Expanding HIV Testing in Ontario? Dr. Rita Shahin October 1, 2013
|
|
|
- Juliana Sandra Lawson
- 6 years ago
- Views:
Transcription
1
2 Expanding HIV Testing in Ontario? Dr. Rita Shahin October 1, 2013
3 Objectives Overview of HIV in Toronto Introduction to routine testing, the treatment cascade and treatment as prevention HIV testing in Ontario Estimates of those infected but undiagnosed in Toronto HIV continuum/cascade in Ontario
4 Number of reported cases Reported cases per 100,000 population 700 Figure 1.23: Incidence of HIV infection by year. Toronto, the rest of Ontario and Canada, Toronto cases Toronto rates Ontario less Toronto rates Canada rates NA NA 0.0 NA: Canadian data for 2010 and 2011 are not available. Year
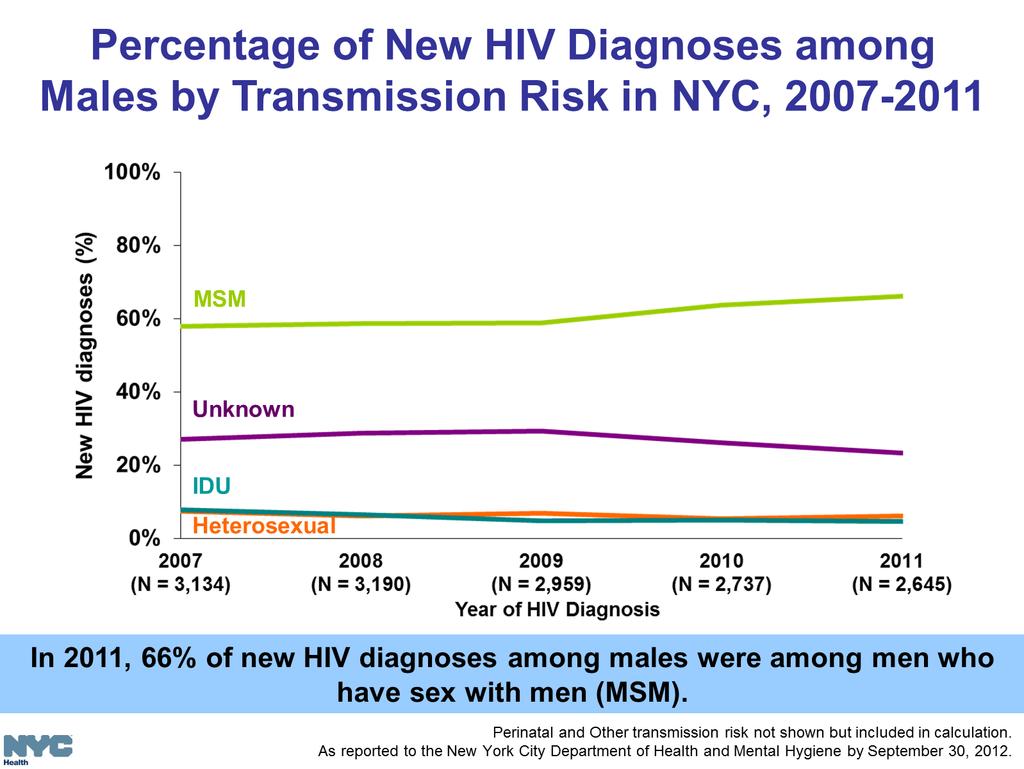
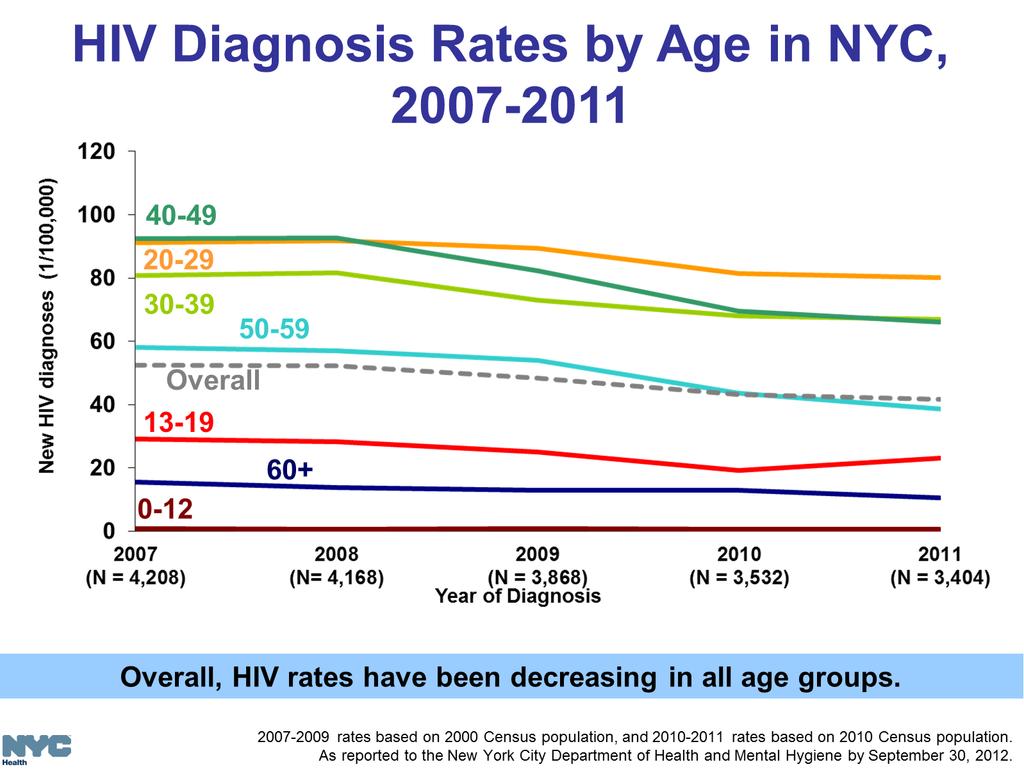
5 Reported cases per 100,000 population 80.0 Figure 1.27: Incidence rates of HIV infection by age group and sex. Toronto, Male rates Female rates Overall rates Male cases Female cases
6 HIV Exposure Categories Table 1.11: Number and proportion of HIV infections by exposure category* and sex. Toronto, Exposure category* MSM 317 (76) N/A 317 (63) MSM/Illicit drug use 15 (4) N/A 15 (3) Illicit drug use 9 (2) 4 (5) 13 (3) Perinatal 1 (<1) 0 (0) 1 (<1) Received blood or blood products 2 (<1) 3 (3) 5 (<1) HIV-Endemic 43 (10) 67 (76) 110 (22) HET-Partner 2 (<1) 2 (2) 4 (<1) NIR-HET 25 (6) 10 (11) 35 (7) Other 5 (1) 2 (2) 7 (1) Total with a known exposure 419 (100) 88 (100) 507 (100) No identifiable risk / Unknown Total N/A: Not Applicable *Definitions for each exposure category are included in the glossary. Cases may report one or more exposures but are counted in the category considered the highest risk according to an exposure category hierarchy. The categories are listed in descending order from those that are considered to carry the highest risk of HIV infection to those considered to carry the low est risk. As of the 2011 report, the exposure category "No identifiable risk/unknow n" has been updated to include all clients w ho have missing or unknow n risk factors. Number of cases (%) Male Female Overall
7
8 Early/Acute HIV Infection Usually the first 6 months of infection Very high viral loads that make individuals highly infectious to their partners The proportion of new infections attributed to EHI has been estimated to be in the range of 25-50% within certain populations Treatment as prevention attempts to reduce the risk of onward transmission USA and UK have issued clinical guidelines for the treatment of individuals with early infection (with caveats about the strength of evidence).

9 HIV Clinical Progression
10 HPTN 052 Study The HIV Prevention Trials Network 052 study was a randomized control trial comparing early vs. delayed ART in 1763 serodiscordant heterosexual couples in 9 countries. 39 HIV transmission occurred, with 28 attributable to the infected partner 27 transmissions were in the delayed group and 1 in the early treatment group with evidence of 96% effectiveness

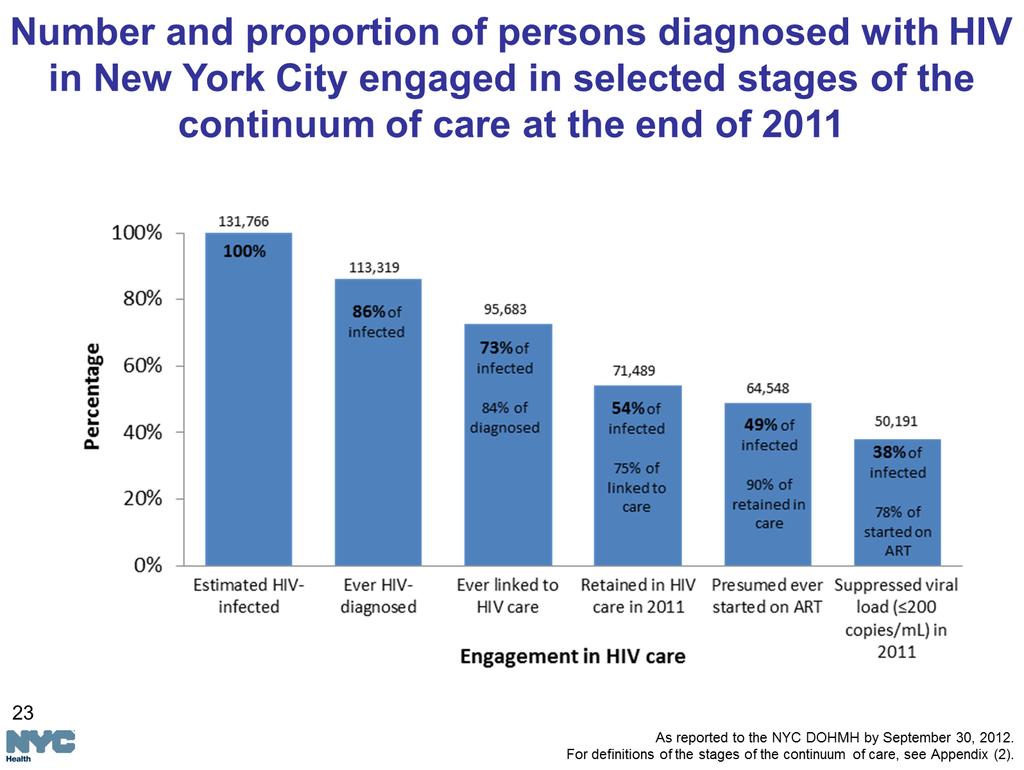
11 Number and percentage of HIV-infected persons engaged in selected stages of the continuum of HIV care United States MMWR (47);
12 Expanded Cascade Sexually Active Exposed Infected Diagnosed Linked to Care Retained in Care On ART Suppressed Viral Load
13 HIV Testing in Ontario Approximately 425,000 tests annually The HIV-positivity rate has decreased continuously since The HIV-positivity rate in Ontario was 0.19% in 2012 and 0.16% in 2013 compared to 0.30% to 0.35% from 1996 to HIV testing is thought to be cost effective if positivity rate is 0.1% or greater.
