Evaluation Report of the Community Development Block Grant (CDBG)-Funded HIV/AIDS Prevention Initiative
|
|
|
- Eustacia Kelly
- 6 years ago
- Views:
Transcription
 Peggy Shaffer-King, M.A. (Kent State University) William J.")
 College of Public Health Kent State University 330.672.")
1 Evaluation Report of the Community Development Block Grant (CDBG)-Funded HIV/AIDS Prevention Initiative Sonia Alemagno, Ph. D. (Kent State University) Peggy Shaffer-King, M.A. (Kent State University) William J. Miller, Ph.D. (Southeast Missouri State University) College of Public Health Kent State University October, P age
2 Evaluation of CDBG HIV Prevention Programs Annual Report July 2009 June 2010 Table of Contents Executive Summary.3 Introduction.4 General Report.5 Site.6 Race.7 Sexual Orientation.8 Gender.9 Education 10 Age..11 Income..12 Zip Codes.13 Knowledge Scale.15 HIV Risk Scale.16 HIV Risk by Knowledge.18 Impact of Programming on Knowledge and Risk.19 Results.19 Results by Site.20 Recommendations and Global Findings.20 Aggregate Pretest Report 22 Individual Site Reports AGAPE.26 AIDS Taskforce.77 Free Clinic.95 NEON.134 Proyecto Luz 141 Appendix I Client Survey Appendix II Training Survey 2 P age
3 EXECUTIVE SUMMARY In 2009, the Cleveland Department of Public Health (CDPH) continued to offer an intensive evaluation of the HIV prevention programs funded through Community Development Block Grant (CDBG) dollars that CDPH administers. In the grant year, over 2,500 clients were reached with CDBG-funded HIV programming, and 1,203 of these completed the data collection instrument. The discrepancy between the number of clients served and the number of surveys collected is due to evaluation plans for some agencies and objectives not requiring data collection for some funded activities. Clients were part of the program at one of four agencies located throughout the city and each serving its own unique target populations. Given the variability in the type and reach of prevention programming conducted by the various sites, we did expect, as the data reflect, that some sites would reach many more clients than others. Since the contribution in terms of client numbers across sites is highly variable, any program-wide results should be interpreted with caution. However, aggregate data represents the collective efforts of the CDBG HIV prevention program to serve a target population and can be used for general planning purposes. As such, this report presents both aggregate and agency-specific reports. With regards to the general demographics of the clients served, we find that a majority are African- American (77%), heterosexual (83%), female (62%), with a high school diploma, GED, or less (71%), under 24 years old (70%), and with relatively low income (49% of households falling within 0-30% of Average Median Income for a household of the same size). Beyond demographics, clients are tested on their HIV knowledge and asked about potential risk behaviors. From these questions, a table is created to show the number of clients in each categorization, ranging from those individuals deemed the least at risk (High Knowledge, Lower Risk) to those at the highest risk (Low Knowledge, High Risk). In 2009, 5.9% of respondents fell in the least risk categorization while 6.3% of respondents were at the highest end. There were over 48% of respondents considered High Knowledge, Moderate Risk and just under a quarter were High Knowledge, High Risk. Since clients are often given a pre-test before programming and then administered a post-test, it is possible to measure the impact of the programming on knowledge and risk behavior. In regards to knowledge scores of individuals that were successfully tracked pre and post, the average pre-survey knowledge score was 7.53, while the average post-survey knowledge score was 7.68, indicating that most of these respondents were considered high knowledge prior to the programming and as an effect gained little. When looking at risk categorizations, the pre-test results had 10.2% classified as lower risk, 51.3% classified as moderate risk, and 38.6% classified as high risk. After programming, the number of lower risk respondents fell to 9.0%, the number of high risk individuals dropped to 37.0%, and the number of moderate risk respondents rose to 54.0%. 3 P age
4 INTRODUCTION The City of Cleveland Department of Public Health is authorized to administer Community Development Block Grant (CDBG) funds on the behalf of the United States Department of Housing and Urban Development (HUD), in conjunction with the City of Cleveland Department of Community Development. The purpose of the Community Development Block Grant funds allocated toward HIV/AIDS prevention is to directly impact the rate of transmission of HIV among Cleveland residents through providing education and intervention strategies to those at greatest risk. Providing significant resources specifically to those programs that target populations within the City of Cleveland ensures that the City s diverse populations are reached with messages that most effectively address their particular concerns. Consequently, programs seeking funding were required to target City of Cleveland residents in at least one of the following risk groups: High-Risk Heterosexual Women of Color Injection Drug Users Men who have Sex with Men HIV Prevention for Positives Youth-General Youth- LGBTQ Seniors General Public Information The focus of the CDBG HIV prevention funds is on prevention strategies that utilize innovative methods to effectively reach target populations. Programs requesting funding were also required to demonstrate their effectiveness in successfully meeting the complex needs of the target populations. Additionally, given the increase in new HIV infections, the fact that the epidemic has changed due to new therapies, scientific advances, new community attitudes, and beliefs, agencies were encouraged to create interventions that meet these challenging times and were required to show: An indication of evidence-based effectiveness, A commitment to innovation, and A willingness to create the types of programs and services that have made Cleveland a leader in the HIV prevention effort both nationally and worldwide. To that end awards were only granted to agencies: To support new programs which pilot innovative methods of HIV/AIDS prevention; To support or expand existing programs that have a demonstrated record of success; or To extend projects funded through previous CDBG grants that have successfully met their evaluation objectives. 4 P age
5 In 2009, the Cleveland Department of Public Health (CDPH) continued to offer an intensive evaluation of the HIV prevention programs funded through Community Development Block Grant (CDBG) dollars that CDPH administers. In order to maximize the impact and value of the evaluation, it was designed to span two years and to incorporate extensive technical assistance for the community agencies providing the HIV prevention programming and collecting the evaluation data. The Institute for Health and Social Policy (IHSP) at The University of Akron was contracted to design and conduct the evaluation, in partnership with CDPH and AFC, and provide technical assistance. The first year of the evaluation, July 2007-June 2008, focused heavily on 1) establishing measurable objectives for each goal of the prevention programs, and 2) designing and implementing a standard data collection instrument to be used across all funded programs focused on documenting the HIV knowledge, HIV risk factors, and demographic information for all clients served by the CDBG-funded HIV prevention programs. It should be noted that several of the funded programs engaged in a variety of prevention activities so the evaluators worked to help specify prevention goals for each of these activities. Year one results are available online at: AIDS/Publications.html. Ultimately, results from the year one analysis demonstrated that many clients served under the program do not report the risk factors we attempt to examine. This may be due to true lower risk or reluctance to report. In terms of knowledge, the results did indicate that the majority of clients served had high HIV knowledge of the items included in the knowledge scale. This was thought to potentially demonstrate the historic focus of the overall program on health education and the relative success within these programs to address knowledge gaps. When moving to year two, a finalized instrument was utilized by all agencies the entire year. Consequently, all data is now based on the same measures and will allow for a fuller and more valid dataset. Second, each of the eight agencies had to have objectives (formulated during meetings between the agency staff, CDPH, and evaluators) that involved follow-up data being collected to actually allow for the measuring of the effects of the intervention. The web-based reporting system continued to be used and data was collected by each agency and then picked up monthly by IHSP staff to be scanned. Regular interaction occurred between the agencies, evaluators, City of Cleveland, and AFC. The agencies also performed well during an unexpected transition as the evaluators (Dr. Sonia Alemagno and Peggy Shaffer-King) moved from IHSP to the Institution for the Study and Prevention of Violence at Kent State University. In year three, agencies were familiar at the beginning with the finalized instrument which should continue to offer us a more full and valid dataset. As with year two, all agencies were required to have objectives that involved follow-up data collection in order to permit a measure of the effect of programming on knowledge and risk. Agencies continued to utilize the web-based reporting system; the system was adjusted to include the opportunity for agencies to report free-response answers regarding activity, progress, barriers, and recommendations that supplement their data for each month. This addition has allowed the evaluators the opportunity to assess actions being taken by agencies to assure goals are met and to begin determining common barriers to implementing these programs both within and across agencies. As with previous years, regular interaction continued between agencies, evaluators, and the City of Cleveland. 5 P age
6 DEMOGRAPHICS OF CLIENTS REACHED In the grant year, over 2,500 clients were reached with CDBG-funded HIV programming, and 1,203 of these completed the data collection instrument. The discrepancy between the number of clients served and the number of surveys collected is due to evaluation plans for some agencies and objectives not requiring data collection for some funded activities. The table below presents detailed information about those who completed the survey. Site Frequency Percent AGAPE Free Clinic NEON Proyecto Luz TOTAL This data largely demonstrates a substantial decrease from last year s report (and even the report). Last year the report saw 3,353 individuals take pre-surveys while the prior year witnessed 2,689. Three agencies experienced losses in instruments collected while one agency saw an approximate 20% gain. It should be noted, however, that overall the program worked with three fewer agencies than in previous years. The three agencies not participating in accounted for over 50% of all pre-survey responses in As a result, fewer respondents were expected this year. Given the variability in the type and reach of prevention programming conducted by the various sites, we did expect, as the data reflect, that some sites would reach many more clients than others. Since the contribution in terms of client numbers across sites is highly variable, any program-wide results should be interpreted with caution. However, aggregate data represents the collective efforts of the CDBG HIV prevention program to serve a target population and can be used for general planning purposes. A full aggregate report is available starting on page P age

7 The annual demographic profile is presented below, including race 1, sexual orientation, gender, educational level, and age. As reported below, we also collected zip code data from clients to assess the geographic reach of the programs. Race Frequency Percent Black-African American White Other Multi Racial Black-African American & White American Indian- Alaskan Native & Black American Indian-Alaskan Native Asian Total The race numbers indicate a continuation of a trend that emerged during the reporting period. We see a larger percentage of Black-African Americans and a smaller percentage of all other racial groups. Each year of the data has indicated an increase of 8% in Black-African American respondents. This shows more efforts being placed on working with African-Americans which is welcomed given that Black-African Americans typically represent a previously identified higher risk population for transmitting HIV. It should also be noted that 11.1% of respondents (128) are of Hispanic/Latino descent. 1 Definitions of racial categories were dictated by federal government H.U.D. race reporting requirements. 7 P age
8 Given the potential complexities associated with identifying sexual orientation using the data provided by survey respondents, we have chosen to present a standard cross-tabulation to show verbatim identifications of each respondent. The complexity arises, for example, from having to label the orientation of a trans male. One could utilize an identity or behavior-based definition to determine sexual orientation in such a case, consequently meaning that a trans male that has sex with males could be identified as hetero- or homosexual based on the definition used. Sexual Orientation (n = 1136) Male Female Transgender (Male to Female) Transgender (Female to Male) Sex with Men 38 (3.3%) 601 (52.9%) 0 (.0%) 0 (.0%) Sex with Women 347 (30.5%) 27 (2.4%) 3 (.3%) 0 (.0%) Sex with Both 3 (.3%) 28 (2.5%) 0 (.0%) 0 (.0%) Never had Sex 29 (2.6%) 60 (5.3%) 0 (.0%) 0 (.0%) Compared to last year s sexual orientation demographics, we have a significantly smaller percentage of homosexual and bisexual respondents. Overall, we see a drop of approximately 8 percentage points. Likewise, we have far fewer transgendered individuals in our baseline survey pool. 8 P age
9 Gender Frequency Percent Female Male Transgender Male to Female 3.3 Transgender Female to Male 0.0 Total When comparing the gender breakdown in to , we see a significant drop in the number of transgendered respondents. After seeing a move toward more gender equality from to , the data shows a higher percentage of females than males being included in the baseline. Further, we should note that 69.4% of respondents claimed that they lived in households headed by females. 9 P age
10 Education Frequency Percent Less than a high school diploma High school diploma or GED Some college College degree More than a college degree Total Overall, the data collected in describes a more polarized population when examining the educational attainments of respondents. Building on trends observed in , we see more respondents with less than a high school diploma and also more respondents with a college degree than in previous years. 10 P age
11 Age Frequency Percent 18 and under and above Total Continuing with trends that emerged in previous years of the data, we find almost a 10% increase in those 18 and under and those between 19 and 24. For all age groups between 25 and 59, we see roughly a 5% drop. As compared to previous years of data, the current round skews significantly toward younger individuals. 11 P age
12 For income, respondents are asked to select a letter corresponding to the following table which asks them to utilize the size of their household and their annual income. Household Size Annual Income You You + 1 You + 2 You + 3 You + 4 or more A low to Maximum $12,599 $14,399 $16,199 $17,999 $19,449 B low to 12,600 14,400 16,200 18,000 19,450 Maximum 20,999 23,999 26,999 29,999 32,399 C low to 21,000 24,000 27,000 30,000 32,400 Maximum 33,599 38,399 43,199 47,999 51,849 D 33, , , , ,850+ Household Income Range Frequency Percent 0-30% of Average Median Income % % > 80.1% Total When comparing the income breakdown for the current year s data with that from , we see relatively similar numbers within each category. Our most noticeable differences are a 2% decrease in the 0-30% of Average Median Income category and a 1.4% increase in those in the highest income bracket. 12 P age
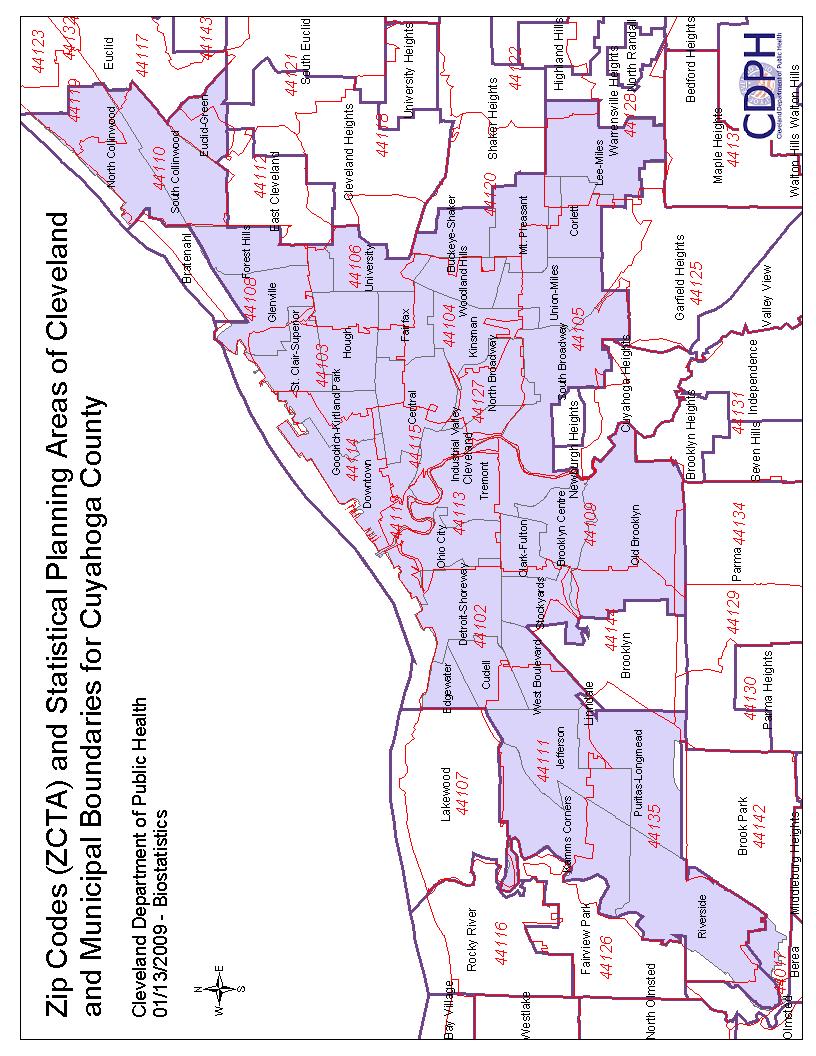
13 Zip Code ZIP Freq. % ZIP Freq. % ZIP Freq. % N.P.A Missing Overall, twenty-seven respondents (2.2) reported having no permanent address and consequently have no zip code. Second, out of the 100 plus zip codes reported by clients that are served by CDBG projects, 16 account for over 75% of the clients served. These zip codes represent Cleveland proper and its adjacent communities. This is consistent with data from and P age
14 14 P age
15 CLIENTS HIV KNOWLEDGE AND RISK In order to examine the key concepts of HIV knowledge and HIV risk, we calculated two new scale variables. The knowledge and risk scales were not calculated for The AIDS Taskforce of Greater Cleveland because this agency is exclusively involved in a training program for professionals. The knowledge scale variable was based on 10 knowledge questions. Therefore, a client s knowledge score could range from 0-10, with 0 being the lowest knowledge and 10 being the highest. Aggregate results showed that the majority of clients served this year across programs had high or relatively high knowledge. In fact, just fewer than 70% of those reached in the program scored a 7 or higher on the HIV knowledge scale. Over 40% scored 9 or 10 out of 10. This suggests that spending a significant portion of time during these HIV prevention programs on key HIV knowledge may not be an efficient effort, and time could be better used to address other knowledge issues or behavioral risk. Such findings remain consistent with data from and In fact, the current year s data suggests that respondents are even more educated at the time of pretesting than in previous years. Knowledge Cumulative Frequency Percent Score Percent Missing X Total P age
16 The risk score was based on a series of behavior questions (pertaining to sexual behavior and drug use patterns). Ultimately, we calculated a score intended to separate respondents into three groups: high risk, lower risk, and moderate risk. In order to be considered high risk, respondents had to respond with one (1) or more of the following four (4) responses: 1) Responding that they have had 5 or more sexual partners in the last 30 days 2) Responding that most of their sexual encounters take place in bath houses, adult bookstores, sex parties, massage parlors, or spas 3) Responding that they have injected or shot drugs to get high (by drug we mean any drug that a doctor or pharmacist has not given the respondent) 4) Responding that they never use a condom or they had to respond that their partners were HIV positive and that during sex they either never or only sometimes used a condom. In order to be considered lower risk, respondents had to respond according to ALL of the following responses: 1) Responding that they have had no sexual partners in the last 30 days 2) Responding that they do not believe that their sexual partner(s) have had any other sexual partners in the past 30 days or they have not had sex in the last 30 days. 3) Responding that they have never used non-prescription drugs or alcohol before or during sex in the last 30 days. 4) Responding that they have never used drugs to get high in the last 30 days. 5) Responding that they have not injected or shot drugs to get high (by drug we mean any drug that a doctor or pharmacist has not given the respondent) 6) Responding that they either do not have sex or always ask about a partner s past sexual relationships before having sex with them. 7) Responding that they either do not have sex or always ask about a partner s use of drugs and steroids, including their use of needles, before having sex with them. 8) Responding that they either do not have sex or always use a condom. 9) Responding that they have never had an STD. 10) Responding that their sexual partner/s is/are not HIV positive. 11) Responding that they have never traded sex for money, drugs, or a place to stay. If respondents were not classified as high risk or lower risk, they fell into the moderate risk category. If individuals did not answer a necessary question, they did not have a risk score calculated. Examining the valid data percents (adjusted for missing data), we find that overall, over 30% of respondents are identified as being high risk for acquiring HIV, or if already HIV+ for transmitting HIV. Only 8% of respondents meet all the criteria set forth to qualify as being at lower risk. As one would expect, the majority of respondents (approximately 61%) fall into our moderate risk category. Compared to previous years, this demonstrates roughly ten percent fewer respondents that enter programming classified as high risk and just fewer than ten percent more in moderate risk. 16 P age
")
17 Risk Score Frequency Percent Lower Risk Moderate Risk High Risk Total All Sites Scale N Mean Std. Deviation Std. Mean Knowledge Risk We conceptualize these scales into categories of knowledge grouped with categories of risk, based on the following conceptualization: Low Knowledge, High Risk (Our highest risk population) High Knowledge, High Risk Low Knowledge, Moderate Risk High Knowledge, Moderate Risk Low Knowledge, Lower Risk High Knowledge, Lower Risk (Our lowest risk population) Low knowledge was determined by answering between 0 to 6 questions correctly on the objective HIV knowledge scale. Based on this conceptualization and including only pre-test data, we find that the annual data shows that the overall program clients reached included only 59 clients at low knowledge and high risk (that is, 6.3% of the population reached by the program were in the highest overall risk category). This is a drop from 14.5% in and 15.5% in Given the new conceptualization, 17 P age

18 however, we find that our second-most populated category is those with high knowledge and high risk (23.4%); the same result was found in , although at a higher percentage. What this potentially suggests is that being knowledgeable of the threat of HIV is not serving as an adequate measure to prevent respondents from practicing high risk behaviors. This overall categorization allows for some general assessment of clients overall risk levels, but does possess some limitations. Consider the idea of a community viral load (which accounts for both the prevalence of HIV in a community and the degree to which those who are HIV+ have access to medical care which can lower their level of virus). This measure tells us that a client with moderate risk according to the scale may in fact be at high risk for acquiring HIV if the community viral load in her/his social network is high. In other words, someone at moderate risk in a community with a high viral load may be at more risk than an individual at high risk in a community with a low viral load. HIV Risk by Knowledge Number Percent Low Knowledge, High Risk High Knowledge, High Risk Low Knowledge, Moderate Risk High Knowledge, Moderate Risk Low Knowledge, Lower Risk High Knowledge, Lower Risk Total P age
19 IMPACT OF PROGRAMMING ON KNOWLEDGE AND RISK In order to examine the change in knowledge and risk from the time respondents completed their initial survey to the time they received the intervention and completed the follow-up survey, we matched all respondents pre- and post-surveys according to the unique identification number provided by each agency for tracking purposes. After doing so, we were left with two hundred and fifty-four individuals that were able to be compared although not all respondents answered all questions in the risk and knowledge scales. Agencies were asked to have individuals complete a pre-test survey as they enter agency programming. The Cleveland Department of Public Health and the evaluators, Kent State University, worked with each agency to determine the appropriate follow up time frame. Post-test follow up ranged from thirty (30) days to three (3) months following the pre-test. In regards to knowledge scores of individuals that were successfully tracked pre and post, the average pre-survey knowledge score was 7.53, while the average post-survey knowledge score was 7.68, indicating that most of these respondents were considered high knowledge prior to the programming and as an effect gained little. Compared to last year, this shows both a larger programming effect and a high level of knowledge, overall. When looking at risk categorizations, the pre-test results had 10.2% classified as lower risk, 51.3% classified as moderate risk, and 38.6% classified as high risk. After programming, the number of lower risk respondents fell to 9.0%, the number of high risk individuals dropped to 37.0%, and the number of moderate risk respondents rose to 54.0%. Using a comparison of means test between pre and post scores, we fail to find any significant difference. However, we should note that the decrease in high risk individuals is a positive sign. Unfortunately, there is a corresponding decrease in the number of individuals that find themselves in the lower risk category. The data from had shown the same gain in individuals that demonstrate lower risk but that year also demonstrated a subsequent decrease in high risk individuals after receiving programming. RESULTS Data for demonstrates much of the same result as those from the previous year. Many clients served under this program do not report the risk factors that we examine. The retooled risk analysis method developed in year two was again used and more accurately matches responses to the risk analysis questions with likelihood of contracting HIV from stated behavior. We still have concerns regarding the willingness of respondents to report risk behaviors even with the anonymity of survey responses. With regards to knowledge, the results clearly show that the majority of clients served have high HIV knowledge of the items included in the knowledge scale. This may demonstrate the historic focus of the overall program on health education and the relative success within these programs of addressing the knowledge gap. Looking at specific questions, only two questions were correctly answered by fewer than 70% of those surveyed (whether natural skin condoms work better than latex at preventing the contraction of HIV and whether HIV can be transmitted through deep kissing). These questions have been regularly answered incorrectly in previous rounds of data analysis. A new trend related to specific knowledge questions is that less than 75% correctly answered that there is a vaccine that will prevent an individual from contracting HIV. Future 19 P age
20 trainings may want to be sure to clearly address these questions given the relatively lower levels of knowledge of them. As was stated in previous annual reports, there are still concerns regarding the high number of high knowledge, high risk respondents (although the number has dropped 8% from last year s report). Since they are clearly demonstrating the knowledge to understand how HIV is spread, programming that is designed to examine behavior change will likely be of more use to that population. Riskknowledge results vary for individual sites, but the aggregate data clearly demonstrates that CDBG agencies are reaching a substantial group of clients who are in the moderate risk category for contracting HIV. RESULTS BY SITE A cursory examination of the mean knowledge scale scores and mean risk categorizations by site shows that there is substantial variation in the risk levels of clients being served. Below is a breakdown of each individual site and their reports for the agency as a whole and by objective. These results could be used to provide technical assistance to sites on their client recruitment efforts and the ability to assure that clients are receiving programming that best fits their needs. RECOMMENDATIONS AND GLOBAL FINDINGS As in previous reports, we must begin by noting the willingness of community agencies to work with the evaluators to make the changes necessary to assure effective programming. They worked diligently to assure reachable, meaningful objectives, effective follow-ups, and proper client tracking. While agencies have been working toward evidence based or standardizes programs for the clients served with CDBG dollars, the current year assisted them further by asking them to provide evaluators with an assessment of their perceived barriers to fulfilling objectives every month. As we advance further into the program, it will be essential to utilize the perceived barriers when agencies, evaluators, and city officials meet to discuss future plans and objectives. Only by learning from these barriers and determining how to work within the given framework will we be able to assure that agencies are able to meet all objectives in the most efficient manner possible. Similar to previous reports, it is important to point out the vital role played by the personnel at the community agencies. Personnel changes in these smaller agencies had a significant impact on agencies as they tried to continue toward the completion of their objectives. Most of the agencies implemented their programs with only one or two staff and if the person in charge of the program left, data collection was often left up in the air until new staff could be hired and trained. While we witnessed fewer staff changes than in previous years of data collection, we still find it necessary to point out the time and effort put forth by all of our community agencies. The data indicates that like in previous years, most of the agencies were generally serving clients with relatively high knowledge and relatively moderate risk. Like in year 2, follow up data for year 3 shows that there is no statistically significant improvement in increasing knowledge or reducing risk for clients served although scores moved in the desired direction. During the first two years of this project each agency received multiple site visits. As part of those initial year one site visits, agencies were asked to participate in helping to develop a single instrument 20 P age
21 that would be used by all CDBG sites. It should always be noted that year one represented multiple survey instruments that reflected changes in question wording, placement, agency needs, etc. Beyond an agency s willingness to use a new instrument, each agency worked with the Cleveland Department of Health and the evaluators to develop agency specific objectives based on the proposals currently funded for year one of the evaluation. Again, it should be noted that this was a totally new approach for agencies regarding how agencies addressed the populations served with their CDBG dollars and how data needed to be collected. Once objectives were developed, site visits generally addressed issues around appropriately developing objective numbering systems that worked for the agency. This was an important step for agencies since they were now working toward specific objectives that addressed special populations with target numbers to reach. By the end of year one, a final instrument was completed and prepared for use in year two. Because the Cleveland Department of Public Health saw this as a two year commitment, we were then able to work with each agency to refine their objectives based on data from year one and move all agencies toward the collection of follow up data for at least some of their objectives in year two. As agencies became more familiar with numbering and survey administration, technical support began addressing issues of follow up. During the course of year two, most technical support revolved around learning and supporting the development of follow up techniques that were appropriate for each agency and each objective within the agency. For many agencies this was a developmental process of trying something, learning from what worked and did not work, and then improving on and/or changing strategies to find something that worked better. In year three, as previously discussed, most of the technological advances dealt with making it possible to provide additional information to evaluators that was not available in previous years of data collection. This information including activity, progress, barriers to completion, and recommendations will provide helpful tips as agencies plan future programming. From the first year to present, agencies have been able to use collected data to better articulate objectives that reflect populations in-need of HIV education and awareness. In year two, agencies did a better job of assuring that they completed pretests but struggled with post-test follow up collection. In year three, we found agencies devoting more energy to collecting follow up data and having variable success in doing so. In future years, we will want to continue assuring that we strive to achieve as many follow-up surveys as possible. 21 P age
22 Survey Item Analysis CDBG: Year Two OVERALL Client Pretest Report Facility AGAPE 122 Free Clinic 210 NEON 600 Proyecto Luz 271 Demographic information is reported on pp Risk Questions How many sexual partners have you had in the last 30 days? (n = 1180) 5 or more 6.1% % % None 25.9% Do you think your sexual partner(s) have had any sexual partners other than you in the last 30 days? (n = 1203) Yes 26.4% No 52.5% No sex in the last 30 days 21.2% Where do you have most of your sexual encounters (select one answer)? (n = 1169) In your or your partner s home 69.8% In bath houses, adult bookstores, sex parties, massage parlors, or spas 0.8% In hotel/motels rooms, cars, or bars 1.8% Someplace else 10.0% Not sexually active 17.6% How many times in the last 30 days, did you use non-prescription drugs or alcohol before or during sex? (n = 1182) 5 or more 7.2% % 1 8.0% Never 75.5% 22 P age
23 How many times in the last 30 days, did you use drugs to get high? (n = 1155) 5 or more 10.6% % 1 5.7% Never 78.5% Have you ever injected or shot drugs to get high (by drug we mean any drug that a doctor or pharmacist did not give to you)? (n = 1160) Yes 7.1% Before you have sex with someone, do you ask about their past sexual relationships? (n = 1154) Always 34.4% Sometimes 39.7% Never 12.7% Do not have sex 13.3% Do you ask sexual partners before you have sex about their use of drugs and steroids, including their use of needles? (n = 1145) Always 28.1% Sometimes 26.4% Never 31.7% Do not have sex 13.8% How often do you use a condom? (n = 1145) Always 26.6% Sometimes 42.8% Never 16.9% Do not have sex 13.8% Have you ever had an STD (such as gonorrhea, syphilis, Chlamydia, genital warts, or genital herpes)? (n = 1153) Yes 30.8% No 64.1% Don t know 5.1% When was the last time you had an HIV test? (n = 1144) In the past few weeks 8.7% In the past few months 20.9% In the past year 16.9% More than a year ago 19.2% Never 34.3% 23 P age
24 Are you HIV positive? (n = 1154) Yes 0.9% No 84.3% Don t know 14.8% Is/Are your sexual partner/s HIV positive? (n = 1137) Yes 0.5% No 80.5% Don t know 19.0% Have you ever traded sex for money, drugs, or a place to stay? (n = 1144) Yes 7.5% No 90.8% Don t know 1.7% Risk Scores (n = 1002) Lower Risk 8.1% Moderate Risk 61.1% High Risk 30.8% Knowledge Questions Percent Correct Pulling out the penis before a man climaxes/cums keeps a woman from getting HIV during sex. (n = 1161) 83.6% A woman can get HIV if she has anal sex with a man. (n = 1156) 82.3% Showering or washing one s genitals/private parts after sex keeps a persona from getting HIV. (n = 1154) 85.1% There is a vaccine that can stop adults from getting HIV. (n = 1156) 74.5% People are likely to get HIV by deep kissing, putting their tongue in their partner s mouth, if their partner has HIV. (n = 1153) 49.4% A woman cannot get HIV if she has sex during her period. (n = 1157) 75.8% A natural skin condom works better against HIV than a latex condom does. (n = 1154) 66.1% Having sex with more than one partner can increase a person s chance of being infected with HIV. (n = 1156) 85.4% A person can get HIV from oral sex. (n = 1152) 79.3% Using Vaseline or baby oil with condoms lowers the chance of getting HIV. (n = 1153) 76.8% Knowledge Scores (Maximum score of 10) (n = 1082) Range 0-10 Average 7.63 Knowledge Scores (n = 1203) Score Frequency % C % Score Frequency % C % Score Frequency % C % Miss X P age
25 HIV Risk by Knowledge Number Percent High Risk-Low Knowledge High Risk-High Knowledge Moderate Risk-Low Knowledge Moderate Risk-High Knowledge Lower Risk-Low Knowledge Lower Risk-High Knowledge Total Risk Scores Pre (n = 197) Post (n = 189) Lower Risk 10.2% Lower Risk 9.0% Moderate Risk 51.3% Moderate Risk 54.0% High Risk 38.6% High Risk 37.0% Knowledge Scores (Maximum score of 10) Pre (n = 207) 7.53 Post (n = 212) P age
26 Agency Name: AGAPE Program (Antioch Development Corporation) Agency Address: 8869 Cedar Avenue, Cleveland, Ohio Program Name: The Faith-Based Circle of Care Project Target Population: African American Females, Aged years Program Staff: Gena Austin, Program Manager Grant Amount: $40,000 Program Description: The Faith-Based Circle of Care Project is focused on creating active partnerships with six community-involved pastors and their congregations. AGAPE expects to raise awareness among African Americans who may not otherwise be reached. These faith-based congregations typically include large cohorts of heterosexual females aged 25-44, one of the largest populations at-risk for contracting HIV. The recruited congregations will become members of AGAPEs Faith Community Network, a consortium of urban churches in six City of Cleveland wards. Through their membership congregants will be dedicated to the prevention and containment of HIV/AIDS via education, lifestyle change and HIV testing within the African American community. Objective Actual Target % of Recruit 3 churches to become participants in the Circle of Care Project 3 total Three churches will be recruited to participate in the Circle of Care Project MOU will be completed by each participating church Recruit and train 3 site coordinators 3 total Site coordinators will complete the pre/post test training surveys Site coordinators will complete an HIV/STD curriculum Church congregants will complete HIV/STD Prevention sessions 60 total Congregation members will participate in HIV/STD educational curriculum All participants will complete the pre/post test client surveys 2nd year churches (5) will sponsor 3 5 events during the year 3 total 5 second year churches will collaborate to sponsor 3 to 5 community HIV health and/or awareness events All participants of the health/awareness events will complete pre-test client surveys Symposiums will be conducted at third year churches 60 total All participants will complete pre/post surveys & workshop evaluation 20 women will be recruited per symposium Decisions We Make Workshop will be presented Quarterly meeting with site coordinators 4 total No pre/post test survey data collection required Clients surveys from health/awareness events P age
27 AGAPE has been successful in working toward their objectives in year three. Outside of the measurable survey responses, AGAPE has worked to recruit new churches to the Circle of Care project, recruited site coordinators at the new churches, helped second year churches begin developing events related to community HIV health and awareness events, held symposiums at third year churches, and also held meetings with all site coordinators to align projects. There are, however, barriers to implementation with some objectives. Looking at adding churches, recruitment is often hindered by the availability of someone at the church to take responsibility for the program. As a means to combat this potential barrier, AGAPE will be attempting to have smaller churches join together to share the responsibility of implementing the programs. Likewise, finding individuals to take over as site coordinators has proved to be a potential barrier. With regards to having congregations complete HIV/STD prevention sessions, AGAPE has found that church people do not like completing surveys that are sexual in nature and are working to find ways for respondents to feel more secure in their decision to participate. Third year symposiums have been difficult to schedule given the full schedules of most churches. This was ultimately their weakest objective with regards to accomplishment. Getting people to change events or add another has proven to be problematic. Quarterly meetings have been difficult to schedule. Lastly, the health and awareness events (including Langston Hughes, Lion of Judah, Ecumenical HIV Task Force, First Ladies Breakfast, and Golden Ciphers Training) have gone well, but people are still reluctant to participate out of fear that the survey may be linked back to them. As such, AGAPE is considering making it possible for respondents to drop their completed surveys anonymously into envelopes during events. Overall, AGAPE is facing barriers related to time and responsibility. Busy schedules at churches and the time commitment to running this program have both been noted as barriers to implementation and AGAPE has identified ways to help share the burden for churches. They have further been proactive in attempting to come up with mechanisms to alleviate citizen concern about surveys being linked back to the respondent. Results Summary: Data indicate that AGAPE s Circle of Care program continues to successfully reach heterosexual, African-American women its target audience. With regards to age, they could look for improvement in reaching individuals between 25 and 44 as presently that age range accounts for only 48.6% of their surveys. Attendees of the church programs demonstrate relatively high knowledge and low risk, with roughly a third never being tested for HIV. Year three data shows a greater percentage of program attendees being high risk for contraction of HIV mainly due to a large number of respondents claiming to never use a condom. This fact may be due to the fact that almost 90% of those surveyed have either not had sex in the past 30 days or are in monogamous relationships. Post-surveys indicate fairly static numbers with regards to knowledge and risk. While not statistically significant, the analysis actually shows respondents measuring less knowledgeable in post-surveys. 27 P age
28 CDBG: Year Three Client Pretest Report Facility AGAPE 122 Demographics Are you of Hispanic or Latino descent? (n = 118) Yes 21.2% Race (check only one) (n = 104) White 12.5% Black-African American 81.7% Asian 1.0% American Indian-Alaskan Native 0.0% Native Hawaiian-Other Pacific Islander 0.0% Asian & White 0.0% Black-African American & White 1.9% American Indian-Alaskan Native & Black 2.9% Other Multi Racial 0.0% Gender (n = 118) Male 21.2% Female 78.8% Transgender Male to Female 0.0% Transgender Female to Male 0.0% Sexual Orientation (n = 115) Sex with Men Sex with Women Sex with Both Never Had Sex Male 2 (1.7%) 20 (17.4%) 0 (0.0%) 3 (2.6%) Female 83 (72.2%) 5 (4.3%) 2 (1.7%) 0 (0.0%) Transgender Male to Female 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) Transgender Female to Male 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) Education (check highest level) (n = 117) Less than high school diploma 7.7% High school diploma or GED 25.6% Some college 30.8% College degree 25.6% More than a college degree 10.3% 28 P age
29 Zip Code (n = 122) Zip Frequency % Zip Frequency % Zip Frequency % Missing N.P.A Age (n = 119) 18 and under 3.4% % % % % % 60 and above 16.0% Is a female your head of household? (n = 118) Yes 61.9% Household income range (n = 119) 0-30% of Average Median Income 31.1% % 18.5% % 25.2% > 80.1% 25.2% Risk Questions How many sexual partners have you had in the last 30 days? (n = 117) 5 or more 1.7% % % None 36.8% 29 P age
30 Do you think your sexual partner(s) have had any sexual partners other than you in the last 30 days? (n = 97) Yes 9.3% No 67.0% No sex in the last 30 days 23.7% Where do you have most of your sexual encounters (select one answer)? (n = 113) In your or your partner s home 63.7% In bath houses, adult bookstores, sex parties, massage parlors, or spas 0.9% In hotel/motels rooms, cars, or bars 1.8% Someplace else 5.3% Not sexually active 28.3% How many times in the last 30 days, did you use non-prescription drugs or alcohol before or during sex? (n = 116) 5 or more 6.9% % 1 6.0% Never 81.9% How many times in the last 30 days, did you use drugs to get high? (n = 117) 5 or more 5.1% % 1 0.0% Never 92.3% Have you ever injected or shot drugs to get high (by drug we mean any drug that a doctor or pharmacist did not give to you)? (n = 119) Yes 1.7% Before you have sex with someone, do you ask about their past sexual relationships? (n = 113) Always 35.4% Sometimes 26.5% Never 17.7% Do not have sex 20.4% Do you ask sexual partners before you have sex about their use of drugs and steroids, including their use of needles? (n = 114) Always 28.9% Sometimes 18.4% Never 31.6% Do not have sex 21.1% 30 P age
31 How often do you use a condom? (n = 111) Always 16.2% Sometimes 27.9% Never 33.3% Do not have sex 22.5% Have you ever had an STD (such as gonorrhea, syphilis, Chlamydia, genital warts, or genital herpes)? (n = 115) Yes 27.3% No 70.7% Don t know 2.0% When was the last time you had an HIV test? (n = 113) In the past few weeks 3.5% In the past few months 14.2% In the past year 21.2% More than a year ago 27.4% Never 33.6% Are you HIV positive? (n = 117) Yes 0.9% No 83.8% Don t know 15.4% Is/Are your sexual partner/s HIV positive? (n = 108) Yes 0.9% No 87.0% Don t know 12.0% Have you ever traded sex for money, drugs, or a place to stay? (n = 114) Yes 7.0% No 92.1% Don t know 0.9% Risk Scores (n = 91) Lower Risk 13.2% Moderate Risk 41.8% High Risk 45.1% 31 P age
32 Knowledge Questions Percent Correct Pulling out the penis before a man climaxes/cums keeps a woman from getting HIV during sex. (n = 116) 82.8% A woman can get HIV if she has anal sex with a man. (n = 117) 78.6% Showering or washing one s genitals/private parts after sex keeps a persona from getting HIV. (n = 117) 90.6% There is a vaccine that can stop adults from getting HIV. (n = 118) 83.9% People are likely to get HIV by deep kissing, putting their tongue in their partner s mouth, if their partner has HIV. (n = 115) 56.5% A woman cannot get HIV if she has sex during her period. (n = 116) 77.6% A natural skin condom works better against HIV than a latex condom does. (n = 115) 71.3% Having sex with more than one partner can increase a person s chance of being infected with HIV. (n = 115) 82.6% A person can get HIV from oral sex. (n = 114) 71.1% Using Vaseline or baby oil with condoms lowers the chance of getting HIV. (n = 115) 82.6% Knowledge Scores (Maximum score of 10) (n = 104) Range 0-10 Average 7.79 Knowledge Scores (n = 104) Score Frequency % C % Score Frequency % C % Score Frequency % C % Miss X HIV Risk by Knowledge Number Percent High Risk-Low Knowledge High Risk-High Knowledge Moderate Risk-Low Knowledge Moderate Risk-High Knowledge Lower Risk- Low Knowledge Lower Risk- High Knowledge Total Risk Scores Pre (n = 20) Post (n = 15) Lower Risk 20.0% Lower Risk 13.3% Moderate Risk 20.0% Moderate Risk 33.3% High Risk 60.0% High Risk 53.3% Knowledge Scores (Maximum score of 10) Pre (n = 19) 8.68 Post (n = 19) 7.95 CDBG: Year Three Client Pretest Objective Report 32 P age
Evaluation Report of the Community Development Block Grant (CDBG)-Funded HIV/AIDS Prevention Initiative
-Funded HIV/AIDS Prevention Initiative") Evaluation Report of the Community Development Block Grant (CDBG)-Funded HIV/AIDS Prevention Initiative 2007-2008 Sonia Alemagno, Ph. D. Peggy Shaffer-King, MA Institute for the Study and Prevention of
Evaluation Report of the Community Development Block Grant (CDBG)-Funded HIV/AIDS Prevention Initiative 2007-2008 Sonia Alemagno, Ph. D. Peggy Shaffer-King, MA Institute for the Study and Prevention of
Until recently, countries in Eastern
 10 C H A P T E R KNOWLEDGE OF HIV/AIDS TRANSMISSION AND PREVENTION Until recently, countries in Eastern Europe, the, and Central Asia had not experienced the epidemic levels of HIV/AIDS found in other
10 C H A P T E R KNOWLEDGE OF HIV/AIDS TRANSMISSION AND PREVENTION Until recently, countries in Eastern Europe, the, and Central Asia had not experienced the epidemic levels of HIV/AIDS found in other
Just the FACTS: You can help! Join the NMDP Registry. Vital Statistics
 Just the FACTS: You can help! Join the NMDP Registry Vital Statistics Every year, more than 10,000 men, women and children get life-threatening diseases such as leukemia and lymphoma, and do not have a
Just the FACTS: You can help! Join the NMDP Registry Vital Statistics Every year, more than 10,000 men, women and children get life-threatening diseases such as leukemia and lymphoma, and do not have a
Trends in Reportable Sexually Transmitted Diseases in the United States, 2007
 Trends in Reportable Sexually Transmitted Diseases in the United States, 2007 National Surveillance Data for Chlamydia, Gonorrhea, and Syphilis Sexually transmitted diseases (STDs) remain a major public
Trends in Reportable Sexually Transmitted Diseases in the United States, 2007 National Surveillance Data for Chlamydia, Gonorrhea, and Syphilis Sexually transmitted diseases (STDs) remain a major public
Estimates of New HIV Infections in the United States
 Estimates of New HIV Infections in the United States CDC HIV/AIDS FactS A u g u s t 28 Accurately tracking the HIV epidemic is essential to the nation s HIV prevention efforts. Yet monitoring trends in
Estimates of New HIV Infections in the United States CDC HIV/AIDS FactS A u g u s t 28 Accurately tracking the HIV epidemic is essential to the nation s HIV prevention efforts. Yet monitoring trends in
Estimates of New HIV Infections in the United States
 Estimates of New HIV Infections in the United States CDC HIV/AIDS FACT S A UGUS T 28 Accurately tracking the HIV epidemic is essential to the nation s HIV prevention efforts. Yet monitoring trends in new
Estimates of New HIV Infections in the United States CDC HIV/AIDS FACT S A UGUS T 28 Accurately tracking the HIV epidemic is essential to the nation s HIV prevention efforts. Yet monitoring trends in new
Influence of STIs on Condom Use Behavior in College Age Women
 Influence of STIs on Condom Use Behavior in College Age Women Emily VanEyll, Laura Van Wyck Faculty Sponsor: Betsy Morgan, Department of Psychology ABSTRACT Sexually transmitted infections (STIs) are an
Influence of STIs on Condom Use Behavior in College Age Women Emily VanEyll, Laura Van Wyck Faculty Sponsor: Betsy Morgan, Department of Psychology ABSTRACT Sexually transmitted infections (STIs) are an
