Managing Medication Costs: Focus on Appropriate Utilization
|
|
|
- Julian Hampton
- 6 years ago
- Views:
Transcription

1 Managing Medication Costs: Focus on Appropriate Utilization Dr. Brian Stwalley, Pharm.D., CGP 1 Managing Costs Through Appropriate Utilization Which medications/classes of medications are driving up your costs? Are medications being appropriately used? Do you see patterns month after month? What can be done to manage these costs? What tools can Omnicare provide to assist you with managing these costs? 2 1
2 Managing Costs Through Appropriate Utilization Focus on High Risk, High Cost, Highly Utilized Medications Injectable Anticoagulants (enoxaparin) Proton Pump Inhibitors ESAs (Procrit, Aranesp) Appetite Stimulants Antibiotics (Vancomycin) Other: Antipsychotics/Lidoderm Drug Utilization: Top 50 Dollar Usage Product Description Product Description ARANESP 100 MCG/0.5 ML SYRINGE ARICEPT 10 MG TABLET LOVENOX INJ 40/0.4ML ARIXTRA 2.5 MG SYRINGE NOVOLOG 100 UNIT/ML VIAL ZYVOX 600 MG TABLET NORMAL SALINE IV FLUSH SYR LOVENOX 40 MG PREFILLED SYRN PLAVIX 75 MG TABLET NAMENDA 10 MG TABLET FRAGMIN 5,000 UNITS SYRINGE PANTOPRAZOLE SOD 40 MG TAB DR PROCRIT 20,000/ML *MDV* (*1ML) LANTUS 100 UNITS/ML VIAL PROCRIT 40,000U/ML VL (*1ML) OMEPRAZOLE 20 MG CAPSULE DR ADVAIR DISKUS HEPARIN IV FLUSH 100 UNITS/ML NOVOLIN R 100 UNITS/ML VIAL TPN* 1525ML IPRATR-ALBUTEROL MG/3 ML XOPENEX 0.63MG NEB LIDODERM 5% PATCH PLAVIX TAB 75MG INSULIN LANTUS 100U/ML INJ IV*PRIMAXIN 500MG/100ML NS MB IV*TIMENTIN 3.1GM/100ML NS EXELON 4.6 MG/24HR PATCH LOVENOX 30 MG PREFILLED SYRN SANTYL OINTMENT OMEPRAZOLE 40 MG CAPSULE DR VANCOCIN HCL 250 MG PULVULE ARICEPT 5 MG TABLET LOVENOX 80 MG PREFILLED SYRN SEROQUEL 25 MG TABLET RISPERDAL CONSTA 50 MG SYR NOVOLOG MIX VIAL APLISOL SYRINGE (PPD) MEGESTROL ACET 40 MG/ML SUSP LEVAQUIN 500 MG TABLET PNEUMOVAX 23 VIAL FLOMAX 0.4MG CAPSULE LOVENOX INJ 30/0.3ML RISPERIDONE 0.5 MG TABLET MEGACE ES 625 MG/5 ML SUSP IV*AMPIC/SULBAC 3G/100ML NS MB VANCOMYCIN HCL 1G/200ML D5W BG SEROQUEL 50 MG TABLET INSULIN NOVOLOG 100U/ML NEXIUM 40 MG CAPSULE 2

3 LMWHs Identify prescribers and referral trends from discharging hospitals Establish a stop order policy for these agents Determine date therapy was initiated in acute care Dispense only enough doses to cover remaining days Establish a policy to ensure a CrCl is calculated when these agents are ordered and the dose adjusted for renal impairment Consider bridge to warfarin for residents requiring longer term therapy ( generics first ) Routinely monitor and measure success of utilization management approaches 5 Lovenox (enoxaparin) Dosing Card 3

4 Lovenox (enoxaparin) Worksheet Managing Costs Through Appropriate Utilization: PPIs Are Proton Pump Inhibitors (PPIs) highly utilized? Evaluate transfer/admission orders for initiation in acute care to determine continued need Ask if resident used a PPI before entry into an acute care setting? Assure a current supporting diagnosis if medically necessary Consider trial discontination Implement a generics first program Omeprazole is most commonly the preferred PPI by PDP s Facilitates Medicare Part D coverage without prior authorization, step therapy, or exception processes Evaluate use of PPI and Plavix (clopidogrel) 8 4
5 Proton Pump Inhibitor Evaluation Proton Pump Inhibitor (PPI) Evaluation Purpose: To provide a guideline for the appropriate use of proton pump inhibitors including diagnosis, patient selection criteria and use of formulary agent. Target Drugs: Aciphex, Nexium, omeprazole, Prilosec, Prilosec OTC, Prevacid, Protonix, pantoprazole, lansoprazole Procedure: Contact physician for medication order change based upon results of evaluation Resident Admission Date Current therapy Date Started Nursing questions to ask: 1. Evaluate transfer/admission orders for initiation in acute care to determine continued need; was PPI therapy started during hospital stay? 2. Ask if resident used a PPI before entry into an acute care setting? 3. Assure a current supporting diagnosis if medically necessary (see below). 4. Implement a generics first medication choice: omeprazole. i. omeprazole is most commonly the preferred PPI by PDP s ii. facilitates Medicare Part D coverage without prior authorization, step therapy, or exception processes 5. The concomitant use of omeprazole and clopidogrel should be avoided because of the effect on clopidogrel's active metabolite levels and anticlotting activity. Patients at risk for heart attacks or strokes, who are given clopidogrel to prevent blood clots, may not get the full protective anticlotting effect if they also take prescription omeprazole or the OTC form (Prilosec OTC). There is insufficient information about drug interactions between clopidogrel and PPIs other than omeprazole and esomeprazole to make specific recommendations about their coadministration. Ranitidine and famotidine are available by prescription and OTC to relieve and prevent heartburn and antacids are available OTC to relieve heartburn. At least one of the following diagnoses must be the treating diagnosis: GERD (supporting documentation available in medical record) Peptic Ulcer Disease (PUD) Prevention of ulcers due to non-steroidal anti-inflammatory drugs (NSAIDS,COX-2s) Healing and maintenance treatment for gastric or duodenal ulcers Diagnosis of Helicobacter Pylori (confirmed with testing) Hypersecretory condition: Barrett s Esophagitis, Zollinger-Ellison Syndrome Chronic ventilator patients at risk for stress ulcers Evaluator recommendation to Prescriber Discontinuing current PPI therapy until symptoms return Discontinuing current PPI therapy and start calcium therapy (calcium carbonate 500mg prn or pc and hs) Continuing current therapy and re-evaluate resident in Discontinuing current PPI therapy and start omeprazole 20mg QD (or an alternative PPI covered by beneficiaries payer) Continuing current therapy Other Evaluator: Date: Additional Comments ESAs Are ESA s (Procrit, Aranesp ) highly utilized in your facility? Verify indication, Hgb, and when next dose needed at time of admission Verify dose is appropriate based on underlying cause of anemia (CKD, Cancer Chemotherapy) Evaluate medication regimen for inclusion of oral iron therapy when on an ESA Dialysis Center to provide medication for dialysis patients 10 5
6 ESAs Weight based dosing Savings All orders for Procrit >20,000 units/week and Aranesp >100 mcg/week should be evaluated for appropriateness Monitoring of Hgb (for CKD patients) ESA doses should be held and adjustment made when a Hgb of greater than 10 g/dl is achieved Evaluate need if hgb exceeds 11 due to greater risk of death, serious adverse cardiovascular reactions and stroke Appetite Stimulants Are Appetite Stimulants highly utilized in your facility to promote weight gain? (Megestrol suspension/megace ES) Evaluate progress towards goals Weight gain, increased appetite Re-evaluate frequently History of thromboembolic disease Contraindicated History of depression Consider Mirtazapine 6
7 Appetite Stimulants Statement in F325 regarding the use of appetite stimulants: To date, the evidence is limited about benefits from appetite stimulants. While their use may be appropriate in specific circumstances, they are not a substitute for appropriate investigation and management of potentially modifiable risk factors and underlying causes of anorexia and weight loss Appetite Stimulants Assessment of Appetite Stimulants All residents with nutritional problems should be reviewed for medication-related issues Have medications been reviewed to see if they cause alterations in taste, decreased appetite or dry mouth Work with your Consultant Pharmacist to identify and assess these residents Interdisciplinary communication and cooperation is critical 7
8 Other Examples Is vancomycin highly utilized in your facility to treat Clostridium difficile diarrhea? Carefully assess cause & severity of diarrhea Use metronidazole 1st line for mild to moderate episode; use Vancomycin only for severe initial episode according to Infectious Diseases Society of America & the CDC Metronidazole is much less expensive Use 2 courses Metronidazole before utilizing vancomycin unless second episode is more severe If vancomycin needed, use PO, NOT IV Order oral solution if vancomycin needed 15 Other Examples Antibiotics Culture and Sensitivity information confirms that the organism is susceptible to antibiotic ordered Understand the results of the antibiogram Is organism susceptible to less expensive alternative? Question multiple orders for antibiotics Ensure duration of therapy verified- (e.g. antibiotics initiated in hospital)-obtain stop date if not specified IV Oral: Is resident capable of using oral formulation? (e.g. Zyvox, Levaquin) 8
9 Other Examples Antipsychotics General Management Goals These agents should not be used as first-line considerations for managing behavioral symptoms associated with dementia in older adults without psychotic symptoms due to lack of controlled efficacy data and/or significant safety concerns First-line treatment for such individuals should be non-pharmacologic Underlying conditions or disease states that can cause or exacerbate behavioral symptoms should be assessed and managed appropriately If pharmacotherapy is deemed appropriate, the most appropriate agent at the lowest effective dose should be selected and used carefully for the shortest duration necessary Response to therapy should be monitored and documented frequently and treatment should be evaluated for GDR, tapering or discontinuation Other Examples Antipsychotics Often prescribed during hospitalization for agitation On admission, review for possible non-pharmacologic interventions for agitation Agents can cause sedation, dizziness, etc. which can lead to falls Even short-term use (e.g. 30 days) has been associated with increased risk of serious adverse events Boxed warnings about an increased risk of mortality when used in patients with dementia Many of these agents also increase the risk of stroke and diabetes in the elderly 9
10 Other Examples Recent trial DART-AD Trial Dementia Antipsychotic Withdrawal Trial-Alzheimer s Disease Less than 10% of patients taken off of antipsychotics had to be restarted, and they were able to stay off at least a year before they need to be restarted Another trial CATIE-AD Trial Clinical Antipsychotic Trials of Intervention Effectiveness- Alzheimer s Disease Concluded that adverse effects offset advantages Recent analysis showed worsening of cognition Recent Attention on Antipsychotic Use In May, 2011, the Office of the Inspector General (OIG) of the US Dep t of Health and Human Services issued a report stating 83% of Medicare claims for atypical antipsychotic drugs for elderly nursing homes residents were associated with off-label conditions; 88% were associated with the condition specified in the FDA boxed warning (based on 2007 data) Also in May, 2011, the American Health Care Association released a Talking Points document, that stated we agree that the number of patients using antipsychotic drugs in nursing facilities should be less and that more efforts need to be done to look at how to manage dementia patients with behavior problems without medications 20 10
11 Other Examples Analgesic Patches (e.g. Lidoderm patch) Pain assessment upon admission to the facility and continual reassessment thereafter Non-pharmacological and (if necessary) judicious pharmaceutical approaches to pain management Continual monitoring for effectiveness and adverse effects of interventions Adjusting pain management interventions if necessary, based on resident outcome Regulatory Aspect According to F329 Each resident s drug regimen must be free from unnecessary drugs. An unnecessary drug is any drug when used: (i) In excessive dose (including duplicate therapy); or (ii) For excessive duration; or (iii) Without adequate monitoring; or (iv) Without adequate indication for its use; or (v) In the presence of adverse consequences which indicate the dose should be reduced or discontinued; or (vi) Any combinations of the reasons above. CFR (I), Unnecessary Drugs 11

12 Regulatory Aspect Has the disease state resolved that the drug was originally prescribed for? Are non-pharmacological interventions being used or are there alternative non-drug options that could be tried? Is there another drug more effective for the disease? Is there an equally effective, lower-cost drug available? Have treatment goals been achieved? Are there any adverse effects to the medication observed? Are 2+ drugs of the same class/pharmacological action being used? Are there any drug-drug or drug-disease interactions? Is there a lower effective dose of the medication? Should the dosage be adjusted based on age, renal, or liver status? Has there been any recent change in ADL status? Medication Appropriateness Checklist Hanlon JT, Schmader KE et al. J Clin Epidemiol 1992 ;45 :1045 Fitzgerald LS, Hanlon JT et al. Ann Pharmacother 1997 ;31 : Schmader KE. Hanlon JT. Pieper CF et al. Am J Med 2004;116(6):
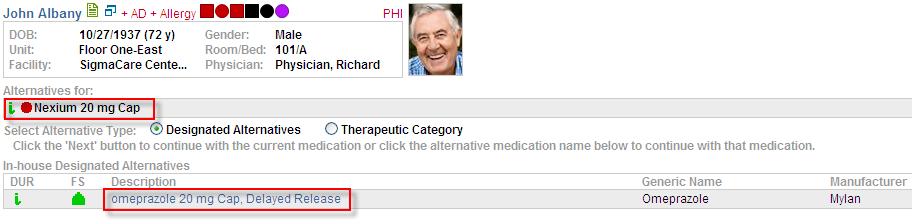
13 Focus on Medication Selection Omnicare s Therapeutic Interchange Programs Patient Specific Therapeutic Interchange Facility Formulary Implementation Omnicare can assist facility in implementing a facility formulary in states where Omnicare s Electronic Medical Record System Reduce non-covered pharmaceutical costs Formulary Management Focus on Medication Selection Therapeutic Interchange: Therapeutic Interchange is defined as substitution of a drug that has comparable or superior therapeutic effects as the drug originally prescribed based on appropriate authorization of the prescriber. Therapeutic Interchange among clinically comparable medications will reduce the price of medications to the payer TI protocols are based on the clinical evidence provided in Omnicare s Geriatric Pharmaceutical Care Guidelines and the relative effectiveness, safety and/or pricing of comparable drugs 13

14 Summary of Omnicare Therapeutic Program Select Agents Managing Costs Through Appropriate Utilization: Focus on Medication Selection Generics first approach Generic products have become available that provide therapeutically equivalent alternatives that demonstrate equal Efficacy Safety Tolerability, and May be offered at a lower price to the payer Generics first approach aligns with PDP formulary covered medications 14

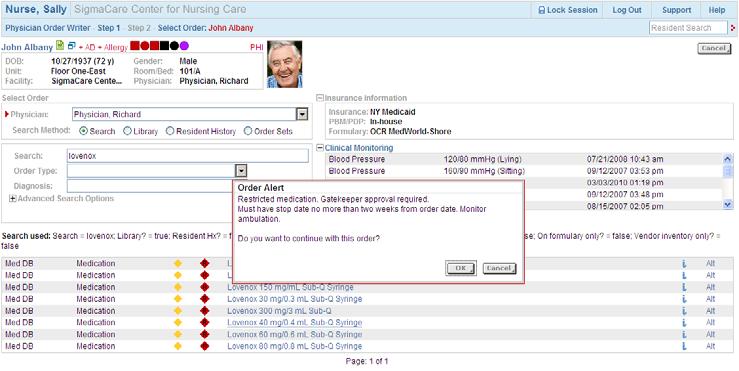
15 Focus on Medication Selection SigmaCare: Omnicare s Electronic Medical Records System Order entry with real-time DUR, formulary and prior authorization alerts Alerts non-formulary or non-covered medication for intervention Promotes formulary compliance before medication is ordered Allows prescriber/nursing staff to modify order based on prompts from system Managing Costs Through Appropriate Utilization: Focus on Medication Selection Generic omeprazole oxybutyniner meloxicam mupirocin lisinopril brimonidine fenofibrate albuterol finasteride ropinirole fluticasone nasal spray losartan losartan/hctz donepezil tamsulosin atorvastatin 30 15
16 FACILITY FORMULARY PARTICIPATION FORM Account Name (Print) Corporate City and State (Print) Omnicare Representative (Print) Omnicare s Geriatric Pharmaceutical Care Guidelines is the Formulary adopted by this National/Regional Account s Pharmacy and Therapeutics (P&T) Committee, or equivalent committee. Based on the Formulary, the following FACILITY FORMULARY THERAPEUTIC INTERCHANGE PROTOCOLS (Protocols) have been adopted by the National/Regional Account s P&T Committee, or equivalent committee, for its Facilities. Each Protocol sets forth criteria that must be satisfied for a therapeutic interchange to take place. The interchanges are to medications that offer comparable effectiveness, safety and tolerability at a generally lower price to the payer, or to medications that have clinically superior effectiveness, safety or tolerability profiles potentially at a higher price to the payer. The Following Formulary Facility Adopts Page When this Medication is Prescribed Medication will be Dispensed Interchange YES 2 All ACEIs except captopril, benazepril or enalapril generic lisinopril 3 Rapaflo, Alfuzosin, or Uroxatral generic tamsulosin 4 Nexium, Prevacid, Lansoprazole, Dexilant, Aciphex generic omeprazole 20 mg 4 Omeprazole 40 mg, Nexium 40 mg, Dexilant 60 mg generic omeprazole 20 mg 5-6 Immediate release oxybutynin, Vesicare, Detrol, Detrol LA generic oxybutynin ER Sanctura, Sanctura XR, trospium, Toviaz or Gelnique 7 Generic triamcinolone acetonide, Nasacort AQ, Nasonex, generic fluticasone Rhinocort Aqua, Veramyst, or Omnaris 8 Celebrex generic meloxicam 9 Alphagan P 0.1% and 0.15% generic brimonidine tartrate 0.2% 10 Humulin Insulins Novo Insulins unit for unit 10 Humalog 75/25 Mix Novolog 70/30 Mix unit for unit 10 Humalog Novolog unit for unit 11 Bactroban cream generic mupirocin ointment 12 Miacalcin Nasal Spray or calcitonin salmon Fortical 13 Tricor, Antara, or Trilipix generic fenofibrate 14 Exelon Capsules, rivastigmine, Razadyne or galantamine generic donepezil 15 Avodart generic finasteride 16 Renagel Renvela 17 ProAir HFA, Proventil HFA or Xopenex HFA Ventolin HFA 18 Levalbuterol or Xopenex Nebulization generic albuterol nebulization 19 Brovana Perforomist nebulization 20 Generic pramipexole generic ropinirole 21 Boniva generic alendronate 22 Actonel Atelvia 23 Vancomycin Capsules (Vancocin ) Vancomycin Oral Solution 24 Symbicort Advair Diskus 25 Flovent HFA Flovent Diskus 26 Betaseron Extavia 27 Dovonex Cream generic calcipotriene ointment Atacand, Avapro, Benicar, Micardis, Teveten generic losartan Atacand HCT, Avalide, Benicar HCT, generic losartan/hctz Micardis HCT, or Teveten HCT 30 Lumigan generic latanoprost 31 Byetta Victoza Crestor, Livalo, Vytorin, Zetia or simvastatin generic atorvastatin 34 Bromday ophthalmic solution generic bromfenac ophthalmic solution 35 Hectorol Zemplar 36 Megace ES generic megestrol acetate 37 Novolog or Levemir vials Novolog & Levemir Flexpen 37 Lantus vials Lantus Solostar By signing below, I am notifying Omnicare that the National/Regional Account s P&T Committee, or equivalent committee, has adopted Omnicare s Geriatric Pharmaceutical Care Guidelines as its Formulary for all its Facilities. Those FACILITY FORMULARY THERAPEUTIC INTERCHANGE PROTOCOLS checked Yes above are adopted for potential use by our prescribing clinicians when they prescribe medications for the facilities residents. I acknowledge that automatic substitution of the formulary drug for the prescribed drug will only occur at the time of dispensing when a prescribing clinician approves of the use of a specific therapeutic interchange protocol for his or her residents in the facilities. The therapeutic interchange is considered void and the originally prescribed medication will be dispensed if the Formulary drug results in an increased price to the facility, third party or patient, unless the interchanged medication is clinically superior. National/Regional Account Representative Name (Print) National/Regional Account Representative Signature Date FAX THIS PAGE TO OMNICARE S FORMULARY COMPLIANCE CENTER FAX NUMBER Other Strategies to Manage Medication Costs SigmaCare: Omnicare s Electronic Medical Records System Order entry with real-time DUR, formulary and prior authorization alerts Alerts non-formulary or non-covered medication for intervention Promotes formulary compliance before medication is ordered Allows prescriber/nursing staff to modify order based on prompts from system 16
17 17

18 Managing Medication Costs: Focus on Available Resources-OMNIVIEW Omniview: # 1 Tool Omniview is a web-based worksite that links our customer and Omnicare employees to common data, such as facility invoices, census information, drug utilization reports, consultant pharmacist reports, resource libraries Omnicare offers the Omniview website to all of its customers at no charge. Value Added, No software fees, no hardware to install 18

19 Omniview Homepage Managing Medication Costs: OMNIVIEW Preview: Pre-Admission Screening Pre-admission medication screening helps identify medication costs and opportunities Identifies TI opportunities and generic substitutions prior to admission maximizing cost savings to the facility Project IV costs over the duration of therapy Preview drug cost as a percentage of revenue based on RUG score and reimbursement Clinical notes and precautionary measures Designate facility team member to review new admission prior to verifying orders with prescriber 19

20 Managing Medication Costs: OMNIVIEW Managing Medication Costs: Focus on Available Resources-OMNIVIEW Review Drug Utilization Report Review Drug utilization for Med A and Managed Care residents Can be run by month, quarter, or year for facility, region, division or corporation Run by dollars spent, number of transactions, alphabetically or OTC only Click on medication to get detail of resident name, doses, pay plan, prescriber Alphabetical sort quick way to focus on one medication 20

21 Managing Medication Costs: OMNIVIEW Managing Medication Costs: Focus on Available Resources-OMNIVIEW Formulary Statistics Report Compliance report for therapeutic interchange categories Detail of select and non-select medications At facility level can drill down to Rx detail Review monthly Trend quarterly Focus on Therapeutic Interchange Programs with most opportunity 21

22 Formulary Statistics Report: Compliance Formulary Savings Spreadsheet (Insert name of account) Formulary Savings Table Based on 1st Quarter 2009 Facility Invoice Data Percentage of Number of Omnicare's Omnicare's Total Number Transactions for Average Current Current Potential Potential Uncaptured Uncaptured Drug Class/ Selected Selected of Transactions Selected Savings Quarterly Annual Average Average Opportunity Opportunity Product Agent Agent in Category Agent Per Change* Savings Savings Quarterly Savings Annual Savings Quarterly Annually BPH finasteride #DIV/0! 0 0 $47.40 $0.00 $0.00 $0.00 $0.00 $0.00 $ alpha reductase ACE Inhibitors lisinopril #DIV/0! 0 0 $9.14 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 Alpha-2 Agonist Ophthalmic brimonidine #DIV/0! 0 0 $32.76 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 (5ml) Topical Anti-Infective Mupirocin #DIV/0! 0 0 $37.23 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 Angiotensin Receptor Blockers Diovan #DIV/0! 0 0 $4.50 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 (Cozaar or Hyzaar) Diovan HCT Alzheimers Aricept #DIV/0! 0 0 $24.11 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 Cholinesterase Inhibitor (Exelon capsules only) Albuterol HFA Ventolin HFA #DIV/0! 0 0 $7.54 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 (Proventil HFA, ProAir HFA,Xopenex) Inhaled Beta Agonists albuterol solution #DIV/0! 0 0 $81.37 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 (Xopenex solution) Fenofibrates fenofibrate #DIV/0! 0 0 $64.51 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 (Tricor & Antara) Insomnia zolpidem #DIV/0! 0 0 $46.29 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 (excludes temazepam & Rozerem) (15 day supply) Nasal fluticasone #DIV/0! 0 0 $29.32 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 Corticosteriod Prostaglandin Analog-ophthalmic Travatan #DIV/0! 0 0 $5.37 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 (Lumigan & Xalatan) Osteoporosis Nasal Spray Fortical #DIV/0! 0 0 $16.79 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 (Miacalcin & Calcitonin-salmon) Pain Management meloxicam #DIV/0! 0 0 $83.21 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 (Celebrex only) Proton Pump Inhibitors omeprazole #DIV/0! 0 0 $18.33 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 (7 day protocol) (Prilosec OTC excluded) SNRI Antidepressant venlafaxine ER #DIV/0! 0 0 $21.88 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 (Effexor XR) Urinary Incontinence oxybutynin ER #DIV/0! 0 0 $56.30 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 (excludes oxybutynin IR & Sanctura) Current Total Quarterly Savings: $0.00 Current Total Annual Savings: $0.00 Potential Total Quarterly Savings: $0.00 Figures based on facility invoice data, primarily representing MCR, Mgd Care & other Third Party paytypes assigned to account Potential Total Annual Savings: $0.00 *-based on either weighted average or AWP difference Uncaptured Opportunity Quarterly*: $0.00 Uncaptured Opportunity Annually*: *Opportunities defined as 70% of uncaptured savings, based on known clinical variability $
23 Omnicare s Role We can assist your facility in: Formulary Management strategies Insuring Appropriate Medication Utilization Implementing cost savings strategies Implementing and monitoring quality measures to insure quality of care Providing education and tools to insure compliance with state and federal regulations Managing Medication Costs: Your Consultant Pharmacist s Role Resource to your facility Discuss/Identify key focus areas during entrance conference/review during exit Focus on high risk, high cost, and highly utilized medication Target inappropriate medication usage and polypharmacy Implement new tools to improve the quality of care of your residents 23
Cost Effectiveness Recommendations For Kentucky Retirement Systems MTM Plan 2011
 Medication Tier 2 options Tier 1 options Nexium- Tier 3 Aciphex Lansoprazole Omeprazole Pantoprazole Crestor- Tier 3 Lipitor Simvastatin Vytorin- Tier 3 Atacand- Tier 3 Avapro Benicar Cozaar Micardis Tevetan
Medication Tier 2 options Tier 1 options Nexium- Tier 3 Aciphex Lansoprazole Omeprazole Pantoprazole Crestor- Tier 3 Lipitor Simvastatin Vytorin- Tier 3 Atacand- Tier 3 Avapro Benicar Cozaar Micardis Tevetan
ADHD STIMULANTS-S(SHC)
") Step Therapy Simply Health Care 2014 Formulary ID: 14406 Version: 14 Last Updated: 08/01/2014 ADHD STIMULANTS-S(SHC) Daytrana Focalin Xr Strattera Patient needs to have a paid claim for one Step 1 drug
Step Therapy Simply Health Care 2014 Formulary ID: 14406 Version: 14 Last Updated: 08/01/2014 ADHD STIMULANTS-S(SHC) Daytrana Focalin Xr Strattera Patient needs to have a paid claim for one Step 1 drug
STEP THERAPY ALGORITHMS PUP Select Formulary
 The Step Therapy drug will be dispensed if the drug has been dispensed within 120 days of current fill or if alternative (Step 1) drugs have been used first. If the member s prescription claim fails the