14 HIV Undiagnosed Prevalence in Toronto Based on OHEMU modelling data, as of 2009 there were approximately 5,798 undiagnosed HIV+ individuals in Toronto Given a population of 2,126,275 people over 18 years of age, the undiagnosed prevalence in adults is approximately 0.27% in Toronto A. Modelled prevalence (Table 6.3a) B. Proportion diagnosed (for Ontario Table 6.2) C. Modelled diagnosed (A*B) D. Modelled undiagnosed (A- C) MSM 10, % 7,508 3,067 MSM-IDU % IDU % HIV-End 3, % 1,625 1,395 HET 2, % 1,214 1,056 Clotting % 45 0 Transfusion % 5 0 Total: 16,920 11,122 5,798
15 Ontario 30,800 HIV infections have been diagnosed in Ontario by end of ,107 individuals with HIV estimated to be in care in 2009 based on billing records (T. Antoniou) OHTN Cohort Study follows people in specialty HIV care in 10 sites in Ontario The mean number of days to the first viral load test among HIV-positive individuals who had nominally tested positive was 65 days (median = 36 days). (POWER study) Eighty-two percent of women and 81 percent of men who were newly diagnosed with HIV had a viral test within three months of testing HIV-positive; however seven percent of women and ten percent of men who were newly diagnosed with HIV had not had a viral load test conducted within 12 months of testing positive for HIV. (POWER study) Mean CD4 count of Ontario Cohort Study participants when entering care was 379 (entered care between 1985 and 2009). (POWER study)
16 Mean CD4 entering care for OCS participants, Mean CD4 count when entering care declined significantly by age. Mean CD4 count was lower for Aboriginal women and men and Black/African women and men. IDUs in the OCS had higher CD4 counts than people from other HIV exposure categories. Men whose exposure category was heterosexual (including HIV endemic and heterosexual transmission) had the lowest CD4 counts when entering care.
17 HIV Continuum in Ontario, 2011 Among 3273 OCS participants in care in 2011, 86.2% were in continuous care, 91.5% were on ART, 87.7% had a suppressed viral load and 84% had an undetectable viral load. (L. Light, ohtn.on.ca) Little variation between regions of Ontario Older adults living with HIV were most likely to be in continuous care and successfully undetectable on ART (M. Manno, ohtn.on.ca)
18 Expanding HIV Testing? People infected with HIV will decrease high-risk behaviours once aware of their status. Early initiation of ART reduces clinical progression and transmission to partners 2006 CDC recommended routine opt-out screening in health care settings 2013 PHAC recommendations promote routine testing The offer of a routine test should be made as part of periodic routine medical care. (guide does not supercede provincial guidelines)
19 Expanding HIV Testing? Challenges include addressing HIV stigma, confidentiality, counseling and consent, costs/resources (lab, linkage to care and ARV treatment) Routine testing vs. expanding targeted testing efforts in groups or neighbourhoods with higher rates?
20 Thank You!

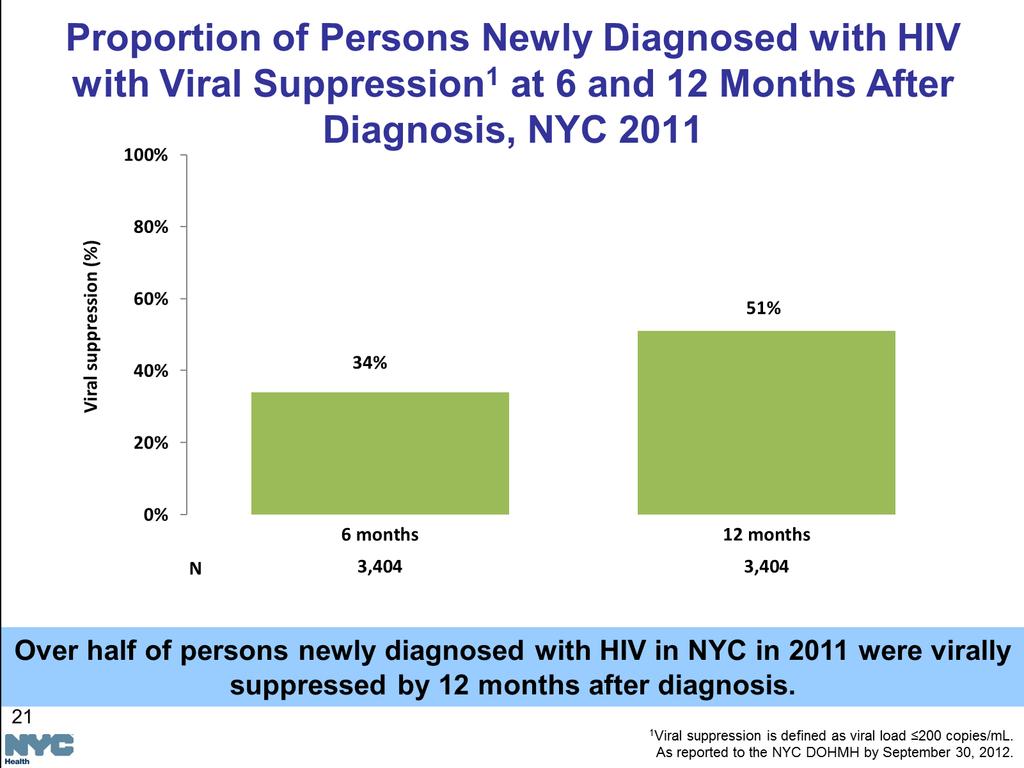
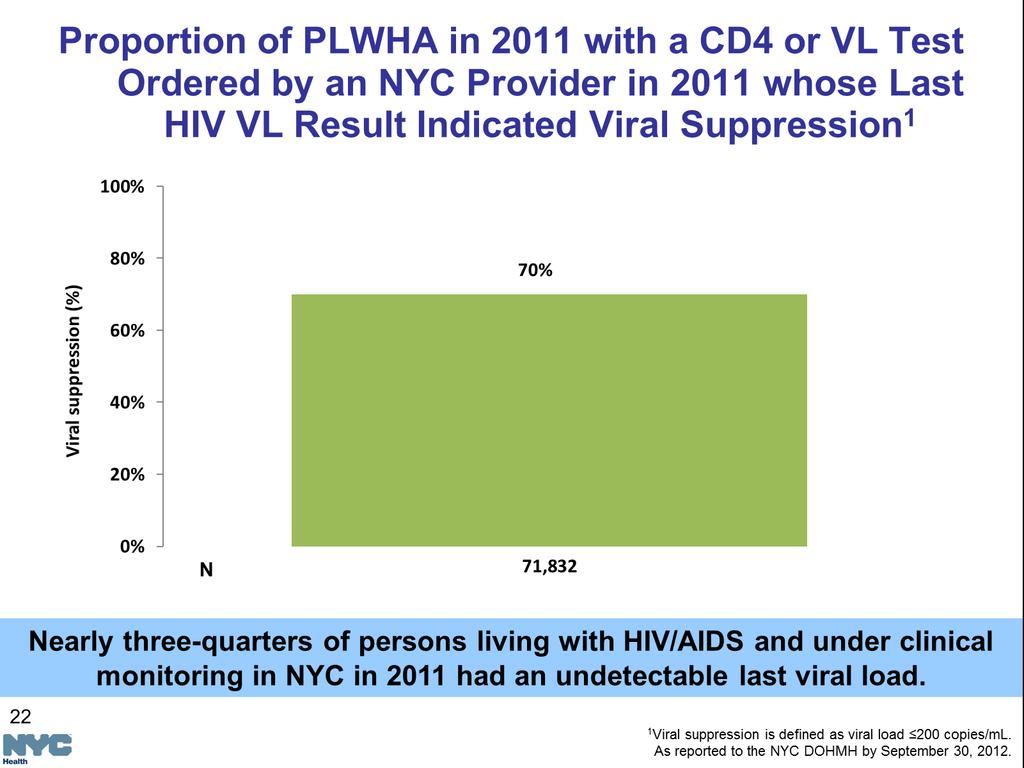
21 Routinizing HIV Testing in New York City: Successes and Lessons Learned Benjamin Tsoi, MD, MPH Director of HIV Testing Bureau of HIV/AIDS Prevention and Control NYC Department of Health and Mental Hygiene

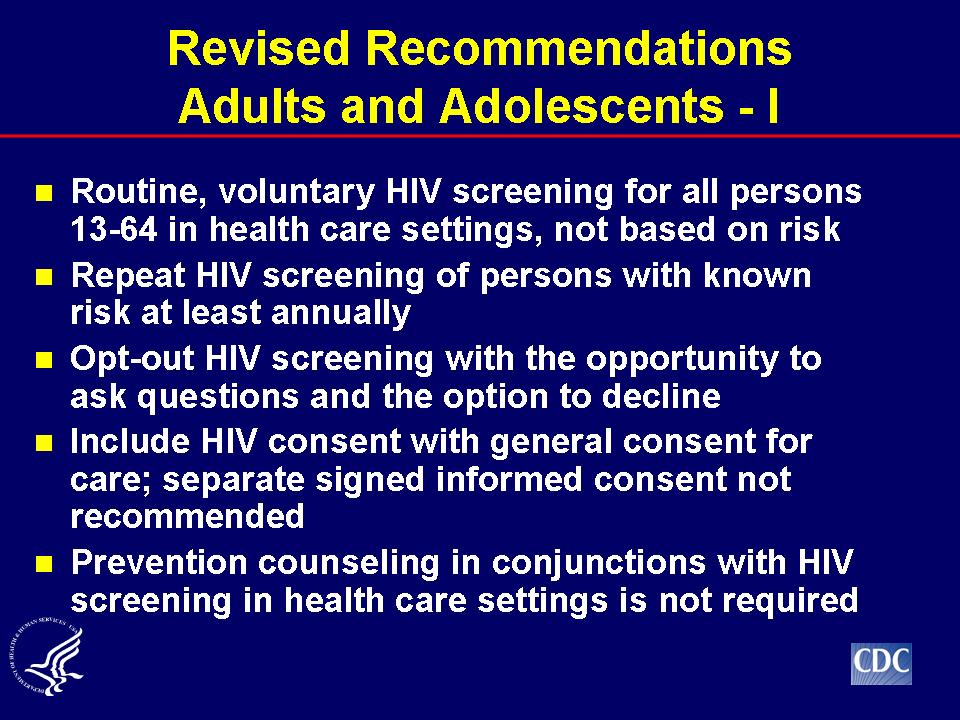
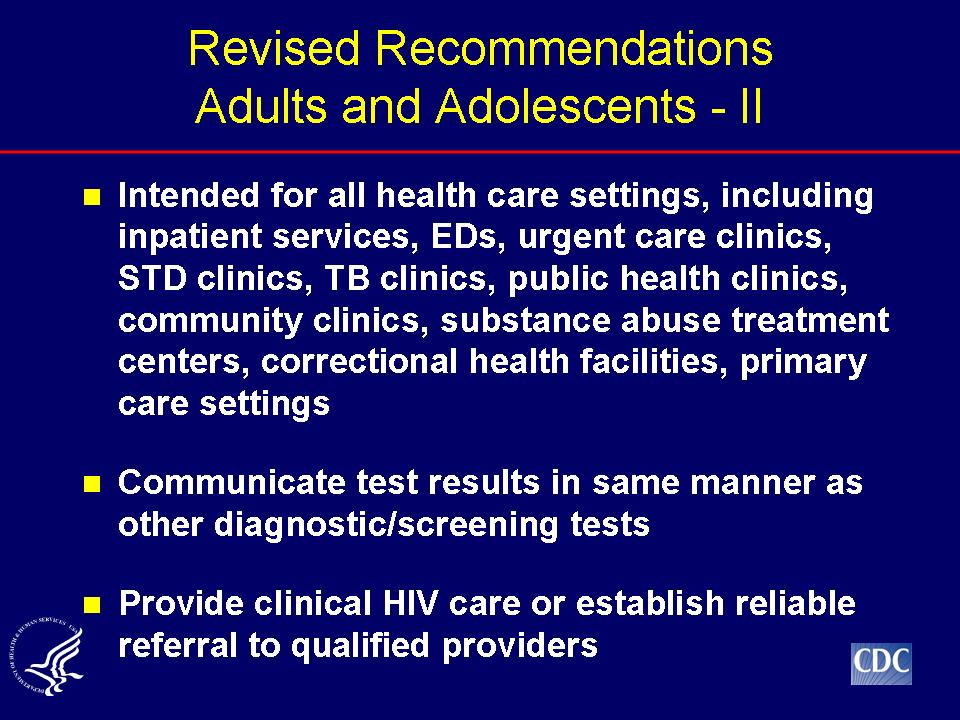
22 CDC Recommendations Routine, voluntary HIV screening for all persons age in health-care settings, not based on risk Patient notified that HIV testing will be performed unless they decline (opt-out screening)
23
24 Previous CDC Recommendations Adults and Adolescents Routinely recommend HIV screening in settings with high HIV prevalence ( 1%) Targeted testing based on risk assessment Routinely recommend HIV testing for those seeking treatment for STDs Annual testing for sexually active MSM
25
26 Recommendations Are Not Having Their Intended Effect in Acute Care Settings EDs account for 10% of all ambulatory care visits ED visits 108 million 107 million 110 million Age million 69.4 million 69.6 million HIV serology 215, , ,000
27 Many with Reactive Rapid Tests in ED Have No Identified Risk Characteristics N= 83 Number (%) No previous test 47 (57%) Risk factors MSM 30 (34%) IDU 8 (10%) High risk hetero partner 3 (4%) No identified risk 42 (51%) Cook County Bureau of Health Services, 2003
28 Missed Opportunities to Screen for HIV Many HIV-Infected Persons Access Health Care, But Are Not Tested Risk-based approach doesn t work
29 HIV Cases in South Carolina, ,315 newly reported HIV cases matched to registry of health care visits ( ) 3,157 (73%) made >20,000 health care visits prior to their first HIV diagnosis 77% did not have diagnosis code to prompt for HIV test Risk-based screening would have missed majority of HIV cases MMWR December 1, 2006
30 Late Testers with HIV in South Carolina ,784 (41%) developed AIDS within 1 year 1,302 (73%) made 7,988 previous healthcare visits, but were not tested for HIV Median: 4 per patient; range:1 133 MMWR December 1, 2006
31 HIV Cases in Kaiser Permanente 440 patients with new HIV diagnosis Mean: 8.6 health-care contacts before positive HIV test CD4 count at diagnosis: 62% < % < % <50 Only 26% had risk factors documented in chart Majority eligible for treatment at time of diagnosis - Klein D, et al JAIDS 2003
32 Patients May Not Disclose Risks
33 Patients May Not Disclose Risks NYC National HIV Behavioral Surveillance project ( ) Thirty-nine percent (39%) of all men who reported at least one male sex partner in past year & self-reported HIV seronegative, did not disclose to their healthcare provider Black and Hispanic men who have sex with men (MSM) were less likely to disclose than white MSM Bernstein et al. Arch Intern Med. 2008;168(13):
34 Sexual Identity Don t Always Match Sexual Behavior Random digit-dialed telephone survey of NYC residents (2003) 12% reported sex with other men Of those, 61% straight identified Racial minority, be foreign-born, have lower education and income levels, and be married 36% gay identified 3% bisexual identified Pathela et al. Ann Intern Med. 2006;145:
35
36 Routine Screening Works
37 Previous CDC Recommendations Pregnant Women Routine, voluntary HIV testing as part of prenatal care, as early as possible, for all pregnant women Simplified pretest counseling Flexible consent process
38

39 New York City Experience with Routine Screening
 Median income: Congressional district with lowest median income: 16 (Bronx) 21 st highest: Upper")
40 New York City Most populous city in U.S. Population: 8,175,133 (2010 Census) 5 boroughs Area: sq mi (1,213 km 2 ) Median income: Congressional district with lowest median income: 16 (Bronx) 21 st highest: Upper East Side in Manhattan

41 NYC Demographics Non-Hispanic (NH) White: 33.3% Hispanic: 28.6% NH Black: 22.8% Asian/Pacific Islander: 12.6% Other: 2.7%
42
43
44
45
46
47
48
49
50

51 New York State HIV Testing Law, 2010
52 NYS Chapter 308 of the Laws of 2010 Amended HIV Testing Law Signed on July 30, 2010 Effective September 1, 2010 NYS DOH Regulations Developed with input of many partners Published in November 2011 Adopted in February
53 NYS Chapter 308 of the Laws of 2010 Key Provisions HIV testing must be offered to all patients Aged receiving hospital or primary care services, with limited exceptions Consent for HIV testing May be part of a general consent to medical care, with specific opt-out language included Can be oral for rapid HIV testing (except in correctional facilities) and must be noted in the medical record Can remain in effect for a period of time stipulated by the patient or until revoked by the patient
54 NYS Chapter 308 of the Laws of 2010 Key Provisions (cont.) Prior to being asked to consent to HIV testing, patients must be provided information about HIV required by the Public Health Law Clinicians authorizing HIV testing must arrange, with the consent of the patient, an appointment for medical care for those confirmed as HIV positive
55 Laboratory Testing Testing volume was stable in the baseline period and increased at a significant rate after Sept , , , ,000 80,000 60,000 40,000 20,000 0 Total Conventional Rapid
56 NYS Testing Law: Early Impact CHCs and Small Practice Sites Percent of Patients with HIV Test Results at CHCs and Small Practice Sites By Age ( , n=97) NYS HIV Testing Law Begins NYC DOHMH, Primary Care Information Project,
57 Lessons Learned
58 Keys to Implementing Change Obtain buy-in Have a champion Develop a plan Provide training & technical assistance Provide ongoing feedback Be flexible
