CLOSER LOOK AT SpA. Dr. Mohamed Bedaiwi. Consultant Rheumatologist Rheumatology Unit - KKUH
|
|
|
- Rudolph Hudson
- 5 years ago
- Views:
Transcription


1 CLOSER LOOK AT SpA Dr. Mohamed Bedaiwi Consultant Rheumatologist Rheumatology Unit - KKUH

2
3
4 Closer look at SpA I. Categories II. SIGN & SYMPTOMS III. X-RAY IV. MRI V. MANAGMENT
5 Spondyloarthritis (SpA) diseases:??? What are they? 1. Ankylosing spondylitis (AS) 2. Non-radiographic axial spondyloarthritis (nraxspa 3. PsA 4. IBD related arthritis 5. ReA 6. Undifferentiated Peripheral SpA
6 Spondyloarthritis (SpA) diseases:??? What are they? 1. Ankylosing spondylitis (AS) 2. Non-radiographic axial spondyloarthritis (nraxspa 3. PsA 4. IBD related arthritis 5. ReA 6. Undifferentiated Peripheral SpA
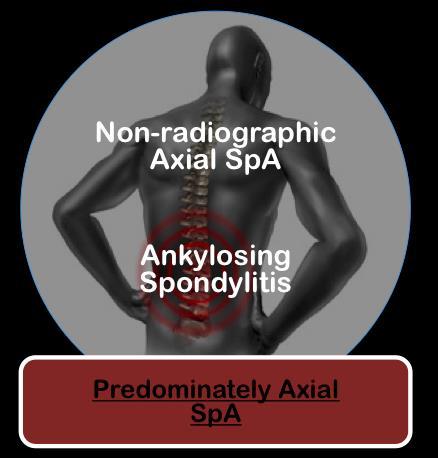
7 Complex disease 2 Broad Overlapping Categories Axial Spondyloarthritis Peripheral Spondyloarthritis PsA nr-axspa AS ReA IBD-SpA Undifferentiated Periphere SpA
8 Complex disease 2 Broad Overlapping Categories Axial Spondyloarthritis Periphere Spondyloarthritis PsA nr-axspa AS ReA IBD-SpA Undifferentiated Periphere SpA

9 SpA IS MISSED Observational prospective crosssectional cohort study at 48 community and academic centres in Germany 1511 patients with psoriasis Patients with joint symptoms were referred to a rheumatologist Among 1511 patients 20.6% had PsA 85% newly Dx
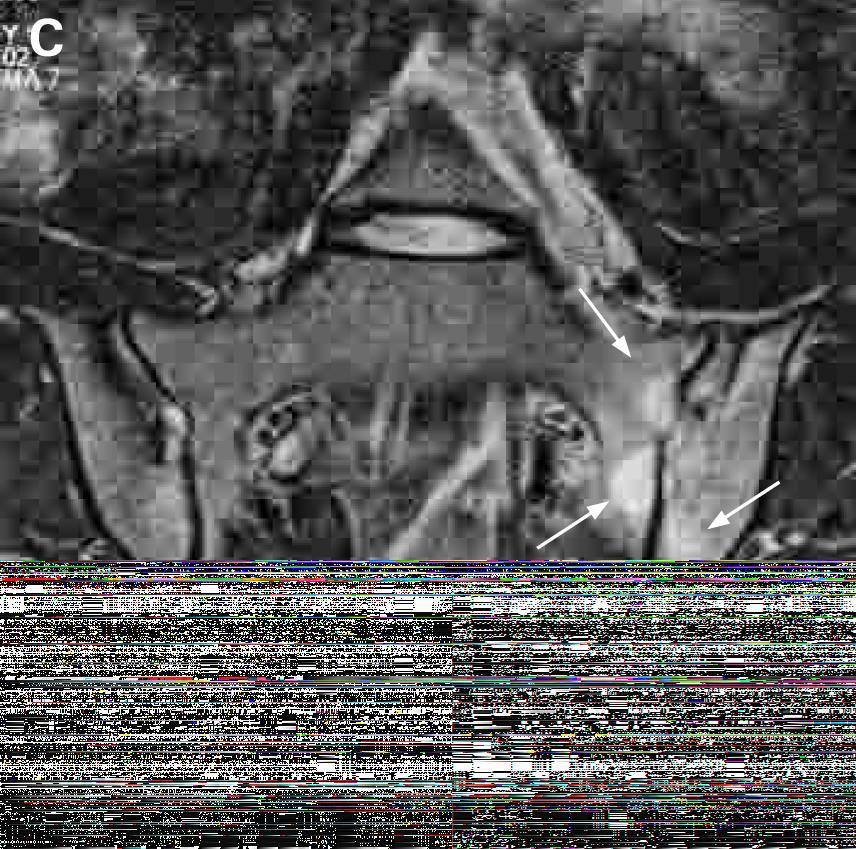
10 Ankylosing spondylitis Family medicine practice MRI?? is very valuable



11 Tips Good response to NSAIDs Symptoms Patient History Lab Genetics Imaging Dealing with a Solvable Problem
12 Back Pain 80% of the population will experience back pain during their lifetime. More than 85% cannot attribute it to a specific disease or spinal abnormality. Up to one third (1/3) of patients report persistent back pain of at least moderate intensity 1 year after an acute episode.


 Cancer")
13 Low Back Pain is caused by a specific disorder: Compression fracture Symptomatic herniated disc Spinal stenosis Ankylosing spondylitis (3%) Cancer Spinal infection



14 Inflammation is bad Inflammation is treatable Inflammation x Time = Damage

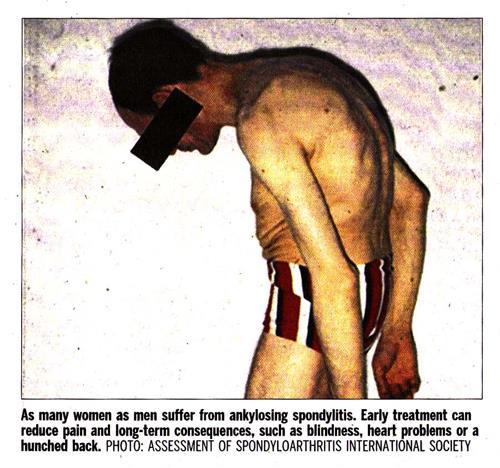
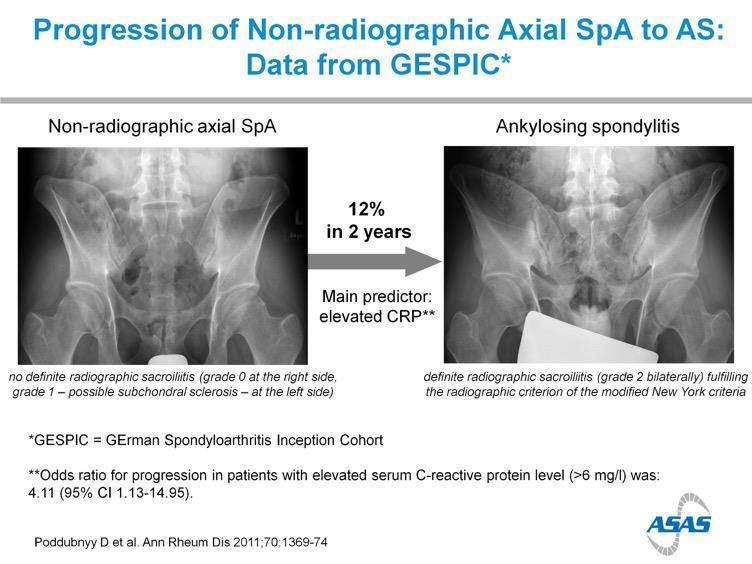
15 AS is progressive disease
16
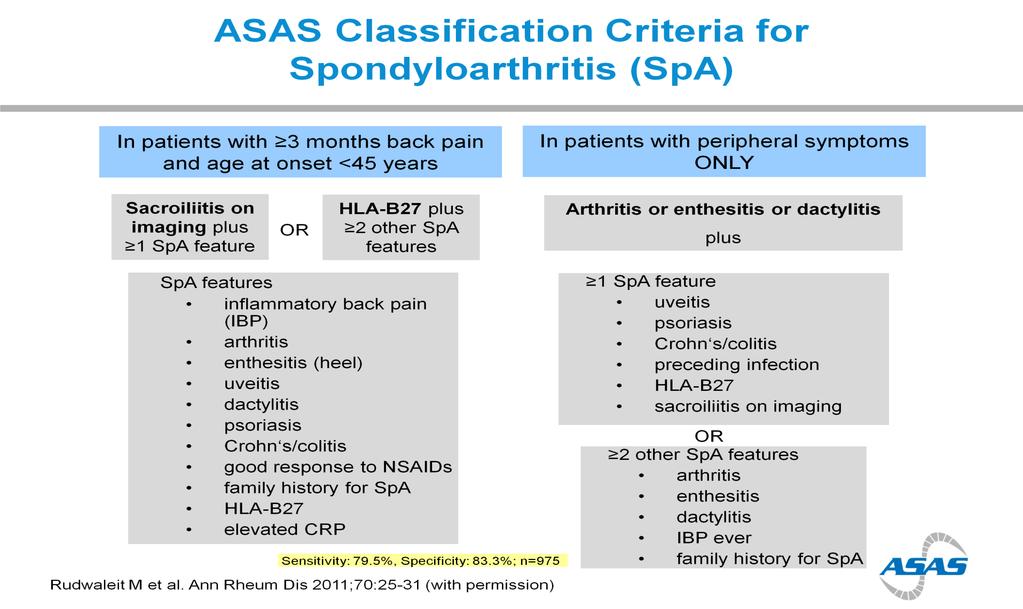
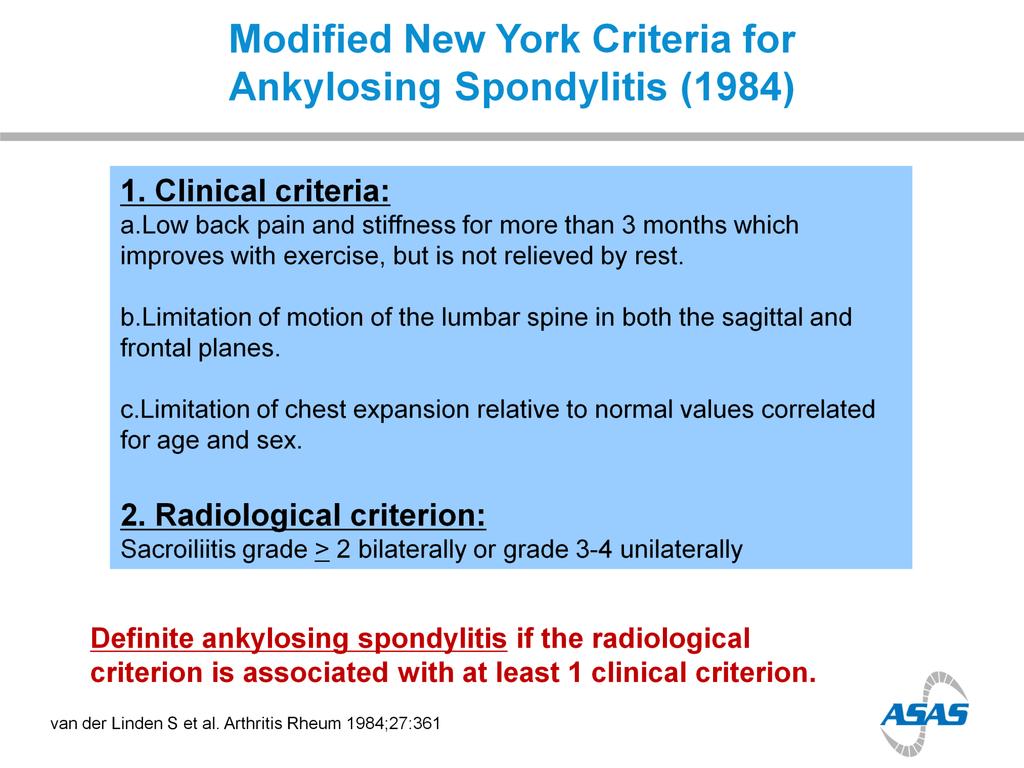
17 NEW YORK CRITERIA MRI?? Extra-articular features?? HLA-B27
18
19 ?

