Accepted for Publication, Published online October 26, 2015; doi: /ajtmh
|
|
|
- Mervyn Mitchell
- 6 years ago
- Views:
Transcription
1 Accepted for Publication, Published online October 26, 2015; doi: /ajtmh The latest version is at In order to provide our readers with timely access to new content, papers accepted by the American Journal of Tropical Medicine and Hygiene are posted online ahead of print publication. Papers that have been accepted for publication are peer-reviewed and copy edited but do not incorporate all corrections or constitute the final versions that will appear in the Journal. Final, corrected papers will be published online concurrent with the release of the print issue. RICHARDS AND OTHERS ONE HUNDRED YEARS AFTER ITS DISCOVERY IN GUATEMALA BY RODOLFO ROBLES, ONCHOCERCA VOLVULUS HAS BEEN ELIMINATED FROM THE CENTRAL ENDEMIC ZONE One Hundred Years After Its Discovery in Guatemala by Rodolfo Robles, Onchocerca volvulus Transmission Has Been Eliminated from the Central Endemic Zone Frank Richards Jr.,* Nidia Rizzo, Carlos Enrique Diaz Espinoza, Zoraida Morales Monroy, Carol Guillermina Crovella Valdez, Renata Mendizabal de Cabrera, Oscar de Leon, Guillermo Zea- Flores, Mauricio Sauerbrey, Alba Lucia Morales, Dalila Rios, Thomas R. Unnasch, Hassan K. Hassan, Robert Klein, Mark Eberhard, Ed Cupp, and Alfredo Domínguez River Blindness Elimination Program, The Carter Center, Atlanta, Georgia; Centro de Estudios en Salud of the Universidad del Valle de Guatemala (UVG), Guatemala City, Guatemala; Ministerio de Salud Pública y Asistencia Social, Guatemala City, Guatemala; Onchocerciasis Elimination Program for the Americas (OEPA), The Carter Center, Guatemala City, Guatemala; Global Health Infectious Disease Program, Department of Global Health, University of South Florida, Tampa, Florida; Division of Parasitic Diseases and Malaria (formerly), Centers for Disease Control and Prevention, Atlanta, Georgia; Division of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, Georgia; Department of Entomology and Plant Pathology, Auburn University, Auburn, Alabama; Onchocerciasis Elimination Program for the Americas (OEPA), Guatemala City, Guatemala * Address correspondence to Frank Richards Jr., River Blindness Elimination Program, The Carter Center, One Copenhill, 453 Freedom Parkway, Atlanta, GA frank.richards@emory.edu Abstract. We report the elimination of Onchocerca volvulus transmission from the Central Endemic Zone (CEZ) of onchocerciasis in Guatemala, the largest focus of this disease in the Americas and the first to be discovered in this hemisphere by Rodolfo Robles Valverde in Mass drug administration (MDA) with ivermectin was launched in 1988, with semiannual MDA coverage reaching at least 85% of the eligible population in > 95% of treatment rounds during the 12-year period, Serial parasitological testing to monitor MDA impact in sentinel villages showed a decrease in microfilaria skin prevalence from 70% to 0%, and polymerase chain reaction (PCR)-based entomological assessments of the principle vector Simulium ochraceum s.l. showed transmission interruption by These assessments, together with a 2010 serological survey in children 9 69 months of age that showed Ov16 IgG4 antibody prevalence to be < 0.1%, meeting World Health Organization (WHO) guidelines for stopping MDA, and treatment was halted after After 3 years an entomological assessment showed no evidence of vector infection or recrudescence of transmission. In 2015, 100 years after the discovery of its presence, the Ministry of Health of Guatemala declared onchocerciasis as having been eliminated from the CEZ. INTRODUCTION Human onchocerciasis (river blindness) is caused by Onchocerca volvulus, a tissue-dwelling filarial nematode transmitted by certain species of the genus Simulium. 1 Adult male and female worms form fibrous, often palpable, subcutaneous onchocercomas ( nodules ), in which fertilized female worms produce microfilariae (mf). The mf leave the nodule and reside in the dermis. They may also enter the eyes. Human disease results largely from death of the mf, which results in inflammation, itching, visual impairment, and blindness. The Simulium ( black fly ) vectors breed Copyright 2015 by the American Society of Tropical Medicine and Hygiene
2 in rapidly flowing rivers and streams and become infected when they ingest mf during a blood meal; in competent black fly species, mf develop into third stage larvae that can infect humans when the vector takes a subsequent blood meal. There are no important animal reservoirs of O. volvulus to maintain the transmission cycle independent of the human population itself. 2 Human onchocerciasis is thought to have originated in Africa when Onchocerca species in ungulates adapted to man; the parasite is believed to have been brought to the Americas through the Atlantic slave trade. 3 Transmission was only focally established in the Americas, in contrast to the extensive transmission zones that exist in Africa. In the Americas, due to a limited distribution of competent vectors, transmission zones ( foci ) are small and sharply delimited geographically, and are generally maintained by high vector biting rates. Before control measures were implemented, there were 13 foci in six countries in Latin America (Brazil, Colombia, Ecuador, Guatemala, Mexico, and Venezuela), with an overall human population at risk in 2013 of just over 500,000 persons. 4 Guatemala accounts for the largest at risk population for onchocerciasis in the Americas (231,467, representing about 41% of the total at risk regional population). The infection is transmitted by Simulium ochraceum s.l., which breeds at an altitude between 500 and 1,500 m in small streams and their tributaries. 5 Guatemala has four foci: Santa Rosa (in the province of Santa Rosa), Huehuetenango (in the province of Huehuetenango), Escuintla-Guatemala (parts of the provinces of Escuintla and Guatemala), and the Central Endemic Zone (CEZ) (parts of the provinces of Suchitepéquez, Sololá, and Chimaltenango). 6 The CEZ (Figure 1) is the largest of the four foci in terms of population (126,430, or 55% of Guatemala s population at risk), and intensity of transmission. Of historical interest, the CEZ was the first onchocerciasis endemic area to be described in the Americas, discovered 100 years ago (1915) by the famed Guatemalan researcher, Rodolfo Robles Valverde. It was Robles work in the CEZ that first described the relationship between the O. volvulus infection, nodule rates, and ocular disease, 7,8 and gave rise to human onchocerciasis in this hemisphere being referred to as Robles Disease. To control onchocerciasis, the Guatemalan Ministry of Public Health and Social Welfare (MSPAS, in its Spanish acronym) established a Department of Robles Disease in the mid-1930s (the current name is Subprograma de Oncocercosis ). Although vector control was done in Escuintla-Guatemala for a short time, 9 the primary activity of the MSPAS against onchocerciasis consisted of sending nodulectomy brigades to the four endemic areas to provide outreach surgical services. The most systematic and sustained nodulectomy activities were in the CEZ. 6 Within 1 year of the 1987 Merck donation of the oral microfilaricidal medicine ivermectin (Mectizan ) to treat onchocerciasis, these brigades initiated mass drug administration (MDA) in parts of the CEZ; in 1990, the MSPAS adopted MDA, with related health education, as the primary intervention for all onchocerciasis-endemic areas of the country. 10 In this report, we review the history of the CEZ MDA program and the monitoring and evaluation activities that led to a 2015 declaration that transmission of O. volvulus had been eliminated, based on fulfillment of the 2001 World Health Organization (WHO) guidelines for elimination of onchocerciasis. 11
3 The central endemic zone. METHODS The CEZ is found in the highlands south of Lake Atitlán in contiguous parts of three provinces: Sololá, Suchitepéquez, and Chimaltenango (Figure 1). The area is largely populated by people of Mayan Indian descent who make their living by working on large coffee or tea estates (fincas). 6,10 There are 321 endemic communities in the CEZ, with a total population at risk of onchocerciasis during the last year of MDA (in 2011) calculated to be 124,498, and a treatment eligible population (which excludes pregnant women and children under 5 years of age) of 112,338 persons. Over 90% of the population and communities are in two provinces: Suchitepéquez and Chimaltenango (Table 1). History of MDA in the CEZ. A cumulative total of 2.9 million directly observed ivermectin treatments were delivered by the MSPAS s CEZ MDA program during the period Figure 2 shows the CEZ treatment coverage (top panel) of the eligible population by treatment round (top panel) and total treatments by year (bottom panel). The MDA program began in 1988 as a pilot study in some of the most affected CEZ communities. 12,13 A MSPAS decentralization policy that moved onchocerciasis operations from the central to provincial levels in the 1990s resulted in major challenges sustaining the MDA strategy; MDA was intermittent, and data reporting was spotty, with no treatments reported for 1991, 1993, and The regional Onchocerciasis Elimination Program for the Americas (OEPA) was established with support from the River Blindness Foundation in 1993 in response to the 1991 Resolution 35:14 of the Directing Council of the Pan American Health Organization (PAHO/WHO) that called for the elimination of onchocerciasis morbidity from the Americas by OEPA (with its headquarters in Guatemala City) together with other partners, began to provide sustained technical and financial support for the MSPAS MDA program in 1994, 15 and by 1996 annual MDA rounds were established in the CEZ. In 2000, the MSPAS made its policy to provide semiannual (every 6 months) MDA in all endemic communities in the CEZ, and to stop routine nodulectomy campaigns. The treatment program provided effective coverage (e.g., directly observed treatment of 85% of the eligible population 13 from 2000 to 2011 (Figure 2, top panel) in 23 (96%) of the 24 MDA rounds. A 2008 unpublished interview survey conducted by the U.S. Centers for Disease Control and Prevention (CDC) (Kim Lindblade, CDC, unpublished data) confirmed the veracity of the program s reported coverage statistics. Based on the assessments conducted in reported in this article, the MDA was halted in 2012 and a 3-year posttreatment surveillance (PTS) period was launched. PTS ended in 2014 with the successful completion of an entomological survey, following OEPA recommendations. 16 Parasitological, ophthalmological, and entomological evaluations in sentinel villages. The impact of the program on onchocerciasis in the CEZ was monitored over time by epidemiological and entomological assessments conducted in nine sentinel villages (SVs). SVs were selected from among the most highly endemic communities for onchocerciasis; the strategy was to monitor the program in communities that had the greatest force of transmission, as these represented the worst case scenario for achieving transmission interruption. Five SVs were in Suchitepéquez, three in Chimaltenango, and one in Sololá (Table 2). The earliest (1981) pre-mda
4 SV baseline mf and ophthalmology data used in this report were for the SVs Santa Isabel, Los Tarrales, and Vesubio, from a publication by Brandling-Bennett and others. 17 Parasitological evaluations. Superficial skin biopsies ( snips ) were obtained from those who were 5 years old and who had resided in the community for at least the last 5 years. Using a 2.0-mm corneoscleral biopsy punch, a snip was taken from each scapular region, as described by Brandling-Bennett and others. 17 The snips were incubated overnight in a saline solution and the fluid then examined microscopically for mf. Results are reported as number of persons positive for mf divided by number of persons examined. Ophthalmological evaluations. Slit lamp examinations were conducted by an experienced ophthalmologist in residents 7 years old and who had resided in the community for at least the last 5 years. The indicator used was the presence of mf in the anterior chamber (MfAC). 18,19 Examinations were conducted in a darkened area after the patients were asked to sit with their head between their legs for 5 minutes. Results are reported as number of persons positive for MfAC divided by number of persons examined. Entomological evaluations. Polymerase chain reaction (PCR)-based entomological monitoring was not launched until 2002, 2 years after the MDA program achieved full geographic and effective treatment coverage with the semiannual MDA strategy. Vector collections took place from November to April (the peak S. ochraceum s.l. biting season in the CEZ) 5 using the method described by Lindblade and others 19 in , , , , and In this report, we will use the convention of naming the transmission season by the last year of vector collections (i.e., will be called the 2002 transmission season). Simulium ochraceum s.l. seeking a blood meal was collected in the SV being studied on at least 2 days/month. Two teams rotated between two collection sites (one in the fields and the other near houses) in each SV. Each team consisted of a collector and paid attractant, the latter being a resident of the SV and 18 years of age. The task of the collector was to capture the vectors from the attractant s exposed back using an aspirator. Black flies were collected just after landing and before taking a blood meal. The attractants provided informed consent to participate and were given ivermectin 1 month before starting collections and 1 month after their completion. They also had Ov16 antibody blood tests (see below) prior to and again after completion of the collections. Collections started between 8:00 and 11:00 AM and ended at 5:00 PM. They took place for 50 minutes each hour, with workers taking 10-minute breaks at the end of every hour and a 1 hour break at noon. The final entomological evaluations during the MDA phase in the CEZ were conducted over two transmission seasons (2010 and 2011) and the data from these two seasons were combined in the analysis. Based on the negative results from these evaluations, and the serological studies, (described below) MDA was halted at the end of PTS entomological collections took place from November 2013 to April 2014.
5 At the laboratory, S. ochraceum s.l. heads were separated from thoraces/abdomen ( bodies ). Head and body pools, having up to 50 heads or 50 bodies per tube, were kept separated by SV, site (field or house), hour, day, and month of collection. The bodies were analyzed first, using the standard O-150 PCR assay to detect O. volvulus deoxyribonucleic acid (DNA). 19,20 Pools that were PCR positive were confirmed by a second PCR. If a positive body pool was confirmed, then all the head pools from that community for that transmission season were tested. However, if all body pools were negative, then the head pools from that community were not tested, based on the fact that bodies (containing first stage larvae [L1] and second stage larvae [L2]) are 4 5 times more likely than heads (containing third stage larvae [L3]) to have parasite stages. 21 Serological evaluation. A serosurvey was conducted from a representative sample of young children to determine the CEZ prevalence of IgG4 antibodies to the O. volvulus recombinant antigen Ov WHO guidelines for elimination require an infection rate of < 0.1% in children under 5 years of age, and to satisfy this requirement, a sample of at least 3,000 was needed to determine a one-sided 95% confidence interval (CI) that excluded 0.1%. Assuming a 20% refusal rate to participate, we determined a target sample of 3,800. Study communities were selected from among the 321 communities under the MDA program. Independent sampling was performed in each of the three provinces (Sololá, Suchitepéquez, and Chimaltenango; Table 1) in accord with the different sizes of the populations at risk in each province, with 89% of the children sampled being from Suchitepéquez and Chimaltenango. Communities in each province were ordered at random and the number of young children under 5 years of age likely to be in those communities estimated based on the latest census data and standard population pyramids for rural Guatemala. A skip interval was calculated, and a random number was chosen to determine in which community on the list the skip interval calculations would begin to be applied. The community selections continued along the skip interval until the necessary number of children for sample for the given province was reached. The sample communities were visited and the purpose of the blood study was explained in community meetings. In those meetings it was stressed that it was the right of each individual and their parents to decide whether to participate and that the results of the tests would be provided on request. Written, informed consent/assent was obtained from the parents or guardians of all participant children. Blood was obtained from children reported to be 9 months of age up to their reported fifth birthday. Using standard sterile finger prick, L blood was placed directly on Whatman filter paper No. 2 and allowed to dry. The dried blood spots (DBSs) were placed in plastic bags with a desiccant, and stored at 20 C until analyzed within 2 months of collection using a standard enzyme-linked immunosorbent assay (ELISA) at the Universidad del Valle de Guatemala (UVG) laboratory in Guatemala City. Two 6-mm punches from the DBS were eluted overnight in a phosphate-buffered saline-tween/bovine serum albumin solution. The eluted solution was run in duplicate in a standard Ov-16 ELISA as previously described. 19,23 Any positive results were repeated before being reported as positive. The IgG4 based ELISA as configured in the Guatemala laboratory has a sensitivity of 67% and a specificity of 100% and performs equally well on sera and filter paper DBSs (Vitaliano Cama, CDC, personal communication). Archival review. After the survey and laboratory work was completed, the communities selected for the serosurvey were compared with available MSPAS records from community level nodulectomy
6 brigade visits over the 11-year pre-mda period ( ) before ivermectin MDA was widely introduced. 24 The data consisted of convenience samples of community residents who presented themselves to MSPAS staff for a palpation examination for onchocercomas. Many of these persons were undoubtedly self-selected (as were their children) for examination, believing that they had nodules that needed to be removed by the brigadistas. Data included the date of the visit, the number of persons examined, the number of persons with nodules, and numbers of children under 5 years of age with nodules (as an indicator of recent incidence). Data from all visits to a sample community over the period were summed to give a single value for pre-mda convenience sample/self-section community nodule rate (number of persons with nodules divided by number of persons examined), as well as the number of children under 5 years of age with nodules. Unfortunately, the total number of children under 5 years who were examined was not available, so a nodule rate among children who presented for examination could not be calculated. Analysis. Critical thresholds were based on the 2001 WHO Guidelines for Elimination of Onchocerciasis, as adapted by OEPA: 1) interruption of transmission infection in vectors; an upper bound of the 95% CI of the prevalence of flies carrying infective larvae of < 1 infective fly/2,000, upper bound of the 95% CI of the seasonal transmission potential (STP) of < 20L3/person/transmission season, and upper bound of the 95% CI of infection rates in young children of < 0.1%; 2) elimination of morbidity MfAC of the eye at a level where the upper bound of the 95% CI of < 1%; and 3) elimination of transmission 3 years after stopping MDA (the PTS phase) infection in vectors remains at a level where the upper bound of the 95% CI is < 1 infective fly/2,000 and the upper bound of the 95% CI of the STP remains < 20 L3/person/transmission season. 11,16,18,19 The one-sided 95% CIs for the prevalence were calculated using the SAS (version 9.0; SAS Institute, Cary, NC) FREQ procedure with the EXACT statement, BINOMIAL option, and an alpha level of Entomological data were analyzed using the Poolscreen 2.0 program, which was used to calculate the proportion of infective flies based on the number of positive pools and the associated 95% CIs. 20,25,26 Biting rates STPs were calculated as described by Lindblade and others. 19 Overall means reported for SVs were an average of the mean infection rate for each SV, in a given survey year. Ethics. Before their execution, the surveys reported herein received appropriate review by the MSPAS, the UVG, the CDC, and Emory University, and were considered as program evaluation necessary in the monitoring of a public health program. Written, informed consent was obtained from all participants over 18 years of age, and from the parents or guardians of all participant children between 12 and 18 years of age. Children under 12 required parental assent. Fly attractants, who were residents of the SVs and so routinely exposed to vector bites in their daily activities, were paid for their time: they were read or had read to them a consent form and indicated their willingness to participate as attractants with their signature or fingerprint.
7 Parasitological evaluations. RESULTS Between 1981 and 2010, there were 47 community visits for skin snip evaluations to determine mf prevalence in the nine SVs of the CEZ (mean: 5.2 assessments per SV, range: 4 6). Figure 3 (top panel) depicts the decrease over time of skin snip prevalence that was first observed after the MDA program reached sustained and effective coverage. Table 2 shows the results of initial baseline ( ) and final ( ) skin snip assessments, by SV. The mean SV baseline mf prevalence (obtained prior to the launching of MDA) was 70% (range 36 90%) for the nine SVs. In the final SV skin snip assessments (based on the examination of 1,032 individuals) no mf positives were found. Ophthalmological evaluations. Between 1981 and 2010, there were 19 community visits for ophthalmological evaluations for onchocerciasis in the nine SVs of the CEZ (mean: 2.1 assessments per SV, range: 2 3). Figure 3 (bottom panel) shows the decrease over time of MfAC prevalence. Table 2 shows the results of baseline ( ) and final ( ) MfAC assessments in the nine SVs of the CEZ, by SV. The mean SV baseline MfAC prevalence was 12.1% (range 0 39%). In the final slit lamp assessments in the SVs, a total of 857 persons were examined; a single person with MfAC was found in Los Tarrales, resulting in a 0.5% prevalence for that community, and a 0.1% overall MfAC prevalence (with a one-sided 95% CI of 0 0.6%). Entomological evaluations. A total of four entomological field exercises were conducted during transmission seasons 2002, 2007, (years combined), and the 2014 PTS period. These exercises consisted of a total of 6,023 person-collecting hours over 351 days during the peak S. ochraceum s.l. biting season of those collection years. 5 Table 3 and its footnote summarize the number of SVs, collection sites, and months of vector collection activities. A total of 328,575 vectors were collected and tested by PCR for O. volvulus DNA. Table 4 shows a summary of PCR PoolScreen results. The trend of the 95% upper CIs of key indices (< 1 infective fly/2,000 vectors and STP < 20 L3/person/transmission season) over the entomological monitoring period in the CEZ is shown in Figure 4. In 2002, 2 years into the full coverage MDA program, the point estimate for the prevalence of flies carrying infective larvae was 1.02/2,000 (95% CI: /2,000; Table 4 and Figure 4 top panel), and the upper 95% CI for the STP was 24.4 (mean 15.6, 95% CI: ; Table 4 and Figure 4, bottom panel), both indicative of being right at the threshold of interrupting transmission by WHO/OEPA criteria. By 2007 (5 years and 10 MDA treatment rounds later), the upper 95% CIs for both the infective rate per 2,000 flies (0.06) and STP (1.0) were below the transmission interruption thresholds. The final entomological evaluations for the CEZ MDA phase in were similarly below the thresholds, with the upper bound of the 95% upper CI of the vector infective rate of 0.1/2,000 flies and the STP was 0 with an upper bound of the 95% upper CI of 2.6. These results, taken together with results from the serological evaluations (described below) led to a MSPAS decision to stop MDA. During PTS entomological surveillance, PCR results from testing over 119,000 flies collected from November 2013 to April 2014 showed no evidence of recrudescence of transmission: 0 infection in the vectors (95% upper CI of 0.03/2,000 flies) and 0 STP (95% upper confidence of 1.1 L3/person/transmission
8 season). The five SVs involved in the PTS evaluation included La Estrellita, Montecarlo, El Brote, Santa Isabel, and Vesubio. An additional non-sentinel village (Nueva Providencia, located in San Lucas Toliman, Solola) that was known to have been hyperendemic prior to MDA was included in the entomological assessment, as a spot check Serological evaluation. Our study design aimed to select 3,800 children with an estimate that we would have a 20% refusal rate; we sampled 3,417 (90% of our target) in 29 communities: 2,171 (63% of sampled children) were from 15 (52% of the sampled) communities in Suchitepequez; 878 (26%) children in 12 (41%) communities in Chimaltenango (including children from La Estrellita, the only SV randomly selected in the sample); and 368 (11%) children in 2 (7%) communities in Sololá (Table 5). All 3,417 children were negative in ELISA testing for Ov16 IgG4 (0% prevalence, upper 95% CI: 0.08%), thus satisfying the WHO guideline that 5-year cumulative prevalence rates in young children should be < 0.1% to demonstrate interruption of O. volvulus transmission. The median age of the children tested was 36 months (range 9 69 months). Archival review. Past (pre-mda) MSPAS convenience sample/self-selection nodule data were available for 22 (76%) of the 29 sample communities (Table 5). Over the period , MSASP brigades visited these 22 communities a total of 84 times (range 1 14 visits/community). Out of 8,456 palpation examinations, 1,009 (12%) were positive for onchocercomas. The range of pre-mda community nodule rates was 0 78%, with the SV La Estrellita having the highest prevalence, followed by Santa Adelaida (28%). Also in the pre-mda surveys conducted between 1980 and 1990, 124 children under 5 years of age were found to have nodules; 99 of these were from Santa Adelaida and 13 from La Estrellita. In contrast, over 20 years later, in a new (2010) generation of 125 children living in those same two communities, none had detectable Ov16 IgG4 antibodies, evidence of an absence of transmission there for many years. DISCUSSION In this report, we review the history of the 24 years of MDA with ivermectin in the CEZ of Guatemala. The MDA program struggled in its first 12 years ( ) to scale up and reach sustained annual treatment coverage. It was not until the year 2000, when, with better financial, administrative, and political support, the CEZ MDA program began delivering effective MDA rounds. This second 12-year phase of programmatic maturity was when, based on results from serial SV monitoring and evaluation activities, O. volvulus transmission interruption was actually accomplished. MDA was suspended in 2012, and after a 3-year ( ) period of PTS, an entomological PCR assessment of over 119,000 flies showed no evidence of vector infection. Transmission was declared eliminated by the Guatemalan Ministry of Health in This declaration occurred 100 years after the discovery of onchocerciasis in the Americas in 1915 by Rodolfo Robles Valverde, whose work was conducted in the CEZ. Robles ( ) was born in Quetzaltenango and at the age of 17 went to France for his education. He was granted his medical degree from The Sorbonne in Paris in 1904, where he specialized in colonial medicine, a field focused on malaria, public health, and microbiology. After his return to Guatemala, he maintained a keen research interest in tropical pathology, and in 1915 encountered an 8-year-old patient with a subcutaneous nodule in which Robles discovered the