59 Obtain Buy In Gain support from leadership Must be backed with accountability Gain support from front line staff Have a multi-discipline approach
60 Have a Champion Someone who is passionate Someone who has the administrative authority to invoke change Have someone with similar training talk to each other, i.e., have emergency medicine (EM) provider talk to other EM providers
61 Plan-Do-Study-Act (PDSA)
62 Develop a Plan Set aims, measures Institutional policy change Map process/work flow How would testing integrate into patient flow? Include quality improvement, including Plan-Do-Study-Act (PDSA) process Set up process to collect & analyze data
63 Provide Training & Technical Assistance Team trainings Collaborative calls Site visits Individualized technical assistance Data calls Offer counseling training to providers Offer CME credits
64 Provide Ongoing Feedback Review baseline data Are agencies able to measure key outcomes? Awareness is a powerful motivator Assess impact of implementation Consider targeted daily chart reviews
65 Daily Chart Review QI Process Days 1-2: monitor charts without telling providers Day 3: tell provider that you are monitoring Days 4-5: provide daily feedback
66 Be Flexible One size does not fit all Choose HIV test appropriate for setting No magic bullet
67 Musings Testing teenagers have its own unique issues and challenges Legislation assist, but not sufficient Electronic health record prompts and alerts are useful, but need monitoring Be aware of provider fatigue Be aware of staff turn over (training) Competition and incentives are good Just Do It!
68 Challenges & Barriers Competing priorities Resource allocation Team stability Electronic health record modifications Data reporting and analysis Testing team buy in Timely data feedback for continuous quality improvement (CQI)
69 Six A s to Successful QI Allocate resources to the project Senior Leaders Assign a champion Activate the team Assess and share results (continuously) Act based on data Agree on final process and sustain
70 Thank you Questions?
71
72
73
74
75
76
77
78
79
80
81 HIV testing: a new paradigm for British Columbia Dr. Réka Gustafson Medical Health Officer and Medical Director of Communicable Disease Control Vancouver Coastal Health
82 Acknowledgements Vancouver s Acute Care Hospitals Vancouver s Family Physicians Ellen Demlow Afshan Nathoo Kendra McPherson Chris Buchner Scott Harrison Val Munroe Dr. David Hall Dr. Julio Montaner Dr. Perry Kendall Dr. Mark Gilbert Dr. Sarah Stone Dr. Rolando Barrios Dr. Jat Sandhu Dr. Patricia Daly Dr. Dean Chittock Julie Kille Miranda Compton Meaghan Thumath
83 STOP HIV/AIDS ( ) A provincially funded pilot to enhance early diagnosis and treatment of HIV, with the goal of altering the course of the epidemic Two pilot sites: Vancouver and Prince George Not accompanied by any changes in testing or treatment recommendations
84 Initial approach Analyse the cascade of care in our community Who is getting infected? Where are they being diagnosed? What stage of their disease are they being diagnosed? How long do they take to engage in care? How well are they retained in care? Do they achieve viral suppression? Do they maintain viral suppression?
85 Treatment How long do people take to engage in care? How well are people retained in care? Do people achieve viral suppression? Do people maintain viral suppression? Peer Navigator Program Outreach Team Enhanced Public Health Follow-up Provincial collaborative Supports for family physicians to retain HIV positive patients in their care Re-designed, seamless system of care
86 Initial approach to testing Expanded hours and locations for HIV testing in the community Point of care testing fairs Point of care testing at St. Paul s Hospital Expanded outreach testing in areas such as bathhouses and parks Outcome of doing more of the same: Additional services were welcomed and well utilised but Little population level change in testing rates and stage of disease at diagnosis
87 US CDC 2006 Testing Recommendations In addition to antenatal and risk-based HIV testing For patients in all health-care settings HIV screening is recommended for patients in all health-care settings after the patient is notified that testing will be performed unless the patient declines (opt-out screening). Persons at high risk for HIV infection should be screened for HIV at least annually. Separate written consent for HIV testing should not be required; general consent for medical care should be considered sufficient to encompass consent for HIV testing. Prevention counseling should not be required with HIV diagnostic testing or as part of HIV screening programs in health-care settings.

88 Health Protection Agency Routine HIV testing in hospitals, primary care and community Feasible Acceptable Ranges of cost per diagnosis overlapped for the three settings
89 Diagnostic Yield Risk- Based Testing Routine Testing in High Prevalence Settings Reach Routine Testing in General Health Care Settings 9
90 In the absence of an existing recommendation, we needed A practice recommendation Rationale An incentive to participate (to overcome the not my problem ) Implementation plan Endorsement Enabling policies Care and treatment plan for all settings Monitoring and evaluation plan
91 New HIV Testing Recommendations BCMJ, 2011, 53:49 Offer an HIV test to all adults in your practice who have not had one in the past year in acute and community care as part of blood work for any other reason every time you test for STIs, HCV, tuberculosis Vancouver Coastal Health Public Health 11
92 New HIV Testing Recommendations BCMJ, 2011, 53:49 If aware of a specific risk, recommend an HIV test now, and more often clinical symptoms every time you diagnose another STI every 3-6 months if you are aware of ongoing high risk Vancouver Coastal Health Public Health 12
93 Rationale Early diagnosis benefits the HIV infected individual Early diagnosis benefits partners of the HIV infected individual Early diagnosis is the exception, rather than the norm People diagnosed late have had multiple missed opportunities for earlier diagnosis in the health care system Risk-based testing has inherent limitations that cannot be overcome by doing more risk-based testing Routine HIV testing is cost effective at relatively low diagnostic yield HIV infection is consistent with all generally accepted criteria that justify screening
94 Early diagnosis benefits the individual Life expectancy as a function of disease stage at start of treatment Disease stage at start of Treatment Can expect to live to (years) CD4< CD CD BMJ 2011; 343:d6016
95 Early Treatment Benefits Patients Asymptomatic Patients DHHS [1] IAS-USA [2] CD4+ cell count < 350 cells/mm³ Start ART Start ART CD4+ cell count cells/mm³ Start ART* Start ART ǂ CD4+ cell count > 500 cells/mm³ Panel divided Should be considered ǂ Clinical Conditions Favoring Initiation of Therapy Regardless of CD4+ Cell Count DHHS [1] IAS-USA [2] Symptomatic HIV disease Pregnancy HIV-associated nephropathy HIV-1 RNA > 100,000 copies/ml CD4+ count decline > 100 cells/mm 3 per year Hepatitis B co-infection (when active or needing treatment) History of AIDS-defining illness Certain acute opportunistic infections ǂ Symptomatic HIV disease Pregnancy in women HIV-1 RNA > 100,000 copies/ml Rapid decline in CD4+ cell count (> 100 cells/ mm³/yr) Active HBV or HCV infection Active or high risk for CVD Symptomatic primary HIV infection HIVAN Serodiscordant couples

96 Early diagnosis benefits partners 16
97 Early treatment benefits partners 1,763 couples HIV positive partner with CD % heterosexual N=886 Immediate ART N=877 ART at CD4 of transmission 3 cases of extrapulmonary TB 10 deaths 27 transmissions 17 cases of extrapulmonary TB 13 deaths 17


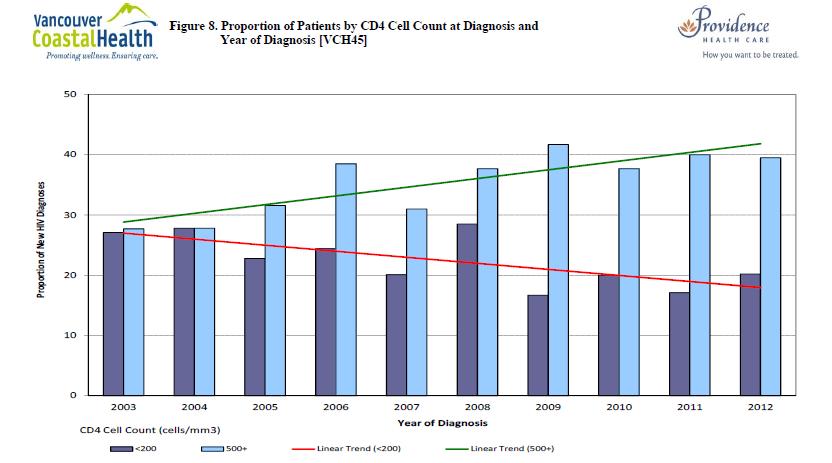
98 Early diagnosis is not the norm CD CD CD4 <
99 Missed Opportunities Analysis Retrospective electronic chart review of new HIV cases in Vancouver from Acute care visits and laboratory tests for three years prior to diagnosis were included in the analysis Data from hospital, emergency departments, outpatient clinics, and hospital laboratories extracted for all cases Acute care visits and laboratory tests prior to and within 3 months of last negative HIV test were excluded from study Acute care visits and laboratory tests within 2 weeks of diagnosis were excluded from study Data do not include health care contacts outside of hospital or laboratory tests. Therefore analysis underestimates total number of missed opportunities.