20 ?
21

22 Back Pain This Back in Focus resource was developed in collaboration with Claire Harris, Susan Gurden, Dr Jane Martindale, Claire Je ries and organized and funded by AbbVie. Date of Preparation: August 2015 Job Code: AXHUR150732
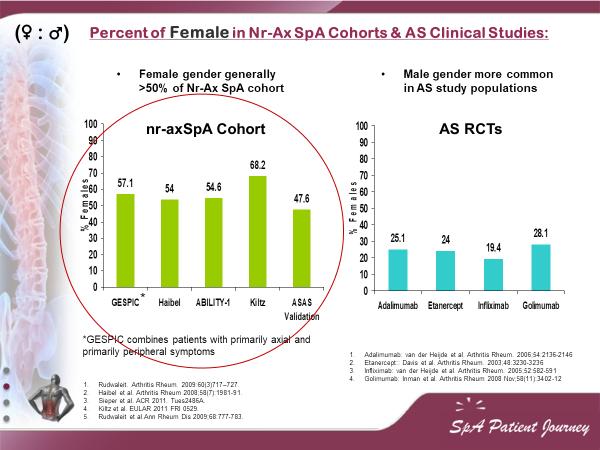
23 M vs F
24



25 Spondyloarthropathies SpA Is it only SPINE?
26 Updated ASAS Concept of Spondyloarthritis (SpA) Groups Diseases into 2 Broad Overlapping Categories Axial Spondyloarthritis nr-axspa AS Periphere Spondyloarthritis PsA ReA IBD-SpA Undifferentiated Periphere SpA van den Berg R, et al. Polskie Archiwum Medycyny Wewnętrznej. 2010;120(11):
27
, IBP")



28 Inflammatory Back Pain Tips Symptoms Patient History In patients with chronic back pain (>3 months), IBP criteria are fulfilled if at least 4 out of 5 parameters are present: I P A I N Lab Genetics Imaging Insidious onset No improvement with rest Pain at night Age at onset <45 years An insidious disease is any disease that comes on slowly and does not have obvious symptoms at first. The person is not aware of it developing. Improvement with exercise
 10% of")

29 Extra-articular Manifestations Uveitis 25-40% of patients affected Uveitis 25% of patients affected Psoriasis 16% of patients affected Axial Disease 40% of patients affected Inflammatory bowel Disease (IBD) 10% of patients affected (UC & CD) Nail Psoriasis 80-90% of patients affected at some point Dactylitis 21.5% of patients affected Synovial joint involvement Enthesitis 25-58% of patients affected Enthesitis 20% of patients affected
30 Heel Pain - Enthesitis Tips Symptoms Patient History Lab Enthesitis is inflammation of Entheses. Entheses are sites where tendons, ligaments, joint capsules, or fascia attach to bone. Heel Enthesitis is most common. Tenosynovitis Enthesitis Achilles heel Enthesitis Genetics Imaging Eshed I, et al. Ann Rheum Dis 2007;66:1553 9
31 Tips Symptoms Patient History Lab Genetics Imaging 25-58% of patients affected
32 Dactylitis Tips Symptoms Patient History Lab Genetics Imaging 21.5% of patients affected
33 Tips Symptoms Patient History Lab Genetics Imaging 25-40% of patients affected



34 Tips ESR & C-reactive protein Symptoms Patient History Lab Genetics Imaging Levels are increased up to 70% in most As. Patient. No relation with disease activity. If ESR or CRP is normal this doesn t reflect that there is no AS.
35 Tips Symptoms HLA-B27 Patient History Lab Genetics Imaging 90% to 95% of AS patient. Is neither necessary nor sufficient for the diagnosis of patient that their history and physical examination suggest AS. If the radiographic finding is not clear the lab, Test may be confirmatory.

36 Tips Symptoms HLA-B27 Patient History Lab Genetics Imaging
37
38 Tips Symptoms Patient History Lab Genetics Imaging
39 Tips Symptoms Patient History Lab Genetics Imaging
40 Tips Symptoms Patient History Lab Genetics Imaging
41 Q 22 y.o male. Inflammatory back pain for a year. Recurrent iritis. Family Hx of SpA Good response to NSAIDs What's the diagnosis Whats the next step?
42

43 Tips Symptoms Patient History Lab Genetics Imaging

44 Tips Symptoms Patient History Lab Genetics Imaging
45 Bilateral Grade 3 Radiographic Sacroiliitis: Bony Changes Inflammation is not Visible on Plain X-ray Tips Symptoms Patient History Lab Genetics Imaging Arrows point to sacroiliac (SI) joints *Note loss of the clear SI joint line and fluffy white area surrounding both SI joints
 joints *Note loss of the clear SI joint line and fluffy white area surrounding both SI")
46 Bilateral Grade 3 Radiographic Sacroiliitis: Bony Changes Inflammation is not Visible on Plain X-ray Tips Symptoms Patient History Lab Genetics Imaging Arrows point to sacroiliac (SI) joints *Note loss of the clear SI joint line and fluffy white area surrounding both SI joints

47 Bilateral Grade Radiographic Sacroiliitis: Bony Changes Tips Symptoms Patient History Lab Genetics Imaging



48 Spondylitis Tips Symptoms Patient History Lab Genetics Imaging Normal Ankylosing Spondylitis: Bamboo Spine, Lumbar Vertebrae Rheumatology Image Bank 2011 ACR AS Bamboo Spine Image Kelley s Textbook of Rheumatology. 2009:813.: Figure Radiopaedia.org

49 Ask Your Patients to bring their lumber MRI"
50
51 MRI

52 MRI
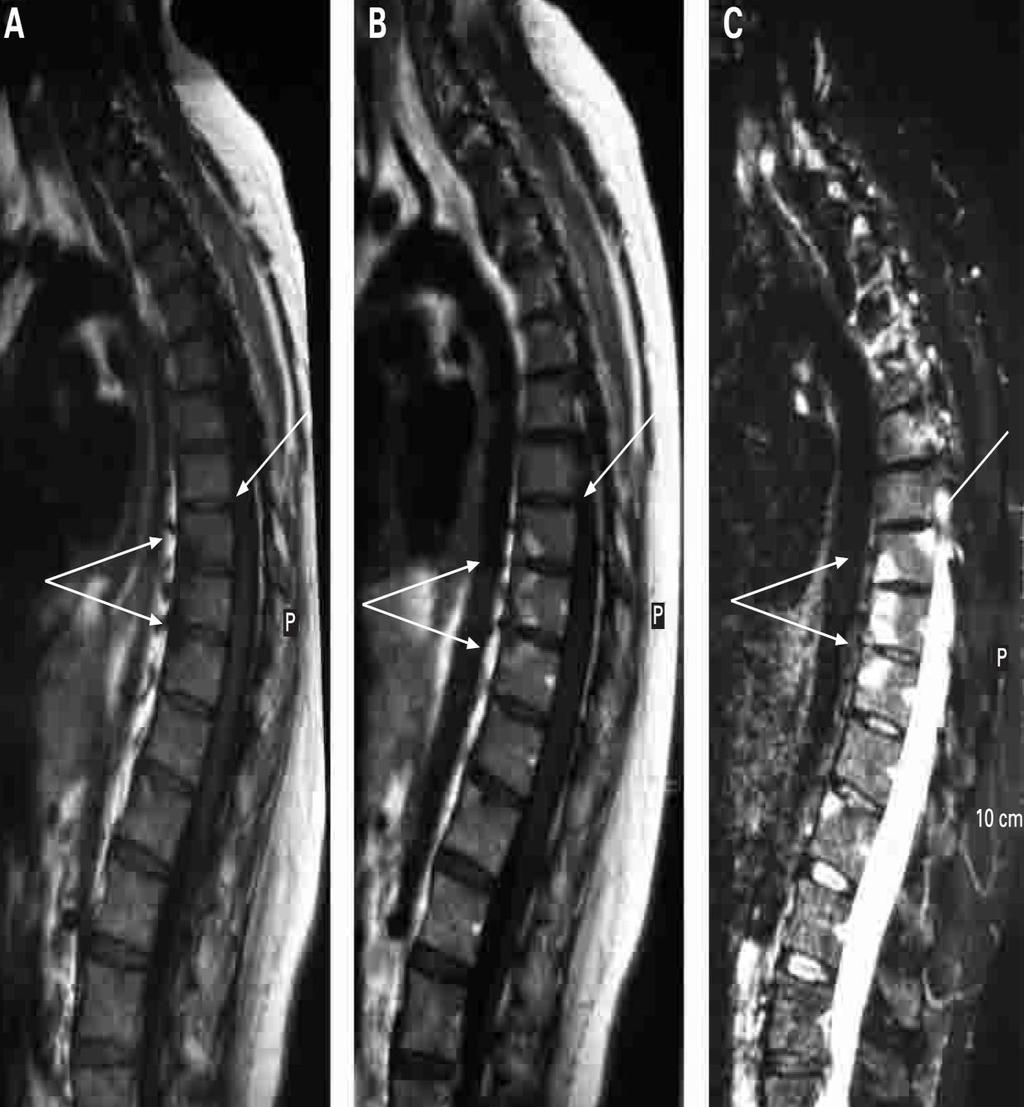
53 MRI
54
55 Complex disease SpA - Complex Overlapping diseases Axial Spondyloarthritis Periphere Spondyloarthritis PsA nr-axspa AS ReA IBD-SpA Undifferentiated Periphere SpA
56 Updated ASAS Concept of Spondyloarthritis (SpA) Groups Diseases into 2 Categories Axial Spondyloarthritis nr-axspa AS Periphere Spondyloarthritis PsA ReA IBD-SpA Undifferentiated Periphere SpA van den Berg R, et al. Polskie Archiwum Medycyny Wewnętrznej. 2010;120(11):
57 Tips Patterns Pathogene sis Morbidity





58 PsA is a chronic progressive disease Skin changes Swelling Affected nails Mutations Time/Years Psoriatic arthritis: Pictures of symptoms and progression
59 PsA Arthritis associated with psoriasis, Tips Patterns Pathogene sis Morbidity (a scaly rash, most frequently occurring on the elbows, knees, and scalp) Identifying features Psoriasis Other manifestations such as: peripheral arthritis, spondylitis, tenosynovitis, enthesitis, dactylitis. Olivieri I, et al. Imaging of psoriatic arthritis Reumatismo. 2007;59 Suppl 1:73-6 Khan MA. Ann Intern Med Update on Spondyloarthropathies Page 900 Kelley s Textbook of Rheumatology, 8th ed, 2009:
60 PsA Tips Patterns Pathogene sis Morbidity Psoriatic plaques typically precede development of the arthritic component. 7 42% of psoriasis (Ps) patients (in patient populations with severe Ps) may develop PsA. No correlation between the severity of psoriatic plaques and PsA has been identified. Equal gender distribution. ( : ) Peak years of onset typically between the ages of 20 and 40 Kelley s Textbook of Rheumatology. 2009, Page Moll JM, et al Semin Arthritis Rheum 1973;3:55 78; Kelley s Textbook of Rheumatology, 8th ed, 2009:
61 Patterns in PsA Pattern Features Rate Tips Asymmetrical Usually involves small joints, less frequently involves large joints Normally oligoarthritis ( 4 joints) ~ 47% Patterns Pathogene sis Symmetrical Involves small joints and large joints May be RF positive (clinically similar to RA) Arthritis may develop concurrently with psoriasis ~ 25% Morbidity Spondylitis SIJ and vertebrae affected asymmetrically More common in men May coexist with peripheral PsA Enthesitis prevalent ~ 23% DIP synovitis Restricted to only DIP joints Arthritis mutilans SIJ: sacroiliac joint Joint lysis Telescoping movement Gottlieb AB. Dermatol Nurs 2003;15:107 10; Harrison s Principles of Internal Medicine, 15th ed, 2001:2003 5



62 Patterns in PsA Some features are common to nearly all patterns of PsA: Tips Patterns Morning stiffness Nail disease Joint pain Pathogene sis Morbidity Harrison s Principles of Internal Medicine, 15th ed, 2001:2003 5

63 Asymmetric Psoriatic Arthritis Tips Patterns Pathogene sis Morbidity Asymmetric psoriatic arthritis typically involves one to three joints in the body -- large or small -- such as the knee, hip, or one or several fingers. Asymmetric psoriatic arthritis does not affect matching pairs of joints on opposite sides of the body.

64 Symmetric Psoriatic Arthritis Tips Patterns Pathogene sis Morbidity Symmetric psoriatic arthritis affects the same joints -- usually in multiple matching pairs -- on opposite sides of the body. Symmetric psoriatic arthritis can be disabling, causing varying degrees of progressive, destructive disease and loss of function in 50% of people with this type of arthritis. Symmetric psoriatic arthritis resembles rheumatoid arthritis.

65 Distal Interphalangeal Predominant (DIP) Tips Patterns Pathogene sis Morbidity Distal interphalangeal predominant psoriatic arthritis involves primarily the small joints in the fingers and toes closest to the nail. DIP psoriatic arthritis is sometimes confused with osteoarthritis, a chronic disease that causes the deterioration of joint cartilage and bone at the joints.

66 Arthritis Mutilans Tips Patterns Pathogene sis Morbidity Arthritis mutilans is a severe, deforming, and destructive form of psoriatic arthritis that primarily affects the small joints in the fingers and toes closest to the nail. This leads to loss of function of the involved joints. Fortunately, this severe type of psoriatic arthritis is rare.
67 Pathogenesis of PsA Tips Patterns Pathogene sis Morbidity Synovial hyperplasia and cellular infiltration. Pannus formation Cartilage erosion Prominent role for cytotoxic (CD8+) T cells Increased levels of TNFα found in joint. Pro-inflammatory effect Stimulation of proteases Associated enthesitis present. Veale DJ, et al. Ann Rheum Dis 2005;64(suppl 2):ii26 9 Gladman DD. Rheum Dis Clin North Am 1998;24:829 44
68 Median blister TNFα (pg/ml) TNFα Levels in Psoriatic skin blister fluids In a clinical trial, TNFα levels in psoriatic skin blister fluids were found to be much greater than in healthy control subjects Tips Patterns Control (normal skin blister fluids) Pathogene sis Morbidity Psoriatic involved skin blister fluids N = 30 (P = ) Bonifati, 384/2/Table 1 and 384/1/2 Bonifati C, et al. Clin Exp Dermatol. 1994;19:
69 Morbidity Associated With PsA Tips 40 57% of patients have deforming erosive arthropathy* Patterns Pathogene sis Morbidity 16% of patients with at least five deformed joints* 11 19% of patients with disability* *Data published in 1987 and These data may not accurately reflect current morbidity trends following recent medical advances Torre Alonso JC, et al. Br J Rheumatol 1991;30: Gladman DD, et al. Q J Med 1987;62:127 41

70 Diagnosis of PsA Patients Subclinical Clinical Imaging Criteria



71 Arthritis in the presence of psoriasis is the key to clinical diagnosis. Subclinical Clinical Imaging Criteria The onset depends on the subtype: Delayed after psoriasis onset: asymmetrical, spondylitis. Concurrent with psoriasis: symmetrical. Diagnosis is clinical and radiographic. Harrison's Principles of Internal Medicine, 15th ed, 2001: Gladman DD, et al. Q J Med 1987;62:127 41
72 Clinical Features of PsA Subclinical Clinical Imaging Criteria ACR: American College of Rheumatology Gladman DD, et al. Q J Med 1987;62: Clinical feature Patients (%) Actively inflamed joints 97 Plaque psoriasis 94 Nail lesions 83 DIP joint disease 54 Morning stiffness 52 Deformities: 1 / 5 43 / 16 Skin and joints flaring simultaneously 35 Dactylitis 33 Inflammatory neck pain and stiffness 23 Inflammatory back pain and stiffness 19 ACR functional class III/IV 11 Sacroiliac stress pain 10 Iritis 7

73 Actively inflamed joints Subclinical 97% of patients affected Clinical Imaging Criteria Plaque psoriasis 94% of patients affected scaly rash, most frequently occurring on the scalp, elbows and knees ACR: American College of Rheumatology Gladman DD, et al. Q J Med 1987;62:127 41

74 Subclinical Nails Clinical Imaging Criteria 83% of patients affected Fingernail pitting ACR: American College of Rheumatology Gladman DD, et al. Q J Med 1987;62:127 41



75 PIP and DIP synovitis Subclinical Clinical Imaging Criteria PIP = proximal interphalangeal. DIP = distal interphalangeal. ACR: American College of Rheumatology Gladman DD, et al. Q J Med 1987;62: Kelley s Textbook of Rheumatology, 8th ed, 2009: % of patients affected



76 Morning stiffness Subclinical 52% of patients affected Clinical Imaging Criteria Inflammatory neck pain and stiffness 23% of patients affected Inflammatory back pain and stiffness 19% of patients affected ACR: American College of Rheumatology Gladman DD, et al. Q J Med 1987;62:127 41
77 Subclinical Clinical Imaging Criteria ACR: American College of Rheumatology Gladman DD, et al. Q J Med 1987;62:127 41
78 Dactylitis Subclinical Clinical Imaging Criteria 33% of patients affected ACR: American College of Rheumatology Gladman DD, et al. Q J Med 1987;62:127 41

79 Heel Pain - Enthesitis Enthesitis is inflammation of Entheses. Entheses are sites where tendons, ligaments, joint capsules, or fascia attach to bone. Subclinical Heel Enthesitis is most common. Clinical Imaging Tenosynovitis Enthesitis Achilles heel Enthesitis Criteria Eshed I, et al. Ann Rheum Dis 2007;66:1553 9

80 Subclinical Clinical Imaging Criteria 20% of patients affected
81 Subclinical Clinical Imaging Criteria 25% of patients affected




82 PsA Radiologic Features Subclinical Clinical Imaging Characteristic peripheral joint destruction progresses to cause a pencil in cup appearance. Criteria In spondylitis subtype, may also see sacroiliitis and changes in the spine. Mease, P.J., et al. J Am Acad Dermatol 2005;52:1 19 Kelley s Textbook of Rheumatology, 8th ed, 2009:1207: Figure 72-5
83 Symptoms at presentation determine which pathway Subclinical Clinical Imaging Axial ± peripheral symptoms at time of presentation Purely peripheral symptoms at time of presentation* Criteria Apply ASAS Criteria for Axial SpA 1 Apply ASAS Criteria for Peripheral SpA 2 *Past inflammatory back pain allowed 1 Rudwaleit et al. Ann Rheum Dis 2009;68: Rudwaleit et al. Ann Rheum Dis 2011;70:25-31.
84 Subclinical Clinical Imaging Criteria
85 PsA Patient Equal gender distribution ( : ) Age at onset years Neck Pain & Stiffness Plaque psoriasis (a scaly rash, most frequently occurring on the elbows, knees, and scalp) DIP joint disease Nail lesions or pitting Tenosynovitis (inflammation of the synovium that surrounds a tendon, typically leading to joint pain, swelling, and stiffness. It can be either infectious or noninfectious) Morning stiffness Deformities Family History of SpA +ve HLA-B27 Eye inflammation Inflammatory Back Pain (IBP) Crohn s/ Colitis Joints Arthritis Dactylitis Enthesitis

86 Axial-SpA Patient Journey Derma Clinic 7 42% of psoriasis (Ps) patients may develop PsA. No correlation between the severity of psoriatic plaques and PsA has been identified. Ophtha Clinic 25% of patients may have uveitis Pain Clinic Family Medicine Clinic






87 Derma Clinic Ophtha Clinic Pain Clinic Family Medicine Clinic ESR,CRP, HLA-B27









88 Arthritis Dactylitis Enthesitis or or Age at onset years old Psoriasis Uveitis IBP Crohn s/ Colitis Family History or or or or Yes Start confirmation -Involved joints X-ray -HLA B27 Connect to Rheumatologist
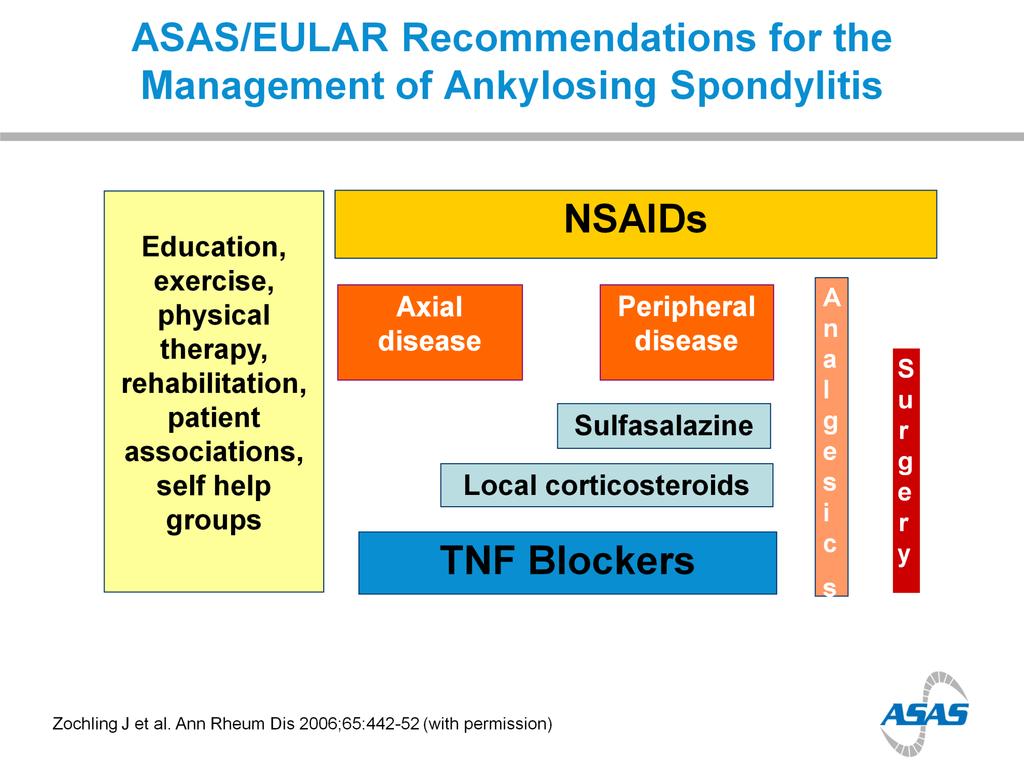
89 EULAR Treatment Algorithm for PsA Phase I Adverse prognostic factors (± major skin involvement) Go directly to phase II Clinical diagnosis of active psoriatic arthritis Start NSAIDS ± local glucocorticoid injections Major skin involvement (also in phase II IV) Consider consulting a dermatologist Failure phase I: go to phase II No Achieve target within 3 6 months Yes Continue Recommendation Algorithm Phase II Contraindication for methotrexate Lack of efficacy and/or toxicity in phase I (or adverse prognostic factors) Predominantly axial disease or severe enthesitis Start leflunomide or sulfasalazine (or cyclosporine A) Start methotrexate (consider appropriate dosage) Go directly to phase III Failure phase II: go to phase III No Achieve target within 3 6 months Yes Continue Gossec L et al., Ann Rheum Dis Jan;71(1):4-12
90 EULAR Treatment Algorithm for PsA Phase III Arthritis with adverse prognostic factors Start a TNF-inhibitor (± DMARD) Lack of efficacy and/or toxicity in phase II No Predominant axial disease or enthesis Achieve target within 3 6 months Arthritis without adverse prognostic factors Start a second synthetic DMARD Leflunomide, Sulfasalazine, MTX, or Cyclosporine A (or combination therapy) Recommendation Algorithm Failure phase III: go to phase IV Phase IV Achieve target No Yes Continue within 3 6 months Lack of efficacy and/or toxicity in phase III Change the biologic treatment. Switch to a second TNF-blocking drug (± DMARD) Gossec L et al., Ann Rheum Dis Jan;71(1):4-12 Achieve target No Yes Continue within 3 6 months
91 GRAPPA Treatment Recommendations for PsA (2009) Establish diagnosis of PsA Peripheral arthritis Skin and nail disease Axial disease Dactylitis Enthesitis Recommendation Algorithm Initiate therapy: NSAIDs IA steroids DMARDs ((MTX, CsA, SSZ, LEF) Biologics (anti-tnfs) Initiate therapy: Topicals PUVA/UVB Systemics (MTX, CsA, etc.) Biologics (anti-tnfs) Initiate therapy: NSAID Physiotherapy Biologics (anti-tnfs) Initiate therapy: NSAID Injection Biologics (anti-tnfs) Initiate therapy: NSAID Injection Biologics (anti-tnfs) Reassess response to therapy and toxicity Ritchlin C, et al. ARD 2009; 68:
92 Reactive arthritis Reactive arthritis is a rare disease even among rheumatology practices. Reactive arthritis has been defined by consensus as a form of arthritis that is associated with a coexisting extraarticular infection.
93 Reactive arthritis Only certain enteric and genitourinary pathogens are conventionally accepted as capable of causing reactive arthritis. Chlamydia trachomatis, Yersinia, Salmonella, Shigella, Campylobacter, Clostridioides (formerly Clostridium) difficile, and Chlamydia pneumoniae.
94 Reactive arthritis Musculoskeletal features of reactive arthritis typically develop one to four weeks following an acute infection with one of the triggering organisms. At least one of the following is seen in all patients with this condition: asymmetric oligoarthritis (often affecting the lower extremities) enthesitis dactylitis inflammatory back pain.
95 Extraarticular manifestations occur in some patients, but none are specific for reactive arthritis. These include eye involvement, most often with conjunctivitis, but infrequently with anterior uveitis genitourinary tract symptoms oral mucosal ulcers cutaneous manifestations such as keratoderma blennorrhagica, circinate balanitis, and psoriasis-like nail changes.
96 Laboratory findings may include evidence of the infection, elevated acute phase reactants, and findings of inflammatory joint fluid in patients with arthritis.
97 Antibiotic therapy should be used for treatment of active Chlamydia trachomatis infection, if present. In general, antibiotics are not indicated for uncomplicated enteric infections or for treatment of the arthritis itself. We suggest treatment of arthritis in most patients initially with nonsteroidal antiinflammatory drugs (NSAIDs) In patients who do not respond adequately to NSAIDs, we suggest intraarticular glucocorticoids, rather than initiating therapy with daily oral glucocorticoids or a DMARD.
98 In patients who do not respond adequately to NSAIDs and intraarticular glucocorticoid injections, we suggest low to moderate doses of systemic glucocorticoids, rather than initiating treatment with a DMARD. A typical dose would be prednisone, 20 mg daily, titrated to the lowest dose required to control symptoms
99 In patients who have not responded adequately to NSAIDs over at least four weeks and who require ongoing therapy with more than 7.5 mg of prednisone or equivalent for more than three to six months we suggest a trial of a nonbiologic DMARD, rather than continuing moderate to high dose glucocorticoids without a DMARD. We usually prescribe sulfasalazine. Methotrexate is an alternative to SSZ.
100 The prognosis is good in the majority of patients, with spontaneous remission within 6 to 12 months of onset of arthritis. However, some patients have persistent but mild musculoskeletal symptoms, and others develop radiologic evidence of joint injury and evolve to a more chronic form of SpA.
101
102
103
Seronegative Spondyloarthropathies (SpA)
") Seronegative Spondyloarthropathies (SpA) Objectives: Introduction SpA disease information Pathogenesis Clinical features Team Members: Ameera Niazi - Lulwah AlShiha - Qaiss Almuhaideb - Abdullah Hashem
Seronegative Spondyloarthropathies (SpA) Objectives: Introduction SpA disease information Pathogenesis Clinical features Team Members: Ameera Niazi - Lulwah AlShiha - Qaiss Almuhaideb - Abdullah Hashem
What is Axial Spondyloarthritis?
 Physiotherapist Module 2 What is Axial Spondyloarthritis? How does it apply to physiotherapists? Claire Harris, Senior Physiotherapist, London North West Healthcare NHS Trust Susan Gurden, Advanced Physiotherapy
Physiotherapist Module 2 What is Axial Spondyloarthritis? How does it apply to physiotherapists? Claire Harris, Senior Physiotherapist, London North West Healthcare NHS Trust Susan Gurden, Advanced Physiotherapy
Juvenile Spondyloarthritis / Enthesitis Related Arthritis (SpA-ERA)
") www.printo.it/pediatric-rheumatology/gb/intro Juvenile Spondyloarthritis / Enthesitis Related Arthritis (SpA-ERA) Version of 2016 1. WHAT IS JUVENILE SPONDYLOARTHRITIS/ENTHESITIS- RELATED ARTHRITIS (SpA-ERA)
www.printo.it/pediatric-rheumatology/gb/intro Juvenile Spondyloarthritis / Enthesitis Related Arthritis (SpA-ERA) Version of 2016 1. WHAT IS JUVENILE SPONDYLOARTHRITIS/ENTHESITIS- RELATED ARTHRITIS (SpA-ERA)
 www.fisiokinesiterapia.biz Peak onset between 20 and 30 years Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27 Prevalence as high
www.fisiokinesiterapia.biz Peak onset between 20 and 30 years Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27 Prevalence as high
EXAMINING THE CRUCIAL COALITION BETWEEN DERMATOLOGY AND RHEUMATOLOGY IN PSORIATIC ARTHRITIS
 EXAMINING THE CRUCIAL COALITION BETWEEN DERMATOLOGY AND RHEUMATOLOGY IN PSORIATIC ARTHRITIS ACTIVITY 1: EARLY COLLABORATION IN THE TREATMENT OF PSA Key Slides COMMON COMORBIDITIES OF PSORIATIC DISEASE
EXAMINING THE CRUCIAL COALITION BETWEEN DERMATOLOGY AND RHEUMATOLOGY IN PSORIATIC ARTHRITIS ACTIVITY 1: EARLY COLLABORATION IN THE TREATMENT OF PSA Key Slides COMMON COMORBIDITIES OF PSORIATIC DISEASE
Rheumatology and Internal Diseases Clinic of the Central Clinical Hospital in Warsaw 137 Woloska St. WARSAW POLAND prof. Małgorzata Wisłowska
 Rheumatology and Internal Diseases Clinic of the Central Clinical Hospital in Warsaw 137 Woloska St. WARSAW 02-507 POLAND prof. Małgorzata Wisłowska MD, PhD 1 Klinika Chorób Wewnętrznych i Reumatologii
Rheumatology and Internal Diseases Clinic of the Central Clinical Hospital in Warsaw 137 Woloska St. WARSAW 02-507 POLAND prof. Małgorzata Wisłowska MD, PhD 1 Klinika Chorób Wewnętrznych i Reumatologii
EARLY INFLAMMATORY ARTHRITIS. Cristina Tacu Consultant Rheumatologist Brighton and Sussex University Hospital
 EARLY INFLAMMATORY ARTHRITIS Cristina Tacu Consultant Rheumatologist Brighton and Sussex University Hospital EIA: Introduction National priority Preventable cause of disability Very common condition High
EARLY INFLAMMATORY ARTHRITIS Cristina Tacu Consultant Rheumatologist Brighton and Sussex University Hospital EIA: Introduction National priority Preventable cause of disability Very common condition High
A Patient s Guide to Psoriatic Arthritis
 A Patient s Guide to Psoriatic Arthritis Glendale Adventist Medical Center 1509 Wilson Terrace Glendale, CA 91206 Phone: (818) 409-8000 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Psoriatic Arthritis Glendale Adventist Medical Center 1509 Wilson Terrace Glendale, CA 91206 Phone: (818) 409-8000 DISCLAIMER: The information in this booklet is compiled from a variety
Identification of Psoriatic Arthritis and Ankylosing Spondylitis Early Detection to Facilitate Appropriate Care
 Identification of Psoriatic Arthritis and Ankylosing Spondylitis Early Detection to Facilitate Appropriate Care Joy Schechtman D.O. Professor Midwestern University 64C-1876207 Disclosures None 3 64C-1876207
Identification of Psoriatic Arthritis and Ankylosing Spondylitis Early Detection to Facilitate Appropriate Care Joy Schechtman D.O. Professor Midwestern University 64C-1876207 Disclosures None 3 64C-1876207
Axial Spondyloarthritis. Doug White, Rheumatologist Waikato Hospital
 Axial Spondyloarthritis Doug White, Rheumatologist Waikato Hospital Disclosures Presentations / Consulting Abbott Laboratories AbbVie MSD Novartis Roche Clinical Trials Abbott Laboratories AbbVie Actelion
Axial Spondyloarthritis Doug White, Rheumatologist Waikato Hospital Disclosures Presentations / Consulting Abbott Laboratories AbbVie MSD Novartis Roche Clinical Trials Abbott Laboratories AbbVie Actelion
8/29/2012. Outline Juvenile idiopathic arthritis. 1. Classification-ILAR. 1. Classification-clinical diagnosis. 1. JIA classification
 Outline Juvenile idiopathic arthritis 1. Classification and symptoms (ILAR-International league of Associations for Rheumatology) 2. Imaging J. Herman Kan, M.D. Section chief, musculoskeletal imaging Edward
Outline Juvenile idiopathic arthritis 1. Classification and symptoms (ILAR-International league of Associations for Rheumatology) 2. Imaging J. Herman Kan, M.D. Section chief, musculoskeletal imaging Edward
Assessing the Signs, Symptoms, and Clinical Manifestations of Axial SpA
 Physiotherapist Module 3 Assessing the Signs, Symptoms, and Clinical Manifestations of Axial SpA Enhance your patient examination skills Claire Harris, Senior Physiotherapist, London North West Healthcare
Physiotherapist Module 3 Assessing the Signs, Symptoms, and Clinical Manifestations of Axial SpA Enhance your patient examination skills Claire Harris, Senior Physiotherapist, London North West Healthcare
SpA non-radiografica: fase precoce di spondilite anchilosante o altro?
 Rheumatology Department of Lucania, S. Carlo Hospital of Potenza and Madonna delle Grazie Hospital of Matera SpA non-radiografica: fase precoce di spondilite anchilosante o altro? Ignazio Olivieri Disclosures
Rheumatology Department of Lucania, S. Carlo Hospital of Potenza and Madonna delle Grazie Hospital of Matera SpA non-radiografica: fase precoce di spondilite anchilosante o altro? Ignazio Olivieri Disclosures
9 Lecture. Spondyloarthropathy แพทย หญ งน นทนา กส ตานนท คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม
 9 Lecture Spondyloarthropathy แพทย หญ งน นทนา กส ตานนท คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม Spondyloarthritis: SpA Nuntana Kasitanon Division of Rheumatology Department of Medicine Spondyloarthritis: SpA
9 Lecture Spondyloarthropathy แพทย หญ งน นทนา กส ตานนท คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม Spondyloarthritis: SpA Nuntana Kasitanon Division of Rheumatology Department of Medicine Spondyloarthritis: SpA
37 year old male with several year history of back pain
 37 year old male with several year history of back pain Inflammatory Low Back Pain Clues onset before the age of 40 years insidious onset, chronic (>3 months) pain morning stiffness for longer than 30
37 year old male with several year history of back pain Inflammatory Low Back Pain Clues onset before the age of 40 years insidious onset, chronic (>3 months) pain morning stiffness for longer than 30
Chapter 2. Overview of ankylosing spondylitis
 Chapter 2 Overview of ankylosing spondylitis The concept and classification of spondyloarthritis The term spondyloarthritis (SpA) comprises AS, reactive arthritis, arthritis/spondylitis associated with
Chapter 2 Overview of ankylosing spondylitis The concept and classification of spondyloarthritis The term spondyloarthritis (SpA) comprises AS, reactive arthritis, arthritis/spondylitis associated with
Differentiating Inflammatory and Mechanical Back Pain
 This resource was organised and funded by AbbVie. It has been developed in collaboration with Claire Harris, Susan Gurden, Dr Jane Martindale, Claire Jeffries and NASS. For UK healthcare professionals
This resource was organised and funded by AbbVie. It has been developed in collaboration with Claire Harris, Susan Gurden, Dr Jane Martindale, Claire Jeffries and NASS. For UK healthcare professionals
Assessing the Signs, Symptoms, and Clinical Manifestations of Axial SpA
 This resource was organised and funded by AbbVie. It has been developed in collaboration with Claire Harris, Susan Gurden, Dr Jane Martindale, Claire Jeffries and NASS. For UK healthcare professionals
This resource was organised and funded by AbbVie. It has been developed in collaboration with Claire Harris, Susan Gurden, Dr Jane Martindale, Claire Jeffries and NASS. For UK healthcare professionals
Update - Imaging of the Spondyloarthropathies. Spondyloarthropathies. Spondyloarthropathies
 Update - Imaging of the Spondyloarthropathies Donald J. Flemming, M.D. Dept of Radiology Penn State Hershey Medical Center Spondyloarthropathies Family of inflammatory arthritides of synovium and entheses
Update - Imaging of the Spondyloarthropathies Donald J. Flemming, M.D. Dept of Radiology Penn State Hershey Medical Center Spondyloarthropathies Family of inflammatory arthritides of synovium and entheses
Concept of Spondyloarthritis (SpA)
") Concept of Spondyloarthritis (SpA) Spondyloarthritis: Characteristic Parameters Used for Diagnosis I Symptoms Inflammatory back pain Imaging Lab ESR/CRP Patient s history Good response to NSAIDs Spondyloarthritis-Characteristic
Concept of Spondyloarthritis (SpA) Spondyloarthritis: Characteristic Parameters Used for Diagnosis I Symptoms Inflammatory back pain Imaging Lab ESR/CRP Patient s history Good response to NSAIDs Spondyloarthritis-Characteristic
1. Joining the Dots in Psoriatic Arthritis; 2. Reaching for a Cure for Hep C
 Dr Daniel Ching Consultant Rheumatologist Timaru Hospital Dr Catherine Stedman Gastroenterologist Hepatologist, Christchurch Hospital, Clinical Senior Lecturer, University Otago 7:00-8:00 Abbvie Breakfast
Dr Daniel Ching Consultant Rheumatologist Timaru Hospital Dr Catherine Stedman Gastroenterologist Hepatologist, Christchurch Hospital, Clinical Senior Lecturer, University Otago 7:00-8:00 Abbvie Breakfast
Dr Tracey Kain. Associate Professor Ed Gane
 Associate Professor Ed Gane New Zealand Liver Transplant Unit Auckland Dr Tracey Kain Consultant Rheumatologist Grace Orthopaedic Centre Tauranga Hospital Tauranga 7:00-7:55 Abbvie Breakfast Session 1.
Associate Professor Ed Gane New Zealand Liver Transplant Unit Auckland Dr Tracey Kain Consultant Rheumatologist Grace Orthopaedic Centre Tauranga Hospital Tauranga 7:00-7:55 Abbvie Breakfast Session 1.
2018 ReachMD Page 1 of 10
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Rheumatoid Arthritis. Rheumatoid Arthritis. RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling. Rheumatic Diseases
 RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling Rheumatic Diseases The prevalence of rheumatoid arthritis in most Caucasian populations approaches 1% among adults 18 and over and
RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling Rheumatic Diseases The prevalence of rheumatoid arthritis in most Caucasian populations approaches 1% among adults 18 and over and
Psoriatic Arthritis Shared Decision Making
 Psoriatic Arthritis Shared Decision Making Disease Modifying Drug Therapy DMARDs Therapy El Miedany et al. Ann Rheum Dis 74(Suppl2): 1002 DOI: 10.1136/annrheumdis-2015-eular.1410 www.rheumatology4u.com
Psoriatic Arthritis Shared Decision Making Disease Modifying Drug Therapy DMARDs Therapy El Miedany et al. Ann Rheum Dis 74(Suppl2): 1002 DOI: 10.1136/annrheumdis-2015-eular.1410 www.rheumatology4u.com
A Patient s Guide to Spondyloarthropathies
 A Patient s Guide to Spondyloarthropathies 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Spondyloarthropathies 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is compiled from a variety
Juvenile Idiopathic Arthritis (JIA)
") Juvenile Idiopathic Arthritis (JIA) Kaveh Ardalan, MD, MS Division of Rheumatology Ann & Robert H. Lurie Children s Hospital of Chicago Assistant Professor, Pediatrics and Medical Social Sciences Northwestern
Juvenile Idiopathic Arthritis (JIA) Kaveh Ardalan, MD, MS Division of Rheumatology Ann & Robert H. Lurie Children s Hospital of Chicago Assistant Professor, Pediatrics and Medical Social Sciences Northwestern
Seronegative Arthritis. Dr Mary Gayed 25 th April 2018
 Seronegative Arthritis Dr Mary Gayed 25 th April 2018 Overview Description of the conditions Discussion of symptoms & investigations that may be required Discussion of management and treatment Questions
Seronegative Arthritis Dr Mary Gayed 25 th April 2018 Overview Description of the conditions Discussion of symptoms & investigations that may be required Discussion of management and treatment Questions
Gender differences in effectiveness of treatment in rheumatic diseases
 Gender differences in effectiveness of treatment in rheumatic diseases Irene van der Horst-Bruinsma Associate Professor Rheumatology Center of Excellence of Axial Spondyloarthritis ARC/VU University Medical
Gender differences in effectiveness of treatment in rheumatic diseases Irene van der Horst-Bruinsma Associate Professor Rheumatology Center of Excellence of Axial Spondyloarthritis ARC/VU University Medical
DIFFERENTIATING INFLAMMATORY AND MECHANICAL BACK PAIN
 DIFFERENTIATING INFLAMMATORY AND MECHANICAL BACK PAIN CHALLENGE YOUR DECISION MAKING Claire Harris, Senior Physiotherapist, The North West London Hospitals NHS Trust Susan Gurden, Advanced Physiotherapy
DIFFERENTIATING INFLAMMATORY AND MECHANICAL BACK PAIN CHALLENGE YOUR DECISION MAKING Claire Harris, Senior Physiotherapist, The North West London Hospitals NHS Trust Susan Gurden, Advanced Physiotherapy
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Proposed Health Technology Appraisal Secukinumab for treating ankylosing spondylitis after inadequate response to non-steroidal anti-inflammatory drugs
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Proposed Health Technology Appraisal Secukinumab for treating ankylosing spondylitis after inadequate response to non-steroidal anti-inflammatory drugs
Spondyloarthritis: Practice. New Concepts in. Epidemiology and Clinical
 New Concepts in Spondyloarthritis: Epidemiology and Clinical Practice Atul Deodhar MD Professor of Medicine Oregon Health & Science University Portland, OR Northwest Rheumatism Society, Seattle, April
New Concepts in Spondyloarthritis: Epidemiology and Clinical Practice Atul Deodhar MD Professor of Medicine Oregon Health & Science University Portland, OR Northwest Rheumatism Society, Seattle, April
Juvenile Spondyloarthritis / Enthesitis Related Arthritis (SpA-ERA)
") www.printo.it/pediatric-rheumatology/gb/intro Juvenile Spondyloarthritis / Enthesitis Related Arthritis (SpA-ERA) Version of 2016 1. WHAT IS JUVENILE SPONDYLOARTHRITIS/ENTHESITIS- RELATED ARTHRITIS (SpA-ERA)
www.printo.it/pediatric-rheumatology/gb/intro Juvenile Spondyloarthritis / Enthesitis Related Arthritis (SpA-ERA) Version of 2016 1. WHAT IS JUVENILE SPONDYLOARTHRITIS/ENTHESITIS- RELATED ARTHRITIS (SpA-ERA)
Hands On PSORIATIC ARTHRITIS ITS PRESENTATION AND MANAGEMENT IN PRIMARY CARE. Introduction EDITORIAL. How common is psoriatic arthritis?
 REPORTS ON THE RHEUMATIC DISEASES SERIES 6 Hands On Practical advice on management of rheumatic disease PSORIATIC ARTHRITIS ITS PRESENTATION AND MANAGEMENT IN PRIMARY CARE Philip S Helliwell Senior Lecturer
REPORTS ON THE RHEUMATIC DISEASES SERIES 6 Hands On Practical advice on management of rheumatic disease PSORIATIC ARTHRITIS ITS PRESENTATION AND MANAGEMENT IN PRIMARY CARE Philip S Helliwell Senior Lecturer
Spondylarthropathies
 www.fisiokinesiterapia.biz Spondylarthropathies Spondylarthropathies Undifferentiated Ankylosis spondylitis Psoriatic arthritis Enteropathic arthritis Reactive arthritis (and Reiter syndrome) Spondylarthropathies
www.fisiokinesiterapia.biz Spondylarthropathies Spondylarthropathies Undifferentiated Ankylosis spondylitis Psoriatic arthritis Enteropathic arthritis Reactive arthritis (and Reiter syndrome) Spondylarthropathies
JUVENILE SPONDYLOARTHROPATHIES
 www.pediatric-rheumathology.printo.it JUVENILE SPONDYLOARTHROPATHIES What is it? The juvenile spondyloarthropathies constitute are a group of chronic inflammatory diseases of the joints (arthritis) and
www.pediatric-rheumathology.printo.it JUVENILE SPONDYLOARTHROPATHIES What is it? The juvenile spondyloarthropathies constitute are a group of chronic inflammatory diseases of the joints (arthritis) and
Assessment of Inflammatory Back Pain: New Concepts in Diagnosis
 Assessment of Inflammatory Back Pain: New Concepts in Diagnosis March 2 nd, 2018 Spine Therapy Network Interprofessional Synposium Sheraton Toronto Airport Hotel, Toronto, CANADA Laura Passalent PT, BScPT,
Assessment of Inflammatory Back Pain: New Concepts in Diagnosis March 2 nd, 2018 Spine Therapy Network Interprofessional Synposium Sheraton Toronto Airport Hotel, Toronto, CANADA Laura Passalent PT, BScPT,
Where has SARA gone? Prof. David Kane Consultant Rheumatologist Beacon & Tallaght Hospitals. Clinical Professor in Rheumatology Trinity College Dublin
 Where has SARA gone? Prof. David Kane Consultant Rheumatologist Beacon & Tallaght Hospitals Clinical Professor in Rheumatology Trinity College Dublin 1 Reactive Arthritis Seronegative Asymmetrical Arthritis
Where has SARA gone? Prof. David Kane Consultant Rheumatologist Beacon & Tallaght Hospitals Clinical Professor in Rheumatology Trinity College Dublin 1 Reactive Arthritis Seronegative Asymmetrical Arthritis
Sronegative Spondyloarthropathies. Dr. M Jokar
 Sronegative Spondyloarthropathies Dr. M Jokar 1 Definition The spondyloarthropathies are a group of disorders that share certain clinical features and an association with the HLA-B27 allele 2 Spondyloarthropathies
Sronegative Spondyloarthropathies Dr. M Jokar 1 Definition The spondyloarthropathies are a group of disorders that share certain clinical features and an association with the HLA-B27 allele 2 Spondyloarthropathies
2004 Health Press Ltd.
 ... Ankylosing spondylitis Maxime Dougados MD Professor of Rheumatology Hôpital Cochin René Descartes University Paris, France Désirée van der Heijde MD PhD Professor of Rheumatology University Hospital
... Ankylosing spondylitis Maxime Dougados MD Professor of Rheumatology Hôpital Cochin René Descartes University Paris, France Désirée van der Heijde MD PhD Professor of Rheumatology University Hospital
Axial Spondyloarthritis: Issues & Controversies
 Axial Spondyloarthritis: Issues & Controversies Atul Deodhar, MD Professor of Medicine Oregon Health & Science University Portland, OR WRA 2018 Annual Meeting, Leavenworth, WA. 16 th September, 2018 Disclosures:
Axial Spondyloarthritis: Issues & Controversies Atul Deodhar, MD Professor of Medicine Oregon Health & Science University Portland, OR WRA 2018 Annual Meeting, Leavenworth, WA. 16 th September, 2018 Disclosures:
Remicade (Infliximab)
") Remicade (Infliximab) Policy Number: Original Effective Date: MM.04.016 11/18/2003 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 07/26/2013 Section: Prescription Drugs Place(s)
Remicade (Infliximab) Policy Number: Original Effective Date: MM.04.016 11/18/2003 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 07/26/2013 Section: Prescription Drugs Place(s)
Seronegative spondyloarthropathies : A Pictorial Review
 Seronegative spondyloarthropathies : A Pictorial Review Poster No.: P-0008 Congress: ESSR 2012 Type: Scientific Exhibit Authors: J. Acosta Batlle, B. Palomino Aguado, M. D. Lopez Parra, S. 1 2 3 2 4 1
Seronegative spondyloarthropathies : A Pictorial Review Poster No.: P-0008 Congress: ESSR 2012 Type: Scientific Exhibit Authors: J. Acosta Batlle, B. Palomino Aguado, M. D. Lopez Parra, S. 1 2 3 2 4 1
Clinical Practice Guideline. Psoriatic Arthritis (PsA) Version
 Version") Clinical Practice Guideline Psoriatic Arthritis (PsA) Version 1.1.2016 August 2016 Table of Contents Introduction...5 Diagnosis...6 Patient Assessment... 7 Management of Patients with PsA...8 Peripheral
Clinical Practice Guideline Psoriatic Arthritis (PsA) Version 1.1.2016 August 2016 Table of Contents Introduction...5 Diagnosis...6 Patient Assessment... 7 Management of Patients with PsA...8 Peripheral
Understanding Rheumatoid Arthritis
 Understanding Rheumatoid Arthritis Understanding Rheumatoid Arthritis What Is Rheumatoid Arthritis? 1,2 Rheumatoid arthritis (RA) is a chronic autoimmune disease. It causes joints to swell and can result
Understanding Rheumatoid Arthritis Understanding Rheumatoid Arthritis What Is Rheumatoid Arthritis? 1,2 Rheumatoid arthritis (RA) is a chronic autoimmune disease. It causes joints to swell and can result
Patient #1. Rheumatoid Arthritis. Rheumatoid Arthritis. 45 y/o female Morning stiffness in her joints >1 hour
 Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Jurnal Medical Aradean (Arad Medical Journal) Vol. XVIII, issue 1, 2015, pp Vasile Goldis University Press (www.jmedar.
 Vol. XVIII, issue 1, 2015, pp Vasile Goldis University Press (www.jmedar.") Vol. XVIII, issue 1, 15, pp. 4-45 15 Vasile Goldis University Press (www.jmedar.ro) DEMOGRAPHIC AND CLINICAL PARAMETERS EVALUATION FOR PATIRNTS WITH PSORIATIC VERSUS RHEUMATOID ARTHRITIS Camelia Ciacli
Vol. XVIII, issue 1, 15, pp. 4-45 15 Vasile Goldis University Press (www.jmedar.ro) DEMOGRAPHIC AND CLINICAL PARAMETERS EVALUATION FOR PATIRNTS WITH PSORIATIC VERSUS RHEUMATOID ARTHRITIS Camelia Ciacli
Introduction. Natural Progression of AS. Sacroiliac Joint. Clinical Features and Assessment of Ankylosing Spondylitis
 Clinical Features and Assessment of Ankylosing Spondylitis Dr. YIM, Cheuk Wan Specialist in Rheumatology United Christian Hospital Introduction Ankylo=fusion Spondylitis=inflammation of spine Affect 0.1-0.5%
Clinical Features and Assessment of Ankylosing Spondylitis Dr. YIM, Cheuk Wan Specialist in Rheumatology United Christian Hospital Introduction Ankylo=fusion Spondylitis=inflammation of spine Affect 0.1-0.5%
Rheumatoid arthritis and Psoriatic arthritis: a guide for Primary Care. Nina Flavin, MD Rheumatology Confluence Health April 13 th, 2018
 Rheumatoid arthritis and Psoriatic arthritis: a guide for Primary Care Nina Flavin, MD Rheumatology Confluence Health April 13 th, 2018 No Disclosures Objectives Recognize early signs of RA/PsA what to
Rheumatoid arthritis and Psoriatic arthritis: a guide for Primary Care Nina Flavin, MD Rheumatology Confluence Health April 13 th, 2018 No Disclosures Objectives Recognize early signs of RA/PsA what to
Ultrasound in Rheumatology
 Arthritis Research UK Primary Care Centre Winner of a Queen s Anniversary Prize For Higher and Further Education 2009 Ultrasound in Rheumatology Alison Hall Consultant MSK Sonographer/Research Fellow Primary
Arthritis Research UK Primary Care Centre Winner of a Queen s Anniversary Prize For Higher and Further Education 2009 Ultrasound in Rheumatology Alison Hall Consultant MSK Sonographer/Research Fellow Primary
PHARMACY POLICY STATEMENT Ohio Medicaid
 DRUG NAME BILLING CODE BENEFIT TYPE SITE OF SERVICE ALLOWED COVERAGE REQUIREMENTS LIST OF DIAGNOSES CONSIDERED NOT MEDICALLY NECESSARY PHARMACY POLICY STATEMENT Ohio Medicaid Enbrel (etanercept) Must use
DRUG NAME BILLING CODE BENEFIT TYPE SITE OF SERVICE ALLOWED COVERAGE REQUIREMENTS LIST OF DIAGNOSES CONSIDERED NOT MEDICALLY NECESSARY PHARMACY POLICY STATEMENT Ohio Medicaid Enbrel (etanercept) Must use
Subject: Remicade (Page 1 of 5)
") Subject: Remicade (Page 1 of 5) Objective: I. To ensure that Health Share/Tuality Health Alliance (THA) has a process by which the appropriate utilization of Remicade (Infliximab) for members whose diagnosis
Subject: Remicade (Page 1 of 5) Objective: I. To ensure that Health Share/Tuality Health Alliance (THA) has a process by which the appropriate utilization of Remicade (Infliximab) for members whose diagnosis
Health Technology Appraisal: etanercept, infliximab and adalimumab for the treatment of psoriatic arthritis (rev 104, 125)
") Health Technology Appraisal: etanercept, infliximab and adalimumab for the treatment of psoriatic arthritis (rev 104, 125) Personal view of etanercept, infliximab and adalimumab for psoriatic arthritis
Health Technology Appraisal: etanercept, infliximab and adalimumab for the treatment of psoriatic arthritis (rev 104, 125) Personal view of etanercept, infliximab and adalimumab for psoriatic arthritis
The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R
 The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R 2011 MFMER slide-1 Disclosures None 2011 MFMER slide-2 Learning Objectives Review indications for obtaining imaging studies
The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R 2011 MFMER slide-1 Disclosures None 2011 MFMER slide-2 Learning Objectives Review indications for obtaining imaging studies
C. Assess clinical response after the first three months of treatment.
 Government Health Plan (GHP) of Puerto Rico Authorization Criteria Tumor Necrosis Factor Alpha (TNFα) Adalimumab (Humira ) Managed by MCO Section I. Prior Authorization Criteria A. Physician must submit
Government Health Plan (GHP) of Puerto Rico Authorization Criteria Tumor Necrosis Factor Alpha (TNFα) Adalimumab (Humira ) Managed by MCO Section I. Prior Authorization Criteria A. Physician must submit
New developments in the diagnosis and treatment of axial spondyloarthritis
 Review: Clinical Trial Outcomes New developments in the diagnosis and treatment of axial spondyloarthritis Clin. Invest. (2013) 3(2), 153 171 Spondyloarthritis (SpA) is an umbrella term for a group of
Review: Clinical Trial Outcomes New developments in the diagnosis and treatment of axial spondyloarthritis Clin. Invest. (2013) 3(2), 153 171 Spondyloarthritis (SpA) is an umbrella term for a group of
JuvenileIdiopathicArthritis. Dr Johan Siebert
 JuvenileIdiopathicArthritis Dr Johan Siebert 1 NORMAL DIARTHRODIAL JOINT Synovial is a thin membrane enclosing the joint space The joint space contains fluid that bathes the joint and reduces friction
JuvenileIdiopathicArthritis Dr Johan Siebert 1 NORMAL DIARTHRODIAL JOINT Synovial is a thin membrane enclosing the joint space The joint space contains fluid that bathes the joint and reduces friction
Imaging and intervention of sacroiliac joint. Dr Ryan Lee Ka Lok Associate Consultant Prince of Wales Hospital
 Imaging and intervention of sacroiliac joint Dr Ryan Lee Ka Lok Associate Consultant Prince of Wales Hospital Introduction 15%-25% of low back pain is related to sacroiliac joint (SIJ) pain SIJ pain is
Imaging and intervention of sacroiliac joint Dr Ryan Lee Ka Lok Associate Consultant Prince of Wales Hospital Introduction 15%-25% of low back pain is related to sacroiliac joint (SIJ) pain SIJ pain is
Seronegative Spondyloarthropathies: A Radiological Persepctive
 Seronegative Spondyloarthropathies: A Radiological Persepctive Poster No.: C-1816 Congress: ECR 2016 Type: Educational Exhibit Authors: K. Shindi, H. Nejadhamzeeigilani, P. Nagtode, C. Nel ; 1 1 2 2 3
Seronegative Spondyloarthropathies: A Radiological Persepctive Poster No.: C-1816 Congress: ECR 2016 Type: Educational Exhibit Authors: K. Shindi, H. Nejadhamzeeigilani, P. Nagtode, C. Nel ; 1 1 2 2 3
Regulatory Status FDA- approved indication: Simponi and Simponi ARIA are tumor necrosis factor (TNF) blockers indicated for the treatment of:
 blockers indicated for the treatment of:") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 8 Last Review Date: March 17, 2017 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 8 Last Review Date: March 17, 2017 Simponi / Simponi
Remicade (infliximab)
") Remicade (infliximab) Line(s) of Business: HMO; PPO; QUEST Integration Akamai Advantage Original Effective Date: 11/18/2003 Current Effective Date: 10/01/2015 POLICY A. INDICATIONS The indications below
Remicade (infliximab) Line(s) of Business: HMO; PPO; QUEST Integration Akamai Advantage Original Effective Date: 11/18/2003 Current Effective Date: 10/01/2015 POLICY A. INDICATIONS The indications below
First Presentation of Joint Pain
 First Presentation of Joint Pain Andrew Harrison Rheumatologist Wellington Regional Rheumatology Unit, HVDHB Bowen Centre, Crofton Downs, Wellington Assoc. Prof. in Medicine, University of Otago Wellington
First Presentation of Joint Pain Andrew Harrison Rheumatologist Wellington Regional Rheumatology Unit, HVDHB Bowen Centre, Crofton Downs, Wellington Assoc. Prof. in Medicine, University of Otago Wellington
ARTHRITIS ADVISORY COMMITTEE MEETING
 ARTHRITIS ADVISORY COMMITTEE MEETING July 23, 2013 sbla 125057/323: adalimumab for the treatment of Active non-radiographic axial spondyloarthritis in adults with objective signs of inflammation by elevated
ARTHRITIS ADVISORY COMMITTEE MEETING July 23, 2013 sbla 125057/323: adalimumab for the treatment of Active non-radiographic axial spondyloarthritis in adults with objective signs of inflammation by elevated
SPONDYLOARTHRITIS: PATHOGENESIS, CLINICAL MANIFESTATIONS, DIAGNOSIS, AND MANAGEMENT
 SPONDYLOARTHRITIS: PATHOGENESIS, CLINICAL MANIFESTATIONS, DIAGNOSIS, AND MANAGEMENT *Pilar S. del Río-Martínez Hospital Clínico Universitario Lozano Blesa, Zaragoza, Spain *Correspondence to psdelrio@yahoo.es
SPONDYLOARTHRITIS: PATHOGENESIS, CLINICAL MANIFESTATIONS, DIAGNOSIS, AND MANAGEMENT *Pilar S. del Río-Martínez Hospital Clínico Universitario Lozano Blesa, Zaragoza, Spain *Correspondence to psdelrio@yahoo.es
Objectives. Joint Pain. Case 1. Rheumatology for the Primary MD (Not just your grandmother s disease) 12/4/2010
 12/4/2010") Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
Grigorios T. Sakellariou, 1 Athanasios D. Anastasilakis, 2 Ilias Bisbinas, 3 Anastasios Gketsos, 4 and Charalampos Berberidis 1. 1.
 ISRN Rheumatology Volume 2013, Article ID 907085, 4 pages http://dx.doi.org/10.1155/2013/907085 Clinical Study Efficacy of Anti-TNF Agents as Adjunctive Therapy for Knee Synovitis Refractory to Disease-Modifying
ISRN Rheumatology Volume 2013, Article ID 907085, 4 pages http://dx.doi.org/10.1155/2013/907085 Clinical Study Efficacy of Anti-TNF Agents as Adjunctive Therapy for Knee Synovitis Refractory to Disease-Modifying
Humira (adalimumab) Line(s) of Business: HMO; PPO; QUEST Integration. Original Effective Date: 10/01/2015 Current Effective Date: 03/01/201811/01/2018
 Line(s) of Business: HMO; PPO; QUEST Integration. Original Effective Date: 10/01/2015 Current Effective Date: 03/01/201811/01/2018") Humira (adalimumab) Line(s) of Business: HMO; PPO; QUEST Integration Original Effective Date: 10/01/2015 Current Effective Date: 03/01/201811/01/2018 POLICY A. INDICATIONS The indications below including
Humira (adalimumab) Line(s) of Business: HMO; PPO; QUEST Integration Original Effective Date: 10/01/2015 Current Effective Date: 03/01/201811/01/2018 POLICY A. INDICATIONS The indications below including
Update on Enthesitis-Related Arthritis, a Subtype of Juvenile Idiopathic Arthritis
 Hong Kong Bull Rheum Dis 2010;10:15-19 Review Article Update on Enthesitis-Related Arthritis, a Subtype of Juvenile Idiopathic Arthritis Tsz-Leung Lee Abstract: Keywords: Enthesitis related arthritis (ERA)
Hong Kong Bull Rheum Dis 2010;10:15-19 Review Article Update on Enthesitis-Related Arthritis, a Subtype of Juvenile Idiopathic Arthritis Tsz-Leung Lee Abstract: Keywords: Enthesitis related arthritis (ERA)
Sacroiliac Joint Imaging
 Sacroiliac Joint Imaging Jacob Jaremko, MD, PhD Edmonton, Canada SPR, May 2017 Longview, Alberta Overview SI joint anatomy Sacroiliitis pathophysiology Sacroiliitis imaging Disease features Imaging protocols
Sacroiliac Joint Imaging Jacob Jaremko, MD, PhD Edmonton, Canada SPR, May 2017 Longview, Alberta Overview SI joint anatomy Sacroiliitis pathophysiology Sacroiliitis imaging Disease features Imaging protocols
Rheumatoid Arthritis. Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011
 Rheumatoid Arthritis Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011 The security of experience. The power of innovation. www.rgare.com Case Study
Rheumatoid Arthritis Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011 The security of experience. The power of innovation. www.rgare.com Case Study
Disclosures. Enteropathic Arthritis. Definition. Outline. Pathogenesis 5/4/2018. How Often do Patients with SpA Have Intestinal Inflammation?
 Disclosures Enteropathic Arthritis Site PI on UCB NR-Ax-SpA trial Site PI on Abbvie AS trial Mark C. Fisher, MD MPH Outline SpA and Colitis IBD and Arthritis Other intestinal processes associated with
Disclosures Enteropathic Arthritis Site PI on UCB NR-Ax-SpA trial Site PI on Abbvie AS trial Mark C. Fisher, MD MPH Outline SpA and Colitis IBD and Arthritis Other intestinal processes associated with
Rheumatology. Ankylosing Spondylitis (Bechterew s Disease) Symptoms and Classifications. Definition of Ankylosing Spondylitis. Spondyloarthropathies
 Symptoms and Classifications. Definition of Ankylosing Spondylitis. Spondyloarthropathies") Rheumatology Ankylosing Spondylitis (Bechterew s Disease) Symptoms and Classifications See online here Ankylosing spondylitis, formerly known as Bechterew s disease or Marie- Strümpell disease, is a type
Rheumatology Ankylosing Spondylitis (Bechterew s Disease) Symptoms and Classifications See online here Ankylosing spondylitis, formerly known as Bechterew s disease or Marie- Strümpell disease, is a type
Clinical Policy: Etanercept (Enbrel) Reference Number: PA.CP.PHAR.250 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid
 Reference Number: PA.CP.PHAR.250 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid") Clinical Policy: (Enbrel) Reference Number: PA.CP.PHAR.250 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid Coding Implications Revision Log Description (Enbrel ) is tumor necrosis
Clinical Policy: (Enbrel) Reference Number: PA.CP.PHAR.250 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid Coding Implications Revision Log Description (Enbrel ) is tumor necrosis
Concept of Spondyloarthritis (SpA)
") Concept of Spondyloarthritis (SpA) Undifferentiated SpA Juvenile SpA Ankylosing Spondylitis Psoriatic Arthritis Arthritis associated with Ulcerative Colitis/ Crohn s Disease Reactive Arthritis Acute anterior
Concept of Spondyloarthritis (SpA) Undifferentiated SpA Juvenile SpA Ankylosing Spondylitis Psoriatic Arthritis Arthritis associated with Ulcerative Colitis/ Crohn s Disease Reactive Arthritis Acute anterior
Clinical Policy: Certolizumab (Cimzia) Reference Number: PA.CP.PHAR.247 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid
 Reference Number: PA.CP.PHAR.247 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid") Clinical Policy: (Cimzia) Reference Number: PA.CP.PHAR.247 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid Coding Implications Revision Log Description (Cimzia ) is a tumor necrosis
Clinical Policy: (Cimzia) Reference Number: PA.CP.PHAR.247 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid Coding Implications Revision Log Description (Cimzia ) is a tumor necrosis
Heel pain in spondyloarthritis: results of a cross-sectional study of 275 patients
 Heel pain in spondyloarthritis: results of a cross-sectional study of 275 patients E. Koumakis, L. Gossec, M. Elhai, V. Burki, A. Durnez, I. Fabreguet, M. Meyer, J. Payet, F. Roure, S. Paternotte, M. Dougados
Heel pain in spondyloarthritis: results of a cross-sectional study of 275 patients E. Koumakis, L. Gossec, M. Elhai, V. Burki, A. Durnez, I. Fabreguet, M. Meyer, J. Payet, F. Roure, S. Paternotte, M. Dougados
RHEUMATOLOGY OVERVIEW. Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center
 RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
Jeopardy. What s the rash? $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400
 Jeopardy Antibodies & more antibodies Aching joints What s the rash? Potpourri Image Challenge $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500
Jeopardy Antibodies & more antibodies Aching joints What s the rash? Potpourri Image Challenge $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500
Rheumatologic Manifestations of Gastrointestinal Diseases
 Rheumatologic Manifestations of Gastrointestinal Diseases NATASHA DEHGHAN, MD, FRCPC CLINICAL ASSISTANT PROFESSOR VASCULITIS CLINIC, MARY PACK ARTHRITIS CENTRE Objectives To discuss a few common rheumatologic
Rheumatologic Manifestations of Gastrointestinal Diseases NATASHA DEHGHAN, MD, FRCPC CLINICAL ASSISTANT PROFESSOR VASCULITIS CLINIC, MARY PACK ARTHRITIS CENTRE Objectives To discuss a few common rheumatologic
SCIENTIFIC DISCUSSION
 European Medicines Agency London, 20 September 2007 Product name: Remicade Procedure number: EMEA/H/C/240/II/95 SCIENTIFIC DISCUSSION 7 Westferry Circus, Canary Wharf, London, E14 4HB, UK Tel. (44-20)
European Medicines Agency London, 20 September 2007 Product name: Remicade Procedure number: EMEA/H/C/240/II/95 SCIENTIFIC DISCUSSION 7 Westferry Circus, Canary Wharf, London, E14 4HB, UK Tel. (44-20)
Psoriasis. Jessica Kaffenberger, M.D. Assistant Professor of Dermatology Division of Dermatology The Ohio State University Wexner Medical Center
 Psoriasis Jessica Kaffenberger, M.D. Assistant Professor of Dermatology Division of Dermatology The Ohio State University Wexner Medical Center Learning objectives Recognize the different types of psoriasis
Psoriasis Jessica Kaffenberger, M.D. Assistant Professor of Dermatology Division of Dermatology The Ohio State University Wexner Medical Center Learning objectives Recognize the different types of psoriasis
Effective management of arthritis. Gail Dolan Victoria ACH Liz McIvor Stobhill ACH
 Effective management of arthritis Gail Dolan Victoria ACH Liz McIvor Stobhill ACH Role Types of arthritis Drugs Self Management Role Of CNS Advanced level nurses offering specialist care in a specific
Effective management of arthritis Gail Dolan Victoria ACH Liz McIvor Stobhill ACH Role Types of arthritis Drugs Self Management Role Of CNS Advanced level nurses offering specialist care in a specific
COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP)
") European Medicines Agency Pre-Authorisation Evaluation of Medicines for Human Use London, 23 April 2009 Doc. Ref. CPMP/EWP/4891/03 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON CLINICAL
European Medicines Agency Pre-Authorisation Evaluation of Medicines for Human Use London, 23 April 2009 Doc. Ref. CPMP/EWP/4891/03 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON CLINICAL
axial spondyloarthritis including ankylosing spondylitis
 1 What is spondyloarthritis? Spondyloarthritis is a general term that describes a number of types of inflammatory arthritis which share many articular and extra-articular features. Conditions which fall
1 What is spondyloarthritis? Spondyloarthritis is a general term that describes a number of types of inflammatory arthritis which share many articular and extra-articular features. Conditions which fall
Clinical Policy: Certolizumab (Cimzia) Reference Number: ERX.SPMN.24
 Reference Number: ERX.SPMN.24") Clinical Policy: (Cimzia) Reference Number: ERX.SPMN.24 Effective Date: 10/2016 Last Review Date: 12/2016 Coding Implications Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Cimzia) Reference Number: ERX.SPMN.24 Effective Date: 10/2016 Last Review Date: 12/2016 Coding Implications Revision Log See Important Reminder at the end of this policy for important
Infliximab Remicade (infliximab) Inflectra (infliximab-dyyb) Renflexis (infliximab-abda)
 Inflectra (infliximab-dyyb) Renflexis (infliximab-abda)") Infliximab Remicade (infliximab) Inflectra (infliximab-dyyb) Renflexis (infliximab-abda) Line(s) of Business: HMO; PPO; QUEST Integration Akamai Advantage Original Effective Date: 11/18/2003 Current Effective
Infliximab Remicade (infliximab) Inflectra (infliximab-dyyb) Renflexis (infliximab-abda) Line(s) of Business: HMO; PPO; QUEST Integration Akamai Advantage Original Effective Date: 11/18/2003 Current Effective
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES HUMIRA PEDIATRIC
 Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 HUMIRA PEDIATRIC GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Is the patient currently taking Humira? If
Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 HUMIRA PEDIATRIC GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Is the patient currently taking Humira? If
AOS 3: Rheumatoid Arthritis
 AOS 3: Rheumatoid Arthritis Arthritis (General) = inflamed joint - NOT a single disease: covers >100 types - Involves disability + decreased quality of life o Can also occur in young people (not just the
AOS 3: Rheumatoid Arthritis Arthritis (General) = inflamed joint - NOT a single disease: covers >100 types - Involves disability + decreased quality of life o Can also occur in young people (not just the
A Patient s Guide to. Treatments for Psoriatic Arthritis
 A Patient s Guide to Treatments for Psoriatic Arthritis Who should read this guide? This guide is aimed at people with psoriatic arthritis (abbreviated as PsA), or those who care for a person with this
A Patient s Guide to Treatments for Psoriatic Arthritis Who should read this guide? This guide is aimed at people with psoriatic arthritis (abbreviated as PsA), or those who care for a person with this
Types of osteoarthritis
 ARTHRITIS Osteoarthritis is a degenerative joint disease is the most common joint disorder. It is a frequent part of aging and is an important cause of physical disability in persons older than 65 years
ARTHRITIS Osteoarthritis is a degenerative joint disease is the most common joint disorder. It is a frequent part of aging and is an important cause of physical disability in persons older than 65 years
Case reports CASE 1. A 67-year-old white man had back pain since the age. our clinic several years later with progressive symptoms.
 Annals of the Rheumatic Diseases, 1982, 41, 574-578 Late-onset peripheral joint disease in ankylosing spondylitis MARC D. COHEN AND WILLIAM W. GINSBURG From the Division ofrheumatology and Internal Medicine,
Annals of the Rheumatic Diseases, 1982, 41, 574-578 Late-onset peripheral joint disease in ankylosing spondylitis MARC D. COHEN AND WILLIAM W. GINSBURG From the Division ofrheumatology and Internal Medicine,
Rheumatoid Arthritis 2. Inflammatory Diseases. Definition. Imaging Signs
 Rheumatoid Arthritis 2 Definition " Epidemiology Affects 2% of the population Peak incidence (diagnosis) in 4th and 5th decades Women affected 3 4 times more often than men Increased familial incidence
Rheumatoid Arthritis 2 Definition " Epidemiology Affects 2% of the population Peak incidence (diagnosis) in 4th and 5th decades Women affected 3 4 times more often than men Increased familial incidence
Ankylosing Spondylitis: Overarching Concerns New Concepts and New Treatment for Spondyloarthritis
 Ankylosing Spondylitis: Overarching Concerns New Concepts and New Treatment for Spondyloarthritis NCNP #320 April 21 Friday 3:30-5:00 Richard S Pope MPAS, PA-C, DFAAPA, CPAAPA Western CT Medical Group
Ankylosing Spondylitis: Overarching Concerns New Concepts and New Treatment for Spondyloarthritis NCNP #320 April 21 Friday 3:30-5:00 Richard S Pope MPAS, PA-C, DFAAPA, CPAAPA Western CT Medical Group
Comparison of comorbidities between rheumatoid and psoriatic arthritis in a tertiary care rheumatic center
 Original Research Article Comparison of comorbidities between rheumatoid and psoriatic arthritis in a tertiary care rheumatic center T.N. Tamil Selvam 1, V.A. Sowndhariya 2*, N.K. Senthil Nathan 3 1 Associate
Original Research Article Comparison of comorbidities between rheumatoid and psoriatic arthritis in a tertiary care rheumatic center T.N. Tamil Selvam 1, V.A. Sowndhariya 2*, N.K. Senthil Nathan 3 1 Associate
Horizon Scanning Centre November Secukinumab for active and progressive psoriatic arthritis. SUMMARY NIHR HSC ID: 5330
 Horizon Scanning Centre November 2012 Secukinumab for active and progressive psoriatic arthritis. SUMMARY NIHR HSC ID: 5330 Secukinumab is a high-affinity fully human monoclonal antibody that antagonises
Horizon Scanning Centre November 2012 Secukinumab for active and progressive psoriatic arthritis. SUMMARY NIHR HSC ID: 5330 Secukinumab is a high-affinity fully human monoclonal antibody that antagonises
Hello, I m Christopher Ritchlin, from the University of Rochester Medical Center, and I have the pleasure today of discussing with you abstracts
 Hello, I m Christopher Ritchlin, from the University of Rochester Medical Center, and I have the pleasure today of discussing with you abstracts presented at the 2012 American College of Rheumatology meeting
Hello, I m Christopher Ritchlin, from the University of Rochester Medical Center, and I have the pleasure today of discussing with you abstracts presented at the 2012 American College of Rheumatology meeting
INFLIXIMAB Remicade (infliximab), Inflectra (infliximab-dyyb), Renflexis (infliximab-abda)
, Inflectra (infliximab-dyyb), Renflexis (infliximab-abda)") RATIONALE FOR INCLUSION IN PA PROGRAM Background Remicade, Renflexis and Inflectra are tumor necrosis factor (TNFα) blockers. Tumor necrosis factor is an endogenous protein that regulates a number of physiologic
RATIONALE FOR INCLUSION IN PA PROGRAM Background Remicade, Renflexis and Inflectra are tumor necrosis factor (TNFα) blockers. Tumor necrosis factor is an endogenous protein that regulates a number of physiologic