Rheumatology Potpourri. Dr. Philip A. Baer Seacourses Asia CME December 2017
|
|
|
- Collin Underwood
- 6 years ago
- Views:
Transcription
1 Rheumatology Potpourri Dr. Philip A. Baer Seacourses Asia CME December 2017
2 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of Sea Courses Inc. except where permitted by law. Sea Courses is not responsible for any speaker or participant s statements, materials, acts or omissions.
3 Learning Objectives Diagnose and treat polymyalgia rheumatica (PMR) and giant cell arteritis (GCA) while minimizing the adverse effects of steroid therapy. Distinguish CPPD arthritis from other forms of crystal-induced arthritis, and manage CPPD arthritis appropriately. Recognize different muscle problems associated with statin use, particularly necrotizing autoimmune myopathy (NAM).
4 Case 1 History 76 y.o. woman Controlled hypertension and angina Usually active 2 months history of aching pain in shoulders, upper arms, thighs Morning stiffness 1 hour Limited in daily activities Appetite down; weight loss 8 pounds
5 Case 1 Exam & Labs Exam: Vital signs normal OA hands Tender proximal muscles No weakness Labs: Hgb 106, MCV 88, ESR 65 CK normal, slightly low albumin
6 Musculoskeletal Pain in Older Patients Think polymyalgia rheumatica when Age >60 Proximal muscle myalgias and stiffness without specific muscle weakness High ESR Anemia
7 Polymyalgia Rheumatica (PMR) A clinical syndrome characterized by aching and stiffness of the shoulder and hip girdle muscles affecting older patients, associated with an elevated ESR, lasting over 1 month and responsive to low dose steroids First description in 1888 (Bruce) Barber suggested the present name in 1957
8 PMR: Epidemiology Incidence in Canada: Approximately 50/100,000 patients over age 50/year Predominant age: 60 or older. Incidence increases with age (rare under 50 years old) Predominant gender: Female > Male (2:1)
9

10 PMR: Core Inclusion Criteria
11 PMR: Core Exclusion Criteria Active infection Active cancer Active giant cell arteritis (GCA)
12 PMR: Features Suggesting GCA Abrupt-onset headache (usually temporal) and temporal tenderness Visual disturbance, including diplopia Jaw or tongue claudication Prominence, beading or diminished pulse on examination of the temporal artery Upper cranial nerve palsies Limb claudication or other evidence of large-vessel involvement
13 PMR: Other Diseases to Exclude Other inflammatory rheumatic diseases Drug-induced myalgia Chronic pain syndromes Endocrine disease Neurological conditions, e.g. Parkinson s disease

14 PMR: General Principles
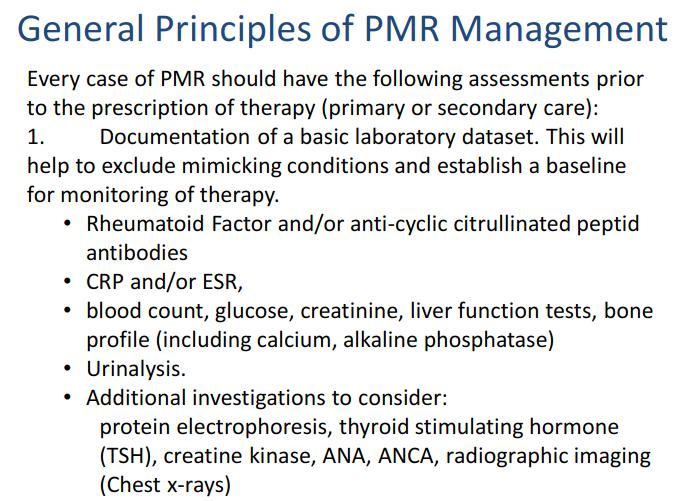
15 PMR: Lab Evaluation

16 PMR: Initial Steroid Dose
17 PMR: Initial Therapy and Follow-up A patient-reported global improvement of 70% within a week of commencing steroids is consistent with PMR, with normalization of inflammatory markers in 4 weeks A lesser response should prompt the search for an alternative condition The diagnosis of PMR should be confirmed on further follow-up. Follow-up visits should include vigilance for mimicking conditions Consider low-dose ASA, CV risk assessment, and osteoporosis prophylaxis during follow-up

18 PMR: High Dose Steroids?

19 PMR: NSAIDs?
20 PMR: Steroid Tapering

21 PMR: Steroid Tapering
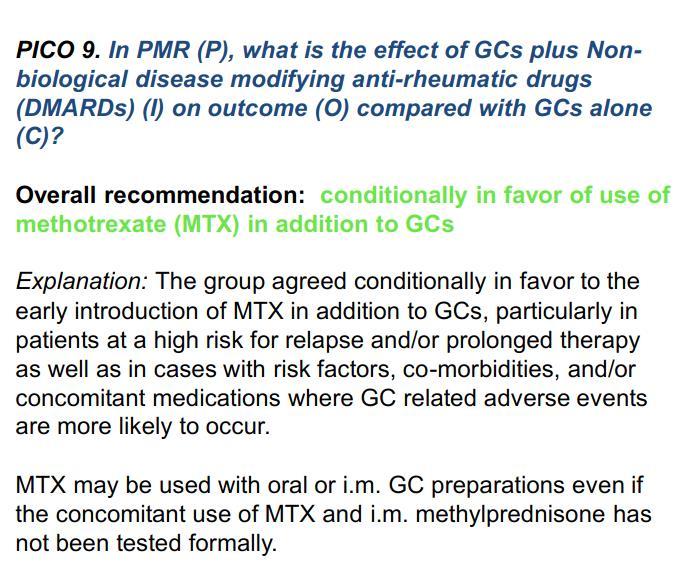
22 PMR: Immunosuppressants?

23 PMR: Biologics?
24 PMR: Duration of Therapy Usually 1 3 years of treatment, although some will require small doses of steroids beyond this. Steroids may be stopped when the patient is asymptomatic from their inflammatory symptoms. Isolated raised ESR or CRP is not an indication for continuing steroid therapy but may require investigation and referral. Persistent pain may arise from co-existing OA and rotator cuff tears.
25 PMR: Therapy of Relapses Relapse is the recurrence of symptoms of PMR or onset of GCA, and not just unexplained raised ESR or CRP Treatment of relapse: Clinical features of GCA: treat as GCA (usually oral prednisone 40 60mg daily) Clinical features of PMR: increase prednisone to previous higher dose Single i.m. injection of methylprednisolone 120mg can also be used Further relapses: consider introducing DMARD therapy after two relapses
26 Resources

27

28

29

30 ACR/EULAR PMR Algorithm

31 Relationship between PMR & GCA 10-15% of patients with PMR have GCA 40-60% of patients with GCA have PMR GCA PMR PMR GCA
32 Case 2: History A 68-year-old man presents with complaints of diffuse muscle pain, weakness, and total body fatigue. He reports: Gradual onset over past 6 months Morning stiffness lasting 2 to 3 hours Difficulty with getting out of a chair and combing his hair Recent onset of right-sided headache Recent onset of jaw pain when eating

33 Case 2: Exam and Labs Proximal muscle tenderness without objective weakness Tender right temporal scalp region Normal visual acuity Hgb 98 g/l ESR 85 CK 32
34 Case 2: Question Based on the clinical findings, what is the most important next step? A. Treat now with prednisone 5 mg bid, and observe B. Schedule a temporal artery biopsy for tomorrow morning and use the results to determine whether prednisone will be used C. Start an NSAID at maximal dose D. Treat now with prednisone at 40 to 60 mg per day and schedule temporal artery biopsy in the next few days
35 Case 2: Answer D. Treat now with prednisone at 40 to 60 mg per day and schedule temporal artery biopsy for next week Sudden visual loss may occur in GCA Visual loss occurs in 1/3 of untreated patients The visual loss is usually not reversible Nordberg E, et al. Rheum Dis Clin North Am. 1995;21:

36 Don t Hesitate For probable temporal arteritis: TREAT NOW! BIOPSY LATER! Biopsy as soon as possible Hunder GC. Primer on Rheum Dis. 11th edition. 1997:

37 Elastic stain of temporal artery in GCA: Disruption of elastic lamina and narrowing of the lumen

38 GCA - granulomatous inflammation and multinucleated giant cells

39 DIAGNOSIS OF GCA Halo sign

40 GCA: Dilated Temporal Artery

41 GCA: Optic Atrophy

42 Giant Cell Aortitis Risk of Thoracic Aortic Aneurysm in GCA: 15%
43 GCA: Steroid Therapy GCA without visual symptoms: Prednisone mg daily for 8 weeks Reduce by 5 mg q3-4 weeks to 10 mg daily Then treat as PMR GCA with possible or definite visual symptoms: Prednisone mg daily for 8 weeks Reduce over 4 weeks to 20 mg daily Then treat as uncomplicated GCA
44 GCA: Other Therapies Methotrexate, azathioprine, and other immunosuppressive drugs have been used to limit dosage and duration of corticosteroid therapy. No clear-cut data suggest that any of these drugs is superior to corticosteroid therapy. Anti-TNF therapy with infliximab failed in GCA studies. Anti-IL6 therapy with tocilizumab is now approved for GCA (USA)
45 Resources

46
47
48 Case 3: History 80 y.o. woman, independent, lives alone Occasional aches in knees, wrists Acute swelling of right knee with pain, local warmth and redness Prior episode in L wrist and hand No trauma Low grade fever, no recent infection

49 X-ray: Chondrocalcinosis

50 Aspiration: Bloody fluid
51 Case 3: Labs CBC: WBC 14,000 with left shift egfr 55, uric acid 200 Calcium/PO 4 /Alkaline Phosphatase normal Synovial fluid: WBC 15,000 Thin, bloody fluid Gram stain/culture negative

52 CPPD Disease: Crystals Calcium pyrophosphate crystals Ordinary, polarized, and compensated polarized light microscopy
53 CPPD Disease: Classification Chondrocalcinosis Acute Pseudogout Pyrophosphate Arthropathy

54 Chondrocalcinosis
55 Chondrocalcinosis: Epidemiology Elderly Radiographic evidence: 65-74yr 15% 75-84yr 36% >84yr 50% Male = Female No geographic or racial predisposition
56 CPPD Disease: Clinical Features Acute synovitis Monoarthritis Polyarticular: rare Any joint: commonest in knee : wrist, shoulder, ankle Rapid onset of pain, stiffness and swelling (6-24 hrs) Low-grade fever common
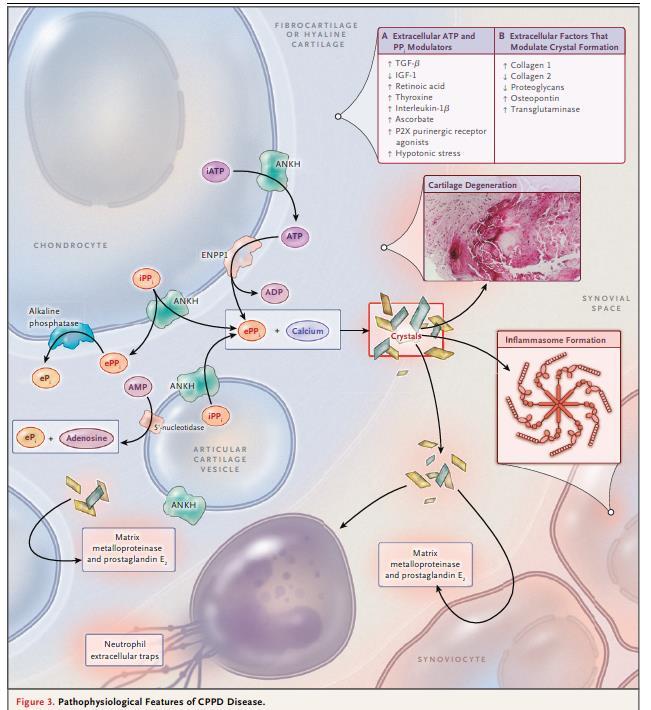
57 CPPD: Pathophysiology

58 CPPD Disease: Triggers
59 CPPD Disease: Diagnosis Observation of calcium pyrophosphate dihydrate crystals in synovial fluid leukocytes in a patient with acute synovitis CPPD crystals are Rhomboid Positively birefringent

60 Synovial Fluid Crystals
61 CPPD Disease: Treatment Principles No definitive therapy for prevention Goals in managing acute attacks reduce symptoms identify and treat any associated or triggering illnesses encourage mobility as inflammation subsides
62 Acute CPPD Disease: Treatment Options Joint aspiration NSAIDs Colchicine (not as effective as for gout) Steroids (not as effective as for gout) oral intra-articular Analgesics
63 Acute CPP Crystal Arthritis: Treatment Options
64 Chronic Pyrophosphate Arthropathy: Clinical Features Findings mimic any type of arthritis Terminology -Pseudo RA -Pseudo OA -Pseudo neuropathic joint disease Distinguishing points-pattern of involvement -Inflammation -Superimposed pseudogout
65 Chronic Pyrophosphate Arthropathy: Epidemiology and Distribution Elderly Female Large/medium joints Knees Wrists, shoulders, elbows Hips, midtarsal, MCPs (2+3)

66 Knee radiograph showing hypertrophic OA features. Note prominent patello-femoral involvement, typical of pyrophosphate arthropathy.
67 Chronic CPPD Arthropathy: Treatment Options Steroid injection Colchicine NSAID + PPI Oral low dose steroids Hydroxychloroquine Methotrexate Surgery to preserve function
68 Resources
69

70

71 June 30, 2016

72 Muscle Fibre: Normal Anatomy
73 Statin-induced Myopathy 1.5-3% of statin users in RCTs and 10-13% of participants enrolled in prospective clinical studies develop myalgias; rates of myositis lower (~ %) & dose-dependent Mean duration of statin therapy before onset of symptoms: 6 months Mean duration of myalgias after stopping statin therapy: 2 months

74
75 Statin-induced Myopathy: Questions What if a patient develops a myopathy after several years of taking a statin? Not likely to be statin-induced. 2/3 develop symptoms within 6 months of starting therapy, however it is still possible to develop muscle symptoms at ANY time during treatment. Are some statins more likely to cause muscle damage? Which ones? Lipophilic statins (for example, simvastatin, atorvastatin, lovastatin) are more likely to produce muscular effects than are relatively hydrophilic agents (such as pravastatin, rosuvastatin, and fluvastatin). Lipophilic compounds are more likely to penetrate into muscle tissue, enhancing the potential for myotoxic effects.

76

77
78
79 Statin-Induced Myopathy: Management Significant muscle symptoms: discontinue statin Asymptomatic but with CK>10x ULN: discontinue statin Rhabdomyolysis: no statins at any time due to risk of recurrence If patient requires a statin but muscle toxicity other than rhabdomyolysis: discontinue statin Once symptoms have resolved and the CK has returned to baseline, can try pravastatin or fluvastatin with careful monitoring
80 Statin-induced Myopathy: Questions When are EMG or muscle biopsy necessary in suspected statin myopathy? EMG and muscle biopsy are often done in atypical cases of statin induced myopathy. These would include those patients with persistent muscle pain after D/C of statin or with persistent, worsening weakness after D/C of statin, or persistently elevated CK long after D/C of statin (several months). Electromyography findings are commonly reported to show myopathic changes, usually in the proximal muscles, in agreement with clinical findings. Muscle pathology in statin induced myopathy is nonspecific, with necrosis, degeneration, and regeneration of fibres and phagocytic infiltration. Is Coenzyme Q10 helpful? Unclear. In one small RCT, 41 patients taking statins who had muscle pain received either coenzyme Q10 or vitamin E. After one month of treatment, 18 of 21 patients taking coenzyme Q10 reported improvement in muscle pain, compared with three of 20 taking vitamin E (P<0.001).
81 Statin-associated necrotizing myopathy Myopathy which persists or progresses after stopping statin Linked to autoantibodies against HMG-CoA reductase Distinct muscle biopsy findings: Macrophagocytic infiltrate engulfing necrotic muscle fibers Responds to immunosuppressant therapy


82 Necrotizing Autoimmune Myositis
 & excessive variability of muscle fibre size.")
83 Statin-associated necrotizing myopathy (NAM) Necrotic muscle fibre undergoing myophagia WITHOUT inflammatory infiltrate (no lymphocytes or neutrophils) & excessive variability of muscle fibre size. The absence of inflammation distinguishes this entity from the idiopathic inflammatory myopathies.

84 Statin-associated necrotizing myopathy (NAM)
85 EMG findings (All Inflammatory Myopathies) Fibrillation, PSWs, CRDs at rest Increased insertional activity
86 Myositis: Non-medical therapies Physiotherapy and Occupational Therapy Aerobic exercise programs after the acute phase Prevent contractures May help with steroid side effects (weight gain, osteoporosis, type 2 fibre atrophy) Speech therapy Especially if concomitant dysphagia

87 Pharmacologic Treatment of Myositis

88 Myositis: Resources

89 Myositis: Resources

90 Myositis: Resources
91 Myositis: Resources
92 Statin-Associated Autoimmune Myopathy: Approach
93 Statin-Associated Autoimmune Myopathy: Approach
94 PEARLs: Rheumatology Potpourri Think of PMR if over age 65 with proximal joint/muscle pain Start high dose steroids immediately if GCA suspected to prevent visual loss Think CPPD in older women with acute monoarthritis and aspirate joint if possible for crystal analysis Consider autoimmune statin-induced myopathy (NAM) in patients where myopathy persists after stopping statins
95 Barriers to Change: Rheum. Potpourri PMR/GCA: Difficulty distinguishing flares from OA and other comorbidities, leading to higher than required use of steroids CPPD: Confusion with gout and with cellulitis Statin-induced NAM: Difficulty recognizing this syndrome given so many patients on statins present with myalgias and high CKs

96 Questions?
The Joints are Painful & Swollen: Do I give Steroids? Dr Tom Kennedy
 The Joints are Painful & Swollen: Do I give Steroids? Dr Tom Kennedy Learning Objectives When to use an acute rheumatology service Appropriate use of steroids by condition Injection or Oral or Intramuscular
The Joints are Painful & Swollen: Do I give Steroids? Dr Tom Kennedy Learning Objectives When to use an acute rheumatology service Appropriate use of steroids by condition Injection or Oral or Intramuscular
Rheumatology Review Update in Internal Medicine COPYRIGHT. Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center.
 Rheumatology Review Update in Internal Medicine Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston MA Case #1 True statement(s) regarding etanercept and leflunomide, for the treatment
Rheumatology Review Update in Internal Medicine Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston MA Case #1 True statement(s) regarding etanercept and leflunomide, for the treatment
Rheumatologic Emergencies It s not just swollen joints. Joanne Homik Rheumatologist University of Alberta
 Rheumatologic Emergencies It s not just swollen joints Joanne Homik Rheumatologist University of Alberta Or is it? Disclosures No relevant conflicts of interest regarding the content of this presentation
Rheumatologic Emergencies It s not just swollen joints Joanne Homik Rheumatologist University of Alberta Or is it? Disclosures No relevant conflicts of interest regarding the content of this presentation
RHEUMATOLOGY OVERVIEW. Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center
 RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
APPROACH TO PATIENTS WITH POLYARTHRALGIA
 APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
GIANT CELL ARTERITIS. Page 1 of 6 Reproduction of this material requires written permission of the Vasculitis Foundation. Copyright 2018.
 What is giant cell arteritis (GCA)? Giant cell arteritis (GCA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
What is giant cell arteritis (GCA)? Giant cell arteritis (GCA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
Polymyalgia rheumatica and giant cell arteritis
 Polymyalgia rheumatica and giant cell arteritis What is polymyalgia rheumatica? Polymyalgia rheumatica is a rheumatic disorder associated with moderate-to-severe musculoskeletal pain and stiffness in the
Polymyalgia rheumatica and giant cell arteritis What is polymyalgia rheumatica? Polymyalgia rheumatica is a rheumatic disorder associated with moderate-to-severe musculoskeletal pain and stiffness in the
A CRP B FBC C LFT D blood culture E uric acid
 1 A 39 year old lady with rheumatoid arthritis is admitted to hospital with a hot, swollen and painful right knee. Which is the most important blood test? A CRP B FBC C LFT D blood culture E uric acid
1 A 39 year old lady with rheumatoid arthritis is admitted to hospital with a hot, swollen and painful right knee. Which is the most important blood test? A CRP B FBC C LFT D blood culture E uric acid
9/11/11. Temporal Arteritis. Background. Background. Richard E. Castillo, OD, DO NORTHEASTERN STATE UNIVERSITY Director, Ophthalmic Surgery Service
 Temporal Arteritis Richard E. Castillo, OD, DO NORTHEASTERN STATE UNIVERSITY Director, Ophthalmic Surgery Service 1 Background Giant Cell Arteritis Temporal Arteritis Cranial Arteritis Granulomatous Arteritis
Temporal Arteritis Richard E. Castillo, OD, DO NORTHEASTERN STATE UNIVERSITY Director, Ophthalmic Surgery Service 1 Background Giant Cell Arteritis Temporal Arteritis Cranial Arteritis Granulomatous Arteritis
Objectives. Joint Pain. Case 1. Rheumatology for the Primary MD (Not just your grandmother s disease) 12/4/2010
 12/4/2010") Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
Osteoarthritis. Rheumatology Update. Gout 1/17/2013
 Osteoarthritis Rheumatology Update Richard Zweig, MD January, 2013 Degeneration of cartilage over time accompanied by increase in bone density and bone formation around the joint Risks include: aging,
Osteoarthritis Rheumatology Update Richard Zweig, MD January, 2013 Degeneration of cartilage over time accompanied by increase in bone density and bone formation around the joint Risks include: aging,
Polymyalgia, Temporal Arteritis and pineapples
 Polymyalgia, Temporal Arteritis and pineapples Rod Hughes Consultant Rheumatologist Ashford St Peter s Hospital Trust Chertsey Wed 11 th May 2011 Meeting aims Pineapples their significance in disease Defining
Polymyalgia, Temporal Arteritis and pineapples Rod Hughes Consultant Rheumatologist Ashford St Peter s Hospital Trust Chertsey Wed 11 th May 2011 Meeting aims Pineapples their significance in disease Defining
BSR and BHPR guidelines for the management of polymyalgia rheumatica
 RHEUMATOLOGY Guidelines Rheumatology 2010;49:186 190 doi:10.1093/rheumatology/kep303a Advance Access publication 12 November 2009 BSR and BHPR guidelines for the management of polymyalgia rheumatica Bhaskar
RHEUMATOLOGY Guidelines Rheumatology 2010;49:186 190 doi:10.1093/rheumatology/kep303a Advance Access publication 12 November 2009 BSR and BHPR guidelines for the management of polymyalgia rheumatica Bhaskar
1. To review the diagnosis of gout and its differential. 2. To understand the four stages of gout
 Objectives 1. To review the diagnosis of gout and its differential GOUT 2. To understand the four stages of gout 3. To develop an approach for the acute treatment of gout Anthony Lim 9/13/12 Cycle 3 4.
Objectives 1. To review the diagnosis of gout and its differential GOUT 2. To understand the four stages of gout 3. To develop an approach for the acute treatment of gout Anthony Lim 9/13/12 Cycle 3 4.
Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition
 Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition Firestein, G ISBN-13: 9781437717389 Table of Contents VOLUME I STRUCTURE AND FUNCTION OF BONE,
Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition Firestein, G ISBN-13: 9781437717389 Table of Contents VOLUME I STRUCTURE AND FUNCTION OF BONE,
Patient with Daily Headache NTERNATIONAL CLASSIFICATION HEADACHE DISORDERS. R. Allan Purdy, MD, FRCPC,FACP. Professor of Medicine (Neurology)
") Patient with Daily Headache NTERNATIONAL CLASSIFICATION of R. Allan Purdy, MD, FRCPC,FACP HEADACHE DISORDERS Professor of Medicine (Neurology) 2nd edition (ICHD-II) Learning Issues Headaches in the elderly
Patient with Daily Headache NTERNATIONAL CLASSIFICATION of R. Allan Purdy, MD, FRCPC,FACP HEADACHE DISORDERS Professor of Medicine (Neurology) 2nd edition (ICHD-II) Learning Issues Headaches in the elderly
Dr Kusala S. Gunasekara MBBS(Col),MD(Med),MRCP(UK) Acting Consultant Rheumatologist DGH-Matale
,MD(Med),MRCP(UK) Acting Consultant Rheumatologist DGH-Matale") Dr Kusala S. Gunasekara MBBS(Col),MD(Med),MRCP(UK) Acting Consultant Rheumatologist DGH-Matale Patient 67 yr old female First presentation to the rheumatology unit in May 2013 Referred by GP as the patient
Dr Kusala S. Gunasekara MBBS(Col),MD(Med),MRCP(UK) Acting Consultant Rheumatologist DGH-Matale Patient 67 yr old female First presentation to the rheumatology unit in May 2013 Referred by GP as the patient
Rheumatology Cases for the Internist
 Rheumatology Cases for the Internist Marc C. Hochberg, MD, MPH Professor of Medicine Head, Division of Rheumatology and Clinical Immunology Vice Chair, Department of Medicine University of Maryland School
Rheumatology Cases for the Internist Marc C. Hochberg, MD, MPH Professor of Medicine Head, Division of Rheumatology and Clinical Immunology Vice Chair, Department of Medicine University of Maryland School
Rheumatology Red Flags and Emergencies :Workshop DR. MICHAEL STARR DIVISION OF RHEUMATOLOGY MUHC
 Rheumatology Red Flags and Emergencies :Workshop DR. MICHAEL STARR DIVISION OF RHEUMATOLOGY MUHC Family Medicine Review Course, November 28th, 2018 Disclosures Amgen Janssen Roche BMS Pfizer UCB Novartis
Rheumatology Red Flags and Emergencies :Workshop DR. MICHAEL STARR DIVISION OF RHEUMATOLOGY MUHC Family Medicine Review Course, November 28th, 2018 Disclosures Amgen Janssen Roche BMS Pfizer UCB Novartis
First Presentation of Joint Pain
 First Presentation of Joint Pain Andrew Harrison Rheumatologist Wellington Regional Rheumatology Unit, HVDHB Bowen Centre, Crofton Downs, Wellington Assoc. Prof. in Medicine, University of Otago Wellington
First Presentation of Joint Pain Andrew Harrison Rheumatologist Wellington Regional Rheumatology Unit, HVDHB Bowen Centre, Crofton Downs, Wellington Assoc. Prof. in Medicine, University of Otago Wellington
Pharmacology Challenges: Managing Statin Myalgia
 Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
REFERRAL GUIDELINES: RHEUMATOLOGY
 Outpatient Page 1 1 REFERRAL GUIDELINES: RHEUMATOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential Referral Content Referring
Outpatient Page 1 1 REFERRAL GUIDELINES: RHEUMATOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential Referral Content Referring
Overview INTRODUCTION 3/15/2018. Headache Emergencies. Other way to differentiate between them? Is there an easy way to differentiate between them?
 Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Patient #1. Rheumatoid Arthritis. Rheumatoid Arthritis. 45 y/o female Morning stiffness in her joints >1 hour
 Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Rheumatology for the Nurse Practitioner. Mary Derlacki, FNP Eugene Rheumatology
 Rheumatology for the Nurse Practitioner Mary Derlacki, FNP Eugene Rheumatology Financial Relationships Amgen Genentech AbbVie IS THIS LUPUS? S.T. is a 45 y/o woman with 9 months of joint pain, fatigue,
Rheumatology for the Nurse Practitioner Mary Derlacki, FNP Eugene Rheumatology Financial Relationships Amgen Genentech AbbVie IS THIS LUPUS? S.T. is a 45 y/o woman with 9 months of joint pain, fatigue,
Prognosis and management of polymyalgia rheumatica
 Annals of the Rheumatic Diseases, 1981, 40, 1-5 Prognosis and management of polymyalgia rheumatica J. G. JONES AND B. L. HAZLEMAN From Addenbrooke's Hospital, Hills Road, Cambridge SUMMARY Polymyalgia
Annals of the Rheumatic Diseases, 1981, 40, 1-5 Prognosis and management of polymyalgia rheumatica J. G. JONES AND B. L. HAZLEMAN From Addenbrooke's Hospital, Hills Road, Cambridge SUMMARY Polymyalgia
Rheumatoid arthritis
 Rheumatoid arthritis 1 Definition Rheumatoid arthritis is one of the most common inflammatory disorders affecting the population worldwide. It is a systemic inflammatory disease which affects not only
Rheumatoid arthritis 1 Definition Rheumatoid arthritis is one of the most common inflammatory disorders affecting the population worldwide. It is a systemic inflammatory disease which affects not only
Case Presentation VASCULITIS. Case Presentation. Case Presentation. Vasculitis
 Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
For more information about how to cite these materials visit
 Author(s): Seetha Monrad, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Seetha Monrad, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
VASCULITIS. Case Presentation. Case Presentation
 VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abatacept, for rheumatoid arthritis, 789 Acetaminophen, for low back pain, 735 Acupuncture for fibromyalgia, 753 for low back pain, 738
Index Note: Page numbers of article titles are in boldface type. A Abatacept, for rheumatoid arthritis, 789 Acetaminophen, for low back pain, 735 Acupuncture for fibromyalgia, 753 for low back pain, 738
Polymyalgia Rheumatica; Giant Cell Arteritis Paul Katzenstein, MD
 Polymyalgia Rheumatica; Giant Cell Arteritis Paul Katzenstein, MD What is it; is it not? How is this thought about, characterized, understood, treated Time honored published clinical experience Clinical
Polymyalgia Rheumatica; Giant Cell Arteritis Paul Katzenstein, MD What is it; is it not? How is this thought about, characterized, understood, treated Time honored published clinical experience Clinical
Ultrasound in Rheumatology
 Arthritis Research UK Primary Care Centre Winner of a Queen s Anniversary Prize For Higher and Further Education 2009 Ultrasound in Rheumatology Alison Hall Consultant MSK Sonographer/Research Fellow Primary
Arthritis Research UK Primary Care Centre Winner of a Queen s Anniversary Prize For Higher and Further Education 2009 Ultrasound in Rheumatology Alison Hall Consultant MSK Sonographer/Research Fellow Primary
When is it Rheumatoid Arthritis When to Refer
 When is it Rheumatoid Arthritis When to Refer Nancy A. Brown, DO Spring 2015 When is it Rheumatoid Arthritis When to Refer Learning objectives To review the definition and epidemiology of Rheumatoid Arthritis
When is it Rheumatoid Arthritis When to Refer Nancy A. Brown, DO Spring 2015 When is it Rheumatoid Arthritis When to Refer Learning objectives To review the definition and epidemiology of Rheumatoid Arthritis
Rheumatoid Arthritis. Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011
 Rheumatoid Arthritis Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011 The security of experience. The power of innovation. www.rgare.com Case Study
Rheumatoid Arthritis Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011 The security of experience. The power of innovation. www.rgare.com Case Study
1 DOS CME Course 2011
 Statin Myopathy February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation 1 Case 1 50 y/o woman with hyperlipidemia presents with one year history of deep
Statin Myopathy February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation 1 Case 1 50 y/o woman with hyperlipidemia presents with one year history of deep
Acute hot swollen joint. Dr Edward Roddy Senior Lecturer in Rheumatology and Consultant Rheumatologist
 Acute hot swollen joint Dr Edward Roddy Senior Lecturer in Rheumatology and Consultant Rheumatologist Acute monoarthritis: differential diagnosis Septic arthritis Crystal arthritis (gout, pseudogout) Haemarthrosis
Acute hot swollen joint Dr Edward Roddy Senior Lecturer in Rheumatology and Consultant Rheumatologist Acute monoarthritis: differential diagnosis Septic arthritis Crystal arthritis (gout, pseudogout) Haemarthrosis
Coverage Criteria: Express Scripts, Inc. monograph dated 12/15/ months or as otherwise noted by indication
 BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
CME for Family Medicine Specialists. Evelyn Sutton, MD, FRCPC, FACP November 17, 2018
 CME for Family Medicine Specialists Evelyn Sutton, MD, FRCPC, FACP November 17, 2018 Disclosures Received $ from Advisory Board Consultant: Amgen, Abvie, Pfizer, Actelion, Lilly, Grants: Arthritis Society,
CME for Family Medicine Specialists Evelyn Sutton, MD, FRCPC, FACP November 17, 2018 Disclosures Received $ from Advisory Board Consultant: Amgen, Abvie, Pfizer, Actelion, Lilly, Grants: Arthritis Society,
Essential Rheumatology. Dr Ellen Bruce Consultant Rheumatologist CMFT
 Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Understanding Rheumatoid Arthritis
 Understanding Rheumatoid Arthritis Understanding Rheumatoid Arthritis What Is Rheumatoid Arthritis? 1,2 Rheumatoid arthritis (RA) is a chronic autoimmune disease. It causes joints to swell and can result
Understanding Rheumatoid Arthritis Understanding Rheumatoid Arthritis What Is Rheumatoid Arthritis? 1,2 Rheumatoid arthritis (RA) is a chronic autoimmune disease. It causes joints to swell and can result
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Definition and Risk Factors Idiopathic vs. Secondary OA Clinical Features Diagnosis Radiologic Features ACR OA
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Definition and Risk Factors Idiopathic vs. Secondary OA Clinical Features Diagnosis Radiologic Features ACR OA
Case Report Pseudoseptic Arthritis: A Case Series and Review of the Literature
 Case Reports in Infectious Diseases Volume 2011, Article ID 942023, 4 pages doi:10.1155/2011/942023 Case Report Pseudoseptic Arthritis: A Case Series and Review of the Literature Brian P. Oppermann, 1
Case Reports in Infectious Diseases Volume 2011, Article ID 942023, 4 pages doi:10.1155/2011/942023 Case Report Pseudoseptic Arthritis: A Case Series and Review of the Literature Brian P. Oppermann, 1
Scintigraphic Findings and Serum Matrix Metalloproteinase 3 and Vascular Endothelial Growth Factor Levels in Patients with Polymyalgia Rheumatica
 The Open General and Internal Medicine Journal, 29, 3, 53-57 53 Open Access Scintigraphic Findings and Serum Matrix Metalloproteinase 3 and Vascular Endothelial Growth Factor Levels in Patients with Polymyalgia
The Open General and Internal Medicine Journal, 29, 3, 53-57 53 Open Access Scintigraphic Findings and Serum Matrix Metalloproteinase 3 and Vascular Endothelial Growth Factor Levels in Patients with Polymyalgia
ACP Rheumatology Pearls. Adam Q Carlson MD Assistant Professor UVA Rheumatology
 ACP Rheumatology Pearls Adam Q Carlson MD Assistant Professor UVA Rheumatology Disclosures I have no personal or professional disclosures Case #1 27 yo woman with a history of systemic lupus complicated
ACP Rheumatology Pearls Adam Q Carlson MD Assistant Professor UVA Rheumatology Disclosures I have no personal or professional disclosures Case #1 27 yo woman with a history of systemic lupus complicated
Chondrocalcinosis after parathyroidectomy*
 Ann. rheum. Dis. (1976), 35, 521 Chondrocalcinosis after parathyroidectomy* J. S. GLASS AND R. GRAHAME From Guy's Arthritis Research Unit, Guy's Hospital Medical School, London SE] 9RT Glass, J. S., and
Ann. rheum. Dis. (1976), 35, 521 Chondrocalcinosis after parathyroidectomy* J. S. GLASS AND R. GRAHAME From Guy's Arthritis Research Unit, Guy's Hospital Medical School, London SE] 9RT Glass, J. S., and
TAKAYASU S ARTERITIS. Second-stage symptoms include:
 What is Takayasu s arteritis (TAK)? Takayasu s arteritis (TAK) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
What is Takayasu s arteritis (TAK)? Takayasu s arteritis (TAK) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
Preventing blindness: Ultrasound in Giant cell arteritis
 Preventing blindness: Ultrasound in Giant cell arteritis Elizabeth Jernberg, MD Associate Clinical Professor of Medicine Division of Rheumatology University of Washington Virginia Mason Medical Center
Preventing blindness: Ultrasound in Giant cell arteritis Elizabeth Jernberg, MD Associate Clinical Professor of Medicine Division of Rheumatology University of Washington Virginia Mason Medical Center
British Journal of Rheumatology 1991; 30:
 British Journal of Rheumatology 1991; 30:468-470 CASE REPORT CARPAL TUNNEL SYNDROME COMPLICATED BY REFLEX SYMPATHETIC DYSTROPHY SYNDROME BY M.-A. FITZCHARLES AND J.M. ESDAILE Rheumatic Disease Unit, McGill
British Journal of Rheumatology 1991; 30:468-470 CASE REPORT CARPAL TUNNEL SYNDROME COMPLICATED BY REFLEX SYMPATHETIC DYSTROPHY SYNDROME BY M.-A. FITZCHARLES AND J.M. ESDAILE Rheumatic Disease Unit, McGill
A patient reported outcome measure for Giant Cell Arteritis UHBristol Research Showcase Tuesday 31st October 2017
 A patient reported outcome measure for Giant Cell Arteritis UHBristol Research Showcase Tuesday 31st October 2017 Joanna Robson Consultant Senior Lecturer in Rheumatology UHBristol University of the West
A patient reported outcome measure for Giant Cell Arteritis UHBristol Research Showcase Tuesday 31st October 2017 Joanna Robson Consultant Senior Lecturer in Rheumatology UHBristol University of the West
Case Based Rheumatology STEVE S LEE, DO FACR SCPMG FONTANA
 Case Based Rheumatology STEVE S LEE, DO FACR SCPMG FONTANA Disclosure Clinical Investigator: EMD Serono Amgen Roche 1 Learning Objectives Crystalline arthropathy GCA/PMR Infectious arthritis Connective
Case Based Rheumatology STEVE S LEE, DO FACR SCPMG FONTANA Disclosure Clinical Investigator: EMD Serono Amgen Roche 1 Learning Objectives Crystalline arthropathy GCA/PMR Infectious arthritis Connective
Joint Disorders. Musculoskeletal Disorders (Part B-2) Module 7 -Chapter 10. Overview Disorders of the Muscular System Disorders of the Skeletal System
 Module 7 -Chapter 10. Overview Disorders of the Muscular System Disorders of the Skeletal System") Musculoskeletal Disorders (Part B-2) Module 7 -Chapter 10 Overview Disorders of the Muscular System Disorders of the Skeletal System Susie Turner, MD 1/9/13 Joint Disorders Arthritis Inflammation of Joint
Musculoskeletal Disorders (Part B-2) Module 7 -Chapter 10 Overview Disorders of the Muscular System Disorders of the Skeletal System Susie Turner, MD 1/9/13 Joint Disorders Arthritis Inflammation of Joint
Muscle Pathology Surgical Pathology Unknown Conference. November, 2008 Philip Boyer, M.D., Ph.D.
 Muscle Pathology Surgical Pathology Unknown Conference November, 2008 Philip Boyer, M.D., Ph.D. Etiologic Approach to Differential Diagnosis Symptoms / Signs / Imaging / Biopsy / CSF Analysis Normal Abnormal
Muscle Pathology Surgical Pathology Unknown Conference November, 2008 Philip Boyer, M.D., Ph.D. Etiologic Approach to Differential Diagnosis Symptoms / Signs / Imaging / Biopsy / CSF Analysis Normal Abnormal
4 2 Osteoarthritis 1
 Osteoarthritis 1 Osteoarthritis ( OA) Osteoarthritis is a chronic disease and the most common of all rheumatological disorders. It particularly affects individuals over the age of 65 years. The prevalence
Osteoarthritis 1 Osteoarthritis ( OA) Osteoarthritis is a chronic disease and the most common of all rheumatological disorders. It particularly affects individuals over the age of 65 years. The prevalence
UNFOLDING NATURE S ORIGAMI: MEDICAL TREATMENT OF TAKAYASU ARTERITIS AND GIANT CELL ARTERITIS
 UNFOLDING NATURE S ORIGAMI: MEDICAL TREATMENT OF TAKAYASU ARTERITIS AND GIANT CELL ARTERITIS CanVasc meeting Montreal Nov 22 2012 Patrick Liang Service de rhumatologie Centre Hospitalier Universitaire
UNFOLDING NATURE S ORIGAMI: MEDICAL TREATMENT OF TAKAYASU ARTERITIS AND GIANT CELL ARTERITIS CanVasc meeting Montreal Nov 22 2012 Patrick Liang Service de rhumatologie Centre Hospitalier Universitaire
Concise guidance: diagnosis and management of giant cell arteritis
 ONISE GUIDANE linical Medicine 2010, Vol 10, No 4: 381 6 oncise guidance: diagnosis and management of giant cell arteritis Bhaskar Dasgupta on behalf of the Giant ell Arteritis Guideline Development Group*
ONISE GUIDANE linical Medicine 2010, Vol 10, No 4: 381 6 oncise guidance: diagnosis and management of giant cell arteritis Bhaskar Dasgupta on behalf of the Giant ell Arteritis Guideline Development Group*
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
CAN WE REPLACE TEMPORAL ARTERY BIOPSY WITH CRANIAL ULTRASOUND FOR THE DIAGNOSIS OF GIANT CELL ARTERITIS?
 CAN WE REPLACE TEMPORAL ARTERY BIOPSY WITH CRANIAL ULTRASOUND FOR THE DIAGNOSIS OF GIANT CELL ARTERITIS? Adam P. Croft (ST3 Rheumatology) Susan Mollan, Paresh Jobunputra Speaker has no disclosures TAB
CAN WE REPLACE TEMPORAL ARTERY BIOPSY WITH CRANIAL ULTRASOUND FOR THE DIAGNOSIS OF GIANT CELL ARTERITIS? Adam P. Croft (ST3 Rheumatology) Susan Mollan, Paresh Jobunputra Speaker has no disclosures TAB
Rheumatoid Arthritis
 Rheumatoid Arthritis Rheumatoid arthritis (RA) is an autoimmune disease that causes chronic inflammation of the joints. Autoimmune diseases are illnesses that occur when the body's tissues are mistakenly
Rheumatoid Arthritis Rheumatoid arthritis (RA) is an autoimmune disease that causes chronic inflammation of the joints. Autoimmune diseases are illnesses that occur when the body's tissues are mistakenly
Rheumatology Updates for the Primary Care Provider
 Rheumatology Updates for the Primary Care Provider Jean Tayar, MD, RhMSUS Associate Professor Section of Rheumatology and Clinical Immunology Department of General Internal Medicine UT MD Anderson Cancer
Rheumatology Updates for the Primary Care Provider Jean Tayar, MD, RhMSUS Associate Professor Section of Rheumatology and Clinical Immunology Department of General Internal Medicine UT MD Anderson Cancer
Types of osteoarthritis
 ARTHRITIS Osteoarthritis is a degenerative joint disease is the most common joint disorder. It is a frequent part of aging and is an important cause of physical disability in persons older than 65 years
ARTHRITIS Osteoarthritis is a degenerative joint disease is the most common joint disorder. It is a frequent part of aging and is an important cause of physical disability in persons older than 65 years
The many faces of myositis. Marianne de Visser Academic Medical Centre Dept of Neurology Amsterdam The Netherlands
 The many faces of myositis Marianne de Visser Academic Medical Centre Dept of Neurology Amsterdam The Netherlands Outline of the presentation Classification Diagnosis Therapy Prognosis Diagnostic criteria
The many faces of myositis Marianne de Visser Academic Medical Centre Dept of Neurology Amsterdam The Netherlands Outline of the presentation Classification Diagnosis Therapy Prognosis Diagnostic criteria
Arthritis. that affects the joints.
 Arthritis that affects the joints. The word arthritis literally means inflammation of the joints. Though joint inflammation is often a symptom, rather than a specific diagnosis itself, the term arthritis
Arthritis that affects the joints. The word arthritis literally means inflammation of the joints. Though joint inflammation is often a symptom, rather than a specific diagnosis itself, the term arthritis
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 7/28/2012 Radiology Quiz of the Week # 83 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 7/28/2012 Radiology Quiz of the Week # 83 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Case 1: History of J.H. Outside Evaluation. Outside Labs. Question #1
 Case 1: History of J.H. 64 yo man seen at UCSF 6-256 25-07. 9 months ago onset progressive weakness of arms and legs, with muscle atrophy in arms. 4 months ago red scaly rash on face, back of hands and
Case 1: History of J.H. 64 yo man seen at UCSF 6-256 25-07. 9 months ago onset progressive weakness of arms and legs, with muscle atrophy in arms. 4 months ago red scaly rash on face, back of hands and
CIBMTR Center Number: CIBMTR Recipient ID: RETIRED. Today s Date: Date of HSCT for which this form is being completed:
 Juvenile Idiopathic Arthritis Pre-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic, allogeneic,
Juvenile Idiopathic Arthritis Pre-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic, allogeneic,
Mary Derlacki, FNP. No financial relationships to disclose. Office Rheumatology for the Nurse Practitioner. Rheumatoid Arthritis
 Office Rheumatology for the Nurse Practitioner Mary Derlacki, FNP Drs. Cassell and Boren Eugene, OR 541-687-0816 mderlacki@comcast.net No financial relationships to disclose Rheumatoid Arthritis 1% of
Office Rheumatology for the Nurse Practitioner Mary Derlacki, FNP Drs. Cassell and Boren Eugene, OR 541-687-0816 mderlacki@comcast.net No financial relationships to disclose Rheumatoid Arthritis 1% of
ERROR CORRECTION FORM
 Juvenile Idiopathic Arthritis Pre-HSCT Data Sequence Number: Registry Use Only Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic, allogeneic, syngeneic unrelated related
Juvenile Idiopathic Arthritis Pre-HSCT Data Sequence Number: Registry Use Only Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic, allogeneic, syngeneic unrelated related
The Johns Hopkins Hospital
 The Johns Hopkins Hospital 19901006 2016/03/21-04/20 (rheumatology) (emergecny medicine) (rheumatology consult team) attending Dr. Haque, R2 Dr. Michailidou, fellow Dr. Adler "She is a so interesting case.
The Johns Hopkins Hospital 19901006 2016/03/21-04/20 (rheumatology) (emergecny medicine) (rheumatology consult team) attending Dr. Haque, R2 Dr. Michailidou, fellow Dr. Adler "She is a so interesting case.
1.0 Abstract. Title. Keywords. Rationale and Background
 1.0 Abstract Title A Prospective, Multi-Center Study in Rheumatoid Arthritis Patients on Adalimumab to Evaluate its Effect on Synovitis Using Ultrasonography in an Egyptian Population Keywords Synovitis
1.0 Abstract Title A Prospective, Multi-Center Study in Rheumatoid Arthritis Patients on Adalimumab to Evaluate its Effect on Synovitis Using Ultrasonography in an Egyptian Population Keywords Synovitis
Additional File 1. ICD9 Codes for chronic pain related diagnoses Dx Diagnosis Description Codes
 Additional File 1. ICD9 Codes for chronic pain related diagnoses Dx Diagnosis Description Dx Diagnosis Description Codes Codes 327.52 Sleep related leg cramps 717 Old bucket handle tear of medial 333.84
Additional File 1. ICD9 Codes for chronic pain related diagnoses Dx Diagnosis Description Dx Diagnosis Description Codes Codes 327.52 Sleep related leg cramps 717 Old bucket handle tear of medial 333.84
GOUT & PSEUDOGOUT OPSC 2018 HOWARD L. FEINBERG, D.O., F.A.C.O.I.., F.A.C.R.
 GOUT & PSEUDOGOUT OPSC 2018 HOWARD L. FEINBERG, D.O., F.A.C.O.I.., F.A.C.R. Everything in excess is opposed by nature Eunuchs do not take the gout, nor become bald. GOUT Hyperuricemia is not gout Gout
GOUT & PSEUDOGOUT OPSC 2018 HOWARD L. FEINBERG, D.O., F.A.C.O.I.., F.A.C.R. Everything in excess is opposed by nature Eunuchs do not take the gout, nor become bald. GOUT Hyperuricemia is not gout Gout
Rheumatoid Arthritis. By: Hadi Esmaily (PharmD., BCCP, MBA) Department of Clinical Pharmacy, Shahid Beheshti Medical University
 Department of Clinical Pharmacy, Shahid Beheshti Medical University") Rheumatoid Arthritis By: Hadi Esmaily (PharmD., BCCP, MBA) Department of Clinical Pharmacy, Shahid Beheshti Medical University Introduction RA is a Chronic, Systemic, Inflammatory disorder of unknown etiology
Rheumatoid Arthritis By: Hadi Esmaily (PharmD., BCCP, MBA) Department of Clinical Pharmacy, Shahid Beheshti Medical University Introduction RA is a Chronic, Systemic, Inflammatory disorder of unknown etiology
Hths 2231 Laboratory 13 Alterations in Musculoskeletal
 Watch Movie: Osteoporosis Answer the movie questions on the worksheet. Complete activities 1-4. Activity #1: Click on the website link in activity 1 to review the structure and function of bone. Activity
Watch Movie: Osteoporosis Answer the movie questions on the worksheet. Complete activities 1-4. Activity #1: Click on the website link in activity 1 to review the structure and function of bone. Activity
Crystal induced arthropathies. Dr. Amitesh Aggarwal
 Crystal induced arthropathies Dr. Amitesh Aggarwal 1 Crystal induced Arthropathies Gout Pseudogout Debilitating illnesses; Recurrent episodes of pain and joint inflammation; Formation and deposition of
Crystal induced arthropathies Dr. Amitesh Aggarwal 1 Crystal induced Arthropathies Gout Pseudogout Debilitating illnesses; Recurrent episodes of pain and joint inflammation; Formation and deposition of
Enhanced Primary Care Pathway: Gout
 Enhanced Primary Care Pathway: Gout 1. Focused summary of gout relevant to primary care Significance: Gout is a chronic, progressive, inflammatory disease requiring appropriate long-term management. Gout
Enhanced Primary Care Pathway: Gout 1. Focused summary of gout relevant to primary care Significance: Gout is a chronic, progressive, inflammatory disease requiring appropriate long-term management. Gout
Case 27 Clinical Presentation
 53 Case 27 Clinical Presentation 40-year-old man presents with acute shoulder pain and normal findings on radiographs. 54 RadCases Musculoskeletal Radiology Imaging Findings (,) Coronal images of the shoulder
53 Case 27 Clinical Presentation 40-year-old man presents with acute shoulder pain and normal findings on radiographs. 54 RadCases Musculoskeletal Radiology Imaging Findings (,) Coronal images of the shoulder
Arthritis of the Shoulder
 Arthritis of the Shoulder Simply defined, arthritis is inflammation of one or more of your joints. In a diseased shoulder, inflammation causes pain and stiffness. Although there is no cure for arthritis
Arthritis of the Shoulder Simply defined, arthritis is inflammation of one or more of your joints. In a diseased shoulder, inflammation causes pain and stiffness. Although there is no cure for arthritis
Rheumatoid arthritis, seronegative spondylarthritides and gout. György Nagy
 Rheumatoid arthritis, seronegative spondylarthritides and gout György Nagy Dec 4, 2017 Rheumatoid arthritis Rheumatoid arthritis Chronic, progressive, autoimmune disorder of the joints with extra-articular
Rheumatoid arthritis, seronegative spondylarthritides and gout György Nagy Dec 4, 2017 Rheumatoid arthritis Rheumatoid arthritis Chronic, progressive, autoimmune disorder of the joints with extra-articular
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Arthritis of the Shoulder
 Arthritis of the Shoulder In 2011, more than 50 million people in the United States reported that they had been diagnosed with some form of arthritis, according to the National Health Interview Survey.
Arthritis of the Shoulder In 2011, more than 50 million people in the United States reported that they had been diagnosed with some form of arthritis, according to the National Health Interview Survey.
Professor Helen Danesh-Meyer. Eye Institute Auckland
 Professor Helen Danesh-Meyer Eye Institute Auckland Bitten by Ophthalmology Emergencies Helen Danesh-Meyer, MBChB, MD, FRANZCO Sir William and Lady Stevenson Professor of Ophthalmology Head of Glaucoma
Professor Helen Danesh-Meyer Eye Institute Auckland Bitten by Ophthalmology Emergencies Helen Danesh-Meyer, MBChB, MD, FRANZCO Sir William and Lady Stevenson Professor of Ophthalmology Head of Glaucoma
Table S1. Read and ICD 10 diagnosis codes for polymyalgia rheumatica and giant cell arteritis
 SUPPLEMENTARY MATERIAL TEXT Text S1. Multiple imputation TABLES Table S1. Read and ICD 10 diagnosis codes for polymyalgia rheumatica and giant cell arteritis Table S2. List of drugs included as immunosuppressant
SUPPLEMENTARY MATERIAL TEXT Text S1. Multiple imputation TABLES Table S1. Read and ICD 10 diagnosis codes for polymyalgia rheumatica and giant cell arteritis Table S2. List of drugs included as immunosuppressant
Pain or stiffness in joints after periods of inactivity or excessive use
 Arthritis Awareness* Some older adults call it Arthur ; others refer to it as their constant compassion, but most describe it as extremely painful Arthritis is a chronic joint disease It is commonly believed
Arthritis Awareness* Some older adults call it Arthur ; others refer to it as their constant compassion, but most describe it as extremely painful Arthritis is a chronic joint disease It is commonly believed
ORIGINAL INVESTIGATION
 ORIGINAL INVESTIGATION Corticosteroid Requirements in Polymyalgia Rheumatica Cornelia M. Weyand, MD; James W. Fulbright, MS; Jonathan M. Evans, MD; Gene G. Hunder, MD; Jörg J. Goronzy, MD, PhD Background:
ORIGINAL INVESTIGATION Corticosteroid Requirements in Polymyalgia Rheumatica Cornelia M. Weyand, MD; James W. Fulbright, MS; Jonathan M. Evans, MD; Gene G. Hunder, MD; Jörg J. Goronzy, MD, PhD Background:
Gout -revisited. Shrenik Shah
 Gout -revisited Shrenik Shah definition Monosodium urate (MSU) crystal deposition episodic and later persistent joint inflammation and tophi All MSU crystal deposition- broader definition EULAR- European
Gout -revisited Shrenik Shah definition Monosodium urate (MSU) crystal deposition episodic and later persistent joint inflammation and tophi All MSU crystal deposition- broader definition EULAR- European
Musculoskeletal Infection and Inflammation
 F.A. Davis: Advantage Musculoskeletal Infection and Inflammation(10.6.15) Page 1 Musculoskeletal Infection and Inflammation The musculoskeletal system is affected by infections and inflammatory conditions.
F.A. Davis: Advantage Musculoskeletal Infection and Inflammation(10.6.15) Page 1 Musculoskeletal Infection and Inflammation The musculoskeletal system is affected by infections and inflammatory conditions.
Identifying statin-associated autoimmune necrotizing myopathy
 REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will recognize autoimmune necrotizing myopathy if it occurs in their patients taking statins JEMIMA ALBAYDA, MD Division of Rheumatology, Department of
REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will recognize autoimmune necrotizing myopathy if it occurs in their patients taking statins JEMIMA ALBAYDA, MD Division of Rheumatology, Department of
2017 PERIOPERATIVE MEDICINE SYMPOSIUM Peri-operative use of immunosuppression in rheumatology patients
 2017 PERIOPERATIVE MEDICINE SYMPOSIUM Peri-operative use of immunosuppression in rheumatology patients Dr Alberta Hoi Rheumatologist MBBS, FRACP, PhD NEW ERA IN MUSCULOSKELETAL MEDICINE New drugs - Biologics,
2017 PERIOPERATIVE MEDICINE SYMPOSIUM Peri-operative use of immunosuppression in rheumatology patients Dr Alberta Hoi Rheumatologist MBBS, FRACP, PhD NEW ERA IN MUSCULOSKELETAL MEDICINE New drugs - Biologics,
Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis
 Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis JIA is the most common rheumatic disease in childhood and a major cause of chronic disability. Etiology: Unknown, but may
Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis JIA is the most common rheumatic disease in childhood and a major cause of chronic disability. Etiology: Unknown, but may
Gout. Crystal deposition disease: Imaging perspectives. Crystal associated arthropathies. Clinical Stages of Gout 07/06/60
 Crystal associated arthropathies Crystal deposition disease: Imaging perspectives Warapat Virayavanich, MD Ramathibodi hospital, Mahidol University Commonly seen arthropathy MSU (gout) CPPD HADD Uncommon
Crystal associated arthropathies Crystal deposition disease: Imaging perspectives Warapat Virayavanich, MD Ramathibodi hospital, Mahidol University Commonly seen arthropathy MSU (gout) CPPD HADD Uncommon
Mr. OA: Case Presentation
 CLINICAL CASES Case 1: Mr. OA OA Mr. OA: Case Presentation 62-year-old lawyer Mild left knee pain for 3 month, but became worse 1 week ago No swelling 1 week earlier: 2-hour walk in the countryside 2 days
CLINICAL CASES Case 1: Mr. OA OA Mr. OA: Case Presentation 62-year-old lawyer Mild left knee pain for 3 month, but became worse 1 week ago No swelling 1 week earlier: 2-hour walk in the countryside 2 days
Vasculitis. Edward Dwyer, M.D. Division of Rheumatology. Vasculitis
 Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Neuro-Ocular Grand Rounds
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
SEPTIC ARTHRITIS. Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA. University of Science and technology Hospital Sanaa Yemen 18/Dec/2014
 SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
4/16/2018. Demystifying weakness: how to approach refractory myositis. Objectives. Disclosures. Off-label uses for medications will be discussed
 Demystifying weakness: how to approach refractory myositis Jemima Albayda, MD Assistant Professor Johns Hopkins Myositis center Disclosures Off-label uses for medications will be discussed Objectives To
Demystifying weakness: how to approach refractory myositis Jemima Albayda, MD Assistant Professor Johns Hopkins Myositis center Disclosures Off-label uses for medications will be discussed Objectives To
Clinical Commissioning Policy Proposition: Tocilizumab for Giant cell arteritis (adults)
") Clinical Commissioning Policy Proposition: Tocilizumab for Giant cell arteritis (adults) Version Number: NHS England A13X12/01 Information Reader Box (IRB) to be inserted on inside front cover for documents
Clinical Commissioning Policy Proposition: Tocilizumab for Giant cell arteritis (adults) Version Number: NHS England A13X12/01 Information Reader Box (IRB) to be inserted on inside front cover for documents
Evaluation and Management of Knee Pain. Michael Cassat, MD University of Arkansas for Medical Sciences
 Evaluation and Management of Knee Pain Michael Cassat, MD University of Arkansas for Medical Sciences Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
Evaluation and Management of Knee Pain Michael Cassat, MD University of Arkansas for Medical Sciences Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.