Complicated Diverticulitis. Evidence Based Recommendations
|
|
|
- Barbra Anthony
- 6 years ago
- Views:
Transcription
1 Complicated Diverticulitis Evidence Based Recommendations Frederick A Moore MD September 10, 2014
2 Complicated Diverticulitis Evidence Based Recommendations I have no financial disclosures
3 A Management Algorithm for Perforated Diverticulitis Objectives Provide a historical perspective on surgical management Discuss current algorithm of surgical management Debate definitive resection vs damage control vs laparoscopic lavage


4 J Trauma Acute Care Surg 2012
5 Complicated Diverticulitis Evidence-based Recommendations Disease of industrial revolution - roller milling wheat fiber by 2/3 rds Relatively rare & high associated M & M - small single center studies 100 years of case series - virtually all retrospective & expert opinion Evolving management strategies - most remarkable over past 20 yrs

6 Acquired Diverticulitis of the Large Intestine Mayo describes 4 resections of the colon for diverticulitis Surg Gynecol Obstet 1907
7 DIVERTICULITIS OF THE COLON By E. Starr Judd,MD and Lee W.Pollock, MD MAYO CLINIC Ann Surg 1924 Perforated Diverticulitis with Peritonitis Colostomy + Irrigation Distal Colon ± Delayed Resection Primary resection too difficult in the acute setting Stirring up the infection results in very high mortality (pre- antibiotic era)
8 DIVERTICULITIS OF THE COLON By E. Starr Judd,MD and Lee W.Pollock, MD MAYO CLINIC Ann Surg 1924 Perforated Diverticulitis with Peritonitis Colostomy + Irrigation Distal Colon ± Delayed Resection Primary resection too difficult in the acute setting Stirring up the infection results in very high mortality (pre- antibiotic era)
9 EXPERIENCE WITH THE SURGICAL MANAGEMENT OF DIVERTICULITIS OF THE SIGMOID Reginald H.Smithwick MD From The Massachusetts General Hospital Ann Surg 1942 Compared numerous operations and concluded that best early mortality and long-term outcomes are achieved with Preliminary proximal colostomy Resection at 3-6 months after inflammation resolved
10 Perforated Diverticulitis with Peritonitis Three - Staged Procedure 1 st : Diverting Colostomy, Suture Closure & Drainage 2 nd : Definitive Resection & Colostomy at 3-6 months 3 rd : Colostomy Closure at 3-6 months
11 Acute Perforated Diverticulitis of the Sigmoid Colon With Generalized Peritonitis HIRAM H. BELDING III,MD, Riverside Calif Arch Surg 1957 With IV Terramycin q 12 hour X 3 days Safely resected diseased colon in 5 cases Two - Staged Procedure (Hartmann s Procedure) 1 st : Resect & Colostomy 2 nd : Delayed Colostomy Closure
12
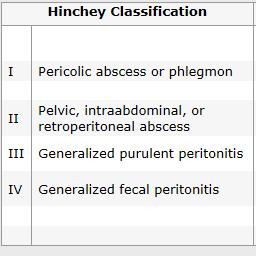
13 WTA Complicated Diverticulitis Score Modified Hinchey Grade I A I B II III IV Characteristic Phlegmon with no abscess Phlegmon with abscess < 4 cm Phlegmon with abscess > 4 cm Purulent peritonitis (no hole in colon) Feculent peritonitis (persistent hole in colon) Other Complications: Stricture or fistula
14 Surgical Treatment of Perforated Diverticulitis of the Sigmoid Colon Jon M. Greif DO, Gregory Fried MD, Charles K.McSherry, MD. Dis, Col & Rect 1980 Retrospective Review of 36 Case Series 821 case with Peritonitis Selection Bias? Staged Staged 145 (29%) Died 39(12%) Died
15 Surgical Treatment of Perforated Diverticulitis of the Sigmoid Colon Jon M. Greif DO, Gregory Fried MD, Charles K.McSherry, MD. Advocates of Acute Resection Dis, Col & Rect 1980 mortality with better antibiotics & supportive care Will not miss colon cancer ( ~ 3 % of cases) morbidity ( 20% fistula in nonresected patients)
16 Treatment of perforated sigmoid diverticulitis: A prospective randomized trial O. Kronborg Br J Surg Peritonitis 46 Purulent Peritonitis (Hinchey III) Single Center Denmark Staged 2 Staged 0 Died 6(24%) Died
17 Br J Surg Generalized Peritonitis (Hinchey III & IV) Multicenter 48 3 Staged 55 2 Staged Postop Peritonitis 10 (20%) 1 (2%) * Mortality 9 (18%) 13 (23%) * P < 0.05
18 Dis Colon Rectum 2000 Perforated Diverticulitis with Peritonitis Procedure of choice is segmental resection with colostomy 2 - Stage Hartmann s Procedure

19 Only ~50% of colostomies are reversed Colostomy reversal is a high morbidity procedure
20 1 Stage PRA Dis Colon Rectum comparative studies published from (13 retrospective, 2 prospective nonrandomized)
21 Mortality Diverticular Disease Diverticular Disease + Emergency OR Diverticular Disease + Hinchey >2 Diverticular Disease + Abscess Favors PRA Favors Hartmann s
22 Mortality Diverticular Disease Diverticular Disease + Emergency OR Diverticular Disease + Hinchey >2 Diverticular Disease + Abscess Favors PRA Favors Hartmann s
23 Surgical Complications Wound Infections Postop Abscess/Peritonitis Stoma Complications (for PADS & Hartsmann s) Favors PRA Favors Hartmann s
24 Obvious Select Bias Hard to Extrapolate But Emergency PRA has low rate of anastomosis leak (6%) PRA and Hartmann s had similar operative time All Hinchey >2 subset : equal mortality (14.1% vs 14.4%)
25 Perforated Diverticulitis with Peritonitis Dis Colon Rectum 2006 Alternatives are Hartmann s procedure or PRA with or without intraoperative lavage. The role proximal diversion remains unsettled.

26 Patients from 17 studies

27 Br J Surg Patient Admitted For Diverticulitis over 7 years 100 (7%) had Peritonitis + Evidence Free Air on X-ray or CT Resuscitated 3 rd Generation Cephalosporin + Flagyl Taken Emergently to OR for Laparoscopy
28 100 Laparoscopic Assessment 92 Hinchey II/III 8 Hinchey IV 92 Lavage/Drained 3 Died 2 Non-resolution 9 Hartman's 88 Resolved 1 IR Drainage 2 Recurrences over 36 month follow-up
 6.6 ± 2.4 16.6 ± 10 0.")
29 Surg Endosc 2012 LLD LHP p value # of Patients OR Time (minutes) 100 ± ± Blood Loss (ml) 34 ± ± Conversion 2 % 15 % 0.05 Complications 4 % 13 % 0.05 Mortality 0 % 2.4% ns Hospital Stay (days) 6.6 ± ± Colostomy Closure na 72% na Elective Resection 45% na na


30 Br J Surg 2013 Contraindicated in: Stage IV Stage III Major Comorbidity Immunosuppression High CRP

31 Used Rectal Contrast CT scanning to rule out stage IV disease Nonoperative Rx 36 Successful
32 Management of Complicated Diverticulitis ED Clinical Dx, Lab Testing, SIRS Severity, Peritonitis, Plain X-rays IV Access, Fluid Bolus, Antibiotics Emergency OR no Pre-operative Optimization no OR Septic Shock Peritonitis Laparoscopy Severe Sepsis Free Air on no Plain X-rays or CT scan? Grade III/IV Grade II Grade I A/B Grade III Grade IV Successful no IR Drain Observe Fail Damage Control Lavage & Drain Definitive Resection

33 Helsinki, Finland Distant Intraperitoneal Air n=71 Nonoperative Management n=29 Distant Retroperitoneal Air n= 17 Nonoperative Management n=14 Failure n=11 Failure n=8
34 Management of Complicated Diverticulitis ED Clinical Dx, Lab Testing, SIRS Severity, Peritonitis, Plain X-rays IV Access, Fluid Bolus, Antibiotics Septic Shock Emergency OR no CT Scan no Grade III/IV Grade II Grade I A/B Pre-operative Optimization ICU 2-3 hours OR Septic Shock no Laparoscopy Grade III Grade IV no IR Drain Successful Observe Fail Damage Control Lavage & Drain Definitive Resection
35 Management of Complicated Diverticulitis ED Clinical Dx, Lab Testing, SIRS Severity, Peritonitis, Plain X-rays IV Access, Fluid Bolus, Antibiotics Septic Shock Emergency OR no CT Scan no Grade III/IV Grade II Grade I A/B Pre-operative Optimization OR Septic Shock no Laparoscopy Grade III Grade IV no IR Drain Successful Observe Fail Damage Control Lavage & Drain Definitive Resection

36 The Septic Abdomen and Sepsis Infection SIRS Sepsis Severe Sepsis Intra-Abdominal Infection Think Damage Control Abdominal Catastrophe Septic Shock

37 Joined New Surgery Department in August 2006 Chair - Barbara Bass

38 The Methodist Hospital (TMH), Houston TX Sepsis in major killer in surgical ICU Picture Methodists
39 Rationale for Damage Control in Trauma The Bloody Vicious Cycle Coagulopathy Hypothermia Shock & Exsanguination Iatrogenic Factors Cellular Shock Acidosis Contact Activation Clotting Factor Deficiencies Tissue Injury Massive Transfusion Pre-Existing Diseases
40 The Persistent Septic Shock Cycle Abdominal Infection Microthrombosis Cellular Shock Endothelial Leak Septic Shock & MOF Contact Activation Excessive Proinflammation Vasodilation, Hypotension & Myocardial Depression Endothelial Activation DIC
41 Break the Persistent Septic Shock Cycle Abdominal Infection Microthrombosis Cellular Shock Endothelial Leak Septic Shock & MOF Contact Activation Excessive Proinflammation Vasodilation, Hypotension & Myocardial Depression Endothelial Activation DIC Prevent Acute Kidney Injury

42
43 Damage Control Pre-operative Optimization Secure airway / vascular access Volume resuscitation Broad spectrum anti-microbials Blood products as necessary Vasopressors as necessary Correct Electrolytes
44 Complete by 6 hours Damage Control Laparotomy Source control Resect & Debride Dead Bowel Close Holes to Limit Contamination Hemorrhage Control/Pack Limited Irrigation/Drain Temporary abdominal closure Perforectomy
45 Damage Control Post-operative Optimization Resuscitation Ventilator support Coagulopathy correction Rewarming Monitoring for ACS Surviving Sepsis Campaign
46 Damage Control Second Operation Re-opening of laparotomy Pack removal Further resection/debridement Ostomy vs Bowel Anastomosis Feeding tubes, drains Close Fascia vs Wound Vac

47 , Delayed Anastomosis = 12% leak Birmingham, Alabama J Trauma 2009 Delayed Anastomosis = 13% leak Surgery 2009
48 Damage Control Laparotomy and the Open Abdomen: Is There an Increased Risk of Colonic Anastomotic Leak Mickey M Ott, MD, Patrick Norris, PhD, Bryan Collier, D0, Oliver L. Gunter MD, William Riordan, MD, Jose Diaz, MD, Vanderbilt University Medical Center Delayed Anastomosis = 27% leak J Trauma 2011 SAFETY OF PERFORMING DELAYED ANASTOMOSIS DURING DAMAGE CONTROL LAPARAROTOMY FOR DESTRUCTIVE COLON INJURIES Carlos Ordenez, MD, Luis Pino, MD, Marisol Badiel, MD,John Loaiza, BSc, Jaun Carlos Puyana, MD, FundaciAfAn Valle del Lili Department of Surgery and Critical Care Cila Columbia Delayed Anastomosis = 8 % leak J Trauma 2011

49 Innsbruck, Austria 51 Patients PRA 13 HP
50 Figure Traditional 3 : Management of Patients with an Abdominal Infection and Septic Shock Septic Abdomen Operating Room Definitive Operation Vasopressors in OR Early Death or AKI MOF
51 Prevent AKI & Live Figure 3 : Paradigm Shift in Management of Patients with an Abdominal Infection and Septic Shock Septic Abdomen Septic Abdomen Operating Room Definitive Operation Vasopressors in OR Early Death or AKI MOF Resuscitation: Volume/Antibiotics Operating Room Damage/Source Control SICU Resuscitation
52 The Availability of Acute Care Surgeons Improves Outcomes in Patients Requiring Emergent Colon Surgery Laura Jane Moore, MD; Krista L Turner, MD; Stephen L Jones, MD; Bridget N Fahy, MD and Frederick A Moore, MD Am J Surg 2011 Establish a Benchmark We queried the NSQIP dataset & our prospective sepsis database to identify patient with: 1) Severe sepsis/septic shock (same definitions) 2) Emergency colon surgery Primary endpoint: 30 day mortality
53 Results ACS (n = 46) NSQIP (n = 1101) Average Age 62.3 ± ± 13.5 Male 45 % 47.2 % APACHE II 31 ± 8.2 Not Available Predicted Mortality (APACHE II)* Actual 30 Day Mortality** 73% Not Available 28.3% 40.4% * Actual vs. Predicted mortality p < ** ACS vs. NSQIP mortality p = 0.06
54 Results ACS (n = 46) NSQIP (n = 1101) Average Age 62.3 ± ± 13.5 Male 45 % 47.2 % APACHE II 31 ± 8.2 Not Available Predicted Mortality (APACHE II)* Actual 30 Day Mortality** 73% Not Available * Actual vs. Predicted mortality p < % 40.4% ** ACS vs. NSQIP mortality p = % of our ACS patients underwent damage control
55 Management of Complicated Diverticulitis ED Clinical Dx, Lab Testing, SIRS Severity, Peritonitis, Plain X-rays IV Access, Fluid Bolus, Antibiotics Septic Shock Emergency OR no Pre-operative Optimization OR Septic Shock no Laparoscopy Low Risk Damage Control Lavage & Drain
56 Management of Complicated Diverticulitis ED Clinical Dx, Lab Testing, SIRS Severity, Peritonitis, Plain X-rays IV Access, Fluid Bolus, Antibiotics Septic Shock no Pre-operative Optimization OR Septic Shock Emergency OR Laparoscopy Stage IV disease no Low Risk High Risk High Risk Immunocompromised Severe co-morbidity Worsening MOF from sepsis Damage Control Lavage & Drain Definitive Resection
57 What is a Definitive Resection proximal margin - back to normal colon no diverticula in the anastomosis distal margin - rectum ureteral stents - selective intraoperative colon lavage - does not work omentoplasty of suture line - does not work
58 Factors to Consider after Definitive Resection Severity of Disease Hinchey 1 Hinchey 2 Hinchey 3 Hinchey 4 Patient Presenting Physiology Stable Tachycardia Hypotensive Septic Shock Patient Co morbidities Healthy HTN DM Immunosuppression Malnourished Advanced Organ Failure Hospital/Situational Factors Tertiary Care Center/well staffed Community Hospital/poorly staffed E Experienced Ancillary Staff Off Hours Operation/Equipment Issues Surgeon Factors Specialized/High Volume Inexperienced/Low Volume Operative Intervention PRA no Stoma PRA + Stoma Hartmann s Procedure
59 Management of Complicated Diverticulitis ED Clinical Dx, Lab Testing, SIRS Severity, Peritonitis, Plain X-rays IV Access, Fluid Bolus, Antibiotics Septic Shock no Emergency OR no CT Scan Grade III/IV Grade II Grade I A/B Pre-operative Optimization OR Septic Shock no Laparoscopy Low Risk High Risk Damage Control Lavage & Drain Definitive Resection
60 Management of Complicated Diverticulitis ED Clinical Dx, Lab Testing, SIRS Severity, Peritonitis, Plain X-rays IV Access, Fluid Bolus, Antibiotics Septic Shock Emergency OR no CT Scan no Grade III/IV Pre-operative Optimization OR Septic Shock no Laparoscopy Low Risk High Risk High Risk Immunocompromised Severe co-morbidity Worsening MOF Damage Control Lavage & Drain Definitive Resection Stage IV disease
61 Management of Complicated Diverticulitis ED Clinical Dx, Lab Testing, SIRS Severity, Peritonitis, Plain X-rays IV Access, Fluid Bolus, Antibiotics Septic Shock Emergency OR no CT Scan no Grade III/IV Grade II Pre-operative Optimization OR Septic Shock no Laparoscopy Low Risk High Risk no IR Drain Successful Damage Control Lavage & Drain Definitive Resection

62 Surg Endosc 2006 Sepsis Abscess Recurrence Fistula Median Delay 14d
63 Management of Complicated Diverticulitis ED Clinical Dx, Lab Testing, SIRS Severity, Peritonitis, Plain X-rays IV Access, Fluid Bolus, Antibiotics Septic Shock no Emergency OR no CT Scan Grade III/IV Grade II Grade I A/B Pre-operative Optimization OR Septic Shock no Laparoscopy Low Risk High Risk no IR Drain Successful Observe Fail Damage Control Lavage & Drain Definitive Resection Home
64 Observation NPO NG tube if symptomatic Broad spectrum IV antibiotics Monitor PE, SIRS Severity and WBC Start diet & PO antibiotics when return of bowel function, resolution of abdominal tenderness & leukocytosis DC home when tolerating diet on a total 14 day course of antibiotics (? shorter duration).
65 Management of Complicated Diverticulitis ED Clinical Dx, Lab Testing, SIRS Severity, Peritonitis, Plain X-rays IV Access, Fluid Bolus, Antibiotics Septic Shock no Emergency OR no CT Scan Grade III/IV Grade II Grade I A/B Pre-operative Optimization OR Septic Shock no Laparoscopy Low Risk High Risk no IR Drain Successful Observe Fail Damage Control Lavage & Drain Definitive Resection Home
66 Follow-up Return to clinic if symptoms recur Return to clinic at 6 weeks for exam If inflammation resolved? schedule colonoscopy
67 Helsinki, Finland Surg Endosc CT Scan Dx Acute Diverticulitis 97 Emergency OR 536 No OR 142 No Colonoscopy 7 Colon Cancer 394 Colonoscopy 17 (2.7%) Colon Cancers 16 Abscesses 1 Pericolic Air ( 11% of all abscesses)
68 Elective Prophylactic Resection After Complicated Diverticulitis Persistent or recurrent symptoms Immunocompromised host Anatomic deformity including a stricture or fistula.
69

70 Pepper

71 Management of Complicated Diverticulitis Clinical Dx, Lab Testing, SIRS Severity, Peritonitis, Plain X-rays IV Access, Fluid Bolus, Antibiotics Septic Shock Emergency OR no CT Scan no Grade III/IV Grade II Grade I A/B Pre-operative Optimization OR Septic Shock no Laparoscopy Low Risk High Risk no IR Drain Successful Observe Fail Damage Control Lavage & Drain Definitive Resection Home
Acute Diverticulitis. Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh
 Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Acute Care Surgery: Diverticulitis
 Acute Care Surgery: Diverticulitis Madhulika G. Varma, MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment of Diverticular Disease Increasing
Acute Care Surgery: Diverticulitis Madhulika G. Varma, MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment of Diverticular Disease Increasing
Severe and Tertiary Peritonitis
 Severe and Tertiary Peritonitis Addison K. May, MD FACS Professor of Surgery and Anesthesiology Division of Trauma and Surgical Critical Care Vanderbilt University Medical Center PS204: The Bad Infections:
Severe and Tertiary Peritonitis Addison K. May, MD FACS Professor of Surgery and Anesthesiology Division of Trauma and Surgical Critical Care Vanderbilt University Medical Center PS204: The Bad Infections:
Perforated diverticulitis: Washout it s happening
 Perforated diverticulitis: Washout it s happening or maybe not! Ori D. Rotstein, M.D. Department of Surgery St. Michael s Hospital University of Toronto 62 year old male 24 hour history of LLQ pain Now-
Perforated diverticulitis: Washout it s happening or maybe not! Ori D. Rotstein, M.D. Department of Surgery St. Michael s Hospital University of Toronto 62 year old male 24 hour history of LLQ pain Now-
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS
 GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
DIVERTICULAR DISEASE. Dr. Irina Murray Casanova PGY IV
 DIVERTICULAR DISEASE Dr. Irina Murray Casanova PGY IV Diverticular Disease Colonoscopy Abdpelvic CT Scan Surgical Indications Overall, approximately 20% of patients with diverticulitis require surgical
DIVERTICULAR DISEASE Dr. Irina Murray Casanova PGY IV Diverticular Disease Colonoscopy Abdpelvic CT Scan Surgical Indications Overall, approximately 20% of patients with diverticulitis require surgical
When should we operate for recurrent diverticulitis. Savvas Papagrigoriadis MD MSc FRCS Consultant Colorectal Surgeon King's College Hospital
 When should we operate for recurrent diverticulitis Savvas Papagrigoriadis MD MSc FRCS Consultant Colorectal Surgeon King's College Hospital ASCRS Practice parameters for the Treatment of Acute Diverticulitis
When should we operate for recurrent diverticulitis Savvas Papagrigoriadis MD MSc FRCS Consultant Colorectal Surgeon King's College Hospital ASCRS Practice parameters for the Treatment of Acute Diverticulitis
Case discussion. Anastomotic leakage. intern superviser
 Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
A Population-Based Analysis of the Clinical Course of Colonic Diverticulitis and its Evolving Management
 A Population-Based Analysis of the Clinical Course of Colonic Diverticulitis and its Evolving Management by Debbie Li A thesis submitted in conformity with the requirements for the degree of Masters of
A Population-Based Analysis of the Clinical Course of Colonic Diverticulitis and its Evolving Management by Debbie Li A thesis submitted in conformity with the requirements for the degree of Masters of
Management of the Open Abdomen
 Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
Prof. Dr. Ahmed ElGeidie Professor of General surgery GEC Dr. Ahmed Abdelrafee
 Prof. Dr. Ahmed ElGeidie Professor of General surgery GEC Dr. Ahmed Abdelrafee Diverticulosis of the colon is the presence of pockets in the wall of the colon called diverticula which may, or may not,
Prof. Dr. Ahmed ElGeidie Professor of General surgery GEC Dr. Ahmed Abdelrafee Diverticulosis of the colon is the presence of pockets in the wall of the colon called diverticula which may, or may not,
Indications and Surgical Techniques In the Treatment of Complicated Acute Diverticulitis. Retrospective Study of a 13 Year Old case History
 Article ID: WMC004324 ISSN 2046-1690 Indications and Surgical Techniques In the Treatment of Complicated Acute Diverticulitis. Retrospective Study of a 13 Year Old case History Corresponding Author: Dr.
Article ID: WMC004324 ISSN 2046-1690 Indications and Surgical Techniques In the Treatment of Complicated Acute Diverticulitis. Retrospective Study of a 13 Year Old case History Corresponding Author: Dr.
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
LONG TERM OUTCOME OF ELECTIVE SURGERY
 LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Determinants of treatment: Outcome measures or how to read studies on diverticular disease
 Determinants of treatment: Outcome measures or how to read studies on diverticular disease Jörg C. Hoffmann, Medizinische Klinik I, Charité, Universitätsmedizin Berlin, Campus Benjamin Franklin Outcome:
Determinants of treatment: Outcome measures or how to read studies on diverticular disease Jörg C. Hoffmann, Medizinische Klinik I, Charité, Universitätsmedizin Berlin, Campus Benjamin Franklin Outcome:
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN
 LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN MCQ A 78 yr. old man (HT, DM, 2 coronary stents) has 3 mos. of irregular bowel habits and 72 hrs. of LBO. Distended, non-tender. Normal blood work. Plain xray,
LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN MCQ A 78 yr. old man (HT, DM, 2 coronary stents) has 3 mos. of irregular bowel habits and 72 hrs. of LBO. Distended, non-tender. Normal blood work. Plain xray,
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
STOMAS AND DIVERTICULITIS
 STOMAS AND DIVERTICULITIS Jean-Jacques Jacques HOUBEN U.L.B. CENTRE HOSPITALIER INTERREGIONAL EDITH CAVELL First Post-Graduate course of the BSCRS colorectal section BRUSSELS 2002 jjhouben@ulb.ac.be gastrospace.com
STOMAS AND DIVERTICULITIS Jean-Jacques Jacques HOUBEN U.L.B. CENTRE HOSPITALIER INTERREGIONAL EDITH CAVELL First Post-Graduate course of the BSCRS colorectal section BRUSSELS 2002 jjhouben@ulb.ac.be gastrospace.com
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT. Simon Radley Consultant Surgeon March 2013
 DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
Discussion of Complex Clinical Scenarios and Variable Review ACS NSQIP Clinical Support Team
 Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Inflammatory Bowel Disease and Surgery: What You Should Know
 Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Future Trends in Diverticular Disease: What is Role of Surgery. President, ISUCRS
 Future Trends in Diverticular Disease: What is Role of Surgery Philip F. Caushaj, MD, PhD, PhD(hon), FACS, FACG, FASCRS, FISUCRS,AGAF, FASGE, FSSO Professor of Surgery, University of Connecticut Vice Chair,
Future Trends in Diverticular Disease: What is Role of Surgery Philip F. Caushaj, MD, PhD, PhD(hon), FACS, FACG, FASCRS, FISUCRS,AGAF, FASGE, FSSO Professor of Surgery, University of Connecticut Vice Chair,
of Trauma Assembly 28 th Page 1
 Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 12 Disease Grading Systemss in Emergency General Surgery January 16, 2015 Disney s Contemporary Resort Lake
Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 12 Disease Grading Systemss in Emergency General Surgery January 16, 2015 Disney s Contemporary Resort Lake
DIVERTICULAR DISEASE HANDS OFF OR HANDS ON?
 DIVERTICULAR DISEASE HANDS OFF OR HANDS ON? TE MADIBA AND M NAIDOO TE MADIBA MMed, LLM, PhD, FCS (SA), FASCRS Emeritus Professor of Surgery & Director of the Gastrointestinal Cancer Research Centre, University
DIVERTICULAR DISEASE HANDS OFF OR HANDS ON? TE MADIBA AND M NAIDOO TE MADIBA MMed, LLM, PhD, FCS (SA), FASCRS Emeritus Professor of Surgery & Director of the Gastrointestinal Cancer Research Centre, University
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University.
 Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Incidence and risk factors of anastomotic leaks. By: khaled Said Assistant professor of colorectal surgery Alexandria
 Incidence and risk factors of anastomotic leaks By: khaled Said Assistant professor of colorectal surgery Alexandria Anastomotic leakage after colorectal surgery is a major and potentially life-threatening
Incidence and risk factors of anastomotic leaks By: khaled Said Assistant professor of colorectal surgery Alexandria Anastomotic leakage after colorectal surgery is a major and potentially life-threatening
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Guideline scope Diverticular disease: diagnosis and management
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Diverticular disease: diagnosis and management The Department of Health in England has asked NICE to develop a clinical guideline on diverticular
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Diverticular disease: diagnosis and management The Department of Health in England has asked NICE to develop a clinical guideline on diverticular
Small Bowel and Colon Surgery
 Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Historical perspective
 Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Does the Presence of Abscesses in Diverticular Disease Prelude Surgery?
 J Gastrointest Surg (2013) 17:540 547 DOI 10.1007/s11605-012-2097-x ORIGINAL ARTICLE Does the Presence of Abscesses in Diverticular Disease Prelude Surgery? B. J. M. van de Wall & W. A. Draaisma & E. C.
J Gastrointest Surg (2013) 17:540 547 DOI 10.1007/s11605-012-2097-x ORIGINAL ARTICLE Does the Presence of Abscesses in Diverticular Disease Prelude Surgery? B. J. M. van de Wall & W. A. Draaisma & E. C.
Colorectal non-inflammatory emergencies
 Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Pediatric SC/SCR Education Session: Difficult Definitions. NSQIP Annual Meeting July 26, 2014
 Pediatric SC/SCR Education Session: Difficult Definitions NSQIP Annual Meeting July 26, 2014 Actual patient Chart Abstraction: The Challenge o Demographics o Risk factors o Events/occurrences Documentation
Pediatric SC/SCR Education Session: Difficult Definitions NSQIP Annual Meeting July 26, 2014 Actual patient Chart Abstraction: The Challenge o Demographics o Risk factors o Events/occurrences Documentation
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 4 2013 Article 6 Case report: Intussusception of the colon through a colostomy: A rare presentation of colonic intussusception. Dr. Nora Trabulsi Dr.
World Journal of Colorectal Surgery Volume 3, Issue 4 2013 Article 6 Case report: Intussusception of the colon through a colostomy: A rare presentation of colonic intussusception. Dr. Nora Trabulsi Dr.
Surgery and Crohn s. Crohn s Disease 70 % Why Operate? Complications of Disease. The Gastrointestinal Tract. Surgery for Inflammatory Bowel Disease
 The Gastrointestinal Tract Surgery for Inflammatory Bowel Disease Jonathan Chun, MD The regon Clinic Gastrointestinal and Minimally Invasive Surgery Crohn s Disease Can affect anywhere in the GI tract,
The Gastrointestinal Tract Surgery for Inflammatory Bowel Disease Jonathan Chun, MD The regon Clinic Gastrointestinal and Minimally Invasive Surgery Crohn s Disease Can affect anywhere in the GI tract,
ONE of the most severe complications of diverticulitis of the sigmoid
 CLEVELAND CLINIC QUARTERLY Copyright 1970 by The Cleveland Clinic Foundation Volume 37, July 1970 Printed in U.S.A. Colonic diverticulitis with perforation to region of left hip: a rare complication Report
CLEVELAND CLINIC QUARTERLY Copyright 1970 by The Cleveland Clinic Foundation Volume 37, July 1970 Printed in U.S.A. Colonic diverticulitis with perforation to region of left hip: a rare complication Report
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Original article Surgical outcomes and their relation to the number of prior episodes of diverticulitis
 Gastroenterology Report 1 (2013) 64 69, doi:10.1093/gastro/got017 Original article Surgical outcomes and their relation to the number of prior episodes of diverticulitis Shota Takano, Cesar Reategui, Giovanna
Gastroenterology Report 1 (2013) 64 69, doi:10.1093/gastro/got017 Original article Surgical outcomes and their relation to the number of prior episodes of diverticulitis Shota Takano, Cesar Reategui, Giovanna
Chapter I 7. Laparoscopic versus open elective sigmoid resection in diverticular disease: six months follow-up of the randomized control Sigma-trial
 Chapter I 7 Laparoscopic versus open elective sigmoid resection in diverticular disease: six months follow-up of the randomized control Sigma-trial Bastiaan R. Klarenbeek Roberto Bergamaschi Alexander
Chapter I 7 Laparoscopic versus open elective sigmoid resection in diverticular disease: six months follow-up of the randomized control Sigma-trial Bastiaan R. Klarenbeek Roberto Bergamaschi Alexander
Current indications and role of surgery in the management of sigmoid diverticulitis
 Online Submissions: http://www.wjgnet.com/1007-9327office wjg@wjgnet.com doi:10.3748/wjg.v16.i7.804 World J Gastroenterol 2010 February 21; 16(7): 804-817 ISSN 1007-9327 (print) 2010 Baishideng. All rights
Online Submissions: http://www.wjgnet.com/1007-9327office wjg@wjgnet.com doi:10.3748/wjg.v16.i7.804 World J Gastroenterol 2010 February 21; 16(7): 804-817 ISSN 1007-9327 (print) 2010 Baishideng. All rights
Diverticulitis is largely a disease of an aging population
 GASTROENTEROLOGY 2010;138:2267 2274 Laparoscopy Improves Short-term Outcomes After Surgery for Diverticular Disease ANDREW J. RUSS, KARI L. OBMA, VICTORIA RAJAMANICKAM, YIN WAN, CHARLES P. HEISE, EUGENE
GASTROENTEROLOGY 2010;138:2267 2274 Laparoscopy Improves Short-term Outcomes After Surgery for Diverticular Disease ANDREW J. RUSS, KARI L. OBMA, VICTORIA RAJAMANICKAM, YIN WAN, CHARLES P. HEISE, EUGENE
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Open abdomen in trauma. Ari Leppäniemi Abdominal Center Meilahti hospital University of Helsinki Finland
 Open abdomen in trauma Ari Leppäniemi Abdominal Center Meilahti hospital University of Helsinki Finland Frequency and causes of open abdomen - in 23% (344/1531) after trauma laparotomies - damage control
Open abdomen in trauma Ari Leppäniemi Abdominal Center Meilahti hospital University of Helsinki Finland Frequency and causes of open abdomen - in 23% (344/1531) after trauma laparotomies - damage control
Assessment of Risk for Recurrent Diverticulitis
 Assessment of Risk for Recurrent A Proposal of Risk Score for Complicated Recurrence Ville Sallinen, MD, PhD, Juha Mali, Med Cand, Ari Leppäniemi, MD, PhD, and Panu Mentula, MD, PhD Abstract: Recurrence
Assessment of Risk for Recurrent A Proposal of Risk Score for Complicated Recurrence Ville Sallinen, MD, PhD, Juha Mali, Med Cand, Ari Leppäniemi, MD, PhD, and Panu Mentula, MD, PhD Abstract: Recurrence
Bile Duct Injury during Lap Chole. Bile Duct Injury during cholecystectomy TOPICS. 1. Prevalence, mechanisms, prevention and diagnosis
 Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Bowel Preparation for Elective Colorectal Surgery: Helpful or Harmful? Michael J Stamos, MD University of California, Irvine
 Bowel Preparation for Elective Colorectal Surgery: Helpful or Harmful? Michael J Stamos, MD University of California, Irvine History of Colon Surgery Early 20 th Century mortality rates for colorectal
Bowel Preparation for Elective Colorectal Surgery: Helpful or Harmful? Michael J Stamos, MD University of California, Irvine History of Colon Surgery Early 20 th Century mortality rates for colorectal
Spectrum of Diverticular Disease. Outline
 Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Clinical Questions. Clinical Questions. Clinical Questions. Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen
 Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
Management of Perforated Colon Cancers
 Management of Perforated Colon Cancers Introduction Colon and rectal cancers are the most common gastrointestinal cancers. They are 3 rd most common and 2 nd most common causes of cancer deaths among men
Management of Perforated Colon Cancers Introduction Colon and rectal cancers are the most common gastrointestinal cancers. They are 3 rd most common and 2 nd most common causes of cancer deaths among men
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: SEPSIS & THE CRITICALLY ILL OR COMPROMISED PATIENT
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: SEPSIS & THE CRITICALLY ILL OR COMPROMISED PATIENT
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Types of peritonitis and management. J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016
 Types of peritonitis and management J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016 Case Presentation xx year old patient presents to ED with complaints of one day of abdominal pain s ince
Types of peritonitis and management J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016 Case Presentation xx year old patient presents to ED with complaints of one day of abdominal pain s ince
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery and Anastomotic Leakage
 Complications of Colorectal Surgery and Diverticulitis Dig Surg 2002;19:150 155 P.B. Soeters a J.P.J.G.M. de Zoete a C.H.C. Dejong a N.S. Williams b C.G.M.I. Baeten a a Department of Surgery, University
Complications of Colorectal Surgery and Diverticulitis Dig Surg 2002;19:150 155 P.B. Soeters a J.P.J.G.M. de Zoete a C.H.C. Dejong a N.S. Williams b C.G.M.I. Baeten a a Department of Surgery, University
Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic Surgery for Colorectal Disease
 ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2018;21(1):38-42 Journal of Minimally Invasive Surgery Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic
ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2018;21(1):38-42 Journal of Minimally Invasive Surgery Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM
 Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM") ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM DATA COLLECTION FORM Most Australian hospitals contribute data
ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM DATA COLLECTION FORM Most Australian hospitals contribute data
Outcomes of Patients with Preoperative Weight Loss following Colorectal Surgery
 Outcomes of Patients with Preoperative Weight Loss following Colorectal Surgery Zhobin Moghadamyeghaneh MD 1, Michael J. Stamos MD 1 1 Department of Surgery, University of California, Irvine Nothing to
Outcomes of Patients with Preoperative Weight Loss following Colorectal Surgery Zhobin Moghadamyeghaneh MD 1, Michael J. Stamos MD 1 1 Department of Surgery, University of California, Irvine Nothing to
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Difficult Abdominal Closure. Mark A. Carlson, MD
 Difficult Abdominal Closure Mark A. Carlson, MD Illustrative case 14 yo boy with delayed diagnosis of appendicitis POD9 Appendectomy 2 wk after onset of symptoms POD4: return to OR for midline laparotomy
Difficult Abdominal Closure Mark A. Carlson, MD Illustrative case 14 yo boy with delayed diagnosis of appendicitis POD9 Appendectomy 2 wk after onset of symptoms POD4: return to OR for midline laparotomy
Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer
 SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
Diverticulitis laparoscopic lavage vs resection (Hartman procedure) for acute diverticulitis with peritonitis
 for acute diverticulitis with peritonitis") Protocol Diverticulitis laparoscopic lavage vs resection (Hartman procedure) for acute diverticulitis with peritonitis DILALA trial A trial within the Scandinavian Surgical Network for Clinical Trials
Protocol Diverticulitis laparoscopic lavage vs resection (Hartman procedure) for acute diverticulitis with peritonitis DILALA trial A trial within the Scandinavian Surgical Network for Clinical Trials
National Emergency Laparotomy Audit. Help Box Text
 National Emergency Laparotomy Audit Help Box Text Version Control Version 1.1 06/12/13 1.2 13/12/13 1.3 20/12/13 1.4 20/01/14 1.5 30/01/14 1.6 13/03/14 1.7 07/04/14 1.8 01/12/14 1.9 05/05/15 1.10 02/07/15
National Emergency Laparotomy Audit Help Box Text Version Control Version 1.1 06/12/13 1.2 13/12/13 1.3 20/12/13 1.4 20/01/14 1.5 30/01/14 1.6 13/03/14 1.7 07/04/14 1.8 01/12/14 1.9 05/05/15 1.10 02/07/15
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT
 STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
Management of Diverticulitis. Sanjay Adusumilli MBBS MS FRACS
 Management of Diverticulitis Sanjay Adusumilli MBBS MS FRACS 0411 051 281 Trained by CSSANZ in Oxford (UK) and Perth Appointments at BMDH, HSS, Norwest Private and SAN Hospital Surgery performed: Laparoscopic
Management of Diverticulitis Sanjay Adusumilli MBBS MS FRACS 0411 051 281 Trained by CSSANZ in Oxford (UK) and Perth Appointments at BMDH, HSS, Norwest Private and SAN Hospital Surgery performed: Laparoscopic
Listed below are some of the words that you might come across concerning diseases and conditions of the bowels.
 Listed below are some of the words that you might come across concerning diseases and conditions of the bowels. Abscess A localised collection of pus in a cavity that is formed by the decay of diseased
Listed below are some of the words that you might come across concerning diseases and conditions of the bowels. Abscess A localised collection of pus in a cavity that is formed by the decay of diseased
Disclosure of Affiliations. The Way We Hope It Goes. Medicines and Surgery for IBD. None. Cases: Sweet and Not So Sweet
 Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
Right Colon, Sigmoid Colon, and Transverse Colon Diverticulitis in the Same Patient: Report of a Case
 Right Colon, Sigmoid Colon, and Transverse Colon Diverticulitis in the Same Patient: Report of a Case Marc Greenwald, M.D., Tzvi Nussbaum, M.D. Department of Surgery, Division of Colon and Rectal Surgery,
Right Colon, Sigmoid Colon, and Transverse Colon Diverticulitis in the Same Patient: Report of a Case Marc Greenwald, M.D., Tzvi Nussbaum, M.D. Department of Surgery, Division of Colon and Rectal Surgery,
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Outcomes of Colostomy Reversal Procedures in Two Teaching Hospitals in Addis Ababa, Ethiopia A. Bekele, B. Kotisso, H. Biluts Correspondence to
 East and Central African Journal of Surgery http://www.bioline.org.br/js 9 Outcomes of Colostomy Reversal Procedures in Two Teaching Hospitals in Addis Ababa, Ethiopia A. Bekele, B. Kotisso, H. Biluts
East and Central African Journal of Surgery http://www.bioline.org.br/js 9 Outcomes of Colostomy Reversal Procedures in Two Teaching Hospitals in Addis Ababa, Ethiopia A. Bekele, B. Kotisso, H. Biluts
A clinical and radiological comparison of sigmoid diverticulitis episodes 1 and 2
 Original article doi:10.1111/j.1463-1318.2011.02642.x A clinical and radiological comparison of sigmoid diverticulitis episodes 1 and 2 P. Gervaz*, A. Platon, L. Widmer, P. Ambrosetti* and P.-A. Poletti
Original article doi:10.1111/j.1463-1318.2011.02642.x A clinical and radiological comparison of sigmoid diverticulitis episodes 1 and 2 P. Gervaz*, A. Platon, L. Widmer, P. Ambrosetti* and P.-A. Poletti
Selective Nonoperative Management of Penetrating Abdominal Trauma. Kings County Hospital Center Verena Liu, MD 10/13/2011
 Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Endoscopic management of sleeve leaks
 Endoscopic management of sleeve leaks Mr Damien Loh Oesophagogastric and Bariatric Surgeon The Alfred The clinical problem Incidence 0.1-7% Inpatient mortality 2-5% High morbidity Prolonged ICU and in-hospital
Endoscopic management of sleeve leaks Mr Damien Loh Oesophagogastric and Bariatric Surgeon The Alfred The clinical problem Incidence 0.1-7% Inpatient mortality 2-5% High morbidity Prolonged ICU and in-hospital
Surgical Management of IBD in the Age of Biologics
 Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Emergency one-stage resection without mechanical bowel preparation for acute sigmoid volvulus
 JMBR: A Peer-review Journal of Biomedical Sciences June 2004, Vol. 3 No. 1 pp 86 90 Emergency one-stage resection without mechanical bowel preparation for acute sigmoid volvulus OO Oludiran a and OC Osime
JMBR: A Peer-review Journal of Biomedical Sciences June 2004, Vol. 3 No. 1 pp 86 90 Emergency one-stage resection without mechanical bowel preparation for acute sigmoid volvulus OO Oludiran a and OC Osime
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Recurrent Left Colonic Diverticulitis Episodes: More Severe Than the Initial Diverticulitis?
 World J Surg (2009) 33:547 552 DOI 10.1007/s00268-008-9898-9 Recurrent Left Colonic Diverticulitis Episodes: More Severe Than the Initial Diverticulitis? Olivier Pittet Æ Nikos Kotzampassakis Æ Sabine
World J Surg (2009) 33:547 552 DOI 10.1007/s00268-008-9898-9 Recurrent Left Colonic Diverticulitis Episodes: More Severe Than the Initial Diverticulitis? Olivier Pittet Æ Nikos Kotzampassakis Æ Sabine
Key words: colostomy closure, colostmy, temporary colostomy, complications, complications of colon surgery
 Key words: colostomy closure, colostmy, temporary colostomy, complications, complications of colon surgery Carcinoma of colon and rectum Trauma Burn Iatrogenic Pelvic abscess Diverticular disease No. of
Key words: colostomy closure, colostmy, temporary colostomy, complications, complications of colon surgery Carcinoma of colon and rectum Trauma Burn Iatrogenic Pelvic abscess Diverticular disease No. of
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
Non Operative Management of Perforated Duodenal Ulcers. Rabih Nemr M.D. Kings County Hospital Sept 2006
 Non Operative Management of Perforated Duodenal Ulcers Rabih Nemr M.D. Kings County Hospital Sept 2006 Case presentation 40 year old male presenting with abdominal pain: Epigastric Worsening over the last
Non Operative Management of Perforated Duodenal Ulcers Rabih Nemr M.D. Kings County Hospital Sept 2006 Case presentation 40 year old male presenting with abdominal pain: Epigastric Worsening over the last
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies
 HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
Percutaneous CT Scan-Guided Drainage vs. Antibiotherapy Alone for Hinchey II Diverticulitis: A Case-Control Study
 Percutaneous CT Scan-Guided Drainage vs. Antibiotherapy Alone for Hinchey II Diverticulitis: A Case-Control Study D. Brandt, M.D., 1 P. Gervaz, M.D., 1 Y. Durmishi, M.D., 1 A. Platon, M.D., 2 Ph. Morel,
Percutaneous CT Scan-Guided Drainage vs. Antibiotherapy Alone for Hinchey II Diverticulitis: A Case-Control Study D. Brandt, M.D., 1 P. Gervaz, M.D., 1 Y. Durmishi, M.D., 1 A. Platon, M.D., 2 Ph. Morel,
LIVER TRAUMA. Jonathan R. Hiatt, MD
 Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
A regional perspective, to improve patient outcomes. Mr Peter F. Burke. Senior Consultant General Surgeon: LRH
 A regional perspective, to improve patient outcomes. Mr Peter F. Burke. Senior Consultant General Surgeon: LRH What is its role? *VASM involves the clinical review of all cases, where patients have died
A regional perspective, to improve patient outcomes. Mr Peter F. Burke. Senior Consultant General Surgeon: LRH What is its role? *VASM involves the clinical review of all cases, where patients have died
Anastomotic Leak After Colonic Resection
 RESIDENT S CORNER Anastomotic Leak After Colonic Resection Senitila Tutone, M.B.Ch.B. Andrew G. Hill, M.B.Ch.B., M.D., Ed.D., F.R.A.C.S. Department of General Surgery, South Auckland Clinical Campus, Middlemore
RESIDENT S CORNER Anastomotic Leak After Colonic Resection Senitila Tutone, M.B.Ch.B. Andrew G. Hill, M.B.Ch.B., M.D., Ed.D., F.R.A.C.S. Department of General Surgery, South Auckland Clinical Campus, Middlemore
... Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment.
 Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Septic Phlebitis and Gas in the Inferior Mesenteric Vein: CT findings in Two Cases and Review of Literature
 ISPUB.COM The Internet Journal of Surgery Volume 16 Number 2 Septic Phlebitis and Gas in the Inferior Mesenteric Vein: CT findings in Two Cases and Review of J McClenathan Citation J McClenathan. Septic
ISPUB.COM The Internet Journal of Surgery Volume 16 Number 2 Septic Phlebitis and Gas in the Inferior Mesenteric Vein: CT findings in Two Cases and Review of J McClenathan Citation J McClenathan. Septic
Management of colorectal anastomotic leakage: differences between salvage and anastomotic takedown
 The American Journal of Surgery (2012) 204, 671 676 Clinical Science Management of colorectal anastomotic leakage: differences between salvage and anastomotic takedown Domenico Fraccalvieri, M.D., Sebastiano
The American Journal of Surgery (2012) 204, 671 676 Clinical Science Management of colorectal anastomotic leakage: differences between salvage and anastomotic takedown Domenico Fraccalvieri, M.D., Sebastiano
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Colorectal Surgery in the Elderly. Stephen Smith
 Colorectal Surgery in the Elderly Stephen Smith Scope WHO >65 Social definition No COI Age specific incidence of CRC in Australia 2016 (new cases/100,000) My data: elective bowel resections
Colorectal Surgery in the Elderly Stephen Smith Scope WHO >65 Social definition No COI Age specific incidence of CRC in Australia 2016 (new cases/100,000) My data: elective bowel resections
Diverticular Disease Dr. Charles H. Knowles (PhD FRCS)
") Diverticular Disease Academic Surgical Unit Barts and the London School of Medicine and Dentistry Queen Mary University of London 1 Overview - diverticular disease Definitions Spectrum of disease Epidemiology
Diverticular Disease Academic Surgical Unit Barts and the London School of Medicine and Dentistry Queen Mary University of London 1 Overview - diverticular disease Definitions Spectrum of disease Epidemiology
Disclosures. Dr. Hall is a paid consultant to the American College of Surgeons (ACS) as Associate Director of ACS-NSQIP
 as Associate Director of ACS-NSQIP") Does Routine Drainage of the Operative Bed following Elective Distal Pancreatectomy reduce Complications? An Analysis of the ACS-NSQIP Pancreatectomy Demonstration Project Stephen W. Behrman, MD 1, Ben
Does Routine Drainage of the Operative Bed following Elective Distal Pancreatectomy reduce Complications? An Analysis of the ACS-NSQIP Pancreatectomy Demonstration Project Stephen W. Behrman, MD 1, Ben