The Step Therapy drug will be dispensed if the drug has been dispensed within 120 days of current fill or if alternative (Step 1) drugs have been used first. If the member s prescription claim fails the
Hospice High Dollar Medications and Possible Alternatives
 Hospice High Dollar Medications and Possible Alternatives Ly M. Dang, PharmD LDang@HospicePharmacySolutions.com Director of Pharmacy Operations Hospice Pharmacy Solutions Topics of Discussion Hospice Coverage
Hospice High Dollar Medications and Possible Alternatives Ly M. Dang, PharmD LDang@HospicePharmacySolutions.com Director of Pharmacy Operations Hospice Pharmacy Solutions Topics of Discussion Hospice Coverage
Generics. Lead with. P r e s c r i p t i o n S t e p T h e r a p y P r o g r a m
 Lead with Generics P r e s c r i p t i o n S t e p T h e r a p y P r o g r a m WWW.BCBSLA.COM 04HQ3972 5/09 Blue Cross and Blue Shield of Louisiana incorporated as Louisiana Health Service & Indemnity
Lead with Generics P r e s c r i p t i o n S t e p T h e r a p y P r o g r a m WWW.BCBSLA.COM 04HQ3972 5/09 Blue Cross and Blue Shield of Louisiana incorporated as Louisiana Health Service & Indemnity
Generics. Lead with. Prescription Step Therapy Program
 Lead with Generics Prescription Step Therapy Program WWW.BCBSLA.COM 04HQ3972 R11/10 Blue Cross and Blue Shield of Louisiana incorporated as Louisiana Health Service & Indemnity Company GENERIC DRUGS: A
Lead with Generics Prescription Step Therapy Program WWW.BCBSLA.COM 04HQ3972 R11/10 Blue Cross and Blue Shield of Louisiana incorporated as Louisiana Health Service & Indemnity Company GENERIC DRUGS: A
2015 Chinese Community Health Plan Senior Program (HMO) Step Therapy Criteria Last Updated 11/1/2015
 Step Therapy Criteria Last Updated 11/1/2015") 2015 Chinese Community Health Plan Senior Program (HMO) Step Therapy Last Updated 11/1/2015 APLENZIN TAB 174MG, 348MG, 522MG Step Therapy requires trial of bupropion SR or bupropion XL in previous 180
2015 Chinese Community Health Plan Senior Program (HMO) Step Therapy Last Updated 11/1/2015 APLENZIN TAB 174MG, 348MG, 522MG Step Therapy requires trial of bupropion SR or bupropion XL in previous 180
II. Angiotensin Receptor Blockers (ARBs) Drug Class Review
 Drug Class Review") DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE DOD BENEFICIARY ADVISORY PANEL I. Uniform Formulary Review Process Under 10 U.S.C. 1074g, as implemented by 32 C.F.R. 199.21,
DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE DOD BENEFICIARY ADVISORY PANEL I. Uniform Formulary Review Process Under 10 U.S.C. 1074g, as implemented by 32 C.F.R. 199.21,
Drug Class Monograph
 Drug Class Monograph Class: Proton Pump Inhibitors Drugs: Aciphex Sprinkle (rabeprazole), Dexilant (dexlansoprazole), Lansoprazole, Nexium (esomeprazole capsule, esomeprazole granules), Omeprazole, Pantoprazole,
Drug Class Monograph Class: Proton Pump Inhibitors Drugs: Aciphex Sprinkle (rabeprazole), Dexilant (dexlansoprazole), Lansoprazole, Nexium (esomeprazole capsule, esomeprazole granules), Omeprazole, Pantoprazole,
Plan Year CCHP Senior Program (HMO) Step Therapy Criteria (ST)
 Step Therapy Criteria (ST)") Plan Year 2016 CCHP Senior Program (HMO) Step Therapy Criteria (ST) Step Therapy: In some cases, CCHP Senior Program (HMO) requires you to first try certain drugs to treat your medical condition before
Plan Year 2016 CCHP Senior Program (HMO) Step Therapy Criteria (ST) Step Therapy: In some cases, CCHP Senior Program (HMO) requires you to first try certain drugs to treat your medical condition before
Proton Pump Inhibitors. Description
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.01 Subject: Proton Pump Inhibitors Page: 1 of 6 Last Review Date: June 24, 2015 Proton Pump Inhibitors
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.01 Subject: Proton Pump Inhibitors Page: 1 of 6 Last Review Date: June 24, 2015 Proton Pump Inhibitors
Step Therapy Requirements
 An Independent Licensee of the Blue Cross and Blue Shield Association Step Therapy Requirements Effective: 12/01/2017 Updated 11/2017 H0302_2_2014 CMS Accepted 05/05/2014 1 ABILIFY Abilify 10 mg tablet
An Independent Licensee of the Blue Cross and Blue Shield Association Step Therapy Requirements Effective: 12/01/2017 Updated 11/2017 H0302_2_2014 CMS Accepted 05/05/2014 1 ABILIFY Abilify 10 mg tablet
2014 Quantity Limits (QL) Criteria
 Criteria") 2014 Quantity Limits (QL) Criteria Certain drugs covered through your EmblemHealth Medicare HMO/PPO Medicare Plan are covered for only a limited quantity. We do this to ensure compliance with the US Food
2014 Quantity Limits (QL) Criteria Certain drugs covered through your EmblemHealth Medicare HMO/PPO Medicare Plan are covered for only a limited quantity. We do this to ensure compliance with the US Food
Proton Pump Inhibitors (PPIs) (Sherwood Employer Group)
 (Sherwood Employer Group)") Proton Pump Inhibitors (PPIs) (Sherwood Employer Group) BCBSKS will review Prior Authorization requests Prior Authorization Form: https://www.bcbsks.com/customerservice/forms/pdf/priorauth-6058ks-st-ippi.pdf
Proton Pump Inhibitors (PPIs) (Sherwood Employer Group) BCBSKS will review Prior Authorization requests Prior Authorization Form: https://www.bcbsks.com/customerservice/forms/pdf/priorauth-6058ks-st-ippi.pdf
LIGHTENING THE LOAD Reducing pill burden with appropriate discontinuation strategies
 LIGHTENING THE LOAD Reducing pill burden with appropriate discontinuation strategies Disclaimer Statement This presentation is for educational purposes only. It is not intended as legal or professional
LIGHTENING THE LOAD Reducing pill burden with appropriate discontinuation strategies Disclaimer Statement This presentation is for educational purposes only. It is not intended as legal or professional
Proton Pump Inhibitors. Description. Section: Prescription Drugs Effective Date: July 1, 2014
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.09.01 Subject: Proton Pump Inhibitors Page: 1 of 7 Last Review Date: June 12, 2014 Proton Pump Inhibitors
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.09.01 Subject: Proton Pump Inhibitors Page: 1 of 7 Last Review Date: June 12, 2014 Proton Pump Inhibitors
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 PROTON PUMP INHIBITORS, NON-PREFERRED FORMS: ACIPHEX (rabeprazole sodium EC) oral tablet ACIPHEX SPRINKLE (rabeprazole sodium DR) oral capsule ESOMEPRAZOLE STRONTIUM (esomeprazole strontium DR) oral capsule
PROTON PUMP INHIBITORS, NON-PREFERRED FORMS: ACIPHEX (rabeprazole sodium EC) oral tablet ACIPHEX SPRINKLE (rabeprazole sodium DR) oral capsule ESOMEPRAZOLE STRONTIUM (esomeprazole strontium DR) oral capsule
ATYPICAL ANTIPSYCHOTICS
 Step Therapy CareOregon 2018 Last Updated: 07/27/2018 ATYPICAL ANTIPSYCHOTICS Fanapt Fanapt Titration Pack Paliperidone Er Vraylar The following criteria applies to members who newly start on the drug:
Step Therapy CareOregon 2018 Last Updated: 07/27/2018 ATYPICAL ANTIPSYCHOTICS Fanapt Fanapt Titration Pack Paliperidone Er Vraylar The following criteria applies to members who newly start on the drug:
Oregon Health Plan prescription benefit updates
 Oregon Health Plan prescription benefit updates EOCCO s prescription program is a pharmacy benefit that offers members a choice of safe and effective medication treatments. The program also helps you save
Oregon Health Plan prescription benefit updates EOCCO s prescription program is a pharmacy benefit that offers members a choice of safe and effective medication treatments. The program also helps you save
ARBS MEDICATION(S) SUBJECT TO STEP THERAPY DIOVAN HCT MG TAB, DIOVAN HCT MG TABLET
 SUBJECT TO STEP THERAPY DIOVAN HCT MG TAB, DIOVAN HCT MG TABLET") ARBS DIOVAN HCT 160-12.5 MG TAB, DIOVAN HCT 80-12.5 MG TABLET 30-day trial of a Step 1 drug in the previous 120 days is required. Step 1 Drugs: Losartan, Losartan/HCTZ PAGE 1 LAST UPDATED 05/2016 BILE
ARBS DIOVAN HCT 160-12.5 MG TAB, DIOVAN HCT 80-12.5 MG TABLET 30-day trial of a Step 1 drug in the previous 120 days is required. Step 1 Drugs: Losartan, Losartan/HCTZ PAGE 1 LAST UPDATED 05/2016 BILE
Calgary Long Term Care Formulary
 Page 1 of 14 Calgary Long Term Care Formulary Pharmacy & Therapeutics Highlights https://www.albertahealthservices.ca/info/page4071.aspx Page 2 of 14 Contents... 3 Formulary Changes (Additions, Changes,
Page 1 of 14 Calgary Long Term Care Formulary Pharmacy & Therapeutics Highlights https://www.albertahealthservices.ca/info/page4071.aspx Page 2 of 14 Contents... 3 Formulary Changes (Additions, Changes,
5-ASA. Products Affected Dipentum 250 mg capsule. Details. Lialda 1.2 gram tablet,delayed release
 5-ASA Dipentum 250 mg capsule Lialda 1.2 gram tablet,delayed release You are required to have previous therapy with balsalazide, Delzicol, Apriso, or Asacol HD before we will cover Lialda or Dipentum.
5-ASA Dipentum 250 mg capsule Lialda 1.2 gram tablet,delayed release You are required to have previous therapy with balsalazide, Delzicol, Apriso, or Asacol HD before we will cover Lialda or Dipentum.
ALLERGIC RHINITIS-NASAL
 ALLERGIC RHINITIS-NASAL FLUNISOLIDE Patient needs to have paid claims for any one of the following Step 1 drugs: NasaCort OTC, fluticasone Rx, fluticasone OTC, Budesonide OTC. Prior to filling the Step
ALLERGIC RHINITIS-NASAL FLUNISOLIDE Patient needs to have paid claims for any one of the following Step 1 drugs: NasaCort OTC, fluticasone Rx, fluticasone OTC, Budesonide OTC. Prior to filling the Step
These medications will require preauthorization (PA) for HMSA Medicare Part D members.
 for HMSA Medicare Part D members.") Medicare Part D November 2014 CHANGES TO HMSA S MEDICARE FORMULARY As part of HMSA s ongoing efforts to provide our members a sustainable and affordable health plan option, it s necessary to make adjustments
Medicare Part D November 2014 CHANGES TO HMSA S MEDICARE FORMULARY As part of HMSA s ongoing efforts to provide our members a sustainable and affordable health plan option, it s necessary to make adjustments
BLUE SHIELD OF CALIFORNIA JUNE 2016 PLUS DRUG FORMULARY CHANGES
 BLUE SHIELD OF CALIFORNIA JUNE 2016 PLUS DRUG FORMULARY CHANGES Blue Shield is committed to covering safe, effective and affordable medications, so we regularly review and update our drug formularies.
BLUE SHIELD OF CALIFORNIA JUNE 2016 PLUS DRUG FORMULARY CHANGES Blue Shield is committed to covering safe, effective and affordable medications, so we regularly review and update our drug formularies.
DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL
 DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL I. Uniform Formulary Review Process Under 10 U.S.C. 1074g, as implemented by 32
DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL I. Uniform Formulary Review Process Under 10 U.S.C. 1074g, as implemented by 32
Proton Pump Inhibitors Drug Class Prior Authorization Protocol
 Proton Pump Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review
Proton Pump Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review
Great Low Cost in SNF-NF Jabbar Fazeli, MD Maine Medical Directors Association
 Great Care @ Low Cost in SNF-NF Jabbar Fazeli, MD Maine Medical Directors Association Principles Best interest of the patient (SNF) and resident (NF) comes first. Lowest cost to achieve the same care.
Great Care @ Low Cost in SNF-NF Jabbar Fazeli, MD Maine Medical Directors Association Principles Best interest of the patient (SNF) and resident (NF) comes first. Lowest cost to achieve the same care.
UF Decision Report FY06-07 Beneficiary Advisory Panel 10 Jan 2008
 UF Decision Report FY06-07 Beneficiary Advisory Panel 10 Jan 2008 Promoting high quality, cost effective drug therapy throughout the Military Health System UF Decisions, May 07 Class FY05 rank, total $
UF Decision Report FY06-07 Beneficiary Advisory Panel 10 Jan 2008 Promoting high quality, cost effective drug therapy throughout the Military Health System UF Decisions, May 07 Class FY05 rank, total $
Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist
 Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist") Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist Disclosures I have no actual or potential conflicts of interest to report in relation to this
Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist Disclosures I have no actual or potential conflicts of interest to report in relation to this
Proton Pump Inhibitors
 Market DC Proton Pump Inhibitors Override(s) Prior Authorization Quantity Limit** Approval Duration Preferred PPI: No Prior Authorization required Preferred PPI quantity override: Lifetime Non-Preferred
Market DC Proton Pump Inhibitors Override(s) Prior Authorization Quantity Limit** Approval Duration Preferred PPI: No Prior Authorization required Preferred PPI quantity override: Lifetime Non-Preferred
MAXIMUM ALLOWABLE COST POLICY CHANGES DECEMBER 5, 2016 QUESTIONS AND ANSWERS
 MAXIMUM ALLOWABLE COST POLICY CHANGES DECEMBER 5, 2016 QUESTIONS AND ANSWERS The November 22, 2016 Mid-Year Financial Report referred to changes to drug coverage under the Saskatchewan Drug Plan. What
MAXIMUM ALLOWABLE COST POLICY CHANGES DECEMBER 5, 2016 QUESTIONS AND ANSWERS The November 22, 2016 Mid-Year Financial Report referred to changes to drug coverage under the Saskatchewan Drug Plan. What
Safe, effective, affordable drug choices: online tool for payers and patients.
 Executive summary: Rising healthcare costs and greater access to medical information drive patients to seek options for their drug therapy. The MedAlternatives database by Gold Standard/Elsevier empowers
Executive summary: Rising healthcare costs and greater access to medical information drive patients to seek options for their drug therapy. The MedAlternatives database by Gold Standard/Elsevier empowers
2013 Preferred Drug List An evidence-based pharmacy program that works for you
 2013 Preferred Drug List An evidence-based pharmacy program that works for you What is the Moda Health Preferred Drug Program? The Moda Health Preferred Drug Program is a pharmacy program that is designed
2013 Preferred Drug List An evidence-based pharmacy program that works for you What is the Moda Health Preferred Drug Program? The Moda Health Preferred Drug Program is a pharmacy program that is designed
2013 Preferred Drug List An evidence-based pharmacy program that works for you
 2013 Preferred Drug List An evidence-based pharmacy program that works for you What is the Moda Health Preferred Drug Program? The Moda Health Preferred Drug Program is a pharmacy program that is designed
2013 Preferred Drug List An evidence-based pharmacy program that works for you What is the Moda Health Preferred Drug Program? The Moda Health Preferred Drug Program is a pharmacy program that is designed
2013 Preferred Drug List An evidence-based pharmacy program that works for you
 2013 Preferred Drug List An evidence-based pharmacy program that works for you What is the Moda Health Preferred Drug Program? The Moda Health Preferred Drug Program is a pharmacy program that is designed
2013 Preferred Drug List An evidence-based pharmacy program that works for you What is the Moda Health Preferred Drug Program? The Moda Health Preferred Drug Program is a pharmacy program that is designed
Relative Cost/Month. Less than $10. Loratadine Liquid* $10-$15 Cetirizine liquid 1mg/mL*
 Allergy Chlorpheniramine Tablet* Diphenhydramine Tablet* Diphenhydramine Liquid* Loratadine Tablet* Cetirizine Tablet* Loratadine 10mg ODT* Less than $10 Loratadine Liquid* $10-$15 Cetirizine liquid 1mg/mL*
Allergy Chlorpheniramine Tablet* Diphenhydramine Tablet* Diphenhydramine Liquid* Loratadine Tablet* Cetirizine Tablet* Loratadine 10mg ODT* Less than $10 Loratadine Liquid* $10-$15 Cetirizine liquid 1mg/mL*
Step Therapy Requirements. Effective: 11/01/2018
 Effective: 11/01/2018 Updated 10/2018 ANTIDEPRESSANTS Sharp Health Plan (HMO) TRINTELLIX 10 MG TABLET TRINTELLIX 20 MG TABLET TRINTELLIX 5 MG TABLET VIIBRYD 10 MG (7)-20 MG (23) TABLETS IN A DOSE PACK
Effective: 11/01/2018 Updated 10/2018 ANTIDEPRESSANTS Sharp Health Plan (HMO) TRINTELLIX 10 MG TABLET TRINTELLIX 20 MG TABLET TRINTELLIX 5 MG TABLET VIIBRYD 10 MG (7)-20 MG (23) TABLETS IN A DOSE PACK
Rpts. GENERAL General Schedule (Code GE) Program Prescriber type: Dental Medical Practitioners Nurse practitioners Optometrists Midwives
 Program Prescriber type: Dental Medical Practitioners Nurse practitioners Optometrists Midwives") Esomeprazole 20mg Name, Restriction, Manner of esomeprazole 20 mg enteric tablet, 30 (8886Q) (029W) Gastric ulcer Peptic ulcer Treatment Phase: Initial treatment The therapy must be for initial treatment
Esomeprazole 20mg Name, Restriction, Manner of esomeprazole 20 mg enteric tablet, 30 (8886Q) (029W) Gastric ulcer Peptic ulcer Treatment Phase: Initial treatment The therapy must be for initial treatment
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: CP.CPA.209 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: CP.CPA.209 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy for important
5-ASA. Products Affected DIPENTUM 250 MG CAPSULE LIALDA 1.2 GRAM TABLET,DELAYED RELEASE. Details
 5-ASA DIPENTUM 250 MG CAPSULE LIALDA 1.2 GRAM TABLET,DELAYED You are required to have previous therapy with balsalazide, Delzicol, Apriso, or Asacol HD before we will cover Lialda or Dipentum. 1 ANTIEMETICS
5-ASA DIPENTUM 250 MG CAPSULE LIALDA 1.2 GRAM TABLET,DELAYED You are required to have previous therapy with balsalazide, Delzicol, Apriso, or Asacol HD before we will cover Lialda or Dipentum. 1 ANTIEMETICS
5-ASA. Products Affected. Details. Dipentum 250 mg capsule. Lialda 1.2 gram tablet,delayed release
 Updated 11/1/17 5-ASA Dipentum 250 mg capsule Lialda 1.2 gram tablet,delayed release You are required to have previous therapy with balsalazide, Delzicol, Apriso, or Asacol HD before we will cover Lialda
Updated 11/1/17 5-ASA Dipentum 250 mg capsule Lialda 1.2 gram tablet,delayed release You are required to have previous therapy with balsalazide, Delzicol, Apriso, or Asacol HD before we will cover Lialda
Date: October 3, 2017 To: Participating Providers From: YourCare Health Plan Provider Relations Subject: 2018 Formulary Changes
 Date: October 3, 2017 To: Participating Providers From: YourCare Health Plan Provider Relations Subject: 2018 Formulary Changes 2018 Formulary-UM Changes What does this mean now, and for 2018? A number
Date: October 3, 2017 To: Participating Providers From: YourCare Health Plan Provider Relations Subject: 2018 Formulary Changes 2018 Formulary-UM Changes What does this mean now, and for 2018? A number
FirstCarolinaCare Insurance Company Step Therapy Requirements
 ANALGESICS, NARCOTICS KADIAN MORPHINE SULFATE ER PRIOR CLAIM FOR MORPHINE SULFATE SUSTAINED ACTION TABLET (MS CONTIN) WITHIN THE PAST 120 DAYS. ANTIBACTERIALS (EENT) BESIVANCE PRIOR CLAIM FOR CIPROFLOXACIN
ANALGESICS, NARCOTICS KADIAN MORPHINE SULFATE ER PRIOR CLAIM FOR MORPHINE SULFATE SUSTAINED ACTION TABLET (MS CONTIN) WITHIN THE PAST 120 DAYS. ANTIBACTERIALS (EENT) BESIVANCE PRIOR CLAIM FOR CIPROFLOXACIN
Step Therapy Requirements. Effective: 05/01/2018
 Step Therapy Requirements Effective: 05/01/2018 ANTIDEPRESSANTS TRINTELLIX 10 MG TABLET TRINTELLIX 20 MG TABLET TRINTELLIX 5 MG TABLET VIIBRYD 10 MG (7)-20 MG (23) TABLETS IN A DOSE PACK VIIBRYD 10 MG
Step Therapy Requirements Effective: 05/01/2018 ANTIDEPRESSANTS TRINTELLIX 10 MG TABLET TRINTELLIX 20 MG TABLET TRINTELLIX 5 MG TABLET VIIBRYD 10 MG (7)-20 MG (23) TABLETS IN A DOSE PACK VIIBRYD 10 MG
ANTIDEPRESSANTS. Details. dose pack Viibryd 10 mg tablet Viibryd 20 mg tablet Viibryd 40 mg tablet. Criteria
 ANTIDEPRESSANTS Trintellix 10 mg tablet Trintellix 20 mg tablet Trintellix 5 mg tablet Viibryd 10 mg (7)-20 mg (23) tablets in a dose pack Viibryd 10 mg tablet Viibryd 20 mg tablet Viibryd 40 mg tablet
ANTIDEPRESSANTS Trintellix 10 mg tablet Trintellix 20 mg tablet Trintellix 5 mg tablet Viibryd 10 mg (7)-20 mg (23) tablets in a dose pack Viibryd 10 mg tablet Viibryd 20 mg tablet Viibryd 40 mg tablet
Berkshire Allergy & Asthma Center 2210 Ridgewood Road, Suite 100 Wyomissing, PA (610)
") Berkshire Allergy & Asthma Center 2210 Ridgewood Road, Suite 100 Wyomissing, PA 19610 (610) 372-0502 It is with pleasure that we welcome you as a new patient to Berkshire Allergy & Asthma Center, a division
Berkshire Allergy & Asthma Center 2210 Ridgewood Road, Suite 100 Wyomissing, PA 19610 (610) 372-0502 It is with pleasure that we welcome you as a new patient to Berkshire Allergy & Asthma Center, a division
2017 Step Therapy (ST) Criteria
 Criteria") 2017 Step Therapy (ST) Some drugs require step therapy pre-approval. This means that your doctor must have you first try a different drug to treat your medical condition before we will cover a drug that
2017 Step Therapy (ST) Some drugs require step therapy pre-approval. This means that your doctor must have you first try a different drug to treat your medical condition before we will cover a drug that
Drugs That Require Step Therapy (ST) Step Therapy Medications
 Step Therapy Medications") Drugs That Require Step Therapy (ST) In some cases, BlueShield of Northeastern New York requires you to first try certain drugs to treat your medical condition before we will cover another drug for that
Drugs That Require Step Therapy (ST) In some cases, BlueShield of Northeastern New York requires you to first try certain drugs to treat your medical condition before we will cover another drug for that
Pharmacy Costs: Can I Make a Difference?
 Pharmacy Costs: Can I Make a Difference? Pharmaceutical Market Dynamics What is driving Rx cost up? No New Blockbusters Patent Expirations OTC Market Dynamics Availability Pharmaceutical Companies Unfortunately,
Pharmacy Costs: Can I Make a Difference? Pharmaceutical Market Dynamics What is driving Rx cost up? No New Blockbusters Patent Expirations OTC Market Dynamics Availability Pharmaceutical Companies Unfortunately,
Part D Pharmacy. An Independent Licensee of the Blue Cross Blue Shield Association ( )
") Part D Pharmacy 1 An Independent Licensee of the Blue Cross Blue Shield Association 044507 (12-21-2017) New MA pharmacy partner We ve selected CVS Caremark to manage our part D pharmacy benefits Providence
Part D Pharmacy 1 An Independent Licensee of the Blue Cross Blue Shield Association 044507 (12-21-2017) New MA pharmacy partner We ve selected CVS Caremark to manage our part D pharmacy benefits Providence
2018 Step Therapy (ST) Criteria
 Criteria") 2018 Step Therapy (ST) Some drugs require step therapy pre-approval. This means that your doctor must have you first try a different drug to treat your medical condition before we will cover a drug that
2018 Step Therapy (ST) Some drugs require step therapy pre-approval. This means that your doctor must have you first try a different drug to treat your medical condition before we will cover a drug that
Drug Utilization Review & Cost Reduction Strategies. Esther Liu, PharmD, MSIA, CGP Clinical Pharmacist Outcome Resources
 Drug Utilization Review & Cost Reduction Strategies Esther Liu, PharmD, MSIA, CGP Clinical Pharmacist Outcome Resources Goals and Objectives Define Drug Utilization Reviews Interpret various performance
Drug Utilization Review & Cost Reduction Strategies Esther Liu, PharmD, MSIA, CGP Clinical Pharmacist Outcome Resources Goals and Objectives Define Drug Utilization Reviews Interpret various performance
Medication and Dose 10/04/ /05/2016 Total % Change Since 10/2012 ABILIFY 10 MG TABLET $18.76 $ %
 Table Comparing NADAC prices for select brand name prescription medications on October 4, 2012 and October 5, 2016 to show how much prices have gone up for these medications. These medications increased
Table Comparing NADAC prices for select brand name prescription medications on October 4, 2012 and October 5, 2016 to show how much prices have gone up for these medications. These medications increased
Beneficiary Advisory Panel Handout Uniform Formulary Decisions 23 June 2011
 Beneficiary Advisory Panel Handout Uniform Formulary Decisions 23 June 211 PURPOSE: The purpose of this handout is to provide BAP Committee members with a reference document for the relative clinical effectiveness
Beneficiary Advisory Panel Handout Uniform Formulary Decisions 23 June 211 PURPOSE: The purpose of this handout is to provide BAP Committee members with a reference document for the relative clinical effectiveness
Polypharmacy and Elders. Leslie Baker, Pharm. D., RPh, CGP Sanford Center for Aging
 Polypharmacy and Elders Leslie Baker, Pharm. D., RPh, CGP Sanford Center for Aging Prescription Medication Use In Elders 1 13% of the US population is age 65+ Age 65 years 13% Age 65+ account for 34% of
Polypharmacy and Elders Leslie Baker, Pharm. D., RPh, CGP Sanford Center for Aging Prescription Medication Use In Elders 1 13% of the US population is age 65+ Age 65 years 13% Age 65+ account for 34% of
Step Therapy Criteria 2019
 Step Therapy 2019 For information on obtaining an updated coverage determination or an exception to a coverage determination please call Freedom Health Member Services at 1-800-401-2740 or, for TTY/TDD
Step Therapy 2019 For information on obtaining an updated coverage determination or an exception to a coverage determination please call Freedom Health Member Services at 1-800-401-2740 or, for TTY/TDD
Quarterly pharmacy formulary change notice
 Provider Bulletin June 2017 The formulary changes listed in the table below apply to all Anthem HealthKeepers Plus patients. These changes were reviewed and approved at the first quarter Pharmacy and Therapeutics
Provider Bulletin June 2017 The formulary changes listed in the table below apply to all Anthem HealthKeepers Plus patients. These changes were reviewed and approved at the first quarter Pharmacy and Therapeutics
Quarterly pharmacy formulary change notice
 Quarterly pharmacy formulary change notice The formulary changes listed in the table below were reviewed and approved at our second quarter 2018 Pharmacy and Therapeutics Committee meeting. Effective October
Quarterly pharmacy formulary change notice The formulary changes listed in the table below were reviewed and approved at our second quarter 2018 Pharmacy and Therapeutics Committee meeting. Effective October
2017 AlohaCare Advantage Plus Formulary (HMO SNP) Drugs with Step Therapy Requirements
 Drugs with Step Therapy Requirements") 2017 AlohaCare Advantage Plus Formulary (HMO SNP) Drugs with Step Therapy Requirements AlohaCare requires you to first try one drug to treat your medical condition before we will cover another drug for
2017 AlohaCare Advantage Plus Formulary (HMO SNP) Drugs with Step Therapy Requirements AlohaCare requires you to first try one drug to treat your medical condition before we will cover another drug for
Quarterly pharmacy formulary change notice
 Provider Bulletin October 2018 Quarterly pharmacy formulary change notice The formulary changes listed in the table below apply to all Anthem HealthKeepers Plus patients. The changes listed in the table
Provider Bulletin October 2018 Quarterly pharmacy formulary change notice The formulary changes listed in the table below apply to all Anthem HealthKeepers Plus patients. The changes listed in the table
Step Therapy Criteria
 ADCIRCA ADCIRCA Coverage will be provided if the member has filled a prescription for sildenafil (at least a 30 day supply within the past 365 ) ELIDEL 76-F ELIDEL Coverage will be provided if the member
ADCIRCA ADCIRCA Coverage will be provided if the member has filled a prescription for sildenafil (at least a 30 day supply within the past 365 ) ELIDEL 76-F ELIDEL Coverage will be provided if the member
RxBlue 2010 ST Criteria
 RxBlue 2010 ST Criteria ANTIDEPRESSANTS - SARAFEM... 10 FLUOXETINE HCL... 10 SARAFEM... 10 SELFEMRA... 10 ANTIDEPRESSANTS- SSRI, SNRI... 11 CELEXA... 11 CITALOPRAM... 11 CYMBALTA... 11 EFFEXOR XR... 11
RxBlue 2010 ST Criteria ANTIDEPRESSANTS - SARAFEM... 10 FLUOXETINE HCL... 10 SARAFEM... 10 SELFEMRA... 10 ANTIDEPRESSANTS- SSRI, SNRI... 11 CELEXA... 11 CITALOPRAM... 11 CYMBALTA... 11 EFFEXOR XR... 11
Step Therapy Requirements
 An Independent Licensee of the Blue Cross and Blue Shield Association Step Therapy Requirements Effective: 05/01/2018 Updated 4/2018 H0302_2_2014 CMS Accepted 05/05/2014 1 BETA-BLOCKERS BYSTOLIC 10 MG
An Independent Licensee of the Blue Cross and Blue Shield Association Step Therapy Requirements Effective: 05/01/2018 Updated 4/2018 H0302_2_2014 CMS Accepted 05/05/2014 1 BETA-BLOCKERS BYSTOLIC 10 MG
PPIs: Good or Bad? 1. Basics of PPIs. Gastric Acid Basics. Outline. Gastric Acid Basics. Proton Pump Inhibitors (PPI)
") Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
ANTINEOPLASTIC DRUGS CHAPTER 21. Antineoplastic drugs - designed to treat malignancies, now also used to treat diseases with inflammatory component
 ANTINEOPLASTIC DRUGS CHAPTER 21 Antineoplastic drugs - designed to treat malignancies, now also used to treat diseases with inflammatory component Tx of malignancies Antineoplastic drugs: methotrexate
ANTINEOPLASTIC DRUGS CHAPTER 21 Antineoplastic drugs - designed to treat malignancies, now also used to treat diseases with inflammatory component Tx of malignancies Antineoplastic drugs: methotrexate
5-ASA. Products Affected Dipentum 250 mg capsule. Details. Lialda 1.2 gram tablet,delayed release
 5-ASA Dipentum 250 mg capsule Lialda 1.2 gram tablet,delayed release You are required to have previous therapy with balsalazide, Delzicol, Apriso, or Asacol HD before we will cover Lialda or Dipentum.
5-ASA Dipentum 250 mg capsule Lialda 1.2 gram tablet,delayed release You are required to have previous therapy with balsalazide, Delzicol, Apriso, or Asacol HD before we will cover Lialda or Dipentum.
Calgary Long Term Care Formulary
 Page 1 of 10 Calgary Long Term Care Formulary Pharmacy & Therapeutics November 2018 Highlights https://www.albertahealthservices.ca/info/page4071.aspx Page 2 of 10 Contents November 2018... 3 Formulary
Page 1 of 10 Calgary Long Term Care Formulary Pharmacy & Therapeutics November 2018 Highlights https://www.albertahealthservices.ca/info/page4071.aspx Page 2 of 10 Contents November 2018... 3 Formulary
2018 PDP Premier Step Therapy Document September 2018 Y0114_18_33144_I_009
 2018 PDP Premier Step Therapy Document September 2018 Aggrenox Y0114_18_33144_I_009 aspirin 25 mg-dipyridamole 200 mg capsule,ext.release 12 hr multiphase drug may be given. Step 1 Drug(s): clopidigrel.
2018 PDP Premier Step Therapy Document September 2018 Aggrenox Y0114_18_33144_I_009 aspirin 25 mg-dipyridamole 200 mg capsule,ext.release 12 hr multiphase drug may be given. Step 1 Drug(s): clopidigrel.
Guide to the Modernized Reference Drug Program
 Guide to the Modernized Reference Drug Program For prescribers and pharmacists Medical Beneficiary and Pharmaceutical Services Division June 1, 2016 Contents 1 Introduction 1 2 About this Guide 2 3 About
Guide to the Modernized Reference Drug Program For prescribers and pharmacists Medical Beneficiary and Pharmaceutical Services Division June 1, 2016 Contents 1 Introduction 1 2 About this Guide 2 3 About
Quarterly pharmacy formulary change notice
 MEDICAID PROVIDER BULLETIN October 2018 The formulary changes listed in the table below were reviewed and approved at the second-quarter 2018 Pharmacy and Therapeutics Committee meeting. Effective October
MEDICAID PROVIDER BULLETIN October 2018 The formulary changes listed in the table below were reviewed and approved at the second-quarter 2018 Pharmacy and Therapeutics Committee meeting. Effective October
Nexium 24HR. Tools and information for you and your pharmacy team NOW OTC FOR FREQUENT HEARTBURN. Consumer Healthcare Pfizer Inc.
 NOW OTC FOR FREQUENT HEARTBURN w e N Nexium 24HR P H A R M A S S I S T K I T Tools and information for you and your pharmacy team 2014 Pfizer Inc. NXM041468 05/14 Q: What is the indication for Nexium 24HR
NOW OTC FOR FREQUENT HEARTBURN w e N Nexium 24HR P H A R M A S S I S T K I T Tools and information for you and your pharmacy team 2014 Pfizer Inc. NXM041468 05/14 Q: What is the indication for Nexium 24HR
Drugs That Require Step Therapy (ST) Step Therapy Medications
 Step Therapy Medications") Drugs That Require Step Therapy (ST) In some cases, HealthNow New York Inc. requires you to first try certain drugs to treat your medical condition before we will cover another drug for that condition.
Drugs That Require Step Therapy (ST) In some cases, HealthNow New York Inc. requires you to first try certain drugs to treat your medical condition before we will cover another drug for that condition.
