Current HIV Treatment A different challenge every time. Sonali Sonecha Lead HIV Pharmacist 22 nd September 2016
|
|
|
- Paula Ferguson
- 6 years ago
- Views:
Transcription
1 Current HIV Treatment A different challenge every time Sonali Sonecha Lead HIV Pharmacist 22 nd September 2016
2 Aims At the end of this session, delegates should be able to Apply the principles of antiretroviral treatment in current usage List side effects and other practical difficulties / problems associated with antiretroviral treatment Demonstrate comprehension of the reasons for / against treatment at various disease stages Apply the current UK treatment guidelines (BHIVA) to clinical practice
3 Session plan General introduction to antiretrovirals When to start treatment What to start Monitoring treatment Drug-drug interactions Switching therapy

4 Natural progression of HIV
5 When to start treatment
6 Guideline Start Consider Defer BHIVA (2016 interim update) All people living with HIV including those with PHI Only if necessary EACS (Oct 15) Symptomatic strongly recommended Asymptomatic and: CD4<350 strongly recommended CD4>350 - recommended Elite controllers with high and stable CD4 count if necessary USA-DHSS (Jul 16) All patients with HIV infection to reduce risk of disease progression & to prevent transmission of HIV - Case by case on basis of clinical or psychosocial factors WHO (Jun 16) All people living with HIV Priority: WHO disease stage 3 & 4 any CD4 & CD4<350 Only if necessary
 or another condition that dictated the use of antiretroviral")
7 Strategic Timing of ART (START) study Study to explore the benefits of starting asymptomatic HIV-positive patients on antiretroviral therapy who have a CD4 of >350 cells/mm 3 2 arms to this study: *or until the development of the acquired immunodeficiency syndrome (AIDS) or another condition that dictated the use of antiretroviral therapy

8 Highlights of IAS 2015 clinicaloptions.com/hiv START: Immediate vs Deferred Therapy for Asymptomatic, ART-Naive Pts Study closed by DSMB following interim analysis HIV-positive, ART-naive adults with CD4+ cell count > 500 cells/mm 3 (N = 4685) Immediate ART ART initiated immediately following randomization (n = 2326) Deferred ART Deferred until CD4+ cell count 350 cells/mm 3, AIDS, or event requiring ART (n = 2359) INSIGHT START Study Group. N Engl J Med. 2015;[Epub ahead of print]. Lundgren J, et al. IAS Abstract MOSY0302.
9 Highlights of IAS 2015 clinicaloptions.com/hiv START: 57% Reduced Risk of Serious Events or Death With Immediate ART 4.1% vs 1.8% in deferred vs immediate arms experienced serious AIDS or non- AIDS related event or death (HR: 0.43; 95% CI: ; P <.001) Cumulative Percent With Event Mo Deferred ART Immediate ART INSIGHT START Group. N Engl J Med. 2015;[Epub ahead of print]. Lundgren J, et al. IAS Abstract MOSY0302. Reproduced with permission.
10 Highlights of IAS 2015 clinicaloptions.com/hiv START: Cancer Events With Immediate vs Deferred ART Cancer Event, n Immediate ART (n = 2326) Deferred ART (n = 2359) Total Kaposi s sarcoma 1 11 Lymphoma, NHL + HL 3 10 Prostate cancer 2 3 Lung cancer 2 2 Anal cancer 1 2 Cervical or testis cancer 1 2 Other types* 4 9 Cumulative % With Event Time to Cancer Event Rate/100 PY: immediate, 0.20; deferred, 0.56 (HR: 0.36; 95% CI: ; P =.001) Mo Deferred ART Immediate ART *Immediate ART: squamous cell carcinoma, plasma cell myeloma, bladder cancer, fibrosarcoma. Deferred ART: gastric adenocarcinoma, breast cancer, ureteric cancer, malignant melanoma, myeloid leukemia, thyroid cancer, leiomyosarcoma, liver cancer, squamous cell carcinoma of head and neck. INSIGHT START Group. N Engl J Med. 2015;[Epub ahead of print]. Lundgren J, et al. IAS Abstract MOSY0302. Reproduced with permission.
11 Date of preparation: August /UK/12-08/MMAR/1019 HPTN 052 Prevention of HIV with Early Antiretroviral Therapy Multicenter, international, randomized, NIH-funded Phase III study HIV serodiscordant adult couples ART-naïve, HIV-infected partner CD4 between N=1,763 couples HIV infected partner: 50% male Early Arm (n=886) Start ART when CD4 between Delayed Arm (n=877) Start ART when CD4 250 or AIDS diagnosis Primary Clinical Endpoint (in HIV-positive partner) Clinical Event: Pulmonary tuberculosis, severe bacterial infection, a World Health Organization stage 4 event, or death 41% relative risk reduction in clinical events with early vs. delayed treatment Primary Prevention Endpoint (in HIV-negative partner) Linked HIV transmission to HIV-1 negative partners DSMB recommended study be stopped early on 28 th April DSMB = Data and Safety Monitoring Board Adapted from Cohen MS, et al. N Engl J Med 2011;365:
12 HTPN052 transmission results 39 transmissions in study 35 delayed treatment arm of which 27 linked 4 in immediate treatment arm (p<0.001) of which 1 linked Immediate tx arm = 96% reduction linked HIV transmission In multivariate analysis associated with increased risk of linked transmission: higher baseline CD4+ cell count higher baseline HIV-1 RNA reduced condom use 12
13 HTPN052 clinical outcomes results This is the first RCT to examine benefits of ART initiated at CD4 count between compared to <250 There was a trend towards a shorter time to a primary clinical event (AIDS and non-aids defining) with delayed compared to immediate therapy (HR=1.4, p=0.07) Delayed therapy was associated with a significantly shorter time to AIDS events and TB Non-AIDS defining events were rare and similar between arms The overall incidence of clinical events was significantly lower in patients on immediate therapy (IRR=0.8, P=0.02) This difference was driven by clinical events directly related to HIV infection (e.g. TB, HSV, Zoster, Candida and skin conditions)
14 What to start: antiretroviral agents

15 Classes of ARV drugs Plus Cobicistat boosting agent for elvitegravir, darunavir or atazanavir

16 HIV lifecycle 1. Binding to CD4 cell 2. Reverse transcription of RNA to DNA 3. Integration 4. Transcription into nucleic DNA 5. Translation from mrna 6. Viral assembly 16



17

18
19 Nucleoside/tide Reverse Transcriptase Inhibitors First drug available to treat HIV AZT (Zidovudine) in 1987 Often backbone of therapy Mimic natural purine and pyrimidine bases, competitive inhibition of reverse transcriptase enzyme Action Incorporated into DNA terminate the DNA chain incomplete parts of DNA Excretion: unchanged in urine so interactions minimal
20 Key Adverse effects: NRTIs Most occur within first 1/12 and are transient, class effects All drugs: nausea, vomiting, diarrhoea Abacavir hypersensitivity reaction (HLAB5701 positive) CV risk D.A.D. study D drugs: pancreatitis, lactic acidosis and peripheral neuropathy Stavudine & zidovudine: lipodystrophy Tenofovir DF an NtRTI Hypophosphotaemia: SPC recommends initial weekly monitoring Renal effects: Fanconi syndrome Reduced BMD


21
22 Non-Nucleoside/tide Reverse Transcriptase Inhibitors Action Non-competitive, selectively binds to the enzyme inactivates catalytic site, preventing pro-viral DNA synthesis of HIV-1 Metabolised by CYP450 enzyme system Levels may be affected by other drugs Drug CYP iso-enzymes induced CYP iso-enzymes inhibited Efavirenz Potent 3A4, strong 2B6 Potent 3A4, moderate 2C9 & 2C19 Etravirine Weak 3A4 Weak 2C9, moderate 2C19 Nevirapin e Potent 3A4 & 2B6 - Rilpivirine Moderate 2C19, slight 1A2, 2B6, 3A4 -
23 Key Adverse Effects - NNRTIs Rash Most common with Nevirapine (black box warning) May be able to treat through Rare: Stephen s-johnson Syndrome CNS toxicity Most common with efavirenz Often resolves within few weeks Hepatotoxicity Most common with OD nevirapine (2NN study) LFT s checked every 2/52 for first month Caution in Hepatitis B and C patients Rare: fulminant hepatitis


24
25 Lopinavir 3A4 & 2D6 lesser extent UGT, Possibly 1A2, 2C19, 2C9 Protease Inhibitors Act directly on the protease enzyme to stop the final stage of the HIV lifecycle Action: Stop maturation of the viral particle by enzyme cleavage of proteins Metabolised by 3A4 levels may be affected by other drugs Boosted PI: Low dose ritonavir is utilised as CYP3A4 inhibitor decrease dose or frequency Drug Ritonavir CYP iso-enzyme inhibited Potent (in order) 3A>2D6>2C9, 2C19>> 2A6,2E1 UGT enzymes CYP iso-enzyme induced Other 1A2, 2B6, 2C9, 2C19 Induces glucoronidation Inhibits P-gp, OATP1B1/1B3 & MATE1 Atazanavir 3A4, UGT1A1, weak 2C8 - Boosted induces glucoronidation Darunavir 3A4 - -
26 Key Adverse effects - PIs All PIs Fatigue, nausea, diarrhoea short-term Lipid, hepatic & metabolic effects Ritonavir Metallic taste, bloating Atazanavir Hyperbilirubinaemia, jaundice & renal stones Darunavir Sulfonamide allergy, rash Kaletra GI effects, dyslipidaemia & high triglycerides
27 Cobicistat Licensed pharmacokinetic enhancer but no antiviral activity Used as an alternative to ritonavir boosting with PI s and with elvitegravir in Stribild or Genvoya Strong inhibitor of CYP3A4 enzyme but less so of other CYP agents, different interaction profile to RTV Impairs renal tubular secretion of creatinine resulting in small increase in serum Cr, but does not affect gfr


28

29
30 Integrase Inhibitors Prevent integration of viral DNA into host genome DDI: PPIs and antacids / chelation Raltegravir First licensed Integrase. Requires BD dosing Elvitegravir (as Stribild) Requires boosting with Cobicistat, CYP3A4 inhibitor Do not start if baseline CrCl<70mls / min Dolutegravir Once daily except in integrase resistance BD dose DDI UGT inhibitors or inducers will impact DTG 30
31 Key Adverse Effects - INIs Generally they are all well tolerated RAL Report of transient GI effects Rash DTG CNS toxicities insomnia mainly Rash / hypersensitivity EVG/COB Nausea and diarrhoea RTV like effects
32 Entry Inhibitors Fusion inhibitor: Enfuvirtide (T-20) Binds to HIV gp-41 and thus inteferes with entry to CD4 cells Administered by sub-cutaneous injection BD Rarely used Key side effects local injection site reactions CCR5 antagonist: Maraviroc Selective antagonist, blocks interaction between human CCR5 and HIV gp120 preventing cell entry Need tropism or geno-to-pheno CCR5 at baseline CYP3A4 substrate so dosing varies dependent on other ARVs Key side effects GI, cough, rash & hepatotoxicity 32



33
34 What to start: guidelines
35 A brief history of HIV treatment 1987 Zidovudine available (monotherapy given) By TC, DDI and DDC licensed 1996 First PI saquinavir launched Delta study showed 2 drugs better than ACTG320 trial showed improved mortality and morbidity with 3 drugs vs CDC guidelines Hit early, hit hard New Millennium toxicity, liver morbidities, do not start tx until CD4<250 Since 2008 start CD4<350, better comparison between treatments 2012 Treatment as Prevention; availability of generics 2015 START: Treatment of all people living with HIV
36 PROGRESSION TO AIDS/DEATH 30 % of patients progressing No therapy Mono-therapy Dual-therapy 8 Triple therapy Months JAMA 1998 & CMAJ
37 How has Treatment Changed Since 1997 Atripla 2008 Combivir Nevirapine 2000 Stavudine Didanosine Indinavir 1997 In 1997 the medication patients took was not only larger and greater in number but also meant they had to plan all meals carefully! Breakfast Lunch Dinner 6am 12pm 6pm 12am

38 HAART / cart Highly Active Anti-Retroviral Therapy (combination therapy) Aims Extend life expectancy HIV now considered a chronic condition Higher quality of life Improve/strengthen the immune system s function Prevention of further transmission Actions Reduce HIV viral load to below detectable levels <40 copies/ml Increase CD4 counts
39 TDF + 3TC (or FTC) + EFV AZT + 3TC + EFV Regimens containing ABC or Guideline Recommended Alternative Comments BHIVA (2015) EACS (Oct 15) TDF/FTC (Truvada) or TAF/ FTC RPV^ ATV/r DRV/r EVG/c RAL DTG TFV/FTC + RPV^ TFV/FTC + DRV/r TFV/FTC + RAL ABC/3TC + DTG (ANY VL) TFV/FTC + DTG TFV/FTC + EVG/c if CrCl> 70mls/min ABC*^/3TC (Kivexa) EFV ABC/3TC* + RAL TFV/FTC + EFV ABC/3TC* + EFV TFV/FTC or ABC/3TC* + ATZ/r TFV/FTC or ABC/3TC* + ATZ/c ABC/3TC* + DRV/r TFV/FTC or ABC/3TC* + DRV/c TFV/FTC + LPV/r Alternative combinations: DRV/r + RAL* LPV/r + 3TC *if HLAB5701 negative ^ if VL<100,000 copies/ml except when ABC/3TC with DTG Guidelines do not consider cost-effectiveness & thus there may be further national or local guidelines in place Generics only if do not break FDC *if HLAB5701 negative & caution if high CVD risk & VL>100K ^ if VL<100,000 copies/ml * If CD4>200 & VL<100K US-DHSS (Jul 16) DTG + ABC*/3TC DTG + TDF/FTC or TAF/FTC RAL + TDF/FTC or TAF/FTC EVG/c + TDF/FTC or TAF/FTC DRV/r + TDF/FTC + TAF/FTC DRV/r# + ABC*/3TC ATV/r# + TDF/FTC RAL + ABC*/3TC EFV + TDF/FTC RPV + TDF/FTC^ & CD4>200 Alternative combinations only recommended if both TDF & ABC are contra-indicated * if HLAB5701 negative ^ if VL<100,000 copies/ml # Cobicistat instead of ritonavir an option
40 BHIVA 2015: What to start with NRTI backbone Third Agent Preferred Tenofovir DF + emtricitabine (Truvada) Tenofovir AF + Emtricitibine (Descovy) Atazanavir/ritonavir Darunavir/ritonavir Dolutegravir Rilpivirine 2 Elvitegravir/cobicistat Raltegravir Alternative Abacavir 1,3 + lamivudine (2) (Kivexa) Efavirenz 1. Contraindicated if HLA B*5701 positive 2. Not recommended if baseline viral load greater than 100,000 copies/ml 3. Not recommended if high estimated cardiovascular risk (see Section 6.6 Cardiovascular disease) Churchill D et al BHIVA treatment guidelines
41 Naïve studies for ARVs EFV RPV RAL EVG/c DTG ATV/r DRV/r EFV ECHO THRIVE STARTMRK GILEAD 102 SINGLE ACTG5202 X RPV ECHO THRIVE X X X X X RAL STARTMRK X X SPRING-2 ACTG5257 ACTG5257 EVG/c GILEAD 102 X X X GILEAD 103 X DTG SINGLE X SPRING-2 X X FLAMINGO ATV/r ACTG5202 X ACTG5257 GILEAD 103 X ACTG5257 DRV/r X X ACTG5257 X FLAMINGO ACTG5257
42 What to Start With: 2NRTIs + NNRTI Recommended Rilpivirine VL<100K Alternative Efavirenz Studied extensively vs. NVP, RPV, RAL, DTG, EVG/c & ATV Recent studies have shown impact of side effect profile on outcome, hence this is now alternative Easier adherence But low resistance barrier Consider primary resistance 42

43 What to start with: 2NRTIs + INI Recommended: Raltegravir or Elvitegravir/ cobicistat or dolutegravir 50mg OD No direct head-head between all 3 DTG vs. RAL (Spring 2)
44 What to Start With: 2NRTIs + boosted PI Recommended: Boosted Atazanavir or Darunavir 800mg OD first line ATV/r versus DRV/r versus Raltegravir (ACTG5257) Less resistance at virological failure But - possible increased toxicity and drug interactions 44
45 NRTI backbone choice 3TC or FTC plus one of: Preferred -Tenofovir DF or Tenofovir AF Alternative - Abacavir if HLA b5701 negative & VL <100K (unless with DTG) Co-formulations Kivexa abacavir + 3TC OD Truvada tenofovir DF + FTC OD Descovy tenofoir AF + FTC OD 45
46 ACTG 5202 Study Design HIV-1 RNA 1000 c/ml Any CD4+ count > 16 years of age Arm A TDF/FTC QD ABC/3TC Placebo QD EFV QD Phase IIIb ART-naive 1857 enrolled Randomised 1:1:1:1 Stratified by screening HIV-1 RNA (< or 100,000 c/ml) B C ABC/3TC QD TDF/FTC Placebo QD TDF/FTC QD ABC/3TC Placebo QD EFV QD ATV/r QD Enrolled Followed through Sept 2009, 96 wks after last pt enrolled D ABC/3TC QD TDF/FTC Placebo QD ATV/r QD Daar, E. et al. 17th CROI, San Francisco, CA, 2010, presentation 59LB. 46
47 ACTG 5202 ABC/3TC vs TDF/FTC high viral load stratum ABC/3TC vs. TDF/FTC: primary virologic endpoint (High viral load stratum at DSMB action) ABC/3TC vs. TDF/FTC with Hazard Ratio EFV HR 2.46 (95% CI 1.20, 5.25) ATV/r HR 2.22 (95% CI, 1.19, 4.14) -4 Favors ABC/3TC 1 Favors TDF/FTC 5 Daar, E. et al. 17th CROI, San Francisco, CA, 2010, presentation 59LB. 47
48 ACTG 5202 ABC/3TC vs TDF/FTC low viral load stratum ABC/3TC vs. TDF/FTC: primary virologic endpoint (Low viral load stratum; n=1060) ABC/3TC vs. TDF/FTC with Hazard Ratio (whole study) EFV HR 1.23 (95% CI, 0.77,1.96) Probability VF free at Week 96: 87.4% vs 89.2% diff -1.8% (95% CI -7.5, 3.9) ATV/r HR 1.26 (95% CI, 0.76,2.05) Probability VF free at Week 96: 88.3% vs 90.3% diff -2.0% (95% CI -7.5, 3.4) -4 Favors ABC/3TC 1 Favors TDF/FTC 5 Daar, E. et al. 17th CROI, San Francisco, CA, 2010, presentation 59LB. 48
49 ACTG 5202 Atazanavir/r vs Efavirenz overall population Primary Efficacy Endpoint Time to Virologic Failure (ITT) Atazanavir/r vs Efavirenz overall population Hazard Ratio (whole study) Atazanavir/r vs. Efavirenz with ABC/3TC HR 1.13 (95% CI 0.82, 1.56) Probability VF free at Week 96: 83.4% vs 85.3% diff -1.9% (95% CI -6.8, 2.6) TDF/FTC HR 1.01 (95% CI 0.7, 1.46) Probability VF free at Week 96: 89% vs 89.8% diff -0.8% (95% CI -4.9, 3.3) 0 Favors ATV/r 1 Favors EFV 2 Daar, E. et al. 17th CROI, San Francisco, CA, 2010, presentation 59LB. 49
50 HIV/AIDS Update From Boston 2014 clinicaloptions.com/hiv ACTG 5257: Open-Label ATV/RTV vs RAL vs DRV/RTV in First-line ART Stratified by HIV-1 RNA < or 100,000 c/ml, participation in metabolic substudy, CV risk Wk 96 after last patient enrolled ART-naive patients with HIV-1 RNA 1000 c/ml (N = 1809) ATV/RTV 300/100 mg QD + TDF/FTC (n = 605) RAL 400 mg BID + TDF/FTC (n = 603) DRV/RTV 800/100 mg QD + TDF/FTC Primary endpoints (n = 601) Virologic failure: time to HIV-1 RNA > 1000 c/ml (at Wk 16 or before Wk 24) or > 200 c/ml (at or after Wk 24) Tolerability failure: time to discontinuation of randomized component for toxicity Composite endpoint: the earlier occurrence of either VF or TF in a given participant Switch of regimens allowed for tolerability Landovitz R, et al. CROI Abstract 85.
51 HIV/AIDS Update From Boston 2014 clinicaloptions.com/hiv ACTG 5257: Primary Endpoint Analyses at Wk 96 Virologic Failure Tolerability Failure Composite Endpoint Regimens equivalent in time to VF Significantly greater incidence of treatment failure with ATV/RTV vs RAL or DRV/RTV In part due to high proportion of pts with hyperbilirubinemia Considering both efficacy and tolerability, RAL superior to either boosted PI DRV/RTV superior to ATV/RTV ATV/RTV vs RAL 3.4% (-0.7 to 7.4) DRV/RTV vs RAL 5.6% ( ) ATV/RTV vs DRV/RTV -2.2% (-6.7 to 2.3) Favors RAL ATV/RTV vs RAL 13% ( ) DRV/RTV vs RAL 3.6% ( ) Favors DRV/RTV ATV/RTV vs DRV/RTV 9.2% ( ) Difference in 96-Wk Cumulative Incidence (97.5% CI) Landovitz R, et al. CROI Abstract 85. Reproduced with permission Favors RAL ATVRTV vs RAL 15% (10-20) Favors RAL DRV/RTV vs RAL 7.5% ( ) Favors DRV/RTV ATV/RTV vs DRV/RTV 7.5% ( )
52 HIV/AIDS Update From Boston 2014 clinicaloptions.com/hiv ACTG 5257: Virologic Efficacy In ITT analysis with ART changes allowed (per protocol), regimens similar in virologic efficacy at Wk 96 and through Wk 144 In ITT analysis when change = failure (Snapshot), RAL superior to both boosted PIs at Wk 96 and DRV/RTV superior to ATV/ RTV at Wks 96 and 144 Similar mean change in CD4+ count across arms ATV/RTV (+284); RAL (+288) DRV/RTV (+256) cells/mm 3 Proportion With HIV-1 RNA 50 c/ml ITT, Regardless of ART Change 94% 89% 88% ITT, NC = Failure (Snapshot) 80% 73% 63% RAL DRV/RTV ATV/RTV RAL DRV/RTV ATV/RTV Landovitz R, et al. CROI Abstract 85. Reproduced with permission Study Wk







53
54 ARV Generics Already some ARV generics in UK Lamivudine & efavirenz most commonly used Key 1 st line agents soon going generic: Kivexa in Dec 2016 & tenofovir in July 2017 savings for NHS over next 5 years (Hill et al) Switch from single to multi-tablet regimens Engagement & education of patients and clinicians 54
55 Monitoring treatment BHIVA Guidelines 2016
56 Counselling patients starting treatment 2 way conversation, answer questions and address concerns Practical details on medication itself: What medication is called, details of administration, food requirements, dose timings How treatment works & will be monitored Understanding of disease, CD4 & VL, importance of adherence, drug resistance, treatment plan and goal of treatment Other points: Drug-drug interactions, travelling with medications What to do if missed/ late dose, vomits post-take Contact details for staff and clinics, OOH
57 ART initiation: Baseline Within 3 months before starting ART History: adherence, medication, drug & EtOH use, vaccination, knowledge & beliefs re: HIV, social hx Examination: weight, BP, BMI, waist circumference Assessment: CVD risk, fracture risk in over 50s Investigations FBC, U&E, LFT, lipid & bone profiles, urinalysis, UP:Cr CD4 & VL, VRT (not integrase unless indicated) HLAB*5701 / tropism if ABC / MVC considered HBV & HCV status
58 ART initiation: cont Re-assess patient within 2-4 weeks of starting treatment and repeat each visit first 6/12 History Side effects Adherence Investigations Renal and liver profile CD4 after 3/12 if <350 or repeat annually VL at 1, 3 & 6 months Should fall 10-fold within 1/12, otherwise repeat at 8/52 Should be undetectable within 6/12
59 Monitoring of undetectable ART History: medication hx & drug use, adherence, mood, adverse effects & patient concerns Examination: weight, BP, targeted physical exam, if new symptoms or signs Investigations: Cr, egfr, LFTs, glucose, bone profile, urinalysis, UP:Cr, VL every 6/12 patients Annual CVD risk & lipid profile if >40yrs, smoker or obese STI & Hepatitis status FBC, renal & liver profile Cervical cytology (women) Other assessments Fracture risk (FRAX score) in pts >50yrs every 3 yrs CD4 every year if >200; if >350 on 2 occasions >1yr apart only

60 Drug-drug interactions
61 Interactions Most likely to occur with NNRTIs and PI s as these go through and affect the Cytochrome P450 system in the liver Tenofovir also interacts with some ARV s AZT myelosuppressive use cautiously with similar agents Maraviroc substrate for CYP Raltegravir - glucoronidation Always check interaction status Consider following: Meds from other sources e.g. GP, dentist, OTC Herbal meds (e.g. St. John s Wort and PI s) Recreational / Party drugs (e.g. poppers, Chemsex) Contraception Impact of GI motility or acidity on drugs 61
62 To avoid problems Check for potential interactions (contact HIV pharmacist if necessary) If interaction is unavoidable what is the expected outcome? ie toxicity or failure of ARV or co-prescribed drug(s) Can you monitor for toxicity or adjust dose of coprescribed drug? eg reduce atorvastatin dose when prescribed with PI Therapeutic drug monitoring (TDM) of ARVs NNRTIs and PIs
63 Common interactions PPIs, antacids & rilpivirine rilpivirine to sub-optimal levels Steroid injections / inhalers & PI s levels corticosteroids Cushing s syndrome Simvastatin & PI s Simvastatin concentrations ~200% PI s and G potentially fatal increase in G levels 63
64 Drug interactions Prescribers of ARV need a good understanding of basic pharmacology principles to ensure effective and appropriate prescribing It is very important to consider potential drug interactions- this can not be over emphasised Places to look: - the bible! drugs_interact.html the lesser known bible - SPCs

65
66 Switching treatment
67 Reasons for switch Toxicity Virological failure Co-morbidity Management of drug-drug interactions Treatment simplification Patient preference New clinical data Cost Locally ~8% switch treatment annually 1 1 Boyle et al Int Cong HIV Tx and Inf 2012,


68 Reasons for switching ARVs in cohort of patients at C&W Boyle et al, BHIVA 2012 oral abstract O28
69 Switching treatment: Key points Consider combinations being switched: Interactions between old and new agents? Patient counselling Old stocks of medications Patient VL status at time of switch Other co-morbidities or medications
70 Switching practicalities Switching one agent Usually for toxicity Review resistance profile pre-switch Switching due to virological failure Low level viraemia or blip repeat VL Check adherence & drug Hx Resistance test +/- tropism Where possible switch whole combination to 3 active drugs as soon as possible
71 Useful links

72 Questions
Antiretroviral Dosing in Renal Impairment
 Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
HIV Treatment Update. Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London
 HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
HIV - Therapy Principles
 HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Antiretroviral Therapy: What to Start
 FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
 Antiretroviral Medications: What you need to know Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Associate Professor, Department of Pharmacy Practice Jefferson College of Pharmacy, Thomas Jefferson University
Antiretroviral Medications: What you need to know Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Associate Professor, Department of Pharmacy Practice Jefferson College of Pharmacy, Thomas Jefferson University
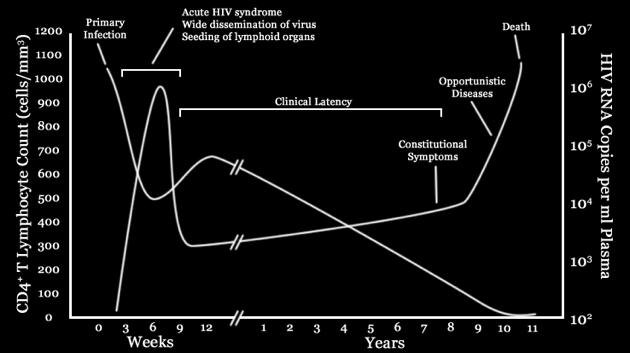
This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts
 1 2 This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts decreased. This period of acute infection or serocnversion
1 2 This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts decreased. This period of acute infection or serocnversion
HIV Treatment: State of the Art 2013
 HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
Simplifying HIV Treatment Now and in the Future
 Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
The next generation of ART regimens
 The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
The ART of Managing Drug-Drug Interactions in Patients with HIV
 The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches
 Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Principles of Antiretroviral Therapy
 Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
HIV Treatment: New and Veteran Drugs Classes
 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
Selecting an Initial Antiretroviral Therapy (ART) Regimen
 Regimen") Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
BHIVA antiretroviral treatment guidelines 2015
 BHIVA antiretroviral treatment guidelines 2015 Duncan Churchill Brighton & Sussex University Hospitals NHS Trust Laura Waters Mortimer Market Centre, CNWL Duncan Churchill GENERAL POINTS & WHEN TO START
BHIVA antiretroviral treatment guidelines 2015 Duncan Churchill Brighton & Sussex University Hospitals NHS Trust Laura Waters Mortimer Market Centre, CNWL Duncan Churchill GENERAL POINTS & WHEN TO START
COMPREHENSIVE ANTIRETROVIRAL TABLE: ADULT DOSING, DOSAGE FORM MODIFICATIONS, ADVERSE REACTIONS and INTERACTION POTENTIAL
 Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
Are the current doses of ARV correct. Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine
 Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
Disclosures. Update on HIV Drug Therapy: A Case based Discussion. Case # 1: Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv
 Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Update Allegra CPD Day Program Port Elizabeth Dr L E Nojoko
 HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
Antiretroviral Treatment Strategies: Clinical Case Presentation
 Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
BHIVA guidelines on the treatment of HIV-1-positive adults with antiretroviral therapy. START & other changes
 BHIVA guidelines on the treatment of HIV-1-positive adults with antiretroviral therapy START & other changes Contents Introduction & treatment aims Major changes When to start What to start BHIVA: what
BHIVA guidelines on the treatment of HIV-1-positive adults with antiretroviral therapy START & other changes Contents Introduction & treatment aims Major changes When to start What to start BHIVA: what
Continuing Education for Pharmacy Technicians
 Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
ART: The New, The Old and The Ugly
 ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
STRIBILD (aka. The Quad Pill)
") NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
Didactic Series. CROI 2014 Update. March 27, 2014
 Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
SA HIV Clinicians Society Adult ART guidelines
 SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
INTERGRASE INHIBITORS- WHAT S NEW?
 INTERGRASE INHIBITORS- WHAT S NEW? Professor Margaret Johnson Royal Free London Foundation Trust October 2018 Targeting the HIV life-cycle NEW HIV VIRON MATURATION CO-RECEPTOR BINDING FUSION BUDDING CD4
INTERGRASE INHIBITORS- WHAT S NEW? Professor Margaret Johnson Royal Free London Foundation Trust October 2018 Targeting the HIV life-cycle NEW HIV VIRON MATURATION CO-RECEPTOR BINDING FUSION BUDDING CD4
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
Antiretroviral Drugs
 Antiretroviral Drugs Dr Paddy Mallon UCD HIV Molecular Research Group Associate Dean for Research and Innovation UCD School of Medicine and Medical Science paddy.mallon@ucd.ie UCD School of Medicine &
Antiretroviral Drugs Dr Paddy Mallon UCD HIV Molecular Research Group Associate Dean for Research and Innovation UCD School of Medicine and Medical Science paddy.mallon@ucd.ie UCD School of Medicine &
The Future of HIV: Advances in Drugs and Research. Shauna Gunaratne December 17, 2018
 The Future of HIV: Advances in Drugs and Research Shauna Gunaratne December 17, 2018 Overview Epidemiology Science of HIV How HIV treatment and management have changed over the years New medicines and
The Future of HIV: Advances in Drugs and Research Shauna Gunaratne December 17, 2018 Overview Epidemiology Science of HIV How HIV treatment and management have changed over the years New medicines and
Actualización y Futuro en VIH
 Actualización y Futuro en VIH Dr. Santiago Moreno Servicio de Enfermedades Infecciosas Hospital U. Ramón y Cajal. Universidad de Alcalá. IRYCIS. Madrid Agenda Control of the HIV-epidemic Coinfections Antiretroviral
Actualización y Futuro en VIH Dr. Santiago Moreno Servicio de Enfermedades Infecciosas Hospital U. Ramón y Cajal. Universidad de Alcalá. IRYCIS. Madrid Agenda Control of the HIV-epidemic Coinfections Antiretroviral
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
Clinical support for reduced drug regimens. David A Cooper The University of New South Wales Sydney, Australia
 Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
Clinical Commissioning Policy: Use of cobicistat (Tybost ) as a booster in treatment of HIV positive adults and adolescents
 as a booster in treatment of HIV positive adults and adolescents") Clinical Commissioning Policy: Use of cobicistat (Tybost ) as a booster in treatment of HIV positive adults and adolescents 1 Clinical Commissioning Policy: Use of cobicistat (Tybost ) as a booster in
Clinical Commissioning Policy: Use of cobicistat (Tybost ) as a booster in treatment of HIV positive adults and adolescents 1 Clinical Commissioning Policy: Use of cobicistat (Tybost ) as a booster in
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
SELECTING THE BEST ART FOR EACH PATIENT
 SELECTING THE BEST ART FOR EACH PATIENT Corklin R Steinhart, MD, PhD Head, Global Medical Directors ViiV Healthcare CNVX/HIVP/0025/16 5th Asian Conference on Hepatitis & AIDS 第五届亚洲肝炎与艾滋病学术会议 28-29 May
SELECTING THE BEST ART FOR EACH PATIENT Corklin R Steinhart, MD, PhD Head, Global Medical Directors ViiV Healthcare CNVX/HIVP/0025/16 5th Asian Conference on Hepatitis & AIDS 第五届亚洲肝炎与艾滋病学术会议 28-29 May
12th European AIDS Conference / EACS ARV Therapies and Therapeutic Strategies A CME Newsletter
 EACS 2009 11-14, November 2009 Cologne, Germany Course Director Jürgen K. Rockstroh, MD Co-Chairman, 12th European AIDS Conference Professor, University of Bonn Bonn, Germany Faculty Calvin Cohen, MD,
EACS 2009 11-14, November 2009 Cologne, Germany Course Director Jürgen K. Rockstroh, MD Co-Chairman, 12th European AIDS Conference Professor, University of Bonn Bonn, Germany Faculty Calvin Cohen, MD,
TDF containing ART: Efficacy and Safety. Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia
 TDF containing ART: Efficacy and Safety Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia 1 Indications Treatment of HIV-1 in combination with other antiretroviral
TDF containing ART: Efficacy and Safety Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia 1 Indications Treatment of HIV-1 in combination with other antiretroviral
COMPETING INTEREST OF FINANCIAL VALUE
 BHIVA AUTUMN CONFERENCE 2012 Including CHIVA Parallel Sessions Dr Ian Williams University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Ian Williams
BHIVA AUTUMN CONFERENCE 2012 Including CHIVA Parallel Sessions Dr Ian Williams University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Ian Williams
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV
 POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
HIV 101. Applications of Antiretroviral Therapy
 HIV 101. Applications of Antiretroviral Therapy Michael S. Saag, MD Professor of Medicine Associate Dean for Global Health Jim Straley Chair in AIDS Research University of Alabama at Birmingham Birmingham,
HIV 101. Applications of Antiretroviral Therapy Michael S. Saag, MD Professor of Medicine Associate Dean for Global Health Jim Straley Chair in AIDS Research University of Alabama at Birmingham Birmingham,
HIV Drugs and the HIV Lifecycle
 HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
An HIV Update Jan Clark, PharmD Specialty Practice Pharmacist
 An HIV Update - 2019 Jan Clark, PharmD Specialty Practice Pharmacist 2 The goal of this program is to provide a review and update of HIV care and to provide a forum for discussing the current local and
An HIV Update - 2019 Jan Clark, PharmD Specialty Practice Pharmacist 2 The goal of this program is to provide a review and update of HIV care and to provide a forum for discussing the current local and
COMPREHENSIVE ANTIRETROVIRAL TABLE: ADULT DOSING**, DOSAGE FORM MODIFICATIONS, ADVERSE REACTIONS and INTERACTION POTENTIAL
 COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir) Stavudine
COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir) Stavudine
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care
 Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
DRUGS IN PIPELINE. Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015
 DRUGS IN PIPELINE Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015 N(t)RTI The Development of TAF TAF Delivers the High Potency of TDF While Minimizing Off- Target Kidney and Bone Side Effects
DRUGS IN PIPELINE Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015 N(t)RTI The Development of TAF TAF Delivers the High Potency of TDF While Minimizing Off- Target Kidney and Bone Side Effects
Third Agent Advantages Disadvantages. Component Tenofovir/emtricitabine (TDF/FTC) 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily
 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily") Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
First line ART Rilpirivine A New NNRTI. Chris Jack Physician, Durdoc Centre ethekwini
 First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
ART Treatment. ART Treatment
 Naïve Experienced Strategies ARV in pregnancy ART Treatment Naïve studies: ART Treatment Abstract 37 Atazanavir/r vs Lopinavir/r: Castle study Abstract 774 Kivexa vs Truvada: HEAT study Abstract 775 Lopinavir/r
Naïve Experienced Strategies ARV in pregnancy ART Treatment Naïve studies: ART Treatment Abstract 37 Atazanavir/r vs Lopinavir/r: Castle study Abstract 774 Kivexa vs Truvada: HEAT study Abstract 775 Lopinavir/r
Case # 1. Case #1 (cont d)
") Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
SINGLE. Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects
 in treatment-naïve subjects") SINGLE Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects SE/HIV/0023/14 January 2014 PHASE III DTG TRIALS IN TREATMENT-NAÏVE ADULT SUBJECTS WITH HIV SINGLE 1 N=833 Phase III non-inferiority,
SINGLE Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects SE/HIV/0023/14 January 2014 PHASE III DTG TRIALS IN TREATMENT-NAÏVE ADULT SUBJECTS WITH HIV SINGLE 1 N=833 Phase III non-inferiority,
New HIV EACS and Italian Guidelines
 Original Article HIV correlated pathologies and other infections Marco Borderi New HIV EACS and Italian Guidelines Infectious Disease Unit - S. Orsola-Hospital - University of Bologna Corresponding author:
Original Article HIV correlated pathologies and other infections Marco Borderi New HIV EACS and Italian Guidelines Infectious Disease Unit - S. Orsola-Hospital - University of Bologna Corresponding author:
BHIVA Best of CROI Feedback Meetings. London Birmingham North West England Cardiff Gateshead Edinburgh
 BHIVA Best of CROI Feedback Meetings London Birmingham North West England Cardiff Gateshead Edinburgh BHIVA Best of CROI Feedback Meetings 2010 ANTIRETROVIRAL TREATMENT STRATEGIES AND NEW DRUGS A5202:
BHIVA Best of CROI Feedback Meetings London Birmingham North West England Cardiff Gateshead Edinburgh BHIVA Best of CROI Feedback Meetings 2010 ANTIRETROVIRAL TREATMENT STRATEGIES AND NEW DRUGS A5202:
HIV Management Update 2015
 9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
Integrase Strand Transfer Inhibitors on the Horizon
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Integrase Strand Transfer Inhibitors on the Horizon David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Integrase Strand Transfer Inhibitors on the Horizon David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, University of Washington Presentation
What are the most promising opportunities for dose optimisation?
 What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Antiretroviral Treatment 2014
 Activity Code FM285 Antiretroviral Treatment 2014 Rajesh Gandhi, MD Masssachusetts General Hospital Disclosures: Educational grants to my institution from Janssen, Viiv, Abbott Learning Objectives Upon
Activity Code FM285 Antiretroviral Treatment 2014 Rajesh Gandhi, MD Masssachusetts General Hospital Disclosures: Educational grants to my institution from Janssen, Viiv, Abbott Learning Objectives Upon
Friday afternoon Programme
 Friday afternoon Programme Pharmacology and TDM Dr Marta Boffito Consultant Physician, C&W Resistance to new anti-retrovirals Dr Steve Taylor Consultant Physician, Birmingham HIVPA Annual Conference 2008
Friday afternoon Programme Pharmacology and TDM Dr Marta Boffito Consultant Physician, C&W Resistance to new anti-retrovirals Dr Steve Taylor Consultant Physician, Birmingham HIVPA Annual Conference 2008
VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects
 VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects IL/DLG/0040/14 June 2014 GSK (Israel) Ltd. Basel 25, Petach Tikva. Tel-03-9297100 Medical information service: il.medinfo@gsk.com
VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects IL/DLG/0040/14 June 2014 GSK (Israel) Ltd. Basel 25, Petach Tikva. Tel-03-9297100 Medical information service: il.medinfo@gsk.com
Update on Antiretroviral Treatment for HIV Infection 2008
 Update on Antiretroviral Treatment for HIV Infection 2008 Janet Gilmour MD FRCP(C) Clinical Associate Professor of Medicine University of Calgary November 2008 Disclosure and Acknowledgements Disclosure:
Update on Antiretroviral Treatment for HIV Infection 2008 Janet Gilmour MD FRCP(C) Clinical Associate Professor of Medicine University of Calgary November 2008 Disclosure and Acknowledgements Disclosure:
Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi
 6 th INFECtivology TOday Paestum 15-16 -17 maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie
6 th INFECtivology TOday Paestum 15-16 -17 maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie
ARVs in Development: Where do they fit?
 The picture can't be displayed. ARVs in Development: Where do they fit? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker
The picture can't be displayed. ARVs in Development: Where do they fit? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker
Second-Line Therapy NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
Antiretroviral Treatment (ART) of Adult HIV Infection*
 of Adult HIV Infection*") Antiretroviral Treatment (ART) of Adult HIV Infection* Prepared by J Montaner for the BC- CfE Therapeutic Guidelines Committee of the British Columbia - Centre for Excellence in HIV/AIDS. *Based on M Thompson,
Antiretroviral Treatment (ART) of Adult HIV Infection* Prepared by J Montaner for the BC- CfE Therapeutic Guidelines Committee of the British Columbia - Centre for Excellence in HIV/AIDS. *Based on M Thompson,
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
 Initial Therapy for Antiretroviral Naïve HIV Infected Patients Michelle Cespedes, MD, MS Associate Professor of Medicine Division of Infectious Disease Icahn School of Medicine at Mount Sinai Disclosures
Initial Therapy for Antiretroviral Naïve HIV Infected Patients Michelle Cespedes, MD, MS Associate Professor of Medicine Division of Infectious Disease Icahn School of Medicine at Mount Sinai Disclosures
What next? Francois Venter. ART new drugs, new studies. Wits Reproductive Health & HIV Institute
 Thanks: Polly Clayden, Francesca Conradie, Loyd Mulenga, Gary Maartens, Andrew Hill, David Ripin, Elli Katabira, Chris Duncombe, Nathan Ford, Marco Vitoria, WHO Industry: Gilead, Janssen, ViivV Abbott,
Thanks: Polly Clayden, Francesca Conradie, Loyd Mulenga, Gary Maartens, Andrew Hill, David Ripin, Elli Katabira, Chris Duncombe, Nathan Ford, Marco Vitoria, WHO Industry: Gilead, Janssen, ViivV Abbott,
More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD
 More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD More Options, Some Opinions: Initial Therapies for HIV Judith S. Currier, MD University of California Los Angeles Los Angeles,
More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD More Options, Some Opinions: Initial Therapies for HIV Judith S. Currier, MD University of California Los Angeles Los Angeles,
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
WESTERN CAPE ART GUIDELINES PRESENTATION 2013
 WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
Medication Errors Focus on the HIV-Infected Patient
 Medication Errors Focus on the HIV-Infected Patient Nimish Patel, Pharm.D., Ph.D., AAHIVP Associate Professor Albany College of Pharmacy & Health Sciences I do not have any conflict of interest in relation
Medication Errors Focus on the HIV-Infected Patient Nimish Patel, Pharm.D., Ph.D., AAHIVP Associate Professor Albany College of Pharmacy & Health Sciences I do not have any conflict of interest in relation
London Therapeu-c Tender Implementa-on: Guidance for Clinical Use. 14 January 2015
 London Therapeu-c Tender Implementa-on: Guidance for Clinical Use 14 January 2015 Contents 2 3. General principles 4. Financial impact of therapeu-c tendering for branded ARVs 5. London ARV algorithm:
London Therapeu-c Tender Implementa-on: Guidance for Clinical Use 14 January 2015 Contents 2 3. General principles 4. Financial impact of therapeu-c tendering for branded ARVs 5. London ARV algorithm:
HIV in in Women Women
 HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
Treatment update. Bronagh McBrien June 2016
 Treatment update Bronagh McBrien June 2016 Speaker Name Bronagh McBrien Statement Received educational funding and support from Gilead, Merck, Boehringer Ingelheim, Janssen-Cilag Date : 27 June 2016 BHIVA
Treatment update Bronagh McBrien June 2016 Speaker Name Bronagh McBrien Statement Received educational funding and support from Gilead, Merck, Boehringer Ingelheim, Janssen-Cilag Date : 27 June 2016 BHIVA
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Didactic Series. Switching Regimens in the Setting of Virologic Suppression
 Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update
 Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
HIV MEDICATIONS AT A GLANCE. Atripla 600/200/300 mg tablet tablet daily. Complera 200/25/300 mg tablet tablet daily
 HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ alafenamide Emtricitabine/
HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ alafenamide Emtricitabine/
Fluconazole dimenhydrinate, diphenhydramine. Raltegravir or dolutegravir with antacids
 Supportive therapy Summary of interactions Table 1. Summary of potential interactions between antiretroviral agents and supportive therapy Interactions with enzyme inhibitors (protease inhibitors and elvitegravir/cobicistat)
Supportive therapy Summary of interactions Table 1. Summary of potential interactions between antiretroviral agents and supportive therapy Interactions with enzyme inhibitors (protease inhibitors and elvitegravir/cobicistat)
Exploring HIV in 2017: What a pharmacist needs to know
 Exploring HIV in 2017: What a pharmacist needs to know Lifecycle of the HIV virus a. HIV spread through mucous membrane contact, damaged tissue contact, or blood contact with: blood, semen, rectal fluids,
Exploring HIV in 2017: What a pharmacist needs to know Lifecycle of the HIV virus a. HIV spread through mucous membrane contact, damaged tissue contact, or blood contact with: blood, semen, rectal fluids,
Professor Jeffery Lennox
 BHIVA AUTUMN CONFERENCE 2014 Including CHIVA Parallel Sessions Professor Jeffery Lennox Emory University School of Medicine Atlanta, Georgia, USA 9-10 October 2014, Queen Elizabeth II Conference Centre,
BHIVA AUTUMN CONFERENCE 2014 Including CHIVA Parallel Sessions Professor Jeffery Lennox Emory University School of Medicine Atlanta, Georgia, USA 9-10 October 2014, Queen Elizabeth II Conference Centre,
Drug toxicities: Safest PIs. Michelle Moorhouse 14 Apr 2016
 Drug toxicities: Safest PIs Michelle Moorhouse 14 Apr 2016 Impact of PIs on AIDS mortality CDC.gov. Epidemiology of HIV infection. Evolution of PIs http://www.clinicaloptions.com/hiv/treatment%20updates/boosted%20pis/interactive%20virtual%20presentation/slideset.aspx
Drug toxicities: Safest PIs Michelle Moorhouse 14 Apr 2016 Impact of PIs on AIDS mortality CDC.gov. Epidemiology of HIV infection. Evolution of PIs http://www.clinicaloptions.com/hiv/treatment%20updates/boosted%20pis/interactive%20virtual%20presentation/slideset.aspx
0% 0% 0% Parasite. 2. RNA-virus. RNA-virus
 HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
Starting and Switching ART: 2016
 Starting and Switching ART: 2016 Luke Jerram Rajesh T. Gandhi, M.D. Massachusetts General Hospital Harvard Medical School Disclosures: grant support from EBSCO, Gilead, Merck, Viiv Thanks to Henry Sunpath,
Starting and Switching ART: 2016 Luke Jerram Rajesh T. Gandhi, M.D. Massachusetts General Hospital Harvard Medical School Disclosures: grant support from EBSCO, Gilead, Merck, Viiv Thanks to Henry Sunpath,
Switching antiretroviral therapy to safer strategies based on integrase inhibitors
 Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop
 HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
Structured Treatment Interruption in HIV Positive Patients. Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007
 Structured Treatment Interruption in HIV Positive Patients Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007 Objectives To become re-acquainted with the basics of HAART for HIV infection
Structured Treatment Interruption in HIV Positive Patients Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007 Objectives To become re-acquainted with the basics of HAART for HIV infection
treatment passport 1
 treatment passport 1 Why keep a treatment history? Keeping a short record of your treatment history can help in many ways. It can help you understand your health and treatment. It can help if your doctor
treatment passport 1 Why keep a treatment history? Keeping a short record of your treatment history can help in many ways. It can help you understand your health and treatment. It can help if your doctor
Kees Brinkman OLVG- Amsterdam The Netherlands
 integrase inhibitors in clinical practice in the Netherlands HIV Clinical Forum 2018 Kees Brinkman OLVG- Amsterdam The Netherlands Disclosures relevant activities to dislose companies advisory boards Gilead
integrase inhibitors in clinical practice in the Netherlands HIV Clinical Forum 2018 Kees Brinkman OLVG- Amsterdam The Netherlands Disclosures relevant activities to dislose companies advisory boards Gilead
Treatment experience in South Africa. Dr Ian Sanne Clinical HIV Research Unit University of the Witwatersrand
 Treatment experience in South Africa Dr Ian Sanne Clinical HIV Research Unit University of the Witwatersrand Overview South African Prevalence Adherence Combination ddi + d4t Nevirapine Hepatotoxicity
Treatment experience in South Africa Dr Ian Sanne Clinical HIV Research Unit University of the Witwatersrand Overview South African Prevalence Adherence Combination ddi + d4t Nevirapine Hepatotoxicity
Antiretroviral Therapy: Panel Discussion
 disclosures Antiretroviral Therapy: Panel Discussion Medical Management of HIV December 9, 217 Panelists: Harry Lampiris, MD; Annie Luetkemeyer, MD; Carina Marquez, MD Moderator: Oliver Bacon, MD none
disclosures Antiretroviral Therapy: Panel Discussion Medical Management of HIV December 9, 217 Panelists: Harry Lampiris, MD; Annie Luetkemeyer, MD; Carina Marquez, MD Moderator: Oliver Bacon, MD none
CROI 2013: New Drugs for Treatment and PrEP
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER CROI 2013: New Drugs for Treatment and PrEP Brian R. Wood, MD Medical Director, NW AETC Project ECHO Assistant Professor of Medicine, University of Washington
NORTHWEST AIDS EDUCATION AND TRAINING CENTER CROI 2013: New Drugs for Treatment and PrEP Brian R. Wood, MD Medical Director, NW AETC Project ECHO Assistant Professor of Medicine, University of Washington
Management of ART Failure. EACS Advanced HIV Course 2015 Dr Nicky Mackie
 Management of ART Failure EACS Advanced HIV Course 2015 Dr Nicky Mackie Outline Defining treatment success Defining treatment failure Reasons for ART failure Management of ART failure Choice of second
Management of ART Failure EACS Advanced HIV Course 2015 Dr Nicky Mackie Outline Defining treatment success Defining treatment failure Reasons for ART failure Management of ART failure Choice of second
Clinical Commissioning Policy: Use of cobicistat as a booster in treatment of HIV positive adults and adolescents
 Clinical Commissioning Policy: Use of cobicistat as a booster in treatment of HIV positive adults and adolescents Reference: NHS England F03/P/b NHS England INFORMATION READER BOX Directorate Medical Commissioning
Clinical Commissioning Policy: Use of cobicistat as a booster in treatment of HIV positive adults and adolescents Reference: NHS England F03/P/b NHS England INFORMATION READER BOX Directorate Medical Commissioning