Anaphylaxis. By Eric Schultz, DO, MPH Assistant Clinical Professor Texas A&M Health Sciences Greater Austin Allergy Asthma and Immunology
|
|
|
- Buddy Boone
- 6 years ago
- Views:
Transcription
1 Anaphylaxis By Eric Schultz, DO, MPH Assistant Clinical Professor Texas A&M Health Sciences Greater Austin Allergy Asthma and Immunology
2 Clinical vignette Anaphylaxis 46 yo male from India eating at a Chinese restaurant with his family, on no meds, avoids seafood (fish allergy) Felt itchy and flushed after a bite of beef SOB within minutes, severe 911 called, patient collapse within 15 min 5 attempts at intubation: laryngeal edema Epi given, dead upon arrival ED (45 min)
3
4 Clinical Vignette Anaphylaxis What could have been done better? Could the death have been prevented? Are there risk factors for fatal anaphylaxis? How can the diagnosis be made?
5 Objectives Define anaphylaxis Identify the various types of anaphylaxis Review epidemiology Evaluate differential diagnosis Provide clinical/laboratory diagnosis Review treatment
6 Definition of anaphylaxis Anaphylaxis is a severe, life-threatening, generalized or systemic hypersensitivity reaction. It is commonly, but not always, mediated by an allergic mechanism, usually by IgE. Allergic (immunologic) non-ige-mediated anaphylaxis also occurs. Non-allergic anaphylactic reactions, formerly called anaphylactoid or pseudo-allergic reactions, may also occur. Johansson SGO et al JACI 2004,113:832-6
7 Gell and Coombs classification of hypersensitivity Type I Type II Type III Type IV Immediate hypersensitivity Cytotoxic reactions Immune complex reactions Delayed hypersensitivity Anaphylaxis can occur through Types I, II and III immunopathologic mechanisms Kemp SF and Lockey RF. J Allergy Clin Immunol 2002;110:341-8
8 Acutely released mediators of anaphylaxis Degranulation of mast cells and basophils causes the release of: - preformed granule-associated substances (eg: histamine, tryptase, chymase, carboxypeptidase, and cytokines) - newly-generated lipid-derived mediators (eg: prostaglandin D 2, leukotriene (LT) B 4, LTC 4, LTD 4, LTE 4, and platelet activating factor) Kemp SF and Lockey RF. J Allergy Clin Immunol 2002; 110:341-8
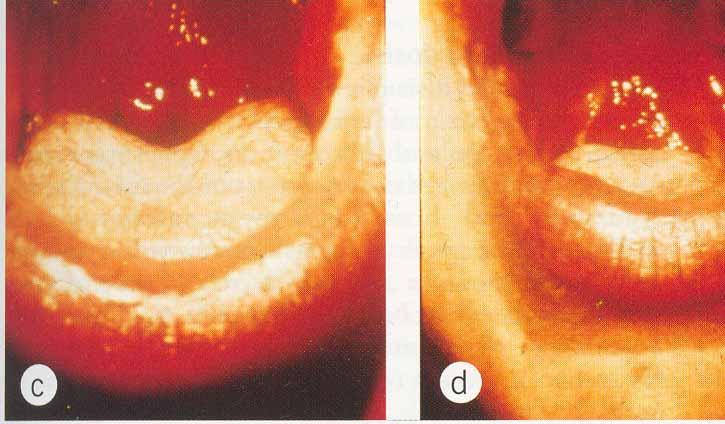
9 Primary symptoms of anaphylaxis Skin: flushing, itching, urticaria, angioedema Gastrointestinal: Respiratory: dysphonia, cough, stridor, wheezing, dyspnea, chest tightness, asphyxiation, death nausea, vomiting, bloating, cramping, diarrhea Cardiovascular: tachycardia, hypotension, dizziness, collapse, death Other: feeling of impending doom, metallic taste
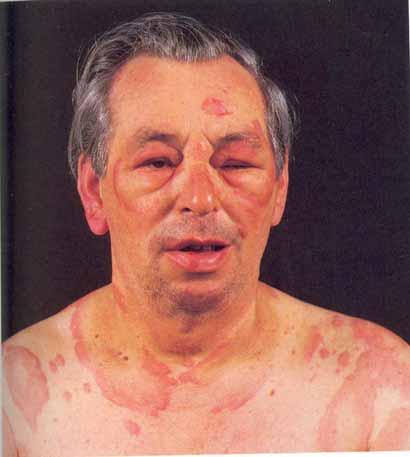
10 Urticaria/Angioedema

11 Laryngeal Edema
12 Comments about anaphylaxis signs and symptoms skin symptoms occur most commonly ( > 90% of patients) skin, oral, and throat symptoms are often the first ones noted respiratory symptoms occur in 40% to 70% of patients gastrointestinal symptoms occur in about 30% of patients shock occurs in about 10% of patients signs and symptoms are usually seen within 5 to 30 minutes the more rapid the onset, the more serious the reaction Lieberman P. In: Middleton s Allergy: Principles and Practice, 6th edition, Mosby Inc., St. Louis, MO, 2003
13 Biphasic and protracted anaphylaxis biphasic anaphylaxis is defined as return of symptoms after resolution of initial symptoms, without subsequent allergen exposure usually, symptoms return within 1 to 8 hours (sometimes longer) up to 20% of anaphylactic reactions are biphasic patients with biphasic anaphylaxis may require more epinephrine to control initial symptoms in protracted anaphylaxis, symptoms may be continuous for 5-32 hrs Lieberman P. Ann Allergy Asthma Immunol 2005;95:217-26
14 Biphasic/late-phase reaction Cellular infiltrates: 3 to 6 hours (LPR) Histamine IL-4, IL-6 Eosinophil CysLTs, GM-CSF, TNF-, IL-1, IL-3, PAF, ECP, MBP Allergen PGs Proteases CysLTs 3 to 6 hours (CysLTs, PAF, IL-5) Basophil Monocyte Histamine, CysLTs, TNF-, IL-4, IL-5, IL-6 CysLTs, TNF-, PAF, IL-1 Return of Symptoms Mast cell EPR 15 min (Early-Phase Reaction) Lymphocyte IL-4, IL-13, IL-5, IL-3, GM-CSF
15 Bi-phasic Reaction Bi-phasic reactions noted in one-third of patients with (food induced) fatal or near fatal reactions Patients seem to have fully recovered when severe bronchospasm suddenly recurs Recurrence is typically more refractory to standard therapy and often requires intubation and mechanical ventilation Sampson HA. N Engl J Med. 2002;346:
16 Incidence and prevalence of anaphylaxis anaphylaxis in the US: an investigation into its epidemiology" - on the basis of a literature review, more than 1.21% of the population may be affected independent US Omnibus Studies (2002 and 2003) - 32 million have had 2 or more symptoms - 18 million diagnosed - 11 million have suffered a life-threatening reaction Neugut AI et al. Arch Intern Med 2001;161:15-21 Dey, L.P. Independent omnibus studies. Data on file
17 Incidence and prevalence of anaphylaxis (cont.) 5-year review of 1.15 million persons in Manitoba, Canada dispensing patterns of epinephrine for out-of-hospital treatment 0.95% of the general population had epinephrine dispensed dispensing rates in the general population varied with age: % for individuals <17 years of age - 0.9% for those years of age % for those >65 years of age interpretation: anaphylaxis from all triggers, occurring out of hospital, appears to peak in childhood, and then gradually decline Simons FER et al. J Allergy Clin Immunol 2002;110:647-51
18 Risk Factors for Anaphylaxis Asthma (Sampson H, NEJM, 1992) Prior Severe reactions Atopy (food, hymenoptera) Occupational (latex) Systemic mastocytosis Once Sensitized Atopic (Asthma) higher risk for fatal anaphylaxis (Lockley et al, JACI, 1987)
19 Effect of Gender on Incidence of Anaphylaxis Number of Patients Females Males Age Ranges Webb, et al. J Allergy Clin Immunol. 2004;113:s241.
20 Causes of Anaphylaxis Adults Other Medications Foods Idiopathic 70% Webb, et al. J Allergy Clin Immunol. 2004;113:241. E
21 Children May Be Different 46 children Median age first episode 5.8 years Males > Females Only small proportion idiopathic Atopic derm, urticaria/angiodema, sensitivity predictive of recurrence Number of Children Recurrence Cianferoni A, et al. Annals of Allergy, Asthma, & Immunology. 2004;92:
22 International collaborative study of Objective severe anaphylaxis To quantify the risk of anaphylaxis due to drugs and other exposures in hospital patients Methods Hospitals in Sweden, Hungary, India and Spain Incident cases Clinical diagnosis using a priori agreed criteria, independent of presumed trigger Epidemiology 1998;9:141-46
23 International collaborative study of severe anaphylaxis (cont.) Main findings 123/481,752 i.e. risk of 15-20/100,000 admissions 33% males Median age ~53 79% respiratory symptoms; 70% cardiovascular symptoms; 49% both Death in 2% of cases Epidemiology 1998;9:141-46
24 UK anaphylaxis death registery Objective To understand the circumstances leading to fatal anaphylaxis Methods Running since 1992; ONS mortality data coded for anaphylaxis since 1993 Detailed information obtained from medical records, medical staff, coroners officers and mast cell serum tryptase Pumphrey RSH, Clin Exp Aller 2000; J Clin Pathol 2000; Novartis Found Symp 2004
25 UK anaphylaxis death registery (cont.) Main findings ~20 recorded deaths/year i.e. ~1:2.8 million 50% iatrogenic; 25% food and 25% venom ~50% died from asphyxia (food) and 50% from shock (iatrogenic and venom) Median time to death: 5 mins if iatrogenic; 15 mins venom; and 30 mins food Adrenaline rarely used before cardiac arrest Pumphrey RSH, Clin Exp Aller 2000; J Clin Pathol 2000; Novartis Found Symp 2004
26 Agents that cause anaphylaxis: IgE-dependent triggers foods (eg: peanut, tree nuts, seafood) medications (eg: β-lactam antibiotics) venoms latex allergen immunotherapy diagnostic allergens exercise (with food or medication co-trigger) hormones animal or human proteins colorants (insect-derived, eg: carmine) enzymes polysaccharides aspirin and NSAIDs (possibly through IgE) Kemp SF and Lockey RF, J Allergy Clin Immunol 2002;110:341-8
27 Risk of anaphylaxis estimated risk in US: 1-3% fatalities per year in the US: - food-induced: antibiotic-induced: venom-induced: 50 Kemp SF and Lockey RF, J Allergy Clin Immunol 2002;110:341-8
28 Food-induced anaphylaxis many anaphylactic reactions are caused by food - accidental food exposures are common and unpredictable - anaphylaxis from food can occur at any age, but children, teens and young adults are at highest risk prevalence of peanut allergy has doubled in children <5 years of age in the last 5 years seafood allergy is reported by 2.3% of the US population, and is more common in adults than in children Sampson HA. J Allergy Clin Immunol 2004;113: Sicherer SH et al. J Allergy Clin Immunol 2004;114:159-65



29 Most common food allergies peanut tree nut shellfish fin fish milk egg soy wheat

30 Fatal food-induced anaphylaxis in a retrospective analysis of 32 deaths in patients age 2-33 years - peanut and tree nuts caused >90% of reactions - most patients had a history of asthma - most did not have injectable epinephrine available at the time of their reaction and death Bock SA et al. J Allergy Clin Immunol 2001;107:191-3
31 Latex Allergy Risk Groups Health Care Workers (5-10%) Rubber Industry Workers Spina Bifida (18-28%) Urogenital Abnormalities
32 Latex-Induced Anaphylaxis: Common Triggers Proteins in natural rubber latex Component of ~40,000 commonly used items Rubber bands Elastic (eg, undergarments) Hospital and dental equipment Latex-dipped products are biggest culprits Balloons, gloves, bandages, hot water bottles Patients undergoing surgery especially vulnerable Latex is common in medical supplies: disposable gloves, airway and intravenous tubing, syringes, stethoscopes, catheters, dressings, bandages ACAAI Web site. Available at: Accessed November 9, 2004.
33 Latex Allergy Diagnosis Risk Group Latex Associated Reactions Cross-reactive foods: avocado, mango, chestnut, banana, kiwi Testing 1. RAST (38-82%) 2. Skin Test (100%)
34 Anaphylaxis: Idiopathic 1. Recurrent, often severe 2. No Identifiable Precipitant 3. 50% Atopic 4. Refractory to Therapy
35 Idiopathic Anaphylaxis 37 Patients ( ) Age (mean 48) 43% Atopic Frequency: > 5/Year 31% Follow-up: 2.5 year (mean) 21 Patients (60%) resolved 9 Decreased Frequency 2 Increased Frequency 3 Same 3 Frequent Episodes 2 Chronic Glucocorticoids Khan & Yocum, Annals Allergy 1994; 73:371
36 Exercise-Induced Anaphylaxis: Flushing, pruritus, wheezing, syncope Running, jogging, dancing, skating Food ingestion 4 hours prior >50% cases (wheat 60% cases) Recommendations: Discontinue Exercise if notice earliest Symptom, Limit Exercise on Hot, Humid Days, Avoid Exercise 4-6 hrs Post Prandial, Avoid Exercise Post Allergy Immunotherapy, Avoid Beta-Blockers and ACE Inhibitors Medi-Alert Bracelet Shadick et al JACI 1999
37

38


39 Venom-Induced Anaphylaxis: Incidence 0.5% to 5% or 1.36 million to 13 million Americans are sensitive to 1 or more insect venoms Hymenoptera order of insects Bees Wasps Yellow jackets Hornets Fire ants At least 40 to 100 deaths per year Incidence increasing due to Rise in the number of fire ants and Africanized bees Increase in people engaging in outdoor activities Immunotherapy 98-99% effective to prevent reactions Neugut AI, Ghatak AT, Miller RL. Arch Intern Med. 2001;161:15-21.
40 Hymenoptera Sting Natural History: 60% Re-sting reaction rate The more severe the initial anaphylactic symptoms, the more likely there will be a resting reaction The severity of the sting reaction is not related to the degree of skin test sensitivity or titer of serum venom-specific IgE
41 Risk of Systemic Reaction to Sting for VIT-Treated and Untreated Patients Golden, et al. JACI 2000
42 Frequency of Systemic Reactions to Stings after Discontinuing VIT Golden, et al. JACI 2000

43 Allergen immunotherapy-induced anaphylaxis fatal reactions are uncommon: 1 per 62,000,000 injections risk factors for fatality include: - dosing errors - poorly controlled asthma (FEV 1 < 70%) - concomitant β-blocker use - lack of proper equipment and trained personnel - inadequate epinephrine treatment Stewart GE and Lockey RF. J Allergy Clin Immunol 1992;90: Bernstein DI et al, J Allergy Clin Immumol 2004;113:
44 estimated 550,000 serious allergic reactions to drugs/year in US hospitals Iatrogenic anaphylaxis most common drug triggers - penicillin (highest number of documented deaths from anaphylaxis) - sulfa drugs - non-steroidal anti-inflammatory drugs - muscle relaxants most common biologic triggers - anti-sera for snakebite - anti-lymphocyte globulin - vaccines - allergens Neugut AI et al. Arch Intern Med 2001;161:15-21 Lazarou J et al. JAMA 1998;279:1200-5
45 Anaphylaxis: non-immunologic causes MULTIMEDIATOR COMPLEMENT ACTIVATION/ACTIVATION OF CONTACT SYSTEM radiocontrast media ethylene oxide gas on dialysis tubing (possibly through IgE) protamine (possibly) ACE-inhibitor administered during renal dialysis with sulfonated polyacrylonitrile, cuprophane, or polymethylmethacrylate dialysis membranes Kemp SF and Lockey RF, J Allergy Clin Immunol 2002;110:341-8
46 Anaphylaxis: non-immunologic causes NONSPECIFIC DEGRANULATION OF MAST CELLS AND BASOPHILS opiates physical factors: - exercise (no food or medication co-trigger) - temperature (cold, heat) Kemp SF and Lockey RF, J Allergy Clin Immunol 2002;110:341-8
47 Differential Diagnosis of Anaphylaxis Condition Clinical Differentiation from Anaphylaxis Scombroid Syndrome History of Antecedent Ingestion of Suspect Fish Oral Burning, Tingling, Blistering, or Peppery Taste after Ingestion Emesis Common Episode May Last Days (Though More Commonly Hours)
48 Differential Diagnosis of Anaphylaxis Condition Vasovagal Syndrome Globus Hystericus Clinical Differentiation from Anaphylaxis Bradycardia, not tachycardia Pallor rather than Flushing No Pruritus, Urticaria, Angioedema, Upper Respiratory Obstruction, or Bronchospasm Nausea, but no abdominal pain No Clinical or Radiological Evidence of Upper Respiratory Obstruction No Flushing, Pruritis, Urticaria, Bronchospasm, Abdominal Pain or Hypotension
49 Differential Diagnosis of Anaphylaxis Condition Mastocytosis Carcinoid Syndrome Clinical Differentiation from Anaphylaxis No Upper Respiratory Obstruction, Bronchospasm Uncommon Urticaria Pigmentosa Often Present Slower Onset of Attacks; Chronic Low-Grade Symptomatology between Attacks No Upper Respiratory Obstruction, Urticaria, or Angioedema Slower Onset of Attacks May have Cutaneous Stigmata, Including Telangiectases on trunk
50 Diagnosing anaphylaxis Allergists can identify specific causes by: complete and accurate medical/allergy history skin tests/specific IgE levels - foods - insect venoms - drugs (some) challenge tests: (selected patients, physician-monitored, preferably in hospital) - foods - NSAIDs - exercise Simons FER. J Allergy Clin Immunol 2006;117:367-77
51 Anaphylaxis: Diagnosis 1. Histamine Levels Increased A. Plasma B. 24 Hour Urine 2. Tryptase, carboxypeptidase A 3. Complement Activation 4. Antigen-Specific IgE A. RAST B. Skin Testing
52 Laboratory tests in the diagnosis of anaphylaxis Plasma histamine Serum tryptase 24-hr Urinary histamine metabolite Minutes
53 Problems with laboratory tests histamine and tryptase levels may not correlate with each other histamine level was elevated in 42 of 97 patients in the Emergency Department, but only 20 of 97 had an elevated tryptase level histamine levels correlated better with symptoms and signs plasma histamine levels only remain elevated for one hour after symptom onset; therefore, this test is usually not practical Lin RY et al. J Allergy Clin Immunol 2000;106:65-71


54 Tryptase Levels in Anaphylaxis and Systemic Mastocytosis Schwartz, NEJM1987
55 Anaphylaxis in the emergency department chart review study in 21 North American Emergency Departments random sample of 678 charts of patients presenting with food allergy management: - 72% received antihistamines - 48% received systemic corticosteroids - 16% received epinephrine (24% of those with severe reactions) - 33% received respiratory medication (eg. inhaled albuterol) - only 16% received Rx for self-injectable epinephrine at discharge - only 12% referred to an allergist Clark S et al. J Allergy Clin Immunol 2004;347-52
56 Acute Management of Anaphylaxis Castells al et Allergy 2005 ACLS guideline 2005 AAAAI Practice parameters Administer ml 1/1000 epinephrine IM while patient is recumbent no supine or sitting position (empty heart) repeat X 2 at 5 to 10 min intervals if SBP < Anti-histamines, steroids, bronchodilators 3. If β blockade is present use glucagon 5-15 μ/min i.v. continuous infusion 4. Observation for a minimum of 4-5 hours 5. At discharge, educate patient to avoid future episodes 6. Assess whether patient needs EpiPen prescription 7. Assess whether patient needs Allergy referral

57 Use of Anti-IgE Antibody to Reduce Responsivenes to Allergens: Xolair Metzger. NEJM 2003
58 Clinical Vignette Anaphylaxis What could have done better? Repeated epi and trachestomy Could the death be prevented? Diagnosis and education What were the risk factors for fatal anaphylaxis? Asthma and a prior severe reaction How can the diagnosis be made? Tryptase, carboxypeptidase A (2006), ST/CAP
59 State Statutes Protecting Students Rights to Carry and Use Asthma and Anaphylaxis Medications

60 Questions?
Myth: Prior Episodes Predict Future Reactions REALITY: No predictable pattern Severity depends on: Sensitivity of the individual Dose of the allergen
 Myth: Prior Episodes Predict Future Reactions REALITY: No predictable pattern Severity depends on: Sensitivity of the individual Dose of the allergen Anaphylaxis Fatalities Estimated 500 1000 deaths annually
Myth: Prior Episodes Predict Future Reactions REALITY: No predictable pattern Severity depends on: Sensitivity of the individual Dose of the allergen Anaphylaxis Fatalities Estimated 500 1000 deaths annually
EPIPEN INSERVICE Emergency Administration of Epinephrine for the Basic EMT. Michael J. Calice MD, FACEP St. Mary Mercy Hospital
 EPIPEN INSERVICE Emergency Administration of Epinephrine for the Basic EMT Michael J. Calice MD, FACEP St. Mary Mercy Hospital Case #1 NR is an 8 yo male c/o hot mouth and stomach ache after eating jelly
EPIPEN INSERVICE Emergency Administration of Epinephrine for the Basic EMT Michael J. Calice MD, FACEP St. Mary Mercy Hospital Case #1 NR is an 8 yo male c/o hot mouth and stomach ache after eating jelly
Recognition & Management of Anaphylaxis in the Community. S. Shahzad Mustafa, MD, FAAAAI
 Recognition & Management of Anaphylaxis in the Community S. Shahzad Mustafa, MD, FAAAAI Disclosures None Outline Define anaphylaxis Pathophysiology Common causes Recognition and Management Definition Acute,
Recognition & Management of Anaphylaxis in the Community S. Shahzad Mustafa, MD, FAAAAI Disclosures None Outline Define anaphylaxis Pathophysiology Common causes Recognition and Management Definition Acute,
Case Report. Mechanisms of Anaphylaxis. Case Report. Case Report 37 y/o WF Is this anaphylaxis? What would you do at this point?
 Mechanisms of Anaphylaxis Richard F. Lockey, M.D. Division of Allergy and Immunology Department of Internal Medicine University of South Florida Morsani College of Medicine and James A. Haley Veterans
Mechanisms of Anaphylaxis Richard F. Lockey, M.D. Division of Allergy and Immunology Department of Internal Medicine University of South Florida Morsani College of Medicine and James A. Haley Veterans
Allergic Emergencies and Anaphylaxis. George Porfiris MD, CCFP(EM),FCFP TEGH
,FCFP TEGH") Allergic Emergencies and Anaphylaxis George Porfiris MD, CCFP(EM),FCFP TEGH Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Allergic Emergencies and Anaphylaxis George Porfiris MD, CCFP(EM),FCFP TEGH Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Terms What is Anaphylaxis? Causes Signs & Symptoms Management Education Pictures Citations. Anaphylaxis; LBodak
 Leslie Bodak, EMT-P Terms What is Anaphylaxis? Causes Signs & Symptoms Management Education Pictures Citations Allergic Reaction: an abnormal immune response the body develops when a person has been previously
Leslie Bodak, EMT-P Terms What is Anaphylaxis? Causes Signs & Symptoms Management Education Pictures Citations Allergic Reaction: an abnormal immune response the body develops when a person has been previously
7/25/2016. Use of Epinephrine in the Community. Knowledge Amongst Paramedics. Knowledge Amongst Paramedics survey of 3479 paramedics
 Recognition & Management of Anaphylaxis in the Community S. Shahzad Mustafa, MD, FAAAAI Disclosures Speaker s bureau Genentech, Teva Consultant Genentech, Teva Outline Knowledge gap Definition Pathophysiology
Recognition & Management of Anaphylaxis in the Community S. Shahzad Mustafa, MD, FAAAAI Disclosures Speaker s bureau Genentech, Teva Consultant Genentech, Teva Outline Knowledge gap Definition Pathophysiology
Urticaria Moderate Allergic Reaction Mild signs/symptoms with any of following: Dyspnea, possibly with wheezes Angioneurotic edema Systemic, not local
 Allergic Reactions & Anaphylaxis Incidence In USA - 400 to 800 deaths/year Parenterally administered penicillin accounts for 100 to 500 deaths per year Hymenoptera stings account for 40 to 100 deaths per
Allergic Reactions & Anaphylaxis Incidence In USA - 400 to 800 deaths/year Parenterally administered penicillin accounts for 100 to 500 deaths per year Hymenoptera stings account for 40 to 100 deaths per
Five things to know about anaphylaxis
 Five things to know about anaphylaxis Magdalena Berger, MD FRCPC Allergist and Clinical Immunologist New Brunswick Internal Medicine Update April 22, 2016 Disclosures None relevant to this presentation
Five things to know about anaphylaxis Magdalena Berger, MD FRCPC Allergist and Clinical Immunologist New Brunswick Internal Medicine Update April 22, 2016 Disclosures None relevant to this presentation
Course Objectives: Upon completion of this presentation, the attendee will be able to:
 Course Objectives: Upon completion of this presentation, the attendee will be able to: Kevin Letz DNP, MBA, MSN, RN, CNE, CEN, FNP-C, PNP-BC, ANP-BC, FAPPex, FAANP 1. Identify the newest diagnostic criteria
Course Objectives: Upon completion of this presentation, the attendee will be able to: Kevin Letz DNP, MBA, MSN, RN, CNE, CEN, FNP-C, PNP-BC, ANP-BC, FAPPex, FAANP 1. Identify the newest diagnostic criteria
ANAPHYLAXIS EMET 2015
 ANAPHYLAXIS EMET 2015 ANA = AGAINST PHYLAX = PROTECTION No standardised definition (they re working on it) All include the similar concept of: A serious, generalised or systemic, allergic or hypersensitivity
ANAPHYLAXIS EMET 2015 ANA = AGAINST PHYLAX = PROTECTION No standardised definition (they re working on it) All include the similar concept of: A serious, generalised or systemic, allergic or hypersensitivity
Kevin Letz DNP, MBA, MSN, RN, CNE, CEN, FNP-C, PNP-BC, ANP-BC, FAPPex, FAANP. Course Objectives:
 Kevin Letz DNP, MBA, MSN, RN, CNE, CEN, FNP-C, PNP-BC, ANP-BC, FAPPex, FAANP Course Objectives: Upon completion of this presentation, the attendee will be able to: 1. Identify the newest diagnostic criteria
Kevin Letz DNP, MBA, MSN, RN, CNE, CEN, FNP-C, PNP-BC, ANP-BC, FAPPex, FAANP Course Objectives: Upon completion of this presentation, the attendee will be able to: 1. Identify the newest diagnostic criteria
Anaphylaxis in the Community
 Anaphylaxis in the Community ACES101210 Copyright 2010, AANMA www.aanma.org ACES2015 ACES101210 Copyright Copyright 2015 2010, Allergy AANMA & Asthma www.aanma.org Network AllergyAsthmaN Anaphylaxis Community
Anaphylaxis in the Community ACES101210 Copyright 2010, AANMA www.aanma.org ACES2015 ACES101210 Copyright Copyright 2015 2010, Allergy AANMA & Asthma www.aanma.org Network AllergyAsthmaN Anaphylaxis Community
Policy for the Treatment of Anaphylaxis in Adults and Children
 Policy for the Treatment of Anaphylaxis in Adults and Children June 2008 Policy Title: Policy for the Treatment of Anaphylaxis in Adults or Children Policy Reference Number: PrimCare08/17 Implementation
Policy for the Treatment of Anaphylaxis in Adults and Children June 2008 Policy Title: Policy for the Treatment of Anaphylaxis in Adults or Children Policy Reference Number: PrimCare08/17 Implementation
UCSF High Risk Emergency Medicine Anaphylaxis February 2019
 UCSF High Risk Emergency Medicine Anaphylaxis February 2019 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN True
UCSF High Risk Emergency Medicine Anaphylaxis February 2019 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN True
OBJECTIVES DEFINITION TYPE I HYPERSENSITIVITY TYPES OF HYPERSENSITIVITY ACUTE ALLERGIC REACTION 11/5/2016
 OBJECTIVES ACUTE ALLERGIC REACTION Wei Zhao, MD, PhD Ambulatory Medical Director Children s Hospital of Richmond at VCU Associate Professor, Chief Chief, Division of Allergy and Immunology Virginia Commonwealth
OBJECTIVES ACUTE ALLERGIC REACTION Wei Zhao, MD, PhD Ambulatory Medical Director Children s Hospital of Richmond at VCU Associate Professor, Chief Chief, Division of Allergy and Immunology Virginia Commonwealth
VACCINE-RELATED ALLERGIC REACTIONS
 VACCINE-RELATED ALLERGIC REACTIONS Management of Anaphylaxis Public Health Immunization Program June 2018 VACCINE-RELATED ADVERSE EVENTS Local reactions pain, edema, erythema Systemic reactions fever,
VACCINE-RELATED ALLERGIC REACTIONS Management of Anaphylaxis Public Health Immunization Program June 2018 VACCINE-RELATED ADVERSE EVENTS Local reactions pain, edema, erythema Systemic reactions fever,
Anaphylaxis ASCIA Education Resources Information for health professionals
 Anaphylaxis ASCIA Education Resources Information for health professionals Anaphylaxis is a rapidly evolving, generalised multi-system allergic reaction characterized by one or more symptoms or signs of
Anaphylaxis ASCIA Education Resources Information for health professionals Anaphylaxis is a rapidly evolving, generalised multi-system allergic reaction characterized by one or more symptoms or signs of
Allergy Management Policy
 Allergy Management Policy Food Allergy People with allergies have over-reactive immune systems that target otherwise harmless elements of our diet and environment. During an allergic reaction to food,
Allergy Management Policy Food Allergy People with allergies have over-reactive immune systems that target otherwise harmless elements of our diet and environment. During an allergic reaction to food,
Food Allergy & Anaphylaxis
 Food Allergy & Anaphylaxis Selina Gierer, DO Marissa Love, MD University of Kansas Hospital Division of Allergy, Immunology and Rheumatology July 21, 2016 Insert in USA Today December 2010 Generated a
Food Allergy & Anaphylaxis Selina Gierer, DO Marissa Love, MD University of Kansas Hospital Division of Allergy, Immunology and Rheumatology July 21, 2016 Insert in USA Today December 2010 Generated a
Systemic Allergic & Immunoglobulin Disorders
 Systemic Allergic & Immunoglobulin Disorders Bryan L. Martin, DO, MMAS, FACAAI, FAAAAI, FACP, FACOI Emeritus Professor of Medicine and Pediatrics President, American College of Allergy, Asthma & Immunology
Systemic Allergic & Immunoglobulin Disorders Bryan L. Martin, DO, MMAS, FACAAI, FAAAAI, FACP, FACOI Emeritus Professor of Medicine and Pediatrics President, American College of Allergy, Asthma & Immunology
Anaphylaxis: The Atypical Varieties
 Anaphylaxis: The Atypical Varieties John Johnson, D.O., PGY-4 Allergy/Immunology Fellow University Hospitals of Cleveland Case Western Reserve University School of Medicine Disclosures: None What is Anaphylaxis?
Anaphylaxis: The Atypical Varieties John Johnson, D.O., PGY-4 Allergy/Immunology Fellow University Hospitals of Cleveland Case Western Reserve University School of Medicine Disclosures: None What is Anaphylaxis?
Allergy Immunotherapy in the Primary Care Setting
 Allergy Immunotherapy in the Primary Care Setting New York State College Health Association 2008 COMBINED ANNUAL MEETING October 2008 Mary Madsen RN BC University of Rochester Issues in Primary Care Practice
Allergy Immunotherapy in the Primary Care Setting New York State College Health Association 2008 COMBINED ANNUAL MEETING October 2008 Mary Madsen RN BC University of Rochester Issues in Primary Care Practice
Anaphylaxis/Latex Allergy
 Children s Acute Transport Service CATS Clinical Guideline Anaphylaxis/Latex Allergy Document Control Information Author D Lutman Author Position Consultant Document Owner E Polke Document Owner Position
Children s Acute Transport Service CATS Clinical Guideline Anaphylaxis/Latex Allergy Document Control Information Author D Lutman Author Position Consultant Document Owner E Polke Document Owner Position
Managing Allergies and Anaphylaxis at School EPI-PEN TRAINING FOR SCHOOL PERSONNEL
 Managing Allergies and Anaphylaxis at School EPI-PEN TRAINING FOR SCHOOL PERSONNEL Objective: Attendees will be able to: Increase their knowledge about allergies to food and other allergens. Describe the
Managing Allergies and Anaphylaxis at School EPI-PEN TRAINING FOR SCHOOL PERSONNEL Objective: Attendees will be able to: Increase their knowledge about allergies to food and other allergens. Describe the
Anaphylaxis: Treatment in the Community
 : Treatment in the Community is likely if a patient who, within minutes of exposure to a trigger (allergen), develops a sudden illness with rapidly progressing skin changes and life-threatening airway
: Treatment in the Community is likely if a patient who, within minutes of exposure to a trigger (allergen), develops a sudden illness with rapidly progressing skin changes and life-threatening airway
Allergy & Anaphylaxis
 Allergy & Anaphylaxis (why, where, and what to do) Robert H. Brown, M.D., M.P.H. Professor Departments of Anesthesiology, Environmental Health Sciences, Medicine, and Radiology The Johns Hopkins Medical
Allergy & Anaphylaxis (why, where, and what to do) Robert H. Brown, M.D., M.P.H. Professor Departments of Anesthesiology, Environmental Health Sciences, Medicine, and Radiology The Johns Hopkins Medical
Path2220 INTRODUCTION TO HUMAN DISEASE ALLERGY. Dr. Erika Bosio
 Path2220 INTRODUCTION TO HUMAN DISEASE ALLERGY Dr. Erika Bosio Research Fellow Centre for Clinical Research in Emergency Medicine, Harry Perkins Institute of Medical Research University of Western Australia
Path2220 INTRODUCTION TO HUMAN DISEASE ALLERGY Dr. Erika Bosio Research Fellow Centre for Clinical Research in Emergency Medicine, Harry Perkins Institute of Medical Research University of Western Australia
VACCINE-RELATED ALLERGIC REACTIONS
 VACCINE-RELATED ALLERGIC REACTIONS Management of Anaphylaxis IERHA Immunization Program September 2016 VACCINE-RELATED ADVERSE EVENTS Local reactions pain, edema, erythema Systemic reactions fever, lymphadenopathy
VACCINE-RELATED ALLERGIC REACTIONS Management of Anaphylaxis IERHA Immunization Program September 2016 VACCINE-RELATED ADVERSE EVENTS Local reactions pain, edema, erythema Systemic reactions fever, lymphadenopathy
contact activation in formation diseases 67 endothelial cells and kinin formation 73 processing and degradation 68 70
 Subject Index Adenosine, mast cell activation modulation 60 Age, risk factor 17, 18 Allergen elicitors 9, 10 insects, see Insect venom-induced microarrays for 136 overview of characteristics 23 recognition
Subject Index Adenosine, mast cell activation modulation 60 Age, risk factor 17, 18 Allergen elicitors 9, 10 insects, see Insect venom-induced microarrays for 136 overview of characteristics 23 recognition
Eczema: also called atopic dermatitis; a chronic, itchy, scaly rash not due to a particular substance exposure
 Allergy is a condition in which the immune system causes sneezing, itching, rashes, and wheezing, or sometimes even life-threatening allergic reactions. The more you know about allergies, the better prepared
Allergy is a condition in which the immune system causes sneezing, itching, rashes, and wheezing, or sometimes even life-threatening allergic reactions. The more you know about allergies, the better prepared
Food allergy in children. nice bulletin. NICE Bulletin Food Allergy in Chlidren.indd 1
 nice bulletin Food allergy in children NICE provided the content for this booklet which is independent of any company or product advertised NICE Bulletin Food Allergy in Chlidren.indd 1 23/01/2012 11:04
nice bulletin Food allergy in children NICE provided the content for this booklet which is independent of any company or product advertised NICE Bulletin Food Allergy in Chlidren.indd 1 23/01/2012 11:04
Anaphylaxis. Emergencies for the general physician. Shuaib Nasser Consultant in Allergy and Asthma Cambridge University Hospitals NHS Foundation Trust
 Anaphylaxis Emergencies for the general physician Shuaib Nasser Consultant in Allergy and Asthma Cambridge University Hospitals NHS Foundation Trust Definition- Anaphylaxis A potentially life-threatening
Anaphylaxis Emergencies for the general physician Shuaib Nasser Consultant in Allergy and Asthma Cambridge University Hospitals NHS Foundation Trust Definition- Anaphylaxis A potentially life-threatening
Anaphylaxis School First results of a national multicenter study
 Anaphylaxis School First results of a national multicenter study J. Kupfer, S. Schallmayer, I. Fell, U. Gieler for the German study group Anaphylaxis is an acute, potentially life-threatening hypersensitivity
Anaphylaxis School First results of a national multicenter study J. Kupfer, S. Schallmayer, I. Fell, U. Gieler for the German study group Anaphylaxis is an acute, potentially life-threatening hypersensitivity
Student Health Center
 Referring Allergist Agreement Your patient is requesting that the University of Mary Washington Student Health Center (UMWSHC) administer allergy extracts provided by your office. Consistent with our policies
Referring Allergist Agreement Your patient is requesting that the University of Mary Washington Student Health Center (UMWSHC) administer allergy extracts provided by your office. Consistent with our policies
PERIOPERATIVE ANAPHYLAXIS: A BRIEF REVIEW
 PERIOPERATIVE ANAPHYLAXIS: A BRIEF REVIEW DEC 2011 ANDREW TRIEBWASSER DEPARTMENT OF ANESTHESIA HASBRO CHILDREN S HOSPITAL ADVERSE DRUG REACTIONS (ADR) IN THE PERIOPERATIVE ENVIRONMENT: OVERVIEW most perioperative
PERIOPERATIVE ANAPHYLAXIS: A BRIEF REVIEW DEC 2011 ANDREW TRIEBWASSER DEPARTMENT OF ANESTHESIA HASBRO CHILDREN S HOSPITAL ADVERSE DRUG REACTIONS (ADR) IN THE PERIOPERATIVE ENVIRONMENT: OVERVIEW most perioperative
CCSD School Nurses. Support of Students with Life Threatening Allergies
 CCSD School Nurses Support of Students with Life Threatening Allergies The Clark County School District is committed to provide a safe, supportive environment in which all students can learn and achieve.
CCSD School Nurses Support of Students with Life Threatening Allergies The Clark County School District is committed to provide a safe, supportive environment in which all students can learn and achieve.
Allergic Reactions and Anaphylaxis. William Mapes, NRP, I/C Chief, Brandon Area Rescue Squad Brandon, VT
 Allergic Reactions and Anaphylaxis William Mapes, NRP, I/C Chief, Brandon Area Rescue Squad Brandon, VT Allergy to Anaphylaxis Defined as a histamine-mediated spectrum of physiologic events that include:
Allergic Reactions and Anaphylaxis William Mapes, NRP, I/C Chief, Brandon Area Rescue Squad Brandon, VT Allergy to Anaphylaxis Defined as a histamine-mediated spectrum of physiologic events that include:
Emergency Preparedness for Anaphylaxis in School
 10/19/2017 Emergency Preparedness for Anaphylaxis in School Michael Corjulo APRN, CPNP, AE-C ASNC April 20, 2017 Objectives Review a brief overview of anaphylaxis related to the school environment Demonstrate
10/19/2017 Emergency Preparedness for Anaphylaxis in School Michael Corjulo APRN, CPNP, AE-C ASNC April 20, 2017 Objectives Review a brief overview of anaphylaxis related to the school environment Demonstrate
Anaphylaxis. History of anaphylaxis. Epidemiology. Definition. Type I Hypersensitivity. Pathophysiology
 History of anaphylaxis Anaphylaxis William Reisacher, MD FACS FAAOA Assistant Professor Department of Otorhinolaryngology Weill Cornell Medical College 2640 BC: Menes, an Egyptian pharaoh, was depicted
History of anaphylaxis Anaphylaxis William Reisacher, MD FACS FAAOA Assistant Professor Department of Otorhinolaryngology Weill Cornell Medical College 2640 BC: Menes, an Egyptian pharaoh, was depicted
Hymenoptera Venom Allergy. David F. Graft, M.D.
 Hymenoptera Venom Allergy David F. Graft, M.D. Stinging Insect Hypersensitivity: A Practice Parameter Update 2010 * Chief Editors David B.K. Golden, MD, John Moffit, MD and Richard A. Nicklas, MD Work
Hymenoptera Venom Allergy David F. Graft, M.D. Stinging Insect Hypersensitivity: A Practice Parameter Update 2010 * Chief Editors David B.K. Golden, MD, John Moffit, MD and Richard A. Nicklas, MD Work
Anaphylaxis in the Clinic: Are you prepared?
 Anaphylaxis in the Clinic: Are you prepared? Dewey Hahlbohm, PA-C, AE-C Thanks Dr. Mike Zacharisen for your help! Conflict of Interest: none Have you read this book? A. Yes B. No C. I can t remember D.
Anaphylaxis in the Clinic: Are you prepared? Dewey Hahlbohm, PA-C, AE-C Thanks Dr. Mike Zacharisen for your help! Conflict of Interest: none Have you read this book? A. Yes B. No C. I can t remember D.
Idiopathic Anaphylaxis. Paul A. Greenberger, MD, FAAAAI 2/28/2014 Course # 1605
 Idiopathic Anaphylaxis Paul A. Greenberger, MD, FAAAAI 2/28/2014 Course # 1605 Objectives Review definition and classification of idiopathic anaphylaxis Consider the differential diagnosis Critique lab
Idiopathic Anaphylaxis Paul A. Greenberger, MD, FAAAAI 2/28/2014 Course # 1605 Objectives Review definition and classification of idiopathic anaphylaxis Consider the differential diagnosis Critique lab
Emergency Department Guideline. Anaphylaxis
 Emergency Department Guideline Inclusion criteria: 1. Acute onset of an illness (minutes to hours) with a AND (b OR c): a. Skin and/or mucosa (pruritus, flushing, hives, angioedema) b. Respiratory compromise
Emergency Department Guideline Inclusion criteria: 1. Acute onset of an illness (minutes to hours) with a AND (b OR c): a. Skin and/or mucosa (pruritus, flushing, hives, angioedema) b. Respiratory compromise
Michaela Lucas. Clinical Immunologist/Immunopathologist. Pathwest, QE2 Medical Centre, Princess Margaret Hospital
 Michaela Lucas Clinical Immunologist/Immunopathologist Pathwest, QE2 Medical Centre, Princess Margaret Hospital School of Medicine and Pharmacology, School of Pathology and Laboratory Medicine University
Michaela Lucas Clinical Immunologist/Immunopathologist Pathwest, QE2 Medical Centre, Princess Margaret Hospital School of Medicine and Pharmacology, School of Pathology and Laboratory Medicine University
Management of ANAPHYLAXIS in the School Setting. Updated September 2010
 Management of ANAPHYLAXIS in the School Setting Updated September 2010 What is an Allergy? Allergies occur when the immune system becomes unusually sensitive and over reacts to common substance that are
Management of ANAPHYLAXIS in the School Setting Updated September 2010 What is an Allergy? Allergies occur when the immune system becomes unusually sensitive and over reacts to common substance that are
Allergy Awareness & EpiPen Administration
 Allergy Awareness & EpiPen Administration 2017-18 Common Allergens in Children! Shellfish! Milk! Egg! Peanut! Tree Nuts! Fish! Soy! Latex! Insect Stings! Exercise What is an allergy? * An allergy is an
Allergy Awareness & EpiPen Administration 2017-18 Common Allergens in Children! Shellfish! Milk! Egg! Peanut! Tree Nuts! Fish! Soy! Latex! Insect Stings! Exercise What is an allergy? * An allergy is an
Chapter 65 Allergy and Immunology for the Internist. ingestion provoke an IgE antibody response and clinical symptoms in sensitive individuals.
 Chapter 65 Allergy and Immunology for the Internist 1 I. Basic Information A. Definition of Allergens: Proteins of appropriate size that after inhalation, injection (e.g. drug, venom) or ingestion provoke
Chapter 65 Allergy and Immunology for the Internist 1 I. Basic Information A. Definition of Allergens: Proteins of appropriate size that after inhalation, injection (e.g. drug, venom) or ingestion provoke
Immunocompetence The immune system responds appropriately to a foreign stimulus
 Functions of the immune system Protect the body s internal environment against invading organisms Maintain homeostasis by removing damaged cells from the circulation Serve as a surveillance network for
Functions of the immune system Protect the body s internal environment against invading organisms Maintain homeostasis by removing damaged cells from the circulation Serve as a surveillance network for
Allergic reactions anaphylaxis *** CME Version *** Aaron J. Katz, AEMT-P, CIC
 Allergic reactions anaphylaxis *** CME Version *** Aaron J. Katz, AEMT-P, CIC www.es26medic.net Some terms Allergic reaction Exaggerated immune system response to an allergen Allergen The thing that causes
Allergic reactions anaphylaxis *** CME Version *** Aaron J. Katz, AEMT-P, CIC www.es26medic.net Some terms Allergic reaction Exaggerated immune system response to an allergen Allergen The thing that causes
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Anaphylaxis in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Anaphylaxis in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
EPI PEN TRAINING KAREN, RN, BSN FARGO SOUTH SCHOOL NURSE
 EPI PEN TRAINING KAREN, RN, BSN FARGO SOUTH SCHOOL NURSE Why use an Epipen? Anaphylaxis Anaphylaxis is a severe, potentially lifethreatening allergic reaction caused by contact with certain triggers CAUSES
EPI PEN TRAINING KAREN, RN, BSN FARGO SOUTH SCHOOL NURSE Why use an Epipen? Anaphylaxis Anaphylaxis is a severe, potentially lifethreatening allergic reaction caused by contact with certain triggers CAUSES
Which Factors Might Enhance Safety of Immunotherapy in Your Clinic?
 Which Factors Might Enhance Safety of Immunotherapy in Your Clinic? David I. Bernstein MD FAAAI Professor of Medicine and Environmental Health Division of Immunology and Allergy University of Cincinnati
Which Factors Might Enhance Safety of Immunotherapy in Your Clinic? David I. Bernstein MD FAAAI Professor of Medicine and Environmental Health Division of Immunology and Allergy University of Cincinnati
IMMUNOLOGY. Referral Guidelines NATIONAL REFERRAL GUIDELINES : IMMUNOLOGY. As above Specialist assessment is essential.
 PAGE 1 IMMUNOLOGY National PRIMARY IMMUNODEFICIENCY Primary immunodeficiency should be suspected in any patient with recurrent or persistent infection or unusual infection. Recurrent sinopulmonary infections
PAGE 1 IMMUNOLOGY National PRIMARY IMMUNODEFICIENCY Primary immunodeficiency should be suspected in any patient with recurrent or persistent infection or unusual infection. Recurrent sinopulmonary infections
2/10/2017 THE NUTS AND BOLTS OF FOOD ALLERGY LEARNING OBJECTIVES DEFINITIONS
 THE NUTS AND BOLTS OF FOOD ALLERGY Amanda Hess, MMS, PA-C San Tan Allergy & Asthma Arizona Allergy & Immunology Research Gilbert, Arizona LEARNING OBJECTIVES 1. Discuss the epidemiology, natural history
THE NUTS AND BOLTS OF FOOD ALLERGY Amanda Hess, MMS, PA-C San Tan Allergy & Asthma Arizona Allergy & Immunology Research Gilbert, Arizona LEARNING OBJECTIVES 1. Discuss the epidemiology, natural history
SAN JOAQUIN COUNTY EMERGENCY MEDICAL SERVICES AGENCY. Administration of Epinephrine Auto-Injector Training
 SAN JOAQUIN COUNTY EMERGENCY MEDICAL SERVICES AGENCY Administration of Epinephrine Auto-Injector Training Disclaimer: Authorization - EMT Optional Skills Only authorized Emergency Medical Technicians (EMT)
SAN JOAQUIN COUNTY EMERGENCY MEDICAL SERVICES AGENCY Administration of Epinephrine Auto-Injector Training Disclaimer: Authorization - EMT Optional Skills Only authorized Emergency Medical Technicians (EMT)
West Houston Allergy & Asthma, P.A.
 Consent to Receive Immunotherapy (ALLERGY SHOTS) Procedure Allergy injections are usually started at a very low dose. This dose is gradually increased on a regular (usually 1-2 times per week) basis until
Consent to Receive Immunotherapy (ALLERGY SHOTS) Procedure Allergy injections are usually started at a very low dose. This dose is gradually increased on a regular (usually 1-2 times per week) basis until
Immunologic Mechanisms of Tissue Damage. (Immuopathology)
") Immunologic Mechanisms of Tissue Damage (Immuopathology) Immunopathology Exaggerated immune response may lead to different forms of tissue damage 1) An overactive immune response: produce more damage than
Immunologic Mechanisms of Tissue Damage (Immuopathology) Immunopathology Exaggerated immune response may lead to different forms of tissue damage 1) An overactive immune response: produce more damage than
Rand E. Dankner, M.D. Jacqueline L. Reiss, M. D.
 Tips to Remember: Food allergy Up to 2 million, or 8%, of children, and 2% of adults in the United States are estimated to have food allergies. With a true food allergy, an individual's immune system will
Tips to Remember: Food allergy Up to 2 million, or 8%, of children, and 2% of adults in the United States are estimated to have food allergies. With a true food allergy, an individual's immune system will
Allergic Reactions and Envenomations. Chapter 16
 Allergic Reactions and Envenomations Chapter 16 Allergic Reactions Allergic reaction Exaggerated immune response to any substance Histamines and leukotrienes Chemicals released by the immune system Anaphylaxis
Allergic Reactions and Envenomations Chapter 16 Allergic Reactions Allergic reaction Exaggerated immune response to any substance Histamines and leukotrienes Chemicals released by the immune system Anaphylaxis
Anaphylaxis: treatment in the community
 : treatment in the community Item Type Guideline Authors Health Service Executive Citation Health Service Executive. : treatment in the community. Dublin: Health Service Executive;. 5p. Publisher Health
: treatment in the community Item Type Guideline Authors Health Service Executive Citation Health Service Executive. : treatment in the community. Dublin: Health Service Executive;. 5p. Publisher Health
MANAGING COMMON PRESENTATIONS OF ALLERGY IN PRIMARY CARE. Helen Bourne Consultant Immunologist
 MANAGING COMMON PRESENTATIONS OF ALLERGY IN PRIMARY CARE Helen Bourne Consultant Immunologist AIMS Presentation of Allergic Disease in Adults Rhinitis/ Rhinoconjuctivitis Urticaria and Angioedema Food
MANAGING COMMON PRESENTATIONS OF ALLERGY IN PRIMARY CARE Helen Bourne Consultant Immunologist AIMS Presentation of Allergic Disease in Adults Rhinitis/ Rhinoconjuctivitis Urticaria and Angioedema Food
Anaphylactic Hypersensitivity Reactions 2.0 Contact Hours Presented by: CEU Professor
 Anaphylactic Hypersensitivity Reactions 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Anaphylactic Hypersensitivity Reactions 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
: ALLERGIC REACTION
 6208.05: ALLERGIC REACTION INTRODUCTION Allergic (hypersensitivity) reactions are most often secondary to an exaggerated immune system response to a harmless foreign antigen (e.g. insect bite or sting,
6208.05: ALLERGIC REACTION INTRODUCTION Allergic (hypersensitivity) reactions are most often secondary to an exaggerated immune system response to a harmless foreign antigen (e.g. insect bite or sting,
Anaphylaxis: clinical features and GP s role in management
 n PRESCRIBING IN PRACTICE Anaphylaxis: clinical features and GP s role in management Priya Sellaturay BSc, MRCP, Krzysztof Rutkowski MD, MRCP and Shuaib Nasser MA, MD, FRCP SPL Anaphylaxis can be fatal
n PRESCRIBING IN PRACTICE Anaphylaxis: clinical features and GP s role in management Priya Sellaturay BSc, MRCP, Krzysztof Rutkowski MD, MRCP and Shuaib Nasser MA, MD, FRCP SPL Anaphylaxis can be fatal
Who Should Be Premediciated for Contrast-Enhanced Exams?
 Who Should Be Premediciated for Contrast-Enhanced Exams? Jeffrey C. Weinreb, MD,FACR Yale University School of Medicine jeffrey.weinreb@yale.edu Types of Intravenous Contrast Media Iodinated Contrast Agents
Who Should Be Premediciated for Contrast-Enhanced Exams? Jeffrey C. Weinreb, MD,FACR Yale University School of Medicine jeffrey.weinreb@yale.edu Types of Intravenous Contrast Media Iodinated Contrast Agents
The Diagnosis and Management of Anaphylaxis
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-allergy/the-diagnosis-and-management-of-anaphylaxis/3919/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-allergy/the-diagnosis-and-management-of-anaphylaxis/3919/
TREATMENT OF ANAPHYLACTIC REACTION WITH EPINEPHRINE
 TREATMENT OF ANAPHYLACTIC REACTION WITH EPINEPHRINE FILE: JGCDC Background: The Bibb County School System recognizes the growing concern with severe life-threatening allergic reactions to food items, latex,
TREATMENT OF ANAPHYLACTIC REACTION WITH EPINEPHRINE FILE: JGCDC Background: The Bibb County School System recognizes the growing concern with severe life-threatening allergic reactions to food items, latex,
FDA/NSTA Web Seminar: Teach Science Concepts and Inquiry with Food
 LIVE INTERACTIVE LEARNING @ YOUR DESKTOP FDA/NSTA Web Seminar: Teach Science Concepts and Inquiry with Food Thursday, November 15, 2007 Food allergy Stefano Luccioli, MD Office of Food Additive Safety
LIVE INTERACTIVE LEARNING @ YOUR DESKTOP FDA/NSTA Web Seminar: Teach Science Concepts and Inquiry with Food Thursday, November 15, 2007 Food allergy Stefano Luccioli, MD Office of Food Additive Safety
New Developments in Food Allergies, Prevention & Treatment
 New Developments in Food Allergies, Prevention & Treatment Michael Daines, M.D. Associate Professor, Pediatric Allergy and Immunology Division director, Pediatric Allergy, Immunology, and Rheumatology
New Developments in Food Allergies, Prevention & Treatment Michael Daines, M.D. Associate Professor, Pediatric Allergy and Immunology Division director, Pediatric Allergy, Immunology, and Rheumatology
Impact of Asthma in the U.S. per Year. Asthma Epidemiology and Pathophysiology. Risk Factors for Asthma. Childhood Asthma Costs of Asthma
 American Association for Respiratory Care Asthma Educator Certification Prep Course Asthma Epidemiology and Pathophysiology Robert C. Cohn, MD, FAARC MetroHealth Medical Center Cleveland, OH Impact of
American Association for Respiratory Care Asthma Educator Certification Prep Course Asthma Epidemiology and Pathophysiology Robert C. Cohn, MD, FAARC MetroHealth Medical Center Cleveland, OH Impact of
Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October
 Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October Allergic Reactions ( Immediate Hypersensitivity ) Hay fever, food, drug & animal allergies, reactions to bee stings, etc. Symptoms may include
Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October Allergic Reactions ( Immediate Hypersensitivity ) Hay fever, food, drug & animal allergies, reactions to bee stings, etc. Symptoms may include
Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October
 Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October Allergic Reactions ( Immediate Hypersensitivity ) Hay fever, food, drug & animal allergies, reactions to bee stings, etc. Symptoms may include
Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October Allergic Reactions ( Immediate Hypersensitivity ) Hay fever, food, drug & animal allergies, reactions to bee stings, etc. Symptoms may include
ALLERGIC EMERGENCIES 5/8/2015. Objectives for Pharmacists. Patient Case. Objectives for Technicians. Definition of Anaphylaxis.
 ALLERGIC EMERGENCIES Kristina Dawson, PharmD, BCPS Objectives for Pharmacists Describe the immunologic pathways to cause an allergic response Identify the most common triggers to cause Choose the appropriate
ALLERGIC EMERGENCIES Kristina Dawson, PharmD, BCPS Objectives for Pharmacists Describe the immunologic pathways to cause an allergic response Identify the most common triggers to cause Choose the appropriate
Anaphylaxis for House Staff: Rapid Recognition and Treatment
 8/2/14 2:00 am Rapid Response Anaphylaxis for House Staff: Rapid Recognition and Treatment You are covering a patient with urosepsis. She is receiving her second dose of ceftriaxone. You are called for
8/2/14 2:00 am Rapid Response Anaphylaxis for House Staff: Rapid Recognition and Treatment You are covering a patient with urosepsis. She is receiving her second dose of ceftriaxone. You are called for
Urticaria and Angioedema. Allergy and Immunology Awareness Program
 Urticaria and Angioedema Allergy and Immunology Awareness Program 1 Urticaria and Angioedema Allergy and Immunology Awareness Program Urticaria Commonly known as hives, urticarial is an itchy rash with
Urticaria and Angioedema Allergy and Immunology Awareness Program 1 Urticaria and Angioedema Allergy and Immunology Awareness Program Urticaria Commonly known as hives, urticarial is an itchy rash with
Anaphylaxis: clinical features, management and avoidance
 Anaphylaxis: clinical features, management and avoidance James Bateman MRCP and Robin Ferner MSc, MD, FRCP VM Our series on serious ADRs focusses on rare but potentially fatal drug reactions and how to
Anaphylaxis: clinical features, management and avoidance James Bateman MRCP and Robin Ferner MSc, MD, FRCP VM Our series on serious ADRs focusses on rare but potentially fatal drug reactions and how to
Queen City Independent School District Stock Epinephrine Policy/Protocol
 Queen City Independent School District Stock Epinephrine Policy/Protocol In accordance with Texas SB 66 as well as Chapter 38 of the Education Code Subchapter E, and the NASN guidelines for stock Epinephrine
Queen City Independent School District Stock Epinephrine Policy/Protocol In accordance with Texas SB 66 as well as Chapter 38 of the Education Code Subchapter E, and the NASN guidelines for stock Epinephrine
FAUQUIER COUNTY PUBLIC SCHOOLS Policy: Adopted: 04/10/2012 Revised: 07/23/12, 7/08/13, 08/11/14, 08/14/17 ADMINISTERING MEDICINES TO STUDENTS
 ACCOMPANYING REGULATION REGULATION 7-5.3(B): ADMINISTRATION OF EPINEPHRINE (Severe Allergic Reaction) 1. Generally 1.1. Fauquier County Public Schools Public Schools ( FCPS) anaphylaxis regulation is developed
ACCOMPANYING REGULATION REGULATION 7-5.3(B): ADMINISTRATION OF EPINEPHRINE (Severe Allergic Reaction) 1. Generally 1.1. Fauquier County Public Schools Public Schools ( FCPS) anaphylaxis regulation is developed
ANAPHYLAXIS POLICY & PROCEDURES
 PHOENIX P-12 COMMUNITY COLLEGE ANAPHYLAXIS POLICY & PROCEDURES Policy Statement Anaphylaxis is a severe, rapidly progressive allergic reaction that involves various areas of the body simultaneously and
PHOENIX P-12 COMMUNITY COLLEGE ANAPHYLAXIS POLICY & PROCEDURES Policy Statement Anaphylaxis is a severe, rapidly progressive allergic reaction that involves various areas of the body simultaneously and
Chapter 20 - Immunologic Emergencies
 1 2 3 4 5 6 7 8 9 10 National EMS Education Standard Competencies (1 of 2) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an
1 2 3 4 5 6 7 8 9 10 National EMS Education Standard Competencies (1 of 2) Medicine Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an
Introduction: Severe adverse reactions:
 Immunotherapy and Anaphylaxis: Risks, Prevention, Recognition and Treatment by Frederick M. Schaffer, M.D. Associate Professor, The Medical University of South Carolina Introduction: Immunotherapy (IT)
Immunotherapy and Anaphylaxis: Risks, Prevention, Recognition and Treatment by Frederick M. Schaffer, M.D. Associate Professor, The Medical University of South Carolina Introduction: Immunotherapy (IT)
Epidemiology of anaphylaxis among children and adolescents enrolled in a health maintenance organization
 Epidemiology of anaphylaxis among children and adolescents enrolled in a health maintenance organization Kari Bohlke, ScD, a Robert L. Davis, MD, MPH, a,b Frank DeStefano, MD, MPH, c S. Michael Marcy,
Epidemiology of anaphylaxis among children and adolescents enrolled in a health maintenance organization Kari Bohlke, ScD, a Robert L. Davis, MD, MPH, a,b Frank DeStefano, MD, MPH, c S. Michael Marcy,
FOOD ALLERGY. Dr Colin J Lumsden. Senior Lecturer and Honorary Consultant Paediatrician. Royal Preston Hospital
 FOOD ALLERGY Dr Colin J Lumsden Senior Lecturer and Honorary Consultant Paediatrician Royal Preston Hospital LEARNING OUTCOMES Pathophysiology Presentation Diagnosis Investigation Management Milk Allergy
FOOD ALLERGY Dr Colin J Lumsden Senior Lecturer and Honorary Consultant Paediatrician Royal Preston Hospital LEARNING OUTCOMES Pathophysiology Presentation Diagnosis Investigation Management Milk Allergy
Implications on therapy. Prof. of Medicine and Allergy Faculty of Medicine, Cairo University
 Implications on therapy Dr. Hisham Tarraf MD,FRCP(Edinb.) Prof. of Medicine and Allergy Faculty of Medicine, Cairo University Need for better understanding Global health problem Impact on quality of life
Implications on therapy Dr. Hisham Tarraf MD,FRCP(Edinb.) Prof. of Medicine and Allergy Faculty of Medicine, Cairo University Need for better understanding Global health problem Impact on quality of life
About the immune system
 The immune system and anaphylaxis edward.purssell@kcl.ac.uk About the immune system The immune system Protects the body from infectious organisms, foreign bodies and malignancies Surface barriers Innate
The immune system and anaphylaxis edward.purssell@kcl.ac.uk About the immune system The immune system Protects the body from infectious organisms, foreign bodies and malignancies Surface barriers Innate
Investigation and diagnosis of lifethreatening
 Investigation and diagnosis of lifethreatening allergies in childhood SA Journal of Child Health P C Potter, MD, FCP (SA), DCH (SA), FAAAAI, FACAAI, BSc (Hons) Immunology Allergy Diagnostic and Clinical
Investigation and diagnosis of lifethreatening allergies in childhood SA Journal of Child Health P C Potter, MD, FCP (SA), DCH (SA), FAAAAI, FACAAI, BSc (Hons) Immunology Allergy Diagnostic and Clinical
Anaphylaxis. Will Davies May 2014
 Anaphylaxis Will Davies May 2014 Anaphylaxis Algorithm EMCore 2014 History suggestive of anaphylactic reaction? Acute onset of illness associated with trigger Relative bradycardia with hypotension without
Anaphylaxis Will Davies May 2014 Anaphylaxis Algorithm EMCore 2014 History suggestive of anaphylactic reaction? Acute onset of illness associated with trigger Relative bradycardia with hypotension without
S:\Admin Staff\100 Administration\2010\109 Policy\Operational Plans\Anaphylaxis Policy.doc
 Growing Together Principal: Mr Paul Andrijich Deputy Principal: Mr Paul Westcott Registrar: Mrs Kerry Vine 65 Coast Road West Swan WA 6055 Telephone: 9250 2711 Mobile: 0434734390 Fax: 9250 2416 EDUCATE
Growing Together Principal: Mr Paul Andrijich Deputy Principal: Mr Paul Westcott Registrar: Mrs Kerry Vine 65 Coast Road West Swan WA 6055 Telephone: 9250 2711 Mobile: 0434734390 Fax: 9250 2416 EDUCATE
Administering epinephrine for acute anaphylactic type allergic reactions
 Administering epinephrine for acute anaphylactic type allergic reactions Training for first aiders People known to be allergic (1.5 hours) MAJ 2012-3 2 Objectives of the training Understand the legal context
Administering epinephrine for acute anaphylactic type allergic reactions Training for first aiders People known to be allergic (1.5 hours) MAJ 2012-3 2 Objectives of the training Understand the legal context
Managing Allergies and Anaphylaxis at School: Training for School Personnel
 Managing Allergies and Anaphylaxis at School: Training for School Personnel Recognizing Severe Allergic Response Use of Epinephrine Auto-Injectors The resources for this presentation were created by the
Managing Allergies and Anaphylaxis at School: Training for School Personnel Recognizing Severe Allergic Response Use of Epinephrine Auto-Injectors The resources for this presentation were created by the
An allergic reaction is an exaggerated response by the immune system to a foreign substance
 ALLERGIC REACTION An allergic reaction is an exaggerated response by the immune system to a foreign substance Anaphylaxis is an unusual or exaggerated allergic reaction; is a life threatening emergency
ALLERGIC REACTION An allergic reaction is an exaggerated response by the immune system to a foreign substance Anaphylaxis is an unusual or exaggerated allergic reaction; is a life threatening emergency
02/06/2013. Goal of program. A few definitions. Objectives of the training. Legal context. Legal context in schools
 2 Goal of program Administering epinephrine for acute anaphylactic type allergic reactions Reduce the morbidity and mortality associated with acute anaphylactic type allergic reactions. Training for first
2 Goal of program Administering epinephrine for acute anaphylactic type allergic reactions Reduce the morbidity and mortality associated with acute anaphylactic type allergic reactions. Training for first
Anaphylaxis: Exactly what you need to know. Dr. David Carr February 23 rd 2014
 Anaphylaxis: Exactly what you need to know Dr. David Carr February 23 rd 2014 Disclosures I AM NOT AN ALLERGIST OR IMMUNOLOGIST But I treat acute allergic reactions nearly every single shift I also work
Anaphylaxis: Exactly what you need to know Dr. David Carr February 23 rd 2014 Disclosures I AM NOT AN ALLERGIST OR IMMUNOLOGIST But I treat acute allergic reactions nearly every single shift I also work
What s new (and old!) in food allergy. Adelle R. Atkinson, MD, FRCPC Sea Courses May/June 2017
 in food allergy. Adelle R. Atkinson, MD, FRCPC Sea Courses May/June 2017") What s new (and old!) in food allergy Adelle R. Atkinson, MD, FRCPC Sea Courses May/June 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
What s new (and old!) in food allergy Adelle R. Atkinson, MD, FRCPC Sea Courses May/June 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
St. Joseph s Primary School Numurkah
 St. Joseph s Primary School Numurkah Anaphylaxis Procedure March 2014 Basic Beliefs: Our school community nurtures the development of the whole child. Our School is built on respect and an appreciation
St. Joseph s Primary School Numurkah Anaphylaxis Procedure March 2014 Basic Beliefs: Our school community nurtures the development of the whole child. Our School is built on respect and an appreciation
Immunology of Asthma. Kenneth J. Goodrum,Ph. Ph.D. Ohio University College of Osteopathic Medicine
 Immunology of Asthma Kenneth J. Goodrum,Ph Ph.D. Ohio University College of Osteopathic Medicine Outline! Consensus characteristics! Allergens:role in asthma! Immune/inflammatory basis! Genetic basis!
Immunology of Asthma Kenneth J. Goodrum,Ph Ph.D. Ohio University College of Osteopathic Medicine Outline! Consensus characteristics! Allergens:role in asthma! Immune/inflammatory basis! Genetic basis!
Food-allergy-FINAL.mp3. Duration: 0:07:39 START AUDIO
 BMJ LEARNING VIDEO TRANSCRIPT File: Duration: 0:07:39 Food-allergy-FINAL.mp3 START AUDIO Adam Fox: Food allergy is an inappropriate immune response to food. Our immune systems should ignore food completely,
BMJ LEARNING VIDEO TRANSCRIPT File: Duration: 0:07:39 Food-allergy-FINAL.mp3 START AUDIO Adam Fox: Food allergy is an inappropriate immune response to food. Our immune systems should ignore food completely,
Anaphylaxis. Choosing Wisely with Academic Detailing Conference October 21, 2017
 Anaphylaxis Choosing Wisely with Academic Detailing Conference October 21, 2017 Disclosure Natasha Rodney-Cail, Pharmacist, Drug Evaluation Unit DEU funded by the Drug Evaluation Alliance of Nova Scotia
Anaphylaxis Choosing Wisely with Academic Detailing Conference October 21, 2017 Disclosure Natasha Rodney-Cail, Pharmacist, Drug Evaluation Unit DEU funded by the Drug Evaluation Alliance of Nova Scotia
Assessing the Relative Risks of Subcutaneous and Sublingual Allergen Immunotherapy
 Assessing the Relative Risks of Subcutaneous and Sublingual Allergen Immunotherapy Tolly Epstein, MD, MS Assistant Professor of Clinical Medicine Division of Immunology, Allergy & Rheumatology University
Assessing the Relative Risks of Subcutaneous and Sublingual Allergen Immunotherapy Tolly Epstein, MD, MS Assistant Professor of Clinical Medicine Division of Immunology, Allergy & Rheumatology University