Diagnosis of Tuberculosis Infection and Disease
|
|
|
- Jesse Nichols
- 5 years ago
- Views:
Transcription
1 Diagnosis of Tuberculosis Infection and Disease David E. Griffith, M.D. Assistant Medical Director Heartland National TB Center The Medical Evaluation for Diagnosing Tuberculosis Traditional Approach Patient History Physical examination Radiologic evaluation Laboratory testing A New Approach Define: 1. The Host 2. The Syndrome 3. The Microbiology 4. The Treatment TB Control Programs Healthcare System and Cultural Barriers Case identification Early recognition of drug resistant disease Availability of appropriate TB meds Administration of adequate TB regimens Treatment of co-existing medical problems Administrative and engineering controls to prevent TB transmission Isolation of contagious cases Quarantine for nonadherent patients Contact investigation/treatment of LTBI 1
2 Factors Contributing to the Increase in TB Morbidity: Deterioration of the TB public health infrastructure Immigration from countries where TB is common HIV/AIDS epidemic Homelessness, drug and alcohol abuse Socioeconomic Characteristics of TB in the US Among non-immigrants, TB significantly associated with Poverty and unemployment Homelessness Congregate settings Incarceration Alcoholism and drug abuse HIV infection rates also high in some of these populations Tuberculosis and Substance Abuse in the United States, Oeltmann et al Arch Int Med 2008, 169; 189 Substance abuse is the most commonly reported behavioral risk factor among patients with TB in the U.S. Patients who abuse substances are more contagious and remain contagious longer because treatment failure extends periods of infectiousness 2

3 Trends in TB Cases in Foreign-born Persons, United States, * No. of Cases 10,000 8,000 6,000 4,000 2, Percentage No. of Cases Percentage of Total Cases *Updated as of March 29, Estimated Migrants Entering U.S. Visitors without visas ~ 30,000,000 Non-immigrant visas 27,907,139 Immigrants and refugees 411,266 Undocumented migrants ~ 275,000???? N= ~ 59,000,000 Status adjusters in U.S.: 679,305 Source: U.S. Department of Homeland Security, 2003 (2002 data) In 2005, approximately one half of the foreign-born MDR TB patients were from Mexico, the Philippines and Vietnam. 3
4 XDR TB in the United States Probably relatively little acquired MDR and XDR TB in the U.S. Major source of MDR and XDR TB patients foreign-born patients (33% Hispanic) Suspicion of drug resistance paramount May be difficult to devise initial empiric regimens Summary TB rates continues to decline in the U.S. Rate of decline has slowed Foreign-born and racial/ethnic minorities continue to be disproportionately impacted Unknown HIV status for almost 1/3 of TB cases Proportion of TB cases that are MDR remains constant LATENT TUBERCULOSIS INFECTION (LTBI) AJRCCM, April 2000; 161: S221-S243 4
5 Who Should be Tested for TB Infection? Targeted testing of high risk individuals and groups to identify those at risk of recent infection Contacts of active cases Foreign born who entered US in last 5 years High risk populations where transmission of TB likely to have occurred (HCW, prisons, nursing homes, other congregate settings) Over half of lifetime risk occurs in the first 1-2 years after infection Who Should be Tested for TB Infection? Persons with medical risk factors that increase risk of progression to disease HIV infection Chronic renal failure Immunosuppressive Rx Diabetes mellitus Malignancy TNF Alpha blocker therapy Transplant recipients > 15 mg Prednisone/day Silicosis LTBI - Criteria for PPD 5mm cut-point HIV positive persons Recent contacts of TB cases Fibrotic Changes on CXR c/w old (not treated) TB Patients with organ transplants or other immunosuppression Prednisone therapy 15 mg/day > 1 month Patients receiving TNF-alpha blockers 5
6 Warning: Risk Of Infections Infliximab, Etanercept, Adalimuamab Tuberculosis (frequently disseminated or extrapulmonary at clinical presentation), and other opportunistic infections have been observed in patients receiving Remicade some of these infections have been fatal. Patients should be evaluated for LTBI with a TST. Treatment of LTBI should be initiated prior to therapy with Remicade. SEE WARNINGS» PDR 2004 LTBI - Criteria for PPD 10 mm cut-point Recent arrivals (<5 yrs) high prevalence countries IVDU Residents/employees - high-risk congregate facilities (health care, prisons, shelters, etc.) TB lab personnel Persons with high-risk medical conditions Children <4 yrs or exposed to adults at risk LTBI - Criteria for PPD 15 mm cut-point Persons with no risk factors Usually shouldn t be tested unless as part of baseline assessment for those at risk due to jobs in high risk settings 6
7 Tuberculin Skin Testing Requires two visits. Experienced personnel needed for placement and interpretation. Inter and intra-observer variability. Complex guidelines defining LTBI. Does not differentiate infection from disease Frequently negative in high risk patients and patients with active disease M. TUBERCULOSIS- SPECIFIC ANTIGENS Sequencing the TB genome has revealed three antigens, ESAT-6 (early secreted antigenic target 6 kd protein), CFP10 (culture filtrate protein 10) and TB7.7 that are not present in BCG or in most environmental mycobacteria ESAT-6, CFP-10 and TB 7.7 stimulate IFN-γ production by PBMC CYTOKINES PRODUCED BY M. TUBERCULOSIS-STIMULATED PBMC The predominant host response to M. tuberculosis infection consists of antigenspecific memory T cells releasing IFN-γ in response to previously encountered mycobacterial antigens PBMC from healthy tuberculin reactors produce high concentrations of IFN-γ (with appropriate stimulation) 7
8 PRINCIPLES FOR IFN-GAMMA BASED TB DIAGNOSTIC TESTS Tuberculin skin test Multiple (hundreds) potential antigens Complex immune response, multiple immune mediators Interferon-gamma based tests 3antigens (ESAT-6, CFP-10, TB7.7) One immune mediator INTERFERON GAMMA (IFN-GAMMA) BASED TESTS FOR DIAGNOSING LTBI BLOOD TESTS FOR LTBI Quantiferon (Cellestis) Quantiferon TB-GOLD (Cellestis) T-SPOT TB (Oxford Immunotec) Quantiferon TB-Gold In-Tube (Cellestis) 8
9 QuantiFERON-TB Gold (ELISA) Nil ESAT-6 CFP-10 Mitogen Control Control Obtain blood Transfer blood to wells and add antigens Culture overnight. TBinfected individuals secrete IFN-γ COLOR TMB OD Standard Curve Harvest supernatants and perform ELISA Wash, add substrate, incubate 30 min IFN-γ IU/ml Measure OD and determine IFN-γ levels QuantiFERON-TB Gold In Tube Stage One Blood Incubation and Harvesting Nil Control ESAT-6 CFP-10 Mitogen Control 1. Collect blood. Incubate at 37ºC for hrs. Stage Two Human IFN-γ ELISA 2. Centrifuge tubes for 5 minutes. IFN-γ stable refrigerated for at least 8 weeks. 3. Add plasma and conjugate to ELISA plate. Incubate for 120 mins. 4. Wash and add substrate. Read absorbance after 30 min. Quantiferon Interpretation Positive: ESAT-6 and/or CFP-10 level > 0.35 iu and 50% > placebo (negative) control Negative: ESAT-6 and/or CFP-10 level < 0.35 iu Indeterminate: low mitogen (positive) control or high placebo (negative) control 9
10 INDETERMINATE IGRA RESULTS 1) Poor response to mitogen that resolves with repeat assay - Delayed specimen processing - Technical errors 2) Persistent poor response to mitogen - Anergy from immunosuppression - May occur in healthy persons 3) High background - Often persistent, reasons unclear - IGRA not useful Elispot Test Also based on ESAT-6 and CFP-10 stimulation of primed lymphocytes. Does not quantitate INFγ in supernatants of cells. Assay Quantitates the number of INFγ producing cells. Currently requires separation of cells from blood (Automated system developed). T-SPOT TB (ELISPOT) Add cells to wells coated with anti-ifn-gamma antibodies IFN-gamma binds to antibodies Each spot represents one IFN-gamma-producing cell Add second antibody and substrate, which gives color change 10
11 DIAGNOSIS OF LTBI IGRAs more specific than TST in BCG-vaccinated Relative sensitivity of TST and IGRA s unknown. IGRAs may be more sensitive than TST for recent infection, but less sensitive for remote infection Relative sensitivity in immune suppressed patients unknown (T-Spot may be most sensitive) QFT-Gold, QFT-Gold IT, T-Spot FDA Approved IFN-G-BASED BLOOD TESTS ADVANTAGES Lack of inter-individual variability in test administration. More objective read-out (? reproducibility). Requires one visit (no return visit unless test is positive). More specific and (?) equally sensitive compared with TST. Guidelines for Using the QuantiFERON-TB Gold test for detecting MTB infection, U.S. MMWR 2005; 54 (No. RR-15, 49-55) IFN-gamma Based Diagnostic Tests for TB-Future Study Iatrogenic immunosuppression (dialysis, organ transplantation, anti-tnf-alpha). Young children, HIV infected. Evaluate risk of progression to TB disease in patients with (+) IFN-gamma tests. Head to head evaluation of ELLISPOT vs. QFN- TB-Gold. Short and longterm variability Boosting after TST 11

12 IFN-gamma Based Diagnostic Tests for TB Be familiar with the cutoffs for a positive test USE ONE TEST, IGRA or TST (except under unusual circumstances): disparate results are still hard to interpret The gold standard is still elusive, but we have made some progress Rationale for Treatment of LTBI Prevent progression of infection to disease Aid in the diagnosis of TB disease Interrupt transmission of disease The next step that must be taken to move toward TB elimination in the US 12


13 Abnormal CXR and (+) TST 50 yo physician from China who entered the U.S. as a post-doctoral fellow Known abnormal CXR with negative sputum smears Asymptomatic, history of partial TB treatment in China QFT-TB Gold (+) 13
 and no radiographic change treat as LTBI Advantages: Minimizes public health risk, 2 mos of 4 drug Rx adequate for LTBI Disadvantages: Possible medication")
14 Managing patients with abnormal CXR s and (+) PPD s Option #1: Collect sputum for AFB analysis Begin multidrug tuberculosis Rx Reevaluate at 2 months: if (+) cultures or radiographic improvement treat as active case If cultures (-) and no radiographic change treat as LTBI Advantages: Minimizes public health risk, 2 mos of 4 drug Rx adequate for LTBI Disadvantages: Possible medication toxicity Managing patients with abnormal CXR s and (+) PPD s Option #2: Collect sputum for AFB analysis Reevaluate at 2 months: if (+) cultures or radiographic progression treat as active case, if (-) cultures and radiographic stability treat as LTBI Disadvantages: Unavoidably involves at least some public health risk Advantages: Avoids risk of medication toxicity 14
15 Diagnosis of Tuberculosis Symptoms Radiologic Findings Microbiologic Findings Diagnosis of Tuberculosis Clinical suspicion is the single most important factor in the timely diagnosis of tuberculosis. The greatest risk for nosocomial transmission of tuberculosis is exposure to an undiagnosed case of TB. There is no diagnostic substitute for thinking about the diagnosis. Good Outcomes Depend on Complete Evaluation and a Correct Diagnosis Medical Evaluation Signs and symptoms History of risk factors and/or exposures Physical exam Chest X-ray Bacteriology Cultures of suspected site Susceptibility testing of positive isolate Rapid diagnostic tests (HPLC, NAA) 15
16 Where Are Patients Diagnosed With TB? California, 18 counties with highest TB morbidity Hospital inpatient evaluation 45% Outpatient clinic evaluation 32% TB clinic 12% Seattle, Washington Outpatient evaluation 48% Hospital evaluation 32% TB clinic 2% Symptoms of Tuberculosis Cough Fever Nite Sweats Weight Loss Hemoptysis Chronicity is the key Guidelines for Evaluation of Pulmonary TB in Adults Any cough 2-3 wks plus at least one additional symptom: fever, night sweats, weight loss or hemoptysis Any high risk for TB; unexplained illness including respiratory symptoms 2-3 wks CXR: if suggestive of TB collect 3 sputum specimens for AFB and culture CXR: if suggestive of TB collect 3 sputum specimens for AFB and culture Controlling TB in U.S. MMWR: Nov
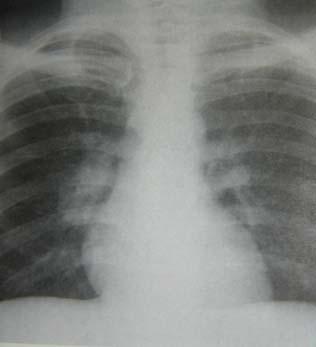
17 Guidelines for Evaluation of Pulmonary TB in Adults Any HIV infected with unexplained cough and fever Any at high risk for TB with dx CAP & not improved >7days Any at high risk for TB with incidental findings on CXR of TB even minimal/no sx CXR and collect 3 sputum for AFB smear and culture CXR and 3 sputum for AFB smear and culture Review prior CXR if available, 3 sputum for AFB smear and culture Controlling TB in U.S. MMWR: Nov 2005 Postprimary (Reactivation) TB:Radiographic Findings Primarily apical/posterior segments of the upper lobes, superior segments of lower lobes (90%) Prediliction for Reactivation TB to involve the upper lung zones Relatively higher oxygen tension in the upper lung zones Impaired lymphatic drainage in the upper lung zones Post Primary (Reactivation) TB: Radiographic findings Patchy consolidation with streaky opacities (100%) Cavitation 45% Bronchogenic spread of disease with illdefined nodules (20-25%) Fibrosis (30%) Pleural effusion (20%) 17
18 18


19 19
 TB Cavities Cavities usually multiple with thin and smooth to thick and irregular walls Air-fluid levels in cavities unusual (9-20%) Anterior segment of upper lobes or basilar segments")
20 Postprimary (Reactivation) TB Cavities Sites of cavitary disease 83%-85% apical/posterior segments upper lobes 11%-14% superior segments lower lobes Usually involves more than one segment Postprimary (Reactivation) TB Cavities Cavities usually multiple with thin and smooth to thick and irregular walls Air-fluid levels in cavities unusual (9-20%) Anterior segment of upper lobes or basilar segments of lower lobes without typical pattern of involvement-5% 20


21 Atypical Presentation of TB HIV infection, chronic renal disease, diabetes, immunosuppression may alter presentation CXR may be atypical; lower lobe infiltrate, adenopathy or completely normal Negative TST or QTF Gold Negative smear in up to 50% Atypical clinical presentation 21
22 Radiographic Assessment of Disease Activity Normal CXR: high negative predictive value, but false negatives occur 1% immunocompetent, 7%-15% HIV seropositive Lack of radiographic change over a 4 to 6 month interval generally indicates inactive disease (radiographically stable). Postprimary (Reactivation) TB CT Findings Lobular (airspace) consolidation (41%) Cavity (51%) Poorly defined nodule (endobronchial spread) (61%) Bronchial wall thickening (73%) Nodule or branching linear structure (95%) Hematogenous spread with small difuse nodules Resolution: disappearance of lobular consolidation, poorly defined nodules, and cetrilobular nodules or branching linear lesions (in that order) Primary TB: Progressive Primary TB in 5-10% the infection is poorly controlled, resulting in progressive primary tuberculosis. The most common form of pulmonary tuberculosis in infants and children % of all adult cases of tuberculosis (primarily HIV-associated) 22


23 Progressive Primary TB: Radiographic Findings Parenchymal disease: areas of greatest ventialtion-lower and middle lobes Lymphadenopathy Pleural effusion Miliary tuberculosis Obstructive atelectasis due to lymphadenopathy Normal chest radiograph Progressive Primary TB: Lymphadenopathy 83%-96% of pediatric cases Prevalence of lymphadenopathy decreases with increasing age Right paratracheal, hilar nodes most common, bilateral 15% Lymphadenopathy may result in lobar atelectasis due to bronchial compression. By CT: central areas of low attenuation with peripheral rim enhancement 23

24 24


25 Miliary TB Normal radiographic findings in the early stages, 25%-40% at initial presentation, can occur with progressive primary or reactivation disease Characterized by innumerable, 1-3mm noncalcified nodules in both lungs with mild basilar predominance 30% with associated TB findings including consolidation, cavitation, lymphadenopathy ARDS-rare 25

 Severe immunosuppression (CD4 < 200): findings c/w primary disease or")
26 TB and AIDS: Radiographic Appearance The radiographic manifestations of HIVassociated pulmonary TB are dependent on the level of immuno-suppression. Relatively intact cellular immune function (CD4 > 200): radiographic findings similar to non-hiv infected individuals (upper lobe, cavitary disease) Severe immunosuppression (CD4 < 200): findings c/w primary disease or normal chest radiographs or dissemination with miliary pattern or extrapulmonary disease 26


27 TB and AIDS: Radiographic Appearance The presence of intrathoracic adenopathy in a patient with AIDS and poor immune function (very low CD4 count), without an explanation, should be considered TB until proven otherwise. 27
28 Role of CT in the Diagnosis of TB CT is not the primary radiologic diagnostic test for TB (CT is overused) Usually don t need CT for cavitary consolidation If TB is a possible diagnosis, sputum for AFB should be obtained prior to CT In most instances, CT should be reserved for patients in whom the diagnosis is unclear Role of CT in the Diagnosis of TB Reveals occult lung disease in patients with pleural effusion, pericarditis, etc. Reveals intrathoracic lymphadenopathy (children, HIV co-infected) Can suggest miliary disease Reveals alternative diagnoses (lung cancer) Diagnosis of Tuberculosis: Microbiology AFB Smears AFB Cultures Rapid Diagnostic Techniques: HPLC, Nucleic Acid Amplification Studies 28
29 Diagnosis of TB AFB Smears Most rapid diagnostic test Need 10³ organisms/ml sputum for (+) Sensitivity and Specificity poor (+) in only about 70% of active TB cases (+) in patients with non-tuberculous mycobacterial disease Necessary for determining contagiousness Diagnosis of TB: AFB Cultures Remains the gold standard for diagnosis Processing kills up to 90% of AFB More sensitive than smear (10¹ organisms/ml) Liquid media culture the standard technique (+) in > 90% of patients with cavitary disease, < 70% of patients with non-cavitary disease. Necessary for in-vitro susceptibility testing Lengthy: 1-3 weeks for liquid media (2-6 solid) Diagnosis of TB: AFB Cultures More sensitive than smear (10¹ organisms/ml sputum) Required for drug susceptibilities Requires a quality specimen Processing kills up to 90% of AFB Positive for only ~ 80% active disease Lengthy: 1-3 weeks for liquid media 2-6 weeks by solid media 29
30 Culture Negative (-) TB 10-15% of pulmonary cases Re-evaluation of patient after 2 months of treatment Repeat CXR (or CT chest if done) Clinical status Sputum cultures If there is any clinical OR radiographic improvement while on treatment during the first 2 months = tuberculosis clinically diagnosed and continue treatment for active disease 6 mo of 4 drugs OR 2 mo INH/RFP/PZA/EMB + 2 mo INH/RFP Diagnosis of Tuberculosis: Rapid Diagnostic Techniques High Performance Liquid Chromatography (HPLC) : State of Texas Mycobacteriology Laboratory-routinely done for AFB smear (+) sputum specimens (> 90% sensitivity and specificity if smear (+)) Rapid Diagnositic Techniques: Nucleic Acid Amplification (NAA) Tests Mycobacterium tuberculosis Direct Test (E-MTD, Gen-Probe) Approved for AFB smear (+) and (-) >95% sensitivity smear (+), 75-90% smear (-) Amplicor Mycobacterium tuberculosis test > 95% sensitivity smear (+), 60-70% smear (-) >95% specificity for both tests Neither approved for non-respiratory specimens 30
31 Nucleic Acid Amplification (NAA) Tests NAAT should be performed on at least one respiratory speciemen from each patient with signs and symptoms of pulmonary TB for whom a diagnosis of TB is being considered but has not yet been established, and for whom the test result would alter case management or TB control activities MMWR, January 2009, 58:7-10 Increasing Complexity of TB Control Efforts Foreign born Drug Resistant TB recipients of TNF alpha blockers TB in transplants TB in dialysis and chronic renal failure HIV TB MDR TB/XDR TB Decreasing clinical experience Loss of traditional experienced workers Providers may see only one case in a lifetime of practice TB care is more specialized When to Ask for Consultation HIV TB Renal Disease Drug resistance Slow to convert Treatment relapse Treatment failure Toxicity Management of treatment interruptions When you have a question you need answered 31
: 1-800-428-7432 Heartland National Tuberculosis Center: 1-800-TEX-LUNG")
32 Tuberculosis Consultation Center for Pulmonary and Infectious Disease Control (CPIDC): Heartland National Tuberculosis Center: TEX-LUNG 32
TB Intensive Tyler, Texas December 2-4, 2008
 TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Diagnosis and Medical Management of LTBI
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Diagnosis and Medical Management of LTBI Barbara Seaworth, MD December 8, 2009 CLINICAL DIAGNOSIS AND MANAGEMENT OF LATENT TB INFECTION Barbara
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Diagnosis and Medical Management of LTBI Barbara Seaworth, MD December 8, 2009 CLINICAL DIAGNOSIS AND MANAGEMENT OF LATENT TB INFECTION Barbara
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014
 TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Screening for Tuberculosis Infection. Harlingen, TX. Linda Dooley, MD has the following disclosures to make:
 TB Infection Diagnosis Recommendations Talk Developed by Lisa Y. Armitige, MD, PhD Medical Consultant, Heartland National TB Center Associate Professor Internal Medicine/Pediatrics/Infectious Disease UT
TB Infection Diagnosis Recommendations Talk Developed by Lisa Y. Armitige, MD, PhD Medical Consultant, Heartland National TB Center Associate Professor Internal Medicine/Pediatrics/Infectious Disease UT
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Using Interferon Gamma Release Assays for Diagnosis of TB Infection
 Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
Learning Objectives Using Interferon Gamma Release Assays for Diagnosis of TB Infection 1. Describe available Interferon Gamma Release Assay tests for TB infection and how they work. 2. Understand interpretation
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
Diagnosis and Medical Case Management of Latent TB. Bryan Rock, MD April 27, 2010
 TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis and Medical Case Management of Latent TB Infection Bryan Rock, MD April 27, 2010 DIAGNOSIS AND MANAGEMENT OF LATENT TUBERCULOSIS
TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis and Medical Case Management of Latent TB Infection Bryan Rock, MD April 27, 2010 DIAGNOSIS AND MANAGEMENT OF LATENT TUBERCULOSIS
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
LTBI: Who to Test & When to Treat
 LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Conflict of Interest Disclosures:
 Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
Mady Slater, M.D. Stanford University Medical Center Division of Infectious Diseases 04/23/14 WOEMA webinar Conflict of Interest Disclosures: I have no financial relationships with commercial entities
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Technical Bulletin No. 172
 CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
CPAL Central Pennsylvania Alliance Laboratory QuantiFERON -TB Gold Plus Assay Contact: J Matthew Groeller, MPA(HCM), MT(ASCP), 717-851-4516 Operations Manager, Clinical Pathology, CPAL Jennifer Thebo,
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director, SF and North Coast AETC March 13, 2014 ACCREDITATION STATEMENT:
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
Self-Study Modules on Tuberculosis Targe te d Te s ting and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 TB Epidemiology Robert Petrossian July 18, 2012 Robert Petrossian has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 TB Epidemiology Robert Petrossian July 18, 2012 Robert Petrossian has the following disclosures to make: No conflict of interests No relevant
Latent TB Infection (LTBI)
") Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Core Curriculum on Tuberculosis: What the Clinician Should Know
 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
These recommendations will remain in effect until the national shortage of PPD solution has abated.
 Maryland Recommendations Regarding the National Shortage of Purified Protein Derivative (PPD) Solution; Attachment to Health Officer Memorandum National Shortages of Tubersol and Aplisol for TB Skin Testing;
Maryland Recommendations Regarding the National Shortage of Purified Protein Derivative (PPD) Solution; Attachment to Health Officer Memorandum National Shortages of Tubersol and Aplisol for TB Skin Testing;
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines
 Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Interferon Gamma Release Assay Testing for Latent Tuberculosis Infection: Physician Guidelines Historically, Latent Tuberculosis Infection (LTBI) diagnosis was based on risk assessment, chest x-ray (CXR)
Peggy Leslie-Smith, RN
 Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
Peggy Leslie-Smith, RN EMPLOYEE HEALTH DIRECTOR - AVERA TRAINING CONTENT 1. South Dakota Regulations 2. Iowa Regulations 3. Minnesota Regulations 4. Interferon Gamma Release Assay (IGRA)Testing 1 SOUTH
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Didactic Series. Latent TB Infection in HIV Infection
 Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Didactic Series Latent TB Infection in HIV Infection Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director SF, North Coast and East Bay AETC January 8, 2015 ACCREDITATION
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Contact Investigation
 Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Dr Francis Ogaro MTRH ELDORET
 Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining
 Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
TB Nurse Case Management San Antonio, Texas March 7 9, Clinical Diagnosis and
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Clinical Diagnosis and Management of LTBI Lynn Horvath, MD March 7, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Clinical Diagnosis and Management of LTBI Lynn Horvath, MD March 7, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict
TUBERCULOSIS CONTACT INVESTIGATION
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Essential Mycobacteriology Laboratory Services in the Era of MDR- and XDR-TB: A TB Controller s Perspective
 Essential Mycobacteriology Laboratory Services in the Era of MDR- and XDR-TB: A TB Controller s Perspective James Watt, MD, MPH Acting Chief, Tuberculosis Control Branch California Department of Public
Essential Mycobacteriology Laboratory Services in the Era of MDR- and XDR-TB: A TB Controller s Perspective James Watt, MD, MPH Acting Chief, Tuberculosis Control Branch California Department of Public
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Latent TB Infection (LTBI) Strategies for Detection and Management
 Strategies for Detection and Management") Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal
 Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Contact Investigation in the Correctional Setting Jessica Quintero, BAAS March 24, 2011 Jessica Quintero, BAAS has the following disclosures to make: No
TB in Corrections Phoenix, Arizona March 24, 2011 Contact Investigation in the Correctional Setting Jessica Quintero, BAAS March 24, 2011 Jessica Quintero, BAAS has the following disclosures to make: No
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis Pathogenesis and Treatment f Latent TB Infection Lynn Horvath, MD October 15, 2013 Lynn Horvath, MD has the following disclosures to make: No
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis Pathogenesis and Treatment f Latent TB Infection Lynn Horvath, MD October 15, 2013 Lynn Horvath, MD has the following disclosures to make: No
Interpretation of TST & IGRA results. Objectives
 Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Preventing Tuberculosis (TB) Transmission in Ambulatory Surgery Centers. Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program
 Transmission in Ambulatory Surgery Centers. Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program") Preventing Tuberculosis (TB) Transmission in Ambulatory Surgery Centers Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program Topics of Discussion TB Overview Epidemiology of TB in Oregon Annual Facility
Preventing Tuberculosis (TB) Transmission in Ambulatory Surgery Centers Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program Topics of Discussion TB Overview Epidemiology of TB in Oregon Annual Facility
The Origin of Swine Flu
 How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Yakima Health District BULLETIN
 Yakima Health District BULLETIN Summary Volume 13, Issue 1 February, 2014 Tuberculosis in Yakima County The rate of active tuberculosis (TB) in Yakima County has declined by about two-thirds over the past
Yakima Health District BULLETIN Summary Volume 13, Issue 1 February, 2014 Tuberculosis in Yakima County The rate of active tuberculosis (TB) in Yakima County has declined by about two-thirds over the past
Testing for TB. Bart Van Berckelaer Territory Manager Benelux. Subtitle
 Testing for TB Bart Van Berckelaer Territory Manager Benelux Subtitle Agenda TB infection pathway TB immunisation Testing options Pre lab considerations of the whole blood ELISA test The T-SPOT.TB test
Testing for TB Bart Van Berckelaer Territory Manager Benelux Subtitle Agenda TB infection pathway TB immunisation Testing options Pre lab considerations of the whole blood ELISA test The T-SPOT.TB test
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Annual Tuberculosis Report Oregon 2007
 Annual Tuberculosis Report Oregon 7 Oregon Department of Human Services Public Health Division TB Program April 8 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-7.. page
Annual Tuberculosis Report Oregon 7 Oregon Department of Human Services Public Health Division TB Program April 8 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-7.. page
Appendix B. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case