Learning Objectives. Epidemiology 5/3/2013. Treponema pallidum Diagnosis, Treatment and Prevention. Anne Rompalo, MD, ScM Professor of Medicine
|
|
|
- Tiffany Mills
- 6 years ago
- Views:
Transcription


1 Treponema pallidum Diagnosis, Treatment and Prevention Anne Rompalo, MD, ScM Professor of Medicine Learning Objectives Describe the epidemiology of syphilis in the U.S.Describe the pathogenesis of Treponema pallidum. Discuss the clinical manifestations of syphilis. Identify common methods used in the diagnosis of syphilis. List the CDC recommended treatment regimens for syphilis. Summarize appropriate prevention counseling messages for patients with syphilis. Describe public health measures for the prevention of syphilis Epidemiology 1

2 2011 Fig 36. SR 2011 Fig 37. SR 2011 Fig 40. SR 5/3/2013 Syphilis Reported Cases by Stage of Infection, United States, Primary and Secondary Syphilis by Sex and Sexual Behavior, 33 Areas*, *32 states and Washington, DC reported sex of partner data for 70% of cases of P&S syphilis for each year during MSM=men who have sex with men; MSW=men who have sex with women only. Primary and Secondary Syphilis Rates by State, United States and Outlying Areas, 2011 NOTE: The total rate of primary and secondary syphilis for the United States and outlying areas (Guam, Puerto Rico, and Virgin Islands) was 4.5 per 100,000 population. 2
 of 3,142 counties in the United States reported no cases of primary and secondary syphilis.")
3 2011 Fig 41. SR 2011 Fig 42. SR 2011 Fig 45. SR 5/3/2013 Primary and Secondary Syphilis Rates by County, United States, 2011 NOTE: In 2011, 2,154 (68.5%) of 3,142 counties in the United States reported no cases of primary and secondary syphilis. Primary and Secondary Syphilis Rates by Age and Sex, United States, 2011 Primary and Secondary Syphilis Rates by Race/Ethnicity, United States,

4 2011 Fig 46. SR 2011 Fig 47. SR 2011 Fig 48. SR 5/3/2013 Primary and Secondary Syphilis Reported Cases* by Stage, Sex, and Sexual Behavior, United States, 2011 *Of the reported male cases of primary and secondary syphilis, 17.0% were missing sex of sex partner information. MSM=men who have sex with men; MSW=men who have sex with women only. Primary and Secondary Syphilis Reported Cases* by Sex, Sexual Behavior, and Race/Ethnicity, United States, 2011 *Of the reported male cases of primary and secondary syphilis, 17.0% were missing sex of sex partner information; 2.4% of sex partner data were missing race/ethnicity data. MSW=men who have sex with women only; MSM=men who have sex with men; Primary and Secondary Syphilis Reported Cases by Reporting Source and Sex, United States,

5 2011 Fig 49. SR 2011 Fig 50. SR 5/3/2013 Primary and Secondary Syphilis Percentage of Reported Cases* by Sex, Sexual Behavior, and Selected Reporting Sources, 2011 *Of the reported male cases of primary and secondary syphilis, 17.0% were missing sex of sex partner information; 3.9% of sex partner data were missing race/ethnicity data. HMO=health maintenance organization; MSW=men who have sex with women only; MSM=men who have sex with men Congenital Syphilis Reported Cases Among Infants by Year of Birth and Rates of Primary and Secondary Syphilis Among Women, United States, * CS=congenital syphilis; P&S=primary and secondary syphilis. Syphilis Clinical Manifestations 5
6 Clinical Stages of Syphilis 50% Exposure 1 o 2 o Early Late 3 o 33% 50% < 1 year > 1 year 30% 9 90 days 1 6 wks 1 6 wks STOP OR 5 30 years Infectious Syphilis: Transmission Major routes: sexual and in utero from infected pregnant women to her fetus (vertical) Risk of infection after 1 exposure: 40% Index patient is most contagious to sexual partners during 1 o and 2 o stage, less so in early latent stage 6
7 Syphilis: Pathogenesis Penetration: Enters via skin or mucus membranes Divides every hours Smaller the inoculum, longer the incubation period (9 90 days) Dissemination: Before clinical signs/symptoms, it travels via lymphatic system to regional lymph nodes and then through body via blood Syphilis: Pathogenesis Some spirochetes lodge at entry site, proliferate, sensitize lymphocytes and activate macrophages Primary lesion (chancre) results at this site of inoculation about 3 6 weeks after initial infection Chancre heals spontaneously, usually without scar, within 3 8 weeks Secondary syphilis T. pallidum can traverse the tight junctions between endothelial cells to enter the perivascular spaces, where large number of treponemes and immune cells accumulate It can induce production of MMP 1, which degrades collagen and may facilitate acccess to and egress from the bloodstream, resulting in systemic spread Usually within 3 months of infection, symptoms of secondary syphilis appear 7



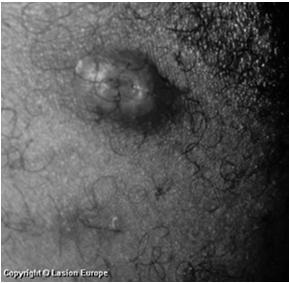
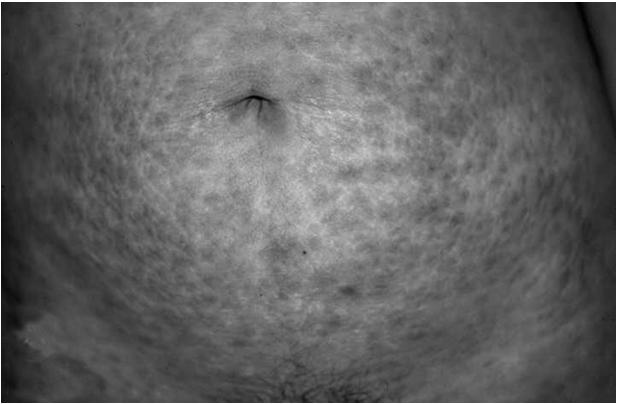
8 Clinical Spectrum of Secondary syphilis Syphilis: Pathogenesis Eventually, the host suppresses the secondary infection enough so that no lesions are clinically apparent This is latency; 60 85% of patients remain asymptomatic Some progress to tertiary stage in 1 20 years Immunity is present with chronic infection but lost after treatment Primary syphilis Chancre: appears 2 3 wks after exposure (range 3 90 days) local lesion at site of inoculation typically painless, indurated, clean base 25% have multiple lesions Regional adenopathy: classically rubbery, painless, bilateral 8





9 More primary syphilis Secondary Syphilis Onset 4 10 weeks following 1 o and may overlap with it Rash: macular, papular, pustular, combination; usually nonpruritis 60% or more involve palms and soles Mucus patches (5 30%) flat patches in mouth, pharynx, genitals More secondary syphilis Condylomata lata (5 25%) heaped, moist wart like papules in warm intertriginous areas teaming with spirochetes Constitutional symptoms: malaise, headache, slight fever, myalgia liver/kidney involvement patchy alopecia 9



10 More Secondary Syphilis Latent syphilis No clinical manifestations Only evidence is positive serology Early latent syphilis: <1 year duration Late latent syphilis: >1 year duration After 4 years patient is noninfectious; resistant to reinfection if not treated Tertiary syphilis Late benign syphilis: gummatous lesions in skeletal, spinal and mucosal areas, eye and viscera average onset 4 12 years Cardiovascular syphilis: endarteritis of aortic vasovasorum present as aortic aneurysm, Aortic insufficiency average onset 15 years 10




11 More tertiary syphilis Neurosyphilis CNS involvement occurs early Clinical manifestations may appear early or late and include: Asymptomatic neurosyphilis, meningeal involvement (acute meningitis), meningovascular involvement, choreoretinitis, parenchymatous disease (paresis, tabes dorsalis, optic atrophy) Congenital syphilis Vertical transmission can occur at any time during pregnancy and at any stage Among women with syphilis, perinatal transmission occurs in: 50% with 1 o and 2 o stages 40% with early latent 10% with late latent 10% with tertiary 11


12 Adverse Fetal Outcomes among Pregnant Women with Untreated Syphilis 20% of children born to these mothers will be normal Intrauterine growth restriction Stillbirth (4%) Neonatal death Preterm birth Congenital infection and anomalies Primary syphilis: Male chancre Primary chancre: Females 12



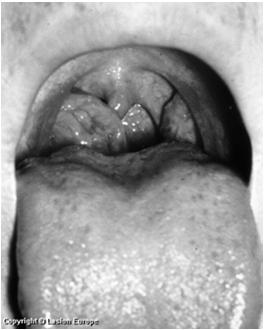
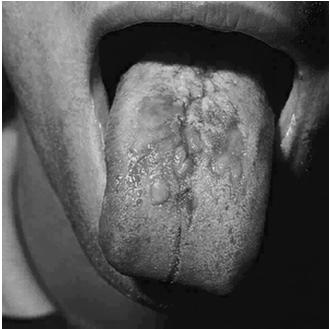
13 Oral Chancres Oral chancres 13




14 Extragenital chancres Secondary syphilis Secondary Syphilis 14


15 Mucous Patches 15




16 Oral Chancre Condylomata lata Gumma 16
17 Diagnosis What s recommended? Primary/Secondary Syphilis Lesions? Darkfield microscopy Direct immunofluorescence Polymerase chain reaction (PCR) Early Latent Syphilis Late Latent Syphilis Syphilis of Unknown Duration Late Syphilis Serology Diagnostic Points A positive darkfield or DFA of lesion exudate or tissue is a DEFINITIVE DX For presumptive diagnosis you need: + nontreponemal test (VDRL/RPR) AND + confirmatory treponemal test (FTA ABS) 17

 are used to evaluate response to")
18 Syphilis Treponema pallidum on darkfield Few clinics have darkfield microscopes Few clinicians know how to use them Syphilis Treponema pallidum on DFA Few labs offer this test; takes time to perform Selecting Syphilis Tests Select and interpret lesion and serologic tests appropriately Lesion based tests used only for Primary Stage Sensitivity and specificity of serology varies by stage Presence of antibody doesn t distinguish past from present infection Quantitative Titers (RPR/VDRL) are used to evaluate response to therapy 18
 (RPR or VDRL) Nontreponemal (qualitative")


19 Serologic Tests for Syphilis Two types Treponemal (qualitative) (RPR or VDRL) Nontreponemal (qualitative and quantitative) (FTA ABS, TPPA, TPI, ELISA, TPHA) Need both types to make an accurate diagnosis of syphilis Screening Tests for Syphilis Nontreponemal tests RPR Card Test: read directly VDRL Test: read via microscope Qualitative RPR Test 19
20 Diagnosis Unusual serologic responses have been reported, most concerning high STS titers, but false negative STS reported These are UNUSUAL Serologic Tests for Syphilis Monitor titers to determine cure, failure, reinfection/relapse After therapy: Cure = 4 fold (or 2 dilution) decrease (e.g. from 1:32 to 1:8) Failure = no change or increase Reinfection = documented titer response then a 4 fold increase 20
21 Natural History of Titer Decay Titer 3 M 9 M 2 Years Years from Infection SEROLOGIC TITERS OF RPR/VDRL 1 : : : : : 64 1 : 32 1 : 16 1 : 8 1 : 4 1 : 2 1 : 1 2-fold decline 2-fold decline Sensitivity of Serologic Tests for Syphilis From Larson et al., 1995 Years PRIMARY SECONDAR Y Weeks from exposure LATE DISEASE Years from exposure 21

22 Interpretation of Syphilis Tests Changing Times in Syphilis Serology Prevalence of syphilis is extremely low in many industrialized countries Labor costs have increased Introduction of treponemal tests which can be fully automated 22
23 Syphilis Laboratory testing and the EIA dilemma Two licensed tests for screening and confirmation Trinity Captia Syphilis G (sonicated treponemes) Trepchek G (cloned antigens) Increased use of treponemal EIA for screening; clinical management problems Quantitative non treponemal testing to guide patient management; if test is negative, perform a second treponemal test to determine reactivity Recommendations for laboratory syphilis testing algorithm with treponemal EIA (or CIA) as initial test A1 (EIA or CIA A1+ A1 Negative for syphilis A2 (quantitative nontreponemal i.e. RPR) A1+ A2+ Consistent with syphilis (past or current) A1+ A2 A3Treponemal test that uses a different Ag platform from A1 (i.e. TPPA, FTA ABS) A1+ A2 - A3+ Possible syphilis A1+ A2 A3 - Unconfirmed EIA Biggest question? How to interpret a positive treponemal, but negative non treponemal result! Treatment? Contact investigation? Reporting? 23



24 CDC recommended algorithm for reverse sequence syphilis screening followed by nontreponemal test confirmation What are the implications for public health practice? Your best friend in the interpretation of serologic tests for syphilis to determine management and treatment is your local HEALTH DEPARTMENT 24

25 Syphilis: Treatment Therapy for Syphilis Parenteral penicillin G is drug of choice for all stages of syphilis It is the ONLY therapy with documented efficacy for neurosyphilis or for syphilis during pregnancy 25

26 Primary and Secondary Syphilis: Therapy Benzathine penicillin G, 2.4 million units IM in a single dose Penicillin Allergic Nonpregnant Patients Doxycycline 100 mg PO BID for 2 weeks 26
27 Follow up Re examine patients clinically and serologically at 6 months and 12 months after treatment Rolfs study states that 15% of patients with early syphilis will not achieve a two dilution decline in nontreponemal titer at 1 year What are the serological criteria for treatment failure? Failure: recurrence, persistence or progression of symptoms or by rising titer The frequency of serological follow up for 1 o and 2 o HIV uninfected syphilis patients is every 3 months For latent syphilis, titers may decline 4 fold by months, but data conflict HIV Infected Patients Primary and Secondary Syphilis 2.4 million units IM benzathine penicillin G Follow up: 3,6,9,12,and 24 months Treatment failure within 6 12 months: CSF examination Retreat with 7.2 million units penicillin if CSF if normal 27
28 Latent Syphilis Early latent Syphilis Benzathine penicillin G 2.4 million units UM in a single dose Late Latent Syphilis or Syphilis of Unknown Duration Benzathine penicillin G 7.2 million units total, given as three doses of 2.4 million units IM each at 1 week intervals What if they miss a week? Pharmacology data suggest that an interval of days between doses might be acceptable before starting over. If the patient is pregnant, adhere strictly to the weekly dose regimen. If she misses a week, start over. Follow up Repeat nontreponemal titer at 6, 12 and 24 months. If failure, consider LP Patients with a normal CSF exam, re treat if: Titers increase 4 fold A high titer (>1:32) fails to decline at least 4 fold Signs or symptoms attributable to syphilis develop Some patients remain serofast with negative CSF exam. Unclear what to do. 28

29 Jarisch Herxheimer reaction Self limited reaction to anti treponemal therapy, seen more commonly with treatment of early stages Characterized by fever, malaise, nasea/vomiting, sometimes with chills and exacerbation of rash Occurs within 24 hours after therapy and resolves within 24 hours Warn patient that it is NOT ALLERGIC reaction Can be treated with symptomatic support Pregnant women should be aware that it may precipitate early labor and to notify obstetrician or go to ER is problems occur Diagnosis of Neurosyphilis No single test can be used Dx can be made with any combination of: abnormal CSF cell count (> 5 WBC) abnormal CSF protein Reactive CSF VDRL with or without symptoms CSF FTA yields more false positives, but is very sensitive; some believe a neg CSF FTA excludes neurosyphilis 29

30 Treatment Aqueous crystalline penicillin G million units a day, given as 3 4 million units IV every 4 hours or continuous infusion for 10 to 14 days OR Procaine penicillin 2.4 million units IM a day, PLUS probenecid 500 mg orally four times a day, both for days Other treatment Ceftriaxone 2 grams daily IV or IM for days Other regimens have not been adequately evaluated for treatment of neurosyphilis 30
31 AND Some experts administer benzathine penicillin, 2.4 million units IM after completion of neurosyphilis treatment to provide a comparable total duration of therapy for late latent disease Syphilis in Pregnancy All women should be screened serologically for syphilis during the early stages of pregnancy In pop n where prenatal care is suboptimal, RPRcard test screening and treatment should be done at time pregnancy is diagnosed In high risk pop n, screen early, at 28 weeks and at delivery Syphilis in Pregnancy Any woman who delivers a stillborn after 20 weeks gestation should be tested for syphilis No infant should leave the hospital without the maternal serologic status having been determined at least once during pregnancy or at the time of delivers 31
32 Syphilis in Pregnancy 2.4 million units benzathine penicillin G is effective therapy for 1 o,2 o, and early latent antepartum syphilis 98% success with carefully defined congenital syphilis Fetal treatment failures are more frequent when moms are treated after the 20th week of gestation and with secondary syphilis Syphilis in Pregnancy 4.8 million units of benzathine penicillin G over 2 weeks is effective for antepartum syphilis BUT One U.S. retrospective case control study found no improvement in prevention of CS in high risk setting of secondary syphilis African retrospective study found no treatment better than a single 2.4 million unit does of benzathine penicillin in preventing preterm birth, still birth, and CS Syphilis in Pregnancy Are there alternatives to penicillin? NO No clinical trial with other medicines Fetal azithromycin serum, amniotic fluid levels are low 32
33 Jarisch Herxheimer Reaction Acute febrile reaction often accompanied by headaches, myalgia, and other symptoms Often occurs within the first 24 hours after any syphilis treatment More common with early syphilis Patients should be advised of this Antipyretics may be recommended but no proven methods prevent reaction Syphilis in Pregnancy Women treated during the second half of pregnancy are at risk for premature labor and/or fetal distress if therapy precipitates the Jarisch Herxheimer reaction Advise the women to seek obstetric attention if they notice any contractions or decrease in fetal movements Stillbirth is a rare complication of treatment and should not delay it Syphilis in Pregnancy Follow UP Serologic titers should be repeated in the third trimester and at delivery Monthly checks are not necessary but may be checked in women at high risk for reinfection or in high geographic prevalence areas The clinical and antibody response should be appropriate for the stage of the disease Most women will deliver before their serologic response to treatment can be definitively assessed 33
34 34
Learning Objectives. Syphilis. Lessons. Epidemiology: Disease in the U.S. Syphilis Definition. Transmission. Treponema pallidum
 Learning Objectives Syphilis Treponema pallidum 1 Upon completion of this content, the learner will be able to 1. Describe the epidemiology of syphilis in the U.S. 2. Describe the pathogenesis of T. pallidum.
Learning Objectives Syphilis Treponema pallidum 1 Upon completion of this content, the learner will be able to 1. Describe the epidemiology of syphilis in the U.S. 2. Describe the pathogenesis of T. pallidum.
Syphilis Treatment Protocol
 STD, HIV, AND TB SECTION Syphilis Treatment Protocol CLINICAL GUIDANCE FOR PRIMARY AND SECONDARY SYPHILIS AND LATENT SYPHILIS www.lekarzol.com (4/2016) Page 1 of 8 Table of Contents Description... 3 Stages
STD, HIV, AND TB SECTION Syphilis Treatment Protocol CLINICAL GUIDANCE FOR PRIMARY AND SECONDARY SYPHILIS AND LATENT SYPHILIS www.lekarzol.com (4/2016) Page 1 of 8 Table of Contents Description... 3 Stages
SYPHILIS. The Great Pretender K. Amen Eguakun, MSN, APRN, AAHIVS
 SYPHILIS The Great Pretender K. Amen Eguakun, MSN, APRN, AAHIVS Learning Objectives At the end of this presentation, the participants will be able to 1. Describe the epidemiology of syphilis in the United
SYPHILIS The Great Pretender K. Amen Eguakun, MSN, APRN, AAHIVS Learning Objectives At the end of this presentation, the participants will be able to 1. Describe the epidemiology of syphilis in the United
Public/Private Partnerships: Intervening in the Spread of Syphilis
 Public/Private Partnerships: Intervening in the Spread of Diana Torres-Burgos MD, MPH Gerard Castaneda, BSN Alana Thomas, BS STD/HIV Update Conference Grand Rapids, MI 3/11/2014 Outline overview Stages
Public/Private Partnerships: Intervening in the Spread of Diana Torres-Burgos MD, MPH Gerard Castaneda, BSN Alana Thomas, BS STD/HIV Update Conference Grand Rapids, MI 3/11/2014 Outline overview Stages
Syphilis Update: New Presentations of an Old Disease
 Syphilis Update: New Presentations of an Old Disease Bradley Stoner, MD, PhD Washington University in St. Louis Disclosure: Bradley Stoner, MD, PhD STDs in the United States Where do we stand right now?
Syphilis Update: New Presentations of an Old Disease Bradley Stoner, MD, PhD Washington University in St. Louis Disclosure: Bradley Stoner, MD, PhD STDs in the United States Where do we stand right now?
Sexually Transmitted Diseases Treatment Guidelines, 2015
 Morbidity and Mortality Weekly Report Recommendations and Reports / Vol. 64 / No. 3 June 5, 2015 Sexually Transmitted Diseases Treatment Guidelines, 2015 U.S. Department of Health and Human Services Centers
Morbidity and Mortality Weekly Report Recommendations and Reports / Vol. 64 / No. 3 June 5, 2015 Sexually Transmitted Diseases Treatment Guidelines, 2015 U.S. Department of Health and Human Services Centers
Lisa Villarroel, MD MPH Medical Director, Division of Public Health Preparedness Arizona Department of Health Services.
 Lisa Villarroel, MD MPH Medical Director, Division of Public Health Preparedness Arizona Department of Health Services Disclosures: None 1 PRIMARY Fitzgerald TJ, Cleveland P, Johnson RC et al: Scanning
Lisa Villarroel, MD MPH Medical Director, Division of Public Health Preparedness Arizona Department of Health Services Disclosures: None 1 PRIMARY Fitzgerald TJ, Cleveland P, Johnson RC et al: Scanning
9/9/2015. Began to see a shift in 2012 Early syphilis cases more than doubled from year before
 George Walton, MPH, CPH, MLS(ASCP) CM STD Program Manager Bureau of HIV, STD, and Hepatitis September 15, 2015 1 1) Discuss the changing epidemiology of syphilis in Iowa; 2) Explore key populations affected
George Walton, MPH, CPH, MLS(ASCP) CM STD Program Manager Bureau of HIV, STD, and Hepatitis September 15, 2015 1 1) Discuss the changing epidemiology of syphilis in Iowa; 2) Explore key populations affected
SYPHILIS (Treponema pallidum) IMMEDIATE NOTIFICATION STD PROGRAM
 IMMEDIATE NOTIFICATION STD PROGRAM") SYPHILIS (Treponema pallidum) IMMEDIATE NOTIFICATION STD PROGRAM Event Name: Event Time Period: Clinical Description (CDC 2014) Syphilis 180 days Syphilis is a complex sexually transmitted disease that
SYPHILIS (Treponema pallidum) IMMEDIATE NOTIFICATION STD PROGRAM Event Name: Event Time Period: Clinical Description (CDC 2014) Syphilis 180 days Syphilis is a complex sexually transmitted disease that
The Great Imitator Revealed: Syphilis
 The Great Imitator Revealed: Syphilis Jeffrey D. Klausner, MD, MPH Professor of Medicine and Public Health University of California Los Angeles David Geffen School of Medicine Los Angeles, California Learning
The Great Imitator Revealed: Syphilis Jeffrey D. Klausner, MD, MPH Professor of Medicine and Public Health University of California Los Angeles David Geffen School of Medicine Los Angeles, California Learning
Neurosyphilis as an Emerging Feature in the HIV Setting. Christina M. Marra, MD University of Washington Seattle, WA, USA
 Neurosyphilis as an Emerging Feature in the HIV Setting Christina M. Marra, MD University of Washington Seattle, WA, USA Syphilis in the Developing World Region 1995 1999 Sub-Saharan 3,530,000 3,828,000
Neurosyphilis as an Emerging Feature in the HIV Setting Christina M. Marra, MD University of Washington Seattle, WA, USA Syphilis in the Developing World Region 1995 1999 Sub-Saharan 3,530,000 3,828,000
SYPHILIS (REPORTABLE)
") SYPHILIS (REPORTABLE) PREAMBLE In BC, the diagnosis of syphilis is determined by the BCCDC Provincial STI/HIV Clinic physician directly or in coordination with the*physician or nurse practitioner (NP)
SYPHILIS (REPORTABLE) PREAMBLE In BC, the diagnosis of syphilis is determined by the BCCDC Provincial STI/HIV Clinic physician directly or in coordination with the*physician or nurse practitioner (NP)
January Dear Physician:
 Richard F. Daines, M.D. Commissioner Wendy E. Saunders Executive Deputy Commissioner January 2009 Dear Physician: The purpose of this letter is to bring your attention to the significant increase in reported
Richard F. Daines, M.D. Commissioner Wendy E. Saunders Executive Deputy Commissioner January 2009 Dear Physician: The purpose of this letter is to bring your attention to the significant increase in reported
Management of Syphilis in Patients with HIV
 Management of Syphilis in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the Guideline Increase the numbers of NYS
Management of Syphilis in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the Guideline Increase the numbers of NYS
To view an archived recording of this presentation please click the following link:
 To view an archived recording of this presentation please click the following link: http://pho.adobeconnect.com/p16lj8z0qm3/ Please scroll down this file to view a copy of the slides from the session.
To view an archived recording of this presentation please click the following link: http://pho.adobeconnect.com/p16lj8z0qm3/ Please scroll down this file to view a copy of the slides from the session.
Syphilis Technical Instructions for Civil Surgeons
 National Center for Emerging and Zoonotic Infectious Diseases Syphilis Technical Instructions for Civil Surgeons Joanna J. Regan, MD, MPH, FAAP Medical Officer Medical Assessment and Policy Team Immigrant,
National Center for Emerging and Zoonotic Infectious Diseases Syphilis Technical Instructions for Civil Surgeons Joanna J. Regan, MD, MPH, FAAP Medical Officer Medical Assessment and Policy Team Immigrant,
WHAT DO U KNOW ABOUT STIS?
 WHAT DO U KNOW ABOUT STIS? Rattiya Techakajornkeart MD. Bangrak STIs Cluster, Bureau of AIDS, TB and STIs, Department of Disease Control, MOPH, Thailand SEXUALLY TRANSMITTED INFECTIONS? STIs Infections
WHAT DO U KNOW ABOUT STIS? Rattiya Techakajornkeart MD. Bangrak STIs Cluster, Bureau of AIDS, TB and STIs, Department of Disease Control, MOPH, Thailand SEXUALLY TRANSMITTED INFECTIONS? STIs Infections
Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046)
") Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046) Kenneth A. Katz, MD, MSc, MSCE Dermatologist, Kaiser Permanente, San Francisco, CA AAD Annual Meeting, San Diego, CA February
Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046) Kenneth A. Katz, MD, MSc, MSCE Dermatologist, Kaiser Permanente, San Francisco, CA AAD Annual Meeting, San Diego, CA February
Michigan Guidelines: HIV, Syphilis, HBV in Pregnancy
 Michigan Guidelines: HIV, Syphilis, HBV in Pregnancy Presenter: Theodore B. Jones, MD Maternal Fetal Medicine Wayne State University School of Medicine Beaumont Dearborn Hospital HIV, Syphilis, HBV in
Michigan Guidelines: HIV, Syphilis, HBV in Pregnancy Presenter: Theodore B. Jones, MD Maternal Fetal Medicine Wayne State University School of Medicine Beaumont Dearborn Hospital HIV, Syphilis, HBV in
SEXUALLY TRANSMITED DISEASES SYPHILIS ( LUES ) Dr D. Tenea Department of Dermatology University of Pretoria
 Dr D. Tenea Department of Dermatology University of Pretoria") SEXUALLY TRANSMITED DISEASES SYPHILIS ( LUES ) Dr D. Tenea Department of Dermatology University of Pretoria INTRODUCTION Venereal disease = old term STD infections transmitted by sexual contact Sexually
SEXUALLY TRANSMITED DISEASES SYPHILIS ( LUES ) Dr D. Tenea Department of Dermatology University of Pretoria INTRODUCTION Venereal disease = old term STD infections transmitted by sexual contact Sexually
Replaces: 04/13/17. / Formulated: 7/05 SYPHLIS
 Effective Date: 81017 Replaces: 041317 Page 1 of 7 POLICY: The Texas Department of Criminal Justice (TDCJ) will identify, test, and manage all offenders with suspected or confirmed syphilis with a uniform
Effective Date: 81017 Replaces: 041317 Page 1 of 7 POLICY: The Texas Department of Criminal Justice (TDCJ) will identify, test, and manage all offenders with suspected or confirmed syphilis with a uniform
Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046)
") Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046) Kenneth A. Katz, MD, MSc, MSCE Dermatologist, Kaiser Permanente, San Francisco, CA AAD Annual Meeting, Orlando, FL March 4, 2017
Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046) Kenneth A. Katz, MD, MSc, MSCE Dermatologist, Kaiser Permanente, San Francisco, CA AAD Annual Meeting, Orlando, FL March 4, 2017
Use of Treponemal Immunoassays for Screening and Diagnosis of Syphilis
 Use of Treponemal Immunoassays for Screening and Diagnosis of Syphilis Guidance for Medical Providers and Laboratories in California These guidelines were developed by the California Department of Public
Use of Treponemal Immunoassays for Screening and Diagnosis of Syphilis Guidance for Medical Providers and Laboratories in California These guidelines were developed by the California Department of Public
EPIDEMIC OF SYPHILIS
 Brian Sandoval Governor Richard Whitley, MS Director Julie Kotchevar, PhD Administrator Ihsan Azzam, PhD, Md Chief Medical Officer EPIDEMIC OF SYPHILIS Understanding the Clinical & Public Health Need for
Brian Sandoval Governor Richard Whitley, MS Director Julie Kotchevar, PhD Administrator Ihsan Azzam, PhD, Md Chief Medical Officer EPIDEMIC OF SYPHILIS Understanding the Clinical & Public Health Need for
Medical Bacteriology Lecture 11
 Medical Bacteriology Lecture 11 Spirochaetaceae Treponema Borrelia 1 Spirochaetaceae Characteristics - Gran negative rods - spiral single cells, or cork-screw-shaped, extremely thin and can be very long
Medical Bacteriology Lecture 11 Spirochaetaceae Treponema Borrelia 1 Spirochaetaceae Characteristics - Gran negative rods - spiral single cells, or cork-screw-shaped, extremely thin and can be very long
CHAPTER-X SYPHILIS R.KAVITHA, M.PHARM, LECTURER, DEPARTMENT OF PHARMACEUTICS, SRM COLLEGE OF PHARMACY, SRM UNIVERSITY, KATTANKULATHUR.
 CHAPTER-X SYPHILIS R.KAVITHA, M.PHARM, LECTURER, DEPARTMENT OF PHARMACEUTICS, SRM COLLEGE OF PHARMACY, SRM UNIVERSITY, KATTANKULATHUR. Trepanoma pallidum D. Clinical Infection: Syphilis Transmission Usually
CHAPTER-X SYPHILIS R.KAVITHA, M.PHARM, LECTURER, DEPARTMENT OF PHARMACEUTICS, SRM COLLEGE OF PHARMACY, SRM UNIVERSITY, KATTANKULATHUR. Trepanoma pallidum D. Clinical Infection: Syphilis Transmission Usually
Didactic Series. STD Screening & Management: Syphilis. Christian B. Ramers, MD, MPH
 Didactic Series STD Screening & Management: Syphilis Christian B. Ramers, MD, MPH Assistant Medical Director Family Health Centers of San Diego Ciaccio Memorial Clinic 3/26/15 ACCREDITATION STATEMENT:
Didactic Series STD Screening & Management: Syphilis Christian B. Ramers, MD, MPH Assistant Medical Director Family Health Centers of San Diego Ciaccio Memorial Clinic 3/26/15 ACCREDITATION STATEMENT:
Spirochetes. Treponema pallidum
 Spirochetes Treponema pallidum Dr. Hala Al Daghistani - Spirochetes are a large, heterogeneous group of spiral, motile bacteria. - One family Spirochaetaceae consists of two genera whose members are human
Spirochetes Treponema pallidum Dr. Hala Al Daghistani - Spirochetes are a large, heterogeneous group of spiral, motile bacteria. - One family Spirochaetaceae consists of two genera whose members are human
2/13/ Graphic photographs or cartoons used during this presentation might be offensive to some; for this I apologize in advance.
 Leon Bullard, MD, MA Medical Consultant, DHEC, DADE The 23 rd Annual APRN Conference Charleston, SC February 24, 2017 1. Provide a brief (very) review of the syphilis story. 2. Define and discuss the stages
Leon Bullard, MD, MA Medical Consultant, DHEC, DADE The 23 rd Annual APRN Conference Charleston, SC February 24, 2017 1. Provide a brief (very) review of the syphilis story. 2. Define and discuss the stages
Sexually Transmitted Disease Treatment Tables
 Sexually Transmitted Disease Treatment Tables Federal Bureau of Prisons Clinical Practice Guidelines June 2011 Clinical guidelines are made available to the public for informational purposes only. The
Sexually Transmitted Disease Treatment Tables Federal Bureau of Prisons Clinical Practice Guidelines June 2011 Clinical guidelines are made available to the public for informational purposes only. The
Nothing to disclose.
 Update on Diagnosis and Treatment Lisa Winston, MD University of California, San Francisco/ Zuckerberg San Francisco General Nothing to disclose. 1 This talk will be a little depressing Rising incidence
Update on Diagnosis and Treatment Lisa Winston, MD University of California, San Francisco/ Zuckerberg San Francisco General Nothing to disclose. 1 This talk will be a little depressing Rising incidence
Syphilis Update. roadmap
 AND Nurse Practitioners!!! AND Physician Assistants!!! Oliver Bacon, MD, MPH Physician, SF City Clinic Disease Prevention and Control Branch Population Health Division roadmap 1. Syphilis: diagnosis and
AND Nurse Practitioners!!! AND Physician Assistants!!! Oliver Bacon, MD, MPH Physician, SF City Clinic Disease Prevention and Control Branch Population Health Division roadmap 1. Syphilis: diagnosis and
Revisions to the Syphilis Surveillance Case Definitions, 2018
 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Revisions to the Syphilis Surveillance Case Definitions, 2018 Sarah Kidd, MD, MPH Medical Epidemiologist Division of STD Prevention
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Revisions to the Syphilis Surveillance Case Definitions, 2018 Sarah Kidd, MD, MPH Medical Epidemiologist Division of STD Prevention
5/1/2017. Sexually Transmitted Diseases Burning Questions
 Sexually Transmitted Diseases Burning Questions Jeffrey D. Klausner, MD, MPH Professor of Medicine and Public Health University of California Los Angeles Los Angeles, California FORMATTED: 04-03-17 Financial
Sexually Transmitted Diseases Burning Questions Jeffrey D. Klausner, MD, MPH Professor of Medicine and Public Health University of California Los Angeles Los Angeles, California FORMATTED: 04-03-17 Financial
STDs in HIV Clinical Care: New Guidelines on Treatment and Prevention
 STDs in HIV Clinical Care: New Guidelines on Treatment and Prevention Palliative Care Conference Faculty Development Conference August 13, 2015 Steven C. Johnson M.D. Director, University of Colorado HIV/AIDS
STDs in HIV Clinical Care: New Guidelines on Treatment and Prevention Palliative Care Conference Faculty Development Conference August 13, 2015 Steven C. Johnson M.D. Director, University of Colorado HIV/AIDS
MID 15. Syphilis. Simon Tsiouris, MD, MPH. 1. Introduction
 Syphilis Simon Tsiouris, MD, MPH 1. Introduction Syphilis is a chronic infection caused by the bacterium Treponema pallidum which was first described over 500 years ago. The manifestations of disease are
Syphilis Simon Tsiouris, MD, MPH 1. Introduction Syphilis is a chronic infection caused by the bacterium Treponema pallidum which was first described over 500 years ago. The manifestations of disease are
Syphilis Update. Dr. Bauer has no disclosures. STD Clinical Update San Diego California Prevention Training Center October 11, 2018
 Heidi M. Bauer, MD MS MPH Chief, STD Control Branch, California Department of Public Health California STD/HIV Prevention Training Center San Diego Dr. Bauer has no disclosures 1 Learning Objectives 1.
Heidi M. Bauer, MD MS MPH Chief, STD Control Branch, California Department of Public Health California STD/HIV Prevention Training Center San Diego Dr. Bauer has no disclosures 1 Learning Objectives 1.
ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES
 ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES A. Screening Page Chlamydia and Gonorrhea 1 HIV 1 Syphilis 1 Genital Herpes 2 Hepatitis A 2 Hepatitis B 2 Hepatitis
ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES A. Screening Page Chlamydia and Gonorrhea 1 HIV 1 Syphilis 1 Genital Herpes 2 Hepatitis A 2 Hepatitis B 2 Hepatitis
Dr Edward Coughlan. Clinical Director Christchurch Sexual Health
 Dr Edward Coughlan Clinical Director Christchurch Sexual Health Christchurch Sexual Health 33 St Asaph Street Dr Edward Coughlan Clinical Director Why this Work Shop on Syphilis? Because it is here Very
Dr Edward Coughlan Clinical Director Christchurch Sexual Health Christchurch Sexual Health 33 St Asaph Street Dr Edward Coughlan Clinical Director Why this Work Shop on Syphilis? Because it is here Very
Susanne Norris Zanto, MPH, MLS (ASCP) CM, SM Montana Public Health Laboratory
 CM, SM Montana Public Health Laboratory") Susanne Norris Zanto, MPH, MLS (ASCP) CM, SM Montana Public Health Laboratory Describe the challenges in syphilis diagnostics Present two testing algorithms Non-treponemal test as initial screen Treponemal
Susanne Norris Zanto, MPH, MLS (ASCP) CM, SM Montana Public Health Laboratory Describe the challenges in syphilis diagnostics Present two testing algorithms Non-treponemal test as initial screen Treponemal
STDs and Hepatitis C
 STDs and Hepatitis C Catherine S. O Neal, MD Assistant Professor of Clinical Medicine, Infectious Diseases Louisiana State University Health Sciences Center March 3, 2018 Objectives Review patient risk
STDs and Hepatitis C Catherine S. O Neal, MD Assistant Professor of Clinical Medicine, Infectious Diseases Louisiana State University Health Sciences Center March 3, 2018 Objectives Review patient risk
Syphilis in the 21 st Century: Sex, Sores, Science, and Surveillance. Syphilis in Men
 Syphilis in the 21 st Century: Sex, Sores, Science, and Surveillance Syphilis in Men Kenneth A. Katz, MD, MSc, MSCE Kaiser Permanente, San Francisco, CA AAD Annual Meeting Washington, D.C. March 2, 2019
Syphilis in the 21 st Century: Sex, Sores, Science, and Surveillance Syphilis in Men Kenneth A. Katz, MD, MSc, MSCE Kaiser Permanente, San Francisco, CA AAD Annual Meeting Washington, D.C. March 2, 2019
Bacteriology. Spirochetes. Three important genera: 1. Treponema 2. Borrelia 3. Leptospira. Treponema pallidum. Causes syphilis.
 Bacteriology Spirochetes Three important genera: 1. Treponema 2. Borrelia 3. Leptospira Treponema pallidum Causes syphilis Organism: - Spirochetes with 6-14 regularly spaced spirals - Its length is the
Bacteriology Spirochetes Three important genera: 1. Treponema 2. Borrelia 3. Leptospira Treponema pallidum Causes syphilis Organism: - Spirochetes with 6-14 regularly spaced spirals - Its length is the
Annual Epidemiological Report
 Annual Epidemiological Report November 2018 Key Facts 1 Early infectious syphilis in Ireland, 2017 There were 398 confirmed cases of early infectious syphilis (EIS) notified in 2017 The notification rate
Annual Epidemiological Report November 2018 Key Facts 1 Early infectious syphilis in Ireland, 2017 There were 398 confirmed cases of early infectious syphilis (EIS) notified in 2017 The notification rate
12/1/2014 GLOBAL HEALTH CASE STUDY RACHEL LE HISTORY OF PRESENT ILLNESS ANY IDEAS? Location: Vadodara, India Gender: female
 GLOBAL HEALTH CASE STUDY RACHEL LE HISTORY OF PRESENT ILLNESS Location: Vadodara, India Gender: female Age: 14 years Complains: perforation, anterior hard palate, difficulty eating, difficulty speaking
GLOBAL HEALTH CASE STUDY RACHEL LE HISTORY OF PRESENT ILLNESS Location: Vadodara, India Gender: female Age: 14 years Complains: perforation, anterior hard palate, difficulty eating, difficulty speaking
10/19/2012. Serologic Testing for Syphilis. Disclosures. Comparison of the Traditional and Reverse Screening Algorithms. Outline.
 Serologic Testing for Syphilis Comparison of the Traditional and Reverse Screening Algorithms Disclosures Elli S. Theel, Ph.D. Director, Infectious Diseases Serology Laboratory Assistant Professor of Laboratory
Serologic Testing for Syphilis Comparison of the Traditional and Reverse Screening Algorithms Disclosures Elli S. Theel, Ph.D. Director, Infectious Diseases Serology Laboratory Assistant Professor of Laboratory
Syphilis: Screening (USPSFT) Syphilis: Screening. Sexually Transmitted Diseases. Family Medicine Board Review Course. Reference
 Syphilis: Screening. Sexually Transmitted Diseases. Family Medicine Board Review Course. Reference") Sexually Transmitted Diseases Family Medicine Board Review Course March 26, 2012 Ronald H. Goldschmidt, MD Reference Centers for Disease Control and Prevention Guidelines for Treatment of Sexually Transmitted
Sexually Transmitted Diseases Family Medicine Board Review Course March 26, 2012 Ronald H. Goldschmidt, MD Reference Centers for Disease Control and Prevention Guidelines for Treatment of Sexually Transmitted
Dr. R. Someshwaran, MBBS, MD., Assistant professor, Dept. of Microbiology, KFMS&R
 Dr. R. Someshwaran, MBBS, MD., Assistant professor, Dept. of Microbiology, KFMS&R 1 What is Syphilis? Syphilis is a systemic, sexually transmitted disease (STD) caused by the Treponema pallidum bacterium.
Dr. R. Someshwaran, MBBS, MD., Assistant professor, Dept. of Microbiology, KFMS&R 1 What is Syphilis? Syphilis is a systemic, sexually transmitted disease (STD) caused by the Treponema pallidum bacterium.
6/11/15. BACTERIAL STDs IN A POST- HIV WORLD. Learning Objectives. How big a problem are STIs in the U.S.?
 BACTERIAL STDs IN A POST- HIV WORLD Tracey Graney, PhD, MT(ASCP) Monroe Community College Learning Objectives Describe the epidemiology and incidence of bacterial STDs in the U.S. Describe current detection
BACTERIAL STDs IN A POST- HIV WORLD Tracey Graney, PhD, MT(ASCP) Monroe Community College Learning Objectives Describe the epidemiology and incidence of bacterial STDs in the U.S. Describe current detection
Urogenital Tract / 3 rd year Syphilis, HPV. Dr Hamed Al-Zoubi MD, PhD Associate Prof. of Medical Microbiology
 Urogenital Tract / 3 rd year Syphilis, HPV Dr Hamed Al-Zoubi MD, PhD Associate Prof. of Medical Microbiology What you need to know about syphilis? Etiology of syphilis Transmission & Epidemiology Pathogenesis
Urogenital Tract / 3 rd year Syphilis, HPV Dr Hamed Al-Zoubi MD, PhD Associate Prof. of Medical Microbiology What you need to know about syphilis? Etiology of syphilis Transmission & Epidemiology Pathogenesis
Emerging Issues in STDs and Resistance
 Emerging Issues in STDs and Resistance Toye H. Brewer, MD Asst. Professor of Clinical Medicine University of Miami School of Medicine Co-Director- Fogarty International Training Program Outline Syphilis-
Emerging Issues in STDs and Resistance Toye H. Brewer, MD Asst. Professor of Clinical Medicine University of Miami School of Medicine Co-Director- Fogarty International Training Program Outline Syphilis-
Medical Bacteriology- Lecture 13 Spirochaetales 1- Spirochaetaceae Treponema Borrelia 2- Leptospiraceae Leptospira
 Medical Bacteriology- Lecture 13 Spirochaetales 1- Spirochaetaceae Treponema Borrelia 2- Leptospiraceae Leptospira OS = outer sheath AF = axial fibrils AF Leptospira interrogans Characteristics: Spirochaetaceae
Medical Bacteriology- Lecture 13 Spirochaetales 1- Spirochaetaceae Treponema Borrelia 2- Leptospiraceae Leptospira OS = outer sheath AF = axial fibrils AF Leptospira interrogans Characteristics: Spirochaetaceae
26. Screening for Syphilis
 26. Screening for Syphilis RECOMMENDATION Routine serologic screening for syphilis is recommended for all pregnant women and for persons at increased risk of infection (see Clinical Inter - vention). See
26. Screening for Syphilis RECOMMENDATION Routine serologic screening for syphilis is recommended for all pregnant women and for persons at increased risk of infection (see Clinical Inter - vention). See
Timby/Smith: Introductory Medical-Surgical Nursing, 9/e
 Timby/Smith: Introductory Medical-Surgical Nursing, 9/e Chapter 62: Caring for Clients With Sexually Transmitted Diseases Slide 1 Epidemiology Introduction Study of the occurrence, distribution, and causes
Timby/Smith: Introductory Medical-Surgical Nursing, 9/e Chapter 62: Caring for Clients With Sexually Transmitted Diseases Slide 1 Epidemiology Introduction Study of the occurrence, distribution, and causes
Con temporary. An OldDisease, a. Pwinatal Problem. ]( ;n PRINCIPLES Q: PRACTICE. Pathogenesis. May/June 1992 J O G N N 209
 ]( ;n PRINCIPLES Q: PRACTICE JILL TILLMAN, RN, MSN An OldDisease, a Con temporary Pwinatal Problem he incidence of syphilis peaked during World War 11, with 600,000 new cases reported per year. Six thousand
]( ;n PRINCIPLES Q: PRACTICE JILL TILLMAN, RN, MSN An OldDisease, a Con temporary Pwinatal Problem he incidence of syphilis peaked during World War 11, with 600,000 new cases reported per year. Six thousand
Serological screening for syphilis in HIV-infected individuals: is a non-treponemal test adequate in the era of increasing of new syphilis infections?
 Abstract no. WEPE 494 Serological screening for syphilis in HIV-infected individuals: is a non-treponemal test adequate in the era of increasing of new syphilis infections? G.Chrysos 1, D.Karageorgopoulos
Abstract no. WEPE 494 Serological screening for syphilis in HIV-infected individuals: is a non-treponemal test adequate in the era of increasing of new syphilis infections? G.Chrysos 1, D.Karageorgopoulos
Elimination of Congenital Syphilis in South Africa Where are we and what needs to be done?
 Elimination of Congenital Syphilis in South Africa Where are we and what needs to be done? Presented by: Dr Saiqa Mullick (Director: Implementation Science, Wits RHI) Co-authors: Diantha Pillay (Researcher:
Elimination of Congenital Syphilis in South Africa Where are we and what needs to be done? Presented by: Dr Saiqa Mullick (Director: Implementation Science, Wits RHI) Co-authors: Diantha Pillay (Researcher:
Disclosures. STD Screening for Women. Chlamydia & Gonorrhea. I have no disclosures or conflicts of interest to report.
 Disclosures Management of STIs: Challenges in Practice I have no disclosures or conflicts of interest to report. Alison O. Marshall, MSN, FNP-C Associate Professor of Practice & Director of the Family
Disclosures Management of STIs: Challenges in Practice I have no disclosures or conflicts of interest to report. Alison O. Marshall, MSN, FNP-C Associate Professor of Practice & Director of the Family
Background. Restricted Siemens Healthcare GmbH, >1 year Late latent syphilis. Restricted Siemens Healthcare GmbH, 2017
 Background Nonneutralizing The Evolution of Syphilis Testing: Clinical Benefits of a Reverse Screening Algorithm Katherine Soreng PhD Lafond RE, et al. Clin Microbiol Rev. 06;19(1):29 49. Disease course:
Background Nonneutralizing The Evolution of Syphilis Testing: Clinical Benefits of a Reverse Screening Algorithm Katherine Soreng PhD Lafond RE, et al. Clin Microbiol Rev. 06;19(1):29 49. Disease course:
Validation of a New Testing Algorithm for Syphilis in Trinidad & Tobago
 Validation of a New Testing Algorithm for Syphilis in Trinidad & Tobago R. Dass, A. Sebro, J. Edwards Ministry of Health, Trinidad and Tobago rianna.dass@hotmail.com, asebro@yahoo.com, jeffreye2000@gmail.com
Validation of a New Testing Algorithm for Syphilis in Trinidad & Tobago R. Dass, A. Sebro, J. Edwards Ministry of Health, Trinidad and Tobago rianna.dass@hotmail.com, asebro@yahoo.com, jeffreye2000@gmail.com
The Resurgence of Syphilis in British Columbia: Who is affected? What are the challenges? How can we improve our response?
 The Resurgence of Syphilis in British Columbia: Who is affected? What are the challenges? How can we improve our response? Gillian Hill-Carroll Travis Salway Hottes Pacific AIDS Network Webinar Series
The Resurgence of Syphilis in British Columbia: Who is affected? What are the challenges? How can we improve our response? Gillian Hill-Carroll Travis Salway Hottes Pacific AIDS Network Webinar Series
Sexually transmitted infections
 Sexually transmitted infections Dr Caroline CHARLIER-WOERTHER Université Paris Descartes Paris, France Learning objectives Counsel patients about the risk of STD Know how to diagnose and treat a sexuallytransmitted
Sexually transmitted infections Dr Caroline CHARLIER-WOERTHER Université Paris Descartes Paris, France Learning objectives Counsel patients about the risk of STD Know how to diagnose and treat a sexuallytransmitted
Management of infants at risk of congenital syphilis
 Management of infants at risk of congenital syphilis Version: Issued: Review date: Author: Dr Sanjay Patel (Paediatric Infectious Diseases Consultant), Dr Emanuela Pelosi (Consultant Virologist), Dr Mildred
Management of infants at risk of congenital syphilis Version: Issued: Review date: Author: Dr Sanjay Patel (Paediatric Infectious Diseases Consultant), Dr Emanuela Pelosi (Consultant Virologist), Dr Mildred
Sexually transmitted infections (in women)
") Sexually transmitted infections (in women) Timothy Kremer, MD Assistant Professor, Department of Obstetrics and Gynecology University of North Texas Health Science Center Last official CDC guidelines:
Sexually transmitted infections (in women) Timothy Kremer, MD Assistant Professor, Department of Obstetrics and Gynecology University of North Texas Health Science Center Last official CDC guidelines:
Women s Sexual Health: STI and HIV Screening. Barbara E. Wilgus, MSN, CRNP STD/HIV Prevention Training Center at Johns Hopkins
 Women s Sexual Health: STI and HIV Screening Barbara E. Wilgus, MSN, CRNP STD/HIV Prevention Training Center at Johns Hopkins I have no disclosures! Review most recent rates of STIs and HIV across the
Women s Sexual Health: STI and HIV Screening Barbara E. Wilgus, MSN, CRNP STD/HIV Prevention Training Center at Johns Hopkins I have no disclosures! Review most recent rates of STIs and HIV across the
GENITAL HERPES. 81.1% of HSV-2 infections are asymptomatic or unrecognized. Figure 14 HSV-2 seroprevalence among persons aged years by sex.
 GENITAL HERPES Genital herpes is a chronic, lifelong, sexually transmitted disease caused by herpes simplex virus type 1 (HSV-1) and type 2 (HSV-2). HSV-1 typically causes small, painful, fluid-filled,
GENITAL HERPES Genital herpes is a chronic, lifelong, sexually transmitted disease caused by herpes simplex virus type 1 (HSV-1) and type 2 (HSV-2). HSV-1 typically causes small, painful, fluid-filled,
SEXUALLY TRANSMITTED DISEASES
 SEXUALLY TRANSMITTED DISEASES Kaya Süer MD, Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology True or false 1. Most people with an STD experience painful symptoms.
SEXUALLY TRANSMITTED DISEASES Kaya Süer MD, Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology True or false 1. Most people with an STD experience painful symptoms.
Edward W. Hook, III, M.D.
 Challenging Cases Edward W. Hook III M.D. Professor and Director Division of Infectious Diseases University of Alabama at Birmingham And PI, Alabama/North Carolina STD PTC Edward W. Hook, III, M.D. Grant/Research
Challenging Cases Edward W. Hook III M.D. Professor and Director Division of Infectious Diseases University of Alabama at Birmingham And PI, Alabama/North Carolina STD PTC Edward W. Hook, III, M.D. Grant/Research
Chapter 11. Sexually Transmitted Diseases
 Chapter 11. Sexually Transmitted Diseases General Guidelines Persons identified as having one sexually transmitted disease (STD) are at risk for others and should be screened as appropriate. Partners of
Chapter 11. Sexually Transmitted Diseases General Guidelines Persons identified as having one sexually transmitted disease (STD) are at risk for others and should be screened as appropriate. Partners of
CASE-BASED SMALL GROUP DISCUSSION
 MHD I, Session IV, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION IV Wednesday, September 18, 2013 MHD I, Session IV, STUDENT Copy Page 2 Resource for cases: Robbins Basic Pathology,
MHD I, Session IV, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION IV Wednesday, September 18, 2013 MHD I, Session IV, STUDENT Copy Page 2 Resource for cases: Robbins Basic Pathology,
Syphilis New spread of an old disease. Erika Vlieghe STD/HIV unit
 Syphilis New spread of an old disease Erika Vlieghe STD/HIV unit Institute of Tropical Medicine, Antwerp 1. Epidemiology 3 waves of syphilis in 20th century: 1. Post-world war II: mainly heterosexual
Syphilis New spread of an old disease Erika Vlieghe STD/HIV unit Institute of Tropical Medicine, Antwerp 1. Epidemiology 3 waves of syphilis in 20th century: 1. Post-world war II: mainly heterosexual
BURNING & SQUIRMING WHAT S NEW IN SEXUALLY TRANSMITTED INFECTIONS
 BURNING & SQUIRMING WHAT S NEW IN SEXUALLY TRANSMITTED INFECTIONS Dr. Joss Reimer MD MPH FRCPC Medical Officer of Health, WRHA & Manitoba Health Assistant Professor, Departments of Community Health Sciences
BURNING & SQUIRMING WHAT S NEW IN SEXUALLY TRANSMITTED INFECTIONS Dr. Joss Reimer MD MPH FRCPC Medical Officer of Health, WRHA & Manitoba Health Assistant Professor, Departments of Community Health Sciences
Syphilis Screening and Prevalence: Past, Present, Future
 Syphilis Screening and Prevalence: Past, Present, Future Allison Haynes, MD University of Kansas School of Medicine- Wichita Family Medicine Residency at Smoky Hill- Salina 1 https://www.cdc.gov/std/syphilis/images/treponema-pallidum.htm
Syphilis Screening and Prevalence: Past, Present, Future Allison Haynes, MD University of Kansas School of Medicine- Wichita Family Medicine Residency at Smoky Hill- Salina 1 https://www.cdc.gov/std/syphilis/images/treponema-pallidum.htm
STD Essentials for the Busy Clinician. Stephanie E. Cohen, MD, MPH
 STD Essentials for the Busy Clinician Stephanie E. Cohen, MD, MPH Assistant Professor, Division of Infectious Diseases, UCSF Medical Director, City Clinic San Francisco Department of Public Health Disclosures
STD Essentials for the Busy Clinician Stephanie E. Cohen, MD, MPH Assistant Professor, Division of Infectious Diseases, UCSF Medical Director, City Clinic San Francisco Department of Public Health Disclosures
CASE-BASED SMALL GROUP DISCUSSION
 MHD I, Session 4, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION 4 Tuesday, September 15, 2015 MHD I, Session 4, STUDENT Copy Page 2 Resource for cases: Robbins Basic Pathology, Chapter
MHD I, Session 4, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION 4 Tuesday, September 15, 2015 MHD I, Session 4, STUDENT Copy Page 2 Resource for cases: Robbins Basic Pathology, Chapter
Another New HIV Diagnosis
 Another New HIV Diagnosis P. Young, RPAC Shelley A Gilroy, MD Albany Medical College June 3, 2014 The Patient 21-year-old male college student with rash x 1 month, beginning on his face Non-tender & non-pruritic
Another New HIV Diagnosis P. Young, RPAC Shelley A Gilroy, MD Albany Medical College June 3, 2014 The Patient 21-year-old male college student with rash x 1 month, beginning on his face Non-tender & non-pruritic
Clinical Cases from the STD Clinical Consultation Network
 Clinical Cases from the STD Clinical Consultation Network Christine Johnston STD TCG April 24, 2017 Last Updated: uwptc@uw.edu uwptc.org 206-685-9850 STD Clinical Consultation Network (STDCCN) Developed
Clinical Cases from the STD Clinical Consultation Network Christine Johnston STD TCG April 24, 2017 Last Updated: uwptc@uw.edu uwptc.org 206-685-9850 STD Clinical Consultation Network (STDCCN) Developed
Clinical Practice Objectives
 STD Essentials for the Busy Clinician Susan S. Philip, MD, MPH Assistant Professor, Division of Infectious Diseases, UCSF Director, STD Prevention and Control Services San Francisco Department of Public
STD Essentials for the Busy Clinician Susan S. Philip, MD, MPH Assistant Professor, Division of Infectious Diseases, UCSF Director, STD Prevention and Control Services San Francisco Department of Public
Syphilis Update: Defense Against a Resurgent Foe. June 23, 2017 Stephen A. Berry, MD PhD
 Syphilis Update: Defense Against a Resurgent Foe June 23, 2017 Stephen A. Berry, MD PhD sberry8@jhmi.edu Disclosures None Non FDA labeled uses: Extragenital NAATs Objectives State at which stage(s) of
Syphilis Update: Defense Against a Resurgent Foe June 23, 2017 Stephen A. Berry, MD PhD sberry8@jhmi.edu Disclosures None Non FDA labeled uses: Extragenital NAATs Objectives State at which stage(s) of
Current standards for diagnosis and treatment of syphilis: selection of some practical issues, based on the European (IUSTI) and U.S.
 and U.S.") Special paper Current standards for diagnosis and treatment of syphilis: selection of some practical issues, based on the European (IUSTI) and U.S. (CDC) guidelines Maciej Pastuszczak, Anna Wojas-Pelc
Special paper Current standards for diagnosis and treatment of syphilis: selection of some practical issues, based on the European (IUSTI) and U.S. (CDC) guidelines Maciej Pastuszczak, Anna Wojas-Pelc
Annals of Internal Medicine. 1991;114:
 Serologic Response to Treatment of Infectious Syphilis Barbara Romanowski, MD; Ruth Sutherland, DPH, RN; Gordon H. Fick, PhD; Debbie Mooney, BSc; and Edgar J. Love, MD, PhD Objective: To evaluate the serologic
Serologic Response to Treatment of Infectious Syphilis Barbara Romanowski, MD; Ruth Sutherland, DPH, RN; Gordon H. Fick, PhD; Debbie Mooney, BSc; and Edgar J. Love, MD, PhD Objective: To evaluate the serologic
Syphilis among MSM: Clinical Care and Public Health Reporting
 Massachusetts Department of Public Health Bureau of Infectious Disease and Laboratory Sciences Syphilis among MSM: Clinical Care and Public Health Reporting Kevin Ard, MD, MPH, Medical Director, National
Massachusetts Department of Public Health Bureau of Infectious Disease and Laboratory Sciences Syphilis among MSM: Clinical Care and Public Health Reporting Kevin Ard, MD, MPH, Medical Director, National
The Use of a Rapid Syphilis Test with Specimens from an HIV Cluster Investigation in Rural West Virginia
 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention The Use of a Rapid Syphilis Test with Specimens from an HIV Cluster Investigation in Rural West Virginia Lara E. Pereira, Ph.D. Centers
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention The Use of a Rapid Syphilis Test with Specimens from an HIV Cluster Investigation in Rural West Virginia Lara E. Pereira, Ph.D. Centers
Syphilis Testing in Northern California Kaiser
 Syphilis Testing in Northern California Kaiser Jen Shieh, MS, CLS Test Development Scientist Kaiser Permanente TPMG Regional Laboratory Microbiology Department Kaiser Permanente 3.3 million members 22
Syphilis Testing in Northern California Kaiser Jen Shieh, MS, CLS Test Development Scientist Kaiser Permanente TPMG Regional Laboratory Microbiology Department Kaiser Permanente 3.3 million members 22
* Proposed new case definition; to be confirmed by AFHSC following analyses of data
 1 ID 13 * Proposed new case definition; to be confirmed by AFHSC following analyses of data SYPHILIS Includes Early Syphilis (Primary, Secondary, Early Latent) and Late Syphilis (Tertiary, Late Latent);
1 ID 13 * Proposed new case definition; to be confirmed by AFHSC following analyses of data SYPHILIS Includes Early Syphilis (Primary, Secondary, Early Latent) and Late Syphilis (Tertiary, Late Latent);
4/18/2018. Syphilis Testing. Disclosure. Learner Objectives. Outline. Employee and stockholder of Bio-Rad Laboratories, Inc.
 Disclosure Employee and stockholder of Bio-Rad Laboratories, Inc. Unraveling the Complexities of Syphilis Testing Maria Crisostomo, April 30 & May 1, 2018 2 Learner Objectives Syphilis Testing Upon completion
Disclosure Employee and stockholder of Bio-Rad Laboratories, Inc. Unraveling the Complexities of Syphilis Testing Maria Crisostomo, April 30 & May 1, 2018 2 Learner Objectives Syphilis Testing Upon completion
1.4.5 SYPHILIS IN PREGNANCY AND THE NEWBORN DIAGNOSIS AND TREATMENT
 WOMEN AND NEWBORN HEALTH SERVICE CLINICAL GUIDELINES SECTION B : GUIDELINES RELEVANT TO OBSTETRICS & MIDWIFERY 1 ANTEPARTUM CARE 1.4 INFECTIONS IN PREGNANCY Authorised by: OGCCU and the Newborn. 1.4.5
WOMEN AND NEWBORN HEALTH SERVICE CLINICAL GUIDELINES SECTION B : GUIDELINES RELEVANT TO OBSTETRICS & MIDWIFERY 1 ANTEPARTUM CARE 1.4 INFECTIONS IN PREGNANCY Authorised by: OGCCU and the Newborn. 1.4.5
Division of Dermatology Dr A Motau
 Division of Dermatology Dr A Motau CASE 1 Histopathology H&E H&E H&E Wartin Starry Immunohistochemical stain for T. pallidum Investigations FBC, U&E, LFT Normal T. pallidum Abs Reactive RPR screen
Division of Dermatology Dr A Motau CASE 1 Histopathology H&E H&E H&E Wartin Starry Immunohistochemical stain for T. pallidum Investigations FBC, U&E, LFT Normal T. pallidum Abs Reactive RPR screen
Sexually transmitted infections (in women)
") Sexually transmitted infections (in women) Timothy Kremer, MD Assistant Professor, Department of Obstetrics and Gynecology University of North Texas Health Science Center Last official CDC guidelines:
Sexually transmitted infections (in women) Timothy Kremer, MD Assistant Professor, Department of Obstetrics and Gynecology University of North Texas Health Science Center Last official CDC guidelines:
STI Update Including PrEP
 STI Update Including PrEP Gordon Liu, M.D, AAHIVS HIV/Hep C Director Latterman Family Health Center UPMC McKeesport Family Medicine Clinical Assistant Professor Department of Family Medicine University
STI Update Including PrEP Gordon Liu, M.D, AAHIVS HIV/Hep C Director Latterman Family Health Center UPMC McKeesport Family Medicine Clinical Assistant Professor Department of Family Medicine University
Welcome to Pathogen Group 6
 Welcome to Pathogen Group 6 Human herpesviruses 1 (HHV-1) and 2 (HHV-2 or HSV-2) Varicella-zoster virus (chickenpox and shingles) Neisseria gonorrhoeae Treponema pallidum Human papillomaviruses (HPV) Human
Welcome to Pathogen Group 6 Human herpesviruses 1 (HHV-1) and 2 (HHV-2 or HSV-2) Varicella-zoster virus (chickenpox and shingles) Neisseria gonorrhoeae Treponema pallidum Human papillomaviruses (HPV) Human
STI Treatment Guidelines. Teodora Wi. Training Course in Sexual and Reproductive Health Research
 Teodora Wi Geneva, 28 August 2017 STI Treatment Guidelines Teodora Wi Training Course in Sexual and Reproductive Health Research 2017 Twitter @HRPresearch 1 STI treatment guidelines Neisseria gonorrhoeae
Teodora Wi Geneva, 28 August 2017 STI Treatment Guidelines Teodora Wi Training Course in Sexual and Reproductive Health Research 2017 Twitter @HRPresearch 1 STI treatment guidelines Neisseria gonorrhoeae
Sexually Transmitted Diseases:
 Sexually Transmitted Diseases: Diagnosis and Management Department of Internal Medicine, Division of Infectious Diseases University of New Mexico A 21 year old woman comes to your clinic asking to be checked
Sexually Transmitted Diseases: Diagnosis and Management Department of Internal Medicine, Division of Infectious Diseases University of New Mexico A 21 year old woman comes to your clinic asking to be checked
Profile of Syphilis. By Karley Delahoussaye
 Profile of Syphilis By Karley Delahoussaye Etiologic Agent: Treponema pallidum₁ Transmission: People transmit syphilis to each other directly through contact with a sore. The sores are known as chancres
Profile of Syphilis By Karley Delahoussaye Etiologic Agent: Treponema pallidum₁ Transmission: People transmit syphilis to each other directly through contact with a sore. The sores are known as chancres
Syphilis MID yo man is seen at an STD clinic for a painless ulcer on his penis
 Syphilis Simon J. Tsiouris, MD, MPH Assistant Professor of Clinical Medicine and Clinical Epidemiology Division of Infectious Diseases College of Physicians and Surgeons Columbia University 43 yo woman
Syphilis Simon J. Tsiouris, MD, MPH Assistant Professor of Clinical Medicine and Clinical Epidemiology Division of Infectious Diseases College of Physicians and Surgeons Columbia University 43 yo woman
EVALUATION OF ENZYME IMMUNOASSAY AND IMMUNOBLOT TESTING FOR THE DIAGNOSIS OF SYPHILIS IN ALBERTA
 EVALUATION OF ENZYME IMMUNOASSAY AND IMMUNOBLOT TESTING FOR THE DIAGNOSIS OF SYPHILIS IN ALBERTA Arto Ohinmaa, Anderson Chuck, Thanh Nguyen, Janice Varney, Philip Jacobs Supported by a financial contribution
EVALUATION OF ENZYME IMMUNOASSAY AND IMMUNOBLOT TESTING FOR THE DIAGNOSIS OF SYPHILIS IN ALBERTA Arto Ohinmaa, Anderson Chuck, Thanh Nguyen, Janice Varney, Philip Jacobs Supported by a financial contribution
Professor Adrian Mindel
 Causes of genital ulceration viruses and others Professor Adrian Mindel University of Sydney VIM 16 th August 2012 Outline Definition Causes Epidemiology Diagnosis Definition of genital ulcer A defect
Causes of genital ulceration viruses and others Professor Adrian Mindel University of Sydney VIM 16 th August 2012 Outline Definition Causes Epidemiology Diagnosis Definition of genital ulcer A defect
Trends in Sexually Transmitted Infections (STIs) C. Junda Woo, MD, MPH, Medical Director San Antonio Metropolitan Health District June 3, 2017
 C. Junda Woo, MD, MPH, Medical Director San Antonio Metropolitan Health District June 3, 2017") Trends in Sexually Transmitted Infections (STIs) C. Junda Woo, MD, MPH, Medical Director San Antonio Metropolitan Health District June 3, 2017 1 Speaker Disclosure Dr. Woo has disclosed that she has no
Trends in Sexually Transmitted Infections (STIs) C. Junda Woo, MD, MPH, Medical Director San Antonio Metropolitan Health District June 3, 2017 1 Speaker Disclosure Dr. Woo has disclosed that she has no
NIH Public Access Author Manuscript Clin Infect Dis. Author manuscript; available in PMC 2009 October 1.
 NIH Public Access Author Manuscript Published in final edited form as: Clin Infect Dis. 2008 October 1; 47(7): 893 899. doi:10.1086/591534. Normalization of Serum Rapid Plasma Reagin Titer Predicts Normalization
NIH Public Access Author Manuscript Published in final edited form as: Clin Infect Dis. 2008 October 1; 47(7): 893 899. doi:10.1086/591534. Normalization of Serum Rapid Plasma Reagin Titer Predicts Normalization