COMPREHENSIVE HIV/AIDS NEEDS ASSESSMENT 2014
|
|
|
- Neal King
- 6 years ago
- Views:
Transcription

1 COMPREHENSIVE HIV/AIDS NEEDS ASSESSMENT 2014 LAS VEGAS TGA RYAN WHITE PART A HIV/AIDS PROGRAM Modern Consultants Transforming Health Care Data into Solutions
2 COMPREHENSIVE HIV/AIDS NEEDS ASSESSMENT LAS VEGAS TGA RYAN WHITE PART A HIV/AIDS PROGRAM ACKNOWLEDGEMENTS This project is made possible by a grant from the U.S. Health Resources and Services Administration HIV/AIDS Bureau under Part A of the HIV/AIDS Treatment Extension Act, with support of the Ryan White Part A Planning Council and Clark County Social Services Ryan White Part A HIV/AIDS Program. Additionally, thank you to the Ryan White Part A service providers and consumers that participated in this project without whom this document would never have been possible. Page 1 of 123
3 TABLE OF CONTENTS SERVICE AREA... 3 Description of the Las Vegas Transitional Grant Area... 3 EXECUTIVE SUMMARY Introduction and Methodology Epidemiological Profile 4 Results....5 Suggestions.. 7 INTRODUCTION... 9 METHODOLOGY... 9 EPIDEMOLOGICAL PROFILE. 11 ASSESSMENT OF SERVICE NEEDS AND ASSESSMENT OF UNMET NEED/SERVICE GAPS Consumer In Care Survey Results 16 General Info..16 Education, Employment and Insurance.28 Household and Income..32 Access and Barriers to HIV Care.. 36 Mental Health and Substance Abuse...41 Sexual Health.46 Services and Service Needs.. 56 Consumer Focus Group Results...65 Consumer Out of Care Survey Results 76 General Info, Testing and Health Status.. 76 Pregnancy, Substance Use and Mental Health...88 Service Needs 93 PROFILE OF PROVIDER CAPACITY AND CAPABILITY...95 RESOURCE INVENTORY 109 Consumer In Care Survey..Appendix A Consumer Out of Care Survey...Appendix B Provider Survey.Appendix C Page 2 of 123

4 SERVICE AREA Description of the Las Vegas Transitional Grant Area (TGA) The Las Vegas TGA is comprised of three counties Clark and Nye Counties in Nevada, and Mohave County, Arizona covering a vast area of 39,368 square miles that crosses state borders. As of December 31, 2013 there were a total of 7,885 persons living with HIV/AIDS (PLWH/A) in Clark and Nye County alone as reported by the Nevada State Health Division-HIV/AIDS Surveillance Program. They also reported that there were 4,091 persons living with AIDS (PLWA) in Clark and Nye County and 3,794 people living with HIV (PLWH) in Clark and Nye County as of December 31, The State of Arizona HIV/AIDS Surveillance Program listed the HIV/AIDS prevalence for Mohave County as of December 31, 2013 at 264 people. This brings the total of HIV/AIDS prevalence in the Las Vegas TGA to 8,149 as of December 31, Page 3 of 123
5 EXECUTIVE SUMMARY Introduction and Methodology The intent of the 2014 Comprehensive HIV/AIDS Needs Assessment is to aid the council in collecting data by identify service needs, gaps in care, barriers to care, and other important information reported by people living with HIV/AIDS throughout the Las Vegas TGA. This project was designed to include all five of the necessary components, as directed by HRSA, which brands a needs assessment comprehensive in nature. These five components are; an epidemiological profile to discuss the overall status of the epidemic in the TGA, an assessment of service needs which includes barriers to care as collected through the consumer survey, a resource inventory of organizations in the TGA that provide services to PLWH/A, a profile of provider capacity and capability that identifies the extent to which services are accessible and available for PLWH/A, and finally an assessment of unmet need and service gaps which brings together both quantitative and qualitative data on service needs including an assessment of those that know their HIV status but are not in care. All of these components together allow for a comprehensive approach to meeting the needs of local consumers. Qualitative and quantitative data was collected through three surveys and six focus groups. The Consumer In Care survey yielded 273 responses, the Consumer Out of Care survey yielded 51 responses, and the Provider Survey yielded 18 responses. All data was collected through a convenience based model via online through the web-based program survey monkey and/or on paper through the mail or at one of the ten Ryan White Part A funded agencies. Six focus groups were also held with four of those in Clark County, one in Mohave County Arizona, and one in Nye County Nevada. Of the Clark County groups; one was for MSM s only, one for men infected through heterosexual contact or drug use, one female group, and one non-specific group. Epidemiological Profile As of December 31, 2013 there were a total of 7,885 persons living with HIV/AIDS (PLWH/A) in Clark and Nye County alone as reported by the Nevada State Health Division-HIV/AIDS Surveillance Program. They also reported that there were 4,091 persons living with AIDS (PLWA) in Clark and Nye County and 3,794 people living with HIV (PLWH) in Clark and Nye County as of December 31, The State of Arizona HIV/AIDS Surveillance Program listed the HIV/AIDS prevalence for Mohave County as of December 31, 2013 at 264 people. This brings the total of HIV/AIDS prevalence in the Las Vegas TGA to 8,149 as of December 31, Page 4 of 123
6 Results Consumer In Care Survey With regard to service needs the Consumer In Care survey clients were provided a list of services and asked to check the 10 most important services that help them manage their HIV diagnosis. The top ten services were listed as; 1. Dental care 2. Vision 3. Food Assistance 4. Outpatient/Ambulatory Medical Care 5. Medication Assistance 6. Emergency Financial Assistance 6. Housing Assistance 7. Transportation 8. Case Management 9. Nutrition Services 10. Health Insurance Assistance Each focus group was supplied with this information and asked if they agree or disagree. All but one group disagreed and provided their own ranking with medical care and/or medications listed in the number one spot. The female group however agreed with this list and supported the ranking with comments such as, it depends on where you are at in your life and what s important to you at that moment. When looking at year over data with regard to this same question, for the first time Outpatient/Ambulatory Medical Care was not ranked as the most important services to clients to help them manage their HIV/AIDS status. The number one most important service that clients indicated was Dental Care/Oral Healthcare followed by Vision services and then Food Bank/Food Vouchers with Outpatient/Ambulatory Medical Care ranked as the 4th most important service followed by HIV/AIDS medication. Additionally, this could be due to the new healthcare reform policies allowing clients to access medical care through another funding source such as Medicaid or health insurance. Whereas there may not be other funding sources to cover their dental care needs. When clients were asked about their barriers to accessing care reported reasons are; I didn t know where to go 20%, I was in denial 20%, didn t want anyone to know I have HIV 18%, I was too Page 5 of 123
7 nervous to see a doctor 12%, transportation issues 12%, I didn t feel sick 12%, and wait time was too long for an appointment 10%. Focus Groups Common themes in all focus groups included; issues with transportation whether it be proximity to care or keeping track of bus pass info/utilizing the bus pass system, eligibility paperwork along with how often eligibility has to be completed/along with the need for a more streamlined process and wait times for medical appointments while at the facility. Many clients state they wait for hours in the waiting room in addition to wait times in the exam room and then again to get discharged. Many clients also have a lack of understanding of the system of care and federal rules and regulations. Consumer Out of Care Survey When we asked respondents when they saw their HIV/AIDS physician last, just 16% said it was over 12 months ago. This means that this select few are the only people technically out of care, as defined as 12 months or more without medical care. However, each person that received the letter asking them to participate in the out of care survey had no record of any Ryan White service contacts in the previous 12 months or more dating back to This is a positive in the sense that these people are truly accessing medical care for their HIV/AIDS status somewhere. The down side is that this survey was tailored to collect data from those that are out of the HIV/AIDS medical care system completely. However, the questions and responses throughout this survey give insight into several aspects of care and services that are essential to the planning and shaping of the HIV/AIDS system of care as a whole. The Consumer Out of Care Survey respondents were asked what they think the ten most important services are that help people with HIV/AIDS manage their disease. They stated; 1. Medication 2. Outpatient/Ambulatory Medical Care 3. Food Bank/Home Delivered Meals 4. Dental Care 5. Health Insurance Assistance 6. Vision 6. Emergency Financial Assistance 7. Transportation 8. Mental Health Services 9. Housing Services 10. Specialty Care Page 6 of 123
8 Provider Survey The providers were also asked to check the ten most important services that they think help their clients manage their HIV status. Their answers included; 1. Medication 2. Outpatient/Ambulatory Medical Care 3. Transportation 4. Mental Health 5. Dental Care 6. Case Management 7. Specialty Care 7. Early Intervention Services 8. Vision 8. Health Insurance Continuation 8. Substance Abuse 8. Emergency Financial Assistance 9. Food Bank/Home Delivered Meals 9. Housing Assistance 10. HIV and Health Classes 10. Outreach 10. Psychosocial Support Providers were asked what they see as the three most pressing things that their clients are in need of. Their answers were; transportation, medication, and housing. When asked about barriers to care and new and emerging trends providers are seeing in the community, they indicated a high level of confusion regarding their healthcare options including enrollment in Medicaid as well as more transgender individuals seeking services. Suggestions There are a few issues that may need to be addressed within the client community. Many clients expressed an overall misunderstanding of the Ryan White system of care as far as where the money comes from, who receives it, and how it is divided amongst providers for service delivery. Also, there is a general lack of knowledge, or lack of sharing information, regarding federal guidelines that come along with federal dollars and how each service must be tied to a medical outcome. This could be addressed through more presentations to clients, educational question and answer groups, and possibly printed information. Page 7 of 123
9 Transportation may need to be addressed with regard for the HRSA requirement that all services be tied to a medical outcome and how difficult and sometimes complicated that can be when issuing bus passes. The eligibility process was also a topic of passion for many with the request for less paperwork and a more streamlined eligibility process especially amongst all Ryan White parts. As a more streamlined process has been visited in the past perhaps all Ryan White parts could benefit from ongoing communication about this issue. Additionally, stigma is a huge concern for many clients as we can see from the surveys and focus groups. Many clients report feeling ashamed and don t want to share their status. Some clients also report feeling this from providers in the HIV community. Ongoing education in the community is vital to combat this stigma. Finally, wait times for medical appointments while on premises. Clients report waiting up to three hours at times with an actual face to face time of less than ten minutes. Perhaps scheduling could be reviewed as a source of this issue. Increasing wait times discourage clients from accessing medical care and could lead them to drop out of care entirely. Page 8 of 123
10 INTRODUCTION The Ryan White Planning Council of the Las Vegas TGA is entrusted each year with prioritizing resources and allocating Ryan White dollars by service category, unrelated to who provides these services, to help meet the needs of those living with HIV/AIDS. In order to effectively plan for services and set funding priorities the Planning Council must base decisions on data provided by this needs assessment and other related documents regarding service utilization, gaps in care, barriers to care, and the needs and availability of services to PLWH/A. The intent of the 2014 Comprehensive HIV/AIDS Needs Assessment is to aid the council in collecting data by identify service needs, gaps in care, barriers to care, and other important information reported by people living with HIV/AIDS throughout the Las Vegas TGA. This project was designed to include all five of the necessary components, as directed by HRSA, which makes a needs assessment comprehensive in nature. These five components are; an epidemiological profile to discuss the overall status of the epidemic in the TGA, an assessment of service needs which includes barriers to care as collected through the consumer survey, a resource inventory of organizations in the TGA that provide services to PLWH/A, a profile of provider capacity and capability that identifies the extent to which services are accessible and available for PLWH/A, and finally an assessment of unmet need and service gaps which brings together both quantitative and qualitative data on service needs including an assessment of those that know their HIV status but are not in care. All of these components together allow for a comprehensive approach to meeting the needs of our consumers. METHODOLOGY This project consists of a three separate survey s for three different audiences. The first being the Consumer In Care Survey which was administered to clients currently accessing Ryan White Part A services yielding 273 respondents. A convenience sample approach was used to allow for a large number of responses without incurring the cost or time required for other more labor intensive methods. This self-administered survey was distributed and collected from clients at several HIV/AIDS service locations that are currently under contract to deliver Part A services. Survey researchers were on hand to assist clients with this process. Participants were provided a $20 stipend for their time. This survey was also available online via Survey Monkey for clients in rural areas or those unable to participate face to face. The goal of the Consumer In Care Survey was to pinpoint information from our consumer base regarding diagnosis, mode of transmission, demographics, income/employment status, education, health insurance status, housing situation, co-infections, drug use, mental health, priorities within the service system, service barriers, gaps in care, service needs, and out of care status. The survey was Page 9 of 123
11 designed by the Modern Consultants research team and reviewed and approved by the Planning Council. Administering a survey on such a large scale produced data limitations that were somewhat minimized through the field teams one-to-one interaction with the clients. Limitations include; weekly sampling profiles were not in place to ensure adequate representation by emerging or priority populations, and time constraints limited survey data collection to a four week period restricting the number of respondents that had an opportunity to participate. The Consumer Out of Care Survey was administered via online through Survey Monkey and also through the mail yielding 50 responses. A list of clients that did not a Ryan White Part A service for twelve months or more was pulled from the client level data system CAREWare. Those clients were mailed a generic letter asking them to contact the survey team if they had interest in participating or visit the enclosed survey link to respond online. Participants were also provided a $20 stipend for their time. When designing the Consumer Out of Care Survey the Modern Consultants research team focused on medical care and medication adherence, reasons/motivation for falling out of care, reasons/motivation for missing medication doses, sexual health, overall health status, insurance status, and service needs in addition to demographic information. Limitations to the Out of Care Survey included difficulty targeting PLWH/A that were truly out of care. Although many clients had not accessed care through Ryan White Part A in twelve months or more many had enrolled in Medicaid or purchased private insurance through the healthcare exchange and were thus receiving medical care for their HIV/AIDS diagnosis. Finally, the Provider Survey was administered to all Ryan White Part A employees at each currently funded Part A agency in the TGA. This survey was administered online via Survey Monkey and yielded 18 respondents. It was designed to collect data from a broad spectrum of employees that interact on different levels with consumers. Providers were asked questions relating to funding streams, client transportation, hours of operation, wait times, capacity and development needs, emerging issues/trends, funding and training needs, and barriers to care for clients accessing services in addition to barriers providers face when administering services. No specific limitations to data collection were noted for the provider survey. Focus groups were also conducted as a means of gathering supportive qualitative data. Six focus groups were held with four of those in Clark County, one in Mohave County Arizona, and one in Nye County Nevada. Of the Clark County groups; one was for MSM s only, one for men infected through Page 10 of 123
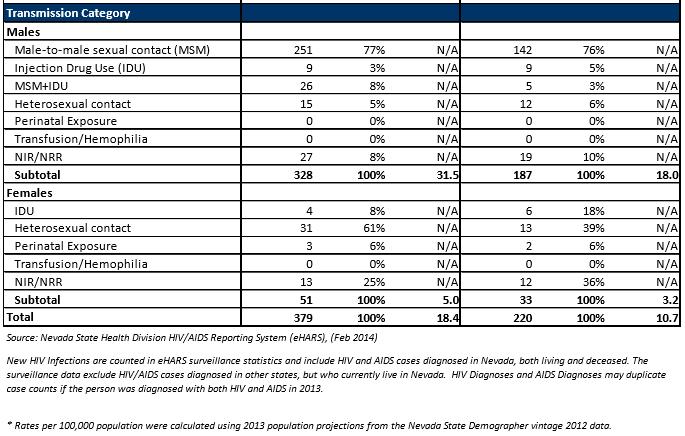
12 heterosexual contact or drug use, one female group, and one non-specific group. A group was also scheduled for transgender individuals but unfortunately no one came. EPIDEMOLOGIAL PROFILE The Nevada State Health Division HIV/AIDS Surveillance Program reported that as of December 31, 2013 there were 7,808 PLWH/A in Clark County alone and an additional 77 PLWH/A in Nye County for a total of 7,885 PLWH/A in the southern Nevada region. The State of Arizona HIV/AIDS Surveillance Division reported an HIV/AIDS prevalence of 264 in Mohave as of December 31, This brings the total of PLWH/A in the Las Vegas TGA to 8,149 as of December 31, In 2013 there were 379 new HIV infections reported in Clark and Nye County with 328 of those being male and 51 female. New diagnosis were predominately in the White, non-hispanic population with 140, followed by the Hispanic population with 117, Black, non-hispanic with 93, and Asian/Hawaiian/Pacific Islander 17. Male to male sexual contact (MSM) continues to be the primary mode of transmission in Clark and Nye County representing 251 of all new infections which is an astounding 77% of all new infections for This is followed by MSM+IDU (injection drug user) at 26 and 8%, Heterosexual contact with 46 and 12%, and IDU with 13 or 3% respectively. New diagnosis were predominately in the age range at 132 and 35%, followed by at 86 and 23%, at 69 and 18%, and at 60 and 16% respectively. New AIDS diagnosis in 2013 for Clark and Nye Counties followed somewhat of a similar trend. Total new AIDS diagnosis in the area were 220 for Males represented 85% of all new AIDS diagnosis and females just 15%. With regard to race/ethnicity the White, non-hispanic population represented 35% of new cases, Black non-hispanic 30%, Hispanic 28% and Asian/Hawaiian/Pacific Islander 5%. MSM also dominated new AIDS diagnosis with 76% in 2013 followed by Heterosexual contact at 11%, IDU at 6% and MSM at 5%. With regard to age the majority, 27%, are 25-34, 24% in the age bracket, and 23% are 45-54, finally 14% respectively. Incidence and prevalence are primarily in the over 45 and year age bracket in Mohave County with the vast majority being White, not Hispanic, male, and MSM. Epidemiological data can be found in the following tables for 2013 which include gender, risk factor, age at diagnosis, and race/ethnicity. Unfortunately due to the differences between states and reporting methods with regard to subgroup headings there is not an all-encompassing table for the entire TGA however, Clark and Nye County are combined. Page 11 of 123


13 Page 12 of 123


14 Page 13 of 123

15 Page 14 of 123
16 Demographic Group/Exposure Category Age at Diagnosis (Years) Race/Ethnicity AIDS Incidence AIDS Incidence Percentage HIV Incidence HIV Incidence Percentage AIDS Prevalance AIDS Prevalence Percentage HIV Prevalence HIV Prevalence Percentage <13 years 0 0% 0 0% 0 0% 0 0% years 0 0% 0 0% 0 0% 1 0% years 4 80% 4 50% 32 22% 44 38% 45 + years 1 20% 4 50% % 72 62% Unknown 0 0% 0 0% 0 0% 0 0% Total % % % White, not Hispanic 4 80% 7 88% % 88 75% African-American, not Hispanic 1 20% 1 12% 2 1% 8 7% Hispanic 0 0% 0 0% 14 10% 12 10% Asian/Pacific Islander 0 0% 0 0% 0 0% 2 2% American Indian/Alaska Native 0 0% 0 0% 9 6% 4 3% Multi-race /Other 0 0% 0 0% 2 1% 3 3% Total 5 100% 8 100% % % Gender Exposure Category Mohave County Arizona Male 4 80% 8 100% % 89 76% Female 1 20% 0 0% 18 12% 28 24% Total 5 100% 8 100% % % Men who have sex with men 3 60% 6 75% 76 52% 49 42% Injection drug users 1 20% 0 0% 20 14% 23 20% Men who have sex with men and inject drugs 0 0% 0 0% 31 21% 18 15% Hemophilia/coagulation Disorder 0 0% 0 0% 0 0% 0 0% Heterosexuals 0 0% 0 0% 15 10% 11 9% Receipt of blood transfusion, blood components or tissue 0 0% 0 0% 1 1% 1 1% Adult/Other 0 0% 0 0% 0 0% 0 0% Risk not reported or identified 1 20% 2 25% 4 3% 14 12% Mother with/at risk for HIV Infection 0 0% 0 0% 0 0% 1 100% Total 5 100% 8 100% % % Data provided by the State of Arizona HIV/AIDS Surveillance Program as of December 31, Page 15 of 123


17 ASSESSMENT OF SERVICE NEEDS and ASSESSMENT OF UNMET NEED/SERVICE GAPS Consumer In Care Survey Results The Consumer In Care Survey gathered an array of information in order to identify trends and common themes among PLWH/A. Of the 273 completed survey s 40 of them were in Spanish. Respondent s answers can be found in the tables and charts below. Many questions have been crosstabulated for more in depth analysis. General Information The majority of respondents indicated that they are asymptomatic with nearly 16% having received an AIDS diagnosis which is defined as a CD4 count <200 OR being diagnosed with an opportunistic infection. The majority of respondents were told of their HIV diagnosis in a hospital or emergency department setting (22%), followed by private doctors office (20%), and local clinic or health care center (17%). One person indicated that they took a home HIV test. Of the 11% that indicated other answers included; immigration office, donating blood or plasma, homeless shelter, prison or jail, going into the military and purchasing life insurance. Page 16 of 123


18 Most respondents (49%) indicated they found out they were HIV positive in Clark County Nevada, with just over 40% indicating they were in a state other than Nevada or Arizona. Nearly 2% of our respondents were tested internationally. Page 17 of 123
19 Respondents were asked what year they were diagnosed. There is a large spike in 2000 when 16 respondents indicated they were diagnosed and again a spike in 2013 when 20 respondents indicated they were diagnosed. Year of Year of Year of Diagnosis Response Percentage Diagnosis Response Percentage Diagnosis Response Percentage % % % % % % % % % % % % % % % % % % % % % % % % % % % % % % % % % Total % Page 18 of 123
20 Respondents were also asked how old they were at the time of diagnosis. This chart illustrates that the majority found out about their diagnosis in their 30 s. Twelve were under 20 when diagnosed, 77 were diagnosed in their 20 s, 90 in their 30 s, 51 in their 40 s and 21 diagnosed at 50 or older. Age at Diagnosis Age at Response Diagnosis Response Age at Diagnosis Response Page 19 of 123


21 With regard to mode of transmission, the majority of respondents report they were infected by having sex with a man followed by having sex with a woman and don t know. Comments include; domestic violence, rape and biohazard material. Page 20 of 123



22 The Black or African American population claimed 37% of respondents followed by the White or Caucasian population at 30% and the Hispanic or Latino/a population at 24%. Comments include Creole and Biracial. The majority of our respondents are male at 68%, 28% female with just under 2% indicating they are transgender. Page 21 of 123




23 When gender and mode of transmission are cross-tabulated we see that 61% of respondents are MSM and 35% contracted HIV through heterosexual contact. Our respondents are 70% male and 30% female when asked what sex they were assigned at birth. Page 22 of 123


24 When asked about current age the majority are currently in their 40 s and 50 s. Page 23 of 123

25 The vast majority of respondents report being single at 61% followed by married at 11% and have a domestic partner at 9%. Not married but living with a partner and divorced were tied with each at 5.28%. The number of children our respondents reported varied greatly with the vast majority, 118 or 50%, reporting that they have no children followed by 17% or 40 that report they have 2. Eleven percent report they have 3, 10% report they have 1, 2% report 5, and 3% report 6. Just one person reported having 7 or more children. Number of Children Response Percentage % % % % % 5 4 2% 6 7 3% 7 1 0% Total % Page 24 of 123
. Respondents were asked if they had ever been diagnosed with any of the following infections.")

26 Nearly half of respondents consider themselves to be Straight/heterosexual (48%), followed by Gay/homosexual (36%), with the third largest category indicating Bisexual (9%). Respondents were asked if they had ever been diagnosed with any of the following infections. The majority, 22% chose prefer not to answer, with 17% indicating they had previously been diagnosed with Herpes, 15% Gonorrhea, 13% Hepatitis C, 12% Hepatitis B, 11% none of the above, 10% genital warts along with 10% Hepatitis A and 10% Chlamydia. HPV and TB came in the lowest at 9% and 4% respectively. Page 25 of 123



27 With the same list respondents were asked if they had been diagnosed with any of the following in the last 12 months. Again, the majority indicated prefer not to answer at 40% with none and don t know very close at 17% and 15%. Herpes and Hepatitis C were both 6%, with Syphilis and HPV at 5%, and the rest coming in at 3% or below. About 7% of respondents said they waited more than 6 months before they had a medical appointment with a doctor after diagnosis and under 1% stated they still have not had a medical appointment with a doctor. On the positive end almost half, 46%, said they got into medical care immediately after diagnosis while 16% waited less than a month and 17% waited 1-3 months. Page 26 of 123



28 To follow-up we asked respondents what barriers they faced while trying to get into medical care after diagnosis. The biggest roadblocks and issues were; not knowing where to go, in denial, not wanting anyone to know I have HIV, too nervous to see a doctor, transportation issues, and not feeling sick. Page 27 of 123

29 Education, Employment and Insurance Most of our respondents indicated they completed some college but did not receive a degree, 28%, followed by 26% that reported they completed high school or received their GED. When it comes to higher education less than 2% have a master s degree, less than 9% have a bachelor s degree, and less than 6% have an associate s degree. An astounding 7% of respondents or 19 people stated that they completed 8 th grade or less and just under 13% or 34 participants did not graduate high school. These varying education levels make it particularly challenging to ensure clients understand the care system especially the new health care laws in addition to prevention and safer sex practices. Page 28 of 123


30 When describing their current work situation 58% indicated that they are not working, while 12% work full-time and 17% work parttime. Less than 2% are selfemployed or have their own business and 7% work on and off jobs. Reasons for not working are reported as; Health reasons on disability at 43%, looking for a job 24%, Health reasons not on disability 13%, with Retired and Waiting for benefits tied at 7%. Student was indicated by 6% and Criminal background by 3%. Page 29 of 123


31 With the new healthcare laws unfolding it is imperative that Ryan White clients know their options for medical care to ensure no lapse in medical treatment occurs. Fortunately, 42% indicated that they have applied, qualified and received their Medicaid card. Unfortunately, 9% have applied for Medicaid but haven t received their card. The real target audience is the 6% or 17 people that answered No, I do not want to enroll in Medicaid or insurance at this time, the 7% or 19 that answered Not yet, I need help figuring out where to go/how to fill out an application, and the combined 7% that indicated Don t know or Prefer not to answer. Supporting comments from respondents include; V.A., I applied but make too much money, Already disabled before diagnosed, and Haven t applied but getting assistance. Page 30 of 123


32 Sixty-one percent of respondents indicated they are on Medicare or Medicaid at this time. Five percent indicated they have insurance through work, 2% are on COBRA, and 4% have health care through the Veterans Administration. Again the focus here is on the 11% or 29 people who indicated they have no insurance, 5% or 12 people that said they Don t know, and 3% or 7 people that said they Prefer not to answer. These are the people that may need assistance enrolling in Medicaid or purchasing insurance through the exchange. Many respondents commented Ryan White or Ryan White Part B which is not a form of insurance but a federal program that provides medical care and support services to those living with HIV/AIDS that don t qualify for other avenues of healthcare coverage. Other comments include; moving from California, had medical but no more, Tricare and ACCHS, and current plan recently ended. Page 31 of 123

33 Overall satisfaction with healthcare coverage regarding Medicaid or private health insurance was very high with 32% indicating services are Excellent; all services and medication covered, with 23% indicating Good; almost all services and medications are covered, Average; most services and medications covered was reported by 14%, with Very poor; very few services and medications are covered reported by 3%. Household and Income When asked about their current housing situation the majority reported that they rent/own an apartment, house, condominium, or mobile home, 15% said they live with family, while 7% report they stay with friends and 2% reside in military housing. Of serious concern are those that report that they are homeless or live on the street at just under 4%, the 2% that live in shelters, 2% that live in a halfway house or drug treatment program, and 2% that live in a weekly or daily motel or single room occupancy hotel. Without stable housing these consumers at times place medical care and medication regimens on the back burner as they strive to keep a roof over their head and meet their physical needs. Comments include; Casa de Esperanza, HUD housing, TBRA Housing Authority, senior housing, rent a room, almost on the street and homeless. Housed by HOPWA, and live with lifepartner, who rents a home. Page 32 of 123


34 Eighteen percent or 48 respondents indicated that they have been homeless in the past 6 months, 3% checked prefer not to answer. Respondents were also asked how many people live in their household. The chart below indicates their responses. Numb e r o f Pe o p le Re sp o nse Page 33 of 123



35 With regard to zip code, the majority of respondents live in the heart of the Las Vegas valley with the 89101, 89104, and indicated most frequently. Page 34 of 123


36 Total household income can be seen in the chart above. The majority of respondents indicated that their total household income for last year was less than $10,000 followed by between $10,001 and $20,000 with a large portion indicating $0. Over half reported that they need help paying rent or mortgage expenses every month with just 32% saying they can make expenses on their own. Page 35 of 123

37 Monthly income and assistance is across the board with nearly half reporting they receive food stamps. A large portion are also on SSDI 22%, SSI 20%, and rental subsidy/section 8 at 15%. Comments include; I receive from AFAN, HOPWA for housing, applied but lost it HUD, employee disability through job, SS Retirement, gas vouchers, have transitioned from SSI to SSI & SSA, food bank assistance, Ryan White dental, Social Security, small retirement benefit, make $600 gross per month playing piano at a local dining room, and rental income. Access and Barriers to HIV Care When asked about their overall health the majority of respondents had a positive outlook. Just 11% or 29 people stated poor, and under 2% said don t know. Fair and good were nearly tied at 27% and 29% respectively. Excellent and very good were tied at 16%. Overall, well over half or 61% reported their health is good, very good, or excellent. Page 36 of 123



38 The overwhelming majority indicated that they received HIV/AIDS related medical care during the last 12 months at 84%, with just 12% indicating they had not. Four percent said they didn t know and 3 people declined to answer. A follow-up question was asked regarding the amount of medical care they received. Sixty-three percent said I received enough medical care with 23% indicating I need MORE medical care than I received. Again, 6% did not receive any medical care in the last 12 months with 3% indicating don t know, 3% prefer not to answer, and 3% say it doesn t apply. Page 37 of 123

39 A list was provided of reasons one might not seek out medical care. The biggest reason is don t know, followed by they couldn t get an appointment and not knowing where to go. Other top choices are no transportation, depression or mental health challenges, can t afford it, and not feeling sick. Several comments were also included which are; no Medicaid, very bad access could not get a lab so I could get meds, I had no problems, no insurance, no gas, time, I have HIV care at north country, and Humana Primary Care Dr's are good. It would be more helpful to see my HIV Dr. in Las Vegas. The Ryan White program is amazing it's hard to schedule last minute appointments to Las Vegas because the schedule is full. Limiting access to the HIV Dr. This program is amazing and contributes to my well-being greatly. However, I have full-blown AIDS and would prefer my HIV Dr. manage my care. How could I get a last minute trip to the HIV Dr. In Las Vegas? Without creating problems for everyone else?. With regard to where they regularly receive their HIV/AIDS related medical care, 1% or 3 people indicated the Emergency Room which is very costly and burdensome to the overall healthcare system. About 5% access care through the VA and 18% through a private physician s office, which would be through a pay source other than Ryan White. Over half or 62% presumably receive their regular medical care through Ryan White funding as they indicated an HIV clinic such as UMC Wellness Center or Community Outreach Medical Center, with 6% stating they visit another type of Page 38 of 123


40 community clinic for their HIV care. Comments include: Faces Place in New Orleans Louisiana, I am a new resident from Florida, and Avella. Participants were asked how often they are supposed to take their medication each day followed by how many pills they are supposed to take each day. Page 39 of 123


41 Almost half of participants (49%) reported that they hadn t missed any doses of their HIV medication in the last month. However, an overwhelming 10% state they had missed more than 4, with 3% missing 4, 4% missing 3 doses, 10% missing 2, and 12% missing one dose. The leading reasons for not taking their prescribed medications is having trouble remembering to take them and not feeling sick. Some clients also report that they can t afford them, 5%, which should be addressed as the ADAP program should be able to assist them depending on their situation. Other reasons are, I don t know where to get them and I m on a break from taking my HIV Page 40 of 123


42 medication, decided by myself. Comments include; need to find a doctor asap, bad refills!, and my blood type is pharmaceutical. Mental Health and Substance Abuse Clients were asked, Over the past two weeks, how often have you been bothered by any of the following programs?. These questions were adapted from PRIME-MD 1. These questions come from the Primary Care Evaluation of Mental Disorders screening questionnaire for depressive symptoms. Twenty percent of respondents indicated that they feel tired or have little energy nearly every day which could be related to a variety of factors including the disease process, medication side effects or their mental health. 1 Copyright 2012 Prime MD. All Rights Reserved. Page 41 of 123

43 Little interest or pleasure in doing things. Feeling down, or depressed, or hopeless. Trouble falling or staying asleep or sleeping too much Feeling tired or having little energy. Poor appetite or overeating Feeling bad about yourself, or that you are a failure, or have let yourself or your family down Trouble concentrating on things, such as reading the newspaper or watching television Moving or speaking so slowly that other people could have noticed. Or the opposite-being so fidgety or restless that you have been moving around a lot more than usual Trouble falling or staying asleep or sleeping too much was answered nearly every day by 20% with trouble concentrating on things, such as reading the newspaper or watching television by 15%. Nearly 14% indicated nearly every day they feel down or depressed or hopeless, and 12% also stated nearly every day they have a poor appetite or are overeating. Page 42 of 123


44 Nearly half, 45%, of respondents said they have accessed mental health services during the last 12 months. Seven percent say they have been hospitalized for mental health reasons in the last 12 months. Thirty-one percent said they have been prescribed medicine for mental health reasons in the last 12 months. Page 43 of 123




45 When asked about substance use, 5% say they have been in treatment in the last 12 months, with 1% that preferred not to answer, and just under 1% that said don t know. The following questions are from the C.A.G.E. questionnaire, a screening test for alcohol dependence 2. Just 4% indicated that they feel annoyed by people complaining about their drinking. Twelve percent reported they felt they need to cut down on their drinking. Eight percent said they feel guilty about their drinking, with 5% that said they drink an eye-opener in the morning to relieve the shakes. 2 Counseling Resource Mental Health Library Page 44 of 123
 at 18%, and meth at 7%. The comment listed states, I drink one to 4 drinks a month at the most.")

46 The most widely used drug amongst this group is reported to be tobacco products at 46%, alcohol at 32%, marijuana (non-medical use) at 18%, and meth at 7%. The comment listed states, I drink one to 4 drinks a month at the most. When asked if they have a desire to stop using; 13% said no, 9% said yes, I am currently drug free and in recovery, 7% said yes, and I am taking steps to do so, and 5% said yes, but I have not started to work on it. Page 45 of 123

47 Thirty-two percent of respondents said that they smoked cigarettes every day during the past 30 days. Seven percent said they smoked days in the last 30 days, 4% said 1-2 days, 3% said days, and 1% said 6-9 days, with 1% at 3-5 days. Twenty-four percent said they did not smoke at all. Sexual Health The following set of questions are regarding our participant s sexual health. They were asked if they engaged in sexual activity with another person in the last 12 months. Forty-six percent reported yes, 43% no, 9% indicated they prefer not to answer, and 1% said don t know. Page 46 of 123


48 Regarding oral sex practices, 27% report they didn t have oral sex in the last 12 months. Of those that engaged in this type of sex 14% stated they never used a condom, 24% reported they always used a condom, 6% said often used a condom, 4% reported they sometimes used a condom, and 4% rarely used a condom. This question was then cross-tabulated with race/ethnicity, those that reported they rarely or never used a condom were primarily Native Hawaiian or Pacific Islander, White or Caucasian, Black or African American, and Asian populations. Page 47 of 123


49 The chart below illustrates the number breakdown of this crosstabulation so that you can see the actual number in relation to the percentage. From this we can see that condom use for this type of sex was very low in the White or Caucasian community and the Black or African American community. It was also very high in the Hispanic and Black or African American communities. Page 48 of 123


50 This question was also crosstabulated with mode of transmission. Those that reported they rarely use a condom during this type of sex are from the MSM, heterosexual female and IDU communities as those that reported having sex with a man were primarily MSM. Those that reported they rarely used a condom were from the having sex with a transgender individual mode of transmission group which in reality was one individual. Many respondents also reported they always used condoms and that was primarily from the having sex with a woman mode of transmission group. Page 49 of 123


51 When asked about vaginal sex; 30% said they didn t have this type of sex, 30% always used a condom, 7% never used a condom, 4% said they sometimes used a condom, and 3% said they rarely used a condom. When cross-tabulated with race/ethnicity, 50% of the Native Hawaiian/Pacific Islander population that reported having this type of sex said they never used a condom which in reality was just one individual. In the Black or African American community 10 out of 100 individuals reported they never used a condom while engaging in this type of sex. In the Caucasian or White community 6 out of 80 respondents said they never used a condom. Page 50 of 123

52 Again the chart below illustrates the specific numbers associated with those percentages. Those that reported they never used a condom while engaging in this type of sex were primarily in the having sex with a man mode of transmission group. Page 51 of 123


53 When asked about anal sex practices; 37% reported they did not have this type of sex, 6% said they never used a condom, 4% reported they rarely used a condom, 3% said they sometimes used a condom, 2% often used a condom, and 27% said they always used a condom. Page 52 of 123
54 In the White or Caucasian population 8 out of 80 said they never used a condom when engaging in this type of sex while 5 out of 100 Black or African participants also said they never used a condom during this sex practice. Nearly half, 43% or 28 out of 65, of Hispanic respondents indicated they always used a condom while engaging in anal sex. Page 53 of 123

55 When cross-tabulated with mode of transmission, 8% or 14 out of 168 that contracted HIV through having sex with a man reported they never used a condom when engaging in this practice. Five percent or 2 out of 39 that engaged in this type of sexual activity that were infected by having sex with a woman also reported they never used a condom during anal sex. The chart below details further the specifics. When asked if they would like more information on sexual health; 20% said yes, nearly 2% said they would like more MSM health info, with 38% saying no, I feel that I have enough information, and 31% said no, I do not need this. Page 54 of 123


56 When cross-tabulated with race/ethnicity we see that 20% or more of the American Indian or Alaskan Native population, the Black or African American population, and the Hispanic population all indicated they would like more info on sexual health. A small portion of the Black and Hispanic communities indicated they would like more information on MSM health. Page 55 of 123

57 When cross-tabulated with mode of transmission, nearly 20% of the having sex with a man, having sex with a woman, and sharing needles populations indicated they would like more information on sexual health. A small portion of the having sex with a man and having sex with a woman populations indicated they would like more MSM health info. Services and Service Needs In order to assess gaps in care participants were presented with a grid that included all Ryan White services, currently funded and not funded. They were then asked to check the corresponding box for each listed service, which read; didn t need this service, didn t know about this service, asked for this service but did NOT receive it, RECEIVED this service and it did NOT meet my needs, or service RECEIVED and met my needs. The grid below displays those responses. Under the heading didn t know about this service, anything over 15% is highlighted for review. Additionally, in the column received this service and it did NOT meet my needs, anything over 5% is highlighted for review. Page 56 of 123


58 Page 57 of 123

59 Page 58 of 123

60 Page 59 of 123


61 Page 60 of 123
, Vision (appointment with optometrist, eyeglasses), Early Intervention Services (finding HIV positive people and getting them into care), Health Insurance")
, and Legal services (help with a do not resuscitate order, estate planning, discrimination).")
62 Fifteen percent or more of clients indicated they didn t know about this service with regards to the following services in the table above; Specialty Care (an appointment with a specialist, for example dermatologist or gynecologist), Vision (appointment with optometrist, eyeglasses), Early Intervention Services (finding HIV positive people and getting them into care), Health Insurance Assistance (help with premiums and co-payments to private health insurance plans, including COBRA), Emergency Financial Assistance (short term money for utilities, rent/mortgage), Housing services (help with rent/mortgage payment), and Legal services (help with a do not resuscitate order, estate planning, discrimination). This could be due to several factors including; not enough advertisement and distribution of the local resource directory for clients, clients not divulging their need for this type of assistance to case management staff, or case management staff not discussing this service option with the clients. A few services are also outlined as Asked for this service but did not receive it by 10% or more of clients. These are; Dental care (annual teeth cleaning, visit with a dentist), Vision (appointment with optometrist, eyeglasses), Emergency Financial Assistance (short term money for utilities, rent/mortgage), and Housing services (help with rent/mortgage payment). With regard to RECEIVED this service and did NOT meet my needs, several services are highlighted that were indicated by 5% or more or respondents. These services are; Outpatient Medical Care (an appointment with a doctor to take care of your ongoing HIV treatment including CD4 and viral load), Specialty Care (an appointment with a specialist, for example dermatologist or gynecologist), Nutrition Page 61 of 123
63 Services (meeting with a registered dietician, access to supplements such as Boost), Mental Health Services (individual or group counseling for mental health issues-including support groups), Case Management (someone to help coordinate the services you need, provide referrals for services, and help getting public and financial assistance), Treatment Adherence Counseling (someone to help you understand your medications and doctor s instructions, and strategies to keep with your prescribed medications schedule), Emergency Financial Assistance (short term money for utilities, rent/mortgage), Food Assistance (food voucher, basket of food, food pantry), Housing services (help with rent/mortgage payment), Transportation (bus pass, gas voucher, van transportation all for medically related needs only), and Psychosocial Support (support groups). The issue of services not meeting the needs of those that accessed them was visited during the focus groups to unveil more information. As far as Outpatient/Ambulatory care, focus group participants stated that wait times at the facility are generally very long and same day or short notice appointments are very hard to get. Nye County participants stated they have no choice for medical care other than being bused into Las Vegas. In order to do so they get up very early in the morning as their appointments are generally scheduled during a block of time early in the day to ensure all clients traveling in the van together are seen in succession. Thus one medical care appointment takes their entire day. They also stated they would like an HIV clinic in Pahrump so they don t have to travel so far to access medical care. Issues around Medical Nutrition Therapy were that clients wanted to be able to have an unlimited amount of Boost and supplements. They feel as though these items are rationed and they would like to have more access to them. Along the same lines is Food Assistance, participants said that getting food from a food pantry is labor intensive and they don t always have the items they need. They would like to receive monthly food vouchers instead of trying to make due with what s available at the food pantry. Additionally, they stated that these facilities don t carry hygiene products and therefore food vouchers are primarily used for those items. Transportation was also discussed as a hot topic with participants stating they have to go through too much red tape to get and or use bus passes. They preferred the old way when monthly passes were distributed and there was no keeping track with an envelope and signatures of every place that was visited. Mohave County residents stated they are dissatisfied with Mental Health Services and Psychosocial Support because there are no support groups in Kingman Arizona. The nearest one is in Laughlin Nevada and many people don t have transportation that far or cannot drive at night. See the focus group section for more comments regarding services. Page 62 of 123
64 In order to determine the 10 most important services that currently aid clients in dealing with their HIV/AIDS status, respondents were given a list and asked to check the most important services to them. The top ten most important services from the client s perspective are in order as follows. Ra nk When looking at year over data with regard to this same question, for the first time Outpatient/Ambulatory Medical Care was not ranked as the most important services to clients to help them manage their HIV/AIDS status. The number one most important service that clients indicated was Dental Care/Oral Healthcare followed by Vision services and then Food Bank/Food Vouchers with Outpatient/Ambulatory Medical Care ranked as the 4 th most important service followed by HIV/AIDS medication. Answer Options Re sp o nse Pe rce nt Re sp o nse Co unt 1 Dental Care (annual teeth cleaning, visit with a dentist) 70.8% Vision (appointment with optometrist, eyeglasses) 66.3% Food Assistance (food voucher, basket of food, food pantry) 64.8% 173 Outpatient Medical Care (an appointment with a doctor to take care of your ongoing HIV treatment, including 4 labs-cd4 and viral load) 58.1% Medication (help paying for and getting HIV/AIDS related medications including ADAP) 56.2% Emergency Financial Assistance (short term money for utilities, rent/mortgage) 54.7% Housing services (help with rent/mortgage payment) 54.7% Transportation (bus pass, gas voucher, van transportation all for medically related needs only) 53.2% 142 Case Management (someone to help coordinate the services you need, provide referrals for services, and 8 help getting public and financial assistance) 46.1% Nutrition Services (meeting with a registered dietician, access to supplements such as Boost) 45.3% 121 Health Insurance Assistance (help with premiums and co-payments to private health insurance plans, including 10 COBRA) 43.4% Mental Health Services (individual or group counseling for mental health issues - including support groups) 37.1% Specialty Care (an appointment with a specialist, for example dermatologist or gynecologist) 36.7% Referrals for Health Care/Supportive Services 21.0% HIV and Health Classes (healthy relations, HIV 101) 20.6% Legal services (help with a do not resuscitate order, estate planning, discrimination) 20.2% Psychosocial Support (support groups) 16.5% Home Health Care (doctor ordered skilled nursing care in the patients home) 15.7% Early Intervention Services (finding HIV positive people and getting them into care) 12.7% Outreach (HIV Testing and linkage to medical and support services) 12.7% 34 Treatment adherence counseling (someone to help you understand your medications and doctor's 19 instructions, and strategies to keep with your prescribed medications schedule) 12.0% Substance Use Services (individual or group counseling for substance use issues - including support groups) 10.5% Rehabilitation Services (occupational therapy, speech therapy) 7.9% Partner Notification Services (help confidentially informing people that you might have put at risk for HIV) 7.1% Language Services (interpretation and translation) 7.1% Hospice Services (comfort care and pain management for terminally ill or seriously ill patient) 6.0% Child Care Services (child care while you are at doctors appointments) 6.0% Substance Abuse Services-Residential (treatment in a residential health setting that is short term) 6.0% Respite Care (break for HIV caregivers) 5.6% 15 This could be due to the new healthcare reform policies allowing clients to access medical care through another funding source such as Medicaid or health insurance. Clarification on this issue was discussed further in the focus groups. Page 63 of 123
65 Think about the most important services that you currently need and use. Of the list of services below please check only 10 that are the most important to you for your HIV/AIDS status. Service Category HIV/AIDS Medical Care (including doctor visits and labs- CD4 and Viral Load) 2014-NA Ranking 2013/2014- CS Ranking 2013 Ranking 2012 Ranking 2011 Ranking 2010 Ranking 2009 Ranking HIV/AIDS Medication Food Bank/Food Vouchers Dental Care/Oral Care Emergency Financial Assistance (with utilities and housing) Access to Medication Transportation Assistance with health insurance and insurance related issues Case Management Housing Assistance (short term assistance with housing or referrals for available housing) Mental Health Services Health Insurance Co-Payments and Premiums Medical Nutrition Therapy (nutrition supplements, Boost, meeting with a registered dietician) Legal Services (do not resuscitate orders, discrimination or breach of confidentiality) Substance Abuse Services Child Care Services Interpretation and/or language translation services Page 64 of 123
66 Referrals for Health Care/ Support Services HIV Testing (EIS and Outreach) Rehabilitation Services Substance Abuse-Residential 18 Vision 2 Specialty Care 12 Health Education/Risk Reduction 14 Psychosocial (support groups) 16 Home Healthcare 17 Treatment and Adherence Counseling 19 Hospice 23 Respite Care 24 Clients were asked if there are any services they need but cannot get. Those responses include; dietitian, transportation, all of them, finding out about long-term rental assistance but not sure about it, rental assistance, housing and disability, help with rent, gas vouchers, housing, medical so that I can keep taking my meds, dental, medical premium co-pay, rental assistance, cover some medication, beds/furniture, food stamps, PREP knowledge, rent help, utilities, clothes, chiropractic, dermatologist, head/body scan, toiletries, lab test co-pays, and rest of my rent. Consumer Focus Group Results A total of seven focus groups were scheduled; one in Kingman for Mohave County clients, one in Pahrump for Nye County clients and five in Las Vegas. The Las Vegas groups were divided into; one for MSM s, one for men infected through injection drug use (IDU) or heterosexual contact as not enough participants were able to make up one entire group of IDU s, one specifically for women, one with no specific specifications other than being HIV positive, and one for transgender individuals. However, of the transgender group scheduled in Las Vegas unfortunately no participants came. Las Vegas Focus Group for MSM s Three of the ten scheduled participants attended the MSM group. What services are you most satisfied with and least satisfied with? Page 65 of 123
67 Participants indicated that they are least satisfied with the attitudes of providers. Comments include; AFAN is hard to talk to about anything. They are too snobbish and bias. The director needs to get out in the community and talk to people. Providers aren t in the community enough. Where does all the money go? They need more people that are HIV positive working there and that care. We got much more info from Action Red then we ever have at AFAN. We can t get through to Access on the phone, it s a joke. We want to speak to real people on the phone. Other comments included dissatisfaction with the location of service providers and the need for one stop shopping or having all providers in one easily accessible location. Other issues were recertification for Part A and Part C through UMC Wellness. The client stated; I brought all my paperwork from the list they gave me but didn t have a rental agreement and they wouldn t renew my Part C even though I had another paper off the list instead of that [rental agreement]. Also clients were unhappy that they have to bring paperwork back, they aren t allowed to fax it. One participant stated; UMC has a monopoly on Part C, you can only use it at UMC, AIDS Healthcare Foundation is great, they only deal with HIV patients. Other discussion around this topic included; providers giving clients the run around and not giving straight answers, there needs to be more people working at the agencies with HIV because they don t have enough compassion they are not in our shoes, Access to Healthcare moved and didn t tell anyone their new address, and case management staff needs to provide more help and guidance. Several comments were made about the St Therese food pantry and how grateful clients are for their services. At times they felt different workers were bias and let people in they shouldn t have but overall they provide a great service. Clients were read the list of services indicated by over 5% as received but didn t meet my needs and asked if they agreed with this list and why? Clients agreed that services didn t meet their needs because; They make you feel like you have to go tight rope walking to get help. Page 66 of 123
68 When discussing Medical Nutrition Therapy clients said, they don t give out enough info, they are just there for a paycheck, they don t tell you important things like don t eat grapefruit with certain meds. When discussing housing, transportation, and case management clients said; that sounds like AFAN issues for those services. Discussion surrounding transportation included too much red tape to use the bus pass system and who cares if you use a bus pass to go to a movie or to see your mother, I can t even use a bus pass to go to the pride festival or the gym. Another participant said they ve stopped using the bus passes because they didn t want to deal with the hassle anymore. Clients were read the ranking of services from the survey and asked if they agree with the order of rank respondents had outlined, being; #1 dental care, #2 vision services, #3 food bank/food vouchers, #4 HIV/AIDS medical care, and #5 access to medication. This group said they absolutely do not agree with this and would rank them as medical care and medication tied for number one, food assistance in second place and housing at least fourth. They also said it may have something to do with the doctors because they don t listen to you or take into consideration that you live in your body and they don t. They also said that it is hard to get referrals for dental care and they aren t always able to provide the dental care that is needed. If you could change one thing about the system of care what would it be? Customer service, act like you care, and more places to go for services in the city like more big places to go other than AFAN. One stop shopping that doesn t include CCSS that has infected and affected employees and understands what we re going through. Other comments included bringing back the old staff at UMC s front check in that cared about clients and taking down the glass partitions. Also decreasing wait times for medical care. One client said he waited one hour in the lobby and an additional hour and a half in the medical room waiting to see someone. Las Vegas Focus Group for Men IDU s or Infected through Heterosexual Contact Four of the seven people confirmed for this group came. One of the clients was newly diagnosed within the last 60 days. What services are you most satisfied with and least satisfied with? Page 67 of 123
69 One participant stated that he would like a case manager but hasn t ever had one. He would like someone to talk to about services he needs and help him navigate the system. Additionally, clients said they have trouble getting assistance with co-pays and are also upset that they can t qualify for Medicaid. The newly diagnosed individual stated he is very happy with everything and his case manager form the health district has helped him get everything he needs including getting into stable housing. Others said they are most satisfied with care from the UMC Wellness center and least satisfied with AFAN as they report they don t return any phone calls. Overall clients reported being very grateful for the services they do receive. Clients were read the ranking of services from the survey and asked if they agree with the order of rank respondents had outlined, being; #1 dental care, #2 vision services, #3 food bank/food vouchers, #4 HIV/AIDS medical care, and #5 access to medication. Participants said they did not agree with this ranking order and that number one should be a tie between medical care and medications. Number two should be food assistance and nutrition services with number three being health insurance assistance. They also said that it depends on where you are in the system and sometimes you focus is on dental. Clients were asked about services they are in need of but can t get or haven t received. The only comment was utility assistance is difficult to get and with bills in excess of $200 per month it s hard to stay on top of the payments. If you could change on thing about the system of care what would it be? More reaching out to those in need and those that are scared. More help with co-pays. Other concerns are that it takes so much time to attend a doctor visit when all they do is read the labs and that providers need to be out in the community more. Las Vegas Focus Group for Women All eleven of the invited participants for the women s group attended. What services are you most satisfied with and least satisfied with? Page 68 of 123
70 Participants were least satisfied with case management as they said case managers don t often return phone calls and are hard to get ahold of. They also said that case managers should be held to the high standards they hold us to when discussing being on top of things and returning calls. Other said, they but you through the ringer for trying to get stuff when referring to services and feel that services are hard to get. Nutrition services were also discussed as not meeting client needs. A newly enrolled consumer said that she couldn t get an appointment with the nutrition therapy department and was never called back. A client that previously lived in Lincoln County said she was forced to move to Las Vegas to be close to services because nothing is offered in her area. Additionally, the amount of gas vouchers she was given didn t cover her gas costs to drive into Las Vegas for care. She would like to see more outreach and care in rural areas. Others said that transportation is difficult as they don t always live near bus stops and would like a van or taxi service to get to their appointments. Services they are most satisfied with include dental, vision, medical and the eligibility staff at UMC Wellness center. Clients were read the ranking of services from the survey and asked if they agree with the order of rank respondents had outlined, being; #1 dental care, #2 vision services, #3 food bank/food vouchers, #4 HIV/AIDS medical care, and #5 access to medication. This group agreed with the ranking order with the exception of one person who said that housing would be her number one because without housing one cannot function to accomplish anything else. The group also agreed that service needs vary based on what is going on in each individual s life at the time and what each person s priorities are. Clients were read the list of services indicated by over 5% as received but didn t meet my needs and asked if they agreed with this list and why? They agreed with case management stating they would like to have their own case manager assigned to them so they could have a more personal relationship. They feel as though they have to go into case management appointments with a good attitude or the staff won t help them and it s hard to always maintain a positive attitude when living with the repercussions of the disease both physically and mentally. They have to have all their paperwork together or else case management staff won t help them at all. Page 69 of 123
71 Are there any services you are in need of but can t get? Help with Section 8 housing. Food vouchers were mentioned as clients discussed wanting the old food voucher system back when they received $40 in food vouchers every month. They also mentioned hygiene products as something they have a hard time getting. There are rules on vouchers so you can t buy things like toothpaste or bleach to clean your house. They also talked about the need for a peer network or group of people that have been in the system for a long period of time to help those who are newly diagnosed or new to the care system. If you could change on thing about the HIV/AIDS system of care what would it be? Services before salary s. In general they stated that they just need help getting the right information, such as what services are available and how to access them. They would also like providers to be more educated on services that are offered in the community and compassionate. They would like to be treated with more respect and dignity when trying to access services. They feel that providers treat them like they are paying for assistance out of their own pockets and it s hard to get help. They also said please keep dental, vision and transportation going as they are very important services. Las Vegas Focus Group for General Attendees This general focus group had three attendees. Are you currently accessing HIV/AIDS medical care and/or support services and what is your motivation for accessing care? Responses include, currently getting care despite horrible treatment and obstacles, these obstacles are defined as mainly lack of knowledge regarding disease. Other motivation is dying, God, and material incentives (such as the Walmart gift card). Do you feel you have a support system, and if so who is your support system? Family, Friends, God, spiritual community and religion were mentioned. One person had no support system. Medical personal were not identified as support group. Have you ever not accessed care for a period of 12 months or more and what caused you to stop accessing care? Page 70 of 123
72 Yes, the specific reasons given were; no access to care, rude administration/ horrible customer service, paperwork, long wait times between appointments, not enough case workers, medical cost-would rather buy it in Canada or India, and stigma when getting care. What could have kept you in care? Reduced paperwork was mentioned in addition to support groups and general disease information. Also information on how to deal with depression and psychiatric/psychological issues as most patients refuse to go to psychologist. What made you want to access care again? A basic desire to survive. What led you to your decision to get tested for HIV? Motivations were mentioned as; symptoms, heart attack, casual check-up, blood CBC levels, and routine blood bank procedure. How long after you were tested did you seek medical care for your diagnosis and was there anything holding you back from accessing care? Range was from 0 to 5 years. The major reason for not seeking treatment was T-cell count, second major reason was availability of immediate services. How has your HIV/AIDS diagnosis affected your emotional health and mental stability? Have you sought support groups or counseling since your diagnosis? Yes, it has caused severe depression, anxiety and other mental illness. There are currently no support groups available in the area that they know of. Most patients express they don't trust mental health providers. They believe that medical staff want you to die and would trust support groups instead. What are the 5 most important services to you that help you manage your HIV/AIDS diagnosis? Access to medication, support groups, case managers, AFAN (specifically Denise Burns), and qualification services (specifically case manager Magdalena). What services are you most satisfied with and least satisfied with in the current sys-tem of care and why? They reported being least satisfied with medication, medical billing, healthcare access, clerical services-paper-work, transportation, and AFAN employees in the front desk-very cold. Page 71 of 123
73 They are most satisfied with St. Teresa food services. Are there any barriers that you have experienced while trying to access services in your community? Barriers are reported as; stigma-treated very badly, transportation issues, paperwork, lack of access to medications, lack of access to health care, rude treatment that makes you want to stop going to services, and dementia due to HIV status and medications-most people providing services don't understand this health disability and are not compassionate towards it. If you could change one thing in the HIV/AIDS system of care what would it be? Bureaucracy, improve customer service and more humane treatment, increase patient advocacy, centralize services, decrease paperwork and increase number of employees. Client report that some recordings actually state, "if you leave more than one message we won t call you back". Are there any services you need but can t get or aren t offered in your area? Medical billing services, lack of referrals to specialists, and help regarding the Medicaid system. Do you ever miss appointments? What are the reasons you miss appointments? Yes, due to transportation issues, paperwork issues, and dementia. There are no appointment reminders. What do you think about HIV prevention and/or education services offered in your community? They are bad, people don't seem to know or care, their is a lack of knowledge regarding transmission. HIV staff has poor education on disease and customer service. There is a lack of safe sex propaganda especially in there homosexual community. Describe the ideal HIV prevention program for your community? A program that promotes safe sex, equal treatment, addresses stigma, address issues specifically regarding penetration and HIV. Homosexual community seems to have good programs. What behaviors do you think put MSM at risk for HIV transmission? Of those behaviors, which are the biggest problems in your community? Drugs and alcohol which relax inhibition, the sharing of needles and drug abuse in general. What types of drugs are you using now and what types have you used in the past? Page 72 of 123
74 Marijuana and methamphetamines. What is the frequency of drug use? How many years have you been using the sub-stance? Currently clients self-described as not using. Years of use ranged from years. Does using drugs or alcohol impair your ability to take care of your HIV/AIDS related medical needs? Yes, due to appointment failures, failure in medication adherence and destruction of support system. Have you sought substance abuse treatment? If so what kind of treatment (inpatient, outpatient, support groups, AA etc.)? Was it easy or hard to get and why? Yes, AA meetings, substance abuse treatment through Westcare, and support through family. Is there any additional information you would like to add? AFAN and Ryan White Part B do a "horrible" job at providing care, no medication access and bad customer service. There was also a strong desire for centralized care. Access to care program should be abolished and clients report they receive 2 nd class citizen treatment. Mohave County Focus Group in Kingman Arizona Three of the six confirmed participants came to the group. Are you currently accessing medical care and if so what is your motivation for staying in care? Comments included; survival, to keep costs down, and respondents also said that ADAP is a vital service. Do you have a support system? Only each other and some family was noted. Clients also said there are no support groups in Kingman and clients desperately want one. Are there any services you need and can t get? Clients again reported their need for support groups as the nearest one is in Laughlin which is too far to travel when transportation is an issue. All three respondents commented on how lonely they are and how hard it is to have a social life, it would be nice to go out one a year. They also would like more doctors and more choices for health care. Page 73 of 123
75 The girls at the Ryan White office are great and dental and vision is also great. What are your barriers to accessing care? Client said that transportation is difficult and the only real solution would be a shuttle with door to door service to all of their appointments. Also, paperwork was noted as a barrier as they feel they fill out the same forms every six months even when nothing changes. If you could change one thing about the HIV/AIDS system of care what would it be? Comments include again a shuttle service or better transportation options. They would also like to remove the stigma associated with HIV/AIDS in the Kingman area. They feel like they can t share their status with their friends and neighbors and be an advocate for people living with HIV/AIDS in the area. One participant would like to be able to use HOPWA funding to help with his mortgage payment. Another participant would like to be able to get HOPWA funding but cannot because of a previous felony. Overall this group reported that they are very satisfied with the services they receive through Ryan White and appreciate the help greatly. Nye County Focus Group in Pahrump Nevada This group consisted of nine participants, two women and seven men, all residing in Pahrump Nevada. Clients were read the ranking of services from the survey and asked if they agree with the order of rank respondents had outlined, being; #1 dental care, #2 vision services, #3 food bank/food vouchers, #4 HIV/AIDS medical care, and #5 access to medication. Clients agreed that those are the most important services but not in that order. They would rank them differently with #1 medical care, #2 medication, #3 transportation, #4 EFA, #5 Dental and Vision, and #6 food bank. One client stated he would put dental care before EFA. One client stated that dental care is hard to get and he hasn t been able to get an appointment after both were canceled and rescheduled. Two clients also stated that they couldn t be seen at the dental school because they were too sick and had too many conditions. Clients said they, teach the fear meaning they teach students to be afraid of treating complex cases. Another client said the care he received through the dental school was excellent and he got right through without any issues. Page 74 of 123
76 When discussing medical care clients stated that they receive referral upon referral upon referral for their ailments and the HIV doctors don t treat anything other than HIV. When discussing transportation clients felt that their case manager/driver is so busy now with the increase of clients that they would like to have an additional driver on hand. Are there any services you need and can t get? When discussing the food bank clients stated they need protein powder, vitamins, and ensure. They would also like more meat products and fresh vegetables. More access to entertainment was discussed. Clients said they get very depressed and bored and would like to go into Las Vegas to recreate at least once a month but are unable to get there. One client stated that once he gets to Las Vegas he is too tired to drive home and would like to have transportation to bring him home. They also talked about the need for more of a social life. They said that Pahrump is boring and there isn t enough social activities. One client stated that he would like some emotional intelligence classes, psychology classes, and some classes on how to deal with doctors and family members. One client stated he would like the hospital in Pahrump to have more specialists. Difficulty getting on section 8 was also mentioned. The length in wait time is upward of two years. More mental health services in the area was also mentioned as some people can no longer qualify for the mobile mental health. What are your barriers to accessing care? Clients said there are no HIV doctors in the area and very few specialists. They stated that they length of the eligibility process is too long and cumbersome. They can t get help with co-payments for medications. Again transportation was also mentioned as a barrier because it isn t always readily available. If you could change one thing about the HIV/AIDS system of care what would it be? Accessibility of services was noted as a change that would improve the system of care. Along with more physicians and specialists in the area and changing how often eligibility has to be completed, every six months is repetitive. One client stated that he is experiencing difficulty getting on SSI and SSDI as he can t get a physician to sign his paperwork. He also stated that it s hard just dealing with the day to day struggle and when you have issues accessing your benefits it makes life difficult. Page 75 of 123


77 Other comments included more quality of life activities and educational assistance. He can t find any HIV grants and would like to pursue a doctoral degree. Clients also said there are so many hoops to jump through when accessing services that the process should be made easier, mainly talking about Medicaid and SSI. Consumer Out of Care Survey Results This survey targeted those PLWH/A that have been out of Ryan White care for 12 months or more. Again, participants were found by running a report in CAREWare of all the clients that had not accessed Ryan White services in 12 months or more. Those clients were contacted via mail and asked to participate in the survey. This survey yielded 51 participants and their responses can be found in the following tables and charts. General Information, Testing and Health Status The majority of respondents, 57%, report they are HIV positive with no symptoms, followed by 27% that are HIV positive with symptoms, and 16% that have been diagnosed with AIDS. When asked about where they tested positive; 20% were in a hospital/emergency room, 20% at a local health center or clinic, and another 20% at the Southern Nevada Health District. Eighteen percent tested positive at a private doctor s office, 8% at an HIV/AIDS community based organization, and 4% said an organization providing other services (family planning, substance use treatment, etc.). Of the 12% that said other their responses include; Clark County Detention Center, insurance application, Page 76 of 123

78 Response Mayo Clinic in Rochester MN, prison intake, on the phone, and health clinic in Florida. The majority of respondents indicated they were residing in Clark County, Nevada when they were tested. Twenty-two were in a state other than Nevada or Arizona, 4% were somewhere else in Nevada, and 4% were tested outside of the US. When asked about year of diagnosis, a large number of respondents indicated 2002, 2005, 2008, and Year of Diagnosis Year Clients were also asked what their age was at diagnosis. The majority was diagnosed in their mid to late twenties with 6 people saying they were diagnosed at age 27, 4 at age 28, 3 at 24 and 3 at 26. Page 77 of 123

79 Response Age at Diagnosis Response Age at Diagnosis Age When asked about mode of transmission the vast majority, 75%, said they contracted HIV through having sex with a man, with just 16% that said sharing needles, 12% who said they don t know, and nearly 10% said having sex with a woman. When asked about sexual orientation the majority or 57% of respondents reported they are gay/homosexual, 27% said straight/heterosexual, and 6% said they are bisexual. Page 78 of 123


80 Most of the respondents are White or Caucasian at 48%, with 26% reporting they are Black or African American, 14% are Hispanic or Latino/a. Under multiple ethnicities/other one person said Italian. Page 79 of 123


81 The vast majority are male at 84% with 14% stating female and 2% indicating transgender. When asked about their assigned sex at birth, 86% said male and 14% female. Current Age Response Our respondents current ages range from 26 to 64 with 4 reporting 30, 4 reporting 42, and 4 reporting 52 as the most indicated ages. Page 80 of 123


82 We asked respondents when they saw their HIV/AIDS physician last, just 16% said it was over 12 months ago. This means that this select few are the only people technically out of care, as defined as 12 months or more without medical care. However, each person that received the letter asking them to participate in the out of care survey had no record of any Ryan White services in the previous 12 months or more, dating back to This is a positive in the sense that these people are truly accessing medical care for their HIV/AIDS status somewhere. The down side is that this survey was tailored to collect data from those that are out of the HIV/AIDS medical care system completely. However, the questions and responses throughout this survey give insight into several aspects of care and services that are essential to the planning and shaping of the HIV/AIDS system of care as a whole. With regard to taking prescribed medication 68% of people reported they have taken it within the last month. Just 10% report the last 1-5 months, 2% the last 6-12 months and 14% over 12 months ago. Again the majority said they had a blood draw for their labs within the last month 30% or 1-5 months ago at 48%. Just Page 81 of 123

83 8% said 6-12 months ago, and 12% over 12 months ago. Motivations for getting tested varied however, the most indicated reason for testing was going to the hospital for another health reason at 36%. Other reasons include; I chose to get tested at 20%, I was tested as part of a routine physical examination at 16%, 14% said other, 8% said I tested as part of an outreach clinic or street outreach program that offered HIV testing, with 6% stating I asked a health care provider to test me for HIV, and 6% that said I was tested because my partner/someone asked me to get tested like a health care worker. Comments in the other category include; I was in jail, my partner was diagnosed, feeling tired and weight loss, got sick, I was contacted by Nevada Health District saying someone who I ve come in contact with tested positive and they wanted me to come in for a test, I was sick with what I thought was the flu, and found out by arrest. Page 82 of 123


, and 36% said they were referred to case management.")
84 The major reason for not seeing a doctor lately was; I am undetectable indicated by 24%, with 14% stating I cannot afford it. In the other category statements included; I don t have a Nevada ID, waiting for an appointment, full time work and no transportation, depressed after my mother died and didn t care, and interferes with my work schedule. Just 60% of clients said they were referred for medical care following their HIV diagnosis, only 44% said they were referred to an AIDS Service Organization (ASO), and 36% said they were referred to case management. Three people said they weren t referred for any services at all. The other comment was, I found out when a friend took me to emergency. Page 83 of 123


85 Sixty-two percent said they got into medical care immediately following their diagnosis with 8% saying they waited less than a month, 8% waited 1-3 months, 12% waited 6 months or more and 8% don t remember. The reasons for not seeking medical care immediately are primarily I was depressed and Didn t know where to go to get medical care. Responses in the other category include; went to Honduras-thought there was a cure, and I did seek health. Page 84 of 123

86 The top reasons for not seeking medical care are; I don t have transportation to get to medical care appointments, I can t afford medical care right now, I get anxious about going to the HIV doctor, I don t want anyone to know I have HIV, I don t have the money for a bus pass/parking or lunch, and wait times are too long for an appointment. Reasons in the other category are; don t have a Nevada ID, I received medical care since I find out I was HIV positive, I have seen my doctor as he directed, and I did not care about it due to depression and drug abuse. Clients were asked what would help them get to the doctor. Top answers included; transportation, insurance, free medical care, shorter wait times for appointments, and better quality of services. Qualitative responses were; getting my ID, not having to wait for refills for days on end, location, at the emergency room they gave me a referral to wellness center, and I see a doctor. Page 85 of 123

87 Page 86 of 123


88 We asked clients why they think people don t get medical care and the top reasons were; denial, stigma, drugs, transportation, don t want to take medication, can t afford it, and they feel healthy. We asked clients what would help them get into medical care and lower cost of medical care/medications was number one. Among others were; referrals, more information about the services offered, transportation, mental health treatment, and outreach services. The other responses were; getting my ID, people that understand me, to own a car, and heavy emphasis on mental health treatment. Page 87 of 123



89 Pregnancy, Substance Use, and Mental Health None of our female respondents indicated that they had been pregnant in the last 12 months, therefore they didn t require and pregnancy related medical treatment. Page 88 of 123



90 Tobacco was the most widely used substance followed by alcohol and marijuana. Street drugs were reportedly used by a few respondents with 10% saying they used meth, 4% ecstasy, and 4% heroine. The other comment stated; I used to smoke 9 months ago and I quit. Just 4% said they do not have a desire to stop using drugs. Eight percent haven t started working on it, 19% are currently taking steps to stop using, and 30% are drug free and in recovery at this time. Page 89 of 123



91 Twenty eight percent said they have used injection drugs, with 70% stating no and 2% prefer not to answer. Two percent said they currently use injection drugs while 98% indicated no. Six percent of those that report using injection drugs said they sometimes share needles or works, 16% said they never share needles or works and 76% said it doesn t apply. Four percent said they always clean or disinfect the needles or works, another 4% said they do most of the time, and 6% or 3 people said they never do. Page 90 of 123


92 When asked about their sexual health, 15% of clients said they have been diagnosed with syphilis in the last 12 months while 10% said hepatitis C and 6% gonorrhea. When asked about infections they had been diagnosed with ever, responses included; 32% syphilis, 28% gonorrhea, 18% hepatitis c, 16% chlamydia, 12% hepatitis B, and 10% herpes. Page 91 of 123

93 Half of respondents said they engaged in sexual activity with a partner within the last 12 months with 42% indicating no and 8% that prefer not to answer. Of concern are the 18% that said they did not use a condom or dental dam while engaging in sexual activity. Another 10% said they only sometimes use a condom or dental dam with 2% indicating most of the time. Page 92 of 123


94 Service Needs We asked this group the same question as the In Care Survey group, regarding the importance of services, while providing them a list and asking what do you think are the ten most important services that help people with HIV/AIDS manage their diagnosis. The results can be found in the graph below. Page 93 of 123
95 Finally we asked clients if there was anything else they would like to add. Their comments are as follows; Refills are a major issue because it's not like you are ever gonna stop taking the meds prescribed to you and if you have to wait so long its bad news for your status. Thank you. I have been ban from St. Theresa, no more food vouchers because he said I was cussing but I didn't so they are tripping. Thank you for caring, a lot of people don't care. Thanks for Nevada for helping people with HIV and caring. Some don't care but you do. Thanks. I feel giving people quicker access to the programs will help foster further participation. Currently it is difficult and time consuming to get the available services. I do not have anything else to comment I feel that your question where good and to the point thank you. I feel alone, death is the only answer, not by my hand. My comment is when I get to see the the takes too long about 5 hours, the nurses are too slow, at wellness center, same is in emergency room at UMC. Need better healthcare. I am good thank you. It would be nice to have free healthcare like most other countries. The healthcare system is in poor state. But there are some good organizations that help people with hiv which is good news. I think we need more doctors in town other than the wellness center because they are over booked and over loaded.also more doctors need to accept Medicaid. There needs to be a organization or one place where services for all assistance needs, whether it be medical, prescriptions, transportation, food & financial can be done in one location. Its very difficult for people who are in need of all these programs to apply because they are all in different parts of the city. Extremely difficult & stressful to get to these locations, sign up & make an appointments. Because of that most people are not treating their disease. There needs to be a better system in place here in las vegas. There is such a fear of the chance of ones work place finding out and letting you go because of the nature of the Disease. i live in Fear daily. Page 94 of 123

96 PROFILE OF PROVIDER CAPACITY AND CAPABILITY The profile of provider capacity and capability was completed through the provider survey and identifies the extent to which services in the resource inventory are accessible, available, and appropriate for PLWHA, including specific subpopulations. Estimates of capacity describe how much of which services a provider can deliver. The assessment of capability describes the degree to which a provider is actually accessible and has the needed expertise to provide services appropriate for specific subpopulations. A careful assessment of barriers to PLWHA receiving services is an important aspect of this component. These provider profile also explores client perceptions of service quality and appropriateness. A total of 18 providers responded to the survey. It should be noted that this survey was sent to all employees that work on Ryan White in any respect at each Part A funded agency. General Information The chart below illustrates the employment position of each respondent. Page 95 of 123


97 The specifics of each organization can be found in the chart below. The funding streams received at the organizations vary from federal funding through Ryan White parts A, B, C, and D to revenue and private contributions. Page 96 of 123


98 Seventy-two percent of participants said that their agency has foreign translation services. Seventy-seven percent of respondents state their agency has bi-lingual staff on hand with 69% that also use a language line. Nearly half, 46%, said they translate patient material into languages besides English. Additionally, when asked what language besides English is requested most often at their agency all participants stated Spanish. Page 97 of 123



99 The majority of providers serve Clark County with 61% serving Nye County, and 22% Mohave County. As we ve seen in both consumer survey s transportation is a top priority and concern for many. Seventy eight percent say there is public transportation located near their agency however 22% say there is not. In general all facilities are open from 8am to 5pm Monday through Friday. Comments included; weekdays 9am- 4pm, weekday hours from 9am to 12pm and 1pm to 4pm, and one Saturday/month, ½ day. Page 98 of 123


100 When asked about wait times for newly diagnosed clients; 33% said no wait, we get them in quickly, 22% said less than a week, 39% said 1-2 weeks, and 6% said doesn t apply. Nearly all respondents reported they have seen an increase in the number of clients seeking services in addition to many saying they ve had an increase in demand for services from clients. Along with that 20% say they ve had a decrease in the amount of funding received from one or more of their funding sources. Page 99 of 123



101 When asked what their agency needs to increase its capacity to serve more persons living with HIV/AIDS just 8% said nothing more is needed. Top choices were; 77% that said more funding to expand current capacity, 62% said funding to develop new capacity, 46% said an increased partnership with other HIV/AIDS specialty agencies and organizations, and 23% need more training. Specifics on that training were listed as; case management training and Trans 101 training, funding to expand certain programs, Mental illness and HIV (especially neurocognitive effects of the disease over time. Substance abuse and behavioral manifestations, motivational interviewing. Providers were asked about the most pressing issues and needs among clients that they come into contact with. They answered most often; housing, transportation and medication. Housing, Meds Transportation help for appointments Transitional housing options for clients who are homeless (i.e., housing first), child care, lab copays MEDICATION, TRANSPORTATION, HOUSING Housing & nutrition issues "Home Health, Hospice, Emergency medications" Homeless prevention, medical equipment / medications not covered under Ryan White or other funding sources, long-term housing for persons with no income Transportation, medication assistance, applying for Ryan White Part B Page 100 of 123
102 "1. Bus passes 2. More Case Managers 3. Housing" "Poverty, Homelessness, Malnutrition" "Spanish Speaking, Proprietary actions of other agencies, Transportation assistance" Long term medications, psychiatric care, adherence, intensive outpatient substance abuse treatment. Hospice care Providers were then asked about new and emerging issues or trends they have seen within the consumer community. One of the issues mentioned more than once is confusion with the new Affordable Care Act (ACA). Homelessness Confusion with new medicaid insurances Make sure ryan white program to continue services barriers to health insurance NA "Lack of the ability to navigate the healthcare system Increased paperwork for workers and patients with new insurance Confusion on coverage." No Show No Call rate is increasing "1. More Transgender Clients 2. New clients moving into Clark County" The majority of the clients we serve are below the federal poverty line, estimated (75%) Confusion and delays with ACA Patients on medicaid...there is horrific difficulty our nurses have in accessing case management, referral and other services by their medicaid provider. People in Medicaid offer conflicting information, do not return phone calls and rude and testy with us when we call. Major barriers to care that clients have discussed with providers over the past 12 months are listed below. Transportation is reported to be a big issue along with confusion about the health care system and ACA. Page 101 of 123

103 Distance from medical facilities Unemployment Finances, losing insurance, cost of medications, difficulty getting transportation to appointments Medical insurance Health insurance, homelessness, unemployment PAY SOURCE "Many the lack of understanding in keeping their appointments improves outcomes Need services not HIV related but that impacts their healthcare and still can't get them. Getting the insurance information sent to them to get what is needed covered." One of their major barriers is having to go to and follow-up with so may different agencies and organizations. Many of them get confused, which leads to frustration and a host of unwanted feelings. Some of them drop out of care because of it. Cost of medications and the health care system not being easy to access Housing and financial stability "Confusion or not really knowing where to go for help Confusion or not knowing what each part of Ryan White provides" Conflicting information about how to navigate the system, what paperwork is required. Many have never been medically covered by insurance in the past. They are medically naive and do not understand the complexities of the system and self-care responsibilities. Providers were asked the same question that was asked in both client survey s regarding the most important services they feel help client s management their HIV/AIDS diagnosis. Providers ranked #1 as medication, #2 as outpatient/ambulatory medical care, #3 as transportation, #4 mental health services, #5 dental care, #6 case management, #7 was tied between specialty care and early intervention services, #8 was tied four ways; vision, health insurance assistance, substance use services and emergency financial assistance. Food assistance and housing services tied for 9 th place while HIV health classes, outreach and psychosocial support tied for 10 th place. The rest of their responses can be found in the table below. Page 102 of 123

104 Rank Answer Options Providers were also asked what barriers their agency typically encounters when trying to provide services to clients. The most indicated reasons were; clients routinely miss appointments, clients don t have a payment source, and clients have trouble getting to our offices. Response Percent 1 Medication (help paying for and getting HIV/AIDS related medications including ADAP) 94.4% 17 2 Outpatient Medical Care (an appointment with a doctor to take care of your ongoing HIV treatment, including labs-cd4 and 88.9% 16 3 Transportation (bus pass, gas voucher, van transportation all for medically related needs only) 83.3% 15 4 Mental Health Services (individual or group counseling for mental health issues - including support groups) 77.8% 14 5 Dental Care (annual teeth cleaning, visit with a dentist) 66.7% 12 6 Case Management (someone to help coordinate the services you need, provide referrals for services, and help getting public 61.1% 11 7 Specialty Care (an appointment with a specialist, for example dermatologist or gynecologist) 50.0% 9 7 Early Intervention Services (finding HIV positive people and getting them into care) 50.0% 9 8 Vision (appointment with optometrist, eyeglasses) 44.4% 8 8 Health Insurance Assistance (help with premiums and co-payments to private health insurance plans, including COBRA) 44.4% 8 8 Substance Use Services (individual or group counseling for substance use issues - including support groups) 44.4% 8 8 Emergency Financial Assistance (short term money for utilities, rent/mortgage) 44.4% 8 9 Food Assistance (food voucher, basket of food, food pantry) 38.9% 7 9 Housing services (help with rent/mortgage payment) 38.9% 7 10 HIV and Health Classes (healthy relations, HIV 101) 27.8% 5 10 Outreach (HIV Testing and linkage to medical and support services) 27.8% 5 10 Psychosocial Support (support groups) 27.8% 5 Treatment adherence counseling (someone to help you understand your medications and doctor's instructions, and 11 strategies to keep with your prescribed medications schedule) 22.2% 4 12 Nutrition Services (meeting with a registered dietician, access to supplements such as Boost) 16.7% 3 12 Hospice Services (comfort care and pain management for terminally ill or seriously ill patient) 16.7% 3 12 Substance Abuse Services-Residential (treatment in a residential health setting that is short term) 16.7% 3 13 Child Care Services (child care while you are at doctors appointments) 11.1% 2 13 Language Services (interpretation and translation) 11.1% 2 13 Referrals for Health Care/Supportive Services 11.1% 2 14 Partner Notification Services (help confidentially informing people that you might have put at risk for HIV) 5.6% 1 14 Home Health Care (doctor ordered skilled nursing care in the patients home) 5.6% 1 15 Legal services (help with a do not resuscitate order, estate planning, discrimination) 0.0% 0 15 Rehabilitation Services (occupational therapy, speech therapy) 0.0% 0 15 Respite Care (break for HIV caregivers) 0.0% 0 Response Count Page 103 of 123


105 Providers were asked what services their agency provides and what they have the capacity to provide with more funding/training. Several service providers indicated they have the capacity to expand with more funding into services such as; substance abuse residential, home health care, hospice services, home delivered meals, respite care, and child care. Page 104 of 123


106 Page 105 of 123

107 Page 106 of 123


108 Just one provider said they have a wait time at their agency with 94% saying they do not. The wait time was outlined as long term housing, months. Providers were also asked how they stay up to date with services in the community. Most responses included some type of meeting and/or the internet. A suggestion for keeping everyone up to date was is a newsletter from the grantee or planning council. Meetings, internet Weekly meetings with health district Make sure ryan white program to continue services Attend community meetings, call community partners for updates Through the action planning meetings, Gathering, s Page 107 of 123


109 Monthly meetings with community partners We network with agencies to see what is happening in the community Attend Meetings with others in the community who provide services for HIV/AIDS. Pick up the phone and ask Community meetings once a month A monthly newsletter from the Grant Administrators or Planning Council would be helpful Bringing the A's B's and C's together Make sure ryan white program to continue services Transportation to appointments Streamline services and programs We need more funds for emergencies. More transportation is definitely needed. People should have transportation to food banks 5 days a week. The Grant Administrator needs to think about how they can assist the providers in accessing Medicaid services for their patients. Then develop an algorithm detailing what medical staff/case managers need to do to assist their clients in obtaining the services they need. Make sure ryan white program to continue services We need funds to help individuals with furniture and house hold needs. I know individuals who do not have a bed. Maybe we could hire PR people to seek out funds for all agencies use. Page 108 of 123
Needs Assessment of People Living with HIV in the Boston EMA. Needs Resources and Allocations Committee March 10 th, 2016
 Needs Assessment of People Living with HIV in the Boston EMA Needs Resources and Allocations Committee March 10 th, 2016 Presentation Overview 1. What is a Needs Assessment? 2. The Numbers o Epidemiological
Needs Assessment of People Living with HIV in the Boston EMA Needs Resources and Allocations Committee March 10 th, 2016 Presentation Overview 1. What is a Needs Assessment? 2. The Numbers o Epidemiological
Ryan White Consumer Satisfaction Project Grant Year
 Ryan White Consumer Satisfaction Project Grant Year 2014-2015 Ryan White Part A Las Vegas TGA HIV/AIDS Program Consumer Satisfaction Project Grant Year 2014-2015: Las Vegas Transitional Grant Area Ryan
Ryan White Consumer Satisfaction Project Grant Year 2014-2015 Ryan White Part A Las Vegas TGA HIV/AIDS Program Consumer Satisfaction Project Grant Year 2014-2015: Las Vegas Transitional Grant Area Ryan
Housing Needs Assessment Survey Tool
 Appendix II -Year Chicago Area HIV/AIDS Housing Plan A-9 Housing Needs Assessment Survey Tool Appendix II consists of the English Housing Needs Assessment Survey tool (the Spanish-language survey is not
Appendix II -Year Chicago Area HIV/AIDS Housing Plan A-9 Housing Needs Assessment Survey Tool Appendix II consists of the English Housing Needs Assessment Survey tool (the Spanish-language survey is not
2014 County of Marin Fact Sheet: HIV/AIDS in Marin County
 2014 County of Marin Fact Sheet: HIV/AIDS in Marin County HIV/AIDS epidemiology data is from the enhanced HIV/AIDS Reporting System (ehars) maintained by the Office of AIDS. The data presented here are
2014 County of Marin Fact Sheet: HIV/AIDS in Marin County HIV/AIDS epidemiology data is from the enhanced HIV/AIDS Reporting System (ehars) maintained by the Office of AIDS. The data presented here are
2009 CONSUMER FOCUS GROUP DEMOGRAPHIC & ASSESSMENT OF SERVICES SURVEY
 2009 CONSUMER FOCUS GROUP DEMOGRAPHIC & ASSESSMENT OF SERVICES SURVEY Thank you for participating in the 2009 Consumer Focus Group Project. The New York City Department of Health and Mental Hygiene administers
2009 CONSUMER FOCUS GROUP DEMOGRAPHIC & ASSESSMENT OF SERVICES SURVEY Thank you for participating in the 2009 Consumer Focus Group Project. The New York City Department of Health and Mental Hygiene administers
Gaps Analysis BARRIERS
 Gaps Analysis MOST COMMONLY REPORTED BARRIERS Core Services For the core services, the three barriers reported most often by all 764 survey respondents were difficulties making or keeping appointments,
Gaps Analysis MOST COMMONLY REPORTED BARRIERS Core Services For the core services, the three barriers reported most often by all 764 survey respondents were difficulties making or keeping appointments,
Location of RSR Client-level Data Elements in CAREWare Updated Sept 2017
 Location of RSR Client-level Data Elements in CAREWare Updated Sept 2017 Demographics Required of all clients that received any core medical or support service if they are ELIGIBLE for RWHAP services.
Location of RSR Client-level Data Elements in CAREWare Updated Sept 2017 Demographics Required of all clients that received any core medical or support service if they are ELIGIBLE for RWHAP services.
THE EMERGE SURVEY ON TAKING PART IN BIOBANK RESEARCH: VERSION A
 THE EMERGE SURVEY ON TAKING PART IN BIOBANK RESEARCH: VERSION A What is this survey about? This survey is about your views on taking part in medical research. We want to understand what you think about
THE EMERGE SURVEY ON TAKING PART IN BIOBANK RESEARCH: VERSION A What is this survey about? This survey is about your views on taking part in medical research. We want to understand what you think about
New Hampshire Continua of Care. PATH Street Outreach Program Entry Form for HMIS
 Please refer to the 2014 HUD HMIS Data Standards Version 5.1, available on the NH-HMIS website: www.nh-hmis.org for an explanation of the data elements in this form. Date form completed: Outreach worker
Please refer to the 2014 HUD HMIS Data Standards Version 5.1, available on the NH-HMIS website: www.nh-hmis.org for an explanation of the data elements in this form. Date form completed: Outreach worker
Ryan White Part A Overview Kimberlin Dennis Melissa Rodrigo March 21, 2018
 Ryan White Part A Overview Kimberlin Dennis Melissa Rodrigo March 21, 2018 Part A Program = Partnership Regional HIV Planning Council Cuyahoga County Board of Health One Purpose Ryan White Legislation
Ryan White Part A Overview Kimberlin Dennis Melissa Rodrigo March 21, 2018 Part A Program = Partnership Regional HIV Planning Council Cuyahoga County Board of Health One Purpose Ryan White Legislation
Respond to the following questions for all household members each adult and child. A separate form should be included for each household member.
 HMIS Data Collection Template for Project ENTRY CoC Program This form can be used by all CoC-funded project types: Prevention, Street Outreach, Safe Haven, Transitional Housing, Rapid Re-housing, Permanent
HMIS Data Collection Template for Project ENTRY CoC Program This form can be used by all CoC-funded project types: Prevention, Street Outreach, Safe Haven, Transitional Housing, Rapid Re-housing, Permanent
Nashville HMIS Intake Template Use COC Funded Projects: HMIS Intake at Entry Template
 HMIS Data Collection Template for Project ENTRY CoC Program This form can be used by all CoC-funded project types: Prevention, Street Outreach, Safe Haven, Transitional Housing, Rapid Re-housing, Permanent
HMIS Data Collection Template for Project ENTRY CoC Program This form can be used by all CoC-funded project types: Prevention, Street Outreach, Safe Haven, Transitional Housing, Rapid Re-housing, Permanent
RSR Crosswalk. Variable Client Race Race ID Values White 1 Black 2 Asian 3 Hawaiian / PI 4 Native American (AK native) 5
 5") October 2017 Purpose RSR Crosswalk This document can help you compare the data you currently collect in your data management system to the data required in the Ryan White Services Report (RSR). The Crosswalk
October 2017 Purpose RSR Crosswalk This document can help you compare the data you currently collect in your data management system to the data required in the Ryan White Services Report (RSR). The Crosswalk
HIV Prevention Service Provider Survey 2014
 Respondent Demographics This survey will help the Florida HIV Prevention Planning Group (PPG) establish the resources and unmet needs of the communities we serve. Please take a few minutes to complete
Respondent Demographics This survey will help the Florida HIV Prevention Planning Group (PPG) establish the resources and unmet needs of the communities we serve. Please take a few minutes to complete
Homeless veterans in Minnesota 2006
 Homeless veterans in Minnesota 2006 Statewide survey of veterans without permanent shelter summary November 2007 Wilder Research Center 1295 Bandana Boulevard North, Suite 210 Saint Paul, Minnesota 55108
Homeless veterans in Minnesota 2006 Statewide survey of veterans without permanent shelter summary November 2007 Wilder Research Center 1295 Bandana Boulevard North, Suite 210 Saint Paul, Minnesota 55108
The Homeless Census & Homeless Point-in-time Survey Summary report Metro Louisville, 2009
 The Homeless Census & Homeless Point-in-time Survey Summary report Metro Louisville, 2009 Prepared by the Coalition for the Homeless 1 Each year, the Coalition for the Homeless prepares two annual counts.
The Homeless Census & Homeless Point-in-time Survey Summary report Metro Louisville, 2009 Prepared by the Coalition for the Homeless 1 Each year, the Coalition for the Homeless prepares two annual counts.
Home and Community Based Services (HCBS)
") To Whom It May Concern: To be considered for membership, the following must be submitted: 1. A Fountain House Membership Application and supplementary substance abuse questionnaire (included at the end
To Whom It May Concern: To be considered for membership, the following must be submitted: 1. A Fountain House Membership Application and supplementary substance abuse questionnaire (included at the end
First Name Middle Name Last Name Name You Prefer Date
 Supportive Housing for Homeless Women & Families Application for Residency First Fruit Ministries 2750 Vance Street Wilmington, NC 28412 Phone 910.794.9656 Fax 910.794.9657 First Name Middle Name Last
Supportive Housing for Homeless Women & Families Application for Residency First Fruit Ministries 2750 Vance Street Wilmington, NC 28412 Phone 910.794.9656 Fax 910.794.9657 First Name Middle Name Last
Enhanced Housing Placement Assistance (EHPA): Baseline Characteristics of Homeless PLWHA in New York City
: Baseline Characteristics of Homeless PLWHA in New York City") Enhanced Housing Placement Assistance (EHPA): Baseline Characteristics of Homeless PLWHA in New York City Rachel Johnson, MPH John Rojas, MPA NEW YORK CITY DEPARTMENT OF HEALTH AND MENTAL HYGIENE North
Enhanced Housing Placement Assistance (EHPA): Baseline Characteristics of Homeless PLWHA in New York City Rachel Johnson, MPH John Rojas, MPA NEW YORK CITY DEPARTMENT OF HEALTH AND MENTAL HYGIENE North
Transitional Housing Application
 Transitional Housing Application Applicant Information Name: Date of birth: SSN: ID Number: Current address: City: State: ZIP Code: Phone: Email: Name of Last Social Worker or Probation Officer:: Original
Transitional Housing Application Applicant Information Name: Date of birth: SSN: ID Number: Current address: City: State: ZIP Code: Phone: Email: Name of Last Social Worker or Probation Officer:: Original
Glossary of Terms. Commercial Sex Worker: Self-reported as having received money, drugs or favors in exchange for sex.
 ADAP: AIDS Drug Assistance Program funded through Part B. Congress earmarks funds that must be used for ADAP, an important distinction since other Part B spending decisions are made locally. AIDS: Acquired
ADAP: AIDS Drug Assistance Program funded through Part B. Congress earmarks funds that must be used for ADAP, an important distinction since other Part B spending decisions are made locally. AIDS: Acquired
HIV Initiative HIV Initiative Companion
 HIV Initiative 2017-18 HIV Initiative Companion 1 Contents OVERVIEW...3 GOAL 3 DATES 3 SLOGAN 3 DISCLOSURES 3 OUTREACH BUDGET 3 TIPS FOR PERFORMING OUTREACH...4 KNOW THE BASICS OF HIV 4 REVIEW THE OLDER
HIV Initiative 2017-18 HIV Initiative Companion 1 Contents OVERVIEW...3 GOAL 3 DATES 3 SLOGAN 3 DISCLOSURES 3 OUTREACH BUDGET 3 TIPS FOR PERFORMING OUTREACH...4 KNOW THE BASICS OF HIV 4 REVIEW THE OLDER
Community Homelessness Assessment, Local Education and Networking Groups (CHALENG)
") June 2016 Community Homelessness Assessment, Local Education and Networking Groups (CHALENG) Community Homelessness Assessment, Local Education and Networking Groups for, commonly referred to as Project
June 2016 Community Homelessness Assessment, Local Education and Networking Groups (CHALENG) Community Homelessness Assessment, Local Education and Networking Groups for, commonly referred to as Project
The AETC-NMC Webinar entitled: will begin shortly.
 The AETC-NMC Webinar entitled: 1 will begin shortly. The AETC-NMC Webinar entitled: 2 will begin shortly. Kindly enjoy the following informative slides while you wait for the presentation to begin.. 3
The AETC-NMC Webinar entitled: 1 will begin shortly. The AETC-NMC Webinar entitled: 2 will begin shortly. Kindly enjoy the following informative slides while you wait for the presentation to begin.. 3
HIV Testing Survey, 2002
 Special Surveillance Report Number 5 HIV Testing Survey, 2002 DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service Centers for Disease Control and Prevention Atlanta, Georgia 30333 . The HIV/AIDS
Special Surveillance Report Number 5 HIV Testing Survey, 2002 DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service Centers for Disease Control and Prevention Atlanta, Georgia 30333 . The HIV/AIDS
WELCOME TO AGEWELL MEDICAL ASSOCIATES
 WELCOME TO AGEWELL MEDICAL ASSOCIATES We offer the following checklist and suggestions to help make your first visit as easy and pleasant as possible. What to bring with you: [ ] All of your medications
WELCOME TO AGEWELL MEDICAL ASSOCIATES We offer the following checklist and suggestions to help make your first visit as easy and pleasant as possible. What to bring with you: [ ] All of your medications
Registration Form Women s Health Initiative
 YWCA WHI 1500 14 th St. Lubbock, Texas 79401 Phone: (806) 687-8858 Fax: (806) 784-0698 1 Registration Form Women s Health Initiative Date: Name (Last, First, middle, Maiden) Age: Date of Birth SS # Mailing
YWCA WHI 1500 14 th St. Lubbock, Texas 79401 Phone: (806) 687-8858 Fax: (806) 784-0698 1 Registration Form Women s Health Initiative Date: Name (Last, First, middle, Maiden) Age: Date of Birth SS # Mailing
Teen Sexual Health Survey
 Instructions Teen Sexual Health Survey Thank you for taking part in our survey. DO NOT write your name on this survey. The answers you give will be kept private. No one will know what you write. Answer
Instructions Teen Sexual Health Survey Thank you for taking part in our survey. DO NOT write your name on this survey. The answers you give will be kept private. No one will know what you write. Answer
To: Our Medicare Patients. Subject: Your Welcome to Medicare Exam
 To: Our Medicare Patients Subject: Your Welcome to Medicare Exam Medicare covers a one-time Welcome to Medicare visit. The Welcome to Medicare visit must occur during your first twelve months as a Medicare
To: Our Medicare Patients Subject: Your Welcome to Medicare Exam Medicare covers a one-time Welcome to Medicare visit. The Welcome to Medicare visit must occur during your first twelve months as a Medicare
YMCA of Reading & Berks County Housing Application
 YMCA of Reading & Berks County Housing Application Overall Eligibility Criteria To be eligible for these programs (not including SRO), applicants must be: Homeless Drug and alcohol free for at least 5
YMCA of Reading & Berks County Housing Application Overall Eligibility Criteria To be eligible for these programs (not including SRO), applicants must be: Homeless Drug and alcohol free for at least 5
CBT Intake Form. Patient Name: Preferred Name: Last. First. Best contact phone number: address: Address:
 Patient Information CBT Intake Form Patient Name: Preferred Name: Last Date of Birth: _// Age: _ First MM DD YYYY Gender: Best contact phone number: Email address: _ Address: _ Primary Care Physician:
Patient Information CBT Intake Form Patient Name: Preferred Name: Last Date of Birth: _// Age: _ First MM DD YYYY Gender: Best contact phone number: Email address: _ Address: _ Primary Care Physician:
2016 Houston HIV Care Services Needs Assessment: Profile of African American Men Who Have Sex with Men (MSM)
") 2016 Houston HIV Care Services Needs Assessment: Profile of African American Men Who Have Sex with Men (MSM) Page 1 PROFILE OF AFRICAN AMERICAN MSM A recent analysis of national HIV diagnosis rates revealed
2016 Houston HIV Care Services Needs Assessment: Profile of African American Men Who Have Sex with Men (MSM) Page 1 PROFILE OF AFRICAN AMERICAN MSM A recent analysis of national HIV diagnosis rates revealed
2-1-1 Database Benefits of Services
 Nevada 2-1-1 is part of a nationwide network of call centers that provide information and referral (I&R) services to Nevada residents. Available information includes basic human services, physical and
Nevada 2-1-1 is part of a nationwide network of call centers that provide information and referral (I&R) services to Nevada residents. Available information includes basic human services, physical and
Persons Living with HIV/AIDS, San Mateo County Comparison
 Persons Living with HIV/AIDS, San Mateo County Comparison As of December 2008, there were 1,152 persons living with HIV or HIV/AIDS in San Mateo County (Table 1). Compared to California and the United
Persons Living with HIV/AIDS, San Mateo County Comparison As of December 2008, there were 1,152 persons living with HIV or HIV/AIDS in San Mateo County (Table 1). Compared to California and the United
Conscious Living Counseling & Education Center 3239 Oak Ridge Loop East, West Fargo ND (701)
") Conscious Living Counseling & Education Center 3239 Oak Ridge Loop East, West Fargo ND 58078 (701) 478-7199 INTAKE FORM BIRTH DATE: / / Age: Email: YOUR NAME FIRST: MIDDLE INITIAL: LAST: YOUR ADDRESS COMPLETE
Conscious Living Counseling & Education Center 3239 Oak Ridge Loop East, West Fargo ND 58078 (701) 478-7199 INTAKE FORM BIRTH DATE: / / Age: Email: YOUR NAME FIRST: MIDDLE INITIAL: LAST: YOUR ADDRESS COMPLETE
Data: Access, Sources, and Systems
 EXEMPLARY INTEGRATED HIV PREVENTION AND CARE PLAN SECTIONS Data: Access, Sources, and Systems REGION PLAN TYPE JURISDICTIONS HIV PREVALENCE Midwest Integrated state-only prevention and care plan State
EXEMPLARY INTEGRATED HIV PREVENTION AND CARE PLAN SECTIONS Data: Access, Sources, and Systems REGION PLAN TYPE JURISDICTIONS HIV PREVALENCE Midwest Integrated state-only prevention and care plan State
Albany County Coordinated Entry Assessment version 12, 11/29/16
 Referral Completed by: PRE-SCREENING INFORMATION FOR SHELTER REFERRAL 1. First Name Last Name Date/Time: Other names (including nicknames): 2. Has client previously completed an application for assistance
Referral Completed by: PRE-SCREENING INFORMATION FOR SHELTER REFERRAL 1. First Name Last Name Date/Time: Other names (including nicknames): 2. Has client previously completed an application for assistance
State of Alabama AIDS Drug Assistance Program (ADAP) Quarterly Report
 Quarterly Report") State of Alabama AIDS Drug Assistance Program (ADAP) Quarterly Report This report reflects active clients currently enrolled in ADAP Full-pay Prescription Program (ADAP-Rx), Alabama s Insurance Assistance
State of Alabama AIDS Drug Assistance Program (ADAP) Quarterly Report This report reflects active clients currently enrolled in ADAP Full-pay Prescription Program (ADAP-Rx), Alabama s Insurance Assistance
Respond to the following questions for all household members each adult and child. A separate form should be included for each household member.
 HMIS Data Collection Template for Project EXIT CoC Program This form can be used by all CoC-funded project types: Street Outreach, Safe Haven, Transitional Housing, Rapid Rehousing, and Permanent Supportive
HMIS Data Collection Template for Project EXIT CoC Program This form can be used by all CoC-funded project types: Street Outreach, Safe Haven, Transitional Housing, Rapid Rehousing, and Permanent Supportive
Transitional, Intergenerational Group Residence Application. Texas ID# Primary Language: Address: City, State, Zip Code: Phone-home ( ) Phone-work ( )
 Phone-work ( )") PERSONAL/FAMILY INFORMATION Name Date Date of Birth / / SS # Gender Texas ID# Primary Language: Marital Status: Single Divorced Common Law Living Together Married & living with Spouse not living with Spouse
PERSONAL/FAMILY INFORMATION Name Date Date of Birth / / SS # Gender Texas ID# Primary Language: Marital Status: Single Divorced Common Law Living Together Married & living with Spouse not living with Spouse
2016 Houston HIV Care Services Needs Assessment: Profile of the Recently Released
 2016 Houston HIV Care Services Needs Assessment: Profile of the Recently Released Page 1 PROFILE OF THE RECENTLY RELEASED The Texas Department of Criminal Justice (TDCJ) estimates that 386 people living
2016 Houston HIV Care Services Needs Assessment: Profile of the Recently Released Page 1 PROFILE OF THE RECENTLY RELEASED The Texas Department of Criminal Justice (TDCJ) estimates that 386 people living
UNC Family Health Study
 Health Cognition & Behavior Lab Person County Pilot Study on HPV Vaccination (2006) Updated 04/30/2010 This study was conducted with women (n=146) in two healthcare facilities in Person County (a rural
Health Cognition & Behavior Lab Person County Pilot Study on HPV Vaccination (2006) Updated 04/30/2010 This study was conducted with women (n=146) in two healthcare facilities in Person County (a rural
Substance Abuse Services. AIDS Drug Assistance. Oral Health Care. Program (ADAP) Medical Care
 Medical Care") 2017-2018 Council for HIV/AIDS Care and Prevention Core Medical Service Area Paired Comparison Analysis Prioritization Worksheet Medical Case Management Services Substance Abuse Services - Outpatient AIDS
2017-2018 Council for HIV/AIDS Care and Prevention Core Medical Service Area Paired Comparison Analysis Prioritization Worksheet Medical Case Management Services Substance Abuse Services - Outpatient AIDS
Lions Sight & Hearing Foundation Phone: Fax: Hearing Aid: Request for assistance
 Lions Sight & Hearing Foundation Phone: 602-954-1723 Fax: 602-954-1768 Hearing Aid: Request for assistance 3427 N 32 nd Street office use only Date received Case number Applicant: (Name; please print clearly)
Lions Sight & Hearing Foundation Phone: 602-954-1723 Fax: 602-954-1768 Hearing Aid: Request for assistance 3427 N 32 nd Street office use only Date received Case number Applicant: (Name; please print clearly)
Responding to HIV/AIDS in Illinois Remarks to the Adequate Health Care Task Force
 Responding to HIV/AIDS in Illinois Remarks to the Adequate Health Care Task Force AIDS Foundation of Chicago June 27, 2006 AIDS-Related Deaths Since 1981 United States: 530,000 Illinois: 18,000 Chicago:
Responding to HIV/AIDS in Illinois Remarks to the Adequate Health Care Task Force AIDS Foundation of Chicago June 27, 2006 AIDS-Related Deaths Since 1981 United States: 530,000 Illinois: 18,000 Chicago:
Health Care Professional Questionnaire
 Methodology An online survey, titled Let's Talk About Sexual Health Warts and All, was fielded from February 25 March 28, 2016 by HealthyWomen, in partnership with PharmaDerm, a division of Fougera Pharmaceuticals
Methodology An online survey, titled Let's Talk About Sexual Health Warts and All, was fielded from February 25 March 28, 2016 by HealthyWomen, in partnership with PharmaDerm, a division of Fougera Pharmaceuticals
WASHINGTON STATE COMPARISONS TO: KITSAP COUNTY CORE PUBLIC HEALTH INDICATORS May 2015
 WASHINGTON STATE COMPARISONS TO: KITSAP COUNTY CORE PUBLIC HEALTH INDICATORS This is a companion document to the Core Public Health Indicators that provides a comparison of to Washington State for the
WASHINGTON STATE COMPARISONS TO: KITSAP COUNTY CORE PUBLIC HEALTH INDICATORS This is a companion document to the Core Public Health Indicators that provides a comparison of to Washington State for the
Medicare Wellness Visit
 of Birth: Today s : Medicare Wellness Visit Dear Patient, Your Medicare benefits include an Annual Wellness Visit to assist in preventing illness or detect illness at an early stage. Your Annual Wellness
of Birth: Today s : Medicare Wellness Visit Dear Patient, Your Medicare benefits include an Annual Wellness Visit to assist in preventing illness or detect illness at an early stage. Your Annual Wellness
Terms related to Epidemiologic Data. Needs Assessment Components:
 Using Data, Assessing Needs: Quick Definitions and Descriptions for Data-Related Terms and Concepts Used by Ryan White HIV/AIDS Program (RWHAP) Planning Bodies 1 Terms related to Epidemiologic Data Population:
Using Data, Assessing Needs: Quick Definitions and Descriptions for Data-Related Terms and Concepts Used by Ryan White HIV/AIDS Program (RWHAP) Planning Bodies 1 Terms related to Epidemiologic Data Population:
National Survey of Young Adults on HIV/AIDS
 Topline Kaiser Family Foundation National Survey of Young Adults on HIV/AIDS November 30, 2017 The 2017 Kaiser Family Foundation National Survey of Young Adults on HIV/AIDS is based on interviews with
Topline Kaiser Family Foundation National Survey of Young Adults on HIV/AIDS November 30, 2017 The 2017 Kaiser Family Foundation National Survey of Young Adults on HIV/AIDS is based on interviews with
Advancing the National HIV/AIDS Strategy: Housing and the HCCI. Housing Summit Los Angeles, CA
 Advancing the National HIV/AIDS Strategy: Housing and the HCCI Housing Summit Los Angeles, CA October 21, 2014 The National HIV/AIDS Strategy Facets of the Strategy Limited number of action steps Sets
Advancing the National HIV/AIDS Strategy: Housing and the HCCI Housing Summit Los Angeles, CA October 21, 2014 The National HIV/AIDS Strategy Facets of the Strategy Limited number of action steps Sets
NJ s Transitional Housing Initiative
 NJ s Transitional Housing Initiative SARA WALLACH, DOH DHSTS PROGRAM MANAGEMENT OFFICER ANNIE CHEN, ARFC CHIEF OPERATING OFFICER Definition of Homeless person According to the Department of Housing and
NJ s Transitional Housing Initiative SARA WALLACH, DOH DHSTS PROGRAM MANAGEMENT OFFICER ANNIE CHEN, ARFC CHIEF OPERATING OFFICER Definition of Homeless person According to the Department of Housing and
problems/medications: Current supplements/vitamins/herbs: Past medical problems/medications: Other doctors/clinics seen regularly:
 Main Purpose of the consultation (Please give a brief summary of the main problems) What happened to make you seek evaluation at this time? MEDICAL HISTORY Current medical Prior Attempts to correct the
Main Purpose of the consultation (Please give a brief summary of the main problems) What happened to make you seek evaluation at this time? MEDICAL HISTORY Current medical Prior Attempts to correct the
Guidelines for Implementing Pre-Exposure Prophylaxis For The Prevention of HIV in Youth Peter Havens, MD MS Draft:
 Guidelines for Implementing Pre-Exposure Prophylaxis For The Prevention of HIV in Youth Peter Havens, MD MS Draft: 10-2-2015 Clinical studies demonstrate that when a person without HIV infection takes
Guidelines for Implementing Pre-Exposure Prophylaxis For The Prevention of HIV in Youth Peter Havens, MD MS Draft: 10-2-2015 Clinical studies demonstrate that when a person without HIV infection takes
LET S TALK about Sticking with your treatment plan
 LET S TALK about Sticking with your treatment plan HOW ONGOING HIV CARE HELPS YOU LIVE A LONGER AND HEALTHIER LIFE Your treatment plan is vital to your overall health (and to reducing HIV transmission)
LET S TALK about Sticking with your treatment plan HOW ONGOING HIV CARE HELPS YOU LIVE A LONGER AND HEALTHIER LIFE Your treatment plan is vital to your overall health (and to reducing HIV transmission)
St. Louis County Project Homeless Connect. Summary of guests served on November 5, 2008
 St. Louis County Project Homeless Connect Summary of guests served on November 5, 2008 D E C E M B E R 2 0 0 8 St. Louis County Project Homeless Connect Summary of guests served on November 5, 2008 December
St. Louis County Project Homeless Connect Summary of guests served on November 5, 2008 D E C E M B E R 2 0 0 8 St. Louis County Project Homeless Connect Summary of guests served on November 5, 2008 December
Next, I m going to ask you to read several statements. After you read each statement, circle the number that best represents how you feel.
 Participant ID: Interviewer: Date: / / The [clinic name], Devers Eye Institute, and the Northwest Portland Area Indian Health Board are doing a survey about beliefs and behaviors related to eye health
Participant ID: Interviewer: Date: / / The [clinic name], Devers Eye Institute, and the Northwest Portland Area Indian Health Board are doing a survey about beliefs and behaviors related to eye health
1 3/04/15. University of California Global Food Initiative - Got Food? Survey. 1) Where do you currently live? Agree a lot.
 Where do you currently live? Agree a lot.") 1) Where do you currently live? o Campus residence hall o Fraternity or sorority house college/university housing o Parent/guardian s home off-campus housing o With a friend until I find other housing
1) Where do you currently live? o Campus residence hall o Fraternity or sorority house college/university housing o Parent/guardian s home off-campus housing o With a friend until I find other housing
2017 Social Service Funding Application Non-Alcohol Funds
 2017 Social Service Funding Application Non-Alcohol Funds Applications for 2017 funding must be complete and submitted electronically to the City Manager s Office at ctoomay@lawrenceks.org by 5:00 pm on
2017 Social Service Funding Application Non-Alcohol Funds Applications for 2017 funding must be complete and submitted electronically to the City Manager s Office at ctoomay@lawrenceks.org by 5:00 pm on
4 Ways to Provide Housing and Healthcare to Homeless Persons Living with HIV/AIDS
 4 Ways to Provide Housing and Healthcare to Homeless Persons Living with HIV/AIDS White Paper / October 2016 702.605.6870 / support@clarityhs.com / www.clarityhumanservices.com / www.bitfocus.com EXECUTIVE
4 Ways to Provide Housing and Healthcare to Homeless Persons Living with HIV/AIDS White Paper / October 2016 702.605.6870 / support@clarityhs.com / www.clarityhumanservices.com / www.bitfocus.com EXECUTIVE
Palm Beach County Integrated Prevention and Patient Care Plan
 Palm Beach County Integrated Prevention and Patient Care Plan Introduction The Palm Beach County Coordinated Services Network (CSN) is a partnership of state and federal funding sources, planning authorities,
Palm Beach County Integrated Prevention and Patient Care Plan Introduction The Palm Beach County Coordinated Services Network (CSN) is a partnership of state and federal funding sources, planning authorities,
Substance Abuse Treatment/Counseling
 Substance Abuse Treatment/Counseling Pg Service Category Definition - Part A 1 Public Comment re Substance Abuse Block Grant Funds, February 2018 2016 Houston HIV Care Services Needs Assessment Substance
Substance Abuse Treatment/Counseling Pg Service Category Definition - Part A 1 Public Comment re Substance Abuse Block Grant Funds, February 2018 2016 Houston HIV Care Services Needs Assessment Substance
2016 Collier County Florida Health Assessment Executive Summary
 2016 Florida Health Assessment Executive Summary Prepared by: The Health Planning Council of Southwest Florida, Inc. www.hpcswf.com Executive Summary To access the report in its entirety, visit http://www.hpcswf.com/health-planning/health-planningprojects/.
2016 Florida Health Assessment Executive Summary Prepared by: The Health Planning Council of Southwest Florida, Inc. www.hpcswf.com Executive Summary To access the report in its entirety, visit http://www.hpcswf.com/health-planning/health-planningprojects/.
Miami-Dade County Getting to Zero HIV/AIDS Task Force Implementation Report
 1 Miami-Dade County Getting to Zero HIV/AIDS Task Force Implementation Report Make HIV History! Know the Facts Get Tested Get Treated 2017-2018 7/9/2018 1 2 7/9/2018 2 3 Progress on the Getting to Zero
1 Miami-Dade County Getting to Zero HIV/AIDS Task Force Implementation Report Make HIV History! Know the Facts Get Tested Get Treated 2017-2018 7/9/2018 1 2 7/9/2018 2 3 Progress on the Getting to Zero
USING A QUALITY IMPROVEMENT COHORT MODEL TO ACHIEVE HEALTH EQUITY
 USING A QUALITY IMPROVEMENT COHORT MODEL TO ACHIEVE HEALTH EQUITY Katrease Hale Ryan White Quality Manager Leanne F. Savola HIV/STI Programs Director OBJECTIVES Describe a Metro Detroit quality improvement
USING A QUALITY IMPROVEMENT COHORT MODEL TO ACHIEVE HEALTH EQUITY Katrease Hale Ryan White Quality Manager Leanne F. Savola HIV/STI Programs Director OBJECTIVES Describe a Metro Detroit quality improvement
Personal Information. Full Name: Address: Primary Phone: Yes No Provider Yes No. Alternate Phone: Yes No Provider Yes No
 OFFICE USE ONLY: Date of Intake: ID#: Staff mbr: Personal Information Full Name: Address: _ Last First M.I. Street Address Apartment/Unit # City State Zip Code County Date of Birth: Age: Mobile phone?
OFFICE USE ONLY: Date of Intake: ID#: Staff mbr: Personal Information Full Name: Address: _ Last First M.I. Street Address Apartment/Unit # City State Zip Code County Date of Birth: Age: Mobile phone?
ADULT INTAKE QUESTIONNAIRE. Ok to leave message? Yes No. Present psychological difficulties please check any that apply to you at this time.
 ADULT INTAKE QUESTIONNAIRE Name: Today s Date: Age: Date of Birth: Address: Home phone: Work phone: Cell phone: Ok to leave message? Yes No Ok to leave message? Yes No Ok to leave message? Yes No Email:
ADULT INTAKE QUESTIONNAIRE Name: Today s Date: Age: Date of Birth: Address: Home phone: Work phone: Cell phone: Ok to leave message? Yes No Ok to leave message? Yes No Ok to leave message? Yes No Email:
2013 HOUSING STATUS SURVEY RESULTS. A Report on the Sheltered and Unsheltered Homeless in Billings
 2013 HOUSING STATUS SURVEY RESULTS A Report on the Sheltered and Unsheltered Homeless in Billings HUD Defined Homeless To be counted as homeless under HUD s definition, respondents had to indicate that
2013 HOUSING STATUS SURVEY RESULTS A Report on the Sheltered and Unsheltered Homeless in Billings HUD Defined Homeless To be counted as homeless under HUD s definition, respondents had to indicate that
History and Program Information
 History and Program Information Rita da Cascia/ / Project Positive Match, San Francisco, CA Housing Opportunities for People with AIDS (HOPWA) Special Projects of National Significance (SPNS) Multiple
History and Program Information Rita da Cascia/ / Project Positive Match, San Francisco, CA Housing Opportunities for People with AIDS (HOPWA) Special Projects of National Significance (SPNS) Multiple
Missouri St. Louis TGA 2016 HIV Epidemiological Profile
 Missouri St. Louis TGA 2016 HIV Epidemiological Profile St. Louis TGA Part A Planning Council Prepared by the City of St. Louis Department of Health Center for Health Information, Research, and Planning
Missouri St. Louis TGA 2016 HIV Epidemiological Profile St. Louis TGA Part A Planning Council Prepared by the City of St. Louis Department of Health Center for Health Information, Research, and Planning
EXECUTIVE SUMMARY. Findings:
 Samaritan Center and Rescue Mission Participant Satisfaction Survey Housing and Homeless Coalition of Syracuse & Onondaga County By Patrick Whelan April 2016 EXECUTIVE SUMMARY Introduction: This study
Samaritan Center and Rescue Mission Participant Satisfaction Survey Housing and Homeless Coalition of Syracuse & Onondaga County By Patrick Whelan April 2016 EXECUTIVE SUMMARY Introduction: This study
Northside Mental Health Center Intake Questionnaire
 Name: _ Date of Birth: Age: SS# Address: City & State: Zip Code: GOALS How may we help you today? What type of help would you like? Circle all that apply Counseling Medication See a doctor What would you
Name: _ Date of Birth: Age: SS# Address: City & State: Zip Code: GOALS How may we help you today? What type of help would you like? Circle all that apply Counseling Medication See a doctor What would you
HIV Integrated Epidemiological Profile December 2011 State of Alabama
 HIV Integrated Epidemiological Profile December 2011 State of Alabama 12/31/2011 Alabama Department of Public Health Division of HIV/AIDS Prevention and Control TABLE OF CONTENTS List of Figures 3 List
HIV Integrated Epidemiological Profile December 2011 State of Alabama 12/31/2011 Alabama Department of Public Health Division of HIV/AIDS Prevention and Control TABLE OF CONTENTS List of Figures 3 List
Note: Staff who work in case management programs should attend the AIDS Institute training, "Addressing Prevention in HIV Case Management.
 Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
Addressing Prevention with HIV Positive Clients This one-day training will prepare participants to help people living with HIV to avoid sexual and substance use behaviors that can result in transmitting
Results from the South Dakota Health Survey. Presented by: John McConnell, Bill Wright, Donald Warne, Melinda Davis & Norwood Knight Richardson
 Results from the South Dakota Health Survey Presented by: John McConnell, Bill Wright, Donald Warne, Melinda Davis & Norwood Knight Richardson May 2015 Overview Why the interest in South Dakota? Survey
Results from the South Dakota Health Survey Presented by: John McConnell, Bill Wright, Donald Warne, Melinda Davis & Norwood Knight Richardson May 2015 Overview Why the interest in South Dakota? Survey
Kitsap County Annual Point-in-Time Count
 Kitsap County Annual Point-in-Time Count 2018 JANUARY 25TH WELCOME! Thank you for joining us, we are excited that you are willing to help us with the Annual Kitsap County Point-in-Time Count. The Point-in-Time
Kitsap County Annual Point-in-Time Count 2018 JANUARY 25TH WELCOME! Thank you for joining us, we are excited that you are willing to help us with the Annual Kitsap County Point-in-Time Count. The Point-in-Time
WELCOME! PLANNING COUNCIL MEETING September 7, 2017
 WELCOME! PLANNING COUNCIL MEETING September 7, 2017 Moment of Silence INTRODUCTIONS Please state your name for the record. Please note: You do NOT have to disclose your status during the introduction if
WELCOME! PLANNING COUNCIL MEETING September 7, 2017 Moment of Silence INTRODUCTIONS Please state your name for the record. Please note: You do NOT have to disclose your status during the introduction if
The 2009 Memphis TGA Ryan White HIV/AIDS Care Needs Assessment
 The 2009 Memphis TGA Ryan White HIV/AIDS Care Needs Assessment June 1, 2009 Prepared by, Thomas G. McGowan, Ph. D. Rhodes College 2000 North Parkway Memphis, TN 38112 Table of Contents Acknowledgements
The 2009 Memphis TGA Ryan White HIV/AIDS Care Needs Assessment June 1, 2009 Prepared by, Thomas G. McGowan, Ph. D. Rhodes College 2000 North Parkway Memphis, TN 38112 Table of Contents Acknowledgements
Additional North Carolina Projects
 Additional North Carolina Projects William Zule, Dr.P.H. www.rti.org RTI International is a trade name of Research Triangle Institute Risk Groups Injecting drug users (IDUs) Non-injecting drug users (non-idus)
Additional North Carolina Projects William Zule, Dr.P.H. www.rti.org RTI International is a trade name of Research Triangle Institute Risk Groups Injecting drug users (IDUs) Non-injecting drug users (non-idus)
Christina Pucel Counseling 416 W. Main St Monongahela, PA /
 ADULT INTAKE Name: Gender: M F DOB: Address: City: State: Zip: Telephone: Home Mobile Highest Level Education: Occupation: Emergency Contact: Relationship: Phone: Referred by: Family Members: Name Gender
ADULT INTAKE Name: Gender: M F DOB: Address: City: State: Zip: Telephone: Home Mobile Highest Level Education: Occupation: Emergency Contact: Relationship: Phone: Referred by: Family Members: Name Gender
INITIAL ASSESSMENT (TCU METHADONE OUTPATIENT FORMS)
") INITIAL ASSESSMENT (TCU METHADONE OUTPATIENT FORMS) [FORM 200; CARD 01] A. SITE:... [6] B. CLIENT ID NUMBER:... [7-10] C. SOURCE OF REFERRAL:... [11] 1. None/self 5. Other drug treatment program 2. Family
INITIAL ASSESSMENT (TCU METHADONE OUTPATIENT FORMS) [FORM 200; CARD 01] A. SITE:... [6] B. CLIENT ID NUMBER:... [7-10] C. SOURCE OF REFERRAL:... [11] 1. None/self 5. Other drug treatment program 2. Family
3726 E. Hampton St., Tucson, AZ Phone (520) Fax (520)
 Fax (520)") 3726 E. Hampton St., Tucson, AZ 85716 Phone (520) 319-1109 Fax (520)319-7013 Exodus Community Services Inc. exists for the sole purpose of providing men and women in recovery from addiction with safe,
3726 E. Hampton St., Tucson, AZ 85716 Phone (520) 319-1109 Fax (520)319-7013 Exodus Community Services Inc. exists for the sole purpose of providing men and women in recovery from addiction with safe,
Supplement to HIV and AIDS Surveillance (SHAS)
") Supplement to HIV and AIDS Surveillance (SHAS) Introduction SHAS was a CDC-funded project designed to provide an in depth description of people diagnosed with HIV/AIDS in MN, including information about
Supplement to HIV and AIDS Surveillance (SHAS) Introduction SHAS was a CDC-funded project designed to provide an in depth description of people diagnosed with HIV/AIDS in MN, including information about
A Sexual Health Study with Africans in Frankfurt am Main
 A Sexual Health Study with Africans in Frankfurt am Main Working together for Health Promotion INFORMATION FOR STUDY PARTICIPANTS WHO ARE WE? We are a group of Africans, researchers and persons doing
A Sexual Health Study with Africans in Frankfurt am Main Working together for Health Promotion INFORMATION FOR STUDY PARTICIPANTS WHO ARE WE? We are a group of Africans, researchers and persons doing
Sec on 1 Demographic Informa on
 The Priority Care Center A Program of the Humboldt IPA Primary Care Physician: Sec on 1 Demographic Informa on How were you referred: Name (Last, First, M.I.): A.K.A.: Date of Birth: Mailing Address: /
The Priority Care Center A Program of the Humboldt IPA Primary Care Physician: Sec on 1 Demographic Informa on How were you referred: Name (Last, First, M.I.): A.K.A.: Date of Birth: Mailing Address: /
2017 PIT Summary: Arapahoe County
 A Point-in-Time (PIT) count provides a snapshot of homelessness by interviewing those who are homeless at a particular time. The Metropolitan Denver Homeless Initiative (MDHI) conducted a PIT study of
A Point-in-Time (PIT) count provides a snapshot of homelessness by interviewing those who are homeless at a particular time. The Metropolitan Denver Homeless Initiative (MDHI) conducted a PIT study of
PARTICIPATION APPLICATION and AGREEMENT for CULINARY SCHOOL PROGRAM
 Page 1 PARTICIPATION APPLICATION and AGREEMENT for CULINARY SCHOOL PROGRAM PERSONAL INFORMATION First Name Middle Initial Last Name Current Street Address City State Zip code ( ) CELL _( )_HOME @ Email
Page 1 PARTICIPATION APPLICATION and AGREEMENT for CULINARY SCHOOL PROGRAM PERSONAL INFORMATION First Name Middle Initial Last Name Current Street Address City State Zip code ( ) CELL _( )_HOME @ Email
Epidemiology of HIV Among Women in Florida, Reported through 2014
 To protect, promote and improve the health of all people in Florida through integrated state, county, and community efforts. Created: 12/4/14 Revision: 1/27/15 Epidemiology of HIV Among Women in Florida,
To protect, promote and improve the health of all people in Florida through integrated state, county, and community efforts. Created: 12/4/14 Revision: 1/27/15 Epidemiology of HIV Among Women in Florida,
State of Iowa Outcomes Monitoring System
 State of Iowa Outcomes Monitoring System THE IOWA CONSORTIUM FOR SUBSTANCE ABUSE RESEARCH AND EVALUATION Year 16 Annual Outcome Evaluation Trend Report November 2014 With Funds Provided By: Iowa Department
State of Iowa Outcomes Monitoring System THE IOWA CONSORTIUM FOR SUBSTANCE ABUSE RESEARCH AND EVALUATION Year 16 Annual Outcome Evaluation Trend Report November 2014 With Funds Provided By: Iowa Department
2014 Butte County BUTTE COUNTY COMMUNITY HEALTH ASSESSMENT
 2014 Butte County BUTTE COUNTY COMMUNITY HEALTH ASSESSMENT EXECUTIVE SUMMARY 2015 2017 EXECUTIVE SUMMARY TOGETHER WE CAN! HEALTHY LIVING IN BUTTE COUNTY Hundreds of local agencies and community members
2014 Butte County BUTTE COUNTY COMMUNITY HEALTH ASSESSMENT EXECUTIVE SUMMARY 2015 2017 EXECUTIVE SUMMARY TOGETHER WE CAN! HEALTHY LIVING IN BUTTE COUNTY Hundreds of local agencies and community members
The Heterosexual HIV Epidemic in Chicago: Insights into the Social Determinants of HIV
 The Heterosexual HIV Epidemic in Chicago: Insights into the Social Determinants of HIV Nikhil Prachand, MPH Board of Health Meeting January 19, 2011 STI/HIV/AIDS Division Today s Presentation Epidemiology
The Heterosexual HIV Epidemic in Chicago: Insights into the Social Determinants of HIV Nikhil Prachand, MPH Board of Health Meeting January 19, 2011 STI/HIV/AIDS Division Today s Presentation Epidemiology
Women + Girls Research Alliance. Homelessness and Rapid Re-Housing in Mecklenburg County
 Women + Girls Research Alliance Homelessness and Rapid Re-Housing in Mecklenburg County Homelessness and Rapid Re-Housing in Mecklenburg County The UNC Charlotte Urban Institute prepared this report in
Women + Girls Research Alliance Homelessness and Rapid Re-Housing in Mecklenburg County Homelessness and Rapid Re-Housing in Mecklenburg County The UNC Charlotte Urban Institute prepared this report in
FULTON COUNTY GOVERNMENT RYAN WHITE PART A PROGRAM. Atlanta Eligible Metropolitan Area HIV/AIDS Unmet Need Estimate
 FULTON COUNTY GOVERNMENT RYAN WHITE PART A PROGRAM Atlanta Eligible Metropolitan Area HIV/AIDS Unmet Need Estimate Southeast AIDS Training and Education Center Department of Family and Preventative Medicine
FULTON COUNTY GOVERNMENT RYAN WHITE PART A PROGRAM Atlanta Eligible Metropolitan Area HIV/AIDS Unmet Need Estimate Southeast AIDS Training and Education Center Department of Family and Preventative Medicine
SECTION IV: IDU Syringe Exchange Data
 SECTION IV: IDU Syringe Exchange Data 1 IDU/SYRINGE EXCHANGE SURVEY ANALYSIS From the opening of the Needs Assessment process, it was acknowledged that there would be significant challenges in gathering
SECTION IV: IDU Syringe Exchange Data 1 IDU/SYRINGE EXCHANGE SURVEY ANALYSIS From the opening of the Needs Assessment process, it was acknowledged that there would be significant challenges in gathering
2016 Social Service Funding Application Non-Alcohol Funds
 2016 Social Service Funding Application Non-Alcohol Funds Applications for 2016 funding must be complete and submitted electronically to the City Manager s Office at ctoomay@lawrenceks.org by 5:00 pm on
2016 Social Service Funding Application Non-Alcohol Funds Applications for 2016 funding must be complete and submitted electronically to the City Manager s Office at ctoomay@lawrenceks.org by 5:00 pm on
HIV/AIDS Surveillance Technical Notes
 HIV/AIDS Surveillance Technical Notes Surveillance of HIV/AIDS The Minnesota Department of Health (MDH) collects case reports of HIV infection and AIDS diagnoses through a passive and active HIV/AIDS surveillance
HIV/AIDS Surveillance Technical Notes Surveillance of HIV/AIDS The Minnesota Department of Health (MDH) collects case reports of HIV infection and AIDS diagnoses through a passive and active HIV/AIDS surveillance
CMBHS Clinical Management of Behavioral Health Services
 Client: CMBHS Clinical Management of Behavioral Health Services Case Management AST022 Assessment Information Assessment Number Assessment Date Assessment Type Contact Type Assessment Site Referred By
Client: CMBHS Clinical Management of Behavioral Health Services Case Management AST022 Assessment Information Assessment Number Assessment Date Assessment Type Contact Type Assessment Site Referred By
Name: Date of Birth: Age: Grade: ID Number: Bob M Jones 4/21/ Gender: Sexual Orientation: Sex at Birth: Preferred Pronoun:
 JUST HEALTH PATIENT REPORT Name: Date of Birth: Age: Grade: ID Number: Bob M Jones 4/21/2000 17 12 1234567 Gender: Sexual Orientation: Sex at Birth: Preferred Pronoun: Femal Gay or Lesbian Female No pronouns,
JUST HEALTH PATIENT REPORT Name: Date of Birth: Age: Grade: ID Number: Bob M Jones 4/21/2000 17 12 1234567 Gender: Sexual Orientation: Sex at Birth: Preferred Pronoun: Femal Gay or Lesbian Female No pronouns,
PATIENT NAME: DATE OF DISCHARGE: DISCHARGE SURVEY
 PATIENT NAME: DATE OF DISCHARGE: DISCHARGE SURVEY Please indicate whether you feel Living Hope Eating Disorder Treatment Center provided either Satisfactory or Unsatisfactory service for each number listed
PATIENT NAME: DATE OF DISCHARGE: DISCHARGE SURVEY Please indicate whether you feel Living Hope Eating Disorder Treatment Center provided either Satisfactory or Unsatisfactory service for each number listed
FOR THE PERIOD JANUARY TO DECEMBER
 2016 YEAR REPORT FOR THE PERIOD JANUARY TO DECEMBER 2016 TCE YUEXI IN PARTNERSHIP WITH U-LANDSHJELP FRA FOLK TIL FOLK, NORGE HUMANA PEOPLE TO PEOPLE CHINA The project at a glance 1 Project name TCE Yuexi
2016 YEAR REPORT FOR THE PERIOD JANUARY TO DECEMBER 2016 TCE YUEXI IN PARTNERSHIP WITH U-LANDSHJELP FRA FOLK TIL FOLK, NORGE HUMANA PEOPLE TO PEOPLE CHINA The project at a glance 1 Project name TCE Yuexi