Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
|
|
|
- Julie Lucas
- 5 years ago
- Views:
Transcription
1 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP
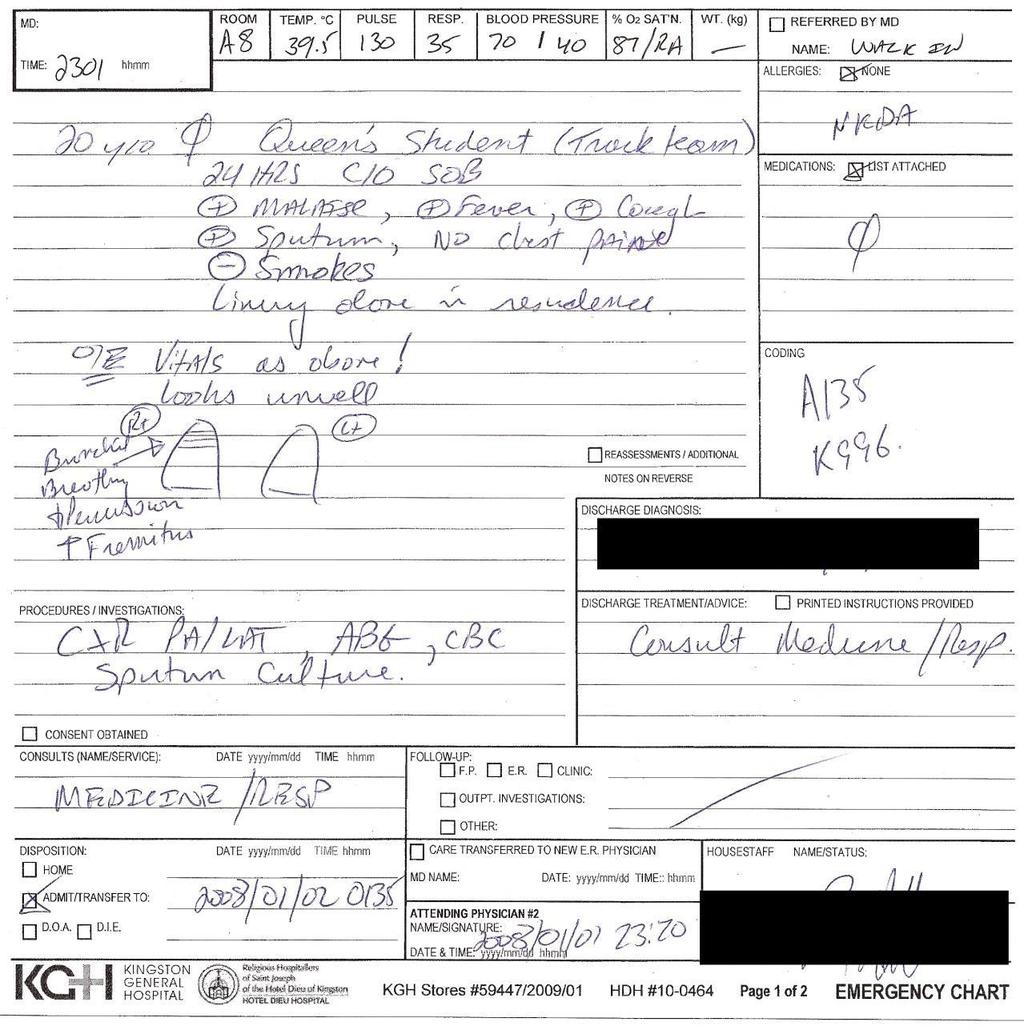
2 A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent vomitting. His wife had similar symptoms 1 week ago which improved with an unknown antibiotic. Patient is requesting to go home with antibiotic. He previously had tongue swelling and skin rash with use of augmentin. Reports good health otherwise. Denies chest pain, swelling of extremities, or diarrhea. His vital signs are T 38.5 C, P 76, BP 128/82, spo2 94%, RR 16. Patient is alert and oriented. Crackles were heard over left lower lung field. Labs showed WBC 14, BUN 20 mg/dl. Chest X-ray had a consolidation in left lower lobe. What is the best way to further manage this patient? A. Send home with oral azithromycin B. Send home with oral levofloxacin C. Admit to medicine floor with iv levofloxacin D. Admit to medicine floor with iv ceftriaxone and azithromycin E. Admit to ICU with iv ceftriaxone and iv azithromycin
3
4
5 What are the features of Jane s history that suggest which organisms are most likely to be responsible for her presentation? What additional information from her history would you like to know and why?. What are the features of Jane s physical examination that indicate pneumonia?.what are signs of pleural involvement? Does she have any?.what are signs of serious sepsis? Does she have any? Bonus: What are examples of extra-pulmonary infection that may complicate pneumonia? Where should Jane be managed?
6 Definition Lower respiratory tract infection in a nonhospitalized person associated with symptoms of acute infection with or without new infiltrate on chest radiograph Acute infection of the pulmonary parenchyma acquired outside of a health care setting.
7 Types of CAP Typical CAP (60-70%) Streptococcus pneumoniae Atypical CAP (30-40%) Influenza virus Mycoplasma Chlamydia Legionella
8 Signs & Symptoms Clinical symptoms Cough (productive or non-productive) Fever Chills/Rigors Dyspnea Fatigue/Myalgia Gastrointestinal (Legionella)
9 Signs & Symptoms Physical exam Dullness to percussion of chest Crackles on auscultation Bronchial breath sounds Egophony ( E to A changes)
10 Risk factors Older age The risk of CAP rises with age]. The annual incidence of hospitalization for CAP among adults 65 years old Chronic comorbidities (COPD), chronic lung disease (eg, bronchiectasis, asthma), chronic heart disease (particularly congestive heart failure), stroke, diabetes mellitus, malnutrition and immunocompromising conditions Viral respiratory tract infection Viral respiratory tract infections can lead to primary viral pneumonias and also predispose to secondary bacterial pneumonia. Impaired airway protection Conditions that increase risk of macroaspiration of stomach contents and/or microaspiration of upper airway secretions predispose to CAP, such as alteration in consciousness (eg, due to stroke, seizure, anesthesia, drug or alcohol use) or dysphagia due to esophageal lesions or dysmotility Smoking and alcohol overuse Smoking, alcohol overuse (eg, >80 g/day), and opioid use are key modifiable behavioral risk factors for CAP. Other lifestyle factors Other factors that have been associated with an increased risk of CAP include crowded living conditions (eg, prisons, homeless shelters), residence in low-income settings, and exposure to environmental toxins (eg, solvents, paints, or gasoline)
11 MICROBIOLOGY Streptococcus pneumonia (pneumococcus) and respiratory viruses are the most frequently detected pathogens in patients with CAP.
12 Typical bacteria S. pneumoniae (most common bacterial cause) Haemophilus influenzae Moraxella catarrhalis Staphylococcus aureus Group A streptococci Aerobic gram-negative bacteria anaerobes (associated with aspiration)
13 Atypical bacteria Legionella spp Mycoplasma pneumoniae Chlamydia pneumoniae Chlamydia psittaci Coxiella burnetii
14 Respiratory viruses Influenza A and B viruses Rhinoviruses Parainfluenza viruses Adenoviruses Respiratory syncytial virus Human metapneumovirus Coronaviruses (eg, Middle East respiratory syndrome coronavirus) Human bocaviruses
15 Diagnosis- Labs All patients with suspected CAP should have chest radiograph Leukocyte count Sputum Gram stain Blood cultures x 2 Serum/urine antigens
16 Inflammatory markers, (ESR), (CRP) procalcitonin. CBC organ dysfunction such as renal dysfunction, liver dysfunction, and/or thrombocytopenia. Blood cultures Sputum Intensive care unit admission Failure of antibiotic therapy (either outpatients or hospitalized patients Cavitary lesions Active alcohol abuse Severe obstructive or structural lung disease Immunocompromised host Pleural effusion MERS-CoV. Urinary antigen
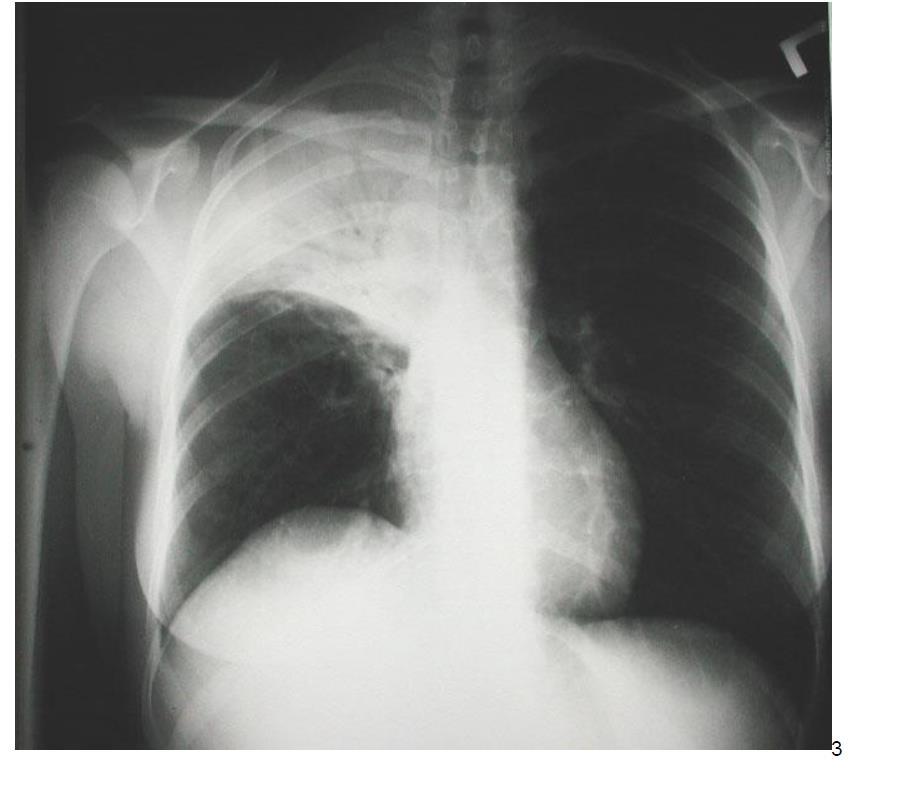
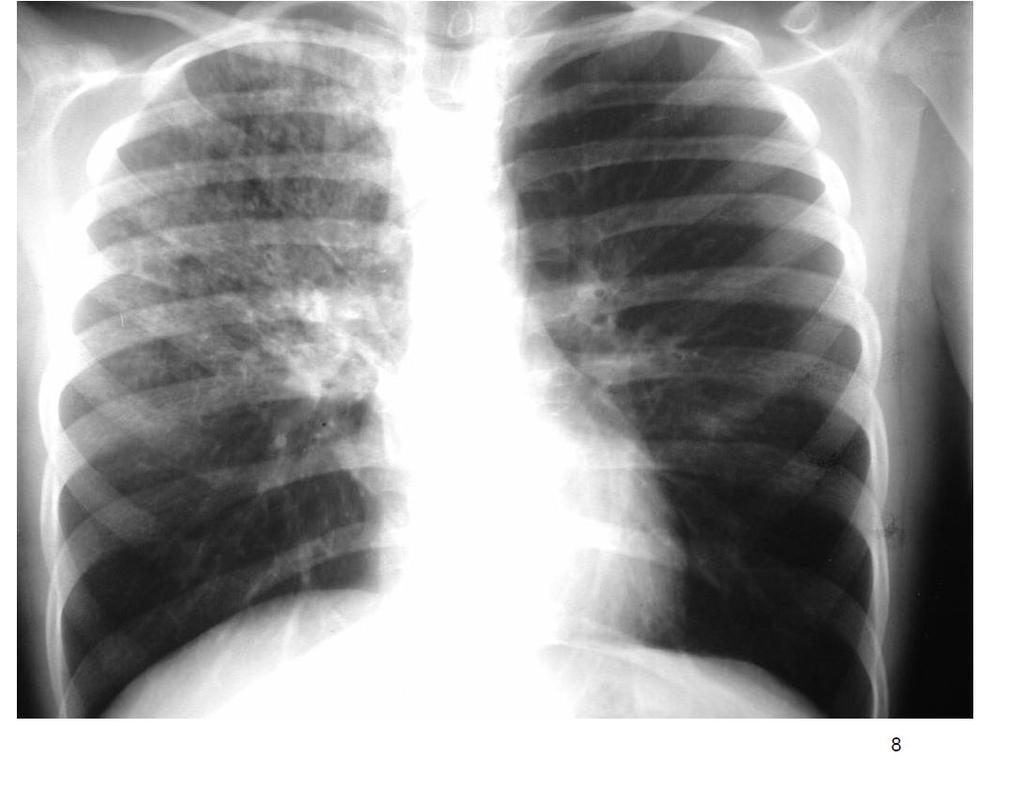
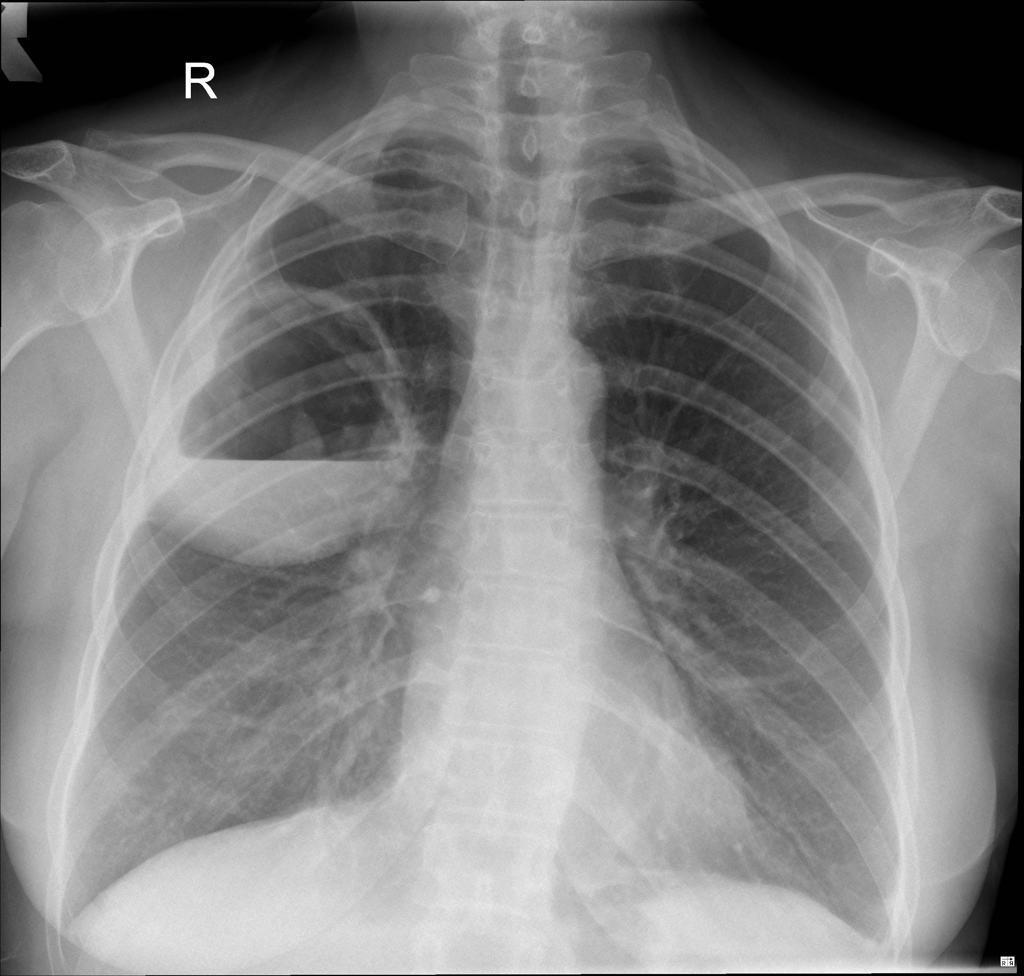
17 RADIOLOGIC EVALUATION Consolidation interstitial infiltrates Cavitation
18
19
20
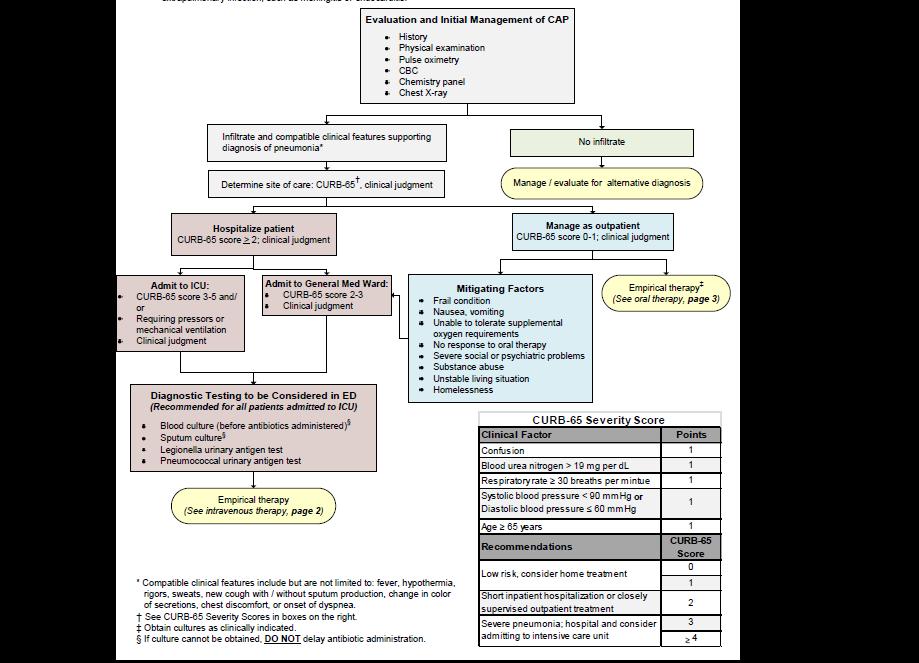
21 Evaluation and Initial Management of Community-Acquired Pneumonia (CAP)
22
23
24

25
Pneumonia. Dr. Rami M Adil Al-Hayali Assistant professor in medicine
 Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center
 Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Antimicrobial Stewardship in Community Acquired Pneumonia
 Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
PNEUMONIA. I. Background 6 th most common cause of death in U.S. Most common cause of infection related mortality
 Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Upper...and Lower Respiratory Tract Infections
 Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Catherine Casey S. Jones,
 Community Acquired Pneumonia Catherine Casey S. Jones, PhD, RN, ANP-C, AE-C Catherine Casey S. Jones, PhD, RN, ANP-C, AE-C Texas Pulmonary & Critical Care Consultants, PA & Adjunct Professor at Texas Woman
Community Acquired Pneumonia Catherine Casey S. Jones, PhD, RN, ANP-C, AE-C Catherine Casey S. Jones, PhD, RN, ANP-C, AE-C Texas Pulmonary & Critical Care Consultants, PA & Adjunct Professor at Texas Woman
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Respiratory Infections
 Respiratory Infections NISHANT PRASAD, MD THE DR. JAMES J. RAHAL, JR. DIVISION OF INFECTIOUS DISEASES NEWYORK-PRESBYTERIAN QUEENS Disclosures Stockholder: Contrafect Corp., Bristol-Myers Squibb Co Research
Respiratory Infections NISHANT PRASAD, MD THE DR. JAMES J. RAHAL, JR. DIVISION OF INFECTIOUS DISEASES NEWYORK-PRESBYTERIAN QUEENS Disclosures Stockholder: Contrafect Corp., Bristol-Myers Squibb Co Research
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
WORKSHOP. The Multiple Facets of CAP. Community acquired pneumonia (CAP) continues. Jennifer s Situation
 continues. Jennifer s Situation") Practical Pointers pointers For for Your your Practice practice The Multiple Facets of CAP Dr. George Fox, MD, MSc, FRCPC, FCCP Community acquired pneumonia (CAP) continues to be a significant health burden
Practical Pointers pointers For for Your your Practice practice The Multiple Facets of CAP Dr. George Fox, MD, MSc, FRCPC, FCCP Community acquired pneumonia (CAP) continues to be a significant health burden
POLICY FOR TREATMENT OF LOWER RESPIRATORY TRACT INFECTIONS
 POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
Bacterial pneumonia with associated pleural empyema pleural effusion
 EMPYEMA Synonyms : - Parapneumonic effusion - Empyema thoracis - Bacterial pneumonia - Pleural empyema, pleural effusion - Lung abscess - Complicated parapneumonic effusions (CPE) 1 Bacterial pneumonia
EMPYEMA Synonyms : - Parapneumonic effusion - Empyema thoracis - Bacterial pneumonia - Pleural empyema, pleural effusion - Lung abscess - Complicated parapneumonic effusions (CPE) 1 Bacterial pneumonia
Community Acquired Pneumonia Pediatric Ages 3 month to 18 years Clinical Practice Guideline MedStar Health Antibiotic Stewardship
 Community Acquired Pneumonia Pediatric Ages 3 month to 18 years Clinical Practice Guideline MedStar Health Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians
Community Acquired Pneumonia Pediatric Ages 3 month to 18 years Clinical Practice Guideline MedStar Health Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians
Critical Care Nursing Theory. Pneumonia. - Pneumonia is an acute infection of the pulmonary parenchyma
 - is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
- is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
URIs and Pneumonia. Elena Bissell, MD 10/16/2013
 URIs and Pneumonia Elena Bissell, MD 10/16/2013 Objectives Recognize and treat community acquired PNA in children/adults Discern between inpatient and outpatient treatment of PNA Recognize special populations/cases
URIs and Pneumonia Elena Bissell, MD 10/16/2013 Objectives Recognize and treat community acquired PNA in children/adults Discern between inpatient and outpatient treatment of PNA Recognize special populations/cases
Exam 1 Review. Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies
 Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Community-Acquired Pneumonia OBSOLETE 2
 Community-Acquired Pneumonia OBSOLETE 2 Clinical practice guidelines serve as an educational reference, and do not supersede the clinical judgment of the treating physician with respect to appropriate
Community-Acquired Pneumonia OBSOLETE 2 Clinical practice guidelines serve as an educational reference, and do not supersede the clinical judgment of the treating physician with respect to appropriate
COPD exacerbation. Dr. med. Frank Rassouli
 Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA
 KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
Sheet: Patho-Pulmonary infections Done by: Maen Faoury
 Sheet: Patho-Pulmonary infections Done by: Maen Faoury Pneumonitis : might be an infection or not. Chemical Pneumonitis : not an infection. Parenchyma : an infection.( تندرج تحت ال pneumonitis) Lung Parenchyma
Sheet: Patho-Pulmonary infections Done by: Maen Faoury Pneumonitis : might be an infection or not. Chemical Pneumonitis : not an infection. Parenchyma : an infection.( تندرج تحت ال pneumonitis) Lung Parenchyma
Chapter 16. Lung Abscess. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
and localized ground glass opacities, or bronchiolar focal or multifocal micronodules;
 E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Supplementary Online Content
 Supplementary Online Content Torres A, Sibila O, Ferrer M, et al. Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory
Supplementary Online Content Torres A, Sibila O, Ferrer M, et al. Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Turkish Thoracic Society
 Türk Toraks Derneği Turkish Thoracic Society Pocket Books Series Diagnosis and Treatment of Community Acquired Pneumonia in Children Short Version (Handbook) in English www.toraks.org.tr This report was
Türk Toraks Derneği Turkish Thoracic Society Pocket Books Series Diagnosis and Treatment of Community Acquired Pneumonia in Children Short Version (Handbook) in English www.toraks.org.tr This report was
Pneumonia Aetiology Why is it so difficult to distinguish pathogens from innocent bystanders?
 Pneumonia Aetiology Why is it so difficult to distinguish pathogens from innocent bystanders? David Murdoch Department of Pathology University of Otago, Christchurch Outline Background Diagnostic challenges
Pneumonia Aetiology Why is it so difficult to distinguish pathogens from innocent bystanders? David Murdoch Department of Pathology University of Otago, Christchurch Outline Background Diagnostic challenges
Pathology of Pneumonia
 Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Community Acquired Pneumonia - Pediatric Clinical Practice Guideline MedStar Health Antibiotic Stewardship
 Community Acquired Pneumonia - Pediatric Clinical Practice Guideline MedStar Health Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Community Acquired Pneumonia - Pediatric Clinical Practice Guideline MedStar Health Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Pneumonia 2017 OMAR PIRZADA
 Pneumonia 2017 OMAR PIRZADA Pneumonia Pneumonia is common 0.5-1% of adults per year, 5-12% presenting to GP with LRTi 22-42% will be admitted to hospital Symptoms and signs Case 1 26 year old man Sudden
Pneumonia 2017 OMAR PIRZADA Pneumonia Pneumonia is common 0.5-1% of adults per year, 5-12% presenting to GP with LRTi 22-42% will be admitted to hospital Symptoms and signs Case 1 26 year old man Sudden
Problem Based Learning Session. Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days.
 Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
1/9/ :00:00AM 1/9/ :40:15AM 6/9/2017 9:19:16AM A/c Status. Test Name Results Units Bio. Ref. Interval. Nasal Swab
 LL - LL-ROHINI (NATIONAL REFERENCE 135091523 Age 36 Years Gender Female 1/9/2017 120000AM 1/9/2017 114015AM 6/9/2017 91916AM Ref By Final RESIRATORY COMREHENSIVE ANEL (33 ATHOGENS) RESIRATORY ANEL 1 #
LL - LL-ROHINI (NATIONAL REFERENCE 135091523 Age 36 Years Gender Female 1/9/2017 120000AM 1/9/2017 114015AM 6/9/2017 91916AM Ref By Final RESIRATORY COMREHENSIVE ANEL (33 ATHOGENS) RESIRATORY ANEL 1 #
To Study The Cinico-Radiological Features And Associated Co-Morbid Conditions
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 7 Ver. 16 (July. 2018), PP 58-62 www.iosrjournals.org To study the clinico-radiological features
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 7 Ver. 16 (July. 2018), PP 58-62 www.iosrjournals.org To study the clinico-radiological features
Infections of the head, neck, and lower respiratory tract
 Infections of the head, neck, and lower respiratory tract Infections of the upper respiratory tract Common 25% bacteria antibiotics 75% viruses Diagnosis on clinical grounds Nonspecific infections of the
Infections of the head, neck, and lower respiratory tract Infections of the upper respiratory tract Common 25% bacteria antibiotics 75% viruses Diagnosis on clinical grounds Nonspecific infections of the
Emerging Respiratory Infections NZ Amanda McNaughton Respiratory Physician CCDHB Wellington
 Emerging Respiratory Infections NZ 2015 Amanda McNaughton Respiratory Physician CCDHB Wellington Respiratory Infection: overview Influenza virus Clinical picture Emerging infection New Zealand Influenza
Emerging Respiratory Infections NZ 2015 Amanda McNaughton Respiratory Physician CCDHB Wellington Respiratory Infection: overview Influenza virus Clinical picture Emerging infection New Zealand Influenza
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
CAP, HCAP, HAP, VAP. 1. In 1898, William Osler described community-acquired pneumonia as:
 1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
Getting Smart About: Upper Respiratory Infections
 Getting Smart About: Upper Respiratory Infections Daniel Z. Uslan, MD Assistant Clinical Professor Director, Antimicrobial Stewardship Program UCLA Health System Disclosures None relevant to the topic
Getting Smart About: Upper Respiratory Infections Daniel Z. Uslan, MD Assistant Clinical Professor Director, Antimicrobial Stewardship Program UCLA Health System Disclosures None relevant to the topic
Acute pneumonia Simple complement
 Acute pneumonia Simple complement 1. Clinical variants of acute pneumonia in children are, except: A. Bronchopneumonia B. Lobar confluent pneumonia C. Viral pneumonia D. Interstitial pneumonia E. Chronic
Acute pneumonia Simple complement 1. Clinical variants of acute pneumonia in children are, except: A. Bronchopneumonia B. Lobar confluent pneumonia C. Viral pneumonia D. Interstitial pneumonia E. Chronic
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Guidelines/Guidance/CAP/ Hospitalized Child. PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014
 Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
Management of Acute Exacerbations
 15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
Nosocomial Pneumonia. <5 Days: Non-Multidrug-Resistant Bacteria
 Nosocomial Pneumonia Meredith Deutscher, MD Troy Schaffernocker, MD Ohio State University Burden of Hospital-Acquired Pneumonia Second most common nosocomial infection in the U.S. 5-10 episodes per 1000
Nosocomial Pneumonia Meredith Deutscher, MD Troy Schaffernocker, MD Ohio State University Burden of Hospital-Acquired Pneumonia Second most common nosocomial infection in the U.S. 5-10 episodes per 1000
Management of Common Respiratory Disorders in Children. Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016
 Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children. Disclosures. Roadmap 6/10/2016
 Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Creating a User Defined Pneumonia-Specific Syndrome in ESSENCE. Preventive Medicine Directorate September 2016
 Creating a User Defined Pneumonia-Specific Syndrome in ESSENCE Preventive Medicine Directorate September 2016 0 Pneumonia-Specific Syndrome NMCPHC retrospective analyses suggest that surveillance using
Creating a User Defined Pneumonia-Specific Syndrome in ESSENCE Preventive Medicine Directorate September 2016 0 Pneumonia-Specific Syndrome NMCPHC retrospective analyses suggest that surveillance using
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION. OSCE 5: Cough
 BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 5: Cough This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. So Ms. Chen, tell me what is your average
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 5: Cough This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. So Ms. Chen, tell me what is your average
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
PNEUMONIA. Dr. A.Torossian, M.D., Ph. D. Department of Respiratory Diseases
 PNEUMONIA Dr. A.Torossian, M.D., Ph. D. Department of Respiratory Diseases Definition Pneumonia is an infection of the lungs caused by bacteria, viruses, fungi and other microorganisms. Classifications
PNEUMONIA Dr. A.Torossian, M.D., Ph. D. Department of Respiratory Diseases Definition Pneumonia is an infection of the lungs caused by bacteria, viruses, fungi and other microorganisms. Classifications
9/15/2017. Joyce Turner RN Director of Clinical Program Development
 Joyce Turner RN Director of Clinical Program Development A toxic response to an infection that spirals out of control attacking the body s own organs and tissues. The infection can be bacterial, viral
Joyce Turner RN Director of Clinical Program Development A toxic response to an infection that spirals out of control attacking the body s own organs and tissues. The infection can be bacterial, viral
Community Acquired Pneumonia in Adults Clinical Practice Guideline Antibiotic Stewardship
 Community Acquired Pneumonia in Adults Clinical Practice Guideline Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians in making decisions regarding the care
Community Acquired Pneumonia in Adults Clinical Practice Guideline Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians in making decisions regarding the care
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Advance Pathology Services, P.C Professional Drive, Suite 3 Cadillac, MI Phone: Fax:
 Advance Pathology Services, P.C. 8865 Professional Drive, Suite 3 Cadillac, MI 49601 Phone: 231-468-2346 Fax: 231-468-2349 Pathology Analysis: Pneumonia and Pulmonary Hemorrhage Cause Death; Clinically
Advance Pathology Services, P.C. 8865 Professional Drive, Suite 3 Cadillac, MI 49601 Phone: 231-468-2346 Fax: 231-468-2349 Pathology Analysis: Pneumonia and Pulmonary Hemorrhage Cause Death; Clinically
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF
 Maximizing Care for Community- Acquired Pneumonia Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu 1. In 1898, William Osler described community-acquired
Maximizing Care for Community- Acquired Pneumonia Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu 1. In 1898, William Osler described community-acquired
MICROBIOLOGICAL TESTING IN PICU
 MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
Community Acquired Pneumonia-Adults Clinical Practice Guideline MedStar Health
 Community Acquired Pneumonia-Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding the care of their patients.
Community Acquired Pneumonia-Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding the care of their patients.
Adult CAP. How to approach for diagnosis. Natpatou Sanguanwongse, MD. Bureau of Emerging Infectious Disease July Sunday, July 8, 12
 Adult CAP How to approach for diagnosis Natpatou Sanguanwongse, MD. Bureau of Emerging Infectious Disease July 2012 Community-acquired pneumonia (CAP) one of several disease in which individuals (who have
Adult CAP How to approach for diagnosis Natpatou Sanguanwongse, MD. Bureau of Emerging Infectious Disease July 2012 Community-acquired pneumonia (CAP) one of several disease in which individuals (who have
Outpatient Management of Patients With Community Acquired Pneumonia Clinical Practice Guideline September 2013
 Clinical Practice Guideline September 2013 General Principles: Community Acquired Pneumonia (CAP), together with influenza, remains the seventh leading cause of death in the United States. According to
Clinical Practice Guideline September 2013 General Principles: Community Acquired Pneumonia (CAP), together with influenza, remains the seventh leading cause of death in the United States. According to
Patient information: Pneumonia in adults (Beyond the Basics)
") Page 1 of 8 Official reprint from UpToDate www.uptodate.com 2014 UpToDate Patient information: Pneumonia in adults (Beyond the Basics) Authors Thomas J Marrie, MD Thomas M File, Jr, MD Section Editor John
Page 1 of 8 Official reprint from UpToDate www.uptodate.com 2014 UpToDate Patient information: Pneumonia in adults (Beyond the Basics) Authors Thomas J Marrie, MD Thomas M File, Jr, MD Section Editor John
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT
 PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
Respiratory tract infections. Krzysztof Buczkowski
 Respiratory tract infections Krzysztof Buczkowski Etiology Viruses Rhinoviruses Adenoviruses Coronaviruses Influenza and Parainfluenza Viruses Respiratory Syncitial Viruses Enteroviruses Etiology Bacteria
Respiratory tract infections Krzysztof Buczkowski Etiology Viruses Rhinoviruses Adenoviruses Coronaviruses Influenza and Parainfluenza Viruses Respiratory Syncitial Viruses Enteroviruses Etiology Bacteria
Objectives. Pneumonia. Pneumonia. Epidemiology. Prevalence 1/7/2012. Community-Acquired Pneumonia in infants and children
 Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
May. Pathology #2. part. Rahaf Al-yousef. Mohammad Al-Qudah
 8 th May Pathology #2 nd Pneumonias 2 part Mohammad Al-Qudah Rahaf Al-yousef In the first part of our lectures today, we will define pneumonia clinically and pathologically(which is an infection of the
8 th May Pathology #2 nd Pneumonias 2 part Mohammad Al-Qudah Rahaf Al-yousef In the first part of our lectures today, we will define pneumonia clinically and pathologically(which is an infection of the
The Importance of Appropriate Treatment of Chronic Bronchitis
 ...CLINICIAN INTERVIEW... The Importance of Appropriate Treatment of Chronic Bronchitis An interview with Antonio Anzueto, MD, Associate Professor of Medicine, University of Texas Health Science Center,
...CLINICIAN INTERVIEW... The Importance of Appropriate Treatment of Chronic Bronchitis An interview with Antonio Anzueto, MD, Associate Professor of Medicine, University of Texas Health Science Center,
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Lower respiratory tract infections and community acquired pneumonia in adults
 Cough THEME Lower respiratory tract infections and community acquired pneumonia in adults BACKGROUND Lower respiratory tract infections acute bronchitis and community acquired pneumonia (CAP) are important
Cough THEME Lower respiratory tract infections and community acquired pneumonia in adults BACKGROUND Lower respiratory tract infections acute bronchitis and community acquired pneumonia (CAP) are important
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
APPENDIX EXHIBITS. Appendix Exhibit A2: Patient Comorbidity Codes Used To Risk- Standardize Hospital Mortality and Readmission Rates page 10
 Ross JS, Bernheim SM, Lin Z, Drye EE, Chen J, Normand ST, et al. Based on key measures, care quality for Medicare enrollees at safety-net and non-safety-net hospitals was almost equal. Health Aff (Millwood).
Ross JS, Bernheim SM, Lin Z, Drye EE, Chen J, Normand ST, et al. Based on key measures, care quality for Medicare enrollees at safety-net and non-safety-net hospitals was almost equal. Health Aff (Millwood).
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF -- William Osler, M.D.
 Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu a. An ailment that often leads to suffocation and death. b. A friend of the aged. c. A common
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu a. An ailment that often leads to suffocation and death. b. A friend of the aged. c. A common
66YM Chronic obstructive pulmonary disease annual review. H Chronic obstructive pulmonary disease
 Supplementary materials Table S1. Read codes to define COPD Read code Medical code Clinical event Read term 66YM.00 11287 382901 Chronic obstructive pulmonary disease annual review H3...00 1001 338812
Supplementary materials Table S1. Read codes to define COPD Read code Medical code Clinical event Read term 66YM.00 11287 382901 Chronic obstructive pulmonary disease annual review H3...00 1001 338812
Respiratory System Virology
 Respiratory System Virology Common Cold: Rhinitis. A benign self limited syndrome caused by several families of viruses. The most frequent acute illness in industrialized world. Mild URT illness involving:
Respiratory System Virology Common Cold: Rhinitis. A benign self limited syndrome caused by several families of viruses. The most frequent acute illness in industrialized world. Mild URT illness involving:
RESPIRATORY TRACT INFECTIONS. CLS 212: Medical Microbiology Zeina Alkudmani
 RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Zeina Alkudmani Lower Respiratory Tract Upper Respiratory Tract Anatomy of the Respiratory System Nasopharynx Oropharynx Respiratory Tract Infections
RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Zeina Alkudmani Lower Respiratory Tract Upper Respiratory Tract Anatomy of the Respiratory System Nasopharynx Oropharynx Respiratory Tract Infections
PANEL KEGAWAT DARURATAN SISTEM PERNAPASAN (SERANGAN ASMA AKUT, PNEUMONIA DAN COPD) dan EDEMA PARU
 dan EDEMA PARU") 1 PANEL KEGAWAT DARURATAN SISTEM PERNAPASAN (SERANGAN ASMA AKUT, PNEUMONIA DAN COPD) dan EDEMA PARU ASTHMA 2 2 Agonist Bronchodilator Response Anticholinergic Asthma Response Panel A COPD Response Panel
1 PANEL KEGAWAT DARURATAN SISTEM PERNAPASAN (SERANGAN ASMA AKUT, PNEUMONIA DAN COPD) dan EDEMA PARU ASTHMA 2 2 Agonist Bronchodilator Response Anticholinergic Asthma Response Panel A COPD Response Panel
Respiratory Multiplex Array. Rapid, simultaneous detection of 22 bacterial and viral pathogens of the upper and lower respiratory tract
 Rapid, simultaneous detection of 22 bacterial and viral pathogens of the upper and lower respiratory tract Rapid, simultaneous detection of 22 bacterial and viral pathogens within the upper and lower respiratory
Rapid, simultaneous detection of 22 bacterial and viral pathogens of the upper and lower respiratory tract Rapid, simultaneous detection of 22 bacterial and viral pathogens within the upper and lower respiratory
Skin reactivity to autologous bacteria isolated from respiratory tract of patients with obstructive pulmonary disease
 Skin reactivity to autologous bacteria 149 Original Article Skin reactivity to autologous bacteria isolated from respiratory tract of patients with obstructive pulmonary disease J. Halasa 1, M. Halasa
Skin reactivity to autologous bacteria 149 Original Article Skin reactivity to autologous bacteria isolated from respiratory tract of patients with obstructive pulmonary disease J. Halasa 1, M. Halasa
Clinical Diagnosis and Severity Assessment in Immunocompetent Adult Patients with Community-Acquired Pneumonia
 Chapter 5 Clinical Diagnosis and Severity Assessment in Immunocompetent Adult Patients with Community-Acquired Pneumonia Fernando Peñafiel Saldías, Orlando Díaz Patiño and Pablo Aguilera Fuenzalida Additional
Chapter 5 Clinical Diagnosis and Severity Assessment in Immunocompetent Adult Patients with Community-Acquired Pneumonia Fernando Peñafiel Saldías, Orlando Díaz Patiño and Pablo Aguilera Fuenzalida Additional
INTRODUCTION TO UPPER RESPIRATORY TRACT DISEASES
 Upper Respiratory Tract Infections Return to Syllabus INTRODUCTION TO UPPER RESPIRATORY TRACT DISEASES General Goal: To know the major mechanisms of defense in the URT, the major mechanisms invaders use
Upper Respiratory Tract Infections Return to Syllabus INTRODUCTION TO UPPER RESPIRATORY TRACT DISEASES General Goal: To know the major mechanisms of defense in the URT, the major mechanisms invaders use
Pneumonia: The Forgotten Killer
 Pneumonia: The Forgotten Killer David Glenn Weismiller, MD, ScM, FAAFP Department of Family and Community Medicine University of Nevada, Las Vegas School of Medicine Disclosure Statement It is the policy
Pneumonia: The Forgotten Killer David Glenn Weismiller, MD, ScM, FAAFP Department of Family and Community Medicine University of Nevada, Las Vegas School of Medicine Disclosure Statement It is the policy
Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP /15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain,
 Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP 1.0 10/15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain, headache Links with smoking, pollen count, FH of asthma
Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP 1.0 10/15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain, headache Links with smoking, pollen count, FH of asthma
Pneumonia, Pleurisy, Lung cancer
 Pneumonia, Pleurisy, Lung cancer Pneumonia is an infection of lung parenchyma, which leads to inflammation and exudates filling air spaces with fluid (consolidation). This leads to reduced lung compliance
Pneumonia, Pleurisy, Lung cancer Pneumonia is an infection of lung parenchyma, which leads to inflammation and exudates filling air spaces with fluid (consolidation). This leads to reduced lung compliance
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Isolation Precautions in Clinics
 Purpose Audience General principles Possible Exposures To define isolation precautions in a clinic setting. Clinics Isolation status should be determined primarily by the suspected disease and/or pathogen.
Purpose Audience General principles Possible Exposures To define isolation precautions in a clinic setting. Clinics Isolation status should be determined primarily by the suspected disease and/or pathogen.
12/12/2011. Atypical Pneumonia. Objectives. Causative Agents of Acute Pneumonia Bacteria. Causative Agents of Acute Pneumonia Other Agents
 Objectives Atypical Pneumonia K. Sue Kehl, Ph.D., D(ABMM) Associate Professor, Pathology Medical College of Wisconsin Associate Director of Clinical Pathology & Technical Director of Microbiology, Children's
Objectives Atypical Pneumonia K. Sue Kehl, Ph.D., D(ABMM) Associate Professor, Pathology Medical College of Wisconsin Associate Director of Clinical Pathology & Technical Director of Microbiology, Children's
Viruses, bacteria, fungus, parasites (in rare cases) or other organisms can cause pneumonia.
 or other organisms can cause pneumonia.") 1 Pneumonia Pneumonia is an infection which inflames the air sacs either in one or both of the lungs. The air sacs are generally filled with fluid or pus, causing cough along with phlegm or pus, fever,
1 Pneumonia Pneumonia is an infection which inflames the air sacs either in one or both of the lungs. The air sacs are generally filled with fluid or pus, causing cough along with phlegm or pus, fever,
RESPIRATORY TRACT INFECTIONS. CLS 212: Medical Microbiology
 RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Anatomy of the Respiratory System Respiratory Infections Respiratory tract can be divided into: Upper Respiratory Tract (URT): Sinuses Nasopharynx,.
RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Anatomy of the Respiratory System Respiratory Infections Respiratory tract can be divided into: Upper Respiratory Tract (URT): Sinuses Nasopharynx,.
General Medical Concerns
 General Medical Concerns General Medical Concerns Fred Reifsteck MD Head Team Physician University of Georgia Missed Time: school, work, practice, games Decreased Performance Physical/ Mental stress: New
General Medical Concerns General Medical Concerns Fred Reifsteck MD Head Team Physician University of Georgia Missed Time: school, work, practice, games Decreased Performance Physical/ Mental stress: New
Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians
 MEMORANDUM DATE: October 1, 2009 TO: FROM: SUBJECT: Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians Michael
MEMORANDUM DATE: October 1, 2009 TO: FROM: SUBJECT: Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians Michael