Pulmonary Function and Flow Volume Loop Patterns in Patients with. *Adnan Majid, MD ¹, FCCP *Andres F.
|
|
|
- Hester Goodman
- 6 years ago
- Views:
Transcription
1 Pulmonary Function and Flow Volume Loop Patterns in Patients with Tracheobronchomalacia. *Adnan Majid, MD ¹, FCCP *Andres F. Sosa, MD² Armin Ernst, MD 4, FCCP David Feller-Kopman, MD 5 (dfellerk@jhmi.edu); Erik Folch,(efolch@bidmc.harvard.edu); Anup Singh MD ¹, (asingh@unityhealth.org) ; Sidhu Gangadharan, MD¹ (sgangadh@bidmc.harvard.edu) ¹Chest Disease Center, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA ²Division of Pulmonary, Allergy and Critical Care Medicine, University of Massachusetts Medical School, Worcester, MA 4 Division of Pulmonary, Critical Care and Sleep Medicine, St Elizabeth s Hospital, Boston, MA 5 Interventional Pulmonology, Johns Hopkins Hospital, Baltimore, MD Corresponding author: Adnan Majid, MD, FCCP (amajid@bidmc.harvard.edu) Institution where study was performed: Beth Israel Deaconess Medical Center, Boston, MA Dr. Majid has no conflicts of interest to disclose; Dr. Sosa has no conflicts of interest to disclose; Dr. Ernst has no conflicts of interest to disclose; Dr. Feller-Kopman has no conflicts of interest to disclose; Dr. Folch has no conflicts of interest to disclose; Dr. Anup Singh has no conflicts of interest to disclose; Dr. Gangadharan has no conflicts of interest to disclose.
2 *Both authors contributed equally to planning, data collection, data analysis and writing of the manuscript. Abbreviations: PFTs= Pulmonary function tests FVLs= Flow volume loops TBM= tracheobronchomalacia FEFmax= maximal forced expiratory flow CT= Computed Tomography GOLD= Global Obstructive Lung Disease initiative TLC= Total Lung Capacity ATS= American Thoracic Society BMI= Body Mass Index FEV1= Forced expiratory volume in first second FVC= Forced Volume capacity
3 Abstract BACKGROUND: Patterns of pulmonary function tests (PFTs) and flow-volume loops (FVLs) among patients with clinically significant tracheobronchomalacia (TBM) are not well described. Small studies suggest four main FVL morphologies: low maximal forced expiratory flow (FEFmax), biphasic expiratory curve, flow oscillations and notching. OBJECTIVE: To describe common pulmonary function test (PFT) and FVL patterns among the largest prospective series of patients to date undergoing clinical evaluation for symptomatic moderate to severe TBM. METHODS: We conducted a retrospective analysis of prospectively collected data from patients who were referred to the Chest Disease Center from January 2002 to December 2008 with respiratory symptoms that were attributed primarily to TBM. PFT results of 90 patients with symptomatic moderate to severe TBM were evaluated. RESULTS: By PFTs, 40 (44.4%) patients had an obstructive ventilatory defect, 16 (17.8%) had a definite or highly likely restrictive ventilatory defect, 15 (16.7%) had a mixed defect, and 19 (21.1%) were within normal limits. Among 76 patients with available FVLs, the most frequent finding was low FEFmax in 62 (81.6%) cases, followed by biphasic morphology 15 (19.7%), notched expiratory loop 7 (9.2%) and expiratory oscillations 2 (2.6%).The balance of 13 patients (17.1%) had no distinctive FVL abnormality. CONCLUSION: PFTs and FVLs are normal in a significant number of patients with moderate to severe TBM and should not be used to decide whether tracheobronchomalacia is present or clinically significant.
4 Introduction Tracheobronchomalacia (TBM) is an increasingly recognized condition associated with hypercompliant central airways. 1,2,3 While the pathogenesis of diffuse TBM is often not known, it frequently occurs in patients with chronic airway inflammation. 1,2 TBM has been identified in 1 to 4.5% of all patients undergoing bronchoscopy, 23% of patients with chronic bronchitis undergoing bronchoscopy, and 14.1% of patients with chronic cough. 4-7 The most frequent presenting signs and symptoms include dyspnea on exertion, intractable cough, orthopnea, mucostasis and recurrent infections. 2,4,8,9 The diagnosis of TBM may be challenging, as patients often have other chronic pulmonary conditions such as asthma or COPD that may explain their symptoms. Formal diagnosis can be made with dynamic flexible bronchoscopy (Image 1) and dynamic airway computed tomography (CT) (Image 2). 2,3 However, most patients will have pulmonary function tests (PFTs) as part of the initial work up for their presenting symptoms. While some characteristic PFT and FVL patterns have been described in patients with TBM, the prevalence and diagnostic utility of these patterns have not been determined in a large, well defined, cohort of patients. 2-4 With increased awareness of TBM as an independent cause of clinical symptoms and functional impairment, the need for a standard diagnostic workup becomes more important. This is especially true in light of effective available therapies, such as airway stenting, tracheoplastic
5 surgery and continuous positive airway pressure Therefore, the role of PFTs in the initial evaluation of TBM needs to be better defined. Our objective is to describe the most common PFT and FVL patterns in a large series of patients undergoing evaluation for symptomatic moderate to severe diffuse TBM. Materials and Methods This protocol was approved by the Institutional Review Board, Committee on Clinical Investigation at Beth Israel Deaconess Medical Center (research protocol #2005P ), and all patients undergoing evaluation for symptomatic TBM were asked to provide informed consent to become a part of the TBM database for future publications. We conducted a retrospective analysis of prospectively collected data from patients who were referred to the Chest Disease Center from January 2002 to December 2008 with respiratory symptoms that were attributed primarily to TBM. These patients are referred to our center by primary care physicians, pulmonologists and thoracic surgeons from around the country for further evaluation and treatment of suspected TBM. All patients with baseline PFTs prior to any airway intervention were included. Exclusion criteria included a prior airway intervention and mild or no TBM. Moderate to severe TBM was defined as more than 75% collapse of the airway lumen anywhere along the trachea, mainstem bronchi and bronchus intermedius on forced expiration during a dynamic flexible bronchoscopy. Age, sex, comorbidities, and respiratory symptoms were also recorded. Dynamic flexible bronchoscopies were performed under light sedation and topical anesthesia. 2,8,9 The bronchoscope was advanced into the proximal trachea and the patient was instructed to
6 forcefully inhale and exhale. This sequence was repeated at the mid- trachea, distal trachea, proximal to the ostium of both mainstem bronchi and bronchus intermedius. The procedure was video recorded in order to generate airway images for subsequent quantitative analysis. PFTs were all performed using NSpire equipment (NSpire Health- LLC, Louisville,CO). The equipment meets ATS standards and follows daily calibration. All maneuvers were done ensuring proper patient effort and reproducibility. Spirometry, lung volumes, and diffusing capacity for carbon monoxide (DLCO) were performed following the ATS guidelines All results were interpreted by a board certified pulmonologist. Statistical Analysis The study is descriptive and results are expressed as frequencies, proportions, medians, means and standard deviations as appropriate. The program used was Microsoft Office Excel 2007 (Redmond, Washington, USA). Statistical analyses were performed by one of the study authors (AFS). Results At the time of data collection, 172 patients were referred for evaluation of symptomatic TBM. Ninety patients had both confirmed moderate to severe TBM, and baseline PFTs performed prior to any airway intervention. FVLs were available in 76 (84.4%) of those patients (Figure 1). Fifty-eight (33.7%) had moderate or severe TBM but were excluded due to prior airway interventions (i.e. T-tubes, tracheotomies, stents). Twenty-one patients (12.2%) who had mild TBM and three (1.7%) patients those did not have TBM were also excluded. The median age of patients in this sample was 65 years (31-95 years), 40 (44%) patients were men, and mean BMI was 30 (+/-6). Forty-three (47.8%) had been diagnosed with COPD, and 21
