Cerebral Toxoplasmosis in HIV-Infected Patients. Ahmed Saad,MD,FACP
|
|
|
- Erik Lang
- 6 years ago
- Views:
Transcription


1 Cerebral Toxoplasmosis in HIV-Infected Patients Ahmed Saad,MD,FACP
2
3 Introduction Toxoplasmosis: Caused by the intracellular protozoan, Toxoplasma gondii. Immunocompetent persons with primary infection are usually asymptomatic. Latent infection can persist for life. In immunosuppressed patients, especially with AIDS, the parasite can reactivate and cause disease.
4 Epidemiology Seroprevalence rates of toxoplasmosis vary significantly among countries. The rate is approximately 15% in the US. It is over 50% in some European countries.
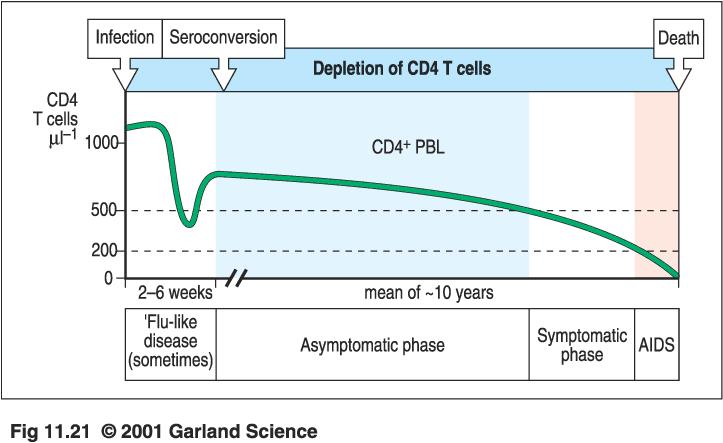
5 Epidemiology AIDS patients: In those with CD4 <100, who are seropositive, there is a 30% probability of developing reactivated toxoplasmosis if effective prophylaxis is not taken. The introduction of anti-toxoplasma prophylaxis and HAART has decreased the occurrence.
6 Clinical Presentation When T. gondii reactivates in an AIDS patient, it usually does so in the CNS, leading to cerebral abscesses. The most common presenting symptom is headache. Other common symptoms include: Confusion Fever Focal neurologic deficits Seizures
7 Diagnosis The majority of patients are seropositive for anti-toxoplasma IgG antibodies. Anti-toxoplasma IgM antibodies are usually absent. The absence of antibodies makes the diagnosis less likely, but does not exclude the possibility.
8 Diagnosis Most patients with AIDS will have multiple, ring-enhancing brain lesions often associated with edema. There is a predilection for involvement of the basal ganglia and periventricular white matter of the brain. MRI is more sensitive than CT for identifying lesions.

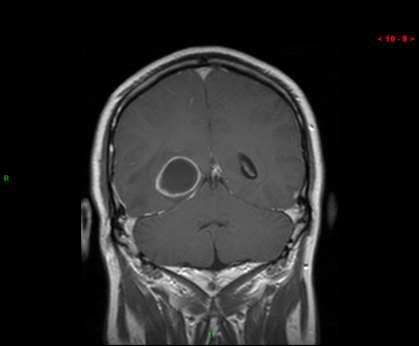
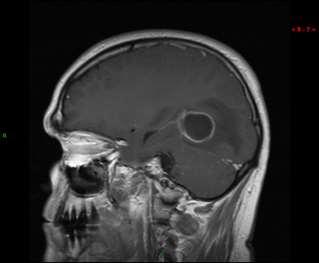
9 Findings: ring enhancement T1 post contrast
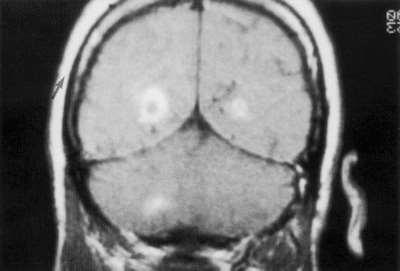
10 Cerebral toxoplasmosis

11 Diagnosis The differential diagnosis includes: CNS lymphoma Aspergillosis Tuberculosis Histoplasmosis syphilitic gummas
12 Diagnosis Toxoplasmosis and CNS lymphoma are the two most common entities. Toxoplasmosis accounts for 50% of cases. CNS lymphoma accounts for 30% of cases.
13 Diagnosis If these criteria are met, there is a 90% probability of the diagnosis. D4 count <100 Seropositive for T. gondii IgG. Not receiving prophylaxis for PCP & toxo Multiple ring-enhancing lesions.
14 Diagnosis Therefore, it is common to treat empirically. If only one brain lesion is detected on imaging, CNS lymphoma rises on the differential diagnosis list, despite positive toxoplasma serology.
15 Diagnosis When to perform brain biopsy or another diagnostic test: If all four criteria are not met. If there is no clinical or radiographic response to empiric therapy.
16 Diagnosis In patients with focal brain lesions already receiving prophylaxis or who are seronegative to T. gondii, PCR testing for other pathogens to be considered, including: EBV JC virus Mycobacterium tuberculosis Cryptococcus neoformans
17 Diagnosis Lumbar puncture may be performed to analyze CSF, which: May have mild mononuclear pelocytosis and elevated protein. With DNA amplification, can detect T. gondii in most patients. When cytocentrifuged and stained with Giemsa, can sometimes show tachyzoites.

18 ASPERGILLOMA T2 and DWI of a patient with aspergillosis. There are bilateral foci of patchy increased T2 signal consistent with edema.
 uptake in primary brain")
19 Primary CNS Lymphoma positron emission tomography very intense FDG(18 Fluoro-deoxyglucose) uptake in primary brain lymphoma
20 PML(progressive multifocal leucoencephaopathy ) Reactivation of JC virus (Papova virus) CD4 counts typically <100 Subacute evolution of focal disease Subcortical white matter disease commonly temporal lobe. Diagnosis: PCR on CSF for JCV (90%)
21
22 Approach to a Patient Sn's +/or Sx's of CNS Disease CD4 >200 CD4 <200 Evaluate for Non-HIV Related Diagnosis Image Brain India Ink Cryptococcal Ag Cytology TB culture Routine Culture Image Negative LP Image Positive Treat for Toxoplasmosis
23 Approach to a Patient (Cont) Treat for Toxo Responds No Response Continue RX Brain Biopsy
24 Treatment First-line therapy: Pyrimethamine 200 mg po loading dose followed by 75 mg/day plus SMX-TMP (10mg/kg) DS BID For sulfa allergic patients, pyrimethamine 200 mg po loading dose followed by 75 mg/day plus clindamycin 600 to 1200IV TID. Clindamycin plus SMX-TMP All pyrimethamine regimens should include folinic acid to prevent drug-induced hematologic toxicity (10 to 25 mg/day po).
25 Treatment Alternative regimens: Used in patients unable to tolerate other medications: Pyrimethamine plus azithromycin (1200 to 1500 mg po qd) Pyrimethamine plus atovaquone (750 mg po qid) Sulfadiazine (1500 mg po qid) plus atovaquone (1500 mg po bid)
26 Secondary Prophylaxis Also known as chronic suppressive therapy: Following six weeks of therapy for treatment of cerebral toxoplasmosis, patients can receive lower doses of medication. First choice for treatment: Sulfadiazine 2-4 gm/day divided qid plus pyrimethamine mg/day. Folinic acid mg/day is given concurrently.
27 Treatment Anticonvulsants: Should be given to patients with a history of seizures. Should not be given routinely for seizure prophylaxis to all patients with cerebral toxoplasmosis.
28 Duration of Therapy For patients who respond, the duration of therapy is typically six weeks at the recommended doses. After treatment is complete, the dose of medication can be decreased for secondary prophylaxis.
29 Steroids Adjunctive corticosteroids should be used for patients with: Radiographic evidence of midline shift. Signs of critically elevated intracranial pressure. Clinical deterioration within the first 48 hours of therapy. Dexamethasone: Used most commonly Dosed at 8mg TID Tapered over several days
30 Monitoring of Therapy Careful clinical evaluations No value to serial assessment of IgG toxoplasma antibody titers Radiographic reassessment should be deferred for 2-3 weeks unless there has been clinical worsening or lack of improvement.
31 Primary Prophylaxis Indicated for patients with HIV and CD4 counts <100 who are T. gondii IgG positive. TMP/SMX 1 DS 3/w Patients with negative toxoplasma serology should be counseled to: Avoid eating undercooked meat. Not to avoid household cats entirely.
32 Primary Prophylaxis If the CD4 count rises above 200 for three months, primary prophylaxis can be safely discontinued. If the CD4 drops below 200, prophylaxis should be reinitiated.
33 Hypocalcemia and AIDS Vitamin D deficiency has been found to be a relatively common cause of hypocalcemia in HIV-positive adults. Increased incidence of osteopenia and osteoporosis in an HIV-infected pediatric population Association of HIV with calcium homeostasis, resulting in decreased bone density in children
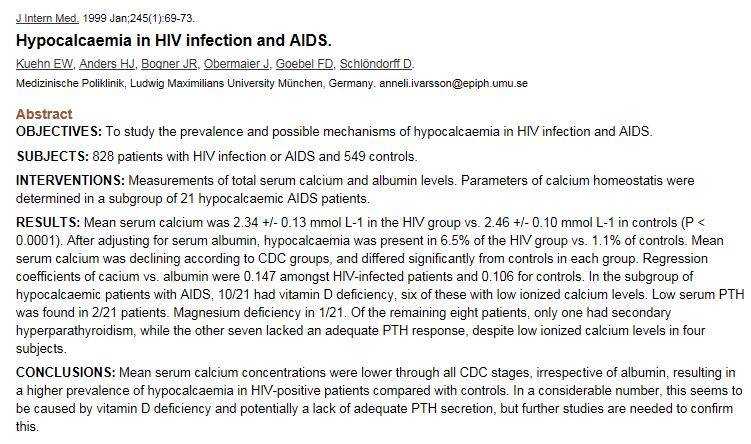
34 Hypocalcemia In HIV
35 Low PTH In HIV Various mechanisms including Impaired secretion PTH resistance. Infiltration and destruction of the parathyroid in Pneumocystis or CMV Chronic viral infection Altered immune function Abnormal cytokine production
36 Summary Diagnosis of cerebral toxoplasmosis is usually made in AIDS patient with a CD4 count <100 T. gondii IgG antibodies No prophylaxis against pcp & toxo Multiple ring-enhancing lesions on brain imaging.

37
GUIDELINE FOR THE MANAGEMENT OF TOXOPLASMOSIS ENCEPHALITIS
 GUIDELINE FOR THE MANAGEMENT OF TOXOPLASMOSIS ENCEPHALITIS Full title of guideline Guideline for the management of toxoplasmosis encephalitis Author Dr P Venkatesan (ID consultant) Division and specialty
GUIDELINE FOR THE MANAGEMENT OF TOXOPLASMOSIS ENCEPHALITIS Full title of guideline Guideline for the management of toxoplasmosis encephalitis Author Dr P Venkatesan (ID consultant) Division and specialty
Toxoplasma gondii. Jarmila Kliescikova, MD 1. LF UK
 Toxoplasma gondii Jarmila Kliescikova, MD 1. LF UK Toxoplasma gondii Apicomplexa, Koccidia Obligate intracellular parasite Distribution: cosmopolite Transmission: alimentary transplacentary (transfusions,
Toxoplasma gondii Jarmila Kliescikova, MD 1. LF UK Toxoplasma gondii Apicomplexa, Koccidia Obligate intracellular parasite Distribution: cosmopolite Transmission: alimentary transplacentary (transfusions,
Opportunistic infections in the era of cart, still a problem in resource-limited settings
 Opportunistic infections in the era of cart, still a problem in resource-limited settings Cristiana Oprea Victor Babes Clinical Hospital for Infectious and Tropical Diseases, Bucharest, Romania Assessment
Opportunistic infections in the era of cart, still a problem in resource-limited settings Cristiana Oprea Victor Babes Clinical Hospital for Infectious and Tropical Diseases, Bucharest, Romania Assessment
May He Rest in Peace
 May He Rest in Peace Neurologic Complications of AIDS Medical Knowledge Fiesta 2012 Paul K. King MD pkingmd@yahoo.com Objectives definition of HIV/AIDS what are the neurologic complications of AIDS how
May He Rest in Peace Neurologic Complications of AIDS Medical Knowledge Fiesta 2012 Paul K. King MD pkingmd@yahoo.com Objectives definition of HIV/AIDS what are the neurologic complications of AIDS how
A challenging neurological complication in a young HIV-infected woman
 A challenging neurological complication in a young HIV-infected woman Ianache Irina-Cristiana Vi tor Ba es Clini al Hospital for Infectious and Tropical Diseases Bucharest - HIV/AIDS department Assessment
A challenging neurological complication in a young HIV-infected woman Ianache Irina-Cristiana Vi tor Ba es Clini al Hospital for Infectious and Tropical Diseases Bucharest - HIV/AIDS department Assessment
Neuroradiology of AIDS
 Neuroradiology of AIDS Frank Minja,, HMS IV Gillian Lieberman MD September 2002 AIDS 90% of HIV patients have CNS involvement 1 10% of AIDS patients present first with neurological symptoms 2 73-80% of
Neuroradiology of AIDS Frank Minja,, HMS IV Gillian Lieberman MD September 2002 AIDS 90% of HIV patients have CNS involvement 1 10% of AIDS patients present first with neurological symptoms 2 73-80% of
Opportunistic infections
 Opportunistic infections Opportunistic infections Decrease in number of CD4 lymphocytes is condition for development of opportunistic infections Risk is started, when number of CD4 lymphocytes drops to
Opportunistic infections Opportunistic infections Decrease in number of CD4 lymphocytes is condition for development of opportunistic infections Risk is started, when number of CD4 lymphocytes drops to
Toxoplasma gondii. Definitive Host adult forms sexual reproduction. Intermediate Host immature forms asexual reproduction
 Toxoplasma gondii cosmopolitan distribution seropositive prevalence rates vary generally 20-75% generally causes very benign disease in immunocompetent adults tissue cyst forming coccidia predator-prey
Toxoplasma gondii cosmopolitan distribution seropositive prevalence rates vary generally 20-75% generally causes very benign disease in immunocompetent adults tissue cyst forming coccidia predator-prey
AIDS at 25. Epidemiology and Clinical Management MID 37
 AIDS at 25 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Regional HIV and
AIDS at 25 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Regional HIV and
Lecture-7- Hazem Al-Khafaji 2016
 TOXOPLASMOSIS Lecture-7- Hazem Al-Khafaji 2016 TOXOPLASMOSIS It is a disease caused by Toxoplasma gondii which is a protozoan parasite that is infects a variety of mammals and birds throughout the world.
