Exacerbations. Ronald Dahl, Aarhus University Hospital, Denmark
|
|
|
- Lee McDaniel
- 6 years ago
- Views:
Transcription
1 1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark
2 The health professional that care for patients with asthma exacerbation must be able to Identificafy and diagnose asthma exacerbation Evaluate the severity of exacerbation Evaluate complications and co-morbidities Treat and monitor
3 Agenda The abnormality in the airways, lungs and the clinical consequences Clinical evaluation and classification of the severity of asthma exacerbation Treatment and monitoring Prevention
4


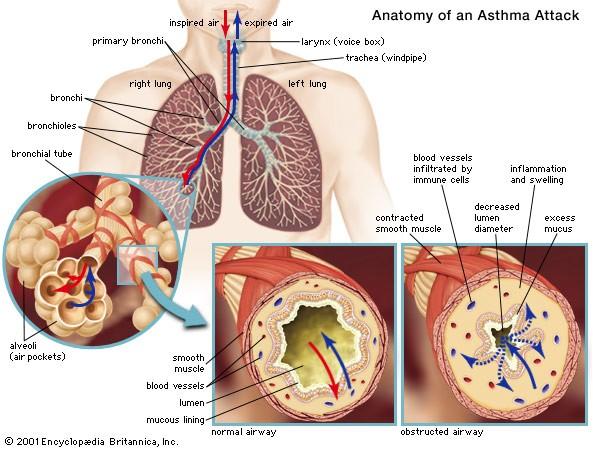
5 Acute Severe Asthma Pathology Airway obstruction and symptoms by: Bronchoconstriction Mucus plugs Mucosal edema Inflammatory cell infiltration/activation Bousquet J et al. Am J Respir Crit Care Med 2000;161: ; Beckett PA et al. Thorax 2003;58:
6 Features of an asthma attack Appear rather sudden After exposure to an irritant Last from few min to few hours Respond immediately to bronchodilators No gradual worsening occur Seem not closely related to airway inflammation Features of an asthma exacerbation Gradual progression over days Increasing symptoms and nocturnal asthma Respond partial or little to bronchodilators Related to increased airway inflammation Leads to hospital admission Responds to corticosteroids
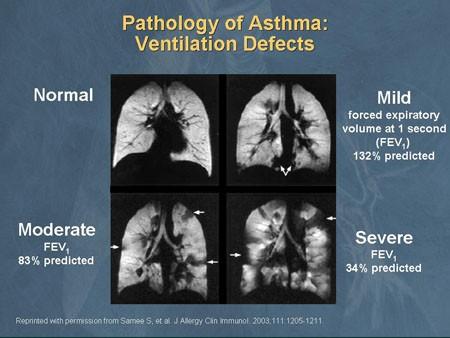
7 Exacerbation of bronchial asthma Ventilation = Spirometric abnormalities Respiration = Gas exchange abnormality Central airway narrowing Peripheral airway narrowing Bronchospasm Airway wall inflammation Bronchospasm Airway wall inflammation
8 Exacerbation of bronchial asthma Ventilation = Spirometric abnormalities Respiration = Gas exchange abnormality Central airway narrowing Peripheral airway narrowing Bronchospasm Airway wall inflammation Bronchospasm Airway wall inflammation Treatments must be directed towards these two components Smooth muscle spasm Inflammation, edema, plugs
9
10 Acute severe asthma monitoration slight Normo ventilation moderate severe Hyper Hypoventilation ventilation exhaustion

11 Acute severe asthma monitoration the cross-road of death slight Normo ventilation moderate severe Hyper Hypoventilation ventilation exhaustion
12 Acute severe asthma monitoration Clinical condition PEF or FEV1 PaO2 and PaCO2
13 Asthma severity stage 0 Respiratory rate Pulse rate Minute ventilation PEF
14 Acute severe asthma klinical evaluation Respiratory rate: (number/min) Speaking: short sentenses, single word Use of auxilary respiratory muscles Position: prefer sitting, can lay down? Airways obstruction: ronchi, silent chest (PEF) Respiration: cyanoses, (SaO2, a-blood gasses) General evaluation: degree of normal activities, pulse frequency
15 Clinical staging of severity of acute asthma exacerbation stage 0 Unaffected Few ronchi
16 Clinical staging of severity of acute asthma exacerbation stage 1 Breathlessness but unaffected physical activities Can lie down Ronchi during expiration
17 Clinical staging of severity of acute asthma exacerbation stage 2 Some restriction in physical activity Prefer to sit Use of auxilary resp. muscles (neck) Ronchi during in- and expiration
18 Clinical staging of severity of acute asthma exacerbation stage 3 Severe restriction in physical performance Prefer not to lie down Conversational dyspnoea Use of auxilary resp. muscles (neck, abdomen)
19 Clinical staging of severity of acute asthma exacerbation stage 4 Sit quiet bent forward Answer with single word Mental alert and orientated Use of auxilary resp. muscles (neck, abdomen, arms) Decreasing ronchi
20 Clinical staging of severity of acute asthma exacerbation stage 5 Affected consciousness Fast, superficial respiration Silent chest
21 Near fatal asthma acute severe asthma Respiratory arrest or PaCO2 above 6.7 kpa and/or Altered conscious state or Inability to speak Campbell et al. ERJ 1994; 7:490-7
22 Near fatal asthma acute severe asthma Pretreatment SaO2 below 90% Normal or high PaCO2 after therapy Persistent metabolic acidosis Severe obstruction that improve less than 30% or worsen after beta-2-agonist Mc Fadden ER Jr. Lancet 1995;345:
23 Near fatal asthma acute severe asthma Asthma severity (before attack) Death cases% Near fatal attacks cases% mild 5 7 moderate severe All asthma severities are at risk Campbell et al. ERJ 1994; 7:490-7
24 Acute severe asthma Monitoring Clinical condition PEF or FEV1 PaO2 and PaCO2
25 The responsible staff must be able to: Assess asthma severity Assess improvement and worsening Treat properly Guidance
26 Measurements for evaluation of severity and evolution improvement worsening? Ventilatory capacity Movement of air Spirometry FEV1 etc. Respiratory capacity gas exchange in alveoli Arterial blood PaO2 PaCO2 SaO2
27 Measurements for evaluation of severity and evolution improvement worsening? Cardiac function and Circulation Chest x-ray Heart frequency Blood pressure EKG Pneumothorax Pneumonia Left ventricle failure
28 ACUTE ASTHMA MONITORING CHART Name: Birth date: Date: Time first seen: Time Pulse rate History: Respiratory rate Use of accessory muscles PEF Pulse oximetry (SaO2) Cyanosis Exhaustion Oxygen flow Neck l/m Abdomen Arms Neck l/m Abdomen Arms Neck l/m Abdomen Arms Treatment Salbutamol/Terbutaline Dose: Delivery: Nebuliser/Spacer Oral steroid : Inhaled steroid: Salbutamol/Terbutaline Dose: Delivery: Nebuliser/Spacer Oral steroid : Inhaled steroid: Salbutamol/Terbutaline Dose: Delivery: Nebuliser/Spacer Oral steroid : Inhaled steroid:
29 Acute severe asthma Admission and close monitoration in hospital unit: Clinical stage 4 PEF or FEV1 < 30% of personal best (if unknown < 30% predicted) PaCO2 > 6 kpa PaO2 < 8 kpa Poor response to initial treatment
30 Acute severe asthma differential diagnosis - complications Hyperventilation syndrome Vocal cord dysfunction Vaso-vagal reaction Anaphylactic reaction (urticaria, BP-pulse, etc) Aspiration - foreing body pneumonia Pneumothorax Cardiac failure COPD exacerbation
31 Acute severe asthma treatment Oxygen
32 Acute severe asthma treatment Oxygen Nebulised beta-2-agonist combined with anticholinergic, each 20 min first hour, then hourly as necessary
33 FEV1 at presentation 30% (left panel) or > 30% (right panel)
34 Acute severe asthma treatment Oxygen Nebulised beta-2-agonist combined with anticholinergic each 20 min first hour, then hourly as necessary Oral or i.v. corticosteroid 80 mg Methylprednisolon repeat after 12 hours, following days usually 40 mg Methylprednisolon or equivalent
35 Acute severe asthma treatment Oxygen nebulised beta-2-agonist combined with anticholinergic each 20 min first hour, then hourly as necessary Oral or i.v. corticosteroid 80 mg Methylprednisolon repeat after 12 hours, following days usually 40 mg Methylprednisolon or equivalent Start inhaled high dose steroid as soon as possible
36 Acute severe asthma treatment Dangerous or at least without effect Sedation Mucolytic Physiotherapy Antihistamine
37 Acute severe asthma treatment Consider: Infusion of ß2-agonist Infusion of theophylline Antibiotic Fluid
38 Change in FEV1 in BPV group (BiPAP) and control group during 4 h
39

40 Influence of illness severity on response to magnesium
41 Acute severe asthma Treat the condition symptomatical Determine what caused the reaction
42 Acute severe asthma Determine what caused the reaction inhalant allergen food allergen drug reaction (ASA,vaccination,etc) infection worsening of a chronic condition compliance treatment need adjustment
43 The health professional that care for patients with asthma exacerbation must be able to Identificafy and diagnose asthma exacerbation Evaluate the severity of exacerbation Evaluate complications and co-morbidities Treat and monitor
44 Thank you for your attention
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Bronchospasm & SOB. Kim Kilmurray Senior Clinical Teaching Fellow
 Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
