Greenwich Academic Literature Archive (GALA) the University of Greenwich open access repository
|
|
|
- Abigayle Austin
- 6 years ago
- Views:
Transcription

1 Greenwich Academic Literature Archive (GALA) the University of Greenwich open access repository Citation for published version: Frempong, Kwadwo K., Walker, Martin, Cheke, Robert, Tetevi, Edward J., Gyan, Ernest T., Owusu, Ebenezer O., Wilson, Michael D., Boakye, Daniel A., Taylor, Mark J., Biritwum, Nana-Kwadwo, Osei- Atweneboana, Mike and Basanez, Maria-Gloria (2016) Does increasing treatment frequency address sub-optimal responses to ivermectin for the control and elimination of river blindness? Clinical Infectious Diseases (Advance Access). ISSN (Print), (Online) (doi: /cid/ciw144) Publisher s version available at: Please note that where the full text version provided on GALA is not the final published version, the version made available will be the most up-to-date full-text (post-print) version as provided by the author(s). Where possible, or if citing, it is recommended that the publisher s (definitive) version be consulted to ensure any subsequent changes to the text are noted. Citation for this version held on GALA: Frempong, Kwadwo K., Walker, Martin, Cheke, Robert, Tetevi, Edward J., Gyan, Ernest T., Owusu, Ebenezer O., Wilson, Michael D., Boakye, Daniel A., Taylor, Mark J., Biritwum, Nana-Kwadwo, Osei- Atweneboana, Mike and Basanez, Maria-Gloria (2016) Does increasing treatment frequency address sub-optimal responses to ivermectin for the control and elimination of river blindness?. London: Greenwich Academic Literature Archive. Available at: Contact: gala@gre.ac.uk
2 Clinical Infectious Diseases Advance Access published March 21, Does Increasing Treatment Frequency Address Sub-optimal Responses to Ivermectin for the Control and Elimination of River Blindness? Kwadwo K. Frempong 1,, Martin Walker 2,, Robert A. Cheke 2,3, Edward Jenner Tettevi 4, Ernest Tawiah Gyan 4, Ebenezer O. Owusu 5, Michael D. Wilson 1, Daniel A. Boakye 1, Mark J. Taylor 6, Nana-Kwadwo Biritwum 7, Mike Osei-Atweneboana 4, María-Gloria Basáñez 2 1 Noguchi Memorial Institute for Medical Research, University of Ghana, Legon, Ghana 2 London Centre for Neglected Tropical Disease Research (LCNTDR), Department of Infectious Disease Epidemiology, School of Public Health, Imperial College London, UK 3 Natural Resources Institute, University of Greenwich at Medway, Chatham Maritime, UK 4 Council for Scientific and Industrial Research-Water Research Institute, Accra, Ghana 5 Department of Animal Biology & Conservation Science, University of Ghana, Legon, Ghana 6 Department of Parasitology, Liverpool School of Tropical Medicine, Liverpool, UK 7 Ghana Health Service, Accra, Ghana Correspondence to: Prof María-Gloria Basáñez, Department of Infectious Disease Epidemiology, Imperial College London, St Mary s campus, Norfolk Place, London, W2 1PG, UK, Office: +44 (0) , m.basanez@imperial.ac.uk Alternative contact: Dr Mike Osei-Atweneboana, Department of Environmental Biology and Health, Council for Scientific and Industrial Research, Water Research Institute, P.O. Box M 32, Accra, Ghana, Office: +233 (0) , ext. 1002, oseiatweneboana@yahoo.co.uk The Author Published by Oxford University Press for the Infectious Diseases Society of America. This is an Open Access article distributed under the terms of the Creative Commons Attribution License ( which permits unrestricted reuse, distribution, and reproduction in any medium, provided the original work is properly cited.
3 2 Contributed equally to this work Summary of key points: The first 3 years of biannual ivermectin distribution in Ghana have substantially reduced Onchocerca volvulus infection levels in 10 sentinel communities, but longitudinal analysis indicates that some communities are still consistently responding sub-optimally to treatment, with implications for onchocerciasis elimination. Abstract Background. Several African countries have adopted a biannual ivermectin distribution strategy in some foci to control and eliminate onchocerciasis. In 2010, the Ghana Health Service started biannual distribution to combat transmission hotspots and sub-optimal responses to treatment. We assessed the epidemiological impact of the first 3 years of this strategy and quantified responses to ivermectin over two consecutive rounds of treatment in 10 sentinel communities. Methods. We evaluated Onchocerca volvulus microfilarial intensity and prevalence in those aged 20 years before the first, second and fifth (or sixth) biannual treatment rounds using skin snip data from 956 participants. We used longitudinal regression modelling to estimate rates of microfilarial repopulation of the skin in a cohort of 217 participants who were followed-up over the first two rounds of biannual treatment. Results. Biannual treatment has had a positive impact, with substantial reductions in infection intensity after 4 or 5 rounds in most communities. We identified three communities all having been previously recognised as responding sub-optimally to ivermectin with statistically significantly high microfilarial repopulation rates. We did not find any clear association between microfilarial repopulation rate and the number of years of prior intervention, coverage, or the community level of infection.
4 3 Conclusions. The strategy of biannual ivermectin treatment in Ghana has reduced O. volvulus microfilarial intensity and prevalence, but sub-optimal responses to treatment remain evident in a number of previously and consistently implicated communities. Whether increasing the frequency of treatment will be sufficient to meet the World Health Organization s 2020 elimination goals remains uncertain. In 1987, soon after ivermectin became licensed for human use [1], and following the first community trials [2], Ghana became one of the first countries to introduce mass treatment to control onchocerciasis (River Blindness). Ivermectin kills Onchocerca volvulus microfilariae (the larval progeny of adult worms that are transmissible to Simulium blackfly vectors) and temporarily sterilizes female worms such that numbers of microfilariae remain suppressed for at least three months following treatment [3]. Subsequently, females regain fertility and microfilariae repopulate the skin. Hence, ivermectin can only control onchocerciasis-associated disease caused by immunopathological responses to chronic infection of the skin and ocular tissue by microfilariae [4] when given at regular intervals. Infection can be eliminated if microfilariae are suppressed long enough to ensure that transmission is interrupted for at least 10 years, the average lifespan of adult worms [5]. Mass treatments with ivermectin have successfully eliminated onchocerciasis from foci in Mali and Senegal [6] (with annual or biannual distribution), Nigeria [7], Mexico [8], Colombia [9], Ecuador [10] and northern Venezuela [11]. (The strategy in Latin America has been mostly biannual treatment.) National programmes in Ethiopia and Uganda, among others, have adopted biannual distribution in some foci to accelerate progress towards elimination [12-14]. Despite years of ivermectin treatment in Ghana, and vector control in its savannah habitats, onchocerciasis still affects thousands of communities within 66 districts [15], and approximately 3.2 million people remain at risk of infection [16]. The resilience of onchocerciasis is probably partly due to poor responses to ivermectin in several Ghanaian communities [17, 18], raising fears of decreased ivermectin efficacy. In a community of normally responding individuals, microfilariae are expected to
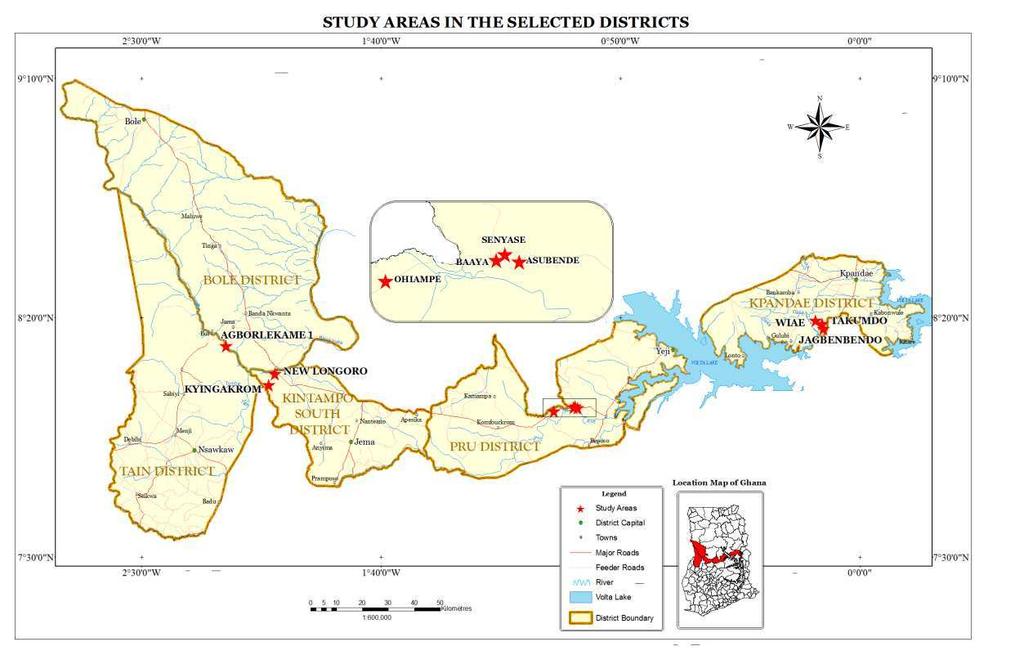
5 4 reach about 10% of their pre-treatment numbers 6 months after treatment, and about 20% 1 year after treatment [3, 17]. In sub-optimally responding communities, microfilarial repopulation rates 6 months after treatment have been observed at over 50% [19]. Some of these communities are those that have been treated with most rounds of ivermectin [20]. In 2010, in response to the persistence of onchocerciasis in Ghana, the Neglected Tropical Diseases Programme (NTDP) of the Ghana Health Service (GHS) adopted a biannual treatment strategy in 44 out of 77 endemic communities [21]. Here, we report microfilarial loads and prevalence in 10 NTDP sentinel communities some previously identified as responding sub-optimally to ivermectin before and after 4 (or 5) rounds of biannual treatment. We evaluate responses to ivermectin by estimating rates of microfilarial repopulation in cohorts of individuals followed-up at 3 and 6 months after treatment, comparing skin repopulation rates with community endemicity, therapeutic coverage and number of years of prior ivermectin treatment. We discuss our results in the contexts of historical epidemiological data collected from these communities during annual ivermectin distribution and the World Health Organization (WHO) s goals to eliminate onchocerciasis [22]. Methods Ethical approval Ethical approval was obtained from the ethics review committees of the Noguchi Memorial Institute for Medical Research, Ghana [NMIMR-IRB CPN ], the Ghana Health Service [GHS ERC 04_3_11], and Imperial College London Research and Ethics Committee [ICREC_11_2_4]. Study site The study was conducted in 10 onchocerciasis endemic communities within savannah regions of Ghana (Figure 1). The communities were selected from some of the endemic areas where concerns on ivermectin efficacy have been previously reported [19]. By the time of this investigation, study communities had received between 14 and 23 rounds of annual ivermectin treatment.
6 5 Study design The 10 selected communities had been scheduled to receive mass biannual treatments with ivermectin from July We used the inclusion/exclusion criteria for selecting communities described in [19], including communities previously identified as responding sub-optimally to ivermectin [17, 18, 20]. We recruited adults aged 20 years, randomly selected from different households. The number of eligible participants represented about 50 70% of the total population within the 10 studied communities. Those who were included represented about 10 40% of the total population and, of the total eligible population, approximately 70% in small communities (such as Asubende, with a population of 87) and roughly 20% in larger communities (such as New Longoro and Wiae with, respectively, populations of 1,650 and 1,611). The objectives and schedules of the study were explained to every individual, and those who agreed to participate signed a consent form. Figure 2 illustrates the study design and times of treatment with ivermectin (150µg/kg, directly observed) using an example timeline of six trial participants. Skin snips of 956 consenting participants were taken in July 2010 just before the first round of biannual ivermectin treatment. All 956 participants were skin snipped six months later, in January 2011, just before the second biannual treatment round. A total of 217 (22.7%) of these participants (Table 1), who were positive for microfilariae in July 2010 (e.g. participants 1 5 in Figure 2), formed a cohort for evaluating rates of skin microfilarial repopulation. Within this cohort, the 186 participants (Table 1) positive for microfilariae in January 2011 (e.g. participants 1 4 in Figure 2) were skin snipped in April 2011 and in July 2011, just before the third round of biannual ivermectin treatment (some participants were lost to follow-up, e.g. participants 3 and 4 in Figure 2). Three further rounds of ivermectin treatment were distributed approximately every six months, in April 2012, December 2012 and June 2013, as part of GHS NTDP activities. Before the final round of treatment, in June 2013, a final round of skin snipping of consenting participants (e.g. participants 1, 3, 4 and 6 in Figure 2) was repeated. Techniques used to count microfilariae in skin snip biopsies are described in Supplementary Methods, Parasitological methods.
