Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
|
|
|
- Bernice Barber
- 5 years ago
- Views:
Transcription


1 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin
2 Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the obese patient 4. Antibiotics for respiratory infections Some sweeping generalisations
3 Acute severe asthma
4 Problems with assessment Studies show severity assessment is done poorly by SMOs, RMOs and nurses Over-reliance on the end of the bed assessment
5 Best markers on history Recent hospital admission Previous ICU admission (ever) β-agonist use last 24 hours
6 4 clinical markers of: 1. Severe asthma 2. Life-threatening asthma
7 Severe asthma Any one of 1. PEFR < 50% 2. Heart rate > 110/min 3. Resp rate > 24/min 4. Unable to complete a sentence
8 Any one of Life threatening asthma 1. PEFR < 33% 2. PaO 2 < 55mmHg despite oxygen 3. Normal or elevated PaCO 2 4. Drowsy, confused, exhausted, silent chest
9 Management Oxygen Bronchodilators Corticosteroids Magnesium IV Salbutamol? IV aminophylline? NIV?
10 Randomised controlled trial of high concentration versus titrated oxygen therapy in acute severe asthma Perrin et al Thorax 2011; 66:
11 The proportion of patients with a rise in PtCO 2 from baseline at 60 minutes High concentration n (%) Titrated n (%) Relative risk (95% CI) P value Change in PtCO 2 4 mmhg 22 (44%) 10 (19%) 2.3 (1.2 to 4.4) Change in PtCO 2 8 mmhg 11 (22%) 3 (6%) 3.9 (1.2 to 13.1) 0.016
12 Improvement in PEF, PaCO 2 and clinical index before and after treatment 200 NEB group IV group PEF PaCO 2 Clinical index Time (hours) Salmeron et al. Am J Respir Crit Care Med 1994; 149:
13 Acute exacerbations of COPD
14 What are they? A change in the patient's baseline dyspnea, cough, and/or sputum that is beyond normal day-to-day variations, is acute in onset, and may warrant a change in regular medication
15 Pneumonia What are they not? LVF PE Pneumothorax
16 Standard management Titrated oxygen therapy Evidence grade A Short acting bronchodilators Evidence grade C Corticosteroids Evidence grade A Antibiotics Evidence grade B/C
17 John 68 years with moderately severe COPD FEV1 40% predicted Smokes 2-3 cigarettes a day Works as a petrol station attendant Normally SOB on moderate exertion
18 John Developed SOB, wheeze and cough with green sputum 4 days ago SOB worsened over the next 3 days By the morning of admission was SOB at rest and called the ambulance
19 Alert and afebrile Examination RR 32/min, not able to speak in sentences O2 sats 95% on 6L via a Hudson mask Chest hyper-resonant with quiet breath sounds FBC and CRP normal

20
21 Diagnosis Acute exacerbation COPD
22 1 st ABG After 20 minutes in ED (on 6L/min oxygen) ph 6.7 CO 2 81 O HCO 3 23
23 Initial Management Prednisone Oral augmentin Nebulised bronchodilators O2 therapy titrated down to 3-4L/min NP Sats 88%
24 Review 1 hour later RR remains 30/min Sats 85-89% on 3-4L O2 2 nd ABG ph 6.8 CO2 84 O2 59 HCO3 28
25 What now? Most appropriate next management is ICU for consideration of invasive ventilation
26 Management Admitted to HDB, trial of NIV Poorly tolerant of mask, problem with leaks 3 further ABGs with little improvement Referred to ICU at 3am
27 The risk of serious adverse outcomes associated with hypoxaemia and hyperoxaemia in acute exacerbations of COPD Cameron L, Pilcher J, Weatherall M, Beasley R, Perrin K Postgraduate Medical Journal 2012 (in press)
28
29
30 Results Clinical data for 9716 patients were received from 232 units Overall mean age was 73 Mean FEV 1 % predicted was 42% In-hospital mortality was 7.7% 90day mortality was 13.9%
31 Results Many had severe acidosis with NIV used as the ceiling of care Some with metabolic acidosis receive NIV inappropriately while a proportion of patients who meet the RCT inclusion criteria of persisting respiratory acidosis do not receive NIV NIV was often given late
32 Results In 12% of cases managed with NIV who subsequently died there was no plan in the case notes of what the ceiling of treatment was in the event of failure of NIV In 30% of cases who died following NIV a DNR order was not signed
33 Results The observed mortality in patients treated with NIV was higher than patients matched by arterial blood gas ph who did not receive NIV Only 1% were intubated
34 Results In contrast, the group of patients for whom there exists the strongest evidence base for the effectiveness of NIV (ph range of ) form only a minority of those overall receiving NIV
35 What's going on?
36 Obesity
37 Obstructive sleep apnoea Upper airway obstruction during sleep leads to frequent nocturnal arousals Main clinical symptom is daytime somnolence Other adverse physiological effects (cardiovascular) The majority of patients have normal daytime ventilation and gas exchange (normal PaO 2 and PaCO 2 )
38 Obesity-hypoventilation syndrome Definition Obesity associated with daytime hypercapnia (type 2 respiratory failure) in the absence of pulmonary disease or airflow obstruction May overlap with OSA but some obese people have predominantly OHS
39 Obesity-hypoventilation syndrome Can lead to Chronic hypoxia Polycythemia Pulmonary hypertension Right heart failure Death
40 Obesity-hypoventilation syndrome Why do some obese people develop daytime respiratory failure but most don't? Mechanical loading vs. Central control Patients with OHS normalise their PaCO 2 with voluntary hyperventilation with no change in lung mechanics/volumes
41 Obesity-hypoventilation syndrome Most people with OHS who present acutely will not have an established diagnosis Low threshold for an ABG in obese patients with hypoxaemia A screening serum bicarbonate is a useful test Bi-level NIV is the treatment of choice.
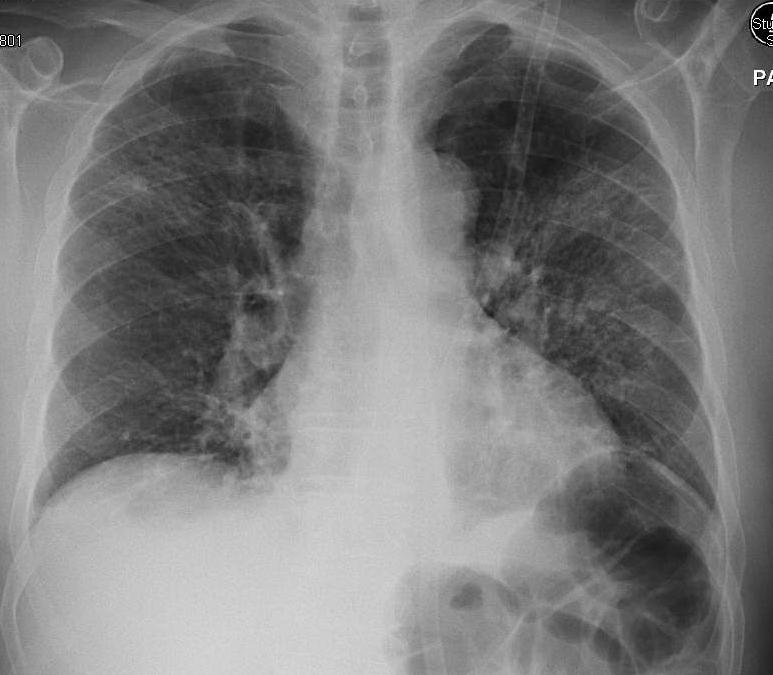
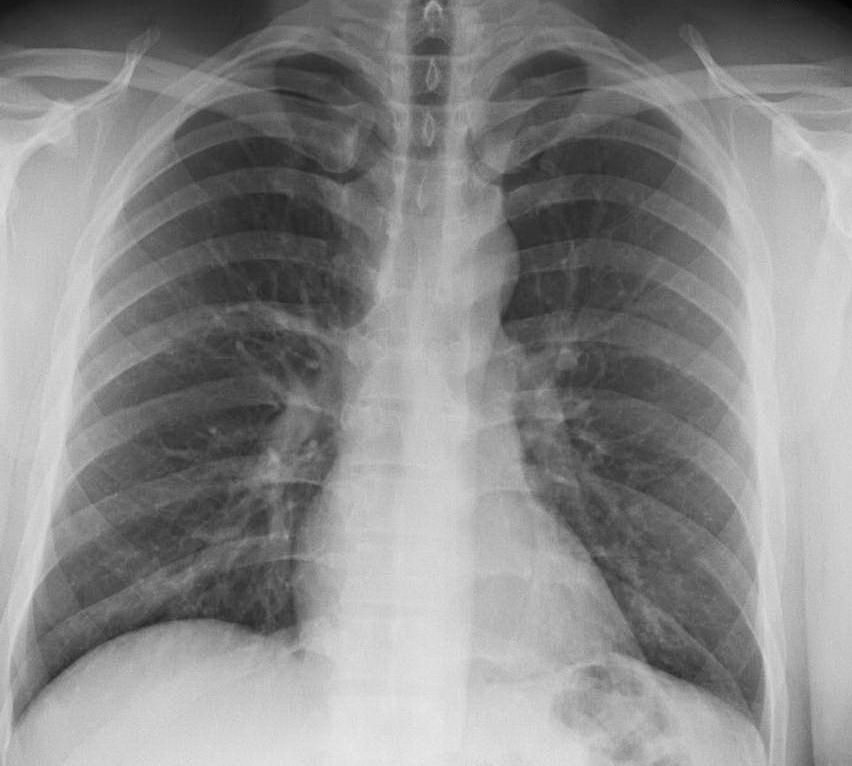
42 Normal
43 OSA
44 OSA with severe OHS
45 Antibiotics for respiratory infections
46 Case 1: David 26 year old non-smoking student 2-3 days of fever and malaise, now coughing rusty sputum with left sided pleurisy O/E Temp 39, RR 24/min, HR 90/min, BP 120/82 Sats 93% Left basal crackles WCC 16

47
48 Diagnosis and management? Mild CAP CURB65 score 0/5 Discharge on oral antibiotics amoxicillin and roxithromycin (CCDHB guidelines)
49 Given: IV cefuroxime Oral roxithromycin
50 Case 2 82 yr old widower lives alone and normally quite well,1 hour per day home help Ex smoker but no COPD 1 week of cough and fatigue then feverish for 2 days so stayed in bed Found by carer on floor.
51 Case 2 O/E slightly drowsy (GCS 14) but rousable AMT 6/10 BP 98/55, HR 110/min, RR 26/min Sats 90% on 4L/min Bilateral crackles Bloods WCC 24, CRP 228, Cr 124
52
53 Diagnosis and management? Severe CAP CURB65 score 4/5 Admit ICU consult to determine ceiling of care IV cefuroxime IV erythromycin
54 Given: IV cefuroxime Oral roxithromycin
55 Case 3 57 year old truck driver with longstanding idiopathic bronchiectasis Normally produces 1-2 cups of green sputum per day Unwell for 3 days with increased sputum volume and darker colour. Increased SOB but no fever
56 Case 3 O/E Afebrile BP and HR normal Sats 95% RA, RR 20/min Coarse crackles both lung bases Bloods all normal
57
58 Diagnosis and management? Exacerbation of bronchiectasis with no pneumonia Review previous sputum samples (in his case usually grows haemophillus) Augmentin a reasonable empirical treatment No need for atypical cover if no pneumonia
59 Given: IV cefuroxime Oral roxithromycin
60 Case 4 71 year old, lives with husband, diagnosed with COPD (FEV1 around 40% predicted) Manages all daily activities but SOB up stairs Unwell with cold 3 days ago, now coughing green sputum and breathless with daily activities
61 Case 4 O/E Alert and speaking sentences Fruity cough Afebrile RR 24/min, sats 90% RA, BP and HR normal Hyper-inflated with reduced breath sounds but nothing else

62
63 Diagnosis and management? Acute exacerbation of COPD (not pneumonia) Oral antibiotics, choose one from: Augmentin Doxycyline Cefaclor
64 Given: IV cefuroxime Oral roxithromycin
65 Message Avoid the term chest infection Be as precise as you can with what you are treating and do a severity assessment in CAP There will always be grey areas, so some patients need broad spectrum IV treatment at the front door, but modify the next day!
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Bronchospasm & SOB. Kim Kilmurray Senior Clinical Teaching Fellow
 Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Acute NIV in COPD and what happens next. Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital
 Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
COPD Challenge CASE PRESENTATION
 Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Exacerbations. Ronald Dahl, Aarhus University Hospital, Denmark
 1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
SIMPLY Arterial Blood Gases Interpretation. Week 4 Dr William Dooley
 SIMPLY Arterial Blood Gases Interpretation Week 4 Dr William Dooley Plan Structure for interpretation 5-step approach Works for majority of cases Case scenarios Some common concerns A-a gradient BE Anion
SIMPLY Arterial Blood Gases Interpretation Week 4 Dr William Dooley Plan Structure for interpretation 5-step approach Works for majority of cases Case scenarios Some common concerns A-a gradient BE Anion
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
Respiratory Failure how the respiratory physicians deal with airway emergencies
 Respiratory Failure how the respiratory physicians deal with airway emergencies Dr Michael Davies MD FRCP Consultant Respiratory Physician Respiratory Support and Sleep Centre Papworth Hospital NHS Foundation
Respiratory Failure how the respiratory physicians deal with airway emergencies Dr Michael Davies MD FRCP Consultant Respiratory Physician Respiratory Support and Sleep Centre Papworth Hospital NHS Foundation
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Management of acute asthma in children in emergency department. Moderate asthma
 152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
2/13/2018 OBESITY HYPOVENTILATION SYNDROME
 OBESITY HYPOVENTILATION SYNDROME David Claman, MD UCSF Professor of Medicine Director, UCSF Sleep Disorders Center Disclosures: None. 1 COMPLICATIONS OF OSA Cardiovascular HTN, CHF, CVA, arrhythmia, Pulm
OBESITY HYPOVENTILATION SYNDROME David Claman, MD UCSF Professor of Medicine Director, UCSF Sleep Disorders Center Disclosures: None. 1 COMPLICATIONS OF OSA Cardiovascular HTN, CHF, CVA, arrhythmia, Pulm
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Oxygen: Is there a problem? Tom Heaps Acute Physician
 Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic
 COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Oxygen therapy increases the arterial partial pressure of
 High flow or titrated oxygen for obese medical inpatients: a randomised crossover trial Janine Pilcher 1, Michael Richards 1, Leonie Eastlake 1, Steven J McKinstry 1, George Bardsley 1, Sarah Jefferies
High flow or titrated oxygen for obese medical inpatients: a randomised crossover trial Janine Pilcher 1, Michael Richards 1, Leonie Eastlake 1, Steven J McKinstry 1, George Bardsley 1, Sarah Jefferies
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
Allwin Mercer Dr Andrew Zurek
 Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
(To be filled by the treating physician)
") CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
COPD Treatable. Preventable.
 My COPD Action Plan Patient s Copy (Patient s Name) Date Canadian Respiratory COPD Treatable. Preventable. This is to tell me how I will take care of myself when I have a COPD flare-up. My goals are My
My COPD Action Plan Patient s Copy (Patient s Name) Date Canadian Respiratory COPD Treatable. Preventable. This is to tell me how I will take care of myself when I have a COPD flare-up. My goals are My
Management of Acute Exacerbations
 15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
A whistle stop tour of Respiratory Medicine and what the RUH & IMPACT offer
 A whistle stop tour of Respiratory Medicine and what the RUH & IMPACT offer Jay Suntharalingam, Respiratory Physician, RUH Claire Bullard, IMPACT Team Leader, Sirona Outline Respiratory 5 year strategy
A whistle stop tour of Respiratory Medicine and what the RUH & IMPACT offer Jay Suntharalingam, Respiratory Physician, RUH Claire Bullard, IMPACT Team Leader, Sirona Outline Respiratory 5 year strategy
Over the last several years various national and
 Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Deep discoveries: the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine
 Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine") Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
Chris Cameron Clinical pharmacologist & General Physician CCDHB. Oxygen- A prescribing Blindspot?
 Chris Cameron Clinical pharmacologist & General Physician CCDHB Oxygen- A prescribing Blindspot? Ms J, 70yo Lives with partner, who has a recent diagnosis of breast cancer Works 3 days a week Weight 46kg
Chris Cameron Clinical pharmacologist & General Physician CCDHB Oxygen- A prescribing Blindspot? Ms J, 70yo Lives with partner, who has a recent diagnosis of breast cancer Works 3 days a week Weight 46kg
1. What is delayed sequence intubation? Can it be used for severe Asthma exacerbation? 2. What about pregnancy and Asthma is so important?
 Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
Supplementary Online Content
 Supplementary Online Content Murphy PB, Rehal S, Arbane G, et al. Effect of home noninvasive ventilation with oxygen therapy vs oxygen therapy alone on hospital readmission or death after an acute COPD
Supplementary Online Content Murphy PB, Rehal S, Arbane G, et al. Effect of home noninvasive ventilation with oxygen therapy vs oxygen therapy alone on hospital readmission or death after an acute COPD
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Guideline on the Management of Asthma in adults SHSCT
 CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Management of Asthma in adults Dr A John, Dr J Lindsay Respiratory Medicine/ MUSC Medicine Date Uploaded: 23/11/15 Review Date
CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Management of Asthma in adults Dr A John, Dr J Lindsay Respiratory Medicine/ MUSC Medicine Date Uploaded: 23/11/15 Review Date
Management of acute severe asthma in adults in general practice. Moderate asthma Acute severe asthma Life-threatening asthma INITIAL ASSESSMENT
 British guideline on the management of asthma Annex 2 Management of acute severe asthma in adults in general practice Many deaths from asthma are preventable. Delay can be fatal. Factors leading to poor
British guideline on the management of asthma Annex 2 Management of acute severe asthma in adults in general practice Many deaths from asthma are preventable. Delay can be fatal. Factors leading to poor
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Chronic Obstructive Pulmonary Disease (COPD)
") Chronic Obstructive Pulmonary Disease (COPD) Definition of COPD Airflow obstruction that is: o Not fully reversible o Progressive o Does not change markedly over several months Combination of airway and
Chronic Obstructive Pulmonary Disease (COPD) Definition of COPD Airflow obstruction that is: o Not fully reversible o Progressive o Does not change markedly over several months Combination of airway and
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
10/17/16. Acute Respiratory Failure in the Acute Care Setting. Margaret Rosales, APRN-CNP, FNP
 Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Safer Tracheostomy Care Course
 Patients Name: Samira Patel Patients Age / DOB: 65 year old female on a general ward Major Medical Problem Blocked tracheostomy tube Learning Goal Medical Early recognition of respiratory distress Understanding
Patients Name: Samira Patel Patients Age / DOB: 65 year old female on a general ward Major Medical Problem Blocked tracheostomy tube Learning Goal Medical Early recognition of respiratory distress Understanding
COPD exacerbation. Dr. med. Frank Rassouli
 Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
ASTHMA (SEE BTS GUIDELINES NEXT PAGE)
") ASTHMA (SEE BTS GUIDELINES NEXT PAGE) RESPIRATORY Signs of Severe asthma Unable to speak in sentences? Peak flow < 50% predicted or best? Respiratory Rate >25/min? Pulse>110/min? Sa0 2
ASTHMA (SEE BTS GUIDELINES NEXT PAGE) RESPIRATORY Signs of Severe asthma Unable to speak in sentences? Peak flow < 50% predicted or best? Respiratory Rate >25/min? Pulse>110/min? Sa0 2
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
Title Protocol for the Management of Asthma
 Document Control Title Protocol for the Management of Asthma Author Author s job title Professional Lead, Minor Injuries Unit Directorate Emergency Services, Logistics and Resilience Department Version
Document Control Title Protocol for the Management of Asthma Author Author s job title Professional Lead, Minor Injuries Unit Directorate Emergency Services, Logistics and Resilience Department Version
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
1. What is the acid-base disturbance in this patient?
 /ABG QUIZ QUIZ 1. What is the acid-base disturbance in this patient? Presenting complaint: pneumonia 1 point Uncompensated metabolic alkalosis Partially compensated respiratory alkalosis Mixed alkalosis
/ABG QUIZ QUIZ 1. What is the acid-base disturbance in this patient? Presenting complaint: pneumonia 1 point Uncompensated metabolic alkalosis Partially compensated respiratory alkalosis Mixed alkalosis
BTS Guideline for Home Oxygen use in adults Appendix 9 (online only) Key Questions - PICO 10 December 2012
 Key Questions - PICO 10 December 2012") BTS Guideline for Home Oxygen use in adults Appendix 9 (online only) Key Questions - PICO 10 December 2012 Evidence base for Home Oxygen therapy in COPD, non-copd respiratory disease and nonrespiratory
BTS Guideline for Home Oxygen use in adults Appendix 9 (online only) Key Questions - PICO 10 December 2012 Evidence base for Home Oxygen therapy in COPD, non-copd respiratory disease and nonrespiratory
This is a cross-sectional analysis of the National Health and Nutrition Examination
 SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
Asthma/wheeze management plan
 Asthma/wheeze management plan Name of Patient Date of Birth NHS Number GP surgery Telephone Next appointment Children s Assessment unit/ward telephone Out of hours call 111 Open access Y/N Until date Some
Asthma/wheeze management plan Name of Patient Date of Birth NHS Number GP surgery Telephone Next appointment Children s Assessment unit/ward telephone Out of hours call 111 Open access Y/N Until date Some
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
Learning Lessons from Complaints to the Ombudsman Charles Turton. Society for Acute Medicine May 2013
 Learning Lessons from Complaints to the Ombudsman Charles Turton Society for Acute Medicine May 2013 Society for Acute Medicine The Parliamentary and Health Service Ombudsman Final Stage of NHS Complaints
Learning Lessons from Complaints to the Ombudsman Charles Turton Society for Acute Medicine May 2013 Society for Acute Medicine The Parliamentary and Health Service Ombudsman Final Stage of NHS Complaints
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Referring for specialist respiratory input. Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL
 Referring for specialist respiratory input Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL Respiratory Specialist- who? GPSI Community Team Secondary Care Respiratory physician and
Referring for specialist respiratory input Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL Respiratory Specialist- who? GPSI Community Team Secondary Care Respiratory physician and
Clinical guideline for acute wheeze & asthma in children 5 years and over Hospital care
 Clinical guideline for acute wheeze & asthma in children years and over Hospital care Airedale NHS Trust Bradford Teaching Hospitals NHS Foundation Trust NHS Bradford and Airedale DOB: A&E/Hospital : Weight:
Clinical guideline for acute wheeze & asthma in children years and over Hospital care Airedale NHS Trust Bradford Teaching Hospitals NHS Foundation Trust NHS Bradford and Airedale DOB: A&E/Hospital : Weight:
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research
 Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Acute noninvasive ventilation what s the evidence? Respiratory Medicine Update: Royal College of Physicians & BTS Thu 28 th January 2016
 Acute noninvasive ventilation what s the evidence? Respiratory Medicine Update: Royal College of Physicians & BTS Thu 28 th January 2016 Annabel Nickol Consultant in Respiratory Medicine, Sleep & Ventilation
Acute noninvasive ventilation what s the evidence? Respiratory Medicine Update: Royal College of Physicians & BTS Thu 28 th January 2016 Annabel Nickol Consultant in Respiratory Medicine, Sleep & Ventilation
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Acute Respiratory Emergencies. Martin Johnson Consultant Physician Gartnavel / Western
 Acute Respiratory Emergencies Martin Johnson Consultant Physician Gartnavel / Western Summary What to expect - what are the common respiratory emergencies? How to recognise the problem? How to manage the
Acute Respiratory Emergencies Martin Johnson Consultant Physician Gartnavel / Western Summary What to expect - what are the common respiratory emergencies? How to recognise the problem? How to manage the
Tracheostomy Sim Course
 Patients Name: Robert Smith Patients Age / DOB: 45 year old gentleman on medical ward Major Medical Problem Displaced tracheostomy tube Learning Goal Medical Early recognition of displaced tracheostomy
Patients Name: Robert Smith Patients Age / DOB: 45 year old gentleman on medical ward Major Medical Problem Displaced tracheostomy tube Learning Goal Medical Early recognition of displaced tracheostomy
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
COPD GOLD Guidelines & Barnet inhaler choices. Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust
 COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
Managing Exacerbations of COPD (Version 3.0)
") Managing Exacerbations of COPD (Version 3.0) Guideline Readership This guideline is intended for use in patients with a confirmed diagnosis of a chronic obstructive pulmonary disease (COPD) exacerbation.
Managing Exacerbations of COPD (Version 3.0) Guideline Readership This guideline is intended for use in patients with a confirmed diagnosis of a chronic obstructive pulmonary disease (COPD) exacerbation.
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS
 RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
CLINICAL PATHWAY. Acute Medicine. Chronic Obstructive Pulmonary Disease
 CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Web Appendix 1: Literature search strategy. BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up. Sources to be searched for the guidelines;
 write-up. Sources to be searched for the guidelines;") Web Appendix 1: Literature search strategy BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up Sources to be searched for the guidelines; Cochrane Database of Systematic Reviews (CDSR) Database of
Web Appendix 1: Literature search strategy BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up Sources to be searched for the guidelines; Cochrane Database of Systematic Reviews (CDSR) Database of
By Mark Bachand, RRT-NPS, RPFT. I have no actual or potential conflict of interest in relation to this presentation.
 By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Pulmonary Emergencies. Emergency Medicine Clerkship Lecture Series Primary Author: David Gordon, MD Edited: Darren Manthey, MD 4/2012
 Pulmonary Emergencies Emergency Medicine Clerkship Lecture Series Primary Author: David Gordon, MD Edited: Darren Manthey, MD 4/2012 Learning Objectives Review commonly encountered pulmonary emergencies
Pulmonary Emergencies Emergency Medicine Clerkship Lecture Series Primary Author: David Gordon, MD Edited: Darren Manthey, MD 4/2012 Learning Objectives Review commonly encountered pulmonary emergencies
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist. This program has been approved for 1 hour of continuing education credit.
 Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
2 nd Year Revision Respiratory. Michael Hodkinson
 2 nd Year Revision Respiratory Michael Hodkinson Before we start This is a quick run through of topics Obviously there will be more to learn than what s in these slides but hopefully it will provide a
2 nd Year Revision Respiratory Michael Hodkinson Before we start This is a quick run through of topics Obviously there will be more to learn than what s in these slides but hopefully it will provide a
Paediatric Wheeze and pneumonia. RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa
 Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Acute Respiratory Infection. Dr Anthony Gibson
 Acute Respiratory Infection Dr Anthony Gibson Range of Conditions Upper tract Common Cold coryza Sore Throat- Pharyngitis Sinusitis Epiglottitis Range of Conditions Lower Acute Bronchitis Acute Exacerbation
Acute Respiratory Infection Dr Anthony Gibson Range of Conditions Upper tract Common Cold coryza Sore Throat- Pharyngitis Sinusitis Epiglottitis Range of Conditions Lower Acute Bronchitis Acute Exacerbation
Reference Guide for Group Education
 A p l a n o f a c t i o n f o r l i f e Reference Guide for Group Education Session 5 Plan of Action: Part I Overview of the Plan of Action and Management of Respiratory Infections Plan of Action: Objectives
A p l a n o f a c t i o n f o r l i f e Reference Guide for Group Education Session 5 Plan of Action: Part I Overview of the Plan of Action and Management of Respiratory Infections Plan of Action: Objectives
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease