Emerging Issues in HIV and Pregnancy. Lynne M. Mofenson, MD. HIV Senior Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation
|
|
|
- Evan Mason
- 5 years ago
- Views:
Transcription



1 Emerging Issues in HIV and Pregnancy Lynne M. Mofenson, MD HIV Senior Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation
2 Perinatal Transmission in the ART Era What s New? Antepartum ARV drug choice Timing of ART initiation in pregnancy Use of intrapartum intravenous zidovudine Acute HIV in pregnancy Pregnancy in perinatally-infected women Controversies on breastfeeding in the United States



3 ART in Pregnancy and Perinatal Transmission Life-long ART is recommended for all individuals with HIV infection regardless of CD4 cell count, including pregnant women. 3 components to perinatal prevention: Lowering maternal viral load with ART: However ARV drugs reduce transmission even with low viral load and even when antenatal drugs not given Pre-exposure prophylaxis of infant (through transplacental drug passage mother to infant) Post-exposure prophylaxis of infant (through continued ARV after birth)

4 Importance of the Infant Pre- and Post-Exposure Prophylaxis Component of PACTG 076 Regimen Wade N et al. N Engl J Med 1999;339:1409 Data on 939 HIV-exposed infants born in New York State AP+IP+PP IP+PP PP<24 hr PP>48 hr No AZT Even When No Maternal AP AZT Given, Infant AZT Started Within 24 Hours Reduces Transmission
5 ARV Drug Choice in Pregnancy In general, ART guidelines during pregnancy are similar to non-pregnant with some modifications, primarily based on limited experience (PK/dosing and fetal safety) with new drugs during pregnancy. Goal of ART in pregnancy is full viral suppression, as in non-pregnant individuals. Risk/benefit for drug choice differs for ART-naive women first starting drugs during pregnancy compared to ART-experienced women who may require drugs with less data for their own health due to resistance, or other factors. Thus, considerations for ARV drug choices differ for naïve vs experienced women.
6 ARV Drug Choice in Pregnancy Pharmacokinetics (PK) of NRTI and NNRTI similar in pregnant and non-pregnant women. PI PK are more variable, particularly in late pregnancy. With standard dosing, ATV/r, DRV/r, and LPV/r levels reduced in 2 nd -3 rd trimester. Need for dose adjustment depends on specific PI, ART experience, concomitant meds, side effects. Careful viral load monitoring recommended. Once daily DRV/r or LPV/r not recommended in pregnancy. Limited data suggest RAL levels in 3 rd trimester very variable, but dose modification not needed. No data on newer drugs (ETV, DTG, EVG, COBI) yet.
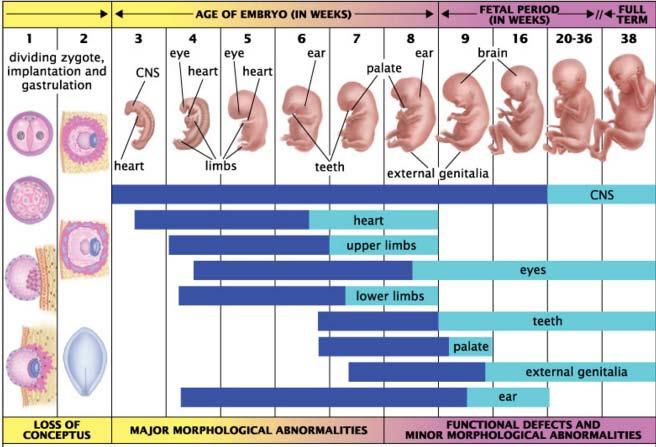
7 ARV Drug Choice in Pregnancy Most older ARV drugs appear safe in pregnancy and for fetus, but dearth of data on newer drugs which form preferred regimens in non-pregnant persons. Antiretroviral Pregnancy Registry has not indicated increase birth defects for current NRTIs, PIs and most NNRTIs, but data insufficient for newer drugs such as etravirine, entry/integrase inhibitors. There has been controversy regarding use of EFV and TDF in pregnancy.
8 Efavirenz Initial concern from non-human primate studies and retrospective human case reports regarding potential rare CNS birth defects (neural tube defects) with 1 st trimester EFV exposure Led to black box warning about use of EFV in 1 st trimester of pregnancy. Recent meta-analysis of 2,026 live-births with first trimester exposure to EFV found no evidence of increased risk overall birth defects or CNS defects; incidence neural tube defects was 0.05%, similar to general population.
9 Safety of Efavirnez in the First Trimester of Pregnancy Ford N et al. AIDS 2014 (Suppl 2): S Relative risk of birth defects with EFV vs non-efv regimens in 1 st trimester
.")
10 Efavirenz Data sufficient to rule-out >3-fold risk of rare neural tube defects (NTD) with 1 st trimester exposure (e.g., can rule out NTD incidence of >0.2% with 1 st trimester exposure). Neural tube defect risk restricted to the first 5-6 weeks of pregnancy (before most pregnancies are recognized). Change in ARVs during pregnancy may be associated with lack of viral suppression and increased risk of perinatal transmission (Floridia et al. HIV Clin Trials 2010;11:303-11). EFV now a preferred NNRTI in pregnancy; guidelines recommend that if initiating EFV in ARV-naïve women to start after 8 weeks gestation. Women on EFV-ART presenting for care in 1 st trimester should have it continued, provided there is viral suppression.


11 Tenofovir Disoproxil Fumerate (TDF) Studies of high dose TDF (2-fold higher than human dosing) in non-human primates showed maternal toxicity with decreased fetal growth and reduction fetal bone porosity. Human studies demonstrate no effect on intrauterine growth but conflicting data on growth at 6-12 months. One study suggested decreased neonatal bone mineral density with 1 st trimester TDF exposure, but duration and clinical significance of finding requires further evaluation. Given potency of TDF, activity against HBV, less toxicity than AZT, and ability for once daily dosing, benefits of TDF outweigh risk for use in ART-naïve women, and is a preferred NtRTI in guidelines.
12 PROMISE 1084s: Impact of Maternal TDF on Infant Bone Mineral Content (BMC) Siberry GK et al. CROI 2016 Boston Abs 36 PROMISE: African PMTCT trial comparing AZT/sdNVP+tail to TDF/FTC/LPV/r vs AZT/3TC/LPV/r in women with CD4 >350. Neonatal DXA substudy in infants from all arms. No significant difference in newborn mean LS BMC between study arms p = 0.82 p = 0.05 p = 0.09 Mean WB-BMC lower in triple than AZT arm but not between AZT triple vs TDF triple P<0.001 P<0.001 p = 0.41 Lumbar Spine Bone Mineral Density DXA Whole Body Bone Mineral Density DXA
13 August 2015 Antenatal ARV Regimens Recommended for ARV-Naïve HIV-Infected Pregnant Women Combination regimen Dual NRTI plus PI or NNRTI or Integrase inhibitor ARVs in Pregnancy Recommendation NRTI/NtRTI* PI NNRTI Entry/Integrase Inhibitors Preferred TDF/3TC or FTC ABC/3TC AZT/3TC ATV/r, DRV/r EFV after 8 weeks gestation RAL Alternative LPV/r RPV Insufficient Data TAF F-APV Not Recommended ddi, d4t IDV, NFV, SQV *Recommend at least 1 NRTI with good placental transfer NVP, ETV, TPV DTG, EVG/ COBI, MVC T20

14 Timing of ART Initiation in Pregnancy

15 Transmission Rates by HIV RNA Levels in HAART Era 4,738 HIV+ Pregnant Women on ART In UK/Ireland Townsend CL et al. AIDS 2014;28:
16 For Maximal Efficacy: Early ART Initiation Needed 4,327 HIV+ Women Starting ART in Pregnancy, UK/Ireland Townsend CL et al. AIDS 2014;28: Duration Antenatal ART, Baseline RNA at ART Start, and MTCT Baseline HIV RNA % MTCT Duration of antenatal ART MTCT declined rapidly initially as duration of ART increased but varied by baseline viral load at time ART started
 vs Control: non-transmitter (N=60) matched on maternity unit and birth")
17 Early Sustained Viral Control Needed for Lowest MTCT: Risk Factors for MTCT in Women With Delivery RNA <500 Tubiana R et al. CID 2010;50: ANRS Perinatal Cohort case/control study - mothers all with delivery RNA <500: Case: transmitted HIV (N=19) vs Control: non-transmitter (N=60) matched on maternity unit and birth date. Earlier viral suppression (RNA <500 at wks) only significant factor in multivariate analysis (P<0.001). CASES (transmitted) CONTROLS (no transmission) HIV RNA level (log 10 copies/ml) 16% on ART before conception 47%% on ART before conception
18 Enhanced Efficacy with Early ART, Especially Preconception, with Viral Suppression Mandelbrot L et al. Clin Infect Dis 2015;61: French Perinatal Cohort: Overall MTCT 0.7% and was 0% (95% CI 0-0.1%) in 2,651 women starting ART before conception and RNA <50 at delivery. Delivery RNA and MTCT According to Time ART Initiation Started pre-conception Started 1 st trimester Started 2 nd trimester Started 3 rd trimester MTCT 0.2% MTCT 0.4% MTCT 0.9% MTCT 2.2% *threshold if assay LLD >50 c/ml
19 Pre-Conception ART and Prematurity Nachega J et al Meta-Analysis for WHO 2015 Guidelines Systematic review and meta-analysis pregnancy outcome in women initiating ART pre-conception vs during pregnancy: 12 papers ( ). Still significant (RR 1.29 [ ]) after adjusting for confounders including age, parity, race, smoking, CD4 count, type ART

20 Timing of ART Initiation Early and sustained control of viral replication is critical for maximal reduction transmission. HIV+ women considering pregnancy should ideally be on fully suppressive ART prior to pregnancy. For pregnant women not already on ART, data favor initiating ART sufficiently early including 1 st trimester to suppress replication by 3 rd trimester. Initiation in 1 st trimester particularly important in women with high baseline viral load. There are some potential risks with very early/preconception ART in terms of possible preterm delivery, but in high resource setting like US, benefits in lower transmission likely outweigh risk.
21 Intrapartum AZT


22 Intrapartum (IP) ART Management The availability of safe and suppressive ART regimens for pregnant women have changed IP management. PACTG 076 evaluated a 3-part preventive regimen targeting different times of transmission: Antepartum AZT: target in utero transmission Intrapartum intravenous AZT: target IP transmission Infant AZT: post-exposure prophylaxis IP exposure AZT given intravenously IP because achieves rapid and sustained AZT drug levels in infant. Combination ART now recommended for all HIV+ pregnant women, continued during labor and delivery. Is there an additional benefit of IV AZT with ART?

23 Changing Risk Factors for Perinatal Transmission in ART Era Cotter AM et al. Am J Ob Gyn 2012:207:482.e HIV+ women on ART delivering U. Miami When control for viral load and ART, traditional risk factors drop out. No longer associated with risk of transmission in women on ART: Not receiving intrapartum AZT Duration membrane rupture Premature delivery Low birth weight


24 Is Intrapartum AZT Still Required in the Combination ARV Era? Briand N et al. Clin Infect Dis 2013;57: ,538 HIV+ women who delivered between ; 10,984 received IV AZT; 554 did not receive IV AZT p=0.01 p=0.06 p=0.17 p=0.61 IV AZT did not affect efficacy if HIV RNA <1000 c/ml



25 August 2015 Intrapartum Recommendations for HIV-Infected Pregnant Women Continue combination AP ARV regimen during labor and delivery. If on ART and HIV RNA <1,000 c/ml consistently in late pregnancy/near delivery and no adherence concerns, addition of IV AZT is not required. If HIV RNA >1,000 c/ml near delivery or unknown, IV AZT recommended in addition to ART regimen along with elective cesarean delivery.


26 Acute HIV in Pregnancy
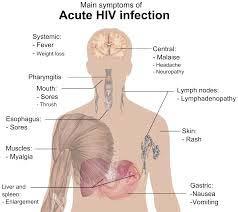
27 Acute Infection in Pregnancy and Breastfeeding Conflicting data on whether pregnancy increases HIV acquisition studies in Africa, rates are high (possibly due to endemic state of HIV in these countries). Acute infection represents a significant proportion of residual perinatal transmission in the United States. High rates of perinatal transmission with acute infection, likely related to the combination of: high viral load associated with acute infection, and diagnosis is easy to miss, resulting in lost opportunities for prevention. Repeat HIV testing in 3 rd trimester should be considered for all pregnant women, and recommended for high risk (including facilities with prevalence >0.1%).
 Postpartum 4.7 (3.3, 6.1) Pregnancy and Postpartum 2.9 (1.8, 4.")
28 Incidence of HIV during Pregnancy/Postpartum: Meta-analysis 19 Studies (All in Africa) Drake AL et al. PLosMed 2014;11:e Pregnancy Incidence per 100 person-years (95% CI) Postpartum 4.7 (3.3, 6.1) Pregnancy and Postpartum 2.9 (1.8, 4.0) Overall 2.5 (1.8, 3.2) 3.8 (2.0, 4.6)
29 Perinatal Transmission in Mothers with Incident vs Chronic HIV during Pregnancy/Postpartum: Meta-analysis Drake AL et al. PLosMed 2014;11:e studies compared risk perinatal transmission among women with incident versus chronic HIV infection 9-15-fold in US women with acute infection as ART lowers transmission with chronic infection 2.8 (0.9,4.7)
30 Acute HIV in Pregnancy United States Singh S et al. CROI 2013 Atlanta, GA. Data from15 areas conducting Enhanced Perinatal Surveillance between were examined. Included 10,308 HIV+ pregnant women who delivered live infants during that period: 1.2% (124) were identified as seroconverting during pregnancy. Perinatal transmission rate was 8-fold higher among women who seroconverted during pregnancy: Acute infection (seroconverted during pregnancy): transmission 12.9% Chronic infection (infected prior to pregnancy): transmission 1.6% (p<0.0001).
31 Acute HIV in Pregnancy New York State Birkhead GS, et al. Obstet Gynecol 2010;115: New York State: 3,396 HIV-exposed infants born MTCT 65 infants born to 63 mothers (2.1%) Acquisition of HIV during pregnancy significant risk factor: 22% infected with acute infection vs 1.8% with chronic Risk factor Adjusted Odds Ratio (95% CI) P value Acute HIV in pregnancy ( ) <0.001 Late/no prenatal care 2.37 ( ) Maternal HIV diagnosis at delivery or PP Illicit drug use during pregnancy 3.24 ( ) ( ) BW <2500 gm 2.46 ( ) 0.007
32 Management of Acute Infection in Pregnancy or Breastfeeding If suspect acute infection, obtain plasma HIV RNA test with HIV antibody test (4 th generation test preferred). Although positive RNA test should be confirmed, do not wait to initiate ART if RNA +. While resistance test should be obtained, initiation of ART should not be delayed; consider initiating PIbased ART (NNRTI transmitted resistance more likely). If pregnant, cesarean section (and IV AZT) likely needed due to insufficient time to achieve suppression. If breastfeeding, interrupt breastfeeding (can express and store milk awaiting confirmation); consult pediatric HIV specialist re: infant ARV management.


33 Jim Oleske, UMDNJ Newark Long-term survivors, 2003 Pregnancy in Perinatally-Infected Girls

34 Growing Population in Need of Contraception: Perinatally-Infected Young Women With availability potent ART, morbidity/mortality have decreased for perinatally-infected children. number girls with perinatal infection reaching childbearing age and becoming pregnant. Resource-rich countries: 17 publications on 305 pregnancies published between Most pregnancies unplanned; repeat pregnancy not uncommon. Some studies show higher rates adverse pregnancy outcomes than behaviorally-infected pregnant women. However, since most treated, MTCT uncommon (3 infections/ 176 live births, 1.7%).
35 HIV, Pregnancy and Maternal Health: Perinatally-Infected vs Behaviorally-Infected Women Munjal I et al. Adoles Health Med Ther. 2013;4:51-58 Bronx, NY: 37 pregnancies/30 perinatally-infected women vs 45/39 age-matched behaviorally-infected women Perinatal women more likely earlier GA and lower BW. CD4 lower, RNA higher perinatal women; 4 deaths perinatal group vs 0 death in behavioral group. CD4 count lower in perinatal women RNA higher in perinatal women
36 Management of Pregnant Women with Perinatal HIV Infection General principles of antepartum care and ART do not differ with perinatal vs horizontal infection; however, are more likely to be young/adolescent. ART adherence key challenge for women with longstanding HIV infection and adolescents. May be at risk of drug resistance due to extensive ART exposure prior to pregnancy; choice ART based on resistance testing, prior ART history. Nonpreferred drugs in pregnancy may be needed to achieve optimal viral suppression. Careful monitoring for adverse pregnancy outcome due to combination of risk factors: HIV infection, perinatal infection, ART, adolescence.

37 Breastfeeding and HIV in the US
38 Recommendations on Breastfeeding and HIV in the United States August 2015 Avoidance of breastfeeding is strongly recommended for HIV+ women in the United States because: maternal ART reduces but doesn t eliminate postnatal transmission safe and affordable replacement feeding available formula feeding is not associated with excess infant morbidity/mortality potential infant toxicity from ARV in breast milk (variable penetration depending on drug) potential for multi-drug resistant virus should infant become infected
39 Breastfeeding and HIV in the United States However, women may face social, familial, and person pressures to consider breastfeeding despite recommendation. Without effective education and support, HIV+ women may breastfeed or use mixed feeding in resolving infant feeding pressures or conflicts, and increase risk transmission to infant. A 31-year-old HIV+ Nigerian woman just arrived in the United States, 34 weeks pregnant and on ART with an undetectable viral load. She plans to return to Nigeria when the baby is 6 weeks old. Because formula feeding was not a feasible or safe option when she returned home, she wanted to breastfeed her baby. She has only disclosed her HIV diagnosis to her husband; she has not disclosed to other family members or her community. There is a close Nigerian community in the area, and the patient explains that people suspect that a woman has HIV infection if she does not breastfeed.
40 Breastfeeding and HIV-Infected Women in the US: Harm-Reduction Counseling Strategies Levison J et al. Clin Infect Dis 2014;59:304-9 Important to discuss infant feeding choice with patient in antepartum period to: allow addressing possible barriers to formula-feeding before delivery, allow women to understand risk of HIV transmission even if she is on suppressive ART, offer safe alternatives to breastfeeding, and for women who choose to breastfeed provide a harm-reduction approach to minimize transmission risk, including healthcare plan to achieve specific targets, such as an undetectable HIV viral load.

41 Potential Risks and Benefits of Different Feeding Options for HIV-Exposed Infants in the US Levison J et al. Clin Infect Dis 2014;59:304-9

42 If Woman Decides to Breastfeed Despite Counseling: Harm-Reduction Strategies Levison J et al. Clin Infect Dis 2014;59:304-9 Discuss timing and methods of weaning and option to switch to replacement feeding at any time. Discuss what is known/not known about transmission with maternal ART, ARV penetration into milk, and infant safety. Explain exclusive breastfeeding for 1 st 6 months appears safer than mixed formula/breastfeeding; provide support. Ensure woman receiving/adhering to fully suppressive ART. Monitor maternal viral load monthly while breastfeeding. HIV PCR testing for infant monthly while breastfeeding and 1, 3, and 6 months after weaning. Educate about need for immediate care if signs of mastitis and need for prompt treatment to minimize HIV shedding in milk.


43 Some Resources August 2015 AIDSInfo.nih.gov: current US guidelines for maternal ART and prevention perinatal transmission. registry of birth outcomes for women on ART critical participate to enable monitoring for safety Perinatal HIV Hotline : 24-7 availability for expert consultation






