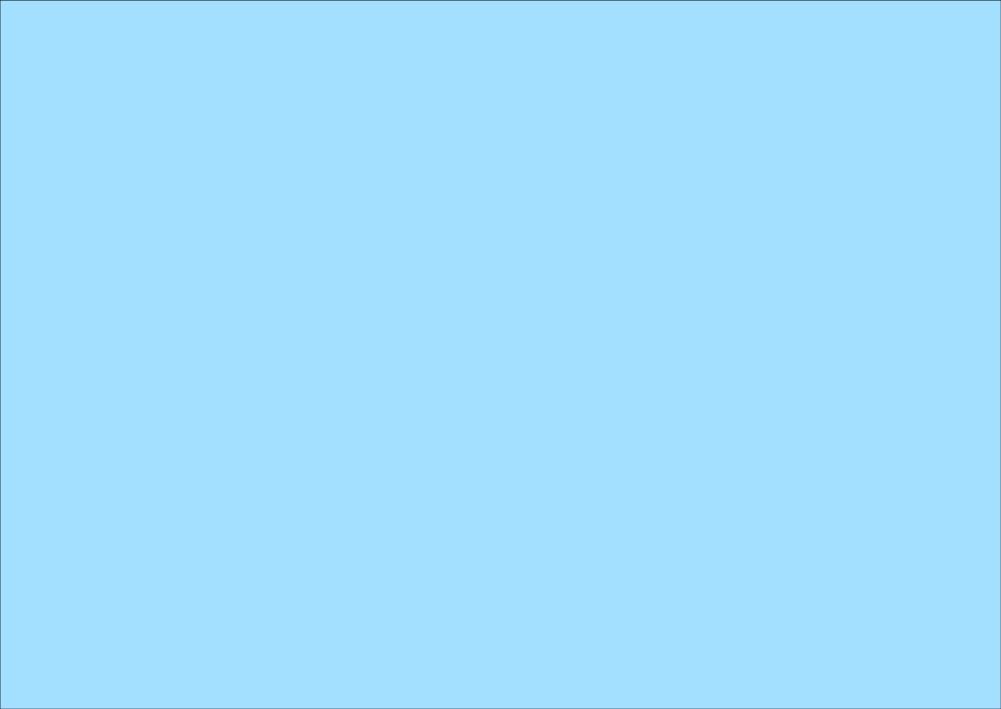
 Entry inhibitors PRO140 (CCR5 mab) Cenicriviroc (CCR5/CCR2 antagonist) Ibalizumab (CD4 mab) BMS 663068 (pro-drug of gp120")
3 Investigational Agents of Interest NRTIs Tenofovir Alafenamide Festinavir (formerly BMS ) NNRTI Doravirine (formerly MK-1439) Rilpivirine (long-acting parenteral nanosuspension) Integrase inhibitor Cabotegravir (oral and long-acting parenteral nanosuspension) Entry inhibitors PRO140 (CCR5 mab) Cenicriviroc (CCR5/CCR2 antagonist) Ibalizumab (CD4 mab) BMS (pro-drug of gp120 attachment inhibitor) Maturation inhibitors BMS Drug Delivery: TDF vs. Tenofovir Alafenamide Fumarate (TAF) 3
 (Elvitegravir/cobicistat/ emtricitabine/taf) E/C/F/TDF qd (n=867) (Elvitegravir/cobicistat/ emtricitabine/tenofovir DF) Week 0 144 E/C/F:")
4 Studies 104 and 111: Tenofovir Alafenamide (TAF) in a Single-Tablet Regimen in Initial HIV Therapy Phase 3 (2 trials combined) Treatment-naive HIV RNA >1000 copies/ml egfr >50 ml/min No HBV or HCV coinfection Randomization 1:1 E/C/F/TAF qd (n=866) (Elvitegravir/cobicistat/ emtricitabine/taf) E/C/F/TDF qd (n=867) (Elvitegravir/cobicistat/ emtricitabine/tenofovir DF) Week E/C/F: elvitegravir/cobicistat/emtricitabine. TAF: tenofovir alafenamide 10 mg; TDF: tenofovir DF 300 mg. Non-inferiority margin: 12% (based on week 48 FDA snapshot analysis of percentage of patients with HIV RNA <50 copies/ml). Baseline characteristics: Median age: years. Male: 85%. Black race/ethnicity: 26%. Median HIV RNA: 4.5 log 10 copies/ml. Median CD4 count: 405 cells/µl. Median egfr: ml/min. Sax PE, et al. Lancet. 2015;385:
 High and similar response rates irrespective of age, sex, baseline HIV RNA level, and baseline CD4 count Gain in CD4 count Significantly greater increase with TAF versus TDF (211 versus 181")

5 Patients (%) Studies 104 and 111: Overall Results With TAF in a Single-Tablet Regimen in Initial HIV Therapy HIV RNA <50 copies/ml TAF was non-inferior to TDF Treatment difference: 2.0% (- 0.7, 4.7) High and similar response rates irrespective of age, sex, baseline HIV RNA level, and baseline CD4 count Gain in CD4 count Significantly greater increase with TAF versus TDF (211 versus 181 cells/µl; P=0.024) Treatment-emergent resistance <1% in both arms HIV RNA <50 Copies/mL (FDA Snapshot Analysis) 92% 90% E/C/F: elvitegravir/cobicistat/emtricitabine. TAF: tenofovir alafenamide; TDF: tenofovir DF. Non-inferiority margin: 12%. Sax PE, et al. Lancet. 2015;385: E/C/F/TAF (n=866) E/C/F/TDF (n=867) Studies 104 and 111: Safety E/C/F/TAF (n=866) E/C/F/TDF (n=867) Discontinuations due to adverse events (%) Most common adverse events (%) Diarrhea Nausea Headache Upper respiratory tract infection Grade 3 or 4 laboratory abnormality (%) Creatine kinase elevation LDL elevation Hypercholesterolemia Hematuria AST elevation Serum amylase elevation Neutropenia (<1000 cells/µl) ALT elevation E/C/F: elvitegravir/cobicistat/emtricitabine; TAF: tenofovir alafenamide; TDF: tenofovir DF. Sax PE, et al. Lancet. 2015;385:
6 Mean Change (%) Mean Change (%) Mean Change (ml/min) Studies 104 and 111: Change in egfr (Cockcroft-Gault) With TAF or TDF TAF versus TDF Significantly smaller decreases in egfr (Cockcroft-Gault) (P<0.001) Significantly less proteinuria, albuminuria, and tubular proteinuria (P<0.001) No cases of tubulopathy/fanconi syndrome in either arm Discontinuations due to renal adverse events E/C/F/TAF: 0 (0%) E/C/F/TDF: 4 (0.5%) Mean Change in egfr E/C/F/TAF (n=866) E/C/F/TDF (n=867) -6.6 P< E/C/F: elvitegravir/cobicistat/emtricitabine. TAF: tenofovir alafenamide; TDF: tenofovir DF Treatment Week Sax PE, et al. Lancet. 2015;385: Studies 104 and 111: Changes in Spine and Hip BMD With TAF or TDF Spine BMD Hip BMD E/C/F/TAF (n=845) E/C/F/TDF (n=850) E/C/F/TAF (n=836) E/C/F/TDF (n=848) P< P< Treatment Week E/C/F: elvitegravir/cobicistat/emtricitabine. TAF: tenofovir alafenamide; TDF: tenofovir DF Treatment Week Sax PE, et al. Lancet. 2015;385:

. Sax PE, et al. Lancet. 2015;385:2606-2615.")

7 Median Values (mg/dl) Studies 104 and 111: Fasting Lipids at Week E/C/F/TAF Baseline Week 48 E/C/F/TDF Baseline Week Total Cholesterol LDL HDL Triglycerides TC:HDL Ratio P<0.001 P<0.001 P<0.001 P=0.027 P=0.84 E/C/F: elvitegravir/cobicistat/emtricitabine; TAF: tenofovir alafenamide; TDF: tenofovir DF. P values are versus comparator arm. Patients initiating lipid-modifying medications: 3.6% E/C/F/TAF versus 2.9% E/C/F/TDF (P=0.42). Sax PE, et al. Lancet. 2015;385: Tenofovir Alafenamide-Containing Single- Tablet PI Regimen in Treatment-Naïve Patients Once-Daily Regimens Phase 2 study (48 weeks) Treatment-naïve Double-blind HIV RNA >5000 copies/ml CD4 >50 cells/mm 3 egfr >70 ml/min No HBV, HCV Randomization 2:1 Darunavir/Cobicistat/ Emtricitabine/Tenofovir Alafenamide 1 Fixed-Dose Combination Tablet (n=103) Darunavir + Cobicistat + Emtricitabine/Tenofovir DF 4 tablets (n=50) Primary Endpoint Week 24 HIV RNA <50 Copies/mL (FDA Snapshot) Mills A, et al. JAIDS. 2015;69:
 90 88 Median HIV RNA (log 10 copies/ml) >100K copies/ml (%) Median CD4 (cells/mm 3 ) <200 cells/mm 3 (%) Estimated GFR (ml/min)")

 DRV + COBI + FTC/TDF (n=50) Weighted Difference:-6.")
