Pitfalls of doing ANA immunofluorescence Can we define false positive? Can we define false negative? Can results be compared between labs?
|
|
|
- Naomi Cannon
- 6 years ago
- Views:
Transcription
1 Pitfalls of doing ANA immunofluorescence Can we define false positive? Can we define false negative? Can results be compared between labs? Amsterdam March 2011
2 Background: HEp-2 IIF Current literature and reports from laboratories on different IIF HEp-2 cell staining patterns is commoly use often rather primitive terms e.g. Homogeneous ANA Speckled ANA Nucleolar ANA Mitotic spindle staining Cytoplasmic staining Can not be linked with a disease phenotype!
3 Proposed taxonomy of HEp-2 cell staining patterns elaborated in our EU CANTOR project Membranous nuclear patterns: Smooth membranous nuclear Punctate membranous nuclear Nucleoplasmic patterns: Homogeneous nucleoplasmic Large speckled nucleoplasmic Coarse speckled nucleoplasmic Fine speckled nucleoplasmic Fine grainy nucleoplasmic Pleomorphic speckled (PCNA) Centromere Multiple nuclear dots Coiled bodies (few nuclear dots) Nucleolar patterns: Homogeneous nucleolar Clumpy nucleolar Punctate nucleolar Spindle apparatus patterns: Centriole (centrosome) Spindle pole (NuMa)(MSA-1) Spindle fibre Midbody (MSA-2) CENP-F (MSA-3) Cytoplasmic patterns: Diffuse cytoplasmic Fine speckled cytoplasmic Mitochondrial-like Lysosomal-like Golgi Contact proteins Vimentin-like Negative Undeterminable Wiik A. et al. J.Autoimmun. 2010
4 IIF staining patterns on HEp-2 cell substrate. Membranous nuclear patterns: Smooth membranous nuclear Punctate membranous nuclear Nucleoplasmic patterns: Homogeneous nucleoplasmic pattern Large speckled nucleoplasmic Coarse speckled nucleoplasmic Fine speckled nucleoplasmic Fine grainy Scl-70 like nucleoplasmic Pleomorphic speckled (anti- PCNA) Centromere Multiple nuclear dots Coiled bodies (few nuclear dots) Nucleolar patterns: Homogeneous nucleolar Clumpy nucleolar Punctate nucleolar Spindle apparatus patterns: Centriole (centrosome) Spindle pole (NuMa)(MSA-1) Spindle fibre Midbody (MSA-2) CENP-F (MSA-3) Cytoplasmic patterns: Diffuse cytoplasmic Fine speckled cytoplasmic Mitochondrial-like Lysosomal-like All of these have clinical Golgi-like Contact proteins associations with signs and features! Vimentin-like Negative Undeterminable
5 IIF versus different solid phase assays Membranous nuclear patterns: Smooth membranous nuclear Punctate membranous nuclear Nucleoplasmic patterns: Homogeneous nucleoplasmic pattern Large speckled nucleoplasmic Coarse speckled nucleoplasmic Fine speckled nucleoplasmic Fine grainy Scl-70 like nucleoplasmic Pleomorphic speckled (anti- PCNA) Centromere Multiple nuclear dots Coiled bodies (few nuclear dots) Nucleolar patterns: Homogeneous nucleolar Clumpy nucleolar Punctate nucleolar All of these have clinical symptom associations! Spindle apparatus patterns: Centriole (centrosome) Spindle pole (NuMa)(MSA-1) Spindle fibre Midbody (MSA-2) CENP-F (MSA-3) Cytoplasmic patterns: Diffuse cytoplasmic Fine speckled cytoplasmic Mitochondrial-like Lysosomal-like Golgi-like Contact proteins Vimentin-like Negative Undeterminable But- most of the antigens have not been isolated and antibody specificity cannotbe determined by other routine techniques!
6 Why use HEp-2 cells for the screening technique? Only intact permeable cells contain all the relevant autoantigens in situ and cells can be seen in different stages of division. But the reactivity with autoantibodies depends on whether the right conformational state of the antigen has been preserved. Morphological recognition of HEp-2 cell staining patterns using one good HEp-2 cell substrate is a natural talent of many people: The European multicenter study (CANTOR) proved that! Autoantigen mixtures coated on solid phase supports (ELISA plates, beads, arrays etc.) are unsuited for recognition of a number of diagnostically important single autoantigens.
7 Relative percentage of positive results using ELISA screen vs. IIF HEp-2cell screen HEp-2 cells: set at 100% ELISA An example: SSA, SSB, Scl- 70, CENP-B, U1RNP, U1RNP/Sm, Jo-1, histones, dsdna, ribosomal P, PM- Scl, fibrillarin, PCNA, Mi-2 Some assays: additionally contain cell extract of HEp-2 cells Solid phase assays like ELISA thus contain a limited no. of autoantigens (10-14). But- these targets are wellknown for their clinical associations with inflammatory rheumatic diseases and therefore % of sera that are positive for ANA by IIF test are also positive by ELISA screen.. Some exceptions: JCA, DM/PM, SSc
8 Percentage of autoantigens in HEp-2 cell testing positive by screen ELISA Nuclear and cytoplasmic targets seen by IIF HEp-2 cell screen (set at 100%) Relative percentage of IIF nuclear and cytoplasmic targets detected by composite ELISA: (about 10-15%!) Many of these IIF staining patterns have well-known clinical associations!
9 Screening for ANA using IIF technique versus composite solid phase assay SJS SLE SSC MCTD PM/DM JCA dsdna U1RNP SSA/B Each column represents IIF ANA positive sera The bar shows the % sera found positive by ELISA
10 Indirect immunofluorescence Very sensitive Clinically meaningful cut-off setting is crucial! How do you determine such cut-off? F Broad screening potential Fluorescence - Fluorochrome conjugate ANA HEp-2 cell



11 Five main HEp-2 cellular regions Nuclear envelope Nucleoplasm Nucleoli Mitotic spindle Cytoplasm
12 Computer-assisted project to attain an agreed HEp-2 cell nomenclature: the EU-supported CANTOR project ( ) Aim: To attempt to bring order out of HEp-2 cell terminological and conceptual chaos To harmonize existing nomenclature using previous terms supplemented by description of visual characteristics as illustrated on agreed reference images To supplement terms with the exact location of the stained structure(s) when necessary To set up a rational taxonomy for the terms Wiik et al. 2010, J Autoimmun
13 Substrate and images used All images had to be classified at two magnifications: 200 x and 400 x. All slides derived from one carefully selected batch of HEp-2 cell slides from one provider. All laboratories used the same conjugate specific for human γ-chains (DAKO, Glostrup, DK). All laboratories used incident light illumination microscopes with objectives possessing high numerical apertures for bright conjugate excitation
14 Initial harmonization of terms The three expert centres digitized images found by routine testing and brought them to sessions where 5 experts first judged them with regard to photographic quality Images that were assumed to represent prototype staining patterns were selected as accepted reference patterns for the CANTOR study Positive and negative staining characteristics were noted down and gradually agreed upon as new proposed and accurate descriptions of each pattern for the study Each pattern was given a name that did not overlap with any other terms used among others stating the location of the staining if that was felt needed (nucleus, cytoplasm, mitotic spindle apparatus etc.)


15 Example of reference image display Large speckled nucleoplasmic pattern ( nuclear matrix ) 200 X 400 X


16 Another example Coarse speckled nucleoplasmic pattern 200 X 400 X


17 Two rather similar IIF patterns 400 x 400 x Meta-phase chromatin plate negative Smooth membranous nuclear Punctate membranous nuclear
18 Example of textual help: Nuclear membrane staining patterns Smooth membranous staining pattern: -A smooth homogeneous ring-like fluorescence of the nuclear membrane in interphase cells. -Some samples with strong fluorescence may give an impression of whole nuclear staining -A similar pattern is seen in the telophase cells. -In metaphase cells the fluorescence is diffusely localized in the cytoplasm, and chromosomal material is unstained. Punctate membranous staining pattern: -A discontinuous punctate fluorescence along the nuclear membrane. -On focusing through the nucleus the punctate staining can be seen on the surface of the entire nucleus. -A similar pattern is seen in telophase. -In metaphase the fluorescence is diffusely localized throughout the cytoplasm. -Some samples with strong antibodies may give an impression of whole nuclear staining.
19 Local and merged data All data from each classification and each participant in each laboratory were recorded on local computers using the DOORS software and later merged into one common database. It was now possible to compare intra- and interobserver variability between persons, groups and laboratories, calculate and compare kappa values between individuals, groups and laboratories using perceptometric tools of the software. Expert classifications earlier agreed on (facit list) served as the key answers
20 Sessions in the CANTOR project Phases: Inexper: Experienced: Experts: Education 29 ref. Images 29 ref. images N.A. Baseline 40 images 40 images 40 images Training 1 45 images 45 images 45 images Training 2 45 images 45 images 45 images Training 3 45 images 45 images 45 images Exam 40 images 40 images 40 images Between introduction of reference images, baseline test and the 3 training sessions graphic and statistical tools were used to illustrate results measured as a mean against the experts.
21 Kappa Learning effect by computer-assisted Delphi round training with software Kappa value at start of course Kappa value at end of course Participants T E E T E T T N T N T N T= trained, E= experienced, Non-experienced

22 Homogeneous nucleoplasmic pattern Reflex tests Lab.test: SLE, RA, JCA Chromatin constituents: dsdna, histones, nucleosomes, HMGs Anti-dsDNA Anti-histone Anti-nucleosome Farr assay, Crithidia IF ELISA Line IA ELISA Line IA ELISA Line IA SLE? DI-LE? SLE? Anti-HMG At present: no assay JCA? Note that the choice of assay technique for anti-dsdna has a strong influence on the value for clinical interpretation and use!!!
