Prof. Sandrine Florquin Department of Pathology Academic Medical Center University of Amsterdam Amsterdam, The Netherlands. Slide 1.
|
|
|
- Gary Parker
- 6 years ago
- Views:
Transcription

1 Interleukin 17 in renal biopsies as risk factor for progression Sandrine Florquin, Amsterdam, The Netherlands Chairs: Mohamed R. Daha, Leiden, The Netherlands Pierre Ronco, Paris, France Prof. Sandrine Florquin Department of Pathology Academic Medical Center University of Amsterdam Amsterdam, The Netherlands Slide 1 Slide 2


2 Good morning ladies and gentlemen, Mr Chairman. First of all, I would like to thank the organizing committee of this meeting for giving me the opportunity to discuss with you some issues about the role of IL-17 in renal allografts as a risk factor for progression. As far as the literature I know goes there is no published data about the role of these cytokines in primary renal disease, I will focus my talk on allograft biopsies. Slide 3 So as you all will know, acute rejection is a major risk for graft failure and most importantly late episodes of acute rejection are associated with an increased risk of graft loss. Also the severity and the type of acute rejection is associated with an increase of risk of graft loss and also rejection episodes of rejections resistant to conventional therapy is also associated with an increased graft loss. Slide 4


3 Beyond the classical direct and indirect pathway of alloreactivity leading to acute rejection, it's not recognising that other alternative pathways might also be playing a role in an episode of acute rejection. Among which the TH-2 type cells have been involved in these memory CD8+ T cells, TH-17 cells, B cells, natural Killer cells, eosinophils and neutrophils. Today I will focus on the role eventually of IL-17 in these pathways of acute rejection. Slide 5 So as you all will probably know, naïve T cells may differentiate into different types of

4 polarised T cells. For example, upon exposure in vitro to IFN-γ and IL-12 these naïve cells can actually differentiate into the so-called TH-1 T cells that are producing IFN-γ and other cytokines. Upon IL-4 and IL-2 exposure, these naive T cells might differentiate into TH-2 which is important for fighting parasites and also play a role in allergy and asthma. More recently, it has also been shown that these naive T cells in vitro upon exposure to TGF-β and IL-2 can differentiate into so-called regulatory T cells, which are characterised by the transcription factor FoxP3, and these cells are major players in immune tolerance and are secreting among other cytokines TGF-β and IL-10. More recently, even these naive T cells have been shown that upon exposure to TGF-β and IL-6, IL-21 and IL-23 might actually differentiate into the socalled TH-17 type of T cells which are major pro-inflammatory T cells which are important to fight extracellular bacteria, fungi and are playing also a role in autoimmunity and as recently has been shown also an important role in allograft rejection. Slide 6 IL-17 might be produced after activation of two different types of receptors. I will not go into the details but most importantly IL-17 might act on different cell types among which neutrophils, endothelial cells, keratinocytes and fibroblasts leading really to a spectrum of activity, recruitment of neutrophils leading to a lot of inflammation and also --- cells leading to an increase of vascular permeability but also angiogenesis. IL-17 has also been shown to induce metalloproteinases. So it's a major pleiotropic and pleomorphic I would say cytokine. Slide 7

5 Importantly IL-17 is a family of cytokines of 6 members, A to F among which A and F are the best characterised and studied. A and F are massively produced by the so-called TH-17. But most importantly, these cytokines might also be produced by other cell types among which CD8, natural cursors, gamma delta, neutrophils but also mastcells. It's important to remember that IL-17 A and F share among 50% of aminoacids. Slide 8

6 So what's known about IL-17 and allograft rejection? As I told you, there is nothing published at least about these cytokines and pulmonary renal disease but it's about 15 years ago already that Cees van Kooten from Leiden described that IL-17 might activate human renal epithelial cells in vitro and that these cytokines were expressed during allograft rejection. After there was kind of nothing and then about 5 years later the first publication came out studying the mrna levels of IL-17 in different settings of transplantation including renal transplantation, lung, liver and cardiac transplantation. But in all these studies the clinical relevance of IL-17 as well as the cellular source of these cytokines was not evaluated. Slide 9 So we aimed to evaluate the predictive value eventually of this IL-17 expression in allograft rejection upon acute rejection and also the cellular source of IL-17. Slide 10


7 For that we studied 3 different cohorts. First of all, the test cohort including 50 patients, a validation cohort also with 50 patients and control patients and 10 protocol renal biopsy were taken 6 months after transplantation without any significant histological features. Regarding acute rejection we had 40 pure I would say acute T cell-mediated rejections and 8 combined antibody-mediated rejections and T cells-mediated rejection. So we performed the BANFF classification and we performed double staining for IL-17 and T cells using CD3, mastcells for tryptase, neutrophils CD-15 and importantly we used a polyclonal antibody from R&D that was really extensively validated in our lab. These antibodies recognised both IL-17 A and F. We looked mostly for the response to conventional antirejection therapy and renal outcome in this setting. Slide 11 The 3 next slides will give you a characteristic expression I would say of IL-17 in the different settings. So here, we have the double staining for CD3 and IL-17. IL-17 being in blue and CD3 in red. As you see, upon acute rejection there are a lot of T cells invading the kidney. Here you have glomeruli where there is no counterstaining, a few single blue cells which are IL-17 positive cells. You can appreciate that in this infiltrate we could hardly find double positive cells such as these ones which are also here turning to purple, we have red and blue, turning to purple but they were really only a few cells that expressed both CD 3 and IL- 17.

8 Slide 12 In contrast when we stained for tryptase, a marker for mastcells and IL-17, we could find quite a lot of purple cells such as these ones, so meaning that quite a lot of mastcells were also expressing IL-17. Slide 13


9 This was also true for the neutrophil marker CD15 showing that a lot of these IL-17 positive cells were also neutrophils. Slide 14 So first, we looked at the potential to discriminate between protocol and acute rejection looking at these IL-17 positive cells. As you can see, hardly any IL-17 positive cells were found in protocol renal biopsy without histological changes after transplantation at 6 months. But in contrast, when we put all acute rejections together, we had a major increase in IL-17 positive cells invading the graft. You can see that it discriminates really well between no ejection and acute rejection. Slide 15

10 When we looked at the distribution of these IL-17 positive cells, we were quite surprised I would say to see that the majority of these IL-17 positive cells turned out to be neutrophils. That's the blue. About 25% were mastcells. Less than 1% of all IL-17 positive cells were T cells. So we also discarded I would say these double positive cells from further analysis because it was just one or two cells per renal biopsy so probably not really clinically relevant. Slide 16 So we focused on the mastcells and neutrophils and IL-17. This is the correlation between IL- 17 positive cell types and the BANFF score and clinical parameters at the time of renal biopsy. As you can see for all IL-17 positive cells there is a correlation with the total and inflammatory infiltrates meaning that IL-17 just parallels the inflammation in the renal biopsy and there is a negative correlation with the renal function at the time of biopsy. Interestingly, when we looked at the mastcells positive for IL-17, there was also a clear correlation with the tubular atrophy and interstitial fibrosis meaning that it might be that these mastcells producing IL-17 might be involved in fibrosis. But this is just a hypothesis that we have to test further. Slide 17


11 Importantly, we looked at the eventual role of potential prediction value of these IL-17 in response to therapy but we couldn't see any association between IL-17 positive cells and response to anti-rejection therapy and in line also no correlation between IL-17 positive cells, infiltration and CD4 positivity, so a marker for antibody-mediated rejection. Slide 18 So we performed univariate analysis. I will skip that but from this univariate analysis it turned out that 3 parameters were associated with the occurrence of late graft dysfunction defined as a graft function less than 30 ml/minute at the last follow-up or return to dialysis. These 3 parameters were the time from transplantation to biopsy. So late rejection was associated in the univariate analysis to late outcome as known in the literature and also the C4d positivity, so antibody-mediated rejection in this univariate analysis was associated with late graft dysfunction. But when we put the 3 parameters in the multivariate analysis, we found that one lady IL-17 positivity was associated with late renal outcome and it was true for poor renal function and return to dialysis. Slide 19


12 So we wanted to validate these findings in an independent cohort. So we included almost 50 additional renal biopsies and we performed the same staining. So in red you have the validation cohort and on the black line is the test cohort and as you can see, it's about the same showing that indeed the total IL-17 positive infiltrates correlate with a poor renal function at the last follow-up. So there is a clear correlation between a lot of IL-17 positive cells and poor late function and it is was also true for return to dialysis. After we looked at the best cut-off for the number of IL-17 positivity regarding sensitivity and specificity and we found that 4 IL-17 positive cells for each --- was the best cut-off in our study and using that we found in this Kaplan-Meier curve that indeed the renal biopsy with more than four IL-17 positive cells was associated with higher priority to graft dysfunction at last follow-up. The grey area is the 95% confidence interval. Slide 20 So clearly from this study we could say that yes IL-17 positivity parallels the inflammation in renal allograft upon acute rejection. That in our hands at least major sources of intragraft IL- 17 were neutrophils and mast cells, that we couldn't find any predictive value regarding the anti-rejection therapy response but that IL-17 infiltration in the renal biopsy independently predicts poor renal outcome.


13 Slide 21 In this study they had more or less the same conclusion but what they did is they included about 56 patients among which 40 were acute T cell-mediated rejections and 16 were combined T cell and antibody-mediated rejections. But in this study they also performed staining for FoxP3 disease, this transcription factor is characteristic for the regulatory T cells, so inducing tolerance and IL-17. They looked at response to therapy and 1- and 5-year graft survival. Slide 22 They performed just a single staining and this is an example of this publication showing single FoxP3 positive cells and a few IL-17 positive cells. In this study using this ratio between FoxP3, so tolerance inducer and IL-17 a potentially inflammatory inducer, they found that indeed the renal biopsy with a lot of FoxP3 and low IL-17 had a good response to steroids after rejection. But in contrast, they had a biopsy with a high ratio of IL-17 compared to FoxP3 had a poor response to steroid treatment. Also in this study combing FoxP3 and IL-17


14 they showed that renal biopsy with a high FoxP3 ratio had a good follow-up of allograft survival after 1 and 5 years after transplantation. In contrast and significantly the renal biopsy with a lot of IL-17 and low FoxP3 had poor prognosis. Slide 23 In this study, they also looked at the correlation eventually with the marker for antibodymediated rejection, C4d but they couldn't find any correlation between IL-17 and FoxP3 for this marker and indeed, they found that this high IL-17 FoxP3 ratio significantly correlated with steroid resistant rejection and also correlated with an allograft outcome in a multivariate analysis. So more or less comparable to our study. Slide 24 But in contrast, there was at the same time another study also looking at the same I would say namely the IL-17 expression in allografts upon acute rejection showing quite different results that I will discuss with you. In this study, they included 20 renal biopsies with acute

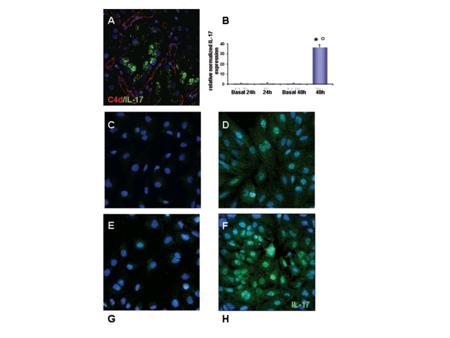
15 antibody-mediated rejection. Slide with T cells and they used another antibody and I would just like to go through these results showing that regarding T cell-mediated rejection we could find an increase in IL-17 cells. But interestingly in this study on antibody- mediated rejection they found mostly an expression of IL-17 in tubular epithelial cells and they performed also double staining showing that 80% of these IL-17 positive cells were T cells in contrast to our results showing that it's less than 1%. Slide 26
16 So a big discrepancy. Slide 27


17 I won't go into the details of the in vitro study which are really interesting but go to the conclusions of this study showing that most of these IL-17 positive T cells are CD14 cells in acute T cell-mediated rejection. That upon antibody-mediated rejection tubules are the major source of IL-17 and that complement may induce IL-17 gene and protein in tubular epithelial cells. Slide 28 I think I have now just some issues showing what is finally the major source of IL-17 upon acute renal rejection, what might be the different expression of IL-17 in acute and antibodymediated rejection and we can discuss that also. Slide 29 I haven't found any available data on real time Slide 30


18 Pcr for IL-17 in renal biopsy so far. Slide 31 I had some slides about the discussion Slide 32


19 but we can just use it for the discussion eventually. Slide 33 I would like to finish by thanking all these people mentioning that this work has been done mostly by Unsal Yapici in the lab with also the support of the Dutch Kidney Foundation and I would like to thank you for your attention. Thank you. Slide 34

20 - So thank you very much Sandrine, I think a very nice overview and very exciting results. While people come to the microphone actually the main question is if you take the IL-17 family, there are 6 members and for instance, from the work of the TGF for instance, TGF-β and TGF-α, we know that only a minor change, let's say 1 aminoacid change, determines whether it's α or β and the functional activities of these two molecules are so very much different. So the question is actually whether looking at this full spectrum, I assume your antibody sees the full spectrum of all family members, is there any possibility to distinguish between the 6 family members? - Ok thank you, indeed that's really an important point that I think that there is no actual antibody discriminating between the 6 members of this family and the antibodies which are working are all polyclonal antibodies so they recognize both IL-17 A and F. So we cannot discriminate between both. You are perfectly right that it might be really important for the function of these cytokines and discriminating might give more insight into the pathogenesis of the role of IL-17 in allograft rejection. - So my co-chair Piero Ronco from Paris also has a question. Please go ahead. - Thank you Mo and thank you for a nice presentation. You showed that IL-17 was associated with late graft dysfunction but how does it work? There is this paper by Cees van Kooten showing that IL-17 affects, alters proximal tubular epithelial cells. Could you speculate a little bit, very briefly? - Yes, using antibody IL-17 expression on tubular epithelial cells in contrast to the other study. So I think that the most important thing is that IL-17 in our hands at least, is produced by mast cells and neutrophils. And as you know, mast cells are major profibrotic cells that might then induce late renal fibrosis leading to poor renal outcome. So I think it's the combination of neutrophils and mast cells producing this IL-17 leading to remodelling of the matrix through activation of metalloproteinases and so on that might lead finally to poor outcome in terms of renal fibrosis and tubular atrophy. Because response to conventional therapy in our small cohort did not show any difference so I think it might be much later leading to the scarring of your graft. - Thank you.
21 - Thank you very much Sandrine. Unfortunately, we don't have more time to go into more detail.
MOLECULAR PREDICTORS OF OUTCOME Ondrej Viklicky, Prague, Czech Republic. Chair: Daniel Abramowicz, Brussels, Belgium Rosanna Coppo, Turin, Italy
 MOLECULAR PREDICTORS OF OUTCOME Ondrej Viklicky, Prague, Czech Republic Chair: Daniel Abramowicz, Brussels, Belgium Rosanna Coppo, Turin, Italy Prof Ondrej Viklicky Department of Nephrology Transplant
MOLECULAR PREDICTORS OF OUTCOME Ondrej Viklicky, Prague, Czech Republic Chair: Daniel Abramowicz, Brussels, Belgium Rosanna Coppo, Turin, Italy Prof Ondrej Viklicky Department of Nephrology Transplant
Prof. Rosanna Coppo Director of the Nephrology, Dialysis and Transplantation Department Regina Margherita Hospital Turin, Italy. Slide 1.
 ROLE OF PATHOLOGY AND CLINICAL FEATURES IN PREDICTING PROGRESSION OF IGA NEPHROPATHY: RESULTS FROM THE ERA-EDTA RESEARCH VALIGA Rosanna Coppo, Turin, Italy Chairs: François Berthoux, Saint-Etienne, France
ROLE OF PATHOLOGY AND CLINICAL FEATURES IN PREDICTING PROGRESSION OF IGA NEPHROPATHY: RESULTS FROM THE ERA-EDTA RESEARCH VALIGA Rosanna Coppo, Turin, Italy Chairs: François Berthoux, Saint-Etienne, France
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Krediet slide di 18
 1 di 18 Assessment of fluid status in PD patients Raymond T. Krediet, Amsterdam, Netherlands Chairs:Walther H. Boer, Utrecht, The Netherlands F. Fevzi Ersoy, Antalya, Turkey Prof. Raymond T. Krediet DDivision
1 di 18 Assessment of fluid status in PD patients Raymond T. Krediet, Amsterdam, Netherlands Chairs:Walther H. Boer, Utrecht, The Netherlands F. Fevzi Ersoy, Antalya, Turkey Prof. Raymond T. Krediet DDivision
Prof. Andrzej Wiecek Department of Nephrology, Endocrinology and Metabolic Diseases Medical University of Silesia Katowice, Poland.
 What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
PREVENTION AND TREATMENT OF BKV NEPHROPATHY Petra Reinke, Berlin, Germany. Chair: Daniel Abramowicz, Brussels, Belgium Rosanna Coppo, Turin, Italy
 PREVENTION AND TREATMENT OF BKV NEPHROPATHY Petra Reinke, Berlin, Germany Chair: Daniel Abramowicz, Brussels, Belgium Rosanna Coppo, Turin, Italy Prof Petra Reinke Department of Nephrology University Hospital
PREVENTION AND TREATMENT OF BKV NEPHROPATHY Petra Reinke, Berlin, Germany Chair: Daniel Abramowicz, Brussels, Belgium Rosanna Coppo, Turin, Italy Prof Petra Reinke Department of Nephrology University Hospital
Effector T Cells and
 1 Effector T Cells and Cytokines Andrew Lichtman, MD PhD Brigham and Women's Hospital Harvard Medical School 2 Lecture outline Cytokines Subsets of CD4+ T cells: definitions, functions, development New
1 Effector T Cells and Cytokines Andrew Lichtman, MD PhD Brigham and Women's Hospital Harvard Medical School 2 Lecture outline Cytokines Subsets of CD4+ T cells: definitions, functions, development New
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference
 The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
Statement of Disclosure
 Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Prof. Michael Joannidis Medical Intensive Care and Emergency Unit Department of Internal Medicine Medical University Innsbruck Innsbruck, Austria
 1 di 27 Prevention of AKI: experimental promises and clinical realities Michael Joannidis, Innsbruck, Austria Chairs:Norbert Lameire, Ghent, Belgium Gert Mayer, Innsbruck, Austria Prof. Michael Joannidis
1 di 27 Prevention of AKI: experimental promises and clinical realities Michael Joannidis, Innsbruck, Austria Chairs:Norbert Lameire, Ghent, Belgium Gert Mayer, Innsbruck, Austria Prof. Michael Joannidis
EARLY VERSUS LATE STEROID WITHDRAWAL Julio Pascual, Barcelona, Spain Chairs: Ryszard Grenda, Warsaw, Poland
 EARLY VERSUS LATE STEROID WITHDRAWAL Julio Pascual, Barcelona, Spain Chairs: Ryszard Grenda, Warsaw, Poland Julio Pascual, Barcelona, Spain Prof. Julio Pascal Hospital del Mar Nephrology Department Barcelona,
EARLY VERSUS LATE STEROID WITHDRAWAL Julio Pascual, Barcelona, Spain Chairs: Ryszard Grenda, Warsaw, Poland Julio Pascual, Barcelona, Spain Prof. Julio Pascal Hospital del Mar Nephrology Department Barcelona,
As outlined under External contributions (see appendix 7.1), the group of Prof. Gröne at the
, the group of Prof. Gröne at the") 3 RESULTS As outlined under External contributions (see appendix 7.1), the group of Prof. Gröne at the DKFZ in Heidelberg (Dept. of Cellular and Molecular pathology) contributed to this work by performing
3 RESULTS As outlined under External contributions (see appendix 7.1), the group of Prof. Gröne at the DKFZ in Heidelberg (Dept. of Cellular and Molecular pathology) contributed to this work by performing
Prof. Armando Torres Nephrology Section Hospital Universitario de Canarias University of La Laguna Tenerife, Canary Islands, Spain.
 Does RAS blockade improve outcomes after kidney transplantation? Armando Torres, La Laguna, Spain Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain Prof. Armando Torres Nephrology
Does RAS blockade improve outcomes after kidney transplantation? Armando Torres, La Laguna, Spain Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain Prof. Armando Torres Nephrology
DRUG MINIMISATION FROM BENCH TO BEDSIDE SOME LESSONS FROM THE RISET PROGRAM Hans-Dieter Volk, Berlin, Germany
 DRUG MINIMISATION FROM BENCH TO BEDSIDE SOME LESSONS FROM THE RISET PROGRAM Hans-Dieter Volk, Berlin, Germany Chair: Josep M. Grinyo, Barcelona, Spain Marian Klinger, Wroclaw, Poland Prof Hans-Dieter Volk
DRUG MINIMISATION FROM BENCH TO BEDSIDE SOME LESSONS FROM THE RISET PROGRAM Hans-Dieter Volk, Berlin, Germany Chair: Josep M. Grinyo, Barcelona, Spain Marian Klinger, Wroclaw, Poland Prof Hans-Dieter Volk
Renal Pathology- Transplantation. Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic
 Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
THE ROLE OF URIC ACID IN THE PROGRESSION OF CKD Mehmet Kanbay, Istanbul, Turkey
 THE ROLE OF URIC ACID IN THE PROGRESSION OF CKD Mehmet Kanbay, Istanbul, Turkey Chairs: Gerjan Navis, Groningen, The Netherlands Kamil Serdengecti, Istanbul, Turkey Dr. M. Kanbay Division of Nephrology
THE ROLE OF URIC ACID IN THE PROGRESSION OF CKD Mehmet Kanbay, Istanbul, Turkey Chairs: Gerjan Navis, Groningen, The Netherlands Kamil Serdengecti, Istanbul, Turkey Dr. M. Kanbay Division of Nephrology
Th17 Pathway Research By Bio-Plex
 Th17 Pathway Research By Bio-Plex Zhiyang Shen, Senior Product Manager Bio-Rad Laboratories, Inc 2011 年 6 月 28 日星期二 T helper cell research Timeline: advances on T helper research. Figure depicts some of
Th17 Pathway Research By Bio-Plex Zhiyang Shen, Senior Product Manager Bio-Rad Laboratories, Inc 2011 年 6 月 28 日星期二 T helper cell research Timeline: advances on T helper research. Figure depicts some of
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
ANAEMIA MANAGEMENT: THE KDIGO RECOMMENDATIONS Patrick S. Parfrey, St. John s, Canada
 ANAEMIA MANAGEMENT: THE KDIGO RECOMMENDATIONS Patrick S. Parfrey, St. John s, Canada Chair: Kai- Uwe Eckardt, Erlangen, Germany Pierre- Yves Martin, Geneva, Switzerland Prof. Patrick S. Parfrey Division
ANAEMIA MANAGEMENT: THE KDIGO RECOMMENDATIONS Patrick S. Parfrey, St. John s, Canada Chair: Kai- Uwe Eckardt, Erlangen, Germany Pierre- Yves Martin, Geneva, Switzerland Prof. Patrick S. Parfrey Division
HLA and Non-HLA Antibodies in Transplantation and their Management
 HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
Prof. Michel Jadoul Cliniques universitaires St-Luc Université Catholique de Louvain Brussels, Belgium. Slide 1
 Phosphate and cardiovascular disease beyond CKD: is phosphate a new cholesterol? Michel Jadoul, Brussels, Belgium Chairs: Pablo Urena Torres, Saint-Ouen, France Carmine Zoccali, Reggio Calabria, Italy
Phosphate and cardiovascular disease beyond CKD: is phosphate a new cholesterol? Michel Jadoul, Brussels, Belgium Chairs: Pablo Urena Torres, Saint-Ouen, France Carmine Zoccali, Reggio Calabria, Italy
Section 4 Decision-making
 Decision-making : Decision-making Summary Conversations about treatments Participants were asked to describe the conversation that they had with the clinician about treatment at diagnosis. The most common
Decision-making : Decision-making Summary Conversations about treatments Participants were asked to describe the conversation that they had with the clinician about treatment at diagnosis. The most common
Clinical Trials: Non-Muscle Invasive Bladder Cancer. Tuesday, May 17th, Part II
 Clinical Trials: Non-Muscle Invasive Bladder Cancer Tuesday, May 17th, 2016 Part II Presented by Yair Lotan, MD is holder of the Helen J. and Robert S. Strauss Professorship in Urology and Chief of Urologic
Clinical Trials: Non-Muscle Invasive Bladder Cancer Tuesday, May 17th, 2016 Part II Presented by Yair Lotan, MD is holder of the Helen J. and Robert S. Strauss Professorship in Urology and Chief of Urologic
The Importance of Biomarkers in Asthma Clinical Phenotypes
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/hot-topics-in-allergy/the-importance-of-biomarkers-in-asthma-clinicalphenotypes/3889/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/hot-topics-in-allergy/the-importance-of-biomarkers-in-asthma-clinicalphenotypes/3889/
T cell-mediated immunity
 T cell-mediated immunity Overview For microbes within phagosomes in phagocytes.cd4+ T lymphocytes (TH1) Activate phagocyte by cytokines studies on Listeria monocytogenes For microbes infecting and replicating
T cell-mediated immunity Overview For microbes within phagosomes in phagocytes.cd4+ T lymphocytes (TH1) Activate phagocyte by cytokines studies on Listeria monocytogenes For microbes infecting and replicating
Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification
 Banff 1 Banff Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification Department of Nephrology, Japanese Red Cross Nagoya Daini Hospital Morozumi Kunio,
Banff 1 Banff Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification Department of Nephrology, Japanese Red Cross Nagoya Daini Hospital Morozumi Kunio,
Immunopathology of T cell mediated rejection
 Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
number Done by Corrected by Doctor Mousa Al-Abbadi
 number 11 Done by Husam Abu-Awad Corrected by Muhammad Tarabieh Doctor Mousa Al-Abbadi The possible outcomes of an acute inflammation are the following: 1- A complete resolution in which the tissue returns
number 11 Done by Husam Abu-Awad Corrected by Muhammad Tarabieh Doctor Mousa Al-Abbadi The possible outcomes of an acute inflammation are the following: 1- A complete resolution in which the tissue returns
Restrictive lung diseases
 Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Incidence of Rejection in Renal Transplant Surgery in the LVHN Population Leading to Graft Failure: 6 Year Review
 Incidence of Rejection in Renal Transplant Surgery in the LVHN Population Leading to Graft Failure: 6 Year Review Jessica Ludolph 1 Lynsey Biondi, MD 1,2 and Michael Moritz, MD 1,2 1 Department of Surgery,
Incidence of Rejection in Renal Transplant Surgery in the LVHN Population Leading to Graft Failure: 6 Year Review Jessica Ludolph 1 Lynsey Biondi, MD 1,2 and Michael Moritz, MD 1,2 1 Department of Surgery,
DNA vaccine, peripheral T-cell tolerance modulation 185
 Subject Index Airway hyperresponsiveness (AHR) animal models 41 43 asthma inhibition 45 overview 41 mast cell modulation of T-cells 62 64 respiratory tolerance 40, 41 Tregs inhibition role 44 respiratory
Subject Index Airway hyperresponsiveness (AHR) animal models 41 43 asthma inhibition 45 overview 41 mast cell modulation of T-cells 62 64 respiratory tolerance 40, 41 Tregs inhibition role 44 respiratory
Chronic injury to the microcirculation in EMB
 Chronic injury to the microcirculation in EMB Dylan V Miller MD M Patricia Revelo MD Disclosures Miller: None Revelo: None Goals & Objectives Characterize the tissue-level pathologic changes occurring
Chronic injury to the microcirculation in EMB Dylan V Miller MD M Patricia Revelo MD Disclosures Miller: None Revelo: None Goals & Objectives Characterize the tissue-level pathologic changes occurring
Fight-or-Flight: Understanding Our Body's Response to Adrenaline
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/primary-care-today/fight-or-flight-understanding-our-bodys-response-toadrenaline/10349/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/primary-care-today/fight-or-flight-understanding-our-bodys-response-toadrenaline/10349/
Immune System. Biology 105 Lecture 16 Chapter 13
 Immune System Biology 105 Lecture 16 Chapter 13 Outline: Immune System I. Functions of the immune system II. Barrier defenses III. Non-specific defenses A. Immune system cells B. Inflammatory response
Immune System Biology 105 Lecture 16 Chapter 13 Outline: Immune System I. Functions of the immune system II. Barrier defenses III. Non-specific defenses A. Immune system cells B. Inflammatory response
T-cell activation T cells migrate to secondary lymphoid tissues where they interact with antigen, antigen-presenting cells, and other lymphocytes:
 Interactions between innate immunity & adaptive immunity What happens to T cells after they leave the thymus? Naïve T cells exit the thymus and enter the bloodstream. If they remain in the bloodstream,
Interactions between innate immunity & adaptive immunity What happens to T cells after they leave the thymus? Naïve T cells exit the thymus and enter the bloodstream. If they remain in the bloodstream,
T-cell activation T cells migrate to secondary lymphoid tissues where they interact with antigen, antigen-presenting cells, and other lymphocytes:
 Interactions between innate immunity & adaptive immunity What happens to T cells after they leave the thymus? Naïve T cells exit the thymus and enter the bloodstream. If they remain in the bloodstream,
Interactions between innate immunity & adaptive immunity What happens to T cells after they leave the thymus? Naïve T cells exit the thymus and enter the bloodstream. If they remain in the bloodstream,
CAN WE PREDICT THE RISK FOR ADVERSE EVENTS? Andrzej Wiecek, Katowice, Poland
 CAN WE PREDICT THE RISK FOR ADVERSE EVENTS? Andrzej Wiecek, Katowice, Poland Chair: Kai- Uwe Eckardt, Erlangen, Germany Pierre- Yves Martin, Geneva, Switzerland Prof. Andrzej Więcek Departm ent of Nephrology,
CAN WE PREDICT THE RISK FOR ADVERSE EVENTS? Andrzej Wiecek, Katowice, Poland Chair: Kai- Uwe Eckardt, Erlangen, Germany Pierre- Yves Martin, Geneva, Switzerland Prof. Andrzej Więcek Departm ent of Nephrology,
Why Are So Many Clinicians Choosing to Practice Functional Medicine?
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/integrative-and-functional-medicine-in-practice/why-are-so-manyclinicians-choosing-practice-functional-medicine/8424/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/integrative-and-functional-medicine-in-practice/why-are-so-manyclinicians-choosing-practice-functional-medicine/8424/
Disease Modifying Therapies in MS: Highlights from ACTRIMS 2018
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Autoimmune disorders: An emerging risk factor for CV disease
 Autoimmune disorders: An emerging risk factor for CV disease DR. SHARON MULVAGH: Greetings. I'm Dr Sharon Mulvagh, professor of medicine and director of Mayo Clinic Women's Heart Clinic. During today's
Autoimmune disorders: An emerging risk factor for CV disease DR. SHARON MULVAGH: Greetings. I'm Dr Sharon Mulvagh, professor of medicine and director of Mayo Clinic Women's Heart Clinic. During today's
that number is extremely high. It s 16 episodes, or in other words, it s 14, one-four, ICD shocks per patient per day.
 Doctor Karlsner, Doctor Schumosky, ladies and gentlemen. It s my real pleasure to participate in this session on controversial issues in the management of ventricular tachycardia and I m sure that will
Doctor Karlsner, Doctor Schumosky, ladies and gentlemen. It s my real pleasure to participate in this session on controversial issues in the management of ventricular tachycardia and I m sure that will
Diagnosis and Management of Acute and Chronic Humoral Rejection. Lars Pape
 Diagnosis and Management of Acute and Chronic Humoral Rejection Lars Pape Immunosuppression Acute rejection Chronic rejection Side effects Infections Nephrotoxicity Adult population Nearly all late rejection-related
Diagnosis and Management of Acute and Chronic Humoral Rejection Lars Pape Immunosuppression Acute rejection Chronic rejection Side effects Infections Nephrotoxicity Adult population Nearly all late rejection-related
Lymphoid System: cells of the immune system. Answer Sheet
 Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
renoprotection therapy goals 208, 209
 Subject Index Aldosterone, plasminogen activator inhibitor-1 induction 163, 164, 168 Aminopeptidases angiotensin II processing 64 66, 214 diabetic expression 214, 215 Angiotensin I intrarenal compartmentalization
Subject Index Aldosterone, plasminogen activator inhibitor-1 induction 163, 164, 168 Aminopeptidases angiotensin II processing 64 66, 214 diabetic expression 214, 215 Angiotensin I intrarenal compartmentalization
Attribution: University of Michigan Medical School, Department of Microbiology and Immunology
 Attribution: University of Michigan Medical School, Department of Microbiology and Immunology License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Attribution: University of Michigan Medical School, Department of Microbiology and Immunology License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Immune response. This overview figure summarizes simply how our body responds to foreign molecules that enter to it.
 Immune response This overview figure summarizes simply how our body responds to foreign molecules that enter to it. It s highly recommended to watch Dr Najeeb s lecture that s titled T Helper cells and
Immune response This overview figure summarizes simply how our body responds to foreign molecules that enter to it. It s highly recommended to watch Dr Najeeb s lecture that s titled T Helper cells and
Immunotherapy Narrative Script:
 Immunotherapy Narrative Script: In order to understand immunotherapy, there are a few things we need to get straight in our heads first. The first thing we need to get a general understanding of is what
Immunotherapy Narrative Script: In order to understand immunotherapy, there are a few things we need to get straight in our heads first. The first thing we need to get a general understanding of is what
Kidney Summary. Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA
 Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
No evidence of C4d association with AMR However, C3d and AMR correlated well
 C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
Neonatal Diabetes: A Special Case of Type 1 Diabetes
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/neonatal-diabetes-a-special-case-of-type-1-
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/neonatal-diabetes-a-special-case-of-type-1-
Non Muscle Invasive Bladder Cancer (NMIBC) Experts Discuss Treatment Options. Part II: The Future Treatment of NMIBC
 Experts Discuss Treatment Options. Part II: The Future Treatment of NMIBC") Non Muscle Invasive Bladder Cancer (NMIBC) Experts Discuss Treatment Options Wednesday, June 14, 2017 Part II: The Future Treatment of NMIBC Presented by Dr. Arlene Siefer-Radtke is an Associate Professor
Non Muscle Invasive Bladder Cancer (NMIBC) Experts Discuss Treatment Options Wednesday, June 14, 2017 Part II: The Future Treatment of NMIBC Presented by Dr. Arlene Siefer-Radtke is an Associate Professor
Immune System. Biol 105 Chapter 13
 Immune System Biol 105 Chapter 13 Outline Immune System I. Function of the Immune system II. Barrier Defenses III. Nonspecific Defenses A. Immune system cells B. Inflammatory response C. Complementary
Immune System Biol 105 Chapter 13 Outline Immune System I. Function of the Immune system II. Barrier Defenses III. Nonspecific Defenses A. Immune system cells B. Inflammatory response C. Complementary
Supplementary Table 1 Clinicopathological characteristics of 35 patients with CRCs
 Supplementary Table Clinicopathological characteristics of 35 patients with CRCs Characteristics Type-A CRC Type-B CRC P value Sex Male / Female 9 / / 8.5 Age (years) Median (range) 6. (9 86) 6.5 (9 76).95
Supplementary Table Clinicopathological characteristics of 35 patients with CRCs Characteristics Type-A CRC Type-B CRC P value Sex Male / Female 9 / / 8.5 Age (years) Median (range) 6. (9 86) 6.5 (9 76).95
Fluid movement in capillaries. Not all fluid is reclaimed at the venous end of the capillaries; that is the job of the lymphatic system
 Capillary exchange Fluid movement in capillaries Not all fluid is reclaimed at the venous end of the capillaries; that is the job of the lymphatic system Lymphatic vessels Lymphatic capillaries permeate
Capillary exchange Fluid movement in capillaries Not all fluid is reclaimed at the venous end of the capillaries; that is the job of the lymphatic system Lymphatic vessels Lymphatic capillaries permeate
Cytokines modulate the functional activities of individual cells and tissues both under normal and pathologic conditions Interleukins,
 Cytokines http://highered.mcgraw-hill.com/sites/0072507470/student_view0/chapter22/animation the_immune_response.html Cytokines modulate the functional activities of individual cells and tissues both under
Cytokines http://highered.mcgraw-hill.com/sites/0072507470/student_view0/chapter22/animation the_immune_response.html Cytokines modulate the functional activities of individual cells and tissues both under
The transcriptome of the renal transplant biopsy: the lessons. Philip F Halloran
 The transcriptome of the renal transplant biopsy: the lessons Philip F Halloran Alberta Transplant Applied Genomics Centre April 27 th 2009 Congratulations on your 50 th anniversary ATAGC Learning objectives:
The transcriptome of the renal transplant biopsy: the lessons Philip F Halloran Alberta Transplant Applied Genomics Centre April 27 th 2009 Congratulations on your 50 th anniversary ATAGC Learning objectives:
Immune System. Biol 105 Lecture 16 Chapter 13
 Immune System Biol 105 Lecture 16 Chapter 13 Outline Immune System I. Function of the Immune system II. Barrier Defenses III. Nonspecific Defenses A. Immune system cells B. Inflammatory response C. Complementary
Immune System Biol 105 Lecture 16 Chapter 13 Outline Immune System I. Function of the Immune system II. Barrier Defenses III. Nonspecific Defenses A. Immune system cells B. Inflammatory response C. Complementary
Tumor Immunology: A Primer
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Physiology (6) 2/4/2018. Rahmeh Alsukkar
 2/4/2018. Rahmeh Alsukkar") Physiology (6) 2/4/2018 Rahmeh Alsukkar **unfortunately the sheet does not involve the slides. ** the doctor repeat a lot of things from the previous lecture so this sheet will begin from slide 139 to
Physiology (6) 2/4/2018 Rahmeh Alsukkar **unfortunately the sheet does not involve the slides. ** the doctor repeat a lot of things from the previous lecture so this sheet will begin from slide 139 to
Effector mechanisms of cell-mediated immunity: Properties of effector, memory and regulatory T cells
 ICI Basic Immunology course Effector mechanisms of cell-mediated immunity: Properties of effector, memory and regulatory T cells Abul K. Abbas, MD UCSF Stages in the development of T cell responses: induction
ICI Basic Immunology course Effector mechanisms of cell-mediated immunity: Properties of effector, memory and regulatory T cells Abul K. Abbas, MD UCSF Stages in the development of T cell responses: induction
Title: NATURAL KILLER CELL FUNCTIONS AND SURFACE RECEPTORS
 LECTURE: 14 Title: NATURAL KILLER CELL FUNCTIONS AND SURFACE RECEPTORS LEARNING OBJECTIVES: The student should be able to: Describe the general morphology of the NK-cells. Enumerate the different functions
LECTURE: 14 Title: NATURAL KILLER CELL FUNCTIONS AND SURFACE RECEPTORS LEARNING OBJECTIVES: The student should be able to: Describe the general morphology of the NK-cells. Enumerate the different functions
THE BIOLOGY OF PLATELET-GEL THERAPY
 THE BIOLOGY OF PLATELET-GEL THERAPY The synopsis of normal healing includes a well known sequence of coordinated phases. The unique process leading to healing is ontologically partitioned in three sequential
THE BIOLOGY OF PLATELET-GEL THERAPY The synopsis of normal healing includes a well known sequence of coordinated phases. The unique process leading to healing is ontologically partitioned in three sequential
Type 1 Diabetes: Control and Cure
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/type-1-diabetes-control-and-cure/1771/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/type-1-diabetes-control-and-cure/1771/
Immunology for the Rheumatologist
 Immunology for the Rheumatologist Rheumatologists frequently deal with the immune system gone awry, rarely studying normal immunology. This program is an overview and discussion of the function of the
Immunology for the Rheumatologist Rheumatologists frequently deal with the immune system gone awry, rarely studying normal immunology. This program is an overview and discussion of the function of the
Pharmaceutical pathology
 Pharmaceutical pathology Livia Vida 2018 1. Necrosis, types, examples. Apoptosis. 2. Adaptations I. Degeneration, atrophy. 3. Adaptations II. Hypertrophy, hyperplasia. 4. Pigments. Calcification. 5. Inflammation
Pharmaceutical pathology Livia Vida 2018 1. Necrosis, types, examples. Apoptosis. 2. Adaptations I. Degeneration, atrophy. 3. Adaptations II. Hypertrophy, hyperplasia. 4. Pigments. Calcification. 5. Inflammation
Immunology lecture: 14. Cytokines: Main source: Fibroblast, but actually it can be produced by other types of cells
 Immunology lecture: 14 Cytokines: 1)Interferons"IFN" : 2 types Type 1 : IFN-Alpha : Main source: Macrophages IFN-Beta: Main source: Fibroblast, but actually it can be produced by other types of cells **There
Immunology lecture: 14 Cytokines: 1)Interferons"IFN" : 2 types Type 1 : IFN-Alpha : Main source: Macrophages IFN-Beta: Main source: Fibroblast, but actually it can be produced by other types of cells **There
Immunomodulator y effects of CMV disease
 Immunomodulator y effects of CMV disease Oriol Manuel MD Service of Infectious Diseases and Transplantation Center University Hospital of Lausanne Switzerland Outline The transplant troll The indirect
Immunomodulator y effects of CMV disease Oriol Manuel MD Service of Infectious Diseases and Transplantation Center University Hospital of Lausanne Switzerland Outline The transplant troll The indirect
The Lymphatic System and Body Defenses
 PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Lymphatic System and Body Defenses 12PART B Adaptive Defense System: Third Line of Defense Immune
PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Lymphatic System and Body Defenses 12PART B Adaptive Defense System: Third Line of Defense Immune
JAK-STAT Signaling and Disease Pathogenesis in RA and IBD
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Microbiology 204: Cellular and Molecular Immunology
 Microbiology 204: Cellular and Molecular Immunology Class meets MWF 1:00-2:30PM (*exceptions: no class Fri Sept 23, Fri Oct 14, Nov 11, or Wed Nov 23) Lectures are open to auditors and will be live-streamed
Microbiology 204: Cellular and Molecular Immunology Class meets MWF 1:00-2:30PM (*exceptions: no class Fri Sept 23, Fri Oct 14, Nov 11, or Wed Nov 23) Lectures are open to auditors and will be live-streamed
Antibody Mediated Rejection (AMR) in LUNG TRANSPLANT Recipients
 in LUNG TRANSPLANT Recipients") Antibody Mediated Rejection (AMR) in LUNG TRANSPLANT Recipients Lorriana Leard, MD UCSF Transplant Pulmonologist Associate Professor of Clinical Medicine Vice Chief of Clinical Activities Pulmonary, Critical
Antibody Mediated Rejection (AMR) in LUNG TRANSPLANT Recipients Lorriana Leard, MD UCSF Transplant Pulmonologist Associate Professor of Clinical Medicine Vice Chief of Clinical Activities Pulmonary, Critical
vi Preface Table 2 Association of Fibrosis With Types of Injury: Representative Examples
 Fibrosis or scar, defined pathologically as inappropriate repair by connective tissue, is increasingly recognized as an important feature of many chronic diseases (Table 1), and as such, represents an
Fibrosis or scar, defined pathologically as inappropriate repair by connective tissue, is increasingly recognized as an important feature of many chronic diseases (Table 1), and as such, represents an
ACTIVATION AND EFFECTOR FUNCTIONS OF CELL-MEDIATED IMMUNITY AND NK CELLS. Choompone Sakonwasun, MD (Hons), FRCPT
, FRCPT") ACTIVATION AND EFFECTOR FUNCTIONS OF CELL-MEDIATED IMMUNITY AND NK CELLS Choompone Sakonwasun, MD (Hons), FRCPT Types of Adaptive Immunity Types of T Cell-mediated Immune Reactions CTLs = cytotoxic T lymphocytes
ACTIVATION AND EFFECTOR FUNCTIONS OF CELL-MEDIATED IMMUNITY AND NK CELLS Choompone Sakonwasun, MD (Hons), FRCPT Types of Adaptive Immunity Types of T Cell-mediated Immune Reactions CTLs = cytotoxic T lymphocytes
BBC LEARNING ENGLISH 6 Minute English Cigarettes v e-cigarettes
 BBC LEARNING ENGLISH 6 Minute English Cigarettes v e-cigarettes NB: This is not a word-for-word transcript Hello I'm. Welcome to 6 Minute English. I'm joined today by. Hello. Today we are going to talk
BBC LEARNING ENGLISH 6 Minute English Cigarettes v e-cigarettes NB: This is not a word-for-word transcript Hello I'm. Welcome to 6 Minute English. I'm joined today by. Hello. Today we are going to talk
Jones slide di 23
 1 di 23 The patient with ANCA- associated vasculitis and pulmonary haemorrhage Rachel B Jones, Cambridge, UK Chairs:Hans-Joachim Anders, Munich, Germany Vladimir Tesar, Prague, Czech Republic Prof. Rachel
1 di 23 The patient with ANCA- associated vasculitis and pulmonary haemorrhage Rachel B Jones, Cambridge, UK Chairs:Hans-Joachim Anders, Munich, Germany Vladimir Tesar, Prague, Czech Republic Prof. Rachel
Asthma. - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness.
 Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Progressive histological damage in renal allografts is associated with expression of innate and adaptive immunity genes
 http://www.kidney-international.org & 2011 International Society of Nephrology see commentary on page 1254 Progressive histological damage in renal allografts is associated with expression of innate and
http://www.kidney-international.org & 2011 International Society of Nephrology see commentary on page 1254 Progressive histological damage in renal allografts is associated with expression of innate and
IL-24 AND ITS ROLE IN WOUND HEALING
 IL-24 AND ITS ROLE IN WOUND HEALING Nancy J. Poindexter, Ryan Williams, Garth Powis, Sunil Chada, and Elizabeth A. Grimm & Introgen Therapeutics, Inc., Houston, TX IL-24/MDA 24/MDA-77 is a Tumor Suppressor
IL-24 AND ITS ROLE IN WOUND HEALING Nancy J. Poindexter, Ryan Williams, Garth Powis, Sunil Chada, and Elizabeth A. Grimm & Introgen Therapeutics, Inc., Houston, TX IL-24/MDA 24/MDA-77 is a Tumor Suppressor
Tissue repair. (3&4 of 4)
") Tissue repair (3&4 of 4) What will we discuss today: Regeneration in tissue repair Scar formation Cutaneous wound healing Pathologic aspects of repair Regeneration in tissue repair Labile tissues rapid
Tissue repair (3&4 of 4) What will we discuss today: Regeneration in tissue repair Scar formation Cutaneous wound healing Pathologic aspects of repair Regeneration in tissue repair Labile tissues rapid
Biopsy Features of Kidney Allograft Rejection Banff B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Page # Lecture 8: Immune Dysfunction - Immunopathology. Four Types of Hypersensitivity. Friend of Foe? Autoimmune disease Immunodeficiency
 Lecture 8: Immune Dysfunction - Immunopathology Autoimmune disease Immunodeficiency Allergy and Asthma Graft rejection and Lupus Friend of Foe? Four Types of Hypersensitivity Allergic Responses - Type
Lecture 8: Immune Dysfunction - Immunopathology Autoimmune disease Immunodeficiency Allergy and Asthma Graft rejection and Lupus Friend of Foe? Four Types of Hypersensitivity Allergic Responses - Type
Immune Responses KEY CONCEPT The immune system has many responses to pathogens and foreign cells.
 SECTION 31.3 Immune Responses KEY CONCEPT The immune system has many responses to pathogens and foreign cells. Student text pages 950 954 SC.912.L.14.52 Many body systems work to produce nonspecific responses.
SECTION 31.3 Immune Responses KEY CONCEPT The immune system has many responses to pathogens and foreign cells. Student text pages 950 954 SC.912.L.14.52 Many body systems work to produce nonspecific responses.
IL-17 in health and disease. March 2014 PSO13-C051n
 IL-17 in health and disease March 2014 PSO13-C051n Originally Researchers Suggested That IL-12 and IL-4 drove Th Cell Differentiation Naïve CD4 + T cell Question: Which of these cell types is responsible
IL-17 in health and disease March 2014 PSO13-C051n Originally Researchers Suggested That IL-12 and IL-4 drove Th Cell Differentiation Naïve CD4 + T cell Question: Which of these cell types is responsible
White Blood Cells (WBCs)
") YOUR ACTIVE IMMUNE DEFENSES 1 ADAPTIVE IMMUNE RESPONSE 2! Innate Immunity - invariant (generalized) - early, limited specificity - the first line of defense 1. Barriers - skin, tears 2. Phagocytes - neutrophils,
YOUR ACTIVE IMMUNE DEFENSES 1 ADAPTIVE IMMUNE RESPONSE 2! Innate Immunity - invariant (generalized) - early, limited specificity - the first line of defense 1. Barriers - skin, tears 2. Phagocytes - neutrophils,
Kun Jiang 1, He-Bin Chen 1, Ying Wang 1, Jia-Hui Lin 2, Yan Hu 1, Yu-Rong Fang 1
 Original Article Changes in interleukin-17 and transforming growth factor beta 1 levels in serum and bronchoalveolar lavage fluid and their clinical significance among children with asthma Kun Jiang 1,
Original Article Changes in interleukin-17 and transforming growth factor beta 1 levels in serum and bronchoalveolar lavage fluid and their clinical significance among children with asthma Kun Jiang 1,
Hypersensitivity is the term used when an immune response results in exaggerated or inappropriate reactions harmful to the host.
 Hypersensitivity is the term used when an immune response results in exaggerated or inappropriate reactions harmful to the host. Hypersensitivity vs. allergy Hypersensitivity reactions require a pre-sensitized
Hypersensitivity is the term used when an immune response results in exaggerated or inappropriate reactions harmful to the host. Hypersensitivity vs. allergy Hypersensitivity reactions require a pre-sensitized
Introduction. Acute sodium overload produces renal tubulointerstitial inflammation in normal rats
 Acute sodium overload produces renal tubulointerstitial inflammation in normal rats MI Roson, et al. Kidney International (2006) Introduction Present by Kanya Bunnan and Wiraporn paebua Tubular sodium
Acute sodium overload produces renal tubulointerstitial inflammation in normal rats MI Roson, et al. Kidney International (2006) Introduction Present by Kanya Bunnan and Wiraporn paebua Tubular sodium
ACTIVATION OF T LYMPHOCYTES AND CELL MEDIATED IMMUNITY
 ACTIVATION OF T LYMPHOCYTES AND CELL MEDIATED IMMUNITY The recognition of specific antigen by naïve T cell induces its own activation and effector phases. T helper cells recognize peptide antigens through
ACTIVATION OF T LYMPHOCYTES AND CELL MEDIATED IMMUNITY The recognition of specific antigen by naïve T cell induces its own activation and effector phases. T helper cells recognize peptide antigens through
The Diagnosis and Management of Anaphylaxis
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-allergy/the-diagnosis-and-management-of-anaphylaxis/3919/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-allergy/the-diagnosis-and-management-of-anaphylaxis/3919/
Role of Th17 cells in the immunopathogenesis of dry eye disease
 Role of Th17 cells in the immunopathogenesis of dry eye disease The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Chauhan,
Role of Th17 cells in the immunopathogenesis of dry eye disease The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Chauhan,
Promising Bifunctional Agents in Immuno- Oncology: A Roundtable Discussion with the Experts
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Cell-mediated Immunity
 Cellular & Molecular Immunology Cell-mediated Immunity Nicholas M. Ponzio, Ph.D. Department of Pathology & Laboratory Medicine April 6, 2009 Today s Presentation: Overview Cellular Interactions In Humoral
Cellular & Molecular Immunology Cell-mediated Immunity Nicholas M. Ponzio, Ph.D. Department of Pathology & Laboratory Medicine April 6, 2009 Today s Presentation: Overview Cellular Interactions In Humoral
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies
 Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Histological and immunological characteristics of colitis associated with anti-ctla 4 antibody therapy
 Histological and immunological characteristics of colitis associated with anti-ctla 4 antibody therapy M. Perdiki 2, G. Bamias 1, D. Pouloudi 2, H. Gogas 3, I. Delladetsima 2 1 Academic Dpt. of Gastroenterology,
Histological and immunological characteristics of colitis associated with anti-ctla 4 antibody therapy M. Perdiki 2, G. Bamias 1, D. Pouloudi 2, H. Gogas 3, I. Delladetsima 2 1 Academic Dpt. of Gastroenterology,
Immuno-Oncology: Perspectives on Current Therapies & Future Developments
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/medical-industry-feature/immuno-oncology-perspectives-currenttherapies-future-developments/9502/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/medical-industry-feature/immuno-oncology-perspectives-currenttherapies-future-developments/9502/
Immunity. Acquired immunity differs from innate immunity in specificity & memory from 1 st exposure
 Immunity (1) Non specific (innate) immunity (2) Specific (acquired) immunity Characters: (1) Non specific: does not need special recognition of the foreign cell. (2) Innate: does not need previous exposure.
Immunity (1) Non specific (innate) immunity (2) Specific (acquired) immunity Characters: (1) Non specific: does not need special recognition of the foreign cell. (2) Innate: does not need previous exposure.
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Immunology: an overview Lecture
 Slide #2: Immunology is sometimes regarded as part of microbiology department because it started there as an investigation of ways used to prevent against infectious agents (e.g. microorganisms ). However
Slide #2: Immunology is sometimes regarded as part of microbiology department because it started there as an investigation of ways used to prevent against infectious agents (e.g. microorganisms ). However
Andrea s Final Exam Review PCB 3233 Spring Practice Final Exam
 NOTE: Practice Final Exam Although I am posting the answer key for this practice exam, I want you to use this practice to gauge your knowledge, and try to figure out the right answer by yourself before
NOTE: Practice Final Exam Although I am posting the answer key for this practice exam, I want you to use this practice to gauge your knowledge, and try to figure out the right answer by yourself before