TOXOPLASMOSIS Lecture-7- Hazem Al-Khafaji 2016 TOXOPLASMOSIS It is a disease caused by Toxoplasma gondii which is a protozoan parasite that is infects a variety of mammals and birds throughout the world.
AIDS at 30 Epidemiology and Clinical Epidemiology and Management MID 37
 AIDS at 30 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Adults and children
AIDS at 30 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Adults and children
FOCAL NEUROLOGICAL DEFICIT in HIV PATIENTS -a case based approach. Dr Jency Maria Koshy, CMC, Ludhiana
 FOCAL NEUROLOGICAL DEFICIT in HIV PATIENTS -a case based approach Dr Jency Maria Koshy, CMC, Ludhiana Case 1 Middle aged gentleman Diagnosed to have HIV 5 months prior to admission CD4 at the time of detection-132
FOCAL NEUROLOGICAL DEFICIT in HIV PATIENTS -a case based approach Dr Jency Maria Koshy, CMC, Ludhiana Case 1 Middle aged gentleman Diagnosed to have HIV 5 months prior to admission CD4 at the time of detection-132
The Neurology of HIV Infection. Carolyn Barley Britton, MD, MS Associate Professor of Clinical Neurology Columbia University
 The Neurology of HIV Infection Carolyn Barley Britton, MD, MS Associate Professor of Clinical Neurology Columbia University HIV/AIDS Epidemiology World-wide pandemic, 40 million affected U.S.- Disproportionate
The Neurology of HIV Infection Carolyn Barley Britton, MD, MS Associate Professor of Clinical Neurology Columbia University HIV/AIDS Epidemiology World-wide pandemic, 40 million affected U.S.- Disproportionate
Clinical Policy: Pyrimethamine (Daraprim) Reference Number: ERX.NPA.44 Effective Date:
 Reference Number: ERX.NPA.44 Effective Date:") Clinical Policy: (Daraprim) Reference Number: ERX.NPA.44 Effective Date: 12.01.15 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Daraprim) Reference Number: ERX.NPA.44 Effective Date: 12.01.15 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Recurring and Emerging Questions Related to Management of HIV-Related Opportunistic Infections. Objectives. Henry Masur MD
 Recurring and Emerging Questions Related to Management of HIV-Related Opportunistic Infections Henry Masur MD Clinical Professor of Medicine George Washington University School of Medicine Objectives To
Recurring and Emerging Questions Related to Management of HIV-Related Opportunistic Infections Henry Masur MD Clinical Professor of Medicine George Washington University School of Medicine Objectives To
Natural History of Untreated HIV-1 Infection
 Opportunistic infections Dr. Guido van den Berk December 2009 HIV [e] EDUCATION Natural History of Untreated HIV-1 Infection 1000 + CD4 Cells 800 600 400 Constitutional Symptoms Early Opportunistic Infections
Opportunistic infections Dr. Guido van den Berk December 2009 HIV [e] EDUCATION Natural History of Untreated HIV-1 Infection 1000 + CD4 Cells 800 600 400 Constitutional Symptoms Early Opportunistic Infections
Overview on Opportunistic Infections of the Central Nervous System
 Second HIV Infection and the Central Nervous System: Developed and Resource-Limited Settings Venice, Italy April 14 16, 2007 Overview on Opportunistic Infections of the Central Nervous System Adriana Ammassari
Second HIV Infection and the Central Nervous System: Developed and Resource-Limited Settings Venice, Italy April 14 16, 2007 Overview on Opportunistic Infections of the Central Nervous System Adriana Ammassari
CNS Infections. Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London. Hammersmith Acute Medicine 2011
 CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
OI prophylaxis When to start, when to stop. Eva Raphael, MD MPH Family and community medicine, pgy-2 University of California, San Francisco
 OI prophylaxis When to start, when to stop Eva Raphael, MD MPH Family and community medicine, pgy-2 University of California, San Francisco Learning Objectives o Recognize when to start OI prophylaxis
OI prophylaxis When to start, when to stop Eva Raphael, MD MPH Family and community medicine, pgy-2 University of California, San Francisco Learning Objectives o Recognize when to start OI prophylaxis
Meningi&s in HIV NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Meningi&s in HIV Christina M. Marra, MD Neurology and Medicine University of Washington School of Medicine Susceptibility to CNS Opportunistic Infections CD4+
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Meningi&s in HIV Christina M. Marra, MD Neurology and Medicine University of Washington School of Medicine Susceptibility to CNS Opportunistic Infections CD4+
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Daraprim) Reference Number: CP.PMN.44 Effective Date: 11.01.15 Last Review Date: 08.18 Line of Business: Commercial, HIM, Medicaid Revision Log See Important Reminder at the end of this
Clinical Policy: (Daraprim) Reference Number: CP.PMN.44 Effective Date: 11.01.15 Last Review Date: 08.18 Line of Business: Commercial, HIM, Medicaid Revision Log See Important Reminder at the end of this
Disclosure. Learner Objectives. Congenital Infections. Question. Main Categories 4/26/2016
 Communicating Communicability: Imaging of CNS Infections Aaron P. Kamer, MD Assistant Professor of Clinical Radiology Neuroradiology Section April 26, 2016 Disclosure Within the past 12 months: I have
Communicating Communicability: Imaging of CNS Infections Aaron P. Kamer, MD Assistant Professor of Clinical Radiology Neuroradiology Section April 26, 2016 Disclosure Within the past 12 months: I have
Coccidia. Eucoccidioside
 Coccidia Kingdom Sub-Kingdom Phylum Class Order Family Genus Species Protista Protozoa Apicomplexa Sporozoasida Eucoccidioside Sarcocystidae Toxoplasma gondii 1 Toxoplasma gondii (life cycle) Sexual cycle
Coccidia Kingdom Sub-Kingdom Phylum Class Order Family Genus Species Protista Protozoa Apicomplexa Sporozoasida Eucoccidioside Sarcocystidae Toxoplasma gondii 1 Toxoplasma gondii (life cycle) Sexual cycle
Challenging Case Presentation. Clinical History
 Challenging Case Presentation Clinical History By Yahia Ismail,MD,MRCP(UK) Medical Oncology Dept.,NCI 01/04/13 History of Present Illness(HPI) A 21-y-old single female was referred to NCI 7 months ago
Challenging Case Presentation Clinical History By Yahia Ismail,MD,MRCP(UK) Medical Oncology Dept.,NCI 01/04/13 History of Present Illness(HPI) A 21-y-old single female was referred to NCI 7 months ago
Retina Grand Rounds. Stephen Huddleston MD Charles Retina Institute University of Tennessee Hamilton Eye Institute
 Retina Grand Rounds Stephen Huddleston MD Charles Retina Institute University of Tennessee Hamilton Eye Institute Fundus Autoflourescence 2013 2016 Plaquenil Toxicity Excellent treatment for a variety
Retina Grand Rounds Stephen Huddleston MD Charles Retina Institute University of Tennessee Hamilton Eye Institute Fundus Autoflourescence 2013 2016 Plaquenil Toxicity Excellent treatment for a variety
The diffusion-weighted imaging (DWI) MR sequence showed an hyposignal of the lesion eliminating a cerebral pyogenic abscess which usually presents an
 MR sequence showed an hyposignal of the lesion eliminating a cerebral pyogenic abscess which usually presents an") Cerebral toxoplasmosis is one of the most common opportunistic neurological infections in AIDS patients, and is typically observed in the later stages of human immunodeficiency virus (HIV) infection. 1,2
Cerebral toxoplasmosis is one of the most common opportunistic neurological infections in AIDS patients, and is typically observed in the later stages of human immunodeficiency virus (HIV) infection. 1,2
HIV and CNS Stereotactic Biopsy in the diagnosis of brain lesions in AIDS patients
 HIV and CNS Stereotactic Biopsy in the diagnosis of brain lesions in AIDS patients Department of Neurosurgery Infectious Diseases Hospital, University of Buenos Aires, Argentina Definition AIDS Patients
HIV and CNS Stereotactic Biopsy in the diagnosis of brain lesions in AIDS patients Department of Neurosurgery Infectious Diseases Hospital, University of Buenos Aires, Argentina Definition AIDS Patients
British HIV Association guidelines for the treatment of opportunistic infection in HIV-positive individuals 2010
 British HIV Association guidelines for the treatment of opportunistic infection in HIV-positive individuals 2010 M Nelson, D Dockrell, S Edwards on behalf of the BHIVA Guidelines Subcommittee* British
British HIV Association guidelines for the treatment of opportunistic infection in HIV-positive individuals 2010 M Nelson, D Dockrell, S Edwards on behalf of the BHIVA Guidelines Subcommittee* British
Prevention and Treatment of Selected Opportunistic Infections: A Guidelines Update
 Prevention and Treatment of Selected Opportunistic Infections: A Guidelines Update Constance A. Benson, MD Professor of Medicine Division of Infectious Diseases University of California, San Diego Disclosures
Prevention and Treatment of Selected Opportunistic Infections: A Guidelines Update Constance A. Benson, MD Professor of Medicine Division of Infectious Diseases University of California, San Diego Disclosures
Toxoplasmosis FACT SHEET. What is toxoplasmosis? Symptoms CONTACT US. Published 2016
 Toxoplasmosis What is toxoplasmosis? Toxoplasmosis is an infection caused by the parasite Toxoplasma gondii (T. gondii). The parasite is transmitted to people through eating undercooked meat, especially
Toxoplasmosis What is toxoplasmosis? Toxoplasmosis is an infection caused by the parasite Toxoplasma gondii (T. gondii). The parasite is transmitted to people through eating undercooked meat, especially
Challenges in Management of Cryptococcal Meningitis. Yunus Moosa Department of ID NRMSM Durban
 Challenges in Management of Cryptococcal Meningitis Yunus Moosa Department of ID NRMSM Durban Overview Epidemiology Pathogenesis Clinical presentation Diagnosis Prognostic factors Antifungal Treatment
Challenges in Management of Cryptococcal Meningitis Yunus Moosa Department of ID NRMSM Durban Overview Epidemiology Pathogenesis Clinical presentation Diagnosis Prognostic factors Antifungal Treatment
A Child with Cross Eye. Nia Kurniati
 A Child with Cross Eye Nia Kurniati Background When dealing with new case with potential social problem, complication related to ARV treatment may pose difficulties Restricted resource to address potential
A Child with Cross Eye Nia Kurniati Background When dealing with new case with potential social problem, complication related to ARV treatment may pose difficulties Restricted resource to address potential
Management of Immune Reconstitution Inflammatory Syndrome (IRIS)
") Management of Immune Reconstitution Inflammatory Syndrome (IRIS) Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the IRIS Guideline
Management of Immune Reconstitution Inflammatory Syndrome (IRIS) Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the IRIS Guideline
Helpful Information for evaluation of new neurological symptoms in patients receiving TYSABRI
 Helpful Information for evaluation of new neurological symptoms in patients receiving TYSABRI This information is provided as an educational resource for healthcare providers and should be considered current
Helpful Information for evaluation of new neurological symptoms in patients receiving TYSABRI This information is provided as an educational resource for healthcare providers and should be considered current
Deborah J. Nicolls. 2 ND YEAR RESEARCH ELECTIVE RESIDENT S JOURNAL Volume VI, A. Study Purpose and Rationale
 Combined Diagnostic Approach to AIDS-Related Primary CNS Lymphoma Using EBV-DNA Polymerase Chain Reaction in CSF, Thallium-201 Single-Photon Emission Computed Tomography, and Toxoplasma gondii Serologies.
Combined Diagnostic Approach to AIDS-Related Primary CNS Lymphoma Using EBV-DNA Polymerase Chain Reaction in CSF, Thallium-201 Single-Photon Emission Computed Tomography, and Toxoplasma gondii Serologies.
Cryptococcal Meningitis
 Cryptococcal Meningitis Dr N Thumbiran Infectious Diseases Department UKZN Index patient 27 year old female Presented to King Edward Hospital on 17/07/2005 with: Severe headaches Vomiting Photophobia X
Cryptococcal Meningitis Dr N Thumbiran Infectious Diseases Department UKZN Index patient 27 year old female Presented to King Edward Hospital on 17/07/2005 with: Severe headaches Vomiting Photophobia X
Toxoplasmosis in immunocompetent and immunocompromised population of Constanta, Romania
 3rd International Conference on Clinical Microbiology & Microbial Genomics September 24-26, 2014 Valencia, Spain Toxoplasmosis in immunocompetent and immunocompromised population of Constanta, Romania
3rd International Conference on Clinical Microbiology & Microbial Genomics September 24-26, 2014 Valencia, Spain Toxoplasmosis in immunocompetent and immunocompromised population of Constanta, Romania
IMAGING OF INTRACRANIAL INFECTIONS
 IMAGING OF INTRACRANIAL INFECTIONS Dr Carolina Kachramanoglou LYSHOLM DEPARTMENT OF NEURORADIOLOGY NATIONAL HOSPITAL FOR NEUROLOGY AND NEUROSURGERY Plan Introduce MR sequences that are useful in the diagnosis
IMAGING OF INTRACRANIAL INFECTIONS Dr Carolina Kachramanoglou LYSHOLM DEPARTMENT OF NEURORADIOLOGY NATIONAL HOSPITAL FOR NEUROLOGY AND NEUROSURGERY Plan Introduce MR sequences that are useful in the diagnosis
Didactic Series. Fungal Infections: small bother to big mortality
 Didactic Series Fungal Infections: small bother to big mortality Christian B. Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic 8/8/13 ACCREDITATION STATEMENT: University of California,
Didactic Series Fungal Infections: small bother to big mortality Christian B. Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic 8/8/13 ACCREDITATION STATEMENT: University of California,
Dilemmas in the Management of Meningitis & Encephalitis HEADACHE AND FEVER. What is the best initial approach for fever, headache, meningisums?
 Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Dr Keerti Gedela. Chelsea and Westminster Hospital NHS Foundation Trust, London. 19 th Annual Conference of the British HIV Association (BHIVA)
") 19 th Annual Conference of the British HIV Association (BHIVA) Dr Keerti Gedela Chelsea and Westminster Hospital NHS Foundation Trust, London 16-19 April 2013, Manchester Central Convention Complex Value
19 th Annual Conference of the British HIV Association (BHIVA) Dr Keerti Gedela Chelsea and Westminster Hospital NHS Foundation Trust, London 16-19 April 2013, Manchester Central Convention Complex Value
Cerebrospinal Fluid in CNS Infections
 Cerebrospinal Fluid in CNS Infections Osvaldo M. Takayanagui Departamento de Neurologia Faculdade de Medicina de Ribeirão Preto Universidade de São Paulo Diagnosis of CNS Infections 1891- Heinrich Quincke
Cerebrospinal Fluid in CNS Infections Osvaldo M. Takayanagui Departamento de Neurologia Faculdade de Medicina de Ribeirão Preto Universidade de São Paulo Diagnosis of CNS Infections 1891- Heinrich Quincke
Central Nervous System Immune Reconstitution Disease: Pathology
 Central Nervous System Immune Reconstitution Disease: Pathology F.Gray, H.Adle-Biassette, F.Héran, G. Pialoux, A.Moulignier, APHP Hôpital Lariboisière Université Paris VII Introduction of HAART, which
Central Nervous System Immune Reconstitution Disease: Pathology F.Gray, H.Adle-Biassette, F.Héran, G. Pialoux, A.Moulignier, APHP Hôpital Lariboisière Université Paris VII Introduction of HAART, which
Fungal Meningitis. Stefan Zimmerli Institute for infectious diseases University of Bern Friedbühlstrasse Bern
 Fungal Meningitis Stefan Zimmerli Institute for infectious diseases University of Bern Friedbühlstrasse 51 3010 Bern Death due to infectious diseases in sub-saharan Africa Park BJ. Et al AIDS 2009;23:525
Fungal Meningitis Stefan Zimmerli Institute for infectious diseases University of Bern Friedbühlstrasse 51 3010 Bern Death due to infectious diseases in sub-saharan Africa Park BJ. Et al AIDS 2009;23:525
Opportunistic Infections BHIVA Guidelines
 Opportunistic Infections BHIVA Guidelines Mark Nelson David Dockrell Simon Edwards I have.. 1. Read all of the BHIVA guidelines 12% 2. Read some of the BHIVA guidelines in their entirety 3. Browsed some
Opportunistic Infections BHIVA Guidelines Mark Nelson David Dockrell Simon Edwards I have.. 1. Read all of the BHIVA guidelines 12% 2. Read some of the BHIVA guidelines in their entirety 3. Browsed some
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS
 ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
ECMM Excellence Centers Quality Audit
 ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
Only one take home point for the talk 9/26/2018. Infectious Diseases and Donor Derived Infections. Don t forget about donor-derived infections
 Shane Colombo 1993 2018 Infectious Diseases and Donor Derived Infections Peter Chin-Hong, MD Division of Infectious Diseases UCSF Only one take home point for the talk Don t forget about donor-derived
Shane Colombo 1993 2018 Infectious Diseases and Donor Derived Infections Peter Chin-Hong, MD Division of Infectious Diseases UCSF Only one take home point for the talk Don t forget about donor-derived
CNS Infections in the Pediatric Age Group
 CNS Infections in the Pediatric Age Group Introduction CNS infections are frequently life-threatening In the Philippines, bacterial meningitis is one of the top leading causes of mortality in children
CNS Infections in the Pediatric Age Group Introduction CNS infections are frequently life-threatening In the Philippines, bacterial meningitis is one of the top leading causes of mortality in children
Dr Paul Holmes Guy s and St Thomas NHS Foundation Trust, London
 Dr Paul Holmes Guy s and St Thomas NHS Foundation Trust, London HIV and Lumbar punctures in 2018 Paul Holmes Consultant Neurologist Guy s and St Thomas Hospitals I have no competing interests Summary of
Dr Paul Holmes Guy s and St Thomas NHS Foundation Trust, London HIV and Lumbar punctures in 2018 Paul Holmes Consultant Neurologist Guy s and St Thomas Hospitals I have no competing interests Summary of
MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN
 MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN OVERVIEW 1980s: dramatically improved by aciclovir HSV encephalitis in adults Delays treatment(> 48h after hospital admission): associated with a
MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN OVERVIEW 1980s: dramatically improved by aciclovir HSV encephalitis in adults Delays treatment(> 48h after hospital admission): associated with a
MR neuroimaging of HIV infected patients : A pictorial review
 MR neuroimaging of HIV infected patients : A pictorial review Poster No.: R-0198 Congress: 2014 CSM Type: Scientific Exhibit Authors: P. F. Kwan, R. Thomas, A. Dixon; SOUTH YARRA/AU Keywords: Neuroradiology
MR neuroimaging of HIV infected patients : A pictorial review Poster No.: R-0198 Congress: 2014 CSM Type: Scientific Exhibit Authors: P. F. Kwan, R. Thomas, A. Dixon; SOUTH YARRA/AU Keywords: Neuroradiology
A 39 years old HIV-positive black African woman with previously treated cerebral
 1 Abstract A 39 years old HIV-positive black African woman with previously treated cerebral toxoplasmosis experienced a foetal intra-uterine death due to congenital toxoplasmosis. This case demonstrates
1 Abstract A 39 years old HIV-positive black African woman with previously treated cerebral toxoplasmosis experienced a foetal intra-uterine death due to congenital toxoplasmosis. This case demonstrates
Infections in immunocompromised host
 Infections in immunocompromised host Immunodeficiencies Primary immunodeficiencies Neutrophil defect Humoral: B cell defect Humoral: Complement Cellular: T cells Combined severe immunodeficiency Secondary
Infections in immunocompromised host Immunodeficiencies Primary immunodeficiencies Neutrophil defect Humoral: B cell defect Humoral: Complement Cellular: T cells Combined severe immunodeficiency Secondary
Human Herpes Virus-6 Limbic Encephalitis
 Case Studies [1] March 19, 2013 Case history: A 32-year-old Caucasian female with newly diagnosed acute myeloid leukemia (AML) was treated with induction chemotherapy and attained complete remission. She
Case Studies [1] March 19, 2013 Case history: A 32-year-old Caucasian female with newly diagnosed acute myeloid leukemia (AML) was treated with induction chemotherapy and attained complete remission. She
5/15/2017. What Does HIV/AIDS Look Like in DC in Potpourri of Challenges With Opportunistic Infections
 Potpourri of Challenges With Opportunistic Infections Henry Masur, MD Clinical Professor of Medicine George Washington University Washington, DC FORMATTED: 4/28/217 Learning Objectives After attending
Potpourri of Challenges With Opportunistic Infections Henry Masur, MD Clinical Professor of Medicine George Washington University Washington, DC FORMATTED: 4/28/217 Learning Objectives After attending
Medical monitoring: tests available at central hospitals
 medial monitoring: tests available at central hospitals: 1 medical monitoring: tests available at central hospitals Medical monitoring: tests available at central hospitals medial monitoring: tests available
medial monitoring: tests available at central hospitals: 1 medical monitoring: tests available at central hospitals Medical monitoring: tests available at central hospitals medial monitoring: tests available
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Toxoplasmosis Objective :
 Toxoplasmosis Objective : Describe the Life cycle Mention the Infective stages Define Congenital Toxoplasmosis List the Lab.Diagnosis Illustrate the Immunity to Toxoplasmosis Show the relationship between
Toxoplasmosis Objective : Describe the Life cycle Mention the Infective stages Define Congenital Toxoplasmosis List the Lab.Diagnosis Illustrate the Immunity to Toxoplasmosis Show the relationship between
Reasons why we will never forget. Andrea Antinori INMI L. Spallanzani IRCCS, Roma
 Reasons why we will never forget Andrea Antinori INMI L. Spallanzani IRCCS, Roma SMRs according to time spent with CD4 count >500/mm3 after cart initiation in MSM 80,642 HIV-infected individuals eligible
Reasons why we will never forget Andrea Antinori INMI L. Spallanzani IRCCS, Roma SMRs according to time spent with CD4 count >500/mm3 after cart initiation in MSM 80,642 HIV-infected individuals eligible
20 Years of Tears and Triumphs
 20 Years of Tears and Triumphs A Clinical Research Nurse s Perspective on HIV/AIDS Bobi Keenan, RN, ACRN Clinical Research Nurse UC Irvine Dept. of Medicine/Infectious Diseases Objectives 1. Understand
20 Years of Tears and Triumphs A Clinical Research Nurse s Perspective on HIV/AIDS Bobi Keenan, RN, ACRN Clinical Research Nurse UC Irvine Dept. of Medicine/Infectious Diseases Objectives 1. Understand
Management of Cryptococcal Meningitis in HIV-infected children in National Pediatric Hospital
 Management of Cryptococcal Meningitis in HIV-infected children in National Pediatric Hospital Olivier Marcy 1,2, Sam Sophan 2, Ung Vibol 2, Chan Bunthy 2, Pok Moroun 2, Chy Kam Hoy 2, Ban Thy 2, Chhour
Management of Cryptococcal Meningitis in HIV-infected children in National Pediatric Hospital Olivier Marcy 1,2, Sam Sophan 2, Ung Vibol 2, Chan Bunthy 2, Pok Moroun 2, Chy Kam Hoy 2, Ban Thy 2, Chhour
KAP conference 19 th March 2008: Dr Mohamed Hussein Jin.
 SENSITIVITY PATTERNS, SEROTYPES OF CRYPTOCOCCUS NEOFORMANS AND DIAGNOSTIC VALUE OF INDIA INK IN PATIENTS WITH CRYPTOCOCCAL MENINGITIS AT KENYATTA NATIONAL HOSPITAL. KAP conference 19 th March 2008: Dr
SENSITIVITY PATTERNS, SEROTYPES OF CRYPTOCOCCUS NEOFORMANS AND DIAGNOSTIC VALUE OF INDIA INK IN PATIENTS WITH CRYPTOCOCCAL MENINGITIS AT KENYATTA NATIONAL HOSPITAL. KAP conference 19 th March 2008: Dr
International Conference on Parasitology August 24-26, 2015 Philadelphia, Pennsylvania, USA
 International Conference on Parasitology August 24-26, 2015 Philadelphia, Pennsylvania, USA SYMPOSIA THE CHALLENGE OF PARASITES AND IMMUNOSUPRESSION: FROM DIAGNOSIS TO TREATMENT from the bench to the bed
International Conference on Parasitology August 24-26, 2015 Philadelphia, Pennsylvania, USA SYMPOSIA THE CHALLENGE OF PARASITES AND IMMUNOSUPRESSION: FROM DIAGNOSIS TO TREATMENT from the bench to the bed
A Cerebellar Conundrum
 BHIVA AUTUMN CONFERENCE 2011 Including CHIVA Parallel Sessions Dr Lavanya Raman Chelsea and Westminster Hospital, London 17 18 November 2011, Queen Elizabeth II Conference Centre, London A Cerebellar Conundrum
BHIVA AUTUMN CONFERENCE 2011 Including CHIVA Parallel Sessions Dr Lavanya Raman Chelsea and Westminster Hospital, London 17 18 November 2011, Queen Elizabeth II Conference Centre, London A Cerebellar Conundrum
Severe Viral Related Complications Following Allo-HCT for Severe Aplastic Anemia
 Severe Viral Related Complications Following Allo-HCT for Severe Aplastic Anemia Liat Shragian Alon, MD Rabin Medical Center, ISRAEL #EBMT15 www.ebmt.org Patient: 25-year-old male No prior medical history
Severe Viral Related Complications Following Allo-HCT for Severe Aplastic Anemia Liat Shragian Alon, MD Rabin Medical Center, ISRAEL #EBMT15 www.ebmt.org Patient: 25-year-old male No prior medical history
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Review Article Ocular Toxoplasmosis: Controversies in Primary and Secondary Prevention
 Ashdin Publishing Journal of Neuroinfectious Diseases Vol. 4 (2013), Article ID 235689, 5 pages doi:10.4303/jnd/235689 ASHDIN publishing Review Article Ocular Toxoplasmosis: Controversies in Primary and
Ashdin Publishing Journal of Neuroinfectious Diseases Vol. 4 (2013), Article ID 235689, 5 pages doi:10.4303/jnd/235689 ASHDIN publishing Review Article Ocular Toxoplasmosis: Controversies in Primary and
Toxoplasmosis. Life cycle Infective stages Congenital Toxoplasmosis Lab.Diagnosis Immunity to Toxoplasmosis Toxoplasmosis & Pregnancy
 Toxoplasmosis Life cycle Infective stages Congenital Toxoplasmosis Lab.Diagnosis Immunity to Toxoplasmosis Toxoplasmosis & Pregnancy Human Toxoplasmosis Toxoplasmosis is a zoonotic disease Caused by Coccidian
Toxoplasmosis Life cycle Infective stages Congenital Toxoplasmosis Lab.Diagnosis Immunity to Toxoplasmosis Toxoplasmosis & Pregnancy Human Toxoplasmosis Toxoplasmosis is a zoonotic disease Caused by Coccidian
Congenital CMV infection. Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera Utara
 Congenital CMV infection Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera Utara Congenital CMV infection Approximately 0.15 2% of live births
Congenital CMV infection Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera Utara Congenital CMV infection Approximately 0.15 2% of live births
Cerebral toxoplasmosis in an HIV negative patient: the first documented case report in Africa and literature review
 Cerebral toxoplasmosis in an HIV negative patient: the first documented case report in Africa and literature review Background: Cerebral toxoplasmosis in HIV negative persons is extremely rare. To the
Cerebral toxoplasmosis in an HIV negative patient: the first documented case report in Africa and literature review Background: Cerebral toxoplasmosis in HIV negative persons is extremely rare. To the
Outline. Cryptococcosis Pneumocystosis Diarrhea. Case Histories: HIV Related- Opportunistic Infections in 2015
 AU Edited: 05/06/15 Case Histories: HIV Related- Opportunistic Infections in 2015 Henry Masur, MD Clinical Professor of Medicine George Washington University School of Medicine Bethesda, Maryland Washington,
AU Edited: 05/06/15 Case Histories: HIV Related- Opportunistic Infections in 2015 Henry Masur, MD Clinical Professor of Medicine George Washington University School of Medicine Bethesda, Maryland Washington,
Central Nervous System and HIV/AIDS
 UPDATE ARTICLE Central Nervous System and HIV/AIDS Naveet Wig*, J P Wali** Introduction HIV-infection and particularly its late stage of severe immunodeficiency (AIDS) render the nervous system susceptible
UPDATE ARTICLE Central Nervous System and HIV/AIDS Naveet Wig*, J P Wali** Introduction HIV-infection and particularly its late stage of severe immunodeficiency (AIDS) render the nervous system susceptible
Clinical-Radiological-Pathological Correlation. Lymphomatoid Granulomatosis. Michael Leffler-McCabe, MD; H. Brent Clark, MD, PhD*
 1 Clinical-Radiological-Pathological Correlation Lymphomatoid Granulomatosis Michael, MD; H. Brent Clark, MD, PhD* Department of Neurology and *Department of Laboratory Medicine and Pathology, University
1 Clinical-Radiological-Pathological Correlation Lymphomatoid Granulomatosis Michael, MD; H. Brent Clark, MD, PhD* Department of Neurology and *Department of Laboratory Medicine and Pathology, University
Index. B Biological factors, 2 Brain stem encephalitis, Burkitt s lymphoma, 83, 105
 Index A Acquired immunodeficiency syndrome (AIDS) abdomen gallbladder complications, 97, 107 109 gastrointestinal complications, 96, 105 106 liver complications, 97, 107 109 neoplasm, 99, 110 111 pancreas
Index A Acquired immunodeficiency syndrome (AIDS) abdomen gallbladder complications, 97, 107 109 gastrointestinal complications, 96, 105 106 liver complications, 97, 107 109 neoplasm, 99, 110 111 pancreas
Opportunistic Infections and Immune Reconstitution Inflammatory Syndrome
 Disclosures Opportunistic Infections and Immune Reconstitution Inflammatory Syndrome I have received grant funding from the National Institutes of Health and the Gilead Research Scholars Program in HIV.
Disclosures Opportunistic Infections and Immune Reconstitution Inflammatory Syndrome I have received grant funding from the National Institutes of Health and the Gilead Research Scholars Program in HIV.
Disclosures. Learning objectives. Neurosyphilis NEUROINFECTIOUS DISEASES: PRACTICAL TIPS FOR COMMON DISORDERS. I have no disclosures.
 Disclosures NEUROINFECTIOUS DISEASES: PRACTICAL TIPS FOR COMMON DISORDERS Felicia Chow, MD, MAS Assistant Professor of Neurology and Medicine (ID) February 8, 2017 I have no disclosures. Learning objectives
Disclosures NEUROINFECTIOUS DISEASES: PRACTICAL TIPS FOR COMMON DISORDERS Felicia Chow, MD, MAS Assistant Professor of Neurology and Medicine (ID) February 8, 2017 I have no disclosures. Learning objectives
Too Competent for Cryptococcus Starr Steinhilber, MD Victoria Johnson, MD
 SGIM Clinical Vignettes Session F May 12, 2012 Too Competent for Cryptococcus Starr Steinhilber, MD Victoria Johnson, MD 48 yo healthy AAM Sx Fevers Chills Headache Back pain Vomiting Headache Back pain
SGIM Clinical Vignettes Session F May 12, 2012 Too Competent for Cryptococcus Starr Steinhilber, MD Victoria Johnson, MD 48 yo healthy AAM Sx Fevers Chills Headache Back pain Vomiting Headache Back pain
8/11/2015. Febrile neutropenia Bone marrow transplant Immunosuppressant medications
 Dean Van Loo Pharm.D. Febrile neutropenia Bone marrow transplant Immunosuppressant medications Steroids Biologics Antineoplastic Most data from cancer chemotherapy Bone marrow suppression Fever is the
Dean Van Loo Pharm.D. Febrile neutropenia Bone marrow transplant Immunosuppressant medications Steroids Biologics Antineoplastic Most data from cancer chemotherapy Bone marrow suppression Fever is the
Analysis. Answers. Action. Saturday Night Fever. Shaka Brown Capital Congress
 Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Pneumocystis Pneumonia (PCP): Part 2
: Part 2") NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pneumocystis Pneumonia (PCP): Part 2 Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pneumocystis Pneumonia (PCP): Part 2 Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation
Adjunctive Options for Severe PCP. Dr Erica Shaddock Division of Pulmonology and Critical Care Charlotte Maxeke Johannesburg Academic Hospital
 Adjunctive Options for Severe PCP Dr Erica Shaddock Division of Pulmonology and Critical Care Charlotte Maxeke Johannesburg Academic Hospital Is this topic still relevant? Is this topic still relevant?
Adjunctive Options for Severe PCP Dr Erica Shaddock Division of Pulmonology and Critical Care Charlotte Maxeke Johannesburg Academic Hospital Is this topic still relevant? Is this topic still relevant?
Clinical Aspect and Application of Laboratory Test in Herpes Virus Infection. Masoud Mardani M.D,FIDSA
 Clinical Aspect and Application of Laboratory Test in Herpes Virus Infection Masoud Mardani M.D,FIDSA Shahidhid Bh BeheshtiMdi Medical lui Universityit Cytomegalovirus (CMV), Epstein Barr Virus(EBV), Herpes
Clinical Aspect and Application of Laboratory Test in Herpes Virus Infection Masoud Mardani M.D,FIDSA Shahidhid Bh BeheshtiMdi Medical lui Universityit Cytomegalovirus (CMV), Epstein Barr Virus(EBV), Herpes
Case Report Chronic Lymphocytic Inflammation with Pontine Perivascular Enhancement Responsive to Steroids, with Cranial and Caudal Extension
 Hindawi Case Reports in Neurological Medicine Volume 2017, Article ID 2593096, 4 pages https://doi.org/10.1155/2017/2593096 Case Report Chronic Lymphocytic Inflammation with Pontine Perivascular Enhancement
Hindawi Case Reports in Neurological Medicine Volume 2017, Article ID 2593096, 4 pages https://doi.org/10.1155/2017/2593096 Case Report Chronic Lymphocytic Inflammation with Pontine Perivascular Enhancement
Bacterial, viral, protoozal and fungal infections of the CNS
 Bacterial, viral, protoozal and fungal infections of the CNS Prof. Isidro Ferrer, Institut Neuropatologia, Servei Anatomia Patològica, IDIBELL-Hospital Universitari de Bellvitge, Universitat de Barcelona,
Bacterial, viral, protoozal and fungal infections of the CNS Prof. Isidro Ferrer, Institut Neuropatologia, Servei Anatomia Patològica, IDIBELL-Hospital Universitari de Bellvitge, Universitat de Barcelona,
CRANIAL LESION DUE TO T. GONDII IN A PATIENT WITH HIV SEROPOSITIVITY: CASE REPORT
 Indian Journal of Medical s ISSN: 2319 3832(Online) CRANIAL LESION DUE TO T. GONDII IN A PATIENT WITH HIV SEROPOSITIVITY: CASE REPORT *Gulfem Ece 1, Ali Akay 2, Mete Ruksen 2 and Erbay A 3 1 Department
Indian Journal of Medical s ISSN: 2319 3832(Online) CRANIAL LESION DUE TO T. GONDII IN A PATIENT WITH HIV SEROPOSITIVITY: CASE REPORT *Gulfem Ece 1, Ali Akay 2, Mete Ruksen 2 and Erbay A 3 1 Department
Brain Pain Infections of the CNS
 FRIDAY, OCTOBER 28, 2016 Brain Pain Infections of the CNS Suyash Mohan MD, PDCC Assistant Professor of Radiology & Neurosurgery Division of Neuroradiology, Department of Radiology Perelman School of Medicine
FRIDAY, OCTOBER 28, 2016 Brain Pain Infections of the CNS Suyash Mohan MD, PDCC Assistant Professor of Radiology & Neurosurgery Division of Neuroradiology, Department of Radiology Perelman School of Medicine
EBV Protocol
 EBV Protocol 8.26.14 Data From UNOS Summary Stats 1988-2014 CASU + 2009-2014 CAPC Organ Total PTLD Percent PTLD Percent PTLD in Literature Heart 294 21 7 3-9 Heart-Lung 34 3 9 16 Intestine 42 7 17 10-45
EBV Protocol 8.26.14 Data From UNOS Summary Stats 1988-2014 CASU + 2009-2014 CAPC Organ Total PTLD Percent PTLD Percent PTLD in Literature Heart 294 21 7 3-9 Heart-Lung 34 3 9 16 Intestine 42 7 17 10-45
Clinico-Pathological Conference
 Disclosures Clinico-Pathological Conference Andrew W. Bollen DVM, MD Professor of Pathology, UCSF Betjemann- None Bollen- None Larimer- None John Betjemann MD Assistant Professor of Neurology, UCSF Phil
Disclosures Clinico-Pathological Conference Andrew W. Bollen DVM, MD Professor of Pathology, UCSF Betjemann- None Bollen- None Larimer- None John Betjemann MD Assistant Professor of Neurology, UCSF Phil
Immunological Aspects of Parasitic Diseases in Immunocompromised Individuals. Taniawati Supali. Department of Parasitology
 Immunological Aspects of Parasitic Diseases in Immunocompromised Individuals Taniawati Supali Department of Parasitology 1 Defense mechanism in human Th17 (? ) Acute Chronic Th1 Th 2 Intracellular Treg
Immunological Aspects of Parasitic Diseases in Immunocompromised Individuals Taniawati Supali Department of Parasitology 1 Defense mechanism in human Th17 (? ) Acute Chronic Th1 Th 2 Intracellular Treg
Condition First line Alternative Comments Candidemia Nonneutropenic adults
 Recommendations for the treatment of candidiasis. Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious Diseases Society of America. Condition First line Alternative
Recommendations for the treatment of candidiasis. Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious Diseases Society of America. Condition First line Alternative
SLIDE SEMINAR NON NEOPLASTIC LYMPH NODE DISORDERS DR SHEILA NAIR CMC, VELLORE
 SLIDE SEMINAR NON NEOPLASTIC LYMPH NODE DISORDERS DR SHEILA NAIR CMC, VELLORE Case 1 34 year old male, mass right cervical region, for 4 years. No other significant findings. Grossly, the mass was well
SLIDE SEMINAR NON NEOPLASTIC LYMPH NODE DISORDERS DR SHEILA NAIR CMC, VELLORE Case 1 34 year old male, mass right cervical region, for 4 years. No other significant findings. Grossly, the mass was well
Toxoplasmosis. Seminar. For personal use. Only reproduce with permission from The Lancet Publishing Group.
 Seminar Toxoplasmosis J G Montoya, O Liesenfeld Toxoplasma gondii is a protozoan parasite that infects up to a third of the world s population. Infection is mainly acquired by ingestion of food or water
Seminar Toxoplasmosis J G Montoya, O Liesenfeld Toxoplasma gondii is a protozoan parasite that infects up to a third of the world s population. Infection is mainly acquired by ingestion of food or water
HIV and Parasite Load. Keith Keller
 HIV and Parasite Load Keith Keller HIV: Human Immunodeficiency Virus Retrovirus that infects CD4+ T Cells Uses host cell s mechanics to reproduce, by means of reverse transcriptase and integrase which
HIV and Parasite Load Keith Keller HIV: Human Immunodeficiency Virus Retrovirus that infects CD4+ T Cells Uses host cell s mechanics to reproduce, by means of reverse transcriptase and integrase which
A common case definition for PML
 A common case definition for PML Transatlantic workshop: Drug-related Progressive Multifocal Leukoencephalopathy (PML) 25.-26.7.2011, EMA, London Paul-Ehrlich-Institut Dr. Dirk Mentzer, MD Paul-Ehrlich-Str.
A common case definition for PML Transatlantic workshop: Drug-related Progressive Multifocal Leukoencephalopathy (PML) 25.-26.7.2011, EMA, London Paul-Ehrlich-Institut Dr. Dirk Mentzer, MD Paul-Ehrlich-Str.
Challenges in viral CNS infections [encephalitis]
![Challenges in viral CNS infections [encephalitis]](/thumbs/86/93638824.jpg "Challenges in viral CNS infections [encephalitis]") Challenges in viral CNS infections [encephalitis] PIGS Training Course 2013 Basel November 8, 2013 Christoph Aebi christoph.aebi@insel.ch Definition Encephalitis is defined as a syndrome of neurological
Challenges in viral CNS infections [encephalitis] PIGS Training Course 2013 Basel November 8, 2013 Christoph Aebi christoph.aebi@insel.ch Definition Encephalitis is defined as a syndrome of neurological
What prescribers need to know
 HUMIRA Citrate-free presentations in an Electronic Medical Record (EMR) What prescribers need to know 2 / This is your guide to identifying HUMIRA Citrate-free presentations in your Electronic Medical
HUMIRA Citrate-free presentations in an Electronic Medical Record (EMR) What prescribers need to know 2 / This is your guide to identifying HUMIRA Citrate-free presentations in your Electronic Medical
Innovation in Diagnostics. ToRCH. A complete line of kits for an accurate diagnosis INFECTIOUS ID DISEASES
 Innovation in Diagnostics ToRCH A complete line of kits for an accurate diagnosis INFECTIOUS ID DISEASES EN TOXOPLASMOSIS Toxoplasmosis is a parasitic disease caused by with the obligate intracellular
Innovation in Diagnostics ToRCH A complete line of kits for an accurate diagnosis INFECTIOUS ID DISEASES EN TOXOPLASMOSIS Toxoplasmosis is a parasitic disease caused by with the obligate intracellular
Wales Neonatal Network Guideline
 Congenital infection: Diagnosis and management Overview: Infections transmitted and acquired in utero. Most as a result of primary infection of mother during pregnancy, some organisms such as Cytomegalovirus
Congenital infection: Diagnosis and management Overview: Infections transmitted and acquired in utero. Most as a result of primary infection of mother during pregnancy, some organisms such as Cytomegalovirus
Judith A. Aberg, MD; Linda M. Mundy, MD; and William G. Powderly, MD
 Pulmonary Cryptococcosis in Patients Without HIV Infection* Judith A. Aberg, MD; Linda M. Mundy, MD; and William G. Powderly, MD Purpose: To further elucidate the diagnostic and therapeutic approaches
Pulmonary Cryptococcosis in Patients Without HIV Infection* Judith A. Aberg, MD; Linda M. Mundy, MD; and William G. Powderly, MD Purpose: To further elucidate the diagnostic and therapeutic approaches