Antirheumatic drugs. Rheumatic Arthritis (RA)
|
|
|
- Lester Collins
- 5 years ago
- Views:
Transcription
1 Antirheumatic drugs Rheumatic Arthritis (RA)
2
3 Disease Modifying Antirheumatic drugs (DMARDs) DMARDs are used in the treatment of rheumatic arthritis RA and have been shown to slow the course of the disease, induce remission prevent further destruction of the joints and involved tissues. When a patient is diagnosed with RA, DMARDs should be started within 3 months to help stop the progression of the disease at the earlier stages. NSAIDs or corticosteroids may also be used for relief of symptoms if needed.
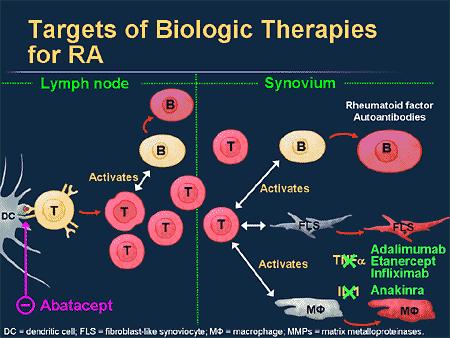
4 A. Choice of drug No one DMARD is efficacious and safe in every patient, and trials of several different drugs may be necessary. Monotherapy may be initiated with any of the DMARDs (methotrexate, leflunomide, hydroxychloroquine, or sulfasalazine) for patients with low disease activity.\ combination DMARD therapy (usually methotrexate based) or use of anti-tnf drugs (adalimumab, certolizumab,etanercept, golimumab, and infliximab) may be needed for: Patients with moderate to high disease activity or Inadequate response to monotherapy. For patients with more established disease, use of other biologic therapies (for example, abatacept, rituximab) can be considered. Most of these agents are contraindicated for use in pregnant women
5 Methotrexate Methotrexate [meth-oh-trex-ate] used alone or in combination therapy, has become a mainstay of treatment in patients with rheumatoid or psoriatic arthritis. Methotrexate is a folic acid antagonist that inhibits cytokine production and purine nucleotide biosynthesis, leading to immunosuppressive and anti-inflammatory effects. Response to methotrexate occurs within 3 to 6 weeks of starting treatment; it can also slow the appearance of new erosions within involved joints. The other DMARDs can be added to methotrexate therapy if there is partial or no response to maximum doses of methotrexate. Doses of methotrexate required for RA treatment are much lower than those needed in cancer chemotherapy and are given once a week, thereby minimizing adverse effects.
6 The most common side effects observed after methotrexate treatment of RA are mucosal ulceration and nausea. Cytopenias (particularly depression of the WBC count), cirrhosis of the liver, and an acute pneumonia-like syndrome may occur with chronic administration. Taking leucovorin (folinic acid) once daily after methotrexate reduces the severity of adverse effects. Folic acid taken on off-days is widely used. Periodic liver enzyme tests, complete blood
7 Hydroxychloroquine Hydroxychloroquine [hye-drox-ee-klor-oh-kwin] is used for early, mild RA, often combined with methotrexate. This agent is also used in the treatment of lupus and malaria. Its mechanism of action in autoimmune disorders is unknown onset of effects takes 6 weeks to 6 months. Hydroxychloroquine has less effects on the liver and immune system than other DMARDs; however, it may cause ocular toxicity, including irreversible retinal damage and corneal deposits. It may also cause CNS disturbances, GI upset, and skin discoloration and eruptions.
8 Leflunomide Leflunomide [le-floo-no-mide] is an immunomodulatory agent that preferentially causes cell arrest of the autoimmune lymphocytes through its action on dihydroorotate dehydrogenase (DHODH). Activated proliferating lymphocytes require constant DNA synthesis to proliferate. Pyrimidines and purines are the building blocks of DNA, and DHODH is necessary for pyrimidine synthesis. After biotransformation, leflunomide becomes a reversible inhibitor of DHODH Leflunomide is approved for the treatment of RA. It can be used as monotherapy or in combination with methotrexate. The most common adverse effects are headache, diarrhea, and nausea. Other untoward effects are weight loss, allergic reactions, including a flulike syndrome, skin rash, alopecia, and hypokalemia. It is not recommended in patients with liver disease, because of a risk of hepatotoxicity. Monitoring parameters include signs of infection, complete blood counts, and liver enzymes.

9 Site of action of leflunomide
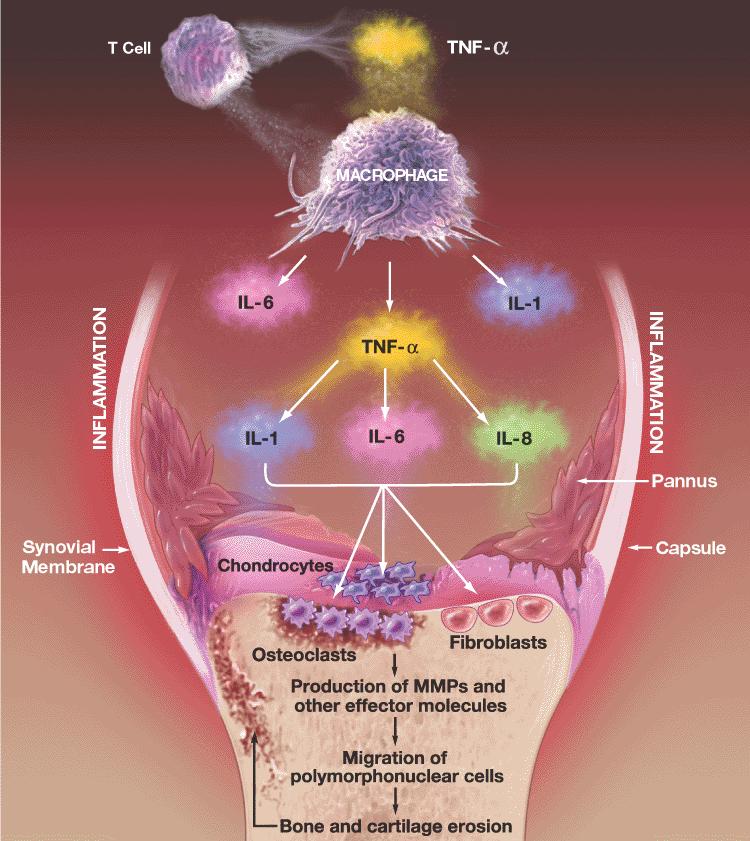
10 BIOLOGIC THERAPIES IN RHEUMATOID ARTHRITIS IL-1 and TNF-α are proinflammatory cytokines involved in the pathogenesis of RA. When secreted by synovial macrophages, IL-1 and TNF-α stimulate synovial cells to proliferate and synthesize collagenase, thereby degrading cartilage, stimulating bone resorption, and inhibiting proteoglycan synthesis. The TNF-α inhibitors (adalimumab, certolizumab, etanercept, golimumab, and infliximab) have been shown to decrease signs and symptoms of RA, reduce progression of structural damage, and improve physical function. Clinical response can be seen within 2 weeks of therapy. As with DMARDs, the decision to continue or stop a biological agent can often be made within 3 months after initiation of therapy.
11 If a patient has failed therapy with one TNF-α inhibitor, a trial with a different TNF-α inhibitor or a non-tnf biologic therapy (abatacept, rituximab, tocilizumab, tofacitinib) is appropriate. TNF-α inhibitors can be administered with any of the other drugs for RA, except for the non-tnf biologic therapies (due to increased risk of infection). Patients receiving TNF-α inhibitors are at increased risk for infections (tuberculosis and sepsis), fungal opportunistic infections, and pancytopenia. Live vaccinations should not be administered while on TNF-α inhibitor therapy. These agents should be used very cautiously in those with heart failure, as they can cause and/or worsen preexisting heart failure. An increased risk of lymphoma and other cancers has been observed with the use of TNF-α inhibitors.
12

13
14 Adalimumab Adalimumab [a-dal-aye-mu-mab] is a recombinant monoclonal antibody that binds to TNF-α, thereby interfering with endogenous TNF-αactivity by blocking its interaction with cell surface receptors. This agent is indicated for treatment of moderate to severe RA, either as monotherapy or in combination with methotrexate. It is also indicated for psoriatic arthritis, ankylosing spondylitis, and Crohn disease. Adalimumab is administered subcutaneously weekly or every other week. It may cause headache, nausea, agranulocytosis, rash, reaction at the injection site, or increased risk of infections, such as urinary tract infections, upper respiratory tract infections, and sinusitis.
15 Certolizumab pegol Certolizumab [ser-toe-liz-oo-mab] is a unique TNF-α blocker that contains a Fab fragment of a humanized antibody and is a potent neutralizer of TNF-α biological actions. It is combined with polyethylene glycol (pegylated) and is administered every 2 weeks via subcutaneous injection. It has similar indications to adalimumab. Adverse effects are similar to other TNF-α inhibitors
16 Etanercept Etanercept [ee-tan-er-cept] is a genetically engineered, soluble, recombinant, fully human receptor fusion protein that binds to TNF-α, thereby blocking its interaction with cell surface TNF-α receptors. This agent is approved for use in patients with moderate to severe RA, either alone or in combination with methotrexate. It is also approved for use in ankylosing spondylitis and psoriasis. The combination of etanercept and methotrexate is more effective than methotrexate or etanercept alone in retarding the RA disease process, improving function, and achieving remission Etanercept is given subcutaneously twice a week. The drug is generally well tolerated. As with all TNF-α inhibitors, it can increase the risk for infections, malignancy, and new or worsening heart failure.
17 Golimumab Golimumab [goe-lim-ue-mab] neutralizes the biological activity of TNF-α by binding to it and blocking its interaction with cell surface receptors. This compound is administered subcutaneously once a month in combination with methotrexate or other nonbiologic DMARDs. Golimumab may increase hepatic enzymes. Reactivation of hepatitis B may occur in chronic carriers. As with other TNF-α inhibitors, this drug may increase the risk of malignancies and serious infections.
18 Infliximab Infliximab [in-flix-i-mab] is a chimeric monoclonal antibody composed of human and murine regions. The antibody binds specifically to human TNF-α and inhibits binding with its receptors. Infliximab is approved for use in combination with methotrexate in patients with RA who have had inadequate response to methotrexate monotherapy. This agent is not indicated for monotherapy, as this leads to the development of anti-infliximab antibodies, resulting in reduced efficacy. Additional indications include plaque psoriasis, psoriatic arthritis, ulcerative colitis, ankylosing spondylitis, and Crohn disease. Infliximab is administered as an IV infusion every 8 weeks. Infusion site reactions, such as fever, chills, pruritus, and urticaria, may occur. Infections (for example, pneumonia, cellulitis, and activation of latent tuberculosis), leukopenia, and neutropenia have also been reported.
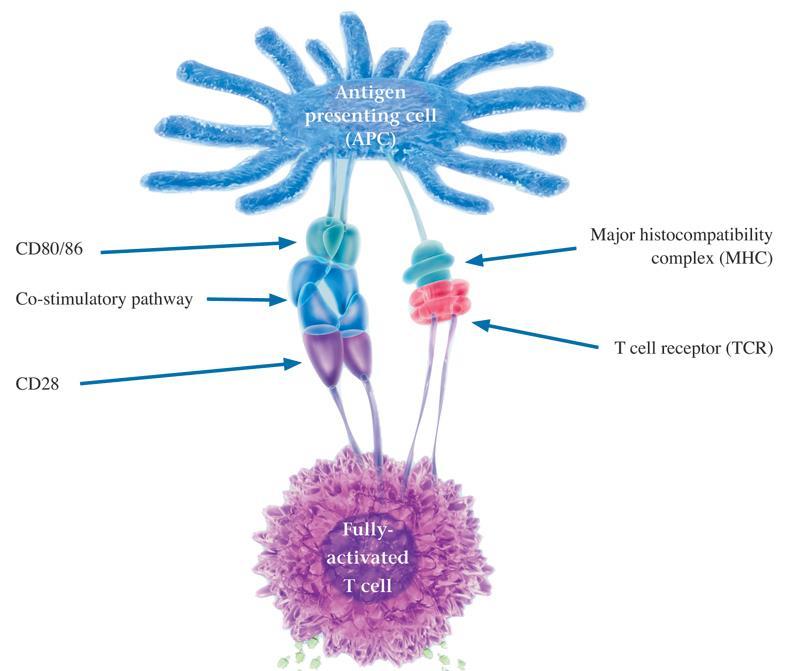
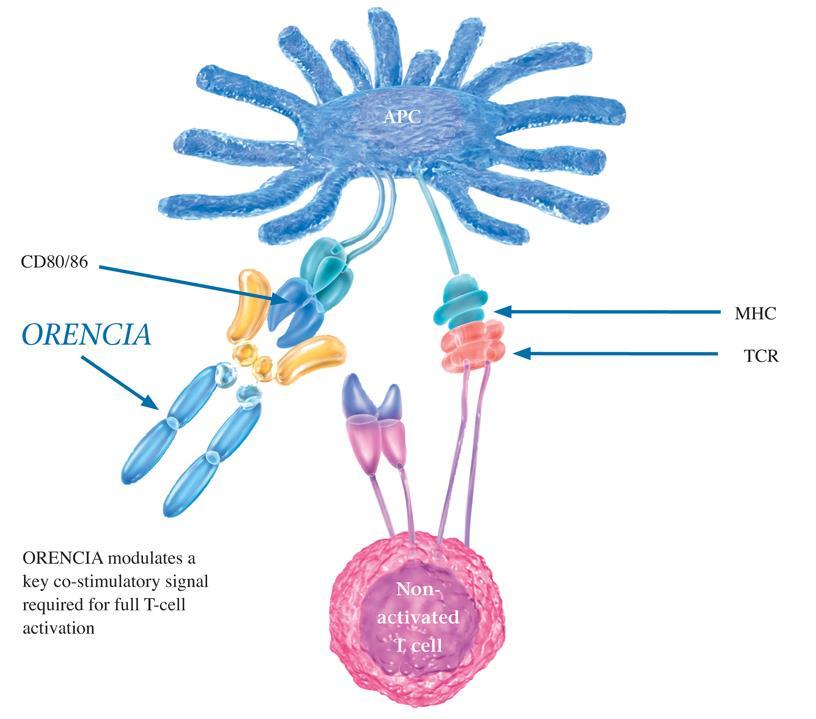
19 Abatacept (ORENCIA ) T lymphocytes need two interactions to become activated: 1) the antigen-presenting cell (that is, macrophages or B cells) must interact with the receptor on the T cell 2) the CD80/CD86 protein on the antigen-presenting cell must interact with the CD28 protein on the T cell. Abatacept [a-bat-ah-cept] is a soluble recombinant fusion protein that competes with CD28 for binding on CD80/CD86 protein, thereby preventing full T-cell activation.
20 Abatacept This agent is indicated for patients with moderate to severe RA who have had an inadequate response to DMARDs or TNF-α inhibitors. Abatacept is administered as an IV infusion every 4 weeks. Common adverse effects include headache, upper respiratory infections, nasopharyngitis, and nausea. Concurrent use with TNF-α inhibitors is not recommended due to increased risk of serious infections
21
22
23 Rituximab B lymphocytes are derived from the bone marrow and are necessary for efficient immune response. In RA, however, B cells can perpetuate the inflammatory process in the synovium by: 1) activating T lymphocytes. 2) producing autoantibodies and rheumatoid factor 3) producing proinflammatory cytokines, such as TNF-α and IL- 1. Rituximab [ri-tuk-si-mab] is a genetically engineered chimeric murine/human monoclonal antibody directed against the CD20 antigen found on the surface of normal and malignant B lymphocytes, resulting in B-cell depletion.
24 Rituximab This agent is indicated for use in combination with methotrexate for patients with moderate to severe RA who have had an inadequate response to TNF-α inhibitors. Rituximab is administered as an intravenous infusion every 16 to 24 weeks. To reduce the severity of infusion reactions, methylprednisolone is administered 30 minutes prior to each infusion. Infusion reactions (urticaria, hypotension, and angioedema) are the most common complaints with this agent and typically occur during the first infusion.

 B cell CD20 MAC Complement-dependent")
25 Anti-CD20: Mechanism of Action Macrophage, monocyte, NK cell Anti-CD20 antibody CD20 Fc RIIIA Antibody-Dependent Cell-Mediated Cytotoxicity (ADCC) B cell CD20 MAC Complement-dependent Cytotoxicity Apoptosis
26 Tocilizumab Tocilizumab [toe-si-liz-ue-mab] is a monoclonal antibody that inhibits the actions of IL-6 by blocking the IL-6 receptor. Tocilizumab is administered as an intravenous infusion every 4 weeks. The drug can be used as monotherapy or in combination with methotrexate or other nonbiologic DMARDs for patients with moderate to severe RA.
27 Tofacitinib Janus kinases are intracellular enzymes that modulate immune cell activity in response to the binding of inflammatory mediators to the cellular membrane. Cytokines, growth factors, interferons, ILs, and erythropoietin can lead to an increase in Janus kinase activity and activation of the immune system. Tofacitinib [toe-fa-sye-ti-nib] is an oral inhibitor of Janus kinases indicated for the treatment of moderate to severe RA in patients who have had an inadequate response or intolerance to methotrexate.
28 Tofacitinib Metabolism of tofacitinib is mediated primarily by CYP3A4, and dosage adjustments may be required if the drug is taken with potent inhibitors or inducers of this isoenzyme. Hemoglobin concentrations must be greater than 9 g/dl to start tofacitinib and must be monitored during therapy due to the risk for anemia. Likewise, lymphocyte and neutrophil counts should be checked prior to initiation of therapy and monitored during treatment. Tofacitinib treatment may also increase the risk for secondary malignancy, opportunistic infections, renal, or hepatic dysfunction.
29 Anakinra IL-1 is induced by inflammatory stimuli and mediates a variety of immunologic responses, including degradation of cartilage and stimulation of bone resorption. Anakinra [an-a-kin-ra] is an IL-1 receptor antagonist. Anakinra treatment leads to a modest reduction in the signs and symptoms of moderate to severe RA in patients who have failed one or more DMARDs. This agent is associated with neutropenia and is infrequently used in the treatment of RA.
MMS Pharmacology Lecture 2. Antirheumatic drugs. Dr Sura Al Zoubi
 MMS Pharmacology Lecture 2 Antirheumatic drugs Dr Sura Al Zoubi Revision Rheumatoid Arthritis Definition (RA): is the most common systemic inflammatory disease characterized by symmetrical inflammation
MMS Pharmacology Lecture 2 Antirheumatic drugs Dr Sura Al Zoubi Revision Rheumatoid Arthritis Definition (RA): is the most common systemic inflammatory disease characterized by symmetrical inflammation
Cimzia. Cimzia (certolizumab pegol) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Section: Prescription Drugs Effective Date: April 1, 2018 Subject: Cimzia Page: 1 of 5 Last Review
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Section: Prescription Drugs Effective Date: April 1, 2018 Subject: Cimzia Page: 1 of 5 Last Review
Cimzia. Cimzia (certolizumab pegol) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Subject: Cimzia Page: 1 of 5 Last Review Date: December 8, 2017 Cimzia Description Cimzia (certolizumab
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Subject: Cimzia Page: 1 of 5 Last Review Date: December 8, 2017 Cimzia Description Cimzia (certolizumab
Cimzia. Cimzia (certolizumab pegol) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Cimzia Page: 1 of 5 Last Review Date: March 17, 2017 Cimzia Description Cimzia (certolizumab pegol)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Cimzia Page: 1 of 5 Last Review Date: March 17, 2017 Cimzia Description Cimzia (certolizumab pegol)
Rheumatoid arthritis
 Rheumatoid arthritis 1 Definition Rheumatoid arthritis is one of the most common inflammatory disorders affecting the population worldwide. It is a systemic inflammatory disease which affects not only
Rheumatoid arthritis 1 Definition Rheumatoid arthritis is one of the most common inflammatory disorders affecting the population worldwide. It is a systemic inflammatory disease which affects not only
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: golimumab_simponi 8/2013 2/2018 2/2019 3/2018 Description of Procedure or Service Golimumab (Simponi and
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: golimumab_simponi 8/2013 2/2018 2/2019 3/2018 Description of Procedure or Service Golimumab (Simponi and
Regulatory Status FDA- approved indication: Simponi and Simponi ARIA are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-3)
 blockers indicated for the treatment of: (2-3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 9 Last Review Date: March 16, 2018 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 9 Last Review Date: March 16, 2018 Simponi / Simponi
What prescribers need to know
 HUMIRA Citrate-free presentations in an Electronic Medical Record (EMR) What prescribers need to know 2 / This is your guide to identifying HUMIRA Citrate-free presentations in your Electronic Medical
HUMIRA Citrate-free presentations in an Electronic Medical Record (EMR) What prescribers need to know 2 / This is your guide to identifying HUMIRA Citrate-free presentations in your Electronic Medical
Xeljanz. Xeljanz, Xeljanz XR (tofacitinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.24 Subject: Xeljanz Page: 1 of 6 Last Review Date: March 16, 2018 Xeljanz Description Xeljanz, Xeljanz
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.24 Subject: Xeljanz Page: 1 of 6 Last Review Date: March 16, 2018 Xeljanz Description Xeljanz, Xeljanz
CIMZIA (certolizumab pegol)
") Pre - PA Allowance None Prior-Approval Requirements Age Diagnoses 18 years of age or older Patient must have ONE of the following: 1. Moderate to severe Crohn s Disease (CD) a. Inadequate response, intolerance
Pre - PA Allowance None Prior-Approval Requirements Age Diagnoses 18 years of age or older Patient must have ONE of the following: 1. Moderate to severe Crohn s Disease (CD) a. Inadequate response, intolerance
The Medical Letter. on Drugs and Therapeutics
 The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
Treating Rheumatologic Disease in Arizona: Good News, Bad News
 Treating Rheumatologic Disease in Arizona: Good News, Bad News Jeffrey R. Lisse, M.D. Ethel P. McChesney Bilby Professor of Medicine Chief, Section of Rheumatology University of Arizona School of Medicine
Treating Rheumatologic Disease in Arizona: Good News, Bad News Jeffrey R. Lisse, M.D. Ethel P. McChesney Bilby Professor of Medicine Chief, Section of Rheumatology University of Arizona School of Medicine
1 P a g e. Systemic Juvenile Idiopathic Arthritis (SJIA) (1.3) Patients 2 years of age and older with active systemic juvenile idiopathic arthritis.
 (1.3) Patients 2 years of age and older with active systemic juvenile idiopathic arthritis.") LENGTH OF AUTHORIZATION: Initial: 3 months for Crohn s or Ulcerative Colitis; 1 year for all other indications. Renewal: 1 year dependent upon medical records supporting response to therapy and review
LENGTH OF AUTHORIZATION: Initial: 3 months for Crohn s or Ulcerative Colitis; 1 year for all other indications. Renewal: 1 year dependent upon medical records supporting response to therapy and review
Cimzia (certolizumab pegol) Data Showed Broad and Rapid Relief From Burden of Symptoms In Rheumatoid Arthritis Patients
 Data Showed Broad and Rapid Relief From Burden of Symptoms In Rheumatoid Arthritis Patients") Cimzia (certolizumab pegol) Data Showed Broad and Rapid Relief From Burden of Symptoms In Rheumatoid Arthritis Patients Rapid, sustained and clinically meaningful improvement in wideranging patient-reported
Cimzia (certolizumab pegol) Data Showed Broad and Rapid Relief From Burden of Symptoms In Rheumatoid Arthritis Patients Rapid, sustained and clinically meaningful improvement in wideranging patient-reported
DRAFT. Remission rates, calculated using observed case (OC) analyses were as follows: Year 1 Year 2 Year 3 Year 4 All patients 62.
 analyses were as follows: Year 1 Year 2 Year 3 Year 4 All patients 62.") DRAFT New Efficacy Data Shows Cimzia (certolizumab pegol) Provides Long-Term Remission of Moderate to Severe Crohn s Disease Regardless of Prior Anti-TNF Exposure, According to Data Presented at DDW Oral
DRAFT New Efficacy Data Shows Cimzia (certolizumab pegol) Provides Long-Term Remission of Moderate to Severe Crohn s Disease Regardless of Prior Anti-TNF Exposure, According to Data Presented at DDW Oral
Stelara. Stelara (ustekinumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.04 Subject: Stelara Page: 1 of 9 Last Review Date: September 20, 2018 Stelara Description Stelara
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.04 Subject: Stelara Page: 1 of 9 Last Review Date: September 20, 2018 Stelara Description Stelara
Rheumatoid Arthritis. Module III
 Rheumatoid Arthritis Module III Management: Biological disease modifying anti-rheumatic drugs, glucocorticoids and special situations (pregnancy & lactation) Dr Ved Chaturvedi MD, DM Senior Consultant
Rheumatoid Arthritis Module III Management: Biological disease modifying anti-rheumatic drugs, glucocorticoids and special situations (pregnancy & lactation) Dr Ved Chaturvedi MD, DM Senior Consultant
Medication Policy Manual. Topic: Xeljanz, tofacitinib Date of Origin: January 21, 2013
 Medication Policy Manual Policy No: dru289 Topic: Xeljanz, tofacitinib Date of Origin: January 21, 2013 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1,
Medication Policy Manual Policy No: dru289 Topic: Xeljanz, tofacitinib Date of Origin: January 21, 2013 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1,
HELPING YOU AND YOUR PATIENTS TALK OPENLY ABOUT MODERATELY TO SEVERELY ACTIVE RA
 SIMPONI ARIA (golimumab) is indicated for the treatment of adults with moderately to severely active rheumatoid arthritis (RA) in combination with MTX, active psoriatic arthritis, and active ankylosing
SIMPONI ARIA (golimumab) is indicated for the treatment of adults with moderately to severely active rheumatoid arthritis (RA) in combination with MTX, active psoriatic arthritis, and active ankylosing
Simponi / Simponi ARIA (golimumab)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 6 Last Review Date: September 15, 2016 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 6 Last Review Date: September 15, 2016 Simponi / Simponi
Cyltezo (adalimumab-adbm) CG-DRUG-64, CG-DRUG-65
 CG-DRUG-64, CG-DRUG-65") Market DC Cyltezo (adalimumab-adbm) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Cyltezo (adalimumab-adbm) 40 mg/0.8 ml prefilled syringe #* ^ Approval Duration 1 year
Market DC Cyltezo (adalimumab-adbm) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Cyltezo (adalimumab-adbm) 40 mg/0.8 ml prefilled syringe #* ^ Approval Duration 1 year
PRIOR AUTHORIZATION REQUEST GUIDE
 PRIOR AUTHORIZATION REQUEST GUIDE Drafting a Prior Authorization Request The following information is presented for informational purposes only and is not intended to provide reimbursement or legal advice.
PRIOR AUTHORIZATION REQUEST GUIDE Drafting a Prior Authorization Request The following information is presented for informational purposes only and is not intended to provide reimbursement or legal advice.
INFLIXIMAB Remicade (infliximab), Inflectra (infliximab-dyyb), Ixifi* (infliximabqbtx), Renflexis (infliximab-abda)
, Inflectra (infliximab-dyyb), Ixifi* (infliximabqbtx), Renflexis (infliximab-abda)") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 6 years of age or older 1. Moderate to severe Crohn s disease (CD) a. Patient has fistulizing disease
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 6 years of age or older 1. Moderate to severe Crohn s disease (CD) a. Patient has fistulizing disease
New Cimzia data, with sites in the US, demonstrate safety and efficacy, increased participation in social activities for adult RA patients
 Long-term Cimzia (certolizumab pegol) data demonstrated rapid sustained improvements in clinical outcomes and quality of life in moderate to severe rheumatoid arthritis (RA) patients New Cimzia data, with
Long-term Cimzia (certolizumab pegol) data demonstrated rapid sustained improvements in clinical outcomes and quality of life in moderate to severe rheumatoid arthritis (RA) patients New Cimzia data, with
Regulatory Status FDA- approved indication: Simponi and Simponi ARIA are tumor necrosis factor (TNF) blockers indicated for the treatment of:
 blockers indicated for the treatment of:") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 8 Last Review Date: March 17, 2017 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 8 Last Review Date: March 17, 2017 Simponi / Simponi
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC)
") DERBYSHIRE JOINT AREA PRERIBING COMMITTEE (JAPC) Derbyshire commissioning guidance on biologic drugs f the treatment of Rheumatoid arthritis with methotrexate This algithm is a tool to aid the implementation
DERBYSHIRE JOINT AREA PRERIBING COMMITTEE (JAPC) Derbyshire commissioning guidance on biologic drugs f the treatment of Rheumatoid arthritis with methotrexate This algithm is a tool to aid the implementation
Announcing HUMIRA. Psoriasis Starter Package
 Announcing HUMIRA (adalimumab) Psoriasis Starter Package HUMIRA is indicated for the treatment of adult patients with moderate to severe chronic plaque psoriasis who are candidates for systemic therapy
Announcing HUMIRA (adalimumab) Psoriasis Starter Package HUMIRA is indicated for the treatment of adult patients with moderate to severe chronic plaque psoriasis who are candidates for systemic therapy
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: abatacept_orencia 4/2008 2/2018 2/2019 2/2018 Description of Procedure or Service Abatacept (Orencia ), a
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: abatacept_orencia 4/2008 2/2018 2/2019 2/2018 Description of Procedure or Service Abatacept (Orencia ), a
Infliximab/Infliximab-dyyb DRUG.00002
 Infliximab/Infliximab-dyyb DRUG.00002 Override(s) Prior Authorization Step Therapy Medications Remicade (infliximab) Inflectra (inflectra-dyyb) Approval Duration 1 year Comment Intravenous administration
Infliximab/Infliximab-dyyb DRUG.00002 Override(s) Prior Authorization Step Therapy Medications Remicade (infliximab) Inflectra (inflectra-dyyb) Approval Duration 1 year Comment Intravenous administration
RHEUMATOID ARTHRITIS DRUGS
 Rheumatology Biologics Criteria from the Exceptional Access Program RHEUMATOID ARTHRITIS DRUGS DRUG NAME BRS REIMBURSED DOSAGE FORM/ STRENGTH Adalimumab Humira 40 mg/0.8 syringe and 40mg/0.8 pen for Anakinra
Rheumatology Biologics Criteria from the Exceptional Access Program RHEUMATOID ARTHRITIS DRUGS DRUG NAME BRS REIMBURSED DOSAGE FORM/ STRENGTH Adalimumab Humira 40 mg/0.8 syringe and 40mg/0.8 pen for Anakinra
Cosentyx. Cosentyx (secukinumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.11 Subject: Cosentyx Page: 1 of 7 Last Review Date: September 20, 2018 Cosentyx Description Cosentyx
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.11 Subject: Cosentyx Page: 1 of 7 Last Review Date: September 20, 2018 Cosentyx Description Cosentyx
Cimzia shows duration of response up to week 26 in moderate to severe Crohn s patients who failed the intravenous infusion treatment infliximab.
 C3073-0409 CIMZIA (certolizumab pegol) PROVIDES LONG-TERM REMISSION AND RESPONSE RATES IN INFLIXIMAB-REFRACTORY CROHN S PATIENTS Cimzia shows duration of response up to week 26 in moderate to severe Crohn
C3073-0409 CIMZIA (certolizumab pegol) PROVIDES LONG-TERM REMISSION AND RESPONSE RATES IN INFLIXIMAB-REFRACTORY CROHN S PATIENTS Cimzia shows duration of response up to week 26 in moderate to severe Crohn
Pharmacy Management Drug Policy
 SUBJECT: Cimzia (Certolizumab pegol) - for Ankylosing Spondylitis, Crohn s Disease, Psoriatic Arthritis and Rheumatoid Arthritis POLICY NUMBER: PHARMACY-07 EFFECTIVE DATE: 5/2009 LAST REVIEW DATE: 6/13/2018
SUBJECT: Cimzia (Certolizumab pegol) - for Ankylosing Spondylitis, Crohn s Disease, Psoriatic Arthritis and Rheumatoid Arthritis POLICY NUMBER: PHARMACY-07 EFFECTIVE DATE: 5/2009 LAST REVIEW DATE: 6/13/2018
Biologics for Autoimmune Diseases
 Biologics for Autoimmune Diseases Goal(s): Restrict use of biologics to OHP funded conditions and according to OHP guidelines for use. Promote use that is consistent with national clinical practice guidelines
Biologics for Autoimmune Diseases Goal(s): Restrict use of biologics to OHP funded conditions and according to OHP guidelines for use. Promote use that is consistent with national clinical practice guidelines
Regulatory Status FDA-approved indication: Orencia is a selective T cell costimulation modulator indicated for: (1)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.18 Subject: Orencia Page: 1 of 8 Last Review Date: March 16, 2018 Orencia Description Orencia (abatacept)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.18 Subject: Orencia Page: 1 of 8 Last Review Date: March 16, 2018 Orencia Description Orencia (abatacept)
ACTEMRA (tocilizumab)
") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 1. Active Polyarticular Juvenile Idiopathic Arthritis (PJIA) b. Patient has an intolerance or has experienced
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 1. Active Polyarticular Juvenile Idiopathic Arthritis (PJIA) b. Patient has an intolerance or has experienced
Remicade (infliximab) DRUG.00002
 DRUG.00002") Applicability/Effective Date *- Florida Healthy Kids Remicade (infliximab) DRUG.00002 Override(s) Prior Authorization Step Therapy Medications Remicade (infliximab) Approval Duration 1 year Comment Intravenous
Applicability/Effective Date *- Florida Healthy Kids Remicade (infliximab) DRUG.00002 Override(s) Prior Authorization Step Therapy Medications Remicade (infliximab) Approval Duration 1 year Comment Intravenous
Regulatory Status FDA-approved indication: Humira and Amjevita are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-3)
 blockers indicated for the treatment of: (2-3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.29 Subject: Humira Page: 1 of 10 Last Review Date: June 22, 2017 Humira Description Humira (adalimumab),
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.29 Subject: Humira Page: 1 of 10 Last Review Date: June 22, 2017 Humira Description Humira (adalimumab),
Actemra. Actemra (tocilizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.12 Subject: Actemra Page: 1 of 13 Last Review Date: September 20, 2018 Actemra Description Actemra
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.12 Subject: Actemra Page: 1 of 13 Last Review Date: September 20, 2018 Actemra Description Actemra
Regulatory Status FDA-approved indication: Orencia is a selective T cell co-stimulation modulator indicated for: (1)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Orencia Page: 1 of 9 Last Review Date: September 20, 2018 Orencia Description Orencia (abatacept)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Orencia Page: 1 of 9 Last Review Date: September 20, 2018 Orencia Description Orencia (abatacept)
Actemra (tocilizumab) CG-DRUG-81
 CG-DRUG-81") Market DC Actemra (tocilizumab) CG-DRUG-81 Override(s) Prior Authorization Approval Duration 1 year Medications Line of Business Quantity Limit Actemra (tocilizumab) vials VA MCD and All L-AGP May be subject
Market DC Actemra (tocilizumab) CG-DRUG-81 Override(s) Prior Authorization Approval Duration 1 year Medications Line of Business Quantity Limit Actemra (tocilizumab) vials VA MCD and All L-AGP May be subject
Regional vs. Systemic Therapy. Corticosteroids. Regional vs. Systemic Therapy for Uveitis. Considerations
 Regional vs. Systemic Therapy for Uveitis Nisha Acharya,, M.D., M.S. Director, Uveitis Service F.I. Proctor Foundation University of California, San Francisco December 4, 2010 No financial disclosures
Regional vs. Systemic Therapy for Uveitis Nisha Acharya,, M.D., M.S. Director, Uveitis Service F.I. Proctor Foundation University of California, San Francisco December 4, 2010 No financial disclosures
Pfizer Announces Modification To Ongoing Tofacitinib FDA Post- Marketing Requirement Study In Patients With Rheumatoid Arthritis
 February 19, 2019 Media Contact: Neha Wadhwa M: +1 212-733-2835 E: Neha.Wadhwa@pfizer.com Investor Contact: Charles Triano O: +1 212-733-3901 E: Charles.E.Triano@pfizer.com Pfizer Announces Modification
February 19, 2019 Media Contact: Neha Wadhwa M: +1 212-733-2835 E: Neha.Wadhwa@pfizer.com Investor Contact: Charles Triano O: +1 212-733-3901 E: Charles.E.Triano@pfizer.com Pfizer Announces Modification
