HIV-HCV Co-Infection. George Mason University Falls Church, Virginia. Overview. Prevalence of HCV co-infection Incidence and Recent Trends
|
|
|
- Noreen Barton
- 6 years ago
- Views:
Transcription
1 HIV-HCV Co-Infection Zobair Younossi MD, MPH, FACG, AGAF, FAASLD Chairman, Department of Medicine, Inova Fairfax Hospital Vice President for Research, Inova Health System Professor of Medicine, VCU-Inova Campus Affiliate Professor of Biomedical Sciences, George Mason University Falls Church, Virginia Overview Epidemiology Prevalence of HCV co-infection Incidence and Recent Trends Consequences of Co-infection Higher level of HCV RNA Accelerated natural history Beneficial effect of antiretroviral therapy Treatment 1



2 Worldwide Prevalence of HCV in Patient with HIV Infection Can Be Very High The Prevalence of HCV in HIV Infected Individuals Differs by Risk Groups Sherman K et al. Clin Infect Dis 2002; Sulkowski M et al. Ann Intern Med
3 Recent Epidemic of HCV Among HIV+ MSM: An Emerging Population Reports of epidemic of sexually transmitted HCV among HIV+ MSM Amsterdam, Netherlands: HIV/HCV coinfection prevalence increased from 14.6% to 20.9% from United States: 6-fold higher incidence rate in HIV+ vs HIV- MSM Swiss HIV Cohort Study: HCV incidence increased 18-fold from 1998 to 2010 Sydney, Australia: 9% of HIV+ MSM coinfected with HCV vs 1.9% HIV- MSM Phylogenic analysis indicates HCV transmission clusters in some areas Witt MD, et al. Clin Infect Dis. 2013;57: Wandeler G, et al. Clin Infect Dis. 2012;55: Lea T, et al. Sexual Health. 2013;10: Urbanus AT, et al. AIDS. 2009;23:F1-F7. MMWR. 2011;60: Risk Factors for Sexual HCV Transmission Among HIV+ MSM Multiple factors associated with HCV transmission Unprotected receptive anal intercourse Online casual sexual partners Sex at sex venues Older age Syphilis Recreational drug use Drinking > 13 alcoholic drinks per week Witt MD, et al. Clin Infect Dis. 2013;57: Larsen C, et al. PLoS ONE. 2011;6:e
4 Outbreak of Acute HCV CASCADE Cohorts Data from 12 cohorts within the Concerted Action on SeroConversion to AIDS and Death in Europe (CASCADE) Collaboration Of 4724 MSM, 3014 had HCV testing at the time of HIV seroconversion 124 (4%) were repeatedly HCV positive 92 (3%) had one negative and subsequent positive HCV test (new HCV infections) 2798 (93%) were HCV negative and remained negative HCV incidence: 1990: per 1000 person-years 1995 : per 1000 person-years 2005: per 1000 person-years 2007: per 1000 person-years Incidence of HCV in HIV-infected MSM from 12 cohorts within CASCADE van der Helm JJ et al. AIDS 2011, 25: HCV is a Sexually Transmitted Disease Among HIV-infected MSMs: NYC HIV-positive MSM diagnosed with HCV reported from Mount Sinai Hospital: (N=74) No IVDU Newly elevated ALT levels and a positive HCV antibody test result Median age 39 years Case Control study was carried out: Cases: HIV-infected MSM with HCV infection Controls: HIV-infected MSM without HCV infection Independent risk factors associated with HCV Receptive anal intercourse (AOR = 23, p=0.009) Sex while on methamphetamine (AOR 28.56, p=0.02) Fierer DS et al. MMWR July 22,
5 HIV-HCV Coninfection Consequences of HIV-HCV Co-infection HIV Co-infection Leads to Higher HCV RNA Pre HIV Seroconversion Post HIV Seroconversion 10 8 V RNA eq/ml HC ME Eyster, MW Fried, AM Di Bisceglie and JJ Goedert. Blood :
 0.2 HIV/HCV coinfected HCV monoinfected 0.1 0.074 0.048 P <.")
6 HIV Co-infection Leads to Accelerated Liver Disease Cirrhosis (%) Thein H-H et al. AIDS. 2008;22: Years Thein H-H et al. Hepatology. 2008;48: Risk of Hepatic Decompensation in HIV-HCV Adjusted HR 1.83 (95% CI: ) 0.2 HIV/HCV coinfected HCV monoinfected P < Yrs to Hepatic Decompensation Lo Re V, et al. IAC Abstract WEAB



7 HIV-HCV Co-infection Leads to Higher Incidence of Hepatocellular Carcinoma in a HIV-HCC (N=82) in 18 hospitals in Spain HCV: 81% HCV/HBV: 12% HBV: 7% In patients with HIV/HCV, incidence of HCC increased Death occurred in 79% of patients with HCC Median survival: 91 days (IR: days) Merchante N et al. Clin Infect Dis Jan;56(1): Due to Increased Rates for Adverse Outcomes, Liver Deaths is One of the Leading Causes of Death Among HIV-HCV Infected Patients 43 % 12 % 8 % 5 % 4 % 4 % 4 % 2 % 6 % 7% Decompensated cirrhosis HCC Post-transplantation Cirrhotic Patients: > 50% deaths related to HCV Non cirrhotic patients : 60% deaths non related to HCV nor HIV HSogni P. Conference on French HIV-HCV Consensus Guidelines,
] Patient Death N= 2482 [Death rate/1000 PY = 13.8 (95% CI 13.2 14.3)]. The overall rate of death fell from 16.")