100 Missed Opportunities among ER, Inpatient, and Hospital Outpatient Visits CD4 at Diagnosis N 1 Prior Encounter Mean # Encounters* < % % % % 4.4 Unknown 52 12% 4.8 Overall % 4.2 Total Missed Opportunities = % of Patients Diagnosed with a CD4 count below 350 had at least one ER, inpatient, or outpatient encounter *Among those with 1 Prior Encounter CD4 at data available for 90% of clients
101 Laboratory Tests CD4 at Diagnosis N 1 Prior Lab Mean # Lab Test (%) Tests* < % % % % 2.8 Unknown 52 4% 2.5 Overall % % of Patients Diagnosed with a CD4 count below 350 had at least one public laboratory test *Among those with 1 Prior Lab Test CD4 at data available for 90% of clients Total Missed Opportunities = 322
102 LIMITATIONS OF RISK-BASED TESTING

103 Limitations of risk-based testing Stigmatizes testing Discourages clinicians from offering an HIV test Discourages patients from seeking and/or accepting the test
104 Limitations of risk-based testing Fails to recognize changes in epidemiology Identified mode of HIV transmission: 58% MSM 25% heterosexual 12% IDU BCCDC HIV Annual Report, 2011 ( 25
105 Limitations of risk based testing Assumes incorrectly-- that people with risk behaviours recognize their risk AND tell their health care provider about them. Venue-based survey of gay men: 20% have never told a health care provider that they have sex with men Mean duration to disclosure was 4 years Mtrack,
106 Limitations of risk-based testing It s not happening 50% of those with HCV are tested for HIV within 3 months of diagnosis Less than 25% of those with a diagnosis of Sexually Transmitted Infection (STI) have an HIV test following their diagnosis 38.6% of individuals with a new HIV diagnosis had their first HIV test at the time of diagnosis ( ) M. Gilbert, BCCDC 27
107 WHO Criteria for Screening Programmes The condition sought should be an important health problem for the individual and community. There should be an accepted treatment or useful intervention for patients with the disease. The natural history of the disease should be adequately understood. There should be a latent or early symptomatic stage. There should be a suitable and acceptable screening test or examination. Facilities for diagnosis and treatment should be available There should be an agreed policy on whom to treat as patients. Treatment started at an early stage should be of more benefit than treatment started later. The cost should be economically balanced in relation to possible expenditure on medical care as a whole. Case finding should be a continuing process and not a once and for all project.
108 Conservative threshold for cost effectiveness is estimated to be 1/1000 new diagnoses* or 2/1000 diagnosed prevalence Paltiel AD, et al. Expanded screening for HIV in the United States - an analysis of cost-effectiveness. N Engl J Med 2005; 352(6): Paltiel AD, et al. Expanded HIV screening in the United States: effect on clinical outcomes, HIV transmission, and costs. Ann Intern Med 2006; 145: Sanders GD, Bayoumi AM, Sundaram V, Bilir SP, Neukermans CP, Rydzak CE et al. Cost-effectiveness of screening for HIV in the era of highly active antiretroviral therapy. N Engl J Med 2005; 352(6): *Walensky RP, et al. Routine human immunodeficiency virus testing: an economic evaluation of current guidelines. Am J Med 2005; 118(3): Yazdanpanah Y et al. Routine HIV Screening in France: Clinical Impact and Cost-Effectiveness. PLoS One. 2010;5(10):e
109 Turning Missed Opportunities into Opportunities Routine HIV testing in acute care Vancouver Hospitals (October 2011-Present) Routine HIV testing in primary care (June 2012)
110 Implementation Endorsement of medical leadership/identifying champions Enabling policies: tailor pre-test information to patient and clinical setting: counseling, posters, printed materials etc Engagement of the community Social Marketing Campaign Pathway for follow-up Delegate follow-up process Website for family physicians to link them to information, public health, primary care guidelines, expert consultation, peer support Peer navigator program in the hospital Education: comprehensive, recurring, sustained Whatever the ward/hospital/clinic needed to get the job done Data, data, and more data
111 Whatever the hospital ward/clinic needed Education embedded where they are already receiving it or where they are working At a conference, or in their lunch room Wording and pictures on posters Translation/lamination of information materials Clerk to process orders Nurse embedded in clinics providing care to high prevalence populations Access to outreach and peers Endorsement of the college
112 Now to the data FEASIBLE
113 Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May June July Aug Sep Oct Nov Dec Number of Tests 2500 Number of HIV Tests at Vancouver Hospitals by Month SPH MSJ VGH UBCH Public Health Surveillance Unit Time Start of Routine Testing
114 Number of Tests Family Practice HIV Testing Volumes January June 2013 Public Health Surveillance Unit Jan Mar May Jul Sep Nov Jan Mar May Jul Sep Nov Jan Mar May Jul Sep Nov Jan Mar May Note: Webinars began April 2012, IPS began July 2012, and Workshops started August 2012 Positives Coastal Rural Coastal Urban Richmond Non_VCH Vancouver
115 ACCEPTABLE
116 Chart Audit Data of Routine Testing Departments of Medicine ONLY: October 2011 March 3, 2013 Site # Admissions % Offered % Tested % Acceptance among Offered # Positives Only 6% refuse when offered Percent Positivity (%) SPH % 39% 97% MSJ % 47% 85% VGH % 28% 96% Total % 36% 94%
117 COST EFFECTIVE
118 Routine Testing among Acute Care Admissions Acute Care Admissions: Total Counts Since Launch of Strategy at Site* Indicator SPH MSJ VGH UBCH Overall Number of Acute Admissions 20,749 4,452 34,252 2,919 62,372 Number of Patients Tested 3,109 1,181 3, ,085 Proportion of Admissions Tested (%) Number Tested Positive Percent Positivity (%) Monthly testing since launch among those admitted has increased greater than 4 fold compared to the historical monthly average ( ) Diagnoses among those admitted has increased 3.0/1000 in 2012 compared with 2011 *Acute Care Initiative Launched at SPH and MSJ October 1, 2011; VGH October 31, 2011; UBCH April 1, 2012 Public Health Surveillance Unit
119 Routine Testing among Emergency Department Visits Emergency Department Visits: Total Counts Since Launch of Strategy at Site* Indicator SPH MSJ VGH Overall Number of ER Visits 51,334 15,497 43, ,884 Number of Patients Tested 1, ,649 4,050 Proportion of Visits Tested (%) Number Tested Positive Percent Positivity (%) Monthly testing since launch in ER has increased almost 12 fold compared to the historical monthly average ( ) Diagnoses in ER has increased 2.1/1000 in 2012 compared with of new Positives Diagnosed as ER Outpatients *Acute Care Initiative Launched in ER at SPH May, 2012 and VGH July 2012 Public Health Surveillance Unit
120 Acute Care HIV Positive Patients Compared to all other Vancouver HIV Patients Heterosexual MSM Advanced stage of disease Mean CD4 ( 193 cells per mm 3 ; 95% CI ) All differences are significant at p<
121 POPULATION EFFECT
122 Vancouver Family Practice Region Indicato r Number Indicator Name Number of Patients VAN-1 Tested Number Tested VAN-2 Positive Total Counts Since Launch at Site* Since Family Practice Strategy 2-year Historical Baseline (July 1, June 30, 2010) Avg (Monthly) Min Max Avg (Monthly) Min Max Year 2013 Year to Date Counts Year 2012 Significance A+H+Y A+H+ VAN-3 Percent Positivity Note: Data subject to change as billing code and test assignment may change. *Launch date standardized for physicians to be August 2012 because all session types began by August Monthly averages, minimum and maximum values since the Family Practice Strategy launched each session type are determined using the first full month of data for all sites (Aug 2012). Data Source: BCCDC Microbiology Lab Prepared by: Public Health Surveillance Unit: September 19, 2013

123 More HIV testing across the city 44
124 Number of HIV tests in the city of Vancouver Before pilot: 18,280 ( ) per quarter 2012: 28,984 ( )
125
126
127

128
129 Summary A significant proportion of patients with late diagnosis have multiple missed opportunities for earlier diagnosis in the health care system Routine HIV testing in acute care and primary care can turn missed opportunities into opportunities in Vancouver is cost effective highly acceptable to patients can provide an additional opportunity for diagnosis even for those who do seek patient initiated testing is not the only answer Addressing missed opportunities for diagnosis in health care settings is a key component of a comprehensive strategy for early diagnosis of HIV
130 What we learned We could do a better job, even in complex system, but we had to engage with the other parts of the health care system in a different way Dollars are necessary, but not sufficient Data are good: many people will argue with you, it is harder to argue with data HIV is a complex psycho/social entity, which the medical system alone can t address, but it is also a medical entity, which we can
131 Next steps: Pilot Program Plan for sustainability Roll out throughout the province New HIV testing Guidelines for British Columbia Drafted by a working group by request of the Provincial Health Officer Working group: Family physicians with support from labs, public health, STI experts, HIV treating physicians Who, when, how often?