1. Background: Infliximab is administered parenterally; therefore, it is not covered under retail pharmacy benefits.
 Subject: Infliximab (Remicade ) Original Original Committee Approval: October 13, 2006 Revised Last Committee Approval: December 3, 2008 Last Review: October 19, 2007 1. Background: Infliximab is a genetically
Subject: Infliximab (Remicade ) Original Original Committee Approval: October 13, 2006 Revised Last Committee Approval: December 3, 2008 Last Review: October 19, 2007 1. Background: Infliximab is a genetically
Humira (adalimumab) DRUG.00002
 DRUG.00002") Humira (adalimumab) DRUG.00002 Override(s) Prior Authorization Quantity Limit Approval Duration 1 year Medications Humira 10 mg/0.2 ml syringe Humira pediatric Crohn s Disease starter pack 40 mg/0.8 ml
Humira (adalimumab) DRUG.00002 Override(s) Prior Authorization Quantity Limit Approval Duration 1 year Medications Humira 10 mg/0.2 ml syringe Humira pediatric Crohn s Disease starter pack 40 mg/0.8 ml
Corporate Medical Policy
 Corporate Medical Policy Rituximab for the Treatment of Rheumatoid Arthritis File Name: Origination: Last CAP Review: Next CAP Review: Last Review: rituximab_for_the_treatment_of_rheumatoid_arthritis 4/2008
Corporate Medical Policy Rituximab for the Treatment of Rheumatoid Arthritis File Name: Origination: Last CAP Review: Next CAP Review: Last Review: rituximab_for_the_treatment_of_rheumatoid_arthritis 4/2008
Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda) DRUG CG-DRUG-64
, Remicade (infliximab), Renflexis (infliximab-abda) DRUG CG-DRUG-64") Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda) DRUG.00002 CG-DRUG-64 Override(s) Prior Authorization *Washington Medicaid See State Specific Mandates Medications Inflectra
Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda) DRUG.00002 CG-DRUG-64 Override(s) Prior Authorization *Washington Medicaid See State Specific Mandates Medications Inflectra
Medical Management of Rheumatoid Arthritis (RA)
") Medical Management of Rheumatoid Arthritis (RA) Dr Lee-Suan Teh Rheumatologist Royal Blackburn Hospital Educational objectives ABC Appreciate the epidemiology of RA Be able to diagnosis of RA Competent
Medical Management of Rheumatoid Arthritis (RA) Dr Lee-Suan Teh Rheumatologist Royal Blackburn Hospital Educational objectives ABC Appreciate the epidemiology of RA Be able to diagnosis of RA Competent
Remicade. Remicade (infliximab), Inflectra (infliximab-dyyb) Description
, Inflectra (infliximab-dyyb) Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Remicade Page: 1 of 9 Last Review Date: June 22, 2017 Remicade Description Remicade (infliximab),
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Remicade Page: 1 of 9 Last Review Date: June 22, 2017 Remicade Description Remicade (infliximab),
(tofacitinib) are met.
 are met.") Xeljanz (tofacitinib) Policy Number: 5.01. 560 Origination: 3/2014 Last Review: 3/2014 Next Review: 3/2015 Policy BCBSKC will provide coverage for Xeljanz (tofacitinib) when it is determined to be medically
Xeljanz (tofacitinib) Policy Number: 5.01. 560 Origination: 3/2014 Last Review: 3/2014 Next Review: 3/2015 Policy BCBSKC will provide coverage for Xeljanz (tofacitinib) when it is determined to be medically
Although this presentation includes information regarding pharmaceuticals (including products under development), the information is not intended as
, the information is not intended as") Although this presentation includes information regarding pharmaceuticals (including products under development), the information is not intended as any advertisement and/or medical advice. Forward-Looking
Although this presentation includes information regarding pharmaceuticals (including products under development), the information is not intended as any advertisement and/or medical advice. Forward-Looking
Immunosuppressants. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Immunosuppressants Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Immunosuppressive Agents Very useful in minimizing the occurrence of exaggerated or inappropriate
Immunosuppressants Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Immunosuppressive Agents Very useful in minimizing the occurrence of exaggerated or inappropriate
Xeljanz (tofacitinib), Xeljanz XR (tofacitinib extended-release)
, Xeljanz XR (tofacitinib extended-release)") Market DC Xeljanz (tofacitinib), Xeljanz XR (tofacitinib extended-release) Override(s) Prior Authorization Quantity Limit Medications Xeljanz (tofacitinib) Approval Duration 1 year Quantity Limit May be
Market DC Xeljanz (tofacitinib), Xeljanz XR (tofacitinib extended-release) Override(s) Prior Authorization Quantity Limit Medications Xeljanz (tofacitinib) Approval Duration 1 year Quantity Limit May be
Remicade. Remicade (infliximab), Inflectra (infliximab-dyyb) Description
, Inflectra (infliximab-dyyb) Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.02 Subsection: Gastrointestinal nts Original Policy Date: May 20, 2011 Subject: Remicade Page: 1 of
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.02 Subsection: Gastrointestinal nts Original Policy Date: May 20, 2011 Subject: Remicade Page: 1 of
Coverage Criteria: Express Scripts, Inc. monograph dated 12/15/ months or as otherwise noted by indication
 BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
Amjevita (adalimumab-atto) CG-DRUG-64, CG-DRUG-65
 CG-DRUG-64, CG-DRUG-65") Market DC Amjevita (adalimumab-atto) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2
Market DC Amjevita (adalimumab-atto) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2
Rheumatoid Arthritis. Improving Outcomes in RA: Three Pillars. RA: Chronic Joint Destruction and Disability What We Try to Prevent
 Rheumatoid Arthritis Modern Management of Common Problems in Rheumatology: Rheumatoid Arthritis Jonathan Graf, M.D. Associate Professor of Medicine, UCSF Division of Rheumatology, SFGH Director, UCSF Rheumatoid
Rheumatoid Arthritis Modern Management of Common Problems in Rheumatology: Rheumatoid Arthritis Jonathan Graf, M.D. Associate Professor of Medicine, UCSF Division of Rheumatology, SFGH Director, UCSF Rheumatoid
Medication Policy Manual. Topic: Otezla, apremilast Date of Origin: May 9, 2014
 Medication Policy Manual Policy No: dru342 Topic: Otezla, apremilast Date of Origin: May 9, 2014 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1, 2015 IMPORTANT
Medication Policy Manual Policy No: dru342 Topic: Otezla, apremilast Date of Origin: May 9, 2014 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1, 2015 IMPORTANT
Rheumatoid Arthritis. By: Hadi Esmaily (PharmD., BCCP, MBA) Department of Clinical Pharmacy, Shahid Beheshti Medical University
 Department of Clinical Pharmacy, Shahid Beheshti Medical University") Rheumatoid Arthritis By: Hadi Esmaily (PharmD., BCCP, MBA) Department of Clinical Pharmacy, Shahid Beheshti Medical University Introduction RA is a Chronic, Systemic, Inflammatory disorder of unknown etiology
Rheumatoid Arthritis By: Hadi Esmaily (PharmD., BCCP, MBA) Department of Clinical Pharmacy, Shahid Beheshti Medical University Introduction RA is a Chronic, Systemic, Inflammatory disorder of unknown etiology
First Name. Specialty: Fax. First Name DOB: Duration:
 Prescriber Information Last ame: First ame DEA/PI: Specialty: Phone - - Fax - - Member Information Last ame: First ame Member ID umber DOB: - - Medication Information: Drug ame and Strength: Diagnosis:
Prescriber Information Last ame: First ame DEA/PI: Specialty: Phone - - Fax - - Member Information Last ame: First ame Member ID umber DOB: - - Medication Information: Drug ame and Strength: Diagnosis:
Carelirst.+.V Family of health care plans
 Carelirst.+.V Family of health care plans CVS Caremark POLICY Document for ACTEMRA The overall objective of this policy is to support the appropriate and cost effective use of the medication, specific
Carelirst.+.V Family of health care plans CVS Caremark POLICY Document for ACTEMRA The overall objective of this policy is to support the appropriate and cost effective use of the medication, specific
CIMZIA (certolizumab pegol)
") CIMZIA (certolizumab pegol) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices
CIMZIA (certolizumab pegol) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices
Cell-Mediated Immunity and T Lymphocytes
 Cell-Mediated Immunity and T Lymphocytes T helper (Th) Cells Peripheral lymhoid tissue thymus Lymphoid stem cell CD8+ CD4+ CD4+ Treg CD8+ CTL + antigen Cytotoxic T lymphocyte CD4+ Th Helper T cell CD4+
Cell-Mediated Immunity and T Lymphocytes T helper (Th) Cells Peripheral lymhoid tissue thymus Lymphoid stem cell CD8+ CD4+ CD4+ Treg CD8+ CTL + antigen Cytotoxic T lymphocyte CD4+ Th Helper T cell CD4+
ADALIMUMAB Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW)
") Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Does the patient have a diagnosis of moderate to severe rheumatoid
Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Does the patient have a diagnosis of moderate to severe rheumatoid
Xeljanz. Xeljanz, Xeljanz XR (tofacitinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.24 Subject: Xeljanz Page: 1 of 5 Last Review Date: March 17, 2017 Xeljanz Description Xeljanz, Xeljanz
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.24 Subject: Xeljanz Page: 1 of 5 Last Review Date: March 17, 2017 Xeljanz Description Xeljanz, Xeljanz
Rheumatoid Arthritis Update
 Rheumatoid Arthritis Update Beth Valashinas, DO, FACOI, FACR Disclosures Speaker for AbbVie Pharmaceuticals Learning Objectives Upon completion of this session, participants should be able to discuss:
Rheumatoid Arthritis Update Beth Valashinas, DO, FACOI, FACR Disclosures Speaker for AbbVie Pharmaceuticals Learning Objectives Upon completion of this session, participants should be able to discuss:
Inflectra infliximab-dyyb. INFLECTRA (infliximab-dyyb) for injection available in the US 1
 for injection available in the US 1") First FDA-approved mab biosimilar 1 INFLECTRA (infliximab-dyyb) for injection available in the US 1 INFLECTRA is biosimilar* to and has the same recommended dosage as Remicade (infliximab) 2 * Biosimilar
First FDA-approved mab biosimilar 1 INFLECTRA (infliximab-dyyb) for injection available in the US 1 INFLECTRA is biosimilar* to and has the same recommended dosage as Remicade (infliximab) 2 * Biosimilar
Anti-TNF biologic agents Dr Lluís Puig
 Department of Dermatology Hospital de la Santa Creu i Sant Pau IPC NOVARTIS PSORIASIS PRECEPTORSHIP Anti-TNF biologic agents Dr Lluís Puig Barcelona, July 9th-10th, 2013 Anti-TNF therapy in the pathophysiology
Department of Dermatology Hospital de la Santa Creu i Sant Pau IPC NOVARTIS PSORIASIS PRECEPTORSHIP Anti-TNF biologic agents Dr Lluís Puig Barcelona, July 9th-10th, 2013 Anti-TNF therapy in the pathophysiology
INFLECTRA (infliximab-dyyb) for injection
 for injection") A-APPROVED INFLECTRA (infliximab-dyyb) for injection Product information INFLECTRA NDC 0069-0809-01 Unit quantity One 20-mL vial containing 100 mg of lyophilized infliximab-dyyb Unit list price $946.28
A-APPROVED INFLECTRA (infliximab-dyyb) for injection Product information INFLECTRA NDC 0069-0809-01 Unit quantity One 20-mL vial containing 100 mg of lyophilized infliximab-dyyb Unit list price $946.28
MEDICATION GUIDE XELJANZ (ZEL JANS ) (tofacitinib)
 (tofacitinib)") MEDICATION GUIDE XELJANZ (ZEL JANS ) (tofacitinib) Read this Medication Guide before you start taking XELJANZ and each time you get a refill. There may be new information. This Medication Guide does not
MEDICATION GUIDE XELJANZ (ZEL JANS ) (tofacitinib) Read this Medication Guide before you start taking XELJANZ and each time you get a refill. There may be new information. This Medication Guide does not
HUMIRA (adalimumab) injection, for subcutaneous use Initial U.S. Approval: 2002
 injection, for subcutaneous use Initial U.S. Approval: 2002") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use HUMIRA safely and effectively. See full prescribing information for HUMIRA. HUMIRA (adalimumab) injection,
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use HUMIRA safely and effectively. See full prescribing information for HUMIRA. HUMIRA (adalimumab) injection,
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: infliximab_remicade 5/2002 2/2017 2/2018 2/2017 Description of Procedure or Service Infliximab (REMICADE
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: infliximab_remicade 5/2002 2/2017 2/2018 2/2017 Description of Procedure or Service Infliximab (REMICADE
Center for Evidence-based Policy
 P&T Committee Brief Targeted Immune Modulators: Comparative Drug Class Review Alison Little, MD Center for Evidence-based Policy Oregon Health & Science University 3455 SW US Veterans Hospital Road, SN-4N
P&T Committee Brief Targeted Immune Modulators: Comparative Drug Class Review Alison Little, MD Center for Evidence-based Policy Oregon Health & Science University 3455 SW US Veterans Hospital Road, SN-4N
PATIENT ASSISTANCE PROGRAM APPLICATION Patient Application for XELJANZ XR (tofacitinib) extended release tablets/xeljanz (tofacitinib) tablets
 extended release tablets/xeljanz (tofacitinib) tablets") PATIENT ASSISTANCE PROGRAM APPLICATION Patient Application for XELJANZ XR (tofacitinib) extended release tablets/xeljanz (tofacitinib) tablets Phone 1-844-XELJANZ (1-844-935-5269) Fax 1-866-297-3471 2730
PATIENT ASSISTANCE PROGRAM APPLICATION Patient Application for XELJANZ XR (tofacitinib) extended release tablets/xeljanz (tofacitinib) tablets Phone 1-844-XELJANZ (1-844-935-5269) Fax 1-866-297-3471 2730
Anti-Tumor Necrosis Factor (Anti-TNF)
") Anti-Tumor Necrosis Factor (Anti-TNF) 110465 Anti-TNF.indd 1 9/20/16 9:01 AM s About your medicine Anti-tumor necrosis factor (anti-tnf) is a type of medicine called biologic agent that targets substance
Anti-Tumor Necrosis Factor (Anti-TNF) 110465 Anti-TNF.indd 1 9/20/16 9:01 AM s About your medicine Anti-tumor necrosis factor (anti-tnf) is a type of medicine called biologic agent that targets substance
TUBERCULOSIS AND THE TNF-α INHIBITORS. Lloyd Friedman, M.D. Yale University Milford Hospital
 TUBERCULOSIS AND THE TNF-α INHIBITORS Lloyd Friedman, M.D. Yale University Milford Hospital Outline TNF-α Anti-TNF-α medications Rates of tuberculosis Lower rates with etanercept Screening for latent tuberculosis
TUBERCULOSIS AND THE TNF-α INHIBITORS Lloyd Friedman, M.D. Yale University Milford Hospital Outline TNF-α Anti-TNF-α medications Rates of tuberculosis Lower rates with etanercept Screening for latent tuberculosis
Drug Class Prior Authorization Criteria Therapeutic Agents in Rheumatic and Inflammatory Diseases
 Drug Class Prior Authorization Criteria Therapeutic Agents in Rheumatic and Inflammatory Diseases Line of Business: Medicaid P & T Approval Date: August 16, 2017 Effective Date: August 16, 2017 This policy
Drug Class Prior Authorization Criteria Therapeutic Agents in Rheumatic and Inflammatory Diseases Line of Business: Medicaid P & T Approval Date: August 16, 2017 Effective Date: August 16, 2017 This policy
To report SUSPECTED ADVERSE REACTIONS, contact UCB, Inc. at or FDA at FDA-1088 or
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use CIMZIA safely and effectively. See full prescribing information for CIMZIA. CIMZIA (certolizumab
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use CIMZIA safely and effectively. See full prescribing information for CIMZIA. CIMZIA (certolizumab
Olumiant (baricitinib) tablets
 tablets") READ THIS FOR SAFE AND EFFECTIVE USE OF YOUR MEDICINE PATIENT MEDICATION INFORMATION OLUMIANTTM (Ō-loo'-mē-ant) baricitinib tablets Read this carefully before you start taking OLUMIANT and each time you
READ THIS FOR SAFE AND EFFECTIVE USE OF YOUR MEDICINE PATIENT MEDICATION INFORMATION OLUMIANTTM (Ō-loo'-mē-ant) baricitinib tablets Read this carefully before you start taking OLUMIANT and each time you
Olumiant (baricitinib) NEW PRODUCT SLIDESHOW
 NEW PRODUCT SLIDESHOW") Olumiant (baricitinib) NEW PRODUCT SLIDESHOW Introduction Brand name: Olumiant Generic name: Baricitinib Pharmacological class: Janus kinase (JAK) inhibitor Strength and Formulation: 2mg; tabs Manufacturer:
Olumiant (baricitinib) NEW PRODUCT SLIDESHOW Introduction Brand name: Olumiant Generic name: Baricitinib Pharmacological class: Janus kinase (JAK) inhibitor Strength and Formulation: 2mg; tabs Manufacturer:
ISSN: (Print) (Online) Journal homepage:
 (Online) Journal homepage:") mabs ISSN: 1942-0862 (Print) 1942-0870 (Online) Journal homepage: https://www.tandfonline.com/loi/kmab20 Certolizumab Pegol Niti Goel & Sue Stephens To cite this article: Niti Goel & Sue Stephens (2010)
mabs ISSN: 1942-0862 (Print) 1942-0870 (Online) Journal homepage: https://www.tandfonline.com/loi/kmab20 Certolizumab Pegol Niti Goel & Sue Stephens To cite this article: Niti Goel & Sue Stephens (2010)
Weeks 2 and 4, followed by 200 mg every other week may be considered.
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use CIMZIA safely and effectively. See full prescribing information for CIMZIA. CIMZIA (certolizumab
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use CIMZIA safely and effectively. See full prescribing information for CIMZIA. CIMZIA (certolizumab
London, 1 June 2006 Product name: REMICADE Procedure number: Remicade-H-240-II-73-AR SCIENTIFIC DISCUSSION 1/8
 London, 1 June 2006 Product name: REMICADE Procedure number: Remicade-H-240-II-73-AR SCIENTIFIC DISCUSSION 1/8 1. Introduction Infliximab is a chimeric human-murine IgG1κ monoclonal antibody, which binds
London, 1 June 2006 Product name: REMICADE Procedure number: Remicade-H-240-II-73-AR SCIENTIFIC DISCUSSION 1/8 1. Introduction Infliximab is a chimeric human-murine IgG1κ monoclonal antibody, which binds
Drug Class Review Targeted Immune Modulators
 Drug Class Review Targeted Immune Modulators Final Update 5 Report June 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
Drug Class Review Targeted Immune Modulators Final Update 5 Report June 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES HUMIRA PEDIATRIC
 Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 HUMIRA PEDIATRIC GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Is the patient currently taking Humira? If
Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 HUMIRA PEDIATRIC GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Is the patient currently taking Humira? If
Steps TO HELP YOU TALK WITH YOUR DOCTOR ABOUT YOUR TREATMENT OPTIONS
 Moderate to Severe Rheumatoid Arthritis (RA) 3 Steps TO HELP YOU TALK WITH YOUR DOCTOR ABOUT YOUR TREATMENT OPTIONS INDICATION/USAGE Adult Rheumatoid Arthritis (RA): ORENCIA (abatacept) is a prescription
Moderate to Severe Rheumatoid Arthritis (RA) 3 Steps TO HELP YOU TALK WITH YOUR DOCTOR ABOUT YOUR TREATMENT OPTIONS INDICATION/USAGE Adult Rheumatoid Arthritis (RA): ORENCIA (abatacept) is a prescription
2. Does the patient have a diagnosis of ulcerative colitis or Crohn s? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH LOUISIAA (MEDICAID) Remicade (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Pharmacy Prior Authorization AETA BETTER HEALTH LOUISIAA (MEDICAID) Remicade (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
HIGHLIGHTS OF PRESCRIBING INFORMATION
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use INFLECTRA safely and effectively. See full prescribing information for INFLECTRA. INFLECTRA (infliximab-dyyb)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use INFLECTRA safely and effectively. See full prescribing information for INFLECTRA. INFLECTRA (infliximab-dyyb)
1 of 61. WARNING: SERIOUS INFECTIONS and MALIGNANCY See full prescribing information for complete boxed warning
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use INFLECTRA safely and effectively. See full prescribing information for INFLECTRA. INFLECTRA (infliximab-dyyb)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use INFLECTRA safely and effectively. See full prescribing information for INFLECTRA. INFLECTRA (infliximab-dyyb)
DMARD s in Clinical Practice
 DMARD s in Clinical Practice Professor Md. Mahabubul Islam Majumder Professor & Head, Department of Medicine Comilla Medical College, Comilla Bangladesh Disease-modifying antirheumatic drugs (DMARDs) A
DMARD s in Clinical Practice Professor Md. Mahabubul Islam Majumder Professor & Head, Department of Medicine Comilla Medical College, Comilla Bangladesh Disease-modifying antirheumatic drugs (DMARDs) A
Xeljanz. Xeljanz, Xeljanz XR (tofacitinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.24 Subject: Xeljanz Page: 1 of 5 Last Review Date: March 18, 2016 Xeljanz Description Xeljanz, Xeljanz
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.24 Subject: Xeljanz Page: 1 of 5 Last Review Date: March 18, 2016 Xeljanz Description Xeljanz, Xeljanz
Immune Modulating Drugs Prior Authorization Request Form
 Patient: HPHC member ID #: Requesting provider: Phone: Servicing provider: Diagnosis: Contact for questions (name and phone #): Projected start and end date for requested Requesting provider NPI: Fax:
Patient: HPHC member ID #: Requesting provider: Phone: Servicing provider: Diagnosis: Contact for questions (name and phone #): Projected start and end date for requested Requesting provider NPI: Fax:
Corporate Medical Policy
 Corporate Medical Policy Infliximab, Infliximab-dyyb, Infliximab-abda File Name: Origination: Last CAP Review: Next CAP Review: Last Review: infliximab 5/2002 2/2018 2/2019 7/2018 Description of Procedure
Corporate Medical Policy Infliximab, Infliximab-dyyb, Infliximab-abda File Name: Origination: Last CAP Review: Next CAP Review: Last Review: infliximab 5/2002 2/2018 2/2019 7/2018 Description of Procedure
Drugs and Applicable Coding: J-code: Enbrel-J1438; Humira-J0135; Remicade-J1745; Inflectra-Q5102; Cimzia-J0718; Simponi-J1602 Renflexis - pending
 Policy Subject: Anti-TNF Agents Policy Number: SHS PBD16 Category: Rheumatology & Autoimmune Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS Individual
Policy Subject: Anti-TNF Agents Policy Number: SHS PBD16 Category: Rheumatology & Autoimmune Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS Individual
Amjevita (adalimumab-atto)
") *- Florida Healthy Kids Amjevita (adalimumab-atto) Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2 #* ^ prefilled
*- Florida Healthy Kids Amjevita (adalimumab-atto) Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2 #* ^ prefilled
Medical Coverage Guidelines are subject to change as new information becomes available.
 ENBREL (etanercept) Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
ENBREL (etanercept) Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
Otezla. Otezla (apremilast) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Otezla Page: 1 of 5 Last Review Date: March 16, 2018 Otezla Description Otezla (apremilast) Background
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Otezla Page: 1 of 5 Last Review Date: March 16, 2018 Otezla Description Otezla (apremilast) Background