23 Pitfalls Homogeneous: some staining shows pos., others neg. nucleoli. The latter was named quasi-homogeneous recently. Both are associated with infl.rheum.dis. And are chromatin pos. Some staining is reminiscent of this with pos. chromatin plates, but gives a very fine dense speckled pattern, directed to LEDGF. Mariz et al A+R. Many classify anti-topo 1 (anti-scl 70) as homogeneous with pos. nucleoli and pos. chromatin, though the pattern is fine grainy.

24 Anti-LEDGF: dense fine speckled nucleoplasmic staining pattern Mostly healthy individuals No reflex test available yet
25 Pitfalls ctd. Large speckled staining is difficult to distinguish from coarse speckled, but the antigenic targets (hnrnps, vs. spliceosomes) and the disease associations different.
26 Coarse granular nucleoplasmic pattern MCTD, SLE Assemblyosome constituents: Smith antigen U1RNP Reflex tests: line-blot, ELISA, haemagglutination

27 Fine granular nucleoplasmic p. Sjögren s syndrome, congenital heart block, SLE, dermatomyositis, healthy individuals SSA/Ro, SSB/La, Mi-2? LEDGF? Reflex tests: ELISA, line blot Reflex tests: RI Precipit. At present no assay

28 Anti-Mi-2 antibodies: intermediate - fine speckled Reflex testing: Radio-immunoprecipitation Dermatomyositis
29 Control line: IgG SmB SmD RNP-70 RNP-A RNP-C Ro 52 SSA/Ro 60 SSB/La CENP-B Scl-70 Jo-1 Ribo P Histones Conjugate Serum + conjugate Line immuno-assay
30 Some examples of HEp-2 cell staining patterns and their most likely relationship to cell biochemistry and diagnostic entities Pattern Disease Biochemistry Most likely not recognized in a solid phase presentation of mixed autoantigens
31 Smooth membranous pattern SLE,sero-negative RA Sjögren s syndrome Anti-phospholipid syndrome Lamins ABC Integral membrane proteins Note chromosomes

32 Punctate membranous pattern Primary biliary cirrhosis Nuclear pore complexes

33 Pleomorphic nuclear pattern (PCNA) SLE, SjS DNA polymerase delta auxiliary protein

34 Multiple nuclear dots Primary biliary cirrhosis SLE PML* body constituents: Sp-100, PML protein, 56K * Pro-myelocytic leukemia

35 Spindle fibre pattern SLE HsEg 5
 Centromere protein F Note zipperlike staining Note different")
36 CENP-F pattern Malignancies (breast, lung, NHL, > 50 %.) Centromere protein F Note zipperlike staining Note different staining intensity
 antibodies: Indicate Ataxia 30% -CENP-F")

37 Less common staining patterns (Examples of esoteric antibodies ) -Antibodies to Golgi complex: 6 known antigens Indicate SjS 60%, SLE 20 % Ataxia 5% -Antibodies to GW bodies: 8 known antigens Indicate SjS 40%, Ataxia 35%, PBC 10% -PCNA antibodies: Indicate SLE 40%, other autoimmunity 60% -Early endosome (EEA-1) antibodies: Indicate Ataxia 30% -CENP-F antibodies: 1 known large 367 kda molecule (mitosin) Indicate malignancies: 50-70% (breast, lung, NHL) -Centrosome antibodies: 6 known antigens Indicate SjS, SLE. -Intracellular exosome antibodies: 7 known antigens Indicate polymyositis/scleroderma overlap, Scleroderma, RA -Nuclear envelope antibodies: 5 known antigens Indicate non-erosive RA, SLE, SjS, CAH
!")
38 Negative Please note that: -A negative ANA result does not exclude presence of SLE or another autoimmune disease! -Anti-SSA/Ro and anti-jo-1 are often not seen by use of several HEp-2 cell substrates (depends on fixation technique)! -Positive cytoplasmic staining is often called a negative result!
39 What are the clinical aspects? Some ANA have well-known clinical associations, but the target antigen specificity needs to be revealed by techniques other than IIF (ELISA, bead assays, chip assays, immunodiffusion etc). Some ANA have less clear-cut clinical utility, mainly because only modest efforts have been spent to harmonize their recognition by IIF and study their antigen specificity by independent techniques, and thus sufficiently large populations of patients have not been available for detailed clinical analyses. Some ANA are very rare [ esoteric ] (<5%) and thus have not been focused on because they were considered clinically insignificant although there is no basis for this assumption. The present concept is that all ANA have clinically significant associations when large cohorts are studied, but that demands set up of co-ordinated multi-centre studies.
40 Autoantibody conundrum: clinical value of esoteric autoantibodies. Studies of disease cohorts indicate low frequency (<5%) of antibodies to CENP-F, PCNA, NuMA, HsEG5, GW bodies, Golgi, early endosomes (EEA-1), PML bodies, coiled bodies But- Studies of serological cohorts of positive sera show a high frequency of certain autoimmune syndromes e.g.: Antibodies to PCNA, NuMA, HsEg5, GW, Golgi, EEA-1 indicate presence of SLE or SjS PML antibodies indicate PBC in 35% of cases! Anti-CENP-F indicates malignancies in 50-80% of cases! Antibodies to Golgi, GW bodies, early endosomes indicate ataxia in a high percentage of cases.
41 Phenotypes of SLE: relation to serum autoantibodies Anti-ribosomal RNP: active systemic lupus with CNS involvement Anti-PCNA: Mostly SLE without a known phenotype Anti-spindle fibre: Mostly SLE or SjS without a known phenotype Anti-phospholipid: Mostly SLE with a propensity to develop arterial or venous thromobosis Anti-SSA/B: active cutaneous lupus, often with secondary SjS Anti-U1RNP: systemic lupus with myositis, RP, ILD and/or overlap SSc Anti-dsDNA: active systemic lupus, mostly with anaemia, nephritis Anti-C1q: active systemic lupus, mostly with lupus nephritis
42 Clinical phenotypes of myositis: from antibody to most likely manifestations Fine speckled nucleoplasmic (Mi-2): clinical signs of proximal myositis plus skin abnormalities compatible with dermato-myositis, histological myositis, increased mm. enzymes and typical electro-myographic changes. Coarse speckled nucleoplasmic (U1RNP): clinical signs of proximal myositis, histological and electro- myographic findings compatible with polymyositis, increased mm. enzymes, often signs of overlap myositis. Homogeneous nucleolar (PM/Scl): clinical signs of proximal myositis, histological and electro-myographic findings compatible with polymyositis, increased mm. enzymes. Sometimes also signs of scleroderma overlap myositis syndrome. Diffuse cytoplasmic (Jo-1, PL-7, PL-12 and others): clinical signs of proximal myositis, histological and electr-myographic findings compatible with polymyositis, increased mm. Enzymes, and often anti-synthetase syndrome (Raynaud s, mechanic s hands, interstitial lung disease, arthritis. Mitochondrial-like cytoplasmic (SRP): Proximal and distal myositis with histological necrotizing myositis and electro-myographic changes.
43 Clinical phenotypes in scleroderma: from manifestations to autoantibody. 5 year survival: Limited SSc with anti-centromere Ab.: 86% CREST symptoms, digital ulcers/digital loss, pulmonary hypertension, primary biliary cirrhosis, Caucasians. Limited SSc with anti-th/to Ab.: 65% Puffy fingers, intestinal involvement, pulmonary hypertension, often associated with hypothyroidism. Overlap SSc with anti-pm/scl. Ab.: 92% Limited skin disease, polymyositis, calcinosis, digital ulcers. Overlap SSc with anti-u1rnp Ab.: 95% Limited SSc, polymyositis, pulmonary fibrosis, pulmonary hypertension, cardial involvement. Diffuse SSc with anti-scl-70 Ab.: 80% pulmonary fibrosis, tendon rubs, digital ischemia, sometimes heart and kidney involvement. Diffuse SSc with anti-u3-rnp Ab.: 77% Digital ulcers, pulmonary hypertension, pulmonary fibrosis, African-Americans Diffuse SSc with anti-rna polymerase Abs.: 90% acute onset, renal crisis, tendon rubs, arthritis, arterial hypertension
44 Conclusions. ANA likely reflect tissue lesion mechanisms, genetic influences, and perhaps etiology, ANA are linked to diagnosis, subsyndrome/ phenotype, manifestations, and prognosis, May help planning of follow-up and therapy, Have particular value in early disease forms, Can best be revealed by IIF HEp-2 assay, Many esoteric auto-abs are important, ANA can be interpreted by many technicians, Optimal use of ANA results depends on a close collaboration between clinics and labs.
45
46 Autoantibodies to citrullinated proteins (ACPA) and diagnosis of patients with rheumatoid arthritis (RA): Genetic, clinical, technical, and epidemiologic aspects

47 Early synovitis in RA?
48 Clinical aspects: RA The disease progresses quickly from a predominantly immmunoinflammatory to a destructive phase where established pannus erodes bone, tendons and joint capsule. The therapeutic window to get control of the early phase is very short (few months), and later conventional therapy has little or no effect on the destructive phase.
49 Diagnostics of chronic inflammatory arthritides -Clinical history -Manifestations -Clinical examination -Radiological signs -Specialist evaluations -Histopathology -Immunopathology -Laboratory tests to look for inflammation -Immunoglobulin levels -Complement activation -Autoantibodies Clinical basis for setting a tentative diagnosis Clinical basis for setting a tentative prognosis
50 Criteria-based early diagnostics Criteria = rigorously defined items Clinical symptom 3: rheumatoid nodules Clinical symptom 1: morning stiffness Not present Clinical symptom 2: bone erosions? Not found yet Specific serologic result: Anti-CCP Diagnosis and Prognosis Particular importance: clinical focus!
51 Differential diagnostics in the clinic and the laboratory Healthy INF OA SLE RA ASp PsA Background Not really useful for differential diagnostics Differential diagnostic patients (signs, symptoms, simple biochemistry, radiology) Great importance for differential diagnostics
52 Differential diagnostics RA Rheumatoid arthritis Small joints Symmetric arthritis Rheumatoid nodules Erosive lesions in joints Rheumatoid factors Anti-CCP (ACPA) PsA Psoriatic arthritis: Larger joints Asymmetric arthritis No nodules Bone destruction occur Rarely rheumatoid factors Anti-CCP (ACPA) rare
53 Prevalence of Anti-CCP and IgM RF in some arthritic conditions INF OA RA PsA Healthy SLE ASp Background Sens. 1-2% 2-10% 1-3% 2-50%! 6-8% 70-80% 6-16% Anti- CCP 5-10% 70-80% 5-20% 5-10% IgM RF Spec. ~ 95%!
54 RF in some non-ra disorders Mixed Cryoglobulinaemia 100% Sjögren's syndrome 60-70% Systemic sclerosis 20 30% Systemic lupus erythematosus 15 35% Polymyositis/dermatomyositis 5 10% Many viral infections! hepatitis B, parvo B19, rubella, mosquitoborne alpha-viruses Healthy individuals 2 10%* * Depends on cut-off setting, age, and F/M ratio
55 Citrullination of arginines in proteins taking place during cell death (apoptosis) H O H O N peptidylarginine deiminase (PAD) N NH Ca mol. NH H 2 N+ NH 2 O NH 2 L-arginine residue (+ charged) L-citrulline residue (neutral) Especially gly/arg - ser/arg repeat motifs are modified
56 Cyclic Citrullinated Peptide: CCP An artificial mimotope cfc1-cyc HQCHQESTXGRSRGRCGRSGS Cyclisation of the peptide enhances its recognition by RA autoantibodies Schellekens et al. Arthritis Rheum 2000, 43:
57 How do synovial antigens become modified: arginine to citrullin? Peptidyl-arginine deiminase enzymes (PAD2 and PAD4) are richly represented in monocytes, macrophages and neutrophils When these cells undergo apoptosis Ca++ ions are permeating into the cells and activate PADs Ca++ concentration in normal cells ~10-7M Threshold for PAD enzyme activity ~10-5M PAD enzymes most likely also act on the enzyme-containing cells themselves (Monos,MФs,PMNs)
58 Association between anti-ccp production and shared epitope HLA DR typing and anti-ccp2 antibodies were studied in 268 RA patients from an early arthritis clinic cohort in Leiden. Radiographic disease progression was measured over 4 years. Carriers of shared epitope DRB1 alleles were more commonly anti-ccp positive than non-carriers (OR 13.3) and also showed the most pronounced radiographic progression. (van Gaalen FA et al.:arthritis Rheum 50: ,2004). Shared epitope-encoding alleles are associated with anti- CCP production, not with RA as such! (Huizinga T et al.: Arthritis Rheum 52: , 2005).
59 Anti-citrullin peptide antibodies, IgM and IgA rheumatoid factors can appear up to 10 to 18 years before the onset of clinical symptoms of RA!!!
60 Production of anti-ccp in RA Anti-CCP level U/ml Cut-off value Detection limit Onset of first clinical symptoms Diagnosis Stable phenotype Time (Years)
61 Genes and environment: tobacco smoking A: Sero-positive RA B: Sero-negative RA Figure 2 Relative risk (RR) for development of rheumatoid arthritis (RA) in current smokers (with different numbers of copies (0-2) of the shared epitope (SE) of HLA-DR) compared with never smokers. (A) RR for seropositive RA and (B) RR for seronegative RA. These graphs are schematic representations of the original data from a case-control study of RA reported in reference 9. Copyright 2004 BMJ Publishing Group Ltd. Klareskog, L et al. Ann Rheum Dis 2004;63:ii28-31ii
62 Genetic and environmental factors in the development of RA Figure 3 Schematic outline of how aetiological studies as well as interventions in the pathways leading to rheumatoid arthritis (RA) should be undertaken before onset of clinical signs of RA. CCP, cyclic citrullinated peptide; RF, rheumatoid factor; SE shared epitope. Klareskog, L et al. Ann Rheum Dis 2004;63:ii28-31ii Copyright 2004 BMJ Publishing Group Ltd.
63 Risk factors in RA. Recent study in 515 Danish RA patients and 769 sex- and age-matched controls Risk factors in anti-ccp positive RA patients: -menarche at = or >15 years of age (OR 1.87) -tobacco smoking (both sexes): confirmed, both former and current smokers, dose dependent effect -coffee consumption > 10 cups/day (OR 2.75) -alcohol consumption > 15 drinks/week (OR 0.58) -moderately demanding exercise (OR 0.51) -pets as adult (ever) (OR 0.73) Pedersen M et al..: Arthritis Res Ther 2006
64 Risk factors in RA Risk factors in anti-ccp negative RA patients: The strongest risk factor was increased body mass index 10 years before the study: -obese (BMI = or >30 kg/m²) (OR 9.79*) -moderate (BMI kg/m², OR 3.53*) *compared to underweight (<18.5 kg/m²) -menarche = or >15 years of age (OR 2.27) -pets (ever) (OR 0.65) -moderately demanding exercise (OR 0.69) Pedersen M et al.: Arthritis Res Ther, 2006
65 Studies done on anti-citrulline antibodies are difficult to compare The citr. antigens are very different The cut-offs used are different The RA populations studied are different The differential diagnostic populations studied for comparison with RA patients are different Some studies include undifferentiated arthritis, palindromic syndrome, RF+JRA, RF+psoriatic arthritis etc. all of which may actually become RA.
66 Nosographic sensitivity (sensitivity in RA patients) Anti-CCP, anti-filaggrin and APF show very similar sentivities: - at diagnosis < 6 months: around 50% - at diagnosis 1 year: around 60% - at diagnosis >2 years: around 70% AKA and anti-sa: usually show lower sensitivity than the above methods
67 Anti-CCP in RA Data collected from 154 studies between 2002 and June AR & T 2010
68 Cut-off setting between sera from RA patients and immuno-inflammatory disease controls. Sensitivity 75% This study compares a RA population vs. differential diagnostic populations If such cut-off setting has been done by the developer there is less need for a study of inhouse immuno-inflammatory disease controls. Chosen specificity Clinical diagnostics need high differential diagnostic specificity! 98% 90% 1 - specificity
69 100% How do you choose the optimal assay? Use the same disease population as comparator for each assay! Sensitivity 77% 70% Choice: blue assay! Since this has the highest sensitivity 50% 65% Chosen specificity AUC high AUC intermediate AUC low Test of 3 ACPA assays Clinical diagnostics need high differential diagnostic specificity! 98% 90% 1 - specificity
70 Test of specificity and sensitivity in RA vs.controls using 3 different assays Bizzaro 100/ Coenen 102/ Damjanovska 566/ Dejaco 164/ n.d Innala 210/ Mutlu 93/ Soos 119/ n.d Van der Cruyssen Van der Cruyssen Van der Cruyssen RA/control Specific. Sens: CCP2 CCP3 MCV 272/ n.d. n.d. 92/ n.d. 180/ n.d. Average: Note: Controls are not identical and stratification only approximated!
71 Comparison of ACPA in terms of positive and negative predictive values. CCP 2 CCP 3 MCV RF Study: Pts/con: PPV: NPV: PPV: NPV: PPV: NPV: PPV: NPV 1 124/ / / / / / / / / / Average:
72 Conclusions Anti-citrullinated protein/peptide antibodies (ACPA) are very specific markers for RA, also useful for differential diagnostics towards other polyarthritides but small subpopulations of other arthritides are ACPA-pos. too! Cyclic citrullinated peptide 2 (CCP2) acts as a sensitive artificial mimotope for ACPA antigens in solid phase assays. Anti-CCP antibodies are present very early in disease, sometimes before inflammation biomarkers rise and before clinical onset of arthritis is recognized. Anti-CCP levels can decrease somewhat with remission induction and increase a little with disease exacerbation, somewhat parallel to but smaller than RF changes.
73 Conclusions ctd. High levels of anti-ccp antibodies are prognostic for an erosive disease course, not only in adult RA. Anti-CCP antibodies prevail in RA patients carrying the HLA-DR4 shared epitope, most of which are RF-positive. Anti-CCP is found in about ¼ of RF-negative RA patients, and these patients run an erosive course. Several environmental factors influence the onset of anti- CCP positive RA (tobacco smoking, coffee consumption, body mass index, alcohol consumption, exercise).
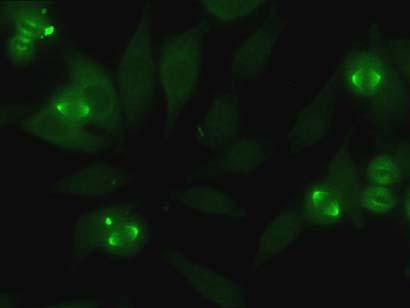
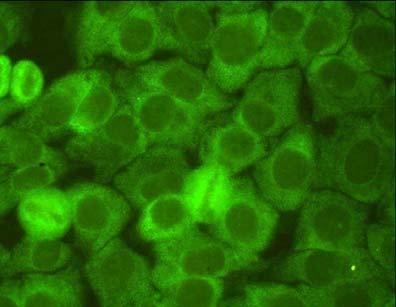
Autoantibodies giving rise to cytoplasmic IIF staining using HEp-2 cell substrate
 Autoantibodies giving rise to cytoplasmic IIF staining using HEp-2 cell substrate Some associations of anticytoplasmic antibodies with clinical diagnoses and features HEp-2 IIF: the gold standard for ANA
Autoantibodies giving rise to cytoplasmic IIF staining using HEp-2 cell substrate Some associations of anticytoplasmic antibodies with clinical diagnoses and features HEp-2 IIF: the gold standard for ANA
Clinical Laboratory. [None
 Clinical Laboratory Procedure Result Units Ref Interval Accession Collected Received Double-Stranded DNA (dsdna) Ab IgG ELISA Detected * [None 18-289-900151 Detected] Double-Stranded DNA (dsdna) Ab IgG
Clinical Laboratory Procedure Result Units Ref Interval Accession Collected Received Double-Stranded DNA (dsdna) Ab IgG ELISA Detected * [None 18-289-900151 Detected] Double-Stranded DNA (dsdna) Ab IgG
Clinical Laboratory. 14:42:00 SSA-52 (Ro52) (ENA) Antibody, IgG 1 AU/mL [0-40] Oct-18
![Clinical Laboratory. 14:42:00 SSA-52 (Ro52) (ENA) Antibody, IgG 1 AU/mL [0-40] Oct-18](/thumbs/95/125595183.jpg "Clinical Laboratory. 14:42:00 SSA-52 (Ro52) (ENA) Antibody, IgG 1 AU/mL [0-40] Oct-18") Clinical Laboratory Procedure Result Units Ref Interval Accession Collected Received Rheumatoid Factor
Clinical Laboratory Procedure Result Units Ref Interval Accession Collected Received Rheumatoid Factor
Clinical Laboratory. 14:41:00 Complement Component 3 50 mg/dl Oct-18
 Clinical Laboratory Procedure Result Units Ref Interval Accession Collected Received Thyroid Peroxidase (TPO) Antibody 5.0 IU/mL [0.0-9.0] 18-289-900139 16-Oct-18 Complement Component 3 50 mg/dl 18-289-900139
Clinical Laboratory Procedure Result Units Ref Interval Accession Collected Received Thyroid Peroxidase (TPO) Antibody 5.0 IU/mL [0.0-9.0] 18-289-900139 16-Oct-18 Complement Component 3 50 mg/dl 18-289-900139
Autoantibodies panel ANA
 Autoantibodies panel ANA Anti-nuclear antibodies, ANA screening General: Anti-nuclear antibodies (ANA) contain all kinds of autoantibodies against nuclear antigens. Their targets are cell components in
Autoantibodies panel ANA Anti-nuclear antibodies, ANA screening General: Anti-nuclear antibodies (ANA) contain all kinds of autoantibodies against nuclear antigens. Their targets are cell components in
Tools to Aid in the Accurate Diagnosis of. Connective Tissue Disease
 Connective Tissue Disease Tools to Aid in the Accurate Diagnosis of Connective Tissue Disease Connective Tissue Disease High quality assays and novel tests Inova offers a complete array of assay methods,
Connective Tissue Disease Tools to Aid in the Accurate Diagnosis of Connective Tissue Disease Connective Tissue Disease High quality assays and novel tests Inova offers a complete array of assay methods,
Budsakorn Darawankul, MD. Maharat Nakhon Ratchasima Hospital
 Budsakorn Darawankul, MD. Maharat Nakhon Ratchasima Hospital Outline What is ANA? How to detect ANA? Clinical application Common autoantibody in ANA diseases Outline What is ANA? How to detect ANA? Clinical
Budsakorn Darawankul, MD. Maharat Nakhon Ratchasima Hospital Outline What is ANA? How to detect ANA? Clinical application Common autoantibody in ANA diseases Outline What is ANA? How to detect ANA? Clinical
Autoantibodies in the Idiopathic Inflammatory Myopathies
 Autoantibodies in the Idiopathic Inflammatory Myopathies Steven R. Ytterberg, M.D. Division of Rheumatology Mayo Clinic Rochester, MN The Myositis Association Annual Conference St. Louis, MO Sept. 25,
Autoantibodies in the Idiopathic Inflammatory Myopathies Steven R. Ytterberg, M.D. Division of Rheumatology Mayo Clinic Rochester, MN The Myositis Association Annual Conference St. Louis, MO Sept. 25,
Test Name Results Units Bio. Ref. Interval
 135091662 Age 45 Years Gender Male 29/8/2017 120000AM 29/8/2017 100215AM 29/8/2017 110825AM Ref By Final RHEUMATOID AUTOIMMUNE COMREHENSIVE ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF), SERUM ----- 20-60
135091662 Age 45 Years Gender Male 29/8/2017 120000AM 29/8/2017 100215AM 29/8/2017 110825AM Ref By Final RHEUMATOID AUTOIMMUNE COMREHENSIVE ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF), SERUM ----- 20-60
Test Name Results Units Bio. Ref. Interval
 LL - LL-ROHINI (NATIONAL REFERENCE 135091593 Age 25 Years Gender Male 30/8/2017 91600AM 30/8/2017 93946AM 31/8/2017 84826AM Ref By Final COLLAGEN DISEASES ANTIBODY ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF),
LL - LL-ROHINI (NATIONAL REFERENCE 135091593 Age 25 Years Gender Male 30/8/2017 91600AM 30/8/2017 93946AM 31/8/2017 84826AM Ref By Final COLLAGEN DISEASES ANTIBODY ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF),
University of Pretoria
 University of Pretoria Serodiagnostic Procedures Performed in the Department of Immunology Dr Pieter WA Meyer 1.Autoimmune Diseases Automated Anti-nuclear antibodies Anti-gliadin/ tissue transglutaminase
University of Pretoria Serodiagnostic Procedures Performed in the Department of Immunology Dr Pieter WA Meyer 1.Autoimmune Diseases Automated Anti-nuclear antibodies Anti-gliadin/ tissue transglutaminase
The Power of the ANA. April 2018 Emily Littlejohn, DO MPH
 Emergent Rheumatologic Diseases and Disorders for Primary Care. The Power of the ANA April 2018 Emily Littlejohn, DO MPH Question 1: the ANA test is: A) A screening test with high specificity to diagnose
Emergent Rheumatologic Diseases and Disorders for Primary Care. The Power of the ANA April 2018 Emily Littlejohn, DO MPH Question 1: the ANA test is: A) A screening test with high specificity to diagnose
ANA Diagnostics Using Indirect Immunofluorescence
 ANA Diagnostics Using Indirect Immunofluorescence EUROIMMUN D-23560 Luebeck (Germany) Seekamp 31 Tel +49 45158550 Fax 5855591 E-mail euroimmun@euroimmun.de Table of Contents Autoantibodies against cell
ANA Diagnostics Using Indirect Immunofluorescence EUROIMMUN D-23560 Luebeck (Germany) Seekamp 31 Tel +49 45158550 Fax 5855591 E-mail euroimmun@euroimmun.de Table of Contents Autoantibodies against cell
Test Name Results Units Bio. Ref. Interval
 135091660 Age 44 Years Gender Male 29/8/2017 120000AM 29/8/2017 100219AM 29/8/2017 105510AM Ref By Final EXTRACTABLENUCLEAR ANTIGENS (ENA), QUANTITATIVE ROFILE CENTROMERE ANTIBODY, SERUM 20-30 Weak ositive
135091660 Age 44 Years Gender Male 29/8/2017 120000AM 29/8/2017 100219AM 29/8/2017 105510AM Ref By Final EXTRACTABLENUCLEAR ANTIGENS (ENA), QUANTITATIVE ROFILE CENTROMERE ANTIBODY, SERUM 20-30 Weak ositive
Advances in Autoantibody Testing & Clinical Applications
 Advances in Autoantibody Testing & Clinical Applications Marvin J. Fritzler PhD MD Member: IUIS-WHO-AF-CDC Serology Committee Director: Advanced Diagnostics Laboratory University of Calgary Introduction
Advances in Autoantibody Testing & Clinical Applications Marvin J. Fritzler PhD MD Member: IUIS-WHO-AF-CDC Serology Committee Director: Advanced Diagnostics Laboratory University of Calgary Introduction
Is it Autoimmune or NOT! Presented to AONP! October 2015!
 Is it Autoimmune or NOT! Presented to AONP! October 2015! Four main jobs of immune system Detects Contains and eliminates Self regulates Protects Innate Immune System! Epithelial cells, phagocytic cells
Is it Autoimmune or NOT! Presented to AONP! October 2015! Four main jobs of immune system Detects Contains and eliminates Self regulates Protects Innate Immune System! Epithelial cells, phagocytic cells
ANA Diagnostics Using Indirect Immunofluorescence
 ANA Diagnostics Using Indirect Immunofluorescence EUROIMMUN AG Seekamp 31 23560 Lübeck (Germany) Tel +49 451/ 58 55-0 Fax 58 55-591 info@euroimmun.de www.euroimmun.com Table of contents Autoantibodies
ANA Diagnostics Using Indirect Immunofluorescence EUROIMMUN AG Seekamp 31 23560 Lübeck (Germany) Tel +49 451/ 58 55-0 Fax 58 55-591 info@euroimmun.de www.euroimmun.com Table of contents Autoantibodies
Disclosures. Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies. None
 Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
This month, we are very pleased to introduce some new tests for Scleroderma as well as some test changes to our existing scleroderma tests/panels.
 February 20, 2017 Client Letter Test Update February 2017 Dear Colleague: This month, we are very pleased to introduce some new tests for Scleroderma as well as some test changes to our existing scleroderma
February 20, 2017 Client Letter Test Update February 2017 Dear Colleague: This month, we are very pleased to introduce some new tests for Scleroderma as well as some test changes to our existing scleroderma
Assays. New. New. Combinations. Possibilities. Patents: EP , AU
 Assays Patents: EP 2362222, AU 2011217190 New Combinations New Possibilities Technology Classical Handling of Autoimmune Diagnostics 2-Step Diagnostics 1 st Screening 2 nd Confirmation Cell based IFA ELISA
Assays Patents: EP 2362222, AU 2011217190 New Combinations New Possibilities Technology Classical Handling of Autoimmune Diagnostics 2-Step Diagnostics 1 st Screening 2 nd Confirmation Cell based IFA ELISA
Rhematologic serum testing is: Before request serologic tests, ANCA associated antigens c-anca: most commonly against the proteinase 3 (PR-3)
") thorough P/E. Rhematologic serum testing is: Useful to confirm a clinical impression or sort out a differential diagnosis Not useful as a screening test A positive test may or may not be associated with
thorough P/E. Rhematologic serum testing is: Useful to confirm a clinical impression or sort out a differential diagnosis Not useful as a screening test A positive test may or may not be associated with
VASCULITIS PRODUCT HIGHLIGHTS
 VASCULITIS PRODUCT HIGHLIGHTS AESKU.DIAGNOSTICS offers a comprehensive and complete diagnostic portfolio in the field of vasculitis diagnostics. Not only are screening and profiling s available but also
VASCULITIS PRODUCT HIGHLIGHTS AESKU.DIAGNOSTICS offers a comprehensive and complete diagnostic portfolio in the field of vasculitis diagnostics. Not only are screening and profiling s available but also
Diagnostic and prognostic serological analyses in RA
 9/9/ Diagnostic and prognostic serological analyses in RA Johan Rönnelid Clinical Immunology and Transfusion medicine Akademiska sjukhuset, Uppsala Department of Immunology, Genetics and Pathology Uppsala
9/9/ Diagnostic and prognostic serological analyses in RA Johan Rönnelid Clinical Immunology and Transfusion medicine Akademiska sjukhuset, Uppsala Department of Immunology, Genetics and Pathology Uppsala
Comparison of indirect immunofluorescence and line immunoassay for autoantibody detection
 Comparison of indirect immunofluorescence and line immunoassay for autoantibody detection Y.L. Jeon, M.H. Kim, W.I. Lee, S.Y. Kang Department of Laboratory Medicine, KyungHee University School of Medicine,
Comparison of indirect immunofluorescence and line immunoassay for autoantibody detection Y.L. Jeon, M.H. Kim, W.I. Lee, S.Y. Kang Department of Laboratory Medicine, KyungHee University School of Medicine,
INTERPRETATION OF LABORATORY TESTS IN RHEUMATIC DISEASE
 INTERPRETATION OF LABORATORY TESTS IN RHEUMATIC DISEASE Laboratory tests are an important adjunct in the clinical diagnosis of rheumatic diseases and are sometimes helpful in monitoring the activity of
INTERPRETATION OF LABORATORY TESTS IN RHEUMATIC DISEASE Laboratory tests are an important adjunct in the clinical diagnosis of rheumatic diseases and are sometimes helpful in monitoring the activity of
Interpreting Rheumatologic Lab Tests
 The black hole of medical knowledge: An internist s view of rheumatologic lab tests Interpreting Rheumatologic Lab Tests Jonathan Graf, M.D. Associate Professor of Clinical Medicine University of California,
The black hole of medical knowledge: An internist s view of rheumatologic lab tests Interpreting Rheumatologic Lab Tests Jonathan Graf, M.D. Associate Professor of Clinical Medicine University of California,
Rheumatoid Arthritis. Manish Relan, MD FACP RhMSUS Arthritis & Rheumatology Care Center. Jacksonville, FL (904)
") Rheumatoid Arthritis Manish Relan, MD FACP RhMSUS Arthritis & Rheumatology Care Center. Jacksonville, FL (904) 503-6999. 1 Disclosures Speaker Bureau: Abbvie 2 Objectives Better understand the pathophysiology
Rheumatoid Arthritis Manish Relan, MD FACP RhMSUS Arthritis & Rheumatology Care Center. Jacksonville, FL (904) 503-6999. 1 Disclosures Speaker Bureau: Abbvie 2 Objectives Better understand the pathophysiology
Advances in Laboratory Testing for Rheumatic Diseases Updates in Testing for Rheumatic Diseases. The ABIM s view of rheumatologic lab testing
 The black hole of medical knowledge: An internist s view of rheumatologic lab tests Advances in Laboratory Testing for Rheumatic Diseases 2010 Jonathan Graf, M.D. Assistant Clinical Professor of Medicine
The black hole of medical knowledge: An internist s view of rheumatologic lab tests Advances in Laboratory Testing for Rheumatic Diseases 2010 Jonathan Graf, M.D. Assistant Clinical Professor of Medicine
Atlas of Antinuclear Antibodies
 Fluorescence patterns of cytoplasmic autoantigens There are many important organelles in the cytoplasm which fulfill various functions of the cell as described in section 1. Various autoantibodies, known
Fluorescence patterns of cytoplasmic autoantigens There are many important organelles in the cytoplasm which fulfill various functions of the cell as described in section 1. Various autoantibodies, known
Use of Serological markers for evaluation of patients with Rheumatoid arthritis
 ISSN: 2319-7706 Volume 4 Number 9 (2015) pp. 61-66 http://www.ijcmas.com Original Research Article Use of Serological markers for evaluation of patients with Rheumatoid arthritis G. Sucilathangam*, G.
ISSN: 2319-7706 Volume 4 Number 9 (2015) pp. 61-66 http://www.ijcmas.com Original Research Article Use of Serological markers for evaluation of patients with Rheumatoid arthritis G. Sucilathangam*, G.
Autoimmune diagnostics. A comprehensive product line for the detection of autoantibodies
 Autoimmune diagnostics A comprehensive product line for the detection of autoantibodies Autoimmune diagnostics Autoimmune diseases are chronic inflammatory processes with an indeterminate etiology. They
Autoimmune diagnostics A comprehensive product line for the detection of autoantibodies Autoimmune diagnostics Autoimmune diseases are chronic inflammatory processes with an indeterminate etiology. They
Rheumatologic Lab Tests
 Rheumatologic Lab Tests What the Practitioner Needs to Know Mary Nakamura M.D. 2008 Rheumatologic Lab Tests Are rarely diagnostic of any specific disease If you do not have in mind a rheumatologic disease
Rheumatologic Lab Tests What the Practitioner Needs to Know Mary Nakamura M.D. 2008 Rheumatologic Lab Tests Are rarely diagnostic of any specific disease If you do not have in mind a rheumatologic disease
Comparison of Performance of ELISA with Indirect Immunofluoresence for the Testing of Antinuclear Antibodies
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 12 (2016) pp. 423-427 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.512.046
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 12 (2016) pp. 423-427 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.512.046
What will we discuss today?
 Autoimmune diseases What will we discuss today? Introduction to autoimmune diseases Some examples Introduction to autoimmune diseases Chronic Sometimes relapsing Progressive damage Epitope spreading more
Autoimmune diseases What will we discuss today? Introduction to autoimmune diseases Some examples Introduction to autoimmune diseases Chronic Sometimes relapsing Progressive damage Epitope spreading more
IdentRA test panel with eta. A clinically proven biomarker for earlier, accurate RA diagnosis and now, prognosis and monitoring
 IdentRA test panel with 14-3-3eta A clinically proven biomarker for earlier, accurate RA diagnosis and now, prognosis and monitoring Did you know there are more than 100 forms of arthritis? Every type
IdentRA test panel with 14-3-3eta A clinically proven biomarker for earlier, accurate RA diagnosis and now, prognosis and monitoring Did you know there are more than 100 forms of arthritis? Every type
Association of anti-mcv autoantibodies with SLE (Systemic Lupus Erythematosus) overlapping with various syndromes
 overlapping with various syndromes") International Journal of Medicine and Medical Sciences Vol. () pp. 21-214, June 211 Available online http://www.academicjournals.org/ijmms ISSN 2-972 211 Academic Journals Full Length Research Paper Association
International Journal of Medicine and Medical Sciences Vol. () pp. 21-214, June 211 Available online http://www.academicjournals.org/ijmms ISSN 2-972 211 Academic Journals Full Length Research Paper Association
Anti-CCP2 testing. The Gold Standard in Diagnosis of Rheumatoid Arthritis. 1 of 11 P a g e
 Anti-CCP2 testing The Gold Standard in Diagnosis of Rheumatoid Arthritis 1 of 11 P a g e 2014-01- 07 Contents 1. Scope... 3 2. CCP2: Definition and Background... 3 3. The market for CCP2 assays... 3 4.
Anti-CCP2 testing The Gold Standard in Diagnosis of Rheumatoid Arthritis 1 of 11 P a g e 2014-01- 07 Contents 1. Scope... 3 2. CCP2: Definition and Background... 3 3. The market for CCP2 assays... 3 4.
Thomas A. Medsger, Jr., MD University of Pittsburgh School of Medicine. Disclosures: None
 Thomas A. Medsger, Jr., MD University of Pittsburgh School of Medicine Disclosures: None 4000+ patients enrolled 1972- present; 5+ visits per patient; 20,000+ patient years of follow- up All clinical and
Thomas A. Medsger, Jr., MD University of Pittsburgh School of Medicine Disclosures: None 4000+ patients enrolled 1972- present; 5+ visits per patient; 20,000+ patient years of follow- up All clinical and
Measurement of Antinuclear Antibodies: Assessment of Different Test Systems
 CLINICAL AND DIAGNOSTIC LABORATORY IMMUNOLOGY, Jan. 2000, p. 72 78 Vol. 7, No. 1 1071-412X/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. Measurement of Antinuclear
CLINICAL AND DIAGNOSTIC LABORATORY IMMUNOLOGY, Jan. 2000, p. 72 78 Vol. 7, No. 1 1071-412X/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. Measurement of Antinuclear
Autoantibody Standardizing Committee
 Autoantibody Standardizing Committee Subcommittee for the IUIS Quality Assessment and Standardization Committee Milan, August 25, 2013 Luís Eduardo Coelho Andrade, M.D., Ph.D. Associate Professor Rheumatology
Autoantibody Standardizing Committee Subcommittee for the IUIS Quality Assessment and Standardization Committee Milan, August 25, 2013 Luís Eduardo Coelho Andrade, M.D., Ph.D. Associate Professor Rheumatology
Disclosures. Clinical Approach: Evaluating CTD-ILD for the pulmonologist. ILD in CTD. connective tissue disease or collagen vascular disease
 Disclosures Clinical Approach: Evaluating CTD-ILD for the pulmonologist Industry relationships: Actelion, atyr Pharma, Boehringer-Ingelheim, Genentech- Roche, Gilead Aryeh Fischer, MD Associate Professor
Disclosures Clinical Approach: Evaluating CTD-ILD for the pulmonologist Industry relationships: Actelion, atyr Pharma, Boehringer-Ingelheim, Genentech- Roche, Gilead Aryeh Fischer, MD Associate Professor
Autoimmune (AI) Disorders
 Disorders") Autoimmune (AI) Disorders Affect up to 50 million people in the U.S. 80 100 types, dozens more suspected #2 cause of chronic illness Women are more likely to be affected than men Symptoms overlap and are
Autoimmune (AI) Disorders Affect up to 50 million people in the U.S. 80 100 types, dozens more suspected #2 cause of chronic illness Women are more likely to be affected than men Symptoms overlap and are
Association of Immunofluorescence pattern of Antinuclear Antibody with Specific Autoantibodies in the Bangladeshi Population
 Bangladesh Med Res Counc Bull 2014; 40: 74-78 Association of Immunofluorescence pattern of Antinuclear Antibody with Specific Autoantibodies in the Bangladeshi Population Sharmin S 1, Ahmed S 2, Abu Saleh
Bangladesh Med Res Counc Bull 2014; 40: 74-78 Association of Immunofluorescence pattern of Antinuclear Antibody with Specific Autoantibodies in the Bangladeshi Population Sharmin S 1, Ahmed S 2, Abu Saleh
Undifferentiated Connective Tissue Disease and Overlap Syndromes. Mark S. Box, MD
 Undifferentiated Connective Tissue Disease and Overlap Syndromes Mark S. Box, MD Overlap Syndromes As many as 25% of patients with rheumatic diseases with systemic symptoms cannot be definitely diagnosed
Undifferentiated Connective Tissue Disease and Overlap Syndromes Mark S. Box, MD Overlap Syndromes As many as 25% of patients with rheumatic diseases with systemic symptoms cannot be definitely diagnosed
Autoimmune diseases. SLIDE 3: Introduction to autoimmune diseases Chronic
 SLIDE 3: Introduction to autoimmune diseases Chronic Autoimmune diseases Sometimes relapsing : and remitting. which means that they present as attacks Progressive damage Epitope spreading more and more
SLIDE 3: Introduction to autoimmune diseases Chronic Autoimmune diseases Sometimes relapsing : and remitting. which means that they present as attacks Progressive damage Epitope spreading more and more
Alida R Harahap & Farida Oesman Department of Clinical Pathology Faculty of Medicine, University of Indonesia
 Alida R Harahap & Farida Oesman Department of Clinical Pathology Faculty of Medicine, University of Indonesia Foreign molecules = antigens Immune response Immune system non-specific specific cellular humoral
Alida R Harahap & Farida Oesman Department of Clinical Pathology Faculty of Medicine, University of Indonesia Foreign molecules = antigens Immune response Immune system non-specific specific cellular humoral
What your autoantibodies tell us about your disease. Mark Gourley, MD
 What your autoantibodies tell us about your disease Mark Gourley, MD The Importance of the Immune System Defends us against foreign invaders Self (cancer) and Nonself (virus, bacteria, etc.) But, if the
What your autoantibodies tell us about your disease Mark Gourley, MD The Importance of the Immune System Defends us against foreign invaders Self (cancer) and Nonself (virus, bacteria, etc.) But, if the
Autoantibodies in the Diagnosis of Systemic Rheumatic Diseases
 I Autoantibodies in the Diagnosis of Systemic Rheumatic Diseases Carlos A, von Mfihlen and Eng M. Tan Distinct profiles of autoantibodies directed to intracellular antigens can be detected in the systemic
I Autoantibodies in the Diagnosis of Systemic Rheumatic Diseases Carlos A, von Mfihlen and Eng M. Tan Distinct profiles of autoantibodies directed to intracellular antigens can be detected in the systemic
Patient #1. Rheumatoid Arthritis. Rheumatoid Arthritis. 45 y/o female Morning stiffness in her joints >1 hour
 Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Screening of Auto Antibodies using Indirect Immunofluorescence in Auto Immune Disease Patients
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 7 Number 02 (2018) Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2018.702.386
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 7 Number 02 (2018) Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2018.702.386
Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? COPYRIGHT
 Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston, MA Diagnostic Tests in Rheumatic Disease: What's Old,
Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston, MA Diagnostic Tests in Rheumatic Disease: What's Old,
AUTOIMMUNITY CLINICAL CORRELATES
 AUTOIMMUNITY CLINICAL CORRELATES Pamela E. Prete, MD, FACP, FACR Section Chief, Rheumatology VA Healthcare System, Long Beach, CA Professor of Medicine, Emeritus University of California, Irvine Colonel
AUTOIMMUNITY CLINICAL CORRELATES Pamela E. Prete, MD, FACP, FACR Section Chief, Rheumatology VA Healthcare System, Long Beach, CA Professor of Medicine, Emeritus University of California, Irvine Colonel
AUTOIMMUNITY TOLERANCE TO SELF
 AUTOIMMUNITY CLINICAL CORRELATES Pamela E. Prete, MD, FACP, FACR Section Chief, Rheumatology VA Healthcare System, Long Beach, CA Professor of Medicine, Emeritus University of California, Irvine Colonel
AUTOIMMUNITY CLINICAL CORRELATES Pamela E. Prete, MD, FACP, FACR Section Chief, Rheumatology VA Healthcare System, Long Beach, CA Professor of Medicine, Emeritus University of California, Irvine Colonel
Anti-CCP antibody testing as a diagnostic and prognostic tool in rheumatoid arthritis
 Q J Med 2007; 100:193 201 doi:10.1093/qjmed/hcm015 Review Anti-CCP antibody testing as a diagnostic and prognostic tool in rheumatoid arthritis T.B. NIEWOLD, M.J. HARRISON and S.A. PAGET From the Department
Q J Med 2007; 100:193 201 doi:10.1093/qjmed/hcm015 Review Anti-CCP antibody testing as a diagnostic and prognostic tool in rheumatoid arthritis T.B. NIEWOLD, M.J. HARRISON and S.A. PAGET From the Department
The Pathogenesis of Bone Erosions in RA FULL VERSION
 The Pathogenesis of Bone Erosions in RA FULL VERSION 1 Key Learning Objectives Understand the role of osteoclasts in normal bone remodeling Comprehend the key processes in pathologic osteoclast functions
The Pathogenesis of Bone Erosions in RA FULL VERSION 1 Key Learning Objectives Understand the role of osteoclasts in normal bone remodeling Comprehend the key processes in pathologic osteoclast functions
Confirmation of anti-dfs70 antibodies is needed in routine clinical samples with DFS staining pattern
 Experimental immunology DOI: 10.5114/ceji.2016.58812 Confirmation of anti-dfs70 antibodies is needed in routine clinical samples with DFS staining pattern Esvet Mutlu, Mete Eyigör, Derya Mutlu, Meral Gültekin
Experimental immunology DOI: 10.5114/ceji.2016.58812 Confirmation of anti-dfs70 antibodies is needed in routine clinical samples with DFS staining pattern Esvet Mutlu, Mete Eyigör, Derya Mutlu, Meral Gültekin
Interpretation of Immunological Investigations in Clinical Practice
 Prof. Uma Kumar Head, Department of Rheumatology All India Institute of Medical Sciences New Delhi WHO Fellow (IEC) President-Elect Delhi Rheumatology Association Recipient GEM OF INDIA award for academic
Prof. Uma Kumar Head, Department of Rheumatology All India Institute of Medical Sciences New Delhi WHO Fellow (IEC) President-Elect Delhi Rheumatology Association Recipient GEM OF INDIA award for academic
Value-added reporting. X. Bossuyt
 Value-added reporting X. Bossuyt COMMUNICATING DIAGNOSTIC ACCURACY Communicating diagnostic accuracy Question 1 Sensitivity: 95% Specificity: 9% Pre-test probability: 2.5% Post-test probability??? 1% 2%
Value-added reporting X. Bossuyt COMMUNICATING DIAGNOSTIC ACCURACY Communicating diagnostic accuracy Question 1 Sensitivity: 95% Specificity: 9% Pre-test probability: 2.5% Post-test probability??? 1% 2%
Overview of Diagnostic Autoantibodies in Inflammatory Myopathy
 Overview of Diagnostic Autoantibodies in Inflammatory Myopathy Minoru Satoh, M.D., Ph.D. Research Associate Professor of Medicine Division of Rheumatology and Clinical Immunology University of Florida
Overview of Diagnostic Autoantibodies in Inflammatory Myopathy Minoru Satoh, M.D., Ph.D. Research Associate Professor of Medicine Division of Rheumatology and Clinical Immunology University of Florida
AUTOANTIBODIES PRECEDING AUTOIMMUNE DISEASES
 AUTOANTIBODIES PRECEDING AUTOIMMUNE DISEASES STUDY GROUP - AUTOANTIBODY STANDARDIZING COMMITTEE Washington, November 12th 2012 Luis Eduardo Coelho Andrade, M.D, Ph.D. Associate Professor Rheumatology Division
AUTOANTIBODIES PRECEDING AUTOIMMUNE DISEASES STUDY GROUP - AUTOANTIBODY STANDARDIZING COMMITTEE Washington, November 12th 2012 Luis Eduardo Coelho Andrade, M.D, Ph.D. Associate Professor Rheumatology Division
Disappearance of anti-mda-5 autoantibodies in clinically amyopathic DM/interstitial lung disease during disease remission
 RHEUMATOLOGY Rheumatology 2012;51:800 804 doi:10.1093/rheumatology/ker408 Advance Access publication 30 December 2011 Concise report Disappearance of anti-mda-5 autoantibodies in clinically amyopathic
RHEUMATOLOGY Rheumatology 2012;51:800 804 doi:10.1093/rheumatology/ker408 Advance Access publication 30 December 2011 Concise report Disappearance of anti-mda-5 autoantibodies in clinically amyopathic
Rheumatoid Arthritis. Improving Outcomes in RA: Three Pillars. RA: Chronic Joint Destruction and Disability What We Try to Prevent
 Rheumatoid Arthritis Modern Management of Common Problems in Rheumatology: Rheumatoid Arthritis Jonathan Graf, M.D. Associate Professor of Medicine, UCSF Division of Rheumatology, SFGH Director, UCSF Rheumatoid
Rheumatoid Arthritis Modern Management of Common Problems in Rheumatology: Rheumatoid Arthritis Jonathan Graf, M.D. Associate Professor of Medicine, UCSF Division of Rheumatology, SFGH Director, UCSF Rheumatoid
ILD and systemic disease
 Department for Pulmonology, University Hospital Berne ILD and systemic disease Dr. med. Manuela Funke-Chambour Oberärztin I Female patient, born 1945 Portuguese Presented with cough and dyspnea, no other
Department for Pulmonology, University Hospital Berne ILD and systemic disease Dr. med. Manuela Funke-Chambour Oberärztin I Female patient, born 1945 Portuguese Presented with cough and dyspnea, no other
Anti-Nuclear Antibodies (ANA). (Incorporating Anti-double stranded DNA (dsdna) and Anti-Extractable Nuclear Antigen (ENA) Antibodies)
. (Incorporating Anti-double stranded DNA (dsdna) and Anti-Extractable Nuclear Antigen (ENA) Antibodies)") Autoimmune Antibody Testing Points of Note: The interpretation of all autoantibody tests is highly dependent on the likelihood of disease in the patient. The results should always be interpreted with the
Autoimmune Antibody Testing Points of Note: The interpretation of all autoantibody tests is highly dependent on the likelihood of disease in the patient. The results should always be interpreted with the
Rheumatologic Testing in Primary Care
 Rheumatologic Testing in Primary Care Fernando Vega, MD October 4, 2008 To help establish a diagnosis in pt with clinical features suggestive of an autoimmune disorder To exclude such disorders in pt with
Rheumatologic Testing in Primary Care Fernando Vega, MD October 4, 2008 To help establish a diagnosis in pt with clinical features suggestive of an autoimmune disorder To exclude such disorders in pt with
NATIONAL LABORATORY HANDBOOK. Laboratory Testing for Antinuclear antibodies
 NATIONAL LABORATORY HANDBOOK Laboratory Testing for Antinuclear antibodies Document reference number CSPD013/2018 Document developed by National Clinical Programme for Pathology Revision number Version
NATIONAL LABORATORY HANDBOOK Laboratory Testing for Antinuclear antibodies Document reference number CSPD013/2018 Document developed by National Clinical Programme for Pathology Revision number Version
International Journal of Pharma and Bio Sciences
 Research Article Microbiology International Journal of Pharma and Bio Sciences ISSN 0975-6299 A COMPARATIVE STUDY OF ENZYME LINKED IMMUNOSORBENT ASSAY (ELISA) WITH IMMUNOFLUORESCENCE ASSAY (IFA) FOR THE
Research Article Microbiology International Journal of Pharma and Bio Sciences ISSN 0975-6299 A COMPARATIVE STUDY OF ENZYME LINKED IMMUNOSORBENT ASSAY (ELISA) WITH IMMUNOFLUORESCENCE ASSAY (IFA) FOR THE
SCLERODERMA OVERLAP SYNDROME: A CASE REPORT Diwakar K. Singh 1, Nataraju H. V 2
 SCLERODERMA OVERLAP SYNDROME: A Diwakar K. Singh 1, Nataraju H. V 2 HOW TO CITE THIS ARTICLE: Diwakar K. Singh, Nataraju H. V. Scleroderma Overlap Syndrome: A Case Report. Journal of Evolution of Medical
SCLERODERMA OVERLAP SYNDROME: A Diwakar K. Singh 1, Nataraju H. V 2 HOW TO CITE THIS ARTICLE: Diwakar K. Singh, Nataraju H. V. Scleroderma Overlap Syndrome: A Case Report. Journal of Evolution of Medical
Jeopardy. What s the rash? $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400
 Jeopardy Antibodies & more antibodies Aching joints What s the rash? Potpourri Image Challenge $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500
Jeopardy Antibodies & more antibodies Aching joints What s the rash? Potpourri Image Challenge $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500
A Multiplex Autoantibody Panel for Early Detection of Autoimmune Disease Activity
 Open Journal of Rheumatology and Autoimmune Diseases, 2018, 8, 43-52 http://www.scirp.org/journal/ojra ISSN Online: 2164-005X ISSN Print: 2163-9914 A Multiplex Autoantibody Panel for Early Detection of
Open Journal of Rheumatology and Autoimmune Diseases, 2018, 8, 43-52 http://www.scirp.org/journal/ojra ISSN Online: 2164-005X ISSN Print: 2163-9914 A Multiplex Autoantibody Panel for Early Detection of
We also assessed the diagnostic significance of the SUBJECTS
 Annals of the Rheumatic Diseases, 1982, 41, 382-387 Antinuclear antibodies in patients with Raynaud's phenomenon: clinical significance of anticentromere antibodies C. G. M. KALLENBERG, G. W. PASTOOR,
Annals of the Rheumatic Diseases, 1982, 41, 382-387 Antinuclear antibodies in patients with Raynaud's phenomenon: clinical significance of anticentromere antibodies C. G. M. KALLENBERG, G. W. PASTOOR,
PATHOGENESIS OF RHEUMATOID ARTHRITIS
 PATHOGENESIS OF RHEUMATOID ARTHRITIS Division of Rheumatology Department of Internal Medicine College of Medicine Seoul National University Seoul National University Bundang Hospital Yun Jong Lee Rheumatoid
PATHOGENESIS OF RHEUMATOID ARTHRITIS Division of Rheumatology Department of Internal Medicine College of Medicine Seoul National University Seoul National University Bundang Hospital Yun Jong Lee Rheumatoid
Primary Sample Manual Immunology Issue No Effective Date: 06/11/17 Page 1 of 19 EUROFINS BIOMNIS. Pr. Conleth Feighery, Immunology Consultant
 Issue No. 2.02 Effective Date: 06/11/17 Page 1 of 19 Written / Revised By: Barry O Dea, Medical Scientist Date: Reviewed By: Date: Pr. Conleth Feighery, Immunology Consultant Authorised By: Jean-Sébastien
Issue No. 2.02 Effective Date: 06/11/17 Page 1 of 19 Written / Revised By: Barry O Dea, Medical Scientist Date: Reviewed By: Date: Pr. Conleth Feighery, Immunology Consultant Authorised By: Jean-Sébastien
Introduce the important components of the immune system Show how they interact & protect the body
 Immunology in Rheumatic Diseases Knowledge of immunology forms the basis of understanding many of the Rheumatologic diseases and has become the focus of many exciting new treatment strategies. AIMS OF
Immunology in Rheumatic Diseases Knowledge of immunology forms the basis of understanding many of the Rheumatologic diseases and has become the focus of many exciting new treatment strategies. AIMS OF
Autoantibodies in childhood connective tissue diseases
 Archives of Disease in Childhood, 1975, 50 419, Autoantibodies in childhood connective tissue diseases and in normal children K. M. GOEL, R. A. SHANKS, K. WHALEY, MARY MASON, and R. N. M. MacSWEEN From
Archives of Disease in Childhood, 1975, 50 419, Autoantibodies in childhood connective tissue diseases and in normal children K. M. GOEL, R. A. SHANKS, K. WHALEY, MARY MASON, and R. N. M. MacSWEEN From
What are Autoantibodies and how do they work in Myositis?
 What are Autoantibodies and how do they work in Myositis? Neil McHugh, University of Bath and Royal National Hospital for Rheumatic Diseases Orlando September 2015 Royal National Hospital for Rheumatic
What are Autoantibodies and how do they work in Myositis? Neil McHugh, University of Bath and Royal National Hospital for Rheumatic Diseases Orlando September 2015 Royal National Hospital for Rheumatic
Autoantibodies in Idiopathic Inflammatory Myopathies. Vidya Limaye Rheumatology Department Royal Adelaide Hospital
 Autoantibodies in Idiopathic Inflammatory Myopathies Vidya Limaye Rheumatology Department Royal Adelaide Hospital Idiopathic Inflammatory Myopathies (IIM) Heterogeneous group of systemic autoimmune syndromes
Autoantibodies in Idiopathic Inflammatory Myopathies Vidya Limaye Rheumatology Department Royal Adelaide Hospital Idiopathic Inflammatory Myopathies (IIM) Heterogeneous group of systemic autoimmune syndromes
Clinic of Neurology, Carol Davila University of Medicine and Pharmacy, Colentina Clinical Hospital, Bucharest, Romania c
 Mædica - a Journal of Clinical Medicine EDITORIALS Autoimmunity to cyclic citrullinated peptide in rheumatoid arthritis Manole COJOCARU, MD, PhD a, Inimioara Mihaela COJOCARU MD, PhD b, Isabela SILOSI
Mædica - a Journal of Clinical Medicine EDITORIALS Autoimmunity to cyclic citrullinated peptide in rheumatoid arthritis Manole COJOCARU, MD, PhD a, Inimioara Mihaela COJOCARU MD, PhD b, Isabela SILOSI
CTD-related Lung Disease
 13 th Cambridge Chest Meeting King s College, Cambridge April 2015 Imaging of CTD-related Lung Disease Dr Sujal R Desai King s College Hospital, London Disclosure Statement No Disclosures / Conflicts of
13 th Cambridge Chest Meeting King s College, Cambridge April 2015 Imaging of CTD-related Lung Disease Dr Sujal R Desai King s College Hospital, London Disclosure Statement No Disclosures / Conflicts of
Understanding Autoimmune Diseases: Evolving Issues. Alvina D. Chu, M.D. April 23, 2009
 Understanding Autoimmune Diseases: Evolving Issues Alvina D. Chu, M.D. April 23, 2009 Objectives Define the key pathogenic characteristics of: Type I diabetes mellitus Multiple sclerosis Rheumatoid arthritis
Understanding Autoimmune Diseases: Evolving Issues Alvina D. Chu, M.D. April 23, 2009 Objectives Define the key pathogenic characteristics of: Type I diabetes mellitus Multiple sclerosis Rheumatoid arthritis
ANA testing can now be ordered in several ways, depending on the clinical circumstances:
 LAB TEST CONNECT Multiplex ANA Screen Dr. Joseph Schappert, M.D.,Medical Director Chief Medical Offi cer ANA has been the primary screening test for connective tissue diseases (CTD s) for many years. While
LAB TEST CONNECT Multiplex ANA Screen Dr. Joseph Schappert, M.D.,Medical Director Chief Medical Offi cer ANA has been the primary screening test for connective tissue diseases (CTD s) for many years. While
Myositis and Your Lungs
 Myositis and Your Lungs 2013 TMA Annual Patient Meeting Louisville, Kentucky Chester V. Oddis, MD University of Pittsburgh Director, Myositis Center Myositis Heterogeneous group of autoimmune syndromes
Myositis and Your Lungs 2013 TMA Annual Patient Meeting Louisville, Kentucky Chester V. Oddis, MD University of Pittsburgh Director, Myositis Center Myositis Heterogeneous group of autoimmune syndromes
Insights into the DX of Pediatric SLE
 Insights into the DX of Pediatric SLE Dr. John H. Yost Pediatric Rheumatology Children s Hospital at Dartmouth Assistant Professor of Medicine Geisel School of Medicine at Dartmouth john.h.yost@hitchcock.org
Insights into the DX of Pediatric SLE Dr. John H. Yost Pediatric Rheumatology Children s Hospital at Dartmouth Assistant Professor of Medicine Geisel School of Medicine at Dartmouth john.h.yost@hitchcock.org
Rheumatology 101 A Pediatrician s Guide
 Rheumatology 101 A Pediatrician s Guide Pediatric Staff and Alumni Day 2016 Dawn M. Wahezi, Yonit Sterba, Tamar Rubinstein Disclosures None Pick a Group Group 1 A child with a limp Group 2 ANA To test
Rheumatology 101 A Pediatrician s Guide Pediatric Staff and Alumni Day 2016 Dawn M. Wahezi, Yonit Sterba, Tamar Rubinstein Disclosures None Pick a Group Group 1 A child with a limp Group 2 ANA To test
Relevance of Autoantibodies in RA
 Relevance of Autoantibodies in RA Tom Huizinga Malmo 2012 Quiz: How much of a patient IgG is ACPA in the peripheral blood? a) 0.005% b) 0.05% b) 0.5% c) 5% d) 50% Amount of ACPA producing B cells ACPA
Relevance of Autoantibodies in RA Tom Huizinga Malmo 2012 Quiz: How much of a patient IgG is ACPA in the peripheral blood? a) 0.005% b) 0.05% b) 0.5% c) 5% d) 50% Amount of ACPA producing B cells ACPA
PATHOGENESIS OF RHEUMATOID ARTHRITIS
 PATHOGENESIS OF RHEUMATOID ARTHRITIS Division of Rheumatology Department of Internal Medicine College of Medicine Seoul National University Seoul National University Bundang Hospital Yun Jong Lee Rheumatoid
PATHOGENESIS OF RHEUMATOID ARTHRITIS Division of Rheumatology Department of Internal Medicine College of Medicine Seoul National University Seoul National University Bundang Hospital Yun Jong Lee Rheumatoid
Detection of serum antinuclear antibodies in lymphoma patients
 Detection of serum antinuclear antibodies in lymphoma patients H.Y. Zou 1 *, X. Gu 2 *, W.Z. Yu 1, Z. Wang 1 and M. Jiao 1 1 Institute of Clinical Medicine, Urumqi General Hospital of Lanzhou Military
Detection of serum antinuclear antibodies in lymphoma patients H.Y. Zou 1 *, X. Gu 2 *, W.Z. Yu 1, Z. Wang 1 and M. Jiao 1 1 Institute of Clinical Medicine, Urumqi General Hospital of Lanzhou Military
LAB TESTING IN RHEUMATOLOGY DR. PHILIP A. BAER SEACOURSES ASIA CME DECEMBER 2017
 LAB TESTING IN RHEUMATOLOGY DR. PHILIP A. BAER SEACOURSES ASIA CME DECEMBER 2017 COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
LAB TESTING IN RHEUMATOLOGY DR. PHILIP A. BAER SEACOURSES ASIA CME DECEMBER 2017 COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Essential Rheumatology. Dr Ellen Bruce Consultant Rheumatologist CMFT
 Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Systemic sclerosis (SSC)
") Systemic sclerosis (SSC) -Is a multi system autoimmune disease, characterized by fibrosis of the skin and variable pattern of other visceral -SSC: Is a relatively UN common disease -Prevalence in U S A
Systemic sclerosis (SSC) -Is a multi system autoimmune disease, characterized by fibrosis of the skin and variable pattern of other visceral -SSC: Is a relatively UN common disease -Prevalence in U S A
Marilina Tampoia, MD; Vincenzo Brescia, MD; Antonietta Fontana, MD; Antonietta Zucano, PhD; Luigi Francesco Morrone, MD; Nicola Pansini, MD
 Application of a Combined Protocol for Rational Request and Utilization of Antibody Assays Improves Clinical Diagnostic Efficacy in Autoimmune Rheumatic Disease Marilina Tampoia, MD; Vincenzo Brescia,
Application of a Combined Protocol for Rational Request and Utilization of Antibody Assays Improves Clinical Diagnostic Efficacy in Autoimmune Rheumatic Disease Marilina Tampoia, MD; Vincenzo Brescia,
Scott Vogelgesang, MD Division of Rheumatology/Immunology University of Iowa
 Scott Vogelgesang, MD Division of Rheumatology/Immunology University of Iowa Basic Concepts ANA DsDNA Sm RNP SSA SSB RF/CCP ESR/CRP ANCA Cases Summary Rheumatology Tests Lie and Mislead! Rheumatology Rally
Scott Vogelgesang, MD Division of Rheumatology/Immunology University of Iowa Basic Concepts ANA DsDNA Sm RNP SSA SSB RF/CCP ESR/CRP ANCA Cases Summary Rheumatology Tests Lie and Mislead! Rheumatology Rally
IMTEC-ANA-LIA MAXX. Design Verification
 Design Verification IMTEC-ANA-LIA MAXX CONTENTS 1 Intended Use... 2 2 Diagnostic Sensitivity and Specificity... 2 3 Interferences... 4 4 Imprecision... 6 4.1 Within-Run Imprecision... 6 4.2 Between-Run
Design Verification IMTEC-ANA-LIA MAXX CONTENTS 1 Intended Use... 2 2 Diagnostic Sensitivity and Specificity... 2 3 Interferences... 4 4 Imprecision... 6 4.1 Within-Run Imprecision... 6 4.2 Between-Run
Autoimmunity. Autoimmunity arises because of defects in central or peripheral tolerance of lymphocytes to selfantigens
 Autoimmunity Autoimmunity arises because of defects in central or peripheral tolerance of lymphocytes to selfantigens Autoimmune disease can be caused to primary defects in B cells, T cells and possibly
Autoimmunity Autoimmunity arises because of defects in central or peripheral tolerance of lymphocytes to selfantigens Autoimmune disease can be caused to primary defects in B cells, T cells and possibly
Rheumatoid Arthritis: Assessing Diagnostic Results in the Primary Care Setting
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
The Study of Cells The diversity of the cells of the body The following figure shows the proportion of cell size of the variety of cells in the body
 Adapted from Martini Human Anatomy 7th ed. Chapter 2 Foundations: The Cell Introduction There are trillions of cells in the body Cells are the structural building blocks of all plants and animals Cells
Adapted from Martini Human Anatomy 7th ed. Chapter 2 Foundations: The Cell Introduction There are trillions of cells in the body Cells are the structural building blocks of all plants and animals Cells
Detection of Anti-nuclear Antibodies in Women with Hyperprolactinaemia
 Detection of Anti-nuclear Antibodies in Women with Hyperprolactinaemia Salahdeen Ismail Mohammed 12, Alaaeldeen Balal Ahmed 1, Nuha Abdurhaman 2, Abdalla Hassan Sharief 2 1 Faculty of Medical Laboratory
Detection of Anti-nuclear Antibodies in Women with Hyperprolactinaemia Salahdeen Ismail Mohammed 12, Alaaeldeen Balal Ahmed 1, Nuha Abdurhaman 2, Abdalla Hassan Sharief 2 1 Faculty of Medical Laboratory
Laboratory diagnosis of autoimmune diseases
 Laboratory diagnosis of autoimmune diseases By Marc Golightly, Ph.D. and Candace Golightly, MS Introduction The rheumatic and autoimmune diseases can generally be classified into two groups: those that
Laboratory diagnosis of autoimmune diseases By Marc Golightly, Ph.D. and Candace Golightly, MS Introduction The rheumatic and autoimmune diseases can generally be classified into two groups: those that
Technical Article Series Scleroderma ANA and Antibody Testing
 Technical Article Series Scleroderma ANA and Antibody Testing ANA Testing Basics The long-standing way of doing ANA testing is a method called indirect immunofluorescence (IFA). It is a time consuming,
Technical Article Series Scleroderma ANA and Antibody Testing ANA Testing Basics The long-standing way of doing ANA testing is a method called indirect immunofluorescence (IFA). It is a time consuming,
RHEUMATOLOGY OVERVIEW. Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center
 RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases