4 Cartilage Palisades in Underlay Tympanoplasty Techniques
|
|
|
- Shanna Arnold
- 6 years ago
- Views:
Transcription
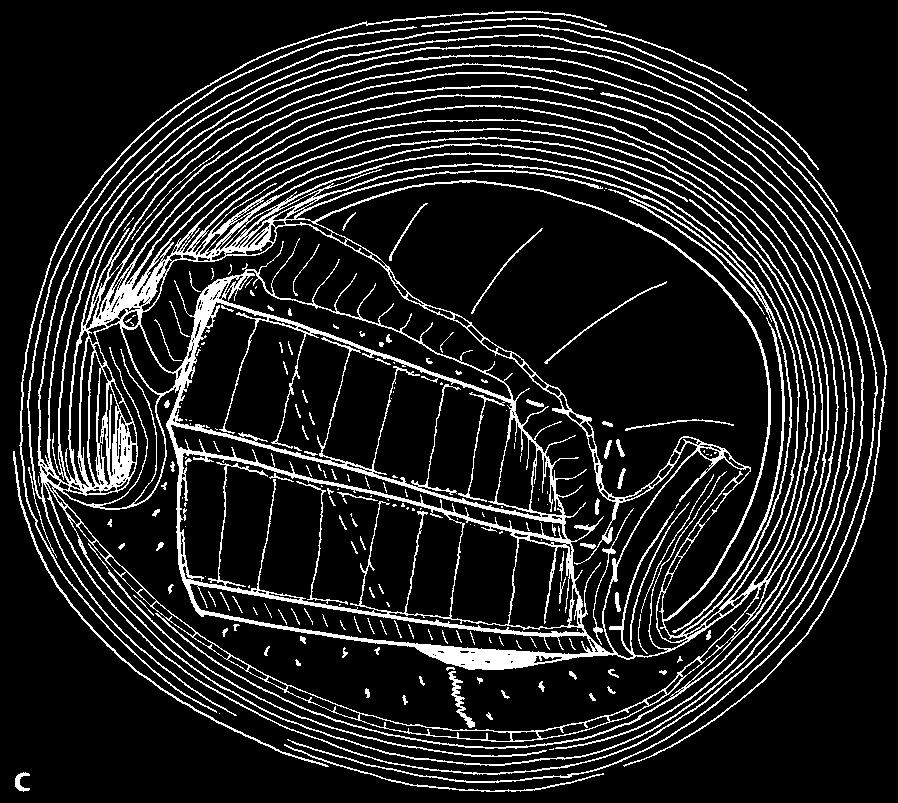
1 52 4 Cartilage Palisades in Underlay Tympanoplasty Techniques Definition Cartilage underlay palisade technique is the oldest and the most popular technique in cartilage tympanoplasty. As shown in Chapter 1, during the 1960s and 1970s Heermann gradually developed the method as used today:parallel placement of mm wide full-thickness cartilage strips in the inferosuperior direction of the tympanic cavity. Palisades are usually cut from pieces of tragal or conchal cartilagecoveredontheconcavesidewiththeperichondrium.althoughthepalisadesareplacedsidebysideand close to each other there will be some distance between the palisades. The edges of the perichondrium on the outer side of the palisade are supposed to stick to each other and close the gaps, facilitating the epithelialization of the eardrum. Cartilage palisades have most often been used as underlay grafts (Heermann and Heermann 1967; Heermann et al. 1970; Heermann 1977, 1978, 1991, 1992; Wiegand 1978; Milewski 1989, 1991, 1993; Amedee et al. 1989; Péré 1989; Helms 1991, 1995; Hildmann et al. 1996; Velepic et al. 2001; Andersen et al. 2002, 2004; Neumann et al. 2003; Neumann and Jahnke 2005). The superior ends of the palisades are often supported by the architrave, a piece of cartilage placed onto the eminence of the tensor tympani muscle (Heermann and Heermann, 1967; Heermann et al. 1970; Heermann 1992). In the posterior part of the tympanic cavity the superior endsofthepalisadearesupportedbythechordatympani, incudostapedial joint, stapes head, and interposition prosthesis. The inferior end of the first palisade, the simmering, placed under the bony annulus is sometimes supported by a piece of cartilage placed in the anterior part of the hypotympanum. Heermann places the inferior ends of the remaining palisades onto the bony annulus with no need for inferior support by Gelfoam. I often prefer to place the inferior ends at the level of and close to the bony annulus, not onto and not under the bony annulus, and often support the palisades with Gelfoam. Superiorly, the support by Gelfoam is sometimes needed. In my opinion the architrave can often be replaced by Gelfoam. I regularly support the short palisade connecting the undersurface of the umbo with Gelfoam. Some groups and some surgeons never apply Gelfoam within the middle ear, claiming that it causes formation of adhesions in the middle ear. Some other groups and surgeons use always Gelfoam to support the eardrum grafts or interposed ossicles. I frequently use Gelfoam to support the underlay grafts and have not found adhesions caused by Gelfoam. Indications for Surgery Heermann considered wide indications for palisade technique and used cartilage palisades in nearly all cases with chronic otitis media and its sequelae. Since1995Ihavealwaysusedunderlaytechniquesin posterior perforation and in total perforation after removal of retractions, in sinus cholesteatoma, after tensa retraction cholesteatoma, and in adhesive otitis media. Primary and late results after surgery of sinus cholesteatoma and tensa retraction cholesteatoma in children have been published. The hearing results and stability of reconstructed eardrum were surprisingly good (Andersen et al. 2002, 2004; Uzun et al. 2003; 2004). Palisade techniques can be used in endaural approaches, as used by Heermann, or in retroauricular approaches, as used by Milewski, Helms and Hildmann, or as I prefer in transcanal approaches with fixed ear speculum. Generally retractions, atelectasis, adhesive otitis and recurrent surgery cases with poor tubal function or poor tubal patency, expressed in negative preoperative Valsalva test, will be absolute candidates for cartilage palisade technique. Harvesting and Shaping of Palisades Harvesting and shaping of palisades is easy (Chapter 3). A piece of conchal or tragal cartilage is removed with the perichondrium attached on both sides. The size for a total perforation is 10 mm 8mm.Theconvexsideofthepalisade is turned toward the tympanic cavity and should not be covered with perichondrium; the perichondrium is thereforeremovedfromtheanteriorsideofthetragal cartilage, or from the posterior side of the conchal cartilage. The palisades are cut as 0.5 3mm wide strips. Even when they are placed close to one another there will al-
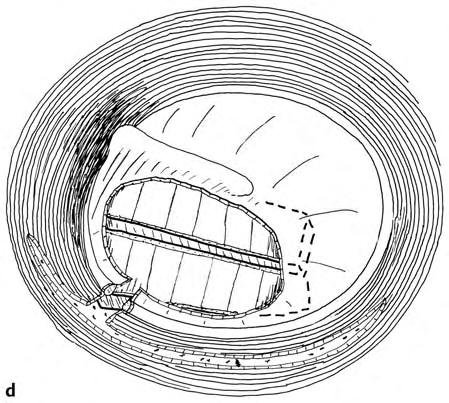
2 53 ways be a small separation between the palisades, but this gap will soon be filled with tissue fluid. The perichondrium on the outer side sticks to the overlying remnant of the eardrum or/and the fibrous annulus. Tissue fluid connects the neighboring strips of perichondrium as well, allowing epithelialization of the new eardrum without any ingrowth of the epithelium around the edges of the palisades into the inner side of the eardrum. Surgical Techniques The surgical techniques are adapted to location and size of theperforationaswellastheextensionoftheactivedisease. The ossicular pathology will also decide the choice of surgical technique. Posterior Perforation In posterior perforation the tympanomeatal flap, including the fibrous annulus and the remnants of the eardrum have to be elevated. The tympanomeatal flap may be cut at the 9-o clock position, resulting in swing-door technique with excellent view of the tympanic sinuses. The technique involving raising a large tympanomeatal flap (MMES_1, Figs ) is most often used in the retroauricular approach, but can also be used in the endaural approach. The elevation of a tympanomeatal flap is suitable for underlay palisade technique, because the inferoposterior bony annulus is visualized, facilitating placement of the palisades either onto or close to the bony annulus. Swing-Door Technique The most popular method is the swing-door technique with a superior and an inferior skin flap providing a good visibility to the tympanic cavity. Epithelium around the edges of the perforation is removed carefully. A tympanomeatal flap is raised after a medial circumferential incision of the posterior ear canal skin. A medial radial incision divides the flap into a superior and inferior flap (Fig. 4.1a). The skin flaps, together with the fibrous annulus and the eardrum remnant, are elevated together with epithelium surrounding the chorda tympani and continuing into the posterior tympanum as a remnant of a retraction. To provide sufficient visibility over the tympanic sinuses, it is often necessary to drill the posterosuperior bony annulus (Fig. 4.1b). The first palisade is placed in the superoinferior direction, slightly posterior to the malleus handle. The second palisade is placed superiorly onto the edge of the bony annulusand onto the chordatympani (Fig. 4.1c). The saved and replaced epithelial flaps will adhere to the palisades (Fig. 4.1 d) and it is often not necessary to support the palisades with Gelfoam. Another option is placement of the palisades at a slightly deeper level. The superior ends of the two palisades just touch the superior bony annulus and the anterior palisade is placed at the level of the malleus handle, but not on it (Fig. 4.1e). The palisades rest mainly on the chorda tympani and the long process of the incus (Fig. 4.1 f). Inferior ends of the palisades are supported with Gelfoam balls. After replacement of the flaps the palisades will usually remain stable (Fig. 4.1 g) because the epithelium sticks to the palisades. It is therefore always advantageous to save all epithelial flaps. Large Tympanomeatal Flap Technique This incision provides a good view to the entire posterior tympanum and even to the anterior tympanum when tilting the patient forward. After the edges of the perforation are cleaned, a large posterior tympanotomy incision is performed (Fig. 4.2a); the tympanomeatal flap is elevated, and pushed together with the eardrum remnants anterior to the malleus handle (Fig. 4.2b). The posterior part of the malleushandleiscleanedofepitheliumtoprovidegood contact to the cartilage palisade. The first palisade is placed closetotheposterioredgeofthemalleushandle.inferiorly, all palisades are placed onto the bony annulus; superiorly, the palisades just touch the superior bony annulus (Fig. 4.2c). After replacement of the tympanomeatal flap, good contact with the palisades is established (Fig. 4.2 d). Thus, in posterior perforation there are two options in placement of palisades in relation to the bony annulus: either close to or onto the bony annulus, but we do not know which option is better. Instead of placing the inferior ends of the palisades onto the bony annulus they can be placed at the level of the bony annulus (Fig. 4.2e). Avoiding placement of the palisades onto the bony annulus may increase the vibratility of the palisades. Inferior Perforation Application of cartilage palisades in underlay technique in inferior perforation is less common than in posterior or total perforation. However, in reoperation, poor function of the eustachian tube, retraction, and previous cholesteatoma, or in adhesive otitis media, underlay palisade technique can be a good solution. Swing-door technique or large tympanomeatal flap technique can be employed, but even the simple technique without tympanomeatal flaps can be used. Technique without Tympanomeatal Flap In this technique the removal of the epithelium around the perforation and scarification of the mucosa under the edges of the perforation are important. This can be achieved with a sickle knife, round knife, curved cup forces, or curved small elevator (Fig. 4.3a). Gelfoam balls


3 54 4 Cartilage Palisades in Underlay Tympanoplasty Techniques




4 Surgical Techniques 55 Fig. 4.1a g Underlay swing-door cartilage palisade technique in a posterior perforation with intact ossicular chain. a Theedgesoftheperforationaredeepithelialized.Aposterior circumferential medial incision and a radial incision at the 9-o clock position are made. b A superior and an inferior skin flap and all epithelial flaps around the perforation are elevated. Using a round knife, the mucous membrane of the underside of the eardrum is removed around the perforation to facilitate a better attachment of the palisade to the eardrum. c Two large palisades are placed close to the malleus handle and superiorly onto the bony annulus. Inferiorly, the palisades are most often placed just under the eardrum remnant with the contact to the denuded mucosa. d All flaps are replaced, but superiorly and anteriorly only small flaps cover the palisades. e An alternative placement of the palisades in a slightly deeper level in a posterior perforation. The first palisade is placed closed to and parallel to the malleus handle, resting on the chorda tympani. The palisade is thus placed slightly deeper. f The following two palisades are also placed onto the chorda tympani. The palisades may also touch the long process of the incus. g The epithelial flaps are replaced. Fig. 4.2a e Underlay cartilage palisade technique with large tympanomeatal flaps in posterior perforation andintact ossicular chain. a Theedgeoftheperforationwiththekeratinizedepitheliumis excised. The skin incision is placed relatively laterally in the ear canal. b Alargetympanomeatalflap iselevated together with the fibrous annulus and the remnants of the posterior half of the eardrum and the epithelium covering the posterior half of the malleus handle. c The palisades are placed onto the inferoposterior bony annulus. The first palisade is placed on the posterior edge of the malleus handle. Superiorly, the palisades are placed close, but not onto, the bony annulus. Fig. 4.2d, e e
5 56 4 Cartilage Palisades in Underlay Tympanoplasty Techniques Fig. 4.2d e d The tympanomeatal flap with the fibrous annulus and the remnants of the eardrum are replaced. e Alternative placement of the palisades under the eardrum remnant close to the bony annulus. Fig. 4.3a c A variation of placement the palisades close to the bony annulus insteadof onto the bony annulus. a The edge of the perforation is cleaned of the epithelium. Mucosa under the eardrum remnant is removed and scarified using the cup forceps, sickle knife, round knife, or a curved elevator. b After placement of Gelfoam balls, the palisades are placed close to the inferior bony annulus. Superiorly, the palisades are placed onto the Gelfoam balls. The palisades are positioned under the eardrum remnant and will stick to the eardrum remnant. c Gelfoam balls cover the lower part of the eardrum stabilizing the palisades.
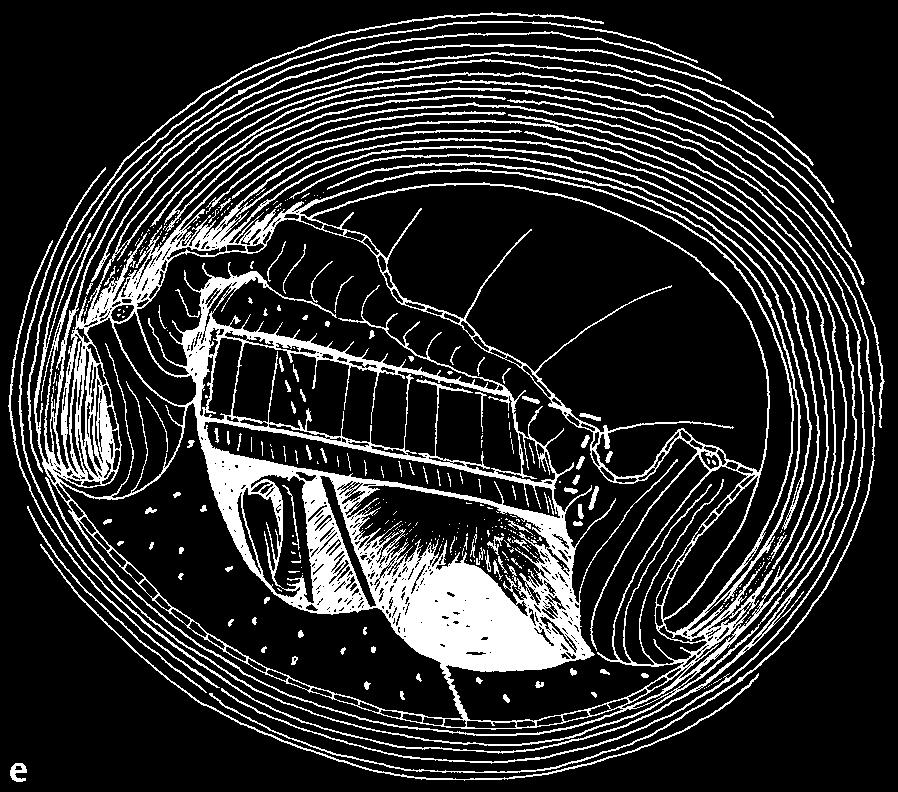
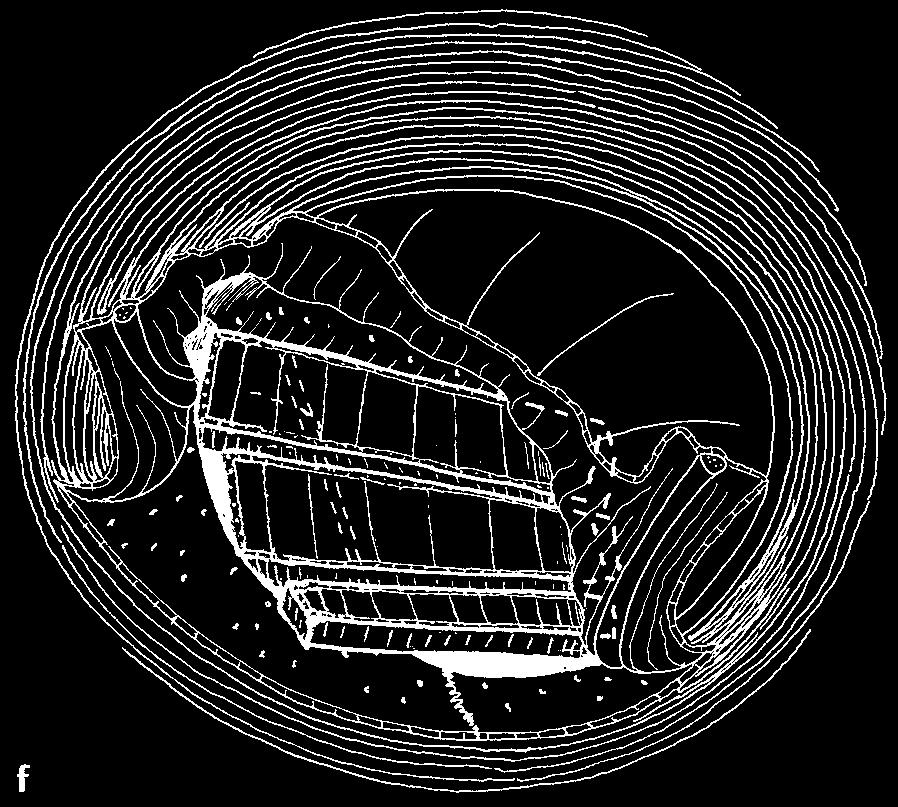
6 Surgical Techniques 57 Fig. 4.4a g Underlay swing-door cartilage palisade technique in a large inferior perforation with intact ossicular chain. a Epithelium is removed from the borders of the perforation. A circumferential incision and a radial incision are made. b The superior and inferior flaps are elevated. At the anterior border of the perforation, the fibrousannulusiselevated,exposing the bony annulus. Epithelium from the umbo is elevated and a small epithelial flap is elevated. c d The anterior palisade is placed onto the anterior and inferior bony annulus. The second palisade is placed onto the anterior edge of the umbo. The third palisade is placed onto the posterior edge of the umbo. Inferior ends of the palisades are placed onto the inferior bony annulus. The tympanomeatal flaps are replaced. Fig. 4.4e g e are placed into the tympanic cavity to support the palisades positioned under the denuded eardrum (Fig. 4.3b). Finally, the edges of the perforation are covered with Gelfoam balls for three weeks to fix the palisades (Fig. 4.3c) Swing-Door Technique Theedgesoftheperforationarecleanedofepithelium.A circumferential incision between the 10-o clock and 3- o clock positions and a radial incision at the 9-o clock positions are made (Fig. 4.4a). Two flaps are elevated. Anteriorly,theannulusfibrosisiselevatedtogetherwith the eardrum remnant. Epithelium from the umbo is elevated and a small epithelial flap is created (Fig. 4.4b). Gelfoam balls are placed in the central part of the tympanic cavity to support the superior ends of the palisades. The anterior palisade is placed onto the anterior bony annulus. Two palisades have contact with the umbo. Inferiorly, the palisades lie on the inferior bony annulus (Fig. 4.4c). The superior ends of the palisades may be supported by Gelfoam, especially in the umbo region. The tympanomeatal flap and the remnant of the eardrum are replaced (Fig. 4.4 d). The epithelial flap of the umbo is replaced. The eardrum is covered with several Gelfoam balls (Fig. 4.4e).
7 58 4 Cartilage Palisades in Underlay Tympanoplasty Techniques Fig. 4.4e g e The eardrum is covered with Gelfoam balls. f Placement of the palisades at the level of the bony annulus. The palisades touch the bony annulus, but they are not placed onto it. The palisades are supported by Gelfoam balls. g The epithelial flaps are replaced and the eardrum remnant is in good contact with the palisades. The alternative of placing the inferior and posterior ends of the palisades close to and at the level of the bony annulus (Fig. 4.4 f) requires extensive scarification of the eardrum remnant to promote gluing of the palisades to the undersurface of the denuded eardrum (Fig. 4.4 g) Large Tympanomeatal Flap Technique After removal of the epithelium from the edges of the perforation, an inferior circumferential incision is made (Fig. 4.5a). A large tympanomeatal flap is elevated and the umbo is cleaned of epithelium (Fig. 4.5b). Gelfoam balls are placed into the tympanic cavity to support the superior ends of the palisades. In this example the most anterior palisade is placed under the bony annulus, but it could be placed onto the bony annulus (Fig. 4.5c, d). The short palisade is placed under the umbo, but it can be placed onto the umbo as well. The tympanomeatal flap is replaced (Fig. 4.5e) and the eardrum covered with Gelfoam (Fig. 4.5 f, g). In inferior perforation, the inferior ends of the palisades are placed onto the bony annulus, but they could be placed close to the bony annulus or even under it. In such cases a support of Gelfoam balls should be applied (Fig. 4.5h). After replacement of the tympanomeatal flap the palisades will come into contact with the eardrum remnant (Fig. 4.5e, f) and be stabilized. Total Perforation Reconstruction of the eardrum with cartilage palisades or cartilage strips is often indicated in total perforation, in particular with signs of previous retraction. Cartilage tympanoplasty is also indicated in cases of previously unsuccessful surgery of a total perforation. In cases with a dry total perforation with negative preoperative Valsalva maneuver, cartilage tympanoplasty is absolutely indicated. Cartilage palisades can also be employed in slightly moist ears with some thickness of the mucosa.
8 104 6 Tympanoplasty with Broad Cartilage Palisades cavity, the reconstructed eardrum has a mosaic appearance (see Chapter 7). Indications for Tympanoplasty with Broad Cartilage Palisades Based on nine years of experience with broad palisades, Bernal-Sprekelsen and co-workers (2003) recommend the following indications for tympanoplasty with broad palisades: P Total and subtotal perforations P Perforations with tympanosclerotic plaques P Perforation with atrophic membranes P Revision surgery for failed myringoplasty or tympanoplasty type 1 P Anterior and inferior perforation with tubal discharge P Retraction pockets P Partially or completely atelectatic tympanic membranes P Tympanic adherences P Revision surgery for failed tympanoplasties of type 2 and type 3 as well as tympanomastoidectomies. The Bernal-Sprekelsen Broad Palisade Techniques Broad palisades are mainly used in total and subtotal perforation as underlay graft. They are supported by 2mm 3 mm pieces of cartilage placed vertically into the hypotympanum or into other regions such as the eminence of the tensor tympani muscle (Fig. 6.1b). Total Perforation with Intact Ossicular Chain The tympanoplasty may be performed in a transcanal, endaural, or retroauricular approach. The supports for the palisades are two or three 2 mm 3 mm pieces of cartilage. Gelfoam can be used as well. The posterosuperior end of the palisade can rest on the chorda tympani and/or on the long process of the incus. In an endaural approach, the edges of the perforation and around the malleus handle are cleaned. A medial circumferential incision with a radial incision is performed and two tympanomeatal flaps are elevated (Fig. 6.2a, b). The fibrous annulus is further elevated, exposing the bony annulus (Fig. 6.2c). Two sufficiently small pieces of cartilage are placed into the hypotympanum and along the eminence of the tensor tympani muscle to support the palisades (Fig. 6.2 d). An anterior semicircular palisade and a posterior palisade are placed onto the small pieces of cartilage (Fig. 6.2e). A small palisade is placed between thetwolargepalisadesclosetotheumboandissupported with Gelfoam balls (Fig. 6.2 f). The tympanomeatal flaps with the eardrum remnant are replaced (Fig. 6.2 g). Bernal-Sprekelsen and his group use several thin bluish silicone foils to cover the eardrum and the ear canal. After packing the ear canal with Gelfoam, the outer ends of the foils are turned inward (Fig. 6.2h), to stabilize the reconstructed eardrum and promote its epithelialization. When suturing the skin incisions laterally in the ear canal, the silicone foils are turned outward to cover the sutures and prevent formation of granulations. Total Perforation with Missing Ossicles Even if the entire malleus is missing, the reconstruction of theeardrumwillbethesameaswhenthemalleusheadis present. The support for the superior ends of the palisades will be a 1 mm 3 mm piece of cartilage positioned partly onto the eminence of the facial nerve, partly onto the eminence of the tensor tympani muscle. In the hypotympanum a similar piece of cartilage is placed to support the broad anterior palisade (Fig. 6.3a). Onto the footplate an oval cartilage guide 0.3 mm thick is placed with a hole for the foot of the TORP prosthesis (see Fig. 3.37). The second palisade is placed at the site of the malleus and is supported in the same manner as the anterior palisade. The second palisade rests partly on the head of the TORP prosthesis. The posterior semilunar palisade is supported partly by the TORP and partly by the superior small piece of cartilage (Fig. 6.3b). The tympanomeatal flaps and eardrum remnants are replaced (Fig. 6.3c, d). Total Perforation with Missing Long Process of Incus Tympanoplasty type 2 with interposition of a partial ossicular replacement prosthesis (PORP) of various materials andshapesisillustratedinnumerouschaptersofthisbook (see Chapters 4, 5, 7, 8, 9; see also MMES_1, pp ). Here only an example of the most common ossiculoplasty, the incus interposition, will be shown in connection with cartilage tympanoplasty with broad palisades, in particular to illustrate the need for reduction and careful shaping of the incus to accommodate the broad palisades. In endaural approach the edges of the total perforation are cleaned. Using a swing-door technique, two tympanomeatal flaps are elevated, and the defective incus is extruded, reduced, and shaped to accommodate the undersurface of the broad palisade. First the anterior semilunar palisade is placed in the anterior tympanum, then the shaped incus is interposed between the head of the stapes and the malleus handle (Fig. 6.4a). Inferiorly, the palisade is supported by a piece of cartilage, placed into the hypotympanum, superiorly it is supported by an architrave. A palisade is adapted to the malleus handle and a semilunar broad posterior palisade is placed at the level of the bony
9 The Bernal-Sprekelsen Broad Palisade Techniques 105 Fig. 6.2a h Cartilage tympanoplasty with broad palisades harvested from the cymba in a case with total perforation and intact ossicular chain. a The edges of the perforation and around the malleus handle are cleaned and the epithelium is removed all the way around the entire edge. A medial circumferential incision is made. At the 9-o clock position,a small radial incision separates the tympanomeatal flap into a superior and an inferior flap. b Both flaps are elevated together with the fibrous annulus,exposing the bony annulus. c Further elevation of the remnants of the eardrum and the inferior fibrous annulus. d Further elevation of the anterior fibrous annulus and the eardrum remnant. Placement of a small piece of cartilage in the hypotympanum and one along the eminence of tensor tympani muscle to support the palisades. e The first palisade is placed onto the piece of the cartilage previously placed into the hypotympanum and onto the cartilage placed along the eminence of the tensor tympani muscle. The palisade is placed at the level of the bony annulus and beside the malleus handle under the small eardrum remnant. The posterior broad palisade is placed onto the small inferior and superior cartilage supports. The palisades are positioned at the level of the bony annulus and along the malleus handle. Fig. 6.2f h e
10 106 6 Tympanoplasty with Broad Cartilage Palisades Fig. 6.2f h f A small palisade is placed between the umbo and the inferior support cartilage. A superoposterior defect of the scutum is covered with a small palisade. A Gelfoam ball supports the upper end of the malleus palisade; support of the palisade with a Gelfoam ball is easy and effective. g The tympanomeatal flaps are replaced,together with the fibrous annulus and remnants of the eardrum. h Side view of underlay tympanoplasty type 1 with broad cartilage palisades at the level of the umbo,and packing of the ear canal. Two broad palisades are positioned at the level of the bony annulus. Several strips of blue silicone foil cover the eardrum and the ear canal skin. After placing several pieces of Gelfoam,the foils are turned inward. The lateral end of the ear canal is closed by gauze moistened with hydrocortisone oxytetracycline ointment. annulus and supported by the interposed incus (Fig. 6.4b). After replacement of the tympanomeatal flaps (Fig. 6.4c), the connection between the shaped and reduced interposed autogenous incus and the broad palisades is good (Fig. 6.4 d). Similar solid interposition prostheses can be made and shaped from cortical bone, tragal cartilage, and homogenous incus. Retracted and Adherent Malleus Handle in a Total Perforation with Defective Incus Thepathogenesisofsuchaconditionisasfollows:Chronic or recurrent secretory otitis media and long-lasting tubal dysfunction cause diffuse atrophy and retraction of the entire pars tensa, including resorption of the long process of the incus and adhesion of the umbo to the promontory. Because of severe purulent acute otitis media, the thin and atrophic pars tensa becomes necrotic and may disappear, resulting in a total perforation. In the endaural approach, the edges of the perforation are cleaned and the two tympanomeatal flaps with the anterior fibrous annulus are elevated. The defective incus is removed. Using a curved incudostapedial knife, the adhesions between the umbo and the promontory are cut and the eardrum remnant is separated from the promontory. Under the inferior half of the bony annulus three small pieces of cartilage are placed to support the inferior semilunar palisade (Fig. 6.5a). The eardrum remnants connected to the umbo and to the retracted malleus handle are elevated as a malleus flap. Then the malleus handle is elevated to its normal position (Fig. 6.5b). The autogenous incus is shaped to become more flat and is placed onto the stapes head and under the malleus handle (Bernal-Sprekelsen, personal communication 2006). The large semi-
11 The Bernal-Sprekelsen Broad Palisade Techniques 107 Fig. 6.3a d Reconstruction of a total perforation without ossicles using broad cartilage palisades and titanium TORP prosthesis. a The edges of the perforation are cleaned of epithelium. In endaural approach and swing-door technique,an inferior and a superior tympanomeatal flap are elevated together with the fibrous annulus,exposing the bony annulus. The epithelium around the attic region is elevated. The footplate is cleaned and a Hüttenbrink cartilage guide is placed onto the footplate (Hüttenbrink et al. 2004). A Kurz titanium TORP prosthesis is placed through the hole of the guide onto the footplate. Onto the eminence of the tensor tympani muscle a small cartilage palisade is placed,similar to the architrave. In the hypotympanum a 3 mm 2 mm piece of cartilage is placed to support the inferior ends of the palisades. The anterior semilunar palisade is b c d placed onto the architrave and onto the cartilage in the hypotympanum. The second palisade replaces the malleus,it is supported by the cartilage and the head of the TORP prosthesis. Thethirdpalisadecoverstheposteriorhalfofthetympanic cavity. It is placed and adapted to the head of the TORP prosthesis and the chorda tympani as well as the palisade on the tensor tympani and partly on the facial nerve. The bony defect after drilling of the posterosuperior scutum is covered with a small palisade. The tympanomeatal flaps with the eardrum remnant are replaced. Side view with some perspective at the level of the footplate of an underlay cartilage tympanoplasty type 3 with broad palisades. The Kurz titanium TORP prosthesis has contact with two palisades,which are placed at the level of the bony annulus.
8 External Ear Canal Surgery
 30 Chapter 8 8 External Ear Canal Surgery Henning Hildmann, Holger Sudhoff Surgery in the external auditory canal without surgery in the middle ear may be necessary: 1. After surgery 2. After trauma 3.
30 Chapter 8 8 External Ear Canal Surgery Henning Hildmann, Holger Sudhoff Surgery in the external auditory canal without surgery in the middle ear may be necessary: 1. After surgery 2. After trauma 3.
UC SF. Safe Surgery Rule #1. Cholesteatoma. It s hard to have a surgical complication when you are not operating
 UC SF Cholesteatoma Chronic Ear Surgery: Staying Out of Trouble! Lawrence R. Lustig, MD Department of Oto-HNS University of California San Francisco Ligaments and folds Spaces NU Epitympanic Cholesteatoma
UC SF Cholesteatoma Chronic Ear Surgery: Staying Out of Trouble! Lawrence R. Lustig, MD Department of Oto-HNS University of California San Francisco Ligaments and folds Spaces NU Epitympanic Cholesteatoma
Cartilage Palisades in Type 3 Tympanoplasty: Functional and Hearing Results
 DOI 10.1007/s12070-014-0717-3 ORIGINAL ARTICLE Cartilage Palisades in Type 3 Tympanoplasty: Functional and Hearing Results Ashish Vashishth Neeraj Narayan Mathur Deepak Verma Received: 30 January 2014
DOI 10.1007/s12070-014-0717-3 ORIGINAL ARTICLE Cartilage Palisades in Type 3 Tympanoplasty: Functional and Hearing Results Ashish Vashishth Neeraj Narayan Mathur Deepak Verma Received: 30 January 2014
Cartilage Tympanoplasty: A method for hearing reconstruction
 Original article: Cartilage Tympanoplasty: A method for hearing reconstruction 1. Dr. Sandeep B. Dabhekar, 2. Dr.Parag V. Doifode, 3 Dr. A.S. Deshpande 1. Assistant Professor, Department of ENT, Government
Original article: Cartilage Tympanoplasty: A method for hearing reconstruction 1. Dr. Sandeep B. Dabhekar, 2. Dr.Parag V. Doifode, 3 Dr. A.S. Deshpande 1. Assistant Professor, Department of ENT, Government
Exposure of facial nerve and endolymphatic sac
 Exposure of facial nerve and endolymphatic sac 1 7 4 2 3 5 6 8 1 Vertical part of the facial nerve exposed 1 Second genu of facial nerve. 2 Vertical part of facial nerve. 3 Horizontal part of facial nerve.
Exposure of facial nerve and endolymphatic sac 1 7 4 2 3 5 6 8 1 Vertical part of the facial nerve exposed 1 Second genu of facial nerve. 2 Vertical part of facial nerve. 3 Horizontal part of facial nerve.
Sliced Island Tragal Cartilage Perichondrial Composite Graft in Type I Tympanoplasty: Early Results and Experience
 Journal of Rhinolaryngo-Otologies, 2014, 2, 000-000 1 Sliced Island Tragal Cartilage Perichondrial Composite Graft in Type I Tympanoplasty: Early Results and Experience Mubarak M. Khan * and Sapna R. Parab
Journal of Rhinolaryngo-Otologies, 2014, 2, 000-000 1 Sliced Island Tragal Cartilage Perichondrial Composite Graft in Type I Tympanoplasty: Early Results and Experience Mubarak M. Khan * and Sapna R. Parab
Glasgow Temporal Bone Skills Course
 Glasgow Temporal Bone Skills Course INTRODUCTION The aspiring otologist needs to develop surgical skills in the laboratory prior to entering the operating theatre. This is because the anatomy of the temporal
Glasgow Temporal Bone Skills Course INTRODUCTION The aspiring otologist needs to develop surgical skills in the laboratory prior to entering the operating theatre. This is because the anatomy of the temporal
COMPLICATION. Complications
 Complications COMPLICATION COMPLICATIONS MANAGEMENT OF A FIXED FOOTPLATE IN CHRONIC OTITIS MEDIA BENOIT GRATACAP, MD, ROBERT VINCENT, MD, JEAN-BERNARD CAUSSE, MD From the Jean Causse Clinic, Colombiers,
Complications COMPLICATION COMPLICATIONS MANAGEMENT OF A FIXED FOOTPLATE IN CHRONIC OTITIS MEDIA BENOIT GRATACAP, MD, ROBERT VINCENT, MD, JEAN-BERNARD CAUSSE, MD From the Jean Causse Clinic, Colombiers,
AUDITORY APPARATUS. Mr. P Mazengenya. Tel 72204
 AUDITORY APPARATUS Mr. P Mazengenya Tel 72204 Describe the anatomical features of the external ear Describe the tympanic membrane (ear drum) Describe the walls of the middle ear Outline the structures
AUDITORY APPARATUS Mr. P Mazengenya Tel 72204 Describe the anatomical features of the external ear Describe the tympanic membrane (ear drum) Describe the walls of the middle ear Outline the structures
Cholesteatoma-Pathogenesis and Surgical Management. Grand Rounds Presentation February 24, 1999 Kyle Kennedy, M.D. Jeffrey Vrabec,, M.D.
 Cholesteatoma-Pathogenesis and Surgical Management Grand Rounds Presentation February 24, 1999 Kyle Kennedy, M.D. Jeffrey Vrabec,, M.D. Introduction Cholesteatoma (keratoma)-essentially an accumulation
Cholesteatoma-Pathogenesis and Surgical Management Grand Rounds Presentation February 24, 1999 Kyle Kennedy, M.D. Jeffrey Vrabec,, M.D. Introduction Cholesteatoma (keratoma)-essentially an accumulation
Original Research Article
 COMPARATIVE STUDY OF PALISADE CARTILAGE TYMPANOPLASTY WITH TEMPORALIS FASCIA TYMPANOPLASTY IN CSOM WITH SUBTOTAL PERFORATIONS Sathish Kumar K. N 1, M. K. Veenapani 2, Swathi V. M 3 1Assistant Professor,
COMPARATIVE STUDY OF PALISADE CARTILAGE TYMPANOPLASTY WITH TEMPORALIS FASCIA TYMPANOPLASTY IN CSOM WITH SUBTOTAL PERFORATIONS Sathish Kumar K. N 1, M. K. Veenapani 2, Swathi V. M 3 1Assistant Professor,
STAPEDECTOMY Surgical Management. Bruce Black MD
 STAPEDECTOMY Surgical Management Bruce Black MD Small fenestrum stapedotomy with a teflon-wire prosthesis. Stapedectomy surgery is done under operating microscopy. Local anaesthesia is commonly used but
STAPEDECTOMY Surgical Management Bruce Black MD Small fenestrum stapedotomy with a teflon-wire prosthesis. Stapedectomy surgery is done under operating microscopy. Local anaesthesia is commonly used but
The Outcome of Shield Graft Tympanoplasty: A Single Center Descriptive Study at KAMC
 ISSN: 2250-0359 VOLUME 4 ISSUE 2 2014 The Outcome of Shield Graft Tympanoplasty: A Single Center Descriptive Study at KAMC Mohamed Sa ad Eldin Aly, MD 1, Malak Jamal Gazzaz, MBBS 2, Doaa Abdelmoety, MD
ISSN: 2250-0359 VOLUME 4 ISSUE 2 2014 The Outcome of Shield Graft Tympanoplasty: A Single Center Descriptive Study at KAMC Mohamed Sa ad Eldin Aly, MD 1, Malak Jamal Gazzaz, MBBS 2, Doaa Abdelmoety, MD
The Ear. Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology
 The Ear Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology The Ear The ear consists of the external ear; the middle ear (tympanic cavity); and the internal ear (labyrinth), which contains
The Ear Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology The Ear The ear consists of the external ear; the middle ear (tympanic cavity); and the internal ear (labyrinth), which contains
The Ear The ear consists of : 1-THE EXTERNAL EAR 2-THE MIDDLE EAR, OR TYMPANIC CAVITY 3-THE INTERNAL EAR, OR LABYRINTH 1-THE EXTERNAL EAR.
 The Ear The ear consists of : 1-THE EXTERNAL EAR 2-THE MIDDLE EAR, OR TYMPANIC CAVITY 3-THE INTERNAL EAR, OR LABYRINTH 1-THE EXTERNAL EAR Made of A-AURICLE B-EXTERNAL AUDITORY MEATUS A-AURICLE It consists
The Ear The ear consists of : 1-THE EXTERNAL EAR 2-THE MIDDLE EAR, OR TYMPANIC CAVITY 3-THE INTERNAL EAR, OR LABYRINTH 1-THE EXTERNAL EAR Made of A-AURICLE B-EXTERNAL AUDITORY MEATUS A-AURICLE It consists
CHOLESTEATOMA I DO IT?? TYMPANOPLASTY. Mohamed BADR-EL-DINE, M.D.
 CHOLESTEATOMA HOW AND I DO IT?? TYMPANOPLASTY Mohamed BADR-EL-DINE, M.D. Otologie et Neurotologie; Service d Otorhinolaryngologie Université d Alexandrie - EGYPTE. Panelists: Prof. Aziz Belal Prof. Douglas
CHOLESTEATOMA HOW AND I DO IT?? TYMPANOPLASTY Mohamed BADR-EL-DINE, M.D. Otologie et Neurotologie; Service d Otorhinolaryngologie Université d Alexandrie - EGYPTE. Panelists: Prof. Aziz Belal Prof. Douglas
Bruce Black MD EAC TRAUMA
 EAC TRAUMA Bruising in the deep canal due to cotton bud/q-tip selfcleaning attempts. No action required. A granuloma of the deep Lt. EAC. Superficial trauma has become secondarily infected. Clean thoroughly,
EAC TRAUMA Bruising in the deep canal due to cotton bud/q-tip selfcleaning attempts. No action required. A granuloma of the deep Lt. EAC. Superficial trauma has become secondarily infected. Clean thoroughly,
1. Axial view, left temporal bone. Plane through the upper antrum (A), superior semicircular canal (SSC) and IAC.
, superior semicircular canal (SSC) and IAC.") PA IAC SSC A 1. Axial view, left temporal bone. Plane through the upper antrum (A), superior semicircular canal (SSC) and IAC. IAC VII M I LSC Plane through the IAC, malleus head and incus and the lateral
PA IAC SSC A 1. Axial view, left temporal bone. Plane through the upper antrum (A), superior semicircular canal (SSC) and IAC. IAC VII M I LSC Plane through the IAC, malleus head and incus and the lateral
The Zone-Based Approach for Selection of Tympanoplasty Technique
 12 The Zone-Based Approach for Selection of Tympanoplasty Technique 1 Otolaryngol Pol 2012; 66 (1): 12-19 SUMMARY panoplastyk /Received: 04.11.2011 /Accepted: 24.11.2011 1 Associate Professor of Otolaryngology
12 The Zone-Based Approach for Selection of Tympanoplasty Technique 1 Otolaryngol Pol 2012; 66 (1): 12-19 SUMMARY panoplastyk /Received: 04.11.2011 /Accepted: 24.11.2011 1 Associate Professor of Otolaryngology
The ear: some applied basic science
 Chapter 1 The ear: some applied basic science The pinna The external ear or pinna is composed of cartilage with closely adherent perichondrium and skin. It is developed from six tubercles of the first
Chapter 1 The ear: some applied basic science The pinna The external ear or pinna is composed of cartilage with closely adherent perichondrium and skin. It is developed from six tubercles of the first
Surgery for Congenital Ear Malformations
 21 Surgery for Congenital Ear Malformations Robert A. Jahrsdoerfer and Bradley W. Kesser Classification Congenital malformations of the ear can be broadly classified into two categories: Minor malformations
21 Surgery for Congenital Ear Malformations Robert A. Jahrsdoerfer and Bradley W. Kesser Classification Congenital malformations of the ear can be broadly classified into two categories: Minor malformations
Surgery performed for Chronic Otitis Media at Chris Hani Baragwanath Academic Hospital: an 18- month retrospective clinical audit
 Surgery performed for Chronic Otitis Media at Chris Hani Baragwanath Academic Hospital: an 18- month retrospective clinical audit Candidate: Dr Wynand Joubert Student No: 0617912K Supervisor: Adjunct Professor
Surgery performed for Chronic Otitis Media at Chris Hani Baragwanath Academic Hospital: an 18- month retrospective clinical audit Candidate: Dr Wynand Joubert Student No: 0617912K Supervisor: Adjunct Professor
MIDDLE EAR SURGERY. For Better Health and Hearing
 MIDDLE EAR SURGERY For Better Health and Hearing Help for Ongoing Ear Problems Your doctor has found a problem with your middle ear. This is a part of the ear that you can t see. You may have taken medication,
MIDDLE EAR SURGERY For Better Health and Hearing Help for Ongoing Ear Problems Your doctor has found a problem with your middle ear. This is a part of the ear that you can t see. You may have taken medication,
Research Article Inferior Flap Tympanoplasty: A Novel Technique for Anterior Perforation Closure
 BioMed Research International Volume 2013, Article ID 758598, 4 pages http://dx.doi.org/10.1155/2013/758598 Research Article Inferior Flap Tympanoplasty: A Novel Technique for Anterior Perforation Closure
BioMed Research International Volume 2013, Article ID 758598, 4 pages http://dx.doi.org/10.1155/2013/758598 Research Article Inferior Flap Tympanoplasty: A Novel Technique for Anterior Perforation Closure
General overview and history
 TYMPANOPLASTY (TPL) 3 3.1 General overview and history According to the definition established in 1965 by the American Academy of Ophtalmology and Otolaryngology, Subcommittee on Conservation of Hearing,
TYMPANOPLASTY (TPL) 3 3.1 General overview and history According to the definition established in 1965 by the American Academy of Ophtalmology and Otolaryngology, Subcommittee on Conservation of Hearing,
Myringoplasty in Simple Chronic Otitis Media: Critical Analysis of Long-Term Results in a 1,000-Adult Patient Series
 Otology & Neurotology 33:48Y53 Ó 2011, Otology & Neurotology, Inc. Myringoplasty in Simple Chronic Otitis Media: Critical Analysis of Long-Term Results in a 1,000-Adult Patient Series *Massimiliano Nardone,
Otology & Neurotology 33:48Y53 Ó 2011, Otology & Neurotology, Inc. Myringoplasty in Simple Chronic Otitis Media: Critical Analysis of Long-Term Results in a 1,000-Adult Patient Series *Massimiliano Nardone,
Introduction. Pediatric tympanoplasty: Decision making and technical aspects. pediatric CHL. specific entities 4/11/2013. Blake C.
 Pediatric tympanoplasty: Decision making and technical aspects Blake C. Papsin Introduction pediatric CHL incidence /impact specific entities tympanoplasty ossiculoplasty 1 Tympanoplasty most common otologic
Pediatric tympanoplasty: Decision making and technical aspects Blake C. Papsin Introduction pediatric CHL incidence /impact specific entities tympanoplasty ossiculoplasty 1 Tympanoplasty most common otologic
Endoscope assisted myringoplasty
 ISSN 2250-0359 VOLUME 2 SUPPLEMENT 1 2012 Endoscope assisted myringoplasty Balasubramanian Thiagarajan 1 Venkatesan Ulaganathan 2 1 Stanley Medical College 2 Meenakshi Medical College Abstract: Myringoplasty
ISSN 2250-0359 VOLUME 2 SUPPLEMENT 1 2012 Endoscope assisted myringoplasty Balasubramanian Thiagarajan 1 Venkatesan Ulaganathan 2 1 Stanley Medical College 2 Meenakshi Medical College Abstract: Myringoplasty
Outcome of intact canal wall mastoidectomy for limited attic cholesteatoma
 International Journal of Otorhinolaryngology and Head and Neck Surgery Reddy R. Int J Otorhinolaryngol Head Neck Surg. 2017 Jul;3(3):596-600 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937 Original
International Journal of Otorhinolaryngology and Head and Neck Surgery Reddy R. Int J Otorhinolaryngol Head Neck Surg. 2017 Jul;3(3):596-600 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937 Original
Results of single stage ossicular reconstruction by incus transposition in patients with chronic otitis media
 Original Article Results of single stage ossicular reconstruction by incus transposition in patients with chronic otitis media Masoud Naderpour, 1 Yalda Jabbari-Moghaddam, 1 Reza Radfar, 2 Sina Zarrintan,
Original Article Results of single stage ossicular reconstruction by incus transposition in patients with chronic otitis media Masoud Naderpour, 1 Yalda Jabbari-Moghaddam, 1 Reza Radfar, 2 Sina Zarrintan,
CHAPTER 9. MIDDLE EAR SURGERY
 CHAPTER 9. MIDDLE EAR SURGERY 1. OTOSCLEROSIS has no other clinical implications other than its effect on hearing Otosclerosis is an aberrant proliferation of immature bone that develops on the footplate
CHAPTER 9. MIDDLE EAR SURGERY 1. OTOSCLEROSIS has no other clinical implications other than its effect on hearing Otosclerosis is an aberrant proliferation of immature bone that develops on the footplate
Anatomy of the ear: Lymphatics
 Anatomy of the ear: 1. External ear which consist of auricle and external auditory canal. The auricle has a framework of cartilage except the lobule, the skin is closely adherent to perichonderium at the
Anatomy of the ear: 1. External ear which consist of auricle and external auditory canal. The auricle has a framework of cartilage except the lobule, the skin is closely adherent to perichonderium at the
Comparison of visualization of the middle ear by microscope and endoscopes of 30 and 45 through posterior tympanotomy
 Case report Videosurgery Comparison of visualization of the middle ear by microscope and endoscopes of 30 and 45 through posterior tympanotomy Emilia B. Karchier, Kazimierz Niemczyk, Adam Orłowski Department
Case report Videosurgery Comparison of visualization of the middle ear by microscope and endoscopes of 30 and 45 through posterior tympanotomy Emilia B. Karchier, Kazimierz Niemczyk, Adam Orłowski Department
Mastoid cavities CAUSES OF FAILURE?
 Management of troublesome mastoid cavities J. Magnan, Université de la Mediterranée Marseille, France ALEXANDRIA 2009 Mastoid cavities CAUSES OF FAILURE? Facial bridge Pneumatisation Skin Mucosa Meatoplasty
Management of troublesome mastoid cavities J. Magnan, Université de la Mediterranée Marseille, France ALEXANDRIA 2009 Mastoid cavities CAUSES OF FAILURE? Facial bridge Pneumatisation Skin Mucosa Meatoplasty
EXPERIENCE WITH OVERLAY TYMPANOPLASTY IN 83 CHINESE PATIENTS
 JOURNAL OF OTOLOGY EXPERIENCE WITH OVERLAY TYMPANOPLASTY IN 83 CHINESE PATIENTS PENG Bengang, MIAO Xutao, WANG Xin, ZHU Sixiang, SUN Yiqing Abstract Background In many European and American hospitals,
JOURNAL OF OTOLOGY EXPERIENCE WITH OVERLAY TYMPANOPLASTY IN 83 CHINESE PATIENTS PENG Bengang, MIAO Xutao, WANG Xin, ZHU Sixiang, SUN Yiqing Abstract Background In many European and American hospitals,
Anatomy and Physiology of Hearing
 Anatomy and Physiology of Hearing The Human Ear Temporal Bone Found on each side of the skull and contains the organs for hearing and balance Divided into four major portions: - squamous - mastoid - tympanic
Anatomy and Physiology of Hearing The Human Ear Temporal Bone Found on each side of the skull and contains the organs for hearing and balance Divided into four major portions: - squamous - mastoid - tympanic
Surgery for Conductive Hearing Loss
 THE NEW YORK OTOLARYNGOLOGY GROUP, P.C. The Ear, Nose and Throat Specialists Neil M. Sperling, M.D. Otology/Neuro-Otology Diseases of the Ear Facial Nerve Balance Disorders Surgery for Conductive Hearing
THE NEW YORK OTOLARYNGOLOGY GROUP, P.C. The Ear, Nose and Throat Specialists Neil M. Sperling, M.D. Otology/Neuro-Otology Diseases of the Ear Facial Nerve Balance Disorders Surgery for Conductive Hearing
Sohil Vadiya, Vibhuti Parikh, Saumya Shah, Parita Pandya, and Anuj Kansara
 Scientifica Volume 2016, Article ID 8092328, 4 pages http://dx.doi.org/10.1155/2016/8092328 Research Article Comparison of Modified Cartilage Shield Tympanoplasty with Tympanoplasty Using Temporalis Fascia
Scientifica Volume 2016, Article ID 8092328, 4 pages http://dx.doi.org/10.1155/2016/8092328 Research Article Comparison of Modified Cartilage Shield Tympanoplasty with Tympanoplasty Using Temporalis Fascia
ICW MASTOIDECTOMY Attic Wall Defect Repair Past techniques. Bruce Black MD
 ICW MASTOIDECTOMY Attic Wall Defect Repair Past techniques EAC WALL REPAIRS Surgical Variants, Difficulties Onlay Inlay Occlusion of EAC Prone to under-flanking recurrence Unstable Prone to out-flanking
ICW MASTOIDECTOMY Attic Wall Defect Repair Past techniques EAC WALL REPAIRS Surgical Variants, Difficulties Onlay Inlay Occlusion of EAC Prone to under-flanking recurrence Unstable Prone to out-flanking
Hearing is one of the most important special senses
 Comparative Study of Autologous Ossicular Graft versus Titanium Prosthesis (TORP & PORP) in Ossiculoplasty P Thamizharasan, 1 K Ravi 1 ABSTRACT Introduction This prospective cohort study aims to analyze
Comparative Study of Autologous Ossicular Graft versus Titanium Prosthesis (TORP & PORP) in Ossiculoplasty P Thamizharasan, 1 K Ravi 1 ABSTRACT Introduction This prospective cohort study aims to analyze
Index. Index. Note: page numbers in italics refer to figures and tables
 383 Note: page numbers in italics refer to figures and tables A air bone gap closure 115, 116 atretic ear surgery 148 FTT 118, 120 incus interposition 116, 117 replacement with stapedotomy 274 incus-stapedotomy
383 Note: page numbers in italics refer to figures and tables A air bone gap closure 115, 116 atretic ear surgery 148 FTT 118, 120 incus interposition 116, 117 replacement with stapedotomy 274 incus-stapedotomy
OPEN CAVITY / CANAL WALL DOWN MASTOIDECTOMY. Bruce Black MD
 OPEN CAVITY / CANAL WALL DOWN MASTOIDECTOMY Plan of an open cavity (CWD: canal wall down surgery). The middle ear is essentially gutted/amputated to eliminate cholesteatoma. Plan of classic CWD (radical
OPEN CAVITY / CANAL WALL DOWN MASTOIDECTOMY Plan of an open cavity (CWD: canal wall down surgery). The middle ear is essentially gutted/amputated to eliminate cholesteatoma. Plan of classic CWD (radical
ANTERIOR TUCKING VS CARTILAGE SUPPORT TYMPANOPLASTY
 ANTERIOR TUCKING VS CARTILAGE SUPPORT TYMPANOPLASTY K S Burse*, S. V. Kulkarni**, C. C. Bharadwaj***, S. Shaikh****, G. S. Roy***** ABSTRACT Objectives: To compare and analyze two methods of tympanoplasty
ANTERIOR TUCKING VS CARTILAGE SUPPORT TYMPANOPLASTY K S Burse*, S. V. Kulkarni**, C. C. Bharadwaj***, S. Shaikh****, G. S. Roy***** ABSTRACT Objectives: To compare and analyze two methods of tympanoplasty
Tympanoplasty June 1999
 TITLE: Tympanoplasty SOURCE: Grand Rounds Presentation, The University of Texas Medical Branch in Galveston, Department of Otolaryngology DATE: June 9, 1999 RESIDENT PHYSICIAN: Kevin Katzenmeyer, MD FACULTY
TITLE: Tympanoplasty SOURCE: Grand Rounds Presentation, The University of Texas Medical Branch in Galveston, Department of Otolaryngology DATE: June 9, 1999 RESIDENT PHYSICIAN: Kevin Katzenmeyer, MD FACULTY
Gross Anatomy of the. TEMPORAL BONE, EXTERNAL EAR, and MIDDLE EAR
 Gross Anatomy of the TEMPORAL BONE, EXTERNAL EAR, and MIDDLE EAR M1 Gross and Developmental Anatomy 9:00 AM, December 11, 2008 Dr. Milton M. Sholley Professor of Anatomy and Neurobiology Assignment: Head
Gross Anatomy of the TEMPORAL BONE, EXTERNAL EAR, and MIDDLE EAR M1 Gross and Developmental Anatomy 9:00 AM, December 11, 2008 Dr. Milton M. Sholley Professor of Anatomy and Neurobiology Assignment: Head
Original Article Factors affecting surgical outcome of myringoplasty
 Bangladesh J Otorhinolaryngol 2011; 17(2): 82-87 Original Article Factors affecting surgical outcome of myringoplasty Md. Zakaria Sarker 1, Mesbauddin Ahmed 2, Khabiruddin Patwary 3, Rabiul Islam 4, Abul
Bangladesh J Otorhinolaryngol 2011; 17(2): 82-87 Original Article Factors affecting surgical outcome of myringoplasty Md. Zakaria Sarker 1, Mesbauddin Ahmed 2, Khabiruddin Patwary 3, Rabiul Islam 4, Abul
Anatomy of External and Middle ear. Dr Sai Manohar
 Anatomy of External and Middle ear. Dr Sai Manohar 1 Human Ear For Anatomical description, Ear is divided into Auricle (or pinna) The external auditory canal The Middle Ear and its derivatives The Inner
Anatomy of External and Middle ear. Dr Sai Manohar 1 Human Ear For Anatomical description, Ear is divided into Auricle (or pinna) The external auditory canal The Middle Ear and its derivatives The Inner
ORIGINAL ARTICLE. The Yung Percutaneous Mastoid Vent. middleearcanleadtovariouspathologicconditions,
 The Yung Percutaneous Mastoid Vent A Medium-Term Follow-up Study Matthew Man-Wah Yung, PhD, FRCS, DLO ORIGINAL ARTICLE Background: I designed a percutaneous mastoid vent to provide permanent ventilation
The Yung Percutaneous Mastoid Vent A Medium-Term Follow-up Study Matthew Man-Wah Yung, PhD, FRCS, DLO ORIGINAL ARTICLE Background: I designed a percutaneous mastoid vent to provide permanent ventilation
Middle Ear Surgery: Pointers and Pitfalls
 Archives of Otolaryngology & Rhinology Lee K J* Department of Otolaryngology, North Shore-LIJ- Hofstra School of Medicine, Yale University, USA Dates: Received: 28 April, 2015; Accepted: 12 May, 2015;
Archives of Otolaryngology & Rhinology Lee K J* Department of Otolaryngology, North Shore-LIJ- Hofstra School of Medicine, Yale University, USA Dates: Received: 28 April, 2015; Accepted: 12 May, 2015;
Lateral Tympanoplasty for Total or Near-Total Perforation: Prognostic Factors
 The Laryngoscope Lippincott Williams & Wilkins, Inc. 2006 The American Laryngological, Rhinological and Otological Society, Inc. Lateral Tympanoplasty for Total or Near-Total Perforation: Prognostic Factors
The Laryngoscope Lippincott Williams & Wilkins, Inc. 2006 The American Laryngological, Rhinological and Otological Society, Inc. Lateral Tympanoplasty for Total or Near-Total Perforation: Prognostic Factors
Medialization of Total Ossicular Replacement Prosthesis in Mastoid Obliteration
 Int. Adv. Otol. 2013; 9:(1) 110-114 CLINICAL STUDY Medialization of Total Ossicular Replacement Prosthesis in Mastoid Obliteration Ali Sanei-Moghaddam, Sanjiv Kumar, Neil Donnelly, Patrick Axon ENT, Medway
Int. Adv. Otol. 2013; 9:(1) 110-114 CLINICAL STUDY Medialization of Total Ossicular Replacement Prosthesis in Mastoid Obliteration Ali Sanei-Moghaddam, Sanjiv Kumar, Neil Donnelly, Patrick Axon ENT, Medway
Incus Footplate Assembly: Indication and Surgical Outcome
 The Laryngoscope VC 2016 The American Laryngological, Rhinological and Otological Society, Inc. Incus Footplate Assembly: Indication and Surgical Outcome Mina Park, MD; Sungjun Han, MD; Byung Yoon Choi,
The Laryngoscope VC 2016 The American Laryngological, Rhinological and Otological Society, Inc. Incus Footplate Assembly: Indication and Surgical Outcome Mina Park, MD; Sungjun Han, MD; Byung Yoon Choi,
Chronic Ear Disease. Daekeun Joo Resident Lecture Series 11/18/09
 Chronic Ear Disease Daekeun Joo Resident Lecture Series 11/18/09 ETD URIs Viral-induced damage to ET lining resulting in decreased mucociliary clearance Viral invasion of ME mucosa results in inflamm Reflux
Chronic Ear Disease Daekeun Joo Resident Lecture Series 11/18/09 ETD URIs Viral-induced damage to ET lining resulting in decreased mucociliary clearance Viral invasion of ME mucosa results in inflamm Reflux
Cartilage Tympanoplasty for Management of TM Perforation: A Comparison with the Temporalis Fascia Graft Technique
 World Articles of Ear, Nose and Throat ---------------------Page 1 Cartilage Tympanoplasty for Management of TM Perforation: A Comparison with the Temporalis Fascia Graft Technique Authors: Dr Sudhakar
World Articles of Ear, Nose and Throat ---------------------Page 1 Cartilage Tympanoplasty for Management of TM Perforation: A Comparison with the Temporalis Fascia Graft Technique Authors: Dr Sudhakar
Introduction. Types of Cholesteatoma
 TITLE: Cholesteatoma SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: January 25, 2006 RESIDENT PHYSICIAN: Garrett Hauptman, MD FACULTY PHYSICIAN: Tomoko Makishima, MD, PhD SERIES
TITLE: Cholesteatoma SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: January 25, 2006 RESIDENT PHYSICIAN: Garrett Hauptman, MD FACULTY PHYSICIAN: Tomoko Makishima, MD, PhD SERIES
The Value of Computed Tomography Scanning in Assessment of Aditus ad Antrum Patency and Choice of Treatment Line in Revision Myringoplasty
 Med. J. Cairo Univ., Vol. 77, No. 2, September: 53-57, 2009 www.medicaljournalofcairouniversity.com The Value of Computed Tomography Scanning in Assessment of Aditus ad Antrum Patency and Choice of Treatment
Med. J. Cairo Univ., Vol. 77, No. 2, September: 53-57, 2009 www.medicaljournalofcairouniversity.com The Value of Computed Tomography Scanning in Assessment of Aditus ad Antrum Patency and Choice of Treatment
ORIGINAL ARTICLE. A New Staging System for Tympano-mastoid Cholesteatoma. Aziz Belal, Mahmoud Reda, Ahmed Mehana, Yousef Belal
 Int. Adv. Otol. 2012; 8:(1) 63-68 ORIGINAL ARTICLE A New Staging System for Tympano-mastoid Cholesteatoma Aziz Belal, Mahmoud Reda, Ahmed Mehana, Yousef Belal Alexandria Ear Hospital Alexandria Egypt (AB,
Int. Adv. Otol. 2012; 8:(1) 63-68 ORIGINAL ARTICLE A New Staging System for Tympano-mastoid Cholesteatoma Aziz Belal, Mahmoud Reda, Ahmed Mehana, Yousef Belal Alexandria Ear Hospital Alexandria Egypt (AB,
ORIGINAL ARTICLE ABSTRACT INTRODUCTION
 Synchronous Ossiculoplasty with Ossicular Replacement Prosthesis during 10.5005/jp-journals-10003-1204 Canal Wall Down Mastoidectomy ORIGINAL ARTICLE Synchronous Ossiculoplasty with Ossicular Replacement
Synchronous Ossiculoplasty with Ossicular Replacement Prosthesis during 10.5005/jp-journals-10003-1204 Canal Wall Down Mastoidectomy ORIGINAL ARTICLE Synchronous Ossiculoplasty with Ossicular Replacement
A Working Classification of Retraction for the Whole Tympanic Membrane
 International Journal of Otolaryngology and Head & Neck Surgery, 2013, 2, 143-147 http://dx.doi.org/10.4236/ijohns.2013.24031 Published Online July 2013 (http://www.scirp.org/journal/ijohns) A Working
International Journal of Otolaryngology and Head & Neck Surgery, 2013, 2, 143-147 http://dx.doi.org/10.4236/ijohns.2013.24031 Published Online July 2013 (http://www.scirp.org/journal/ijohns) A Working
Audiological outcome of tympanoplasties a single center experience
 Original article Audiological outcome of tympanoplasties a single center experience Selma Hodžić-Redžić*, Lana Kovač-Bilić, Srećko Branica Department of Ear, Nose and Throat and Head and Neck Surgery,
Original article Audiological outcome of tympanoplasties a single center experience Selma Hodžić-Redžić*, Lana Kovač-Bilić, Srećko Branica Department of Ear, Nose and Throat and Head and Neck Surgery,
Selective Epitympanic Dysventilation Syndrome
 The Laryngoscope VC 2010 The American Laryngological, Rhinological and Otological Society, Inc. Selective Epitympanic Dysventilation Syndrome Daniele Marchioni, MD; Matteo Alicandri-Ciufelli, MD; Gabriele
The Laryngoscope VC 2010 The American Laryngological, Rhinological and Otological Society, Inc. Selective Epitympanic Dysventilation Syndrome Daniele Marchioni, MD; Matteo Alicandri-Ciufelli, MD; Gabriele
Surgery of Sinus Tympani Cholesteatoma: Endoscopic Necessity*
 Int. Adv. Otol. 2009; 5:(2) 158-165 ORIGINAL ARTICLE Surgery of Sinus Tympani Cholesteatoma: Endoscopic Necessity* Mohamed M.K. Badr-El-Dine Department of Otorhinolaryngology, Alexandria School of Medicine
Int. Adv. Otol. 2009; 5:(2) 158-165 ORIGINAL ARTICLE Surgery of Sinus Tympani Cholesteatoma: Endoscopic Necessity* Mohamed M.K. Badr-El-Dine Department of Otorhinolaryngology, Alexandria School of Medicine
The Vibrant Soundbridge
 REVIEW RTICLE IJOC Emeritus Professor, Padmashree Dr DY Patil Medical College, Honorary Consultant, Lilavati Hospital and Medical Research Center, Mumbai, Maharashtra, India Correspondence:, Om partments,
REVIEW RTICLE IJOC Emeritus Professor, Padmashree Dr DY Patil Medical College, Honorary Consultant, Lilavati Hospital and Medical Research Center, Mumbai, Maharashtra, India Correspondence:, Om partments,
(FIG.1) Landmarks of the external ear in dogs. (FIG.2) Anatomy of the ear.
 Landmarks of the external ear in dogs. (FIG.2) Anatomy of the ear.") SURGICAL ANATOMY of Ear (FIG.1) Landmarks of the external ear in dogs. (FIG.2) Anatomy of the ear. An aural (auricular) hematoma is a collection of blood within the cartilage plate of the ear. Suture placement
SURGICAL ANATOMY of Ear (FIG.1) Landmarks of the external ear in dogs. (FIG.2) Anatomy of the ear. An aural (auricular) hematoma is a collection of blood within the cartilage plate of the ear. Suture placement
Narrowest segment of the ear canal. Limited microscopic. Wide endoscopic. field of view. field of view
 Endoscopic Transcanal Management of Cholesteatoma M. Tarabichi American Hospital-Dubai The Endoscope in Otology Mostly for documentation. Mostly diagnostic. Exploration of old mastoid cavities Endoscopic
Endoscopic Transcanal Management of Cholesteatoma M. Tarabichi American Hospital-Dubai The Endoscope in Otology Mostly for documentation. Mostly diagnostic. Exploration of old mastoid cavities Endoscopic
Gross Anatomy of the. TEMPORAL BONE, EXTERNAL EAR, and MIDDLE EAR. Assignment: Head to Toe Temporomandibular Joint (TMJ)
") Gross Anatomy the TEMPORAL BONE, EXTERNAL EAR, and MIDDLE EAR M1 Gross and Developmental Anatomy 9:00 AM, December 11, 2008 Dr. Milton M. Sholley Pressor Anatomy and Neurobiology Assignment: Head to Toe
Gross Anatomy the TEMPORAL BONE, EXTERNAL EAR, and MIDDLE EAR M1 Gross and Developmental Anatomy 9:00 AM, December 11, 2008 Dr. Milton M. Sholley Pressor Anatomy and Neurobiology Assignment: Head to Toe
Bilateral same day type I tympanoplasty is not. Simultaneous Bilateral Type I Tympanoplasty as a Day Care Procedure.
 Our Experience Simultaneous Bilateral Type I Tympanoplasty as a Day Care Procedure Abhishek Vijay Sahu, 1 Dhrubajyoti Datta, 1 Jeumon Talukdar, 1 Narendranath Dutta 1 ABSTRACT Introduction: Bilateral same
Our Experience Simultaneous Bilateral Type I Tympanoplasty as a Day Care Procedure Abhishek Vijay Sahu, 1 Dhrubajyoti Datta, 1 Jeumon Talukdar, 1 Narendranath Dutta 1 ABSTRACT Introduction: Bilateral same
Tympanoplasty conchal cavum approach
 Man and Nunez Journal of Otolaryngology - Head and Neck Surgery (2016) 45:1 DOI 10.1186/s40463-015-0113-3 HOW I DO IT ARTICLE Open Access Tympanoplasty conchal cavum approach S. Christopher Man 1* and
Man and Nunez Journal of Otolaryngology - Head and Neck Surgery (2016) 45:1 DOI 10.1186/s40463-015-0113-3 HOW I DO IT ARTICLE Open Access Tympanoplasty conchal cavum approach S. Christopher Man 1* and
No conflicts of interest were identified by the planning committee, faculty, authors and reviewers for this program.
 Disclosure: Is that a Hole? Evaluation and Treatment of TM Perforations Kristi McGowin, MSN, CPNP Children s Mercy Hospital Kansas City, MO No conflicts of interest were identified by the planning committee,
Disclosure: Is that a Hole? Evaluation and Treatment of TM Perforations Kristi McGowin, MSN, CPNP Children s Mercy Hospital Kansas City, MO No conflicts of interest were identified by the planning committee,
Tympanoplasty January 2003
 TITLE: Tympanoplasty SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: January 15, 2003 RESIDENT PHYSICIAN: Christopher Muller, M.D. FACULTY PHYSICIAN: Arun Gadre, M.D. SERIES EDITORS:
TITLE: Tympanoplasty SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: January 15, 2003 RESIDENT PHYSICIAN: Christopher Muller, M.D. FACULTY PHYSICIAN: Arun Gadre, M.D. SERIES EDITORS:
Shashikant K. Mhashal*, Neeraj R. Shetty, Amit S. Rathi, Vinod A. Gite
 International Journal of Otorhinolaryngology and Head and Neck Surgery Mhashal SK et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):821-825 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937
International Journal of Otorhinolaryngology and Head and Neck Surgery Mhashal SK et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):821-825 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Year 6 ENT SMC Otitis Media (Dr.
 Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Year 6 ENT SMC Otitis Media (Dr. Jalal Almarzooq) - Anatomy of the ear: The ear is divided into 3 parts: External ear.
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Year 6 ENT SMC Otitis Media (Dr. Jalal Almarzooq) - Anatomy of the ear: The ear is divided into 3 parts: External ear.
Middle ear CT imaging: Review of anatomy and common pathology
 Middle ear CT imaging: Review of anatomy and common pathology Poster No.: C-0665 Congress: ECR 2017 Type: Educational Exhibit Authors: M. R. Campos Arenas, M. C. Sánchez-Porro, J. Garrido Rull ; 1 1 2
Middle ear CT imaging: Review of anatomy and common pathology Poster No.: C-0665 Congress: ECR 2017 Type: Educational Exhibit Authors: M. R. Campos Arenas, M. C. Sánchez-Porro, J. Garrido Rull ; 1 1 2
Congenital aural atresia surgery: Transmastoid approach, complications and outcomes
 DOI 10.1007/s00405-011-1785-6 OTOLOGY Congenital aural atresia surgery: Transmastoid approach, complications and outcomes Faramarz Memari Marjan Mirsalehi Ali Jalali Received: 29 March 2011 / Accepted:
DOI 10.1007/s00405-011-1785-6 OTOLOGY Congenital aural atresia surgery: Transmastoid approach, complications and outcomes Faramarz Memari Marjan Mirsalehi Ali Jalali Received: 29 March 2011 / Accepted:
Clinical analysis of secondary acquired cholesteatoma.
 Research Article Clinical analysis of secondary acquired cholesteatoma. http://www.alliedacademies.org/archives-of-general-internal-medicine/ ISSN : 2591-7951 Takashi Yamatodani 1 *, Kunihiro Mizuta 2,
Research Article Clinical analysis of secondary acquired cholesteatoma. http://www.alliedacademies.org/archives-of-general-internal-medicine/ ISSN : 2591-7951 Takashi Yamatodani 1 *, Kunihiro Mizuta 2,
Repair of the middle ear
 Repair of the middle ear Information for families Great Ormond Street Hospital for Children NHS Foundation Trust This leaflet explains repair of the middle ear and what to expect when your child comes
Repair of the middle ear Information for families Great Ormond Street Hospital for Children NHS Foundation Trust This leaflet explains repair of the middle ear and what to expect when your child comes
An optical coherence tomography study for imaging the round window niche and the promontorium tympani
 An optical coherence tomography study for imaging the round window niche and the promontorium tympani T. Just *a, E. Lankenau b, G. Hüttmann b, H.W. Pau a a Department of Otorhinolaryngology, University
An optical coherence tomography study for imaging the round window niche and the promontorium tympani T. Just *a, E. Lankenau b, G. Hüttmann b, H.W. Pau a a Department of Otorhinolaryngology, University
Cone Beam CT Atlas of the Normal Suspensory Apparatus of the Middle Ear Ossicles
 Cone Beam CT Atlas of the Normal Suspensory Apparatus of the Middle Ear Ossicles Poster No.: C-2036 Congress: ECR 2013 Type: Authors: Educational Exhibit B. Smet 1, I. De Kock 2, P. Gillardin 2, M. Lemmerling
Cone Beam CT Atlas of the Normal Suspensory Apparatus of the Middle Ear Ossicles Poster No.: C-2036 Congress: ECR 2013 Type: Authors: Educational Exhibit B. Smet 1, I. De Kock 2, P. Gillardin 2, M. Lemmerling
Cochlear Schwannoma Removed Through the External Auditory Canal by a Transcanal Exclusive Endoscopic Technique
 The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. Case Report Cochlear Schwannoma Removed Through the External Auditory Canal by a Transcanal Exclusive Endoscopic
The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. Case Report Cochlear Schwannoma Removed Through the External Auditory Canal by a Transcanal Exclusive Endoscopic
Dr. K. Ravi M.S 1, Dr. S. Kalyan Kumar M.S 2 1 Associate professor, 2 Assistant professor
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 4 Ver. III (April. 2017), PP 40-44 www.iosrjournals.org Management of Chronic Otitis Media
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 4 Ver. III (April. 2017), PP 40-44 www.iosrjournals.org Management of Chronic Otitis Media
RECONSTRUCTION OF POSTERIOR MEATAL AND/OR LATERAL ATTIC WALLS IN CHOLESTEATOMA SURGERY
 -857- RECONSTRUCTION OF POSTERIOR MEATAL AND/OR LATERAL ATTIC WALLS IN CHOLESTEATOMA SURGERY Mohammed Elsayed Elmaghawry, Mohammed Kamal Mobasher,Magdy Mohammed Abd-Elfattah, Adly Ahmed Tantawy,Atef Hamed
-857- RECONSTRUCTION OF POSTERIOR MEATAL AND/OR LATERAL ATTIC WALLS IN CHOLESTEATOMA SURGERY Mohammed Elsayed Elmaghawry, Mohammed Kamal Mobasher,Magdy Mohammed Abd-Elfattah, Adly Ahmed Tantawy,Atef Hamed
Nasal septal perichondrium versus temporalis fascia in transmeatal myringoplasty
 Egyptian Journal of Ear, Nose, Throat and Allied Sciences (2011) 12, 1 6 Egyptian Society of Ear, Nose, Throat and Allied Sciences Egyptian Journal of Ear, Nose, Throat and Allied Sciences www.esentas.org
Egyptian Journal of Ear, Nose, Throat and Allied Sciences (2011) 12, 1 6 Egyptian Society of Ear, Nose, Throat and Allied Sciences Egyptian Journal of Ear, Nose, Throat and Allied Sciences www.esentas.org
Usefulness of a ventilation tube as a partial ossicular replacement prosthesis (PORP) in ossiculoplasty in patients with chronic otitis media
 in ossiculoplasty in patients with chronic otitis media") CLINICAL RESEARCH e-issn 1643-375 DOI: 1.12659/MSM.89447 Received: 214.1.27 Accepted: 214.2.25 Published: 214.6.13 Usefulness of a ventilation tube as a partial ossicular replacement prosthesis (PORP)
CLINICAL RESEARCH e-issn 1643-375 DOI: 1.12659/MSM.89447 Received: 214.1.27 Accepted: 214.2.25 Published: 214.6.13 Usefulness of a ventilation tube as a partial ossicular replacement prosthesis (PORP)
Unit VIII Problem 9 Physiology: Hearing
 Unit VIII Problem 9 Physiology: Hearing - We can hear a limited range of frequency between 20 Hz 20,000 Hz (human hearing acuity is between 1000 Hz 4000 Hz). - The ear is divided into 3 parts. Those are:
Unit VIII Problem 9 Physiology: Hearing - We can hear a limited range of frequency between 20 Hz 20,000 Hz (human hearing acuity is between 1000 Hz 4000 Hz). - The ear is divided into 3 parts. Those are:
Printable version - Hearing - OpenLearn - The Open University
 Skip to content Accessibility Sign in Contact Search the OU The Open University Study at the OU Research at the OU OU Community About the OU Hearing Printable page generated Saturday, 12 November 2011,
Skip to content Accessibility Sign in Contact Search the OU The Open University Study at the OU Research at the OU OU Community About the OU Hearing Printable page generated Saturday, 12 November 2011,
A STUDY OF EFFICIENCY OF AUTOLOGOUS PLATELET RICH PLASMA IN MYRINGOPLASTY
 A STUDY OF EFFICIENCY OF AUTOLOGOUS PLATELET RICH PLASMA IN MYRINGOPLASTY Dissertation submitted to THE TAMIL NADU DR.M.G.R. MEDICAL UNIVERSITY In partial fulfillment of the regulations For the award of
A STUDY OF EFFICIENCY OF AUTOLOGOUS PLATELET RICH PLASMA IN MYRINGOPLASTY Dissertation submitted to THE TAMIL NADU DR.M.G.R. MEDICAL UNIVERSITY In partial fulfillment of the regulations For the award of
The Visible Ear Simulator Dissection Manual.
 The Visible Ear Simulator Dissection Manual. Stereoscopic Tutorialized Version 3.1, August 2017 Peter Trier Mikkelsen, the Alexandra Institute A/S, Aarhus, Denmark Mads Sølvsten Sørensen & Steven Andersen,
The Visible Ear Simulator Dissection Manual. Stereoscopic Tutorialized Version 3.1, August 2017 Peter Trier Mikkelsen, the Alexandra Institute A/S, Aarhus, Denmark Mads Sølvsten Sørensen & Steven Andersen,
Hearing. By Jack & Tori
 Hearing By Jack & Tori 3 Main Components of the Human Ear. Outer Ear. Middle Ear. Inner Ear Outer Ear Pinna: >Visible part of ear and ear canal -Acts as a funnel to direct sound Eardrum: >Airtight membrane
Hearing By Jack & Tori 3 Main Components of the Human Ear. Outer Ear. Middle Ear. Inner Ear Outer Ear Pinna: >Visible part of ear and ear canal -Acts as a funnel to direct sound Eardrum: >Airtight membrane
Original Article. Hearing results after myringoplasty. Kathmandu University Medical Journal (2006), Vol. 4, No. 4, Issue 16,
, Vol. 4, No. 4, Issue 16,") Kathmandu University Medical Journal (2006), Vol. 4, No. 4, Issue 16, 455-459 Hearing results after myringoplasty Original Article Shrestha S 1, Sinha K 2 1 Lecturer, Kathmandu Medical ollege Teaching
Kathmandu University Medical Journal (2006), Vol. 4, No. 4, Issue 16, 455-459 Hearing results after myringoplasty Original Article Shrestha S 1, Sinha K 2 1 Lecturer, Kathmandu Medical ollege Teaching
Finite Element Analysis of the Human Middle Ear and an Application for Clinics for Tympanoplasty (Static and Harmonic Vibration Analysis)
") 2015 American Transactions on Engineering & Applied Sciences. American Transactions on Engineering & Applied Sciences http://tuengr.com/ateas Finite Element Analysis of the Human Middle Ear and an Application
2015 American Transactions on Engineering & Applied Sciences. American Transactions on Engineering & Applied Sciences http://tuengr.com/ateas Finite Element Analysis of the Human Middle Ear and an Application
Tympanoplasty with and without cortical mastoidectomy in CSOM: A comparative study
 Original article: Tympanoplasty with and without cortical in CSOM: A comparative study 1 Dr. Parag V. Doifode, 2 Dr. Sandeep Dabhekar, 3 Dr. S. H. Gawarle 1Assistant Professor, Department of ENT, Government
Original article: Tympanoplasty with and without cortical in CSOM: A comparative study 1 Dr. Parag V. Doifode, 2 Dr. Sandeep Dabhekar, 3 Dr. S. H. Gawarle 1Assistant Professor, Department of ENT, Government
Transcanal Endoscopic Approach to the Sinus Tympani: A Clinical Report
 Otology & Neurotology 30:758Y765 Ó 2009, Otology & Neurotology, Inc. Transcanal Endoscopic Approach to the Sinus Tympani: A Clinical Report Daniele Marchioni, Francesco Mattioli, Matteo Alicandri-Ciufelli,
Otology & Neurotology 30:758Y765 Ó 2009, Otology & Neurotology, Inc. Transcanal Endoscopic Approach to the Sinus Tympani: A Clinical Report Daniele Marchioni, Francesco Mattioli, Matteo Alicandri-Ciufelli,
Feasibility and Advantages of Transcanal Endoscopic Myringoplasty
 Otology & Neurotology 35:e140Ye145 Ó 2014, Otology & Neurotology, Inc. Feasibility and Advantages of Transcanal Endoscopic Myringoplasty Takatoshi Furukawa, Tomoo Watanabe, Tsukasa Ito, Toshinori Kubota,
Otology & Neurotology 35:e140Ye145 Ó 2014, Otology & Neurotology, Inc. Feasibility and Advantages of Transcanal Endoscopic Myringoplasty Takatoshi Furukawa, Tomoo Watanabe, Tsukasa Ito, Toshinori Kubota,
10/15/2013. Disclosures (Dr. Backous) United States Hearing Loss Projections
 United States Hearing Loss Projections") Diagnostic Pearls for Hearing Evaluation: Intersting Cases Disclosures (Dr. Backous) Douglas D. Backous, MD, FACS Medical Director, Swedish Center for Hearing and Skull Base Surgery Seattle, Washington
Diagnostic Pearls for Hearing Evaluation: Intersting Cases Disclosures (Dr. Backous) Douglas D. Backous, MD, FACS Medical Director, Swedish Center for Hearing and Skull Base Surgery Seattle, Washington
Dr. Sami Zaqout Faculty of Medicine IUG
 Auricle External Ear External auditory meatus The Ear Middle Ear (Tympanic Cavity) Auditory ossicles Internal Ear (Labyrinth) Bony labyrinth Membranous labyrinth External Ear Auricle External auditory
Auricle External Ear External auditory meatus The Ear Middle Ear (Tympanic Cavity) Auditory ossicles Internal Ear (Labyrinth) Bony labyrinth Membranous labyrinth External Ear Auricle External auditory
14/08/2010. João Flávio Nogueira Sinus Centro Fortaleza, Ceará IWGEES International Working Group on Endoscopic Ear Surgery SINUS CENTRO
 SINUS CENTRO João Flávio Nogueira Sinus Centro Fortaleza, Ceará IWGEES International Working Group on Endoscopic Ear Surgery 1 2 Nogueira JF Jr, et al. A brief history of otorhinolaryngolgy: otology, laryngology
SINUS CENTRO João Flávio Nogueira Sinus Centro Fortaleza, Ceará IWGEES International Working Group on Endoscopic Ear Surgery 1 2 Nogueira JF Jr, et al. A brief history of otorhinolaryngolgy: otology, laryngology
Anatomy of the Ear Region. External ear Middle ear Internal ear
 Ear Lecture Objectives Make a list of structures making the external, middle, and internal ear. Discuss the features of the external auditory meatus and tympanic membrane. Describe the shape, position,
Ear Lecture Objectives Make a list of structures making the external, middle, and internal ear. Discuss the features of the external auditory meatus and tympanic membrane. Describe the shape, position,
Malleus Neck-Anchoring Malleostapedotomy: Preliminary Results
 Otology & Neurotology 33:1477Y1481 Ó 2012, Otology & Neurotology, Inc. Malleus Neck-Anchoring Malleostapedotomy: Preliminary Results *Mun Young Chang, Jeong Hun Jang, *Jae-Jin Song, *Kyu-Hee Han, * Jun
Otology & Neurotology 33:1477Y1481 Ó 2012, Otology & Neurotology, Inc. Malleus Neck-Anchoring Malleostapedotomy: Preliminary Results *Mun Young Chang, Jeong Hun Jang, *Jae-Jin Song, *Kyu-Hee Han, * Jun
Ossiculoplasty with Sculpted Incus; Hearing Results and Risk Factors
 Journal of Hearing Sciences and Otolaryngology 2016 Winter; 2(1): 1-6 Ossiculoplasty with Sculpted Incus; Hearing Results and Risk Factors Farhad Mokhtarinejad 1, Masoud Motasaddi Zarandy 2, Farzaneh Barzegar
Journal of Hearing Sciences and Otolaryngology 2016 Winter; 2(1): 1-6 Ossiculoplasty with Sculpted Incus; Hearing Results and Risk Factors Farhad Mokhtarinejad 1, Masoud Motasaddi Zarandy 2, Farzaneh Barzegar
MASTOID EXPLORATION (MASTOID SURGERY) AND MASTOIDECTOMY
 AND MASTOIDECTOMY") MASTOID EXPLORATION (MASTOID SURGERY) AND MASTOIDECTOMY This information leaflet is to support your decision with your Specialist. This leaflet will explain about the ear are and what surgery can be offered
MASTOID EXPLORATION (MASTOID SURGERY) AND MASTOIDECTOMY This information leaflet is to support your decision with your Specialist. This leaflet will explain about the ear are and what surgery can be offered