Bronchiectasis exacerbations; differences and management. Michael Loebinger Royal Brompton Imperial College
|
|
|
- Myron Cummings
- 6 years ago
- Views:
Transcription

1 Bronchiectasis exacerbations; differences and management Michael Loebinger Royal Brompton Imperial College
2 Plan Bronchiectasis background and burden Exacerbation and Management Longer term Management Cases and practical management

3 Bronchiectasis
 1) 1/100000 2) 10/100000 13")
 nobody knows 7) I don t know 0 1 2")
4 What is the prevalence of bronchiectasis in the UK? (x600 for number) 1) 1/ ) 10/ ) 100/ ) 500/ ) 1000/ ) nobody knows 7) I don t know
5 Prevalence What is the prevalence of bronchiectasis in the UK? 1 1/ / / / / nobody knows 7 I don t know 52/ adults in US (Weycker clin pulm med 2005) Clinical Practice Research database 500/ (Quint ERJ 2015)

 greater inpatient stay and")
 (Weycker clin")
6 Morbidity and mortality Morbidity 321 clinic attendances from 100pts in 6/12 (Kelly et al E J Int Med 2003) greater inpatient stay and annual cost/pt than other chronic diseases (CCF, DM) (Weycker clin pulm med 2005)
7 Morbidity and mortality Mortality UK 12 yr survival 68.3% (Loebinger et al ERJ 2009) UK 4yr survival 89.8% (Chalmers et al ARJCCM 2014) Spain 5 yr survival 81.2% (Martinez-Garcia et al ERJ 2014) Turkey 4 yr survival 58% (Onen et al Respir med 2007) Increasing mortality (Roberts et al Respir Med 2010)
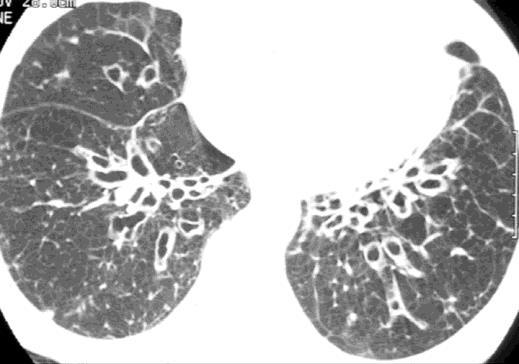
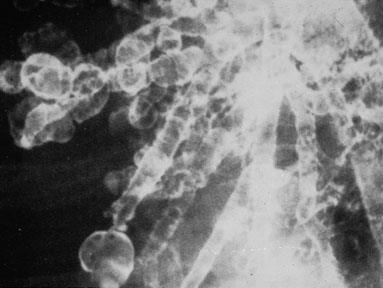
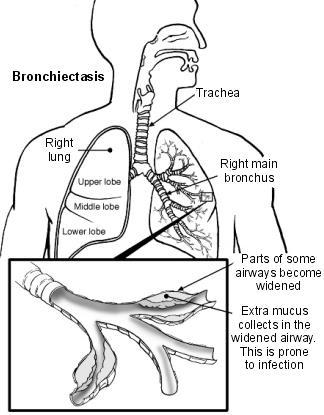
8 Pathophysiology
9 Aetiology P o s t-in fe c tiv e Id io p a th ic C O P D A s th m a Im m u n o d e fic ie n c y A B P A R h e u m a to id a rth ritis P C D G O R D IB D A lp h a -1 -a n titry p s in d e fic ie n c y o th e rs
10 Exacerbation definition Pulmonary Exacerbation in Adults with Bronchiectasis: A Consensus Definition from the First World Bronchiectasis Conference A person with bronchiectasis with a deterioration in three or more of the following key symptoms for at least 48 hours: 1) Cough 2) Sputum volume and / or consistency 3) Sputum purulence 4) Breathlessness and / or exercise tolerance 5) Fatigue and / or malaise 6) Haemoptysis AND a clinician determines a change in bronchiectasis treatment is required*
11 Microbiology and Treatment 14 days of antibiotics (conditional recommendation, very low quality of evidence).

12 Longer term management Treat underlying cause Physiotherapy Mucolytics/ HTS
13 Management airway clearance Treat underlying cause Physiotherapy Mucolytics/ HTS Mannitol Ph3 (Bilton 2014 Thorax) HTS small studies varied results (Kellett dose, /12; Nicholson 12/ )


14 Management long term antibiotics Treat underlying cause Physiotherapy Mucolytics/ HTS Antibiotics Long term Nebulised Oral Cyclical IVs Bacterial load (CFU/ml)



15 141 patients exacerbation 500mg MWF 6/12 then 6/12 no treatment 83 patients exacerbation 250mg od 12/12, 90/7 run out 117 patients exacerbation 400mg bd erythromycin 11/12, 1/12 wash out
16 Management long term inhaled Colistin - exacerb in PP (Haworth et al ARJCCM 2014) AZLI no change in QoLB (Barker et al Lancet Resp Med 2014) Gentamicin - bacterial, exacerbations, QoL (Murray et al 2011 AJRCCM)
17 Management alternative anti-inflammatories Oral CSx No evidence Inhaled CSx 6RCTs Cochrane Some sputum and i0 markers No good evidence Statins LCQ NSAIDs Inhaled indomethacin 25pt Some sputum and SOB No good evidence Development CXCR2 antags / N0 elastase inhibs / PDE4 inhibs

18 Case 1 RL 20 female Well as child Cough at sputum age 14 Referred to local hospital at 17 CT LLL and lingula lobectomy

19 Case 1 RL 20 female Well but relapse few months later 2/3 pot green sputm 4-5 infection/yr 2011 repeat CT scan Referred to RBH IgG <2, A<0.1, M<0.3g/L Normal B and T subsets almost absent memory B cells Diagnosed with CVID Started azithromycin IVIG (when trough 7.2 azithro discontinued) Case 1 underlying diagnosis

20 Case 2 VR 63 female Asthma as child Cough and sputum late 40s Bronchiectasis diagnosed 2009 Idiopathic Pseudomonas Relatively stable 1-2 infection/yr

21 Case 2 VR 63 female Deterioration last couple of years More sputum More SOB More infections Limited effect of antibiotics Treated with steroids Case 2 additional diagnosis


22 Case 3 EM 78 female Well as child, young adult 8 yr history of productive cough 6 infections/yr Widespread bronchiectasis Host defence screen unremarkable Some reflux symptoms PPI Physio review, Acapella, HTS, positive pressure Significant improvement 2 infections/yr Case 3 - optimisation
23 Case 4 JW 53 female Primary Ciliary Dyskinesia Deterioration age 40 Multiple infections - Pseudomonas PSA eradication unsuccessful Colomycin nebulised Some stabilisation but increased infections Increased physiotherapy Addition of azithromycin

24 Case 4 JW 53 female More recently repeated need for antibiotics Needing several admissions for IV therapy per year Anxiety and Depression All management optimised Cyclical intravenous antibiotics Case 4 additional therapies

25 Management - practical Adapted from Loebinger et al 2007
26 Summary Assessment Optimisation Further therapies
CCLI. Bronchiectasis Treatment Antibiotics. Charles Haworth. Physician / Patient Conference, Georgetown University, May 2017
 Physician / Patient Conference, Georgetown University, May 2017 Bronchiectasis Treatment Antibiotics Charles Haworth CCLI Cambridge Centre for Lung Infection Disclosures Educational talks and / or consultancy
Physician / Patient Conference, Georgetown University, May 2017 Bronchiectasis Treatment Antibiotics Charles Haworth CCLI Cambridge Centre for Lung Infection Disclosures Educational talks and / or consultancy
Inhaled Antibiotics in Non-CF. Dr Michael Loebinger Host Defence Unit Royal Brompton Hospital London, United Kingdom
 Inhaled Antibiotics in Non-CF Dr Michael Loebinger Host Defence Unit Royal Brompton Hospital London, United Kingdom Advantages Increased drug concentrations locally Reduced systemic adverse effects Home
Inhaled Antibiotics in Non-CF Dr Michael Loebinger Host Defence Unit Royal Brompton Hospital London, United Kingdom Advantages Increased drug concentrations locally Reduced systemic adverse effects Home
Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Conference Bronchiectasis A Growing Problem
 Conference 2015 Bronchiectasis A Growing Problem Bronchiectasis (in Children) What is it? Why such a concern in NZ? What to look out for? Management Positives? Just a note that the bar for diagnosis, referral
Conference 2015 Bronchiectasis A Growing Problem Bronchiectasis (in Children) What is it? Why such a concern in NZ? What to look out for? Management Positives? Just a note that the bar for diagnosis, referral
NON-CF BRONCHIECTASIS IN ADULTS
 Séminaire de Pathologie Infectieuse Jeudi 25 juin 2008 Cliniques Universitaires UCL de Mont-Godinne, Yvoir NON-CF BRONCHIECTASIS IN ADULTS Dr Robert Wilson Royal Brompton Hospital, London, UK Aetiology
Séminaire de Pathologie Infectieuse Jeudi 25 juin 2008 Cliniques Universitaires UCL de Mont-Godinne, Yvoir NON-CF BRONCHIECTASIS IN ADULTS Dr Robert Wilson Royal Brompton Hospital, London, UK Aetiology
Bronchiectasis Domiciliary treatment. Prof. Adam Hill Royal Infirmary and University of Edinburgh
 Bronchiectasis Domiciliary treatment Prof. Adam Hill Royal Infirmary and University of Edinburgh Plan of talk Background of bronchiectasis Who requires IV antibiotics Domiciliary treatment Results to date.
Bronchiectasis Domiciliary treatment Prof. Adam Hill Royal Infirmary and University of Edinburgh Plan of talk Background of bronchiectasis Who requires IV antibiotics Domiciliary treatment Results to date.
How To Assess Severity and Prognosis
 How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
Bronchiectasis it s effects on the NZ population and what we can do to address this
 NZ Respiratory Conference - 2017 Bronchiectasis it s effects on the NZ population and what we can do to address this Conroy Wong Middlemore Hospital Auckland, NZ Bronchiectasis in NZ and new developments
NZ Respiratory Conference - 2017 Bronchiectasis it s effects on the NZ population and what we can do to address this Conroy Wong Middlemore Hospital Auckland, NZ Bronchiectasis in NZ and new developments
The management of bronchiectasis in Europe
 The management of bronchiectasis in Europe Data from the European Bronchiectasis Registry James Chalmers University of Dundee, UK Presenter disclosures Clinical Trials AstraZeneca, Aradigm corporation,
The management of bronchiectasis in Europe Data from the European Bronchiectasis Registry James Chalmers University of Dundee, UK Presenter disclosures Clinical Trials AstraZeneca, Aradigm corporation,
INHALED ANTIBIOTICS THERAPY IN NON-CF LUNG DISEASE
 INHALED ANTIBIOTICS THERAPY IN NON-CF LUNG DISEASE Hannah Blau MBBS Pulmonary Institute and Graub CF Center SCHNEIDER CHILDREN S MEDICAL CENTER OF ISRAEL Chipap 18 th February 2015 Inhaled antibiotic therapy:
INHALED ANTIBIOTICS THERAPY IN NON-CF LUNG DISEASE Hannah Blau MBBS Pulmonary Institute and Graub CF Center SCHNEIDER CHILDREN S MEDICAL CENTER OF ISRAEL Chipap 18 th February 2015 Inhaled antibiotic therapy:
Management of bronchiectasis in adults
 STATE OF THE ART MANAGEMENT OF BRONCHIECTASIS IN ADULTS Management of bronchiectasis in adults James D. Chalmers 1, Stefano Aliberti 2 and Francesco Blasi 3 Affiliations: 1 Tayside Respiratory Research
STATE OF THE ART MANAGEMENT OF BRONCHIECTASIS IN ADULTS Management of bronchiectasis in adults James D. Chalmers 1, Stefano Aliberti 2 and Francesco Blasi 3 Affiliations: 1 Tayside Respiratory Research
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis. Introduction. Key points
 15 Bronchiectasis Introduction i Key points Patients with bronchiectasis typically have chronic airway infection, punctuated by acute exacerbations and accompanied by progressive airflow obstruction. Bronchiectasis
15 Bronchiectasis Introduction i Key points Patients with bronchiectasis typically have chronic airway infection, punctuated by acute exacerbations and accompanied by progressive airflow obstruction. Bronchiectasis
Bronchiectasis. What is bronchiectasis? What causes bronchiectasis?
 This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
Efficacy of Pseudomonas aeruginosa eradication regimens in bronchiectasis
 Efficacy of Pseudomonas aeruginosa eradication regimens in bronchiectasis Vallières, E., Tumelty, K., Tunney, M. M., Hannah, R., Hewitt, O., Elborn, J. S., & Downey, D. G. (2017). Efficacy of Pseudomonas
Efficacy of Pseudomonas aeruginosa eradication regimens in bronchiectasis Vallières, E., Tumelty, K., Tunney, M. M., Hannah, R., Hewitt, O., Elborn, J. S., & Downey, D. G. (2017). Efficacy of Pseudomonas
Bronchiectasis. Grant Waterer. Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago
 Bronchiectasis Grant Waterer MBBS PhD MBA FRACP FCCP Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago Conflicts of Interest I have
Bronchiectasis Grant Waterer MBBS PhD MBA FRACP FCCP Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago Conflicts of Interest I have
COPD Bronchiectasis Overlap Syndrome.
 COPD Bronchiectasis Overlap Syndrome. John R Hurst 1, J Stuart Elborn 2, and Anthony De Soyza 3 on Behalf of the BRONCH-UK Consortium (D Bilton, J Bradley, JS Brown, J Duckers, F Copeland, A Floto, J Foweraker,
COPD Bronchiectasis Overlap Syndrome. John R Hurst 1, J Stuart Elborn 2, and Anthony De Soyza 3 on Behalf of the BRONCH-UK Consortium (D Bilton, J Bradley, JS Brown, J Duckers, F Copeland, A Floto, J Foweraker,
Prof Neil Barnes. Respiratory and General Medicine London Chest Hospital and The Royal London Hospital
 Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Palliative and Supportive Care in Cystic Fibrosis
 Palliative and Supportive Care in Cystic Fibrosis Dr William Flight Consultant in Respiratory Medicine Oxford Adult Cystic Fibrosis Centre 27 th January 2017 Overview 1. Cystic Fibrosis Clinical Aspects
Palliative and Supportive Care in Cystic Fibrosis Dr William Flight Consultant in Respiratory Medicine Oxford Adult Cystic Fibrosis Centre 27 th January 2017 Overview 1. Cystic Fibrosis Clinical Aspects
Assessing response to treatment of exacerbations of bronchiectasis in adults
 Eur Respir J 2009; 33: 312 317 DOI: 10.1183/09031936.00122508 CopyrightßERS Journals Ltd 2009 Assessing response to treatment of exacerbations of bronchiectasis in adults M.P. Murray, K. Turnbull, S. MacQuarrie
Eur Respir J 2009; 33: 312 317 DOI: 10.1183/09031936.00122508 CopyrightßERS Journals Ltd 2009 Assessing response to treatment of exacerbations of bronchiectasis in adults M.P. Murray, K. Turnbull, S. MacQuarrie
Understanding the heterogeneity of the disease
 Symposium: Bronchiectasis in Europe: an update from the European Bronchiectasis Network (EMBARC) Understanding the heterogeneity of the disease Stefano Aliberti Health Science Department University of
Symposium: Bronchiectasis in Europe: an update from the European Bronchiectasis Network (EMBARC) Understanding the heterogeneity of the disease Stefano Aliberti Health Science Department University of
NON-CYSTIC FIBROSIS BRONCHIECTASIS
 NON-CYSTIC FIBROSIS BRONCHIECTASIS MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the
NON-CYSTIC FIBROSIS BRONCHIECTASIS MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the
Pseudomonas aeruginosa eradication guideline
 SCOTTISH PAEDIATRIC CYSTIC FIBROSIS MCN Pseudomonas aeruginosa eradication guideline Date Created: 27 th June 2013 Date Approved by Steering Group: 30 th May 2014 Date of Review: 31 st May 2016 Lead Author:
SCOTTISH PAEDIATRIC CYSTIC FIBROSIS MCN Pseudomonas aeruginosa eradication guideline Date Created: 27 th June 2013 Date Approved by Steering Group: 30 th May 2014 Date of Review: 31 st May 2016 Lead Author:
Non-cystic fibrosis bronchiectasis
 Non-cystic fibrosis bronchiectasis Maeve P Murray MB ChB MRCP, Clinical Research Fellow Adam T Hill MB ChB MD FRCPE, Consultant Respiratory Physician and Honorary Senior Lecturer Department of Respiratory
Non-cystic fibrosis bronchiectasis Maeve P Murray MB ChB MRCP, Clinical Research Fellow Adam T Hill MB ChB MD FRCPE, Consultant Respiratory Physician and Honorary Senior Lecturer Department of Respiratory
Deep discoveries: the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine
 Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine") Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
Pulmonary Exacerbations:
 Pulmonary Exacerbations: Better Understanding Needed Michael Tracy, MD Clinical Assistant Professor Pediatric Pulmonary CF Pulmonary Exacerbations Definition Importance Causes Treatment Research opportunities
Pulmonary Exacerbations: Better Understanding Needed Michael Tracy, MD Clinical Assistant Professor Pediatric Pulmonary CF Pulmonary Exacerbations Definition Importance Causes Treatment Research opportunities
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Systemic markers of inflammation in stable bronchiectasis
 Eur Respir J 1998; 12: 820 824 DOI: 10.1183/09031936.98.12040820 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1998 European Respiratory Journal ISSN 0903-1936 Systemic markers of inflammation
Eur Respir J 1998; 12: 820 824 DOI: 10.1183/09031936.98.12040820 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1998 European Respiratory Journal ISSN 0903-1936 Systemic markers of inflammation
How do we define pneumonia?
 Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Update on bronchiectasis guidelines. James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK
 Update on bronchiectasis guidelines James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK University of Dundee Bronchiectasis guidelines 2017 2010 2006 2008 2015 2015 Currently valid guidelines
Update on bronchiectasis guidelines James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK University of Dundee Bronchiectasis guidelines 2017 2010 2006 2008 2015 2015 Currently valid guidelines
COPD: From Phenotypes to Endotypes. MeiLan K Han, M.D., M.S. Associate Professor of Medicine University of Michigan, Ann Arbor, MI
 COPD: From Phenotypes to Endotypes MeiLan K Han, M.D., M.S. Associate Professor of Medicine University of Michigan, Ann Arbor, MI Presenter Disclosures MeiLan K. Han Consulting Research support Novartis
COPD: From Phenotypes to Endotypes MeiLan K Han, M.D., M.S. Associate Professor of Medicine University of Michigan, Ann Arbor, MI Presenter Disclosures MeiLan K. Han Consulting Research support Novartis
Effect of sputum bacteriology on the quality of life of patients with bronchiectasis
 Eur Respir J 1997; 10: 1754 1760 DOI: 10.1183/09031936.97.10081754 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1997 European Respiratory Journal ISSN 0903-1936 Effect of sputum bacteriology
Eur Respir J 1997; 10: 1754 1760 DOI: 10.1183/09031936.97.10081754 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1997 European Respiratory Journal ISSN 0903-1936 Effect of sputum bacteriology
Appendix D Clinical specialist statement template
 Appendix D Colistimethate sodium powder and tobramycin powder for inhalation for the treatment of pseudomonas lung infection in cystic fibrosis Thank you for agreeing to give us a statement on your organisation
Appendix D Colistimethate sodium powder and tobramycin powder for inhalation for the treatment of pseudomonas lung infection in cystic fibrosis Thank you for agreeing to give us a statement on your organisation
A Place For Airway Clearance Therapy In Today s Healthcare Environment
 A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
Chronic Cough. Dr Peter George Consultant Respiratory Physician Royal Brompton and Harefield Hospitals
 Chronic Cough Dr Peter George Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Overview Common causes of chronic cough Important diagnoses not to miss How to investigate a cough
Chronic Cough Dr Peter George Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Overview Common causes of chronic cough Important diagnoses not to miss How to investigate a cough
Shared Care Guideline
 Shared Care Guideline Gentamicin for Nebulisation For the long term prophylaxis of chronic lung infections in non CF bronchiectasis Executive Summary Indication Nebulised gentamicin is indicated in patients
Shared Care Guideline Gentamicin for Nebulisation For the long term prophylaxis of chronic lung infections in non CF bronchiectasis Executive Summary Indication Nebulised gentamicin is indicated in patients
National Horizon Scanning Centre. Mannitol dry powder for inhalation (Bronchitol) for cystic fibrosis. April 2008
 for cystic fibrosis. April 2008") Mannitol dry powder for inhalation (Bronchitol) for cystic fibrosis April 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not
Mannitol dry powder for inhalation (Bronchitol) for cystic fibrosis April 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not
SABA: VENTOLIN EVOHALER (SALBUTAMOL) SAMA: ATROVENT IPRATROPIUM. Offer LAMA (discontinue SAMA) OR LABA
 SAMA: ATROVENT IPRATROPIUM. Offer LAMA (discontinue SAMA) OR LABA") COPD GUIDELINES DIAGNOSIS >35 years of age Symptoms of cough, breathlessness, sputum, wheeze, Risk factor (SMOKING) Spirometry (post bronchodilator) FEV1/FVC = 0.7 ENCOURAGE PATIENTS TO BRING INHALERS
COPD GUIDELINES DIAGNOSIS >35 years of age Symptoms of cough, breathlessness, sputum, wheeze, Risk factor (SMOKING) Spirometry (post bronchodilator) FEV1/FVC = 0.7 ENCOURAGE PATIENTS TO BRING INHALERS
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Inhaled antibiotics for stable non-cystic fibrosis bronchiectasis: a systematic review
 ORIGINAL ARTICLE BRONCHIECTASIS Inhaled antibiotics for stable non-cystic fibrosis bronchiectasis: a systematic review Alessandra Monteiro Brodt 1, Elizabeth Stovold 2 and Linjie Zhang 1 Affiliations:
ORIGINAL ARTICLE BRONCHIECTASIS Inhaled antibiotics for stable non-cystic fibrosis bronchiectasis: a systematic review Alessandra Monteiro Brodt 1, Elizabeth Stovold 2 and Linjie Zhang 1 Affiliations:
Management of the Symptomatic PCD
 Management of the Symptomatic PCD Andrew Bush MD FRCP FRCPCH FERS Imperial College & Royal Brompton Hospital a.bush@imperial.ac.uk Conflict of Interest AB has no financial or other COI There will be discussion
Management of the Symptomatic PCD Andrew Bush MD FRCP FRCPCH FERS Imperial College & Royal Brompton Hospital a.bush@imperial.ac.uk Conflict of Interest AB has no financial or other COI There will be discussion
Update on management of respiratory symptoms. Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT
 Update on management of respiratory symptoms Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT Topics The common respiratory symptoms Cough: causes, diagnosis and therapy Update
Update on management of respiratory symptoms Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT Topics The common respiratory symptoms Cough: causes, diagnosis and therapy Update
REFERRAL GUIDELINES RESPIRATORY
 REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines
 Treatment Guidelines") Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Predicting, Preventing and Managing Asthma Exacerbations. Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa
 Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Community COPD Service Protocol
 Community COPD Service Protocol Acknowledgements This protocol is based on the following documents: 1. Chronic obstructive pulmonary disease: Management of chronic obstructive pulmonary disease in adults
Community COPD Service Protocol Acknowledgements This protocol is based on the following documents: 1. Chronic obstructive pulmonary disease: Management of chronic obstructive pulmonary disease in adults
Asthma - An update BTS Asthma Guidelines 2016
 Asthma - An update BTS Asthma Guidelines 2016 Dr Ian Clifton Overview Diagnosis Supported self-management Non-pharmacological management Drugs / inhaled therapy Difficult asthma services Case discussions
Asthma - An update BTS Asthma Guidelines 2016 Dr Ian Clifton Overview Diagnosis Supported self-management Non-pharmacological management Drugs / inhaled therapy Difficult asthma services Case discussions
Bronchiectasis (non-cystic fibrosis), acute exacerbation: antimicrobial prescribing
, acute exacerbation: antimicrobial prescribing") National Institute for Health and Care Excellence Bronchiectasis (non-cystic fibrosis), acute exacerbation: antimicrobial prescribing Evidence review NICE guideline NG117 December 2018 Disclaimer The
National Institute for Health and Care Excellence Bronchiectasis (non-cystic fibrosis), acute exacerbation: antimicrobial prescribing Evidence review NICE guideline NG117 December 2018 Disclaimer The
Research priorities in bronchiectasis: a consensus statement from the EMBARC Clinical Research Collaboration
 ERJ Express. Published on June 10, 2016 as doi: 10.1183/13993003.01888-2015 TASK FORCE REPORT IN PRESS CORRECTED PROOF Research priorities in bronchiectasis: a consensus statement from the EMBARC Clinical
ERJ Express. Published on June 10, 2016 as doi: 10.1183/13993003.01888-2015 TASK FORCE REPORT IN PRESS CORRECTED PROOF Research priorities in bronchiectasis: a consensus statement from the EMBARC Clinical
What is Cystic Fibrosis? CYSTIC FIBROSIS. Genetics of CF
 What is Cystic Fibrosis? CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Chronic, progressive and life limiting autosomal recessive genetic disease characterized by chronic
What is Cystic Fibrosis? CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Chronic, progressive and life limiting autosomal recessive genetic disease characterized by chronic
Physiotherapy in lung disease - top tips for clinicians. Sita Kansagra Specialist Outpatient Physiotherapist
 Physiotherapy in lung disease - top tips for clinicians Sita Kansagra Specialist Outpatient Physiotherapist Aims: Run through current physiotherapy practice Airway clearance Pulmonary rehabilitation Dysfunctional
Physiotherapy in lung disease - top tips for clinicians Sita Kansagra Specialist Outpatient Physiotherapist Aims: Run through current physiotherapy practice Airway clearance Pulmonary rehabilitation Dysfunctional
Northumbria Healthcare NHS Foundation Trust. Bronchiectasis. Issued by Respiratory Medicine
 Northumbria Healthcare NHS Foundation Trust Bronchiectasis Issued by Respiratory Medicine The aim of this booklet is to help you manage your bronchiectasis. It contains information which you should find
Northumbria Healthcare NHS Foundation Trust Bronchiectasis Issued by Respiratory Medicine The aim of this booklet is to help you manage your bronchiectasis. It contains information which you should find
Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom
 Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom 2 BEYOND SYMPTOMS ADDRESSING FUTURE RISK IN ASTHMA South GP CME 2013,
Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom 2 BEYOND SYMPTOMS ADDRESSING FUTURE RISK IN ASTHMA South GP CME 2013,
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX
 Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX Pioneer of Respiratory Medicine 2016 marked 200th anniversary of his
Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX Pioneer of Respiratory Medicine 2016 marked 200th anniversary of his
ASTHMA. Dr Liz Gamble BRI
 ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
The team. Medical staff Dr Adam Hill Vacant post- Dr Lithgow Dr Ruzanna Frangulyan Specialist Trainee
 Bronchiectasis The team Medical staff Dr Adam Hill Vacant post- Dr Lithgow Dr Ruzanna Frangulyan Specialist Trainee Specialist staff Kim Turnbull Denise Gillian Jenny Scott Jo Pentland Research nurses
Bronchiectasis The team Medical staff Dr Adam Hill Vacant post- Dr Lithgow Dr Ruzanna Frangulyan Specialist Trainee Specialist staff Kim Turnbull Denise Gillian Jenny Scott Jo Pentland Research nurses
Patient characteristics Intervention Comparison Length of followup
 ORAL MUCOLYTICS Ref ID: 2511 Bachh AA, Shah NN, Bhargava R et al. Effect oral N- in COPD - A randomised controlled trial. JK Practitioner. 2007; 14(1):12-16. Ref ID: 2511 RCT Single blind; unclear allocation
ORAL MUCOLYTICS Ref ID: 2511 Bachh AA, Shah NN, Bhargava R et al. Effect oral N- in COPD - A randomised controlled trial. JK Practitioner. 2007; 14(1):12-16. Ref ID: 2511 RCT Single blind; unclear allocation
Changes in the management of children with Cystic Fibrosis. Caroline Murphy & Deirdre O Donovan CF Nurses
 Changes in the management of children with Cystic Fibrosis Caroline Murphy & Deirdre O Donovan CF Nurses What Is Cystic Fibrosis? Cystic fibrosis (CF) is an inherited chronic disease that primarily affects
Changes in the management of children with Cystic Fibrosis Caroline Murphy & Deirdre O Donovan CF Nurses What Is Cystic Fibrosis? Cystic fibrosis (CF) is an inherited chronic disease that primarily affects
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Do processing time and storage of sputum influence quantitative bacteriology in bronchiectasis?
 Journal of Medical Microbiology (), 59, 89 833 DOI.99/jmm..6683- Do processing time and storage of sputum influence quantitative bacteriology in bronchiectasis? Maeve P. Murray, Catherine J. Doherty, John
Journal of Medical Microbiology (), 59, 89 833 DOI.99/jmm..6683- Do processing time and storage of sputum influence quantitative bacteriology in bronchiectasis? Maeve P. Murray, Catherine J. Doherty, John
Francesco Blasi Head Respiratory Medicine Section Cardio-Thoracic Department University of Milan, Italy
 COPD EXACERBATIONS Francesco Blasi Head Respiratory Medicine Section Cardio-Thoracic Department University of Milan, Italy COPD OUTCOMES Cazzola M et al. ERJ 2008 COPD AND CARDIOVASCULAR DISEASE Cumulative
COPD EXACERBATIONS Francesco Blasi Head Respiratory Medicine Section Cardio-Thoracic Department University of Milan, Italy COPD OUTCOMES Cazzola M et al. ERJ 2008 COPD AND CARDIOVASCULAR DISEASE Cumulative
COPD and Asthma: Similarities and differences Prof. Peter Barnes
 and Asthma: Similarities and Differences and Asthma: 1 Imperial College Peter Barnes FRS, FMedSci, National Heart & Lung Institute Imperial College, London, UK p.j.barnes@imperial.ac.uk Royal Brompton
and Asthma: Similarities and Differences and Asthma: 1 Imperial College Peter Barnes FRS, FMedSci, National Heart & Lung Institute Imperial College, London, UK p.j.barnes@imperial.ac.uk Royal Brompton
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
The long term effect of inhaled hypertonic saline 6% in non-cystic fibrosis bronchiectasis
 Respiratory Medicine (2012) 106, 661e667 Available online at www.sciencedirect.com journal homepage: www.elsevier.com/locate/rmed The long term effect of inhaled hypertonic saline 6% in non-cystic fibrosis
Respiratory Medicine (2012) 106, 661e667 Available online at www.sciencedirect.com journal homepage: www.elsevier.com/locate/rmed The long term effect of inhaled hypertonic saline 6% in non-cystic fibrosis
Salford COPD Treatment Pathway
 Salford COPD Treatment Pathway Development led by Helen Pyne with Salford Asthma and Respiratory Team (SART) Department Respiratory Medicine Salford Royal NHS Foundation Trust Hope Hospital, Stott Lane,
Salford COPD Treatment Pathway Development led by Helen Pyne with Salford Asthma and Respiratory Team (SART) Department Respiratory Medicine Salford Royal NHS Foundation Trust Hope Hospital, Stott Lane,
Cystic fibrosis: From childhood to adulthood. Eitan Kerem Department of Pediatrics and CF Center Hadassah University Hospital Jerusalem Israel
 Cystic fibrosis: From childhood to adulthood Eitan Kerem Department of Pediatrics and CF Center Hadassah University Hospital Jerusalem Israel Vas deference H 2 O Cl - Na + H 2 O Na + Cl - Cl - Cl -
Cystic fibrosis: From childhood to adulthood Eitan Kerem Department of Pediatrics and CF Center Hadassah University Hospital Jerusalem Israel Vas deference H 2 O Cl - Na + H 2 O Na + Cl - Cl - Cl -
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
What is COPD? COPD Pharmacotherapy. COPD Mortality Is Increasing
 COPD Pharmacotherapy Chronic Bronchitis What is COPD? 75% 17.5% Emphysema Laura C. Feemster, MD, MS Assistant Professor University of Washington Division of Pulmonary & Critical Care April 23,2015 COPD
COPD Pharmacotherapy Chronic Bronchitis What is COPD? 75% 17.5% Emphysema Laura C. Feemster, MD, MS Assistant Professor University of Washington Division of Pulmonary & Critical Care April 23,2015 COPD
Turning Science into Real Life Roflumilast in Clinical Practice. Roland Buhl Pulmonary Department Mainz University Hospital
 Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
A. Service Specifications
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No: 170050S Service Primary Ciliary Dyskinesia Management Service (adults) Commissioner Lead Provider Lead 1. Scope 1.1 Prescribed
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No: 170050S Service Primary Ciliary Dyskinesia Management Service (adults) Commissioner Lead Provider Lead 1. Scope 1.1 Prescribed
CYSTIC FIBROSIS OBJECTIVES NO CONFLICT OF INTEREST TO DISCLOSE
 CYSTIC FIBROSIS Madhu Pendurthi MD MPH Staff Physician, Mercy Hospital Springfield, MO NO CONFLICT OF INTEREST TO DISCLOSE OBJECTIVES Epidemiology of Cystic Fibrosis (CF) Genetic basis and pathophysiology
CYSTIC FIBROSIS Madhu Pendurthi MD MPH Staff Physician, Mercy Hospital Springfield, MO NO CONFLICT OF INTEREST TO DISCLOSE OBJECTIVES Epidemiology of Cystic Fibrosis (CF) Genetic basis and pathophysiology
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Management of bronchiectasis
 P.T. King 1 E. Daviskas 2 1 Dept of Respiratory and Sleep Medicine/Dept of Medicine, Monash Medical Centre, Melbourne, and 2 Dept of Respiratory and Sleep Medicine, Royal Prince Alfred Hospital, Sydney,
P.T. King 1 E. Daviskas 2 1 Dept of Respiratory and Sleep Medicine/Dept of Medicine, Monash Medical Centre, Melbourne, and 2 Dept of Respiratory and Sleep Medicine, Royal Prince Alfred Hospital, Sydney,
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research
 Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Patient-focussed device design - the clinician s perspective. Prof. Mark L. Everard
 Patient-focussed device design - the clinician s perspective Prof. Mark L. Everard User-focussed device design? Patient-focussed device design If it ain t broke don t fix it Effective treatment to control
Patient-focussed device design - the clinician s perspective Prof. Mark L. Everard User-focussed device design? Patient-focussed device design If it ain t broke don t fix it Effective treatment to control
New Medicine Assessment
 September 2015 New Medicine Assessment Colistimethate sodium/colistin sulfomethate sodium (Colomycin ) Non-Cystic Fibrosis in Patients with Bronchiectasis Colonised with Pseudomonas Aeruginosa Recommendation:
September 2015 New Medicine Assessment Colistimethate sodium/colistin sulfomethate sodium (Colomycin ) Non-Cystic Fibrosis in Patients with Bronchiectasis Colonised with Pseudomonas Aeruginosa Recommendation:
A whistle stop tour of Respiratory Medicine and what the RUH & IMPACT offer
 A whistle stop tour of Respiratory Medicine and what the RUH & IMPACT offer Jay Suntharalingam, Respiratory Physician, RUH Claire Bullard, IMPACT Team Leader, Sirona Outline Respiratory 5 year strategy
A whistle stop tour of Respiratory Medicine and what the RUH & IMPACT offer Jay Suntharalingam, Respiratory Physician, RUH Claire Bullard, IMPACT Team Leader, Sirona Outline Respiratory 5 year strategy
Commissioning Brief - Background Information. Sputum colour charts to guide antibiotic self-treatment of acute exacerbation of COPD
 Commissioning Brief - Background Information Sputum colour charts to guide antibiotic self-treatment of acute exacerbation of COPD HTA no 17/128 This background document provides further information to
Commissioning Brief - Background Information Sputum colour charts to guide antibiotic self-treatment of acute exacerbation of COPD HTA no 17/128 This background document provides further information to
Chronic productive cough: An approach to management
 Chronic productive cough: An approach to management Key Points Conditions most likely to cause chronic productive cough outlined. Epidemiology, clinical presentation, pathology and treatment of these conditions
Chronic productive cough: An approach to management Key Points Conditions most likely to cause chronic productive cough outlined. Epidemiology, clinical presentation, pathology and treatment of these conditions
Acute NIV in COPD and what happens next. Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital
 Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
LRI Children s Hospital
 Title: Prescribing in Cystic Fibrosis Page 1 of 10 LRI Children s Hospital Prescribing in Cystic Fibrosis Staff relevant to: Clinical staff working within the UHL Children s Hospital. Team & AWP approval
Title: Prescribing in Cystic Fibrosis Page 1 of 10 LRI Children s Hospital Prescribing in Cystic Fibrosis Staff relevant to: Clinical staff working within the UHL Children s Hospital. Team & AWP approval
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Airway Vista Background
 Airway Vista 2013 Chronic Obstructive Airway Diseases Symposium Asan Medical Center, Seoul, South Korea When Should Macrolide Antibiotics be Prescribed to Prevent COPD Exacerbations in Usual Clinical Practice?
Airway Vista 2013 Chronic Obstructive Airway Diseases Symposium Asan Medical Center, Seoul, South Korea When Should Macrolide Antibiotics be Prescribed to Prevent COPD Exacerbations in Usual Clinical Practice?
Happy Wheezer/Happy Parent/ Happy Doctor (?)