7 (23%) had been diagnosed with asthma (Tables 1-2). The most common presenting symptoms (Table 3) were dyspnea on exertion 71 (78.9%), severe chronic cough 63 (70%) and recurrent respiratory infections 48 (53.3%). By PFT, 40 of 90 patients (44.4%) had airflow obstruction (defined as FEV1 <80% and FEV1/FVC <70% of predicted), 16 (17.8%) had definite or highly likely restriction defined respectively as TLC <80% of predicted or, in the absence of TLC measurement, reduced FVC with normal FEV1/FVC ratio. 15 (16.7%) had a mixed defect, and 19 (21.1%) were within normal limits. PFT values are shown in table 1. Among patients with FVL (Table 4), the most frequent finding was a below predicted FEFmax in 62 (81.6%), followed by biphasic morphology in 15 (19.7%); this pattern showed a rapid peak and decline in expiratory flow followed by a prolonged plateau extending throughout most of the expiratory maneuver (Figure 1A). Notched expiratory loop was seen in 7 (9.2%) patients who showed a rapid mid-expiratory dip and return of flow without other indications of cough and that was reproducible in several maneuvers (Figure 1B); expiratory oscillations were documented in 2 (2.6%) patients and were characterized by reproducible large amplitude high frequency oscillations over much of the expiratory loop (Figure 1C).The balance of patients 13 (17.1%) had no distinctive abnormal FVL characteristics. These findings were not mutually exclusive, and a below normal FEFmax was also present in the other three patterns. Lung volumes and DLCO were obtained in 63 patients. The mean percent predicted total lung capacity (TLC) was 86.8 (+/-17.7), residual volume (RV) was 105 (+/- 35.5), and RV/TLC was 119 (+/- 32.7). The mean percent predicted DLCO was 70.4 (+/-28.3). The spirometric values from the groups with and without lung volumes did not differ significantly.
8 Discussion In this large series of patients with symptomatic moderate to severe diffuse TBM, we found that pulmonary function tests demonstrate no characteristic and/or common pattern that would help to screen patients during an initial diagnostic workup. Although a substantial number of patients were unable to achieve predicted FEFmax (81.6%), this index does not seem reliable, especially in light of almost 20% of patients showing normal values. The biphasic morphology is also characterized by a low FEF max which is followed by a rapid fall in flow resulting in a plateau of very low flow for the remainder of exhalation. This pattern was described in 8 of 11 patients with TBM in an observational study by Campbell and Faulks. 15 Gandevia 16 also described in 10 patients with emphysema and TBM an initial phase of rapidly exhaled gas, followed by a linear phase of constant, slow flow. Nuutinen et al and Wyss have described a notch in the expiratory limb of the FVL as typical of TBM. 5, 17.The notch was thought to be due to sudden decrease of flow with airway collapse. Their findings contrast with those of the current study, where only 7 (9.2%) patients showed this particular finding. Campbell and Faulks thought that this finding was likely an artifact caused by the water filled spirometer. 15 Reinert and Steurich were unable to correlate this pattern with central bronchial collapse. 18 The finding of reproducible notching in only 7 patients in our study suggests that this does not seem to be a particularly reliable indicator of TBM. Rapid flow oscillations have been defined by Vincken and Cosio as a reproducible sequence of alternating accelerations and decelerations of flow, creating a saw-tooth pattern superimposed on the general contour of the flow-volume loop produced by the awake subject. 19 This pattern can be explained by the fact that rapid changes in either driving pressure or airway resistance, can
9 occur during inspiration and expiration, and have a characteristic frequency of 4-60Hz. These oscillations have been described in different structural or functional disorders of the upper airways including obstructive sleep apnea and neuromuscular disorders (i.e. essential tremor, Parkinson s, Shy-Drager). 19 Garcia-Pachon described oscillations in a patient with TBM. 20 However, in the present study, oscillations were noted in the expiratory curve of only 2 (2.6%) patients. Although the observed frequency is roughly almost twice that described in the general population, it is still quite infrequent. 19 Interestingly, 17.1 % of patients in our series had a normal flow volume loop. This suggests that compression of the central airways due to TBM is not necessarily the cause of airflow obstruction and that expiratory flow limitation occurs in more peripheral airways. This finding is supported by Loring et al., who described airway pressure-area characteristics by relating airway narrowing to the pressure differences measured across the central airway wall during graded expiratory efforts. 21 They concluded that central airway collapse did not correlate with the degree of obstruction assessed by FEV1 and could be seen irrespective of the degree of expiratory flow limitation. Samad et al., found no correlation between degree of airflow obstruction and tracheobronchial collapse during cough. 22 Reinert and Steurich also found no strong correlations between central airway collapse and lung function parameters in 30 unselected male patients. 18 Consistent with this observation, previous studies have shown that clinical improvement after central airway stabilization is not always associated with an increase in FEV1. 8, 9 The low mean DLCO seen in our study is likely explained by the high prevalence of parenchymal lung disease in this patient population. It is possible that patients with emphysema
10 may also have a greater tendency for expiratory central airway collapse due to loss of elastic recoil with reduced airway tethering. It is conceivable that sequelae from copious airway secretions, mucous plugging and from recurrent infections as seen in TBM may lower the diffusing capacity in the absence of primary parenchymal lung disease. We did not find other studies that explore the relationship between diffusing capacity and TBM. An important limitation in the present study includes the absence of a control group, the entire population of patients included had moderate to severe TBM. We therefore cannot assess the specificity of various PFT abnormalities that may predict the presence of TBM. However, there were a significant number of patients with normal PFTs. Since this finding alone allows some speculation to suggest poor sensitivity, one could make an argument that PFTs are not a precise screening tool for the presence of moderate to severe TBM. It is also important to mention that many healthy subjects have a forced expiratory collapse > 75%, so the finding of TBM may not have been pathologic in part of our sample population. 23 Conclusions Pulmonary function tests are often used in the evaluation of patients with symptomatic TBM. Although some characteristic patterns in the expiratory limb of the flow volume loop have been described, these seem unreliable for the diagnosis of TBM. Of particular interest, a significant percentage of these patients may have normal PFTs. This suggests that a diagnosis of TBM should not be ruled out in the setting of persistent symptoms with normal PFTs. At the same time, it is important to keep in mind that forced expiratory collapse exceeding what is currently viewed as normal, may not be a pathologic finding. 23, 24 Based on our findings, the workup of
11 TBM should rely on dynamic airway CTs or bronchoscopy and normal PFTs should not drive one away from pursuing this diagnosis. Acknowledgements: Dr. Majid: contributed to the conception, planning, data collection, data analysis and writing of the manuscript and takes responsibility for the integrity of the work as a whole, from incepton to published article. Dr. Sosa: contributed to the planning, data collection, data analysis and writing of the For Peer Review manuscript and takes responsibility for the integrity of the work as a whole, from incepton to published article. Dr. Ernst: contributed to the planning, data collection, and manuscript review. Dr. Feller-Kopman: contributed to manuscript review. Dr. Folch: contributed manuscript review. Dr. Anup Singh: contributed to manuscript review. Dr. Gangadharan: contributed to manuscript review. Other contributions: We thank Dr. Rabih Bechara, Dr. Arthur Sung, Dr. Jed Gorden, Dr. Chakravarty Reddy, Dr. Saleh Alazemi, Dr. David Berkowitz, Dr. Dilip Nataraj, Dr. Samaan Rafeq and Dr. Archan Shah for help in gathering the data.