All Indiana Medicaid Prescribers and Pharmacy Providers
 P R O V I D E R B U L L E T I N BT200148 NOVEMBER 28, 2001 To: All Indiana Medicaid Prescribers and Pharmacy Providers Subject: Note: The information in this bulletin regarding prior authorization payment
P R O V I D E R B U L L E T I N BT200148 NOVEMBER 28, 2001 To: All Indiana Medicaid Prescribers and Pharmacy Providers Subject: Note: The information in this bulletin regarding prior authorization payment
2014 Preferred Drug List An evidence-based pharmacy program that works for you
 2014 Preferred Drug List An evidence-based pharmacy program that works for you What is the Moda Health Preferred Drug Program? The Moda Health Preferred Drug Program is a pharmacy program that is designed
2014 Preferred Drug List An evidence-based pharmacy program that works for you What is the Moda Health Preferred Drug Program? The Moda Health Preferred Drug Program is a pharmacy program that is designed
Amitriptyline Hydrochloride Heart Health & BP Amlodipine Besylate 5mg Norvasc Antibiotics Amoxicillin 500 mg Amoxil
 School Corp Formulary Antiviral Acyclovir 400mg Zovirax Asthma Advair Diskus Diskus 250/50 Fluticasone/Salmeterol Asthma Albuterol Sulfate 2.5 mg/3 ml Proventil Arthritis and Pain Allendronate Sodium 70
School Corp Formulary Antiviral Acyclovir 400mg Zovirax Asthma Advair Diskus Diskus 250/50 Fluticasone/Salmeterol Asthma Albuterol Sulfate 2.5 mg/3 ml Proventil Arthritis and Pain Allendronate Sodium 70
MARYLAND MEDICAL ASSISTANCE PROGRAM Pharmacy Transmittal No Maryland Pharmacy Assistance Program Transmittal No. 39 February 22, 1999
 1 PT17-99 MARYLAND MEDICAL ASSISTANCE PROGRAM Pharmacy Transmittal No. 160 Maryland Pharmacy Assistance Program Transmittal No. 39 February 22, 1999 TO: FROM: NOTE: RE: Physicians Pharmacists Martin P.
1 PT17-99 MARYLAND MEDICAL ASSISTANCE PROGRAM Pharmacy Transmittal No. 160 Maryland Pharmacy Assistance Program Transmittal No. 39 February 22, 1999 TO: FROM: NOTE: RE: Physicians Pharmacists Martin P.
SmithRx Standard Formulary Step Therapy List
 SmithRx Standard Formulary Step Therapy List Revised: January 27, 2017 The following medications require prior use of at least one other medication for coverage. Please note that any plan-specific customizations
SmithRx Standard Formulary Step Therapy List Revised: January 27, 2017 The following medications require prior use of at least one other medication for coverage. Please note that any plan-specific customizations
Covered vs Non-Covered Medications in Hospice
 Covered vs Non-Covered Medications in Hospice Jim Joyner, PharmD, CGP 1 Hospice Medicare Benefit: Which Drugs Should be Covered? Hospice is responsible for coverage of the drugs considered to be reasonable
Covered vs Non-Covered Medications in Hospice Jim Joyner, PharmD, CGP 1 Hospice Medicare Benefit: Which Drugs Should be Covered? Hospice is responsible for coverage of the drugs considered to be reasonable
ACYCLOVIR OINT (CCHP2017)
") ACYCLOVIR OINT (CCHP2017) acyclovir 5 % topical ointment Step Therapy requires trial of one (1) of the following: oral generic acyclovir, oral generic famciclovir, oral generic valacyclovir. 1 ALPHAGAN
ACYCLOVIR OINT (CCHP2017) acyclovir 5 % topical ointment Step Therapy requires trial of one (1) of the following: oral generic acyclovir, oral generic famciclovir, oral generic valacyclovir. 1 ALPHAGAN
Drugs That Have Quantitiy Limits (QL)
") Drugs That Have Quantitiy Limits (QL) There are Quantity Limits set by your UA Medicare Group Part D Prescription Drug Plan for the drugs listed below. The UA Medicare Group Part D Prescription Drug Plan
Drugs That Have Quantitiy Limits (QL) There are Quantity Limits set by your UA Medicare Group Part D Prescription Drug Plan for the drugs listed below. The UA Medicare Group Part D Prescription Drug Plan
Consultant Pharmacist Report
 Consultant Pharmacist Report Reported in compliance with F-tag 429. Action requested per F-tag 430 **THIS REPORT IS TO BE USED FOR QUALITY IMPROVEMENT PURPOSES ONLY** Patient Name: BOWEN, T Room: A008A
Consultant Pharmacist Report Reported in compliance with F-tag 429. Action requested per F-tag 430 **THIS REPORT IS TO BE USED FOR QUALITY IMPROVEMENT PURPOSES ONLY** Patient Name: BOWEN, T Room: A008A
ACYCLOVIR OINT (CCHP2017)
") ACYCLOVIR OINT (CCHP2017) acyclovir 5 % topical ointment Step Therapy requires trial of one (1) of the following: oral generic acyclovir, oral generic famciclovir, oral generic valacyclovir. 1 ALPHAGAN
ACYCLOVIR OINT (CCHP2017) acyclovir 5 % topical ointment Step Therapy requires trial of one (1) of the following: oral generic acyclovir, oral generic famciclovir, oral generic valacyclovir. 1 ALPHAGAN
Proton Pump Inhibitors:
 Proton Pump Inhibitors: How bad could they be? Andrea Flanagan, Pharm.D. Iowa City VA Medical Center PGY-1 Pharmacy Resident Objectives for Pharmacists At the end of this presentation PHARMACISTS should
Proton Pump Inhibitors: How bad could they be? Andrea Flanagan, Pharm.D. Iowa City VA Medical Center PGY-1 Pharmacy Resident Objectives for Pharmacists At the end of this presentation PHARMACISTS should
MARSHALLTOWN MEDICAL & SURGICAL CENTER Marshalltown, Iowa
 MARSHALLTOWN MEDICAL & SURGICAL CENTER Marshalltown, Iowa PHARMACY POLICY & PROCEDURES Policy Number: 3.26 Subject: Purpose: Policy: Formulary Management through Establishing Guidelines, Policies or Therapeutic
MARSHALLTOWN MEDICAL & SURGICAL CENTER Marshalltown, Iowa PHARMACY POLICY & PROCEDURES Policy Number: 3.26 Subject: Purpose: Policy: Formulary Management through Establishing Guidelines, Policies or Therapeutic
CHICAGO REGIONAL COUNCIL OF CARPENTERS WELFARE FUND RETIREE PRESCRIPTION DRUG BENEFITS October 2013
 CHICAGO REGIONAL COUNCIL OF CARPENTERS WELFARE FUND RETIREE PRESCRIPTION DRUG BENEFITS October 2013 How to Use the Prescription Drug Program The Chicago Regional Council of Carpenters Welfare Fund has
CHICAGO REGIONAL COUNCIL OF CARPENTERS WELFARE FUND RETIREE PRESCRIPTION DRUG BENEFITS October 2013 How to Use the Prescription Drug Program The Chicago Regional Council of Carpenters Welfare Fund has
STEP THERAPY IN MEDICARE PART D
 STEP THERAPY IN MEDICARE PART D Sarkis Kavarian, PharmD Candidate 15 Preceptor Dr. Craig Stern Pro Pharma Pharmaceutical Consultants, Inc. May 1 st, 2015 Objectives Why is this important? Medicare Part
STEP THERAPY IN MEDICARE PART D Sarkis Kavarian, PharmD Candidate 15 Preceptor Dr. Craig Stern Pro Pharma Pharmaceutical Consultants, Inc. May 1 st, 2015 Objectives Why is this important? Medicare Part
Amitriptyline Hydrochloride Heart Health & BP Amlodipine Besylate 5mg Norvasc Antibiotics Amoxicillin 500 mg Amoxil
 Antiviral Acyclovir 400mg Zovirax Asthma Advair Diskus Diskus 250/50 Fluticasone/Salmeterol Asthma Albuterol Sulfate 2.5 mg/3 ml Proventil Arthritis and Pain Allendronate Sodium 70 mg Fosamax Arthritis
Antiviral Acyclovir 400mg Zovirax Asthma Advair Diskus Diskus 250/50 Fluticasone/Salmeterol Asthma Albuterol Sulfate 2.5 mg/3 ml Proventil Arthritis and Pain Allendronate Sodium 70 mg Fosamax Arthritis
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
2013 Step Therapy (ST) Criteria
 Criteria") 2013 Step Therapy (ST) Criteria Some drugs require step therapy pre-approval. This means that your doctor must have you first try a different drug to treat your medical condition before we will cover a
2013 Step Therapy (ST) Criteria Some drugs require step therapy pre-approval. This means that your doctor must have you first try a different drug to treat your medical condition before we will cover a
PHARMACY COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 11/16/17 SECTION: DRUGS LAST REVIEW DATE: 11/16/17 LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 LEVALBUTEROL HFA (levalbuterol tartrate) inhalation aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
LEVALBUTEROL HFA (levalbuterol tartrate) inhalation aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
Drugs That Require Step Therapy (ST) Step Therapy Medications
 Step Therapy Medications") Drugs That Require Step Therapy (ST) In some cases, BlueShield of Northeastern New York requires you to first try certain drugs to treat your medical condition before we will cover another drug for that
Drugs That Require Step Therapy (ST) In some cases, BlueShield of Northeastern New York requires you to first try certain drugs to treat your medical condition before we will cover another drug for that