7 6 Community Microfilarial Load and Community Microfilarial Prevalence We calculated Community Microfilarial Load (CMFL) [23] and Community Microfilarial Prevalence (CMFP) as our primary and secondary indicators of community infection levels in the adult (aged 20 years) population. These were calculated before the first round of biannual treatment in July 2010, before the second round, in January 2011, and before the 5 th or 6 th round in March 2013 or June 2013 (the schedules of each community differed slightly). CMFL and CMFP calculations are given in Supplementary Methods, Community microfilarial load and community microfilarial prevalence. Community treatment history and coverage We obtained data on the community treatment coverage (Supplementary Figure A) at all treatment rounds from the NTDP to facilitate interpretation of CMFL and CMFP throughout the study. Coverage was calculated using treatment and census data provided by the community ivermectin distributors to the NTDP. It refers to the therapeutic coverage in the total population. Historical records of coverage were also obtained from the GHS NTDP. Microfilarial repopulation We constructed log-linear marginal regression models [24] to describe the average number of microfilariae per skin snip (mf/ss) in the longitudinal cohort of 217 individuals (Table 1, Figure 2), adjusting for community, participant age and sex. We constructed two models to analyse the data (Table 2). Both permit repopulation rates to vary among communities but the first (Model 1A and 1B, Table 2) permits repopulation rates to vary between the two consecutive repopulation periods, while the second (Model 2, Table 2) estimates a single community-specific repopulation rate, combining information from both repopulation periods. Mathematical details are given in Supplementary Methods, Marginal regression models. We compared microfilarial repopulation rates graphically and by identifying communities with statistically significantly different estimates compared with a reference community (Takumdo). We also explored graphically how repopulation rates correlated with prior number of years of ivermectin treatment, therapeutic coverage, and CMFL just before the start of biannual treatment.
8 7 Results Trends in community infection Figure 3 presents community-specific CMFLs calculated in July 2010, January 2011 and March (or June) 2013 (CMFPs are presented in Supplementary Figure B). We include the dates when each round of biannual treatment was distributed and the population coverage. The impact of the first round of biannual treatment appears somewhat greater than that in subsequent rounds, as demonstrated by the slightly faster decline in CMFL between round 1 (July 2010), and round 2 (January 2011), compared with that between round 2 and the final assessment of infection levels in March (or June) 2013 (compare the gradients of the dotted lines in Figure 3). This trend is most apparent in Asubende, Jagbenbendo, New Longoro, Senyase and Wiae, and least pronounced in Agborlekame 1 and Takumdo. In Ohiampe, community infection levels were greater in June 2013 than in July 2010, despite 4 rounds of treatment (one round was missed in the first quarter of 2013). Trends in microfilarial repopulation Figure 4 presents the observed and model-fitted (from Model 1A, Table 2) mean number of mf/ss by sampling date and community in the reference demographic stratum of males in the (20,40] age group. We also include the model-predicted mean number of microfilariae per skin snip (mf/ss) in October 2010 (3 months after the first round of biannual treatment), indicating the likely microfilarial dynamics during the first six-month repopulation period. In general, mean numbers of mf/ss per stratum are lower after the second repopulation period than after the first; microfilariae cannot repopulate completely in six months before further suppression by another treatment round. Mean numbers of mf/ss per stratum in January 2011, six months after the start of biannual treatment, are quite high compared with those in July 2010 (one expects microfilariae to reach about 10% of their pre-treatment population level after six months [3]). Microfilarial repopulation rates We define the rate of microfilarial repopulation as the mean number of mf/ss expressed as a percentage of the mean immediately before the preceding treatment with ivermectin. This captures
9 8 how quickly microfilariae reappear in the skin between consecutive treatment rounds. Figure 5 provides standardized six-month repopulation rates, adjusted by the differing exact durations between sampling times (calculated from Model 1B in Table 2; non-standardized repopulation rates are depicted in Supplementary Figure C). These estimates confirm that microfilarial repopulation rates are generally quite high, typically approximately 50% during the first period of repopulation, and similar, albeit somewhat more variable after the second repopulation period. The repopulation rates in Asubende and Kyingakrom after the second round of treatment are statistically significantly higher than in the reference community of Takumdo. Figure 6 presents the single relative rates of repopulation by community (estimated using Model 2, Table 2) compared to Takumdo. Over both repopulation periods, rates of repopulation are statistically significantly (P < 0.05) higher in Asubende, Kyingarom and New Longoro compared with Takumdo. Graphically, we find no obvious association between the relative rate of microfilarial repopulation and: (i) the number of annual treatments with ivermectin before the start of the study (Figure 6B), (ii) the CMFL before the first biannual treatment (Figure 6C), or (iii) the average coverage of ivermectin distribution during the cohort component of the study (Figure 6D, see Supplementary Figure A for disaggregated coverage data). Discussion Onchocerciasis in Ghana remains resilient to the long-standing and large-scale (antivectorial and antiparasitic) interventions implemented over the past 40 years [25]. Despite having been earmarked for elimination as a public health problem by 2015 [16], there exist persistent hotspots of transmission [19, 26, 27] and reports of O. volvulus microfilariae repopulating the skin of patients faster than expected following treatment with ivermectin [19,20], a phenomenon also documented in Cameroon [28]. In 2010, and responding to this challenge, the GHS implemented biannual mass ivermectin treatment in many endemic communities [21]. We report on trends in community-wide infection with O. volvulus in 10 Ghanaian communities over the first 3 years of this biannual strategy and evaluate rates of microfilarial repopulation in cohorts of participants over the first two rounds of treatment.
10 9 The last systematic evaluation of community infection levels in many of the studied communities was in 2004/2005, after annual mass ivermectin treatments [19] (Supplementary Table A and Supplementary Table B). Comparing these values with infection levels in July 2010 shows that the intervening 6 years of annual ivermectin mass treatment have reduced CMFLs generally by at least 50%. Infection levels were further reduced by March or June 2013, after 3 years of biannual treatment. Reductions in CMFL were > 36% in most communities and the CMFP was statistically significantly less than 10% in 5 out of 10 communities (Supplementary Table A and Supplementary Table B). Hence, the biannual strategy has had a positive impact. Whether residual infection levels constitute a public health problem would be best evaluated by measuring levels of onchocerciasis-associated morbidity. However, it is hard to envisage declaring the problem eliminated in communities where microfilarial prevalence is > 10%, or > 20% as in Jagbenbendo. Moreover, whether biannual treatments will ultimately be sufficient to eliminate infection will depend on local transmission and programmatic conditions, particularly on the intensity of blackfly biting [25, 26] and the sustainability of high levels of treatment coverage and adherence [29, 30]. One of the objectives of the NTD Modelling Consortium ( is to determine what intervention strategies will be necessary to eliminate infection in the timelines set out by the WHO Roadmap on NTDs [22]. The six-month rates of repopulation estimated here are broadly around 50% and are high compared with the expected 10% from parasite populations predominantly naïve to ivermectin [3]. They are also higher than those estimated from some of the same communities in 2005, which were typically < 30% (Supplementary Table C). Some of this discrepancy is probably because the 10% value (and the previous estimates from these communities) were based on geometric means which are not strictly comparable with the model-derived repopulation rates presented here (which correspond to arithmetic means). Further, the sampling scheme employed in this study (and previously in the same communities [19]) followed up only participants who were positive for microfilariae at recruitment. This ensures that only people infected with O. volvulus are repeatedly skin snipped, increasing the efficiency of sampling when the prevalence of infection is low. Unfortunately, this necessary protocol
11 10 potentially introduces sampling biases because the sensitivity of skin snipping declines with decreasing infection intensity [31]. Hence, participants with less intense infections are more likely to be erroneously deemed uninfected and not followed up. This will probably upwardly bias repopulation rates because more intensely infected people will have more microfilariae after a period of repopulation than those with less intense infections. Notwithstanding these cautions, the three communities with the highest repopulation rates over the two repopulation periods (Asubende, Kyingakrom, New Longoro) have been previously implicated as responding sub-optimally to ivermectin [19, 20, 27]. A mechanistic cause underlying these observations cannot be determined from the statistical analysis presented here. However, previous suggestions that faster rates of skin repopulation by microfilariae might result from a sudden increase in new infections between treatment rounds perhaps due to programmatic deficiencies in coverage and compliance [32, 33] are difficult to reconcile with the generally high levels of therapeutic coverage observed throughout (Figures 6D) and before (Supplementary Figure A) the study. It is more likely that transmission has been declining since the onset of biannual ivermectin treatment in July 2010, as evidenced by the generally falling CMFL (Figure 3), although noteworthy is the resilience of community infection levels to biannual distribution in Kyingakrom (Supplementary Table A and Supplementary Table B). Work is ongoing to evaluate the genotype of adult parasites extracted from some of the participants of this study. Previous analyses comparing allele frequencies among adult female O. volvulus infecting people in multiply treated and ivermectin-naïve populations in Ghana and Cameroon identified selection of P-glycoprotein and -tubulin genes, both associated with resistance to ivermectin in helminth infections of livestock [34, 35]. Moreover, a genetic analysis of the entire region of the tubulin gene extracted from worms infecting people from Kyingakrom a consistently implicated sub-optimally responding community has identified statistically significantly higher frequencies of 6 single nucleotide polymorphisms [36]. How the phenotypic response of individual worms relates to these genetic changes remains incompletely understood. Worms collected from sub-optimally responding communities have been associated with higher fertility than worms from putatively
12 11 normally responding communities [36], possibly indicative of a faster resumption of fertility following exposure to ivermectin [28]. However, results elsewhere suggest that selection driven by exposure to ivermectin is associated with a pleiotropic fitness cost of decreased fertility [35], so perhaps putatively resistant worms can resume production of microfilariae more rapidly than their susceptible counterparts, but ultimately have less reproductive potential. Our conclusions on microfilarial repopulation rates are based on average, community estimates, adjusted for individual (host) characteristics such as age and sex. This is consistent with the inferential basis of previous, more descriptive, analyses of data from some of the same communities studied here [19, 27]. Yet, particularly for these well-studied and relatively small communities, many of the same individuals have probably repeatedly participated in the epidemiological studies undertaken over the last 15 years. Hence, future analyses should focus on estimating drug responses at the individual level [37, 38]. It is more plausible that certain individuals, rather than entire communities, are consistently responding poorly to ivermectin (and influencing the community-wide response). Poor individual responses to treatment might be caused by host-related factors or given the long life span of adult O. volvulus by drug-tolerant parasites. The biannual ivermectin treatment strategy is markedly reducing O. volvulus infection levels in Ghana. However, despite high and sustained therapeutic coverage, sub-optimal responses to ivermectin persist in previously implicated communities. Whether this is caused by drug-tolerant or resistant parasites, or by host-related factors remains unclear. Analyses are yet to be performed to test the hypothesis that community-level sub-optimal responses are driven by a minority of consistently poorly responding individuals (or their worms) and to identify underlying mechanisms. The EPIONCHO and ONCHOSIM mathematical transmission models are being used to assess the feasibility of meeting the WHO elimination goals with annual or biannual ivermectin treatment [29, 30, 38, 39], and in future they will be used to establish which settings may require alternative or complementary strategies (such as test-and-treat macrofilaricidal doxycycline therapy [40] and/or focal vector control). Such modelling projections cover a wide range of epidemiological and
13 12 programmatic contexts, but should also accommodate the possibility that ivermectin may not be as universally efficacious as hoped. Acknowledgements We would like to acknowledge the contributions from the research team involved in the field work of this study, ivermectin distributors, participants, members of the various communities and the Ghana Health Service s posts within the local districts for their cooperation during the long-term follow-ups. Our gratitude also goes to the NTDP in Accra, Ghana especially to Mr Odame Asiedu and Mr Paul Yikpotey for providing us with the long-term coverage data for this study. The cooperation from the participating institutions is also acknowledged for providing the laboratory space and logistics towards the progress of this research, especially CSIR-WRI and Imperial College London. Funding This work was supported by a Royal Society Leverhulme Trust (Capacity Building) Africa Award [to MYO-A and MGB]. MW and MGB acknowledge funding from the Wellcome Trust [grant no /Z/10/Z] and from the NTD Modelling Consortium by the Bill and Melinda Gates Foundation in partnership with the Task Force for Global Health. MW and MGB also acknowledge that this investigation received financial support from the UNICEF/UNDP/World Bank WHO Special Programme for Research and Training in Tropical Disease (TDR) [grant no. 2015/ ]. Disclaimer The views, opinions, assumptions or any other information set out in this article are solely those of the authors. The funders had no role in writing the manuscript or in the decision to submit it for publication. Potential conflicts of interest The authors declare that they have no conflict of interests.