132 Thank you
STOP HIV/AIDS Semi-Annual Monitoring Report
 STOP HIV/AIDS Semi-Annual Monitoring Report S2 (July 1, 2013 December 31, 2013) Ellen Demlow 1, Tim Chu 1, Dr. Reka Gustafson 2, Dr. Jat Sandhu 1 1 Public Health Surveillance Unit 2 Communicable Disease
STOP HIV/AIDS Semi-Annual Monitoring Report S2 (July 1, 2013 December 31, 2013) Ellen Demlow 1, Tim Chu 1, Dr. Reka Gustafson 2, Dr. Jat Sandhu 1 1 Public Health Surveillance Unit 2 Communicable Disease
STOP HIV/AIDS Pilot Project
 STOP HIV/AIDS Pilot Project QUARTERLY INDICATORS REPORT: 1 April through 30 June 2011 () SUBMITTED TO: The BC Ministry of Health Services SUBMITTED BY: Dr. Rolando Barrios, Dr. Mark Gilbert, Dr. Kate Health,
STOP HIV/AIDS Pilot Project QUARTERLY INDICATORS REPORT: 1 April through 30 June 2011 () SUBMITTED TO: The BC Ministry of Health Services SUBMITTED BY: Dr. Rolando Barrios, Dr. Mark Gilbert, Dr. Kate Health,
Implementation of testing (and other interventions along the Continuum of Care)
") Implementation of testing (and other interventions along the Continuum of Care) Jonathan Mermin, MD, MPH National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention U.S. Centers for Disease Control
Implementation of testing (and other interventions along the Continuum of Care) Jonathan Mermin, MD, MPH National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention U.S. Centers for Disease Control
State of Alabama HIV Surveillance 2014 Annual Report
 State of Alabama HIV Surveillance 2014 Annual Report Prepared by: Division of STD Prevention and Control HIV Surveillance Branch Contact Person: Richard P. Rogers, MS, MPH richard.rogers@adph.state.al.us
State of Alabama HIV Surveillance 2014 Annual Report Prepared by: Division of STD Prevention and Control HIV Surveillance Branch Contact Person: Richard P. Rogers, MS, MPH richard.rogers@adph.state.al.us
STOP HIV/AIDS Pilot Project
 STOP HIV/AIDS Pilot Project QUARTERLY INDICATORS REPORT: 1 January through 31 March 2012 () SUBMITTED TO: The BC Ministry of Health SUBMITTED BY: Dr. Mark Gilbert and Dr. Kate Heath On behalf of The STOP
STOP HIV/AIDS Pilot Project QUARTERLY INDICATORS REPORT: 1 January through 31 March 2012 () SUBMITTED TO: The BC Ministry of Health SUBMITTED BY: Dr. Mark Gilbert and Dr. Kate Heath On behalf of The STOP
HIV EPIDEMIOLOGY IN NEW YORK CITY
 HIV EPIDEMIOLOGY IN NEW YORK CITY Ellen Weiss Wiewel, MHS HIV Epidemiology and Field Services Program New York City Department of Health and Mental Hygiene http://www.nyc.gov/html/doh/html/dires/hivepi.shtml
HIV EPIDEMIOLOGY IN NEW YORK CITY Ellen Weiss Wiewel, MHS HIV Epidemiology and Field Services Program New York City Department of Health and Mental Hygiene http://www.nyc.gov/html/doh/html/dires/hivepi.shtml
Government of Canada Federal AIDS Initiative Milestones
 HIV in Canada: Trends and Issues for Advancing Prevention, Care, Treatment and Support Through Knowledge Exchange Michael R Smith, Senior Policy Advisor, Programs and Coordination Division, Centre for
HIV in Canada: Trends and Issues for Advancing Prevention, Care, Treatment and Support Through Knowledge Exchange Michael R Smith, Senior Policy Advisor, Programs and Coordination Division, Centre for
STOP HIV/AIDS Pilot Project
 STOP HIV/AIDS Pilot Project INDICATORS QUARTERLY REPORT: 1 October through 31 December SUBMITTED TO: The BC Ministry of Health Services SUBMITTED BY: Dr. Rolando Barrios, Dr. Mark Gilbert, Dr. Kate Health,
STOP HIV/AIDS Pilot Project INDICATORS QUARTERLY REPORT: 1 October through 31 December SUBMITTED TO: The BC Ministry of Health Services SUBMITTED BY: Dr. Rolando Barrios, Dr. Mark Gilbert, Dr. Kate Health,
Treatment as Prevention
 Treatment as Prevention The Key to an AIDS-Free Generation Julio Montaner MD, DSc(hon), FRCPC, FCCP, FRSC, OBC Director, BC-Centre for Excellence in HIV/AIDS, Providence Health Care Professor of Medicine
Treatment as Prevention The Key to an AIDS-Free Generation Julio Montaner MD, DSc(hon), FRCPC, FCCP, FRSC, OBC Director, BC-Centre for Excellence in HIV/AIDS, Providence Health Care Professor of Medicine
State of Alabama HIV Surveillance 2013 Annual Report Finalized
 State of Alabama HIV Surveillance 2013 Annual Report Finalized Prepared by: Division of STD Prevention and Control HIV Surveillance Branch Contact Person: Allison R. Smith, MPH Allison.Smith@adph.state.al.us
State of Alabama HIV Surveillance 2013 Annual Report Finalized Prepared by: Division of STD Prevention and Control HIV Surveillance Branch Contact Person: Allison R. Smith, MPH Allison.Smith@adph.state.al.us
Comprehensive Epi Update: HIV, AIDS and STI Mark Gilbert, MD
 Comprehensive Epi Update: HIV, AIDS and STI Mark Gilbert, MD February 2014 Objectives Recognize importance of disease syndemics To review current provincial trends: HIV AIDS Infectious syphilis Chlamydia
Comprehensive Epi Update: HIV, AIDS and STI Mark Gilbert, MD February 2014 Objectives Recognize importance of disease syndemics To review current provincial trends: HIV AIDS Infectious syphilis Chlamydia
Public-Private Collaboration to Re-engage Out-of-Care Persons into HIV Care
 Public-Private Collaboration to Re-engage Out-of-Care Persons into HIV Care Chi-Chi Udeagu, MPH Jamie Huang, MPH Lil Eason Leonard Pickett New York City Department of Health and Mental Hygiene Adherence
Public-Private Collaboration to Re-engage Out-of-Care Persons into HIV Care Chi-Chi Udeagu, MPH Jamie Huang, MPH Lil Eason Leonard Pickett New York City Department of Health and Mental Hygiene Adherence
HIV Testing in Acute Care
 HIV Testing in Acute Care Dr. Réka Gustafson Medical Health Officer Director of Communicable Disease Control Vancouver Coastal Health Afshan Nathoo Clinical Coordinator, HIV testing program in acute care
HIV Testing in Acute Care Dr. Réka Gustafson Medical Health Officer Director of Communicable Disease Control Vancouver Coastal Health Afshan Nathoo Clinical Coordinator, HIV testing program in acute care
GLOBAL AIDS RESPONSE PROGRESS REPORTING (GARPR) 2014 COUNTRY PROGRESS REPORT SINGAPORE
 2014 COUNTRY PROGRESS REPORT SINGAPORE") GLOBAL AIDS RESPONSE PROGRESS REPORTING (GARPR) 2014 COUNTRY PROGRESS REPORT SINGAPORE Reporting period: January 2011 June 2013 Submission date: April 2014 I. Status at a glance Singapore s HIV epidemic
GLOBAL AIDS RESPONSE PROGRESS REPORTING (GARPR) 2014 COUNTRY PROGRESS REPORT SINGAPORE Reporting period: January 2011 June 2013 Submission date: April 2014 I. Status at a glance Singapore s HIV epidemic
Financing Integrated Models of Care and Support The Vancouver STOP HIV Experience
 Financing Integrated Models of Care and Support The Vancouver STOP HIV Experience Presenter: Miranda Compton Manager, Regional HIV Program, Vancouver Coastal Health September 15, 2015 STOP HIV Pilot Initiative
Financing Integrated Models of Care and Support The Vancouver STOP HIV Experience Presenter: Miranda Compton Manager, Regional HIV Program, Vancouver Coastal Health September 15, 2015 STOP HIV Pilot Initiative
PHSKC HIV Testing Survey: Knowledge, Attitudes and Practices
 PHSKC HIV Testing Survey: Knowledge, Attitudes and Practices Page One This anonymous survey is intended to collect information about HIV testing attitudes and practices. Results will be used by Public
PHSKC HIV Testing Survey: Knowledge, Attitudes and Practices Page One This anonymous survey is intended to collect information about HIV testing attitudes and practices. Results will be used by Public
U.S. Counties Vulnerability to Rapid Dissemination of HIV/HCV Infections Among People Who Inject Drugs
 U.S. Counties Vulnerability to Rapid Dissemination of HIV/HCV Infections Among People Who Inject Drugs Michelle Van Handel, MPH Health Scientist National Center for HIV/AIDS, Viral Hepatitis, STDs and
U.S. Counties Vulnerability to Rapid Dissemination of HIV/HCV Infections Among People Who Inject Drugs Michelle Van Handel, MPH Health Scientist National Center for HIV/AIDS, Viral Hepatitis, STDs and
EDMA HIV-AIDS TEAM Fact Sheet November 2007
 EDMA HIV-AIDS TEAM Fact Sheet November 2007 1. HIV Facts AIDS epidemic update UNAIDS Epidemic Update, November 2007 (1) 760,000 people to be living with HIV in Western and Central Europe in 2007. 31,000
EDMA HIV-AIDS TEAM Fact Sheet November 2007 1. HIV Facts AIDS epidemic update UNAIDS Epidemic Update, November 2007 (1) 760,000 people to be living with HIV in Western and Central Europe in 2007. 31,000
Saskatchewan HIV Strategy: Social Network Approach
 Saskatchewan HIV Strategy: Social Network Approach Dr. Johnmark Opondo MHO Provincial Leadership Team (PLT) CATIE Forum: New Science, New Directions in HIV and HCV September 18, 2013 Toronto, Canada A
Saskatchewan HIV Strategy: Social Network Approach Dr. Johnmark Opondo MHO Provincial Leadership Team (PLT) CATIE Forum: New Science, New Directions in HIV and HCV September 18, 2013 Toronto, Canada A
UNGASS COUNTRY PROGRESS REPORT SINGAPORE
 UNGASS COUNTRY PROGRESS REPORT SINGAPORE Submission date: 14 March 2008 Reporting period: January 2006 December 2007 I. Overview of the HIV/AIDS epidemic Singapore is categorized as a low-prevalence epidemic.
UNGASS COUNTRY PROGRESS REPORT SINGAPORE Submission date: 14 March 2008 Reporting period: January 2006 December 2007 I. Overview of the HIV/AIDS epidemic Singapore is categorized as a low-prevalence epidemic.
HIV Testing. Susan Tusher, LMSW Program Coordinator The Kansas AIDS Education and Training Center
 HIV Testing Susan Tusher, LMSW Program Coordinator The Kansas AIDS Education and Training Center The Number of Persons in the US Living with HIV Continues to Increase Over 1 Million people are estimated
HIV Testing Susan Tusher, LMSW Program Coordinator The Kansas AIDS Education and Training Center The Number of Persons in the US Living with HIV Continues to Increase Over 1 Million people are estimated
STRENGTHENING THE COORDINATION, DELIVERY AND MONITORING OF HIV AND AIDS SERVICES IN MALAWI THROUGH FAITH-BASED INSTITUTIONS.
 STRENGTHENING THE COORDINATION, DELIVERY AND MONITORING OF HIV AND AIDS SERVICES IN MALAWI THROUGH FAITH-BASED INSTITUTIONS. Acknowledgements This project was fully funded by Center For Disease Control
STRENGTHENING THE COORDINATION, DELIVERY AND MONITORING OF HIV AND AIDS SERVICES IN MALAWI THROUGH FAITH-BASED INSTITUTIONS. Acknowledgements This project was fully funded by Center For Disease Control
HIV/AIDS. Saskatchewan. Saskatchewan Health Population Health Branch
 HIV/AIDS In Saskatchewan 26 Saskatchewan Health Population Health Branch HIV/AIDS in Saskatchewan to December 31, 26 This epidemiological report profiles HIV and AIDS in Saskatchewan from the commencement
HIV/AIDS In Saskatchewan 26 Saskatchewan Health Population Health Branch HIV/AIDS in Saskatchewan to December 31, 26 This epidemiological report profiles HIV and AIDS in Saskatchewan from the commencement
Lessons learnt from other screening programmes : the case of HIV screening
 Lessons learnt from other screening programmes : the case of HIV screening Caroline Semaille, Stéphane Le Vu, Françoise Cazein, Christine Larsen, Josiane Pillonel, Florence Lot HIV/AIDS-STI-Hepatitis C
Lessons learnt from other screening programmes : the case of HIV screening Caroline Semaille, Stéphane Le Vu, Françoise Cazein, Christine Larsen, Josiane Pillonel, Florence Lot HIV/AIDS-STI-Hepatitis C
Miami-Dade County Getting to Zero HIV/AIDS Task Force Implementation Report
 1 Miami-Dade County Getting to Zero HIV/AIDS Task Force Implementation Report Make HIV History! Know the Facts Get Tested Get Treated 2017-2018 7/9/2018 1 2 7/9/2018 2 3 Progress on the Getting to Zero
1 Miami-Dade County Getting to Zero HIV/AIDS Task Force Implementation Report Make HIV History! Know the Facts Get Tested Get Treated 2017-2018 7/9/2018 1 2 7/9/2018 2 3 Progress on the Getting to Zero
Peer-To-Peer Learning Routine Testing Presenters: Fidel Contreras & Dr. James Tesorerio Thursday 5 November 2015
 Peer-To-Peer Learning Routine Testing Presenters: Fidel Contreras & Dr. James Tesorerio Thursday 5 November 2015 2 Routine HIV Testing in NYS James M. Tesoriero, Ph.D. Director, Division of HIV/STD/HCV
Peer-To-Peer Learning Routine Testing Presenters: Fidel Contreras & Dr. James Tesorerio Thursday 5 November 2015 2 Routine HIV Testing in NYS James M. Tesoriero, Ph.D. Director, Division of HIV/STD/HCV
Understanding HIV/AIDS: The current state of the HIV epidemic in British Columbia Mark Gilbert, MD, MHSc, FRCPC
 Understanding HIV/AIDS: The current state of the HIV epidemic in British Columbia Mark Gilbert, MD, MHSc, FRCPC STOP HIV/AIDS Provincial Expansion Knowledge Kick Off January 31, 2013 Learning objectives
Understanding HIV/AIDS: The current state of the HIV epidemic in British Columbia Mark Gilbert, MD, MHSc, FRCPC STOP HIV/AIDS Provincial Expansion Knowledge Kick Off January 31, 2013 Learning objectives
HIV Partner Services in HIV Care Programs
 Welcome HIV Partner Services in HIV Care Programs Building the Care Continuum: Comprehensive Approaches to HIV Care in California Manny Rios HIV Partner Services Specialist CDPH: Office of AIDS Brett AugsJoost
Welcome HIV Partner Services in HIV Care Programs Building the Care Continuum: Comprehensive Approaches to HIV Care in California Manny Rios HIV Partner Services Specialist CDPH: Office of AIDS Brett AugsJoost
As a result of this training, participants will be able to:
 Addressing Prevention with HIV Positive Clients 1 Day Training This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result
Addressing Prevention with HIV Positive Clients 1 Day Training This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result
Enhanced Skills Program. in HIV/AIDS
 BC Centre for Excellence in HIV/AIDS University of British Columbia Enhanced Skills Program in HIV/AIDS 3-month Postgraduate Training Program BC Centre for Excellence in HIV/AIDS UBC Enhanced Skills Program
BC Centre for Excellence in HIV/AIDS University of British Columbia Enhanced Skills Program in HIV/AIDS 3-month Postgraduate Training Program BC Centre for Excellence in HIV/AIDS UBC Enhanced Skills Program
Getting to Zero in California: Integration of HIV Prevention and Surveillance
 Getting to Zero in California: Integration of HIV Prevention and Surveillance Steve Gibson, MSW and Deanna Sykes, PhD CDPH, Office of AIDS November 27, 2017 Learning Objectives Understand reasons for integrated
Getting to Zero in California: Integration of HIV Prevention and Surveillance Steve Gibson, MSW and Deanna Sykes, PhD CDPH, Office of AIDS November 27, 2017 Learning Objectives Understand reasons for integrated
Epidemiology of HIV Among Women in Florida, Reported through 2014
 To protect, promote and improve the health of all people in Florida through integrated state, county, and community efforts. Created: 12/4/14 Revision: 1/27/15 Epidemiology of HIV Among Women in Florida,
To protect, promote and improve the health of all people in Florida through integrated state, county, and community efforts. Created: 12/4/14 Revision: 1/27/15 Epidemiology of HIV Among Women in Florida,
High Impact HIV Prevention Services and Best Practices
 High Impact HIV Prevention Services and Best Practices David W. Purcell, JD, PhD Deputy Director for Behavioral and Social Science Division of HIV/AIDS Prevention Centers for Disease Control and Prevention
High Impact HIV Prevention Services and Best Practices David W. Purcell, JD, PhD Deputy Director for Behavioral and Social Science Division of HIV/AIDS Prevention Centers for Disease Control and Prevention
Lessons Learned: Community Mobilization & the HIV-Positive Sero-Status Disclosure Intervention
 Mobilizing Across Canada to Build Effective Responses to HIV in African, Caribbean, and Black Communities June 8 th, 2016 AOHC 2016 Lessons Learned: Community Mobilization & the HIV-Positive Sero-Status
Mobilizing Across Canada to Build Effective Responses to HIV in African, Caribbean, and Black Communities June 8 th, 2016 AOHC 2016 Lessons Learned: Community Mobilization & the HIV-Positive Sero-Status
In 2015, blacks comprised 12% of the US population, but accounted for 45% of those infected with HIV. Whites were 62% of the population, but
 1 2 3 In 2015, blacks comprised 12% of the US population, but accounted for 45% of those infected with HIV. Whites were 62% of the population, but accounted for 27% of HIV cases. Hispanics/Latinos were
1 2 3 In 2015, blacks comprised 12% of the US population, but accounted for 45% of those infected with HIV. Whites were 62% of the population, but accounted for 27% of HIV cases. Hispanics/Latinos were
Differentiated Care for Antiretroviral Therapy for Key Populations: Case Examples from the LINKAGES Project
 Differentiated Care for Antiretroviral Therapy for Key Populations: Case Examples from the LINKAGES Project NOVEMBER 2017 An estimated 37 million people are living with HIV today. A response to the need
Differentiated Care for Antiretroviral Therapy for Key Populations: Case Examples from the LINKAGES Project NOVEMBER 2017 An estimated 37 million people are living with HIV today. A response to the need
Bruce D. Agins, MD MPH Medical Director, AIDS Institute Adherence 2017; Miami
 1 1 Bruce D. Agins, MD MPH Medical Director, AIDS Institute Adherence 2017; Miami 3 Defining the End of AIDS Reduce new infections to 750 annually by the end of 2020 Three Point Plan 1. Identify all persons
1 1 Bruce D. Agins, MD MPH Medical Director, AIDS Institute Adherence 2017; Miami 3 Defining the End of AIDS Reduce new infections to 750 annually by the end of 2020 Three Point Plan 1. Identify all persons
Florida s HIV Testing Efforts
 Florida s HIV Testing Efforts Mara Michniewicz, MPH Prevention Program Manager Florida Department of Health (DOH) Bureau of Communicable Diseases HIV/AIDS Section Florida Comprehensive Planning Network
Florida s HIV Testing Efforts Mara Michniewicz, MPH Prevention Program Manager Florida Department of Health (DOH) Bureau of Communicable Diseases HIV/AIDS Section Florida Comprehensive Planning Network
Hepatitis C in Massachusetts Epidemiology and Public Health Response
 Massachusetts Department of Public Health Bureau of Infectious Disease and Laboratory Sciences Hepatitis C in Massachusetts Epidemiology and Public Health Response Shauna Onofrey, MPH, Viral Hepatitis
Massachusetts Department of Public Health Bureau of Infectious Disease and Laboratory Sciences Hepatitis C in Massachusetts Epidemiology and Public Health Response Shauna Onofrey, MPH, Viral Hepatitis
MANITOBA HIV REPORT 2015
 MANITOBA HIV REPORT 2015 The Manitoba HIV Program provides information, specialized care, treatment, and support to approximately 1,250 people living with HIV across the province. The Program has two Winnipeg-based
MANITOBA HIV REPORT 2015 The Manitoba HIV Program provides information, specialized care, treatment, and support to approximately 1,250 people living with HIV across the province. The Program has two Winnipeg-based
Practice Steps for Implementation of Guidelines Recommendations The guideline recommendations are shown schematically -
 ASK SCREEN Test for HIV and STI Practice Steps for Implementation of Guidelines Recommendations The guideline recommendations are shown schematically - Routinely obtain a thorough sexual history from all
ASK SCREEN Test for HIV and STI Practice Steps for Implementation of Guidelines Recommendations The guideline recommendations are shown schematically - Routinely obtain a thorough sexual history from all
NYC s PrEP Network. Julie Myers, MD, MPH New York City Department of Health and Mental Hygiene
 NYC s PrEP Network Julie Myers, MD, MPH New York City Department of Health and Mental Hygiene % persons at epidemiologic risk Continuum of HIV Prevention & Care (Theoretical) 120 100 80 60 40 20 0 Undiagnosed
NYC s PrEP Network Julie Myers, MD, MPH New York City Department of Health and Mental Hygiene % persons at epidemiologic risk Continuum of HIV Prevention & Care (Theoretical) 120 100 80 60 40 20 0 Undiagnosed
2016 NYS HIV Quality of Care Review
 2016 NYS HIV Quality of Care Review A new way forward in four parts Bruce Agins, MD, MPH Medical Director NYSDOH AIDS Institute December 15, 2016 Ending the Epidemic: update! A 3-Point plan announced by
2016 NYS HIV Quality of Care Review A new way forward in four parts Bruce Agins, MD, MPH Medical Director NYSDOH AIDS Institute December 15, 2016 Ending the Epidemic: update! A 3-Point plan announced by
Manitoba Health Statistical Update on HIV/AIDS
 Manitoba Health Statistical Update on HIV/AIDS 1985-2002 Communicable Disease Control Unit Public Health MANITOBA HEALTH STATISTICAL UPDATE ON HIV/AIDS 1985 TO December 2002 HIV January 1, 1985 to December
Manitoba Health Statistical Update on HIV/AIDS 1985-2002 Communicable Disease Control Unit Public Health MANITOBA HEALTH STATISTICAL UPDATE ON HIV/AIDS 1985 TO December 2002 HIV January 1, 1985 to December
Annual Statistical Update on HIV and AIDS 2013
 Annual Statistical Update on HIV and AIDS 2013 Data reported to December 31, 2013 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Healthy
Annual Statistical Update on HIV and AIDS 2013 Data reported to December 31, 2013 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Healthy
To provide you with the basic concepts of HIV prevention using HIV rapid tests combined with counselling.
 Module 2 Integration of HIV Rapid Testing in HIV Prevention and Treatment Programs Purpose Pre-requisite Modules Learning Objectives To provide you with the basic concepts of HIV prevention using HIV rapid
Module 2 Integration of HIV Rapid Testing in HIV Prevention and Treatment Programs Purpose Pre-requisite Modules Learning Objectives To provide you with the basic concepts of HIV prevention using HIV rapid
Fulton County Board of Health Strategy to End the HIV Epidemic in Fulton County
 Fulton County Board of Health Strategy to End the HIV Epidemic in Fulton County April 25, 2018 Derick B. Wilson, MHA Administrator FCBOH HIV Strategy Overview Increase Testing and Supplies availability
Fulton County Board of Health Strategy to End the HIV Epidemic in Fulton County April 25, 2018 Derick B. Wilson, MHA Administrator FCBOH HIV Strategy Overview Increase Testing and Supplies availability
State of Alabama HIV Surveillance 2012 Annual Report Finalized
 State of Alabama HIV Surveillance 2012 Annual Report Finalized Prepared by: Division of HIV/AIDS Prevention and Control HIV Surveillance Branch Contact Person: Allison R. Smith, MPH Allison.Smith@adph.state.al.us
State of Alabama HIV Surveillance 2012 Annual Report Finalized Prepared by: Division of HIV/AIDS Prevention and Control HIV Surveillance Branch Contact Person: Allison R. Smith, MPH Allison.Smith@adph.state.al.us
Note: Staff who work in case management programs should attend the AIDS Institute training, "Addressing Prevention in HIV Case Management.
 Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
2020 Vision: making England s HIV prevention response the best in the world
 DISCUSSION PAPER 2020 Vision: making England s HIV prevention response the best in the world Introduction Effective HIV prevention makes good public health and economic sense. HIV remains one of the fastest-growing
DISCUSSION PAPER 2020 Vision: making England s HIV prevention response the best in the world Introduction Effective HIV prevention makes good public health and economic sense. HIV remains one of the fastest-growing
As a result of this training, participants will be able to:
 Addressing Sexual Risk with Drug Users and their Partners 1 Day Training This one-day training will build participant knowledge and skills in offering sexual harm reduction options to substance users.
Addressing Sexual Risk with Drug Users and their Partners 1 Day Training This one-day training will build participant knowledge and skills in offering sexual harm reduction options to substance users.
HIV Screening in Behavioral Health Settings: The Need is Clear
 HIV Screening in Behavioral Health Settings: The Need is Clear Alyssa A. Bittenbender, MPH Program Director, Arizona AIDS Education and Training Center University of Arizona College of Medicine MISSION
HIV Screening in Behavioral Health Settings: The Need is Clear Alyssa A. Bittenbender, MPH Program Director, Arizona AIDS Education and Training Center University of Arizona College of Medicine MISSION
PS : Comprehensive HIV Prevention Programs for Health Departments
 PS12-1201: Comprehensive HIV Prevention Programs for Health Departments Program Overview Erica K. Dunbar, MPH Program Leader, Health Department Initiatives National Center for HIV/AIDS, Viral Hepatitis,
PS12-1201: Comprehensive HIV Prevention Programs for Health Departments Program Overview Erica K. Dunbar, MPH Program Leader, Health Department Initiatives National Center for HIV/AIDS, Viral Hepatitis,
Routine HIV Testing in Healthcare Settings: Reimbursement & Sustainability Updated October, 2017
 Routine HIV Testing in Healthcare Settings: Reimbursement & Sustainability Updated October, 2017 Overview Importance of routine testing Current recommendations for testing Reimbursement for HIV counseling
Routine HIV Testing in Healthcare Settings: Reimbursement & Sustainability Updated October, 2017 Overview Importance of routine testing Current recommendations for testing Reimbursement for HIV counseling
High Impact Prevention: Science, Practice, and the Future of HIV
 High Impact Prevention: Science, Practice, and the Future of HIV Jonathan Mermin, MD, MPH National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Centers for Disease Control and Prevention
High Impact Prevention: Science, Practice, and the Future of HIV Jonathan Mermin, MD, MPH National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Centers for Disease Control and Prevention
All four components must be present, but Part A funds to be used for HIV testing only as necessary to supplement, not supplant, existing funding.
 EARLY INTERVENTION SERVICES I. DEFINITION OF SERVICE Support of Early Intervention Services (EIS) that include identification of individuals at points of entry and access to services and provision of:
EARLY INTERVENTION SERVICES I. DEFINITION OF SERVICE Support of Early Intervention Services (EIS) that include identification of individuals at points of entry and access to services and provision of:
Annual Statistical Update: HIV and AIDS
 Annual Statistical Update: HIV and AIDS 2015 Data reported to December 31, 2015 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Seniors
Annual Statistical Update: HIV and AIDS 2015 Data reported to December 31, 2015 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Seniors
5/2/2016. Dr Brooks has no relevant financial affiliations to disclose. (Update 04/15/16) Learning Objectives
 Learning Objectives") Persistent Challenge of HIV Transmission Control in Injection Drug Use: The Indiana Outbreak John T. Brooks, MD Senior Medical Advisor, Division of HIV/AIDS Prevention National Center for HIV/AIDS, Viral
Persistent Challenge of HIV Transmission Control in Injection Drug Use: The Indiana Outbreak John T. Brooks, MD Senior Medical Advisor, Division of HIV/AIDS Prevention National Center for HIV/AIDS, Viral
Infectious Diseases New York City Department of Health and Mental Hygiene, Division of Disease Control (Bureau of HIV/AIDS Prevention and Control)
") Infectious Diseases New York City Department of Health and Mental Hygiene, Division of Disease Control (Bureau of HIV/AIDS Prevention and Control) Queens, New York Assignment Description The host site
Infectious Diseases New York City Department of Health and Mental Hygiene, Division of Disease Control (Bureau of HIV/AIDS Prevention and Control) Queens, New York Assignment Description The host site
Estimate of the Number of Persons Living with HIV in Massachusetts
 Estimate of the Number of Persons Living with HIV in Massachusetts Christian Hague, MPH Supervisor, HIV Surveillance Massachusetts Department of Public Health 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV
Estimate of the Number of Persons Living with HIV in Massachusetts Christian Hague, MPH Supervisor, HIV Surveillance Massachusetts Department of Public Health 2016 NATIONAL RYAN WHITE CONFERENCE ON HIV
Quality improvement of the viral load programme in Mopani District, Limpopo Province
 Quality improvement of the viral load programme in Mopani District, Limpopo Province Maidi M Kekana, DPH, RN Susannah Cole-Hamilton MW Mongwe 2 Jean Railton, MB ChB, FCFP, MMed, DMH, Dip HIV Med R P H
Quality improvement of the viral load programme in Mopani District, Limpopo Province Maidi M Kekana, DPH, RN Susannah Cole-Hamilton MW Mongwe 2 Jean Railton, MB ChB, FCFP, MMed, DMH, Dip HIV Med R P H
HIV/AIDS and ART Registry of the Philippines (HARP)
") HIV/AIDS and ART Registry of the Philippines (HARP) Number of Cases Department of Health Epidemiology Bureau FEBRUARY 215 28 21 212 214 215 Number of Newly Diagnosed with HIV per day: 1 4 9 17 2 NEWLY
HIV/AIDS and ART Registry of the Philippines (HARP) Number of Cases Department of Health Epidemiology Bureau FEBRUARY 215 28 21 212 214 215 Number of Newly Diagnosed with HIV per day: 1 4 9 17 2 NEWLY
HIV EPIDEMIC UPDATE: FACTS & FIGURES 2012
 HIV EPIDEMIC UPDATE: FACTS & FIGURES 2012 Number of Cases Note: In this surveillance report, HIV cases include persons reported with HIV infection (non-aids), advanced HIV (non-aids) and AIDS within a
HIV EPIDEMIC UPDATE: FACTS & FIGURES 2012 Number of Cases Note: In this surveillance report, HIV cases include persons reported with HIV infection (non-aids), advanced HIV (non-aids) and AIDS within a
HIV Monitoring and Evaluation Quarterly Report: Technical Report. British Columbia Centre for Excellence in HIV/AIDS
 HIV Monitoring and Evaluation Quarterly Report: Technical Report British Columbia Centre for Excellence in HIV/AIDS V4.0, 25 November 2013 Technical Report: HIV Monitoring and Evaluation Quarterly Report
HIV Monitoring and Evaluation Quarterly Report: Technical Report British Columbia Centre for Excellence in HIV/AIDS V4.0, 25 November 2013 Technical Report: HIV Monitoring and Evaluation Quarterly Report
New Brunswick Report on Sexually Transmitted and Blood Borne Infections, 2016
 New Brunswick Report on Sexually Transmitted and Blood Borne Infections, 6 Table of Contents. Introduction.... Methodology... 3. Data Limitations.... Definitions used... 3 5. Overview of STBBI epidemiology
New Brunswick Report on Sexually Transmitted and Blood Borne Infections, 6 Table of Contents. Introduction.... Methodology... 3. Data Limitations.... Definitions used... 3 5. Overview of STBBI epidemiology
When PrEP fails. Laura Waters MD FRCP Mortimer Market Centre London
 When PrEP fails Laura Waters MD FRCP Mortimer Market Centre London www.aidsunited.org PrEP works If people at risk take it If it s taken in the right way If it s available Commissioned/licensed Affordable
When PrEP fails Laura Waters MD FRCP Mortimer Market Centre London www.aidsunited.org PrEP works If people at risk take it If it s taken in the right way If it s available Commissioned/licensed Affordable
Miami-Dade County Getting to Zero HIV/AIDS Report
 1 Miami-Dade County Getting to Zero HIV/AIDS Report Make HIV History! Know the Facts Get Tested Get Treated Implementation Report 2017-2018 2/12/2018 1 2 2/12/2018 2 3 Progress on the Getting to Zero :
1 Miami-Dade County Getting to Zero HIV/AIDS Report Make HIV History! Know the Facts Get Tested Get Treated Implementation Report 2017-2018 2/12/2018 1 2 2/12/2018 2 3 Progress on the Getting to Zero :
Enhanced Health Promotion and Screening (EHPS) Program Implementation at Clinical Settings and Corrections in Pennsylvania
 Program Implementation at Clinical Settings and Corrections in Pennsylvania") Enhanced Health Promotion and Screening (EHPS) Program Implementation at Clinical Settings and Corrections in Pennsylvania PENNSYLVANIA DEPARTMENT OF HEALTH Bureau of Communicable Diseases, Division of
Enhanced Health Promotion and Screening (EHPS) Program Implementation at Clinical Settings and Corrections in Pennsylvania PENNSYLVANIA DEPARTMENT OF HEALTH Bureau of Communicable Diseases, Division of
NYS PrEP Programming. Lyn Stevens, NP, MS, ACRN Office of the Medical Director, AIDS Institute PrEP Monitoring in NYC and NYS February 19, 2016
 NYS PrEP Programming March 21, 2016 Lyn Stevens, NP, MS, ACRN Office of the Medical Director, AIDS Institute PrEP Monitoring in NYC and NYS February 19, 2016 March 21, 2016 2 New York State Priorities
NYS PrEP Programming March 21, 2016 Lyn Stevens, NP, MS, ACRN Office of the Medical Director, AIDS Institute PrEP Monitoring in NYC and NYS February 19, 2016 March 21, 2016 2 New York State Priorities
Missouri Statewide Integrated HIV Prevention and Care Plan, including the Statewide Coordinated Statement of Need, CY
 Missouri Statewide Integrated HIV Prevention and Care Plan, including the Statewide Coordinated Statement of Need, CY 2017-2021 September 20, 2016 Developed through the collaborative efforts of the following
Missouri Statewide Integrated HIV Prevention and Care Plan, including the Statewide Coordinated Statement of Need, CY 2017-2021 September 20, 2016 Developed through the collaborative efforts of the following
Trends in HIV Incidence and Prevalence in the United States
 Trends in HIV Incidence and Prevalence in the United States Irene Hall, PhD, FACE 7th International Workshop on HIV Transmission Washington, DC, July 20, 2012 National Center for HIV/AIDS, Viral Hepatitis,
Trends in HIV Incidence and Prevalence in the United States Irene Hall, PhD, FACE 7th International Workshop on HIV Transmission Washington, DC, July 20, 2012 National Center for HIV/AIDS, Viral Hepatitis,
Utilizing CQI to Improve the Health of Supportive Housing Residents The North American Housing and HIV/AIDS Research Summit VII September 25-27, 2013
 Utilizing CQI to Improve the Health of Supportive Housing Residents The North American Housing and HIV/AIDS Research Summit VII September 25-27, 2013 Montréal, Canada MISSION To provide 100% access to
Utilizing CQI to Improve the Health of Supportive Housing Residents The North American Housing and HIV/AIDS Research Summit VII September 25-27, 2013 Montréal, Canada MISSION To provide 100% access to
HIV, HBV and HCV testing policy experiences and lessons learned.
 HIV, HBV and HCV testing policy experiences and lessons learned. Contents HIV and viral hepatitis: distinct epidemics at different stages of evolution Epidemiology: transmission, prevalence, incidence
HIV, HBV and HCV testing policy experiences and lessons learned. Contents HIV and viral hepatitis: distinct epidemics at different stages of evolution Epidemiology: transmission, prevalence, incidence
Improving outcomes The UK s achievements in managing and preventing the HIV epidemic and how we should approach public health priorities
 Improving outcomes The UK s achievements in managing and preventing the HIV epidemic and how we should approach public health priorities Professor Kevin Fenton Senior Advisor, Public Health England Director,
Improving outcomes The UK s achievements in managing and preventing the HIV epidemic and how we should approach public health priorities Professor Kevin Fenton Senior Advisor, Public Health England Director,
Manitoba Health Statistical Update on HIV/AIDS
 Manitoba Health Statistical Update on HIV/AIDS 1985 - Dec 2001 Communicable Disease Control Unit Public Health Branch MANITOBA HEALTH STATISTICAL UPDATE ON HIV/AIDS 1985 TO DECEMBER 2001 HIV January 1,
Manitoba Health Statistical Update on HIV/AIDS 1985 - Dec 2001 Communicable Disease Control Unit Public Health Branch MANITOBA HEALTH STATISTICAL UPDATE ON HIV/AIDS 1985 TO DECEMBER 2001 HIV January 1,
Fertility Desires/Management of Serodiscordant HIV + Couples
 Fertility Desires/Management of Serodiscordant HIV + Couples William R. Short, MD, MPH Assistant Professor of Medicine Division Of Infectious Diseases Jefferson Medical College of Thomas Jefferson University
Fertility Desires/Management of Serodiscordant HIV + Couples William R. Short, MD, MPH Assistant Professor of Medicine Division Of Infectious Diseases Jefferson Medical College of Thomas Jefferson University
Monitoring of HIV positive mothers and HIV exposed infants in context of Option B+ implementation
 Monitoring of HIV positive mothers and HIV exposed infants in context of Option B+ implementation Kenya Outline of the presentation Background: Kenya in Context PMTCT Program progress 2012-2015 Option
Monitoring of HIV positive mothers and HIV exposed infants in context of Option B+ implementation Kenya Outline of the presentation Background: Kenya in Context PMTCT Program progress 2012-2015 Option
HIV Epidemiology March 7, Stefanie Rhodes Inova Juniper Program
 HIV Epidemiology March 7, 2019 Stefanie Rhodes Inova Juniper Program Stefanie.Rhodes@inova.org Human Immunodeficiency Virus Virus that attacks and weakens immune system Can be treated, but not cured Transmitted
HIV Epidemiology March 7, 2019 Stefanie Rhodes Inova Juniper Program Stefanie.Rhodes@inova.org Human Immunodeficiency Virus Virus that attacks and weakens immune system Can be treated, but not cured Transmitted
Program Collaboration and Service Integration
 Program Collaboration and Service Integration One Size Does Not Fit All Amanuel Rosario, MD Medical Director, TB Control District of Columbia Department of Health Marcelo Fernandez-Viña, MPH Adult Viral
Program Collaboration and Service Integration One Size Does Not Fit All Amanuel Rosario, MD Medical Director, TB Control District of Columbia Department of Health Marcelo Fernandez-Viña, MPH Adult Viral
Needs Assessment of People Living with HIV in the Boston EMA. Needs Resources and Allocations Committee March 10 th, 2016
 Needs Assessment of People Living with HIV in the Boston EMA Needs Resources and Allocations Committee March 10 th, 2016 Presentation Overview 1. What is a Needs Assessment? 2. The Numbers o Epidemiological
Needs Assessment of People Living with HIV in the Boston EMA Needs Resources and Allocations Committee March 10 th, 2016 Presentation Overview 1. What is a Needs Assessment? 2. The Numbers o Epidemiological
Financial Incentives, Linkage to Care and Viral Suppression HPTN 065 (TLC-Plus) Study. Wafaa El-Sadr ICAP at Columbia University New York, NY
 Study. Wafaa El-Sadr ICAP at Columbia University New York, NY") Financial Incentives, Linkage to Care and Viral Suppression HPTN 065 (TLC-Plus) Study Wafaa El-Sadr ICAP at Columbia University New York, NY Outline of Presentation Background and study rationale Methods
Financial Incentives, Linkage to Care and Viral Suppression HPTN 065 (TLC-Plus) Study Wafaa El-Sadr ICAP at Columbia University New York, NY Outline of Presentation Background and study rationale Methods
Available In person Courses
 Course Catalogue for HIV Education and Training NY www.hivtrainingny.org The NYSDOH AIDS Institute s HIV, STI and Viral Hepatitis Training Programs offer trainings on HIV/AIDS, sexually transmitted infection
Course Catalogue for HIV Education and Training NY www.hivtrainingny.org The NYSDOH AIDS Institute s HIV, STI and Viral Hepatitis Training Programs offer trainings on HIV/AIDS, sexually transmitted infection
The Undetectables Viral Load Suppression (VLS) Project
 Project") The Undetectables Viral Load Suppression (VLS) Project AIDS Institute, Clinical Advisory Committee September 8, 2016 Vaty Poitevien, Chief Medical Officer Housing Works, Inc. www.housingworks.org About
The Undetectables Viral Load Suppression (VLS) Project AIDS Institute, Clinical Advisory Committee September 8, 2016 Vaty Poitevien, Chief Medical Officer Housing Works, Inc. www.housingworks.org About
South Africa Country Report FY14
 USAID ASSIST Project South Africa Country Report FY14 Cooperative Agreement Number: AID-OAA-A-12-00101 Performance Period: October 1, 2013 September 30, 2014 DECEMBER 2014 This annual country report was
USAID ASSIST Project South Africa Country Report FY14 Cooperative Agreement Number: AID-OAA-A-12-00101 Performance Period: October 1, 2013 September 30, 2014 DECEMBER 2014 This annual country report was
Here are some of the steps (greatly simplified) and gaps that can occur in the HIV Treatment Cascade:
 and gaps that can occur in the HIV Treatment Cascade:") CATIE-News CATIE s bite-sized HIV and hepatitis C news bulletins. Alberta Reducing deaths by strengthening the HIV Treatment Cascade 20 May 2014 In Canada and other high-income countries, deaths from AIDS-related
CATIE-News CATIE s bite-sized HIV and hepatitis C news bulletins. Alberta Reducing deaths by strengthening the HIV Treatment Cascade 20 May 2014 In Canada and other high-income countries, deaths from AIDS-related
Ending the Epidemic in New York State
 Ending the Epidemic in New York State HIV Quality of Care Clinical and Consumer Advisory Committee Joint Meeting September 8, 2015 September 10, 2015 Defining the End of AIDS Goal Reduce from 3,000 to
Ending the Epidemic in New York State HIV Quality of Care Clinical and Consumer Advisory Committee Joint Meeting September 8, 2015 September 10, 2015 Defining the End of AIDS Goal Reduce from 3,000 to
HIV in British Columbia: Annual Surveillance Report
 HIV in British Columbia: Annual Surveillance Report 2015 2015 Contact Information BC Centre for Disease Control Clinical Prevention Services 655 West 12th Avenue Vancouver BC V5Z 4R4 Phone: 604-707-5621
HIV in British Columbia: Annual Surveillance Report 2015 2015 Contact Information BC Centre for Disease Control Clinical Prevention Services 655 West 12th Avenue Vancouver BC V5Z 4R4 Phone: 604-707-5621
Improving Chicago's HIV Care Cascade:
 Improving Chicago's HIV Care Cascade: Year 1: Scaling up routine HIV testing Year 2: Exploring new uses for HIV surveillance data Chicago Site Project Summary November 19 th, 2012 Ron Lubelchek, MD Associate
Improving Chicago's HIV Care Cascade: Year 1: Scaling up routine HIV testing Year 2: Exploring new uses for HIV surveillance data Chicago Site Project Summary November 19 th, 2012 Ron Lubelchek, MD Associate
Missouri St. Louis TGA 2016 HIV Epidemiological Profile
 Missouri St. Louis TGA 2016 HIV Epidemiological Profile St. Louis TGA Part A Planning Council Prepared by the City of St. Louis Department of Health Center for Health Information, Research, and Planning
Missouri St. Louis TGA 2016 HIV Epidemiological Profile St. Louis TGA Part A Planning Council Prepared by the City of St. Louis Department of Health Center for Health Information, Research, and Planning
The profile of people living with HIV
 HIV AND AIDS IN SASKATCHEWAN, 212 ANNUAL REPORT RELEASE DATE: NOVEMBER 3, 213 Population Health Branch Purpose This report examines HIV and AIDS surveillance data reported in Saskatchewan to provide an
HIV AND AIDS IN SASKATCHEWAN, 212 ANNUAL REPORT RELEASE DATE: NOVEMBER 3, 213 Population Health Branch Purpose This report examines HIV and AIDS surveillance data reported in Saskatchewan to provide an
Focusing Our Efforts Ontario s Proposed HIV/AIDS Strategy to 2025
 Focusing Our Efforts Ontario s Proposed HIV/AIDS Strategy to 2025 Frank McGee, AIDS & Hepatitis C Programs Ontario Harm Reduction Conference 2015 October 26, 2015 Our successes! We are doing well in Ontario
Focusing Our Efforts Ontario s Proposed HIV/AIDS Strategy to 2025 Frank McGee, AIDS & Hepatitis C Programs Ontario Harm Reduction Conference 2015 October 26, 2015 Our successes! We are doing well in Ontario
Annual Statistical Update: HIV and AIDS
 Annual Statistical Update: HIV and AIDS 2014 Data reported to December 31, 2014 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Healthy
Annual Statistical Update: HIV and AIDS 2014 Data reported to December 31, 2014 Epidemiology & Surveillance Public Health Branch Public Health and Primary Health Care Division Manitoba Health, Healthy
Realizing Universal HIV Testing & LTC:
 Realizing Universal HIV Testing & LTC: Lessons from the Bronx September 2013 Donna Futterman, MD Professor of Clinical Pediatrics, Einstein College of Medicine Director, Adolescent AIDS Program, Children
Realizing Universal HIV Testing & LTC: Lessons from the Bronx September 2013 Donna Futterman, MD Professor of Clinical Pediatrics, Einstein College of Medicine Director, Adolescent AIDS Program, Children
HIV POSITIVE YOUTH: LINKAGE & RETENTION IN CARE
 HIV POSITIVE YOUTH: LINKAGE & RETENTION IN CARE Site C Youth clinic HIV care pathway DAY 1 Test HIV + PIMA point of care CD4 count in in 3-5 days initiation + in session 3 session 4 1 month Youth Club
HIV POSITIVE YOUTH: LINKAGE & RETENTION IN CARE Site C Youth clinic HIV care pathway DAY 1 Test HIV + PIMA point of care CD4 count in in 3-5 days initiation + in session 3 session 4 1 month Youth Club
The HIV testing process
 FACTSHEET The HIV testing process Summary There are a few steps that a person will take in the HIV testing process. To access an HIV test, people can request a test or may be offered a test. There are
FACTSHEET The HIV testing process Summary There are a few steps that a person will take in the HIV testing process. To access an HIV test, people can request a test or may be offered a test. There are
HIV Testing and HIV Prevention
 HIV Testing and HIV Prevention Five Things to Know: Essentials of HIV Prevention Webinar 2 Primary Care Development Corporation Five Things to Know: Essentials of HIV Prevention Social Marketing and HIV
HIV Testing and HIV Prevention Five Things to Know: Essentials of HIV Prevention Webinar 2 Primary Care Development Corporation Five Things to Know: Essentials of HIV Prevention Social Marketing and HIV
Chiang Mai University/Johns Hopkins University HIV/AIDS Research on VCT
 Chiang Mai University/Johns Hopkins University HIV/AIDS Research on VCT David Celentano, Professor of Epidemiology May 26, 2005 Scope of the CMU/JHU Collaborative HIV/AIDS Research Agenda HIV/AIDS research
Chiang Mai University/Johns Hopkins University HIV/AIDS Research on VCT David Celentano, Professor of Epidemiology May 26, 2005 Scope of the CMU/JHU Collaborative HIV/AIDS Research Agenda HIV/AIDS research
Part 1: Introduction & Overview
 Part 1: Introduction & Overview We envision a collaborative, participative partnership around IDU that: Provides all relevant and interested stakeholders with a voice and role. Promotes awareness of the
Part 1: Introduction & Overview We envision a collaborative, participative partnership around IDU that: Provides all relevant and interested stakeholders with a voice and role. Promotes awareness of the
EARLY INTERVENTION SERVICES I. DEFINITION OF SERVICE
 EARLY INTERVENTION SERVICES I. DEFINITION OF SERVICE Support of Early Intervention Services () that include identification of individuals at points of entry and access to services and provision of: 1.
EARLY INTERVENTION SERVICES I. DEFINITION OF SERVICE Support of Early Intervention Services () that include identification of individuals at points of entry and access to services and provision of: 1.