The Global HIV Epidemic. Jerome Larkin, MD
|
|
|
- Victoria Wilcox
- 6 years ago
- Views:
Transcription
1 The Global HIV Epidemic Jerome Larkin, MD
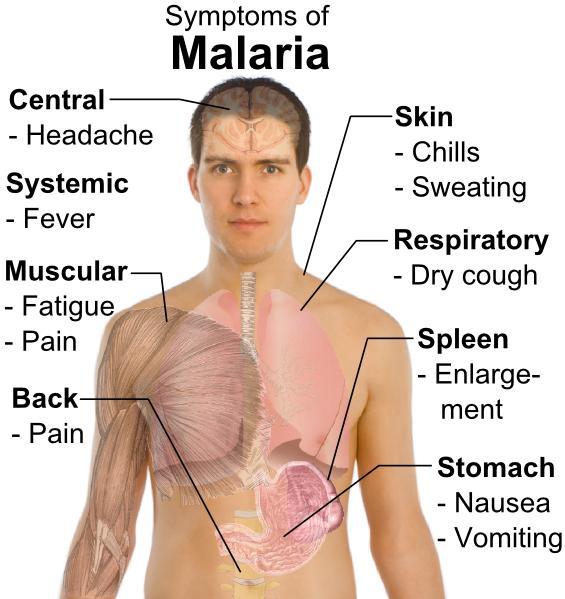
2 Outline Global Epidemiology Natural History of HIV Antiretroviral Therapy Malaria Tuberculosis Prevention of Mother to Child Transmission Post-Exposure Prophylaxis
3
4 Global summary of the AIDS epidemic, 2009 Number of people living with HIV in 2009 Total 33.3 million [ million] Adults 30.8 million [ million] Women (aged 15 and above) 15.9 million [ million] Children under 15 years 2.5 million [ million] People newly infected with HIV in 2009 AIDS-related deaths in 2009 Total 2.6 million [ million] Adults 2.2 million [ million] Children under 15 years 370, 000 [ ] Total 1.8 million [ million] Adults 1.6 million [ million] Children under 15 years [ ] December 2009
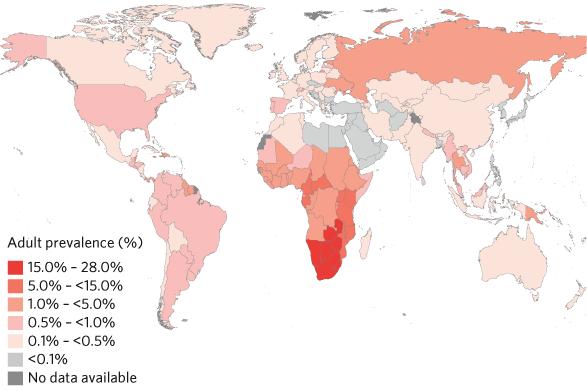
5 Regional HIV and AIDS statistics and features, 2009 Sub-Saharan Africa Middle East & North Africa South and South-East Asia East Asia Latin America Caribbean Eastern Europe & Central Asia Western & Central Europe North America Oceania TOTAL Adults & children living with HIV 22.5 million [ million] [ ] 4.1 million [ million] [ million] 1.4 million [ million] [ ] 1.4 million [ million] [ ] 1.5 million [ million] [ ] 33.3million [ million] Adults & children newly infected with HIV 1.8 million [ million] [ ] [ ] [ ] [ ] [ ] [ ] [ ] [ ] 4500 [ ] 2.6 million [ million] Adult prevalence (15 49) [%] 5.0 [ ] 0.2 [< ] 0.3 [ ] <0.1 [<0.1] 0.5 [ ] 1.0 [ ] 0.8 [ ] 0.2 [ ] 0.5 [ ] 0.3 [< ] 0.8 [< ] Adult & child deaths due to AIDS 1.3 million [ million] [ ] [ ] [ ] [ ] [ ] [ ] 8500 [ ] [ ] 1400 [ ] 1.8 million [ million] December 2009 The ranges around the estimates in this table define the boundaries within which the actual numbers lie, based on the best available information.
6 Global estimates for adults and children, 2009 People living with HIV 33.3 million [ million] New HIV infections in million [ million] Deaths due to AIDS in million [ million] December 2009
7 Adults and children estimated to be living with HIV, 2009 North America 1.5 million [ million] Caribbean [ ] Latin America 1.4 million [ million] Western & Central Europe [ ] Middle East & North Africa [ ] Sub-Saharan Africa 22.5 million [ million] Eastern Europe & Central Asia 1.4 million [ million] East Asia [ million] South & South-East Asia 4.1 million [ million] Oceania [ ] Total: 33.3 million ( million) December 2009
8 Estimated number of adults and children newly infected with HIV, 2009 North America [ ] Caribbean [ ] Latin America [ ] Western & Central Europe [ ] Middle East & North Africa [ ] Sub-Saharan Africa 1.8 million [ million] Eastern Europe & Central Asia [ ] East Asia [ ] South & South-East Asia [ ] Oceania 4500 [ ] Total: 2.6 million ( million) December 2009
9 Estimated adult and child deaths due to AIDS, 2009 North America [ ] Caribbean [ ] Latin America [ ] Western & Central Europe 8500 [ ] Middle East & North Africa [ ] Sub-Saharan Africa 1.3 million [ million] Eastern Europe & Central Asia [ ] East Asia [ ] South & South-East Asia [ ] Oceania 1400 [ ] Total: 1.8 million ( million) December 2009
10 Children (<15 years) estimated to be living with HIV, 2009 North America 4500 [<100] Caribbean [ ] Latin America [ ] Western & Central Europe 1400 [<100] Middle East & North Africa [ ] Sub-Saharan Africa 2.3 million [ million] Eastern Europe & Central Asia [ ] East Asia [ ] South & South-East Asia [ ] Oceania 3100 [< ] Total: 2.5 million ( million) December 2009
11 Estimated number of children (<15 years) newly infected with HIV, 2009 North America <100 [<100 <200] Caribbean 1900 [ ] Latin America 4300 [ ] Western & Central Europe <100 [<100 <200] Middle East & North Africa 6400 [ ] Sub-Saharan Africa [ ] Eastern Europe & Central Asia 3400 [ ] East Asia 1900 [ ] South & South-East Asia [ ] Oceania <1000 [<500 <1000] Total: ( ) December 2009
12 Estimated deaths of children (<15 years) due to AIDS, 2009 North America <100 [<100 <200] Caribbean 1600 [< ] Latin America 2700 [ ] Western & Central Europe <100 [<100 <200] Middle East & North Africa 3300 [ ] Sub-Saharan Africa [ ] Eastern Europe & Central Asia 1800 [< ] East Asia 1000 [< ] South & South-East Asia [ ] Oceania <500 [<100 <500] Total: ( ) December 2009
13 Over 7000 new HIV infections a day in 2009 More than 97% are in low- and middle-income countries About 1000 are in children under 15 years of age About 6000 are in adults aged 15 years and older, of whom: almost 51% are among women about 41% are among young people (15 24) December 2009
14 2009 global HIV and AIDS estimates Children (<15 years) Children living with HIV 2.5 million [ million] New HIV infections in [ ] Deaths due to AIDS in [ ] December 2009
15 Three Epidemics: Sub-Saharan Africa Largely sexually transmitted High prevalence Variable political/economic stability; often catastrophic Resource poor Clusters in urban/professional population N. America, W. Europe: Clusters among MSM/IVDU Low prevalence Stable infrastructure/politics/economics Heavily resourced S. America, Asia More commonly sexually transmitted Relatively low prevalence Intemediate political/economic stability/resources
16 In Africa: At least 77% is heterosexual transmission 5% mother to child Blood transfusion 0.5% Unknown 17%
17
18 Infections in Children 370,000 children newly infected with HIV in the world (2009) Mortality before the age of 2 if untreated is 50% Most (90%) in SubSaharan Africa
19 Infections in Children Most are infected via maternal to child transmissison Most potentially preventable Compounded by geography, decreased access to health care services, most women delivering at home, lack of HIV awareness, lack of testing, poverty
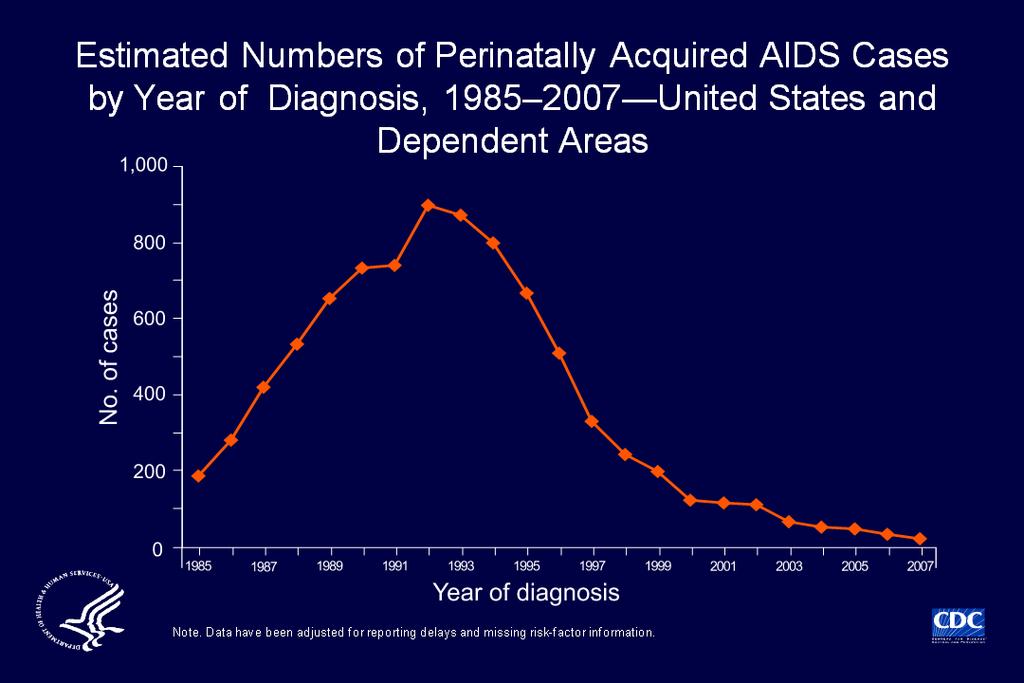
20 In the US... Infections in IVDU is decreasing Perinatal infections now very rare An estimated 280,000 people are positive and do not know it; do not perceive risk Infections in women, MSM, Hispanics and African Americans increasing Most infections in women through heterosexual contact
21 Natural History of HIV
22 Types of HIV There are 2 types of HIV: HIV-1 and HIV-2 Most of the HIV in the world is HIV-1 There are at least 10 subtypes of HIV-1. HIV-2 is found mostly in West Africa (and Mozambique) although only 1% of cases
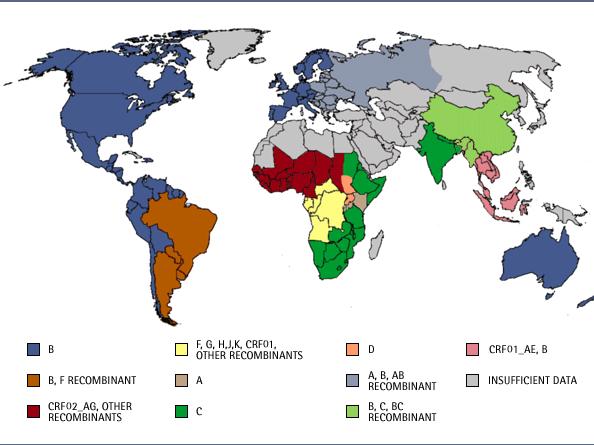
23 HIV 1 Subtypes Multiple subtypes: M, N, O, P Different strains predominate in specific geographic areas M is further subdivided in clades: A-K N and O are very rare B predominates in North America and is the best studied; accounts for ~12% worldwide C is the most common with ~50% world wide (E. Africa, S. Africa, S. Asia, China)
24
25 HIV-2 HIV-2 is a weaker virus It progresses more slowly to AIDS but eventually leads to the same opportunistic infections. Transmission from a mother to a child is relatively rare (0-4% in breastfeeding mothers) Important to diagnose because treatment is different from HIV-1 Less well studied
26 HIV is transmitted via Blood Usually via transfusions or contaminated needles and syringes Semen Usually from sex without a condom Vaginal secretions Usually from sex without a condom Mother-to-child During pregnancy, birth, or breast-feeding
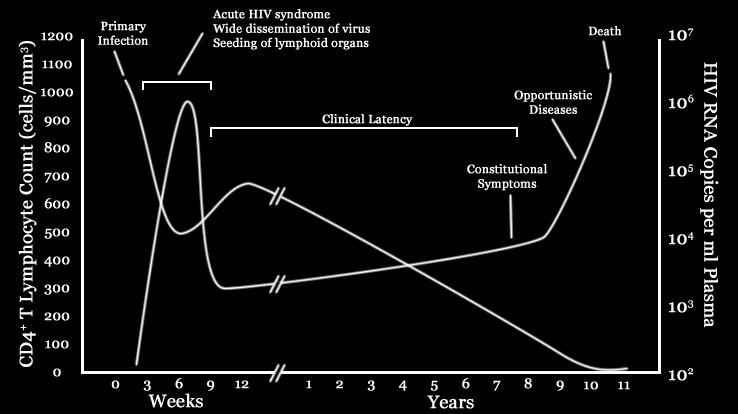
27 Acute HIV Infection An infected person will often become ill a few weeks after infection with HIV: Fever, Rash, Sore throat, Muscle Aches, Headache, Vomitting, Diarrhea, Stiff Neck This usually goes away as the immune system starts to control the infection.
28 Acute HIV Infection Acute infection occurs within 2-6 weeks after HIV enters the body. Virus is then produced rapidly and spreads throughout the body. Patient develops antibodies to control the virus (but these are not detectable for 2-12 weeks on HIV rapid tests)
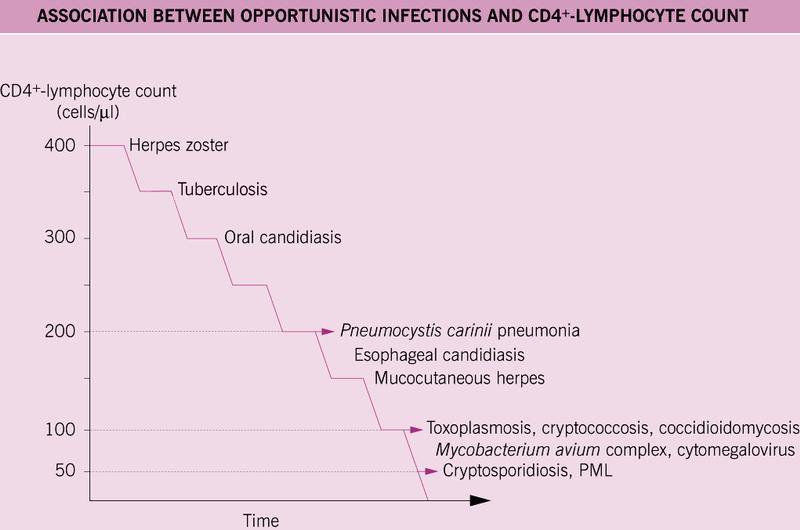
29
30 CD4 Count Normal ; range CD4/CD8 ratio normally >2 Should not be used to diagnose HIV infection
31 CD4 Count With viral load best predictor of disease progression Treatment with antiretrovirals always indicated if CD4<200 Usually indicated if CD4<500 WHO currently recommends treatment at <350 Viral load level indications less clear; most would treat for a viral load >100,000 regardless of CD4 Count
32 CD 4 Count and Percent CD4 % has the best intermeasure consistency: Immune function/ CD4% CD4 Count suppression Normal >30 >350 Moderate Severe <15 < % of CD4 cells are turned over daily; the entire population in around 15 days
33 HIV Replication Billions of new virus made EVERY DAY Takes 24 hours to replicate Entire viral burden turns over in ~72h Error-prone: error rate Replication errors = mutations (slight changes in structure of virus) Selection pressure may select drug-resistant strains Original, non-mutated virus = wild-type
34 HIV to AIDS Median time from HIV infection to symptomatic disease (clinical latency): Adults: 10 years Children: months to 1-2 years 5-10% of adults have stable CD4 counts and no symptoms after 10 years (Elite Controllers) 10% of adults progress to AIDS in 2-3 years
35
36 AIDS Defining Illnesses Candidiasis: esophageal, pulmonary Toxoplasmosis PCP Cryptococcal Meningitis Recurrent Pneumonia
37 AIDS Defining Illnesses Lymphoma GI CNS PEL Kaposi s Sarcoma Invasive Cervical Cancer
38 AIDS Defining Illnesses Wasting PML CMV (not of LN, spleen, liver) Dementia Active TB Disseminated MAC HSV > 1 month Cryptosporidium > 1month
39 AIDS Defining Illnesses Coccidiomycosis Histoplasmosis Isosporosis Nocardiosis Salmonella Strongyloidosis
40 OI s Common in Africa but not in US Malaria Tuberculosis Salmonellosis
41 Antiretroviral Therapy
42 Antiretroviral Therapy Also known as HAART or ART First agent available in 1987: Zidovudine/AZT Had marginal improvement in survival, symptoms but patients always relapsed
43 1995: ACTG 076 demonstrates decreased mother to child transmission: ~25 to 10% Combination therapy became available with development of protease inhibitors circa mortality, AIDS, OI s and hospitalization all decreased 60-80%
44 Indications for ART CD4 <500 Rapid Decline in CD4 Viral load >100,000 (? ,000) Rapid rise in viral load AIDS defining illness Patient Preference Chronic Hep B HIV related nephropathy Pregnancy
45 NRTI Abacavir (ABC) Didanosine (ddi) Emtricitabine (FTC) Lamivudine (3TC) Stavudine (d4t) Tenofovir (TDF) Zidovudine (AZT, ZDV) NNRTI Delavirdine (DLV) Efavirenz (EFV) Etravirine (ETR) Nevirapine (NVP) Current ARV Medications PI Atazanavir (ATV) Darunavir (DRV) Fosamprenavir (FPV) Indinavir (IDV) Lopinavir (LPV) Nelfinavir (NFV) Ritonavir (RTV) Saquinavir (SQV) Tipranavir (TPV) Integrase Inhibitor (II) Raltegravir (RAL) Fusion Inhibitor Enfuvirtide (ENF, T-20) CCR5 Antagonist Maraviroc (MVC) December
46 Current ARV Medications Available in Africa NRTI Abacavir (ABC) Didanosine (ddi) Lamivudine (3TC) Stavudine (d4t) Tenofovir (TDF) Zidovudine (AZT, ZDV) PI Atazanavir (ATZ) Indinavir (IDV) Lopinavir (LPV) Nelfinavir (NFV) Ritonavir (RTV) Saquinavir (SQV) NNRTI Efavirenz (EFV) Nevirapine (NVP) December
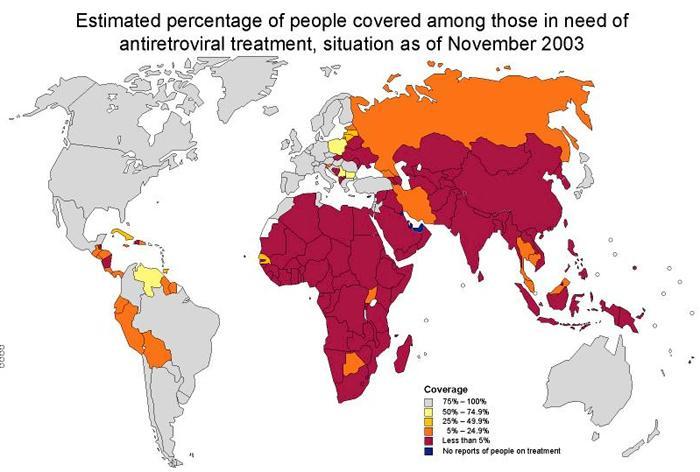
47 ART in Africa Currently generally recommended for CD4 counts <350 or <200 or WHO Stage 3 or 4 disease* Problems with access to care, drugs, monitoring Very few medical providers, limited expertise Lab infrastructure limited, variable; prone to issues of reagent supply, technical support, refrigeration *varies by country guideline
48 However Studies demonstrate that rates of adherence, viral suppression, immune reconstitution and clinical improvement are similar to resourcerich areas of the world. Largely funded by donor agencies: PEPFAR, The Global Fund to Fight AIDS, Tuberculosis and Malaria, Gates Foundation
49 Adult WHO Stage 3 Weight loss, >10% of body weight Unexplained chronic diarrhea > 1 month Unexplained prolonged fever (intermittent or constant) >1 month Oral Candidiasis (thrush) Vulvo-vaginal Candidiasis, chronic (>1/12) or poorly responsive to therapy Oral hairy leukoplakia Pulmonary TB, within the past year Severe bacterial infections (i.e. pneumonia)
50 Adult WHO Stage 4 HIV wasting syndrome Pneumocystitis pneumonia (PCP) Toxoplasmosis of the brain Cryptococcosis, extrapulmonary Cryptosporidiosis with diarrhea >1 month Extrapulmonary TB Cytomegalovirus retinitis (CMV) Herpes simplex virus infection, mucocutaneous >1 month or visceral (any duration) Candidiasis of esophagus, trachea, bronchi Lymphoma Kaposi s sarcoma HIV encephalopathy Progressive multifocal leucoencephalopathy (PML) Any disseminated endemic mycosis Atypical mycobacteriosis, disseminated or pulmonary Non-typhoid Salmonella septicaemia And/or performance scale 4: bedridden >50% of the day during the last month
51
52 HIV and Malaria
53
54
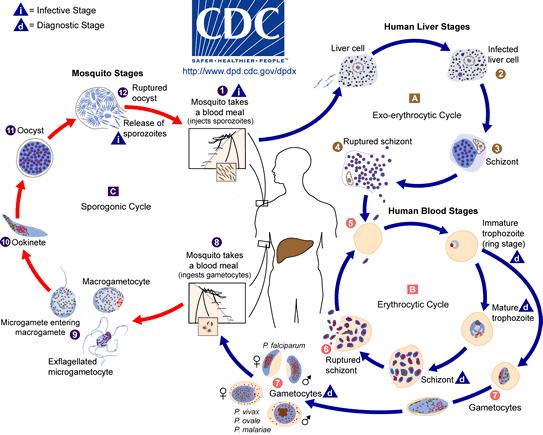
55 Malaria Basics 5 species infect humans; Plasmodium falciparum is the most pathologic and most common in Africa 243 million cases/year worldwide in ,000 deaths; most in children in Africa due to falciparum Pregnant women are susceptible to severe disease Older children, adults and multigravids (>2) acquire immunity
56 Malaria and HIV Increasing prevalence with severity of immunosuppression Increased prevalence of severe malaria: cerebral, hypoglycemia, coma, anemia, placental Episodes of malaria lead to increase in HIV viral load Parasite load is higher in HIV infection Increase risk of treatment failure in adults; children appear to respond similarly to HIV-uninfected Pregnancy: increased maternal death, premature deliver, LBW,? infant mortality Monthly treatment/impregnated bed nets reduce morbidity in pregnancy
57 TMP/Sulfa Prophylaxis Prescribed for PCP prophylaxis Decreases incidence of malaria and parasitemia including at higher CD4 counts Reduces diarrheal illness (Salmonella) Reduces bacterial pneumonia Should be prescribed for all HIV positive individuals regardless of CD4 count
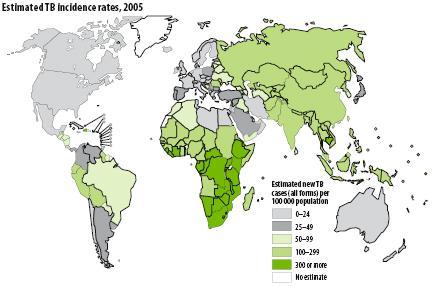
58 HIV and Tuberculosis
59
60 HIV and Tuberculosis Rates of coinfection 30-60% in sub-saharan Africa depending on population studied Activation of latent disease 5-10%/year Presents atypically at CD4 <350 More likely to be disseminated at CD4 <50 May present as an manifestation of immune reconstitution inflammatory syndrom (IRIS) Active disease associated with increased viremia and progression of HIV
61 ART and Anti-TB Treatment 11-45% of patients receiving ART within six weeks of starting treatment for TB develop IRIS High rate of progression/mortality of both associated with delay of treatment for either at low CD4 counts Multiple drug interactions: Rif vs Nevirapine, Protease Inhibitors
62 ART and Anti-TB Treatment Always start treatment for TB first Start ART based on CD4 Count: <100: within 2 weeks : delay 2-8 weeks > : delay 8 weeks
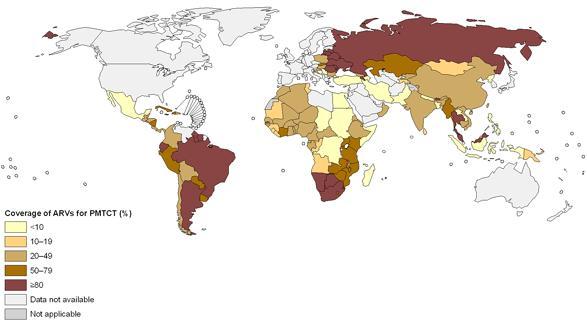
63 Prevention of Mother to Child Transmission
64 Mother-to-Child Transmission of HIV-1 Pregnancy 5-10% Delivery 15% Breastfeeding 5-15% Up to 40% transmission
65 Factors Increasing Transmission: New maternal infection in third trimester Low maternal CD4 count High maternal viral load Mother with AIDS defining illness Chorioamnionitis Exposure of infant to maternal blood ie abruption PROM Prolonged labor Preterm delivery Maternal/fetal HLA discordance
66
67 Prevention of Mother to Child Transmission Currently HIV infection is an absolute indication for three drug antiretroviral therapy in preganancy Typical regimen: Combivir/Kaletra* Combivir: fixed dose combination of zidovudine and lamivudine Kaletra: fixed dose combination of lopinivir and ritonovir Maternal zidovudine in 2 nd /3 rd trimester with nevirapine at delivery and post-natal nevirapine +/- zidovudine still used in resource poor areas of the world
68 Estimated number of children (<15 years) newly infected with HIV, 2009 North America <100 [<100 <200] Caribbean 1900 [ ] Latin America 4300 [ ] Western & Central Europe <100 [<100 <200] Middle East & North Africa 6400 [ ] Sub-Saharan Africa [ ] Eastern Europe & Central Asia 3400 [ ] East Asia 1900 [ ] South & South-East Asia [ ] Oceania <1000 [<500 <1000] Total: ( ) December 2009
69
70 13.0 Preventing mother to child transmission (PMTCT) (For those mothers who are pregnant but not receiving ART). Table 10: Recommended Regimens for PMTCT Intervention. Target Nevirapine (NVP) Zidovudine (ZDV) Mother 200 mg stat at the beginning of labor or latest 30 minutes before delivery 300 mg twice daily for at least 4 weeks before delivery then 300 mg every 3 hrs during labor then 300 mg twice daily for 1 week after delivery Infant (Within 72 hours of birth) Syrup 2 mg/kg stat Syrup 5 mg/kg twice daily for one week
71 Should all HIV infected women be treated with ART? Fertility rates in Africa are very high Breastfeeding is necessary to decrease infant mortality Intermittent therapy can lead to viral resistance Each discontinuation and resumption of therapy is an opportunity for error
72 Post-Exposure Prophylaxis
73 Non-infectious Body Fluid Tears Urine Feces Saliva, Sputum, Vomit Nasal secretions Sweat
74 Potentially Risky Exposure Percutaneous (through the skin) injury with potentially infectious body fluids Contact of mucous membranes (eye, nose, mouth, vagina, rectum) or non-intact skin with infectious body fluids
75 Risk for Occupational Transmission of HIV (23 studies before HAART) Percutaneous exposure to HIV-infected blood: 0.33% (20/6135) Mucous membrane exposure: 0.09% (1/1143) Intact skin exposure: 0% (0/2712)
76 Probable Factors affecting Risk of HIV Medical device visibly contaminated with blood Needle went into vein or artery of infected patient Involving deep injury Traumatic sexual assault Source person has a terminal illness (HIVrelated Sx, AIDS) (increased viral load)
77 Principles of PEP Transmission of HIV can be reduced by 79% by taking ARVs for 1 month Start PEP ASAP (pref. within 2 hours) Efficacy is decreased if delayed Can start up to 72hrs post-exposure
78 Post-Exposure Prophylaxis Initial response is to clean the area of exposure Determined by risk asssessment of source and type of exposure Generally use two or three drugs: -tenofovir/emtricitabine - tenofovir/emtricitabine/lopinavir/r -should not receive nevirapine Initiate treatment as soon as possible within 72 hours Drugs taken for 4 weeks
79 Fin Questions?
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
I. HIV Epidemiology. HIV Infection A Primer. Objectives. Disclosures 7/18/2014
 Objectives HIV Infection A Primer Discuss the worldwide and domestic epidemiology of HIV infection Review HIV Biology Review HIV Transmission and Prevention Review HIV diagnosis Describe the approaches
Objectives HIV Infection A Primer Discuss the worldwide and domestic epidemiology of HIV infection Review HIV Biology Review HIV Transmission and Prevention Review HIV diagnosis Describe the approaches
Sasisopin Kiertiburanakul, MD, MHS
 What s Newin Antiretroviral Therapy? Sasisopin Kiertiburanakul, MD, MHS Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Rotating RCPT,
What s Newin Antiretroviral Therapy? Sasisopin Kiertiburanakul, MD, MHS Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Rotating RCPT,
Update on Antiretroviral Treatment for HIV Infection 2008
 Update on Antiretroviral Treatment for HIV Infection 2008 Janet Gilmour MD FRCP(C) Clinical Associate Professor of Medicine University of Calgary November 2008 Disclosure and Acknowledgements Disclosure:
Update on Antiretroviral Treatment for HIV Infection 2008 Janet Gilmour MD FRCP(C) Clinical Associate Professor of Medicine University of Calgary November 2008 Disclosure and Acknowledgements Disclosure:
/AIDS HIV/ HIV Overview. Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program
 /AIDS HIV/ HIV Overview Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program www.hivresearch.org 1 WRAIR Tropical Medicine Course
/AIDS HIV/ HIV Overview Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program www.hivresearch.org 1 WRAIR Tropical Medicine Course
HIV Overview. Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program
 HIV Overview Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program www.hivresearch.org 1 Outline HIV Virology, Transmission, and Pathogenesis
HIV Overview Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program www.hivresearch.org 1 Outline HIV Virology, Transmission, and Pathogenesis
Epidemiology Testing Clinical Features Management
 Jason Cronin, MD Epidemiology Testing Clinical Features Management In 1981, 1 the first cases of AIDS were identified among gay men in the US. However, scientists later found evidence that the disease
Jason Cronin, MD Epidemiology Testing Clinical Features Management In 1981, 1 the first cases of AIDS were identified among gay men in the US. However, scientists later found evidence that the disease
Continuing Education for Pharmacy Technicians
 Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
When to Start ART. Reduction in HIV transmission. ? Reduction in HIV-associated inflammation and associated complications» i.e. CV disease, neuro, etc
 When to Start ART Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts Current recommendation: ART for all patients with CD4 count of
When to Start ART Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts Current recommendation: ART for all patients with CD4 count of
medical monitoring: clinical monitoring and laboratory tests
 medical monitoring: clinical monitoring and laboratory tests Purpose of monitoring Check on the physical, psychological and emotional condition of the patient Detect other treatable conditions Identify
medical monitoring: clinical monitoring and laboratory tests Purpose of monitoring Check on the physical, psychological and emotional condition of the patient Detect other treatable conditions Identify
HIV in in Women Women
 HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
Overview of HIV. LTC Paige Waterman
 Overview of HIV LTC Paige Waterman Outline Background and Epidemiology HIV Virology, Transmission, and Pathogenesis Acute HIV infection HIV Diagnostics Management of Health Care Personnel Exposed to HIV
Overview of HIV LTC Paige Waterman Outline Background and Epidemiology HIV Virology, Transmission, and Pathogenesis Acute HIV infection HIV Diagnostics Management of Health Care Personnel Exposed to HIV
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course
 Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments - Dr. Christina Polyak - Dr. Julie Ake Disclaimer The views expressed in this presentation are
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments - Dr. Christina Polyak - Dr. Julie Ake Disclaimer The views expressed in this presentation are
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
TB Intensive Tyler, Texas December 2-4, Tuberculosis and HIV Co-Infection. Lisa Y. Armitige, MD, PhD. December 4, 2008.
 TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
HIV Diagnosis and Management 2015 Update. Faria Farhat, MD MedStar Washington Hospital Center
 HIV Diagnosis and Management 2015 Update Faria Farhat, MD MedStar Washington Hospital Center Objectives Describe the epidemiology and pathogenesis of HIV infection Highlight HIV diagnosis algorithm and
HIV Diagnosis and Management 2015 Update Faria Farhat, MD MedStar Washington Hospital Center Objectives Describe the epidemiology and pathogenesis of HIV infection Highlight HIV diagnosis algorithm and
10/17/2015. Chapter 55. Care of the Patient with HIV/AIDS. History of HIV. HIV Modes of Transmission
 Chapter 55 Care of the Patient with HIV/AIDS All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. History of HIV Remains somewhat obscure The earlier
Chapter 55 Care of the Patient with HIV/AIDS All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. History of HIV Remains somewhat obscure The earlier
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
TB/HIV Co-Infection. Tuberculosis and HIV
 TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
Criteria for Oral PrEP
 Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
0% 0% 0% Parasite. 2. RNA-virus. RNA-virus
 HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
PHCP 403 by L. K. Sarki
 PHCP 403 by L. K. Sarki objectives To gain insight into the epidemiology of HIV To gain basic understanding of the etiology of HIV disease To know the clinical manifestations of the disease To gain a basic
PHCP 403 by L. K. Sarki objectives To gain insight into the epidemiology of HIV To gain basic understanding of the etiology of HIV disease To know the clinical manifestations of the disease To gain a basic
PAEDIATRIC HIV INFECTION. Dr Ashendri Pillay Paediatric Infectious Diseases Specialist
 PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
Preventing Mother to Child HIV Transmission: Are We There Yet?!'
 Preventing Mother to Child HIV Transmission: Are We There Yet?!' 2017 Michigan Clincal Nursing Conference for HIV and STD Care May 18, 2017 Frankenmuth MI 1 Theodore B. Jones, MD Maternal Fetal Medicine
Preventing Mother to Child HIV Transmission: Are We There Yet?!' 2017 Michigan Clincal Nursing Conference for HIV and STD Care May 18, 2017 Frankenmuth MI 1 Theodore B. Jones, MD Maternal Fetal Medicine
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV
 POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
HIV basics. Katya Calvo Medical Director of Antimicrobial Stewardship
 HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
World Bank Training Program on HIV/AIDS Drugs
 World Bank Training Program on HIV/AIDS Drugs Training Module 3 Selection and Quantification based on the World Bank document Battling HIV/AIDS: A Decision Maker s Guide to the Procurement of Medicines
World Bank Training Program on HIV/AIDS Drugs Training Module 3 Selection and Quantification based on the World Bank document Battling HIV/AIDS: A Decision Maker s Guide to the Procurement of Medicines
HIV and PEP. LTC Rose Ressner WRNMMC ID staff Oct 2014 UNCLASSIFIED
 HIV and PEP LTC Rose Ressner WRNMMC ID staff Oct 2014 UNCLASSIFIED Disclaimer The views expressed in this presentation are those of the speaker and do not reflect the official policy of the Department
HIV and PEP LTC Rose Ressner WRNMMC ID staff Oct 2014 UNCLASSIFIED Disclaimer The views expressed in this presentation are those of the speaker and do not reflect the official policy of the Department
Page 1. Outline. Outline. Building specialized knowledge: HIV. Biological interactions. Social aspects of the epidemic. Programmatic actions
 Harvard-Brazil Collaborative Public Health Field Course January 2014 Lecture # 8 Building specialized knowledge: HIV Aluisio Segurado Department of Infectious Diseases School of Medicine, University of
Harvard-Brazil Collaborative Public Health Field Course January 2014 Lecture # 8 Building specialized knowledge: HIV Aluisio Segurado Department of Infectious Diseases School of Medicine, University of
The HIV Program UNIT 2 HIV CURRICULUM PARTICIPANT S MANUAL
 T F A R D UNIT 2 The HIV Program UNIT 2 BACKGROUND The HIV Program Poverty and lack of access to basic human rights such as adequate nutrition compound the devastating effects of HIV on communities. Comprehensive
T F A R D UNIT 2 The HIV Program UNIT 2 BACKGROUND The HIV Program Poverty and lack of access to basic human rights such as adequate nutrition compound the devastating effects of HIV on communities. Comprehensive
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Overview of HIV. Christina Polyak, MD, MPH. Research Physician. U.S. Military HIV Research Program, Walter Reed Army Institute of Research
 Overview of HIV Christina Polyak, MD, MPH Research Physician U.S. Military HIV Research Program, Walter Reed Army Institute of Research The views expressed are those of the authors and should not be construed
Overview of HIV Christina Polyak, MD, MPH Research Physician U.S. Military HIV Research Program, Walter Reed Army Institute of Research The views expressed are those of the authors and should not be construed
GUIDELINES FOR THE USE OF ANTIRETROVIRAL THERAPY IN PAPUA NEW GUINEA
 GUIDELINES FOR THE USE OF ANTIRETROVIRAL THERAPY IN PAPUA NEW GUINEA These guidelines were prepared for the Papua New Guinea National AIDS Council and the Papua New Guinea National Department of Health.
