2019 Drug List Negative Changes
|
|
|
- Antonia Blankenship
- 5 years ago
- Views:
Transcription
1 2019 Drug List Negative Changes Updated 03/26/2019 If you are taking a drug that is removed from the formulary (also known as the Drug List), we will tell you. We will also tell you if we add any restrictions on a drug. We will tell you at least 60 days before we make these changes. This gives you time to talk to your doctor about what to do next. If the Food and Drug Administration (FDA) says a drug you are taking is not safe, we will take it off the formulary right away. We will also send you a letter telling you that. The table below shows changes made to our 2019 formulary. Your cost share depends on your coverage stage. Your formulary tells you the tier that applies to each covered drug. Date of Change Drug Name Type of Change Possible Alternative Drug(s) Comments 1/1/2019 GLEOSTINE CAPS 5 MG 1/1/2019 IPRIVASK SOLR 1/1/2019 ISTODAX SOLR This drug was removed from the market. 1/1/2019 PEG-INTRON REDIPEN PAK 4 KIT This drug was removed from the market. 1/1/2019 POTIGA TABS 300 MG 2/1/2019 FINACEA GEL This drug was removed from the formulary. 15% azelaic acid gel 15% 2/1/2019 MENOMUNE- A/C/Y/W-135 INJ 2/1/2019 TRELSTAR SUSR TRELSTAR MIXJECT 2/1/2019 ZYTIGA TAB This drug was removed from the formulary. 250MG abiraterone acetate tabs NORVIR NORVIR tabs Y0020_DrugLstNegChngWebNtc17_NM
2 Date of Change Drug Name Type of Change Possible Alternative Comments Drug(s) PEGASYS PROCLICK PEGASYS mometasone furoate Nasal triamcinolone acetonide Susp 50 MCG/ACT CLINIMIX 2.75%/DEXTROSE 5% CLINIMIX 4.25%/DEXTROSE 5% amifostine SOLR TETANUS/DIPHTHE RIA TOXOIDS- ADSORBED SUSP ketoprofen CAPS 50 MG triamterene & hydrochlorothiazide 4/1/2019 4/1/2019 This drug was removed from the market. This drug was removed from the market. TDVAX SUSP CAPS 50MG-25MG This drug was removed from the market. ADVAIR DISKU AER 100/50 ADVAIR DISKU AER 250/50 ADVAIR DISKU AER 500/50 ELIDEL CRE 1% INVIRASE CAPS 4/1/2019 MOEXIPRIL/HYDRO CHLOROTHIAZIDE TABS 4/1/2019 NUTRESTORE PACK 4/1/2019 PRALUENT SOSY 75 MG/ML This drug was removed from the formulary. This drug was removed from the formulary. This drug was removed from the formulary. Fluticasone-Salmeterol Aer Powder BA MCG/DOSE Fluticasone-Salmeterol Aer Powder BA MCG/DOSE Fluticasone-Salmeterol Aer Powder BA MCG/DOSE This drug was removed from the formulary. Pimecrolimus Cream 1% This drug was removed from the market. This drug was removed from the market.
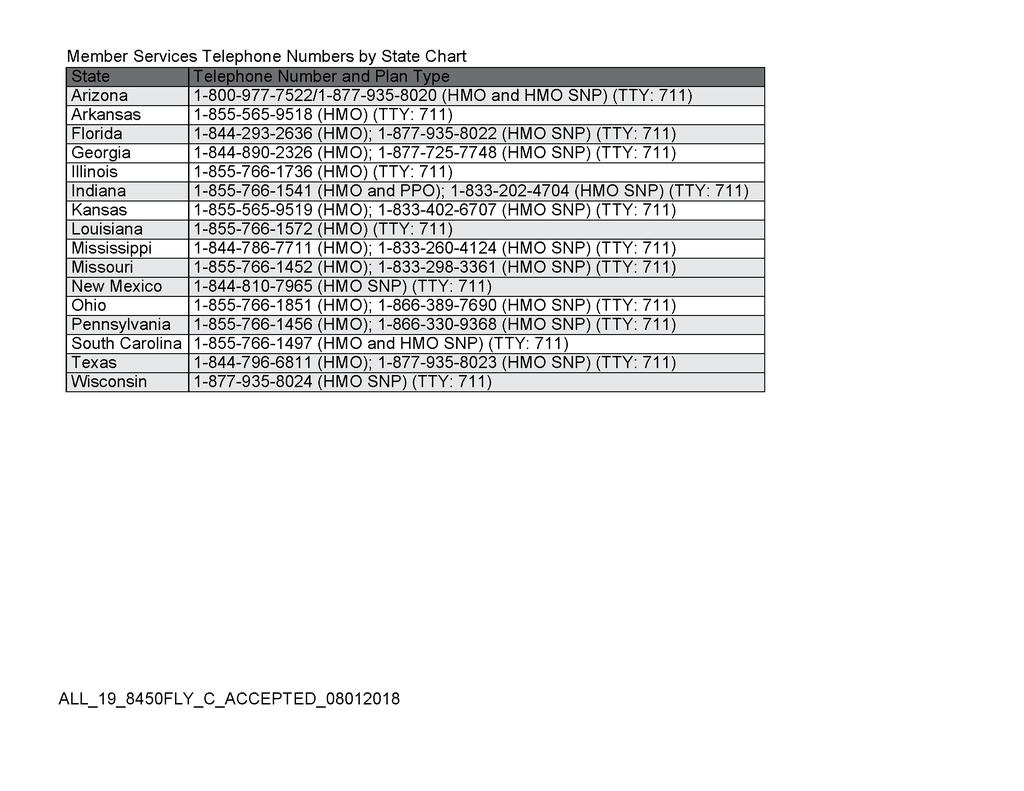
3 Date of Change Drug Name Type of Change Possible Alternative Drug(s) Comments 4/1/2019 REMODULIN INJ This drug was removed from the formulary. Treprostinil Sodium Inj 10 10MG/ML MG/ML 4/1/2019 REMODULIN INJ This drug was removed from the formulary. Treprostinil Sodium Inj 1 1MG/ML MG/ML 4/1/2019 REMODULIN INJ This drug was removed from the formulary. Treprostinil Sodium Inj 2.5MG/ML 2.5 MG/ML 4/1/2019 REMODULIN INJ This drug was removed from the formulary. Treprostinil Sodium Inj 5 5MG/ML MG/ML If you or your doctor disagrees with the change to your drug, you may request an exception. To request an exception, call us at: State Phone Number NM , TTY: 711 PA , TTY: 711 SC , TTY: 711 From October 1 March 31, 7 days a week, 8 a.m. to 8 p.m. From April 1 - September 30, Monday through Friday, 8 a.m. to 8 p.m. A messaging system is used after hours, weekends, and on federal holidays. Your doctor must provide a statement to support your request. For details on asking for an exception, check your Evidence of Coverage.
4 If you don t agree with our decision, you may file a complaint with us. To file a complaint, call us at: State Phone Number NM , TTY: 711 PA , TTY: 711 SC , TTY: 711 From October 1 March 31, 7 days a week, 8 a.m. to 8 p.m. From April 1 - September 30, Monday through Friday, 8 a.m. to 8 p.m. A messaging system is used after hours, weekends, and on federal holidays. Your doctor must provide a statement to support your request. You may also send your complaint to us in writing at the following address. Allwell Attn: Medicare Appeals & Grievances 7700 Forsyth Boulevard St. Louis, MO The Formulary may change at any time. You will receive notice when necessary.
5
6
7
8
9
10
11
2019 Drug List Negative Changes
 2019 Drug List Negative Changes Updated 03/26/2019 If you are taking a drug that is removed from the formulary (also known as the Drug List), we will tell you. We will also tell you if we add any restrictions
2019 Drug List Negative Changes Updated 03/26/2019 If you are taking a drug that is removed from the formulary (also known as the Drug List), we will tell you. We will also tell you if we add any restrictions
2019 Drug List Negative Changes
 2019 Drug List Negative Changes Updated 02/26/2019 If you are taking a drug that is removed from the formulary (also known as the Drug List), we will tell you. We will also tell you if we add any restrictions
2019 Drug List Negative Changes Updated 02/26/2019 If you are taking a drug that is removed from the formulary (also known as the Drug List), we will tell you. We will also tell you if we add any restrictions
Notice of Mid-Year Changes to 2019 Paramount Enhanced Formulary
 Notice of Mid-Year s to 2019 Paramount Enhanced Formulary Paramount Elite (HMO) may immediately remove a brand name drug on our List if we are replacing it with a new generic drug that will appear on the
Notice of Mid-Year s to 2019 Paramount Enhanced Formulary Paramount Elite (HMO) may immediately remove a brand name drug on our List if we are replacing it with a new generic drug that will appear on the
Santa Clara Family Health Plan Cal MediConnect Plan (Medicare-Medicaid Plan) 2017 Drug List
 2017 Drug List") Upcoming Changes to Santa Clara Family Health Plan Cal MediConnect Plan (Medicare-Medicaid Plan) 2017 Drug List Updated 8/1/2017 Santa Clara Family Health Plan (SCFHP) Cal MediConnect Plan (Medicare-Medicaid
Upcoming Changes to Santa Clara Family Health Plan Cal MediConnect Plan (Medicare-Medicaid Plan) 2017 Drug List Updated 8/1/2017 Santa Clara Family Health Plan (SCFHP) Cal MediConnect Plan (Medicare-Medicaid
Changes to the 2018 BlueCross Secure SM (HMO) & BlueCross Total SM (PPO) Formularies
 & BlueCross Total SM (PPO) Formularies") Changes to the 2018 BlueCross Secure SM (HMO) & BlueCross Total SM (PPO) Formularies BlueCross BlueShield of South Carolina may add or remove drugs from the formulary during the year. If we remove drugs
Changes to the 2018 BlueCross Secure SM (HMO) & BlueCross Total SM (PPO) Formularies BlueCross BlueShield of South Carolina may add or remove drugs from the formulary during the year. If we remove drugs
2018 Formulary Notice of Change Prescription Drug Plans
 2018 Formulary Notice of Change Prescription Drug Plans WellCare Prescription Insurance, Inc. Plans in all states: WellCare Classic (PDP) WellCare may add or remove drugs from our formulary during the
2018 Formulary Notice of Change Prescription Drug Plans WellCare Prescription Insurance, Inc. Plans in all states: WellCare Classic (PDP) WellCare may add or remove drugs from our formulary during the
2019 Formulary Update
 MEDICARE ADVANTAGE BlueShield of Northeastern New York Formulary Update BlueShield of Northeastern New York has updated its formulary (drug list) since its original publication in January. This document
MEDICARE ADVANTAGE BlueShield of Northeastern New York Formulary Update BlueShield of Northeastern New York has updated its formulary (drug list) since its original publication in January. This document
2014 Quantity Limits (QL) Criteria
 Criteria") 2014 Quantity Limits (QL) Criteria Certain drugs covered through your EmblemHealth Medicare HMO/PPO Medicare Plan are covered for only a limited quantity. We do this to ensure compliance with the US Food
2014 Quantity Limits (QL) Criteria Certain drugs covered through your EmblemHealth Medicare HMO/PPO Medicare Plan are covered for only a limited quantity. We do this to ensure compliance with the US Food
Memorial Hermann Advantage HMO February 2019 Formulary Addendum
 Memorial Hermann Advantage HMO February 2019 Formulary Addendum Changes may have occurred since the printing of your current Memorial Hermann Advantage HMO Formulary. Medications that may have been added
Memorial Hermann Advantage HMO February 2019 Formulary Addendum Changes may have occurred since the printing of your current Memorial Hermann Advantage HMO Formulary. Medications that may have been added
Formulary Change Notice
 Formulary Change Notice HealthPartners may remove drugs from our formulary (list of covered drugs) or add rules about whether and when certain drugs are covered during the year. The chart below contains
Formulary Change Notice HealthPartners may remove drugs from our formulary (list of covered drugs) or add rules about whether and when certain drugs are covered during the year. The chart below contains
2018 Drug List Negative Changes Updated 10/25/2018 The table below shows changes made to our 2018 List of Covered Drugs (Formulary).