44 Thanks For Your Attention!
45
Historic Perspective on HIV and TB Research in Pregnant Women
 Historic Perspective on HIV and TB Research in Pregnant Women Lynne M. Mofenson, M.D. Senior HIV Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation High Burden of TB/HIV in Women - 2016 TB HIV
Historic Perspective on HIV and TB Research in Pregnant Women Lynne M. Mofenson, M.D. Senior HIV Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation High Burden of TB/HIV in Women - 2016 TB HIV
All HIV+ Women on Antiretroviral Therapy Should Breastfeed in Both Low and High Resource Settings VOTE NO!!
 All HIV+ Women on Antiretroviral Therapy Should Breastfeed in Both Low and High Resource Settings VOTE NO!! Lynne Mofenson MD Elizabeth Glaser Pediatric AIDS Foundation My Esteemed Opponent Will Likely
All HIV+ Women on Antiretroviral Therapy Should Breastfeed in Both Low and High Resource Settings VOTE NO!! Lynne Mofenson MD Elizabeth Glaser Pediatric AIDS Foundation My Esteemed Opponent Will Likely
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES?
 WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
What s New. In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group
 What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
Obstetrics and HIV An Update. Jennifer Van Horn MD University of Utah
 Obstetrics and HIV An Update Jennifer Van Horn MD University of Utah Obstetrics and HIV Perinatal transmission Testing Antiretroviral therapy Antepartum management Intrapartum management Postpartum management
Obstetrics and HIV An Update Jennifer Van Horn MD University of Utah Obstetrics and HIV Perinatal transmission Testing Antiretroviral therapy Antepartum management Intrapartum management Postpartum management
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 3 June 2017 We have effective drugs. There is no reason why any mother should die of AIDS. There
Using new ARVs in pregnancy Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 3 June 2017 We have effective drugs. There is no reason why any mother should die of AIDS. There
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update
 Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Prevention of Perinatal HIV Transmission
 Prevention of Perinatal HIV Transmission Emily Adhikari, MD Division of Maternal-Fetal Medicine Obstetrics and Gynecology University of Texas Southwestern Medical Center February 20, 2018 None Understand
Prevention of Perinatal HIV Transmission Emily Adhikari, MD Division of Maternal-Fetal Medicine Obstetrics and Gynecology University of Texas Southwestern Medical Center February 20, 2018 None Understand
Pediatric HIV Update NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA. Date
 CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
Infertility Treatment and HIV
 Infertility Treatment and HIV Infertility Treatment by IVF Or Intra-cytoplasmic Sperm Injections (ICSC) In Chronic HIV-1 Sero- discordant Couples (Poster 670) Retrospective study of outcome of IVF or ICSC
Infertility Treatment and HIV Infertility Treatment by IVF Or Intra-cytoplasmic Sperm Injections (ICSC) In Chronic HIV-1 Sero- discordant Couples (Poster 670) Retrospective study of outcome of IVF or ICSC
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Dr Kerry Uebel Slides courtesy of Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 5 August 2017 We have effective drugs. There is no reason why
Using new ARVs in pregnancy Dr Kerry Uebel Slides courtesy of Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 5 August 2017 We have effective drugs. There is no reason why
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
Epatite B: fertilità, gravidanza ed allattamento, aspetti clinici e terapeutici. Ivana Maida
 Epatite B: fertilità, gravidanza ed allattamento, aspetti clinici e terapeutici Ivana Maida Positivity for HBsAg was found in 0.5% of tested women In the 70s and 80s, Italy was one of the European countries
Epatite B: fertilità, gravidanza ed allattamento, aspetti clinici e terapeutici Ivana Maida Positivity for HBsAg was found in 0.5% of tested women In the 70s and 80s, Italy was one of the European countries
2016 Perinatal Treatment Guidelines Update
 Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
during conception, pregnancy and lactation at 2 U.S. medical centers
 Use of HIV preexposure prophylaxis during conception, pregnancy and lactation at 2 U.S. medical centers Dominika Seidman, MD Shannon Weber, Maria Teresa Timoney, Karishma Oza, Elizabeth Mullins, Rodney
Use of HIV preexposure prophylaxis during conception, pregnancy and lactation at 2 U.S. medical centers Dominika Seidman, MD Shannon Weber, Maria Teresa Timoney, Karishma Oza, Elizabeth Mullins, Rodney
Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM
 Dept of O+G NRMSM") Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM SA Background Population: 48m Annual number of deliveries:1,2m 97% of women attend the first ANC 71% of women attend 5 th ANC visit 97% of
Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM SA Background Population: 48m Annual number of deliveries:1,2m 97% of women attend the first ANC 71% of women attend 5 th ANC visit 97% of
Mother to Child HIV Transmission
 Koff WC. NEJM 2010;363:e7 Mother to Child HIV Transmission Why We Still Need New Prevention Modalities Lynne M. Mofenson, M.D. Maternal and Pediatric Infectious Disease Branch Eunice Kennedy Shriver National
Koff WC. NEJM 2010;363:e7 Mother to Child HIV Transmission Why We Still Need New Prevention Modalities Lynne M. Mofenson, M.D. Maternal and Pediatric Infectious Disease Branch Eunice Kennedy Shriver National
All HIV-exposed Infants Should Receive Triple Drug Antiretroviral Prophylaxis. Against the motion
 All HIV-exposed Infants Should Receive Triple Drug Antiretroviral Prophylaxis Against the motion Hermione Lyall Imperial Healthcare NHS Trust, London, UK Acknowledgements: Pat Tookey, Ali Judd, Claire
All HIV-exposed Infants Should Receive Triple Drug Antiretroviral Prophylaxis Against the motion Hermione Lyall Imperial Healthcare NHS Trust, London, UK Acknowledgements: Pat Tookey, Ali Judd, Claire
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Management of the HIV-Exposed Infant
 Management of the HIV-Exposed Infant Katherine Knapp, MD Medical Director, Perinatal Program Department of Infectious Diseases St. Jude Children s Research Hospital Disclosures No conflicts of interest
Management of the HIV-Exposed Infant Katherine Knapp, MD Medical Director, Perinatal Program Department of Infectious Diseases St. Jude Children s Research Hospital Disclosures No conflicts of interest
Tunisian recommendations on ART : process and results
 Second Arab Congress of Clinical Microbiology and Infectious Diseases May 24-26, 2012. Tunisian recommendations on ART : process and results M. BEN MAMOU UNAIDS Email: BenmamouM@unaids.org M. CHAKROUN
Second Arab Congress of Clinical Microbiology and Infectious Diseases May 24-26, 2012. Tunisian recommendations on ART : process and results M. BEN MAMOU UNAIDS Email: BenmamouM@unaids.org M. CHAKROUN
PAEDIATRIC HIV INFECTION. Dr Ashendri Pillay Paediatric Infectious Diseases Specialist
 PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
DEPARTMENT. Treatment Recommendations for. Pregnant and Breastfeeding Women: Critical Issues Consolidated ARV Guidelines. Dr.
 2013 Consolidated ARV Guidelines H I V / A I D S Treatment Recommendations for DEPARTMENT Pregnant and Breastfeeding Women: Critical Issues Dr. Nathan Shaffer Objectives of Presentation obackground ooverview
2013 Consolidated ARV Guidelines H I V / A I D S Treatment Recommendations for DEPARTMENT Pregnant and Breastfeeding Women: Critical Issues Dr. Nathan Shaffer Objectives of Presentation obackground ooverview
Science roadmap on antiretroviral drugs for PMTCT and maternal treatment: current guidance, evidence in development and gaps
 Appendix 4 Science roadmap on antiretroviral drugs for PMTCT and maternal treatment: current guidance, evidence in development and gaps Lynne M. Mofenson, MD Eunice Kennedy Shriver National Institute of
Appendix 4 Science roadmap on antiretroviral drugs for PMTCT and maternal treatment: current guidance, evidence in development and gaps Lynne M. Mofenson, MD Eunice Kennedy Shriver National Institute of
HIV/AIDS Prenatal Care for HIV+ Mothers. 1. Algorithm for Prenatal Screening & Care (Antepartum)
") 7/10/18 njm 1. Algorithm for Prenatal Screening & Care (Antepartum) 2. Algorithm for Prenatal HIV Screening and Care (Mother refuses screening) 3. Algorithm for Intrapartum Care 4. Prenatal Care for HIV+
7/10/18 njm 1. Algorithm for Prenatal Screening & Care (Antepartum) 2. Algorithm for Prenatal HIV Screening and Care (Mother refuses screening) 3. Algorithm for Intrapartum Care 4. Prenatal Care for HIV+
The New National Guidelines. Feeding in the Context of HIV. Dr. Godfrey Esiru; National PMTCT Coordinator
 The New National Guidelines (2010) for PMTCT and Infant Feeding in the Context of HIV Dr. Godfrey Esiru; National PMTCT Coordinator Presentation outline Evolution of the PMTCT guidelines in Uganda Rational
The New National Guidelines (2010) for PMTCT and Infant Feeding in the Context of HIV Dr. Godfrey Esiru; National PMTCT Coordinator Presentation outline Evolution of the PMTCT guidelines in Uganda Rational
Breast Feeding for Women with HIV?
 Breast Feeding for Women with HIV? CHIVA / BHIVA Hermione Lyall Imperial Healthcare NHS Trust 17.11.17 Acknowledgements: Nell Freeman-Romilly, Pat Tookey, Claire Townsend, Claire Thorne, Kate Francis,
Breast Feeding for Women with HIV? CHIVA / BHIVA Hermione Lyall Imperial Healthcare NHS Trust 17.11.17 Acknowledgements: Nell Freeman-Romilly, Pat Tookey, Claire Townsend, Claire Thorne, Kate Francis,
Outline. Aim with PMTCT. How are children transmitted. Prevention of mother-to-child transmission of HIV. How does HIV transmit to children?
 Prevention of mother-to-child transmission of HIV Outline AimofPMTCT How HIV is transmitted to children Epidemiology of HIV in children How to reduce HIV transmission to children Guidelines Lars T. Fadnes
Prevention of mother-to-child transmission of HIV Outline AimofPMTCT How HIV is transmitted to children Epidemiology of HIV in children How to reduce HIV transmission to children Guidelines Lars T. Fadnes
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010
 THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Labor & Delivery Management for Women Living with HIV. Pooja Mittal, DO Lisa Rahangdale, MD
 Labor & Delivery Management for Women Living with HIV Pooja Mittal, DO Lisa Rahangdale, MD Statistics for Perinatally Acquired HIV Timing of Perinatal HIV Transmission Most transmission occurs close to
Labor & Delivery Management for Women Living with HIV Pooja Mittal, DO Lisa Rahangdale, MD Statistics for Perinatally Acquired HIV Timing of Perinatal HIV Transmission Most transmission occurs close to
CCC ARV Dosing Recommendations for HIV-exposed infants Updated
 USERS NOTE: Please note this document does not provide guidance on overall decisionmaking regarding what medication(s) to use for HIV-exposed infants. This document is meant to facilitate ARV dosing for
USERS NOTE: Please note this document does not provide guidance on overall decisionmaking regarding what medication(s) to use for HIV-exposed infants. This document is meant to facilitate ARV dosing for
HIV in Pregnancy. In Practice. Cheryl Roth Pauline F. Hrenchir Christine J. Pacheco
 In Practice Photo istock Collection / thinkstockphotos.com IImagine this scenario: You are working on a Saturday afternoon when a woman comes into the obstetrics triage unit. She is pregnant for the fourth
In Practice Photo istock Collection / thinkstockphotos.com IImagine this scenario: You are working on a Saturday afternoon when a woman comes into the obstetrics triage unit. She is pregnant for the fourth
CROI 2016 Update NEAETC, March 21, Sigal Yawetz, MD Brigham and Women s Hospital Harvard Medical School
 CROI 2016 Update NEAETC, March 21, 2016 Sigal Yawetz, MD Brigham and Women s Hospital Harvard Medical School CROI 2016 Update NEAETC, March 21, 2016 UNITED STATES EPIDEMIOLOGY Estimating the lifetime risk
CROI 2016 Update NEAETC, March 21, 2016 Sigal Yawetz, MD Brigham and Women s Hospital Harvard Medical School CROI 2016 Update NEAETC, March 21, 2016 UNITED STATES EPIDEMIOLOGY Estimating the lifetime risk
1. Africa Centre for Health and Population Studies 2. London School of Hygiene and Tropical Medicine 3. University College London
 A systematic review of the effects of interrupted antiretroviral interventions for prevention of mother-to-child transmission of HIV on maternal disease progression and survival Naidu KK 1, Mori R 2, Newell
A systematic review of the effects of interrupted antiretroviral interventions for prevention of mother-to-child transmission of HIV on maternal disease progression and survival Naidu KK 1, Mori R 2, Newell
Preventing Mother to Child HIV Transmission: Are We There Yet?!'
 Preventing Mother to Child HIV Transmission: Are We There Yet?!' 2017 Michigan Clincal Nursing Conference for HIV and STD Care May 18, 2017 Frankenmuth MI 1 Theodore B. Jones, MD Maternal Fetal Medicine
Preventing Mother to Child HIV Transmission: Are We There Yet?!' 2017 Michigan Clincal Nursing Conference for HIV and STD Care May 18, 2017 Frankenmuth MI 1 Theodore B. Jones, MD Maternal Fetal Medicine
HIV IN PREGNANCY. Practices for Maintaining Maternal Health and Preventing Perinatal HIV Transmission. University of Tennessee Health Science Center
 HIV IN PREGNANCY Practices for Maintaining Maternal Health and Preventing Perinatal HIV Transmission Nina K. Sublette, PhD, FNP University of Tennessee Health Science Center College of Nursing: Department
HIV IN PREGNANCY Practices for Maintaining Maternal Health and Preventing Perinatal HIV Transmission Nina K. Sublette, PhD, FNP University of Tennessee Health Science Center College of Nursing: Department
Register for notification of guideline updates at
 Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States Visit the AIDSinfo website
Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States Visit the AIDSinfo website
Objectives. Outline. Section 1: Interaction between HIV and pregnancy. Effects of HIV on Pregnancy. Section 2: Mother-to-Child-Transmission (MTCT)
") Objectives Prevention of Mother-to-Child Transmission (PMTCT) Teen Club Community Partners Training Programme By the end of the session participants will be able to: 1. Identify factors affecting the transmission
Objectives Prevention of Mother-to-Child Transmission (PMTCT) Teen Club Community Partners Training Programme By the end of the session participants will be able to: 1. Identify factors affecting the transmission
HIV/AIDS Prenatal Care for HIV+ Mothers. 1. Algorithm for Prenatal Screening & Care (Antepartum)
") 1. Algorithm for Prenatal Screening & Care (Antepartum) 2. Algorithm for Prenatal HIV Screening and Care (Mother refuses screening) 3. Algorithm for Intrapartum Care 4. Prenatal Care for HIV+ Mothers a.
1. Algorithm for Prenatal Screening & Care (Antepartum) 2. Algorithm for Prenatal HIV Screening and Care (Mother refuses screening) 3. Algorithm for Intrapartum Care 4. Prenatal Care for HIV+ Mothers a.
New Directions on WHO ARV Guidelines 2018
 New Directions on WHO ARV Guidelines 2018 Elaine Abrams Co-chair WHO Guidelines Development Group ICAP at Columbia University, New York Martina Penazzato Paediatric lead for the HIV Department World Health
New Directions on WHO ARV Guidelines 2018 Elaine Abrams Co-chair WHO Guidelines Development Group ICAP at Columbia University, New York Martina Penazzato Paediatric lead for the HIV Department World Health
Updates on Revised Antiretroviral Treatment Guidelines Overview 27 March 2013
 Updates on Revised Antiretroviral Treatment Guidelines 2013 Overview 27 March 2013 Introduction of Fixed Dose combination (FDC) FDCs will be available in facilities on 1 April 2013 The FDC ARV that will
Updates on Revised Antiretroviral Treatment Guidelines 2013 Overview 27 March 2013 Introduction of Fixed Dose combination (FDC) FDCs will be available in facilities on 1 April 2013 The FDC ARV that will
Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20
 Introduction Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20 Proportions HIV infections 19% amongst adolescents (- 29.5% nationally 15
Introduction Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20 Proportions HIV infections 19% amongst adolescents (- 29.5% nationally 15
Early Antiretroviral Therapy in Newborns: Opportunities and Challenges. Ellen Gould Chadwick MD Northwestern University Feinberg School of Medicine
 Early Antiretroviral Therapy in Newborns: Opportunities and Challenges Ellen Gould Chadwick MD Northwestern University Feinberg School of Medicine Conflict of Interest Disclosures for Ellen Chadwick MD
Early Antiretroviral Therapy in Newborns: Opportunities and Challenges Ellen Gould Chadwick MD Northwestern University Feinberg School of Medicine Conflict of Interest Disclosures for Ellen Chadwick MD
ARV Consolidated Guidelines 2015
 ARV Consolidated Guidelines 2015 This document outlines the draft list of PICO questions to support systematic review process for the 2015 ARV guidelines process. PICO questions are grouped by clinical
ARV Consolidated Guidelines 2015 This document outlines the draft list of PICO questions to support systematic review process for the 2015 ARV guidelines process. PICO questions are grouped by clinical
Pregnancy and HIV Reviewing the Vertical Transmission Risks 2015 OCN Education Day V Logan Kennedy RN, MN Research Associate and Clinical Nursing
 Pregnancy and HIV Reviewing the Vertical Transmission Risks 2015 OCN Education Day V Logan Kennedy RN, MN Research Associate and Clinical Nursing Specialist Women s College Research Institute, Women s
Pregnancy and HIV Reviewing the Vertical Transmission Risks 2015 OCN Education Day V Logan Kennedy RN, MN Research Associate and Clinical Nursing Specialist Women s College Research Institute, Women s
Use of a Multidisciplinary Care Model for Pregnant Women Living with HIV & Their Infants Sarah McBeth, MD MPH
 Use of a Multidisciplinary Care Model for Pregnant Women Living with HIV & Their Infants Sarah McBeth, MD MPH University of Pittsburgh Medical Center Disclosures Presenter has no financial interests to
Use of a Multidisciplinary Care Model for Pregnant Women Living with HIV & Their Infants Sarah McBeth, MD MPH University of Pittsburgh Medical Center Disclosures Presenter has no financial interests to
WHO s early release guidelines on PrEP: implications for emtct. Dominika Seidman, MD October 13, 2015
 WHO s early release guidelines on PrEP: implications for emtct Dominika Seidman, MD October 13, 2015 Outline Evidence behind WHO early release guidelines on PrEP PrEP eligibility according to the WHO Rationale
WHO s early release guidelines on PrEP: implications for emtct Dominika Seidman, MD October 13, 2015 Outline Evidence behind WHO early release guidelines on PrEP PrEP eligibility according to the WHO Rationale
Update on global guidelines. and emerging issues on perinatal HIV prevention. WHO 2013 Consolidated ARV Guidelines
 WHO 2013 Consolidated ARV Guidelines Update on global guidelines H I V / A I D S DEPARTMENT and emerging issues on perinatal HIV prevention Children & HIV, St. Petersburg, Russia Sept 25-26, 2014 Dr. Nathan
WHO 2013 Consolidated ARV Guidelines Update on global guidelines H I V / A I D S DEPARTMENT and emerging issues on perinatal HIV prevention Children & HIV, St. Petersburg, Russia Sept 25-26, 2014 Dr. Nathan
Rajesh T. Gandhi, M.D.
 HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV
 TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV Gladwel Muthoni KPA Conference 24 th April, 2018 OUTLINE Burden of HIV in PMTCT Mechanism and timing of Mother to Child Transmission (MTCT) Four
TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV Gladwel Muthoni KPA Conference 24 th April, 2018 OUTLINE Burden of HIV in PMTCT Mechanism and timing of Mother to Child Transmission (MTCT) Four
Pediatric Antiretroviral Therapy
 Update on Pediatric Antiretroviral Therapy Lynne M. Mofenson, M.D. Pediatric, Adolescent and Maternal AIDS Branch National Institute of Child Health and Human Development National Institutes of Health
Update on Pediatric Antiretroviral Therapy Lynne M. Mofenson, M.D. Pediatric, Adolescent and Maternal AIDS Branch National Institute of Child Health and Human Development National Institutes of Health
The next generation of ART regimens
 The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
2009 Revisions of WHO ART Guidelines. November 2009
 2009 Revisions of WHO ART Guidelines November 2009 Guidelines Development Process 01/09 2009 WHO ART guideline revision process Scope of the work 03/09 WHO Guideline review committee approval 04/09 05/09
2009 Revisions of WHO ART Guidelines November 2009 Guidelines Development Process 01/09 2009 WHO ART guideline revision process Scope of the work 03/09 WHO Guideline review committee approval 04/09 05/09
Appendix 1: summary of the modified GRADE system (grades 1A 2D)
") Appendix 1: summary of the modified GRADE system (grades 1A 2D) 1A 1B 1C 1D 2A 2B 2C 2D Strong recommendation High-quality evidence Benefits clearly outweigh risk and burdens, or vice versa Consistent
Appendix 1: summary of the modified GRADE system (grades 1A 2D) 1A 1B 1C 1D 2A 2B 2C 2D Strong recommendation High-quality evidence Benefits clearly outweigh risk and burdens, or vice versa Consistent
Treatment Optimization for EMTCT
 Treatment Optimization for EMTCT Dr Madeleine Muller With thanks to CN Mnyani and Linda-Gail Bekker SA HIV Clinician s Society Meeting 25 Nov 2017 Having children is one of the greatest joys and privileges
Treatment Optimization for EMTCT Dr Madeleine Muller With thanks to CN Mnyani and Linda-Gail Bekker SA HIV Clinician s Society Meeting 25 Nov 2017 Having children is one of the greatest joys and privileges
Perinatal HIV Exposure: Antiretroviral Management. Danielle McDonald, PharmD PGY-2 Pediatric Pharmacotherapy Resident
 Perinatal HIV Exposure: Antiretroviral Management Danielle McDonald, PharmD PGY-2 Pediatric Pharmacotherapy Resident A presentation for HealthTrust Members June 1, 2018 Learning Objectives for Pharmacists
Perinatal HIV Exposure: Antiretroviral Management Danielle McDonald, PharmD PGY-2 Pediatric Pharmacotherapy Resident A presentation for HealthTrust Members June 1, 2018 Learning Objectives for Pharmacists
SA HIV Clinicians Society Adult ART guidelines
 SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
Should we treat hepatitis B positive pregnant women to prevent mother to child transmission?
 Should we treat hepatitis B positive pregnant women to prevent mother to child transmission? Daniel Shouval Liver Unit Hadassah-Hebrew University Hospital Jerusalem, Israel VHPB Vienna June 1-2, 2017 Background
Should we treat hepatitis B positive pregnant women to prevent mother to child transmission? Daniel Shouval Liver Unit Hadassah-Hebrew University Hospital Jerusalem, Israel VHPB Vienna June 1-2, 2017 Background
treatment during pregnancy and breastfeeding
 treatment during pregnancy and breastfeeding Topics covered Introduction. Preventing parent-to-child transmission. AZT as a single therapy. Treatment begun late in pregnancy. Nevirapine for mothers and
treatment during pregnancy and breastfeeding Topics covered Introduction. Preventing parent-to-child transmission. AZT as a single therapy. Treatment begun late in pregnancy. Nevirapine for mothers and
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
Elijah Paintsil, MD, FAAP
 Roadmap to elimination of mother-to-child transmission of HIV in Ghana by 2015 Towards HIV Free Generation Elijah Paintsil, MD, FAAP Assistant Professor of Pediatrics & Pharmacology Yale School of Medicine,
Roadmap to elimination of mother-to-child transmission of HIV in Ghana by 2015 Towards HIV Free Generation Elijah Paintsil, MD, FAAP Assistant Professor of Pediatrics & Pharmacology Yale School of Medicine,
Pediatric HIV Cure Research
 Pediatric HIV Cure Research HIV Cure Research Training Curriculum Pediatric HIV Cure Research Presented by: Priyanka Uprety,MSPH, PhD Laboratory of Deborah Persaud, MD Johns Hopkins University July 2016
Pediatric HIV Cure Research HIV Cure Research Training Curriculum Pediatric HIV Cure Research Presented by: Priyanka Uprety,MSPH, PhD Laboratory of Deborah Persaud, MD Johns Hopkins University July 2016
Prevention of Mother-to-Child Transmission of HIV Infection
 HIV Curriculum for the Health Professional Prevention of Mother-to-Child Transmission of HIV Infection Michael A. Tolle, MD, MPH Daniel Dewey, MD Objectives 1. Describe the scope of mother-to-child transmission
HIV Curriculum for the Health Professional Prevention of Mother-to-Child Transmission of HIV Infection Michael A. Tolle, MD, MPH Daniel Dewey, MD Objectives 1. Describe the scope of mother-to-child transmission
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Rough K, Seage GR III, Williams PL, et al. Birth outcomes for
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Rough K, Seage GR III, Williams PL, et al. Birth outcomes for
California Perinatal Quality Care Collaborative 2013 Standards of Care for the Prevention of Perinatal HIV Transmission
 2013 Revised Edition Authors: David K Hong, MD, Nivedita Srinivas, MD Original Authors: Mary Campbell Bliss, RN, MS, CNS, William Gilbert, MD, Jan Lanouette, MD, Courtney Nisbet, RN, MS, David Wirtschafter,
2013 Revised Edition Authors: David K Hong, MD, Nivedita Srinivas, MD Original Authors: Mary Campbell Bliss, RN, MS, CNS, William Gilbert, MD, Jan Lanouette, MD, Courtney Nisbet, RN, MS, David Wirtschafter,
Infant feeding in the ARV era. Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital
 Infant feeding in the ARV era Gerhard Theron Gerhard Theron Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital Global HIV infections: 2007 12 countries account for
Infant feeding in the ARV era Gerhard Theron Gerhard Theron Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital Global HIV infections: 2007 12 countries account for
What Women Need to Know: The HIV Treatment Guidelines for Pregnant Women
 : The HIV Treatment Guidelines for Pregnant Women : The HIV Treatment Guidelines for Pregnant Women What Women Need to Know: Prepared by Elaine Gross, RN, MS, CNS-C National Pediatric & Family HIV Resource
: The HIV Treatment Guidelines for Pregnant Women : The HIV Treatment Guidelines for Pregnant Women What Women Need to Know: Prepared by Elaine Gross, RN, MS, CNS-C National Pediatric & Family HIV Resource
Treatment of Hepatitis (and HIV) in Pregnancy 2010
 in Pregnancy 2010") Treatment of Hepatitis (and HIV) in Pregnancy 2010 Douglas T. Dieterich, M.D. Professor of Medicine, Division of Liver Diseases, Director of CME, Department of Medicine, Mt Sinai School of Medicine Zidovudine
Treatment of Hepatitis (and HIV) in Pregnancy 2010 Douglas T. Dieterich, M.D. Professor of Medicine, Division of Liver Diseases, Director of CME, Department of Medicine, Mt Sinai School of Medicine Zidovudine
Malaysian Consensus Guidelines on Antiretroviral Therapy Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh
 Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
The Cumulative Incidence of HIV Infection in HIVexposed Infants with a Birth Weight of 1500g Receiving Breast Milk and Daily Nevirapine
 The Cumulative Incidence of HIV Infection in HIVexposed Infants with a Birth Weight of 1500g Receiving Breast Milk and Daily Nevirapine A retrospective, descriptive study conducted at Kalafong hospital,
The Cumulative Incidence of HIV Infection in HIVexposed Infants with a Birth Weight of 1500g Receiving Breast Milk and Daily Nevirapine A retrospective, descriptive study conducted at Kalafong hospital,
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
DECLINE IN POSITIVITY RATES AMONG HIV-EXPOSED INFANTS WITH CHANGES IN PMTCT ARV REGIMENS IN NIGERIA: EVIDENCE FROM 7 YEARS OF FIELD IMPLEMENTATION
 Abst#_O_01 DECLINE IN POSITIVITY RATES AMONG HIV-EXPOSED INFANTS WITH CHANGES IN PMTCT ARV REGIMENS IN NIGERIA: EVIDENCE FROM 7 YEARS OF FIELD IMPLEMENTATION Hadiza Khamofu, 1 Edward Oladele, 1 Uche Ralph-Opara,
Abst#_O_01 DECLINE IN POSITIVITY RATES AMONG HIV-EXPOSED INFANTS WITH CHANGES IN PMTCT ARV REGIMENS IN NIGERIA: EVIDENCE FROM 7 YEARS OF FIELD IMPLEMENTATION Hadiza Khamofu, 1 Edward Oladele, 1 Uche Ralph-Opara,
Prevention of Mother to Child Transmission of HIV: Our Experience in South India
 pg 62-66 Original Article Prevention of Mother to Child Transmission of HIV: Our Experience in South India Karthekeyani Vijaya 1, Alexander Glory 2, Solomon Eileen 3, Rao Sarita 4, Rao P.S.S.Sunder 5 1
pg 62-66 Original Article Prevention of Mother to Child Transmission of HIV: Our Experience in South India Karthekeyani Vijaya 1, Alexander Glory 2, Solomon Eileen 3, Rao Sarita 4, Rao P.S.S.Sunder 5 1
Michigan Guidelines: HIV, Syphilis, HBV in Pregnancy
 Michigan Guidelines: HIV, Syphilis, HBV in Pregnancy Presenter: Theodore B. Jones, MD Maternal Fetal Medicine Wayne State University School of Medicine Beaumont Dearborn Hospital HIV, Syphilis, HBV in
Michigan Guidelines: HIV, Syphilis, HBV in Pregnancy Presenter: Theodore B. Jones, MD Maternal Fetal Medicine Wayne State University School of Medicine Beaumont Dearborn Hospital HIV, Syphilis, HBV in
Visit Reason: Positive Pregnancy Test. HIV Treatment in the Childbearing Woman
 Visit Reason: Positive Pregnancy Test. HIV Treatment in the Childbearing Woman Thi-Thi Nguyen, PharmD, BCPS, AAHIVP Mountain Plains AIDS Education and Training Center Conference August 13th, 2015 1 Objectives
Visit Reason: Positive Pregnancy Test. HIV Treatment in the Childbearing Woman Thi-Thi Nguyen, PharmD, BCPS, AAHIVP Mountain Plains AIDS Education and Training Center Conference August 13th, 2015 1 Objectives
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
HIV, Women, & Pregnancy
 HIV, Women, & Pregnancy Facts, Myths, and Management Nina K. Sublette, PhD, ACRN, AACRN, FNP University of Tennessee Department of Obstetrics and Gynecology St. Jude Children s Research Hospital Department
HIV, Women, & Pregnancy Facts, Myths, and Management Nina K. Sublette, PhD, ACRN, AACRN, FNP University of Tennessee Department of Obstetrics and Gynecology St. Jude Children s Research Hospital Department
Infant feeding and HIV Policy, Evidence and Hospital Challenges
 Infant feeding and HIV Policy, Evidence and Hospital Challenges Max Kroon MMH/SCAH MY BRIEF Overview of infant feeding within the PMTCT program including national policy, feeding choices & research evidence
Infant feeding and HIV Policy, Evidence and Hospital Challenges Max Kroon MMH/SCAH MY BRIEF Overview of infant feeding within the PMTCT program including national policy, feeding choices & research evidence
What are the most promising opportunities for dose optimisation?
 What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
Existing and most needed paediatric ARV formulations
 Existing and most needed paediatric ARV formulations Martina Penazzato Paediatric HIV advisor WHO HIV Department, Geneva Mach 7th 2016 Paediatric coverage still lags behind 45 40 35 30 25 20 15 10 5 0
Existing and most needed paediatric ARV formulations Martina Penazzato Paediatric HIV advisor WHO HIV Department, Geneva Mach 7th 2016 Paediatric coverage still lags behind 45 40 35 30 25 20 15 10 5 0
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
Pregnancy and HIV. Dr Annemiek de Ruiter. September 2009
 Pregnancy and HIV Dr Annemiek de Ruiter September 2009 NSHPC NSHPC update, October 2008 Obstetric and paediatric HIV surveillance data from the UK and Ireland National Study of HIV in Pregnancy and Childhood
Pregnancy and HIV Dr Annemiek de Ruiter September 2009 NSHPC NSHPC update, October 2008 Obstetric and paediatric HIV surveillance data from the UK and Ireland National Study of HIV in Pregnancy and Childhood
Clinical skills building - HIV drug resistance
 Clinical skills building - HIV drug resistance Richard Lessells Clinical case 44-year old HIV-positive male HIV diagnosis 2010 Pre-treatment CD4+ count not known Initiated first-line ART (TDF/FTC/EFV)
Clinical skills building - HIV drug resistance Richard Lessells Clinical case 44-year old HIV-positive male HIV diagnosis 2010 Pre-treatment CD4+ count not known Initiated first-line ART (TDF/FTC/EFV)
HIV. Transmission modes. Transmission modes in children. Prevention of mother-to-child transmission of HIV. HIV identified in 1983
 Prevention of mother-to-child transmission of HIV HIV identified in 1983 HIV AIDS syndrome described in 1981 Kaposi s sarcoma, Pneumocystis jiroveci pnemumonia and wasting often combined Retrospectively,
Prevention of mother-to-child transmission of HIV HIV identified in 1983 HIV AIDS syndrome described in 1981 Kaposi s sarcoma, Pneumocystis jiroveci pnemumonia and wasting often combined Retrospectively,
Phase II clinical trial TEmAA. Didier Koumavi EKOUEVI, MD PhD (Principal Investigator)
") The combination of Tenofovir-Emtricitabine (Truvada ): a new antiretroviral (ARV) regimen for the prevention of mother-to-child transmission of HIV-1 (PMTCT) in resource-limited settings Phase II clinical
The combination of Tenofovir-Emtricitabine (Truvada ): a new antiretroviral (ARV) regimen for the prevention of mother-to-child transmission of HIV-1 (PMTCT) in resource-limited settings Phase II clinical
hiv/aids Programme Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants
 hiv/aids Programme Programmatic update Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants EXECUTIVE SUMMARY April 2012 EXECUTIVE SUMMARY Recent developments
hiv/aids Programme Programmatic update Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants EXECUTIVE SUMMARY April 2012 EXECUTIVE SUMMARY Recent developments
Antiretroviral Treatment Strategies: Clinical Case Presentation
 Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Is current first line ART good enough? Francois Venter Wits Reproductive Health & HIV Research Institute
 Is current first line ART good enough? Francois Venter Wits Reproductive Health & HIV Research Institute Results: by April 2011 Budget: $3.5 billion 80% of 3,686 health facilities providing ARVs 50% ARV
Is current first line ART good enough? Francois Venter Wits Reproductive Health & HIV Research Institute Results: by April 2011 Budget: $3.5 billion 80% of 3,686 health facilities providing ARVs 50% ARV
TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES
 POLICY BRIEF HIV TREATMENT TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES JULY 2017 WHO This policy brief provides advice on a phased approach to transitioning to new WHO-recommended HIV treatment
POLICY BRIEF HIV TREATMENT TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES JULY 2017 WHO This policy brief provides advice on a phased approach to transitioning to new WHO-recommended HIV treatment
HIV in in Women Women
 HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV Treatment: New and Veteran Drugs Classes
 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
Obstetric Complications in HIV-Infected Women. Jeanne S. Sheffield, MD Maternal-Fetal Medicine UT Southwestern Medical School
 Obstetric Complications in HIV-Infected Women Jeanne S. Sheffield, MD Maternal-Fetal Medicine UT Southwestern Medical School Obstetric Complications and HIV Obstetric complications are not increased in
Obstetric Complications in HIV-Infected Women Jeanne S. Sheffield, MD Maternal-Fetal Medicine UT Southwestern Medical School Obstetric Complications and HIV Obstetric complications are not increased in
HIV Infection in Pregnancy. Francis J. Ndowa WHO RHR/STI
 HIV Infection in Pregnancy Francis J. Ndowa WHO RHR/STI FJN_STI_2005 Department of reproductive health and research Département santé et recherche génésiques Session outline Effect of pregnancy on HIV
HIV Infection in Pregnancy Francis J. Ndowa WHO RHR/STI FJN_STI_2005 Department of reproductive health and research Département santé et recherche génésiques Session outline Effect of pregnancy on HIV
The NEW ARV Guidelines FAQs
 The NEW ARV Guidelines FAQs Dr Madeleine Muller MBChB (Pret).MRCGP(Lon).Dip Hiv Man IYDSA Clinical Advisor Acknowledgments IYDSA for materials and support NDOH for slides CDC our funder HIV Clinician Society
The NEW ARV Guidelines FAQs Dr Madeleine Muller MBChB (Pret).MRCGP(Lon).Dip Hiv Man IYDSA Clinical Advisor Acknowledgments IYDSA for materials and support NDOH for slides CDC our funder HIV Clinician Society
Women are the fastest-growing group of persons with
 Clinical Guidelines Prenatal Screening for HIV: A Review of the Evidence for the U.S. Preventive Services Task Force Roger Chou, MD; Ariel K. Smits, MD, MPH; Laurie Hoyt Huffman, MS; Rongwei Fu, PhD; and
Clinical Guidelines Prenatal Screening for HIV: A Review of the Evidence for the U.S. Preventive Services Task Force Roger Chou, MD; Ariel K. Smits, MD, MPH; Laurie Hoyt Huffman, MS; Rongwei Fu, PhD; and
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades