TOG The Way Forward
|
|
|
- Lenard Cain
- 6 years ago
- Views:
Transcription
1
 Long term follow up (till 2 Yr) Daily Regimen for all TB Case Modality of")

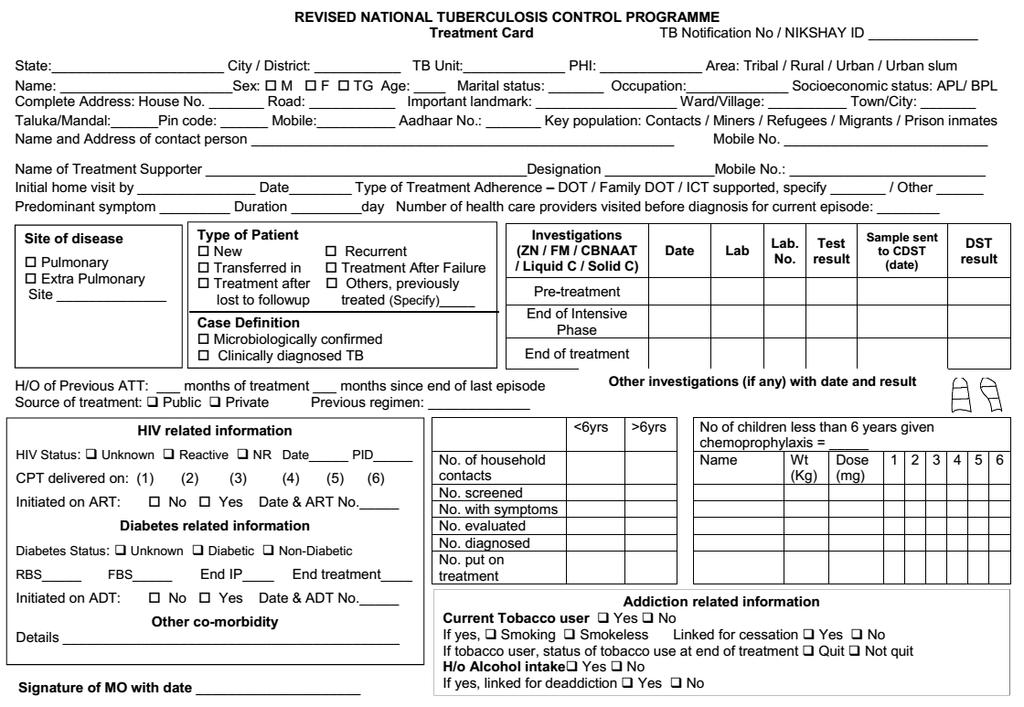
2 TOG The Way Forward Main Changes in Diagnostic algorithm Definition (Type, Classification, Outcome) Registration at the time of Diagnosis (PHI level Notification Register) Long term follow up (till 2 Yr) Daily Regimen for all TB Case Modality of Treatment (DOT, Family DOT, ICT) DR TB Shorter Regimen, BDQ DST Guided Active Case Findings in high risk groups Revised recording and reporting Intensified Supervision and Monitoring 2 Health & Family Welfare Dept, Govt of Gujarat


")


 & CBNAAT Tools for")
3 Diagnostic Tools Sputum Smear Microscopy (for AFB): Zeihl -Neelson Staining & Fluorescent Staining Culture: Solid(Lowenstein Jensen) media & Automated Liquid Culture System eg. BACTEC MGIT Rapid Molecular diagnostic testing: Line Probe Assay (LPA) & CBNAAT Tools for microbiological confirmation of TB
4 Case Definitions
5 Microbiologically confirmed TB : Case definitions presumptive TB patient with biological specimen positive for AFB, or positive for MTB on culture, or positive for TB through Quality Assured Rapid Diagnostic molecular test. Clinically diagnosed TB case : presumptive TB patient who is not microbiologically confirmed, but diagnosed with active TB by a clinician on the basis of X-ray, histopathology or clinical signs with a decision to treat the patient with a full course of Anti-TB treatment. In children, this is based on the presence of abnormalities consistent with TB on radiography, history of exposure to an infectious case, evidence of TB infection (positive TST) & clinical findings suggestive of TB in event of negative or unavailable microbiological results
6 DEFINITIONS OF PRESUMPTIVE TB Presumptive Pulmonary TB refers to a person with any of the symptoms and signs suggestive of TB including cough for > 2 weeks, fever>2 weeks, significant weight loss, haemoptysis, any abnormality in chest radiograph. Note: In addition, contacts of microbiologically confirmed TB patients, PLHIV, Diabetics, Malnourished, cancer patients, patients on immuno- suppressants or steroids should be regularly screened for sign and symptoms of TB Presumptive Extra Pulmonary TB refers to the presence of organ specific symptoms and signs like swelling of lymph node, pain and swelling in joints, neck stiffness, disorientation, etc., and/or constitutional symptoms like significant weight loss, persistent fever for 2 weeks, night sweats. TB Suspect Replaced by PRESUMPTIVE TB
7 DEFINITIONS OF PRESUMPTIVE TB Presumptive Paediatric TB refers to children with persistent fever and / or cough for more than 2 weeks loss of weight*/no weight gain and/or history of contact with infectious TB case**. * History of unexplained weight loss or no weight gain in past 3 months ; loss of weight is defined as loss of more than 5% body weight as compared to highest weight recorded in last 3 months.**in a symptomatic child contact with a person with any form of active TB within last 2 years may be significant. Presumptive DR-TB refers to those Tb patients who have failed treatment with first line drugs, Paediatric TB non responders, TB patients who are contact of DR-TB (or Rif resistance), TB patient who are found positive on any follow - up smear examination during treatment with first line drugs, previously treated TB case, TB patient with HIV coinfection.
8







9 TREATMENT INITIATION- ALGORITHM CBNAAT Result MTB and Rif Res detected MTB detected and Rif Sen MTB Detected and Rif Ind / invalid MTB not detected Error/ no result Invalid H/o Previous Treatment No H/o Previous treatment H/o of previous treatment No H/o Previous treatment Resend fresh sample Rule out other Diff Diag Repeat test on same sample if available Repeat test in second sample Refer to DR TB Centre Confirmatory Repeat CBNAAT Initiate Regimen for PT TB patient Initiate Regimen for new TB patient Rif Indeterminate Rif Res Rif Sen Send fresh sample for C&DST Refer to DR TB Centre Test with LPA/liquid Decide treatment as per result of DST 10
10 Microbiologically confirmed or clinically diagnosed cases of TB are also classified according to: Anatomical site of disease History of previous treatment Drug resistance
11 CLASSIFICATION BY ANATOMICAL SITE OF DISEASE Pulmonary tuberculosis (PTB) : any microbiologically confirmed or clinically diagnosed case of TB involving lung parenchyma or tracheo-bronchial tree. Extra Pulmonary tuberculosis (EPTB) : any microbiologically confirmed or clinically diagnosed case of TB involving organs other than lungs e.g. pleura, lymph nodes, intestine, genitourinary tract, joint and bones, meninges of the brain etc. Miliary TB classified as PTB because there are lesions in the lungs. A patient with both pulmonary and extra-pulmonary TB should be classified as a case of PTB.
12 CLASSIFICATION BY H/O PREVIOUS TB TREATMENT New case - A TB patient who has never had treatment for TB or has taken anti-tb drugs for less than 1 Month. Previously treated patients have received 1 month or more of anti-tb drugs in the past. Recurrent TB case - A TB Patient previously declared as successfully treated (cured/treatment completed) and is subsequently found to be microbiologically confirmed TB case. Treatment After failure those patients who have previously been treated for TB and whose treatment failed at the end of their most recent course of treatment. Treatment after loss to follow-up A TB patient previously treated for TB for 1 month or more and was declared lost to follow-up in their most recent course of treatment and subsequently found microbiologically confirmed TB case. Other previously treated patients are those who have previously been treated for TB but whose outcome after their most recent course of treatment is unknown or undocumented. Transferred In: A TB patient who is received for treatment in a Tuberculosis Unit, after registered for treatment in another TB unit is considered as a case of transferred in.
: A TB patient, whose biological specimen is resistant to more than one first-line anti-tb drug, other than both INH and Rifampicin.")
13 CLASSIFICATION BASED ON DRUG RESISTANCE Mono-resistant (MR): A TB patient, whose biological specimen is resistant to one first-line anti-tb drug only. Poly-Drug Resistant (PDR): A TB patient, whose biological specimen is resistant to more than one first-line anti-tb drug, other than both INH and Rifampicin. Multi Drug Resistant (MDR): A TB patient, whose biological specimen is resistant to both isoniazid and rifampicin with or without resistance to other first line drugs, based on the results from a quality assured laboratory. Rifampicin Resistant (RR): resistance to rifampicin detected using phenotypic or genotypic methods, with or without resistance to other anti-tb drugs excluding INH. Patients, who have any Rifampicin resistance, should also be managed as if they are an MDR TB case. Extensively Drug Resistant (XDR): A MDR TB case whose biological specimen is additionally resistant to a fluoroquinolone (ofloxacin, levofloxacin, or moxifloxacin) and a second-line injectable anti TB drug (kanamycin, amikacin, or capreomycin) from a quality assured laboratory.
14 GUIDELINES FOR TREATMENT INITIATION By suspecting TB in a patient the clinician assumes an important role of providing complete care to the patient including long-term relapse free cure from TB Also assumes public health responsibility of preventing the transmission of disease Treatment initiation should be not be delayed Clinicians who refer the presumptive TB/ drug resistant TB case for diagnosis are encouraged to actively trace the patients. Health facilities that diagnose patients who do not reside in their service delivery area have to refer the patient to the facility where the patient would undergo monitoring of treatment and ensure proper communication of such referral till a feedback is received
15 GUIDELINES FOR TREATMENT INITIATION Before initiating treatment, all TB patients should be counselled thoroughly. It is advisable to involve close family members during the counselling Educate patient and family members about disease (type, mode of spread) and treatment (dosage schedule, duration, common side-effects & methods to prevent them). Counsel the patient & family members to ensure treatment adherence (importance of need for regular treatment and consequences of irregular treatment or premature cessation of treatment, monitoring of progress until completion of treatment) Explain patients on prevention of transmission of disease (cover cough, proper disposal of sputum) and encourage him to get all his close contacts (especially household contacts) screened at the earliest
16 GUIDELINES FOR TREATMENT INITIATION Information required for treatment initiation: drug sensitivity pattern history of anti-tb treatment History of Treatment Drug Sensitivity Status Type of Regimen New Previously treated Drug sensitive or DST unknown / awaited Drug sensitive or DST unknown/ awaited Regimen for new case Regimen for previously treated case New or previously treated Drug resistant Regimen based on DST pattern
17 GUIDELINES FOR TREATMENT INITIATION Record weight of the patient Ideal to record height also to assess Body Mass Index (BMI), to provide a good indicator for prognosis of disease Assess general condition Look for Co-morbidities (diabetes, liver or renal diseases, neurological disorders etc. ) Substance abuse especially tobacco (in any form) & alcohol
18 GUIDELINES FOR TREATMENT INITIATION Socioeconomic status of the patient may be assessed to link him/her with appropriate treatment support schemes. Open a treatment card (in duplicate when required) for each patient at the time of initiation of treatment. Each patient must be given TB Identity Card Appropriate treatment adherence and monitoring mechanisms be planned by the MO at the time of treatment initiation in consultation with the patient and the peripheral health worker who is responsible for monitoring treatment adherence MO should make efforts to get HIV testing done in all cases of TB. Ideally all presumptive TB patients have to undergo HIV screening. If not, HIV screening should be offered. All HIV positive TB patients have to be referred to ART centre for initiation of ART and CPT


/Identity card made prior to initiation of treatment PWB handed over")
19 PROCESS OF INITIATION OF TREATMENT Successful treatment outcome Patient takes daily dose Reveals hidden number ICT based Rx adherence systems Monthly clinical follow-up Weekly supervisory visits and support by health worker Makes free call to number Alerts go to patients & providers real-time patient adherence monitoring Treatment to be prescribed by a Medical Officer Suitable treatment supporter identified TB Treatment Card(s)/Identity card made prior to initiation of treatment PWB handed over to treatment supporter




20 DAILY REGIMEN TB HIV Districts to supply boxes to ART centres (as PHI)




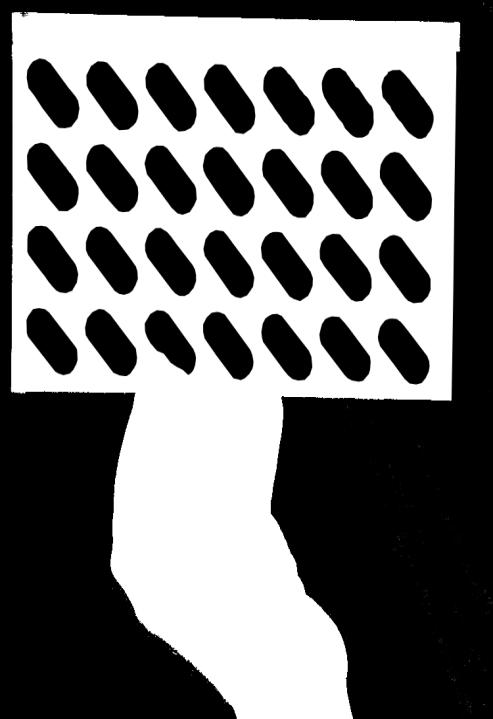
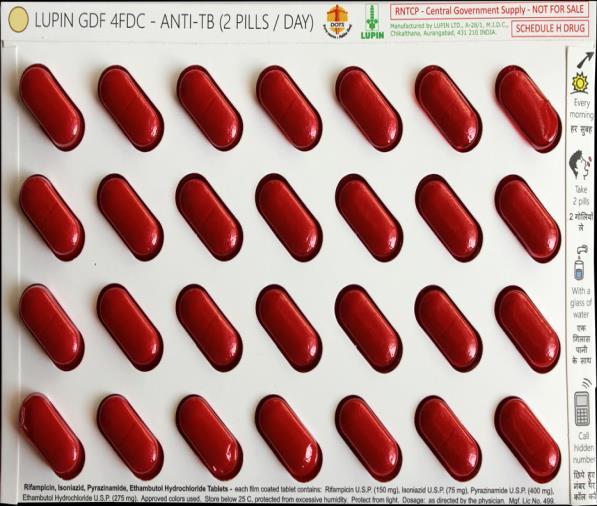
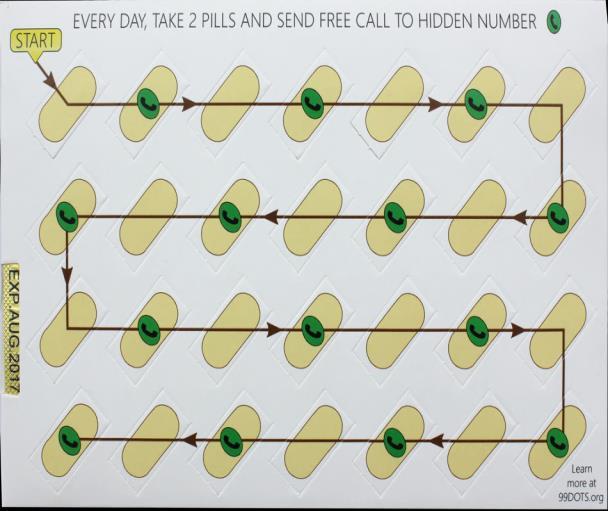
21 99DOTS: (PILL IN HAND) ADHERENCE MONITORING TOOL - TBHIV COINFECTED PATIENTS Courtesy: Bill Thies, Microsoft Research 22


22 99DOTS: TBHIV CO-INFECTED PATIENTS ICT BASED ADHERENCE MONITORING Combination of Caller ID and numbers called shows that doses are in patient s hands. Courtesy: Mr. Bill Thies Microsoft Research 23

23 CALENDAR VIEW OF ADHERENCE
24 FOLLOW UP OF TREATMENT Components of follow up: Clinical follow up Laboratory follow up Clinical follow up at least monthly (Patient visits the clinical facility or the MO reviews during home visit Improvement on chest symptoms, increase in weight etc. may indicate good prognosis Control of co-morbid conditions like HIV and diabetes Symptoms and signs of adverse reactions to drugs should be specifically asked
25 Laboratory investigations FOLLOW UP OF TREATMENT.. In case of pulmonary tuberculosis, sputum smear microscopy should be done at the end of IP and end of treatment. A negative sputum smear microscopy result at the end of IP may indicate good prognosis However, in the presence of clinical deterioration, the medical officer may consider repeating sputum smear microscopy even during CP. This will provide the patient an early opportunity to undergo drug susceptibility testing if s/he is found to be sputum smear positive At completion of treatment, a sputum smear and/or culture should be done for every patient with a productive cough Chest x-ray to be offered to drug sensitive pulmonary TB patients whenever required and available. Response to treatment in extra-pulmonary TB may be best assessed clinically. Help of radiological and other relevant investigations may be taken.
26 LONG TERM FOLLOW UP After completion of treatment, the patients should be followed up at the end of 6, 12, 18 & 24 months. In presence of any clinical symptoms and/or cough, sputum microscopy and/or culture should be considered. This is important in detecting recurrence of TB at the earliest.
27 CONTACT SCREENING All close contacts, especially household contacts should be screened for TB In case of paediatric TB patients, reverse contact tracing for search of any active TB case in the household of the child must be undertaken. Particular attention should be paid to contacts with the highest susceptibility to TB infection
28 The highest priority contacts for active screening Persons with symptoms suggestive of tuberculosis Children aged < 6 years Contacts with known or suspected immuno-compromised patient, particularly HIV infection Contacts with Diabetes Mellitus Contacts with other higher risks including pregnancy, smokers and alcoholics etc. Contacts of patients with DR-TB.
29 ISONIAZID PREVENTIVE THERAPY Children < 6 years of age, who are close contacts of a TB patient, should be evaluated for active TB by a medical officer/ paediatrician After excluding active TB he/she should be given INH preventive therapy irrespective of their BCG or nutritional status The dose of INH for preventive therapy is 10 mg/kg body weight administered daily for a minimum period of 6 months The INH tablets should be collected on monthly basis The contacts should be closely monitored for TB symptoms
30 ISONIAZID PREVENTIVE THERAPY.. INH preventive therapy should also be considered in following situations:- For all HIV infected children who either had a known exposure to an infectious TB case or are Tuberculin skin test (TST) positive (>=5mm induration) but have no active TB disease All TST positive children who are receiving immunosuppressive therapy (e.g. Children with nephrotic syndrome, acute leukemia, etc.). A child born to mother who was diagnosed to have TB in pregnancy should receive prophylaxis for 6 months, provided congenital TB has been ruled out. BCG vaccination can be given at birth even if INH preventive therapy is planned.
31 TREATMENT OUTCOMES FOR DRUG SUSCEPTIBLE TB Cured: Microbiologically confirmed TB patients at the beginning of treatment who was smear or culture negative at the end of the complete treatment Treatment completed: A TB patient who completed treatment without evidence of failure or clinical deterioration BUT with no record to show that the smear or culture results of biological specimen in the last month of treatment was negative, either because test was not done or because result is unavailable. Treatment Success: TB patients either cured or treatment completed Failure: A TB patient whose biological specimen is positive by smear or culture at end of treatment. Failure to Respond A case of paediatric TB who fails to have microbiological conversion to negative status or fails to respond clinically / or deteriorates after 12 weeks of compliant intensive phase shall be deemed to have failed response provided alternative diagnoses/ reasons for non response have been ruled out. Lost to follow up: A TB patient whose treatment was interrupted for 1 consecutive month or more Not Evaluated - A TB Patient for whom no treatment outcome is assigned. This includes former transfer-out Treatment Regimen Changed - A TB patient who is on first line regimen and has been diagnosed as having DRTB and switched to drug resistant TB regimen prior to being declared as failed Died: A patient who has died during the course of anti-tb treatment
32 DEATH AUDIT The MO PHI should conduct an in-depth audit of all deaths occurring amongst TB patients irrespective of initiation of treatment
33 FROM FIELD TO DMC

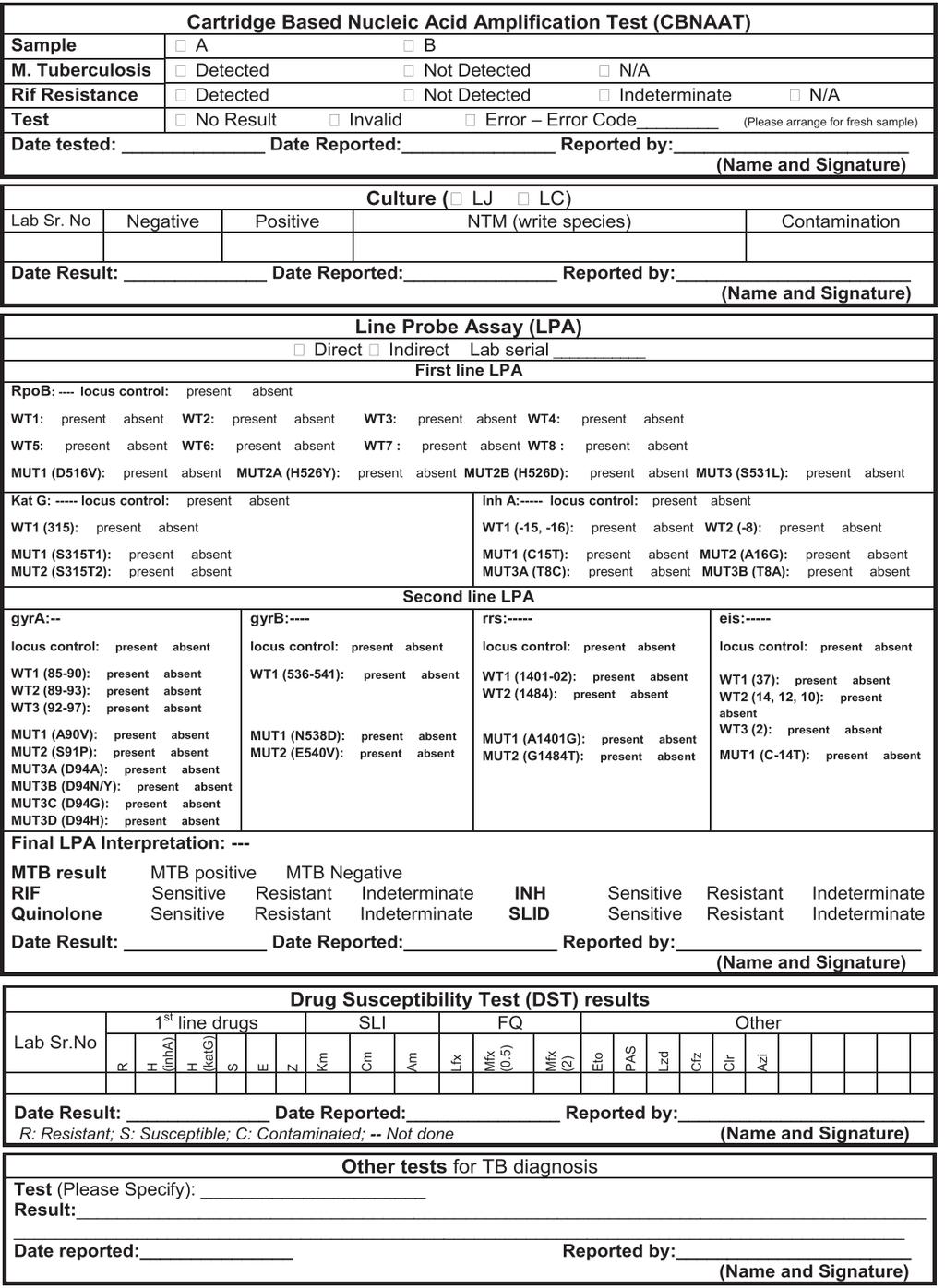
34 LAB INVESTIG ATION CARD
35
36
37
38
39
40
41
42
43
44
45
46
47
48 REPORTS
49
50
51 Thank You
Revised National Tuberculosis Control Programme
 Revised National Tuberculosis Control Programme 2015 C e n t r a l T B D i v i s i o n D i r e c t o r a t e G e n e r a l o f H e a l t h S e r v i c e s M i n i s t r y o f H e a l t h & F a m i l y
Revised National Tuberculosis Control Programme 2015 C e n t r a l T B D i v i s i o n D i r e c t o r a t e G e n e r a l o f H e a l t h S e r v i c e s M i n i s t r y o f H e a l t h & F a m i l y
Definitions and reporting framework for tuberculosis 2013 revision. Dennis Falzon Global Forum of Xpert MTB/RIF Implementers Annecy 17 April 2013
 Definitions and reporting framework for tuberculosis 2013 revision Dennis Falzon Global Forum of Xpert MTB/RIF Implementers Annecy 17 April 2013 2-year revision process WHO/HTM/TB/2013.2 2 www.who.int/iris/bitstream/10665/79199/1/9789241505345_eng.pdf
Definitions and reporting framework for tuberculosis 2013 revision Dennis Falzon Global Forum of Xpert MTB/RIF Implementers Annecy 17 April 2013 2-year revision process WHO/HTM/TB/2013.2 2 www.who.int/iris/bitstream/10665/79199/1/9789241505345_eng.pdf
Revised National Tuberculosis Control Programme (RNTCP) Dr.Kishore Yadav J Assistant Professor
 Dr.Kishore Yadav J Assistant Professor") Revised National Tuberculosis Control Programme (RNTCP) Dr.Kishore Yadav J Assistant Professor Global scenario*: Burden of TB Incidence : 9.6 million (58% SEAR and Western Pacific) Deaths : 1.5 million
Revised National Tuberculosis Control Programme (RNTCP) Dr.Kishore Yadav J Assistant Professor Global scenario*: Burden of TB Incidence : 9.6 million (58% SEAR and Western Pacific) Deaths : 1.5 million
ANNEXURE A: EXPLANATORY NOTES ON THE DMR 164 REPORTING ON HIV AND TB FORM
 ANNEXURE A: EXPLANATORY NOTES ON THE DMR 164 REPORTING ON HIV AND TB FORM The form and content of the explanatory note is to: Inform those responsible for completing the DMR 164 Reporting Form - as to
ANNEXURE A: EXPLANATORY NOTES ON THE DMR 164 REPORTING ON HIV AND TB FORM The form and content of the explanatory note is to: Inform those responsible for completing the DMR 164 Reporting Form - as to
Update on Management of
 Update on Management of DR TB Definitions Presumptive MDR-TB A patient suspected of drug-resistant TB, based on RNTCP criteria for submission of specimens for drug-susceptibility testing MDR-TB Case A
Update on Management of DR TB Definitions Presumptive MDR-TB A patient suspected of drug-resistant TB, based on RNTCP criteria for submission of specimens for drug-susceptibility testing MDR-TB Case A
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
TB IN EMERGENCIES. Disease Control in Humanitarian Emergencies (DCE)
") TB IN EMERGENCIES Department of Epidemic and Pandemic Alert and Response (EPR) Health Security and Environment Cluster (HSE) (Acknowledgements WHO Stop TB Programme WHO/STB) 1 Why TB? >33% of the global
TB IN EMERGENCIES Department of Epidemic and Pandemic Alert and Response (EPR) Health Security and Environment Cluster (HSE) (Acknowledgements WHO Stop TB Programme WHO/STB) 1 Why TB? >33% of the global
Ken Jost, BA, has the following disclosures to make:
 Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
TB/HIV 2 sides of the same coin. Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai
 TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
11/3/2009 SECOND EDITION Madhukar Pai McGill University. ISTC Training Modules Introduction
 SECOND EDITION 2009 Madhukar Pai McGill University Introduction 1 Purpose of ISTC ISTC Version 2: Key Points 21 Standards Differ from existing guidelines: standards present what should be done, whereas,
SECOND EDITION 2009 Madhukar Pai McGill University Introduction 1 Purpose of ISTC ISTC Version 2: Key Points 21 Standards Differ from existing guidelines: standards present what should be done, whereas,
Overview of the Presentation
 Overview of the Presentation Definitions(TBCase, MDR-TB & XDR-TB) Global Tuberculosis (TB,HIV/TB,MDR & XDR)Scenario & Trend Risk factor for TB Natural history of TB Types of TB & Trends of Extra Pulmonary
Overview of the Presentation Definitions(TBCase, MDR-TB & XDR-TB) Global Tuberculosis (TB,HIV/TB,MDR & XDR)Scenario & Trend Risk factor for TB Natural history of TB Types of TB & Trends of Extra Pulmonary
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011
 ART Treatment Guideline Training 31 st January to 4 th February, 2011") TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
INTENSIFIED TB CASE FINDING
 INTENSIFIED TB CASE FINDING My friends call me Intensified Case Finding (ICF) I undertake regularly screening all people with, or at high risk of HIV, for symptoms of TB in health care facilities, communities
INTENSIFIED TB CASE FINDING My friends call me Intensified Case Finding (ICF) I undertake regularly screening all people with, or at high risk of HIV, for symptoms of TB in health care facilities, communities
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
HIV Clinicians Society Conference TB/HIV Treatment Cascade
 HIV Clinicians Society Conference-2012 TB/HIV Treatment Cascade Dr Judith Mwansa-Kambafwile Wits Reproductive Health & HIV Institute University of Witwatersrand TB/HIV Treatment Cascade Overview TB stats
HIV Clinicians Society Conference-2012 TB/HIV Treatment Cascade Dr Judith Mwansa-Kambafwile Wits Reproductive Health & HIV Institute University of Witwatersrand TB/HIV Treatment Cascade Overview TB stats
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf
 Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
INDEX CASE INFORMATION
 Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)
") Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
Assessing the programmatic management of drug-resistant TB
 Assessing the programmatic management of drug-resistant TB a. Review the programmatic management of drug-resistant TB patients with the TB manager. i. What is the size of MDR-TB problem locally? How many
Assessing the programmatic management of drug-resistant TB a. Review the programmatic management of drug-resistant TB patients with the TB manager. i. What is the size of MDR-TB problem locally? How many
Revised National Tuberculosis Control Programme
 Revised National Tuberculosis Control Programme 1 OUTLINE OF PRESENTATION Introduction Burden Of The Disease Evolution Of RNTCP Goals And Objectives Of RNTCP DOTS Stop TB Strategy Organization RNTCP Endorsed
Revised National Tuberculosis Control Programme 1 OUTLINE OF PRESENTATION Introduction Burden Of The Disease Evolution Of RNTCP Goals And Objectives Of RNTCP DOTS Stop TB Strategy Organization RNTCP Endorsed
TB: A Supplement to GP CLINICS
 TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
Let s Talk TB. A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Lancelot M. Pinto, MD, MSc Author Madhukar Pai, MD, PhD co-author and Series Editor Abstract Nearly 50% of patients with
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Lancelot M. Pinto, MD, MSc Author Madhukar Pai, MD, PhD co-author and Series Editor Abstract Nearly 50% of patients with
Contact Follow-Up and Treatment of LTBI in Households of Infectious Cases in Pakistan
 Contact Follow-Up and Treatment of LTBI in Households of Infectious Cases in Pakistan 17 th Annual Conference, The Union-North American Region, Vancouver, Canada. 28 February 2013 Farhana Amanullah Director
Contact Follow-Up and Treatment of LTBI in Households of Infectious Cases in Pakistan 17 th Annual Conference, The Union-North American Region, Vancouver, Canada. 28 February 2013 Farhana Amanullah Director
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
SA TB Guidelines The interface with Advanced Clinical Care
 SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
TB infection control: overview and importance
 TB infection control: overview and importance John Ferguson, Newcastle, NSW Infectious Diseases & Microbiology jferguson@hnehealth.nsw.gov.au Goroka Hospital, September 2014 Patterns of TB disease Latent
TB infection control: overview and importance John Ferguson, Newcastle, NSW Infectious Diseases & Microbiology jferguson@hnehealth.nsw.gov.au Goroka Hospital, September 2014 Patterns of TB disease Latent
Tuberculosis. New TB diagnostics. New drugs.new vaccines. Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012
 Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer
 Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Intensified TB case finding among PLHIV and vulnerable population Identifying contacts Gunta Kirvelaite
 Intensified TB case finding among PLHIV and vulnerable population Identifying contacts Gunta Kirvelaite Riga East Clinical hospital, Centre for tuberculosis and lung diseases. Head of outpatient department.
Intensified TB case finding among PLHIV and vulnerable population Identifying contacts Gunta Kirvelaite Riga East Clinical hospital, Centre for tuberculosis and lung diseases. Head of outpatient department.
Contact Investigation
 Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
Management of MDR TB in special situations. Dr Sarabjit Chadha The Union
 Management of MDR TB in special situations Dr Sarabjit Chadha The Union MDR TB in special situations Pregnancy Breastfeeding Contraception Renal Insufficiency Diabetes Pregnancy and TB Pregnancy is not
Management of MDR TB in special situations Dr Sarabjit Chadha The Union MDR TB in special situations Pregnancy Breastfeeding Contraception Renal Insufficiency Diabetes Pregnancy and TB Pregnancy is not
MODULE SIX. Global TB Institutions and Policy Framework. Treatment Action Group TB/HIV Advocacy Toolkit
 MODULE SIX Global TB Institutions and Policy Framework Treatment Action Group TB/HIV Advocacy Toolkit 1 Topics to be Covered Global TB policy and coordinating structures The Stop TB Strategy TB/HIV collaborative
MODULE SIX Global TB Institutions and Policy Framework Treatment Action Group TB/HIV Advocacy Toolkit 1 Topics to be Covered Global TB policy and coordinating structures The Stop TB Strategy TB/HIV collaborative
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Pediatric tuberculosis (i.e., Tuberculosis
 G U I D E L I N E S Updated National Guidelines for Pediatric Tuberculosis in India, 2012 ASHOK KUMAR, DEVESH GUPTA, SHARATH BURUGINA NAGARAJA, *VARINDER SINGH, # GR SETHI AND JAGADISH PRASAD From Central
G U I D E L I N E S Updated National Guidelines for Pediatric Tuberculosis in India, 2012 ASHOK KUMAR, DEVESH GUPTA, SHARATH BURUGINA NAGARAJA, *VARINDER SINGH, # GR SETHI AND JAGADISH PRASAD From Central
Controlling TB in the era of HIV
 Controlling TB in the era of HIV Christy Hanson, PhD, MPH TB Research Advisor Amy Bloom, MD TB/HIV Advisor TB Incidence rates highest in Africa Estimated new TB cases (all forms) per 100 000 population
Controlling TB in the era of HIV Christy Hanson, PhD, MPH TB Research Advisor Amy Bloom, MD TB/HIV Advisor TB Incidence rates highest in Africa Estimated new TB cases (all forms) per 100 000 population
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
TUBERCULOSIS CONTACT INVESTIGATION
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
The New WHO guidelines on intensified TB case finding and Isoniazid preventive therapy and operational considerations
 Workshop to accelerate the implementation of the Three Is for HIV/TB and earlier initiation of ART in Southern Africa, March 14-18, 2011, Johannesburg, South Africa. The New WHO guidelines on intensified
Workshop to accelerate the implementation of the Three Is for HIV/TB and earlier initiation of ART in Southern Africa, March 14-18, 2011, Johannesburg, South Africa. The New WHO guidelines on intensified
MDR, XDR and Untreatable Tuberculosis and Laboratory Perspectives. Martie van der Walt TUBERCULOSIS EPIDEMIOLOGY & INTERVENTION RESEARCH UNIT
 TUBERCULOSIS EPIDEMIOLOGY & INTERVENTION RESEARCH UNIT MDR, XDR and Untreatable Tuberculosis and Laboratory Perspectives Martie van der Walt IOM Meeting 15-17 January 2013 introduction 1 min 150 words
TUBERCULOSIS EPIDEMIOLOGY & INTERVENTION RESEARCH UNIT MDR, XDR and Untreatable Tuberculosis and Laboratory Perspectives Martie van der Walt IOM Meeting 15-17 January 2013 introduction 1 min 150 words
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
UGANDA NATIONAL TUBERCULOSIS AND LEPROSY CONTROL PROGRAMME
 MINISTRY OF HEALTH UGANDA TIOL TUBERCULOSIS AND LEPROSY CONTROL PROGRAMME Revised Strategic Plan 2015/16-2019/20 Monitoring and Evaluation Plan Narrative of the Operational, Budget and Technical Assistance
MINISTRY OF HEALTH UGANDA TIOL TUBERCULOSIS AND LEPROSY CONTROL PROGRAMME Revised Strategic Plan 2015/16-2019/20 Monitoring and Evaluation Plan Narrative of the Operational, Budget and Technical Assistance
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist, NH GEISELMED.DARTMOUTH.EDU GEISELMED.DARTMOUTH.
 The image part with relationship ID rid2 was not found in the file. MDR TB Management Review of the Evolution (or Revolution?) Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist,
The image part with relationship ID rid2 was not found in the file. MDR TB Management Review of the Evolution (or Revolution?) Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist,
Isoniazid Preventive Therapy (IPT)
") Isoniazid Preventive Therapy (IPT) Josefina Cadorna-Carlos, M.D. Professor of Pediatrics U E R M M M C Objectives 1. Define IPT. 2. Discuss the indications for IPT. 3. Present RCT s for IPT (6H vs 9H).
Isoniazid Preventive Therapy (IPT) Josefina Cadorna-Carlos, M.D. Professor of Pediatrics U E R M M M C Objectives 1. Define IPT. 2. Discuss the indications for IPT. 3. Present RCT s for IPT (6H vs 9H).
Information Note. WHO call for patient data on the treatment of multidrug- and rifampicin resistant tuberculosis
 Information Note WHO call for patient data on the treatment of multidrug- and rifampicin resistant tuberculosis In order to ensure that the upcoming comprehensive revision of WHO policies on treatment
Information Note WHO call for patient data on the treatment of multidrug- and rifampicin resistant tuberculosis In order to ensure that the upcoming comprehensive revision of WHO policies on treatment
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Lancelot M. Pinto, MD, MSc Author Madhukar Pai, MD, PhD co-author and Series Editor Lancelot Pinto is a
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Lancelot M. Pinto, MD, MSc Author Madhukar Pai, MD, PhD co-author and Series Editor Lancelot Pinto is a
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
TB Contact Investigation
 Ann Raftery, RN, PHN, MS Curry International TB Center Overview Contact investigation as a core TB control and elimination activity Components of TB Contact Investigation TB Control Priority Strategies.
Ann Raftery, RN, PHN, MS Curry International TB Center Overview Contact investigation as a core TB control and elimination activity Components of TB Contact Investigation TB Control Priority Strategies.
Latent tuberculosis infection
 EXECUTIVE SUMMARY Latent tuberculosis infection Updated and consolidated guidelines for programmatic management Executive summary Latent tuberculosis infection (LTBI) is defined as a state of persistent
EXECUTIVE SUMMARY Latent tuberculosis infection Updated and consolidated guidelines for programmatic management Executive summary Latent tuberculosis infection (LTBI) is defined as a state of persistent
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE
 Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Tuberculosis Screening and IPT: Experience from India
 Tuberculosis Screening and IPT: Experience from India Dr B.B.Rewari WHO National consultant Care, Support and Treatment National Programme Officer (ART) National AIDS Control Organization New Delhi-110001,
Tuberculosis Screening and IPT: Experience from India Dr B.B.Rewari WHO National consultant Care, Support and Treatment National Programme Officer (ART) National AIDS Control Organization New Delhi-110001,
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Dr Francis Ogaro MTRH ELDORET
 Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
International Standards for Tuberculosis Care Barbara J. Seaworth, MD August 22, 2007
 TB Along the US/Mexico Border El Paso, Texas August 22-23, 2007 International Standards for Tuberculosis Care Barbara J. Seaworth, MD August 22, 2007 Barbara J Seaworth MD Medical Director Heartland National
TB Along the US/Mexico Border El Paso, Texas August 22-23, 2007 International Standards for Tuberculosis Care Barbara J. Seaworth, MD August 22, 2007 Barbara J Seaworth MD Medical Director Heartland National
Screening and Treatment Recommendations for Persons Exposed to MDR TB
 Screening and Treatment Recommendations for Persons Exposed to MDR TB Although all persons at increased risk of tuberculosis (TB) infection should be screened for TB infection per USPTF/CDC guidelines
Screening and Treatment Recommendations for Persons Exposed to MDR TB Although all persons at increased risk of tuberculosis (TB) infection should be screened for TB infection per USPTF/CDC guidelines
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Ministry of Health. National Tuberculosis Control Program INTEGRATED TB HIV PROGRAM REPORT (JANUARY JUNE 2015)
") Ministry of Health National Tuberculosis Control Program INTEGRATED TB HIV PROGRAM REPORT (JANUARY JUNE 2015) Contents Executive summary... 2 Background... 3 National Tuberculosis Program Overview... 3
Ministry of Health National Tuberculosis Control Program INTEGRATED TB HIV PROGRAM REPORT (JANUARY JUNE 2015) Contents Executive summary... 2 Background... 3 National Tuberculosis Program Overview... 3
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Algorithmic Approaches to Child TB Management in Resource-limited Settings
 Algorithmic Approaches to Child TB Management in Resource-limited Settings Steve Graham Centre for International Child Health University of Melbourne Department of Paediatrics Royal Children s Hospital
Algorithmic Approaches to Child TB Management in Resource-limited Settings Steve Graham Centre for International Child Health University of Melbourne Department of Paediatrics Royal Children s Hospital
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Ethiopia. Targeted Tuberculosis Case Finding Interventions in Six Mining Shafts in Remote Districts of Oromia Region in Ethiopia PROJECT CONTEXT
 Technical BRIEF Photo Credit: Challenge TB Targeted Tuberculosis Case Finding Interventions in Six Mining Shafts in Remote Districts of Oromia Region in Ethiopia PROJECT CONTEXT Ethiopia is the second-most
Technical BRIEF Photo Credit: Challenge TB Targeted Tuberculosis Case Finding Interventions in Six Mining Shafts in Remote Districts of Oromia Region in Ethiopia PROJECT CONTEXT Ethiopia is the second-most
Online Annexes (5-8)
") 2016 Online Annexes (5-8) to WHO Policy guidance: The use of molecular line probe assay for the detection of resistance to second-line anti-tuberculosis drugs 1 Contents: Annex 5: GRADE summary of findings
2016 Online Annexes (5-8) to WHO Policy guidance: The use of molecular line probe assay for the detection of resistance to second-line anti-tuberculosis drugs 1 Contents: Annex 5: GRADE summary of findings
Xpert MTB/RIF use for TB diagnosis in TB suspects with no significant risk of drug resistance or HIV infection. Results of Group Work
 Xpert MTB/RIF use for TB diagnosis in TB suspects with no significant risk of drug resistance or HIV infection Results of Group Work DOTS expansion and enhancement Objective This group deals with the majority
Xpert MTB/RIF use for TB diagnosis in TB suspects with no significant risk of drug resistance or HIV infection Results of Group Work DOTS expansion and enhancement Objective This group deals with the majority
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
MULTIDRUG- RESISTANT TUBERCULOSIS. Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic
 MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
TB CAN BE CURED IF YOU TAKE THE TB DRUGS CORRECTLY.
 1. What is Tuberculosis? TB stands for Tuberculosis, a disease caused by the TB bacteria found in the air. The most common presentation of Tuberculosis is the pulmonary TB that affects the lungs and is
1. What is Tuberculosis? TB stands for Tuberculosis, a disease caused by the TB bacteria found in the air. The most common presentation of Tuberculosis is the pulmonary TB that affects the lungs and is
Ongoing Research on LTBI and Research priorities in India
 Ongoing Research on LTBI and Research priorities in India Dr. C.Padmapriyadarsini, MD, MS ICMR-National Institute for Research in Tuberculosis Chennai, India Technical Consultation Meeting on Programmatic
Ongoing Research on LTBI and Research priorities in India Dr. C.Padmapriyadarsini, MD, MS ICMR-National Institute for Research in Tuberculosis Chennai, India Technical Consultation Meeting on Programmatic
IMPACT OF IMPROVED TREATMENT SUCCESS ON THE PREVALENCE OF TB IN A RURAL COMMUNITY BASED ON ACTIVE SURVEILLANCE
 Original Article IMPACT OF IMPROVED TREATMENT SUCCESS ON THE PREVALENCE OF TB IN A RURAL COMMUNITY BASED ON ACTIVE SURVEILLANCE P. G. Gopi, R. Subramani, V. Chandrasekaran, T. Santha and P. R. Narayanan
Original Article IMPACT OF IMPROVED TREATMENT SUCCESS ON THE PREVALENCE OF TB IN A RURAL COMMUNITY BASED ON ACTIVE SURVEILLANCE P. G. Gopi, R. Subramani, V. Chandrasekaran, T. Santha and P. R. Narayanan
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
IPT IMPLEMENTATION- SWAZILAND EXPERIENCE
 IPT IMPLEMENTATION- SWAZILAND EXPERIENCE Gugu Mchunu-National TB/HIV coordinator Programmatic Management of Latent TB infection consultation meeting Seoul, Republic of Korea,27-28 APRIL,2016 TB Epidemiology
IPT IMPLEMENTATION- SWAZILAND EXPERIENCE Gugu Mchunu-National TB/HIV coordinator Programmatic Management of Latent TB infection consultation meeting Seoul, Republic of Korea,27-28 APRIL,2016 TB Epidemiology
Diagnosis of drug resistant TB
 Diagnosis of drug resistant TB Megan Murray, MD, ScD Harvard School of Public Health Brigham and Women s Hospital Harvard Medical School Broad Institute Global burden of TB 9 million new cases year 2 million
Diagnosis of drug resistant TB Megan Murray, MD, ScD Harvard School of Public Health Brigham and Women s Hospital Harvard Medical School Broad Institute Global burden of TB 9 million new cases year 2 million
Online Annexes (5-8)
") Online Annexes (5-8) to WHO Policy guidance: The use of molecular line probe assay for the detection of resistance to second-line anti-tuberculosis drugs THE END TB STRATEGY Online Annexes (5-8) to WHO
Online Annexes (5-8) to WHO Policy guidance: The use of molecular line probe assay for the detection of resistance to second-line anti-tuberculosis drugs THE END TB STRATEGY Online Annexes (5-8) to WHO
How best to structure a laboratory network with new technologies
 How best to structure a laboratory network with new technologies Cristina Gutierrez, MD, PhD Uniting to scale up TB care in Central Asia 14 and 15 April 2011 Tashkent, Uzbekistan New laboratory diagnostics
How best to structure a laboratory network with new technologies Cristina Gutierrez, MD, PhD Uniting to scale up TB care in Central Asia 14 and 15 April 2011 Tashkent, Uzbekistan New laboratory diagnostics
Tuberculosis in Chicago 2007
 City of Chicago Communicable Disease Information Department of Public Health Richard M. Daley, Mayor May 2008 Terry Mason, MD, FACS, Commissioner www.cityofchicago.org/health/ West Side Center For Disease
City of Chicago Communicable Disease Information Department of Public Health Richard M. Daley, Mayor May 2008 Terry Mason, MD, FACS, Commissioner www.cityofchicago.org/health/ West Side Center For Disease
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to