 died AIDS mortality peaked in 1992 11 per 100 person year and declined to 0.")
8 Factors associated with specific causes of death amongst HIV-positive individuals in the D:A:D study D:A:D Cohort study of 33,308 individuals [180,176 person-years ears (PY)] Patient Death N= 2482 [Death rate/1000 PY = 13.8 (95% CI )]. The overall rate of death fell from 16.9 in 1999/2000 to 9.6/ 1000 PY in 2007/2008. Causes of death AIDS, Liver and CVD Smoking was associated with CVD and non-aids cancers HBV and HCV co-infection with liver-related deaths Data Collection on Adverse Events of Anti-HIV drugs (D:A:D) Study Group, Smith C, Sabin CA, Lundgren JD, Thiebaut R, Weber R, Law M, Monforte Ad, Kirk O, Friis-Moller N, Phillips A, Reiss P, El Sadr W, Pradier C, Worm SW. AIDS ;24(10): Death Rate per 100 PY Liver Disease is the Second Leading Cause of Death in Swiss HIV-Cohort Study ( ) SHCS Cohort N=16, (31%) died AIDS mortality peaked in per 100 person year and declined to per 100 PY Cause of death AIDS 78% ( ) liver was not reported Recent SHCS (N=9053) 459 (5.1%) died Causes of death: 19% non-aids malignancy, 18% liver including HCC and 16% AIDS Causes of Death SHCS Weber R, et al. HIV Medicine
9 Consequences of Treatment Treatment of HIV Treatment of HCV Treatment of HIV with Antiretroviral Agents is Associated With a Reduction Risk of Liver-related Complications Limketkai et al. JAMA. July 25, 2012,308(4):
10 Successful Treatment of HCV (SVR) is Associated With Improved Survival SVR No SVR Limketkai et al. JAMA. July 25, 2012,308(4): Treatment of HCV in HIV-HCV Co-infected IFN-based Treatment First Generation DAAs Second Generation DAAs 10
 (n = 6,502) Drug use 39% 56% Alcohol use 44% 48% Depression (major) 18% 23% Bipolar 10% 10% Anemia 12% 24%")

11 Presence of Comorbidities Negatively Impact Candidacy and Tolerance of HIV-HCV Co-infected Patients to IFN-based Therapy Interferon alfa HCV HIV/HCV (n =114,005) (n = 6,502) Drug use 39% 56% Alcohol use 44% 48% Depression (major) 18% 23% Bipolar 10% 10% Anemia 12% 24% Hepatitis B 3% 9% Received HCV treatment 12% 7% Butt A. Alimentary Pharmacology & Therapeutics 2006, Volume 24, Issue 4, Pages Low Efficacy of PEG-IFN and RBV Based Regimen S V R % Hadziyannis SJ et al. Annals Intern Med 2004; Torriani FJ et al. New Eng J Med


12 Treatment of HIV and HCV First Generation DAAs Telaprevir/PR for HCV GT 1 Treatment Naïve HIV Negative and Positive Patients Patients (%) Sulkowski et al AASLD Jacobson et al. New Eng J Med

13 Boceprevir/PR for HCV GT 1 Treatment Naïve HIV Negative and Positive Patients Patients (%) Sulkowski et al AASLD Poordad et al. New Eng J Med Boceprevir/PR for HCV GT 1 Treatment Naïve HIV Negative and Positive Patients Patients (%) These regimens have significant side effects and are no longer recommended Sulkowski et al AASLD Poordad et al. New Eng J Med
 HCV Treatment-Naïve (n=53/27/7) Previous PR Relapsers")

14 Treatment of HIV and HCV Second Generation DAAs Simeprevir + PEG/RBV for HCV GT 1 infection in HIV-Infected patients: SVR12 Patients (%) 80% 74% 64% 79% 89% 57% 87% 78% 100% 70% 50% 67% All patients METAVIR F0-F2 METAVIR F3-F4 57% 57% 60% Overall (n=106/45/22) HCV Treatment-Naïve (n=53/27/7) Previous PR Relapsers (n=15/9/2) Prior PR Partial Responders (n=10/2/3) Prior PR Null Responders (n=28/7/10) 89% of treatment-naïve and prior PR relapsers without cirrhosis met response-guided therapy criteria and were eligible for shortened therapy to 24 weeks, with 87% achieving SVR12. Dieterich D, et al. 21 st CROI. Boston, Abstract



")
15 Study Design (PHOTON-1) Wk 0 Wk 12 Wk 24 Wk 36 Wk 48 GT 1 TN GT 2 or GT 3 TN GT 2 or GT 3 TE SOF + RBV, n=114 SOF + RBV, n=68 SOF + RBV, n=41 Broad inclusion criteria Cirrhosis permitted with no platelet cutoff Hemoglobin: 12 mg/dl (males); 11 mg/dl (females) Wide range of ART regimens allowed Undetectable HIV RNA for >8 weeks on stable ART regimen Baseline CD4 count ART treated: CD4 T-cell count >200 cells/mm 3 and HIV RNA < 50 c/ml ART untreated: CD4 T-cell count >500 cells/mm 3 Sulkowski MS, et al. JAMA. 2014;312: Virologic Response with SOF/RBV for 24 Weeks: Genotype 1 Patients with HCV RNA <LLOQ (%) 110/ /103 87/114 86/114 Week 4 EOT SVR12 SVR24 Sulkowski MS, et al. JAMA. 2014;312:

16 Virologic Response: Genotype 2 Patients with HCV RNA <LLOQ (%) 25/26 22/23 23/26 23/26 24/24 23/23 22/24 22/24 Week 4 EOT SVR12 SVR24 Week 4 EOT SVR12 SVR24 Treatment Naïve 12 Weeks SOF + RBV Sulkowski MS, et al. JAMA. 2014;312: Treatment Experienced 24 Weeks SOF + RBV Virologic Response: Genotype 3 Patients with HCV RNA <LLOQ (%) 41/41 39/40 28/42 28/42 17/17 17/17 16/17 15/17 Week 4 EOT SVR12 SVR24 Week 4 EOT SVR12 SVR24 Treatment Naïve 12 Weeks SOF + RBV Treatment Experienced 24 Weeks SOF + RBV Sulkowski MS, et al. JAMA. 2014;312:
 SVR12 GT 2,3 Experienced SOF + RBV (n = 55) SVR12 Molina et al.")