") Happy Wheezer/Happy Parent/ Happy Doctor (?) Andrew Bush MD FRCP FRCPCH FERS Imperial College & Royal Brompton Hospital a.bush@imperial.ac.uk Conflict of Interest AB has no financial or other COI There
Happy Wheezer/Happy Parent/ Happy Doctor (?) Andrew Bush MD FRCP FRCPCH FERS Imperial College & Royal Brompton Hospital a.bush@imperial.ac.uk Conflict of Interest AB has no financial or other COI There
Journal Club The ELITE Trial. Sandra Katalinic, Pharmacy Resident University Hospital of Northern British Columbia April 28, 2010
 Journal Club The ELITE Trial Sandra Katalinic, Pharmacy Resident University Hospital of Northern British Columbia April 28, 2010 Overview Journal article Title, journal, authors, funding Abstract Introduction
Journal Club The ELITE Trial Sandra Katalinic, Pharmacy Resident University Hospital of Northern British Columbia April 28, 2010 Overview Journal article Title, journal, authors, funding Abstract Introduction
THE WINSTON CHURCHILL MEMORIAL TRUST OF AUSTRALIA. Report by Jamie Wood BSc. (Physiotherapy) Churchill Fellow
 Churchill Fellow") THE WINSTON CHURCHILL MEMORIAL TRUST OF AUSTRALIA Report by Jamie Wood BSc. (Physiotherapy) 2004 2010 Churchill Fellow To study physiotherapy service and techniques for people with cystic fibrosis and
THE WINSTON CHURCHILL MEMORIAL TRUST OF AUSTRALIA Report by Jamie Wood BSc. (Physiotherapy) 2004 2010 Churchill Fellow To study physiotherapy service and techniques for people with cystic fibrosis and
OPAT FOR INFECTION IN BRONCHIECTASIS
 OPAT FOR INFECTION IN BRONCHIECTASIS AN AUDIT EVALUATING THE USAGE OF OUTPATIENT ANTIBIOTIC THERAPY FOR INFECTIVE EXACERBATIONS OF BRONCHIECTASIS AGAINST CURRENT BRITISH THORACIC SOCIETY GUIDELINES Dr
OPAT FOR INFECTION IN BRONCHIECTASIS AN AUDIT EVALUATING THE USAGE OF OUTPATIENT ANTIBIOTIC THERAPY FOR INFECTIVE EXACERBATIONS OF BRONCHIECTASIS AGAINST CURRENT BRITISH THORACIC SOCIETY GUIDELINES Dr
the potentially harmful nature of these secretions3 s even when given in the apparently stable clinical state.
 Thorax 1986;41:559-65 Short term response of patients with bronchiectasis to treatment with amoxycillin given in standard or high doses orally or by inhalation SL HILL, HM MORRISON, D BURNETT, RA STOCKLEY
Thorax 1986;41:559-65 Short term response of patients with bronchiectasis to treatment with amoxycillin given in standard or high doses orally or by inhalation SL HILL, HM MORRISON, D BURNETT, RA STOCKLEY
Exacerbations. Ronald Dahl, Aarhus University Hospital, Denmark
 1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
Acapella versus usual airway clearance during acute exacerbation in bronchiectasis: a randomized crossover trial
 Chronic Respiratory Disease 2007; 4: 67 74 http://crd.sagepub.com ORIGINAL PAPER Acapella versus usual airway clearance during acute exacerbation in bronchiectasis: a randomized crossover trial JE Patterson,
Chronic Respiratory Disease 2007; 4: 67 74 http://crd.sagepub.com ORIGINAL PAPER Acapella versus usual airway clearance during acute exacerbation in bronchiectasis: a randomized crossover trial JE Patterson,
Clinical Commissioning Policy: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages)
") Clinical Commissioning Policy: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages) Reference: NHS England: 16029/P NHS England INFORMATION READER BOX Directorate Medical Operations and
Clinical Commissioning Policy: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages) Reference: NHS England: 16029/P NHS England INFORMATION READER BOX Directorate Medical Operations and
Aboriginal lung health and lung function. Graham Hall Telethon Kids Institute and Curtin University
 Aboriginal lung health and lung function Graham Hall Telethon Kids Institute and Curtin University Why Lung function? Lung function underpins clinical respiratory medicine, vital to: diagnosis of lung
Aboriginal lung health and lung function Graham Hall Telethon Kids Institute and Curtin University Why Lung function? Lung function underpins clinical respiratory medicine, vital to: diagnosis of lung
COPD EXACERBATIONS AND HOSPITAL ADMISSIONS HOW CAN WE PREVENT THEM? Wisia Wedzicha National Heart and Lung Institute, Imperial College London, UK
 COPD EXACERBATIONS AND HOSPITAL ADMISSIONS HOW CAN WE PREVENT THEM? Wisia Wedzicha National Heart and Lung Institute, Imperial College London, UK Presenter Disclosures Wisia Wedzicha All disclosures prior
COPD EXACERBATIONS AND HOSPITAL ADMISSIONS HOW CAN WE PREVENT THEM? Wisia Wedzicha National Heart and Lung Institute, Imperial College London, UK Presenter Disclosures Wisia Wedzicha All disclosures prior
Marcos I. Restrepo, MD, MSc, FCCP
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
The Objective Assessment of Cough Frequency in Bronchiectasis
 Lung (2017) 195:575 585 DOI 10.1007/s00408-017-0038-x COUGH The Objective Assessment of Cough Frequency in Bronchiectasis Arietta Spinou 1 Kai K. Lee 2 Aish Sinha 1 Caroline Elston 2 Michael R. Loebinger
Lung (2017) 195:575 585 DOI 10.1007/s00408-017-0038-x COUGH The Objective Assessment of Cough Frequency in Bronchiectasis Arietta Spinou 1 Kai K. Lee 2 Aish Sinha 1 Caroline Elston 2 Michael R. Loebinger
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Clinical Commissioning Policy Proposition: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages)
") Clinical Commissioning Policy Proposition: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages) Reference: NHS England E03X05/01 Information Reader Box (IRB) to be inserted on inside
Clinical Commissioning Policy Proposition: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages) Reference: NHS England E03X05/01 Information Reader Box (IRB) to be inserted on inside