Management of Acute Asthma Exacerbations in Children 2012 Update. Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch
 Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines
Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Guideline on the Management of Asthma in adults SHSCT
 CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Management of Asthma in adults Dr A John, Dr J Lindsay Respiratory Medicine/ MUSC Medicine Date Uploaded: 23/11/15 Review Date
CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Management of Asthma in adults Dr A John, Dr J Lindsay Respiratory Medicine/ MUSC Medicine Date Uploaded: 23/11/15 Review Date
Medicine Dr. Kawa Lecture 4 - Treatment of asthma :
 Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Recurrent wheezing illnesses 24.9% Similar to Australia Above global averages
 Prof Mike South Department of General Medicine Royal Children s Hospital Melbourne Australia www.mikesouth.org.au Asthma is very common in Australia Approx 25% children have recurrent wheezing illnesses
Prof Mike South Department of General Medicine Royal Children s Hospital Melbourne Australia www.mikesouth.org.au Asthma is very common in Australia Approx 25% children have recurrent wheezing illnesses
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL
 DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Medical Emergencies at Moderate and High Altitude
 Medical Emergencies at Moderate and High Altitude Annalisa Cogo Clinica Pneumologica e Centro Studi Biomedici Applicati allo Sport Università di Ferrara Payer Hutte, Ortler Mountain Environment Barometric
Medical Emergencies at Moderate and High Altitude Annalisa Cogo Clinica Pneumologica e Centro Studi Biomedici Applicati allo Sport Università di Ferrara Payer Hutte, Ortler Mountain Environment Barometric
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Decramer 2014 a &b [21]
![Decramer 2014 a &b [21]](/thumbs/90/101390504.jpg "Decramer 2014 a &b [21]") Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
Pathway diagrams Annex F
 Pathway diagrams Annex F Fig 1 Asthma: The patient journey Asthma is diagnosed Making the diagnosis of asthma Confirming the diagnosis may depend on history, response to treatment, measurement of airflow
Pathway diagrams Annex F Fig 1 Asthma: The patient journey Asthma is diagnosed Making the diagnosis of asthma Confirming the diagnosis may depend on history, response to treatment, measurement of airflow
Chronic obstructive pulmonary disease
 Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Asthma. chapter 7. Overview
 chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
PATHOPHYSIOLOGICAL PROCESS TEMPLATE
 1 PATHOPHYSIOLOGICAL PROCESS TEMPLATE DISEASE: Chronic obstructive pulmonary disease (COPD) DEFINITION: COPD can be defined as a disease in which there is a significant damage to the lungs thus reducing
1 PATHOPHYSIOLOGICAL PROCESS TEMPLATE DISEASE: Chronic obstructive pulmonary disease (COPD) DEFINITION: COPD can be defined as a disease in which there is a significant damage to the lungs thus reducing
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Management of Acute Exacerbations
 15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
15 Management of Acute Exacerbations Cenk Kirakli Izmir Dr. Suat Seren Chest Diseases and Surgery Training Hospital Turkey 1. Introduction American Thoracic Society (ATS) and European Respiratory Society
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
REFERRAL GUIDELINES RESPIRATORY
 REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
Management of acute asthma in children in emergency department. Moderate asthma
 152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 Page 1 of 9 PURPOSE To assure that DOP inmates with Pulmonary Diseases are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers and Chronic Disease Nurses are
Page 1 of 9 PURPOSE To assure that DOP inmates with Pulmonary Diseases are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers and Chronic Disease Nurses are
Respiratory Medicine
 Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
3. Identify the importance in the prehospital setting for the administration of nebulized bronchodilator.
 TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Title Protocol for the Management of Asthma
 Document Control Title Protocol for the Management of Asthma Author Author s job title Professional Lead, Minor Injuries Unit Directorate Emergency Services, Logistics and Resilience Department Version
Document Control Title Protocol for the Management of Asthma Author Author s job title Professional Lead, Minor Injuries Unit Directorate Emergency Services, Logistics and Resilience Department Version
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Breathlessness in advanced disease. February 2017
 Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network
 Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
ASTHMA (SEE BTS GUIDELINES NEXT PAGE)
") ASTHMA (SEE BTS GUIDELINES NEXT PAGE) RESPIRATORY Signs of Severe asthma Unable to speak in sentences? Peak flow < 50% predicted or best? Respiratory Rate >25/min? Pulse>110/min? Sa0 2
ASTHMA (SEE BTS GUIDELINES NEXT PAGE) RESPIRATORY Signs of Severe asthma Unable to speak in sentences? Peak flow < 50% predicted or best? Respiratory Rate >25/min? Pulse>110/min? Sa0 2
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Asthma- THE most common Pediatric Disease JENNIFER MCDANIEL, RRT- NPS
 Asthma- THE most common Pediatric Disease JENNIFER MCDANIEL, RRT- NPS Asthma Usually acquire before the age of 10 These patients exhibit hyper-reactive airways Spasm Constriction Swelling Secretions are
Asthma- THE most common Pediatric Disease JENNIFER MCDANIEL, RRT- NPS Asthma Usually acquire before the age of 10 These patients exhibit hyper-reactive airways Spasm Constriction Swelling Secretions are
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Chronic obstructive pulmonary disease: the management of adults with chronic obstructive pulmonary disease in primary and secondary
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Chronic obstructive pulmonary disease: the management of adults with chronic obstructive pulmonary disease in primary and secondary
Chapter 7. Anticholinergic (Parasympatholytic) Bronchodilators. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Bronchodilators. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.") Chapter 7 Anticholinergic (Parasympatholytic) Bronchodilators Clinical Indications for Use Indication for anticholinergic bronchodilator COPD maintenance Indication for combined anticholinergic and β-agonist
Chapter 7 Anticholinergic (Parasympatholytic) Bronchodilators Clinical Indications for Use Indication for anticholinergic bronchodilator COPD maintenance Indication for combined anticholinergic and β-agonist
Respiratory Emergencies. Chapter 11
 Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
Respiratory Pharmacology
 Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Objectives. Asthma in Primary Care. Definition. Epidemiology. Pathophysiology
 Objectives Asthma in Primary Care Jed Grant, PA-C Program Director, SJVC PA Program Staff PA, AMCH Emergency Department Apply the NAEPP guideline measures of severity and control including current impairment
Objectives Asthma in Primary Care Jed Grant, PA-C Program Director, SJVC PA Program Staff PA, AMCH Emergency Department Apply the NAEPP guideline measures of severity and control including current impairment
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease
 HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
Treatment of Acute Asthma Exacerbations in Adults in the Primary Care or Urgent Care Setting Clinical Practice Guideline MedStar Health.
 Treatment of Acute Asthma Exacerbations in Adults in the Primary Care or Urgent Care Setting Clinical Practice Guideline MedStar Health Background: These guidelines are provided to assist physicians and
Treatment of Acute Asthma Exacerbations in Adults in the Primary Care or Urgent Care Setting Clinical Practice Guideline MedStar Health Background: These guidelines are provided to assist physicians and
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 DRAFT NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Chronic obstructive pulmonary disease: the management of adults with chronic obstructive pulmonary disease in primary
DRAFT NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Chronic obstructive pulmonary disease: the management of adults with chronic obstructive pulmonary disease in primary
patient group direction
 SALBUTAMOL v01 1/12 SALBUTAMOL PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
SALBUTAMOL v01 1/12 SALBUTAMOL PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner
The Changes of Arterial Blood Gases in COPD During Four-year Period
 ORIGINAL ARTICLE doi: 10.5455/medarh.2014.68.14-18 The Changes of Arterial Blood Gases in COPD During Four-year Period Vesna Cukic Clinic for pulmonary diseases and TB Podhrastovi, Clinical Centre of Sarajevo
ORIGINAL ARTICLE doi: 10.5455/medarh.2014.68.14-18 The Changes of Arterial Blood Gases in COPD During Four-year Period Vesna Cukic Clinic for pulmonary diseases and TB Podhrastovi, Clinical Centre of Sarajevo
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Indications for Respiratory Assistance. Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer
 Indications for Respiratory Assistance Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer Respiratory Assistance Non-invasive - Nasal specs - Facemask/ Resevoir
Indications for Respiratory Assistance Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer Respiratory Assistance Non-invasive - Nasal specs - Facemask/ Resevoir
& Guidelines. For The Management Of. Chronic Obstructive Air Way Disease (COPD)
") Guidelines For The Management Of Chronic Obstructive Air Way Disease (COPD) By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs
Guidelines For The Management Of Chronic Obstructive Air Way Disease (COPD) By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs
COPD Challenge CASE PRESENTATION
 Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC
 KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC") Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Some Facts About Asthma
 Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
National Asthma Educator Certification Board Detailed Content Outline
 I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
 β 2004 2004 o β β β β 2004 β β β β β β β β β 2004 2004 2004 2004 2004 β 2004 2004 2004 2004 β β 2004 β β β β β β β 2004 β β β β β β 2004 β β β β STEP 5: CONTINUOUS OR FREQUENT USE OF ORAL
β 2004 2004 o β β β β 2004 β β β β β β β β β 2004 2004 2004 2004 2004 β 2004 2004 2004 2004 β β 2004 β β β β β β β 2004 β β β β β β 2004 β β β β STEP 5: CONTINUOUS OR FREQUENT USE OF ORAL
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
By Mark Bachand, RRT-NPS, RPFT. I have no actual or potential conflict of interest in relation to this presentation.
 By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
The adult with recurrent breathlessness. A/Prof Gerald Chua Medicine NTFGH
 The adult with recurrent breathlessness A/Prof Gerald Chua Medicine NTFGH Dyspnoea Subjective experience of breathing discomfort Variable among individuals with apparently similar degrees of impairment
The adult with recurrent breathlessness A/Prof Gerald Chua Medicine NTFGH Dyspnoea Subjective experience of breathing discomfort Variable among individuals with apparently similar degrees of impairment
You ve come a long way, baby.
 COPD Dr Badri Paudel Dept of Medicine GMC/CHRC 4/22/12 badri@gmc 2 You ve come a long way, baby. Wayne McLaren Former Marlboro Man 4/22/12 badri@gmc 3 Age 30 a robust young man Age 51 riding into the sunset
COPD Dr Badri Paudel Dept of Medicine GMC/CHRC 4/22/12 badri@gmc 2 You ve come a long way, baby. Wayne McLaren Former Marlboro Man 4/22/12 badri@gmc 3 Age 30 a robust young man Age 51 riding into the sunset
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Update on management of respiratory symptoms. Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT
 Update on management of respiratory symptoms Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT Topics The common respiratory symptoms Cough: causes, diagnosis and therapy Update
Update on management of respiratory symptoms Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT Topics The common respiratory symptoms Cough: causes, diagnosis and therapy Update
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Clinical guideline for acute wheeze & asthma in children 5 years and over Hospital care
 Clinical guideline for acute wheeze & asthma in children years and over Hospital care Airedale NHS Trust Bradford Teaching Hospitals NHS Foundation Trust NHS Bradford and Airedale DOB: A&E/Hospital : Weight:
Clinical guideline for acute wheeze & asthma in children years and over Hospital care Airedale NHS Trust Bradford Teaching Hospitals NHS Foundation Trust NHS Bradford and Airedale DOB: A&E/Hospital : Weight:
Respiratory Emergencies. Lesson Goal. Lesson Objectives 9/10/2012
 Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
Anaphylaxis/Latex Allergy
 Children s Acute Transport Service CATS Clinical Guideline Anaphylaxis/Latex Allergy Document Control Information Author D Lutman Author Position Consultant Document Owner E Polke Document Owner Position
Children s Acute Transport Service CATS Clinical Guideline Anaphylaxis/Latex Allergy Document Control Information Author D Lutman Author Position Consultant Document Owner E Polke Document Owner Position
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Treatment. Assessing the outcome of interventions Traditionally, the effects of interventions have been assessed by measuring changes in the FEV 1
 58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Public Dissemination
 1. THE ASTHMA CONDITION 9 18 3 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
1. THE ASTHMA CONDITION 9 18 3 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
Living well with COPD
 This factsheet aims to show people with chronic obstructive pulmonary disease (COPD) and their friends and family how they can live a full life with this disease. What is COPD? COPD is a condition that
This factsheet aims to show people with chronic obstructive pulmonary disease (COPD) and their friends and family how they can live a full life with this disease. What is COPD? COPD is a condition that