NSAID Use in Post- Myocardial Infarction Patients. Leah Jackson, BScPhm Pharmacy Resident Cardiology Rotation February 28, 2007
|
|
|
- Kristian Hunt
- 6 years ago
- Views:
Transcription
1 NSAID Use in Post- Myocardial Infarction Patients Leah Jackson, BScPhm Pharmacy Resident Cardiology Rotation February 28, 2007
2 Objectives By the end of the presentation, the audience will be able to use the evidence discussed to determine if NSAIDs can safely be used in post-myocardial infarction patients
3 Case Mr. CP 45 y.o. male Smoker PMH: cholecystectomy 1991, HTN (untreated),? cholesterol, sports injury to shoulder several years ago flares up every few months Meds on admisson: Ø Rx, Ø herbals ibuprofen prn shoulder pain (may use for days to weeks every months) Presents to hospital with inferior STEMI angiogram shows diffuse CAD (med tx; Ø PCI)
4 Case Discharge medications include: ASA 81mg daily Clopidogrel 75mg daily x 30d Metoprolol 50mg BID Ramipril 5mg daily Atorvastatin 80mg While doing discharge medication reconciliation, I was reminded of his regular ibuprofen use Considering his diseases and drugs, can Mr. CP safely take ibuprofen as needed?

5 Pharmacotherapeutic question In someone who has had an MI, is it safe to use ibuprofen regularly?
6 Cyclooxygenase Part of prostaglandin synthase enzyme converting arachidonic acid into prostanoids (ie/ prostacyclin, thromboxane A 2 ) COX-1 1 and COX-2 isoforms Inhibition of COX-1 1 linked to antiplatelet effects and GI toxicity Inhibition of COX-2 2 implicated in ameliorating inflammation
7 NSAIDs, Coxibs, and Cardio-Renal Physiology: A Mechanism-Based Evaluation. Medscape Continuing Medical Education (CME) Feb 22, 2002.
8 Cyclooxygenase inhibitors 3 types: Acetylsalicylic acid irreversibly acetylates COX Non-selective COX inhibitors (ie( ie/ indomethacin,, ibuprofen, naproxen) competitively inhibit COX COX-2 2 selective inhibitors (ie( ie/ / coxibs coxibs )
9 Fitzgerald GA and Patrono C. The coxibs, selective inhibitors of cyclooxygenase-2. NEJM 2001;345:
10 NSAIDs Abundant use in many populations To reduce fever, treat pain, reduce inflammation Osteoarthritis, rheumatoid arthritis, dysmenorrhea,, headache, sports injuries, dental pain, etc Easy to acquire (ie( ie/ / OTC ibuprofen)
11 Side effects of NSAIDs Dyspepsia GI ulceration and perforation Nephrotoxicity Worsening hypertension and CHF Cardiovascular toxicity
12 CV toxicity remember Vioxx?? COX-2 2 inhibitors developed and prescribed widely due to their possible decreased risk of GI toxicity/bleeding VIGOR trial comparison of upper GI toxicity of rofecoxib 50mg daily vs naproxen 500mg BID in RA patients; no ASA allowed Less upper GI events with rofecoxib,, but increased rate of MI (RR=4.5) high rate in people at highest risk ie/ / people who should have been on ASA The VIGOR study group. Comparison of Upper Gastrointestinal Toxicity of Rofecoxib and Naproxen in Pateints with Rheumatoid Arthritis. NEJM 2000;343:
13 Vioxx continued Merck s APPROVe trial rofecoxib 25mg daily vs placebo for colonic polyps ASA used if indicated incidence of MI and stroke (RR = 1.92) Bresalier RS et al. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. NEJM 2005;352:
14 Health Canada Report June 2006 CV risks of coxibs Clinical studies indicate long-term use of coxibs CV events (MI, stroke) Limited available evidence suggests CV risk with traditional NSAIDs as well; degree of risk differs among agents Monographs for all NSAIDs should be revised to describe available data or lack of data on CV toxicity Health Products and Food Branch. Marketed Health Products Directorate and Therapeutic Products Directorate. Report on the Cardiovascular Risks Associated with COX-2-Selective NSAIDs.. June 2006.
15 Health Canada Summary Rofecoxib has strong evidence of CV toxicity (ie( ie/ / 3 year APPROVe trial; risk became apparent at 18 months) removed from market September 2004 Valdecoxib (Bextra ) no studies longer than 1 year, however short term use in CABG patients showed increased MI and CVA; reports of serious skin reactions removed from market April 2005 Meloxicam available lack of evidence for CV risk (no studies > 1 year); labelling changes
16 Health Canada Summary Evidence of risk for celecoxib not consistent; data from APC trial (cancer prevention, n=2035) indicates that high doses and long- term use CV risk Remains on market given: CV risks appear to be lower than with rofecoxib No evidence for greater risk vs traditional NSAIDs Revised labelling indicating possible risks GI harm appears to be less than most NSAIDs Removal from market would limit NSAID options Solomon SD et al. Cardiovascular risk associated with celecoxib in a clinical trial for colorectal adenoma prevention. NEJM 2005;352:
17 MEDAL November 2006 CV outcomes with etoricoxib and diclofenac in patients with OA and RA Other studies have reported CV adverse events, but none have had the primary aim of assessing relative CV risk vs traditional NSAIDs Randomly assigned etoricoxib 60-90mg/d vs diclofenac 150mg/d patients Cannon CP et al. CV outcomes with etoricoxib and diclofenac in patients with OA and RA in the Multinational Etoricoxib and Diclofenac Arthritis Long-term programme: : a randomised comparison. Lancet 2006; published online Nov 13, 2006.
18 MEDAL continued Aim to estimate RR of thrombotic CV events with etoricoxib vs diclofenac using a non-inferior trial design Broad population, including people with CV risk factors Patients with hx of MI, CABG, or PCI more than 6 months preceding enrolment could participate Average treatment duration 18 months
19 MEDAL outcomes and concerns Results: Event rates 1.24/100 patient years with etoricoxib and 1.30/100 patient years with diclofenac (HR 0.95; 95% CI, ) 1.11) CV events in patients on etoricoxib similar to diclofenac; ; later on in presentation, we ll see why this is not great news Do not know absolute risk increase of either agent since no placebo group More CHF, HTN with etoricoxib More GI and hepatic adverse events with diclofenac
20 COX-2 2 meta-analysis analysis 2006: 138 RCTs (COX-2 vs placebo and COX-2 vs traditional NSAIDS) Effects of COX-2 2 inhibitors and traditional NSAIDS on risk of serious vascular events (=MI, stroke, or CV death) COX-2 vs placebo: 42% relative increase in incidence of serious vascular events (primarily MI) event rates small in both groups (1.2%/yr vs 0.9%/yr = 3 excess events/1000 people treated in a year) Kearney PM et al. Do selective COX-2 2 inhibitors and traditional NSAIDs increase the risk of atherothrombosis?? Meta-analysis analysis of randomised trials. BMJ 2006;332:
21 COX-2 2 meta-analysis analysis Unable to assess dose-response; most events at 25mg/d rofecoxib; ; trend to risk with dose celecoxib Unable to assess timing of hazard (tabular data used for # of events and person years of treatment)
22 COX-2 2 systematic review Review of 23 observational studies (case-control, control, cohort) Compared CV events with COX-2 s, NSAID use, or both with non-use/remote use as reference exposure Rofecoxib 25mg/d: RR = 1.33 (95%CI ) 1.79) Rofecoxib > 25mg/d: RR = 2.19 (95%CI ) Celecoxib RR = 1.06 (95% CI ) 1.23) Early risk associated with rofecoxib (within 30 days) McGettigan P and Henry D. CV risk and inhibition of COX. A systematic review ew of the observational studies of selective and non-selective inhibitors of COX-2. JAMA 2006;296:E1-E12. E12.
23 Are all COX-2 s the same? Meta-analysis analysis and systematic review not in complete agreement State-of of-the-art paper although CV events with coxibs suggesting class effect, numerous studies indicating different degrees of risk associated with different coxibs No head-to to-head comparisons Zarraga IGE and Schwarz ER. Coxibs and Heart Disease: What have we learned and what else do we need to know? J.Am. Coll. Cardiol ;49:
24 Why do coxibs increase CV toxicity? Possible mechanism TxA 2 and PGI 2 in vasculature balance of vasoconstriction, platelet activation vs vasodilation and platelet inhibition TxA 2 important in development of acute arterial thrombosis (use ASA to block synthesis; MI) PGI 2 during episodes of unstable angina (ie( ie/ COX-2 upregulated for protection) If PGI 2 synthesis is blocked by COX-2 2 inhibitors, may tip equilibrium into prothrombotic state
25 NSAIDs, Coxibs, and Cardio-Renal Physiology: A Mechanism- Based Evaluation. Medscape Continuing Medical Education (CME) Feb 22, 2002.
26 Safety of non-selective NSAIDs If the COX-2-selective inhibitors are unsafe due to the mechanism indicated, then non-selective COX inhibitors should be safe Why do the STEMI guidelines specifically ask us to avoid ibuprofen?
27 Remember the question: The case of Mr. CP: In someone who has had an MI, is it safe to use ibuprofen regularly?
28 ACC/AHA Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction Antman EM et al Available at Antiplatelet therapy: Class III: Ibuprofen should not be used because it blocks the antiplatelet effects of aspirin. (Level of Evidence: C) Class III = Conditions for which there is evidence and/or general agreement that a procedure/treatment is not useful/effective and in some cases may be harmful Level of evidence C = Only consensus opinion of experts, case studies, or standard-of of-care.
29 Ibuprofen statement in guidelines Based on 3 studies: 2001 (Catella( Catella-Lawson) 2003 (MacDonald) 2003 (Kurth( Kurth)
30 Catella-Lawson article Structural basis of inhibition of COX-1 1 in platelets by both ASA and NSAIDs had been elucidated both binding sites within the core of the enzyme concerned about competitive interactions between ASA and NSAIDs since patients with arthritis and vascular disease may receive both if NSAIDs compete with ASA and prevent binding, may cardioprotection since platelet function only impaired by NSAIDs for a portion of dosing interval (reversible binding) Catella-Lawson F et al. COX inhibitors and the antiplatelet effects of ASA. NEJM 2001;345:
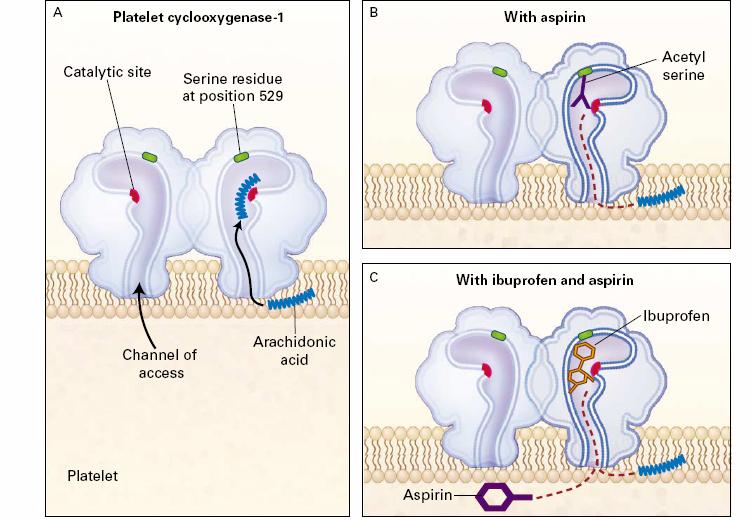
31 NEJM 2001;345:
32
33
34 MacDonald (2003) Postulated that patients with known CV disease who take low-dose ASA and ibuprofen might have risk of CV mortality Accessed UK database retrospectively selected patients diagnosed with MI, angina, stroke or TIA, and peripheral vascular disease 4 groups: discharged home on ASA, ASA + ibuprofen, ASA + diclofenac,, ASA + other NSAID MacDonald TM and Wei L. Effect of ibuprofen on cardioprotective effect of ASA. Lancet 2003;361:573-4.
35 Results Outcomes: all-cause mortality and CV mortality ASA + ibuprofen (mean dose 1210mg/d) vs ASA alone: HR = 1.93 (95% CI ) A statistically and clinically significant increased risk of mortality in users of ASA/ibuprofen vs ASA alone No increase noted in other groups Lends support to hypothesis that ibuprofen combined with ASA given for secondary prevention may be deleterious (antagonism of cardioprotective effects of ASA
36 Kurth (2003) 5 year randomized, DB, PC trial apparently healthy US male MDs 325mg ASA on alternate days vs placebo 139 MIs (ASA group) vs 239 MIs (placebo) Prospective observational data on use of NSAIDs (subgroup analysis of Physicians Health Study) In ASA group: NSAID use <60d/yr: RR of MI = 1.21 (95% CI, ) NSAID use 60d/yr ( regular( use ): RR of MI = 2.86 (95% CI, ) Conclusions: regular but not intermittent use of NSAIDs inhibits clinical benefits of ASA Kurth T et al. Inhibition of Clinical Benefits of ASA on First MI by NSAIDS. Circ 2003;108:
37 Limitations of ibuprofen information Theory makes sense, but evidence to support it is weak MacDonald: retrospective, unclear if patients took prescribed NSAIDs as directed, and no adjustments for severity of CV disease, doses of individual NSAIDs,, smoking or BMI Kurth: observational (bias and confounding possible), post-hoc MDs using NSAIDs regularly also had greater BMI, more arthritis, DM, and HTN, and were more likely to be smokers No information on brand or dose of NSAIDs Few events for comparison in exposed groups
38 Meta-analysis analysis (Kearney) information on ibuprofen Effects of COX-2 2 inhibitors and traditional NSAIDS on risk of serious vascular events (=MI, stroke, or CV death) For CV effects of traditional NSAIDs,, used mostly indirect methods to compare NSAIDs to placebo (in pain trials of NSAIDs,, no placebo control) Statistical methods indicated that high-dose ibuprofen (800mg TID) increased risk of vascular events (RR=1.51, 95% CI ) Unable to assess differing CV effects among ASA users and non-users
39 Systematic review (McGettigan( McGettigan) Review of 23 observational studies (case- control, cohort) Compared CV events with COX-2 s, NSAID use, or both with non-use/remote use as reference exposure CV events no different when ibuprofen compared to placebo (RR=1.07, 95% CI ) RRs close to 1 in users and non-users of ASA
40 What to do for Mr. CP? Ibuprofen should not be used; even if evidence is not strong, it s what we have do no harm (and guidelines are explicit) Based on previous discussion, COX-2 inhibitors do not seem like a good idea How about acetaminophen 1g q6h prn??
41 Outstanding questions What about other non-selective NSAIDs?
42 Kearney meta-analysis analysis High-dose regimens of ibuprofen and diclofenac (75mg BID) associated with a moderate increase in the risk of vascular events Ibuprofen RR=1.51 (95% CI ) Diclofenac rate ratio for vascular events = 1.63 (95% CI, ) 2.37) High-dose naproxen (500mg BID) NOT associated with an excess of CV events RR=0.92 ( )??? no increased risk with naproxen since sustained inhibition of COX-1? (t1/2=14h, BID dosing)
43 McGettigan Systematic Review Diclofenac RR = 1.40 ( ) 1.70) Other traditional NSAIDs had RRs close to 1 Naproxen 0.97 ( ) Piroxicam 1.06 ( ) Ibuprofen 1.07 ( )
44 BMJ meta-analysis analysis Study limitations Relatively small number of events available for analysis; limits assessment of hazards of various agents?timing of hazard Tabular summaries of data Attention limited to CV hazards Systematic review of observational studies Most information from databases; exposure? Self-prescription possible CV risk information was not complete in all studies (ie// smoking, HTN, hyperlipidemia) Differing baseline ages and risks Many of pooled RR estimates are close to null
45 Summary COX-2 2 inhibitors appear to have an increased risk of CV events (ie( ie/ / 3 excess events in 1000 people treated; may be higher in high risk groups) Ibuprofen may or may not increase risk; some evidence to support it, a sensible theory, and a guideline statement Diclofenac may increase risk Naproxen appears not to
46 So can I safely use NSAIDs in people at risk of MI? No clear answer! Some of the data is conflicting, but there appears to be an increase in this rare but serious event Must consider risks and benefits What are CV risks? Immediately post-mi vs no risk factors for CAD Non-NSAID NSAID options for pain Subjective report of efficacy Risk of other adverse events ie/ / GI bleeding
47 Suggestions In patients with high risk of CV events (ie( ie/ / post-mi, post- CABG, multiple risk factors), prudent to avoid If an NSAID must be used, evidence indicates naproxen may be safest choice If at risk for GI bleed, can we use a ulcer prophylaxis and naproxen? If patient needs COX-2 2 inhibitor, may be willing to accept increased risk Dose/duration issue not clear; seems prudent to use lowest dose for shortest period of time possible Good reference article: Antman EM et al. Use of Nonsteroidal Antiinflammatory Drugs. An update for clinicians. A scientific statemnt from the American Heart Association. Circ 2007 (published online e Feb 26, 2007)
48 Pharmaceutical care Involve the patient in the decision explain possible risks and benefits and choose together Questions?
NSAID Use in Post- Myocardial Infarction Patients
 NSAID Use in Post- Myocardial Infarction Patients Leah Jackson, BScPhm Pharmacy Resident Cardiology Rotation February 28, 2007 Objectives By the end of the presentation, the audience will be able to use
NSAID Use in Post- Myocardial Infarction Patients Leah Jackson, BScPhm Pharmacy Resident Cardiology Rotation February 28, 2007 Objectives By the end of the presentation, the audience will be able to use
Disclosure. Learning Objectives 1/17/2018. Pumping the Breaks in Pain Management: An Update on Cardiovascular Risk with NSAID Use
 Disclosure Pumping the Breaks in Pain Management: An Update on Cardiovascular Risk with Liz Van Dril, PharmD, BCPS PGY2 Ambulatory Care Resident January 17 th, 2018 Dr. Liz Van Dril has no actual or potential
Disclosure Pumping the Breaks in Pain Management: An Update on Cardiovascular Risk with Liz Van Dril, PharmD, BCPS PGY2 Ambulatory Care Resident January 17 th, 2018 Dr. Liz Van Dril has no actual or potential
CARDIOVASCULAR RISK and NSAIDs
 CARDIOVASCULAR RISK and NSAIDs Dr. Syed Ghulam Mogni Mowla Assistant Professor of Medicine Shaheed Suhrawardy Medical College, Dhaka INTRODUCTION NSAIDs are most commonly prescribed drugs Recent evidence
CARDIOVASCULAR RISK and NSAIDs Dr. Syed Ghulam Mogni Mowla Assistant Professor of Medicine Shaheed Suhrawardy Medical College, Dhaka INTRODUCTION NSAIDs are most commonly prescribed drugs Recent evidence
NON STEROIDEAL ANTI-INFLAMMATORY DRUGS AND CARDIOVASCULAR RISK. Advances in Cardiac Arrhythmias and Great Innovations in Cardiology
 NON STEROIDEAL ANTI-INFLAMMATORY DRUGS AND CARDIOVASCULAR RISK Advances in Cardiac Arrhythmias and Great Innovations in Cardiology Torino, October 15, 2016 Giuseppe Di Pasquale Direttore Dipartimento Medico
NON STEROIDEAL ANTI-INFLAMMATORY DRUGS AND CARDIOVASCULAR RISK Advances in Cardiac Arrhythmias and Great Innovations in Cardiology Torino, October 15, 2016 Giuseppe Di Pasquale Direttore Dipartimento Medico
Cardiovascular Risk of Celecoxib in 6 Randomized Placebo-controlled Trials: The Cross Trial Safety Analysis
 Cardiovascular Risk of Celecoxib in 6 Randomized Placebo-controlled Trials: The Cross Trial Safety Analysis Scott D. Solomon, MD, Janet Wittes, PhD, Ernest Hawk, MD, MPH for the Celecoxib Cross Trials
Cardiovascular Risk of Celecoxib in 6 Randomized Placebo-controlled Trials: The Cross Trial Safety Analysis Scott D. Solomon, MD, Janet Wittes, PhD, Ernest Hawk, MD, MPH for the Celecoxib Cross Trials
NSAIDs: The Truth About Cardiovascular Risk
 NSAIDs: The Truth About Cardiovascular Risk Adam Grunbaum DO FACOI FACR American College of Osteopathic Internists Annual Convention and Scientific Sessions October 3 rd 2015 Disclosures none 2 Objectives
NSAIDs: The Truth About Cardiovascular Risk Adam Grunbaum DO FACOI FACR American College of Osteopathic Internists Annual Convention and Scientific Sessions October 3 rd 2015 Disclosures none 2 Objectives
Characteristics of selective and non-selective NSAID use in Scotland
 Characteristics of selective and non-selective NSAID use in Scotland Alford KMG 1, Simpson C 1, Williams D 2 1 Department of General Practice & Primary Care, The University of Aberdeen. 2 Department of
Characteristics of selective and non-selective NSAID use in Scotland Alford KMG 1, Simpson C 1, Williams D 2 1 Department of General Practice & Primary Care, The University of Aberdeen. 2 Department of
LOW DOSE ASPIRIN CARDIOVASCULAR DISEASE FOR PROPHYLAXIS OF FOR BACKGROUND USE ONLY NOT TO BE USED IN DETAILING
 LOW DOSE ASPIRIN FOR PROPHYLAXIS OF CARDIOVASCULAR DISEASE FOR BACKGROUND USE ONLY NOT TO BE USED IN DETAILING Use of Low Dose Aspirin to Treat and Prevent Cardiovascular Disease In recent decades, aspirin
LOW DOSE ASPIRIN FOR PROPHYLAXIS OF CARDIOVASCULAR DISEASE FOR BACKGROUND USE ONLY NOT TO BE USED IN DETAILING Use of Low Dose Aspirin to Treat and Prevent Cardiovascular Disease In recent decades, aspirin
NSAIDs: Side Effects and Guidelines
 NSAIDs: Side Effects and James J Hale FY1 Department of Anaesthetics Introduction The non-steroidal anti-inflammatory drugs (NSAIDs) are a diverse group of drugs that have analgesic, antipyretic and anti-inflammatory
NSAIDs: Side Effects and James J Hale FY1 Department of Anaesthetics Introduction The non-steroidal anti-inflammatory drugs (NSAIDs) are a diverse group of drugs that have analgesic, antipyretic and anti-inflammatory
Figure 13-1: Antiplatelet Action of Aspirin (Modified After Taneja et.al 2004) ASPIRIN RESISTANCE
 ASPIRIN RESISTANCE") CHAPTER 13 ASPIRIN Action Aspirin Resistance Aspirin Dose Therapeutic Efficacy - Secondary prevention - Acute coronary syndromes - Primary prevention Limitations and Side Effects Aspirin Aspirin should
CHAPTER 13 ASPIRIN Action Aspirin Resistance Aspirin Dose Therapeutic Efficacy - Secondary prevention - Acute coronary syndromes - Primary prevention Limitations and Side Effects Aspirin Aspirin should
Considerations relevant to Aspirin or NSAIDS use in patients with cardiovascular disease
 Considerations relevant to Aspirin or NSAIDS use in patients with cardiovascular disease Shawn W. Robinson, MD Assistant Professor of Medicine, Physiology University of Maryland School of Medicine Chief
Considerations relevant to Aspirin or NSAIDS use in patients with cardiovascular disease Shawn W. Robinson, MD Assistant Professor of Medicine, Physiology University of Maryland School of Medicine Chief
NSAIDs Overview. Souraya Domiati, Pharm D, MS
 NSAIDs Overview Souraya Domiati, Pharm D, MS Case A 32 years old shows up into your pharmacy asking for an NSAID for his ankle pain He smokes1 pack/day His BP is 125/75mmHg His BMI is 35kg/m2 His is on
NSAIDs Overview Souraya Domiati, Pharm D, MS Case A 32 years old shows up into your pharmacy asking for an NSAID for his ankle pain He smokes1 pack/day His BP is 125/75mmHg His BMI is 35kg/m2 His is on
Coxibs and Heart Disease
 Journal of the American College of Cardiology Vol. 49, No. 1, 2007 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.10.003
Journal of the American College of Cardiology Vol. 49, No. 1, 2007 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.10.003
COX-2 inhibitors: A cautionary tale. October 2, 2006
 COX-2 inhibitors: A cautionary tale October 2, 2006 Molecular interventions in human disease... An approach as old as human civilization. With whom the herbs have come together Like kingly chiefs unto
COX-2 inhibitors: A cautionary tale October 2, 2006 Molecular interventions in human disease... An approach as old as human civilization. With whom the herbs have come together Like kingly chiefs unto
Gastrointestinal Safety of Coxibs and Outcomes Studies: What s the Verdict?
 Vol. 23 No. 4S April 2002 Journal of Pain and Symptom Management S5 Proceedings from the Symposium The Evolution of Anti-Inflammatory Treatments in Arthritis: Current and Future Perspectives Gastrointestinal
Vol. 23 No. 4S April 2002 Journal of Pain and Symptom Management S5 Proceedings from the Symposium The Evolution of Anti-Inflammatory Treatments in Arthritis: Current and Future Perspectives Gastrointestinal
Presentation Outline. Introduction to Biomedical Research Designs. EBM: A Practical Definition. Grade the Evidence (Example McMaster Grading System)
") Presentation Outline Introduction to Biomedical Research Designs Sean D. Sullivan, R.Ph., PhD Professor of Pharmacy, Public Health and Medicine University of Washington Why a course in Biomedical Research
Presentation Outline Introduction to Biomedical Research Designs Sean D. Sullivan, R.Ph., PhD Professor of Pharmacy, Public Health and Medicine University of Washington Why a course in Biomedical Research
PDP 406 CLINICAL TOXICOLOGY
 PDP 406 CLINICAL TOXICOLOGY Pharm.D Fourth Year NON-STEROIDAL ANTI-INFLAMMATORY DRUGS (NSAIDS) Mr.D.Raju.M.Pharm., Lecturer OPTIONS FOR LOCAL IMPLEMENTATION (1) NPC. KEY THERAPEUTIC TOPICS MEDICINES MANAGEMENT
PDP 406 CLINICAL TOXICOLOGY Pharm.D Fourth Year NON-STEROIDAL ANTI-INFLAMMATORY DRUGS (NSAIDS) Mr.D.Raju.M.Pharm., Lecturer OPTIONS FOR LOCAL IMPLEMENTATION (1) NPC. KEY THERAPEUTIC TOPICS MEDICINES MANAGEMENT
New Topics in Aspirin Therapy
 Aspirin Therapy New Topics in Aspirin Therapy JMAJ 47(12): 566 572, 2004 Makoto HANDA Director and Associate Professor, Department of Transfusion Medicine and Cell Therapy, School of Medicine, Keio University
Aspirin Therapy New Topics in Aspirin Therapy JMAJ 47(12): 566 572, 2004 Makoto HANDA Director and Associate Professor, Department of Transfusion Medicine and Cell Therapy, School of Medicine, Keio University
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
SESSION 5 2:20 3:35 PM
 SESSION 5 2:20 3:35 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 5 2:20 3:35 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Ali Jaber, Ph.D. MS in Pharmacy MS in Pharmaceutical Chemistry
 Nonsteroidal antiinflammatory drugs (NSAID) Ali Jaber, Ph.D. MS in Pharmacy MS in Pharmaceutical Chemistry The inflammatory response occurs in vascularised tissues in response to injury. It is part of
Nonsteroidal antiinflammatory drugs (NSAID) Ali Jaber, Ph.D. MS in Pharmacy MS in Pharmaceutical Chemistry The inflammatory response occurs in vascularised tissues in response to injury. It is part of
Anti-inflammatory drugs
 Anti-inflammatory drugs 1 Inflammatory process 1. stimulus (cut) 2. Initial local vasoconstriction( blood loss) 3. vasodilation, local immune/inflammatory reaction (heat, redness) 4. swelling and pain
Anti-inflammatory drugs 1 Inflammatory process 1. stimulus (cut) 2. Initial local vasoconstriction( blood loss) 3. vasodilation, local immune/inflammatory reaction (heat, redness) 4. swelling and pain
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
COX-2 inhibitors: A cautionary tale
 COX-2 inhibitors: A cautionary tale October 1, 2007 Molecular interventions in human disease... An approach as old as human civilization. With whom the herbs have come together Like kingly chiefs unto
COX-2 inhibitors: A cautionary tale October 1, 2007 Molecular interventions in human disease... An approach as old as human civilization. With whom the herbs have come together Like kingly chiefs unto
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Coxib and traditional NSAID Trialists (CNT)
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Coxib and traditional NSAID Trialists (CNT)
British Medical Journal. June 3, 2006;332: Patricia M Kearney, Colin Baigent, Jon Godwin, Heather Halls, Jonathan R Emberson, Carlo Patrono
 Do selective cyclo-oxygenase-2 inhibitors and traditional non-steroidal anti-inflammatory drugs increase the risk of atherothrombosis? Metaanalysis of randomised trials 1 British Medical Journal June 3,
Do selective cyclo-oxygenase-2 inhibitors and traditional non-steroidal anti-inflammatory drugs increase the risk of atherothrombosis? Metaanalysis of randomised trials 1 British Medical Journal June 3,
Managing Musculoskeletal Pain and Injury
 Managing Musculoskeletal Pain and Injury New & Old Drugs: Best Choices MAY 5, 2017 WILLIAM KNOPP, MD Dr. Knopp indicated no potential conflict of interest to this presentation. He does not intend to discuss
Managing Musculoskeletal Pain and Injury New & Old Drugs: Best Choices MAY 5, 2017 WILLIAM KNOPP, MD Dr. Knopp indicated no potential conflict of interest to this presentation. He does not intend to discuss
Effective Health Care Program
 Comparative Effectiveness Review Number 38 Effective Health Care Program Analgesics for Osteoarthritis: An Update of the 2006 Comparative Effectiveness Review Executive Summary Background Osteoarthritis
Comparative Effectiveness Review Number 38 Effective Health Care Program Analgesics for Osteoarthritis: An Update of the 2006 Comparative Effectiveness Review Executive Summary Background Osteoarthritis
SESSION 3 11 AM 12:30 PM
 SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
TABLE OF CONTENTS. COX-2 Inhibitors Cardiovascular and Gastrointestinal Safety
 TABLE OF CONTENTS COX-2 Inhibitors - Cardiovascular and Gastrointestinal Safety 1-2 Oral Erythromycin and Risk of Sudden Cardiac Death 2-3 Common Drug Interactions between Herbal and Prescription Medications
TABLE OF CONTENTS COX-2 Inhibitors - Cardiovascular and Gastrointestinal Safety 1-2 Oral Erythromycin and Risk of Sudden Cardiac Death 2-3 Common Drug Interactions between Herbal and Prescription Medications
Abwägung zwischen Schaden und Nutzen medizinischer Interventionen
 Abwägung zwischen Schaden und Nutzen medizinischer Interventionen Peter Jüni Institut für Sozial and Präventivmedizin, Universität Bern CTU Bern, Inselspital Bern Outline Wall Street, New York, Sept 30,
Abwägung zwischen Schaden und Nutzen medizinischer Interventionen Peter Jüni Institut für Sozial and Präventivmedizin, Universität Bern CTU Bern, Inselspital Bern Outline Wall Street, New York, Sept 30,
To provide information on the use of acetyl salicylic acid in the treatment and prevention of vascular events.
 ACETYL SALICYLIC ACID TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To provide information on the use of acetyl salicylic acid in the treatment and prevention of vascular events.
ACETYL SALICYLIC ACID TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To provide information on the use of acetyl salicylic acid in the treatment and prevention of vascular events.
Conflicts of Interest: None. Aspirin, primary prevention and USPSTF. Primary prevention of ASCVD is important
 Aspirin, primary prevention and USPSTF Presented by: Craig Williams, PharmD., BCPS., FNLA; February 2017 Conflicts of Interest: None Primary prevention of ASCVD is important Myocardial Infarction Incidence
Aspirin, primary prevention and USPSTF Presented by: Craig Williams, PharmD., BCPS., FNLA; February 2017 Conflicts of Interest: None Primary prevention of ASCVD is important Myocardial Infarction Incidence
Review Article. Safety Profile of Nonsteroidal Antiflammatory Drugs (NSAID) Safety Profile of NSAID
 Safety Profile of NSAID") Safety Profile of Nonsteroidal Antiflammatory Drugs (NSAID) R. Stoilov: University Hospital St Ivan Rilski, Clinic of Rheumatology Contact: Rumen Stoilov, Clinic of Rheumatology, University Hospital St
Safety Profile of Nonsteroidal Antiflammatory Drugs (NSAID) R. Stoilov: University Hospital St Ivan Rilski, Clinic of Rheumatology Contact: Rumen Stoilov, Clinic of Rheumatology, University Hospital St
cyclooxygenase-2 (COX-2)-selective
-selective") Risks versus benefits of cyclooxygenase-2-selective nonsteroidal antiinflammatory drugs Cyclooxygenase-2 (COX-2)-selective nonsteroidal antiinflammatory drugs (NSAIDs) have often been used in recent years
Risks versus benefits of cyclooxygenase-2-selective nonsteroidal antiinflammatory drugs Cyclooxygenase-2 (COX-2)-selective nonsteroidal antiinflammatory drugs (NSAIDs) have often been used in recent years
eappendix A. Opioids and Nonsteroidal Anti-Inflammatory Drugs
 eappendix A. Opioids and Nonsteroidal Anti-Inflammatory Drugs Nonsteroidal Anti-Inflammatory Drugs Nonselective nonsteroidal anti-inflammatory drugs Diclofenac, etodolac, flurbiprofen, ketorolac, ibuprofen,
eappendix A. Opioids and Nonsteroidal Anti-Inflammatory Drugs Nonsteroidal Anti-Inflammatory Drugs Nonselective nonsteroidal anti-inflammatory drugs Diclofenac, etodolac, flurbiprofen, ketorolac, ibuprofen,
Use of Aspirin for primary prevention of cardiovascular disease - USPSTF guideline changes
 Use of Aspirin for primary prevention of cardiovascular disease - USPSTF guideline changes Pawan Hari MD MPH Director cardiac catheterization laboratory Dr. Hari indicated no potential conflict of interest
Use of Aspirin for primary prevention of cardiovascular disease - USPSTF guideline changes Pawan Hari MD MPH Director cardiac catheterization laboratory Dr. Hari indicated no potential conflict of interest
Cardiovascular Effects of COX-2 Inhibitors: A Review of the Literature
 Cardiovascular Effects of COX-2 Inhibitors: A Review of the Literature Craig D. Cox, PharmD, BCPS, Brad L. Stanford, PharmD, BCOP, James P. Tsikouris, PharmD, Michael J. Peeters, PharmD, BCPS, and Gar
Cardiovascular Effects of COX-2 Inhibitors: A Review of the Literature Craig D. Cox, PharmD, BCPS, Brad L. Stanford, PharmD, BCOP, James P. Tsikouris, PharmD, Michael J. Peeters, PharmD, BCPS, and Gar
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Risk Management Plan Etoricoxib film-coated tablets
 VI.2 Elements for a Public Summary VI.2.1 Overview of disease epidemiology Osteoarthritis (OA): OA is a condition in which the cartilage of the joints is broken down. This causes stiffness, pain and leads
VI.2 Elements for a Public Summary VI.2.1 Overview of disease epidemiology Osteoarthritis (OA): OA is a condition in which the cartilage of the joints is broken down. This causes stiffness, pain and leads
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital
 Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
THE NON-STEROIDAL ANTI- INFLAMMATORY DRUGS-MYOCARDIAL INFARCTION ASSOCIATION: AN INVESTIGATION OF KENTUCKY MEDICAID PRESCRIPTION CLAIMS
 University of Kentucky UKnowledge Theses and Dissertations--Epidemiology and Biostatistics College of Public Health 2015 THE NON-STEROIDAL ANTI- INFLAMMATORY DRUGS-MYOCARDIAL INFARCTION ASSOCIATION: AN
University of Kentucky UKnowledge Theses and Dissertations--Epidemiology and Biostatistics College of Public Health 2015 THE NON-STEROIDAL ANTI- INFLAMMATORY DRUGS-MYOCARDIAL INFARCTION ASSOCIATION: AN
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Celebrex) Reference Number: CP.CPA.239 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Celebrex) Reference Number: CP.CPA.239 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
FDA strengthens warning that non-aspirin nonsteroidal antiinflammatory drugs (NSAIDs) can cause heart attacks or strokes
 can cause heart attacks or strokes") FDA strengthens warning that non-aspirin nonsteroidal antiinflammatory drugs (NSAIDs) can cause heart attacks or strokes Safety Announcement [7-9-2015] The U.S. Food and Drug Administration (FDA) is strengthening
FDA strengthens warning that non-aspirin nonsteroidal antiinflammatory drugs (NSAIDs) can cause heart attacks or strokes Safety Announcement [7-9-2015] The U.S. Food and Drug Administration (FDA) is strengthening
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Drug Use Criteria: Cyclooxygenase-2 Inhibitors
 Texas Vendor Program Use Criteria: Cyclooxygenase-2 Inhibitors Publication History Developed January 2002. Revised May 2016; October 2014; February 2013; December 2012; March 2011; January 2011; October
Texas Vendor Program Use Criteria: Cyclooxygenase-2 Inhibitors Publication History Developed January 2002. Revised May 2016; October 2014; February 2013; December 2012; March 2011; January 2011; October
Cyclooxygenase-selective inhibition of prostanoid formation: transducing biochemical selectivity into clinical read-outs
 Cyclooxygenase-selective inhibition of prostanoid formation: transducing biochemical selectivity into clinical read-outs Carlo Patrono, 1 Paola Patrignani, 1 and Luis A. García Rodríguez 2 1 Department
Cyclooxygenase-selective inhibition of prostanoid formation: transducing biochemical selectivity into clinical read-outs Carlo Patrono, 1 Paola Patrignani, 1 and Luis A. García Rodríguez 2 1 Department
NONSTEROIDAL ANTI- INFLAMMATORY DRUGS
 NONSTEROIDAL ANTI- INFLAMMATORY DRUGS MRS. M.M. HAS A 3 YR. HX OF PROGRESSIVE RIGHT HIP PAIN. THE PAIN INCREASES WITH WEIGHT BEARING ACTIVITY. PT. HAS BEEN ON ACETAMINOPHEN WITHOUT RELIEF. PERTINENT LABS
NONSTEROIDAL ANTI- INFLAMMATORY DRUGS MRS. M.M. HAS A 3 YR. HX OF PROGRESSIVE RIGHT HIP PAIN. THE PAIN INCREASES WITH WEIGHT BEARING ACTIVITY. PT. HAS BEEN ON ACETAMINOPHEN WITHOUT RELIEF. PERTINENT LABS
Index. B Biotransformation, 112 Blood pressure, 72, 75 77
 Index A Acute gout, treatment, 41 Adenomatous polyposis coli (APC), 224 Adenomatous polyp prevention on Vioxx (APPROVe), 250 Ankylosing spondylitis (AS), 40 41 Antiplatelet therapy, 138 Antithrombotic
Index A Acute gout, treatment, 41 Adenomatous polyposis coli (APC), 224 Adenomatous polyp prevention on Vioxx (APPROVe), 250 Ankylosing spondylitis (AS), 40 41 Antiplatelet therapy, 138 Antithrombotic
Nonsteroidal Anti inflammatory Drugs (NSAIDs)
") Nonsteroidal Anti inflammatory Drugs (NSAIDs) PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.phar, Lecturer Analgesic Antipyretic Anti inflammatory (at higher doses) Common Pharmacological Effects
Nonsteroidal Anti inflammatory Drugs (NSAIDs) PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.phar, Lecturer Analgesic Antipyretic Anti inflammatory (at higher doses) Common Pharmacological Effects
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PRESCRIBING SUPPORT TEAM AUDIT: Etoricoxib hypertension safety evaluation
 PRESCRIBING SUPPORT TEAM AUDIT: Etoricoxib hypertension safety evaluation DATE OF AUTHORISATION: AUTHORISING GP: PRESCRIBING SUPPORT TECHNICIAN: SUMMARY This audit has been designed to ensure that patients
PRESCRIBING SUPPORT TEAM AUDIT: Etoricoxib hypertension safety evaluation DATE OF AUTHORISATION: AUTHORISING GP: PRESCRIBING SUPPORT TECHNICIAN: SUMMARY This audit has been designed to ensure that patients
Update on the clinical pharmacology of etoricoxib, a potent cyclooxygenase-2 inhibitor
 DRUG EVALUATION Update on the clinical pharmacology of etoricoxib, a potent cyclooxygenase-2 inhibitor Alejandro Escudero- Contreras, Janitzia Vazquez-Mellado Cervantes & Eduardo Collantes-Estevez Author
DRUG EVALUATION Update on the clinical pharmacology of etoricoxib, a potent cyclooxygenase-2 inhibitor Alejandro Escudero- Contreras, Janitzia Vazquez-Mellado Cervantes & Eduardo Collantes-Estevez Author
Drug Class Review on Cyclo-oxygenase (COX)-2 Inhibitors and Non-steroidal Anti-inflammatory Drugs (NSAIDs)
-2 Inhibitors and Non-steroidal Anti-inflammatory Drugs (NSAIDs)") Drug Class Review on Cyclo-oxygenase (COX)-2 Inhibitors and Non-steroidal Anti-inflammatory Drugs (NSAIDs) Final Report Update 3 Evidence Tables November 2006 Original Report Date: May 2002 Update 1 Report
Drug Class Review on Cyclo-oxygenase (COX)-2 Inhibitors and Non-steroidal Anti-inflammatory Drugs (NSAIDs) Final Report Update 3 Evidence Tables November 2006 Original Report Date: May 2002 Update 1 Report
Antithrombotics 201: Aspirin and USPSTF. Presented by: Craig Williams, PharmD., BCPS., FNLA; November, Conflicts of Interest: None
 Antithrombotics 201: Aspirin and USPSTF Presented by: Craig Williams, PharmD., BCPS., FNLA; November, 2016 Conflicts of Interest: None 1 What percent of patients who die within 30 days of an MI die before
Antithrombotics 201: Aspirin and USPSTF Presented by: Craig Williams, PharmD., BCPS., FNLA; November, 2016 Conflicts of Interest: None 1 What percent of patients who die within 30 days of an MI die before
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 18 January 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 January 2012 ARCOXIA 30 mg, film-coated tablet B/28 (CIP code: 387 980-8) B/98 (CIP code: 573 530-9) ARCOXIA 60
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 January 2012 ARCOXIA 30 mg, film-coated tablet B/28 (CIP code: 387 980-8) B/98 (CIP code: 573 530-9) ARCOXIA 60
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
INHIBITORS OF COX-2 AND RISK FOR HEART FAILURE DECOMPENSATION: SYSTEMATIC REVIEW
 INHIBITORS OF COX-2 AND RISK FOR HEART FAILURE DECOMPENSATION: SYSTEMATIC REVIEW Gonçalo Colaço Cainé da Silva Nº 4903 Dissertação de Mestrado Integrado em Ciências Farmacêuticas apresentada na Universidade
INHIBITORS OF COX-2 AND RISK FOR HEART FAILURE DECOMPENSATION: SYSTEMATIC REVIEW Gonçalo Colaço Cainé da Silva Nº 4903 Dissertação de Mestrado Integrado em Ciências Farmacêuticas apresentada na Universidade
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials
 Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Attribution: University of Michigan Medical School, Department of Microbiology and Immunology
 Attribution: University of Michigan Medical School, Department of Microbiology and Immunology License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Attribution: University of Michigan Medical School, Department of Microbiology and Immunology License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
NSAID Regional Audit Group Presentation. Audit Group: Dr Richard Latten, Ruth Clark, Dr Sarah Fradsham, Dr Seamus Coyle, Claire Johnston
 NSAID Regional Audit Group Presentation Audit Group: Dr Richard Latten, Ruth Clark, Dr Sarah Fradsham, Dr Seamus Coyle, Claire Johnston Thank you from the audit group for all who participated in the data
NSAID Regional Audit Group Presentation Audit Group: Dr Richard Latten, Ruth Clark, Dr Sarah Fradsham, Dr Seamus Coyle, Claire Johnston Thank you from the audit group for all who participated in the data
Clinical Investigations and Reports. Cardiovascular Thrombotic Events in Controlled, Clinical Trials of Rofecoxib
 Clinical Investigations and Reports Cardiovascular Thrombotic Events in Controlled, Clinical Trials of Rofecoxib Marvin A. Konstam, MD; Matthew R. Weir, MD; Alise Reicin, MD; Deborah Shapiro, DrPh; Rhoda
Clinical Investigations and Reports Cardiovascular Thrombotic Events in Controlled, Clinical Trials of Rofecoxib Marvin A. Konstam, MD; Matthew R. Weir, MD; Alise Reicin, MD; Deborah Shapiro, DrPh; Rhoda
Acetaminophen and NSAIDS. James Moriarity MD University of Notre Dame
 Acetaminophen and NSAIDS James Moriarity MD University of Notre Dame Lecture Goals Understand the indications for acetaminophen and NSAID use in musculoskeletal medicine Understand the role of Eicosanoids
Acetaminophen and NSAIDS James Moriarity MD University of Notre Dame Lecture Goals Understand the indications for acetaminophen and NSAID use in musculoskeletal medicine Understand the role of Eicosanoids
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center
 Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Pain: A Public Health Challenge. NSAIDS for Managing Pain. Iroko: Innovators in Analgesia
 Pain: A Public Health Challenge Despite advances in understanding and treatment, pain remains a major public health challenge 1 that exacts a significant personal and economic toll on Americans. 1 Pain
Pain: A Public Health Challenge Despite advances in understanding and treatment, pain remains a major public health challenge 1 that exacts a significant personal and economic toll on Americans. 1 Pain
This document has not been circulated to either the industry or Consultants within the Suffolk system.
 New Medicine Report Document Status COX II Inhibitors In Acute Analgesia For Suffolk Drug & Therapeutics Committee Date of Last Revision 15 th February 2002 Reviewer s Comments There seems to be a growing
New Medicine Report Document Status COX II Inhibitors In Acute Analgesia For Suffolk Drug & Therapeutics Committee Date of Last Revision 15 th February 2002 Reviewer s Comments There seems to be a growing
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Circulation. 2001;104: ; originally published online October 15, 2001; doi: /hc
 Cardiovascular Thrombotic Events in Controlled, Clinical Trials of Rofecoxib Marvin A. Konstam, Matthew R. Weir, Alise Reicin, Deborah Shapiro, Rhoda S. Sperling, Eliav Barr and Barry J. Gertz Circulation.
Cardiovascular Thrombotic Events in Controlled, Clinical Trials of Rofecoxib Marvin A. Konstam, Matthew R. Weir, Alise Reicin, Deborah Shapiro, Rhoda S. Sperling, Eliav Barr and Barry J. Gertz Circulation.
(i) Is there a registered protocol for this IPD meta-analysis? Please clarify.
 Is there a registered protocol for this IPD meta-analysis? Please clarify.") Reviewer: 4 Additional Questions: Please enter your name: Stefanos Bonovas Job Title: Researcher Institution: Humanitas Clinical and Research Institute, Milan, Italy Comments: The authors report the results
Reviewer: 4 Additional Questions: Please enter your name: Stefanos Bonovas Job Title: Researcher Institution: Humanitas Clinical and Research Institute, Milan, Italy Comments: The authors report the results
Database of Abstracts of Reviews of Effects (DARE) Produced by the Centre for Reviews and Dissemination Copyright 2017 University of York.
 Produced by the Centre for Reviews and Dissemination Copyright 2017 University of York.") A comparison of the cost-effectiveness of five strategies for the prevention of non-steroidal anti-inflammatory drug-induced gastrointestinal toxicity: a systematic review with economic modelling Brown
A comparison of the cost-effectiveness of five strategies for the prevention of non-steroidal anti-inflammatory drug-induced gastrointestinal toxicity: a systematic review with economic modelling Brown
Can We Trust the Clinical Trials? Björn Beermann, MD,PhD, Professor Medical Products Agency Uppsala Sweden
 Can We Trust the Clinical Trials? Björn Beermann, MD,PhD, Professor Medical Products Agency Uppsala Sweden Can We Trust the Clinical Trials? Yes, if they are performed according to GCP etc BUT But do we
Can We Trust the Clinical Trials? Björn Beermann, MD,PhD, Professor Medical Products Agency Uppsala Sweden Can We Trust the Clinical Trials? Yes, if they are performed according to GCP etc BUT But do we
Anneloes van Walsem 1, Shaloo Pandhi 2, Richard M Nixon 2, Patricia Guyot 1, Andreas Karabis 1* and R Andrew Moore 3
 van Walsem et al. Arthritis Research & Therapy (2015) 17:66 DOI 10.1186/s13075-015-0554-0 RESEARCH ARTICLE Open Access Relative benefit-risk comparing diclofenac to other traditional non-steroidal anti-inflammatory
van Walsem et al. Arthritis Research & Therapy (2015) 17:66 DOI 10.1186/s13075-015-0554-0 RESEARCH ARTICLE Open Access Relative benefit-risk comparing diclofenac to other traditional non-steroidal anti-inflammatory
Accounting for cardiovascular risk when prescribing NSAIDs
 MEDICINES OPTIMISATION Accounting for cardiovascular risk when prescribing NSAIDs DAVID LAIGHT It is now recognised that oral NSAIDs can increase the risk of cardiovascular events, including myocardial
MEDICINES OPTIMISATION Accounting for cardiovascular risk when prescribing NSAIDs DAVID LAIGHT It is now recognised that oral NSAIDs can increase the risk of cardiovascular events, including myocardial
Carlo Patrono, MD, FESC. New York, 8 th December Catholic University School of Medicine, Rome, Italy. New York Cardiovascular Symposium
 Aspirin in Primary and Secondary Cardiovascular Disease Prevention. Still Four Questions: About Enteric-Coated, Indicated Doses, Use in Diabetes, Use in PVD Carlo Patrono, MD, FESC Catholic University
Aspirin in Primary and Secondary Cardiovascular Disease Prevention. Still Four Questions: About Enteric-Coated, Indicated Doses, Use in Diabetes, Use in PVD Carlo Patrono, MD, FESC Catholic University
Subgroup Analyses to Determine Cardiovascular Risk Associated With Nonsteroidal Antiinflammatory Drugs and Coxibs in Specific Patient Groups
 Arthritis & Rheumatism (Arthritis Care & Research) Vol. 59, No. 8, August 15, 2008, pp 1097 1104 DOI 10.1002/art.23911 2008, American College of Rheumatology ORIGINAL ARTICLE Subgroup Analyses to Determine
Arthritis & Rheumatism (Arthritis Care & Research) Vol. 59, No. 8, August 15, 2008, pp 1097 1104 DOI 10.1002/art.23911 2008, American College of Rheumatology ORIGINAL ARTICLE Subgroup Analyses to Determine
Cardiovascular safety and gastrointestinal tolerability of etoricoxib vs diclofenac in a randomized controlled clinical trial (The MEDAL study)
") Rheumatology 2009;48:425 432 Advance Access publication 17 February 2009 doi:10.1093/rheumatology/kep005 Cardiovascular safety and gastrointestinal tolerability of etoricoxib vs diclofenac in a randomized
Rheumatology 2009;48:425 432 Advance Access publication 17 February 2009 doi:10.1093/rheumatology/kep005 Cardiovascular safety and gastrointestinal tolerability of etoricoxib vs diclofenac in a randomized
Personalized Aspirin Therapy
 Personalized Aspirin Therapy Nadir Arber, MD, MSc, MHA Head - Integrated Cancer Prevention Center Tel Aviv Medical Centre and Tel Aviv University Heidelberg 2014 CRC is Preventable Early detection Chemoprevention
Personalized Aspirin Therapy Nadir Arber, MD, MSc, MHA Head - Integrated Cancer Prevention Center Tel Aviv Medical Centre and Tel Aviv University Heidelberg 2014 CRC is Preventable Early detection Chemoprevention
Endothelium. A typical endothelial cell is about 30mm long, Accounts for 1% or less of the arterial weight
 Endothelium Discovered in 1845 A typical endothelial cell is about 30mm long, 10mm wide, and 0.2 3 mm thick Accounts for 1% or less of the arterial weight As recently as the late 1960s it was thought of
Endothelium Discovered in 1845 A typical endothelial cell is about 30mm long, 10mm wide, and 0.2 3 mm thick Accounts for 1% or less of the arterial weight As recently as the late 1960s it was thought of
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Optimal lenght of DAPT in different clinical scenarios
 Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Vimovo (delayed-release enteric-coated naproxen with esomeprazole)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.17.01 Subject: Vimovo Page: 1 of 5 Last Review Date: September 18, 2015 Vimovo Description Vimovo (delayed-release
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.17.01 Subject: Vimovo Page: 1 of 5 Last Review Date: September 18, 2015 Vimovo Description Vimovo (delayed-release
Preoperative Cardiac Evaluation:
 Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
- Mohammad Sinnokrot. -Ensherah Mokheemer. - Malik Al-Zohlof. 1 P a g e
 -1 - Mohammad Sinnokrot -Ensherah Mokheemer - Malik Al-Zohlof 1 P a g e Introduction Two of the most important problems you will face as a doctor are coagulation and bleeding, normally they are in balance,
-1 - Mohammad Sinnokrot -Ensherah Mokheemer - Malik Al-Zohlof 1 P a g e Introduction Two of the most important problems you will face as a doctor are coagulation and bleeding, normally they are in balance,
NSAIDs. NSAIDs are important but they can have side effects.
 NSAIDs Pain Treatment Nonsteroidal anti-inflammatory drugs (NSAIDs) are often recommended for initial treatment of pain and can be added to more powerful drugs to treat worse pain. Acetaminophen, such
NSAIDs Pain Treatment Nonsteroidal anti-inflammatory drugs (NSAIDs) are often recommended for initial treatment of pain and can be added to more powerful drugs to treat worse pain. Acetaminophen, such
( Aspirin ) ( Stroke ) ( Dosage ) ( Diabetes ) ( Metabolic syndrome ) ( Primary prevention ) Aspirin Aspirin Aspirin. Aspirin.
 ( Stroke ) ( Dosage ) ( Diabetes ) ( Metabolic syndrome ) ( Primary prevention ) Aspirin Aspirin Aspirin. Aspirin.") 2007 18 1-10 ( 75 150 mg/day ) ( American Heart Association AHA ) ( American Diabetes Association ADA ) 75 150 mg/day ( ) ( ) ( Stroke ) ( Dosage ) ( Diabetes ) ( Metabolic syndrome ) ( Primary prevention
2007 18 1-10 ( 75 150 mg/day ) ( American Heart Association AHA ) ( American Diabetes Association ADA ) 75 150 mg/day ( ) ( ) ( Stroke ) ( Dosage ) ( Diabetes ) ( Metabolic syndrome ) ( Primary prevention
Flaws, Bias, Misinterpretation and Fraud in Randomized Clinical Trials
 Flaws, Bias, Misinterpretation and Fraud in Randomized Clinical Trials Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical companies
Flaws, Bias, Misinterpretation and Fraud in Randomized Clinical Trials Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical companies
Iroko Pharmaceuticals Receives FDA Approval for VIVLODEX - First Low Dose SoluMatrix Meloxicam for Osteoarthritis Pain
 Iroko Pharmaceuticals Receives FDA Approval for VIVLODEX - First Low Dose SoluMatrix Meloxicam for Osteoarthritis Pain VIVLODEX Developed to Align with FDA NSAID Recommendations Proven Efficacy at Low
Iroko Pharmaceuticals Receives FDA Approval for VIVLODEX - First Low Dose SoluMatrix Meloxicam for Osteoarthritis Pain VIVLODEX Developed to Align with FDA NSAID Recommendations Proven Efficacy at Low
Antiplatelet agents treatment
 Session III Comprehensive management of diabetic patients Antiplatelet agents treatment Chonnam National University Hospital Department of Internal Medicine Dong-Hyeok Cho CONTENTS Introduction Prothrombotic
Session III Comprehensive management of diabetic patients Antiplatelet agents treatment Chonnam National University Hospital Department of Internal Medicine Dong-Hyeok Cho CONTENTS Introduction Prothrombotic
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY. Nick Collins February 2017
 GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
Rimoxen. Rimoxen! "The Gastro and Cardio friendly anti-inflammatory ingredient"
 Rimoxen A Botanical Anti-Inflammatory COX-2 Selective Ingredient Question: How doses Rimoxen compare to the prescription COX-2 inhibitors (Vioxx and Celebrex) and the OTC NSAID pain relievers such as aspirin
Rimoxen A Botanical Anti-Inflammatory COX-2 Selective Ingredient Question: How doses Rimoxen compare to the prescription COX-2 inhibitors (Vioxx and Celebrex) and the OTC NSAID pain relievers such as aspirin
IMMEDIATE DICLOFENAC NEW CONTRAINDICATIONS AND WARNINGS AFTER A EUROPE-WIDE REVIEW OF CARDIOVASCULAR SAFETY
 Finance, EHealth and Pharmaceuticals Directorate Pharmacy and Medicines Division T: 0131-244 2528 E: irene.fazakerley@scotland.gsi.gov.uk 1. Medical Directors 2. Directors of Public Health 3. Directors
Finance, EHealth and Pharmaceuticals Directorate Pharmacy and Medicines Division T: 0131-244 2528 E: irene.fazakerley@scotland.gsi.gov.uk 1. Medical Directors 2. Directors of Public Health 3. Directors
RISK MANAGEMENT PLAN (RMP) PUBLIC SUMMARY ETORICOXIB ORION (ETORICOXIB) 30 MG, 60 MG, 90 MG & 120 MG FILM-COATED TABLET DATE: , VERSION 1.
 PUBLIC SUMMARY ETORICOXIB ORION (ETORICOXIB) 30 MG, 60 MG, 90 MG & 120 MG FILM-COATED TABLET DATE: , VERSION 1.") RISK MANAGEMENT PLAN (RMP) PUBLIC SUMMARY ETORICOXIB ORION (ETORICOXIB) 30 MG, 60 MG, 90 MG & 120 MG FILM-COATED TABLET DATE: 07-10-2016, VERSION 1.2 VI.2 Elements for a Public Summary Etoricoxib Orion
RISK MANAGEMENT PLAN (RMP) PUBLIC SUMMARY ETORICOXIB ORION (ETORICOXIB) 30 MG, 60 MG, 90 MG & 120 MG FILM-COATED TABLET DATE: 07-10-2016, VERSION 1.2 VI.2 Elements for a Public Summary Etoricoxib Orion
Dental Management Considerations for Patients on Antithrombotic Therapy
 Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
& Cardiovascular Risk
 Non Steroideal Antinflammatory Drugs & Cardiovascular Risk Andrea Fanelli U.O. Anestesia e Medicina Perioperatoria Istituti Ospitalieri di Cremona NSAIDs NSAIDsare widely used since they are indicated
Non Steroideal Antinflammatory Drugs & Cardiovascular Risk Andrea Fanelli U.O. Anestesia e Medicina Perioperatoria Istituti Ospitalieri di Cremona NSAIDs NSAIDsare widely used since they are indicated