9 adult worms of O. volvulus. He subsequently dedicated much of his research to the study of the transmission, clinical pathology, and epidemiology of this parasite, and most importantly established for the first time that onchocerciasis was linked to visual loss. 7,8 France later awarded him the Legion of Honor. The highest medical award of Guatemala is named in his honor, as is an ophthalmological hospital in Guatemala City. 27 The CEZ is the largest transmission zone (focus) of onchocerciasis in Guatemala, and with a population at risk of 124,498, is larger than the other three Guatemalan foci combined. The CEZ also has the largest at risk population of the 13 onchocerciasis foci in the Americas, comprising 22% of the 565,232 persons originally at risk for contracting the disease. It is followed in size by the south Chiapas focus in Mexico (with 117,825 persons at risk, or 21% of the regional total) and the northeast focus of Venezuela (95,567 persons at risk, 17%). 4 Together these three foci account for 60% of the population at risk in the Americas. MDA has been halted in all three of these foci, 28,29 but only south Chiapas and the CEZ have completed PTS. Overall, MDA has been stopped in 11 of the 13 American foci; the only active MDA program for onchocerciasis in the Americas at this time is in a cross-border focus (shared by Brazil and Venezuela) in the Amazon jungle. The difficult to access indigenous Amerindian population (the Yanomami) who are targeted for treatment in this area comprise only 5% of the population in the Americas originally targeted for MDA. 4 The roadmap for establishing the elimination of onchocerciasis in Guatemala used the WHO guidelines published in 2001, as modified for field operations and observations and conditions reported by Lindblade 19 and OEPA. 16 The modified guidelines have been successfully used by independent verification teams (IVTs), sent under the auspices of the WHO Neglected Tropical Disease Department to verify the elimination of onchocerciasis in Colombia in and Ecuador in In this process, an IVT country visit is undertaken after the submission by a ministry of health of a detailed dossier that provides evidence that all foci in the country have eliminated O. volvulus transmission. In Guatemala, the elimination process has already been completed and published in peer-reviewed journals for three of the four of its onchocerciasis foci: Santa Rosa, 19 Escuintla-Guatemala, 32 Huehuetenango. 33 Based on the completion of elimination evaluations in the CEZ, as reported herein, Guatemala submitted its dossier to WHO in 2015, along with a request for an IVT visit. In the 1990s, several key studies seeking to determine how to best use ivermectin MDA to break O. volvulus transmission were conducted in the CEZ by MSPAS, CDC, the UVG, the University of Arizona, and other partners. 10,12,13,34 The OEPA strategy of providing at least semiannual (every 6 month) treatment rounds in all affected communities, each achieving effective ( 85% directly observed treatment of eligibles) coverage, was based largely on the findings from these studies. An important challenge was that ivermectin, a potent oral microfilaricidal drug, is not immediately lethal to the adult O. volvulus worms. The elimination strategy in the Americas was therefore based on using ivermectin to keep levels of mf in the human population low enough to prevent them from infecting the vector. With the transmission cycle so suppressed, MDA under this strategy would then need to be given for the duration of the reproductive life of remaining adult worms being exposed to the twice per year doses of ivermectin. Cupp and Cupp estimated the reproductive adult female worm life span under such intense ivermectin exposure to be about 6.5 years. 35 Adult male worms are more sensitive to ivermectin than female worms, and perish even more rapidly. Histological studies of nodules showed fewer than 20% of nodules contained male worms and more than 80% of female worms were
10 uninseminated and producing unfertilized oocytes in populations where transmission was broken and twice per year MDA was being provided. 36 The entomological results from this study are worthy of note. The first PCR-based entomological measurements did not begin until 2002, 2 years into effective MDA delivery. These early PCR results showed the infective rate and the STP to be still above the breakpoint thresholds of an upper bound of the 95% CI of < 1/2,000 and < 20 L3/person/transmission season (Figure 4). We can estimate the pre-mda baseline using dissection data from two SVs. Collins and others, working in the SV Los Tarrales from 1976 to 1977 found an S. ochraceum s.l. infective rate of 61/2,000, and an STP of 174 L3/person. 21 Cupp and others, working in the SV Los Andes in 1988, reported a pre-mda STP of 108 L3/person. 13 If the pre-mda baseline STP was assumed to be the mean value from these two studies (141 L3/person/season), then by 2 years into the effective MDA program, transmission had been reduced by approximately 82% (from 141 to 24). By 2007, after 7 years and 14 MDA treatment rounds, the entomological breakpoint thresholds had been achieved (with an STP reduction from pre-mda baseline of > 99%). Effective MDA was continued for another 5 years (10 rounds) past this point, at which time a total absence of Ov16 IgG4 antibody reactivity was demonstrated in > 3,400 children under 5 years of age. These children were sampled from randomly selected communities within the CEZ that included known and unknown endemic villages; in two of the known endemic villages, children under 5 had had nodules noted by the MSPAS brigades in the pre-mda era. The serological results confirmed the 2007 and 2011 entomological data that there had been no parasite transmission for at least 5 years. During the PTS entomological surveillance, PCR results from testing over 119,000 flies in sentinel, as well as an extra sentinel village, showed no evidence of recrudescence of transmission or of human parasite vector contact. These PTS entomological results are strong evidence that the adult O. volvulus worms in the transmission zone were either absent, or at such a low reproductive levels that the population could not recover. 16 A decline in human onchocerciasis prevalence and intensity of infection in the CEZ likely began before full coverage with MDA was achieved in Any such decline in the human population would have been accompanied by a decrease in the force of transmission, although probably insufficient to break transmission, especially in hyperendemic areas. As noted above, the 2002 entomological assessment after only 2 years of full coverage twice per year CEZ MDA showed both the prevalence in flies (with an upper 95% CI of 1.60/2,000) and the STP (with an upper 95% CI: 24.4 L3/person/season) were just above the transmission breakpoint as defined by the current WHO/OEPA guidelines. The 2007 entomological evaluation, conducted 5 years later, was the first time that the breakpoint was documented to have been reached. However, it is highly likely that transmission was broken much earlier than 2007, probably within 2 years of the 2002 survey. Thus we believe the MDA program provided sufficient treatment ( ) for the 6.5 year expected reproductive life span of adult O. volvulus female worms projected under twice per year ivermectin treatment pressure. 35 Although there might have been a small risk with the halting MDA in 2012 (after only 5 years after documenting transmission interruption in 2007) that some adult female worms remained, we could find no evidence that there were sufficient reproductively active parasites to result in the resumption of transmission in the SVs where PTS was conducted. This could also have been due to the impact of MDA on the adult male worm population that appears more sensitive than O. volvulus females to recurrent twice yearly treatments. 36 The success against onchocerciasis in the Americas is in large part due to a durable public private partnership, embodied in OEPA that includes the six endemic countries (Brazil, Colombia,
11 Ecuador, Guatemala, Mexico, and Venezuela), PAHO/WHO, The Carter Center, Merck and the Mectizan Donation Program, and many other partners. Annual meetings (the Inter-American Conferences on Onchocerciasis) of all partners have been held since A small secretariat for the OEPA partnership, based in Guatemala City, provides technical, administrative, advocacy, and some financial support to national programs. 15 The Carter Center has shouldered the administrative responsibilities for the secretariat for the last 20 years. A Program Coordinating Committee meets twice per year to act as the technical steering committee for OEPA. It reviews and approves the annual Weekly Epidemiological Record progress reports of the regional initiative that have been published by WHO since PAHO/WHO provided the initial 1991 and subsequent key regional resolutions to provide the political mandate behind the effort. In 2008, PAHO s Directing Council renewed the call to eliminate onchocerciasis throughout the region in Resolution CD48.R12. The following year the Directing Council issued CD49.R19 that called for the elimination or control of 12 neglected infectious diseases of poverty in the Americas, which includes onchocerciasis elimination as one of its 2015 targets. 4,14 In conclusion, we report the elimination of O. volvulus transmission from the CEZ in Guatemala, the largest focus of onchocerciasis in the Americas and the first to be discovered in this hemisphere by Rodolfo Robles in Elimination was achieved by a national program that delivered semiannual mass ivermectin administration reaching at least 85% of the eligible population over a 12-year period ( ). Progress toward elimination was demonstrated through serial ocular, parasitological, and entomological surveys conducted in nine sentinel villages, as well as in a broad sampling of young children for Ov16 IgG4 antibody reactivity throughout the CEZ prior to stopping the MDA campaign. Three years after halting mass treatment an entomological assessment showed no evidence of vector infection. The Ministry of Health of Guatemala declared onchocerciasis transmission as having been eliminated from the CEZ 100 years after its discovery there by Robles. Received May 15, Accepted for publication July 17, Acknowledgments: We thank colleagues at the Centro de Estudios en Salud of the Universidad del Valle de Guatemala (Nazario Lopez, Julio Illescas, Aura Paniagua, Lisbeth Paniagua, Nancy Zamora, Soledad Rodas, Rodrigo González, Lucía García, Nancy Say, Mynor López, José Luis Boteo, Jorge Sincal, Marvin Xiquitá, Efraín Gramajo Mazariegos, Adriana Santis, Byron Arana, Ricardo Luján, and the late Nancy Cruz-Ortiz); Ministerio de Salud Pública y Asistencia Social (Julio Castro, Eduardo Catú, Arturo Sánchez, Sayra Chanquín, Carlos Blanco, Brenda Villatoro, Juan Carlos Solares, the late Reginaldo Pichillá, Eusebio Efraín Montejo, Luis Blanco, Luis Posada Colindres, Victor Barrios, Pedro Yax and the late Onofre Ochoa); Onchocerciasis Elimination Program for the Americas (OEPA) (Silvia Sagastume, Luis Erchila, Jack Blanks, Edmundo Alvarez, and Oswaldo Mejía); Pan American Health Organization (Steve Ault, Fernando Beltran, John Ehrenberg, Luis Gerardo Castellanos); Division of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, GA (Kim Lindblade, Charles Porter, Vita Cama, Joseph Amann, Patricia Juliao, Monica Parise, George Punkosdy, James MaGuire); Lions Clubs (Alfonso Barahona, Carlos Samuel Arévalo); The Bill and Melinda Gates Foundation (David Brandling-Bennett, Julie Jacobson); The River Blindness Foundation (the late BOL Duke, the late William Baldwin, John Moores), The Carter Center (Don Hopkins, Craig Withers, Nicole Kruse, Emily Howard, Madelle Hatch, Lindsay Rakers, Emily Griswold, Lauri Hudson-Davis, Jennifer Lee and the late Andrew Agle), the International Eye Foundation (Victoria Sheffield, John Barrows), Merck and Co. and the Mectizan Donation Program (Joni Lawrence, Stefanie Meredith, Adrian Hopkins, Ken Gustavsen, Brenda Colatrella) and Richard Collins, Tom Nutman, Kevin Winthrop, Jill Heeringa, John Davies, Rodolfo Zea Flores, Edgar Lobos, Carlos Gonzales-Peralta, and Orlando Oliva. The Onchocerciasis Elimination Program for the Americas (OEPA) coalition includes The Carter Center (as administrative lead), the six endemic countries, PAHO/WHO, the Lions Clubs
12 International Foundation and local Lions Clubs, the Bill and Melinda Gates Foundation, Merck and the Mectizan Donation Program, CDC, USAID, the Carlos Slim Foundation, and multiple regional universities. Financial support: The Guatemalan program received financial support from the Guatemalan Government and the Pan American Health Organization, and from 1993 to 2014 through OEPA/The Carter Center that included grants from the Lions Clubs International Foundation, the Bill and Melinda Gates Foundation, Merck and the Mectizan Donation Program, the U.S. Centers for Disease Control and Prevention (CDC), the United States Agency for International Development (USAID), The Carlos Slim Foundation, The Inter-American Development Bank, The River Blindness Foundation, the OPEC Fund for International Development (OFID), The Alwaleed Bin Talal Foundation, The Starr Foundation, Falconer Charitable Remainder Trust, The Carter Center, The Cartre UK Foundation, The Baxter International Foundation, Alcon Laboratories, John C. and Karyl Kay Hughes Foundation, The Osprey Foundation of Maryland, The UPS Foundation and many private individuals. Prior to OEPA, in the late 1980s and 1990s, key support to Guatemala for ivermectin distribution, in addition to that of the Government of Guatemala, was provided by the River Blindness Foundation, the Pan American Health Organization, the International Eye Foundation, the Japan International Cooperation Agency (JICA), and the Public Welfare Foundation. Ivermectin (Mectizan ) was provided by Merck. Authors addresses: Frank Richards Jr., River Blindness Program, The Carter Center, Atlanta, GA, frank.richards@emory.edu. Nidia Rizzo, Renata Mendizabal de Cabrera, and Oscar de Leon, Centro de Estudios en Salud, Universidad del Valle de Guatemala, Guatemala, Guatemala, s: nrizzo@ces.uvg.edu.gt, rmendizabal@ces.uvg.edu.gt, and odeleon@ces.uvg.edu.gt. Carlos Enrique Diaz Espinoza, Ministerio de Salud Pública y Asistencia Social, Guatemala, Guatemala, carlosenriquediazespinoza@gmail.com. Zoraida Morales Monroy, Programa Nacional de Enfermedades Transmitidas por Vectores, Ministerio de Salud Pública y Asistencia Social de Guatemala, Ciudad de Guatemala, Guatemala, zoraidamoralesmonroy@gmail.com. Carol Guillermina Crovella Valdez, Ministerio de Salud Pública y Asistencia Social de Guatemala, Ciudad de Guatemala, Guatemala, ccrovellav@gmail.com. Guillermo Zea-Flores, Ciudad de Guatemala, Guatemala, gzeaflores@hotmail.com. Mauricio Sauerbrey, Alba Lucia Morales, Dalila Rios, and Alfredo Domínguez, Onchocerciasis Elimination Program for the Americas, Edificio Murano Center, Guatemala City, Guatemala, s: msauercar@gmail.com, almorales@oepa.net, drios@oepa.net, and adominguez59@hotmail.com. Thomas R. Unnasch and Hassan K. Hassan, Global Health Infectious Disease Program, Department of Global Health, University of South Florida, Tampa, FL, E- mails: tunnasch@health.usf.edu and hhassan@health.usf.edu. Robert Klein, Medical Entomology Research and Training Unit/Guatemala, Miami, FL, roeklein64@gmail.com. Mark Eberhard, Centers for Disease Control and Prevention, Atlanta, GA, mle1@cdc.gov. Ed Cupp, Owensboro, KY, cuppedd@auburn.edu. REFERENCES <jrn>1. Cupp EW, Sauerbrey M, Richards FO, Elimination of human onchocerciasis: history of progress and current feasibility using ivermectin (Mectizan ) monotherapy. Acta Trop Suppl 120 (Suppl 1): S100 S108.</jrn> <jrn>2. Richards FO, Miri E, Meredith S, Guderian R, Sauerbrey M, Remme H, Packard R, Ndiaye JM, Onchocerciasis. Bull World Health Organ 76 (Suppl 2): </jrn> <jrn>3. Zimmerman PA, Katholi CR, Wooten MC, Lang-Unnasch N, Unnasch TR, Recent evolutionary history of American Onchocerca volvulus, based on analysis of a tandemly repeated DNA sequence family. Mol Biol Evol 11: </jrn> <jrn>4. Anonymous, Progress toward elimination of onchocerciasis in the Americas. MMWR 87: </jrn> <jrn>5. Porter CH, Collins RC, Seasonality of adult black flies and Onchocerca volvulus transmission in Guatemala. Am J Trop Med Hyg 38: </jrn> <jrn>6. Yamagata Y, Suzuki T, Garcia Manzo GA, Geographical distribution of the prevalence of nodules of Onchocerca volvulus in Guatemala over the last four decades. Trop Med Parasitol 37: </jrn>
13 <unknown>7. Robles R, Calderón V, Enfermedad nueva en Guatemala. Guatemala: Revista de la Juventud Médica, año XVIII, tomo XVII. 8: 9 116, 177.</unknown> <jrn>8. Robles R, Onchocercose humaine au Guatemala produisant la cecite et l erysipe le du littoral (Erisipela de la costa). Bull Soc Pathol Exot 12: </jrn> <jrn>9. Ochoa JO, Castro JC, Barrios VM, Juarez EL, Tada I, Successful control of onchocerciasis vectors in San Vicente Pacaya, Guatemala, Ann Trop Med Parasitol 91: </jrn> <jrn>10. Richards FO, Klein R, Zea-Flores R, Gonzáles-Peralta C, Castro J, Zea-Flores G, Knowledge, attitudes, and perceptions during a community-level ivermectin distribution campaign in Guatemala. Health Policy Plan 10: </jrn> <bok>11. Anonymous, Certification of Elimination of Human Onchocerciasis: Criteria and Procedures, Guidelines. Geneva, Switzerland: WHO WHO/CDS/CPE/CEE.18.b.</bok> <jrn>12. Collins RC, Gonzales-Peralta C, Castro J, Zea-Flores G, Cupp M, Richards FO, Cupp EW, Ivermectin: reduction in prevalence and infection intensity with Onchocerca volvulus following biannual treatments in five Guatemalan communities. Am J Trop Med Hyg 47: </jrn> <jrn>13. Cupp EW, Ochoa JO, Collins RC, Cupp MS, Gonzales-Peralta C, Castro J, Zea-Flores G, The effects of repetitive community-wide ivermectin treatment on transmission of Onchocerca volvulus in Guatemala. Am J Trop Med Hyg 47: </jrn> <jrn>14. Sauerbrey MS, The Onchocerciasis Program for the Americas (OEPA). Ann Trop Med Parasitol 102 (Suppl 1): S25 S29.</jrn> <jrn>15. Blanks J, Richards FO, Beltran F, Collins RC, Alvarez E, Zea-Flores G, Bauler B, Cedillos R, Heisler M, Brandling-Bennett D, Baldwin W, Bayona M, Klein R, Jacox M, The Onchocerciasis Elimination Program of the Americas: a history of partnership. Rev Panam Salud Publica 3: </jrn> <unknown>16. Program Coordinating Committee and OEPA Staff, Guide to detecting a potential recrudescence of onchocerciasis during the post treatment surveillance period: the American paradigm. Res Rep Trop Med 3: </unknown> <jrn>17. Brandling-Bennett AD, Anderson J, Fuglsang H, Collins RC, Onchocerciasis in Guatemala. Epidemiology in fincas with various intensities of infection. Am J Trop Med Hyg 30: </jrn> <jrn>18. Winthrop K, Proaño R, Oliva O, Arana B, Mendoza C, Dominguez A, Amann J, Punkosdy G, Blanco C, Klein R, Sauerbrey M, Richards FO, The reliability of anterior segment lesions as indicators of onchocercal eye disease in Guatemala. Am J Trop Med Hyg 75: </jrn> <jrn>19. Lindblade KA, Arana B, Zea-Flores G, Rizzo N, Porter CH, Dominguez A, Cruz-Ortiz N, Unnasch TR, Punkosdy GA, Richards J, Sauerbrey M, Castro J, Catú E, Oliva O, Richards FO, Elimination of Onchocerca volvulus transmission in the Santa Rosa Focus of Guatemala. Am J Trop Med Hyg 77: </jrn>
14 <jrn>20. Rodrıguez-Perez MA, Katholi CR, Hassan HK, Unnasch TR, Large scale entomologic assessment of Onchocerca volvulus transmission by poolscreen PCR in Mexico. Am J Trop Med Hyg 74: </jrn> <jrn>21. Collins RC, Onchocerciasis transmission potentials of four species of Guatemalan Simuliidae. Am J Trop Med Hyg 28: </jrn> <jrn>22. Lobos E, Weiss N, Karam M, Taylor HR, Ottesen EA, Nutman TB, An immunogenic Onchocerca volvulus antigen: a specific and early marker of infection. Science 251: </jrn> <jrn>23. Oguttu D, Byamukama E, Katholi CR, Habomugisha P, Nahabwe C, Ngabirano M, Hassan HK, Lakwo T, Katabarwa M, Richards FO, Unnasch TR, Serosurveillance to monitor onchocerciasis elimination: the Ugandan experience. Am J Trop Med Hyg 90: </jrn> <edb>24. Richards FO, Using GIS to target onchocerciasis control activities in Guatemala. David B, Hippolyte F, eds. Geographical Targeting for Poverty Alleviation: Methodology and Applications. Washington, DC: The World Bank Regional and Sectoral Studies, </edb> <jrn>25. Katholi CR, Toe L, Merriweather A, Unnasch TR, Determining the prevalence of Onchocerca volvulus infection in vector populations by polymerase chain reaction screening of pools of black flies. J Infect Dis 172: </jrn> <jrn>26. Unnasch TR, Meredith S, The use of degenerate primers in conjunction with strain and species oligonucleotides to classify Onchocerca volvulus. Methods Mol Biol 50: </jrn> <eref>27. Wikipedia, Rodolfo Robles. Available at: Accessed March 13, 2015.</eref> <jrn>28. Rodrıguez-Perez MA, Domınguez-Vazquez A, Unnasch TR, Hassan HK, Arredondo- Jimenez JI, Orozco-Algarra ME, Rodríguez-Morales KB, Rodríguez-Luna IC, Prado-Velasco FG, Interruption of transmission of Onchocerca volvulus in the southern Chiapas Focus, Mexico. PLoS Negl Trop Dis 7: e2133.</jrn> <jrn>29. Convit J, Schuler H, Borges R, Olivero V, Domínguez-Vázquez A, Frontado H, Grillet ME, Interruption of Onchocerca volvulus transmission in northern Venezuela. Parasit Vectors 6: 289. Available at: <jrn>30. Anonymous, Progress towards eliminating onchocerciasis in the WHO Region of the Americas: verification by WHO of elimination of transmission in Colombia. Wkly Epidemiol Rec 88: </jrn> <jrn>31. Anonymous, Progress towards eliminating onchocerciasis in the WHO Region of the Americas: Ecuador s progress towards verification of elimination. Wkly Epidemiol Rec 89: </jrn> <jrn>32. Gonzales RJ, Cruz-Ortiz N, Rizzo N, Richards J, Zea-Flores G, Domínguez A, Sauerbrey M, Catú E, Orlando O, Richards FO, Lindblade KA, Successful interruption of transmission of Onchocerca volvulus in the Escuintla-Guatemala focus, Guatemala. PLoS Negl Trop Dis 3: e404.</jrn>
15 <bok>33. Cruz-Ortiz N, Gonzalez RJ, Lindblade KA, Richards F, Sauerbrey M, Dominguez A, Zea-Flores G, Olivia O, Catú E, Rizzo N, Elimination of Onchocerca volvulus transmission in the Huehuetenango Focus of Guatemala. J Parasitol Res 2012: </bok> <jrn>34. Cupp EW, Ochoa O, Collins RC, Ramberg F, Zea-Flores G, The effect of multiple ivermectin treatments on infection of Simulium ochraceum with Onchocerca volvulus. Am J Trop Med Hyg 40: </jrn> <jrn>35. Cupp EW, Cupp MS, Impact of ivermectin community-level treatments on elimination of adult Onchocerca volvulus when individuals receive multiple treatments per year. Am J Trop Med Hyg 73: </jrn> <jrn>36. Cupp EW, Duke BO, Mackenzie CD, Guzmán JR, Vieira JC, Mendez-Galvan J, Castro J, Richards FO, Sauerbrey M, Dominguez A, Eversole RR, Cupp MS, The effects of longterm community level treatment with ivermectin on adult Onchocerca volvulus in Latin America. Am J Trop Med Hyg 71: </jrn> FIGURE 1. This map of Guatemala shows the three provinces (Sololá, Suchitepéquez, and Chimaltenango) that contribute to the Central Endemic Zone (CEZ) for onchocerciasis in Guatemala. The CEZ (dark polygon) indicates the contiguous parts of the provinces where onchocerciasis transmission took place, just south of Lake Atítlan, in the highlands at elevations from 500 to 1500 m. This figure appears in color at FIGURE 2. The top panel shows the Central Endemic Zone (CEZ) treatment percent coverage of the eligible population during the years , by treatment round (dark bars first round, light bars second round). The horizontal line indicates the coverage goal of 85% per round. The bottom panel shows single bars representing the total treatments provided by year (the bars represent the sum of treatments given during the year in those years when two rounds were given). Mass drug administration (MDA) was halted in 2012 after over 2.9 million cumulative treatments had been delivered over the period. This figure appears in color at FIGURE 3. The top panel shows the results from 47 sentinel village (SV) visits between 1981 and 2010 for skin snip evaluations to determine microfilariae (mf) prevalence in the nine SVs of the Central Endemic Zone (CEZ). Each village was visited between four and six times (mean: 5.2 assessments per SV). The graphic only shows positive results. Zero skin mf prevalence was first observed in 2007 and occurred in Buena Vista, Costa Rica, Los Andes, and Tarrales. In 2010, mf prevalence was zero in El Brote, Buena Vista, La Estrellita, Monte Carlo, Santa Isabel, Tarrales, and Vesubio. The bottom panel shows similar data for fewer (19) SV visits for ophthalmological evaluations to determine mf prevalence in the anterior chamber (MfAC); note that Monte Carlo and El Brote baseline are mf in cornea, not MfAC. Each of the nine SVs of the CEZ was visited at least twice (range 2 3). Zero values MfAC was recorded in 2007 in El Brote, Buena Vista, Costa Rica, La Estrellita, Los Andes, and Monte Carlo. In 2009, MfAC was zero in Santa Isabel and Vesubio. One individual (0.5%) was positive in Tarrales in See text and Table 2 for additional SV information. This figure appears in color at
16 FIGURE 4. The two graphs show the upper 95% confidence intervals for vector infectivity and for annual transmission potential in sentinel villages as calculated by PoolScreen. Horizontal lines indicate the breakpoint thresholds (< 1/2,000 cutoff for vector infectivity and < 20 for seasonal transmission potential [STP]) below which onchocerciasis transmission is not possible. Data are based on the examination of 328,575 vectors in 4,616 polymerase chain reaction (PCR) reactions (pools): 46,160 vectors in 835 pools in 2002, 67,808 flies in 1,260 pools in 2007, 95,306 flies in 1,836 pools in , and 119,301 flies in 685 pools in This figure appears in color at TABLE 1 Number of communities, population at risk, and treatment eligible population at risk in 2011, CEZ, Guatemala Province Number of communities (%) Population at risk (%) Eligible population (%) Suchitepéquez 153 (47) 71,445 (57) 64,559 (57) Chimaltenango 137 (43) 42,846 (34) 38,658 (34) Sololá 31 (10) 10,207 (9) 9,171 (9) Total 321 (100) 124,498 (100) 112,388 (100) CEZ = Central Endemic Zone. TABLE 2 Baseline and final microfilaria prevalences in skin and anterior chamber of the eye, CEZ, Guatemala Microfilaria in skin Microfilaria in the eye Province Municipality SV Baseline Final assessment Baseline Final assessment Prevalence Year Prevalence Year Prevalence Year Prevalence Year Solola Santiago Atitlan El Brote Suchitepequez Chicacao Monte Carlo Santa Barbara Los Andes Vesubio Patulul Santa Isabel Tarrales Chimaltenango San Miguel Pochuta Costa Rica Acatenango Buena Vista San Pedro Yepocapa La Estrellita Mean CEZ = central endemic zone; SV = sentinel village. The latitude and longitude locations of the SVs were El Brote ( , ), Monte Carlo ( , ), Los Andes ( , ), Costa Rica ( , ), Buena Vista ( , ), La Estrellita ( , ), Vesubio ( , ), Santa Isabel ( , ), Tarrales ( , ). Shown are the results of baseline and final assessment parasitological evaluations (superficial skin biopsies ( snips ) for mf prevalence and slit lamp ophthalmological examinations in residents by an experienced ophthalmologist for presence of microfilariae (mf) in the anterior chamber (MfAC).
17 Year of collection Number of SVs sampled TABLE 3 Entomological sampling activities ( ) in SVs in the CEZ, Guatemala Number of Number of Number of collection months of Months collections took place collection sites per SVs collections days Daily periods of collection (hours) Estimated number of collection hours February May January May December 2009 to February (2010) and and February May 2011 (2011) 2, (plus one spot November December 2013 and 4 6 check village) January April ,600 CEZ = central endemic zone; SV = sentinel village; PTS = posttreatment surveillance. Daily collection periods were 50 minutes/hour (see Methods). The six SVs visited in 2002 and 2007 were El Brote, Buena Vista, Costa Rica, La Estrellita, Los Andes, and Montecarlo; in the combined analysis unit, the six SVs were El Carmen Metzabal, Santa Isabel, Tarrales, and Vesubio in 2010 and La Estrellita, Montecarlo, Santa Isabel, and Vesubio in The 2014 PTS assessments took place in five SVs (El Brote, La Estrellita, Montecarlo, Santa Isabel, and Vesubio) and one-spot check village (Nueva Providencia). TABLE 4 Entomological indices ( ) for the CEZ, Guatemala Year of collection Number of flies Seasonal biting rate (range per PCR infection rate per Seasonal transmission tested by PCR community) 2,000 flies (95% CI) potential (95% CI) ,160 30,530 (26,029 35,769) 1.02 ( ) ( ) ,808 33,485 (30,868 36,313) 0 (0 0.06) 0 (0 1.0) ,306 51,704 (23,323 82,863) 0 (0 0.10) 0 (0 2.6) ,301 71,295 (66,243 76,720) 0 (0 0.03) 0 (0 1.1) PCR = polymerase chain reaction; CEZ = Central Endemic Zone; CI = confidence interval.
18 TABLE 5 Results of Ov16 IgG4 serological testing (2010) of young children, CEZ, Guatemala, together with historical (pre- MDA) nodule rates in the sampled communities Province Municipality Community (Pre-MDA) Number of OV16 Pct nodule prevalence* children tested positive Santa Barbara Santa Adelaida Guayabal NA Patulul Santa Luisa NA 77 0 San Juan Bautista Veracruz San Miguel Panan Finca La Concha San José Panan Chicacao Concepción Chinan Suchitepéquez El Recuerdo Finca Chinan Labor Los Mangales NA 74 0 Cantón La Libertad Alejandría Santa Lucía Pamaxan NA Finca Baja Vista El Pito Subtotal 2,171 (63%) 0 San Lucas Tolimán Pampojilá Sololá Xejuyú NA Subtotal 368 (11%) 0 San Miguel Pochuta Finca El Recuerdo Santa Ana NA 52 0 Finca Mirandilla Acatenango Finca Rafael Pacún San Pedro Yepocapa Finca Peña Plata Finca Santa Teresa Chimaltenango Morelia La Estrellita Nueva Victoria NA 34 0 San Francisco El Porvenir Aldea La Cruz Subtotal 878 (26%) 0 Total 3,417 0 (0 0.08) CEZ = Central Endemic Zone; MDA = mass drug administration; NA = data not available. * (Pre-MDA) nodule rates are based on convenience samples, often among individuals who were selfselected based on their belief that they had a nodule, and are therefore not based on a statistically representative sample. Nodules found in children during the pre-mda period. Number in parenthesis, 95% confidence interval.
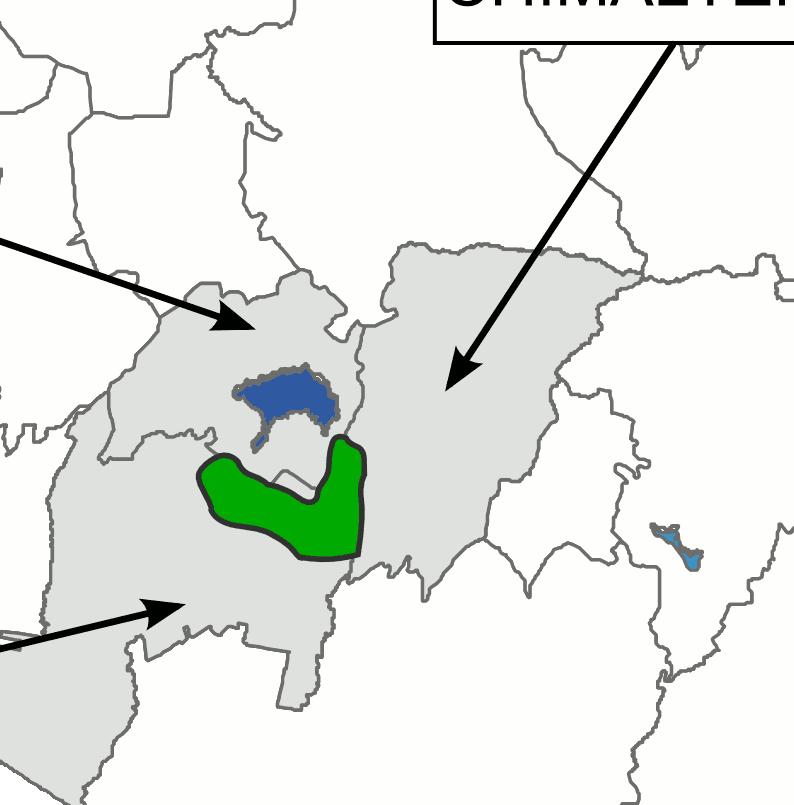
19 Figure 1
Lack of Active Onchocerca volvulus Transmission in the Northern Chiapas Focus of Mexico
 This article is reprinted on the Carter Center s website with permission from the American Society of Tropical Medicine and Hygiene. Am. J. Trop. Med. Hyg., 83(1), 2010, pp. 15 20 doi:10.4269/ajtmh.2010.09-0626
This article is reprinted on the Carter Center s website with permission from the American Society of Tropical Medicine and Hygiene. Am. J. Trop. Med. Hyg., 83(1), 2010, pp. 15 20 doi:10.4269/ajtmh.2010.09-0626
Research Article Elimination of Onchocercavolvulus Transmission in the Huehuetenango Focus of Guatemala
 Journal of Parasitology Research Volume 2012, Article ID 638429, 9 pages doi:10.1155/2012/638429 Research Article Elimination of Onchocercavolvulus Transmission in the Huehuetenango Focus of Guatemala
Journal of Parasitology Research Volume 2012, Article ID 638429, 9 pages doi:10.1155/2012/638429 Research Article Elimination of Onchocercavolvulus Transmission in the Huehuetenango Focus of Guatemala
ONCHOCERCIASIS GUIDELINES FOR STOPPING MASS DRUG ADMINISTRATION AND VERIFYING ELIMINATION OF HUMAN ONCHOCERCIASIS CRITERIA AND PROCEDURES
 ONCHOCERCIASIS GUIDELINES FOR STOPPING MASS DRUG ADMINISTRATION AND VERIFYING ELIMINATION OF HUMAN ONCHOCERCIASIS CRITERIA AND PROCEDURES ONCHOCERCIASIS GUIDELINES FOR STOPPING MASS DRUG ADMINISTRATION
ONCHOCERCIASIS GUIDELINES FOR STOPPING MASS DRUG ADMINISTRATION AND VERIFYING ELIMINATION OF HUMAN ONCHOCERCIASIS CRITERIA AND PROCEDURES ONCHOCERCIASIS GUIDELINES FOR STOPPING MASS DRUG ADMINISTRATION
Interruption of Transmission of Onchocerca volvulus in the Southern Chiapas Focus, México
 Interruption of Transmission of Onchocerca volvulus in the Southern Chiapas Focus, México Mario A. Rodríguez-Pérez 1 *, Alfredo Domínguez-Vázquez 2, Thomas R. Unnasch 3, Hassan K. Hassan 3, Juan I. Arredondo-Jiménez
Interruption of Transmission of Onchocerca volvulus in the Southern Chiapas Focus, México Mario A. Rodríguez-Pérez 1 *, Alfredo Domínguez-Vázquez 2, Thomas R. Unnasch 3, Hassan K. Hassan 3, Juan I. Arredondo-Jiménez
Research Article Transmission of Onchocerciasis in Wadelai Focus of Northwestern Uganda Has Been Interrupted and the Disease Eliminated
 Hindawi Publishing Corporation Journal of Parasitology Research Volume 2012, Article ID 748540, 7 pages doi:10.1155/2012/748540 Research Article Transmission of Onchocerciasis in Wadelai Focus of Northwestern
Hindawi Publishing Corporation Journal of Parasitology Research Volume 2012, Article ID 748540, 7 pages doi:10.1155/2012/748540 Research Article Transmission of Onchocerciasis in Wadelai Focus of Northwestern
Annual Highlights. The accomplishments of the Mectizan Donation Program in its 29th year
 2015 Annual Highlights The accomplishments of the Mectizan Donation Program in its 29th year 10 Years Building Research and Laboratory Capacity in Cameroon: The Center for Research on Filariasis and Other
2015 Annual Highlights The accomplishments of the Mectizan Donation Program in its 29th year 10 Years Building Research and Laboratory Capacity in Cameroon: The Center for Research on Filariasis and Other
Partnering to tackle Neglected Tropical Diseases
 Partnering to tackle Neglected Tropical Diseases 2013 IEEE Global Humanitarian Technology Conference Tala de los Santos Diagnostics Group Leader 21 October 2013 NEGLECTED TROPICAL DISEASES The most important
Partnering to tackle Neglected Tropical Diseases 2013 IEEE Global Humanitarian Technology Conference Tala de los Santos Diagnostics Group Leader 21 October 2013 NEGLECTED TROPICAL DISEASES The most important
Interruption of Onchocerca volvulus Transmission in the Abu Hamed Focus, Sudan
 Accepted for Publication, Published online May 20, 2013; doi:10.4269/ajtmh.13-0112. The latest version is at http://ajtmh.org/cgi/doi/10.4269/ajtmh.13-0112 In order to provide our readers with timely access
Accepted for Publication, Published online May 20, 2013; doi:10.4269/ajtmh.13-0112. The latest version is at http://ajtmh.org/cgi/doi/10.4269/ajtmh.13-0112 In order to provide our readers with timely access
ONCHOCERCIASIS SEROSURVEILLANCE IN UGANDA
 This article is reprinted on the Carter Center s website with permission from the American Society of Tropical Medicine and Hygiene. Accepted for Publication, Published online December 16, 2013; doi:10.4269/ajtmh.13-0546.
This article is reprinted on the Carter Center s website with permission from the American Society of Tropical Medicine and Hygiene. Accepted for Publication, Published online December 16, 2013; doi:10.4269/ajtmh.13-0546.
Modelling the elimination of river blindness using long-term epidemiological and programmatic data from Mali and Senegal
 Modelling the elimination of river blindness using long-term epidemiological and programmatic data from Mali and Senegal Martin Walker, Wilma A Stolk, Matthew A Dixon, Christian Bottomley, Lamine Diawara,
Modelling the elimination of river blindness using long-term epidemiological and programmatic data from Mali and Senegal Martin Walker, Wilma A Stolk, Matthew A Dixon, Christian Bottomley, Lamine Diawara,
NTDs Slated for Elimination and Eradication
 NTDs Slated for Elimination and Eradication Institute of Medicine Forum on Microbial Threats The Causes and Impacts of Neglected Tropical and Zoonotic Diseases September 21-22, 2010 Washington, DC Donald
NTDs Slated for Elimination and Eradication Institute of Medicine Forum on Microbial Threats The Causes and Impacts of Neglected Tropical and Zoonotic Diseases September 21-22, 2010 Washington, DC Donald
BMC Medicine. Open Access. Abstract. BioMed Central
 BMC Medicine BioMed Central Research article Impact of long-term treatment of onchocerciasis with ivermectin in Ecuador: potential for elimination of infection Juan Carlos Vieira 1,2, Philip J Cooper*
BMC Medicine BioMed Central Research article Impact of long-term treatment of onchocerciasis with ivermectin in Ecuador: potential for elimination of infection Juan Carlos Vieira 1,2, Philip J Cooper*
Public Health Entomology
 Public Health Entomology Challenges and Next Steps Haroldo Bezerra PAHO/WHO Contents Background and challenges The proposal to Public Health Entomology in the Americas The TAG Public Health Entomology
Public Health Entomology Challenges and Next Steps Haroldo Bezerra PAHO/WHO Contents Background and challenges The proposal to Public Health Entomology in the Americas The TAG Public Health Entomology
Evidence of suppression of onchocerciasis transmission in the Venezuelan Amazonian focus
 Botto et al. Parasites & Vectors (216) 9:4 DOI 1.1186/s1371-16-1313-z RESEARCH Open Access Evidence of suppression of onchocerciasis transmission in the Venezuelan Amazonian focus Carlos Botto 1, María-Gloria
Botto et al. Parasites & Vectors (216) 9:4 DOI 1.1186/s1371-16-1313-z RESEARCH Open Access Evidence of suppression of onchocerciasis transmission in the Venezuelan Amazonian focus Carlos Botto 1, María-Gloria
Timeline of Carter Center Health Programs, 1982 to 2009
 1982 1985 1986 1991 1992 Timeline of Carter Center Health Programs, 1982 to 2009 is established by former U.S. President Jimmy Carter and his wife, Rosalynn, in partnership with Emory University. Groundbreaking
1982 1985 1986 1991 1992 Timeline of Carter Center Health Programs, 1982 to 2009 is established by former U.S. President Jimmy Carter and his wife, Rosalynn, in partnership with Emory University. Groundbreaking
MectizanTM Program Notes
 MectizanTM Program Notes C e l e b r a t i n g o u r 1 7 t h y e a r Issue 34 Mectizan Donation Program 2004 Controlling River Blindness: Achievements of a 15-Year Public-Private Partnership On 14 May
MectizanTM Program Notes C e l e b r a t i n g o u r 1 7 t h y e a r Issue 34 Mectizan Donation Program 2004 Controlling River Blindness: Achievements of a 15-Year Public-Private Partnership On 14 May
Lecture 5: Dr. Jabar Etaby
 Lecture 5: Dr. Jabar Etaby 1 2 Onchocerca volvulus (Blinding filariasis; river blindness) Microfilaria of Onchocerca volvulus, from skin snip from a patient seen in Guatemala. Wet preparation 3 Some important
Lecture 5: Dr. Jabar Etaby 1 2 Onchocerca volvulus (Blinding filariasis; river blindness) Microfilaria of Onchocerca volvulus, from skin snip from a patient seen in Guatemala. Wet preparation 3 Some important
Progress Toward Rubella and Congenital Rubella Syndrome Elimination in the Western Hemisphere,
 1 Introduction: Progress Toward Rubella and Congenital Rubella Syndrome Elimination in the Western Hemisphere, 2003-2008 1 Enhanced measles elimination activities in the Region of the Americas during the
1 Introduction: Progress Toward Rubella and Congenital Rubella Syndrome Elimination in the Western Hemisphere, 2003-2008 1 Enhanced measles elimination activities in the Region of the Americas during the
Guidelines for revising ivermectin treatment boundaries within the context of onchocerciasis elimination
 When and AFRICAN PROGRAMME FOR ONCHOCERCIASIS CONTROL World Health Organization Guidelines for revising ivermectin treatment boundaries within the context of onchocerciasis elimination AFRICAN PROGRAMME
When and AFRICAN PROGRAMME FOR ONCHOCERCIASIS CONTROL World Health Organization Guidelines for revising ivermectin treatment boundaries within the context of onchocerciasis elimination AFRICAN PROGRAMME
FIRST MEETING OF THE TECHNICAL ADVISORY GROUP ON PUBLIC HEALTH ENTOMOLOGY PAN AMERICAN HEALTH ORGANIZATION
 SUMMARY FIRST MEETING OF THE TECHNICAL ADVISORY GROUP ON PUBLIC HEALTH ENTOMOLOGY PAN AMERICAN HEALTH ORGANIZATION The first meeting of the Technical Advisory Group on Public Health Entomology (TAG PHE),
SUMMARY FIRST MEETING OF THE TECHNICAL ADVISORY GROUP ON PUBLIC HEALTH ENTOMOLOGY PAN AMERICAN HEALTH ORGANIZATION The first meeting of the Technical Advisory Group on Public Health Entomology (TAG PHE),
1,3,7 New Strategy for Malaria surveillance in elimination phases in China. Prof. Gao Qi
 1,3,7 New Strategy for Malaria surveillance in elimination phases in China Prof. Gao Qi Differences in control, elimination and post elimination phases Control Elimination Post Goal Reduce morbidity &
1,3,7 New Strategy for Malaria surveillance in elimination phases in China Prof. Gao Qi Differences in control, elimination and post elimination phases Control Elimination Post Goal Reduce morbidity &
Summary of the Twelfth Meeting of the ITFDE (II) May 6, 2008
 May 6, 2008") Summary of the Twelfth Meeting of the ITFDE (II) May 6, 2008 The Twelfth Meeting of the International Task Force for Disease Eradication (ITFDE) was convened at The Carter Center from 8:30am to 4:00pm
Summary of the Twelfth Meeting of the ITFDE (II) May 6, 2008 The Twelfth Meeting of the International Task Force for Disease Eradication (ITFDE) was convened at The Carter Center from 8:30am to 4:00pm
Wuchereria Morphology 10 cm 250 : m
 Wucheria bancrofti Brugia malayi Lymphatic filariasis Lymphatic Filariasis 119 million infected Elephantiasis Manifestation of lymphatic filariasis Morphology I Adult: White and thread-like. Two rings
Wucheria bancrofti Brugia malayi Lymphatic filariasis Lymphatic Filariasis 119 million infected Elephantiasis Manifestation of lymphatic filariasis Morphology I Adult: White and thread-like. Two rings
Elimination of onchocerciasis from Africa: possible?
 Review Elimination of onchocerciasis from Africa: possible? Charles D. Mackenzie 1, Mamoun M. Homeida 2, Adrian D. Hopkins 3 and Joni C. Lawrence 3 1 Department of Pathobiology and Diagnostic Investigation,
Review Elimination of onchocerciasis from Africa: possible? Charles D. Mackenzie 1, Mamoun M. Homeida 2, Adrian D. Hopkins 3 and Joni C. Lawrence 3 1 Department of Pathobiology and Diagnostic Investigation,
Investigations on the transmission potentials of Simulium damnosum and the risk of human Onchocerciasis in Kaduna metropolis, Kaduna State, Nigeria
 IJMBR 3 (2015) 1-5 ISSN 2053-180X Investigations on the transmission potentials of Simulium damnosum and the risk of human Onchocerciasis in Kaduna metropolis, Kaduna State, Nigeria Maikaje D. B.*, Dibal
IJMBR 3 (2015) 1-5 ISSN 2053-180X Investigations on the transmission potentials of Simulium damnosum and the risk of human Onchocerciasis in Kaduna metropolis, Kaduna State, Nigeria Maikaje D. B.*, Dibal
Summary of the Ninth Meeting of the ITFDE (II) May 12, 2006 (revised)
 May 12, 2006 (revised)") Summary of the Ninth Meeting of the ITFDE (II) May 12, 2006 (revised) The Ninth Meeting of the International Task Force for Disease Eradication (ITFDE) was convened at The Carter Center from 9:00am to
Summary of the Ninth Meeting of the ITFDE (II) May 12, 2006 (revised) The Ninth Meeting of the International Task Force for Disease Eradication (ITFDE) was convened at The Carter Center from 9:00am to
MAJOR ARTICLE. cost effectiveness; economic evaluation; ivermectin; onchocerciasis; treatment frequency.
 MAJOR ARTICLE Reaching the London Declaration on Neglected Tropical Diseases Goals for Onchocerciasis: An Economic Evaluation of Increasing the Frequency of Ivermectin Treatment in Africa Hugo C. Turner,
MAJOR ARTICLE Reaching the London Declaration on Neglected Tropical Diseases Goals for Onchocerciasis: An Economic Evaluation of Increasing the Frequency of Ivermectin Treatment in Africa Hugo C. Turner,
NTDs: update on the progress. Department of Control of Neglected Tropical Diseases
 NTDs: update on the progress Department of Control of Neglected Tropical Diseases WHO Department of control of Neglected Tropical Diseases Two main groups of diseases: IDM (Innovative and Intensified Diseases
NTDs: update on the progress Department of Control of Neglected Tropical Diseases WHO Department of control of Neglected Tropical Diseases Two main groups of diseases: IDM (Innovative and Intensified Diseases
FISCAL YEAR 2020 APPROPRIATIONS REQUESTS (updated ) USAID Global Health Programs (GHP) and State Department
 USAID Global Health Programs (GHP) and State Department") FISCAL YEAR 2020 APPROPRIATIONS REQUESTS (updated 2.13.19) Contact: Brian Massa, Senior Manager for Global Health Advocacy, Shot@Life (bmassa@unfoundation.org) USAID Global Health Programs (GHP) and State
FISCAL YEAR 2020 APPROPRIATIONS REQUESTS (updated 2.13.19) Contact: Brian Massa, Senior Manager for Global Health Advocacy, Shot@Life (bmassa@unfoundation.org) USAID Global Health Programs (GHP) and State
1. The World Bank-GAVI Partnership and the Purpose of the Review
 1. The World Bank-GAVI Partnership and the Purpose of the Review 1.1 The new World Bank Group strategy makes a strong case for an expanded World Bank Group role in global and regional dialogue and collective
1. The World Bank-GAVI Partnership and the Purpose of the Review 1.1 The new World Bank Group strategy makes a strong case for an expanded World Bank Group role in global and regional dialogue and collective
Translating Science to end HIV in Latin America and the Caribbean
 Translating Science to end HIV in Latin America and the Caribbean Mexico City, Mexico, 17 th - 18 th and 21 st April www.iasociety.org IAS 2017 post-conference workshop, 17 April 2018 Challenges for PrEP
Translating Science to end HIV in Latin America and the Caribbean Mexico City, Mexico, 17 th - 18 th and 21 st April www.iasociety.org IAS 2017 post-conference workshop, 17 April 2018 Challenges for PrEP
RESEARCH ON AIDS IN LATIN AMERICA AND THE CARIBBEAN
 ACHR 29/93.10 Original: Spanish RESEARCH ON AIDS IN LATIN AMERICA AND THE CARIBBEAN Division of Communicable Diseases Prevention and Control Program of AIDS and Sexually Transmitted Diseases July 1993.1..
ACHR 29/93.10 Original: Spanish RESEARCH ON AIDS IN LATIN AMERICA AND THE CARIBBEAN Division of Communicable Diseases Prevention and Control Program of AIDS and Sexually Transmitted Diseases July 1993.1..
Controlling Onchocerciasis: The Nigerian Experience
 ISPUB.COM The Internet Journal of Parasitic Diseases Volume 4 Number 1 N Njepuome, P Ogbu-Pearce, C Okoronkwo, M Igbe Citation N Njepuome, P Ogbu-Pearce, C Okoronkwo, M Igbe.. The Internet Journal of Parasitic
ISPUB.COM The Internet Journal of Parasitic Diseases Volume 4 Number 1 N Njepuome, P Ogbu-Pearce, C Okoronkwo, M Igbe Citation N Njepuome, P Ogbu-Pearce, C Okoronkwo, M Igbe.. The Internet Journal of Parasitic
Eliminating malaria in MEXICO
 COUNTRY BRIEFING Eliminating malaria in MEXICO Mexico has nearly eliminated Plasmodium falciparum and reduced malaria cases by 91 percent between 2 and 214 as it works to eliminate all remaining malaria
COUNTRY BRIEFING Eliminating malaria in MEXICO Mexico has nearly eliminated Plasmodium falciparum and reduced malaria cases by 91 percent between 2 and 214 as it works to eliminate all remaining malaria
Thank you for the opportunity to submit testimony on the Fiscal Year (FY) 2014 State
 2014 State") Drugs for Neglected Diseases initiative, North America Jennifer Katz, Policy Director March 2013 Testimony to the Subcommittee on State and Foreign Operations, Committee on Appropriations United States
Drugs for Neglected Diseases initiative, North America Jennifer Katz, Policy Director March 2013 Testimony to the Subcommittee on State and Foreign Operations, Committee on Appropriations United States
State of the Art in the Prevention and Control of Dengue in the Americas May, 2014 Washington DC, USA
 State of the Art in the Prevention and Control of Dengue in the Americas 28-29 May, 2014 Washington DC, USA Agenda Meeting on the State of the Art for the prevention and control of dengue in the Americas
State of the Art in the Prevention and Control of Dengue in the Americas 28-29 May, 2014 Washington DC, USA Agenda Meeting on the State of the Art for the prevention and control of dengue in the Americas
Accepted for Publication, Published online May 20, 2013; doi: /ajtmh
 Accepted for Publication, Published online May 20, 2013; doi:10.4269/ajtmh.13-0037. The latest version is at http://ajtmh.org/cgi/doi/10.4269/ajtmh.13-0037 In order to provide our readers with timely access
Accepted for Publication, Published online May 20, 2013; doi:10.4269/ajtmh.13-0037. The latest version is at http://ajtmh.org/cgi/doi/10.4269/ajtmh.13-0037 In order to provide our readers with timely access
MESA research grants 2014
 MESA research grants 2014 MESA operational research grant Principal investigator Mopping up and getting to zero: mapping residual malaria transmission for targeted response in urban Lusaka, Zambia. Daniel
MESA research grants 2014 MESA operational research grant Principal investigator Mopping up and getting to zero: mapping residual malaria transmission for targeted response in urban Lusaka, Zambia. Daniel
Does onchocerciasis transmission take place in hypoendemic areas? A study in North Region of Cameroon
 Reprinted peer reviewed version with permission from the Journal of Tropical Medicine and International Health, volume 15 no 5 pp645 652 May 2010. For more information on the Carter Center s work to fight
Reprinted peer reviewed version with permission from the Journal of Tropical Medicine and International Health, volume 15 no 5 pp645 652 May 2010. For more information on the Carter Center s work to fight
ONCHOCERCA INFECTION, ONCHOCERCOMATA, VISUAL ACUITY AND NUTRITIONAL STATUS IN CHILDREN IN AN ENDEMIC AREA OF SOUTH EASTERN NIGERIA.
 ONCHOCERCA INFECTION, ONCHOCERCOMATA, VISUAL ACUITY AND NUTRITIONAL STATUS IN CHILDREN IN AN ENDEMIC AREA OF SOUTH EASTERN NIGERIA. Abstract. The association between onchocerca infection, vision and nutritional
ONCHOCERCA INFECTION, ONCHOCERCOMATA, VISUAL ACUITY AND NUTRITIONAL STATUS IN CHILDREN IN AN ENDEMIC AREA OF SOUTH EASTERN NIGERIA. Abstract. The association between onchocerca infection, vision and nutritional
Summary 2004 Program Review for The Lions-Carter Center SightFirst River Blindness Programs Cameroon, Ethiopia, Nigeria, OEPA, Sudan, and Uganda 3-5
 Summary 2004 Program Review for The Lions-Carter Center SightFirst River Blindness Programs Cameroon, Ethiopia, Nigeria, OEPA, Sudan, and Uganda 3-5 March 2005 The Carter Center Atlanta, GA August 2005
Summary 2004 Program Review for The Lions-Carter Center SightFirst River Blindness Programs Cameroon, Ethiopia, Nigeria, OEPA, Sudan, and Uganda 3-5 March 2005 The Carter Center Atlanta, GA August 2005
Western Pacific Region Neglected Tropical Diseases News
 Western Pacific Region Neglected Tropical Diseases News 2015 Issue 1 Welcome to Western Pacific NTD News! This newsletter, to be published quarterly by the WHO Regional Office for the Western Pacific,
Western Pacific Region Neglected Tropical Diseases News 2015 Issue 1 Welcome to Western Pacific NTD News! This newsletter, to be published quarterly by the WHO Regional Office for the Western Pacific,
Reducing malaria in Solomon Islands: lessons for effective aid
 Reducing malaria in Solomon Islands: lessons for effective aid Executive Summary Camilla Burkot and Katherine Gilbert The burden of malaria in Solomon Islands, a small island state of approximately 653,500
Reducing malaria in Solomon Islands: lessons for effective aid Executive Summary Camilla Burkot and Katherine Gilbert The burden of malaria in Solomon Islands, a small island state of approximately 653,500
Report of the 1 st Meeting of the WHO Onchocerciasis Technical Advisory Subgroup. Varembé Conference Centre Geneva, Switzerland October 2017
 Report of the 1 st Meeting of the WHO Onchocerciasis Technical Advisory Subgroup Varembé Conference Centre Geneva, Switzerland 10-12 October 2017 WHO/CDS/NTD/PCT/2018.05 World Health Organization 2018
Report of the 1 st Meeting of the WHO Onchocerciasis Technical Advisory Subgroup Varembé Conference Centre Geneva, Switzerland 10-12 October 2017 WHO/CDS/NTD/PCT/2018.05 World Health Organization 2018
From river blindness control to elimination: bridge over troubled water
 Colebunders et al. Infectious Diseases of Poverty (2018) 7:21 https://doi.org/10.1186/s40249-018-0406-7 OPINION From river blindness control to elimination: bridge over troubled water Open Access Robert
Colebunders et al. Infectious Diseases of Poverty (2018) 7:21 https://doi.org/10.1186/s40249-018-0406-7 OPINION From river blindness control to elimination: bridge over troubled water Open Access Robert
PARASITOLOGY CASE HISTORY #13 (BLOOD PARASITES) (Lynne S. Garcia)
 (Lynne S. Garcia)") PARASITOLOGY CASE HISTORY #13 (BLOOD PARASITES) (Lynne S. Garcia) An epidemiologic survey was undertaken in a small town in Myanmar (Burma) endemic for lymphatic filariasis. Blood specimens were collected
PARASITOLOGY CASE HISTORY #13 (BLOOD PARASITES) (Lynne S. Garcia) An epidemiologic survey was undertaken in a small town in Myanmar (Burma) endemic for lymphatic filariasis. Blood specimens were collected
Ov-16 Meeting Notes Neglected Tropical Diseases Support Center Taskforce for Global Health Decatur, GA, USA May 2 3, 2016
 Ov-16 Meeting Notes Neglected Tropical Diseases Support Center Taskforce for Global Health Decatur, GA, USA May 2 3, 2016 Abbreviations APOC CI DBS DRC ELISA HRP IVM LIPS MDA MF NIH OCP OD OEPA OR PCR
Ov-16 Meeting Notes Neglected Tropical Diseases Support Center Taskforce for Global Health Decatur, GA, USA May 2 3, 2016 Abbreviations APOC CI DBS DRC ELISA HRP IVM LIPS MDA MF NIH OCP OD OEPA OR PCR
Texas Influenza Summary Report, Season (September 28, 2008 April 11, 2009)
") Texas Influenza Summary Report, 2008 2009 Season (September 28, 2008 April 11, 2009) Background Influenza and influenza-like illnesses (ILI) were last reportable by law in any county in Texas in 1993 (1).
Texas Influenza Summary Report, 2008 2009 Season (September 28, 2008 April 11, 2009) Background Influenza and influenza-like illnesses (ILI) were last reportable by law in any county in Texas in 1993 (1).