8 Patients (%) Single-Tablet PI Regimen: Baseline Demographics DRV/COBI/FTC/TAF (n=103) DRV + COBI + FTC/TDF (n=50) Males (%) Median age (years) Race (%) White/ Black/Hispanic 60/35/22 60/34/18 Asymptomatic HIV infection (%) Median HIV RNA (log 10 copies/ml) >100K copies/ml (%) Median CD4 (cells/mm 3 ) <200 cells/mm 3 (%) Estimated GFR (ml/min) (Cockcroft-Gault) TAF: tenofovir alafenamide. Mills A, et al. JAIDS. 2015;69: Single-Tablet PI Regimen: Virologic and Immunologic Outcomes Viral suppression and failure rate were comparable between both arms No patients developed resistance Both arms were well tolerated Discontinuations due to adverse events low (1% versus 4% in the singleversus multiple- tablet regimen, respectively) 1 case of proximal renal tubulopathy in the multipletablet regimen TAF: tenofovir alafenamide. Mills A, et al. JAIDS. 2015;69: HIV RNA <50 Copies/mL DRV/COBI/FTC/TAF (n=103) DRV + COBI + FTC/TDF (n=50) Weighted Difference:-6.2% Weighted (95% CI: -19.9, 7.4) Difference:+3.3% (95% CI: -11.4, 18.1) 84% 75% 77% 74% Week 24 Week 48 8
9 Single-Tablet PI Regimen: Additional Safety and Tolerability Data Select treatment-emergent adverse events (%)* Diarrhea Upper respiratory tract infection Fatigue Nausea Rash Median change at week 48 (mg/dl) Total cholesterol LDL-C HDL Triglycerides Serum creatinine Week 48 change in bone mineral density (%) Spine Hip DRV/COBI/FTC/TAF (n=103) DRV + COBI + FTC/TDF (n=50) (P<0.001) 4 (P<0.001) 3 (P=0.009) -5 (P=0.007) (P=0.003) (P<0.001) TAF: tenofovir alafenamide. *Grades 1-4, occurring in >10% of patients. Mills A, et al. JAIDS. 2015;69: Switching From TDF- to TAF-Based Regimens in Virologically Suppressed Pts Randomized, active-controlled, open-label study Primary Endpoint Wk 48 Pts with HIV-1 RNA < 50 copies/ml ( 96 wks) and egfr > 50 ml/min on stable TDF-based regimen for 48 wks (N = 1436) Switch to EVG/COBI/FTC/TAF QD* (n = 959) Continue previous TDF-based regimen (n = 477) Continue through Wk 96 *EVG/COBI/FTC/TAF (150/150/200/10 mg). Previous TDF-based regimens: EVG/COBI/FTC/TDF (n = 459), EFV/TDF/FTC (n = 376), ATV/(COBI or RTV) + TDF/FTC (n = 601). Primary endpoint: proportion of pts with HIV-1 RNA < 50 copies/ml after 48 wks of treatment Mills A, et al. IAS Abstract TUAB
10 Median % Change in Spine BMD (Q1, Q3) Wk 48 HIV-1 RNA < 50 c/ml (%) Switching From TDF- to TAF-Based Regimens: Virologic Outcomes Primary Endpoint EVG/COBI/FTC/TAF TDF-based regimen P <.001 P =.02 P =.02 P = NS n/n = 0 932/ / 477 All Prior Regimens 241/ / / / 199 Prior Prior EFV/TDF/FTC Boosted ATV + TDF/FTC 301/ / 153 Prior EVG/COBI/ FTC/TDF Mills A, et al. IAS Abstract TUAB0102. Reproduced with permission. Switching From TDF- to TAF-based Regimens: Renal and Bone Outcomes EVG/COBI/FTC/TAF TDF-based regimen Baseline Wk 24 Wk P <.001 Regimen EVG/COBI/ FTC/TAF (n = 959) TDF-based regimen (n = 477) Renal Events Leading to Discontinuation Acute renal failure Interstitial nephritis Chronic kidney disease Elevated serum creatinine Fanconi syndrome (mild jaundice) Increased creatinine Nephritic colic (nephrolithiasis) Hip BMD was similarly increased for pts treated with TAF regimen (P <.001) Mills A, et al. IAS Abstract TUAB0102. Reproduced with permission. 10
11 Pts (%) Switching Pts With HIV/HBV Coinfection to a TAF-Based Regimen International, multicenter, single-arm, open-label phase IIIb trial (N = 72) Pts with virologically suppressed HIV infection on any regimen, chronic HBV coinfection, and egfr > 50 ml/min switched to EVG/COBI/FTC/TAF for 48 Wks HIV-1 RNA < 50 c/ml HBV DNA < 29 IU/mL Wk 24 Wk By Wk 48, 2/70 (3%) pts lost HBsAg/gained HBsAb; 2/30 (7%) pts had lost HBeAg; 1/30 (3%) pts gained HBeAb Significant improvement in median Wk 48 FibroTest score with switch (-.04; P =.018) Gallant J, et al. IAS Abstract WELBPE13. Reproduced with permission. 0 GS-112: Switching to a TAF-Based Regimen in Pts With Renal Impairment Multicenter, open-label phase III trial Virologically suppressed, HIV-positive pts with mild-moderate renal impairment (stable egfr CG [30-69 ml/min]) (N = 242) TDF-Based ART (n = 158) Non-TDF Based ART (n = 84) Wk 24 Wk 48 EVG/COBI/FTC/TAF (N = 242) Wk 96 PI NNRTI INSTI CCR5 Antag. TDF ABC Other NRTI ART use,% Baseline characteristics: Median age: 58 years. Hypertension/diabetes: 40%/14%. Median CD4: 632 cells/mm 3. Median egfr: 56 ml/min (<60 ml/min: 66%). Dipstick proteinuria grade 1/2/3-4: 23%/10%/0%. Primary Endpoint Week 24 Change From Baseline in egfr No NRTI Gupta S, et al. IAS Abstract TUAB
 Baseline Week 24 59 58 63 63 50 49 0.2-0.6-1.")

12 Actual GFR (ml/min) Change in egfr (ml/min) Study 112: Change in GFR After Switch to E/C/F/TAF in Patients With Renal Impairment Actual GFR at Week 24 (Iohexol Clearance) Mean Change in egfr at Week 48 (Cockcroft-Gault) Baseline Week All Patients Yes No TDF in Previous Regimen Baseline egfr (ml/min): All Patients Yes No TDF in Previous Regimen Gupta S, et al. J Int AIDS Soc. 2015;18(suppl 4): Abstract TUAB Study 112: Change in GFR and Other Outcomes After Switch to E/C/F/TAF Actual GFR was unaffected by E/C/F/TAF switch, regardless of previous regimen egfr remained unchanged through week 48 Significant improvements after E/C/F/TAF switch (P<0.05) Spine and hip bone mineral density Urinary tubular proteins and fractional excretion of uric acid Albuminuria and proteinuria Cholesterol fractions in patients not on a TDF-based regimen at time of switch These 48-week data support the renal and bone safety of E/C/F/TAF in HIV patients with renal impairment (egfr ml/min) Gupta S, et al. J Int AIDS Soc. 2015;18(suppl 4): Abstract TUAB
 PK supportive of once-daily dosing Lai AAC 2014;58:1652-1663 Anderson Antivir Ther")
13 Doravirine (DOR) Investigational NNRTI Pre-clinical Potent at low miligram dose Not a CYP450 inhibitor or inducer Metabolized by CYP3A4 Active in vitro against viral strains with K103N, Y181C, G190A, E101K, E138K or K103N/Y181C Clinical Multiple doses in 40 HIV- men X 10d: no rash/cns events (except HA) PK supportive of once-daily dosing Lai AAC 2014;58: Anderson Antivir Ther 2015;20: Doravirine (DOR): Phase Ib Double-blind, randomized, placebo-controlled Study population: HIV+, treatment-naïve (N=18) Schurmann AIDS 2015 (epub 9/13/15) 13
 Morales-Ramirez CROI 2014 #92LB wk 48: 73% 72% 76% 83% 71% Gatell Glasgow 2014 #O434 Doravirine: Phase 2b (Part 2) Randomized: TDF/FTC + DOR 100 mg vs.")
14 Doravirine: Phase 2b Dose Finding (Part 1) Randomized: TDF/FTC + 4 doses of DOR vs. EFV Results: VL <40 Non-CNS tox 48 wk DOR vs. EFV nausea (8% vs. 2%) fatigue (7% vs. 5%) diarrhea (5% vs. 10%) Morales-Ramirez CROI 2014 #92LB wk 48: 73% 72% 76% 83% 71% Gatell Glasgow 2014 #O434 Doravirine: Phase 2b (Part 2) Randomized: TDF/FTC + DOR 100 mg vs. EFV (N=132) Results (combining parts 1 and 2; N=216): CNS Toxicity (48 wks) overall (DOR 22% vs. EFV 44%; p<0.001) dizziness (DOR 9% vs. EFV 28%) insomnia (DOR 6% vs. EFV 3%) abnormal dreams (DOR 6% vs. EFV 17%) nightmares (DOR 6% vs. EFV 8%) Gatell Glasgow 2014 #O434 Significant interaction with rifampin ( DOR >57%) Judge CROI 2015 #521 14
15 P007: DOR + TDF/FTC vs EFV + TDF/FTC in ART-Naive Pts Infected With HIV Double-blind, randomized, 2-part study Pts were stratified by HIV-1 RNA or > 100,000 copies/ml Wk 96 ART-naive, HIV-positive pts with HIV-1 RNA 1000 copies/ml and CD4+ cell count 100 cells/mm 3 (N = 216*) Doravirine + TDF/FTC (n = 108) Efavirenz + TDF/FTC* (n = 108) *Combined pts from 2 study parts: Part 1 was a dose-finding study (n = 84) and Part 2 enrolled additional pts with the current dosing schema (n = 132). Doravirine dosed at 100 mg QD. Efavirenz dosed at 600 mg QD. Wk 24 results reported. Gatell JM, et al. IAS Abstract TUAB0104. P007: Key Results Pts With HIV-1 RNA < 40 c/ml, %* DOR + TDF/FTC (n = 108) EFV + TDF/FTC (n = 108) Wk Wk Wk Baseline HIV-1 RNA 100,000 c/ml (n/n) 83.3 (55/66) Baseline HIV-1 RNA 60.5 > 100,000 c/ml (n/n) (23/38) 85.7 (54/63) 65.8 (25/38) Event, % DOR + TDF/FTC (N = 108) EFV + TDF/FTC (N = 108) One or more AE Serious AE Discontinued due to AE Drug-related AE Pts with 1 CNS event *NC = F approach. Observed failure approach. Most virologic failure was due to low-level viremia Virologic failure, HIV-1 RNA 40 copies/ml: DOR, 15.7%; EFV, 10.2% Virologic failure, HIV-1 RNA 200 copies/ml: DOR, 3.7%; EFV, 0.9% Resistance testing was performed in 1 pt in each arm who failed treatment; no NRTI or NNRTI mutations detected Gatell JM, et al. IAS Abstract TUAB


")






 Adapted from Moore JP,")
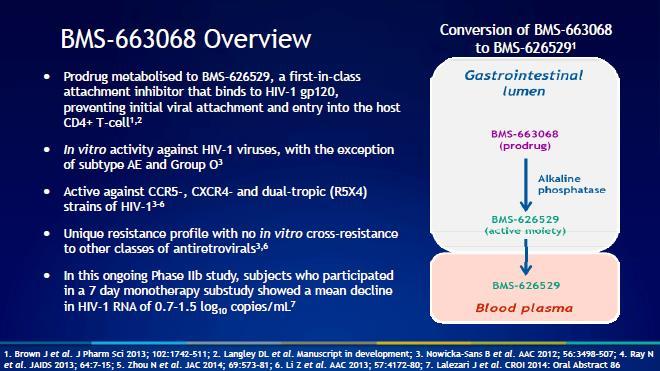
16 DOR Phase 2: Study 007 Study regimen: TDF/FTC + DOR or EFV 100,000 c/ml >100,000 c/ml n/n 55/66 54/63 61/66 58/63 23/38 25/38 35/38 36/38 Patients with >1 CNS event: 27% (DOR) vs. 46% (EFV) *Excludes: Patients who discontinued due to non-treatment related reasons but with last RNA <40 c/ml, or due to AE, or who lack data in week 24 window. Gatell IAS 2015 #TUAB0104 HIV Entry Inhibitors CD4 Binding Coreceptor Binding Virus-Cell Fusion BMS Ibalizumab gp41 gp120 CCR5 Inhibitors maraviroc enfuvirtide V3 loop CD4 Cell Membrane CCR5/CXCR4 (R5/X4) Adapted from Moore JP, PNAS 2003;100:
17 17
 FDA breakthrough")
18 BMS : Resistance, Mechanism, PK gp 160 population sequencing: M426L substitution correlated with resistance (high IC50 and poor VR) no selection of M426L day 1 to 8 Temsavir (BMS ) binds pre-cd4 bound gp120, restricting conformational change No PK Interactions with ATV or ATV/r No PK Interactions with DRV/r or DRV/r + ETR (ETR alone fostemsavir -BMS ) FDA breakthrough designation 7/15 Zhou JAC 2014;69:573 Langley Proteins 2014 (epub) Zhu CROI 2013 #534 Landry CROI 2015 #523 18
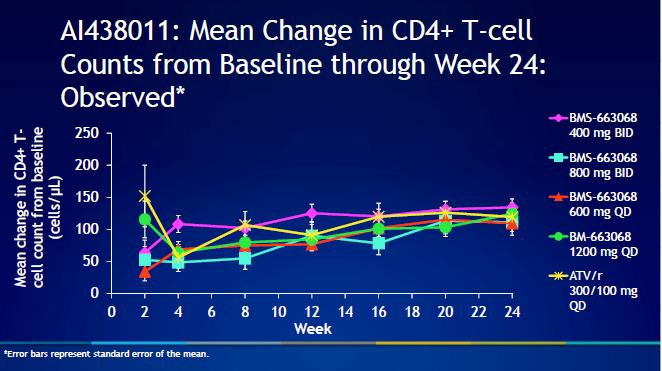
 BMS-626529 binds to HIV-1 gp120 (prevents initial attachment and cell entry in host CD4) HIV RNA >1000")


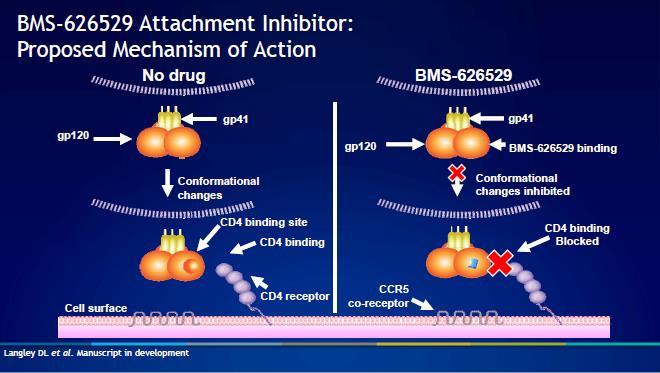
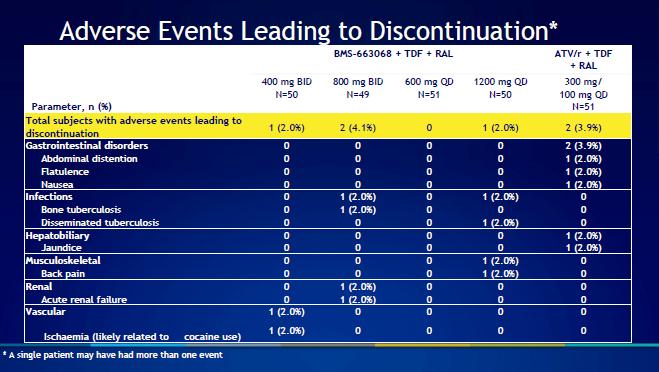
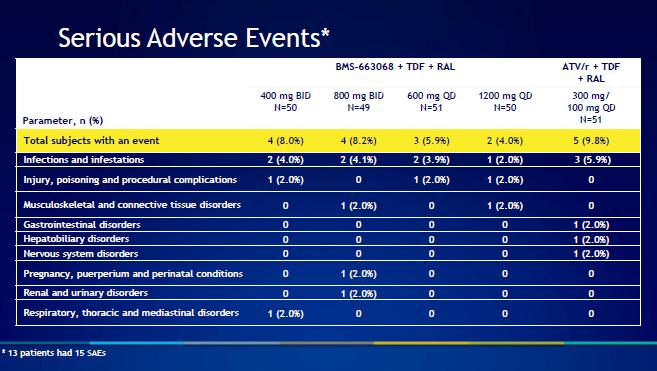
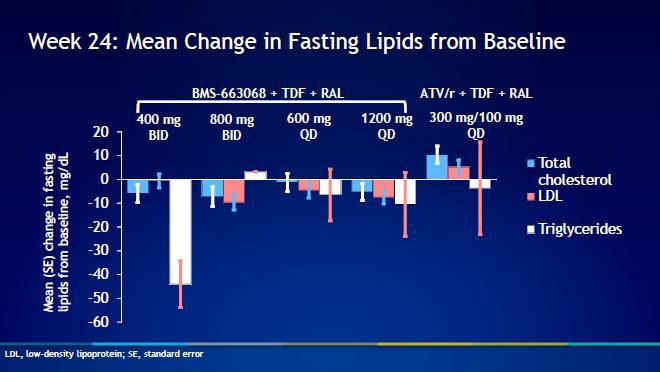
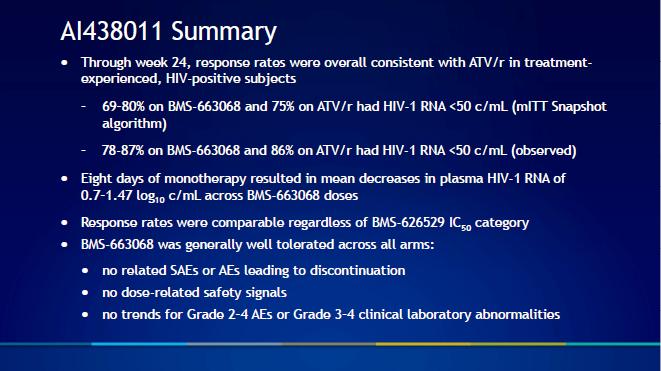
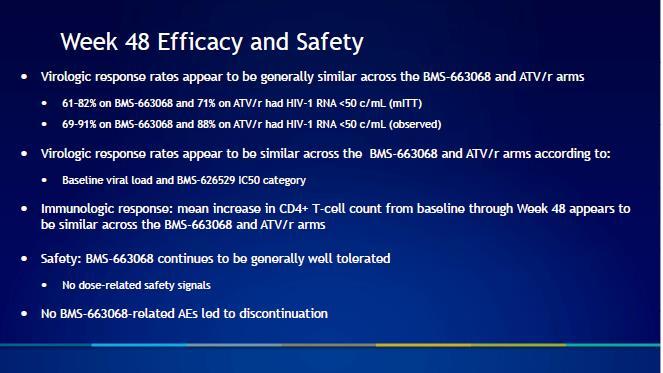
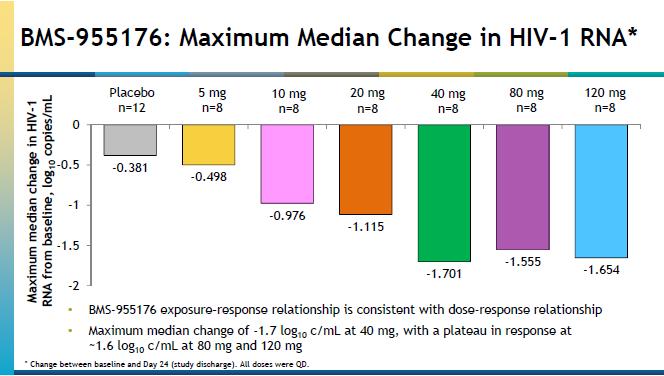
19 Patients (%) BMS (HIV-1 Attachment Inhibitor Prodrug) in ART Experienced Patients (Interim Results) Ongoing, phase 2b, dose-ranging study in treatment-experienced patients (n=251) BMS binds to HIV-1 gp120 (prevents initial attachment and cell entry in host CD4) HIV RNA >1000 copies/ml CD4 >50 cells/mm 3 Randomized arms were raltegravir + tenofovir DF and either BMS or 800 mg bid, 600 or 1200 mg qd Atazanavir/r Similar CD4 gains in all arms Well tolerated with no dose-response safety signal baseline susceptibility in 12% of pts due to envelope polymorphisms; screened by baseline IC 50 Patients were pre-screened for baseline resistance.. Lalezari J, et al. 21 st CROI. Boston, Abstract % 400 bid (n=50) Week 24 Interim Results ( FDA Snapshot ) 69% 800 bid (n=49) 77% 600 qd (n=51) BMS (mg) 72% 1200 qd (n=50) 75% ATV/r qd (n=51) 19
20 20
21 21
22 22
23 23
 Humanized monoclonal")

24 Ibalizumab: HIV-neutralizing mab directed to domain 2 of human CD4 (5A8, TNX-355) Humanized monoclonal antibody Structure of ibalizumab Fab bound to 2-domain CD4 (2.2Å) Freeman et al, Structure, in press 24
25 Maximum percent inhibition (MPI) IC 50 ( g/ml) Breadth and potency of ibalizumab (MPI and IC50) against a panel of 118 HIV clones Viruses 0.01 Ibalizumab Mechanism of Action: HIV-1 entry inhibitor. Ibalizumab, a humanized monoclonal antibody (mab), binds to extracellular domain 2 of the CD4 receptor. Half-life (T½): 3 to 3.5 days on average Currently in Phase III trial for HIVinfected, treatment-experienced adults infected with multi-drug resistant HIV-1. Dose: Loading dose of 2000 mg IV infusion followed by IV ibalizumab 800 mg every 2 weeks 25
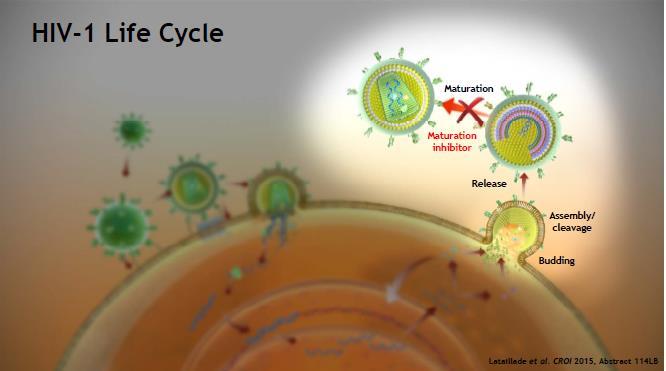
26 Ibalizumab as PrEP? Moving toward proof of principle with the current form: Phase 1 study in healthy volunteers Passive protection against SIV challenge in macaques Making a better ibalizumab: Improve route Improve stability Improve affinity Improve PK Improve breadth Ultimate goal: Decrease dose to <10 mg Decrease frequency to 2 months Decrease cost 51 HIV Maturation Inhibitor 26
27 27
28 28
29 29
30 30
 BMS-955176 40 mg QD + ATV 300 mg QD + RTV 100 mg QD -2.")