.") 2018 Drug List Negative s Updated 10/25/2018 The table below shows changes made to our 2018 List of Covered Drugs (Formulary). Date of 1/1/2018 COLYTE-FLAVOR PACKS SOLR 227.1GM- 21.5GM-5.53GM- 2.82GM-6.36GM
2018 Drug List Negative s Updated 10/25/2018 The table below shows changes made to our 2018 List of Covered Drugs (Formulary). Date of 1/1/2018 COLYTE-FLAVOR PACKS SOLR 227.1GM- 21.5GM-5.53GM- 2.82GM-6.36GM
Blue Cross and Blue Shield of Minnesota GenRx Formulary Updates
 Blue Cross and Blue Shield of Minnesota GenRx Formulary Updates July 2018 TRADE NAME (generic name) or generic name ADVAIR DISKUS (fluticasone-salmeterol aer powder ba 100-50 mcg/dose) Brand Addition ADVAIR
Blue Cross and Blue Shield of Minnesota GenRx Formulary Updates July 2018 TRADE NAME (generic name) or generic name ADVAIR DISKUS (fluticasone-salmeterol aer powder ba 100-50 mcg/dose) Brand Addition ADVAIR
MEMBER GRIEVANCES AND APPEALS PROCEDURES
 MEMBER GRIEVANCES AND APPEALS PROCEDURES We value our members. We want you to let us know right away if you are not happy with our health plan. This includes if you have any questions, complaints or problems
MEMBER GRIEVANCES AND APPEALS PROCEDURES We value our members. We want you to let us know right away if you are not happy with our health plan. This includes if you have any questions, complaints or problems
ICP Formulary Updates
 ICP Formulary Updates July 2017 TRADE NAME (generic name) adapalene cream 0.1% 2017-07-01 Removal adapalene gel 0.3% 2017-07-01 Removal adefovir dipivoxil tab 10 mg 2017-07-01 Removal ADVAIR DISKUS (fluticasone-salmeterol
ICP Formulary Updates July 2017 TRADE NAME (generic name) adapalene cream 0.1% 2017-07-01 Removal adapalene gel 0.3% 2017-07-01 Removal adefovir dipivoxil tab 10 mg 2017-07-01 Removal ADVAIR DISKUS (fluticasone-salmeterol
Aetna Better Health FIDA Plan
 Aetna Better Health FIDA Plan May 2016 Formulary Updates ASCOMP/COD - QL; PA FYAVOLV 5MCG; 1MG- PA METOPROLOL TABS 37.5MG, 75MG CIPRODEX LETAIRIS - QL; PA OFEV - QL; PA OTREXUP - ST PRALUENT - QL; PA RASUVO
Aetna Better Health FIDA Plan May 2016 Formulary Updates ASCOMP/COD - QL; PA FYAVOLV 5MCG; 1MG- PA METOPROLOL TABS 37.5MG, 75MG CIPRODEX LETAIRIS - QL; PA OFEV - QL; PA OTREXUP - ST PRALUENT - QL; PA RASUVO
Health Partners Medicare Prime 2019 Formulary Changes
 Health Partners Medicare Prime 2019 Formulary Changes Changes occur, for example, because new drugs come on the market, a drug is moved to a different cost-sharing level (tier), or a generic version becomes
Health Partners Medicare Prime 2019 Formulary Changes Changes occur, for example, because new drugs come on the market, a drug is moved to a different cost-sharing level (tier), or a generic version becomes
WellCare Signature (PDP) and WellCare Classic (PDP) Formulary Addendum
 and WellCare Classic (PDP) Formulary Addendum") WellCare Signature (PDP) and WellCare Classic (PDP) Formulary Addendum This is a listing of the changes that have occurred in our formulary. Please carefully review these changes and call WellCare if you
WellCare Signature (PDP) and WellCare Classic (PDP) Formulary Addendum This is a listing of the changes that have occurred in our formulary. Please carefully review these changes and call WellCare if you
2019 Drug List Negative Changes Updated 02/26/2019
 2019 Drug List Negative Changes Updated 02/26/2019 If you are taking a drug that is removed from the drug list, we will tell you. We will also tell you if we add any restrictions on a drug. We will tell
2019 Drug List Negative Changes Updated 02/26/2019 If you are taking a drug that is removed from the drug list, we will tell you. We will also tell you if we add any restrictions on a drug. We will tell
2018 Drug List Change Notice Updated 10/25/2018
 2018 Drug List Change Notice Updated 10/25/2018 If you are taking a drug that is removed from the drug list, we will tell you. We will also tell you if we add any restrictions on a drug such as: Quantity
2018 Drug List Change Notice Updated 10/25/2018 If you are taking a drug that is removed from the drug list, we will tell you. We will also tell you if we add any restrictions on a drug such as: Quantity
Mercy Care ALBENDAZOLE. Products Affected. ALBENZA TABLET 200 MG ORAL Details. Criteria. Refer to PA Guideline for approval criteria
 ALBENDAZOLE Mercy Care ALBENZA TABLET 200 MG ORAL Refer to PA Guideline for approval criteria 1 BRIMONIDINE-TIMOLOL COMBIGAN SOLUTION 0.2-0.5 % OPHTHALMIC Requires use of separate ingredients for at least
ALBENDAZOLE Mercy Care ALBENZA TABLET 200 MG ORAL Refer to PA Guideline for approval criteria 1 BRIMONIDINE-TIMOLOL COMBIGAN SOLUTION 0.2-0.5 % OPHTHALMIC Requires use of separate ingredients for at least
Quarterly pharmacy formulary change notice
 Quarterly pharmacy formulary change notice The formulary changes listed in the table below were reviewed and approved at our second quarter 2018 Pharmacy and Therapeutics Committee meeting. Effective October
Quarterly pharmacy formulary change notice The formulary changes listed in the table below were reviewed and approved at our second quarter 2018 Pharmacy and Therapeutics Committee meeting. Effective October
Quarterly pharmacy formulary change notice
 MEDICAID PROVIDER BULLETIN October 2018 The formulary changes listed in the table below were reviewed and approved at the second-quarter 2018 Pharmacy and Therapeutics Committee meeting. Effective October
MEDICAID PROVIDER BULLETIN October 2018 The formulary changes listed in the table below were reviewed and approved at the second-quarter 2018 Pharmacy and Therapeutics Committee meeting. Effective October
August 2016 Formulary Updates
 August 2016 Formulary Updates DOXYCYCLINE HYCLATE TABS DR 50MG, 200MG NALOXONE HCL INJ 0.4MG/ML VANCOMYCIN HCL INJ 500MG, 750MG BRIVIACT INJ - PA BRIVIACT ORAL SOLN - QL; PA BRIVIACT TABS - QL; PA LENVIMA
August 2016 Formulary Updates DOXYCYCLINE HYCLATE TABS DR 50MG, 200MG NALOXONE HCL INJ 0.4MG/ML VANCOMYCIN HCL INJ 500MG, 750MG BRIVIACT INJ - PA BRIVIACT ORAL SOLN - QL; PA BRIVIACT TABS - QL; PA LENVIMA
Quarterly pharmacy formulary change notice
 Provider Bulletin October 2018 Quarterly pharmacy formulary change notice The formulary changes listed in the table below apply to all Anthem HealthKeepers Plus patients. The changes listed in the table
Provider Bulletin October 2018 Quarterly pharmacy formulary change notice The formulary changes listed in the table below apply to all Anthem HealthKeepers Plus patients. The changes listed in the table
Medicare Part D 2012 Formulary Changes Service To Senior and Total Fit
 Medicare Part D 2012 Formulary s Service To Senior and Total Fit Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization,
Medicare Part D 2012 Formulary s Service To Senior and Total Fit Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization,
MEMBER GRIEVANCE/COMPLAINT FORM. Address City State Zip Code
 MEMBER GRIEVANCE/COMPLAINT FORM Date: Please print all information. Complainant information: ( ) ( ) Name Work Telephone Number Home Telephone Number Address City State Zip Code Name of person(s) related
MEMBER GRIEVANCE/COMPLAINT FORM Date: Please print all information. Complainant information: ( ) ( ) Name Work Telephone Number Home Telephone Number Address City State Zip Code Name of person(s) related
3 Tier Formulary Additions
 3 Tier Formulary Additions Drug Name Tier Category Management ACCU-CHECK GUIDE ME GLUCOSE METER 3 Diabetic Supplies Step Therapy applies pyridostigmine bromide 60mg/5ml syrup 1 Antimyasthenic Agents New
3 Tier Formulary Additions Drug Name Tier Category Management ACCU-CHECK GUIDE ME GLUCOSE METER 3 Diabetic Supplies Step Therapy applies pyridostigmine bromide 60mg/5ml syrup 1 Antimyasthenic Agents New
Mercy Care Plan. Acyclovir Ointment. Products Affected. acyclovir ointment 5 % external Details. Criteria. Requires use of oral Acyclovir
 Acyclovir Ointment Mercy Care Plan acyclovir ointment 5 % external Requires use of oral Acyclovir 1 Adcirca ADCIRCA TABLET 20 MG ORAL Requires use of Sildenafil 2 Albenza ALBENZA TABLET 200 MG ORAL Requires
Acyclovir Ointment Mercy Care Plan acyclovir ointment 5 % external Requires use of oral Acyclovir 1 Adcirca ADCIRCA TABLET 20 MG ORAL Requires use of Sildenafil 2 Albenza ALBENZA TABLET 200 MG ORAL Requires
2018 Step Therapy (ST) Criteria
 Criteria") 2018 Step Therapy (ST) Criteria Some drugs require step therapy pre-approval. This means that your doctor must have you first try a different drug to treat your medical condition before we will cover a
2018 Step Therapy (ST) Criteria Some drugs require step therapy pre-approval. This means that your doctor must have you first try a different drug to treat your medical condition before we will cover a
Medicare Part D 2017 Formulary Changes OC Preferred
 Medicare Part D 2017 Formulary Changes OC Preferred Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization,
Medicare Part D 2017 Formulary Changes OC Preferred Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization,
FORMULARY CHANGE NOTICE 2008 JULY
 FORMULARY CHANGE NOTICE 2008 JULY Drug Name Dosage Form Strength Alternative Medicine* Formulary Formulary Change and Reason Status of Alternative Medication Updated Status On Formulary STARLIX TABS 120MG
FORMULARY CHANGE NOTICE 2008 JULY Drug Name Dosage Form Strength Alternative Medicine* Formulary Formulary Change and Reason Status of Alternative Medication Updated Status On Formulary STARLIX TABS 120MG
Step Therapy Criteria
 Tier 5 Formulary Step Therapy 2016 Updated: 05/24/2016 Effective: 06/01/2016 What is Step Therapy? Some prescription drugs require step therapy (ST). In some cases, the plan requires you to first try certain
Tier 5 Formulary Step Therapy 2016 Updated: 05/24/2016 Effective: 06/01/2016 What is Step Therapy? Some prescription drugs require step therapy (ST). In some cases, the plan requires you to first try certain
Medicare Part D Opioid Policies for 2019 Information for Patients
 CENTERS FOR MEDICARE & MEDICAID SERVICES Medicare Part D Opioid Policies for 2019 Information for Patients Introduction Prescription opioid pain medications like oxycodone (OxyContin ), hydrocodone (Vicodin
CENTERS FOR MEDICARE & MEDICAID SERVICES Medicare Part D Opioid Policies for 2019 Information for Patients Introduction Prescription opioid pain medications like oxycodone (OxyContin ), hydrocodone (Vicodin
WellCare s South Carolina Preferred Drug List Update
 WellCare s South Carolina Preferred Drug List Update This is a list of changes to our preferred drug list. These are a result of the latest WellCare Pharmacy & Therapeutics meeting held on 09/21/2017.
WellCare s South Carolina Preferred Drug List Update This is a list of changes to our preferred drug list. These are a result of the latest WellCare Pharmacy & Therapeutics meeting held on 09/21/2017.
PDP Classic Formulary Addendum
 PDP Classic Formulary Addendum The following medications have been added to the WellCare formulary as of March 2009. Drug Name Therapeutic Class Drug Tier Requirements/Limits Changes Made acetazolamide
PDP Classic Formulary Addendum The following medications have been added to the WellCare formulary as of March 2009. Drug Name Therapeutic Class Drug Tier Requirements/Limits Changes Made acetazolamide
Quarterly pharmacy formulary change notice
 Provider update Quarterly pharmacy formulary change notice Summary: The formulary changes listed in the table below were reviewed and approved at our first-quarter 2018, Pharmacy and Therapeutics Committee
Provider update Quarterly pharmacy formulary change notice Summary: The formulary changes listed in the table below were reviewed and approved at our first-quarter 2018, Pharmacy and Therapeutics Committee
Medicare Part D 2016 Formulary Changes Desert Preferred Choice
 Medicare Part D 2016 Formulary s Desert Preferred Choice Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization,
Medicare Part D 2016 Formulary s Desert Preferred Choice Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization,
Medicare Part D 2017 Formulary Changes OC Preferred
 Medicare Part D 017 Formulary s OC Preferred Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization, quantity
Medicare Part D 017 Formulary s OC Preferred Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization, quantity
Quarterly pharmacy formulary change notice
 Quarterly pharmacy formulary change notice Provider update Summary: Effective August 1, 2018, the preferred formulary changes detailed in the table below will apply to District of Columbia Healthy Families
Quarterly pharmacy formulary change notice Provider update Summary: Effective August 1, 2018, the preferred formulary changes detailed in the table below will apply to District of Columbia Healthy Families
ANTICONVULSANTS. Details. Step Therapy Criteria Date Effective: April 1, 2019
 Step Therapy Date Effective: April 1, 2019 ANTICONVULSANTS APTIOM TABLET 200 MG ORAL APTIOM TABLET 400 MG ORAL APTIOM TABLET 600 MG ORAL APTIOM TABLET 800 MG ORAL BANZEL SUSPENSION 40 MG/ML ORAL BANZEL
Step Therapy Date Effective: April 1, 2019 ANTICONVULSANTS APTIOM TABLET 200 MG ORAL APTIOM TABLET 400 MG ORAL APTIOM TABLET 600 MG ORAL APTIOM TABLET 800 MG ORAL BANZEL SUSPENSION 40 MG/ML ORAL BANZEL
Health TALK. Mammograms save lives. Plan to quit.
 Health TALK FALL 2018 VOLTEE PARA ESPAÑOL! Plan to quit. Every November, the Great American Smokeout asks everyone to quit smoking. You can quit for just that one day. Or it could be the fi rst day of
Health TALK FALL 2018 VOLTEE PARA ESPAÑOL! Plan to quit. Every November, the Great American Smokeout asks everyone to quit smoking. You can quit for just that one day. Or it could be the fi rst day of
Medicare Part D 2017 Formulary Changes Service To Senior
 Medicare Part D 2017 Formulary s Service To Senior Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization,
Medicare Part D 2017 Formulary s Service To Senior Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization,
2014 Step Therapy Criteria (List of Step Therapy Criteria)
") Criteria Last Updated: November 1, 2014 2014 Step Therapy Criteria (List of Step Therapy Criteria) PLEASE READ CAREFULLY: IEHP MEDICARE DUALCHOICE (HMO SNP) REQUIRES YOU TO FIRST TRY CERTAIN DRUGS TO TREAT
Criteria Last Updated: November 1, 2014 2014 Step Therapy Criteria (List of Step Therapy Criteria) PLEASE READ CAREFULLY: IEHP MEDICARE DUALCHOICE (HMO SNP) REQUIRES YOU TO FIRST TRY CERTAIN DRUGS TO TREAT
$250 (Deductible does not apply to Tier 1 and Tier 2) $500 (Deductible does not apply to Tier 1 and Tier 2)
 $500 (Deductible does not apply to Tier 1 and Tier 2)") Benefit Summary Outpatient Prescription Drug Illinois 5/50/100/250 Plan 455 Your Co-payment and/or Co-insurance is determined by the tier to which the Prescription Drug List (PDL) Management Committee
Benefit Summary Outpatient Prescription Drug Illinois 5/50/100/250 Plan 455 Your Co-payment and/or Co-insurance is determined by the tier to which the Prescription Drug List (PDL) Management Committee
Medication Policy Manual. Topic: Dupixent, dupilumab Date of Origin: March 10, Committee Approval: March 10, 2017 Next Review Date: May 2018
 Independent licensees of the Blue Cross and Blue Shield Association Medication Policy Manual Policy No: dru493 Topic: Dupixent, dupilumab Date of Origin: March 10, 2017 Committee Approval: March 10, 2017
Independent licensees of the Blue Cross and Blue Shield Association Medication Policy Manual Policy No: dru493 Topic: Dupixent, dupilumab Date of Origin: March 10, 2017 Committee Approval: March 10, 2017
Medicare Part D 2016 Formulary Changes Service To Senior and OC Preferred
 Medicare Part D 2016 Formulary s Service To Senior and OC Preferred Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior
Medicare Part D 2016 Formulary s Service To Senior and OC Preferred Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior
December 2016 Formulary Updates
 December 2016 Formulary Updates ABACAVIR/LAMIVUDINE AMLODIPINE/OLMESARTAN MEDOXOMIL TAB 10-20MG QL AMLODIPINE/OLMESARTAN MEDOXOMIL TAB 10-40MG QL AMLODIPINE/OLMESARTAN MEDOXOMIL TAB 5-20MG QL AMLODIPINE/OLMESARTAN
December 2016 Formulary Updates ABACAVIR/LAMIVUDINE AMLODIPINE/OLMESARTAN MEDOXOMIL TAB 10-20MG QL AMLODIPINE/OLMESARTAN MEDOXOMIL TAB 10-40MG QL AMLODIPINE/OLMESARTAN MEDOXOMIL TAB 5-20MG QL AMLODIPINE/OLMESARTAN
Network Health Insurance Corporation Upcoming Negative Changes to the Medicare Part D Formulary
 Requesting an Exception to the Formulary You can ask Network Health Insurance Corporation to make an exception to our coverage rules. Generally, we will only approve your request for an exception if alternative
Requesting an Exception to the Formulary You can ask Network Health Insurance Corporation to make an exception to our coverage rules. Generally, we will only approve your request for an exception if alternative
Quarterly pharmacy formulary change
 Medi-Cal Managed Care L. A. Care Major Risk Medical Insurance Program Provider Bulletin The formulary changes listed in the table below were reviewed and approved at our first-quarter 2018 Pharmacy and
Medi-Cal Managed Care L. A. Care Major Risk Medical Insurance Program Provider Bulletin The formulary changes listed in the table below were reviewed and approved at our first-quarter 2018 Pharmacy and
November 2016 Formulary Updates
 November 2016 Formulary Updates DAPTOMYCIN LARISSIA NITROGLYCERIN SUBL ORFADIN 20MG CAP PA RELISTOR 150MG TAB PA; QL Over-the-Counter (OTC) Drugs Added* COLEMAN SKINSMART INSECT REP CUTTER BACKWOODS AERO
November 2016 Formulary Updates DAPTOMYCIN LARISSIA NITROGLYCERIN SUBL ORFADIN 20MG CAP PA RELISTOR 150MG TAB PA; QL Over-the-Counter (OTC) Drugs Added* COLEMAN SKINSMART INSECT REP CUTTER BACKWOODS AERO
2018 Formulary Update
 MEDICARE ADVANTAGE BlueShield of Northeastern New York 2018 Formulary Update BlueShield of Northeastern New York has updated its formulary (drug list) since its original publication in January 2018. This
MEDICARE ADVANTAGE BlueShield of Northeastern New York 2018 Formulary Update BlueShield of Northeastern New York has updated its formulary (drug list) since its original publication in January 2018. This
Updates to your prescription benefits
 Updates to your prescription benefits Effective Jan. 1, 2018 Update Summary Within the Prescription Drug List (PDL), medications are grouped by tier. The tier indicates the amount you pay when you fill
Updates to your prescription benefits Effective Jan. 1, 2018 Update Summary Within the Prescription Drug List (PDL), medications are grouped by tier. The tier indicates the amount you pay when you fill
Thank you for being a Premera Blue Cross Medicare Supplement plan member.
 P.O. Box 327 Seattle, WA 98111 February 18, 2019 MSF1 Dear : Thank you for being a Premera Blue Cross Medicare Supplement plan member. The rate table on the next page shows the following rate information:
P.O. Box 327 Seattle, WA 98111 February 18, 2019 MSF1 Dear : Thank you for being a Premera Blue Cross Medicare Supplement plan member. The rate table on the next page shows the following rate information:
Upper Peninsula Health Plan Advantage (HMO) (List of Covered Drugs)
 (List of Covered Drugs)") Analgesics Opioid Analgesics, Long-acting fentanyl 100 mcg/hr patch td72 morphine sulfate 30 mg tablet er Opioid Analgesics, Short-acting fentanyl citrate 200 mcg lozenge hd hydrocodone/acetaminophen 5
Analgesics Opioid Analgesics, Long-acting fentanyl 100 mcg/hr patch td72 morphine sulfate 30 mg tablet er Opioid Analgesics, Short-acting fentanyl citrate 200 mcg lozenge hd hydrocodone/acetaminophen 5
Medicare Part D 2017 Formulary Changes OC Preferred
 Medicare Part D 2017 Formulary s OC Preferred Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization, quantity
Medicare Part D 2017 Formulary s OC Preferred Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization, quantity
Medicare Part D 2017 Formulary Changes Service To Senior
 Medicare Part D 2017 Formulary Changes Service To Senior Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization,
Medicare Part D 2017 Formulary Changes Service To Senior Inter Valley Health Plan may add or remove drugs from our formulary during the year. If we remove a drug from our formulary, add prior authorization,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2116-3 Program Prior Authorization/Medical Necessity Medications Dupixent (dupilumab) P&T Approval Date 1/2017, 5/2017, 7/2017
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2116-3 Program Prior Authorization/Medical Necessity Medications Dupixent (dupilumab) P&T Approval Date 1/2017, 5/2017, 7/2017
Step Therapy Medications
 Step Therapy Medications Step Therapy (ST PA ) is an automated form of prior authorization. It encourages the use of therapies that should be tried first, before other treatments are covered, based on
Step Therapy Medications Step Therapy (ST PA ) is an automated form of prior authorization. It encourages the use of therapies that should be tried first, before other treatments are covered, based on
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Fluticasone/Salmeterol (Advair Diskus, Advair HFA) Reference Number: CP.PMN.31 Effective Date: 10.01.18 Last Review Date: 07.13.18 Line of Business: Oregon Health Plan See Important Reminder
Clinical Policy: Fluticasone/Salmeterol (Advair Diskus, Advair HFA) Reference Number: CP.PMN.31 Effective Date: 10.01.18 Last Review Date: 07.13.18 Line of Business: Oregon Health Plan See Important Reminder
Eucrisa. Eucrisa (crisaborole) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.25 Subject: Eucrisa Page: 1 of 6 Last Review Date: September 15, 2017 Eucrisa Description Eucrisa
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.25 Subject: Eucrisa Page: 1 of 6 Last Review Date: September 15, 2017 Eucrisa Description Eucrisa
2019 Supplemental Drug List
 2019 Supplemental Drug List This supplemental drug list was updated on August 2018. For more recent information or other questions, please contact Blue Cross Medicare Advantage Customer Service, at 1-877-299-1008
2019 Supplemental Drug List This supplemental drug list was updated on August 2018. For more recent information or other questions, please contact Blue Cross Medicare Advantage Customer Service, at 1-877-299-1008
Healthy Michigan Dental Plan Handbook
 Healthy Michigan Dental Plan Handbook Contents 1. Welcome 2. Definitions 3. How to Use Healthy Michigan Plan 4. What Healthy Michigan Plan Covers 5. Questions and Answers 6. Grievances and Appeals 7. General
Healthy Michigan Dental Plan Handbook Contents 1. Welcome 2. Definitions 3. How to Use Healthy Michigan Plan 4. What Healthy Michigan Plan Covers 5. Questions and Answers 6. Grievances and Appeals 7. General
Updates to your prescription benefits
 Updates to your prescription benefits Effective January 1, 2019 Update Summary Within the Prescription Drug List (PDL), medications are grouped by tier. The tier indicates the amount you pay when you fill
Updates to your prescription benefits Effective January 1, 2019 Update Summary Within the Prescription Drug List (PDL), medications are grouped by tier. The tier indicates the amount you pay when you fill
Eucrisa. Eucrisa (crisaborole) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Eucrisa Page: 1 of 7 Last Review Date: June 22, 2018 Eucrisa Description Eucrisa (crisaborole)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Eucrisa Page: 1 of 7 Last Review Date: June 22, 2018 Eucrisa Description Eucrisa (crisaborole)
JANUVIA 50 MG TABLET BYDUREON 2 MG/0.65 ML JARDIANCE 10 MG TABLET SUBCUTANEOUS PEN INJECTOR JARDIANCE 25 MG TABLET BYDUREON BCISE 2 MG/0.
 ANTI DIABETICS BYDUREON 2 MG SUBCUTANEOUS JANUVIA 25 MG TABLET EXTENDED RELEASE SUSPENSION JANUVIA 50 MG TABLET BYDUREON 2 MG/0.65 ML JARDIANCE 10 MG TABLET SUBCUTANEOUS PEN INJECTOR JARDIANCE 25 MG TABLET
ANTI DIABETICS BYDUREON 2 MG SUBCUTANEOUS JANUVIA 25 MG TABLET EXTENDED RELEASE SUSPENSION JANUVIA 50 MG TABLET BYDUREON 2 MG/0.65 ML JARDIANCE 10 MG TABLET SUBCUTANEOUS PEN INJECTOR JARDIANCE 25 MG TABLET
Additional DRUG COVERAGE
 Additional DRUG COVERAGE Lower-cost Medicare prescription drugs Your plan covers some of your Medicare prescription drugs and supplies at a lower drug tier or co-pay than in your formulary (drug list).
Additional DRUG COVERAGE Lower-cost Medicare prescription drugs Your plan covers some of your Medicare prescription drugs and supplies at a lower drug tier or co-pay than in your formulary (drug list).
Remodulin. Advantages and Challenges
 Remodulin Advantages and Challenges 1 Remodulin Background 2002 2004 2006 Continuous SC* infusion Continuous SC or IV infusion Transition from Flolan (epoprostenol sodium) Based on: Phase III trials; Simonneau
Remodulin Advantages and Challenges 1 Remodulin Background 2002 2004 2006 Continuous SC* infusion Continuous SC or IV infusion Transition from Flolan (epoprostenol sodium) Based on: Phase III trials; Simonneau
Additional Drug Coverage
 Additional Drug Coverage Bonus Drug List Your employer group or plan sponsor offers a bonus drug list. The prescription drugs on this list are covered in addition to the drugs on the plan s drug list (formulary).
Additional Drug Coverage Bonus Drug List Your employer group or plan sponsor offers a bonus drug list. The prescription drugs on this list are covered in addition to the drugs on the plan s drug list (formulary).
Health TALK. Heart smart. Plan to quit. Know your cholesterol numbers.
 Health TALK FALL 2018 VOLTEE PARA ESPAÑOL! Plan to quit. Every November, the Great American Smokeout asks everyone to quit smoking. You can quit for just that one day, or it could be the fi rst day of
Health TALK FALL 2018 VOLTEE PARA ESPAÑOL! Plan to quit. Every November, the Great American Smokeout asks everyone to quit smoking. You can quit for just that one day, or it could be the fi rst day of
Drug Class Monograph
 Drug Class Monograph Class: Inhaled Corticosteroids Drugs: Aerospan (flunisolide), Advair Diskus, Advair HFA (fluticasone/salmeterol), Alvesco (ciclesonide), Arnuity Ellipta (fluticasone furoate), Asmanex
Drug Class Monograph Class: Inhaled Corticosteroids Drugs: Aerospan (flunisolide), Advair Diskus, Advair HFA (fluticasone/salmeterol), Alvesco (ciclesonide), Arnuity Ellipta (fluticasone furoate), Asmanex
Plan Year CCHP Senior Program (HMO) Step Therapy Criteria (ST)
 Step Therapy Criteria (ST)") Plan Year 2016 CCHP Senior Program (HMO) Step Therapy Criteria (ST) Step Therapy: In some cases, CCHP Senior Program (HMO) requires you to first try certain drugs to treat your medical condition before
Plan Year 2016 CCHP Senior Program (HMO) Step Therapy Criteria (ST) Step Therapy: In some cases, CCHP Senior Program (HMO) requires you to first try certain drugs to treat your medical condition before
December 2016 Formulary Updates
 December 2016 Formulary Updates ABACAVIR/LAMIVUDINE AMLODIPINE/OLMESARTAN MEDOXOMIL TAB 10-20MG QL AMLODIPINE/OLMESARTAN MEDOXOMIL TAB 10-40MG QL AMLODIPINE/OLMESARTAN MEDOXOMIL TAB 5-20MG QL AMLODIPINE/OLMESARTAN
December 2016 Formulary Updates ABACAVIR/LAMIVUDINE AMLODIPINE/OLMESARTAN MEDOXOMIL TAB 10-20MG QL AMLODIPINE/OLMESARTAN MEDOXOMIL TAB 10-40MG QL AMLODIPINE/OLMESARTAN MEDOXOMIL TAB 5-20MG QL AMLODIPINE/OLMESARTAN
Blue Cross and Blue Shield of Minnesota GenRx Formulary Updates
 Blue Cross and Blue Shield of Minnesota GenRx Formulary Updates April 2018 TRADE NAME (generic name) or generic name Brand/Generic Description of Change abacavir sulfate soln 20 mg/ml (base equiv) Generic
Blue Cross and Blue Shield of Minnesota GenRx Formulary Updates April 2018 TRADE NAME (generic name) or generic name Brand/Generic Description of Change abacavir sulfate soln 20 mg/ml (base equiv) Generic
Chiropractic Services Amendment of the Kaiser Foundation Health Plan, Inc., Evidence of Coverage for SANTA CLARA COUNTY SCHOOLS INSURANCE GROUP
 EOC #82 - Kaiser Foundation Health Plan, Inc. Northern California Region Chiropractic Services Amendment of the Kaiser Foundation Health Plan, Inc., Evidence of Coverage for SANTA CLARA COUNTY SCHOOLS
EOC #82 - Kaiser Foundation Health Plan, Inc. Northern California Region Chiropractic Services Amendment of the Kaiser Foundation Health Plan, Inc., Evidence of Coverage for SANTA CLARA COUNTY SCHOOLS
2016 FORMULARY ADDENDUM NOTICE OF CHANGE
 2016 FORMULARY ADDENDUM NOTICE OF CHANGE (PRESCRIPTION DRUG PLANS) WELLCARE PRESCRIPTION INSURANCE, INC. WellCare Simple (PDP) WellCare Classic (PDP) WellCare Extra (PDP) This is a listing of the changes
2016 FORMULARY ADDENDUM NOTICE OF CHANGE (PRESCRIPTION DRUG PLANS) WELLCARE PRESCRIPTION INSURANCE, INC. WellCare Simple (PDP) WellCare Classic (PDP) WellCare Extra (PDP) This is a listing of the changes
Aetna Better Health of Illinois Medicaid Formulary Updates
 October 2017 o DOXYLAMINE SUCCINATE 25mg-QL o DULOXETINE CAP 40MG DR-QL o GUANFACIN ER TABS (all strengths)-ql o TOBRAMYCIN NEBU SOLUTION- PA August 2017 Aetna Better Health of Illinois Medicaid 2017 Formulary
October 2017 o DOXYLAMINE SUCCINATE 25mg-QL o DULOXETINE CAP 40MG DR-QL o GUANFACIN ER TABS (all strengths)-ql o TOBRAMYCIN NEBU SOLUTION- PA August 2017 Aetna Better Health of Illinois Medicaid 2017 Formulary
Checking your. blood sugar. How frequent blood sugar checks can help you. When to check your blood sugar. Keeping a blood sugar tracker
 Checking your blood sugar How frequent blood sugar checks can help you Checking your blood sugar yourself is an important part of managing diabetes. Checking often will tell you: If your insulin or other
Checking your blood sugar How frequent blood sugar checks can help you Checking your blood sugar yourself is an important part of managing diabetes. Checking often will tell you: If your insulin or other
Managed Health Services (MHS) Candace V. Ervin Market Manager, Indiana Provider Relations October 18, 2017
 Candace V. Ervin Market Manager, Indiana Provider Relations October 18, 2017") Managed Health Services (MHS) Candace V. Ervin Market Manager, Indiana Provider Relations Candace.Ervin@Envolvehealth.com October 18, 2017 1 Today s Agenda MHS ID Card Samples Provider Visits D1110 (Prophylaxis
Managed Health Services (MHS) Candace V. Ervin Market Manager, Indiana Provider Relations Candace.Ervin@Envolvehealth.com October 18, 2017 1 Today s Agenda MHS ID Card Samples Provider Visits D1110 (Prophylaxis
2017 Medicare Part D Formulary Change
 2017 Medicare Part D Formulary Change We may add or remove drugs from our formulary during the year. If we remove drugs from our formulary, or add prior authorizations, quantity limits and/or step therapy
2017 Medicare Part D Formulary Change We may add or remove drugs from our formulary during the year. If we remove drugs from our formulary, or add prior authorizations, quantity limits and/or step therapy
2018 Medicare Part D Formulary Change
 2018 Medicare Part D Formulary Change We may add or remove drugs from our formulary during the year. If we remove drugs from our formulary, or add prior authorizations, quantity limits and/or step therapy
2018 Medicare Part D Formulary Change We may add or remove drugs from our formulary during the year. If we remove drugs from our formulary, or add prior authorizations, quantity limits and/or step therapy
2017 Medicare Part D Formulary Change
 2017 Medicare Part D Formulary Change We may add or remove drugs from our formulary during the year. If we remove drugs from our formulary, or add prior authorizations, quantity limits and/or step therapy
2017 Medicare Part D Formulary Change We may add or remove drugs from our formulary during the year. If we remove drugs from our formulary, or add prior authorizations, quantity limits and/or step therapy
iappeals Screens for the final PSA (May 24) 5
 5") iappeals Screens for the final PSA (May 24) 5 Welcome! This is the starting point to request a review of our medical decision about your eligibility for disability benefits. There are two parts to this
iappeals Screens for the final PSA (May 24) 5 Welcome! This is the starting point to request a review of our medical decision about your eligibility for disability benefits. There are two parts to this
Clinical Policy: Dupilumab (Dupixent) Reference Number: ERX.SPA.49 Effective Date:
 Reference Number: ERX.SPA.49 Effective Date:") Clinical Policy: (Dupixent) Reference Number: ERX.SPA.49 Effective Date: 06.01.17 Last Review Date: 02.19 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Dupixent) Reference Number: ERX.SPA.49 Effective Date: 06.01.17 Last Review Date: 02.19 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
SASKATCHEWAN FORMULARY COMMITTEE BULLETIN UPDATE TO THE 54th EDITION
 Saskatchewan Health Drug Plan and Extended Benefits Branch January 2005 Bulletin #101 ISSN 0708-3246 SASKATCHEWAN FORMULARY COMMITTEE BULLETIN UPDATE TO THE 54th EDITION NEW FULL FORMULARY LISTING: The
Saskatchewan Health Drug Plan and Extended Benefits Branch January 2005 Bulletin #101 ISSN 0708-3246 SASKATCHEWAN FORMULARY COMMITTEE BULLETIN UPDATE TO THE 54th EDITION NEW FULL FORMULARY LISTING: The
Additional drug coverage
 Additional drug coverage Bonus Drug List Your plan sponsor (employer, union or trust) offers a bonus drug list. The prescription drugs on this list are covered in addition to the drugs on the plan s drug
Additional drug coverage Bonus Drug List Your plan sponsor (employer, union or trust) offers a bonus drug list. The prescription drugs on this list are covered in addition to the drugs on the plan s drug
Blue Cross and Blue Shield of New Mexico and Lovelace Health Plan Transactions Frequently Asked Questions
 Blue Cross and Blue Shield of New Mexico and Lovelace Health Plan Transactions Frequently Asked Questions Blue Cross and Blue Shield of New Mexico (BCBSNM), has received regulatory approval to acquire
Blue Cross and Blue Shield of New Mexico and Lovelace Health Plan Transactions Frequently Asked Questions Blue Cross and Blue Shield of New Mexico (BCBSNM), has received regulatory approval to acquire
STEP THERAPY CRITERIA
 STEP THERAPY This is a complete list of drugs that have written coverage determination policies. Drugs on this list do not indicate that this particular drug will be covered under your medical or prescription
STEP THERAPY This is a complete list of drugs that have written coverage determination policies. Drugs on this list do not indicate that this particular drug will be covered under your medical or prescription
Combined Chiropractic and Acupuncture Services Amendment of the Kaiser Foundation Health Plan, Inc., Evidence of Coverage for SAMPLE GROUP AGREEMENT
 EOC #6 - Kaiser Foundation Health Plan, Inc. Southern California Region Combined Chiropractic and Acupuncture Services Amendment of the Kaiser Foundation Health Plan, Inc., Evidence of Coverage for SAMPLE
EOC #6 - Kaiser Foundation Health Plan, Inc. Southern California Region Combined Chiropractic and Acupuncture Services Amendment of the Kaiser Foundation Health Plan, Inc., Evidence of Coverage for SAMPLE
2018 Medicare Part D Formulary Change
 2018 Medicare Part D Formulary Change We may add or remove drugs from our formulary during the year. If we remove drugs from our formulary, or add prior authorizations, quantity limits and/or step therapy
2018 Medicare Part D Formulary Change We may add or remove drugs from our formulary during the year. If we remove drugs from our formulary, or add prior authorizations, quantity limits and/or step therapy
Medication Therapy Management program
 Medication Therapy Management program Your one-on-one review of your medicines Be safe Feel good Save money Safe and sound never felt so good Get the most from your medicine therapy with a personal medicine
Medication Therapy Management program Your one-on-one review of your medicines Be safe Feel good Save money Safe and sound never felt so good Get the most from your medicine therapy with a personal medicine
BlueLink TPA FlexRx Updates
 BlueLink TPA FlexRx Updates April 2018 TRADE NAME (generic name) or generic name abacavir sulfate soln 20 mg/ml (base equiv) Generic Addition, generic for ZIAGEN alclometasone dipropionate cream 0.05%
BlueLink TPA FlexRx Updates April 2018 TRADE NAME (generic name) or generic name abacavir sulfate soln 20 mg/ml (base equiv) Generic Addition, generic for ZIAGEN alclometasone dipropionate cream 0.05%
HMO INSERT TO 2019 EVIDENCE OF COVERAGE
 Optima Medicare HMO INSERT TO 2019 EVIDENCE OF COVERAGE Chapter 4, Section 2.2 on Extra optional supplemental benefits you can buy Dental Optional Supplemental Benefits Optima Medicare offers some extra
Optima Medicare HMO INSERT TO 2019 EVIDENCE OF COVERAGE Chapter 4, Section 2.2 on Extra optional supplemental benefits you can buy Dental Optional Supplemental Benefits Optima Medicare offers some extra
Updates to your prescription benefits
 Updates to your prescription benefits Effective Jan. 1, 2019 Traditional Three-Tier PDL Update Summary Within the Prescription Drug List (PDL), medications are grouped by tier. The tier indicates the amount
Updates to your prescription benefits Effective Jan. 1, 2019 Traditional Three-Tier PDL Update Summary Within the Prescription Drug List (PDL), medications are grouped by tier. The tier indicates the amount
2019 List of Covered Drugs
 2019 List of Covered Drugs Formulary ID: 19391 Version 10 Updated: 02/2019. If you have questions, please call First Choice VIP Care Plus at 1-888-978-0862 (TTY 711), seven days a week, 8 a.m. to 8 p.m.
2019 List of Covered Drugs Formulary ID: 19391 Version 10 Updated: 02/2019. If you have questions, please call First Choice VIP Care Plus at 1-888-978-0862 (TTY 711), seven days a week, 8 a.m. to 8 p.m.
Information for Service Providers
 Information for Service Providers Introduction Advocacy is about helping people speak up about what is important to them in all aspects of their life. It can be carried out by anyone a person wants to
Information for Service Providers Introduction Advocacy is about helping people speak up about what is important to them in all aspects of their life. It can be carried out by anyone a person wants to
Additional Drug Coverage
 Additional Drug Coverage Additional prescription drug coverage Your plan includes extra coverage for certain supplies as shown below. These supplies are either not generally covered under Medicare Part
Additional Drug Coverage Additional prescription drug coverage Your plan includes extra coverage for certain supplies as shown below. These supplies are either not generally covered under Medicare Part