12 References 1. Feist JH, Johnson TH, Wilson RJ. Acquired tracheomalacia: etiology and differential diagnosis. Chest 1975;68(3): Carden KA, Boiselle PM, Waltz DA, Ernst A. Tracheomalacia and Tracheobronchomalacia in Children and Adults. An In-Depth Review. Chest 2005;127(3): Murgu SD, Colt HG. Tracheobronchomalacia and excessive dynamic airway collapse For Peer Review Respirology 2006;11(4): Majid A, Fernandez L, Fernandez-Bussy S, Herth F, Ernst A. Tracheomalacia. Arch Bronconeumol.2010;46(4): Nuutinen J. Acquired tracheobronchomalacia. A clinical study with bronchological correlations. Ann. Clin. Res. 1977;9(6): Jokinen k, Palva T, Nuutinen J. Chronic bronchitis: a bronchologic evaluation. J Otorhinolaryngol Relat Spec 1976;38(3): Palombini BC, Villanova CA, Araujo E, Gastal OL, Alt DC, Stolz DP et al. A pathogenic triad in chronic cough: asthma, post nasal drip, and gastroesophageal reflux disease. Chest 1999;116(6): Ernst A, Majid A, Feller-Kopman D, Guerrero J, Boiselle P, Loring SH et al. Airway stabilization with silicone stents for treating adult tracheobronchomalacia: a prospective observational study. Chest 2007;132(2):
13 9. Majid, A, Guerrero J, Gangadharan S, Feller-Kopman D, Boiselle P, DeCamp M et al. Tracheobronchoplasty for Severe tracheobronchomalacia: A Prospective Outcome Analysis. Chest 2008;134(4): Ferguson GT, Benoist J. Nasal continuous positive airway pressure in the treatment of tracheobronchomalacia. Am Rev Respir Dis1993;147(2): Miller MR, Crapo R, Hankinson J, Brusasco V, Burgos F, Casaburi R et al. General considerations for lung function testing. Eur Respir J 2005;26(1): For Peer Review 12. Wanger J, Clausen JL, Coates A, Pedersen OF, Brusasco V, Burgos F et al. Standardization of the measurement of lung volumes. Eur Respir J 2005;26(3): Macintyre N, Crapo RO, Viegi G, Johnson DC, van der Grinten CP, Brusasco V et al. Standardisation of the single-breath determination of carbon monoxide uptake in the lung. Eur Respir J 2005;26(4): Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A et al. Standardization of Lung Function Testing. Standardisation of spirometry. Eur Respir J 2005;26(2): Campbell AH, Faulks LW. Expiratory air-flow pattern in tracheobronchial collapse. Am Rev Respir Dis 1965;92(5): Gandevia B. The spirogram of gross expiratory tracheobronchial collapse in emphysema. Q J Med 1963;32: Koblet H, Wyss F. Clinical and functional picture of genuine bronchial collapse with lung emphysema. Helv Med Acta 1956;23(4-5): Reinert M, Steurich F. Correlation between lung function and tracheobronchial collapse. Respiration 1976;33(1):47 53.
14 19. Vincken W, Cosio M. Flow oscillations on the flow-volume loop: clinical and physiological implications. Eur Respir J 1989;2(6): Garcia-Pachon E. Tracheobronchomalacia: a cause of flow oscillations on the flowvolume loop. Chest 2000;118(5): Loring SH, O Donnell, CR, Feller-Kopman DJ, Ernst A. Central Airway Mechanics and Flow Limitation in Acquired Tracheobronchomalacia. Chest 2007;131(4): Samad IA, Sanders DE, Suero JT, Woolf CR. The relationship between tracheobronchial collapse and pulmonary function in chronic obstructive pulmonary disease. Dis Chest 1968;53(4): Boiselle PM, O'Donnell CR, Bankier AA, Ernst A, Millet ME, Potemkin A et al. Tracheal Collapsibility in Healthy Volunteers during Forced Expiration: Assessment with Multidetector CT. Radiology 2009;252(1): Litmanovich D, O'Donnell CR, Bankier AA, Ernst A, Millett ME, Loring SH et al. Bronchial Collapsibility in Healthy Volunteers at Forced Expiration: Assessment with Multidetector-row CT. Radiology. 2010;257(2):
15 Table 1. Patient Demographics and PFTs Variables Mean(SD) Median Age (years) 64.34(13) 65 BMI (Kg/meter2) 30.67(5.79) 30 FEV1 (Liter) 1.55(0.8) 1.37 % of Predicted values 61.7(27.59) 61.5 FVC (Liter) 2.42(1.04) 2.26 % of Predicted values 68.51(21.85) 65.5 FEV1/FVC% 63.2(16.36) 66 TLC (liter) (n=63) 4.85(1.38) 4.62 % of Predicted values 86.84(17.71) 89 RV(liter) (n=63) 2.1(0.76) 1.97 % of Predicted values 105(35.46) 99 IC(Liter) 2.3(0.87) 2.13 % of Predicted values 94(26.7) 95 RV/TLC(Liter)(n=63) 44(11.93) 44 % of Predicted values (32.72) 113 DLCO (ml CO/min/mm Hg ) (n=63) 15.72(7.4) % of Predicted values 70.46(28.31) 66 Table 2. Accompanying Diagnosis in Patients with Moderate to Severe Diffuse TBM Diagnosis Total(%) COPD 43(47.78) Asthma 21(23.33) OSA 24(26.66) ILD 2(2.22) GERD 40(44.44) Bronchiectasis 4(4.44) Mounier-Kuhn 2(2.22) Relapsing polychondritis 3(3.33) None 4(4.44) Other 12(13.33) 11 12
16 Table 3. Presenting Symptoms and history in Patients with Moderate to Severe Diffuse TBM Presenting Symptoms and History Total(%) Inability to Clear secretions 9(10) Recurrent Infections 48(53.33) Severe Cough 63(70) Fatigue 1(1.11) SOB/DOE 71(78.88) Choking 4(4.44) Wheezing 7(7.77) Stridor 1(1.11) Respiratory Failure 4(4.44) Sputum production 4(4.44) OTHER 3(3.33) Prior Intubation 1(1.11) Table 4. FVL Morphology in Patients with Moderate to Severe Diffuse TBM FVL Total(%) Low Peak (FEFmax) 62(81.6) Biphasic 15(19.73) Notching 7(9.2) Oscillations 2(2.6) Normal 13(17.1) 26


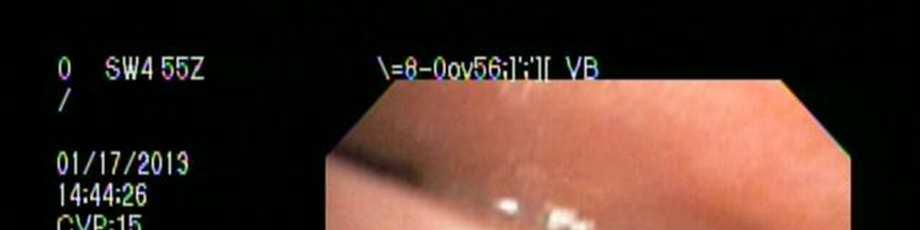


17 Image 1: Dynamic Flexible Bronchoscopy (a) Forced Inhalation (b) Forced Exhalation

")
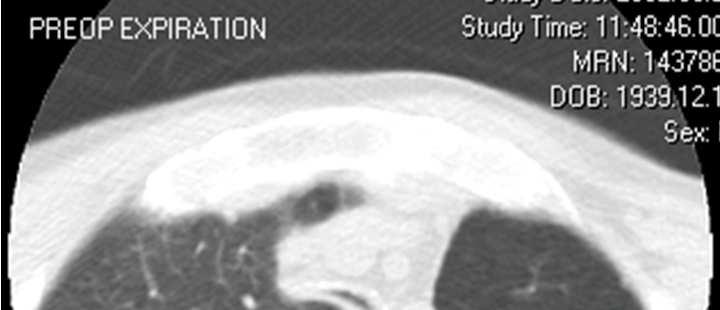
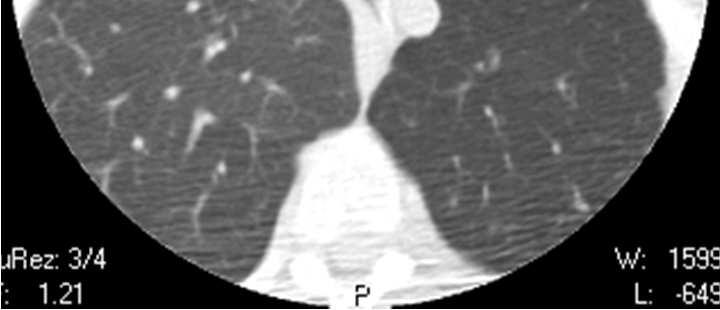
18 Image 2. Dynamic Airway CT (a) Forced Inhalation (b) Forced Exhalation
19 Figure 1. Flow Volume Loop Morphology (a) Biphasic morphology (b) Notched expiratory loop (c) Oscillations
Airway stenting in excessive central airway collapse
 Review Article on Aerodigestive Endoscopy Airway stenting in excessive central airway collapse Mihir Parikh, Jennifer Wilson, Adnan Majid, Sidhu Contributions: (I) Conception and design: All authors; (II)
Review Article on Aerodigestive Endoscopy Airway stenting in excessive central airway collapse Mihir Parikh, Jennifer Wilson, Adnan Majid, Sidhu Contributions: (I) Conception and design: All authors; (II)
Tracheal collapse diagnosed by multidetector computed tomography: evaluation of different image analysis methods
 Syddansk Universitet Tracheal collapse diagnosed by multidetector computed tomography: evaluation of different image analysis methods Nygaard, Mette; Bendstrup, Elisabeth; Dahl, Ronald; Hilberg, Ole; Rasmussen,
Syddansk Universitet Tracheal collapse diagnosed by multidetector computed tomography: evaluation of different image analysis methods Nygaard, Mette; Bendstrup, Elisabeth; Dahl, Ronald; Hilberg, Ole; Rasmussen,
Prevalence of tracheobronchomalacia and excessive dynamic airway collapse in bronchial asthma of different severity
 Dal Negro et al. Multidisciplinary Respiratory Medicine 2013, 8:32 ORIGINAL RESEARCH ARTICLE Prevalence of tracheobronchomalacia and excessive dynamic airway collapse in bronchial asthma of different severity
Dal Negro et al. Multidisciplinary Respiratory Medicine 2013, 8:32 ORIGINAL RESEARCH ARTICLE Prevalence of tracheobronchomalacia and excessive dynamic airway collapse in bronchial asthma of different severity
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Case Report Tracheomalacia Treatment Using a Large-Diameter, Custom-Made Airway Stent in a Case with Mounier-Kuhn Syndrome
 Case Reports in Pulmonology, Article ID 910135, 4 pages http://dx.doi.org/10.1155/2014/910135 Case Report Tracheomalacia Treatment Using a Large-Diameter, Custom-Made Airway Stent in a Case with Mounier-Kuhn
Case Reports in Pulmonology, Article ID 910135, 4 pages http://dx.doi.org/10.1155/2014/910135 Case Report Tracheomalacia Treatment Using a Large-Diameter, Custom-Made Airway Stent in a Case with Mounier-Kuhn
Accepted Manuscript. Robotic tracheobronchoplasty is feasible but which patients truly benefit? Steven Milman, MD, Thomas Ng, MD
 Accepted Manuscript Robotic tracheobronchoplasty is feasible but which patients truly benefit? Steven Milman, MD, Thomas Ng, MD PII: S0022-5223(18)32271-2 DOI: 10.1016/j.jtcvs.2018.08.028 Reference: YMTC
Accepted Manuscript Robotic tracheobronchoplasty is feasible but which patients truly benefit? Steven Milman, MD, Thomas Ng, MD PII: S0022-5223(18)32271-2 DOI: 10.1016/j.jtcvs.2018.08.028 Reference: YMTC
Pulmonary Function Testing. Ramez Sunna MD, FCCP
 Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects
 Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC Benefits and Limitations of Pulmonary Function Testing Benefits
Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC Benefits and Limitations of Pulmonary Function Testing Benefits
Pulmonary Function Testing
 In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
Spirometric protocol
 Spirometric protocol Spirometry is the most common of the Pulmonary Function Test, that measures lung function, specifically the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled.
Spirometric protocol Spirometry is the most common of the Pulmonary Function Test, that measures lung function, specifically the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled.
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Basic approach to PFT interpretation. Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic
 Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
PULMONARY FUNCTION TESTS
 Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
PFT Interpretation and Reference Values
 PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
Exercise-associated Excessive Dynamic Airway Collapse in Military Personnel
 Exercise-associated Excessive Dynamic Airway Collapse in Military Personnel Daniel J. Weinstein 1, James E. Hull 2, Brittany L. Ritchie 3, Jackie A. Hayes 2, and Michael J. Morris 2 1 Internal Medicine
Exercise-associated Excessive Dynamic Airway Collapse in Military Personnel Daniel J. Weinstein 1, James E. Hull 2, Brittany L. Ritchie 3, Jackie A. Hayes 2, and Michael J. Morris 2 1 Internal Medicine
Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology
 Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
Pulmonary Function Testing The Basics of Interpretation
 Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Whistling in the Dark
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e clinical problem-solving Whistling in the Dark Daniel A. Solomon, M.D., Christopher H. Fanta, M.D., Bruce D. Levy, M.D., and Joseph Loscalzo, M.D.,
T h e n e w e ngl a nd j o u r na l o f m e dic i n e clinical problem-solving Whistling in the Dark Daniel A. Solomon, M.D., Christopher H. Fanta, M.D., Bruce D. Levy, M.D., and Joseph Loscalzo, M.D.,
6- Lung Volumes and Pulmonary Function Tests
 6- Lung Volumes and Pulmonary Function Tests s (PFTs) are noninvasive diagnostic tests that provide measurable feedback about the function of the lungs. By assessing lung volumes, capacities, rates of
6- Lung Volumes and Pulmonary Function Tests s (PFTs) are noninvasive diagnostic tests that provide measurable feedback about the function of the lungs. By assessing lung volumes, capacities, rates of
Chronic Cough. Abhishek Kumar, MD, MPH Pulmonary and Critical Care Mercy Medical Center, Cedar Rapids, IA
 Chronic Cough Abhishek Kumar, MD, MPH Pulmonary and Critical Care Mercy Medical Center, Cedar Rapids, IA What we shall discuss? Cough anatomy and pathophysiology Common etiologies Work-up Role of spirometry/pulmonary
Chronic Cough Abhishek Kumar, MD, MPH Pulmonary and Critical Care Mercy Medical Center, Cedar Rapids, IA What we shall discuss? Cough anatomy and pathophysiology Common etiologies Work-up Role of spirometry/pulmonary
S P I R O M E T R Y. Objectives. Objectives 2/5/2019
 S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
PFTs ACOI Board Review 2018
 PFTs ACOI Board Review 2018 Thomas F. Morley, DO, MACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary, Critical Care and Sleep Medicine
PFTs ACOI Board Review 2018 Thomas F. Morley, DO, MACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary, Critical Care and Sleep Medicine
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
Spirometry. Obstruction. By Helen Grim M.S. RRT. loop will have concave appearance. Flows decreased consistent with degree of obstruction.
 1 2 Spirometry By Helen Grim M.S. RRT 3 4 Obstruction loop will have concave appearance. Flows decreased consistent with degree of obstruction. Volumes may be normal, but can decrease with severity of
1 2 Spirometry By Helen Grim M.S. RRT 3 4 Obstruction loop will have concave appearance. Flows decreased consistent with degree of obstruction. Volumes may be normal, but can decrease with severity of
CIRCULAR INSTRUCTION REGARDING ESTABLISHMENT OF IMPAIRMENT DUE TO OCCUPATIONAL LUNG DISEASE FOR THE PURPOSES OF AWARDING PERMANENT DISABLEMENT
 Circular Instruction 195 CIRCULAR INSTRUCTION REGARDING ESTABLISHMENT OF IMPAIRMENT DUE TO OCCUPATIONAL LUNG DISEASE FOR THE PURPOSES OF AWARDING PERMANENT DISABLEMENT COMPENSATION FOR OCCUPATIONAL INJURIES
Circular Instruction 195 CIRCULAR INSTRUCTION REGARDING ESTABLISHMENT OF IMPAIRMENT DUE TO OCCUPATIONAL LUNG DISEASE FOR THE PURPOSES OF AWARDING PERMANENT DISABLEMENT COMPENSATION FOR OCCUPATIONAL INJURIES
PULMONARY FUNCTION. VOLUMES AND CAPACITIES
 PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
Chapter 3. Pulmonary Function Study Assessments. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 3 Pulmonary Function Study Assessments 1 Introduction Pulmonary function studies are used to: Evaluate pulmonary causes of dyspnea Differentiate between obstructive and restrictive pulmonary disorders
Chapter 3 Pulmonary Function Study Assessments 1 Introduction Pulmonary function studies are used to: Evaluate pulmonary causes of dyspnea Differentiate between obstructive and restrictive pulmonary disorders
Interventional Pulmonology
 Interventional Pulmonology The Division of Thoracic Surgery Department of Cardiothoracic Surgery New York Presbyterian/Weill Cornell Medical College p: 212-746-6275 f: 212-746-8223 https://weillcornell.org/eshostak
Interventional Pulmonology The Division of Thoracic Surgery Department of Cardiothoracic Surgery New York Presbyterian/Weill Cornell Medical College p: 212-746-6275 f: 212-746-8223 https://weillcornell.org/eshostak
Difference Between The Slow Vital Capacity And Forced Vital Capacity: Predictor Of Hyperinflation In Patients With Airflow Obstruction
 ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 4 Number 2 Difference Between The Slow Vital Capacity And Forced Vital Capacity: Predictor Of Hyperinflation In Patients With Airflow Obstruction
ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 4 Number 2 Difference Between The Slow Vital Capacity And Forced Vital Capacity: Predictor Of Hyperinflation In Patients With Airflow Obstruction
S P I R O M E T R Y. Objectives. Objectives 3/12/2018
 S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
Outline FEF Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications?
 Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
A Primer on Reading Pulmonary Function Tests. Joshua Benditt, M.D.
 A Primer on Reading Pulmonary Function Tests Joshua Benditt, M.D. What Are Pulmonary Function Tests Used For? Pulmonary function testing provides a method for objectively assessing the function of the
A Primer on Reading Pulmonary Function Tests Joshua Benditt, M.D. What Are Pulmonary Function Tests Used For? Pulmonary function testing provides a method for objectively assessing the function of the
Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation. Susan Blonshine RRT, RPFT, AE-C, FAARC
 Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation Susan Blonshine RRT, RPFT, AE-C, FAARC Objectives Sample Title Recognize acceptable spirometry that meets the start
Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation Susan Blonshine RRT, RPFT, AE-C, FAARC Objectives Sample Title Recognize acceptable spirometry that meets the start
PULMONARY FUNCTION TESTING. Purposes of Pulmonary Tests. General Categories of Lung Diseases. Types of PF Tests
 PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
COMPREHENSIVE RESPIROMETRY
 INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
Coexistence of confirmed obstruction in spirometry and restriction in body plethysmography, e.g.: COPD + pulmonary fibrosis
 Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
UNIT TWO: OVERVIEW OF SPIROMETRY. A. Definition of Spirometry
 UNIT TWO: OVERVIEW OF SPIROMETRY A. Definition of Spirometry Spirometry is a medical screening test that measures various aspects of breathing and lung function. It is performed by using a spirometer,
UNIT TWO: OVERVIEW OF SPIROMETRY A. Definition of Spirometry Spirometry is a medical screening test that measures various aspects of breathing and lung function. It is performed by using a spirometer,
Int. J. Pharm. Sci. Rev. Res., 34(2), September October 2015; Article No. 24, Pages: Role of Spirometry in Diagnosis of Respiratory Diseases
, September October 2015; Article No. 24, Pages: Role of Spirometry in Diagnosis of Respiratory Diseases") Review Article Role of Spirometry in Diagnosis of Respiratory Diseases Dipti Mohapatra 1, Tapaswini Mishra 1, Manasi Behera 1, Nibedita Priyadarsini 1, Arati Mohanty 1, *Prakash Kumar Sasmal 2 1 Department
Review Article Role of Spirometry in Diagnosis of Respiratory Diseases Dipti Mohapatra 1, Tapaswini Mishra 1, Manasi Behera 1, Nibedita Priyadarsini 1, Arati Mohanty 1, *Prakash Kumar Sasmal 2 1 Department
Lung Pathophysiology & PFTs
 Interpretation of Pulmonary Function Tests (PFTs) Course # 1612 2:00 5:00pm Friday February 22, 2013 Lung Pathophysiology & PFTs Mark F. Sands MD, FCCP, FAAAAI Division of Allergy, Immunology & Rheumatology
Interpretation of Pulmonary Function Tests (PFTs) Course # 1612 2:00 5:00pm Friday February 22, 2013 Lung Pathophysiology & PFTs Mark F. Sands MD, FCCP, FAAAAI Division of Allergy, Immunology & Rheumatology
This is a cross-sectional analysis of the National Health and Nutrition Examination
 SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE
 The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene
 Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
behaviour are out of scope of the present review.
 explained about the test, a trial may be done before recording the results. The maneuver consists initially of normal tidal breathing. The subject then inhales to maximally fill the lungs. This is followed
explained about the test, a trial may be done before recording the results. The maneuver consists initially of normal tidal breathing. The subject then inhales to maximally fill the lungs. This is followed
Analysis of Lung Function
 Computer 21 Spirometry is a valuable tool for analyzing the flow rate of air passing into and out of the lungs. Flow rates vary over the course of a respiratory cycle (a single inspiration followed by
Computer 21 Spirometry is a valuable tool for analyzing the flow rate of air passing into and out of the lungs. Flow rates vary over the course of a respiratory cycle (a single inspiration followed by
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Mai ElMallah,MD Updates in Pediatric Pulmonary Care XII: An Interdisciplinary Program April 13, 2012
 Mai ElMallah,MD Updates in Pediatric Pulmonary Care XII: An Interdisciplinary Program April 13, 2012 Recognize the importance of Pulmonary Function Testing in Cystic Fibrosis Be aware of different types
Mai ElMallah,MD Updates in Pediatric Pulmonary Care XII: An Interdisciplinary Program April 13, 2012 Recognize the importance of Pulmonary Function Testing in Cystic Fibrosis Be aware of different types
Interpreting pulmonary function tests: Recognize the pattern, and the diagnosis will follow
 REVIEW FEYROUZ AL-ASHKAR, MD Department of General Internal Medicine, The Cleveland Clinic REENA MEHRA, MD Department of Pulmonary and Critical Care Medicine, University Hospitals, Cleveland PETER J. MAZZONE,
REVIEW FEYROUZ AL-ASHKAR, MD Department of General Internal Medicine, The Cleveland Clinic REENA MEHRA, MD Department of Pulmonary and Critical Care Medicine, University Hospitals, Cleveland PETER J. MAZZONE,
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
SPIROMETRY TECHNIQUE. Jim Reid New Zealand
 Jim Reid New Zealand The Basics Jim Reid Spirometry measures airflow and lung volumes, and is the preferred lung function test in COPD. By measuring reversibility of obstruction, it is also diagnostic
Jim Reid New Zealand The Basics Jim Reid Spirometry measures airflow and lung volumes, and is the preferred lung function test in COPD. By measuring reversibility of obstruction, it is also diagnostic
Pulmonary Function Tests. Mohammad Babai M.D Occupational Medicine Specialist
 Pulmonary Function Tests Mohammad Babai M.D Occupational Medicine Specialist www.drbabai.com Pulmonary Function Tests Pulmonary Function Tests: Spirometry Peak-Flow metry Bronchoprovocation Tests Body
Pulmonary Function Tests Mohammad Babai M.D Occupational Medicine Specialist www.drbabai.com Pulmonary Function Tests Pulmonary Function Tests: Spirometry Peak-Flow metry Bronchoprovocation Tests Body
Understanding the Basics of Spirometry It s not just about yelling blow
 Understanding the Basics of Spirometry It s not just about yelling blow Carl D. Mottram, RRT RPFT FAARC Technical Director - Pulmonary Function Labs and Rehabilitation Associate Professor of Medicine -
Understanding the Basics of Spirometry It s not just about yelling blow Carl D. Mottram, RRT RPFT FAARC Technical Director - Pulmonary Function Labs and Rehabilitation Associate Professor of Medicine -
LUNG FUNCTION TESTING: SPIROMETRY AND MORE
 LUNG FUNCTION TESTING: SPIROMETRY AND MORE OBJECTIVES 1. To describe other lung function testing for toddlers and those who cannot perform spirometry 2. To describe a lung function test on infants 3. To
LUNG FUNCTION TESTING: SPIROMETRY AND MORE OBJECTIVES 1. To describe other lung function testing for toddlers and those who cannot perform spirometry 2. To describe a lung function test on infants 3. To
SPIROMETRY. Marijke Currie (CRFS) Care Medical Ltd Phone: Copyright CARE Medical ltd
 Care Medical Ltd Phone: Copyright CARE Medical ltd") SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual can
SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual can
PULMONARY FUNCTION TEST(PFT)
") PULMONARY FUNCTION TEST(PFT) Objectives: By the end of the present lab, students should be able to: 1. Record lung volumes and capacities and compare them with those of a typical person of the same gender,
PULMONARY FUNCTION TEST(PFT) Objectives: By the end of the present lab, students should be able to: 1. Record lung volumes and capacities and compare them with those of a typical person of the same gender,
Assessment of Bronchodilator Response in Various Spirometric Patterns
 Original Article 2013 NRITLD, National Research Institute of Tuberculosis and Lung Disease, Iran ISSN: 1735-0344 TANAFFOS Assessment of Bronchodilator Response in Various Spirometric Patterns Amir Houshang
Original Article 2013 NRITLD, National Research Institute of Tuberculosis and Lung Disease, Iran ISSN: 1735-0344 TANAFFOS Assessment of Bronchodilator Response in Various Spirometric Patterns Amir Houshang
Triennial Pulmonary Workshop 2012
 Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Spirometry: an essential clinical measurement
 Shortness of breath THEME Spirometry: an essential clinical measurement BACKGROUND Respiratory disease is common and amenable to early detection and management in the primary care setting. Spirometric
Shortness of breath THEME Spirometry: an essential clinical measurement BACKGROUND Respiratory disease is common and amenable to early detection and management in the primary care setting. Spirometric
#8 - Respiratory System
 Page1 #8 - Objectives: Study the parts of the respiratory system Observe slides of the lung and trachea Equipment: Remember to bring photographic atlas. Figure 1. Structures of the respiratory system.
Page1 #8 - Objectives: Study the parts of the respiratory system Observe slides of the lung and trachea Equipment: Remember to bring photographic atlas. Figure 1. Structures of the respiratory system.
