Contact dermatitis in healthcare workers
|
|
|
- Bruno Washington
- 6 years ago
- Views:
Transcription
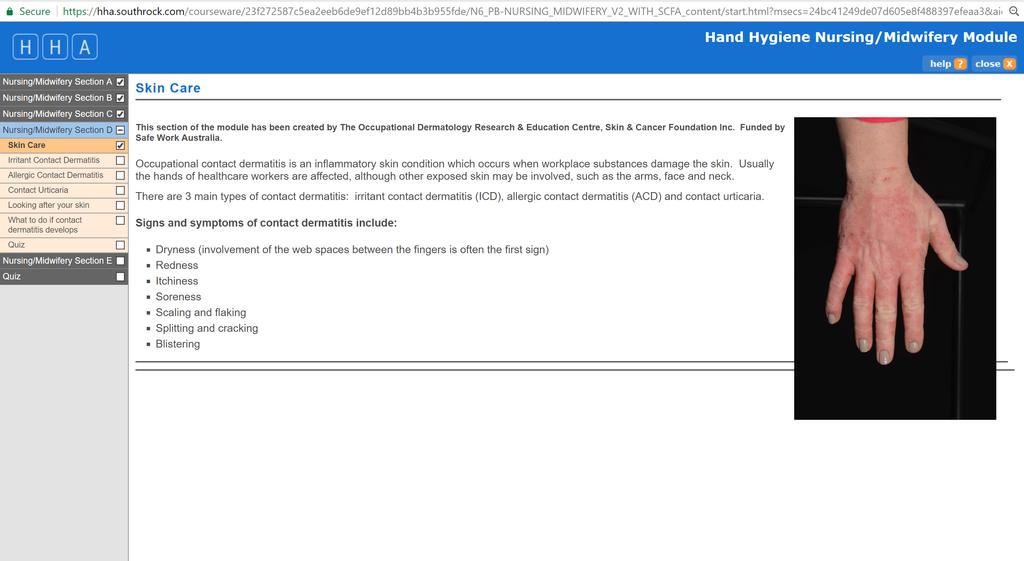
1 Contact dermatitis in healthcare workers Rosemary Nixon AM BSc(Hons) MBBS MPH FACD FAFOEM Dermatologist and occupational physician Clinical Associate Professor Monash University and The University of Melbourne Occupational Dermatology Research & Education Centre Skin & Cancer Foundation, Carlton Victoria, Australia

2
3 Making a diagnosis of contact dermatitis History Exposure assessment Clinical examination Patch testing Blood tests: RASTs especially for latex; total IgE as an indicator of atopy Prick testing, especially for foods contacted by chefs Other-skin biopsy, fungal scrapings etc
4 History History of dermatitis-duration, practitioners consulted, treatments used and the response to treatments, including prescribed and overthe-counter; work relatedness Any immediate symptoms? eg burning, redness with skin contact; wheezing, nocturnal cough suggestive of asthma Background of any skin conditions, especially atopic eczema; hay fever, asthma; hand eczema Allergies: contact, drugs, animals, foods, inhalant
5 History (ii) Other medical history and medications Work details and exposures including gloves, hand washes What they actually do at work-request photos? Hobbies, household activities including childcare (baby wipes!) What does the patient think the rash is due to?
6 Exposure can be assessed in a number of ways History given by patient, doctor or workplace Information regarding substances contacting the skin eg product labels Material safety data sheets Information from websites Chemical analyses- Malmo Occupational hygienist-toronto Workplace visits Photos of workplace-taken with patient s phone

7 Exposure assessment: the worksite visit, seeing is believing!
8 Examination Morphology of rash is very important- is it eczematous? Site of initial rash very important for allergy Can differentiate non-eczematous rashes eg psoriasis, tinea, urticaria, granuloma annulare, porphyria cutanea tarda, scabies Look for evidence of psoriasis, endogenous eczema and tinea elsewhere, especially on feet
9 Differential diagnoses of a rash on the hands Irritant contact dermatitis Allergic contact dermatitis Contact urticaria/protein contact dermatitis Infection- tinea, bacteria Endogenous forms of eczema: Hand eczema, atopic eczema, rarely discoid eczema Psoriasis Porphyria cutanea tarda; scabies Glove-related hand urticaria
10
11 Cannot clinically differentiate causes of contact dermatitis reliably. 390 consecutive patients seen by me in Occupational Dermatology Clinic Pre and post patch test diagnoses compared Only patients with eczema (various types), contact dermatitis and contact urticaria included Accuracy of my clinical diagnosis: 68% Therefore we need to patch test!
12 Diagnosing patients with suspected contact dermatitis History Exposure assessment Clinical examination Patch testing Blood tests: RASTs especially for latex; total IgE as an indicator of atopy Prick testing, especially for foods contacted by chefs Other-skin biopsy, fungal scrapings etc


13 Patch testing for delayed hypersensitivity Tests are applied for 48 hours and then removed Read reactions according to international guidelines

14 Positive reactions- what do they mean?!
15 Positive reactions indicate the presence of allergy (sensitisation) Positive reactions may be classified: Relevant Past relevance Unknown relevance eg nickel commonly of past relevance
16 To make a diagnosis of allergic contact dermatitis we need: Compatible clinical history of dermatitis Positive patch test Evidence of exposure to allergen all indicating that the reaction is relevant to the presenting dermatitis If there is no history of recent dermatitis or of exposure, we diagnose contact allergy
17 However, if patch tests are negative and we have excluded the diagnosis of allergy, then often the default diagnosis is often irritant contact dermatitis (or a form of endogenous eczema) Multiple conditions may co-exist
18
19 Immediate hypersensitivity or Type 1 reactions Common causes include natural rubber latex, foods, ammonium persulphate (hairdressing bleach) Less commonly, inhalant allergens- house dust mite, animals, malassezia furfur, chlorhexidine Present as contact urticaria with immediate burning, redness which usually resolves Repeated episodes may cause protein contact dermatitis Tested RAST test (radioallergosorbent testing) or prick testing, NOT tested by patch testing

20
21 Treatment MAKE A DIAGNOSIS: avoidance of allergens and irritants Appropriate skin protection-gloves SKIN CARE: Soap substitutes and moisturising lotions, creams and ointments Topical steroid ointments to areas of dermatitis Topical calcineurin inhibitors- tacrolimus, pimecrolimus Physical therapies- Grenz ray, UV Systemic therapies-oral corticosteroids and steroid-sparing agents
22 Skin care Appropriate gloves for each activity Soap substitutes-ph balanced Household bar soaps are alkaline and are best for getting the dirt of the knees of toddlers Moisturising lotions, creams and ointmentsthe greasier the better Topical steroids to the area of the dermatitis
23 Case: 51 year old male nurse Night shift supervisor 20 month history of dermatitis, predominantly dominant hand, which he thought might relate to latex sensitivity Improved off work Atopic with past asthma and hay fever
24 My clinical diagnosis Irritant contact dermatitis Cumulative element?
25 Patch testing 1. Coconut diethanolamide 2. Formaldehyde 3. Various samples of diluted Microshield products 4. Fragrance mix 1, Balsam of Peru-? relevance 5. Chloroacetamide-Redwin sorbolene lotionpast relevance 6. Compositae- no relevance Latex RAST-negative IgE 133 (<87)
26 Final diagnoses 1. Allergic contact dermatitis to coconut diethanolamide in various Microshield products 2. Allergic contact dermatitis to formaldehyde in Microshield Angel hand gel 3. Irritant contact dermatitis from wet work 4. Contact allergy to fragrance-possible relevance 5. Contact allergy to chloroacetamide-past relevance
27 This is complicated! But we do need to list all factors possibly contributing to a skin condition, in order to ensure optimum outcomes for patients We are making a diagnosis of our patient s skin condition using patch testing as one of the techniques in diagnosis Other information may be obtained from prick/rast testing
 LARGEST INDUSTRY GROUP")


28 Impact of occupational skin disease (OSD) LARGEST INDUSTRY GROUP Healthcare and social assistance Quality of life Ability to work Direct costs PREVENTION IS A PRIORITY Public health & infection control Indirect costs

 Prevalence 17-50% worldwide, with rates of up to 65% in")
29 Healthcare workers (HCWs) a high risk group for occupational skin disease Lots of exposure to irritants and allergens Hand hygiene requirements PPE gloves, sweating Cleaning/disinfectants, washing Tools of the trade (eg acrylates dentists) Prevalence 17-50% worldwide, with rates of up to 65% in ICU/NICU

30
31 685 HCWs assessed in our tertiary clinic over 22 years 555 HCWs diagnosed with a work-related skin disorder ( study group ) 72.0% nurses 11.2% doctors /medical scientists 8.1% dental practitioners and asistants
32 Primary site of dermatitis Study group (N=555) Primary site of dermatitis on examination n (%)* Hands 497 (89.5) Arms 72 (13.0) Face 55 (9.9) Legs 18 (3.2) Eyelids 17 (3.1) Neck 14 (2.5) Feet 9 (1.6) Chest 7 (1.3) Back 5 (0.9) Oral/lips 4 (0.7) Abdomen 3 (0.5) Generalized 2 (0.4) * Patients could have multiple primary sites of dermatitis, therefore total exceeds number of patients.
33 Most frequent diagnoses in 555 HCWs with a work-related skin disorder (>1) 79 % Irritant contact dermatitis 50 % Allergic contact dermatitis 37 % Endogenous eczema 13 % Latex allergy 4 % Contact urticaria (excluding latex allergy) 65 % Multiple diagnoses 27 % Had lost time from work
34 Major occupational irritants Among 439 HCWs with ICD Water and wet work 60 % Hand cleansers/soaps 39 % Heat and sweating 14 % (the diagnosis of ICD is subjective, no testing is available)
35 Major occupational allergens (237 ACD) 25 most frequent occupational allergens in HCWs with occupational ACD Relevant reactions n Proportion of total tested % ALLERGEN Total tested n Thiuram mix Tetraethylthiuram disulfide Formaldehyde Coconut diethanolamide Dipentamethylenethiuram disulfide Dowicil TM 200 (quaternium 15) Tetramethylthiuram monosulfide Tetramethylthiuram disulfide Methylchloroisothiazolinone Fragrance mix Chlorhexidine diacetate Chlorhexidine digluconate Methylisothiazolinone Amerchol L Lanolin alcohol Germall 115 (imidazolidinylurea) Germall II (diazolidinylurea) Hydroxyethyl methacrylate Glutaraldehyde Zinc diethyldithiocarbamate DMDM Hydantoin Methyl methacrylate Nickel sulfate Myroxolon pereriae Carba mix
36 Major occupational allergens (237) (i) Rubber accelerators Thiurams > carbamates 5 thiurams in the top 10 most common allergens Thiuram allergy - marked downward trend during the study period Annual change in occupational ACD to thiuram mix, N=49.

37 The glove you need to know about! Ansell Micro Touch Nitra-free is accelerator free PINK

38 Accelerator-free surgical glove Ansell Gammex Non-Latex Sensitive
 Latex allergy Down trending during the study")

39 Major occupational allergens (ii) Latex allergy Down trending during the study period Peaked in 1999 Coming down last few years but still occurs % 60% 50% 40% 30% 20% 10% 0% Absolute number Annual rate Annual change in occupational latex allergy, N=72


40 Major occupational allergens (iii) Preservatives Formaldehyde Formaldehyde-releasers: o Imidazolidinyl urea o Diazolididnyl urea o Quaternium 15 o DMDM hydantoin Methylisothiazolinone Methylchloroisothiazolinonen(MIT) Ecolab Glad Hands MIT Microshield Angel Hand Gel Diazolidinyl urea Johnson s Baby Top-to-Toe Bath MIT Johnson s Baby Shampoo MIT
41 New epidemic of contact allergy! Methylisothiazolinone (MI) in baby wipes, skin cleansers, sorbolene lotions, shampoos, deoderants, facial wipes, paints Methylchloroisothiazolininone (MCI)/MI used formerly 15ppm, 3:1 dilution, MI 3.75ppm Since 2005, MI allowable to 100pm Worldwide epidemic Mainly non-occupational especially carers of babies, but also in some hand cleaners, paints
42 Be very suspicious of products containing MI Percentage of total patients patch tested with a positive reaction at SCF % % % % % % % Boyapati A, Tate B, Tam M, Nixon R. Allergic contact dermatitis from methylisothiazolinone: exposure from baby wipes causing hand dermatitis in carers. Australas J Dermatol 2013 Cahill J Toholka R Palmer A Nixon R Med J Aust 2014


43 Allergic contact dermatitis to MI in a facial wipe


44 Major occupational allergens (iv) Excipients in hand cleaners Coconut DEA Lanolin ANTISEPTICS Chlorhexidine Glutaraldehyde Microshield Skin Care Cleanser Lanolin Coconut DEA Microshield Handrub Lanolin Chlorhexidine digluconate Hard to avoid allergens
45 5 hand cleansers among the top 30 causes of ACD 45 Microshield Handwash Mild Neutral Formula ph7 Microshield 4 Chlorhexidine Skin Cleanser Microshield 2 Chlorhexidine Skin Cleanser Ecolab Glad Hands Concentrated Lotion Skin Cleanser RELEVANT REACTIONS n TOTAL TESTED n PROPORTION OF TOTAL TESTED % Microshield Skincare Cleanser ph NB Microshield most common brand of cleanser used in Australian hospitals
46 Hand cleansers vs alcohol-based hand rubs (ABHRs) ACD caused by hand cleansers 8 x rate from ABHRs (12.4 % vs 1.6 %) Hand cleansers major cause of ICD Hand cleansers often being used when ABHRs indicated ABHRs sting on broken skin often misinterpreted as allergy
47 Reported previously... Graham M, Nixon R, Burrell L J, Bolger C, Johnson P D R, Grayson M L. Low rates of cutaneous adverse reactions to alcoholbased hand hygiene solution during prolonged use in a large teaching hospital. Antimicrobial Agents and Chemotherapy 2005; 49:
48 Conclusions ABHRs caused substantially less ACD and less ICD than commercial hand cleansers Stinging allergy! Appreciable number of reactions to so called hard-to-avoid weak allergens present in commercial hand cleaners Rubber glove chemicals trending down Latex allergy trending down High rates of occupational ACD to MI OSD presents a significant burden of disease in Australian HCWs
49 49 SO WHAT CAN WE DO??
50 Individual level Primary prevention - EDUCATION Early management of symptoms Secondary prevention Allergen avoidance and substition Accelerator-free gloves Manufacturer level Mandatory labelling Allergen substitution responding to the evidence Accurate MSDS Management level and beyond Promoting ABHRs instead of hand cleansers where indicated Integrating skin care education with hand hygiene training Overarching national guidelines National OSD registry
51 51 Safework Australia supported the development of skin care within the hand hygiene module Integrating skin care education with hand hygiene training. Healthcare workers - Occupational Dermatitis and Skin Care
52
53 Conclusions Contact dermatitis is not uncommon in HCW Implement skin care measures, particularly with use of moisturiser after work See Hand Hygiene Module However, if problems persist, need to make a diagnosis Establish referral system: Infection Control; Dermatology Units for initial assessment Referral for patch testing may be indicated

54 Thanks for listening! Special thanks to Amanda Palmer Rosemary Nixon
Index. derm.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A ACD. See Allergic contact dermatitis. Acute and recurrent vesicular hand dermatitis, 337 353 Airborne contact dermatitis, 303 Allergen avoidance
Note: Page numbers of article titles are in boldface type. A ACD. See Allergic contact dermatitis. Acute and recurrent vesicular hand dermatitis, 337 353 Airborne contact dermatitis, 303 Allergen avoidance
Contact Dermatitis Challenges for the General Dermatologist. Susan Nedorost, MD
 Contact Dermatitis Challenges for the General Dermatologist Susan Nedorost, MD Contact Dermatitis: Challenges for the General Dermatologist Disclosure Statement I, Susan Nedorost, MD, do not have any relevant
Contact Dermatitis Challenges for the General Dermatologist Susan Nedorost, MD Contact Dermatitis: Challenges for the General Dermatologist Disclosure Statement I, Susan Nedorost, MD, do not have any relevant
A Resource Kit for Career Counsellors
 A Resource Kit for Career Counsellors Occupational Dermatology Research and Education Centre www.occderm.asn.au/skinatwork 2 About this kit The Skin @ Work education kit aims to raise awareness of a potential
A Resource Kit for Career Counsellors Occupational Dermatology Research and Education Centre www.occderm.asn.au/skinatwork 2 About this kit The Skin @ Work education kit aims to raise awareness of a potential
Occupational dermatitis in hairdressers influence of individual and environmental factors
 Contact Dermatitis Original Article COD Contact Dermatitis Occupational dermatitis in hairdressers influence of individual and environmental factors Tanja K. Carøe 1, Niels E. Ebbehøj 1 and Tove Agner
Contact Dermatitis Original Article COD Contact Dermatitis Occupational dermatitis in hairdressers influence of individual and environmental factors Tanja K. Carøe 1, Niels E. Ebbehøj 1 and Tove Agner
Dermatitis. Occupational aspects of management
 Dermatitis Occupational aspects of management Evidence-based guidance for healthcare professionals Introduction This leaflet summarises the findings from a review of the published scientific literature
Dermatitis Occupational aspects of management Evidence-based guidance for healthcare professionals Introduction This leaflet summarises the findings from a review of the published scientific literature
Identifying the causes of contact dermatitis
 Identifying the causes of contact Jones R, Horn H M. Identifying the causes of contact. Practitioner 2014;258 (1772)27-31 Dr Ruth Jones MRCP ST3 Dermatology Dr Helen M. Horn MD FRCP Associate Specialist
Identifying the causes of contact Jones R, Horn H M. Identifying the causes of contact. Practitioner 2014;258 (1772)27-31 Dr Ruth Jones MRCP ST3 Dermatology Dr Helen M. Horn MD FRCP Associate Specialist
Essentials of Contact Dermatitis 2018
 Essentials of Contact Dermatitis 2018 Joseph F. Fowler Jr. MD Clinical Professor of Dermatology U. Of Louisville Pres. No. American Contact Dermatitis Group Disclosures Consultant and speaker, SmartPractice
Essentials of Contact Dermatitis 2018 Joseph F. Fowler Jr. MD Clinical Professor of Dermatology U. Of Louisville Pres. No. American Contact Dermatitis Group Disclosures Consultant and speaker, SmartPractice
Clinico Pathological Test SCPA605-Essential Pathology
 Clinico Pathological Test SCPA605-Essential Pathology Somphong Narkpinit, M.D. Department of Pathogbiology, Faculty of Science, Mahidol University e-mail : somphong.nar@mahidol.ac.th Pathogenesis of allergic
Clinico Pathological Test SCPA605-Essential Pathology Somphong Narkpinit, M.D. Department of Pathogbiology, Faculty of Science, Mahidol University e-mail : somphong.nar@mahidol.ac.th Pathogenesis of allergic
GLOVE ALLERGIES AND HAND HEALTH
 GLOVE ALLERGIES AND HAND HEALTH INTRODUCTION Skin conditions caused by chemical, physical or biological agents in the workplace are common among disposable glove wearers in the industrial sector. Understanding
GLOVE ALLERGIES AND HAND HEALTH INTRODUCTION Skin conditions caused by chemical, physical or biological agents in the workplace are common among disposable glove wearers in the industrial sector. Understanding
6. Contact allergic reactions in patients with atopic eczema
 Acta Derm Venereol 2005; Suppl. 215: 28 32 6. Contact allergic reactions in patients with atopic eczema JOHN MCFADDEN Medicament allergy is a not uncommon problem both with antibiotics and topical corticosteroids.
Acta Derm Venereol 2005; Suppl. 215: 28 32 6. Contact allergic reactions in patients with atopic eczema JOHN MCFADDEN Medicament allergy is a not uncommon problem both with antibiotics and topical corticosteroids.
Skin Reactions to Xenobiotics Ola Bergendorff
 Skin Reactions to Xenobiotics Ola Bergendorff Department of Occupational Dermatology University Hospital Malmö This lecture has been prepared with help from Associate Professors Malin Engfeldt and Cecilia
Skin Reactions to Xenobiotics Ola Bergendorff Department of Occupational Dermatology University Hospital Malmö This lecture has been prepared with help from Associate Professors Malin Engfeldt and Cecilia
CHAPTER 1. Eczema Basics
 CHAPTER 1 Eczema Basics Definition Eczema is an inflammatory skin condition, characterised by ichtyosis (dry skin), erythema (redness), excoriation (interruption of the skin), scratching lesions, lichenification
CHAPTER 1 Eczema Basics Definition Eczema is an inflammatory skin condition, characterised by ichtyosis (dry skin), erythema (redness), excoriation (interruption of the skin), scratching lesions, lichenification
Latex Allergy - the Australian experience Where are we now Prof CH Katelaris University of Western Sydney and Campbelltown Hospital
 Latex Allergy - the Australian experience Where are we now Prof CH Katelaris University of Western Sydney and Campbelltown Hospital Latex conf Dec Latex Allergy - Australian Experience Clinical studies
Latex Allergy - the Australian experience Where are we now Prof CH Katelaris University of Western Sydney and Campbelltown Hospital Latex conf Dec Latex Allergy - Australian Experience Clinical studies
LATEX ALLERGY ASCIA Education Resources patient information
 LATEX ALLERGY ASCIA Education Resources patient information Allergies to latex rubber have only been recognised in the last 20 years. The reasons are uncertain, although increased use of latex gloves in
LATEX ALLERGY ASCIA Education Resources patient information Allergies to latex rubber have only been recognised in the last 20 years. The reasons are uncertain, although increased use of latex gloves in
Practical Patch Testing and Chemical Allergens in Contact Dermatitis
 Practical Patch Testing and Chemical Allergens in Contact Dermatitis Sharon E. Jacob Elise M. Herro Practical Patch Testing and Chemical Allergens in Contact Dermatitis Sharon E. Jacob Division of Dermatology
Practical Patch Testing and Chemical Allergens in Contact Dermatitis Sharon E. Jacob Elise M. Herro Practical Patch Testing and Chemical Allergens in Contact Dermatitis Sharon E. Jacob Division of Dermatology
DRY HANDS SAFETY BRIEFING
 DRY HANDS HOW DRY HANDS POSITIVELY AFFECT PERFORMANCE Providing a glove solution that keeps hands dry will deliver superior worker comfort, leading to greater productivity, and improve workplace safety
DRY HANDS HOW DRY HANDS POSITIVELY AFFECT PERFORMANCE Providing a glove solution that keeps hands dry will deliver superior worker comfort, leading to greater productivity, and improve workplace safety
Contact Dermatitis In Atopic Patients
 Contact Dermatitis In Atopic Patients Jenny Murase, MD Palo Alto Foundation Medical Group Director of Patch Testing University of California, San Francisco Associate Clinical Professor Disclosures Consultant
Contact Dermatitis In Atopic Patients Jenny Murase, MD Palo Alto Foundation Medical Group Director of Patch Testing University of California, San Francisco Associate Clinical Professor Disclosures Consultant
Allergic contact dermatitis caused by cocamide diethanolamine
 Contact Dermatitis Original Article COD Contact Dermatitis Allergic contact dermatitis caused by cocamide diethanolamine Sarien Mertens, Liesbeth Gilissen and An Goossens Department of Dermatology, University
Contact Dermatitis Original Article COD Contact Dermatitis Allergic contact dermatitis caused by cocamide diethanolamine Sarien Mertens, Liesbeth Gilissen and An Goossens Department of Dermatology, University
Children s Hospital Of Wisconsin
 Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
What to do when patch testing is negative?
 What to do when patch testing is negative? Christen M. Mowad MD Clinical Professor of Dermatology Geisinger Medical Center Danville, PA 17821 cmowad@geisinger.edu I have no disclosures. What to do when
What to do when patch testing is negative? Christen M. Mowad MD Clinical Professor of Dermatology Geisinger Medical Center Danville, PA 17821 cmowad@geisinger.edu I have no disclosures. What to do when
An Everyday Guide to Eczema
 An Everyday Guide to Eczema By Dr. Kristel Polder, Board-Certified Dermatologist Developed in Partnership with Who is affected by eczema? 32 million people in the US 1 in 5 children 1 in 12 adults *www.eczema.org
An Everyday Guide to Eczema By Dr. Kristel Polder, Board-Certified Dermatologist Developed in Partnership with Who is affected by eczema? 32 million people in the US 1 in 5 children 1 in 12 adults *www.eczema.org
METHYLISOTHIAZOLINONE AND METHYLCHLOROISOTHIAZOLINONE: NEW INSIGHTS
 METHYLISOTHIAZOLINONE AND METHYLCHLOROISOTHIAZOLINONE: NEW INSIGHTS *Ana Rita Rodrigues-Barata, Luis Conde-Salazar Contact Dermatitis Unit, Department of Dermatology, Grupo Dermatología Pedro Jaén, Madrid,
METHYLISOTHIAZOLINONE AND METHYLCHLOROISOTHIAZOLINONE: NEW INSIGHTS *Ana Rita Rodrigues-Barata, Luis Conde-Salazar Contact Dermatitis Unit, Department of Dermatology, Grupo Dermatología Pedro Jaén, Madrid,
A Guide to Cutaneous Allergy. Dr David Orton Consultant Dermatologist The Hillingdon Hospitals NHS Foundation Trust
 A Guide to Cutaneous Allergy Dr David Orton Consultant Dermatologist The Hillingdon Hospitals NHS Foundation Trust Allergy inappropriate/exaggerated defence reaction to something that is not innately harmful
A Guide to Cutaneous Allergy Dr David Orton Consultant Dermatologist The Hillingdon Hospitals NHS Foundation Trust Allergy inappropriate/exaggerated defence reaction to something that is not innately harmful
Long-term outcome of 160 adult patients with natural rubber latex allergy
 Long-term outcome of 160 adult patients with natural rubber latex allergy Kristiina Turjanmaa, MD, a Mikko Kanto, CM, a Hannu Kautiainen, BA, b Timo Reunala, MD, a and Timo Palosuo, MD c Tampere, Heinola,
Long-term outcome of 160 adult patients with natural rubber latex allergy Kristiina Turjanmaa, MD, a Mikko Kanto, CM, a Hannu Kautiainen, BA, b Timo Reunala, MD, a and Timo Palosuo, MD c Tampere, Heinola,
Clinical Study Methylchloroisothiazolinone/Methylisothiazolinone and Methylisothiazolinone Sensitivity in Hungary
 Dermatology Research and Practice Volume 2016, Article ID 4579071, 5 pages http://dx.doi.org/10.1155/2016/4579071 Clinical Study Methylchloroisothiazolinone/Methylisothiazolinone and Methylisothiazolinone
Dermatology Research and Practice Volume 2016, Article ID 4579071, 5 pages http://dx.doi.org/10.1155/2016/4579071 Clinical Study Methylchloroisothiazolinone/Methylisothiazolinone and Methylisothiazolinone
ATOPIC ECZEMA. What are the aims of this leaflet?
 ATOPIC ECZEMA What are the aims of this leaflet? This leaflet has been written to help you understand more about atopic eczema. It tells you what it is, what causes it, what can be done about it, and where
ATOPIC ECZEMA What are the aims of this leaflet? This leaflet has been written to help you understand more about atopic eczema. It tells you what it is, what causes it, what can be done about it, and where
Safety First Plus. Safety, Health and Environment (SHE) Prevention of Work Related Skin Disease. Maritime Submarines SAFETY FIRST PLUS
 Prevention of Work Related Skin Disease. Maritime Submarines SAFETY FIRST PLUS") Safety First Plus Safety, Health and Environment (SHE) Prevention of Work Related Skin Disease Maritime Submarines THINK SAFE. ACT SAFE. BE SAFE Prevention of Work Related Skin Disease 2013 WHAT IS SKIN
Safety First Plus Safety, Health and Environment (SHE) Prevention of Work Related Skin Disease Maritime Submarines THINK SAFE. ACT SAFE. BE SAFE Prevention of Work Related Skin Disease 2013 WHAT IS SKIN
Allergic versus Contact
 Allergic versus Contact Dermatitis Julie Sterbank, DO Assistant Clinical Professor Allergy/Immunology MetroHealth Medical Center/Case Western Reserve University Disclosure I have no financial disclosures
Allergic versus Contact Dermatitis Julie Sterbank, DO Assistant Clinical Professor Allergy/Immunology MetroHealth Medical Center/Case Western Reserve University Disclosure I have no financial disclosures
Occupational dermatitis in hairdressers: do they claim workers compensation?
 Contact Dermatitis Original Article COD Contact Dermatitis Occupational dermatitis in hairdressers: do they claim workers compensation? Georgina Lyons 1, Tessa Keegel 2,3, Amanda Palmer 1 and Rosemary
Contact Dermatitis Original Article COD Contact Dermatitis Occupational dermatitis in hairdressers: do they claim workers compensation? Georgina Lyons 1, Tessa Keegel 2,3, Amanda Palmer 1 and Rosemary
Texas Children's Hospital Dermatology Service PCP Referral Guidelines- Atopic Dermatitis (AD)
") Diagnosis: ATOPIC DERMATITIS (AD) Texas Children's Hospital Dermatology Service PCP Referral Guidelines- Atopic Dermatitis (AD) PATIENT ADVICE: Unfortunately, there is no cure for atopic dermatitis, so
Diagnosis: ATOPIC DERMATITIS (AD) Texas Children's Hospital Dermatology Service PCP Referral Guidelines- Atopic Dermatitis (AD) PATIENT ADVICE: Unfortunately, there is no cure for atopic dermatitis, so
SKIN CARE AND PREVENTION AND MANAGEMENT OF WORK RELATED DERMATITIS
 SKIN CARE AND PREVENTION AND MANAGEMENT OF WORK RELATED DERMATITIS Version No. Date Comments Date Author/s Approved by Amended Approved 1. 10/10/2011 LCP/GC LCP Skin care & prevention of work related dermatitis
SKIN CARE AND PREVENTION AND MANAGEMENT OF WORK RELATED DERMATITIS Version No. Date Comments Date Author/s Approved by Amended Approved 1. 10/10/2011 LCP/GC LCP Skin care & prevention of work related dermatitis
What is an allergy? Who gets allergies?
 ALLERGY Allergic disorders are on the increase both in this country and across Europe, affecting between 10 and 30% of the population. Allergies come in many forms, ranging from eczema, asthma, hay fever,
ALLERGY Allergic disorders are on the increase both in this country and across Europe, affecting between 10 and 30% of the population. Allergies come in many forms, ranging from eczema, asthma, hay fever,
Constitutional eczema
 Patient information Constitutional eczema What is constitutional eczema? Constitutional eczema, also called atopic eczema, is a form of eczema that mainly occurs in childhood. Eczema usually starts before
Patient information Constitutional eczema What is constitutional eczema? Constitutional eczema, also called atopic eczema, is a form of eczema that mainly occurs in childhood. Eczema usually starts before
Eczema. Most kids get itchy rashes at one time or another. But eczema can be a nuisance that may prompt scratching that makes the problem worse.
 KidsHealth.org The most-visited site devoted to children's health and development Eczema Most kids get itchy rashes at one time or another. But eczema can be a nuisance that may prompt scratching that
KidsHealth.org The most-visited site devoted to children's health and development Eczema Most kids get itchy rashes at one time or another. But eczema can be a nuisance that may prompt scratching that
Atopic Eczema with detail on how to apply wet wraps
 Atopic Eczema with detail on how to apply wet wraps Dr Carol Hlela Consultant Dermatologist Head of Unit, Department of Dermatology, Paediatrics Red Cross Children s Hospital, UCT Red Cross War Memorial
Atopic Eczema with detail on how to apply wet wraps Dr Carol Hlela Consultant Dermatologist Head of Unit, Department of Dermatology, Paediatrics Red Cross Children s Hospital, UCT Red Cross War Memorial
PROTECT YOURSELF FROM TYPE I ALLERGIES.
 PROTECT YOURSELF FROM TYPE I ALLERGIES. 1 PROTECT YOURSELF FROM TYPE I ALLERGIES. Occasionally wearing glove products can cause issues with the health of our skin. This predominantly manifests itself in
PROTECT YOURSELF FROM TYPE I ALLERGIES. 1 PROTECT YOURSELF FROM TYPE I ALLERGIES. Occasionally wearing glove products can cause issues with the health of our skin. This predominantly manifests itself in
What you need to know about ECZEMA
 What you need to know about ECZEMA The Irish Skin Foundation is a national charity with a mission to improve quality of life for people with skin conditions, promote skin health and the prevention of skin
What you need to know about ECZEMA The Irish Skin Foundation is a national charity with a mission to improve quality of life for people with skin conditions, promote skin health and the prevention of skin
What you need to know about ECZEMA
 What you need to know about ECZEMA The Irish Skin Foundation is a national charity with a mission to improve quality of life for people with skin conditions, promote skin health and the prevention of skin
What you need to know about ECZEMA The Irish Skin Foundation is a national charity with a mission to improve quality of life for people with skin conditions, promote skin health and the prevention of skin
BOHRF BOHRF BOHRF BOHRF
 Occupational Contact Dermatitis and Urticaria A Guide for General Practitioners and Practice Nurses March 2010 British Occupational Health Research Foundat ion This leaflet summarises the key evidence
Occupational Contact Dermatitis and Urticaria A Guide for General Practitioners and Practice Nurses March 2010 British Occupational Health Research Foundat ion This leaflet summarises the key evidence
LATEX ALLERGIES. As with many other natural products, natural rubber latex contains proteins to which some individuals may develop an allergy.
 What is Natural Rubber Latex? LATEX ALLERGIES Natural rubber latex (NRL) is a milky fluid obtained from the Heva barsiliensis tree, which is widely grown in South East Asia and other countries. NRL is
What is Natural Rubber Latex? LATEX ALLERGIES Natural rubber latex (NRL) is a milky fluid obtained from the Heva barsiliensis tree, which is widely grown in South East Asia and other countries. NRL is
ALLERGIC CONTACT DERMATITIS IN ATOPICS. Catalina Matiz MD Assistant Professor University of California San Diego Rady Children s Hospital San Diego
 ALLERGIC CONTACT DERMATITIS IN ATOPICS Catalina Matiz MD Assistant Professor University of California San Diego Rady Children s Hospital San Diego When to suspect Allergic contact dermatitis? Look for
ALLERGIC CONTACT DERMATITIS IN ATOPICS Catalina Matiz MD Assistant Professor University of California San Diego Rady Children s Hospital San Diego When to suspect Allergic contact dermatitis? Look for
GUIDE TO... Latex allergy. Learning outcomes. This guide is supported by an educational grant from
 GUIDE Janet Pickles is Chairwoman, RA Medical Services Ltd, Steeton, West Yorkshire Email: janet@ramedical.com TO... Learning outcomes After reading this Guide to Latex Allergy you should: n Understand
GUIDE Janet Pickles is Chairwoman, RA Medical Services Ltd, Steeton, West Yorkshire Email: janet@ramedical.com TO... Learning outcomes After reading this Guide to Latex Allergy you should: n Understand
Understanding. Atopic Dermatitis. National Jewish Health. An educational health series from
 Understanding Atopic Dermatitis An educational health series from National Jewish Health If you would like further information about National Jewish Health, please write to: National Jewish Health 1400
Understanding Atopic Dermatitis An educational health series from National Jewish Health If you would like further information about National Jewish Health, please write to: National Jewish Health 1400
Professor Rohan Ameratunga Clinical Immunologist and Allergist Auckland
 Professor Rohan Ameratunga Clinical Immunologist and Allergist Auckland 16:30-17:25 WS #170: Eczema Management 17:35-18:30 WS #182: Eczema Management (Repeated) Managing ECZEMA A/Prof Rohan Ameratunga
Professor Rohan Ameratunga Clinical Immunologist and Allergist Auckland 16:30-17:25 WS #170: Eczema Management 17:35-18:30 WS #182: Eczema Management (Repeated) Managing ECZEMA A/Prof Rohan Ameratunga
Learning Circle: Jan 26, 2011 Childhood Eczema
 Learning Circle: Jan 26, 2011 Childhood Eczema Wingfield Rehmus, MD MPH BC Children s Hospital Clinical Assistant Professor, UBC Department of Paediatrics Associate Member, UBC Department of Dermatology
Learning Circle: Jan 26, 2011 Childhood Eczema Wingfield Rehmus, MD MPH BC Children s Hospital Clinical Assistant Professor, UBC Department of Paediatrics Associate Member, UBC Department of Dermatology
OCCUPATIONAL CONTACT DERMATITIS IN A TERTIARY CARE CENTRE EPIDEMIOLOGY, CLINICAL PROFILE AND PATCH TEST EVALUATION
 OCCUPATIONAL CONTACT DERMATITIS IN A TERTIARY CARE CENTRE EPIDEMIOLOGY, CLINICAL PROFILE AND PATCH TEST EVALUATION DONE BY : Dr.Ragini Rajan Final year Post Graduate MD(DVL) Govt.Stanley Medical College,
OCCUPATIONAL CONTACT DERMATITIS IN A TERTIARY CARE CENTRE EPIDEMIOLOGY, CLINICAL PROFILE AND PATCH TEST EVALUATION DONE BY : Dr.Ragini Rajan Final year Post Graduate MD(DVL) Govt.Stanley Medical College,
Patch Testing interactive workshop. Susan Nedorost, MD
 Patch Testing interactive workshop Susan Nedorost, MD Disclosure Statement I, Susan Nedorost, MD, do not have any relevant financial interest or other relationships with a commercial entity producing health-care
Patch Testing interactive workshop Susan Nedorost, MD Disclosure Statement I, Susan Nedorost, MD, do not have any relevant financial interest or other relationships with a commercial entity producing health-care
Dental surgeons with natural rubber latex allergy: a report of 20 cases
 Occup. od. Vol. 49,. 2, pp. 103-107, 1999 Copyright C 1999 LJpptncott Williams 4 WilkJns for SO Printed In Great Britain. AH rights reserved 0962-7480/99 Dental surgeons with natural rubber latex allergy:
Occup. od. Vol. 49,. 2, pp. 103-107, 1999 Copyright C 1999 LJpptncott Williams 4 WilkJns for SO Printed In Great Britain. AH rights reserved 0962-7480/99 Dental surgeons with natural rubber latex allergy:
STUDY. Changing Trends and Allergens in the Patch Test Standard Series
 STUDY Changing Trends and Allergens in the Patch Test Standard Series A Mayo Clinic 5-Year Retrospective Review, January 1, 2001, Through December 31, 2005 Mark D. P. Davis, MD; Leigh Ann Scalf, MD; James
STUDY Changing Trends and Allergens in the Patch Test Standard Series A Mayo Clinic 5-Year Retrospective Review, January 1, 2001, Through December 31, 2005 Mark D. P. Davis, MD; Leigh Ann Scalf, MD; James
Pediatric Dermatology. Wingfield Rehmus, MD MPH BC Children s Hospital
 Pediatric Dermatology Wingfield Rehmus, MD MPH BC Children s Hospital Conflict of interest! No financial conflict of interest! Individual products shown are examples only not a product endorsement Pediatric
Pediatric Dermatology Wingfield Rehmus, MD MPH BC Children s Hospital Conflict of interest! No financial conflict of interest! Individual products shown are examples only not a product endorsement Pediatric
Kelly H. Tyler, MD, FACOG, FAAD S052 Gender Dermatology: Diagnosis and Treatment of Genital Skin Disorders Vulvar Dermatitis
 Vulvar Dermatitis Kelly H. Tyler, MD, FACOG, FAAD Assistant Professor The Ohio State University Department of Internal Medicine, Division of Dermatology Department of Obstetrics and Gynecology Center for
Vulvar Dermatitis Kelly H. Tyler, MD, FACOG, FAAD Assistant Professor The Ohio State University Department of Internal Medicine, Division of Dermatology Department of Obstetrics and Gynecology Center for
過敏病科中心. Allergy Centre. Eczema. Allergy Centre 過敏病科中心. Allergy Centre. For enquiries and appointments, please contact us at:
 Allergy Centre 過敏病科中心 Eczema For enquiries and appointments, please contact us at: Allergy Centre 9/F, Li Shu Pui Block Hong Kong Sanatorium & Hospital 2 Village Road, Happy Valley, Hong Kong Tel: 2835
Allergy Centre 過敏病科中心 Eczema For enquiries and appointments, please contact us at: Allergy Centre 9/F, Li Shu Pui Block Hong Kong Sanatorium & Hospital 2 Village Road, Happy Valley, Hong Kong Tel: 2835
Products that contain medications that the FDA calls drugs will list Drug Facts on the label and may include:
 Topical Over-The-Counter (OTC) Medications All content must be TAUGHT by nurses or staff with current DODD Category 1 Certification. TEACH. DO NOT give to personnel to just read. OVERVIEW Most drugs can
Topical Over-The-Counter (OTC) Medications All content must be TAUGHT by nurses or staff with current DODD Category 1 Certification. TEACH. DO NOT give to personnel to just read. OVERVIEW Most drugs can
Workers compensation claims for Occupational Contact Dermatitis: 20 years of data from Victoria, Australia
 Workers compensation claims for Occupational Contact Dermatitis: 20 years of data from Victoria, Australia T Keegel, O Black, R Stuckey, E MacFarlane, R Nixon, M Sim www.coeh.monash.org Background Occupational
Workers compensation claims for Occupational Contact Dermatitis: 20 years of data from Victoria, Australia T Keegel, O Black, R Stuckey, E MacFarlane, R Nixon, M Sim www.coeh.monash.org Background Occupational
Contamination versus Preservation
 Contamination versus Preservation Michael Dyrgaard Lundov Ph.D.-student, Cand.Scient. National Allergy Research Centre and Pharmaceutical Faculty, University of Copenhagen Allergic contact dermatitis to
Contamination versus Preservation Michael Dyrgaard Lundov Ph.D.-student, Cand.Scient. National Allergy Research Centre and Pharmaceutical Faculty, University of Copenhagen Allergic contact dermatitis to
Hand contact dermatitis in hairdressers: clinical and causative allergens, experience in Bangkok
 Original article Hand contact dermatitis in hairdressers: clinical and causative allergens, experience in Bangkok Poohglin Tresukosol and Chanutta Swasdivanich Summary Background: Hand dermatitis in hairdressers
Original article Hand contact dermatitis in hairdressers: clinical and causative allergens, experience in Bangkok Poohglin Tresukosol and Chanutta Swasdivanich Summary Background: Hand dermatitis in hairdressers
Update and Review of Common Occupational Skin Diseases
 Update and Review of Common Occupational Skin Diseases Susan Y. Chon, M.D. Associate Professor Department of Dermatology UT MD Anderson Cancer Center Disclosure Statement I have no financial disclosures
Update and Review of Common Occupational Skin Diseases Susan Y. Chon, M.D. Associate Professor Department of Dermatology UT MD Anderson Cancer Center Disclosure Statement I have no financial disclosures
La sicurezza e la tollerabilità (sterilità dei disinfettanti, i pericoli allergici e tossici dei prodotti)
") Milano, 7 novembre 2017 La sicurezza e la tollerabilità (sterilità dei disinfettanti, i pericoli allergici e tossici dei prodotti) Alessandra Toletone Dipartimento Scienze della Salute Scuola di Scienze
Milano, 7 novembre 2017 La sicurezza e la tollerabilità (sterilità dei disinfettanti, i pericoli allergici e tossici dei prodotti) Alessandra Toletone Dipartimento Scienze della Salute Scuola di Scienze
The skin acts as a protective barrier against a number of hazards within our environment. These hazards can be:
 The skin acts as a protective barrier against a number of hazards within our environment. These hazards can be: chemical, e.g: acids, alkalis, solvents, cutting, or soluble oils; biological,e.g: bacteria,plant
The skin acts as a protective barrier against a number of hazards within our environment. These hazards can be: chemical, e.g: acids, alkalis, solvents, cutting, or soluble oils; biological,e.g: bacteria,plant
The relevance of chlorhexidine contact allergy
 Contact Dermatitis Original Article COD Contact Dermatitis The relevance of chlorhexidine contact allergy Jussi Liippo 1,Päivi Kousa 2 and Kaija Lammintausta 1 1 Department of Dermatology, Turku University
Contact Dermatitis Original Article COD Contact Dermatitis The relevance of chlorhexidine contact allergy Jussi Liippo 1,Päivi Kousa 2 and Kaija Lammintausta 1 1 Department of Dermatology, Turku University
RELEVANT DISCLOSURES ATOPIC DERMATITIS / ECZEMA MANAGING ECZEMA IN INFANTS AND CHILDREN
 RELEVANT DISCLOSURES MANAGING ECZEMA IN INFANTS AND CHILDREN Advisory board member - MEDA (Elidel), Speaking honoraria Bayer (Advantan) Advisory board, consultant, speaker: Pfizer, Abbvie, Janssen, Elli
RELEVANT DISCLOSURES MANAGING ECZEMA IN INFANTS AND CHILDREN Advisory board member - MEDA (Elidel), Speaking honoraria Bayer (Advantan) Advisory board, consultant, speaker: Pfizer, Abbvie, Janssen, Elli
It s all in your hands: Preventing hand dermatitis. Introduction 3/5/2018. Hand hygiene is a cornerstone of effective infection control, but
 It s all in your hands: Preventing hand dermatitis Monica Herrera MHA, CDMP Introduction Hand hygiene is a cornerstone of effective infection control, but Hand sanitization and gloving are essential if
It s all in your hands: Preventing hand dermatitis Monica Herrera MHA, CDMP Introduction Hand hygiene is a cornerstone of effective infection control, but Hand sanitization and gloving are essential if
Diagnosis and Management of Common and Infective Skin Diseases in Children at primary care level
 Diagnosis and Management of Common and Infective Skin Diseases in Children at primary care level Dr Ng Su Yuen Paediatrician and Paediatric Dermatologist Hospital Pulau Pinang Outline Common inflammatory
Diagnosis and Management of Common and Infective Skin Diseases in Children at primary care level Dr Ng Su Yuen Paediatrician and Paediatric Dermatologist Hospital Pulau Pinang Outline Common inflammatory
Food Allergy Testing and Guidelines
 Food Allergy Testing and Guidelines Dr Gosia Skibinska Primary Care Allergy Training Day, 15 th October 2011 Food Allergy Testing and Guidelines Food allergy Testing Guidelines Cases Food Allergy NICE
Food Allergy Testing and Guidelines Dr Gosia Skibinska Primary Care Allergy Training Day, 15 th October 2011 Food Allergy Testing and Guidelines Food allergy Testing Guidelines Cases Food Allergy NICE
Drug allergy and Skin Disorders. Timothy Craig, DO, FACOI Professor of Medicine and Pediatrics Distinguished Educator Penn State University, Hershey
 Drug allergy and Skin Disorders Timothy Craig, DO, FACOI Professor of Medicine and Pediatrics Distinguished Educator Penn State University, Hershey The best screening test for anaphylaxis is? A. histamine
Drug allergy and Skin Disorders Timothy Craig, DO, FACOI Professor of Medicine and Pediatrics Distinguished Educator Penn State University, Hershey The best screening test for anaphylaxis is? A. histamine
2. Has the child had a physician s diagnosis of atopic dermatitis or atopic eczema ever?
 Online Supplement 2: Letter questionnaire RISK FACTORS FOR THE DEVELOPMENT OF ASTHMA 1. Have the child s parents had a history of asthma ever? 2. Has the child had a physician s diagnosis of atopic dermatitis
Online Supplement 2: Letter questionnaire RISK FACTORS FOR THE DEVELOPMENT OF ASTHMA 1. Have the child s parents had a history of asthma ever? 2. Has the child had a physician s diagnosis of atopic dermatitis
Time to Learn. 6 th March 2018 Dr. Shirin Chakera GPwSI Integrated Dermatology Service
 Time to Learn 6 th March 2018 Dr. Shirin Chakera GPwSI Integrated Dermatology Service The Red Face Rosacea Acne Seborrhoeic eczema eczema Psoriasis Slapped cheek syndrome Fungal infection Erysipelas...
Time to Learn 6 th March 2018 Dr. Shirin Chakera GPwSI Integrated Dermatology Service The Red Face Rosacea Acne Seborrhoeic eczema eczema Psoriasis Slapped cheek syndrome Fungal infection Erysipelas...
Dermatologists are trained to evaluate distribution
 The value of patch testing patients with a scattered generalized distribution of dermatitis: Retrospective cross-sectional analyses of North American Contact Dermatitis Group data, 2001 to 2004 Kathryn
The value of patch testing patients with a scattered generalized distribution of dermatitis: Retrospective cross-sectional analyses of North American Contact Dermatitis Group data, 2001 to 2004 Kathryn
Is it allergy? Debbie Shipley
 Is it allergy? Debbie Shipley Topics Food Allergy and Eczema Hand Eczema and Patch Testing Urticaria Tackling Allergy Gell and Coombs classification Skin conditions with possible allergic component Allergy
Is it allergy? Debbie Shipley Topics Food Allergy and Eczema Hand Eczema and Patch Testing Urticaria Tackling Allergy Gell and Coombs classification Skin conditions with possible allergic component Allergy
On the interaction between the skin and the (working) environment. It is really that much of a problem. Elements of a skin management system
 environment. It is really that much of a problem. Elements of a skin management system") Notes to accompany talk by Chris Packham of EnviroDerm Services on 4th December 2017 On the interaction between the skin and the (working) environment The interaction between the skin and the working environment
Notes to accompany talk by Chris Packham of EnviroDerm Services on 4th December 2017 On the interaction between the skin and the (working) environment The interaction between the skin and the working environment
Food allergies and eczema
 Department of Dermatology Food allergies and eczema Information for parents and carers Eczema, also known as atopic eczema or atopic dermatitis, is a skin condition that causes inflammation and irritation.
Department of Dermatology Food allergies and eczema Information for parents and carers Eczema, also known as atopic eczema or atopic dermatitis, is a skin condition that causes inflammation and irritation.
Conflicts of interest
 Vulvar Cases 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology and Surgery(Dermatology)
Vulvar Cases 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology and Surgery(Dermatology)
Patching the Gaps in Our Diagnostic Knowledge. By Tyler Hooton MS3 UWSOM
 Patching the Gaps in Our Diagnostic Knowledge By Tyler Hooton MS3 UWSOM Disclosures The author has no financial disclosures or conflicts of interest The following patient has given permission for this
Patching the Gaps in Our Diagnostic Knowledge By Tyler Hooton MS3 UWSOM Disclosures The author has no financial disclosures or conflicts of interest The following patient has given permission for this
TCIs are only available on prescription and are usually started by a dermatology specialist.
 (TCIs) What are topical calcineurin inhibitors? Topical calcineurin inhibitors are treatments that alter the immune system and have been developed for controlling eczema. There are two types available:
(TCIs) What are topical calcineurin inhibitors? Topical calcineurin inhibitors are treatments that alter the immune system and have been developed for controlling eczema. There are two types available:
IMMUNODEFICIENCIES PRIMARY ALLERGIES PRIMARY IMMUNODEFICIENCIES AND ALLERGIES
 PRIMARY IMMUNODEFICIENCIES ALLERGIES PRIMARY IMMUNODEFICIENCIES AND ALLERGIES 1 PRIMARY IMMUNODEFICIENCIES KEY ABBREVIATIONS IgE CID Immunoglobulin E Combined Immunodeficiency IL5 Interleukin 5 IPOPI PID
PRIMARY IMMUNODEFICIENCIES ALLERGIES PRIMARY IMMUNODEFICIENCIES AND ALLERGIES 1 PRIMARY IMMUNODEFICIENCIES KEY ABBREVIATIONS IgE CID Immunoglobulin E Combined Immunodeficiency IL5 Interleukin 5 IPOPI PID
Dermatologists use the terms eczema and dermatitis interchangeably to describe a
 PATCH TESTING IN OCCUPATIONAL DERMATOLOGY Correspondence to: Dr David Gawkrodger, Department of Dermatology, Royal Hallamshire Hospital, Sheffield S10 2JF, UK d.j.gawkrodger@sth.nhs.uk David J Gawkrodger
PATCH TESTING IN OCCUPATIONAL DERMATOLOGY Correspondence to: Dr David Gawkrodger, Department of Dermatology, Royal Hallamshire Hospital, Sheffield S10 2JF, UK d.j.gawkrodger@sth.nhs.uk David J Gawkrodger
IMMUNOLOGY. Referral Guidelines NATIONAL REFERRAL GUIDELINES : IMMUNOLOGY. As above Specialist assessment is essential.
 PAGE 1 IMMUNOLOGY National PRIMARY IMMUNODEFICIENCY Primary immunodeficiency should be suspected in any patient with recurrent or persistent infection or unusual infection. Recurrent sinopulmonary infections
PAGE 1 IMMUNOLOGY National PRIMARY IMMUNODEFICIENCY Primary immunodeficiency should be suspected in any patient with recurrent or persistent infection or unusual infection. Recurrent sinopulmonary infections
Phototherapy and Photochemotherapy Treatment (Ultraviolet A [PUVA] and B [UBV])
![Phototherapy and Photochemotherapy Treatment (Ultraviolet A [PUVA] and B [UBV])](/thumbs/89/99382632.jpg "Phototherapy and Photochemotherapy Treatment (Ultraviolet A [PUVA] and B [UBV])") Origination: 09/27/07 Revised: 08/2/17 Annual Review: 11/2/17 Purpose: To provide Phototherapy and Photochemotherapy Treatment (PUVA and UBV) guidelines for the Medical Department staff to reference when
Origination: 09/27/07 Revised: 08/2/17 Annual Review: 11/2/17 Purpose: To provide Phototherapy and Photochemotherapy Treatment (PUVA and UBV) guidelines for the Medical Department staff to reference when
Eczema & Dermatitis Clinical features: Histopathological features: Classification:
 Eczema & Dermatitis Eczema is an inflammatory reactive pattern of skin to many and different stimuli characterized by itching, redness, scaling and clustered papulovesicles. Eczema and dermatitis are synonymous
Eczema & Dermatitis Eczema is an inflammatory reactive pattern of skin to many and different stimuli characterized by itching, redness, scaling and clustered papulovesicles. Eczema and dermatitis are synonymous
Patient Education to Enhance Contact Dermatitis Evaluation andtesting
 Patient Education to Enhance Contact Dermatitis Evaluation andtesting Mary C. Smith, RN, MSN KEYWORDS Patient education Patch testing Allergen avoidance Contact dermatitis Patients presenting for evaluation
Patient Education to Enhance Contact Dermatitis Evaluation andtesting Mary C. Smith, RN, MSN KEYWORDS Patient education Patch testing Allergen avoidance Contact dermatitis Patients presenting for evaluation
Allergy Medications. Antihistamines. are very safe. Although usually taken as tablets, they may be prescribed as a liquid or syrup for young children
 The treatments prescribed for allergy control the symptoms and reactions; they do not cure the condition. However, using treatments as prescribed can show a huge change in a patient s health, mood and
The treatments prescribed for allergy control the symptoms and reactions; they do not cure the condition. However, using treatments as prescribed can show a huge change in a patient s health, mood and
VELINDRE NHS TRUST. REF: Black 46. Trust Policy
 VELINDRE NHS TRUST REF: Black 46 POLICY FOR THE MANAGEMENT OF LATEX AND LATEX ALLERGY Health and Safety Manager Ref: Black 46 Page 1 of 14 CONTENTS Executive Summary Page 3 1. Introduction Page 4 2. Scope
VELINDRE NHS TRUST REF: Black 46 POLICY FOR THE MANAGEMENT OF LATEX AND LATEX ALLERGY Health and Safety Manager Ref: Black 46 Page 1 of 14 CONTENTS Executive Summary Page 3 1. Introduction Page 4 2. Scope
Allergic contact dermatitis caused by methylisothiazolinone in hair gel
 Allergic contact dermatitis caused by methylisothiazolinone in hair gel Antoine Badaoui, Olivier Bayrou, Charlotte Fite, Camille Frances, Angele Soria, Catherine Pecquet To cite this version: Antoine Badaoui,
Allergic contact dermatitis caused by methylisothiazolinone in hair gel Antoine Badaoui, Olivier Bayrou, Charlotte Fite, Camille Frances, Angele Soria, Catherine Pecquet To cite this version: Antoine Badaoui,
Hand Hygiene in Focus. MICROSHIELD Product Catalogue
 Hand Hygiene in Focus. MICROSHIELD Product Catalogue In the everyday business of healthcare, no instrument is more in focus than the human hand. From what we know today, our hands represent the greatest
Hand Hygiene in Focus. MICROSHIELD Product Catalogue In the everyday business of healthcare, no instrument is more in focus than the human hand. From what we know today, our hands represent the greatest
Conwy & Denbighshire NHS Trust. Ymddiriedolaeth GIG Siroedd Conwy a Dinbych Conwy & Denbighshire NHS Trust
 Ymddiriedolaeth GIG Siroedd Conwy a Dinbych POLICY FOR ANTISEPTICS AND DISINFECTANTS YELLOW 09 Policy Details: Author job title: Senior Nurse - Infection Control Dept/Working Group(s): Infection Control
Ymddiriedolaeth GIG Siroedd Conwy a Dinbych POLICY FOR ANTISEPTICS AND DISINFECTANTS YELLOW 09 Policy Details: Author job title: Senior Nurse - Infection Control Dept/Working Group(s): Infection Control
Treatments used Topical including cleansers and moisturizer Oral medications:
 Discipline: Dermatology Extended Topic: Acne & Rosacea : Onset: Location: Face Chest Back Menses if female: Regular Irregular PCOS Treatments used Topical including cleansers and moisturizer Oral medications:
Discipline: Dermatology Extended Topic: Acne & Rosacea : Onset: Location: Face Chest Back Menses if female: Regular Irregular PCOS Treatments used Topical including cleansers and moisturizer Oral medications:
TRIGGERS & TREATMENT OF ATOPIC DERMATITIS COA#PCIA0809 CE Activity provided by PCI Journal
 TRIGGERS & TREATMENT OF ATOPIC DERMATITIS COA#PCIA0809 CE Activity provided by PCI Journal INSTRUCTIONS 1. Read the article. 2. Take the test, record your answers in the test answer section (Section B)
TRIGGERS & TREATMENT OF ATOPIC DERMATITIS COA#PCIA0809 CE Activity provided by PCI Journal INSTRUCTIONS 1. Read the article. 2. Take the test, record your answers in the test answer section (Section B)
The skin is the largest organ of the human body. Functions: protection sensation maintain temperature vitamin synthesis
 Dermatology The skin is the largest organ of the human body. Functions: protection sensation maintain temperature vitamin synthesis The image to the left shows an image of skin cells and the proteins which
Dermatology The skin is the largest organ of the human body. Functions: protection sensation maintain temperature vitamin synthesis The image to the left shows an image of skin cells and the proteins which
Can steroids cause rash on arms
 Can steroids cause rash on arms Prednisone is a steroid that may be used to treat cancer. This drug is. Skin reactions such as rash, acne, facial redness, reddish-purple lines on the skin, or shiny skin..
Can steroids cause rash on arms Prednisone is a steroid that may be used to treat cancer. This drug is. Skin reactions such as rash, acne, facial redness, reddish-purple lines on the skin, or shiny skin..
Skin prick testing: Guidelines for GPs
 INDEX Summary Offered testing but where Allergens precautions are taken Skin prick testing Other concerns Caution Skin testing is not useful in these following conditions When skin testing is uninterpretable
INDEX Summary Offered testing but where Allergens precautions are taken Skin prick testing Other concerns Caution Skin testing is not useful in these following conditions When skin testing is uninterpretable
Clinical guideline Published: 12 December 2007 nice.org.uk/guidance/cg57
 Atopic eczema in under 12s: diagnosis and management Clinical guideline Published: 12 December 2007 nice.org.uk/guidance/cg57 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Atopic eczema in under 12s: diagnosis and management Clinical guideline Published: 12 December 2007 nice.org.uk/guidance/cg57 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
GROUP 15 TOPICAL PREPARATIONS
 - 105 - GROUP 15 15.1 DERMATOLOGICAL PREPARATIONS 15.1.1 TOPICAL ANTIFUNGALS CLOTRIMAZOLE Indication: Treatment of susceptible fungal infections, dermatophytoses, superficial mycoses, and cutaneous candidiasis
- 105 - GROUP 15 15.1 DERMATOLOGICAL PREPARATIONS 15.1.1 TOPICAL ANTIFUNGALS CLOTRIMAZOLE Indication: Treatment of susceptible fungal infections, dermatophytoses, superficial mycoses, and cutaneous candidiasis
Allergic Contact Dermatitis: From Workplace to Playpen
 Allergic Contact Dermatitis: From Workplace to Playpen Bruce A. Brod, M.D. Clinical Professor of Dermatology Director of Occupational Dermatology and Contact Dermatitis University of Pennsylvania Perelman
Allergic Contact Dermatitis: From Workplace to Playpen Bruce A. Brod, M.D. Clinical Professor of Dermatology Director of Occupational Dermatology and Contact Dermatitis University of Pennsylvania Perelman
Chronic hand dermatitis often interferes with ability
 32 Practical Dermatology October 2006 Follow these tips on history, exam, and testing in order to make the right diagnosis and institute effective therapy. By Susan Nedorost, MD Chronic hand dermatitis
32 Practical Dermatology October 2006 Follow these tips on history, exam, and testing in order to make the right diagnosis and institute effective therapy. By Susan Nedorost, MD Chronic hand dermatitis
Occupational asthma. Dr Gordon Parker NHS. Consultant / Honorary Lecturer in Occupational Medicine. Lancashire Teaching Hospitals NHS Foundation Trust
 Occupational asthma Dr Gordon Parker Consultant / Honorary Lecturer in Occupational Medicine Lancashire Teaching Hospitals NHS Foundation Trust NHS The good old bad old days Coal workers pneumoconiosis
Occupational asthma Dr Gordon Parker Consultant / Honorary Lecturer in Occupational Medicine Lancashire Teaching Hospitals NHS Foundation Trust NHS The good old bad old days Coal workers pneumoconiosis
Atopic Dermatitis. Atopic dermatitis (AD) is very common with a. Going Skin Deep With. Carl s rashes
 is very common with a. Going Skin Deep With. Carl s rashes") Focus on CME at Dalhousie University Going Skin Deep With Atopic Dermatitis Scott Murray, MD, FRCP(C), BSc Atopic dermatitis (AD) is very common with a tendency for itching and inflammation of the skin.
Focus on CME at Dalhousie University Going Skin Deep With Atopic Dermatitis Scott Murray, MD, FRCP(C), BSc Atopic dermatitis (AD) is very common with a tendency for itching and inflammation of the skin.
Management of eczema in infants and children Assoc Prof David Orchard Director, Department of Dermatology Royal Children s Hospital
 Atopic dermatitis definition Management of eczema in infants and children Assoc Prof David Orchard Director, Department of Dermatology Royal Children s Hospital Atopic dermatitis is long lasting (chronic)
Atopic dermatitis definition Management of eczema in infants and children Assoc Prof David Orchard Director, Department of Dermatology Royal Children s Hospital Atopic dermatitis is long lasting (chronic)
Are you glove aware? RCN. Glove Awareness Week
 Are you glove aware? RCN Glove Awareness Week Be glove aware Protecting your hands is crucial for your own protection and the protection of patients. It is important to decide when to use gloves and the
Are you glove aware? RCN Glove Awareness Week Be glove aware Protecting your hands is crucial for your own protection and the protection of patients. It is important to decide when to use gloves and the
Childhood Eczema Flowchart
 Childhood Eczema Flowchart EXCLUSIONS -Over 15 years of age -Contact dermatitis -Seborrhoeic Eczema -Mild and Moderate Eczema Childhood Eczema Assess Eczema Severity RED FLAGS -Eczema Herpecitum -Severe
Childhood Eczema Flowchart EXCLUSIONS -Over 15 years of age -Contact dermatitis -Seborrhoeic Eczema -Mild and Moderate Eczema Childhood Eczema Assess Eczema Severity RED FLAGS -Eczema Herpecitum -Severe
SECOND ANNUAL NORTHERN ONTARIO PEDIATRICS CONFERENCE DERMATOLOGY. Lyne Giroux BSc, MD, FRCPC dermatology Associate professor of Medicine NOSM
 SECOND ANNUAL NORTHERN ONTARIO PEDIATRICS CONFERENCE DERMATOLOGY Lyne Giroux BSc, MD, FRCPC dermatology Associate professor of Medicine NOSM Sudbury Skin Clinique Team Disclosures I have been a part of
SECOND ANNUAL NORTHERN ONTARIO PEDIATRICS CONFERENCE DERMATOLOGY Lyne Giroux BSc, MD, FRCPC dermatology Associate professor of Medicine NOSM Sudbury Skin Clinique Team Disclosures I have been a part of