14 13 References 1. Crump A, mura S. Ivermectin, 'wonder drug' from Japan: the human use perspective. Proc Jpn Acad Ser B Phys Biol Sci. 2011; 87: Alley ES, Plaisier AP, Boatin BA, Dadzie KY, Remme J, Zerbo G, et al. The impact of five years of annual ivermectin treatment on skin microfilarial loads in the onchocerciasis focus of Asubende, Ghana. Trans R Soc Trop Med Hyg 1994; 88: Basáñez MG, Pion SDS, Boakes E, Filipe JAN, Churcher TS, Boussinesq M. Effect of singledose ivermectin on Onchocerca volvulus: a systematic review and meta-analysis. Lancet Infect Dis 2008; 8: Brattig NW. Pathogenesis and host responses in human onchocerciasis: impact of Onchocerca filariae and Wolbachia endobacteria. Microbes Infect 2004; 6: Plaisier AP, van Oortmarssen GJ, Remme J, Habbema JDF. The reproductive lifespan of Onchocerca volvulus in West African savanna. Acta Trop 1991; 48: Traore MO, Sarr MD, Badji A, Bissan Y, Diawara L, Doumbia K, et al. Proof-of-principle of onchocerciasis elimination with ivermectin treatment in endemic foci in Africa: final results of a study in Mali and Senegal. PLoS Negl Trop Dis 2012; 6: Tekle AH, Elhassan E, Isiyaku S, Amazigo UV, Bush S, Noma M, et al. Impact of long-term treatment of onchocerciasis with ivermectin in Kaduna State, Nigeria: first evidence of the potential for elimination in the operational area of the African Programme for Onchocerciasis Control. Parasit Vectors 2012; 5: Rodríguez-Pérez MA, Fernández-Santos NA, Orozco-Algarra ME, Rodríguez-Atanacio JA, Domínguez-Vázquez A, Rodríguez-Morales KB, et al. Elimination of onchocerciasis from Mexico. PLoS Negl Trop Dis 2015; 9:e
15 14 9. West S, Munoz B, Sommer A. River blindness eliminated in Colombia. Ophthalmic Epidemiol 2013; 20: Lovato R, Guevara A, Guderian R, Proaño R, Unnasch T, Criollo H, et al. Interruption of infection transmission in the onchocerciasis focus of Ecuador leading to the cessation of ivermectin distribution. PLoS Negl Trop Dis 2014; 8:e Convit J, Schuler H, Borges R, Olivero V, Domínguez-Vázquez A, Frontado H, et al. Interruption of Onchocerca volvulus transmission in Northern Venezuela. Parasit Vectors 2013; 6: Katabarwa M, Richards F. Twice-yearly ivermectin for onchocerciasis: the time is now. Lancet Infect Dis 2014; 14: Katabarwa M, Lakwo T, Habomugisha P, Agunyo S, Byamukama E, Oguttu D, et al. Transmission of Onchocerca volvulus by Simulium naevei in Mount Elgon focus of Eastern Uganda has been interrupted 2014; 90: African Programme for Onchocerciasis Control (APOC). Report of the thirty-eighth session of the technical consultative committee. Available at: Accessed 4 March Ministry of Health Ghana Health Service. Two-year strategic plan for integrated neglected tropical diseases control in Ghana Available at: Accessed 4 March Taylor MJ, Awadzi K, Basáñez MG, Biritwum N, Boakye D, Boatin B, et al. Onchocerciasis control: Vision for the future from a Ghanian perspective. Parasit Vectors 2009; 2:7.
16 Awadzi K, Boakye DA, Edwards G, Opoku NO, Attah SK, Osei-Atweneboana MY, et al. An investigation of persistent microfilaridermias despite multiple treatments with ivermectin, in two onchocerciasis-endemic foci in Ghana. Ann Trop Med Parasitol 2004; 98: Awadzi K, Attah SK, Addy ET, Opoku NO, Quartey BT, Lazdins-Helds JK, et al. Thirty-month follow-up of sub-optimal responders to multiple treatments with ivermectin, in two onchocerciasis-endemic foci in Ghana. Ann Trop Med Parasitol 2004; 98: Osei-Atweneboana MY, Eng JKL, Boakye DA, Gyapong JO, Prichard RK. Prevalence and intensity of Onchocerca volvulus infection and efficacy of ivermectin in endemic communities in Ghana: a two-phase epidemiological study. Lancet 2007; 369: Churcher TS, Pion SDS, Osei-Atweneboana MY, Prichard RK, Awadzi K, Boussinesq M, et al. Identifying sub-optimal responses to ivermectin in the treatment of River Blindness. Proc Natl Acad Sci USA 2009; 106: Turner HC, Osei-Atweneboana MY, Walker M, Tettevi EJ, Churcher TS, Asiedu O, et al. The cost of annual versus biannual community-directed treatment of onchocerciasis with ivermectin: Ghana as a case study. PLoS Negl Trop Dis 2013; 7:e World Health Organization. Accelerating work to overcome the global impact of neglected tropical diseases. A roadmap for implementation. Geneva: World Health Organization; Available at: Accessed 4 March Remme J, Ba O, Dadzie KY, Karam M. A force-of-infection model for onchocerciasis and its applications in the epidemiological evaluation of the Onchocerciasis Control Programme in the Volta River basin area. Bull World Health Organ 1986; 64: Diggle P, Heagerty P, Liang KY, Zeger SL. Analysis of Longitudinal Data. 2 nd ed. Oxford: Oxford University Press; 2013.
17 Lamberton PHL, Cheke RA, Winskill P, Tirados I, Walker M, Osei-Atweneboana MY, et al. Onchocerciasis transmission in Ghana: persistence under different control strategies and the role of the simuliid vectors. PLoS Negl Trop Dis 2015; 9:e Lamberton PHL, Cheke RA, Walker M, Winskill P, Osei-Atweneboana MY, Tirados I, et al. Onchocerciasis transmission in Ghana: biting and parous rates of host-seeking sibling species of the Simulium damnosum complex. Parasit Vectors 2014; 7: Osei-Atweneboana MY, Awadzi K, Attah SK, Boakye DA, Gyapong JO, Prichard RK. Phenotypic evidence of emerging ivermectin resistance in Onchocerca volvulus. PLoS Negl Trop Dis 2011; 5:e Pion SDS, Nana-Djeunga HC, Kamgno J, Tendongfor N, Wanji S, Njiokou F, et al. Dynamics of Onchocerca volvulus microfilarial densities after ivermectin treatment in an ivermectin-naïve and multiply treated population from Cameroon. PLoS Negl Trop Dis 2013; 7: e Turner HC, Churcher TS, Walker M, Osei-Atweneboana MY, Prichard RK, Basáñez MG. Uncertainity surrounding projections of the long-term impact of ivermectin treatment on human onchocerciasis. PLoS Negl Trop Dis 2013; 7:e Turner HC, Walker M, Churcher TS, Osei-Atweneboana MY, Biritwum NK, Hopkins A, et al. Reaching the London Declaration on Neglected Tropical Diseases goals for onchocerciasis: an economic evaluation of increasing the frequency of ivermectin treatment in Africa. Clin Infect Dis 2014; 59: Taylor HR, Munoz B, Keyvan-Larijani E, Greene BM. Reliability of detection of microfilariae in skin snips in the diagnosis of onchocerciasis. Am J Trop Med Hyg 1989; 41: Cupp E, Richards F, Lammie P, Eberhard M. Efficacy of ivermectin against Onchocerca volvulus in Ghana. Lancet 2007; 370:1123.
18 Remme JHF, Amazigo U, Engels D, Barryson A, Yameogo L. Efficacy of ivermectin against Onchocerca volvulus in Ghana. Lancet 2007; 370: Eng JK, Prichard PK. A comparison of genetic polymorphism in populations of Onchocerca volvulus from untreated- and ivermectin-treated patients. Mol Biochem Parasitol 2006; 142: Bourguinat C, Pion SDS, Kamgno J, Gardon J, Duke BOL, Boussinesq M, et al. Genetic selection of low fertile Onchocerca volvulus by ivermectin treatment. PLoS Negl Trop Dis 2007; 1:e Osei-Atweneboana MY, Boakye DA, Awadzi K, Gyapong JO, Prichard RK. Genotypic analysis of -tubulin in Onchocerca volvulus from communities and individuals showing poor parasitological response to ivermectin treatment. Int J Parasitol Drugs Drug Resist 2012; 2: Walker M, Churcher TS, Basáñez MG. Models for measuring anthelmintic drug efficacy for parasitologists. Trends Parasitol 2014; 30: Coffeng LE, Stolk WA, Hoerauf A, Habbema D, Bakker R, Hopkins AD, et al. Elimination of African onchocerciasis: modeling the impact of increasing the frequency of ivermectin mass treatment. PLoS One 2014; 9:e Stolk WA, Walker M, Coffeng LE, Basáñez MG, de Vlas SJ. Required duration of mass ivermectin treatment for onchocerciasis elimination in Africa: a comparative modelling analysis. Parasit Vectors 2015; 8: Walker M, Specht S, Churcher TS, Hoerauf A, Taylor MJ, Basáñez MG. Therapeutic efficacy and macrofilaricdal acitivity of doxycyline for the treatment of river blindness. Clin Infect Dis 2015; 60:
19 18 Figure Legends Figure 1. Map of Ghana indicating administrative regions and locations of study communities. Figure 2. Schematic timeline and illustrative history of six trial participants of the study used to evaluate community trends in infection and rates of microfilarial repopulation following the onset of a biannual treatment strategy in 10 Ghanaian communities. Participants 1-6 represent 6 of the 956 consenting individuals from whom skin snips were taken in July 2010 just before the first round of biannual ivermectin treatment and the again, six months later, in January 2011, just before the second round of biannual ivermectin treatment. Participants 1-5 were positive for microfilariae in July 2010 and hence were included in the cohort of 217 individuals for evaluating rates of skin microfilarial repopulation. Participants 1-4 represent 4 of the 186 individuals who were microfilariae positive in January 2011, with participants 1 and 2 successfully followed up and skin snipped in April 2011 and again in July 2011, just before the third round of biannual ivermectin treatment. Participants 1, 3, 4 and 6 represent 4 of the original 956 participants who agreed to be skin snipped for a final time in June 2013, just before the final round of treatments delivered by the Ghana Health Service Neglected Tropical Disease Programme. The months given on the timeline are the modal months of treatment activity among the 10 communities, but there is significant variation in the months and exact dates, especially for the biannual treatments given after July 2011 (see Figure 3 for exact dates). Figure 3. Trends in community microfilarial loads in 10 Ghanaian communities from the onset of a biannual ivermectin treatment strategy. Community Microfilarial Load (CMFL) is defined as the geometric mean number of microfilariae per skin snip in people aged 20 years and above. Coloured arrows indicate dates when mass treatment with ivermectin was distributed, by either the authors or the Community Ivermectin Distributors. Ivermectin was administered directly after skin snipping on dates when microfilarial load was assessed. Data on the community therapeutic coverage of ivermectin were collated by the Ghana Health Service. Note that the six scheduled rounds of biannual ivermectin treatment were successfully delivered to only 5 (Asubende; Baaya; Kyingakrom; New Longoro and Senyase) out of the 10 communities; the others communities (Agborlekame 1;
20 19 Jagbenbendo; Ohiampe; Takumdo, and Wiae) achieved five rounds of biannual treatment. Vertical lines indicate 95% confidence intervals calculated using a non-parametric bootstrap technique (see Supplementary Methods, Community Microfilaria Load and Community Microfilarial Prevalence). Dotted lines join estimated values and are for presentation purposes only. Triangles indicate times of ivermectin treatment and numbers above triangles indicate the therapeutic coverage in the whole community. Figure 4. Trends in mean numbers of microfilariae (mf per skin snip, ss) per participant in 10 Ghanaian communities from the onset of a biannual ivermectin treatment strategy. Data points represent observed mean microfilarial loads, by community, in the reference strata of males within the (20,40] age group. The solid vertical lines are corresponding 95% bootstrap confidence intervals. Triangles indicate when ivermectin was administered to the study participants. Solid lines join fitted estimated values and in the case of October 2010, predicted values from the marginal regression model which includes additive stratum adjustments for age group and sex, and interactive adjustments between sampling date and community (Model 1A in Table 2). Dotted lines join the corresponding 95% confidence bounds calculated using robust sandwich estimators of coefficient standard errors (see Supplementary Methods, Marginal regression models). The predicted values in October 2010 are provided to assist the reader to envisage the likely dynamics in mean numbers of mf/ss between the first and second sampling date. These predictions were generated from the marginal regression model that treats the time since the preceding ivermectin treatment as a continuous variable (Model 2 in Table 2) and assumes that (hypothetical) microfilarial sampling took place midway between the July 2010 and January 2011 sampling times. Note that data from Baaya are not shown because only 1 participant was microfilaria-positive and followed up in this community (Table 1), leading to very large associated estimates of uncertainty. Figure 5. Six-month microfilarial repopulation rates in 10 Ghanaian communities from the onset of a biannual ivermectin treatment strategy. Filled and open data points represent, respectively estimated mean microfilarial loads six months after the first or second round of ivermectin treatment expressed as a percentage of the microfilarial load estimated just before the preceding round of ivermectin
21 20 treatment. These estimates are derived from Model 1B (Table 2) which adjusts for the variable follow-up times among communities, permitting estimation of directly comparable standardized sixmonth rates of repopulation. Note that the six-month microfilarial repopulation rate from Baaya is not shown because only 1 participant was microfilaria-positive and followed up in this community (Table 1), leading to very large associated estimates of uncertainty. Vertical lines indicate 95% confidence bounds, calculated using robust sandwich estimators of coefficient standard errors (see Supplementary Methods, Marginal regression models). Stars indicate P values comparing the rate of repopulation with the reference village of Takumdo: *** P < 0.001; ** P<0.01. Figure 6. Relative six-month microfilarial repopulation rates in 10 Ghanaian communities over the first two rounds of a biannual ivermectin treatment strategy. Data points represent the estimated relative (multiplicative) six-month microfilarial repopulation in each community compared with Takumdo. Six-month repopulation rates are defined as mean microfilarial loads six months after a round of ivermectin treatment expressed as a percentage of the microfilarial load estimated just before the preceding treatment round. Estimates are derived from Model 2 (Table 2) that treats time since the preceding ivermectin treatment as a continuous covariate interacting with the indicator covariate for community. The six-month microfilarial repopulation rate from Baaya is not shown because only 1 participant was microfilaria-positive (Table 1), leading to very large associated estimates of uncertainty. (A) Estimates are plotted side-by-side for the different communities. (B) Estimates are plotted against the number of years of ivermectin treatment preceding the biannual strategy. (C) Estimates are plotted against CMFL preceding the first biannual ivermectin treatment (D) Estimates are plotted against the mean coverage of ivermectin distribution for the years 2010 and 2011 corresponding to the component of the study when the longitudinal cohort of participants was followed up over two consecutive rounds of biannual treatment (see also Supplementary Figure A for disaggregated coverage data from 2005 to 2013). Vertical lines are 95% confidence bounds, calculated using robust sandwich estimators of coefficient standard errors (see Supplementary Methods, Marginal regression models). Solid horizontal lines in panel C indicate 95% confidence bounds associated with the estimated CMFL, calculated using a numerical bootstrap resampling
22 21 method (see Supplementary Methods, Community Microfilarial Load and Community Microfilarial Prevalence). Stars indicate P values comparing with the reference village of Takumdo: * P < 0.05.
23 22 Tables Table 1. Longitudinal cohorts of participants in 10 Ghanaian communities who were followed up and skin snipped over the first two rounds of biannual treatment with ivermectin Community Month and year (months since preceding round of treatment) July 2010 (0) a January 2011 (6) b April 2011 (3) July 2011 (6) Agborlekame Asubende Baaya Jagbenbendo Kyingakrom New Longoro Ohiampe Senyase Takumdo Wiae Total a Only participants positive for microfilariae were followed up in January 2011; b only participants positive for microfilariae followed up in April 2011 and July 2011.
24 23 Table 2. Key features of the log-linear marginal regression models used to describe the observed microfilarial counts in the longitudinal cohort Type Variant Key features Model 1 A & B Response/outcome variable defined by individual microfilarial counts Modelled mean number of microfilariae per participant adjusted for the covariates age group (0,20], (20,40], (40,60] and (60,82], sex and community Microfilarial repopulation rates permitted to vary among communities and between repopulation periods by including sampling time as a categorical covariate interacting with community B Microfilarial repopulation rates adjusted by exact number of days since preceding round of ivermectin treatment yielding standardized repopulation rates (e.g. six-month repopulation rates) Model 2 Response/outcome variable defined by individual microfilarial counts Modelled mean number of microfilariae per participant adjusted for the covariates age group (0,20], (20,40], (40,60] and (60,82], sex and community A single microfilarial repopulation rate estimated for each community, combining information from both repopulation periods, by including sampling time as a continuous covariate defined as days since preceding ivermectin treatment interacting with community Additive, community-wide adjustments for potentially different repopulation rates between two repopulation periods
25 24
26 25
27 Community Microfilarial Load / /2011 Agborlekame 1 Asubende Baaya Jagbenbendo 75% 93% 76% 87% 97% 85% 82% 86% 75% 64% 66% 67% 88% 76% 91% 88% 91% 90% 88% 90% 89% 90% 90% 94% 81% 88% 96% 78% 42% 82% 90% 88% 52% 84% 89% 81% 80% 88% 78% 88% 83% 91% 85% 84% 82% 84% 78% Kyingakrom New Longoro Ohiampe Senyase Takumdo 07/ / / / / / /2011 Date Wiae 07/ / / / /2013 Coverage (%) (40,50] (50,60] (60,70] (70,80] (80,90] (90,100] 81% 85% 82% 71% 83% 84% 83% 88% Downloaded from at University of Greenwich on March 23, 2016
28 Mean number of microfilariae per participant / /2010 Agborlekame 1 Asubende Jagbenbendo Kyingakrom New Longoro Ohiampe Senyase Takumdo Wiae 01/ / /2011 Date 07/ / / / / / / / / /2011 Downloaded from at University of Greenwich on March 23, 2016
29 300% 200% *** 100% ** 0% 400% Agborlekame1 Asubende Jagbenbendo Kyingakrom New Longoro Ohiampe Senyase Takumdo Wiae Community Treatment round round 1, Jul 2010 round 2, Jan 2011 Six month microfilarial repopulation rate
30 0.0 Relative six month microfilarial repopulation rate C Agborlekame1 Asubende Relative six month microfilarial repopulation rate A at University of Greenwich on March 23, 2016 Downloaded from Community microfilarial load at start of biannual treatment Mean coverage % 82.5% 85.0% 87.5% 90.0% 0.0 * ** Relative six month microfilarial repopulation rate 2.5 * ** Jagbenbendo Kyingakrom New Longoro Senyase Ohiampe Takumdo Wiae D Community Years of treatment * * * * * * Relative six month microfilarial repopulation rate B
Modelling the elimination of river blindness using long-term epidemiological and programmatic data from Mali and Senegal
 Modelling the elimination of river blindness using long-term epidemiological and programmatic data from Mali and Senegal Martin Walker, Wilma A Stolk, Matthew A Dixon, Christian Bottomley, Lamine Diawara,
Modelling the elimination of river blindness using long-term epidemiological and programmatic data from Mali and Senegal Martin Walker, Wilma A Stolk, Matthew A Dixon, Christian Bottomley, Lamine Diawara,
MAJOR ARTICLE. cost effectiveness; economic evaluation; ivermectin; onchocerciasis; treatment frequency.
 MAJOR ARTICLE Reaching the London Declaration on Neglected Tropical Diseases Goals for Onchocerciasis: An Economic Evaluation of Increasing the Frequency of Ivermectin Treatment in Africa Hugo C. Turner,
MAJOR ARTICLE Reaching the London Declaration on Neglected Tropical Diseases Goals for Onchocerciasis: An Economic Evaluation of Increasing the Frequency of Ivermectin Treatment in Africa Hugo C. Turner,
Is onchocerciasis elimination in Africa feasible by 2025: a perspective based on lessons learnt from the African control programmes
 Dadzie et al. Infectious Diseases of Poverty (2018) 7:63 https://doi.org/10.1186/s40249-018-0446-z OPINION Open Access Is onchocerciasis elimination in Africa feasible by 2025: a perspective based on lessons
Dadzie et al. Infectious Diseases of Poverty (2018) 7:63 https://doi.org/10.1186/s40249-018-0446-z OPINION Open Access Is onchocerciasis elimination in Africa feasible by 2025: a perspective based on lessons
Access to Safe Water - A way to Mitigating Onchocerciasis in Nigeria
 Access to Safe Water - A way to Mitigating Onchocerciasis in Nigeria Adebayo O. AJALA Social Sector Group, Social and Governance Policy Research Department Nigerian Institute of Social and Economic Research,
Access to Safe Water - A way to Mitigating Onchocerciasis in Nigeria Adebayo O. AJALA Social Sector Group, Social and Governance Policy Research Department Nigerian Institute of Social and Economic Research,
Guidelines for revising ivermectin treatment boundaries within the context of onchocerciasis elimination
 When and AFRICAN PROGRAMME FOR ONCHOCERCIASIS CONTROL World Health Organization Guidelines for revising ivermectin treatment boundaries within the context of onchocerciasis elimination AFRICAN PROGRAMME
When and AFRICAN PROGRAMME FOR ONCHOCERCIASIS CONTROL World Health Organization Guidelines for revising ivermectin treatment boundaries within the context of onchocerciasis elimination AFRICAN PROGRAMME
Research for control: the onchocerciasis experience*
 Tropical Medicine and International Health volume 9 no 2 pp 243 254 february 2004 Research for control: the onchocerciasis experience* Jan H. F. Remme Intervention Development and Implementation Research,
Tropical Medicine and International Health volume 9 no 2 pp 243 254 february 2004 Research for control: the onchocerciasis experience* Jan H. F. Remme Intervention Development and Implementation Research,
Projected number of people with onchocerciasisloiasis co-infection in Africa,
 Projected number of people with onchocerciasisloiasis co-infection in Africa, 1995-2025 Natalie Vinkeles Melchers, Afework H Tekle, Luc E Coffeng, Sébastien DS Pion, Honorat GM Zouré, Belén Pedrique, Michel
Projected number of people with onchocerciasisloiasis co-infection in Africa, 1995-2025 Natalie Vinkeles Melchers, Afework H Tekle, Luc E Coffeng, Sébastien DS Pion, Honorat GM Zouré, Belén Pedrique, Michel
THE GLOBAL BURDEN OF ONCHOCERCIASIS IN 1990
 1 THE GLOBAL BURDEN OF ONCHOCERCIASIS IN 1990 J.H.F. REMME 1 World Health Organization, Geneva, 2004 This paper documents the methods and data sources used for the estimation of the global burden of onchocerciasis
1 THE GLOBAL BURDEN OF ONCHOCERCIASIS IN 1990 J.H.F. REMME 1 World Health Organization, Geneva, 2004 This paper documents the methods and data sources used for the estimation of the global burden of onchocerciasis
Impact of five annual rounds of mass drug administration with ivermectin on onchocerciasis in Sierra Leone
 Koroma et al. Infectious Diseases of Poverty (2018) 7:30 https://doi.org/10.1186/s40249-018-0410-y RESEARCH ARTICLE Open Access Impact of five annual rounds of mass drug administration with ivermectin
Koroma et al. Infectious Diseases of Poverty (2018) 7:30 https://doi.org/10.1186/s40249-018-0410-y RESEARCH ARTICLE Open Access Impact of five annual rounds of mass drug administration with ivermectin
Prospectus Trans-Atlantic Product Development Partnership for a River Blindness Vaccine
 Prospectus Trans-Atlantic Product Development Partnership for a River Blindness Vaccine The London Declaration on Neglected Tropical Diseases of January 2012 called for sustained efforts to expand and
Prospectus Trans-Atlantic Product Development Partnership for a River Blindness Vaccine The London Declaration on Neglected Tropical Diseases of January 2012 called for sustained efforts to expand and
Filaria Journal. Open Access. Abstract
 Filaria Journal BioMed Central Review Advances and challenges in predicting the impact of lymphatic filariasis elimination programmes by mathematical modelling Wilma A Stolk*, Sake J de Vlas and J Dik
Filaria Journal BioMed Central Review Advances and challenges in predicting the impact of lymphatic filariasis elimination programmes by mathematical modelling Wilma A Stolk*, Sake J de Vlas and J Dik
Elimination of onchocerciasis from Africa: possible?
 Review Elimination of onchocerciasis from Africa: possible? Charles D. Mackenzie 1, Mamoun M. Homeida 2, Adrian D. Hopkins 3 and Joni C. Lawrence 3 1 Department of Pathobiology and Diagnostic Investigation,
Review Elimination of onchocerciasis from Africa: possible? Charles D. Mackenzie 1, Mamoun M. Homeida 2, Adrian D. Hopkins 3 and Joni C. Lawrence 3 1 Department of Pathobiology and Diagnostic Investigation,
BMC Medicine. Open Access. Abstract. BioMed Central
 BMC Medicine BioMed Central Research article Impact of long-term treatment of onchocerciasis with ivermectin in Ecuador: potential for elimination of infection Juan Carlos Vieira 1,2, Philip J Cooper*
BMC Medicine BioMed Central Research article Impact of long-term treatment of onchocerciasis with ivermectin in Ecuador: potential for elimination of infection Juan Carlos Vieira 1,2, Philip J Cooper*
International Journal of Current Research in Biosciences and Plant Biology ISSN: Volume 2 Number 8 (August-2015) pp
 pp") International Journal of Current Research in Biosciences and Plant Biology ISSN: 2349-8080 Volume 2 Number 8 (August-2015) pp. 38-42 www.ijcrbp.com Original Research Article Phytoscreening of Different
International Journal of Current Research in Biosciences and Plant Biology ISSN: 2349-8080 Volume 2 Number 8 (August-2015) pp. 38-42 www.ijcrbp.com Original Research Article Phytoscreening of Different
Accepted for Publication, Published online May 20, 2013; doi: /ajtmh
 Accepted for Publication, Published online May 20, 2013; doi:10.4269/ajtmh.13-0037. The latest version is at http://ajtmh.org/cgi/doi/10.4269/ajtmh.13-0037 In order to provide our readers with timely access
Accepted for Publication, Published online May 20, 2013; doi:10.4269/ajtmh.13-0037. The latest version is at http://ajtmh.org/cgi/doi/10.4269/ajtmh.13-0037 In order to provide our readers with timely access
Annual Highlights. The accomplishments of the Mectizan Donation Program in its 29th year
 2015 Annual Highlights The accomplishments of the Mectizan Donation Program in its 29th year 10 Years Building Research and Laboratory Capacity in Cameroon: The Center for Research on Filariasis and Other
2015 Annual Highlights The accomplishments of the Mectizan Donation Program in its 29th year 10 Years Building Research and Laboratory Capacity in Cameroon: The Center for Research on Filariasis and Other
Reproductive Status of Onchocerca volvulus after Ivermectin Treatment in an Ivermectin-Naïve and a Frequently Treated Population from Cameroon
 Reproductive Status of Onchocerca volvulus after Ivermectin Treatment in an Ivermectin-Naïve and a Frequently Treated Population from Cameroon Hugues C. Nana-Djeunga 1,2., Catherine Bourguinat 3.,Sébastien
Reproductive Status of Onchocerca volvulus after Ivermectin Treatment in an Ivermectin-Naïve and a Frequently Treated Population from Cameroon Hugues C. Nana-Djeunga 1,2., Catherine Bourguinat 3.,Sébastien
River Blindness: A Success Story under Threat?
 Neglected Diseases River Blindness: A Success Story under Threat? María-Gloria Basáñez *, Sébastien D. S. Pion, Thomas S. Churcher, Lutz P. Breitling, Mark P. Little, Michel Boussinesq accomplishments
Neglected Diseases River Blindness: A Success Story under Threat? María-Gloria Basáñez *, Sébastien D. S. Pion, Thomas S. Churcher, Lutz P. Breitling, Mark P. Little, Michel Boussinesq accomplishments
Filaria Journal. Open Access. Abstract. BioMed Central
 Filaria Journal BioMed Central Review Impact of ivermectin on onchocerciasis transmission: assessing the empirical evidence that repeated ivermectin mass treatments may lead to elimination/eradication
Filaria Journal BioMed Central Review Impact of ivermectin on onchocerciasis transmission: assessing the empirical evidence that repeated ivermectin mass treatments may lead to elimination/eradication
ONCHOCERCA INFECTION, ONCHOCERCOMATA, VISUAL ACUITY AND NUTRITIONAL STATUS IN CHILDREN IN AN ENDEMIC AREA OF SOUTH EASTERN NIGERIA.
 ONCHOCERCA INFECTION, ONCHOCERCOMATA, VISUAL ACUITY AND NUTRITIONAL STATUS IN CHILDREN IN AN ENDEMIC AREA OF SOUTH EASTERN NIGERIA. Abstract. The association between onchocerca infection, vision and nutritional
ONCHOCERCA INFECTION, ONCHOCERCOMATA, VISUAL ACUITY AND NUTRITIONAL STATUS IN CHILDREN IN AN ENDEMIC AREA OF SOUTH EASTERN NIGERIA. Abstract. The association between onchocerca infection, vision and nutritional
ONCHOCERCIASIS GUIDELINES FOR STOPPING MASS DRUG ADMINISTRATION AND VERIFYING ELIMINATION OF HUMAN ONCHOCERCIASIS CRITERIA AND PROCEDURES
 ONCHOCERCIASIS GUIDELINES FOR STOPPING MASS DRUG ADMINISTRATION AND VERIFYING ELIMINATION OF HUMAN ONCHOCERCIASIS CRITERIA AND PROCEDURES ONCHOCERCIASIS GUIDELINES FOR STOPPING MASS DRUG ADMINISTRATION
ONCHOCERCIASIS GUIDELINES FOR STOPPING MASS DRUG ADMINISTRATION AND VERIFYING ELIMINATION OF HUMAN ONCHOCERCIASIS CRITERIA AND PROCEDURES ONCHOCERCIASIS GUIDELINES FOR STOPPING MASS DRUG ADMINISTRATION
NTDs Slated for Elimination and Eradication
 NTDs Slated for Elimination and Eradication Institute of Medicine Forum on Microbial Threats The Causes and Impacts of Neglected Tropical and Zoonotic Diseases September 21-22, 2010 Washington, DC Donald
NTDs Slated for Elimination and Eradication Institute of Medicine Forum on Microbial Threats The Causes and Impacts of Neglected Tropical and Zoonotic Diseases September 21-22, 2010 Washington, DC Donald
Lecture 5: Dr. Jabar Etaby
 Lecture 5: Dr. Jabar Etaby 1 2 Onchocerca volvulus (Blinding filariasis; river blindness) Microfilaria of Onchocerca volvulus, from skin snip from a patient seen in Guatemala. Wet preparation 3 Some important
Lecture 5: Dr. Jabar Etaby 1 2 Onchocerca volvulus (Blinding filariasis; river blindness) Microfilaria of Onchocerca volvulus, from skin snip from a patient seen in Guatemala. Wet preparation 3 Some important
ONCHOCERCIASIS SEROSURVEILLANCE IN UGANDA
 This article is reprinted on the Carter Center s website with permission from the American Society of Tropical Medicine and Hygiene. Accepted for Publication, Published online December 16, 2013; doi:10.4269/ajtmh.13-0546.
This article is reprinted on the Carter Center s website with permission from the American Society of Tropical Medicine and Hygiene. Accepted for Publication, Published online December 16, 2013; doi:10.4269/ajtmh.13-0546.
Filaria Journal. Open Access. Abstract. BioMed Central
 Filaria Journal BioMed Central Research Combined Utilisation of Rapid Assessment Procedures for Loiasis (RAPLOA) and Onchocerciasis (REA) in Rain forest Villages of Cameroon Samuel Wanji* 1,2, Nicholas
Filaria Journal BioMed Central Research Combined Utilisation of Rapid Assessment Procedures for Loiasis (RAPLOA) and Onchocerciasis (REA) in Rain forest Villages of Cameroon Samuel Wanji* 1,2, Nicholas
Thank you for the opportunity to submit testimony on the Fiscal Year (FY) 2014 State
 2014 State") Drugs for Neglected Diseases initiative, North America Jennifer Katz, Policy Director March 2013 Testimony to the Subcommittee on State and Foreign Operations, Committee on Appropriations United States
Drugs for Neglected Diseases initiative, North America Jennifer Katz, Policy Director March 2013 Testimony to the Subcommittee on State and Foreign Operations, Committee on Appropriations United States
Controlling Onchocerciasis: The Nigerian Experience
 ISPUB.COM The Internet Journal of Parasitic Diseases Volume 4 Number 1 N Njepuome, P Ogbu-Pearce, C Okoronkwo, M Igbe Citation N Njepuome, P Ogbu-Pearce, C Okoronkwo, M Igbe.. The Internet Journal of Parasitic
ISPUB.COM The Internet Journal of Parasitic Diseases Volume 4 Number 1 N Njepuome, P Ogbu-Pearce, C Okoronkwo, M Igbe Citation N Njepuome, P Ogbu-Pearce, C Okoronkwo, M Igbe.. The Internet Journal of Parasitic
Factors affecting onchocerciasis transmission: lessons for infection control
 Publisher: Taylor & Francis Journal: Expert Review of Anti-infective Therapy DOI: 10.1080/14787210.2017.1286980 Factors affecting onchocerciasis transmission: lessons for infection control Robert A. Cheke
Publisher: Taylor & Francis Journal: Expert Review of Anti-infective Therapy DOI: 10.1080/14787210.2017.1286980 Factors affecting onchocerciasis transmission: lessons for infection control Robert A. Cheke
Investigations on the transmission potentials of Simulium damnosum and the risk of human Onchocerciasis in Kaduna metropolis, Kaduna State, Nigeria
 IJMBR 3 (2015) 1-5 ISSN 2053-180X Investigations on the transmission potentials of Simulium damnosum and the risk of human Onchocerciasis in Kaduna metropolis, Kaduna State, Nigeria Maikaje D. B.*, Dibal
IJMBR 3 (2015) 1-5 ISSN 2053-180X Investigations on the transmission potentials of Simulium damnosum and the risk of human Onchocerciasis in Kaduna metropolis, Kaduna State, Nigeria Maikaje D. B.*, Dibal
Analysis of age-dependent trends in Ov16 IgG4 seroprevalence to onchocerciasis
 Golden et al. Parasites & Vectors (2016) 9:338 DOI 10.1186/s13071-016-1623-1 RESEARCH Open Access Analysis of age-dependent trends in Ov16 IgG4 seroprevalence to onchocerciasis Allison Golden 1, Dunia
Golden et al. Parasites & Vectors (2016) 9:338 DOI 10.1186/s13071-016-1623-1 RESEARCH Open Access Analysis of age-dependent trends in Ov16 IgG4 seroprevalence to onchocerciasis Allison Golden 1, Dunia
The Schistosomiasis Control Initiative (SCI) Professor Alan Fenwick
 Professor Alan Fenwick") The Schistosomiasis Control Initiative (SCI) Professor Alan Fenwick Department of Infectious Disease Epidemiology School of Public Health Imperial College (St Mary s campus) Established in 2002 SCI assists
The Schistosomiasis Control Initiative (SCI) Professor Alan Fenwick Department of Infectious Disease Epidemiology School of Public Health Imperial College (St Mary s campus) Established in 2002 SCI assists
An appraisal of the neglected tropical diseases control program in Cameroon: the case of the national program against onchocerciasis
 Njim and Aminde BMC Public Health (2017) 17:103 DOI 10.1186/s12889-017-4037-x RESEARCH ARTICLE An appraisal of the neglected tropical diseases control program in Cameroon: the case of the national program
Njim and Aminde BMC Public Health (2017) 17:103 DOI 10.1186/s12889-017-4037-x RESEARCH ARTICLE An appraisal of the neglected tropical diseases control program in Cameroon: the case of the national program
Does onchocerciasis transmission take place in hypoendemic areas? A study in North Region of Cameroon
 Reprinted peer reviewed version with permission from the Journal of Tropical Medicine and International Health, volume 15 no 5 pp645 652 May 2010. For more information on the Carter Center s work to fight
Reprinted peer reviewed version with permission from the Journal of Tropical Medicine and International Health, volume 15 no 5 pp645 652 May 2010. For more information on the Carter Center s work to fight
MOXIDECTIN FOR ONCHOCERCIASIS ELIMINATION
 MOXIDECTIN FOR ONCHOCERCIASIS ELIMINATION Studies completed Studies in preparation Michel Mandro, Tony Ukety (investigators studies in DRC), Nicholas Opoku (investigator study in Ghana) C. Chesnais, J.
MOXIDECTIN FOR ONCHOCERCIASIS ELIMINATION Studies completed Studies in preparation Michel Mandro, Tony Ukety (investigators studies in DRC), Nicholas Opoku (investigator study in Ghana) C. Chesnais, J.
Downloaded from:
 O Hara, GA; Elliott, AM (2016) HIV and Helminths - Not All Worms Created Equal? Trends in parasitology. ISSN 1471-4922 DOI: https://doi.org/10.1016/j.pt.2016 Downloaded from: http://researchonline.lshtm.ac.uk/3327115/
O Hara, GA; Elliott, AM (2016) HIV and Helminths - Not All Worms Created Equal? Trends in parasitology. ISSN 1471-4922 DOI: https://doi.org/10.1016/j.pt.2016 Downloaded from: http://researchonline.lshtm.ac.uk/3327115/
Timeline of Carter Center Health Programs, 1982 to 2009
 1982 1985 1986 1991 1992 Timeline of Carter Center Health Programs, 1982 to 2009 is established by former U.S. President Jimmy Carter and his wife, Rosalynn, in partnership with Emory University. Groundbreaking
1982 1985 1986 1991 1992 Timeline of Carter Center Health Programs, 1982 to 2009 is established by former U.S. President Jimmy Carter and his wife, Rosalynn, in partnership with Emory University. Groundbreaking
Purushothaman Jambulingam 1, Swaminathan Subramanian 1*, S. J. de Vlas 2, Chellasamy Vinubala 1 and W. A. Stolk 2
 Jambulingam et al. Parasites & Vectors (2016) 9:501 DOI 10.1186/s13071-016-1768-y RESEARCH Mathematical modelling of lymphatic filariasis elimination programmes in India: required duration of mass drug
Jambulingam et al. Parasites & Vectors (2016) 9:501 DOI 10.1186/s13071-016-1768-y RESEARCH Mathematical modelling of lymphatic filariasis elimination programmes in India: required duration of mass drug
Community Directed Intervention for Onchocerciasis Control and Public Health Interventions
 Community Directed Intervention for Onchocerciasis Control and Public Health Interventions USF College of Public Health Tampa Florida, April 9, 2010 Dr. Boakye Boatin 11 University of Medical Sciences
Community Directed Intervention for Onchocerciasis Control and Public Health Interventions USF College of Public Health Tampa Florida, April 9, 2010 Dr. Boakye Boatin 11 University of Medical Sciences
Clinical Manifestations of Onchocerciasis in Imeri: an Endemic Community in Nigeria. *Tel:
 Clinical Manifestations of Onchocerciasis in Imeri: an Endemic Community in Nigeria * 1 OJ Afolabi, 2 CE Okaka, 1 MO Oniya 1 Department of Biology, Federal University of Technology Akure, Ondo State, Nigeria
Clinical Manifestations of Onchocerciasis in Imeri: an Endemic Community in Nigeria * 1 OJ Afolabi, 2 CE Okaka, 1 MO Oniya 1 Department of Biology, Federal University of Technology Akure, Ondo State, Nigeria
Research Article Transmission of Onchocerciasis in Wadelai Focus of Northwestern Uganda Has Been Interrupted and the Disease Eliminated
 Hindawi Publishing Corporation Journal of Parasitology Research Volume 2012, Article ID 748540, 7 pages doi:10.1155/2012/748540 Research Article Transmission of Onchocerciasis in Wadelai Focus of Northwestern
Hindawi Publishing Corporation Journal of Parasitology Research Volume 2012, Article ID 748540, 7 pages doi:10.1155/2012/748540 Research Article Transmission of Onchocerciasis in Wadelai Focus of Northwestern
Interruption of Onchocerca volvulus Transmission in the Abu Hamed Focus, Sudan
 Accepted for Publication, Published online May 20, 2013; doi:10.4269/ajtmh.13-0112. The latest version is at http://ajtmh.org/cgi/doi/10.4269/ajtmh.13-0112 In order to provide our readers with timely access
Accepted for Publication, Published online May 20, 2013; doi:10.4269/ajtmh.13-0112. The latest version is at http://ajtmh.org/cgi/doi/10.4269/ajtmh.13-0112 In order to provide our readers with timely access
Downloaded from:
 Koala, L; Nikiema, A; Post, RJ; Par, AB; Kafando, CM; Drabo, F; Traor, S (2016) RECRUDESCENCE OF ONCHOCERCIASIS IN THE COMO VALLEY IN SOUTHWEST BURKINA FASO. Acta tropica, 166. pp. 96-105. ISSN 0001-706X
Koala, L; Nikiema, A; Post, RJ; Par, AB; Kafando, CM; Drabo, F; Traor, S (2016) RECRUDESCENCE OF ONCHOCERCIASIS IN THE COMO VALLEY IN SOUTHWEST BURKINA FASO. Acta tropica, 166. pp. 96-105. ISSN 0001-706X
Downloaded from:
 Ejere, HO; Schwartz, E; Wormald, R; Evans, JR (2012) Ivermectin for onchocercal eye disease (river blindness). Cochrane Database Syst Rev, 8. CD002219. ISSN 1469-493X DOI: https://doi.org/10.1002/14651858.cd002219.pub2
Ejere, HO; Schwartz, E; Wormald, R; Evans, JR (2012) Ivermectin for onchocercal eye disease (river blindness). Cochrane Database Syst Rev, 8. CD002219. ISSN 1469-493X DOI: https://doi.org/10.1002/14651858.cd002219.pub2
The impact of density-dependent processes on the eradicability of parasitic diseases
 The impact of density-dependent processes on the eradicability of parasitic diseases Hans Peter Duerr Martin Eichner Klaus Dietz Department of Medical Biometry University of Tübingen Oberwolfach 2004 1/12
The impact of density-dependent processes on the eradicability of parasitic diseases Hans Peter Duerr Martin Eichner Klaus Dietz Department of Medical Biometry University of Tübingen Oberwolfach 2004 1/12
From river blindness control to elimination: bridge over troubled water
 Colebunders et al. Infectious Diseases of Poverty (2018) 7:21 https://doi.org/10.1186/s40249-018-0406-7 OPINION From river blindness control to elimination: bridge over troubled water Open Access Robert
Colebunders et al. Infectious Diseases of Poverty (2018) 7:21 https://doi.org/10.1186/s40249-018-0406-7 OPINION From river blindness control to elimination: bridge over troubled water Open Access Robert
Nkiru A. Kamalu 1, Felicia E. Uwakwe 2 1. INTRODUCTION
 International Letters of Natural Sciences Online: 2014-07-23 ISSN: 2300-9675, Vol. 20, pp 139-150 doi:10.18052/www.scipress.com/ilns.20.139 2014 SciPress Ltd., Switzerland Evaluation of different Onchocerciass
International Letters of Natural Sciences Online: 2014-07-23 ISSN: 2300-9675, Vol. 20, pp 139-150 doi:10.18052/www.scipress.com/ilns.20.139 2014 SciPress Ltd., Switzerland Evaluation of different Onchocerciass
Overview of the Malaria Vaccine Implementation Programme (MVIP) Prof. Fred Were SAGE meeting 17 April, 2018
 Prof. Fred Were SAGE meeting 17 April, 2018") Overview of the Malaria Vaccine Implementation Programme (MVIP) Prof. Fred Were SAGE meeting 17 April, 2018 1 Objectives Brief review Background EMA positive opinion and WHO recommendations Funding Description
Overview of the Malaria Vaccine Implementation Programme (MVIP) Prof. Fred Were SAGE meeting 17 April, 2018 1 Objectives Brief review Background EMA positive opinion and WHO recommendations Funding Description
Syllabus. Mathematical Modeling of Infectious diseases
 Syllabus Mathematical Modeling of Infectious diseases - 2009 Credit: 3 credits Faculty: Annelies Van Rie Teaching Assistant for computer practicum: Sarah Radke Time: Spring 2009, Monday, 1 3:50 PM Purpose
Syllabus Mathematical Modeling of Infectious diseases - 2009 Credit: 3 credits Faculty: Annelies Van Rie Teaching Assistant for computer practicum: Sarah Radke Time: Spring 2009, Monday, 1 3:50 PM Purpose
*Corresponding author:
 American Journal of Public Health Research, 2018, Vol. 6, No. 2, 26-30 Available online at http://pubs.sciepub.com/ajphr/6/2/1 Science and Education Publishing DOI:10.12691/ajphr-6-2-1 Entomological Evaluation
American Journal of Public Health Research, 2018, Vol. 6, No. 2, 26-30 Available online at http://pubs.sciepub.com/ajphr/6/2/1 Science and Education Publishing DOI:10.12691/ajphr-6-2-1 Entomological Evaluation
MectizanTM Program Notes
 MectizanTM Program Notes C e l e b r a t i n g o u r 1 7 t h y e a r Issue 34 Mectizan Donation Program 2004 Controlling River Blindness: Achievements of a 15-Year Public-Private Partnership On 14 May
MectizanTM Program Notes C e l e b r a t i n g o u r 1 7 t h y e a r Issue 34 Mectizan Donation Program 2004 Controlling River Blindness: Achievements of a 15-Year Public-Private Partnership On 14 May
Analysis of age-dependent trends in Ov16 IgG4 seroprevalence to onchocerciasis
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 Analysis of age-dependent trends in Ov16 IgG4 seroprevalence to onchocerciasis Allison Golden Diagnostics Global
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 Analysis of age-dependent trends in Ov16 IgG4 seroprevalence to onchocerciasis Allison Golden Diagnostics Global
Innovation, Access and Delivery for Universal Health Coverage
 A side event at the UHC Forum Co-hosted by UNDP and the GHIT Fund Tokyo, Japan 12 December 2017 Innovation, Access and Delivery for Universal Health Coverage From Innovation & Inequality, a UNDP-supported
A side event at the UHC Forum Co-hosted by UNDP and the GHIT Fund Tokyo, Japan 12 December 2017 Innovation, Access and Delivery for Universal Health Coverage From Innovation & Inequality, a UNDP-supported
Measles vaccine: a 27-year follow-up.
 Measles vaccine: a 27-year follow-up. Item type Authors Article Ramsay, M E; Moffatt, D; O'Connor, M Citation Measles vaccine: a 27-year follow-up. 1994, 112 (2):409-12 Epidemiol. Infect. Journal Rights
Measles vaccine: a 27-year follow-up. Item type Authors Article Ramsay, M E; Moffatt, D; O'Connor, M Citation Measles vaccine: a 27-year follow-up. 1994, 112 (2):409-12 Epidemiol. Infect. Journal Rights
Public Health Analysis of Manifestation of Onchocerciasis in Rural Nigeria
 Public Health Analysis of Manifestation of Onchocerciasis in Rural Nigeria Nkeiru A. Kamalu 1, Jacinta A. Opara 2, Felicia E. Uwakwe 3 1 Department of Animal and Environmental Biology, Imo State University,
Public Health Analysis of Manifestation of Onchocerciasis in Rural Nigeria Nkeiru A. Kamalu 1, Jacinta A. Opara 2, Felicia E. Uwakwe 3 1 Department of Animal and Environmental Biology, Imo State University,
GOAL 2: ACHIEVE RUBELLA AND CRS ELIMINATION. (indicator G2.2) Highlights
 Highlights") GOAL 2: ACHIEVE RUBELLA AND CRS ELIMINATION (indicator G2.2) Highlights As of December 2014, 140 Member States had introduced rubella vaccines; coverage, however, varies from 12% to 94% depending on region.
GOAL 2: ACHIEVE RUBELLA AND CRS ELIMINATION (indicator G2.2) Highlights As of December 2014, 140 Member States had introduced rubella vaccines; coverage, however, varies from 12% to 94% depending on region.
more than 6 million people at risk of contracting one or more diseases
 NTDs in Togo Neglected tropical diseases (NTDs) affect all 40 districts in Togo, putting more than 6 million people at risk of contracting one or more diseases. NTDs are debilitating and disproportionately
NTDs in Togo Neglected tropical diseases (NTDs) affect all 40 districts in Togo, putting more than 6 million people at risk of contracting one or more diseases. NTDs are debilitating and disproportionately
Wanji et al. Parasites & Vectors (2015) 8:202 DOI /s
 8:202 DOI /s") Wanji et al. Parasites & Vectors (2015) 8:202 DOI 10.1186/s13071-015-0817-2 RESEARCH Open Access Situation analysis of parasitological and entomological indices of onchocerciasis transmission in three
Wanji et al. Parasites & Vectors (2015) 8:202 DOI 10.1186/s13071-015-0817-2 RESEARCH Open Access Situation analysis of parasitological and entomological indices of onchocerciasis transmission in three
Pearce, N (2016) Analysis of matched case-control studies. BMJ (Clinical research ed), 352. i969. ISSN DOI: https://doi.org/ /bmj.
 Analysis of matched case-control studies. BMJ (Clinical research ed), 352. i969. ISSN DOI: https://doi.org/ /bmj.") Pearce, N (2016) Analysis of matched case-control studies. BMJ (Clinical research ed), 352. i969. ISSN 0959-8138 DOI: https://doi.org/10.1136/bmj.i969 Downloaded from: http://researchonline.lshtm.ac.uk/2534120/
Pearce, N (2016) Analysis of matched case-control studies. BMJ (Clinical research ed), 352. i969. ISSN 0959-8138 DOI: https://doi.org/10.1136/bmj.i969 Downloaded from: http://researchonline.lshtm.ac.uk/2534120/
Acta Tropica 120S (2011) S81 S90. Contents lists available at ScienceDirect. Acta Tropica. journa l h o me pa g e:
 S81 S90. Contents lists available at ScienceDirect. Acta Tropica. journa l h o me pa g e:") Acta Tropica 120S (2011) S81 S90 Contents lists available at ScienceDirect Acta Tropica journa l h o me pa g e: www.elsevier.com/locate/actatropica Integrated rapid mapping of onchocerciasis and loiasis
Acta Tropica 120S (2011) S81 S90 Contents lists available at ScienceDirect Acta Tropica journa l h o me pa g e: www.elsevier.com/locate/actatropica Integrated rapid mapping of onchocerciasis and loiasis
Estimating TB burden. Philippe Glaziou World Health Organization Accra, Ghana
 Estimating TB burden Philippe Glaziou World Health Organization Accra, Ghana Outline Basic facts about TB epidemiology What should we expect with regards TB burden over time? Main indicators of TB disease
Estimating TB burden Philippe Glaziou World Health Organization Accra, Ghana Outline Basic facts about TB epidemiology What should we expect with regards TB burden over time? Main indicators of TB disease
Luc E. Coffeng 1*, Roel Bakker 1, Antonio Montresor 2 and Sake J. de Vlas 1
 Coffeng et al. Parasites & Vectors (2015) 8:541 DOI 10.1186/s13071-015-1151-4 RESEARCH Open Access Feasibility of controlling hookworm infection through preventive chemotherapy: a simulation study using
Coffeng et al. Parasites & Vectors (2015) 8:541 DOI 10.1186/s13071-015-1151-4 RESEARCH Open Access Feasibility of controlling hookworm infection through preventive chemotherapy: a simulation study using
RAM U S. D E P A R T M E N T O F H E A L T H. E D U C A T IO N. AND W E LF A R E. J u l y 1970
 v u L.u n r. i. v, J u l y 1970 n u n w j y q 6/70 S2.2 J D MILLAR, MO, ACTING 01 RECTOR STATE AND COMMUNITY SERVICES D IV ISIO N BLOG B, ROOM 207 RAM I. C U R R E N T S M A L L P O X M O R B I D I T Y
v u L.u n r. i. v, J u l y 1970 n u n w j y q 6/70 S2.2 J D MILLAR, MO, ACTING 01 RECTOR STATE AND COMMUNITY SERVICES D IV ISIO N BLOG B, ROOM 207 RAM I. C U R R E N T S M A L L P O X M O R B I D I T Y
Validation of the rapid assessment procedure for loiasis (RAPLOA) in the democratic republic of Congo
 in the democratic republic of Congo") RESEARCH Open Access Validation of the rapid assessment procedure for loiasis (RAPLOA) in the democratic republic of Congo Samuel Wanji 1,2*, Dowo O Akotshi 3, Maurice N Mutro 4, Floribert Tepage 5, Tony
RESEARCH Open Access Validation of the rapid assessment procedure for loiasis (RAPLOA) in the democratic republic of Congo Samuel Wanji 1,2*, Dowo O Akotshi 3, Maurice N Mutro 4, Floribert Tepage 5, Tony
PARASITOLOGY CASE HISTORY #13 (BLOOD PARASITES) (Lynne S. Garcia)
 (Lynne S. Garcia)") PARASITOLOGY CASE HISTORY #13 (BLOOD PARASITES) (Lynne S. Garcia) An epidemiologic survey was undertaken in a small town in Myanmar (Burma) endemic for lymphatic filariasis. Blood specimens were collected
PARASITOLOGY CASE HISTORY #13 (BLOOD PARASITES) (Lynne S. Garcia) An epidemiologic survey was undertaken in a small town in Myanmar (Burma) endemic for lymphatic filariasis. Blood specimens were collected
MASS TREATMENT COVERAGE FOR NTDS Somalia and neglected tropical diseases
 MASS TREATMENT COVERAGE FOR NTDS - 2016 Somalia and neglected tropical diseases Neglected tropical diseases Neglected tropical diseases are a group of preventable and treatable diseases that affect 1.5
MASS TREATMENT COVERAGE FOR NTDS - 2016 Somalia and neglected tropical diseases Neglected tropical diseases Neglected tropical diseases are a group of preventable and treatable diseases that affect 1.5
Global reductions in measles mortality and the risk of measles resurgence
 Global reductions in measles mortality 2000 2008 and the risk of measles resurgence Measles is one of the most contagious human diseases. In 1980 before the use of measles vaccine was widespread, there
Global reductions in measles mortality 2000 2008 and the risk of measles resurgence Measles is one of the most contagious human diseases. In 1980 before the use of measles vaccine was widespread, there
Trends in HIV prevalence and incidence sex ratios in ALPHA demographic surveillance sites,
 Trends in HIV prevalence and incidence sex ratios in ALPHA demographic surveillance sites, 1990 2010 Zaba B 1, Calvert C 1, Marston M 1, Isingo R 2, Nakiyingi Miiro J 3, Lutalo T 4, Crampin A 1,5, Nyamukapa
Trends in HIV prevalence and incidence sex ratios in ALPHA demographic surveillance sites, 1990 2010 Zaba B 1, Calvert C 1, Marston M 1, Isingo R 2, Nakiyingi Miiro J 3, Lutalo T 4, Crampin A 1,5, Nyamukapa
Technical Note 1 The Epidemiology of Mosquito-borne Diseases Prepared by Dr L. Molineaux
 Technical Note 1 The Epidemiology of Mosquito-borne Diseases Prepared by Dr L. Molineaux 1 Introduction Epidemiology is the science that describes and explains the distribution of disease in human populations:
Technical Note 1 The Epidemiology of Mosquito-borne Diseases Prepared by Dr L. Molineaux 1 Introduction Epidemiology is the science that describes and explains the distribution of disease in human populations:
POLIOMYELITIS ERADICATION: PROGRESS REPORT. Information Document CONTENTS BACKGROUND PROGRESS MADE NEXT STEPS... 12
 5 August 9 REGIONAL COMMITTEE FOR AFRICA ORIGINAL: ENGLISH Fifty-ninth session Kigali, Republic of Rwanda, August 4 September 9 POLIOMYELITIS ERADICATION: PROGRESS REPORT Information Document CONTENTS
5 August 9 REGIONAL COMMITTEE FOR AFRICA ORIGINAL: ENGLISH Fifty-ninth session Kigali, Republic of Rwanda, August 4 September 9 POLIOMYELITIS ERADICATION: PROGRESS REPORT Information Document CONTENTS
ANNEX Page. AFR/RC61/11 4 July 2011 ORIGINAL: ENGLISH REGIONAL COMMITTEE FOR AFRICA
 4 July 2011 REGIONAL COMMITTEE FOR AFRICA ORIGINAL: ENGLISH Sixty-first session Yamoussoukro, Côte d Ivoire, 29 August 2 September 2011 Provisional agenda item 16 PROGRESS REPORT ON POLIOMYELITIS ERADICATION
4 July 2011 REGIONAL COMMITTEE FOR AFRICA ORIGINAL: ENGLISH Sixty-first session Yamoussoukro, Côte d Ivoire, 29 August 2 September 2011 Provisional agenda item 16 PROGRESS REPORT ON POLIOMYELITIS ERADICATION
GUINEA-WORM DISEASE: COUNTDOWN TO ERADICATION
 GUINEA-WORM DISEASE: COUNTDOWN TO ERADICATION GUINEA-WORM DISEASE (DRACUNCULIASIS) Guinea-worm disease, also known as dracunculiasis, is on the verge of eradication. The World Health Organization (WHO)
GUINEA-WORM DISEASE: COUNTDOWN TO ERADICATION GUINEA-WORM DISEASE (DRACUNCULIASIS) Guinea-worm disease, also known as dracunculiasis, is on the verge of eradication. The World Health Organization (WHO)
NTDs: update on the progress. Department of Control of Neglected Tropical Diseases
 NTDs: update on the progress Department of Control of Neglected Tropical Diseases WHO Department of control of Neglected Tropical Diseases Two main groups of diseases: IDM (Innovative and Intensified Diseases
NTDs: update on the progress Department of Control of Neglected Tropical Diseases WHO Department of control of Neglected Tropical Diseases Two main groups of diseases: IDM (Innovative and Intensified Diseases
SUPPLEMENTARY APPENDICES FOR ONLINE PUBLICATION. Supplement to: All-Cause Mortality Reductions from. Measles Catch-Up Campaigns in Africa
 SUPPLEMENTARY APPENDICES FOR ONLINE PUBLICATION Supplement to: All-Cause Mortality Reductions from Measles Catch-Up Campaigns in Africa (by Ariel BenYishay and Keith Kranker) 1 APPENDIX A: DATA DHS survey
SUPPLEMENTARY APPENDICES FOR ONLINE PUBLICATION Supplement to: All-Cause Mortality Reductions from Measles Catch-Up Campaigns in Africa (by Ariel BenYishay and Keith Kranker) 1 APPENDIX A: DATA DHS survey
Newborn Screening for Sickle Cell Disease in Ghana Update
 National Programme of Newborn Screening for Sickle Cell Disease Newborn Screening for Sickle Cell Disease in Ghana ---------- Update Prof. Kwaku Ohene-Frempong, MD Children s Hospital of Philadelphia University
National Programme of Newborn Screening for Sickle Cell Disease Newborn Screening for Sickle Cell Disease in Ghana ---------- Update Prof. Kwaku Ohene-Frempong, MD Children s Hospital of Philadelphia University
Evidence of suppression of onchocerciasis transmission in the Venezuelan Amazonian focus
 Botto et al. Parasites & Vectors (216) 9:4 DOI 1.1186/s1371-16-1313-z RESEARCH Open Access Evidence of suppression of onchocerciasis transmission in the Venezuelan Amazonian focus Carlos Botto 1, María-Gloria
Botto et al. Parasites & Vectors (216) 9:4 DOI 1.1186/s1371-16-1313-z RESEARCH Open Access Evidence of suppression of onchocerciasis transmission in the Venezuelan Amazonian focus Carlos Botto 1, María-Gloria
Partners. hygiene. progress. END in Africa & Burkina Faso. community. support health. e e e e e e e e e e e e e e e. endinafrica.
 thrive control awareness care hygiene prevention assessment treatment access progress Partners on NTDs END in Africa & Burkina Faso community capacity-building support health e e e e e e e e e e e e e
thrive control awareness care hygiene prevention assessment treatment access progress Partners on NTDs END in Africa & Burkina Faso community capacity-building support health e e e e e e e e e e e e e
Effects of Ivermectin therapy on the sperm functions of Nigerian onchocerciasis patients
 Available online at www.scholarsresearchlibrary.com Scholars Research Library Archives of Applied Science Research, 2011, 3 (3):533-543 (http://scholarsresearchlibrary.com/archive.html) ISSN 0975-508X
Available online at www.scholarsresearchlibrary.com Scholars Research Library Archives of Applied Science Research, 2011, 3 (3):533-543 (http://scholarsresearchlibrary.com/archive.html) ISSN 0975-508X
Roadmaps as a Vehicle for Addressing Large- Scale Public Health Challenges: Lessons from the Malaria Vaccine Technology Roadmap
 Background to development of vaccine roadmaps, to include priority areas for research, product development, capacities, and policy and commercialization Roadmaps as a Vehicle for Addressing Large- Scale
Background to development of vaccine roadmaps, to include priority areas for research, product development, capacities, and policy and commercialization Roadmaps as a Vehicle for Addressing Large- Scale
Analytical evaluation of Malaria Research Papers in MEDLINE & SCI during the period of &
 Panigrahi, Mukherjee and Srivastava 1 Analytical evaluation of Malaria Research Papers in & during the period of 1986-9 & 21-5. Panigrahi BK *, Mukherjee T and Srivastava D 28 July 28 Abstract: Vector-borne
Panigrahi, Mukherjee and Srivastava 1 Analytical evaluation of Malaria Research Papers in & during the period of 1986-9 & 21-5. Panigrahi BK *, Mukherjee T and Srivastava D 28 July 28 Abstract: Vector-borne
Wuchereria Morphology 10 cm 250 : m
 Wucheria bancrofti Brugia malayi Lymphatic filariasis Lymphatic Filariasis 119 million infected Elephantiasis Manifestation of lymphatic filariasis Morphology I Adult: White and thread-like. Two rings
Wucheria bancrofti Brugia malayi Lymphatic filariasis Lymphatic Filariasis 119 million infected Elephantiasis Manifestation of lymphatic filariasis Morphology I Adult: White and thread-like. Two rings
Of Mice, Cattle, and Humans: The Immunology and Treatment of River Blindness
 Review Of Mice, Cattle, and Humans: The Immunology and Treatment of River Blindness Judith E. Allen 1, Ohene Adjei 2, Odile Bain 3, Achim Hoerauf 4, Wolfgang H. Hoffmann 5, Benjamin L. Makepeace 6, Hartwig
Review Of Mice, Cattle, and Humans: The Immunology and Treatment of River Blindness Judith E. Allen 1, Ohene Adjei 2, Odile Bain 3, Achim Hoerauf 4, Wolfgang H. Hoffmann 5, Benjamin L. Makepeace 6, Hartwig
Impact of repeated ivermectin treatments against onchocerciasis on the transmission of loiasis: an entomologic evaluation in central Cameroon
 Kouam et al. Parasites & Vectors 2013, 6:283 RESEARCH Open Access Impact of repeated ivermectin treatments against onchocerciasis on the transmission of loiasis: an entomologic evaluation in central Cameroon
Kouam et al. Parasites & Vectors 2013, 6:283 RESEARCH Open Access Impact of repeated ivermectin treatments against onchocerciasis on the transmission of loiasis: an entomologic evaluation in central Cameroon
Summary of the Twelfth Meeting of the ITFDE (II) May 6, 2008
 May 6, 2008") Summary of the Twelfth Meeting of the ITFDE (II) May 6, 2008 The Twelfth Meeting of the International Task Force for Disease Eradication (ITFDE) was convened at The Carter Center from 8:30am to 4:00pm
Summary of the Twelfth Meeting of the ITFDE (II) May 6, 2008 The Twelfth Meeting of the International Task Force for Disease Eradication (ITFDE) was convened at The Carter Center from 8:30am to 4:00pm
Glaucoma screening. A global perspective. Contents. Introduction
 Glaucoma screening A global perspective Introduction Rather than referring to a single condition, glaucoma is a term used to describe a range of disorders affecting the optic nerve. This, combined with
Glaucoma screening A global perspective Introduction Rather than referring to a single condition, glaucoma is a term used to describe a range of disorders affecting the optic nerve. This, combined with
25 million Ghanaians are at risk of contracting one or more diseases
 NTDs in Ghana Neglected tropical diseases (NTDs) affect all 10 regions of Ghana, and an estimated 25 million Ghanaians are at risk of contracting one or more diseases. NTDs are debilitating and disproportionately
NTDs in Ghana Neglected tropical diseases (NTDs) affect all 10 regions of Ghana, and an estimated 25 million Ghanaians are at risk of contracting one or more diseases. NTDs are debilitating and disproportionately
Pharmacologyonline 1: (2011) ewsletter Gaware et al. O CHOCERCIASIS: A OVERVIEW
 ewsletter Gaware et al. O CHOCERCIASIS: A OVERVIEW") O CHOCERCIASIS: A OVERVIEW Vinayak M Gaware *1, Kiran B Dhamak 1, Kiran B Kotade 3, Ramdas T Dolas 2, Sachin B Somwanshi 2, Vikrant K Nikam 2, Atul N Khadse 1 1. Department of Pharmaceutical Chemistry,
O CHOCERCIASIS: A OVERVIEW Vinayak M Gaware *1, Kiran B Dhamak 1, Kiran B Kotade 3, Ramdas T Dolas 2, Sachin B Somwanshi 2, Vikrant K Nikam 2, Atul N Khadse 1 1. Department of Pharmaceutical Chemistry,
Measuring the path toward malaria elimination
 Measuring the path toward malaria elimination Rigorous and achievable targets and milestones can be developed from standard malaria surveillance data. By Thomas S. Churcher, 1 Justin M. Cohen, 2 Joseph
Measuring the path toward malaria elimination Rigorous and achievable targets and milestones can be developed from standard malaria surveillance data. By Thomas S. Churcher, 1 Justin M. Cohen, 2 Joseph
BIOSTATISTICAL METHODS AND RESEARCH DESIGNS. Xihong Lin Department of Biostatistics, University of Michigan, Ann Arbor, MI, USA
 BIOSTATISTICAL METHODS AND RESEARCH DESIGNS Xihong Lin Department of Biostatistics, University of Michigan, Ann Arbor, MI, USA Keywords: Case-control study, Cohort study, Cross-Sectional Study, Generalized
BIOSTATISTICAL METHODS AND RESEARCH DESIGNS Xihong Lin Department of Biostatistics, University of Michigan, Ann Arbor, MI, USA Keywords: Case-control study, Cohort study, Cross-Sectional Study, Generalized
Average Household Size and the Eradication of Malaria
 For General Release Summary of: Average Household Size and the Eradication of Malaria By Lena Huldén, Ross McKitrick and Larry Huldén Journal of the Royal Statistical Society Series A, October 2013 Online
For General Release Summary of: Average Household Size and the Eradication of Malaria By Lena Huldén, Ross McKitrick and Larry Huldén Journal of the Royal Statistical Society Series A, October 2013 Online
Advances in Biomedicine and Pharmacy (An International Journal of Biomedicine, Natural Products and Pharmacy)
") ISSN: 2313-7479 Adv. Biomed. Pharma. 3:3 (2016) 166-172 Advances in Biomedicine and Pharmacy (An International Journal of Biomedicine, Natural Products and Pharmacy) Case Study Prevalence of Onchocerciasis
ISSN: 2313-7479 Adv. Biomed. Pharma. 3:3 (2016) 166-172 Advances in Biomedicine and Pharmacy (An International Journal of Biomedicine, Natural Products and Pharmacy) Case Study Prevalence of Onchocerciasis
GABON. Neglected tropical disease treatment report profile for mass treatment of NTDs
 GABON Neglected tropical disease treatment report 2017 1 2017 profile for mass treatment of NTDs NEGLECTED TROPICAL DISEASES Neglected tropical diseases (NTDs) are a group of preventable and treatable
GABON Neglected tropical disease treatment report 2017 1 2017 profile for mass treatment of NTDs NEGLECTED TROPICAL DISEASES Neglected tropical diseases (NTDs) are a group of preventable and treatable
A Mathematical Model of Dracunculiasis Epidemic and Eradication
 IOSR Journal of Mathematics (IOSR-JM) e-issn: 2278-5728, p-issn:2319-765x. Volume 8, Issue 6 (Nov. Dec. 2013), PP 48-56 A Mathematical Model of Dracunculiasis Epidemic and Eradication Matthew O. Adewole
IOSR Journal of Mathematics (IOSR-JM) e-issn: 2278-5728, p-issn:2319-765x. Volume 8, Issue 6 (Nov. Dec. 2013), PP 48-56 A Mathematical Model of Dracunculiasis Epidemic and Eradication Matthew O. Adewole
Onchocerciasis in Ecuador: ocular findings in Onchocerca volvulus infected individuals
 British Journal of Ophthalmology 1995; 79: 157-162 Onchocerciasis Control Programme, Hospital Vozandes, Quito, Ecuador P J Cooper R Proaflo C Beltran M Anselmi R H Guderian Correspondence to: Dr R H Guderian.
British Journal of Ophthalmology 1995; 79: 157-162 Onchocerciasis Control Programme, Hospital Vozandes, Quito, Ecuador P J Cooper R Proaflo C Beltran M Anselmi R H Guderian Correspondence to: Dr R H Guderian.
DOWNLOAD OR READ : TROPICAL INFECTIOUS DISEASES SECOND EDITION PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : TROPICAL INFECTIOUS DISEASES SECOND EDITION PDF EBOOK EPUB MOBI Page 1 Page 2 tropical infectious diseases second edition tropical infectious diseases second pdf tropical infectious
DOWNLOAD OR READ : TROPICAL INFECTIOUS DISEASES SECOND EDITION PDF EBOOK EPUB MOBI Page 1 Page 2 tropical infectious diseases second edition tropical infectious diseases second pdf tropical infectious
Integrating NTD drug packages into a Child Nutrition Campaign
 Integrating NTD drug packages into a Child Nutrition Campaign Achille Kabore, MD MPH Senior Technical Advisor NTD Control Program RTI International Washington, DC May 4 th 2011 Overview of the Neglected
Integrating NTD drug packages into a Child Nutrition Campaign Achille Kabore, MD MPH Senior Technical Advisor NTD Control Program RTI International Washington, DC May 4 th 2011 Overview of the Neglected
Efficacy of three-week oxytetracycline or rifampicin monotherapy compared with a
 AAC Accepts, published online ahead of print on 18 November 2013 Antimicrob. Agents Chemother. doi:10.1128/aac.01995-13 Copyright 2013, American Society for Microbiology. All Rights Reserved. 1 2 Efficacy
AAC Accepts, published online ahead of print on 18 November 2013 Antimicrob. Agents Chemother. doi:10.1128/aac.01995-13 Copyright 2013, American Society for Microbiology. All Rights Reserved. 1 2 Efficacy
Analysis of the demand for a malaria vaccine: outcome of a consultative study in eight countries
 Briefing Document: National decision-making framework for malaria vaccines Analysis of the demand for a malaria vaccine: outcome of a consultative study in eight countries This is one of seven briefing
Briefing Document: National decision-making framework for malaria vaccines Analysis of the demand for a malaria vaccine: outcome of a consultative study in eight countries This is one of seven briefing
Articles. Funding GlaxoSmithKline, Bill & Melinda Gates Foundation, Partnership for Child Development, and Wellcome Trust.
 Cost-effectiveness of scaling up mass drug administration for the control of soil-transmitted helminths: a comparison of cost function and constant costs analyses Hugo C Turner, James E Truscott, Fiona
Cost-effectiveness of scaling up mass drug administration for the control of soil-transmitted helminths: a comparison of cost function and constant costs analyses Hugo C Turner, James E Truscott, Fiona
Hugo C Turner, James E Truscott, Fiona M Fleming, T Déirdre Hollingsworth, Simon J Brooker, Roy M Anderson
 Cost-effectiveness of scaling up mass drug administration for the control of soil-transmitted helminths: a comparison of cost function and constant costs analyses Hugo C Turner, James E Truscott, Fiona
Cost-effectiveness of scaling up mass drug administration for the control of soil-transmitted helminths: a comparison of cost function and constant costs analyses Hugo C Turner, James E Truscott, Fiona