Content Indica c tion Lung v olumes e & Lung Indica c tions i n c paci c ties
 Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
A 31-year-old female with a rare cause of recurrent lower lobar collapses
 Radhika Banka, Dayle Terrington, Ajay V. Kamath radhika.banka@gmail.com Dept of Respiratory Medicine, Norfolk and Norwich University Hospital, Norwich, UK. A 31-year-old female with a rare cause of recurrent
Radhika Banka, Dayle Terrington, Ajay V. Kamath radhika.banka@gmail.com Dept of Respiratory Medicine, Norfolk and Norwich University Hospital, Norwich, UK. A 31-year-old female with a rare cause of recurrent
Lab 4: Respiratory Physiology and Pathophysiology
 Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
Office Based Spirometry
 Osteopathic Family Physician (2014)1, 14-18 Scott Klosterman, DO; Woodson Crenshaw, OMS4 Spartanburg Regional Family Medicine Residency Program; Edward Via College of Osteopathic Medicine - Virginia Campus
Osteopathic Family Physician (2014)1, 14-18 Scott Klosterman, DO; Woodson Crenshaw, OMS4 Spartanburg Regional Family Medicine Residency Program; Edward Via College of Osteopathic Medicine - Virginia Campus
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
SPIROMETRY METHOD. COR-MAN IN / EN Issue A, Rev INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark
 SPIROMETRY METHOD COR-MAN-0000-006-IN / EN Issue A, Rev. 2 2013-07 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
SPIROMETRY METHOD COR-MAN-0000-006-IN / EN Issue A, Rev. 2 2013-07 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
Impact of the new ATS/ERS pulmonary function test interpretation guidelines
 Respiratory Medicine (2007) 101, 2336 2342 Impact of the new ATS/ERS pulmonary function test interpretation guidelines Mary Elizabeth Kreider a,, Michael A. Grippi a,b a Division of Pulmonary, Allergy,
Respiratory Medicine (2007) 101, 2336 2342 Impact of the new ATS/ERS pulmonary function test interpretation guidelines Mary Elizabeth Kreider a,, Michael A. Grippi a,b a Division of Pulmonary, Allergy,
Expiratory central airway collapse in stable COPD and during exacerbations
 Leong et al. Respiratory Research (2017) 18:163 DOI 10.1186/s12931-017-0646-2 RESEARCH Expiratory central airway collapse in stable COPD and during exacerbations Paul Leong 1,2*, Anne Tran 1, Jhanavi Rangaswamy
Leong et al. Respiratory Research (2017) 18:163 DOI 10.1186/s12931-017-0646-2 RESEARCH Expiratory central airway collapse in stable COPD and during exacerbations Paul Leong 1,2*, Anne Tran 1, Jhanavi Rangaswamy
Clinical Study Bronchial Responsiveness in Patients with Restrictive Spirometry
 BioMed Research International Volume 2013, Article ID 498205, 5 pages http://dx.doi.org/10.1155/2013/498205 Clinical Study Bronchial Responsiveness in Patients with Restrictive Spirometry Jean I. Keddissi,
BioMed Research International Volume 2013, Article ID 498205, 5 pages http://dx.doi.org/10.1155/2013/498205 Clinical Study Bronchial Responsiveness in Patients with Restrictive Spirometry Jean I. Keddissi,
Pulmonary Function Testing
 Pulmonary Function Testing Let s catch our breath Eddie Needham, MD, FAAFP Program Director Emory Family Medicine Residency Program Learning Objectives The Astute Learner will: Become familiar with indications
Pulmonary Function Testing Let s catch our breath Eddie Needham, MD, FAAFP Program Director Emory Family Medicine Residency Program Learning Objectives The Astute Learner will: Become familiar with indications
Objectives. Pulmonary Assessment 12/13/2017
 Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
Importance of fractional exhaled nitric oxide in diagnosis of bronchiectasis accompanied with bronchial asthma
 Original Article Importance of fractional exhaled nitric oxide in diagnosis of bronchiectasis accompanied with bronchial asthma Feng-Jia Chen, Huai Liao, Xin-Yan Huang, Can-Mao Xie Department of Respiratory
Original Article Importance of fractional exhaled nitric oxide in diagnosis of bronchiectasis accompanied with bronchial asthma Feng-Jia Chen, Huai Liao, Xin-Yan Huang, Can-Mao Xie Department of Respiratory
Assessment of the Lung in Primary Care
 Assessment of the Lung in Primary Care Andrew G Veale FRACP Auckland, New Zealand Presentation Cough (productive or dry) Haemoptysis Shortness of breath / dyspnea Wheeze (or noisy breathing) Chest pain
Assessment of the Lung in Primary Care Andrew G Veale FRACP Auckland, New Zealand Presentation Cough (productive or dry) Haemoptysis Shortness of breath / dyspnea Wheeze (or noisy breathing) Chest pain
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
Tracheobronchomalacia
 Originales Revisión Artículo especial Arch Bronconeumol. 2010;46(4):196-202 Archivos de B r o n c o n e u m o l o g í a Volumen 46, Número 3, Marzo 2010 www.archbronconeumol.org Special Article Tracheobronchomalacia
Originales Revisión Artículo especial Arch Bronconeumol. 2010;46(4):196-202 Archivos de B r o n c o n e u m o l o g í a Volumen 46, Número 3, Marzo 2010 www.archbronconeumol.org Special Article Tracheobronchomalacia
Ch 16 A and P Lecture Notes.notebook May 03, 2017
 Table of Contents # Date Title Page # 1. 01/30/17 Ch 8: Muscular System 1 2. 3. 4. 5. 6. 7. 02/14/17 Ch 9: Nervous System 12 03/13/17 Ch 10: Somatic and Special Senses 53 03/27/17 Ch 11: Endocrine System
Table of Contents # Date Title Page # 1. 01/30/17 Ch 8: Muscular System 1 2. 3. 4. 5. 6. 7. 02/14/17 Ch 9: Nervous System 12 03/13/17 Ch 10: Somatic and Special Senses 53 03/27/17 Ch 11: Endocrine System
Tests Your Pulmonologist Might Order. Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital
 Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
Spirometry: Introduction
 Spirometry: Introduction Dr. Badri Paudel 1 2 GMC Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.
Spirometry: Introduction Dr. Badri Paudel 1 2 GMC Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.
Spirometry in primary care
 Spirometry in primary care Wednesday 13 th July 2016 Dr Rukhsana Hussain What is spirometry? A method of assessing lung function Measures volume of air a patient can expel after a full inspiration Recorded
Spirometry in primary care Wednesday 13 th July 2016 Dr Rukhsana Hussain What is spirometry? A method of assessing lung function Measures volume of air a patient can expel after a full inspiration Recorded
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
Supplementary Online Content
 Supplementary Online Content Regan EA, Lynch DA, Curran-Everett D, et al; Genetic Epidemiology of COPD (COPDGene) Investigators. Clinical and radiologic disease in smokers with normal spirometry. Published
Supplementary Online Content Regan EA, Lynch DA, Curran-Everett D, et al; Genetic Epidemiology of COPD (COPDGene) Investigators. Clinical and radiologic disease in smokers with normal spirometry. Published
Using Spirometry to Rule Out Restriction in Patients with Concomitant Low Forced Vital Capacity and Obstructive Pattern
 44 The Open Respiratory Medicine Journal, 2011, 5, 44-50 Using Spirometry to Rule Out Restriction in Patients with Concomitant Low Forced Vital Capacity and Obstructive Pattern Open Access Imran Khalid
44 The Open Respiratory Medicine Journal, 2011, 5, 44-50 Using Spirometry to Rule Out Restriction in Patients with Concomitant Low Forced Vital Capacity and Obstructive Pattern Open Access Imran Khalid
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Respiratory system. Applied Anatomy &Physiology
 Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory Physiology In-Lab Guide
 Respiratory Physiology In-Lab Guide Read Me Study Guide Check Your Knowledge, before the Practical: 1. Understand the relationship between volume and pressure. Understand the three respiratory pressures
Respiratory Physiology In-Lab Guide Read Me Study Guide Check Your Knowledge, before the Practical: 1. Understand the relationship between volume and pressure. Understand the three respiratory pressures
Tracheobronchomalacia: morfologic evaluation in 64-MDTC.
