Pneumonia in the Hospitalized
|
|
|
- Raymond Bond
- 5 years ago
- Views:
Transcription
1 Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic
2 Facts About Pneumonia CAP is the 8 th most common cause of death in the USA In 2006, 1.3 million hospitalizations for pneumonia. 30 day mortality rate for CAP patients requiring hospitalization is about 12%. ALA 2010 NEJM 2015
3 Definition of Infectious Pneumonia Acute infectious process involving the parenchyma of the lung. Requires x-ray evidence or CT chest evidence to really call it pneumonia Pathogens gain access to the lung by micro aspiration, hematogenous spread, direct spread from contiguous focus. Despite current diagnostic tests, no pathogen was detected in the majority of patients diagnosed with pneumonia. (23% viral, 11% bacterial, 1% fungal) ALA 2010 NEJM 2015
4 Community Acquired LUL Pneumonia
5 Causes of Radiographic Pneumonia Viral infections Bacterial infections Fungal infections Drugs reactions Amiodarone, methotrexate, cancer immunotherapies Inhalational exposures Crack cocaine Inflammatory causes Systemic vasculitis, BOOP, eosinophilic pneumonia, sarcoidosis Pulmonary edema Pulmonary embolism with infarct
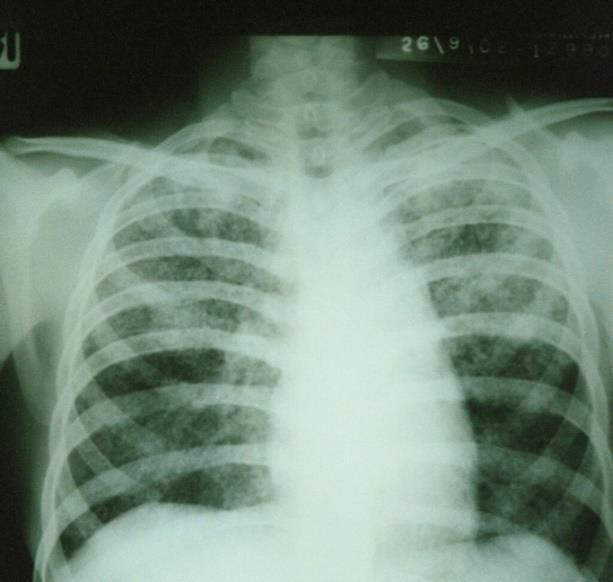
6 Community Acquired Bilateral Pneumonia
7 IDS Guidelines for Treatment of Inpatient Pneumonia General Floor Admission Macrolide plus Ceftriaxone Doxycycline plus Ceftriaxone Fluoroquinolone ICU Admission Macrolide plus Ceftriaxone Fluoroquinolone plus Ceftriaxone Underlying risk factors: add Vancomycin, add extended spectrum beta lactam Clinic Infectious Disease 2007
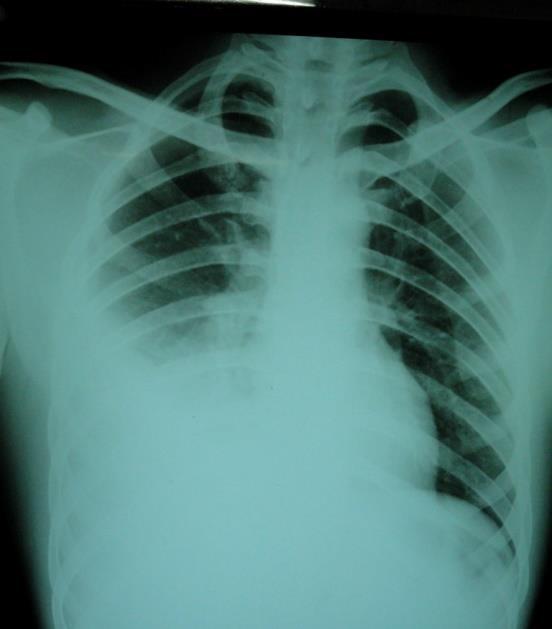
8 Community Acquired RUL Pneumonia
9 ? Admit or Not? General Medicine vs ICU CURB-65 Confusion, Bun >20,RR > 30, BP systolic < 90 or diastolic < 60, Age > 65 yr Pneumonia Severity Index (PSI) 20 different risk factors with point assignment and risk stratification I-V IDS Guidelines Recommend ICU admission RR>30, PaO2/FiO2 <250, multilobar infiltrate, confusion, BUN>20, WBC<4, platelets<100,t<36, hypotension requiring fluid resuscitation
10 What is Happening at a Cellular Level in Pneumonia? Pathogen enters lungs and innate immune system fails to clear pathogen. Cytokine mediated systemic inflammatory response good and bad Local inflammation impairs alveolar gas exchange Systemic inflammation leads to other organ dysfunction Dysregulated immune response Antibiotics target the invading organism but not the immune system. Can systemic steroids attenuate inflammatory response and improve outcome?
11 CT Chest: RUL pneumonia
12 Is There a Role for Steroids in Conjunction with Antibiotics? Multiple studies have been done suggesting steroids may be beneficial. Annals of Internal Medicine 2015 JAMA 2015 Chest Medicine 2016 JAMA 2017 Cochrane Database 2017.
13 Corticosteroid Therapy for Patients Hospitalized with Community Acquired Pneumonia. Systematic Review and Meta-analysis: 13 randomized controlled trials for total 2005 patients. Examine effect of adjunctive corticosteroid therapy on mortality, morbidity, and duration of hospitalization in CAP Various formulations of steroids used: 1 dose 10 days All cause mortality 7.9% control group and 5.3% steroid group RR, 0.67 (CI ) Stratified to severe pneumonia 6 studies RR, 0.39 (CI ) 5% Reduction in need for mechanical ventilation RR 0.45 (CI ) 5% Reduction in risk for ARDS with steroids RR, 0.24 (CI ) Reduction in length of hospitalization by 1 day (CI to -0.21) Annals of Internal Medicine 2015
14 Effect of Corticosteroids on Treatment Failure Among Hospitalized patients with Severe CAP and High Inflammatory Response. Randomized Clinical Trial, double blind, placebo controlled, multicenter Severe CAP and CRP > 150mg/L (convert to mmol/l multiply by 9.524) Methylprednisolone 0.5mg/kg q12 hr x 5 days vs placebo started within 36 hrs of hospitalization Primary outcome: treatment failure (composite outcome early and late) Early treatment failure Development of shock Need for mechanical ventilation Death within 72 hrs Late treatment failure Radiographic progression Persistence of severe respiratory failure Development of shock Need for mechanical ventilation Death between hrs JAMA 2015
15 Effect of Corticosteroids on Treatment Failure Among Hospitalized patients with Severe CAP and High Inflammatory Response. Secondary outcome: in hospital mortality Less treatment failure in steroid group 13% vs 31% (P=.02) Decrease in radiographic progression and late appearance of septic shock In hospital mortality rate same JAMA 2015
16 Adjunct Prednisone Therapy for Patients with CAP: a Multicenter, Double-blind, Randomized, Placebo- Controlled Trial Prednisone 50mg day vs placebo for 7 days Primary endpoint was time to clinical stability Stable vitals for 24hrs, normal mental status, normal oral intake, sats>90% RA Total of 785 patients studied Median time to clinical stability was shorter in prednisone group 3 days vs 4.4 days (CI , p<0.0001) No difference in pneumonia associated complications Higher incidence of in-hospital hyperglycemia needing insulin 19% vs 11%, CI , p=0.001) Lancet 2015
17 Efficacy and Safety of Corticosteroids for Community-Acquired Pneumonia: A Systematic Review and Meta-Analysis 9 RCTs and 6 cohort studies including total of Mean steroid use 30mg day methylprednisolone 7 days Steroids did not have a statistically significant effect on mortality in CAP RR, 0.72, CI ) Steroids did not reduce mortality in patients with severe CAP Secondary outcomes Steroids were associated with decrease risk of ARDS (RR 0.21, CI ) Steroids may help reduce LOS in hospital and ICU and time to clinical stability Steroids not associated with increased rates of adverse events Chest 2016
18 Effect of Oral Prednisone on Symptom Duration and Severity in Non asthmatic Adults With Acute Lower respiratory Track Infection. A Randomized Clinic Trial. Assess oral steroids for acute lower respiratory track infections 40mg day for 5 days vs placebo 398 adults Primary outcomes were duration of cough or worse cough and severity of symptoms on days 2 and 4 No difference in outcomes seen JAMA 2017
19 Steroids in Management of Pneumonia Cochrane data base 2017: 17 RCTs for total of 2264 participants, 13 RCTs were adults and 4 RCTs children. Trials limited to inpatients with CAP Corticosteroids significantly reduced mortality in adults with severe pneumonia (RR 0.58, 95% CI ) Corticosteroids did not significantly reduce mortality in adults with nonsevere pneumonia Steroids shortened hospital length of stay by about 3 days NNT was 18 to prevent 1 death Adverse events included hyperglycemia Cochrane Database 2017
20 Recommendations from Uptodate Use steroids in patients with CAP who have significant inflammatory response with sepsis and respiratory failure Methylprednisolone 0.5mg/kg q 12 hrs or prednisone 50mg day x 5 days Uptodate 2018
21 Why Do Steroids Help in Severe CAP? Contain an over active immune system that is destroying lung parenchyma Steroids are anti inflammatory and are down regulating pro inflammatory cytokines such as IL-6 and IL-8. Steroids help to upregulate anti-inflammatory cytokines such as IL-10. Relative adrenal insufficiency is treated Maybe this is not infectious but mimicking infectious pneumonia
22 Things to Consider that are Steroid Responsive Eosinophilic Pneumonia Cryptogenic organizing pneumonia Hypersensitivity Pneumonia Pulmonary Vasculitis ILD
23 Ct Chest: Diffuse bilateral infiltrates
24 Question #1 63 yr old female with no significant past medical history presents with 2 day hx of cough, fevers, and dyspnea. She feels tired and looks sick. Temp 102, RR 25, BP 100/70, WBC 3.5, BUN 30, ABG shows pao2 60, sats 89% and CXR shows dense infiltrate in RLL and RML. Which of the following are correct in regards to best management of this patient? A. Patient should be treated for pneumonia as an outpatient. B. Patient may benefit from treatment with methylprednisolone 0.5mg/kg q 12. C. Patient should be treated with fluoroquinolone plus vancomycin D. The most common pathogen identified on admission to hospital is streptococcus pneumoniae. 25% 25% 25% 25% A. B. C. D.
25 Community Acquired RLL Pneumonia
26 Question #1 Correct Answer: B) based on current available data, steroids may be beneficial in the management of severe inpatient pneumonia. Explanation: Cochrane Data base 2017: Corticosteroids significantly reduced mortality in adults with severe pneumonia (RR 0.58, 95% CI ). Reductions in mortality were not seen in non severe pneumonia. Per the IDS guidelines the patient has a score of 3 and should be admitted to the ICU RR>30, PaO2/FiO2 <250, multilobar infiltrate, confusion, BUN>20, WBC<4, platelets<100, T<36, hypotension requiring fluid resuscitation Per IDS and ATS guidelines for antibiotics for CAP admitted to the ICU Macrolide plus Ceftriaxone Fluoroquinolone plus Ceftriaxone Underlying risk factors: add Vancomycin, add extended spectrum beta lactam Most common pathogens identified on admission to a hospital are viruses but for the majority of cases no pathogen is identified. Stern, A et al. Corticosteroids for Pneumonia. Cochrane Database Syst Rev Dec 13; 12: CD007720
27 Take Home Pearls Consider the use of steroids in patients admitted with severe CAP but as a general recommendation this should not be used in all patients admitted with community acquired pneumonia. Follow ID guidelines for antibiotics use so we are good stewards of antimicrobial use. Vaccinate everyone with flu vaccines and pneumococcal vaccine per guidelines as this intervention will be impactful on this potentially lethal disease. Expand your differential diagnosis to noninfectious causes of radiographic pneumonia. Better randomized controlled trials are needed to truly answer the question Should steroids be used in the setting of CAP?.
28 END
29 References Stern, A et al. Corticosteroids for Pneumonia. Cochrane Database Syst Rev Dec 13; 12: CD Siemieniuk RA, Meade MO, Alonso-Coello P, et al. Corticosteroid therapy for patients hospitalized with community-acquired pneumonia: a systematic review and metaanalysis. Ann Intern Med. 2015; 163( 7): Steroids Beneficial As Adjunctive Treatment for Community-Acquired Pneumonia. American Family Physician Feb 1;93(3):227. Wan YD, Sun TW, Liu ZQ, Zhang SG, Wang LX, Kan QC. Efficacy and Safety of Corticosteroids for Community-Acquired Pneumonia: A Systematic Review and Meta- Analysis. Chest. 2016;149(1): Tagami T, Matsui H, Horiguchi H, Fushimi K, Yasunaga H. Low-dose corticosteroid use and mortality in severe community-acquired pneumonia patients. The European Respiratory Journal. 2015;45(2): Jain, S et al. Community-Acquired Pneumonia Requiring Hospitalization among U.S. Adults. NEJM 2015; 373:
30 References Infectious Diseases Society of America. Infectious Diseases Society of America/American Thoracic Society consensus guide-lines on the management of community- acquired pneumonia in adults. Clin Infect Dis. 2007;44 Suppl 2:S American Lung Association. Trends in pneumonia and influenza and pneumonia morbidity and mortality; Niederman, M. In The Clinic. Community-Acquired Pneumonia. Annals of Internal Medicine. October 6, Blum CA et al. Adjunct Prednisone Therapy for Patients with Community acquired pneumonia: a multicentre, double-blind, randomized, placebo-controlled trial. Lancet. 2015;385 (9977): Torres A et al. Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory response: a randomized clinical trial. JAMA. 2015;313: Hay, A et al. Effect of Oral Prednisone on Symptom Duration and Severity in Nonasthmatic Adults With Acute Lower respiratory Track Infection. A Randomized Clinic Trial. JAMA. 2017: 318(8):
31 Pneumonia Severity Index Risk class Classes 1 and 2 - outpatient management Class 3 - observation unit or short inpatient stay Classes 4 and 5 inpatient management
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Polmoniti: Steroidi sì, no, quando. Alfredo Chetta Clinica Pneumologica Università degli Studi di Parma
 Polmoniti: Steroidi sì, no, quando Alfredo Chetta Clinica Pneumologica Università degli Studi di Parma Number of patients Epidemiology and outcome of severe pneumococcal pneumonia admitted to intensive
Polmoniti: Steroidi sì, no, quando Alfredo Chetta Clinica Pneumologica Università degli Studi di Parma Number of patients Epidemiology and outcome of severe pneumococcal pneumonia admitted to intensive
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Pneumonia Severity Scores:
 Pneumonia Severity Scores: Are they Accurate Predictors of Mortality? JILL McEWEN, MD FRCPC Clinical Professor Department of Emergency Medicine University of British Columbia Vancouver, BC Canada President,
Pneumonia Severity Scores: Are they Accurate Predictors of Mortality? JILL McEWEN, MD FRCPC Clinical Professor Department of Emergency Medicine University of British Columbia Vancouver, BC Canada President,
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
How do we define pneumonia?
 Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT
 Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
Community-Acquired Pneumonia OBSOLETE 2
 Community-Acquired Pneumonia OBSOLETE 2 Clinical practice guidelines serve as an educational reference, and do not supersede the clinical judgment of the treating physician with respect to appropriate
Community-Acquired Pneumonia OBSOLETE 2 Clinical practice guidelines serve as an educational reference, and do not supersede the clinical judgment of the treating physician with respect to appropriate
Corticosteroids in Severe CAP. Mervyn Mer Department of Medicine & ICU Johannesburg Hospital University of the Witwatersrand
 Corticosteroids in Severe CAP Mervyn Mer Department of Medicine & ICU Johannesburg Hospital University of the Witwatersrand Introduction Much controversy and debate regarding the use of corticosteroids
Corticosteroids in Severe CAP Mervyn Mer Department of Medicine & ICU Johannesburg Hospital University of the Witwatersrand Introduction Much controversy and debate regarding the use of corticosteroids
To develop guidelines for the use of appropriate antibiotics for adult patients with CAP and guidance on IV to PO conversion.
 Page 1 of 5 TITLE: COMMUNITY-ACQUIRED PNEUMONIA (CAP) EMPIRIC MANAGEMENT OF ADULT PATIENTS AND IV TO PO CONVERSION GUIDELINES: These guidelines serve to aid clinicians in the diagnostic work-up, assessment
Page 1 of 5 TITLE: COMMUNITY-ACQUIRED PNEUMONIA (CAP) EMPIRIC MANAGEMENT OF ADULT PATIENTS AND IV TO PO CONVERSION GUIDELINES: These guidelines serve to aid clinicians in the diagnostic work-up, assessment
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA
 KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
Session: How to manage and prevent the different faces of pneumonia Severe CAP
 Athens 19, 20 November 2015 Garyfallia Poulakou Consultant, Infectious Diseases 4 th Department of Internal Medicine, Attikon University Hospital of Athens Session: How to manage and prevent the different
Athens 19, 20 November 2015 Garyfallia Poulakou Consultant, Infectious Diseases 4 th Department of Internal Medicine, Attikon University Hospital of Athens Session: How to manage and prevent the different
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
CARE OF THE ADULT PNEUMONIA PATIENT
 Care Guideline CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: The target audience for this Care Guideline is all MultiCare providers and staff, including those associated with our clinically integrated
Care Guideline CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: The target audience for this Care Guideline is all MultiCare providers and staff, including those associated with our clinically integrated
Acute Respiratory Infection. Dr Anthony Gibson
 Acute Respiratory Infection Dr Anthony Gibson Range of Conditions Upper tract Common Cold coryza Sore Throat- Pharyngitis Sinusitis Epiglottitis Range of Conditions Lower Acute Bronchitis Acute Exacerbation
Acute Respiratory Infection Dr Anthony Gibson Range of Conditions Upper tract Common Cold coryza Sore Throat- Pharyngitis Sinusitis Epiglottitis Range of Conditions Lower Acute Bronchitis Acute Exacerbation
Pneumococcal pneumonia
 Pneumococcal pneumonia Wei Shen Lim Consultant Respiratory Physician & Honorary Professor of Medicine Nottingham University Hospitals NHS Trust University of Nottingham Declarations of interest Unrestricted
Pneumococcal pneumonia Wei Shen Lim Consultant Respiratory Physician & Honorary Professor of Medicine Nottingham University Hospitals NHS Trust University of Nottingham Declarations of interest Unrestricted
Antimicrobial Stewardship in Community Acquired Pneumonia
 Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
CAP, HCAP, HAP, VAP. 1. In 1898, William Osler described community-acquired pneumonia as:
 1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center
 Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center
 CA-MRSA Pneumonia Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center Professor of Clinical Medicine Weill Cornell
CA-MRSA Pneumonia Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center Professor of Clinical Medicine Weill Cornell
Disclosures. Case 1. Acute Bronchitis. Acute Bronchitis. Community-Acquired Pneumonia and other Respiratory Tract Infections. What do you recommend?
 Community-Acquired Pneumonia and other Respiratory Tract Infections none Disclosures Joel T. Katz, M.D. Associate Professor of Medicine Division of Infectious Diseases Brigham and Women s Hospital Case
Community-Acquired Pneumonia and other Respiratory Tract Infections none Disclosures Joel T. Katz, M.D. Associate Professor of Medicine Division of Infectious Diseases Brigham and Women s Hospital Case
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Pneumonia 2017 OMAR PIRZADA
 Pneumonia 2017 OMAR PIRZADA Pneumonia Pneumonia is common 0.5-1% of adults per year, 5-12% presenting to GP with LRTi 22-42% will be admitted to hospital Symptoms and signs Case 1 26 year old man Sudden
Pneumonia 2017 OMAR PIRZADA Pneumonia Pneumonia is common 0.5-1% of adults per year, 5-12% presenting to GP with LRTi 22-42% will be admitted to hospital Symptoms and signs Case 1 26 year old man Sudden
One View of STEROIDS Who is this? EBV/Mono. Infections With Possible Steroid Rx STEROID USE IN PEDIATRIC INFECTION. EBV TB Meningitis Septic Arthritis
 One View of STEROIDS Who is this? STEROID USE IN PEDIATRIC INFECTION Peggy Weintrub Infections With Possible Steroid Rx EBV/Mono EBV TB Meningitis Septic Arthritis Who painted this young woman with mono?
One View of STEROIDS Who is this? STEROID USE IN PEDIATRIC INFECTION Peggy Weintrub Infections With Possible Steroid Rx EBV/Mono EBV TB Meningitis Septic Arthritis Who painted this young woman with mono?
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Community-Acquired Pneumonia. Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital. Nothing to disclose.
 Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Nothing to disclose. Community-Acquired Pneumonia Talk will focus on adults Guideline
Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Nothing to disclose. Community-Acquired Pneumonia Talk will focus on adults Guideline
Pneumonia. Dr. Rami M Adil Al-Hayali Assistant professor in medicine
 Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF
 Maximizing Care for Community- Acquired Pneumonia Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu 1. In 1898, William Osler described community-acquired
Maximizing Care for Community- Acquired Pneumonia Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu 1. In 1898, William Osler described community-acquired
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF -- William Osler, M.D.
 Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu a. An ailment that often leads to suffocation and death. b. A friend of the aged. c. A common
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu a. An ailment that often leads to suffocation and death. b. A friend of the aged. c. A common
Deep discoveries: the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine
 Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine") Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
WORKSHOP. The Multiple Facets of CAP. Community acquired pneumonia (CAP) continues. Jennifer s Situation
 continues. Jennifer s Situation") Practical Pointers pointers For for Your your Practice practice The Multiple Facets of CAP Dr. George Fox, MD, MSc, FRCPC, FCCP Community acquired pneumonia (CAP) continues to be a significant health burden
Practical Pointers pointers For for Your your Practice practice The Multiple Facets of CAP Dr. George Fox, MD, MSc, FRCPC, FCCP Community acquired pneumonia (CAP) continues to be a significant health burden
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Disclosures. Objectives. Procalcitonin: Pearls and Pitfalls in Daily Practice
 Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Supplementary Online Content
 Supplementary Online Content Torres A, Sibila O, Ferrer M, et al. Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory
Supplementary Online Content Torres A, Sibila O, Ferrer M, et al. Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine
 Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: The National Heart, Lung, and Blood Institute Acute Respiratory
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: The National Heart, Lung, and Blood Institute Acute Respiratory
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Managing meningitis not just antibiotics. Helena White December 2013
 Managing meningitis not just antibiotics Helena White December 2013 Case history 43 year old British-born Asian lady Legal advisor Married with a three year old child (on Amoxicillin for recent ear infection)
Managing meningitis not just antibiotics Helena White December 2013 Case history 43 year old British-born Asian lady Legal advisor Married with a three year old child (on Amoxicillin for recent ear infection)
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
SEPSIS RESULTING FROM PNEUMONIA FILE
 13 January, 2018 SEPSIS RESULTING FROM PNEUMONIA FILE Document Filetype: PDF 521.12 KB 0 SEPSIS RESULTING FROM PNEUMONIA FILE Aspiration pneumonia is a type of lung infection. CAP's symptoms are the result
13 January, 2018 SEPSIS RESULTING FROM PNEUMONIA FILE Document Filetype: PDF 521.12 KB 0 SEPSIS RESULTING FROM PNEUMONIA FILE Aspiration pneumonia is a type of lung infection. CAP's symptoms are the result
Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Community acquired pneumonia
 Community acquired pneumonia definition Symptoms of an acute LRTI New focal signs on chest examination At least one systemic feature New radiographic shadow Defination{Crofton} IT IS A SYNDROME CAUSED
Community acquired pneumonia definition Symptoms of an acute LRTI New focal signs on chest examination At least one systemic feature New radiographic shadow Defination{Crofton} IT IS A SYNDROME CAUSED
Is nosocomial infection the major cause of death in sepsis?
 Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
Community Acquired Pneumonia: Measures to Improve Management and Healthcare Quality
 Community Acquired Pneumonia: Measures to Improve Management and Healthcare Quality Gonzalo Bearman MD, MPH Assistant Professor of Internal Medicine Divisions of Quality Health Care & Infectious Diseases
Community Acquired Pneumonia: Measures to Improve Management and Healthcare Quality Gonzalo Bearman MD, MPH Assistant Professor of Internal Medicine Divisions of Quality Health Care & Infectious Diseases
Andrea Blotsky MDCM FRCPC General Internal Medicine, McGill University Thursday, October 15, 2015
 The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
Sepsis: What Is It Really?
 Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Subclinical Problems in the ICU:
 Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis
 All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis Presenter Disclosure Faculty/Speaker: Dr. Brett Finney BSc MD CCFP Relationships with financial sponsors: Grants/Research
All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis Presenter Disclosure Faculty/Speaker: Dr. Brett Finney BSc MD CCFP Relationships with financial sponsors: Grants/Research
Steroid in Paediatric Sepsis. Dr Pon Kah Min Hospital Pulau Pinang
 Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Stroke-associated pneumonia: aetiology and diagnostic challenges
 Stroke-associated pneumonia: aetiology and diagnostic challenges Craig J Smith Greater Manchester Comprehensive Stroke Centre, Salford Royal NHS Foundation Trust University of Manchester Smith and Tyrrell,
Stroke-associated pneumonia: aetiology and diagnostic challenges Craig J Smith Greater Manchester Comprehensive Stroke Centre, Salford Royal NHS Foundation Trust University of Manchester Smith and Tyrrell,
OLB (Open Lung Biopsy) in ARDS
 in ARDS") OLB (Open Lung Biopsy) in ARDS Claude GUERIN MD PhD Réanimation Médicale Hôpital de la Croix-Rousse Université de Lyon Lyon, France CCF Toronto October 28 th 2012 CCF 2012 1 Disclosure No conflict of interest
OLB (Open Lung Biopsy) in ARDS Claude GUERIN MD PhD Réanimation Médicale Hôpital de la Croix-Rousse Université de Lyon Lyon, France CCF Toronto October 28 th 2012 CCF 2012 1 Disclosure No conflict of interest
CLAIRE NOWLAN & SAM SEARLE. Pneumonia in the nursing home
 CLAIRE NOWLAN & SAM SEARLE Pneumonia in the nursing home No disclosures or conflicts of interest PMHX: A. FIB. GERD MIXED DEMENTIA MMSE 16/30 HTN Mr. Hack 86 years old RAMIPRIL 4 MG OD PARIET 20MG OD DONEPEZIL
CLAIRE NOWLAN & SAM SEARLE Pneumonia in the nursing home No disclosures or conflicts of interest PMHX: A. FIB. GERD MIXED DEMENTIA MMSE 16/30 HTN Mr. Hack 86 years old RAMIPRIL 4 MG OD PARIET 20MG OD DONEPEZIL
ESCMID Online Lecture Library. by author
 INFLUENZA IN CHILDREN Cristian Launes Infectious Diseases Unit. Department of Paediatrics. Hospital Sant Joan de Déu (Universitat de Barcelona) Innovation in Severe Acute Respiratory Infections (SARI),
INFLUENZA IN CHILDREN Cristian Launes Infectious Diseases Unit. Department of Paediatrics. Hospital Sant Joan de Déu (Universitat de Barcelona) Innovation in Severe Acute Respiratory Infections (SARI),
COPD Update. Muhammad Talha Khan MD. COPD Exacerbations. COPD Clinical Importance. COPD Pathophysiology. Overview/Objectives
 Overview/Objectives COPD Update Muhammad Talha Khan MD Pulmonologist St Croix Regional Medical Center, St Croix Falls, WI. Overview of COPD and disease impact Classification of COPD Severity Treatment
Overview/Objectives COPD Update Muhammad Talha Khan MD Pulmonologist St Croix Regional Medical Center, St Croix Falls, WI. Overview of COPD and disease impact Classification of COPD Severity Treatment
by author ESCMID Online Lecture Library Steroids in acute bacterial meningitis
 Steroids in acute bacterial meningitis Javier Garau, MD, PhD University of Barcelona Spain ESCMID Summer School, Porto, July 2009 Dexamethasone treatment in childhood bacterial meningitis in Malawi: a
Steroids in acute bacterial meningitis Javier Garau, MD, PhD University of Barcelona Spain ESCMID Summer School, Porto, July 2009 Dexamethasone treatment in childhood bacterial meningitis in Malawi: a
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease
 HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Lung Injury after HCT
 Lung Injury after HCT J. Douglas Rizzo, MD, MS Financial Disclosure None SCS06_1.ppt Background HCT an important therapeutic modality for malignant and non-malignant diseases Pulmonary Toxicity common
Lung Injury after HCT J. Douglas Rizzo, MD, MS Financial Disclosure None SCS06_1.ppt Background HCT an important therapeutic modality for malignant and non-malignant diseases Pulmonary Toxicity common
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
and localized ground glass opacities, or bronchiolar focal or multifocal micronodules;
 E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
THE BEST I HAVE READ THIS YEAR (IN PULMONARY AND CRITICAL CARE)
") 23 March 2018 Boca Raton, Florida THE BEST I HAVE READ THIS YEAR (IN PULMONARY AND Johnson.margaret2@mayo.edu No disclosures or off label uses CRITICAL CARE) Margaret M. Johnson, MD Chair, Division of
23 March 2018 Boca Raton, Florida THE BEST I HAVE READ THIS YEAR (IN PULMONARY AND Johnson.margaret2@mayo.edu No disclosures or off label uses CRITICAL CARE) Margaret M. Johnson, MD Chair, Division of
Objectives. Pneumonia. Pneumonia. Epidemiology. Prevalence 1/7/2012. Community-Acquired Pneumonia in infants and children
 Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Top 5 (Topics) Papers In GIM Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008
 Papers In GIM Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008") Top 5 (Topics) Papers In GIM 2008 Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008 Methods Searched ACPJC/EBM, TOC of top medical journals, MEDSCAPE Best Evidence, consultation
Top 5 (Topics) Papers In GIM 2008 Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008 Methods Searched ACPJC/EBM, TOC of top medical journals, MEDSCAPE Best Evidence, consultation
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
C-reactive protein. An ED perspective Greg Stevens May 2010
 C-reactive protein An ED perspective Greg Stevens May 2010 Basic Biology Is a short Pentraxin Penta 5, ragos berries 224 residue protein 25106 Da Gene 1q21-q23 q23 History Tillett WS, Francis T Jr. Serological
C-reactive protein An ED perspective Greg Stevens May 2010 Basic Biology Is a short Pentraxin Penta 5, ragos berries 224 residue protein 25106 Da Gene 1q21-q23 q23 History Tillett WS, Francis T Jr. Serological
Avian Influenza A (H7N9): Clinical Management. KW Choi Associate Consultant IDCTC, HA/ ICB, CHP
: Clinical Management. KW Choi Associate Consultant IDCTC, HA/ ICB, CHP") Avian Influenza A (H7N9): Clinical Management KW Choi Associate Consultant IDCTC, HA/ ICB, CHP Initial symptoms: nonspecific, similar to most other causes of ILI, CAP High index of suspicion and alertness
Avian Influenza A (H7N9): Clinical Management KW Choi Associate Consultant IDCTC, HA/ ICB, CHP Initial symptoms: nonspecific, similar to most other causes of ILI, CAP High index of suspicion and alertness
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
The Berlin Definition: Does it fix anything?
 The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
Family Medicine Clinical Pharmacy Forum Vol. 3, Issue 1 (January/February 2007)
") 1 Family Medicine Clinical Pharmacy Forum Vol. 3, Issue 1 (January/February 2007) Family Medicine Clinical Pharmacy Forum is a brief bi-monthly publication from the Family Medicine clinical pharmacists
1 Family Medicine Clinical Pharmacy Forum Vol. 3, Issue 1 (January/February 2007) Family Medicine Clinical Pharmacy Forum is a brief bi-monthly publication from the Family Medicine clinical pharmacists
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Getting Smart About: Upper Respiratory Infections
 Getting Smart About: Upper Respiratory Infections Daniel Z. Uslan, MD Assistant Clinical Professor Director, Antimicrobial Stewardship Program UCLA Health System Disclosures None relevant to the topic
Getting Smart About: Upper Respiratory Infections Daniel Z. Uslan, MD Assistant Clinical Professor Director, Antimicrobial Stewardship Program UCLA Health System Disclosures None relevant to the topic
AECOPD: Management and Prevention
 Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
COPD Treatable. Preventable.
 My COPD Action Plan Patient s Copy (Patient s Name) Date Canadian Respiratory COPD Treatable. Preventable. This is to tell me how I will take care of myself when I have a COPD flare-up. My goals are My
My COPD Action Plan Patient s Copy (Patient s Name) Date Canadian Respiratory COPD Treatable. Preventable. This is to tell me how I will take care of myself when I have a COPD flare-up. My goals are My
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids
 Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids Joshua Malo, MD Yuval Raz, MD Linda Snyder, MD Kenneth Knox, MD University of Arizona Medical Center Department of
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids Joshua Malo, MD Yuval Raz, MD Linda Snyder, MD Kenneth Knox, MD University of Arizona Medical Center Department of
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
PNEUMONIA. Patient Case: Chief Complaint: I have been short of breath and have been coughing up rust-colored phlegm for the past 3 days.
 PNEUMONIA Relevant Guidelines: 2008 IDSA CAP guidelines: http://www.idsociety.org/guidelines/patient_care/idsa_practice_guidelines/infections_by_org an_system/lower/upper_respiratory/community-acquired_pneumonia_(cap)/
PNEUMONIA Relevant Guidelines: 2008 IDSA CAP guidelines: http://www.idsociety.org/guidelines/patient_care/idsa_practice_guidelines/infections_by_org an_system/lower/upper_respiratory/community-acquired_pneumonia_(cap)/
Top 5 papers in clinical mycology
 Top 5 papers in clinical mycology Dirk Vogelaers Department of General Internal Medicine University Hospital Ghent Joint symposium BVIKM/BSIMC and SBMHA/BVMDM Influenza-associated aspergillosis in critically
Top 5 papers in clinical mycology Dirk Vogelaers Department of General Internal Medicine University Hospital Ghent Joint symposium BVIKM/BSIMC and SBMHA/BVMDM Influenza-associated aspergillosis in critically
COPD exacerbation. Dr. med. Frank Rassouli
 Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of