GUINEA-WORM DISEASE: COUNTDOWN TO ERADICATION
 GUINEA-WORM DISEASE: COUNTDOWN TO ERADICATION GUINEA-WORM DISEASE (DRACUNCULIASIS) Guinea-worm disease, also known as dracunculiasis, is on the verge of eradication. The World Health Organization (WHO)
GUINEA-WORM DISEASE: COUNTDOWN TO ERADICATION GUINEA-WORM DISEASE (DRACUNCULIASIS) Guinea-worm disease, also known as dracunculiasis, is on the verge of eradication. The World Health Organization (WHO)
Estimating the influenza disease burden in SARI sentinel hospitals using WHO method
 Estimating the influenza disease burden in SARI sentinel hospitals using WHO method Implementation experience in Bolivia, Colombia, Ecuador, and Honduras. Pablo Acosta MD. MPH. Ministry of Public Health
Estimating the influenza disease burden in SARI sentinel hospitals using WHO method Implementation experience in Bolivia, Colombia, Ecuador, and Honduras. Pablo Acosta MD. MPH. Ministry of Public Health
Since the last case of naturally occurring smallpox, in 1977,
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e review article global health Disease Eradication Donald R. Hopkins, M.D., M.P.H. From the Carter Center, Atlanta. Address reprint requests to Dr. Hopkins
T h e n e w e ngl a nd j o u r na l o f m e dic i n e review article global health Disease Eradication Donald R. Hopkins, M.D., M.P.H. From the Carter Center, Atlanta. Address reprint requests to Dr. Hopkins
B. PLAN OF ACTION FOR IMPLEMENTING THE GENDER EQUALITY POLICY
 Page 7 B. PLAN OF ACTION FOR IMPLEMENTING THE GENDER EQUALITY POLICY Background 1. Member States approved the Pan American Health Organization s (PAHO) Gender Equality Policy during the 46th Directing
Page 7 B. PLAN OF ACTION FOR IMPLEMENTING THE GENDER EQUALITY POLICY Background 1. Member States approved the Pan American Health Organization s (PAHO) Gender Equality Policy during the 46th Directing
MINISTERIAL CONFERENCE ON MALARIA
 WORLD HEALTH ORGANIZATION ORGANISATION MONDIALE DE LA SANTE EB91/4 25 November 1992 EXECUTIVE BOARD Ninety-first Session Provisional agenda item 4.2 MINISTERIAL CONFERENCE ON MALARIA Report by the Director-General
WORLD HEALTH ORGANIZATION ORGANISATION MONDIALE DE LA SANTE EB91/4 25 November 1992 EXECUTIVE BOARD Ninety-first Session Provisional agenda item 4.2 MINISTERIAL CONFERENCE ON MALARIA Report by the Director-General
Onchocerciasis among inhabitants of Ibarapa local government community of Oyo state, Nigeria
 Biomedical Research 2010; 21 (2): 174-178 Onchocerciasis among inhabitants of Ibarapa local government community of Oyo state, Nigeria 1 Akinboye, D.O.; 2 Okwong, E., 3 Ajiteru N., 4 Fawole O. 5 Agbolade,
Biomedical Research 2010; 21 (2): 174-178 Onchocerciasis among inhabitants of Ibarapa local government community of Oyo state, Nigeria 1 Akinboye, D.O.; 2 Okwong, E., 3 Ajiteru N., 4 Fawole O. 5 Agbolade,
ANONYMOUS UNLINKED STUDY OF THE PREVALENCE OF ANTI- HIV ANTIBODIES IN MOTHERS OF LIVE NEWBORNS FROM 6 AUTONOMOUS REGIONS
 SECRETARÍA GENERAL DE SANIDAD DIRECCIÓN GENERAL DE SALUD PÚBLICA Y SANIDAD EXTERIOR ANONYMOUS UNLINKED STUDY OF THE PREVALENCE OF ANTI- HIV ANTIBODIES IN MOTHERS OF LIVE NEWBORNS FROM 6 AUTONOMOUS REGIONS
SECRETARÍA GENERAL DE SANIDAD DIRECCIÓN GENERAL DE SALUD PÚBLICA Y SANIDAD EXTERIOR ANONYMOUS UNLINKED STUDY OF THE PREVALENCE OF ANTI- HIV ANTIBODIES IN MOTHERS OF LIVE NEWBORNS FROM 6 AUTONOMOUS REGIONS
Is onchocerciasis elimination in Africa feasible by 2025: a perspective based on lessons learnt from the African control programmes
 Dadzie et al. Infectious Diseases of Poverty (2018) 7:63 https://doi.org/10.1186/s40249-018-0446-z OPINION Open Access Is onchocerciasis elimination in Africa feasible by 2025: a perspective based on lessons
Dadzie et al. Infectious Diseases of Poverty (2018) 7:63 https://doi.org/10.1186/s40249-018-0446-z OPINION Open Access Is onchocerciasis elimination in Africa feasible by 2025: a perspective based on lessons
Technical Advisor. JICA Nicaragua Chagas Disease Control Project Nicaragua
 Kota Yoshioka is currently working as technical advisor for Chagas disease control project which isrun by Japan International Cooperation Agency (JICA) and the Ministry of Health of Nicaragua (2009-2014).
Kota Yoshioka is currently working as technical advisor for Chagas disease control project which isrun by Japan International Cooperation Agency (JICA) and the Ministry of Health of Nicaragua (2009-2014).
Summary 2003 Program Review for The Carter Center/Lions SightFirst River Blindness Programs Cameroon, Ethiopia, Nigeria, OEPA, Sudan, and Uganda 1-3
 Summary 2003 Program Review for The Carter Center/Lions SightFirst River Blindness Programs Cameroon, Ethiopia, Nigeria, OEPA, Sudan, and Uganda 1-3 March 2004 The Carter Center Atlanta, GA July 12, 2004
Summary 2003 Program Review for The Carter Center/Lions SightFirst River Blindness Programs Cameroon, Ethiopia, Nigeria, OEPA, Sudan, and Uganda 1-3 March 2004 The Carter Center Atlanta, GA July 12, 2004
Analysis of the demand for a malaria vaccine: outcome of a consultative study in eight countries
 Briefing Document: National decision-making framework for malaria vaccines Analysis of the demand for a malaria vaccine: outcome of a consultative study in eight countries This is one of seven briefing
Briefing Document: National decision-making framework for malaria vaccines Analysis of the demand for a malaria vaccine: outcome of a consultative study in eight countries This is one of seven briefing
Community Directed Intervention for Onchocerciasis Control and Public Health Interventions
 Community Directed Intervention for Onchocerciasis Control and Public Health Interventions USF College of Public Health Tampa Florida, April 9, 2010 Dr. Boakye Boatin 11 University of Medical Sciences
Community Directed Intervention for Onchocerciasis Control and Public Health Interventions USF College of Public Health Tampa Florida, April 9, 2010 Dr. Boakye Boatin 11 University of Medical Sciences
Steady Ready Go! teady Ready Go. Every day, young people aged years become infected with. Preventing HIV/AIDS in young people
 teady Ready Go y Ready Preventing HIV/AIDS in young people Go Steady Ready Go! Evidence from developing countries on what works A summary of the WHO Technical Report Series No 938 Every day, 5 000 young
teady Ready Go y Ready Preventing HIV/AIDS in young people Go Steady Ready Go! Evidence from developing countries on what works A summary of the WHO Technical Report Series No 938 Every day, 5 000 young
Regional Update EW 31, 2014 Influenza and other respiratory viruses (August 12, 2014)
") Regional Update EW 31, 2014 Influenza and other respiratory viruses (August 12, 2014) PAHO interactive influenza data: Uhttp://ais.paho.org/phip/viz/ed_flu.asp Influenza Regional Reports: www.paho.org/influenzareports
Regional Update EW 31, 2014 Influenza and other respiratory viruses (August 12, 2014) PAHO interactive influenza data: Uhttp://ais.paho.org/phip/viz/ed_flu.asp Influenza Regional Reports: www.paho.org/influenzareports
Yellow fever. Key facts
 From: http://www.who.int/en/news-room/fact-sheets/detail/yellow-fever WHO/E. Soteras Jalil Yellow fever 14 March 2018 Key facts Yellow fever is an acute viral haemorrhagic disease transmitted by infected
From: http://www.who.int/en/news-room/fact-sheets/detail/yellow-fever WHO/E. Soteras Jalil Yellow fever 14 March 2018 Key facts Yellow fever is an acute viral haemorrhagic disease transmitted by infected
Accelerated Rubella Control and Congenital Rubella Syndrome Prevention Strengthen Measles Eradication: The Costa Rican Experience
 SUPPLEMENT ARTICLE Accelerated Rubella Control and Congenital Rubella Syndrome Prevention Strengthen Measles Eradication: The Costa Rican Experience Ana Morice, 1 Xinia Carvajal, 1 Mario León, 2 Vicenta
SUPPLEMENT ARTICLE Accelerated Rubella Control and Congenital Rubella Syndrome Prevention Strengthen Measles Eradication: The Costa Rican Experience Ana Morice, 1 Xinia Carvajal, 1 Mario León, 2 Vicenta
Eye of the Eagle THE CARTER CENTER
 Eye of the Eagle Volume 9, Number 1 THE CARTER CENTER January 2008 Beginning of a New Era IACO 2007 Highlights Status of Transmission The Onchocerciasis Elimination Program of the Americas (OEPA) regional
Eye of the Eagle Volume 9, Number 1 THE CARTER CENTER January 2008 Beginning of a New Era IACO 2007 Highlights Status of Transmission The Onchocerciasis Elimination Program of the Americas (OEPA) regional
Regional Update Pandemic (H1N1) 2009 (May 24, h GMT; 12 h EST)
 2009 (May 24, h GMT; 12 h EST)") Regional Update Pandemic (H1N1) 2009 (May 24, 2010-17 h GMT; 12 h EST) The information contained within this update is obtained from data provided by Ministries of Health of Member States and National
Regional Update Pandemic (H1N1) 2009 (May 24, 2010-17 h GMT; 12 h EST) The information contained within this update is obtained from data provided by Ministries of Health of Member States and National
A framework for malaria elimination
 A framework for malaria elimination What s new? Dr Pedro Alonso, GMP Director Rationale for new malaria elimination framework The malaria landscape has changed dramatically since 2007 - Increased funding
A framework for malaria elimination What s new? Dr Pedro Alonso, GMP Director Rationale for new malaria elimination framework The malaria landscape has changed dramatically since 2007 - Increased funding
FIRST CONFIRMED CASE OF IMPORTED ZIKA VIRUS IN HOUSTON, TEXAS. Preventing Transmission
 FIRST CONFIRMED CASE OF IMPORTED ZIKA VIRUS IN HOUSTON, TEXAS Preventing Transmission Objectives Discuss the epidemiology of Zika virus Describe the Zika case investigation of the first confirmed case
FIRST CONFIRMED CASE OF IMPORTED ZIKA VIRUS IN HOUSTON, TEXAS Preventing Transmission Objectives Discuss the epidemiology of Zika virus Describe the Zika case investigation of the first confirmed case
THE GLOBAL BURDEN OF ONCHOCERCIASIS IN 1990
 1 THE GLOBAL BURDEN OF ONCHOCERCIASIS IN 1990 J.H.F. REMME 1 World Health Organization, Geneva, 2004 This paper documents the methods and data sources used for the estimation of the global burden of onchocerciasis
1 THE GLOBAL BURDEN OF ONCHOCERCIASIS IN 1990 J.H.F. REMME 1 World Health Organization, Geneva, 2004 This paper documents the methods and data sources used for the estimation of the global burden of onchocerciasis
Regional Approaches to NTD Control in the Americas
 Regional Approaches to NTD Control in the Americas Steven K. Ault Parasitic and Neglected Diseases Program Area of Health Surveillance and Disease Control and Prevention PAHO/WHO Workshop The Causes and
Regional Approaches to NTD Control in the Americas Steven K. Ault Parasitic and Neglected Diseases Program Area of Health Surveillance and Disease Control and Prevention PAHO/WHO Workshop The Causes and
My Fellowship Achievements
 Public Health Fellowship Program Field Epidemiology Track My Fellowship Achievements David W. Oguttu, BBLT, Mzoo/PAR Fellow, Cohort 2015 Mandate Host Site: Tororo District Health Office Coordination, planning,
Public Health Fellowship Program Field Epidemiology Track My Fellowship Achievements David W. Oguttu, BBLT, Mzoo/PAR Fellow, Cohort 2015 Mandate Host Site: Tororo District Health Office Coordination, planning,
DIAGNOSTIC SLIDE SESSION CASE 10
 DIAGNOSTIC SLIDE SESSION CASE 10 B.K. Kleinschmidt-DeMasters, MD Disclosures: I am not a trainee Caterina made me do this CASE 2016-10: : The patient is a 5-year-old girl with Down syndrome, obstructive
DIAGNOSTIC SLIDE SESSION CASE 10 B.K. Kleinschmidt-DeMasters, MD Disclosures: I am not a trainee Caterina made me do this CASE 2016-10: : The patient is a 5-year-old girl with Down syndrome, obstructive
Author(s) Takahashi, H. Citation. Issue Date Right. Hygiene.
 Takahashi, H. Citation. Issue Date Right. Hygiene.") NAOSITE: Nagasaki University's Ac Title Author(s) Citation Onchocerciasis in San Vicente Pacay Tada, Isao; Aoki, Yoshiki; Rimola, J. O.; Recinos, C. M.; Sato, S.; Go Takahashi, H. American Journal of Tropical
NAOSITE: Nagasaki University's Ac Title Author(s) Citation Onchocerciasis in San Vicente Pacay Tada, Isao; Aoki, Yoshiki; Rimola, J. O.; Recinos, C. M.; Sato, S.; Go Takahashi, H. American Journal of Tropical
Regional Update Influenza (August 16, h GMT; 12 h EST)
") Regional Update Influenza (August 16, 21-17 h GMT; 12 h EST) The information contained within this update is obtained from data provided by Ministries of Health of Member States and National Influenza
Regional Update Influenza (August 16, 21-17 h GMT; 12 h EST) The information contained within this update is obtained from data provided by Ministries of Health of Member States and National Influenza
16 th session of the Working Group of Experts on People of African Descent Salle XXI, Palais des Nations, Geneva 30 March 2 April 2015
 16 th session of the Working Group of Experts on People of African Descent Salle XXI, Palais des Nations, Geneva 30 March 2 April 2015 Statement on behalf of the Pan American Health Organization/ World
16 th session of the Working Group of Experts on People of African Descent Salle XXI, Palais des Nations, Geneva 30 March 2 April 2015 Statement on behalf of the Pan American Health Organization/ World
CE150/INF/6 (Eng.) Annex A A. SOCIAL DETERMINANTS OF HEALTH. Introduction
 Annex A A. SOCIAL DETERMINANTS OF HEALTH. Introduction") Annex A - 2 - A. SOCIAL DETERMINANTS OF HEALTH Introduction 1. World Health Assembly (WHA) Resolution WHA62.14 (2009), Reducing health inequities through action on the social determinants of health, urges
Annex A - 2 - A. SOCIAL DETERMINANTS OF HEALTH Introduction 1. World Health Assembly (WHA) Resolution WHA62.14 (2009), Reducing health inequities through action on the social determinants of health, urges
International PolioPlus Committee PolioPlus Facts and Figures June Rotary s financial contribution to the polio eradication effort:
 International PolioPlus Committee PolioPlus Facts and Figures June 2018 1. The goal of the PolioPlus program: The goal of the PolioPlus program is the global certification of polio eradication. By eradication,
International PolioPlus Committee PolioPlus Facts and Figures June 2018 1. The goal of the PolioPlus program: The goal of the PolioPlus program is the global certification of polio eradication. By eradication,
Copenhagen, Denmark, September August Malaria
 Regional Committee for Europe 64th session EUR/RC64/Inf.Doc./5 Copenhagen, Denmark, 15 18 September 2014 21 August 2014 140602 Provisional agenda item 3 ORIGINAL: ENGLISH Malaria Following the support
Regional Committee for Europe 64th session EUR/RC64/Inf.Doc./5 Copenhagen, Denmark, 15 18 September 2014 21 August 2014 140602 Provisional agenda item 3 ORIGINAL: ENGLISH Malaria Following the support
Policy and technical topics: Selected neglected tropical diseases targeted for elimination: kala-azar, leprosy, yaws, filariasis and schistosomiasis
 REGIONAL COMMITTEE Provisional Agenda item 8.3 Sixty-eighth Session SEA/RC68/12 Dili, Timor-Leste 7 11 September 2015 21 July 2015 Policy and technical topics: Selected neglected tropical diseases targeted
REGIONAL COMMITTEE Provisional Agenda item 8.3 Sixty-eighth Session SEA/RC68/12 Dili, Timor-Leste 7 11 September 2015 21 July 2015 Policy and technical topics: Selected neglected tropical diseases targeted
Resolution adopted by the General Assembly. [without reference to a Main Committee (A/62/L.39 and Add.1)]
![Resolution adopted by the General Assembly. [without reference to a Main Committee (A/62/L.39 and Add.1)]](/thumbs/96/127242235.jpg "Resolution adopted by the General Assembly. [without reference to a Main Committee (A/62/L.39 and Add.1)]") United Nations General Assembly Distr.: General 7 March 2008 Sixty-second session Agenda item 47 Resolution adopted by the General Assembly [without reference to a Main Committee (A/62/L.39 and Add.1)]
United Nations General Assembly Distr.: General 7 March 2008 Sixty-second session Agenda item 47 Resolution adopted by the General Assembly [without reference to a Main Committee (A/62/L.39 and Add.1)]
Impact of a Community-Based Lymphedema Management Program on Episodes of Adenolymphangitis (ADLA) and Lymphedema Progression - Odisha State, India
 and Lymphedema Progression - Odisha State, India") Impact of a Community-Based Lymphedema Management Program on Episodes of Adenolymphangitis (ADLA) and Lymphedema Progression - Odisha State, India Katherine E. Mues, Emory University Michael Deming, Emory
Impact of a Community-Based Lymphedema Management Program on Episodes of Adenolymphangitis (ADLA) and Lymphedema Progression - Odisha State, India Katherine E. Mues, Emory University Michael Deming, Emory
Ministry of Children and Youth Services. Follow-up to VFM Section 3.01, 2013 Annual Report RECOMMENDATION STATUS OVERVIEW
 Chapter 4 Section 4.01 Ministry of Children and Youth Services Autism Services and Supports for Children Follow-up to VFM Section 3.01, 2013 Annual Report RECOMMENDATION STATUS OVERVIEW # of Status of
Chapter 4 Section 4.01 Ministry of Children and Youth Services Autism Services and Supports for Children Follow-up to VFM Section 3.01, 2013 Annual Report RECOMMENDATION STATUS OVERVIEW # of Status of
Evidence Review Group on MDA, MSAT and FSAT Malaria Policy Advisory Committee Geneva, Switzerland September 2015
 Evidence Review Group on MDA, MSAT and FSAT Malaria Policy Advisory Committee Geneva, Switzerland 16-18 September 2015 Kevin Marsh Chairperson of the Evidence Review Group 1 Outline of the Presentation
Evidence Review Group on MDA, MSAT and FSAT Malaria Policy Advisory Committee Geneva, Switzerland 16-18 September 2015 Kevin Marsh Chairperson of the Evidence Review Group 1 Outline of the Presentation
Influenza Vaccine Use In the Americas
 Influenza Vaccine Use In the Americas Network for Evaluation of Influenza Vaccine Effectiveness REVELAC-i Alba Maria Ropero-Alvarez Comprehensive Family Immunization Unit PAHO/FGL/IM Global Vaccine and
Influenza Vaccine Use In the Americas Network for Evaluation of Influenza Vaccine Effectiveness REVELAC-i Alba Maria Ropero-Alvarez Comprehensive Family Immunization Unit PAHO/FGL/IM Global Vaccine and
Facts & Figures. HIV Estimates
 Facts & Figures HIV Estimates - 2003 Globally, the HIV sentinel surveillance system has been recognised as an optimal mechanism to monitor trends of HIV infection in specific high-risk groups as well as
Facts & Figures HIV Estimates - 2003 Globally, the HIV sentinel surveillance system has been recognised as an optimal mechanism to monitor trends of HIV infection in specific high-risk groups as well as
GUATEMALA S FAMILY PLANNING TRANSITION Successes, Challenges, and Lessons Learned for Transitioning Countries
 GUATEMALA S FAMILY PLANNING TRANSITION Successes, Challenges, and Lessons Learned for Transitioning Countries ATTAINING SUSTAINABLE FINANCING FOR FAMILY PLANNING IN SUB-SAHARAN AFRICA ACCRA, JANUARY 2018
GUATEMALA S FAMILY PLANNING TRANSITION Successes, Challenges, and Lessons Learned for Transitioning Countries ATTAINING SUSTAINABLE FINANCING FOR FAMILY PLANNING IN SUB-SAHARAN AFRICA ACCRA, JANUARY 2018
Ministry of Health and Medical Services Solomon Islands. Dengue Outbreak: External Sitrep No. 3. From Epidemiological Week 33-41, 2016
 Ministry of Health and Medical Services Solomon Islands Dengue Outbreak: External Sitrep No. 3 From Epidemiological Week 33-41, 2016 Summary Since August 2016, an unusual increase in dengue-like illness,
Ministry of Health and Medical Services Solomon Islands Dengue Outbreak: External Sitrep No. 3 From Epidemiological Week 33-41, 2016 Summary Since August 2016, an unusual increase in dengue-like illness,
REVELAC-i: Progress in measuring influenza vaccine effectiveness in Latin America and way forward
 REVELAC-i: Progress in measuring influenza vaccine effectiveness in Latin America and way forward SARInet annual meeting, Punta Cana, May 23 2017 Nathalie El Omeiri On behalf of REVELAC-i network, Alba
REVELAC-i: Progress in measuring influenza vaccine effectiveness in Latin America and way forward SARInet annual meeting, Punta Cana, May 23 2017 Nathalie El Omeiri On behalf of REVELAC-i network, Alba
THE BUTTERFLY TREE MALARIA PREVENTION INITIATIVE. Introduction
 THE BUTTERFLY TREE MALARIA PREVENTION INITIATIVE Introduction Globally malaria is the biggest killer of man Every 60 seconds a child dies from malaria An estimated 3.3 billion people are at risk of malaria
THE BUTTERFLY TREE MALARIA PREVENTION INITIATIVE Introduction Globally malaria is the biggest killer of man Every 60 seconds a child dies from malaria An estimated 3.3 billion people are at risk of malaria
Rift Valley Fever RVF. Enhancing Safe Inter-Regional Livestock Trade Dubai, United Arab Emirates June 13-16, 2011
 Rift Valley Fever RVF Enhancing Safe Inter-Regional Livestock Trade Dubai, United Arab Emirates June 13-16, 2011 Definition Rift valley fever (RVF) is an acute febrile arthropod-borne zoonotic disease.
Rift Valley Fever RVF Enhancing Safe Inter-Regional Livestock Trade Dubai, United Arab Emirates June 13-16, 2011 Definition Rift valley fever (RVF) is an acute febrile arthropod-borne zoonotic disease.
Projected number of people with onchocerciasisloiasis co-infection in Africa,
 Projected number of people with onchocerciasisloiasis co-infection in Africa, 1995-2025 Natalie Vinkeles Melchers, Afework H Tekle, Luc E Coffeng, Sébastien DS Pion, Honorat GM Zouré, Belén Pedrique, Michel
Projected number of people with onchocerciasisloiasis co-infection in Africa, 1995-2025 Natalie Vinkeles Melchers, Afework H Tekle, Luc E Coffeng, Sébastien DS Pion, Honorat GM Zouré, Belén Pedrique, Michel
Clinical Manifestations of Onchocerciasis in Imeri: an Endemic Community in Nigeria. *Tel:
 Clinical Manifestations of Onchocerciasis in Imeri: an Endemic Community in Nigeria * 1 OJ Afolabi, 2 CE Okaka, 1 MO Oniya 1 Department of Biology, Federal University of Technology Akure, Ondo State, Nigeria
Clinical Manifestations of Onchocerciasis in Imeri: an Endemic Community in Nigeria * 1 OJ Afolabi, 2 CE Okaka, 1 MO Oniya 1 Department of Biology, Federal University of Technology Akure, Ondo State, Nigeria
WASH Integration into Ethiopia's Trachoma Action Plan
 WASH Integration into Ethiopia's Trachoma Action Plan WASH Integration in Ethiopia s Trachoma Action Plan A Case Study of Policy Integration Although WASH plays a key part in the WHO-endorsed strategy
WASH Integration into Ethiopia's Trachoma Action Plan WASH Integration in Ethiopia s Trachoma Action Plan A Case Study of Policy Integration Although WASH plays a key part in the WHO-endorsed strategy
Cholera. Report by the Secretariat
 EXECUTIVE BOARD EB128/13 128th Session 9 December 2010 Provisional agenda item 4.10 Cholera Report by the Secretariat 1. In May 2010, the Executive Board at its 127th session considered a report on cholera
EXECUTIVE BOARD EB128/13 128th Session 9 December 2010 Provisional agenda item 4.10 Cholera Report by the Secretariat 1. In May 2010, the Executive Board at its 127th session considered a report on cholera
Global dengue situation and strategy for prevention and control ALERT AND RESPONSE OPERATIONS
 Global dengue situation and strategy for prevention and control 2012-2020 ALERT AND RESPONSE OPERATIONS Global Dengue Risk 2012. Simmons CP et al. N Engl J Med 2012;366:1423-1432 Average /number of Dengue
Global dengue situation and strategy for prevention and control 2012-2020 ALERT AND RESPONSE OPERATIONS Global Dengue Risk 2012. Simmons CP et al. N Engl J Med 2012;366:1423-1432 Average /number of Dengue
_flu.asp. States. North. The Caribbean and (Cuba, South. South. B was observed.
 North America: Influenza activity remained low in the sub-region with co-circulation of influenza A(H1N1)pdm09, A(H3N2) and influenza B. In the United States, no new humann infections with influenza A(H3N2)
North America: Influenza activity remained low in the sub-region with co-circulation of influenza A(H1N1)pdm09, A(H3N2) and influenza B. In the United States, no new humann infections with influenza A(H3N2)
Chagas Disease in the Americas: Impacts and Opportunities for Control
 Chagas Disease in the Americas: Impacts and Opportunities for Control Rick Tarleton Center for Tropical and Emerging Global Diseases University of Georgia The Chagas Disease Foundation Trypanosoma cruzi
Chagas Disease in the Americas: Impacts and Opportunities for Control Rick Tarleton Center for Tropical and Emerging Global Diseases University of Georgia The Chagas Disease Foundation Trypanosoma cruzi
DOWNLOAD OR READ : TROPICAL INFECTIOUS DISEASES SECOND EDITION PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : TROPICAL INFECTIOUS DISEASES SECOND EDITION PDF EBOOK EPUB MOBI Page 1 Page 2 tropical infectious diseases second edition tropical infectious diseases second pdf tropical infectious
DOWNLOAD OR READ : TROPICAL INFECTIOUS DISEASES SECOND EDITION PDF EBOOK EPUB MOBI Page 1 Page 2 tropical infectious diseases second edition tropical infectious diseases second pdf tropical infectious
Eye of the Eagle THE CARTER CENTER
 Eye of the Eagle Volume 13, Number 1 THE CARTER CENTER February 2012 IACO 2011 Marks Beginning of End for River Blindness in the Americas The Carter Center led Onchocerciasis Elimination Program for the
Eye of the Eagle Volume 13, Number 1 THE CARTER CENTER February 2012 IACO 2011 Marks Beginning of End for River Blindness in the Americas The Carter Center led Onchocerciasis Elimination Program for the
Analytical evaluation of Malaria Research Papers in MEDLINE & SCI during the period of &
 Panigrahi, Mukherjee and Srivastava 1 Analytical evaluation of Malaria Research Papers in & during the period of 1986-9 & 21-5. Panigrahi BK *, Mukherjee T and Srivastava D 28 July 28 Abstract: Vector-borne
Panigrahi, Mukherjee and Srivastava 1 Analytical evaluation of Malaria Research Papers in & during the period of 1986-9 & 21-5. Panigrahi BK *, Mukherjee T and Srivastava D 28 July 28 Abstract: Vector-borne