31 AI468002: BMS ATV ± RTV for Treating Pts Infected With HIV Randomized, multipart phase IIa trial Max. Median Decline Day 28* in HIV-1 RNA through Day 42 (log 10 c/ml) BMS mg QD + ATV 300 mg QD + RTV 100 mg QD (n = 8) HIV, subtype B infected PI- and MI-naive pts with HIV-1 RNA 5000 c/ml and CD4+ cell count 200 cells/mm 3 (N = 28) BMS mg QD + ATV 400 mg QD (n = 8) BMS mg QD + ATV 400 mg QD (n = 8) ATV 300 mg QD + RTV 100 mg QD + TDF 300 mg QD/FTC 200 mg QD (n = 4) *Followed through Day 42. BMS prevents viral maturation by inhibiting cleavage between p24 and Gag SP No serious AEs or discontinuations for AEs 1 grade 3/4 Tx-related AE in BMS mg + ATV 400 mg arm (transient neutropenia) Hwang C, et al. IAS Abstract TUAB0106LB. 31
32 Cabotegravir (CAB) Integrase inhibitor similar to DTG; similar resistance Potent in HIV+ individuals (5, 10, 30, 60 mg oral) Margolis EACS 2013; Spreen HIV Clin Trials 2013;14:192 Nanotechology formulation; SC + IM injections T ½ days! Supports monthly or quarterly dosing Safety: ISR (all mild) and nodules with SC dosing Treatment + prevention Spreen JAIDS 2014;67:481 Combination of CAB LAP + RPV-LA Phase 1 pilot study, randomized, repeat doseescalation study with oral lead-in (of CAB) in HIV- individuals (N=47) Monthly and quarterly dosing of CAB LAP IM with co-dosed monthly RPV-LA SC Endpoints: Safety, tolerability, PK Results: generally safe and well-tolerated with grade 1 ISR most common; target drug concentrations achieved Spreen JAIDS 2014;67:487 32
33 LATTE Study: Cabotegravir + Rilpivirine as 2-Drug Oral Maintenance Therapy Phase 2b study (96 weeks) Treatment-naïve Open-label HIV RNA >1000 copies/ml CD4 >200 cells/mm 3 Stratified by HIV RNA and NRTI Induction (24 weeks) Cabotegravir (10, 30, 60 mg) + 2 NRTIs* Maintenance (72 weeks) 744 (10, 30, 60 mg) + Rilpivirine Efavirenz + 2 NRTIs* Week Primary Endpoint HIV RNA <50 copies/ml (FDA Snapshot ) Patients in the cabotegravir arm with HIV RNA <50 copies/ml at week 20 were switched to a maintenance regimen at week 24. Cabotegravir: novel integrase inhibitor that is a dolutegravir analogue (oral and injectable formulations). *Emtricitabine/tenofovir DF or abacavir/lamivudine. Margolis DA, et al. Lancet Infect Dis. 2015;Jul 17. [Epub ahead of print]. LATTE 1: CAB and RPV Oral Maintenance Virologic Success: HIV-1 RNA <50 c/ml by FDA Snapshot (ITT-E) Proportion, % (95% CI) 100 BL CAB 10 mg (n=60) CAB 60 mg (n=61) CAB 30 mg (n=60) EFV 600 mg (n=62) Margolis Lancet ID 2015 (epub 7/17/15) 33
34 LATTE Study: Cabotegravir + Rilpivirine as 2-Drug Oral Maintenance Therapy Oral cabotegravir + rilpivirine maintained HIV RNA suppression at a similar rate as efavirenz + 2 NRTIs Resistance at virologic failure 1 patient with both integrase and NNRTI resistance (previously reported) 2 patients with NNRTI resistance only Cabotegravir regimen was well tolerated, with a low discontinuation rate due to adverse events (3.9%) Cabotegravir 60-mg dose had more adverse events and discontinuations relative to the 10- and 30-mg arms Cabotegravir 30 mg qd was selected for further clinical development HIV RNA <50 copies/ml (%) Week 96 Results Cabotegravir (n=181) EFV (n=62) CD4 gain (cells/mm 3 ) Virologic failure (%) 3 10 Discontinuations due to adverse events (%) Key Outcomes Select grade 3/4 laboratory abnormalities (%) CPK ALT Lipase Total bilirubin Total neutrophils Creatinine Margolis DA, et al. Lancet Infect Dis. 2015;Jul 17. [Epub ahead of print]. Which describes best how HIV Maturation Inhibitors Work? A. Block of release of budding viral progeny from CD4 cell surface B. Block integration of HIV DNA from forming stable pro-virus C. Inhibits protease cleavage step of viral polypeptide D. Engages virus in endless video game play 77% 15% 8% Block of release of buddi.. Block integration of HIV... Inhibits protease cleavag... Engages virus in endless... 0% 34

35 Which describes best how HIV Maturation Inhibitors Work? Block of release of budding viral progeny from CD4 cell surface 8% 8% Block integration of HIV DNA from forming stable pro-virus 15% 15% Inhibits protease cleavage step of viral polypeptide 77% 77% Engages virus in endless video game play 0% 0% First Slide Second Slide Thank you Joseph P. McGowan, MD 35
DRUGS IN PIPELINE. Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015
 DRUGS IN PIPELINE Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015 N(t)RTI The Development of TAF TAF Delivers the High Potency of TDF While Minimizing Off- Target Kidney and Bone Side Effects
DRUGS IN PIPELINE Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015 N(t)RTI The Development of TAF TAF Delivers the High Potency of TDF While Minimizing Off- Target Kidney and Bone Side Effects
Didactic Series. CROI New Antiretroviral Therapies. Daniel Lee, MD Clinical Professor of Medicine UCSD Medical Center Owen Clinic July 14, 2016
 Didactic Series CROI 2016 - New Antiretroviral Therapies Daniel Lee, MD Clinical Professor of Medicine UCSD Medical Center Owen Clinic July 14, 2016 This project is supported by the Health Resources and
Didactic Series CROI 2016 - New Antiretroviral Therapies Daniel Lee, MD Clinical Professor of Medicine UCSD Medical Center Owen Clinic July 14, 2016 This project is supported by the Health Resources and
Disclosures (last 12 months)
") HIV Research What s in the Pipeline? Samir K. Gupta, MD, MS Division of Infectious Diseases Indiana University School of Medicine Disclosures (last 12 months) Independent research grant funding by NIH/NHLBI,
HIV Research What s in the Pipeline? Samir K. Gupta, MD, MS Division of Infectious Diseases Indiana University School of Medicine Disclosures (last 12 months) Independent research grant funding by NIH/NHLBI,
Roy M. Gulick, MD, MPH Rochelle Belfer Professor in Medicine Weill Cornell Medicine New York, New York
 Antiretroviral Therapy: Investigational New Drugs and New Strategies Roy M. Gulick, MD, MPH Rochelle Belfer Professor in Medicine Weill Cornell Medicine New York, New York FORMATTED: MM/DD/YY Antiretroviral
Antiretroviral Therapy: Investigational New Drugs and New Strategies Roy M. Gulick, MD, MPH Rochelle Belfer Professor in Medicine Weill Cornell Medicine New York, New York FORMATTED: MM/DD/YY Antiretroviral
ARVs in Development: Where do they fit?
 The picture can't be displayed. ARVs in Development: Where do they fit? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker
The picture can't be displayed. ARVs in Development: Where do they fit? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker
Tenofovir Alafenamide (TAF)
") Frontier AIDS Education and Training Center Tenofovir Alafenamide (TAF) Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director, Frontier AETC ECHO January 28, 2016
Frontier AIDS Education and Training Center Tenofovir Alafenamide (TAF) Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director, Frontier AETC ECHO January 28, 2016
CROI 2013: New Drugs for Treatment and PrEP
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER CROI 2013: New Drugs for Treatment and PrEP Brian R. Wood, MD Medical Director, NW AETC Project ECHO Assistant Professor of Medicine, University of Washington
NORTHWEST AIDS EDUCATION AND TRAINING CENTER CROI 2013: New Drugs for Treatment and PrEP Brian R. Wood, MD Medical Director, NW AETC Project ECHO Assistant Professor of Medicine, University of Washington
STRIBILD (aka. The Quad Pill)
") NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
HIV Update Allegra CPD Day Program Port Elizabeth Dr L E Nojoko
 HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
Antiretroviral Therapy in 2016
 Antiretroviral Therapy in 2016 Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
Antiretroviral Therapy in 2016 Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
WHEN TO START? CROI 2015: Focus on ART
 CROI 215: Focus on ART FORMATTED: 4-1-15 Washington, DC: May 13, 215 Roy M. Gulick, MD, MPH Gladys and Roland Harriman Professor of Medicine Chief, Division of Infectious Diseases Weill Cornell Medical
CROI 215: Focus on ART FORMATTED: 4-1-15 Washington, DC: May 13, 215 Roy M. Gulick, MD, MPH Gladys and Roland Harriman Professor of Medicine Chief, Division of Infectious Diseases Weill Cornell Medical
Efficacy and Safety of Doravirine 100mg QD vs Efavirenz 600mg QD with TDF/FTC in ART-Naive HIV-Infected Patients: Week 24 Results
 Efficacy and Safety of Doravirine 1mg QD vs Efavirenz 6mg QD with TDF/FTC in ART-Naive HIV-Infected Patients: Week 24 Results Jose M. Gatell, Francois Raffi, Andreas Plettenberg, Don Smith, Joaquin Portilla,
Efficacy and Safety of Doravirine 1mg QD vs Efavirenz 6mg QD with TDF/FTC in ART-Naive HIV-Infected Patients: Week 24 Results Jose M. Gatell, Francois Raffi, Andreas Plettenberg, Don Smith, Joaquin Portilla,
Abstract PS8/2. Double-blind treatment phase D/C/F/TAF. + matching D/C + F/TDF placebo D/C/F/TAF. D/C + F/TDF + matching D/C/F/TAF placebo
 WEEK 8 RESULTS OF AMBER: A PHASE 3, RANDOMISED, DOUBLE-BLIND TRIAL IN ANTIRETROVIRAL TREATMENT (ART)-NAÏVE HIV--INFECTED ADULTS TO EVALUATE THE EFFICACY AND SAFETY OF THE ONCE-DAILY, SINGLE-TABLET REGIMEN
WEEK 8 RESULTS OF AMBER: A PHASE 3, RANDOMISED, DOUBLE-BLIND TRIAL IN ANTIRETROVIRAL TREATMENT (ART)-NAÏVE HIV--INFECTED ADULTS TO EVALUATE THE EFFICACY AND SAFETY OF THE ONCE-DAILY, SINGLE-TABLET REGIMEN
Antiretroviral Therapy: What to Start
 FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
David Cluck, PharmD, BCPS, AAHIVP Associate Professor of Pharmacy Practice Office 326 Phone
 David Cluck, PharmD, BCPS, AAHIVP Associate Professor of Pharmacy Practice Office 326 Phone 423-439-6245 Email cluckd@etsu.edu Recall newly approved antiretrovirals and their respective place in therapy
David Cluck, PharmD, BCPS, AAHIVP Associate Professor of Pharmacy Practice Office 326 Phone 423-439-6245 Email cluckd@etsu.edu Recall newly approved antiretrovirals and their respective place in therapy
Are the current doses of ARV correct. Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine
 Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
The next generation of ART regimens
 The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
Antiretroviral Treatment Strategies: Clinical Case Presentation
 Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Tim Horn Deputy Executive Director, HIV & HCV Programs Treatment Action Group NASTAD Prevention and Care Technical Assistance Meeting Washington, DC
 Tim Horn Deputy Executive Director, HIV & HCV Programs Treatment Action Group NASTAD Prevention and Care Technical Assistance Meeting Washington, DC July 19, 2017 Pipeline is robust! Several drugs, coformulations,
Tim Horn Deputy Executive Director, HIV & HCV Programs Treatment Action Group NASTAD Prevention and Care Technical Assistance Meeting Washington, DC July 19, 2017 Pipeline is robust! Several drugs, coformulations,
Investigational Approaches to Antiretroviral Therapy
 Investigational Approaches to Antiretroviral Therapy Rajesh T. Gandhi, MD Massachusetts General Hospital Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending
Investigational Approaches to Antiretroviral Therapy Rajesh T. Gandhi, MD Massachusetts General Hospital Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending
CROI 2017 Highlights What s New in Antiretrovirals (Part 2)
") Mountain West AIDS Education and Training Center CROI 2017 Highlights What s New in Antiretrovirals (Part 2) Ann Collier, MD This presentation is intended for educational use only, and does not in any
Mountain West AIDS Education and Training Center CROI 2017 Highlights What s New in Antiretrovirals (Part 2) Ann Collier, MD This presentation is intended for educational use only, and does not in any
Didactic Series. CROI Update - II. Christian B. Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic 5/28/15
 Didactic Series CROI Update - II Christian B. Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic 5/28/15 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine
Didactic Series CROI Update - II Christian B. Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic 5/28/15 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine
23 rd CROI Report Back AETC/Community Consortium Harry W. Lampiris, MD Professor of Clinical Medicine, UCSF Chief, ID Section, Medical Service,
 23 rd CROI Report Back AETC/Community Consortium Harry W. Lampiris, MD Professor of Clinical Medicine, UCSF Chief, ID Section, Medical Service, SFVAMC March 23, 2016 Boston, MA, February 22-25, 2016 Disclosures
23 rd CROI Report Back AETC/Community Consortium Harry W. Lampiris, MD Professor of Clinical Medicine, UCSF Chief, ID Section, Medical Service, SFVAMC March 23, 2016 Boston, MA, February 22-25, 2016 Disclosures
Cabotegravir Long-Acting (LA) Injectable Nanosuspension Bill Spreen, for ViiV Healthcare & GSK Development Team. 17 th HIV-HEPPK June 2016
 Injectable Nanosuspension Bill Spreen, for ViiV Healthcare & GSK Development Team. 17 th HIV-HEPPK June 2016") Cabotegravir Long-Acting (LA) Injectable Nanosuspension Bill Spreen, for ViiV Healthcare & GSK Development Team RPV CAB CAB RPV 1 June 2016 Cabotegravir Long-Acting Nanosuspension CAB is an investigational
Cabotegravir Long-Acting (LA) Injectable Nanosuspension Bill Spreen, for ViiV Healthcare & GSK Development Team RPV CAB CAB RPV 1 June 2016 Cabotegravir Long-Acting Nanosuspension CAB is an investigational
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
 ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals Are You Ready? New Drugs Are on the Way!
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals Are You Ready? New Drugs Are on the Way!
Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi
 6 th INFECtivology TOday Paestum 15-16 -17 maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie
6 th INFECtivology TOday Paestum 15-16 -17 maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie
SINGLE. Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects
 in treatment-naïve subjects") SINGLE Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects SE/HIV/0023/14 January 2014 PHASE III DTG TRIALS IN TREATMENT-NAÏVE ADULT SUBJECTS WITH HIV SINGLE 1 N=833 Phase III non-inferiority,
SINGLE Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects SE/HIV/0023/14 January 2014 PHASE III DTG TRIALS IN TREATMENT-NAÏVE ADULT SUBJECTS WITH HIV SINGLE 1 N=833 Phase III non-inferiority,
Case 1 continued. Case 1 (cont) 12/8/16. MMAH Debate Panel Thursday, December 8, Case 1
 12/8/16. MMAH Debate Panel Thursday, December 8, Case 1") MMAH Debate Panel Thursday, December 8, 2016 Case 1 HPI 55 yo man with newly diagnosed HIV initiates care in your clinic. His CD4+ cell count is 600, with HIV VL=90,000 copies/ml. He is asymptomatic at
MMAH Debate Panel Thursday, December 8, 2016 Case 1 HPI 55 yo man with newly diagnosed HIV initiates care in your clinic. His CD4+ cell count is 600, with HIV VL=90,000 copies/ml. He is asymptomatic at
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches
 Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Switching antiretroviral therapy to safer strategies based on integrase inhibitors
 Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
HIV Treatment: State of the Art 2013
 HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
Long-Acting Antiretrovirals for HIV
 Long-Acting Antiretrovirals for HIV R.M. Gulick, MD, MPH Rochelle Belfer Professor in Medicine Chief, Division of Infectious Diseases Weill Cornell Medicine New York City Disclosures None Single Tablet
Long-Acting Antiretrovirals for HIV R.M. Gulick, MD, MPH Rochelle Belfer Professor in Medicine Chief, Division of Infectious Diseases Weill Cornell Medicine New York City Disclosures None Single Tablet
Investigational Approaches to Antiretroviral Therapy: New Strategies and Novel Agents
 Investigational Approaches to Antiretroviral Therapy: New Strategies and Novel Agents Joseph J. Eron MD Professor of Medicine University of North Carolina Chapel Hill, North Carolina Learning Objectives
Investigational Approaches to Antiretroviral Therapy: New Strategies and Novel Agents Joseph J. Eron MD Professor of Medicine University of North Carolina Chapel Hill, North Carolina Learning Objectives
Investigational Approaches to Antiretroviral Therapy
 Investigational Approaches to Antiretroviral Therapy Rajesh T. Gandhi, MD Massachusetts General Hospital Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending
Investigational Approaches to Antiretroviral Therapy Rajesh T. Gandhi, MD Massachusetts General Hospital Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending
CROI 2015: Treatment and Cure Highlights
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER CROI 2015: Treatment and Cure Highlights Shireesha Dhanireddy Robert Harrington March 17, 2014 No financial conflicts of interest Outline Treatment Studies
NORTHWEST AIDS EDUCATION AND TRAINING CENTER CROI 2015: Treatment and Cure Highlights Shireesha Dhanireddy Robert Harrington March 17, 2014 No financial conflicts of interest Outline Treatment Studies
GS-1489: STUDY DESIGN
 A PHASE 3 RANDOMIZED CONTROLLED CLINICAL TRIAL OF BICTEGRAVIR IN A FIXED DOSE COMBINATION,, VS ABC/DTG/3TC IN TREATMENT-NAÏVE ADULTS AT WEEK 48 J. Gallant, A. Lazzarin, A. Mills, C. Orkin, D. Podzamczer,
A PHASE 3 RANDOMIZED CONTROLLED CLINICAL TRIAL OF BICTEGRAVIR IN A FIXED DOSE COMBINATION,, VS ABC/DTG/3TC IN TREATMENT-NAÏVE ADULTS AT WEEK 48 J. Gallant, A. Lazzarin, A. Mills, C. Orkin, D. Podzamczer,
BHIVA Best of CROI Feedback Meetings. London Birmingham North West England Cardiff Gateshead Edinburgh
 BHIVA Best of CROI Feedback Meetings London Birmingham North West England Cardiff Gateshead Edinburgh BHIVA Best of CROI Feedback Meetings 2010 ANTIRETROVIRAL TREATMENT STRATEGIES AND NEW DRUGS A5202:
BHIVA Best of CROI Feedback Meetings London Birmingham North West England Cardiff Gateshead Edinburgh BHIVA Best of CROI Feedback Meetings 2010 ANTIRETROVIRAL TREATMENT STRATEGIES AND NEW DRUGS A5202:
4/14/2016. Breaking News From the 2016 Conference on Retroviruses and Opportunistic Infections
 Breaking News From the 2016 Conference on Retroviruses and Opportunistic Infections Jeffrey L. Lennox, MD Professor of Medicine Associate Dean for Clinical Research Emory University School of Medicine
Breaking News From the 2016 Conference on Retroviruses and Opportunistic Infections Jeffrey L. Lennox, MD Professor of Medicine Associate Dean for Clinical Research Emory University School of Medicine
HIV Treatment Update 8/3/2015. When to Start. Disclosures
 8/3/215 HIV Treatment Update Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
8/3/215 HIV Treatment Update Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
COMPETING INTEREST OF FINANCIAL VALUE
 BHIVA AUTUMN CONFERENCE 2012 Including CHIVA Parallel Sessions Dr Ian Williams University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Ian Williams
BHIVA AUTUMN CONFERENCE 2012 Including CHIVA Parallel Sessions Dr Ian Williams University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Ian Williams
State of the ART: Integrase Inhibitors Clinical Data. Juan Berenguer Hospital General Universitario Gregorio Marañón (IiSGM) Madrid, Spain
 Madrid, Spain") State of the ART: Integrase Inhibitors Clinical Data Juan Berenguer Hospital General Universitario Gregorio Marañón (IiSGM) Madrid, Spain Disclosures Consulting fees and honoraria Gilead, Janssen, MSD,
State of the ART: Integrase Inhibitors Clinical Data Juan Berenguer Hospital General Universitario Gregorio Marañón (IiSGM) Madrid, Spain Disclosures Consulting fees and honoraria Gilead, Janssen, MSD,
Clinical support for reduced drug regimens. David A Cooper The University of New South Wales Sydney, Australia
 Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
The results of the ARTEN study. Vicente Soriano Hospital Carlos III, Madrid, Spain
 The results of the ARTEN study Vicente Soriano Hospital Carlos III, Madrid, Spain Nevirapine: a well-defined efficacy and tolerability profile High efficacy levels 1 3 Well-defined safety profile 4 Favourable
The results of the ARTEN study Vicente Soriano Hospital Carlos III, Madrid, Spain Nevirapine: a well-defined efficacy and tolerability profile High efficacy levels 1 3 Well-defined safety profile 4 Favourable
Development of a protease inhibitor-based single-tablet complete HIV-1 regimen of darunavir/cobicistat/emtricitabine/tenofovir
 Development of a protease inhibitor-based single-tablet complete HIV-1 regimen of darunavir/cobicistat/emtricitabine/tenofovir alafenamide () Bryan Baugh 1, Erika Van Landuyt 2, Simon Vanveggel 2, Herta
Development of a protease inhibitor-based single-tablet complete HIV-1 regimen of darunavir/cobicistat/emtricitabine/tenofovir alafenamide () Bryan Baugh 1, Erika Van Landuyt 2, Simon Vanveggel 2, Herta
IAS 2015: Return to Vancouver
 IAS 2015: Return to Vancouver Paul E. Sax, M.D. Clinical Director, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School NEAETC Memories from 1996 First
IAS 2015: Return to Vancouver Paul E. Sax, M.D. Clinical Director, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School NEAETC Memories from 1996 First
ART Treatment. ART Treatment
 Naïve Experienced Strategies ARV in pregnancy ART Treatment Naïve studies: ART Treatment Abstract 37 Atazanavir/r vs Lopinavir/r: Castle study Abstract 774 Kivexa vs Truvada: HEAT study Abstract 775 Lopinavir/r
Naïve Experienced Strategies ARV in pregnancy ART Treatment Naïve studies: ART Treatment Abstract 37 Atazanavir/r vs Lopinavir/r: Castle study Abstract 774 Kivexa vs Truvada: HEAT study Abstract 775 Lopinavir/r
HIV Treatment: New and Veteran Drugs Classes
 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
Cabotegravir + Rilpivirine as Long-Acting Maintenance Therapy: LATTE-2 Week 32 Results
 Slide 1 Cabotegravir + Rilpivirine as Long-Acting Maintenance Therapy: LATTE-2 Week 32 Results David A. Margolis, 1 Juan Gonzalez-Garcia, 2 Hans-Jürgen Stellbrink, 3 Joe Eron, 4 Yazdan Yazdanpanah, 5 Sandy
Slide 1 Cabotegravir + Rilpivirine as Long-Acting Maintenance Therapy: LATTE-2 Week 32 Results David A. Margolis, 1 Juan Gonzalez-Garcia, 2 Hans-Jürgen Stellbrink, 3 Joe Eron, 4 Yazdan Yazdanpanah, 5 Sandy
More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD
 More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD More Options, Some Opinions: Initial Therapies for HIV Judith S. Currier, MD University of California Los Angeles Los Angeles,
More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD More Options, Some Opinions: Initial Therapies for HIV Judith S. Currier, MD University of California Los Angeles Los Angeles,
Switching antiretroviral therapy to safer strategies based on integrase inhibitors. Pedro Cahn
 Switching antiretroviral therapy to safer strategies based on integrase inhibitors Pedro Cahn Disclosures Research Grants: Abbvie-Merck-Richmond-ViiV Advisory boards: Merck-Sandoz-ViiV Switching in Virologically
Switching antiretroviral therapy to safer strategies based on integrase inhibitors Pedro Cahn Disclosures Research Grants: Abbvie-Merck-Richmond-ViiV Advisory boards: Merck-Sandoz-ViiV Switching in Virologically
Integrase Inhibitors in the Treatment HIV-Infection. Andrew Zolopa, MD Stanford University
 Integrase Inhibitors in the Treatment HIV-Infection Andrew Zolopa, MD Stanford University 1 IAS-USA 212 Guidelines Updated Recommendations When to start ART is now recommended for all patients, regardless
Integrase Inhibitors in the Treatment HIV-Infection Andrew Zolopa, MD Stanford University 1 IAS-USA 212 Guidelines Updated Recommendations When to start ART is now recommended for all patients, regardless
2017 NSTC Annual Meeting Eric Daar April 18, 2017
 Antiretroviral Therapy Update for TB Clinicians Eric S. Daar, M.D. Chief, Division of HIV Medicine Harbor-UCLA Medical Center Professor of Medicine David Geffen School of Medicine at UCLA Grants Consultant
Antiretroviral Therapy Update for TB Clinicians Eric S. Daar, M.D. Chief, Division of HIV Medicine Harbor-UCLA Medical Center Professor of Medicine David Geffen School of Medicine at UCLA Grants Consultant
CROI 2018 Report Back
 CROI 2018 Report Back Monika Roy, MD MAS Assistant Professor Division of HIV, Infectious Diseases, and Global Medicine bayareaaetc.org 1 Disclosures and Conflicts of Interest Nothing to report bayareaaetc.org
CROI 2018 Report Back Monika Roy, MD MAS Assistant Professor Division of HIV, Infectious Diseases, and Global Medicine bayareaaetc.org 1 Disclosures and Conflicts of Interest Nothing to report bayareaaetc.org
Starting and Switching ART: 2016
 Starting and Switching ART: 2016 Luke Jerram Rajesh T. Gandhi, M.D. Massachusetts General Hospital Harvard Medical School Disclosures: grant support from EBSCO, Gilead, Merck, Viiv Thanks to Henry Sunpath,
Starting and Switching ART: 2016 Luke Jerram Rajesh T. Gandhi, M.D. Massachusetts General Hospital Harvard Medical School Disclosures: grant support from EBSCO, Gilead, Merck, Viiv Thanks to Henry Sunpath,
Individual Study Table Referring to the Dossier SYNOPSIS. Final Clinical Study Report for Study AI424138
 Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Reyataz Name of Active Ingredient: Atazanavir () Individual Study Table Referring to the Dossier (For National Authority Use Only)
Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Reyataz Name of Active Ingredient: Atazanavir () Individual Study Table Referring to the Dossier (For National Authority Use Only)
Integrase Strand Transfer Inhibitors on the Horizon
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Integrase Strand Transfer Inhibitors on the Horizon David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Integrase Strand Transfer Inhibitors on the Horizon David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, University of Washington Presentation
HIV Treatment Update. Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London
 HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
5/2/2016. Antiretroviral Therapy (ART) Strategies: A Case-Based, Panel Discussion
 Strategies: A Case-Based, Panel Discussion") Antiretroviral Therapy (ART) Strategies: A Case-Based, Panel Discussion Joseph J. Eron, Jr, MD Professor of Medicine University of North Carolina at Chapel Hill Chapel Hill, North Carolina FORMATTED: 4/13/216
Antiretroviral Therapy (ART) Strategies: A Case-Based, Panel Discussion Joseph J. Eron, Jr, MD Professor of Medicine University of North Carolina at Chapel Hill Chapel Hill, North Carolina FORMATTED: 4/13/216
VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects
 VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects IL/DLG/0040/14 June 2014 GSK (Israel) Ltd. Basel 25, Petach Tikva. Tel-03-9297100 Medical information service: il.medinfo@gsk.com
VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects IL/DLG/0040/14 June 2014 GSK (Israel) Ltd. Basel 25, Petach Tikva. Tel-03-9297100 Medical information service: il.medinfo@gsk.com
Third Agent Advantages Disadvantages. Component Tenofovir/emtricitabine (TDF/FTC) 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily
 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily") Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
12th European AIDS Conference / EACS ARV Therapies and Therapeutic Strategies A CME Newsletter
 EACS 2009 11-14, November 2009 Cologne, Germany Course Director Jürgen K. Rockstroh, MD Co-Chairman, 12th European AIDS Conference Professor, University of Bonn Bonn, Germany Faculty Calvin Cohen, MD,
EACS 2009 11-14, November 2009 Cologne, Germany Course Director Jürgen K. Rockstroh, MD Co-Chairman, 12th European AIDS Conference Professor, University of Bonn Bonn, Germany Faculty Calvin Cohen, MD,
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Kimberly Adkison, 1 Lesley Kahl, 1 Elizabeth Blair, 1 Kostas Angelis, 2 Herta Crauwels, 3 Maria Nascimento, 1 Michael Aboud 1
 Pharmacokinetics of Dolutegravir and Rilpivirine After Switching to the Two-Drug Regimen From an Efavirenz- or Nevirapine- Based Antiretroviral Regimen: SWORD-1 & -2 Pooled PK Analysis Kimberly Adkison,
Pharmacokinetics of Dolutegravir and Rilpivirine After Switching to the Two-Drug Regimen From an Efavirenz- or Nevirapine- Based Antiretroviral Regimen: SWORD-1 & -2 Pooled PK Analysis Kimberly Adkison,
The Integrase Inhibitor Drug Class: A Comparative Clinical Review
 The Integrase Inhibitor Drug Class: A Comparative Clinical Review Ian Frank Professor of Medicine University of Pennsylvania Philadelphia, PA USA franki@pennmedicine.upenn.edu Disclosure Gilead, ViiV/GlaxoSmithKline:
The Integrase Inhibitor Drug Class: A Comparative Clinical Review Ian Frank Professor of Medicine University of Pennsylvania Philadelphia, PA USA franki@pennmedicine.upenn.edu Disclosure Gilead, ViiV/GlaxoSmithKline:
Long Acting ART for Treatment and PrEP
 Long Acting ART for Treatment and PrEP Anton Pozniak MD FRCP Consultant Physician Disclosures I have received honoraria, travel sponsorship and research grants from: Gilead Sciences Janssen MSD ViiV Healthcare
Long Acting ART for Treatment and PrEP Anton Pozniak MD FRCP Consultant Physician Disclosures I have received honoraria, travel sponsorship and research grants from: Gilead Sciences Janssen MSD ViiV Healthcare
IAC Analyst Presentation
 IAC Analyst Presentation David Redfern Chairman, ViiV Healthcare Chief Strategy Officer, GSK July 27, 2012 1 ViiV Healthcare Dr Dominique Limet CEO, ViiV Healthcare July 27, 2012 2 Equity split of 85%
IAC Analyst Presentation David Redfern Chairman, ViiV Healthcare Chief Strategy Officer, GSK July 27, 2012 1 ViiV Healthcare Dr Dominique Limet CEO, ViiV Healthcare July 27, 2012 2 Equity split of 85%
Dolutegravir-Rilpivirine (Juluca)
") Dolutegravir-Rilpivirine (Juluca) David H. Spach, MD Clinical Director, MW AETC Professor of Medicine Division of Infectious Diseases University of Washington Last Updated: November 30, 2017 ANTIRETROVIRAL
Dolutegravir-Rilpivirine (Juluca) David H. Spach, MD Clinical Director, MW AETC Professor of Medicine Division of Infectious Diseases University of Washington Last Updated: November 30, 2017 ANTIRETROVIRAL
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
HIV 101. Applications of Antiretroviral Therapy
 HIV 101. Applications of Antiretroviral Therapy Michael S. Saag, MD Professor of Medicine Associate Dean for Global Health Jim Straley Chair in AIDS Research University of Alabama at Birmingham Birmingham,
HIV 101. Applications of Antiretroviral Therapy Michael S. Saag, MD Professor of Medicine Associate Dean for Global Health Jim Straley Chair in AIDS Research University of Alabama at Birmingham Birmingham,
Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies. Joel Gallant, MD, MPH Johns Hopkins University School of Medicine
 Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies Joel Gallant, MD, MPH Johns Hopkins University School of Medicine Initial Regimen: DHHS Guidelines 3/27/2012 Preferred Regimens
Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies Joel Gallant, MD, MPH Johns Hopkins University School of Medicine Initial Regimen: DHHS Guidelines 3/27/2012 Preferred Regimens
v Dr Anton Pozniak Chelsea and Westminster Hospital, London Injectable ARVs a S.W.O.T Analysis
 18 th Annual Resistance and Antiviral Therapy Meeting v Dr Anton Pozniak Chelsea and Westminster Hospital, London Thursday 18 September 2014, Royal College of Physicians, London Injectable ARVs a S.W.O.T
18 th Annual Resistance and Antiviral Therapy Meeting v Dr Anton Pozniak Chelsea and Westminster Hospital, London Thursday 18 September 2014, Royal College of Physicians, London Injectable ARVs a S.W.O.T
HIV Treatment Update
 HIV Treatment Update Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM Johns Hopkins University School of Medicine University of New Mexico School of Medicine Disclosures Consulting, Advisory Boards,
HIV Treatment Update Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM Johns Hopkins University School of Medicine University of New Mexico School of Medicine Disclosures Consulting, Advisory Boards,
Treatment update. Bronagh McBrien June 2016
 Treatment update Bronagh McBrien June 2016 Speaker Name Bronagh McBrien Statement Received educational funding and support from Gilead, Merck, Boehringer Ingelheim, Janssen-Cilag Date : 27 June 2016 BHIVA
Treatment update Bronagh McBrien June 2016 Speaker Name Bronagh McBrien Statement Received educational funding and support from Gilead, Merck, Boehringer Ingelheim, Janssen-Cilag Date : 27 June 2016 BHIVA
Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary?
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
Simplifying HIV Treatment Now and in the Future
 Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
INTERGRASE INHIBITORS- WHAT S NEW?
 INTERGRASE INHIBITORS- WHAT S NEW? Professor Margaret Johnson Royal Free London Foundation Trust October 2018 Targeting the HIV life-cycle NEW HIV VIRON MATURATION CO-RECEPTOR BINDING FUSION BUDDING CD4
INTERGRASE INHIBITORS- WHAT S NEW? Professor Margaret Johnson Royal Free London Foundation Trust October 2018 Targeting the HIV life-cycle NEW HIV VIRON MATURATION CO-RECEPTOR BINDING FUSION BUDDING CD4
Perspectivesconcernantles InhibiteursNon Nucléosidiquesde la Transcriptase Inverse (INNTI)
") Perspectivesconcernantles InhibiteursNon Nucléosidiquesde la Transcriptase Inverse (INNTI) Gianni Di Perri Dept. de Maladies Infectieuses Universitè de Turin Ospedale Amedeo di Savoia Fusion inhibitors
Perspectivesconcernantles InhibiteursNon Nucléosidiquesde la Transcriptase Inverse (INNTI) Gianni Di Perri Dept. de Maladies Infectieuses Universitè de Turin Ospedale Amedeo di Savoia Fusion inhibitors
CROI 2016: Top Ten for Clinicians
 Hynes Convention Center. Boston, MA; US. Feb 22-25, 2016 CROI 2016: Top Ten for Clinicians Josep M Llibre Hospital Universitari Germans Trias i Pujol Fundació Lluita contra la SIDA Badalona, Barcelona
Hynes Convention Center. Boston, MA; US. Feb 22-25, 2016 CROI 2016: Top Ten for Clinicians Josep M Llibre Hospital Universitari Germans Trias i Pujol Fundació Lluita contra la SIDA Badalona, Barcelona
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort
 Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
Antiretroviral Treatment 2014
 Activity Code FM285 Antiretroviral Treatment 2014 Rajesh Gandhi, MD Masssachusetts General Hospital Disclosures: Educational grants to my institution from Janssen, Viiv, Abbott Learning Objectives Upon
Activity Code FM285 Antiretroviral Treatment 2014 Rajesh Gandhi, MD Masssachusetts General Hospital Disclosures: Educational grants to my institution from Janssen, Viiv, Abbott Learning Objectives Upon
Cases from the Clinic(ians): Case-Based Panel Discussion
: Case-Based Panel Discussion") Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
TAF an overview Who? When? How? co-infected/ monoinfected
 TAF an overview Who? When? How? co-infected/ monoinfected Dr Kosh Agarwal Institute of Liver Studies King s College Hospital ICVH Chicago 2017 Disclosures I am a Hepatologist Involved in the global TAF
TAF an overview Who? When? How? co-infected/ monoinfected Dr Kosh Agarwal Institute of Liver Studies King s College Hospital ICVH Chicago 2017 Disclosures I am a Hepatologist Involved in the global TAF
Disclosures. Update on HIV Drug Therapy: A Case based Discussion. Case # 1: Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv
 Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
New options for new and old patients. Antonella Castagna
 New options for new and old patients Antonella Castagna Disclosures I have received funding for Advisory Boards, Speaker Panels and for preparation of educational materials from the following: Gilead Sciences
New options for new and old patients Antonella Castagna Disclosures I have received funding for Advisory Boards, Speaker Panels and for preparation of educational materials from the following: Gilead Sciences
Didactic Series. CROI 2014 Update. March 27, 2014
 Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Future Perspectives for Delivery of Antiretroviral Drugs
 Future Perspectives for Delivery of Antiretroviral Drugs David Back University of Liverpool UK David Back University of Liverpool Disclosures Honoraria received for advisory boards and lectures from AbbVie,
Future Perspectives for Delivery of Antiretroviral Drugs David Back University of Liverpool UK David Back University of Liverpool Disclosures Honoraria received for advisory boards and lectures from AbbVie,
RESEARCH B/F/TAF in Treatment-Naïve HIV-1 and HIV-1 RNA Suppressed Switch Patients
 RESEARCH B/F/TAF in Treatment-Naïve HIV-1 and HIV-1 RNA Suppressed Switch Patients Kirsten White Gilead Sciences, Inc., Foster City, CA Background Bictegravir (BIC; B) is a novel, unboosted integrase strand
RESEARCH B/F/TAF in Treatment-Naïve HIV-1 and HIV-1 RNA Suppressed Switch Patients Kirsten White Gilead Sciences, Inc., Foster City, CA Background Bictegravir (BIC; B) is a novel, unboosted integrase strand
Actualización y Futuro en VIH
 Actualización y Futuro en VIH Dr. Santiago Moreno Servicio de Enfermedades Infecciosas Hospital U. Ramón y Cajal. Universidad de Alcalá. IRYCIS. Madrid Agenda Control of the HIV-epidemic Coinfections Antiretroviral
Actualización y Futuro en VIH Dr. Santiago Moreno Servicio de Enfermedades Infecciosas Hospital U. Ramón y Cajal. Universidad de Alcalá. IRYCIS. Madrid Agenda Control of the HIV-epidemic Coinfections Antiretroviral
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
Criteria for Oral PrEP
 Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies. Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine
 Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
Update on HIV Drug Resistance. Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School
 Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
First line ART Rilpirivine A New NNRTI. Chris Jack Physician, Durdoc Centre ethekwini
 First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
IAS 2015 Report Back. Disclosures
 IAS 215 Report Back Carina Marquez, MD, MPH Assistant Professor Division of HIV, Infectious Diseases, and Global Medicine San Francisco General Hospital University of California, San Francisco Disclosures
IAS 215 Report Back Carina Marquez, MD, MPH Assistant Professor Division of HIV, Infectious Diseases, and Global Medicine San Francisco General Hospital University of California, San Francisco Disclosures
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
Antiretroviral Therapy in Joel Gallant, MD, MPH Johns Hopkins University School of Medicine
 Antiretroviral Therapy in 2013 Joel Gallant, MD, MPH Johns Hopkins University School of Medicine When to Start When to Start: DHHS Guidelines, February 2013 ART recommended for all HIV+ individuals to
Antiretroviral Therapy in 2013 Joel Gallant, MD, MPH Johns Hopkins University School of Medicine When to Start When to Start: DHHS Guidelines, February 2013 ART recommended for all HIV+ individuals to
Bon Usage des Antirétroviraux dans l Infection par le VIH
 Bon Usage des Antirétroviraux dans l Infection par le VIH Pr. Jean-Michel Molina CHU St Louis, Assistance Publique Hôpitaux de Paris, INSERM U941 et Université Paris 7 Diderot, France 1 Liens d Intérêt
Bon Usage des Antirétroviraux dans l Infection par le VIH Pr. Jean-Michel Molina CHU St Louis, Assistance Publique Hôpitaux de Paris, INSERM U941 et Université Paris 7 Diderot, France 1 Liens d Intérêt
Reduced Drug Regimens
 Dr. Jose R Arribas @jrarribas Financial disclosures JOSE R ARRIBAS Research Support: Speaker s Bureau: Viiv, Janssen, Abbvie, BMS, Gilead, MSD Board Member/Advisory Panel: Merck, Gilead Stock/Shareholder:
Dr. Jose R Arribas @jrarribas Financial disclosures JOSE R ARRIBAS Research Support: Speaker s Bureau: Viiv, Janssen, Abbvie, BMS, Gilead, MSD Board Member/Advisory Panel: Merck, Gilead Stock/Shareholder:
The impact of antiretroviral drugs on renal function
 The impact of antiretroviral drugs on renal function Professor Bruce Hendry Renal Medicine King s College London King s College Hospital NHS Foundation Trust 1 DISCLOSURES: BRUCE HENDRY I have received
The impact of antiretroviral drugs on renal function Professor Bruce Hendry Renal Medicine King s College London King s College Hospital NHS Foundation Trust 1 DISCLOSURES: BRUCE HENDRY I have received
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
 Antiretroviral Medications: What you need to know Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Associate Professor, Department of Pharmacy Practice Jefferson College of Pharmacy, Thomas Jefferson University
Antiretroviral Medications: What you need to know Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Associate Professor, Department of Pharmacy Practice Jefferson College of Pharmacy, Thomas Jefferson University