GUIDELINES FOR THE USE OF ANTIRETROVIRAL THERAPY IN PAPUA NEW GUINEA These guidelines were prepared for the Papua New Guinea National AIDS Council and the Papua New Guinea National Department of Health.
HIV/AIDS HIV/AIDS: Outline. Morbidity and Mortality Weekly Report (MMWR)
") HIV/AIDS: Outline HIV/AIDS 2013 Roy M. Gulick, MD, MPH Professor of Medicine Chief, Division of Infectious Diseases Weill Medical College of Cornell University New York City January 31, 2013 Epidemiology
HIV/AIDS: Outline HIV/AIDS 2013 Roy M. Gulick, MD, MPH Professor of Medicine Chief, Division of Infectious Diseases Weill Medical College of Cornell University New York City January 31, 2013 Epidemiology
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care
 Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
Principles of Antiretroviral Therapy
 Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
DR. SATTI A/RAHIM SATTI CONSULTANT PEDIATRICION
 A I D S IN CHILDREN BY DR. SATTI A/RAHIM SATTI CONSULTANT PEDIATRICION INTRODUCTION AIDS is the end stage of symptomatic HIV infection. HIV infection progresses more rapidly in children than in adults.
A I D S IN CHILDREN BY DR. SATTI A/RAHIM SATTI CONSULTANT PEDIATRICION INTRODUCTION AIDS is the end stage of symptomatic HIV infection. HIV infection progresses more rapidly in children than in adults.
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 03/07/18 SECTION: DRUGS LAST REVIEW DATE: 02/19/19 LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
The Hospitalized HIV+ Patient
 The Hospitalized HIV+ Patient Danny Toub MD dannyt@srheathcenters.org October 8, 2012 Santa Rosa Family Medicine Residency List 3 ways of risk-stratifying known or suspected HIV+ inpatients Perform differential
The Hospitalized HIV+ Patient Danny Toub MD dannyt@srheathcenters.org October 8, 2012 Santa Rosa Family Medicine Residency List 3 ways of risk-stratifying known or suspected HIV+ inpatients Perform differential
HIV Update Objectives. Epidemiology. Epidemiology, Transmission and Natural History. Transmission Risk by Exposure. Transmission 9/29/2014
 Objectives HIV Update 2014 Jay Sizemore, MD, MPH Medical Director Chattanooga CARES Assistant Professor UTCOM Chattanooga 2October 2014 Review HIV epidemiology and screening/testing guidelines Discuss
Objectives HIV Update 2014 Jay Sizemore, MD, MPH Medical Director Chattanooga CARES Assistant Professor UTCOM Chattanooga 2October 2014 Review HIV epidemiology and screening/testing guidelines Discuss
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
TORONTO GENERAL HOSPITAL HIV AMBULATORY CARE ROTATION
 TGH - ambulatory rotation page 1 of 5 TORONTO GENERAL HOSPITAL HIV AMBULATORY CARE ROTATION SITE: Immunodeficiency Clinic, Toronto General Hospital, University Health Network Location: 13 th floor, Norman
TGH - ambulatory rotation page 1 of 5 TORONTO GENERAL HOSPITAL HIV AMBULATORY CARE ROTATION SITE: Immunodeficiency Clinic, Toronto General Hospital, University Health Network Location: 13 th floor, Norman
HIV Update. Divya Ahuja, MD Associate Professor of Medicine University of South Carolina School of Medicine
 HIV Update Divya Ahuja, MD Associate Professor of Medicine University of South Carolina School of Medicine Rates of Diagnoses of HIV Infection among Adults and Adolescents, 2012 United States and 6 Dependent
HIV Update Divya Ahuja, MD Associate Professor of Medicine University of South Carolina School of Medicine Rates of Diagnoses of HIV Infection among Adults and Adolescents, 2012 United States and 6 Dependent
20 Years of Tears and Triumphs
 20 Years of Tears and Triumphs A Clinical Research Nurse s Perspective on HIV/AIDS Bobi Keenan, RN, ACRN Clinical Research Nurse UC Irvine Dept. of Medicine/Infectious Diseases Objectives 1. Understand
20 Years of Tears and Triumphs A Clinical Research Nurse s Perspective on HIV/AIDS Bobi Keenan, RN, ACRN Clinical Research Nurse UC Irvine Dept. of Medicine/Infectious Diseases Objectives 1. Understand
A Fatal Imbalance. Tropical diseases: 18 new drugs (incl. 8 for malaria) 1.3% 21 new drugs for neglected diseases. Tuberculosis: 3 new drugs
 1.3% 21 new drugs for neglected diseases. Tuberculosis: 3 new drugs") ADDRESSING GAPS IN INNOVATION FOR NEGLECTED PATIENTS: DNDI ANDPEDIATRIC HIV/AIDS Rachel Cohen, Regional Executive Director, DNDi North America Proposals for a Global Innovation System that Responds to
ADDRESSING GAPS IN INNOVATION FOR NEGLECTED PATIENTS: DNDI ANDPEDIATRIC HIV/AIDS Rachel Cohen, Regional Executive Director, DNDi North America Proposals for a Global Innovation System that Responds to
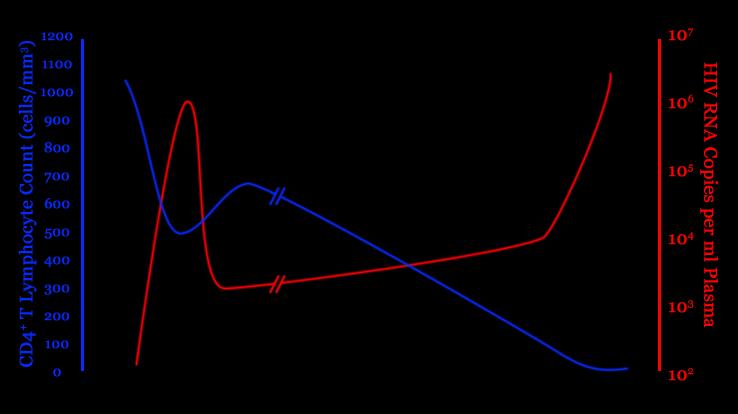
This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts
 1 2 This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts decreased. This period of acute infection or serocnversion
1 2 This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts decreased. This period of acute infection or serocnversion
Nobel /03/28. HIV virus and infected CD4+ T cells
 Mechanism of HIV drug resistance. Rodrigo Brindeiro / Amilcar Tanuri Laboratório de Virologia Molecular UFRJ 2 -Asso ciate Research Scientist, Internatio nal Center fo r Aids Care and Treatment Programs-ICAP,
Mechanism of HIV drug resistance. Rodrigo Brindeiro / Amilcar Tanuri Laboratório de Virologia Molecular UFRJ 2 -Asso ciate Research Scientist, Internatio nal Center fo r Aids Care and Treatment Programs-ICAP,
HIV Update: What the Hospital-Based Provider Should Know
 HIV Update: What the Hospital-Based Provider Should Know Steven C. Johnson M.D. Division of Infectious Diseases, University of Colorado School of Medicine October 6, 2011 45 year old female Case Study
HIV Update: What the Hospital-Based Provider Should Know Steven C. Johnson M.D. Division of Infectious Diseases, University of Colorado School of Medicine October 6, 2011 45 year old female Case Study
 http://www.savinglivesuk.com/ HIV Awareness Study Morning 24 th November 2017 Agenda HIV Basics & Stages of HIV HIV Testing, Health Advising & Sexual Health Saving Lives Antiretroviral Medication Antenatal/Postnatal
http://www.savinglivesuk.com/ HIV Awareness Study Morning 24 th November 2017 Agenda HIV Basics & Stages of HIV HIV Testing, Health Advising & Sexual Health Saving Lives Antiretroviral Medication Antenatal/Postnatal
Nothing to disclose.
 Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital HIV UPDATE FOR THE PRIMARY CARE PROVIDER Nothing to disclose. 1 Outline Epidemiology Screening / testing for HIV
Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital HIV UPDATE FOR THE PRIMARY CARE PROVIDER Nothing to disclose. 1 Outline Epidemiology Screening / testing for HIV
HIV for the Non-ID Pharmacist
 Disclosures HIV for the Non-ID Pharmacist I have nothing to disclose at this time Carmen Faulkner-Fennell, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist--Infectious Diseases Greenville Hospital System
Disclosures HIV for the Non-ID Pharmacist I have nothing to disclose at this time Carmen Faulkner-Fennell, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist--Infectious Diseases Greenville Hospital System
Gaps between Policy and Practice in Managing HIV disease in Asia Pacific
 Gaps between Policy and Practice in Managing HIV disease in Asia Pacific Dr. N. Kumarasamy Chief Medical Officer YRGCARE Medical Centre Voluntary Health Services Chief-Chennai Antiviral Research and Treatment
Gaps between Policy and Practice in Managing HIV disease in Asia Pacific Dr. N. Kumarasamy Chief Medical Officer YRGCARE Medical Centre Voluntary Health Services Chief-Chennai Antiviral Research and Treatment
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010
 THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
Didactic Series. Update: 2012 HIV Treatment Guidelines. Daniel Lee, MD August 30, 2012
 Didactic Series Update: 2012 HIV Treatment Guidelines Daniel Lee, MD August 30, 2012 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited by the Accreditation Council
Didactic Series Update: 2012 HIV Treatment Guidelines Daniel Lee, MD August 30, 2012 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited by the Accreditation Council
WESTERN CAPE ART GUIDELINES PRESENTATION 2013
 WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
Blood-Borne Pathogens and Post-Exposure Prophylaxis
 Blood-Borne Pathogens and Post-Exposure Prophylaxis Christopher Behrens MD Northwest Association of Occupational and Environmental Medicine October 2017 with thanks to Shireesha Dhanireddy MD Disclosures
Blood-Borne Pathogens and Post-Exposure Prophylaxis Christopher Behrens MD Northwest Association of Occupational and Environmental Medicine October 2017 with thanks to Shireesha Dhanireddy MD Disclosures
HIV medications HIV medication and schedule plan
 Living with HIV (human immunodeficiency virus) It may be scary to find out that you re HIV-positive or have AIDS. Coping with this news may be difficult. Although HIV is a serious infection, people with
Living with HIV (human immunodeficiency virus) It may be scary to find out that you re HIV-positive or have AIDS. Coping with this news may be difficult. Although HIV is a serious infection, people with
Simplifying HIV Treatment Now and in the Future
 Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Can we treat our way out of the HIV epidemic?
 Can we treat our way out of the HIV epidemic? Richard E. Chaisson, MD Center for AIDS Research Center for TB Research Johns Hopkins University Schoolboy s (and politician s) tricks for evading the question
Can we treat our way out of the HIV epidemic? Richard E. Chaisson, MD Center for AIDS Research Center for TB Research Johns Hopkins University Schoolboy s (and politician s) tricks for evading the question
AIDS at 25. Epidemiology and Clinical Management MID 37
 AIDS at 25 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Regional HIV and
AIDS at 25 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Regional HIV and
Structured Treatment Interruption in HIV Positive Patients. Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007
 Structured Treatment Interruption in HIV Positive Patients Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007 Objectives To become re-acquainted with the basics of HAART for HIV infection
Structured Treatment Interruption in HIV Positive Patients Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007 Objectives To become re-acquainted with the basics of HAART for HIV infection
Human Immunodeficiency Virus. Acquired Immune Deficiency Syndrome AIDS
 Human Immunodeficiency Virus Acquired Immune Deficiency Syndrome AIDS Sudden outbreak in USA of opportunistic infections and cancers in young men in 1981 Pneumocystis carinii pneumonia (PCP), Kaposi s
Human Immunodeficiency Virus Acquired Immune Deficiency Syndrome AIDS Sudden outbreak in USA of opportunistic infections and cancers in young men in 1981 Pneumocystis carinii pneumonia (PCP), Kaposi s
CLAUDINE HENNESSEY & THEUNIS HURTER
 HIV/AIDS/TB CLAUDINE HENNESSEY & THEUNIS HURTER KEY TERMS Do these sound familiar? What strange terms do you hear in the clinics? Any others to add?? HIV AIDS Viral Load & suppression CD4 count Regimen
HIV/AIDS/TB CLAUDINE HENNESSEY & THEUNIS HURTER KEY TERMS Do these sound familiar? What strange terms do you hear in the clinics? Any others to add?? HIV AIDS Viral Load & suppression CD4 count Regimen
HIV Management Update 2015
 9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
AIDS at 30 Epidemiology and Clinical Epidemiology and Management MID 37
 AIDS at 30 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Adults and children
AIDS at 30 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Adults and children
Distribution and Effectiveness of Antiretrovirals in the Central Nervous System
 Distribution and Effectiveness of Antiretrovirals in the Central Nervous System Scott Letendre, MD Associate Professor of Medicine HIV Neurobehavioral Research Center and Antiviral Research Center University
Distribution and Effectiveness of Antiretrovirals in the Central Nervous System Scott Letendre, MD Associate Professor of Medicine HIV Neurobehavioral Research Center and Antiviral Research Center University
Antiretroviral Therapy
 Antiretroviral Therapy Scott M. Hammer, M.D. 1986 1990 ZDV monorx 1990 1995 Alternative NRTI monorx Combination NRTI Rx Introduction of NNRTI s Antiretroviral resistance Pathogenetic concepts Evolution
Antiretroviral Therapy Scott M. Hammer, M.D. 1986 1990 ZDV monorx 1990 1995 Alternative NRTI monorx Combination NRTI Rx Introduction of NNRTI s Antiretroviral resistance Pathogenetic concepts Evolution
Historic Perspective on HIV and TB Research in Pregnant Women
 Historic Perspective on HIV and TB Research in Pregnant Women Lynne M. Mofenson, M.D. Senior HIV Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation High Burden of TB/HIV in Women - 2016 TB HIV
Historic Perspective on HIV and TB Research in Pregnant Women Lynne M. Mofenson, M.D. Senior HIV Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation High Burden of TB/HIV in Women - 2016 TB HIV
0.14 ( 0.053%) UNAIDS 10% (94) ( ) (73-94/6 ) 8,920
 UNAIDS 10% (94) ( ) (73-94/6 ) 8,920") 0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS IN HIV PREVENTION. Jason E. Vercher, PA-C, AAHIVM
 NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS IN HIV PREVENTION Jason E. Vercher, PA-C, AAHIVM Disclosures No disclosures to report Learning Objectives q Identify Individuals who would benefit from non-occupational
NON-OCCUPATIONAL POST EXPOSURE PROPHYLAXIS IN HIV PREVENTION Jason E. Vercher, PA-C, AAHIVM Disclosures No disclosures to report Learning Objectives q Identify Individuals who would benefit from non-occupational
ART for HIV Prevention:
 ART for HIV Prevention: KENNETH H. MAYER, M.D. Brown University/The Fenway Institute August 22, 2009 APPROACHES TO PREVENT HIV TRANSMISSION DECREASE SOURCE OF INFECTION Barrier Protection Treat STI Antiretroviral
ART for HIV Prevention: KENNETH H. MAYER, M.D. Brown University/The Fenway Institute August 22, 2009 APPROACHES TO PREVENT HIV TRANSMISSION DECREASE SOURCE OF INFECTION Barrier Protection Treat STI Antiretroviral
HIV Drugs and the HIV Lifecycle
 HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
Medscape's Antiretroviral Pocket Guide for the Treatment of HIV Infection
 Table 3. Characteristics of Nucleoside Reverse Transcriptase Inhibitors (NRTIs) Generic Name (Abbreviation) / Trade Name Abacavir (ABC) / Ziagen Trizivir with ZDV + 3TC Epzicom with 3TC Didanosine (ddi)
Table 3. Characteristics of Nucleoside Reverse Transcriptase Inhibitors (NRTIs) Generic Name (Abbreviation) / Trade Name Abacavir (ABC) / Ziagen Trizivir with ZDV + 3TC Epzicom with 3TC Didanosine (ddi)
The Eras of the HIV Epidemic
 The Eras of the HIV Epidemic 1930-1980 1981-1986 1987-1995 1996-2005 2nd Gen. HAART 2006-2011 2006: Disproportionate distribution of HIV 2006: Gates and Clinton at International AIDS conference announce
The Eras of the HIV Epidemic 1930-1980 1981-1986 1987-1995 1996-2005 2nd Gen. HAART 2006-2011 2006: Disproportionate distribution of HIV 2006: Gates and Clinton at International AIDS conference announce
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications
 and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications") Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
Vitamin D Deficiency in HIV: A Shadow on Long-Term Management?