Welcome to Your Reading Assignment
 Welcome to Your Reading Assignment This workbook contains four reading assignments. It is filled with easy-to-read articles you can use to help keep yourself and those you care about safe. After each reading
Welcome to Your Reading Assignment This workbook contains four reading assignments. It is filled with easy-to-read articles you can use to help keep yourself and those you care about safe. After each reading
Missouri Statewide Integrated HIV Prevention and Care Plan, including the Statewide Coordinated Statement of Need, CY
 Missouri Statewide Integrated HIV Prevention and Care Plan, including the Statewide Coordinated Statement of Need, CY 2017-2021 September 20, 2016 Developed through the collaborative efforts of the following
Missouri Statewide Integrated HIV Prevention and Care Plan, including the Statewide Coordinated Statement of Need, CY 2017-2021 September 20, 2016 Developed through the collaborative efforts of the following
State of Alabama HIV Surveillance 2013 Annual Report Finalized
 State of Alabama HIV Surveillance 2013 Annual Report Finalized Prepared by: Division of STD Prevention and Control HIV Surveillance Branch Contact Person: Allison R. Smith, MPH Allison.Smith@adph.state.al.us
State of Alabama HIV Surveillance 2013 Annual Report Finalized Prepared by: Division of STD Prevention and Control HIV Surveillance Branch Contact Person: Allison R. Smith, MPH Allison.Smith@adph.state.al.us
Protecting Your Health: Understanding and Preventing STDs
 Protecting Your Health: Understanding and Preventing STDs A Lesson Plan from Rights, Respect, Responsibility: A K-12 Curriculum Fostering responsibility by respecting young people s rights to honest sexuality
Protecting Your Health: Understanding and Preventing STDs A Lesson Plan from Rights, Respect, Responsibility: A K-12 Curriculum Fostering responsibility by respecting young people s rights to honest sexuality
An evaluation of the STD profiles and safe sex practices of a sample of swingers
 An evaluation of the STD profiles and safe sex practices of a sample of swingers Presented by: Edward M. Fernandes, Ph.D. Assistant Professor of Psychology Barton College, North Carolina George Gaither,
An evaluation of the STD profiles and safe sex practices of a sample of swingers Presented by: Edward M. Fernandes, Ph.D. Assistant Professor of Psychology Barton College, North Carolina George Gaither,
HIV Prevention Service Provider Survey 2014
 Respondent Demographics This survey will help the Florida HIV Prevention Planning Group (PPG) establish the resources and unmet needs of the communities we serve. Please take a few minutes to complete
Respondent Demographics This survey will help the Florida HIV Prevention Planning Group (PPG) establish the resources and unmet needs of the communities we serve. Please take a few minutes to complete
1. What is your date of birth? Month Day Year
 Participant ID # Today's Date 1. What is your date of birth? Month Day Year 2. How would you describe your race / ethnicity? African American / Black European American / White Hispanic Asian Native American
Participant ID # Today's Date 1. What is your date of birth? Month Day Year 2. How would you describe your race / ethnicity? African American / Black European American / White Hispanic Asian Native American
Revised MEN S ATTITUDE SURVEY (the RMAS)
") VISIT #: Visit Date: As before, this questionnaire is intended to assess and track your attitudes, beliefs and other factors that might influence your sexual and other risky or risk-reduction practices
VISIT #: Visit Date: As before, this questionnaire is intended to assess and track your attitudes, beliefs and other factors that might influence your sexual and other risky or risk-reduction practices
MMWR Analysis Provides New Details on HIV Incidence in U.S. Populations
 MMWR Analysis Provides New Details on HIV Incidence in U.S. Populations CDC HIV/AIDS Fa c t s S e p t e m b e r 2008 On August 6, 2008, the Centers for Disease Control and Prevention (CDC) released a new
MMWR Analysis Provides New Details on HIV Incidence in U.S. Populations CDC HIV/AIDS Fa c t s S e p t e m b e r 2008 On August 6, 2008, the Centers for Disease Control and Prevention (CDC) released a new
State of Alabama HIV Surveillance 2014 Annual Report
 State of Alabama HIV Surveillance 2014 Annual Report Prepared by: Division of STD Prevention and Control HIV Surveillance Branch Contact Person: Richard P. Rogers, MS, MPH richard.rogers@adph.state.al.us
State of Alabama HIV Surveillance 2014 Annual Report Prepared by: Division of STD Prevention and Control HIV Surveillance Branch Contact Person: Richard P. Rogers, MS, MPH richard.rogers@adph.state.al.us
Ohio PREP Region 7: Cuyahoga County Board of Health October 2017 through September 2018 Data Report
 Ohio PREP Region 7: Cuyahoga County Board of Health October 2017 through September 2018 Data Report Provided by Ohio University s Voinovich School of Leadership and Public Affairs 1 P age This report covers
Ohio PREP Region 7: Cuyahoga County Board of Health October 2017 through September 2018 Data Report Provided by Ohio University s Voinovich School of Leadership and Public Affairs 1 P age This report covers
Community Homelessness Assessment, Local Education and Networking Groups (CHALENG)
") June 2016 Community Homelessness Assessment, Local Education and Networking Groups (CHALENG) Community Homelessness Assessment, Local Education and Networking Groups for, commonly referred to as Project
June 2016 Community Homelessness Assessment, Local Education and Networking Groups (CHALENG) Community Homelessness Assessment, Local Education and Networking Groups for, commonly referred to as Project
HIV Testing Survey, 2002
 Special Surveillance Report Number 5 HIV Testing Survey, 2002 DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service Centers for Disease Control and Prevention Atlanta, Georgia 30333 . The HIV/AIDS
Special Surveillance Report Number 5 HIV Testing Survey, 2002 DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service Centers for Disease Control and Prevention Atlanta, Georgia 30333 . The HIV/AIDS
What You Need to Know. Sexually Transmitted Infections (STIs)
") What You Need to Know Sexually Transmitted Infections (STIs) What You Need to Know About STIs What are STIs? Sexually transmitted infections (STIs) are diseases that spread through sexual contact. If you
What You Need to Know Sexually Transmitted Infections (STIs) What You Need to Know About STIs What are STIs? Sexually transmitted infections (STIs) are diseases that spread through sexual contact. If you
A Sexual Health Study with Africans in Frankfurt am Main
 A Sexual Health Study with Africans in Frankfurt am Main Working together for Health Promotion INFORMATION FOR STUDY PARTICIPANTS WHO ARE WE? We are a group of Africans, researchers and persons doing
A Sexual Health Study with Africans in Frankfurt am Main Working together for Health Promotion INFORMATION FOR STUDY PARTICIPANTS WHO ARE WE? We are a group of Africans, researchers and persons doing
Today s Webinar will be approximately 1 hour long including breaks for Q and A one in the middle, and one at the end. In order to receive Continuing
 1 Today s Webinar will be approximately 1 hour long including breaks for Q and A one in the middle, and one at the end. In order to receive Continuing Nursing Education, participants must attend the entire
1 Today s Webinar will be approximately 1 hour long including breaks for Q and A one in the middle, and one at the end. In order to receive Continuing Nursing Education, participants must attend the entire
NJ s Transitional Housing Initiative
 NJ s Transitional Housing Initiative SARA WALLACH, DOH DHSTS PROGRAM MANAGEMENT OFFICER ANNIE CHEN, ARFC CHIEF OPERATING OFFICER Definition of Homeless person According to the Department of Housing and
NJ s Transitional Housing Initiative SARA WALLACH, DOH DHSTS PROGRAM MANAGEMENT OFFICER ANNIE CHEN, ARFC CHIEF OPERATING OFFICER Definition of Homeless person According to the Department of Housing and
Trends in U.S. HIV Diagnoses,
 CDC FACT SHEET Trends in U.S. HIV Diagnoses, 2005-2014 More than three decades after the first cases of AIDS were diagnosed in the United States, HIV continues to pose a substantial threat to the health
CDC FACT SHEET Trends in U.S. HIV Diagnoses, 2005-2014 More than three decades after the first cases of AIDS were diagnosed in the United States, HIV continues to pose a substantial threat to the health
PHSKC HIV Testing Survey: Knowledge, Attitudes and Practices
 PHSKC HIV Testing Survey: Knowledge, Attitudes and Practices Page One This anonymous survey is intended to collect information about HIV testing attitudes and practices. Results will be used by Public
PHSKC HIV Testing Survey: Knowledge, Attitudes and Practices Page One This anonymous survey is intended to collect information about HIV testing attitudes and practices. Results will be used by Public
Teen Sexual Health Survey
 Instructions Teen Sexual Health Survey Thank you for taking part in our survey. DO NOT write your name on this survey. The answers you give will be kept private. No one will know what you write. Answer
Instructions Teen Sexual Health Survey Thank you for taking part in our survey. DO NOT write your name on this survey. The answers you give will be kept private. No one will know what you write. Answer
2017 EPIDEMIOLOGY REPORT
 2017 EPIDEMIOLOGY REPORT Volume 4, July 2017 A report on sexually transmitted infection and human immunodeficiency virus testing, positivity, and behavioral trends from 2012 2016 HOWARD BROWN HEALTH 2017
2017 EPIDEMIOLOGY REPORT Volume 4, July 2017 A report on sexually transmitted infection and human immunodeficiency virus testing, positivity, and behavioral trends from 2012 2016 HOWARD BROWN HEALTH 2017
Housing Needs Assessment Survey Tool
 Appendix II -Year Chicago Area HIV/AIDS Housing Plan A-9 Housing Needs Assessment Survey Tool Appendix II consists of the English Housing Needs Assessment Survey tool (the Spanish-language survey is not
Appendix II -Year Chicago Area HIV/AIDS Housing Plan A-9 Housing Needs Assessment Survey Tool Appendix II consists of the English Housing Needs Assessment Survey tool (the Spanish-language survey is not
Persons Living with HIV/AIDS, San Mateo County Comparison
 Persons Living with HIV/AIDS, San Mateo County Comparison As of December 2008, there were 1,152 persons living with HIV or HIV/AIDS in San Mateo County (Table 1). Compared to California and the United
Persons Living with HIV/AIDS, San Mateo County Comparison As of December 2008, there were 1,152 persons living with HIV or HIV/AIDS in San Mateo County (Table 1). Compared to California and the United
Ohio PREP Region 7 Data Report. Prepared by: Ohio University s Voinovich School of Leadership and Public Affairs January 2018
 Ohio PREP Region 7 Data Report Prepared by: Ohio University s Voinovich School of Leadership and Public Affairs January 2018 Introduction This report provides data from 2013 through July 2017 for Ohio
Ohio PREP Region 7 Data Report Prepared by: Ohio University s Voinovich School of Leadership and Public Affairs January 2018 Introduction This report provides data from 2013 through July 2017 for Ohio
Multnomah County Health Department
 Multnomah County Health Department Racial & Ethnic Health Disparities: 2011 Update Racial and Ethnic Health Disparities and Rate Trends Multnomah County: 1994- Healthy Birth Initiative African American
Multnomah County Health Department Racial & Ethnic Health Disparities: 2011 Update Racial and Ethnic Health Disparities and Rate Trends Multnomah County: 1994- Healthy Birth Initiative African American
Advancing the National HIV/AIDS Strategy: Housing and the HCCI. Housing Summit Los Angeles, CA
 Advancing the National HIV/AIDS Strategy: Housing and the HCCI Housing Summit Los Angeles, CA October 21, 2014 The National HIV/AIDS Strategy Facets of the Strategy Limited number of action steps Sets
Advancing the National HIV/AIDS Strategy: Housing and the HCCI Housing Summit Los Angeles, CA October 21, 2014 The National HIV/AIDS Strategy Facets of the Strategy Limited number of action steps Sets
2014 County of Marin Fact Sheet: HIV/AIDS in Marin County
 2014 County of Marin Fact Sheet: HIV/AIDS in Marin County HIV/AIDS epidemiology data is from the enhanced HIV/AIDS Reporting System (ehars) maintained by the Office of AIDS. The data presented here are
2014 County of Marin Fact Sheet: HIV/AIDS in Marin County HIV/AIDS epidemiology data is from the enhanced HIV/AIDS Reporting System (ehars) maintained by the Office of AIDS. The data presented here are
If you are a man that ONLY has sex with women this may not be the brochure for you.
 If you are a man that ONLY has sex with women this may not be the brochure for you. To find resources that best meet your needs check out the following website: http://www.cdc.gov/men Whether you are gay,
If you are a man that ONLY has sex with women this may not be the brochure for you. To find resources that best meet your needs check out the following website: http://www.cdc.gov/men Whether you are gay,
Missouri St. Louis TGA 2016 HIV Epidemiological Profile
 Missouri St. Louis TGA 2016 HIV Epidemiological Profile St. Louis TGA Part A Planning Council Prepared by the City of St. Louis Department of Health Center for Health Information, Research, and Planning
Missouri St. Louis TGA 2016 HIV Epidemiological Profile St. Louis TGA Part A Planning Council Prepared by the City of St. Louis Department of Health Center for Health Information, Research, and Planning
Substance Abuse Treatment, Integrated Care, & the HIV Care Continuum
 Substance Abuse Treatment, Integrated Care, & the HIV Care Continuum Sherry Larkins, Ph.D. University of California, Los Angeles Integrated Substance Abuse Programs May 22, 2014 Does your agency offer
Substance Abuse Treatment, Integrated Care, & the HIV Care Continuum Sherry Larkins, Ph.D. University of California, Los Angeles Integrated Substance Abuse Programs May 22, 2014 Does your agency offer
HIV Testing After 25 Years
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-public-health-policy/hiv-testing-after-25-years/3736/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-public-health-policy/hiv-testing-after-25-years/3736/
How does HBV affect the liver?
 Hepatitis B Why is the liver important? Your liver is a vital organ that performs many essential functions. It s the largest solid organ in the body and is located under your rib cage on the upper right
Hepatitis B Why is the liver important? Your liver is a vital organ that performs many essential functions. It s the largest solid organ in the body and is located under your rib cage on the upper right
HIV/AIDS AND CULTURAL COMPETENCY
 HIV/AIDS AND CULTURAL COMPETENCY Learning Objectives Gain a Basic Understanding of Cultural Competency Discuss the Importance of Cultural Competency in Addressing Health Disparities Review the Relationship
HIV/AIDS AND CULTURAL COMPETENCY Learning Objectives Gain a Basic Understanding of Cultural Competency Discuss the Importance of Cultural Competency in Addressing Health Disparities Review the Relationship
Note: Staff who work in case management programs should attend the AIDS Institute training, "Addressing Prevention in HIV Case Management.
 Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
Patterns of Union Formation Among Urban Minority Youth in the United States
 Archives of Sexual Behavior, Vol. 29, No. 2, 2000 Patterns of Union Formation Among Urban Minority Youth in the United States Kathleen Ford, Ph.D. 1 and Anne Norris, Ph.D., RN 2 Since 1990, several large
Archives of Sexual Behavior, Vol. 29, No. 2, 2000 Patterns of Union Formation Among Urban Minority Youth in the United States Kathleen Ford, Ph.D. 1 and Anne Norris, Ph.D., RN 2 Since 1990, several large
BLACK RESIDENTS VIEWS ON HIV/AIDS IN THE DISTRICT OF COLUMBIA
 PUBLIC OPINION DISPARITIES & PUBLIC OPINION DATA NOTE A joint product of the Disparities Policy Project and Public Opinion and Survey Research October 2011 BLACK RESIDENTS VIEWS ON HIV/AIDS IN THE DISTRICT
PUBLIC OPINION DISPARITIES & PUBLIC OPINION DATA NOTE A joint product of the Disparities Policy Project and Public Opinion and Survey Research October 2011 BLACK RESIDENTS VIEWS ON HIV/AIDS IN THE DISTRICT
Introduction. Behavior Surveillance System (YRBSS),
,") 2015 Prepared for the Colorado Department of Education, Colorado Department of Human Services, and Colorado Department of Public Health & Environment by the University of Colorado Anschutz Community Epidemiology
2015 Prepared for the Colorado Department of Education, Colorado Department of Human Services, and Colorado Department of Public Health & Environment by the University of Colorado Anschutz Community Epidemiology
Number September 15, Abstract. Highlights. Overview
 Number 362 + September 15, 2005 DatainTables8,10,12,andAppendixtable4havebeenrevised. Numberscitedintextonpages3,4,and13havebeenrevised. Sexual Behavior and Selected Health Measures: Men and Women 15 44
Number 362 + September 15, 2005 DatainTables8,10,12,andAppendixtable4havebeenrevised. Numberscitedintextonpages3,4,and13havebeenrevised. Sexual Behavior and Selected Health Measures: Men and Women 15 44
Public Health Communications Awards
 Public Health Communications Awards APPLICATION: MOST INNOVATIVE CAMPAIGN CONTACT INFORMATION Jurisdiction Name: Solano County Health Services Contact Name: Cynthia Coutee Contact Title: Supervising, Communicable
Public Health Communications Awards APPLICATION: MOST INNOVATIVE CAMPAIGN CONTACT INFORMATION Jurisdiction Name: Solano County Health Services Contact Name: Cynthia Coutee Contact Title: Supervising, Communicable
The following report provides details about the strategic plan and the main accomplishments from the 2015 plan.
 INTRODUCTION In Fall 2014, the Denver Public Health Strategic Planning Committee worked with staff and partners to develop the 2015-2017 Strategic Plan. From this plan, the annual 2015 implementation plan
INTRODUCTION In Fall 2014, the Denver Public Health Strategic Planning Committee worked with staff and partners to develop the 2015-2017 Strategic Plan. From this plan, the annual 2015 implementation plan
KNOWLEDGE OF HIV/AIDS AND OTHER SEXUALLY
 KNOWLEDGE OF HIV/AIDS AND OTHER SEXUALLY 8 TRANSMITTED INFECTIONS 8.1 KNOWLEDGE OF HIV/AIDS One of the realms of policy and law agreed to at the Cairo and Beijing conferences is to develop integrated service,
KNOWLEDGE OF HIV/AIDS AND OTHER SEXUALLY 8 TRANSMITTED INFECTIONS 8.1 KNOWLEDGE OF HIV/AIDS One of the realms of policy and law agreed to at the Cairo and Beijing conferences is to develop integrated service,
Strategic Plan to End Homelessness
 Strategic Plan to End Homelessness Approved 2013, Updated October 2016 Ohio Balance of State Continuum of Care 1 Homelessness in the Ohio BoSCoC When most people imagine what homelessness looks like, they
Strategic Plan to End Homelessness Approved 2013, Updated October 2016 Ohio Balance of State Continuum of Care 1 Homelessness in the Ohio BoSCoC When most people imagine what homelessness looks like, they
Ensuring Family Voice While Navigating Multiple Systems: The family team meeting strategy in supportive housing. Challenge
 Notes from the Field Series 1, Issue 3 Ensuring Family Voice While Navigating Multiple Systems: The family team meeting strategy in supportive housing Challenge Families facing severe housing instability
Notes from the Field Series 1, Issue 3 Ensuring Family Voice While Navigating Multiple Systems: The family team meeting strategy in supportive housing Challenge Families facing severe housing instability
Genital Human Papillomavirus (HPV)
") Genital Human Papillomavirus (HPV) At least 50% of sexually active women and men will get it. Most will not know they have it. Alaska Native Women: Learn what HPV is, and what you can do to protect yourself
Genital Human Papillomavirus (HPV) At least 50% of sexually active women and men will get it. Most will not know they have it. Alaska Native Women: Learn what HPV is, and what you can do to protect yourself
HIV/AIDS. National Survey of Teens on PUBLIC KNOWLEDGE AND ATTITUDES ABOUT HIV/AIDS
 PUBLIC KNOWLEDGE AND ATTITUDES ABOUT HIV/AIDS National Survey of Teens on THE KAISER FAMILY FOUNDATION 2000 HIV/AIDS Summary Teens today are concerned about the impact of the HIV/AIDS epidemic on the nation
PUBLIC KNOWLEDGE AND ATTITUDES ABOUT HIV/AIDS National Survey of Teens on THE KAISER FAMILY FOUNDATION 2000 HIV/AIDS Summary Teens today are concerned about the impact of the HIV/AIDS epidemic on the nation
Lessons Learned from HPV Vaccine Study Among Young Adult Women and Men
 Lessons Learned from HPV Vaccine Study Among Young Adult Women and Men Natalie Joseph, MD, MPH Assistant Professor of Pediatrics/Adolescent Medicine Boston University Medical Center Racial and ethnic differences
Lessons Learned from HPV Vaccine Study Among Young Adult Women and Men Natalie Joseph, MD, MPH Assistant Professor of Pediatrics/Adolescent Medicine Boston University Medical Center Racial and ethnic differences
Chapter 7 Reproductive Tract Infections and HIV/AIDS
 Chapter 7 Reproductive Tract Infections and HIV/AIDS Introduction Reproductive Tract Infections (RTIs) Infections caused by a variety of organisms that affect upper and/or lower reproductive tracts Most
Chapter 7 Reproductive Tract Infections and HIV/AIDS Introduction Reproductive Tract Infections (RTIs) Infections caused by a variety of organisms that affect upper and/or lower reproductive tracts Most
Evaluating the impact of an HIV& AIDS Community Training Partnership Programme (CTPP) in five diamond mining communities in South Africa
 in five diamond mining communities in South Africa") Evaluating the impact of an HIV& AIDS Community Training Partnership Programme (CTPP) in five diamond mining communities in South Africa L. Rispel, 1 K. Peltzer, 2 N. Nkomo 3, B.Molomo 4 1 Centre for Health
Evaluating the impact of an HIV& AIDS Community Training Partnership Programme (CTPP) in five diamond mining communities in South Africa L. Rispel, 1 K. Peltzer, 2 N. Nkomo 3, B.Molomo 4 1 Centre for Health
HIV/AIDS Ministry in Churches
 HIV/AIDS Ministry in Churches Educating the Church About HIV/AIDS AIDS Is one of the diseases of the End-Time AIDS causes much preventable death and suffering In our region of the world: (North America,
HIV/AIDS Ministry in Churches Educating the Church About HIV/AIDS AIDS Is one of the diseases of the End-Time AIDS causes much preventable death and suffering In our region of the world: (North America,
CHAPTER 29 HIV/AIDS BOARD OF HEALTH ROLE AT A GLANCE
 CHAPTER 29 HIV/AIDS BOARD OF HEALTH ROLE AT A GLANCE Have an understanding of who can be affected by HIV/AIDS in your community and be able to address any concerns of the general public as well as people
CHAPTER 29 HIV/AIDS BOARD OF HEALTH ROLE AT A GLANCE Have an understanding of who can be affected by HIV/AIDS in your community and be able to address any concerns of the general public as well as people
Global health sector strategies on HIV, viral hepatitis and sexually transmitted infections ( )
") Regional Committee for Europe 65th session EUR/RC65/Inf.Doc./3 Vilnius, Lithuania, 14 17 September 2015 2 September 2015 150680 Provisional agenda item 3 ORIGINAL: ENGLISH Global health sector strategies
Regional Committee for Europe 65th session EUR/RC65/Inf.Doc./3 Vilnius, Lithuania, 14 17 September 2015 2 September 2015 150680 Provisional agenda item 3 ORIGINAL: ENGLISH Global health sector strategies
Howard Brown Health Center
 Howard Brown Health Center STI Annual Report, Background Howard Brown is the largest LGBT health center in the Midwest, providing comprehensive medical and behavioral health services to over, adults and
Howard Brown Health Center STI Annual Report, Background Howard Brown is the largest LGBT health center in the Midwest, providing comprehensive medical and behavioral health services to over, adults and
State of Iowa Outcomes Monitoring System
 State of Iowa Outcomes Monitoring System THE IOWA CONSORTIUM FOR SUBSTANCE ABUSE RESEARCH AND EVALUATION Year 17 Annual Outcome Evaluation Trend Report November 2015 With Funds Provided By: Iowa Department
State of Iowa Outcomes Monitoring System THE IOWA CONSORTIUM FOR SUBSTANCE ABUSE RESEARCH AND EVALUATION Year 17 Annual Outcome Evaluation Trend Report November 2015 With Funds Provided By: Iowa Department
County of Ventura Homeless Survey
 2011 County of Ventura Homeless Survey May 2011 Acknowledgements This report was made possible by the efforts of community volunteers and staff of organizations that provide services for persons who are
2011 County of Ventura Homeless Survey May 2011 Acknowledgements This report was made possible by the efforts of community volunteers and staff of organizations that provide services for persons who are
What do I need to know about HIV and sex? What are my responsibilities and choices?
 Patient and Family Education HIV: Teens and Sex This handout has information about sex and HIV. This handout answers common questions you might ask about sex. It is important for you to talk to your parents
Patient and Family Education HIV: Teens and Sex This handout has information about sex and HIV. This handout answers common questions you might ask about sex. It is important for you to talk to your parents
Community Health Improvement Plan
 Community Health Improvement Plan Methodist University Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee, with 1,650
Community Health Improvement Plan Methodist University Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee, with 1,650
Community-Level HIV Prevention Trials: Design, Implementation and Effectiveness
 Community-Level HIV Prevention Trials: Design, Implementation and Effectiveness Kathleen J. Sikkema, Ph.D. Duke University Professor of Psychology and Neuroscience Research was supported by grant R01-MH42908
Community-Level HIV Prevention Trials: Design, Implementation and Effectiveness Kathleen J. Sikkema, Ph.D. Duke University Professor of Psychology and Neuroscience Research was supported by grant R01-MH42908
Glossary of Acronyms. AIDS - Acquired Immunodeficiency Syndrome. CDC - Centers for Disease Control and Prevention. DHS - Department of Health Services
 Acknowledgements This report was developed by the California Department of Health Services, Office of AIDS (DHS/OA) under cooperative agreement. U6/CCU965-- with support from the Centers for Disease Control
Acknowledgements This report was developed by the California Department of Health Services, Office of AIDS (DHS/OA) under cooperative agreement. U6/CCU965-- with support from the Centers for Disease Control
Introduction. Relationships. Condoms. HIV Testing. DC HIV Behavior Study #1. Here is what we learned:
 Heterosexual Relationships and HIV in Washington, DC GOVERNMENT OF THE DISTRICT OF COLUMBIA DEPARTMENT OF HEALTH Promote. Prevent. Protect. Introduction You re heterosexual. You re living in Washington,
Heterosexual Relationships and HIV in Washington, DC GOVERNMENT OF THE DISTRICT OF COLUMBIA DEPARTMENT OF HEALTH Promote. Prevent. Protect. Introduction You re heterosexual. You re living in Washington,
RACE, EVOLUTION, AND BEHAVIOR:
 RACE, EVOLUTION, AND BEHAVIOR: [Part 3] A Life History Perspective 2nd Special Abridged Edition Professor J. Philippe Rushton University of Western Ontario London, Ontario, Canada N6A 5C2 [Page 4] [Note:
RACE, EVOLUTION, AND BEHAVIOR: [Part 3] A Life History Perspective 2nd Special Abridged Edition Professor J. Philippe Rushton University of Western Ontario London, Ontario, Canada N6A 5C2 [Page 4] [Note:
Update Report # 45. Patterns of Sexual Behaviors and Sexual Risk among HIV Positive People in New York City
 Update Report # 45 Patterns of Sexual Behaviors and Sexual Risk among HIV Positive People in New York City Angela A. Aidala Mary Ann Chiasson Gunjeong Lee Center for Applied Public Health Joseph L. Mailman
Update Report # 45 Patterns of Sexual Behaviors and Sexual Risk among HIV Positive People in New York City Angela A. Aidala Mary Ann Chiasson Gunjeong Lee Center for Applied Public Health Joseph L. Mailman
AlcoholEdu for College
 for College Executive Summary January 2006 California State University, Chico SUMMARY OF KEY FINDINGS Following is a summary of the key findings from California State University s 2005 implementation of
for College Executive Summary January 2006 California State University, Chico SUMMARY OF KEY FINDINGS Following is a summary of the key findings from California State University s 2005 implementation of
Use of Acceptability Research for Development and Implementation of Microbicide Prevention Methods. Margaret Reynolds December 4th, 2004
 Use of Acceptability Research for Development and Implementation of Microbicide Prevention Methods Margaret Reynolds December 4th, 2004 Microbicides: Background Chemical products applied to vagina or rectum
Use of Acceptability Research for Development and Implementation of Microbicide Prevention Methods Margaret Reynolds December 4th, 2004 Microbicides: Background Chemical products applied to vagina or rectum
NATIONAL SURVEY OF YOUNG ADULTS ON HIV/AIDS
 NATIONAL SURVEY OF YOUNG ADULTS ON HIV/AIDS Kaiser Family Foundation November 30, 2017 Introduction More than three and a half decades have passed since the first case of AIDS. An entire generation has
NATIONAL SURVEY OF YOUNG ADULTS ON HIV/AIDS Kaiser Family Foundation November 30, 2017 Introduction More than three and a half decades have passed since the first case of AIDS. An entire generation has
Genital Human Papillomavirus (HPV)
") Genital Human Papillomavirus (HPV) At least 50% of sexually active women and men will get it. Most will not know they have it. Native Women: Learn what HPV is, and what you can do to protect yourself from
Genital Human Papillomavirus (HPV) At least 50% of sexually active women and men will get it. Most will not know they have it. Native Women: Learn what HPV is, and what you can do to protect yourself from
APPENDIX C YEAR ONE EVALUATION REPORT SOUTHERN NEVADA HEALTH DISTRICT GRANT 1 TP1AH July 1, 2015 June 30, 2016
 APPENDIX C YEAR ONE EVALUATION REPORT SOUTHERN NEVADA HEALTH DISTRICT GRANT 1 TP1AH000121-01-00 July 1, 2015 June 30, 2016 SNHD Staff Contributors: Anne Scully Health Educator Xavier Foster, M. Ed. Health
APPENDIX C YEAR ONE EVALUATION REPORT SOUTHERN NEVADA HEALTH DISTRICT GRANT 1 TP1AH000121-01-00 July 1, 2015 June 30, 2016 SNHD Staff Contributors: Anne Scully Health Educator Xavier Foster, M. Ed. Health
AIDS Foundation of Chicago Strategic Vision
 AIDS Foundation of Chicago Strategic Vision 2005-2007 Founded in 1985 by community activists and physicians, the AIDS Foundation of Chicago is a local and national leader in the fight against HIV/AIDS.
AIDS Foundation of Chicago Strategic Vision 2005-2007 Founded in 1985 by community activists and physicians, the AIDS Foundation of Chicago is a local and national leader in the fight against HIV/AIDS.
As a result of this training, participants will be able to:
 Addressing Prevention with HIV Positive Clients 1 Day Training This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result
Addressing Prevention with HIV Positive Clients 1 Day Training This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result
HIV AIDS and Other Infectious Diseases
 HIV AIDS and Other Infectious Diseases Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Chapter 1 - Introduction Despite the availability of a vaccine since
HIV AIDS and Other Infectious Diseases Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Chapter 1 - Introduction Despite the availability of a vaccine since
Australian Research Centre in Sex, Health & Society. EMBARGOED until am 4/8/09 Secondary Students and Sexual Health 2008
 Australian Research Centre in Sex, Health & Society EMBARGOED until 10.30 am 4/8/09 Secondary Students and Sexual Health 2008 Melbourne, Australia Sample 2002 2008 Jurisdictions All All School sectors
Australian Research Centre in Sex, Health & Society EMBARGOED until 10.30 am 4/8/09 Secondary Students and Sexual Health 2008 Melbourne, Australia Sample 2002 2008 Jurisdictions All All School sectors
Key Concepts Guide. Rev. March 2015 Page 1 of 13
 Key Concepts Guide Key concepts are main ideas. They convey big-picture ideas. Birth control is good at preventing pregnancy and Everyone has the right to say who touches their body and how are both key
Key Concepts Guide Key concepts are main ideas. They convey big-picture ideas. Birth control is good at preventing pregnancy and Everyone has the right to say who touches their body and how are both key
Arizona Youth Tobacco Survey 2005 Report
 Arizona Department of Health Services Arizona Department of Health Services Arizona Youth Tobacco Survey 25 Report November 26 Office of Tobacco Education and Prevention Program Prepared by: Evaluation,
Arizona Department of Health Services Arizona Department of Health Services Arizona Youth Tobacco Survey 25 Report November 26 Office of Tobacco Education and Prevention Program Prepared by: Evaluation,
HVTN 505 Study HIV Vaccine Candidate Not Effective
 Subscribe Unsubscribe HVTN 505 Study HIV Vaccine Candidate Not Effective The National Institute of Allergy and Infectious Diseases (NIAID) and the HIV Vaccine Trials Network have announced there will be
Subscribe Unsubscribe HVTN 505 Study HIV Vaccine Candidate Not Effective The National Institute of Allergy and Infectious Diseases (NIAID) and the HIV Vaccine Trials Network have announced there will be
HIV in the UK: Changes and Challenges; Actions and Answers The People Living With HIV Stigma Survey UK 2015 Scotland STIGMA SURVEY UK 2015
 HIV in the UK: Changes and Challenges; Actions and Answers The People Living With HIV Stigma Survey UK 2015 Scotland STIGMA SURVEY UK 2015 SCOTLAND The landscape for people living with HIV in the United
HIV in the UK: Changes and Challenges; Actions and Answers The People Living With HIV Stigma Survey UK 2015 Scotland STIGMA SURVEY UK 2015 SCOTLAND The landscape for people living with HIV in the United
Milk Taste Test. Prepared by Shelley Kuklish Epidemiologist. September 2008
 Milk Taste Test 2008 Prepared by Shelley Kuklish Epidemiologist September 2008 Table of Contents Executive Summary..3 Introduction...6 Methods.. 6 Results. 7 Conclusions.. 12 2 Executive Summary The purpose
Milk Taste Test 2008 Prepared by Shelley Kuklish Epidemiologist September 2008 Table of Contents Executive Summary..3 Introduction...6 Methods.. 6 Results. 7 Conclusions.. 12 2 Executive Summary The purpose
Comprehensive Substance Abuse Prevention Program Evaluation
 Comprehensive Substance Abuse Prevention Program Evaluation THE IOWA CONSORTIUM FOR SUBSTANCE ABUSE RESEARCH AND EVALUATION Comprehensive Substance Abuse Prevention Program Evaluation Annual Report 7/1/2013
Comprehensive Substance Abuse Prevention Program Evaluation THE IOWA CONSORTIUM FOR SUBSTANCE ABUSE RESEARCH AND EVALUATION Comprehensive Substance Abuse Prevention Program Evaluation Annual Report 7/1/2013
GENDER, RACE/ETHNICITY, SEXUAL ORIENTATION AND STI/HIV RELATED RISK AMONG YOUNG U.S. ADULTS 1
 GENDER, RACE/ETHNICITY, SEXUAL ORIENTATION AND STI/HIV RELATED RISK AMONG YOUNG U.S. ADULTS 1 Sanyu A Mojola and Bethany Everett Abstract Few studies consider the impact of combinations of identities,
GENDER, RACE/ETHNICITY, SEXUAL ORIENTATION AND STI/HIV RELATED RISK AMONG YOUNG U.S. ADULTS 1 Sanyu A Mojola and Bethany Everett Abstract Few studies consider the impact of combinations of identities,
HIV and AIDS: A Health Crisis for African Americans
 Fighting HIV among African Americans HIV is a crisis in African American communities, threatening the health, well-being and potential of African American men and women of all ages in the United States.
Fighting HIV among African Americans HIV is a crisis in African American communities, threatening the health, well-being and potential of African American men and women of all ages in the United States.
2008 Ohio State University. Campus Climate Study. Prepared by. Student Life Research and Assessment
 2008 Ohio State University Campus Climate Study Prepared by Student Life Research and Assessment January 22, 2009 Executive Summary The purpose of this report is to describe the experiences and perceptions
2008 Ohio State University Campus Climate Study Prepared by Student Life Research and Assessment January 22, 2009 Executive Summary The purpose of this report is to describe the experiences and perceptions
2017 Health Report ACHA-NCHA-II Data
 2017 Health Report ACHA-NCHA-II Data 2013 2017 TABLE OF CONTENTS Introduction...1 Demographics...2 Impediments to Academic Success...3 Alcohol...5 Interpersonal Violence...8 Mental Health...9 Nutrition
2017 Health Report ACHA-NCHA-II Data 2013 2017 TABLE OF CONTENTS Introduction...1 Demographics...2 Impediments to Academic Success...3 Alcohol...5 Interpersonal Violence...8 Mental Health...9 Nutrition
A Committee for a Better New Orleans Report The New Orleans Citizen Participation Project (NOLA CPP) May 2011
 May 2011") A Committee for a Better New Orleans Report The New Orleans Citizen Participation Project (NOLA CPP) May 2011 4902 Canal Street, Suite 300 New Orleans, LA 70119 (504) 267-4665 nolacpp@gmail.com www.nolacpp.wordpress.com
A Committee for a Better New Orleans Report The New Orleans Citizen Participation Project (NOLA CPP) May 2011 4902 Canal Street, Suite 300 New Orleans, LA 70119 (504) 267-4665 nolacpp@gmail.com www.nolacpp.wordpress.com
Needle and Syringe Programs - 17 October 2013
 Needle and Syringe Programs - 17 October 2013 ANCD Position Paper: Needle and Syringe Programs MEDIA RELEASE 17 October 2013 The Australian National Council on Drugs (ANCD) has today released a position
Needle and Syringe Programs - 17 October 2013 ANCD Position Paper: Needle and Syringe Programs MEDIA RELEASE 17 October 2013 The Australian National Council on Drugs (ANCD) has today released a position
HIV Housing Care Continuum Webinar 1 August 3, 2016
 Page 1 HIV Housing Care Continuum August 3, 2016 Rita Flegel: Hello and welcome. I'm Rita Flegel, the Director of HUD's Office of HIV/AIDS Housing. And presenting with me today is Amy Palilonis also from
Page 1 HIV Housing Care Continuum August 3, 2016 Rita Flegel: Hello and welcome. I'm Rita Flegel, the Director of HUD's Office of HIV/AIDS Housing. And presenting with me today is Amy Palilonis also from
Hosting a Film Viewing Guide
 Hosting a Film Viewing Guide This guide was adapted by the American Academy of Pediatrics (October 2018) from A Guide to Hosting a Film Viewing, created by The Ohio Partners for Cancer Control (OPCC) -
Hosting a Film Viewing Guide This guide was adapted by the American Academy of Pediatrics (October 2018) from A Guide to Hosting a Film Viewing, created by The Ohio Partners for Cancer Control (OPCC) -
Abstract. Keywords: Sexual behavior; oral sex; sexual orientation; National Survey of Family Growth
 Number 36, March 2011 Sexual Behavior, Sexual Attraction, and Sexual Identity in the United States: Data from the 2006-2008 National Survey of Family Growth By Anjani Chandra, PhD, William D. Mosher, PhD,
Number 36, March 2011 Sexual Behavior, Sexual Attraction, and Sexual Identity in the United States: Data from the 2006-2008 National Survey of Family Growth By Anjani Chandra, PhD, William D. Mosher, PhD,
Young Women and STDs: Are Physicians Doing Enough to Empower their Patients and Protect their Health?
 Young Women and STDs: Are Physicians Doing Enough to Empower their Patients and Protect their Health? A Survey of Young Women, Mothers, and Physicians about Sexually Transmitted Diseases (STDs) Introduction
Young Women and STDs: Are Physicians Doing Enough to Empower their Patients and Protect their Health? A Survey of Young Women, Mothers, and Physicians about Sexually Transmitted Diseases (STDs) Introduction
Responsibilities in a sexual relationship - Contact tracing
 P a g e 1 Responsibilities in a sexual relationship - Contact tracing This activity has been designed increase student familiarity with the NSW Health Play Safe website. Suggested duration: 50-60 minutes
P a g e 1 Responsibilities in a sexual relationship - Contact tracing This activity has been designed increase student familiarity with the NSW Health Play Safe website. Suggested duration: 50-60 minutes
LET S TALK about Sticking with your treatment plan
 LET S TALK about Sticking with your treatment plan HOW ONGOING HIV CARE HELPS YOU LIVE A LONGER AND HEALTHIER LIFE Your treatment plan is vital to your overall health (and to reducing HIV transmission)
LET S TALK about Sticking with your treatment plan HOW ONGOING HIV CARE HELPS YOU LIVE A LONGER AND HEALTHIER LIFE Your treatment plan is vital to your overall health (and to reducing HIV transmission)
Ryan White Part A Overview Kimberlin Dennis Melissa Rodrigo March 21, 2018
 Ryan White Part A Overview Kimberlin Dennis Melissa Rodrigo March 21, 2018 Part A Program = Partnership Regional HIV Planning Council Cuyahoga County Board of Health One Purpose Ryan White Legislation
Ryan White Part A Overview Kimberlin Dennis Melissa Rodrigo March 21, 2018 Part A Program = Partnership Regional HIV Planning Council Cuyahoga County Board of Health One Purpose Ryan White Legislation
Health Cognition & Behavior Lab
 Health Cognition & Behavior Lab UNC Men s Health Survey (2009) The UNC Men s Health Study was conducted via an online survey with a national sample of men ages 18-59 in January 2009. Preferred Citations:
Health Cognition & Behavior Lab UNC Men s Health Survey (2009) The UNC Men s Health Study was conducted via an online survey with a national sample of men ages 18-59 in January 2009. Preferred Citations:
4 Ways to Provide Housing and Healthcare to Homeless Persons Living with HIV/AIDS
 4 Ways to Provide Housing and Healthcare to Homeless Persons Living with HIV/AIDS White Paper / October 2016 702.605.6870 / support@clarityhs.com / www.clarityhumanservices.com / www.bitfocus.com EXECUTIVE
4 Ways to Provide Housing and Healthcare to Homeless Persons Living with HIV/AIDS White Paper / October 2016 702.605.6870 / support@clarityhs.com / www.clarityhumanservices.com / www.bitfocus.com EXECUTIVE
HIV, STDs, and TB: An Overview of Testing Results (1997)
") HIV, STDs, and TB: An Overview of Testing Results (1997) prepared for Delaware Department of Health and Social Services Division of Public Health by Edward C. Ratledge and Anne M. Gurchik Center for Applied
HIV, STDs, and TB: An Overview of Testing Results (1997) prepared for Delaware Department of Health and Social Services Division of Public Health by Edward C. Ratledge and Anne M. Gurchik Center for Applied
From Homeless to Housed. Housing is The Foundation for Wholeness.
 From Homeless to Housed Housing is The Foundation for Wholeness. Welcome to your Community Quarterly Meeting Introductions: What is your name? What is the church you attend, if any? What is your role at
From Homeless to Housed Housing is The Foundation for Wholeness. Welcome to your Community Quarterly Meeting Introductions: What is your name? What is the church you attend, if any? What is your role at