 Tracheobronchomalacia: morfologic evaluation in 64-MDTC. Poster No.: C-1779 Congress: ECR 2011 Type: Educational Exhibit Authors: C. A. P. Fontes, A. A. S. M. Santos, A. L. Ferreira Neto, E. Marchiori,
Tracheobronchomalacia: morfologic evaluation in 64-MDTC. Poster No.: C-1779 Congress: ECR 2011 Type: Educational Exhibit Authors: C. A. P. Fontes, A. A. S. M. Santos, A. L. Ferreira Neto, E. Marchiori,
Chapter. Diffusion capacity and BMPR2 mutations in pulmonary arterial hypertension
 Chapter 7 Diffusion capacity and BMPR2 mutations in pulmonary arterial hypertension P. Trip B. Girerd H.J. Bogaard F.S. de Man A. Boonstra G. Garcia M. Humbert D. Montani A. Vonk Noordegraaf Eur Respir
Chapter 7 Diffusion capacity and BMPR2 mutations in pulmonary arterial hypertension P. Trip B. Girerd H.J. Bogaard F.S. de Man A. Boonstra G. Garcia M. Humbert D. Montani A. Vonk Noordegraaf Eur Respir
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
CLINICAL SIGNIFICANCE OF PULMONARY FUNCTION TESTS
 CLINICAL SIGNIFICANCE OF PULMONARY FUNCTION TESTS Upper Airway Obstruction* John C. Acres, M.D., and Meir H. Kryger, M.D.t chronic upper airway obstruction is frequently unrecognized or misdiagnosed as
CLINICAL SIGNIFICANCE OF PULMONARY FUNCTION TESTS Upper Airway Obstruction* John C. Acres, M.D., and Meir H. Kryger, M.D.t chronic upper airway obstruction is frequently unrecognized or misdiagnosed as
How does COPD really work?
 How does COPD really work? by Alex Goodell View online Where does COPD fit in the mix of respiratory diseases? I ve made a map of the major pathologies outlined in Robbins and First Aid (obviously these
How does COPD really work? by Alex Goodell View online Where does COPD fit in the mix of respiratory diseases? I ve made a map of the major pathologies outlined in Robbins and First Aid (obviously these
Spirometry and Flow Volume Measurements
 Spirometry and Flow Volume Measurements Standards & Guidelines December 1998 To serve the public and guide the medical profession Revision Dates: December 1998 Approval Date: June 1998 Originating Committee:
Spirometry and Flow Volume Measurements Standards & Guidelines December 1998 To serve the public and guide the medical profession Revision Dates: December 1998 Approval Date: June 1998 Originating Committee:
Supramaximal flow in asthmatic patients
 Eur Respir J ; 19: 13 17 DOI: 1.113/93193..51 Printed in UK all rights reserved Copyright #ERS Journals Ltd European Respiratory Journal ISSN 93-193 Supramaximal flow in asthmatic patients H. Sala*, A.
Eur Respir J ; 19: 13 17 DOI: 1.113/93193..51 Printed in UK all rights reserved Copyright #ERS Journals Ltd European Respiratory Journal ISSN 93-193 Supramaximal flow in asthmatic patients H. Sala*, A.
Increased difference between slow and forced vital capacity is associated with reduced exercise tolerance in COPD patients
 Yuan et al. BMC Pulmonary Medicine 2014, 14:16 RESEARCH ARTICLE Open Access Increased difference between slow and forced vital capacity is associated with reduced exercise tolerance in COPD patients Wei
Yuan et al. BMC Pulmonary Medicine 2014, 14:16 RESEARCH ARTICLE Open Access Increased difference between slow and forced vital capacity is associated with reduced exercise tolerance in COPD patients Wei
Respiratory System Mechanics
 M56_MARI0000_00_SE_EX07.qxd 8/22/11 3:02 PM Page 389 7 E X E R C I S E Respiratory System Mechanics Advance Preparation/Comments 1. Demonstrate the mechanics of the lungs during respiration if a bell jar
M56_MARI0000_00_SE_EX07.qxd 8/22/11 3:02 PM Page 389 7 E X E R C I S E Respiratory System Mechanics Advance Preparation/Comments 1. Demonstrate the mechanics of the lungs during respiration if a bell jar
The Aging Lung. Sidney S. Braman MD FACP FCCP Professor of Medicine Brown University Providence RI
 The Aging Lung Sidney S. Braman MD FACP FCCP Professor of Medicine Brown University Providence RI Is the respiratory system of the elderly different when compared to younger age groups? Respiratory Changes
The Aging Lung Sidney S. Braman MD FACP FCCP Professor of Medicine Brown University Providence RI Is the respiratory system of the elderly different when compared to younger age groups? Respiratory Changes
Relationship Between FEV1& PEF in Patients with Obstructive Airway Diseases
 OBSTRUCTIVE THE IRAQI POSTGRADUATE AIRWAY MEDICAL DISEASES JOURNAL Relationship Between FEV1& PEF in Patients with Obstructive Airway Diseases Muhammed.W.AL.Obaidy *, Kassim Mhamed Sultan*,Basil Fawzi
OBSTRUCTIVE THE IRAQI POSTGRADUATE AIRWAY MEDICAL DISEASES JOURNAL Relationship Between FEV1& PEF in Patients with Obstructive Airway Diseases Muhammed.W.AL.Obaidy *, Kassim Mhamed Sultan*,Basil Fawzi
Maximal expiratory flow rates (MEFR) measured. Maximal Inspiratory Flow Rates in Patients With COPD*
 measured. Maximal Inspiratory Flow Rates in Patients With COPD*") Maximal Inspiratory Flow Rates in Patients With COPD* Dan Stănescu, MD, PhD; Claude Veriter, MA; and Karel P. Van de Woestijne, MD, PhD Objectives: To assess the relevance of maximal inspiratory flow rates
Maximal Inspiratory Flow Rates in Patients With COPD* Dan Stănescu, MD, PhD; Claude Veriter, MA; and Karel P. Van de Woestijne, MD, PhD Objectives: To assess the relevance of maximal inspiratory flow rates
Pulmonary Function Test
 Spirometry: Introduction Dr. Badri Paudel GMC Spirometry Pulmonary Function Test! Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after
Spirometry: Introduction Dr. Badri Paudel GMC Spirometry Pulmonary Function Test! Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after
Chapter 11 The Respiratory System
 Biology 12 Name: Respiratory System Per: Date: Chapter 11 The Respiratory System Complete using BC Biology 12, page 342-371 11.1 The Respiratory System pages 346-350 1. Distinguish between A. ventilation:
Biology 12 Name: Respiratory System Per: Date: Chapter 11 The Respiratory System Complete using BC Biology 12, page 342-371 11.1 The Respiratory System pages 346-350 1. Distinguish between A. ventilation:
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Clinical pulmonary physiology. How to report lung function tests
 Clinical pulmonary physiology or How to report lung function tests Lung function testing A brief history Why measure? What can you measure? Interpretation/ reporting Examples and case histories Exercise
Clinical pulmonary physiology or How to report lung function tests Lung function testing A brief history Why measure? What can you measure? Interpretation/ reporting Examples and case histories Exercise