 AIDS Rev. 2014;16:59-74 (Supplementary Data) Vitamin D Deficiency in HIV: A Shadow on Long-Term Management? Chloe Orkin, et al.: Vitamin D deficiency in HIV (Supplementary Data) Chloe Orkin 1, David A.
AIDS Rev. 2014;16:59-74 (Supplementary Data) Vitamin D Deficiency in HIV: A Shadow on Long-Term Management? Chloe Orkin, et al.: Vitamin D deficiency in HIV (Supplementary Data) Chloe Orkin 1, David A.
An HIV Update Jan Clark, PharmD Specialty Practice Pharmacist
 An HIV Update - 2019 Jan Clark, PharmD Specialty Practice Pharmacist 2 The goal of this program is to provide a review and update of HIV care and to provide a forum for discussing the current local and
An HIV Update - 2019 Jan Clark, PharmD Specialty Practice Pharmacist 2 The goal of this program is to provide a review and update of HIV care and to provide a forum for discussing the current local and
Measure #161: HIV/AIDS: Adolescent and Adult Patients with HIV/AIDS Who Are Prescribed Potent Antiretroviral Therapy
 Measure #161: HIV/AIDS: Adolescent and Adult Patients with HIV/AIDS Who Are Prescribed Potent Antiretroviral Therapy 2012 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION:
Measure #161: HIV/AIDS: Adolescent and Adult Patients with HIV/AIDS Who Are Prescribed Potent Antiretroviral Therapy 2012 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION:
HIV Lecture. Anucha Apisarnthanarak, MD Division of Infectious Diseases Thammasart University Hospital
 HIV Lecture Anucha Apisarnthanarak, MD Division of Infectious Diseases Thammasart University Hospital End-2001 global estimates for children and adults People living with HIV/AIDS New HIV infections in
HIV Lecture Anucha Apisarnthanarak, MD Division of Infectious Diseases Thammasart University Hospital End-2001 global estimates for children and adults People living with HIV/AIDS New HIV infections in
HIV and AIDS An update
 HIV and AIDS An update Barnet branch 24 th February 2009 Neal Marshall Specialist pharmacist HIV services Royal Free Hampstead NHS Trust Objectives To gain an insight into the epidemiology of HIV To gain
HIV and AIDS An update Barnet branch 24 th February 2009 Neal Marshall Specialist pharmacist HIV services Royal Free Hampstead NHS Trust Objectives To gain an insight into the epidemiology of HIV To gain
The ART of Managing Drug-Drug Interactions in Patients with HIV
 The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
ARVs on an Empty Stomach: Food Interaction Studies in a resource Limited Setting
 ARVs on an Empty Stomach: Food Interaction Studies in a resource Limited Setting Dr. Andrew D Kambugu, FRCP (UK) Infectious Diseases Institute, Makerere University Outline of Discussion Key Definitions
ARVs on an Empty Stomach: Food Interaction Studies in a resource Limited Setting Dr. Andrew D Kambugu, FRCP (UK) Infectious Diseases Institute, Makerere University Outline of Discussion Key Definitions
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course
 Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course The opinions or assertions contained herein are the private views of the author, and are not to be construed as official, or
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course The opinions or assertions contained herein are the private views of the author, and are not to be construed as official, or
2 nd Line Treatment and Resistance. Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012
 2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update
 Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Diagnosis and Initial Management of HIV/AIDS: What the Primary Care Provider Should Know
 Diagnosis and Initial Management of HIV/AIDS: What the Primary Care Provider Should Know Carolyn K. Burr, EdD, RN Co-Clinical Director Deputy Director François-Xavier Bagnoud Center December 17 th, 2013
Diagnosis and Initial Management of HIV/AIDS: What the Primary Care Provider Should Know Carolyn K. Burr, EdD, RN Co-Clinical Director Deputy Director François-Xavier Bagnoud Center December 17 th, 2013
Somnuek Sungkanuparph, M.D.
 HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
Addressing Pediatric Needs of the Most Neglected: next steps
 Addressing Pediatric Needs of the Most Neglected: next steps An updated overview of DNDi Pediatric Focus Nathalie Strub Wourgaft (Medical Director) Janice Lee (HIV Pediatric Clinical Manager) A Fatal Imbalance
Addressing Pediatric Needs of the Most Neglected: next steps An updated overview of DNDi Pediatric Focus Nathalie Strub Wourgaft (Medical Director) Janice Lee (HIV Pediatric Clinical Manager) A Fatal Imbalance
Pediatric Antiretroviral Resistance Challenges
 Pediatric Antiretroviral Resistance Challenges Thanyawee Puthanakit, MD The HIVNAT, Thai Red Cross AIDS research Center The Research Institute for Health Science, Chiang Mai University Outline The burden
Pediatric Antiretroviral Resistance Challenges Thanyawee Puthanakit, MD The HIVNAT, Thai Red Cross AIDS research Center The Research Institute for Health Science, Chiang Mai University Outline The burden
Update on antiretrovirals
 Southern African Journal of Anaesthesia and Analgesia 2018; 24(3)(Supplement 1) Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
Southern African Journal of Anaesthesia and Analgesia 2018; 24(3)(Supplement 1) Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011
 ART Treatment Guideline Training 31 st January to 4 th February, 2011") TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
HIV Testing. HIV Symposium Patient Jane. Outline: 4/13/2010. What are your primary concerns for this patient?
 Patient Jane HIV Symposium 2010 Jess Fogler Waldura, MD Mina Matin, MD National HIV AIDS Clinicians Consultation Center San Francisco General Hospital University of California, San Francisco Referral from
Patient Jane HIV Symposium 2010 Jess Fogler Waldura, MD Mina Matin, MD National HIV AIDS Clinicians Consultation Center San Francisco General Hospital University of California, San Francisco Referral from