17 PHOTON-2: Study Design Wk 0 Wk 12 Wk 24 Wk 36 Wk 48 GT 1,3,4 Naive SOF + RBV (n = 200) SVR12 GT 2 Naïve SOF + RBV (n = 19) SVR12 GT 2,3 Experienced SOF + RBV (n = 55) SVR12 Molina et al., IAS 2014, Melbourne, Australia PHOTON-2 SVR12 Results: SOF + RBV 95/112 17/19 52/57 26/31 5/6 42/49 Treatment Naive Treatment Experienced Molina et al., IAS 2014, Melbourne, Australia 17

 24 weeks SOF")


18 PHOTON-2: SVR12 in GT 1 Treatment-Naïve (Cirrhosis vs No Cirrhosis) 24 weeks SOF + RBV SVR (%) 84/95 11/17 76/87 8/13 7/7 3/4 Molina et al., IAS 2014, Melbourne, Australia AASLD/IDSA GUIDANCE 18
19 AASLD and IDSA HCV Guidance: Regimens for Patients with HCV/HIV Coinfection Genotype 1 HCV treatment-naïve and prior PR relapsers IFN eligible IFN ineligible HCV treatment experienced* Genotype 2 Regardless of HCV treatment history Genotype 3 Regardless of HCV treatment history Genotype 4 Regardless of HCV treatment history IFN eligible IFN ineligible Genotype 5 or 6 Regardless of HCV treatment history Sofosbuvir + PR 12 weeks Sofosbuvir + RBV 24 weeks Sofosbuvir + simeprevir + RBV 12 weeks Sofosbuvir + simeprevir + RBV 12 weeks Sofosbuvir + RBV 12 weeks Sofosbuvir + RBV 24 weeks Sofosbuvir + PR 12 weeks Sofosbuvir + RBV 24 weeks Sofosbuvir + PR 12 weeks *Prior PR non-responders regardless of IFN eligibility. For genotype 1a, baseline resistance testing for Q80K should be performed and alternative treatments considered if present. Allowable ART: Sofosbuvir: all except the NRTIs didanosine and zidovudine. Simeprevir: INSTI (raltegravir); NNRTI (rilpivirine); Entry/Fusion Inhibitor (maraviroc, enfuvirtide); NRTIs (tenofovir, emtricitabine, lamivudine, abacavir). AASLD and IDSA. Version January 29, Treatment of HIV and HCV Second Generation DAAs Future Treatment 19



20 SOF+LDV (Interim Analysis 2014) Osinusi et al. EASL 2014 SOF+LDV (Interim Analysis 2014) Osinusi et al. EASL
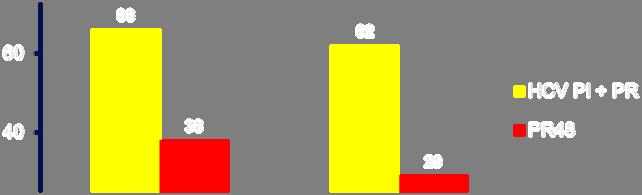
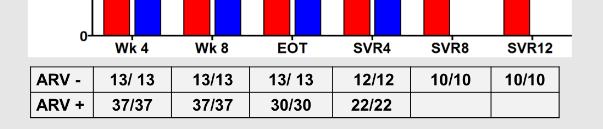
21 TURQUOISE-I: SAFETY AND EFFICACY OF ABT-450/R/OMBITASVIR, DASABUVIR, AND RIBAVIRIN IN PATIENTS CO-INFECTED WITH HEPATITIS C AND HIV-1, Part 1 Study Design Open-label Treatment 3D + RBV (N = 31) 3D + RBV (N = 32) SVR12 SVR4 All patients will be followed for 48 weeks after HCV treatment end Day 1 Week 12 Week 24 Week 36 Sulkowski et al., IAS 2014, Melbourne, Australia TURQUOISE-I Results: Virologic Response Rates % Patients D + RBV Regimen 12-Week Arm 24-Week Arm RVR EOTR SVR4 SVR12 (Week 4) (Week 12 or 24) Sulkowski et al., IAS 2014, Melbourne, Australia 21
 Follow-up Primary endpoint D1 TW2 TW4 TW8 TW12 SVR4 SVR12 SVR24")
: Interim Virological")
22 MK MK /- RBV in GT 1 HIV/HCV-infected patients (C-WORTHY): Study Design N = 29 MK MK RBV Follow-up N = 30 MK MK-8742 (No RBV) Follow-up Primary endpoint D1 TW2 TW4 TW8 TW12 SVR4 SVR12 SVR24 Sulkowski M. et al. EASL 2014, Abstract #O63 MK MK /- RBV in GT 1 HIV/HCV-infected Patients (C-WORTHY): Interim Virological Response * Sulkowski M. et al. EASL 2014, Abstract #O63 22
23 Drug:Drug Interactions Interactions Between HCV & HIV Medications Potential challenges in treating HIV/HCV co-infected patients Altered concentrations of ARVs and/or DAAs: risk of toxicity Anemia: ribavirin, zidovudine, DAAs CNS effects: interferon, efavirenz efficacy, potential development of resistance (HIV and/or HCV) Drug interactions may be difficult to predict CYP3A4 inhibition (ritonavir); induction (efavirenz) 23
24 DDI Example: Simeprevir and Antiretroviral Drugs Simeprevir (SMV) DRV/r May increase SMV concentration ti All other HIV PIs not evaluated in PK EFV Significant reduction in SMV exposure studies, but likely similar to DRV/r ETR, NVP EVG/cobi/TDF/ FTC Reduction in SMV exposure expected Increase in SMV exposure expected TDF; RPV; RAL no significant PK interaction have been identified to date. DTG not evaluated in PK studies, but not expected to alter the PK of SMV; SMV not expected to alter PK of DTG DDI Example: Sofosbuvir and Antiretroviral Drugs Drug Name Effect on Concentration Clinical Comment tipranavir/ritonavir sofosbuvir Coadministration of SOF with tipranavir/ritonavir is expected to decrease SOF concentration leading to reduced therapeutic effect. No interaction between SOF and the following drugs: Cyclosporine Darunavir/ritonavir Efavirenz Emtricitabine Methadone Raltegravir Rilpivirine Tacrolimus Tenofovir disoproxil fumarate 24
25 Summary Prevalence of HCV in HIV infected individuals can be very high and is dependent on the risk profile There is a recent epidemic of HCV infection in HIV + MSM HCV in the setting of HIV is associated with adverse outcomes Liver disease has become a leading cause of death in HIV infected patients Although IFN-based regimens were problematic, the current second generation DAA regimens are safe and efficacious Future generation of DAA regimens seem to be even more promising, suggesting that HIV-HCV will have identical cure rates as mono-infected individuals Nevertheless, drug-drug interactions must be assessed and closely monitored 25
Antiviral treatment in Unique Populations
 Antiviral treatment in Unique Populations Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Unique HCV Populations HIV/HCV co-infected
Antiviral treatment in Unique Populations Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Unique HCV Populations HIV/HCV co-infected
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
HIV-HCV coinfection. Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland
 HIV-HCV coinfection Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland Disclosures Principal investigator for research grants Funds paid to Johns Hopkins
HIV-HCV coinfection Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland Disclosures Principal investigator for research grants Funds paid to Johns Hopkins
Current State of Treatment for HCV. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 Activity Code FA376 Current State of Treatment for HCV Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives Upon completion of this presentation, learners should be
Activity Code FA376 Current State of Treatment for HCV Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives Upon completion of this presentation, learners should be
Global Prevalence of HBV, HCV, HIV
 Treatment of Patients with HCV and HIV Paul Y. Kwo, MD, FACG Professor of Medicine Stanford University email: pkwo@stanford.edu Global Prevalence of HBV, HCV, HIV 24 m Journal of Clinical Virology Page
Treatment of Patients with HCV and HIV Paul Y. Kwo, MD, FACG Professor of Medicine Stanford University email: pkwo@stanford.edu Global Prevalence of HBV, HCV, HIV 24 m Journal of Clinical Virology Page
Dr Janice Main Imperial College Healthcare NHS Trust, London
 BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
HCV/HIV Coinfection ANTON AND MARGARET FUISZ CHAIR IN MEDICINE. HIV and HCV Share Risk Factors PREVALENCE OF CO-INFECTION BY RISK FACTOR 60%
 HCV/HIV Coinfection BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY HIV and HCV Share Risk Factors PREVALENCE
HCV/HIV Coinfection BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY HIV and HCV Share Risk Factors PREVALENCE
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Slide Presentation. Management of HCV Coinfection Susanna Naggie, MD, MHS
 Slide Presentation Management of HCV Coinfection Assistant Professor of Medicine Duke University School of Medicine & Durham VA Medical Center Director of Infectious Diseases Duke Clinical Research Institute
Slide Presentation Management of HCV Coinfection Assistant Professor of Medicine Duke University School of Medicine & Durham VA Medical Center Director of Infectious Diseases Duke Clinical Research Institute
HIV and Hepatitis C Have we finally slayed the beast?
 HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
HIV/HCV Coinfection: Why It Matters and What To Do About It. Cody A. Chastain, MD 10/26/16
 HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
Separate clinical trials for HIV- HCV coinfected patients are NOT a necessity. Patrick Ingiliz, Berlin
 Separate clinical trials for HIV- HCV coinfected patients are NOT a necessity Patrick Ingiliz, Berlin Back in the days when HCV genotype 1 was the problem SVR (%) 100 90 80 70 60 50 40 30 20 10 0 35% PRESCO
Separate clinical trials for HIV- HCV coinfected patients are NOT a necessity Patrick Ingiliz, Berlin Back in the days when HCV genotype 1 was the problem SVR (%) 100 90 80 70 60 50 40 30 20 10 0 35% PRESCO
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HIV Infection with HCV Future Directions
 HIV Infection with HCV Future Directions Dr Ranjababu (Babu) Kulasegaram Consultant Physician in HIV/GU Medicine Guy s and St Thomas NHS Foundation Trust London, UK Presenter disclosure information Dr
HIV Infection with HCV Future Directions Dr Ranjababu (Babu) Kulasegaram Consultant Physician in HIV/GU Medicine Guy s and St Thomas NHS Foundation Trust London, UK Presenter disclosure information Dr
Latest Treatment Updates for GT 2 and GT 3 Patients
 Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Associate Professor of Medicine University of Chicago
 Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Potential Issues in Treating HIV/HCV co-infection with new HCV antivirals
 State of the Art in Hepatitis C Virus Infection in HIV/HCV-Coinfected Patients FORMATTED: 11/17/15 David L. Wyles, MD Associate Professor of Medicine University of California San Diego San Diego, California
State of the Art in Hepatitis C Virus Infection in HIV/HCV-Coinfected Patients FORMATTED: 11/17/15 David L. Wyles, MD Associate Professor of Medicine University of California San Diego San Diego, California
Treatment of Patients with HCV and HIV
 Treatment of Patients with HCV and HIV BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Four Questions Is HIV/HCV
Treatment of Patients with HCV and HIV BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Four Questions Is HIV/HCV
SHOULD EVERYONE WITH HCV/HIV COINFECTION BE TREATED NOW?
 SHOULD EVERYONE WITH HCV/HIV COINFECTION BE TREATED NOW? Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Disclosures
SHOULD EVERYONE WITH HCV/HIV COINFECTION BE TREATED NOW? Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Disclosures
4/30/2015. Interactive Case-Based Presentations and Audience Discussion. Debika Bhattacharya, MD, MSc. Learning Objectives
 4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
HIV/HCV Co-Infection
 HIV/HCV Co-Infection 2015 Kentucky Conference on Viral Hepatitis Matt Cave, M.D. Associate Professor Department of Medicine Division of Gastroenterology, Hepatology, & Nutrition Department of Pharmacology
HIV/HCV Co-Infection 2015 Kentucky Conference on Viral Hepatitis Matt Cave, M.D. Associate Professor Department of Medicine Division of Gastroenterology, Hepatology, & Nutrition Department of Pharmacology
HIV/hepatitis co-infection. Christoph Boesecke Department of Medicine I University Hospital Bonn Germany
 HIV/hepatitis co-infection Christoph Boesecke Department of Medicine I University Hospital Bonn Germany Clinical Management and Treatment of HBV and HCV Co-infection in HIVpositive Persons Hepatitis B
HIV/hepatitis co-infection Christoph Boesecke Department of Medicine I University Hospital Bonn Germany Clinical Management and Treatment of HBV and HCV Co-infection in HIVpositive Persons Hepatitis B
Can a One-Size-Fits-All Approach Be Applied to All Treatment-Naïve GT1 HCV Patients?
 Can a One-Size-Fits-All Approach Be Applied to All Treatment-Naïve GT1 HCV Patients? Ira M. Jacobson, MD Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology
Can a One-Size-Fits-All Approach Be Applied to All Treatment-Naïve GT1 HCV Patients? Ira M. Jacobson, MD Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology
Overview on latest data on IFN-sparing and IFN-free regimens in HCV/HIV patients 10th HIV and hepatitis coinfection workshop June 2014 Paris, France
 Overview on latest data on IFN-sparing and IFN-free regimens in HCV/HIV patients 10th HIV and hepatitis coinfection workshop June 2014 Paris, France Patrick Ingiliz, Berlin Conflicts of Interest Boards,
Overview on latest data on IFN-sparing and IFN-free regimens in HCV/HIV patients 10th HIV and hepatitis coinfection workshop June 2014 Paris, France Patrick Ingiliz, Berlin Conflicts of Interest Boards,
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
HIV-HCV Co-Infection in Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School
 HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened
HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
8/5/2014. A new era of HCV clinical management. Direct-Acting Antivirals for Hepatitis C. Goal of HCV treatment is viral cure HIV HBV HCV
 NS5B NS5B 8/5/214 A new era of HCV clinical management Mark Sulkowski, MD Professor of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Disease and Gastroenterology/Hepatology
NS5B NS5B 8/5/214 A new era of HCV clinical management Mark Sulkowski, MD Professor of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Disease and Gastroenterology/Hepatology
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2)
") Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) PegIFN and RBV remain vital components of HCV therapy-- selected presentations from: Program Disclosure This activity has been planned and
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) PegIFN and RBV remain vital components of HCV therapy-- selected presentations from: Program Disclosure This activity has been planned and
Treatment of chronic hepatitis C in HIV co-infected patients
 Treatment of chronic hepatitis C in HIV co-infected patients Vicente Soriano Department of Infectious Diseases Hospital Carlos III, Madrid, Spain The most prevalent chronic viral infections in humans HBV
Treatment of chronic hepatitis C in HIV co-infected patients Vicente Soriano Department of Infectious Diseases Hospital Carlos III, Madrid, Spain The most prevalent chronic viral infections in humans HBV
Workshop I Planning Committee
 Workshop I Planning Committee Nancy Reau, MD Associate Professor of Medicine University of Chicago School of Medicine Chicago, IL Stuart C. Gordon, MD Professor of Medicine Wayne State University School
Workshop I Planning Committee Nancy Reau, MD Associate Professor of Medicine University of Chicago School of Medicine Chicago, IL Stuart C. Gordon, MD Professor of Medicine Wayne State University School
My HCV patient is co-infected with HIV: how to manage?
 EASL «White Nights of Hepatology 2016» My HCV patient is co-infected with HIV: how to manage? A.V. Кravchenko MD, Professor Russia AIDS Federal Center Central Research Institute of Epidemiology St.-Petersburg,
EASL «White Nights of Hepatology 2016» My HCV patient is co-infected with HIV: how to manage? A.V. Кravchenko MD, Professor Russia AIDS Federal Center Central Research Institute of Epidemiology St.-Petersburg,
HEPATITIS C TREATMENT UPDATE
 HEPATITIS C TREATMENT UPDATE Hepatitis C: Burden of Disease in USA HCV is generally asymptomatic until advanced liver disease 4.1 million persons ever infected; 3.2 million chronic infections Up to 75%
HEPATITIS C TREATMENT UPDATE Hepatitis C: Burden of Disease in USA HCV is generally asymptomatic until advanced liver disease 4.1 million persons ever infected; 3.2 million chronic infections Up to 75%
HIV/Hepatitis C in France: data from real life cohorts LIONEL PIROTH CHU DIJON UNIVERSITY OF BURGUNDY DECEMBER LONDON
 HIV/Hepatitis C in France: data from real life cohorts LIONEL PIROTH CHU DIJON UNIVERSITY OF BURGUNDY DECEMBER 2015 - LONDON The need Decreasing prevalence of chronic hepatitis C in French people living
HIV/Hepatitis C in France: data from real life cohorts LIONEL PIROTH CHU DIJON UNIVERSITY OF BURGUNDY DECEMBER 2015 - LONDON The need Decreasing prevalence of chronic hepatitis C in French people living
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA. Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona
 Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Meet the Professor: HIV/HCV Coinfection
 Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
New developments in HCV research and their implications for front-line practice
 New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
Learning Objective. After completing this educational activity, participants should be able to:
 Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Viral hepatitis in patients living with HIV: can we still speak of special population?
 Viral hepatitis in patients living with HIV: can we still speak of special population? Maurizio Bonacini, M.D., A.G.A.F. Mission Gastroenterology and Hepatology San Francisco, CA YES for HBV Excluded by
Viral hepatitis in patients living with HIV: can we still speak of special population? Maurizio Bonacini, M.D., A.G.A.F. Mission Gastroenterology and Hepatology San Francisco, CA YES for HBV Excluded by
6/2/2015. Interactive Case-Based Presentations and Audience Discussion
 6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
Will difficult-to-treat patients remain difficultto-treat. generation of treatments?
 Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret
 New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING. Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona
 TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona Hepatitis C after LT Survival (%) HCV negative HCV positive Time from LT (years) HCV treatment
TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona Hepatitis C after LT Survival (%) HCV negative HCV positive Time from LT (years) HCV treatment
HIV and Hepatitis C: Advances in Treatment
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and Hepatitis C: Advances in Treatment John Scott, MD, MSc Asst Professor University of Washington Presentation prepared & presented by: John Scott, MD,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and Hepatitis C: Advances in Treatment John Scott, MD, MSc Asst Professor University of Washington Presentation prepared & presented by: John Scott, MD,
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
The HCV Pipeline Ira M. Jacobson, MD, FACP, FACG, AGAF. Slide Presentation. IFN-free DAA combinations (G1)
") Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
New York State HCV Provider Webinar Series
 New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Dost Sarpel, MD Division of Infectious Disease Viral Hepatology Milford Regional Medical Center Objectives Review the epidemiology
New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Dost Sarpel, MD Division of Infectious Disease Viral Hepatology Milford Regional Medical Center Objectives Review the epidemiology
HCV Management in Decompensated Cirrhosis: Current Therapies
 Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Clinical Management: Treatment of HCV Mono-infection
 Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Management of HIV / HCV Coinfection
 Advances in HCV 2015 Albany Medical College & Erie County Medical Center Buffalo, New York 24 June 2015 Management of HIV / HCV Coinfection Norbert Bräu, MD, MBA Prof. of Medicine, Icahn School of Medicine
Advances in HCV 2015 Albany Medical College & Erie County Medical Center Buffalo, New York 24 June 2015 Management of HIV / HCV Coinfection Norbert Bräu, MD, MBA Prof. of Medicine, Icahn School of Medicine
Comparing the Different Guidelines
 Comparing the Different Guidelines Fred Poordad, MD Professor of Medicine University of Texas Health Science Center VP, Academic and Clinical Affairs Texas Liver Institute San Antonio, TX Disclosures Grant/Research
Comparing the Different Guidelines Fred Poordad, MD Professor of Medicine University of Texas Health Science Center VP, Academic and Clinical Affairs Texas Liver Institute San Antonio, TX Disclosures Grant/Research
Hepatitis C Genotype 1 (GT 1) Patients in the United States (US)
 Patients in the United States (US)") Hepatitis C Genotype 1 (GT 1) Patients in the United States (US) INDICATION is indicated with or without ribavirin for the treatment of patients with chronic hepatitis C virus (HCV) genotype 1, 4, 5, or
Hepatitis C Genotype 1 (GT 1) Patients in the United States (US) INDICATION is indicated with or without ribavirin for the treatment of patients with chronic hepatitis C virus (HCV) genotype 1, 4, 5, or
Management of HIV / HCV Coinfection
 Bronx VA Medical Center Mount Sinai School of Medicine Advances in HCV 2015 Albany Medical College & Erie County Medical Center Buffalo, New York 24 June 2015 Management of HIV / HCV Coinfection Norbert
Bronx VA Medical Center Mount Sinai School of Medicine Advances in HCV 2015 Albany Medical College & Erie County Medical Center Buffalo, New York 24 June 2015 Management of HIV / HCV Coinfection Norbert
Evolution of Therapy in HCV
 Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2)
") Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) Goals for Hepatitis C Therapy Compared to PegIFN α/rbv, new treatment regimens for chronic hepatitis C should offer: Improved efficacy Efficacy
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) Goals for Hepatitis C Therapy Compared to PegIFN α/rbv, new treatment regimens for chronic hepatitis C should offer: Improved efficacy Efficacy
Dr. Siddharth Srivastava
 Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
New York State HCV Provider Webinar Series. Treatment of HCV/HIV Co-Infection
 New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Objectives Review the epidemiology of HCV and HIV/HCV co-infection Discuss the burden of HIV/HCV co-infection Discuss the treatment
New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Objectives Review the epidemiology of HCV and HIV/HCV co-infection Discuss the burden of HIV/HCV co-infection Discuss the treatment
Treatement Experienced patients without cirrhosis. Rafael Esteban Hospital Universitario Valle Hebron Barcelona
 Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
Program Disclosure. Provider is approved by the California Board of Registered Nursing, Provider #13664, for 1.5 contact hours.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
6/2/2015. Interactive Case-Based Presentations and Audience Discussion
 Interactive Case-Based Presentations and Audience Discussion Arthur Y. Kim, MD Assistant Professor of Medicine Harvard Medical School Director, Viral Hepatitis Clinic Massachusetts General Hospital Boston,
Interactive Case-Based Presentations and Audience Discussion Arthur Y. Kim, MD Assistant Professor of Medicine Harvard Medical School Director, Viral Hepatitis Clinic Massachusetts General Hospital Boston,
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE?
 IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
Addressing Unmet Medical Needs in HCV Genotype 3
 Addressing Unmet Medical Needs in HCV Genotype 3 Karen Doucette, MD, MSc (Epi), FRCPC Associate Professor, Division of Infectious Diseases, Department of Medicine University of Alberta Objectives Identify
Addressing Unmet Medical Needs in HCV Genotype 3 Karen Doucette, MD, MSc (Epi), FRCPC Associate Professor, Division of Infectious Diseases, Department of Medicine University of Alberta Objectives Identify
Hepatitis C Virus: HIV/Hepatitis C Coinfection Wednesday, August 24, 2016
 Hepatitis C Virus: HIV/Hepatitis C Coinfection Debika Bhattacharya, MD, MSc Associate Clinical Professor University of California Los Angeles Los Angeles, California Washington, DC: August 24, 2016 Slide
Hepatitis C Virus: HIV/Hepatitis C Coinfection Debika Bhattacharya, MD, MSc Associate Clinical Professor University of California Los Angeles Los Angeles, California Washington, DC: August 24, 2016 Slide
Case 2: Coinfection. Patient Case
 Case 2: Coinfection Jennifer J. Kiser, PharmD Assistant Professor University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences Aurora, Colorado FORMATTED: 04-21-14 Learning Objectives After
Case 2: Coinfection Jennifer J. Kiser, PharmD Assistant Professor University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences Aurora, Colorado FORMATTED: 04-21-14 Learning Objectives After
Update on chronic hepatitis C treatment: current trends, new challenges, what next?
 Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
The impact of the treatment of HCV in developing Hepatocellular Carcinoma
 The impact of the treatment of HCV in developing Hepatocellular Carcinoma Paul Y Kwo, MD Professor of Medicine Medical Director, Liver Transplantation Gastroenterology/Hepatology Division Indiana University
The impact of the treatment of HCV in developing Hepatocellular Carcinoma Paul Y Kwo, MD Professor of Medicine Medical Director, Liver Transplantation Gastroenterology/Hepatology Division Indiana University
Treatment of Hepatitis C Recurrence after Liver Transplantation. Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona
 Treatment of Hepatitis C Recurrence after Liver Transplantation Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Agenda 1. Introduction 2. Treatment options for hepatitis C recurrence after transplantation
Treatment of Hepatitis C Recurrence after Liver Transplantation Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Agenda 1. Introduction 2. Treatment options for hepatitis C recurrence after transplantation
Case #1. Case #1. Case #1: Audience vote VS. The Great Debate: When to Treat HCV in our HIV coinfected patients
 Case #1 The Great Debate: When to Treat HCV in our HIV coinfected patients Medical Management of AIDS December, 2012 Moderated by George Beatty,MD 35 year old African American man, CD4 + 450, HIV RNA
Case #1 The Great Debate: When to Treat HCV in our HIV coinfected patients Medical Management of AIDS December, 2012 Moderated by George Beatty,MD 35 year old African American man, CD4 + 450, HIV RNA
Optimal therapy of HIV/HCV co-infected patients with direct acting antivirals
 Liver International ISSN 1478-3223 REVIEW ARTICLE Optimal therapy of HIV/HCV co-infected with direct acting antivirals J urgen K. Rockstroh 1,2 1 Department of Internal Medicine I, Bonn University Hospital,
Liver International ISSN 1478-3223 REVIEW ARTICLE Optimal therapy of HIV/HCV co-infected with direct acting antivirals J urgen K. Rockstroh 1,2 1 Department of Internal Medicine I, Bonn University Hospital,
8/11/2014 HIV/HCV CO-INFECTION: RECENT ADVANCES AND NEW OPPORTUNITIES HISTORY NEVER LOOKS LIKE HISTORY WHEN YOU ARE LIVING THROUGH IT.
 HIV/HCV CO-INFECTION: RECENT ADVANCES AND NEW OPPORTUNITIES Jacob Langness, PharmD, BCPS Clinical Pharmacy Specialist HIV and Hepatology HISTORY NEVER LOOKS LIKE HISTORY WHEN YOU ARE LIVING THROUGH IT
HIV/HCV CO-INFECTION: RECENT ADVANCES AND NEW OPPORTUNITIES Jacob Langness, PharmD, BCPS Clinical Pharmacy Specialist HIV and Hepatology HISTORY NEVER LOOKS LIKE HISTORY WHEN YOU ARE LIVING THROUGH IT
Saeed Hamid, MD Alex Thompson, MD, PhD
 Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Keynote Lecture: Optimal Management of HCV-HIV Coinfection
 THASL Annual Meeting 2015 Keynote Lecture: Optimal Management of HCV-HIV Coinfection 26 February 2015 Prof. Chutima Pramoolsiansap Today s Talk HIV/HCV-coinfection Background and epidemiology When to start
THASL Annual Meeting 2015 Keynote Lecture: Optimal Management of HCV-HIV Coinfection 26 February 2015 Prof. Chutima Pramoolsiansap Today s Talk HIV/HCV-coinfection Background and epidemiology When to start
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/2/2016. Andrew I. Aronsohn, MD Associate Professor of Medicine University of Chicago Chicago, Illinois. Learning Objectives
 Challenges in the Management and Treatment of HIV/Hepatitis C Virus Coinfection Andrew I. Aronsohn, MD Associate Professor of Medicine University of Chicago Chicago, Illinois FORMATTED: 05/02/2016 Chicago,
Challenges in the Management and Treatment of HIV/Hepatitis C Virus Coinfection Andrew I. Aronsohn, MD Associate Professor of Medicine University of Chicago Chicago, Illinois FORMATTED: 05/02/2016 Chicago,
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
Case-Based Scenarios in Hepatitis C
 Case-Based Scenarios in Hepatitis C Alicia Stivala, NP HIV/HCV Co-infection Clinic, Mount Sinai Medical Center New York, NY Final Achieving an SVR is Associated With Improved Outcomes Sustained viral response
Case-Based Scenarios in Hepatitis C Alicia Stivala, NP HIV/HCV Co-infection Clinic, Mount Sinai Medical Center New York, NY Final Achieving an SVR is Associated With Improved Outcomes Sustained viral response
HCV care after cure. This program is supported by educational grants from
 HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College
 Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Treating now vs. post transplant
 Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy
 How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
Management of HIV/HCV Coinfection. Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY
 Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Hepatitis C: Newest Treatment Options and What To Do When We Cure It!
 Hepatitis C: Newest Treatment Options and What To Do When We Cure It! Richard Kalman, MD Division of Hepatology Department of Transplantation Einstein Medical Center Learning Objectives Scope of HCV How
Hepatitis C: Newest Treatment Options and What To Do When We Cure It! Richard Kalman, MD Division of Hepatology Department of Transplantation Einstein Medical Center Learning Objectives Scope of HCV How
Hepatitis C Virus Management
 Hepatitis C Virus Management FORMATTED: 04/20/17 New York, New York: February 24, 2017 Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine University of California San Francisco San
Hepatitis C Virus Management FORMATTED: 04/20/17 New York, New York: February 24, 2017 Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine University of California San Francisco San
HCV Infection: EASL Clinical Practice Guidelines Francesco Negro University Hospital Geneva Switzerland
 HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos
 Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
10/21/2016. Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina. Learning Objectives
 A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
Update on HCV Treatment
 Update on HCV Treatment Ajay Bharti, MD Associate Professor of Medicine Division of Infectious Diseases University of California San Diego 2018 April 28, 2018 Clinically relevant questions in HCV-HIV coinfected
Update on HCV Treatment Ajay Bharti, MD Associate Professor of Medicine Division of Infectious Diseases University of California San Diego 2018 April 28, 2018 Clinically relevant questions in HCV-HIV coinfected
Transformation of Chronic Hepatitis C Treatment
 Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
COMPETING INTEREST OF FINANCIAL VALUE
 Sixth Annual BHIVA Conference for the Management of HIV/Hepatitis Co-Infection in collaboration with BASL and BVHG Dr Ed Wilkins North Manchester General Hospital COMPETING INTEREST OF FINANCIAL VALUE
Sixth Annual BHIVA Conference for the Management of HIV/Hepatitis Co-Infection in collaboration with BASL and BVHG Dr Ed Wilkins North Manchester General Hospital COMPETING INTEREST OF FINANCIAL VALUE
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,