Methacholine versus Mannitol Challenge in the Evaluation of Asthma
|
|
|
- Luke Francis
- 6 years ago
- Views:
Transcription

1 Methacholine versus Mannitol Challenge in the Evaluation of Asthma AAAAI San Antonio Texas February 25 th 2013 Sandra D Anderson PhD, DSc Clinical Professor Royal Prince Alfred Hospital, Camperdown John D Brannan PhD Hospital Scientist Westmead Hospital, Westmead NSW AUSTRALIA sandra.anderson@sydney.edu.au
2 AAAAI Annual Scientific meeting Feb 25 th 2013 Methacholine vs. Mannitol Challenge in the Evaluation of Asthma Monday, February 25, 2013: 4:45 PM-6:00 PM 1.25 CME/ 1.50 CE Moderator: Hee-Bom Moon, MD PhD Primary Panelists: Louis-Philippe Boulet, MD Catherine Lemiere, MD Sandra D. Anderson, PhD DSc Learning Objectives: Compare positive and negative predictive values of methacholine and mannitol inahalation tests Evaluate methacholine and mannitol as potential test for monitoring asthma treatment
3 Conflict of interest Dr Sandra Anderson is the Inventor on the patent that cover these applications for mannitol The patent is owned by her employer SSWAHS The rights to commercialise the intellectual property are licensed to Pharmaxis Ltd Dr Anderson purchased her own shares on the open market and holds no options. Dr Anderson is a consultant to Pharmaxis Ltd Dr Anderson receives a 10% share of the royalties paid to SSWAHS
4 Q: Why do we use methacholine and mannitol challenge in the evaluation of Asthma? Performing the appropriate bronchial challenge test by using either a direct (methacholine) or an indirect (mannitol) stimulus to identify airway hyperresponsiveness (AHR) reduces the possibility of over and under diagnosis of asthma based on history and symptoms.
5 Q: When do we need to know about airway hyperresponsivness? Upon presentation of a person with symptoms suggestive of asthma but with normal or near to normal lung function and doubt about the diagnosis of asthma In a person entering an occupation or recreational activity where AHR could be a problem e.g. SCUBA diving In a person well-controlled on treatment for a long period in whom it may be useful to back titrate treatment e.g. the dose of steroid Following exposure to an occupational irritant or allergen that has induced symptoms of asthma
6 Q: What are the types of Bronchial Challenge Tests that are used to evaluate the airway hyperresponsivness of asthma? DIRECT challenge test: e.g. methacholine The agent is administered and acts on a specific receptor on the bronchial smooth muscle causing it to contract and the airways to narrow. A positive test identifies airway hyperresponsiveness consistent with asthma or with airway injury or airway remodeling. INDIRECT challenge test: e.g. mannitol Indirect challenges act by causing the release of endogenous mediators that cause the airway smooth muscle to contract, with or without effect in inducing microvascular leakage. Joos GF et al. ERS Task Force. Eur Respir J 2003; 21: AAAAI 2013 #4809
7 Q: Why do we need to know about airway hyperresponsiveness? In a person with normal lung function, AHR to an indirect acting stimulus such as mannitol, is consistent with the presence of airway inflammation. The inflammation associated with response to an indirect stimulus involves the mast cell with or without sputum eosinophilia The number of these cells & concentration of mediators of bronchoconstriction are reduced with treatment with inhaled corticosteroids & AHR to exercise or mannitol is reduced or even resolved.
8 Q: What is the source of the mediators that cause Bronchial Smooth Muscle to contract? Mast cells Allergen Increase in osmolarity Indirect means the bronchoconstricting stimulus comes from cells e.g.mast cells, &/or eosinophils or nerve cells Prostaglandins Direct means the bronchoconstricting stimulus e.g.methacholine acts directly on the smooth muscle Histamine Leukotrienes Eosinophils Bronchial smooth muscle
9 Positive and Negative Predictive Values How likely is someone, with a positive test result to methacholine or mannitol, to have asthma (positive predictive value)? How likely is someone, with a negative test result to methacholine or mannitol, to not have asthma (negative predictive value)?
10 Why perform a bronchial challenge test? Is it asthma? to rule out asthma? one needs a sensitive test with a high negative predictive value to rule in asthma? one needs a specific test with a high positive predictive value to manage asthma? one needs a test that correlates with the response of asthma to treatments
11 LEARNING OBJECTIVE Compare positive and negative predictive values of methacholine and mannitol inahalation tests
12 Is Methacholine a Rule Out test? Methacholine challenge has been promoted for its clinical utility in excluding the diagnosis of asthma based on a negative test result and one would expect a high negative predictive value. Is a negative methacholine test result a rule out test with a high negative predictive value?
13 Is Mannitol a Rule in test? In contrast to methacholine, the challenges that act via release of mediators such as mannitol, are promoted as tests that confirm the diagnosis of asthma if the test result is positive but do not rule out asthma if the test result is negative. Thus one would expect a high positive predictive value but not necessarily a high negative predictive value Is it valid to consider mannitol as a rule in test for asthma and if so, what is the positive predictive value?

 Timing between doses (5 min) Timing of FEV 1 (30")
 9 µl per breath 45 µl per dose PC 20 (mg/ml) PD 20 (µg)")
14 Tidal Breathing 2 min tidal breathing 0.13 L/min 90 µl per dose Other aspects identical: Concentrations ( mg/ml) Timing between doses (5 min) Timing of FEV 1 (30 & 90 sec) Calculation of PC 20 Dosimeter 5 Breaths B-hold (@TLC) 9 µl per breath 45 µl per dose PC 20 (mg/ml) PD 20 (µg) PD 20 (µmole) From Cockcroft AAAAI
15 METHODS Rest in lab/assess subject, Rx, etc. Spirometry x 3 assure FEV 1 > 70% Diluent doubling doses Mch q 5 min Single (good) FEV 30 & 90 s (no FVC) Calculate % FEV each concentration PC 20 /PD 20 from log dose vs. response curve Test shortening protocols optional From Cockcroft AAAAI2010
16 DEFINTIONS PC 20 > 16 mg/ml normal PC mg/ml borderline PC mg/ml mild AHR PC mg/ml moderate AHR PC 20 < 0.25 mg/ml severe AHR


17 PROTOCOL for Dry Powder Mannitol Progressive Protocol: 0,5,10,20,40,80,160,160,160mg Measurements : FEV 1 Pre & 1 min post dose with highest value for FEV 1 recorded Positive Response: Fall FEV 1 15% or Fall FEV 1 10% between consecutive doses Sensitivity PD 15 <35mg= Severe PD 15 >35mg<155mg= moderate, PD 15 >155 mg= mild AHR to mannitol Reactivity Response Dose Ratio =Final % fall FEV 1 /Cumulative dose Recovery: Bronchodilator or spontaneous Brannan JD Anderson SD et al Respiratory Research 2005; 6:144 Anderson SD et al Respiratory Research 2009 ; 10:44 Sverrild A et al J Allergy Clin Immunol 2009; 24: Sue Chu M et al Brit J Sports Med 2010;44: Porpodis K, et al J Thoracic Dis 2012;4(S1):AB81.
18 Q; What Population Studies have been performed using mannitol and methacholine? Australian study A301 was the 1st Phase 3 study using mannitol as a BCT. It was carried out in well defined groups including 592 asthmatic and healthy subjects both adults and children. (Brannan JD et al Resp Res 2005;6:144) USA study A305 was the 2 nd Phase 3 study using both mannitol and methacholine and exercise. It was in a group of 375 subjects with symptoms of asthma who entered the study without a definite diagnosis of asthma (Anderson SD et al Respir Res 2009: 10:4) Copenhagen study comprised an unselected sample of 238 young adults and mannitol and methacholine was used to identify those with respiratory physician diagnosed asthma (Sverrild A et al J Allergy Clin Immunol 2010;124:928 ) Greek study in 88 subjects with 61 being given a diagnosis of asthma based on a reversibility test with bronchodialtor (Porpodis K et al J Thoracic Dis 2012;4(S1):AB81) Norwegian study: 58 young elite skiers with asthma like symptoms had provocation tests using mannitol, methacholine and dry air hyperpnea (Sue-Chu M et al Brit J Sports Med 2010;44:827)

19 A 301 Study in well defined populations of asthmatic and healthy subjects Brannan JD Anderson SD et al Respiratory Research 2005; 6:144
20 A301 Phase 3 trial Per Protocol Patients characteristics 592 subjects (466 adults, 126 children) included 487 (82.3%) asthmatics and 105 non asthmatics. Age 6 83 mean 34.8 yr Majority had mild disease Half the asthmatic cohort had infrequent symptoms Only 11.3% reported symptoms interfering with normal activity. Majority had good lung function. 50% of the asthmatics had a FEV1 > 95% of predicted. The mean FEV 1 was 3.0 L in the asthmatics and 3.2 L in the nonasthmatics. 78.4% taking at least one medication. 228 on combination therapy / 164 on monotherapy with ICS Brannan JD et al. Respir Res 2005;6:144
21 Positive and Negative Predictive values in the Phase 3 study in well defined populations A301 Brannan JD et al Respir Res 2005; 6:144 Including all subjects Asthmatic n= 487 Non-asthmatic n=105 Mannitol +ve Mannitol -ve Negative Predictive value 33.7% Positive predictive value 98.3% Excluding subjects negative to mannitol taking inhaled cortico steroids Asthmatic = 328 Non-asthmatic = 105 Mannitol +ve Mannitol -ve Negative Predictive value 72.9% Positive predictive value 98.3%
22 What did we learn from A301? Mannitol had a high positive predictive value and there were very few false positive tests in the healthy population. The low negative predictive value for mannitol to exclude clinically recognised asthma improved from 33.7% to 72.9% when the benefit of current treatment with inhaled corticosteroids was taken into account.
23 Porpodis K, et al Comparison of validity of methacholine and mannitol bronchial challenges in asthma diagnosis. J Thoracic Dis 2012;4(S1):AB81. DOI: /j.issn s081 Including all subjects Asthmatic n= 67 Non-asthmatic n=21 Mannitol +ve 43 1 Mannitol -ve Negative Predictive value 45.4% Positive predictive value 97.7% Asthmatic = 67 Non-asthmatic = 21 Methacholine + ve 42 3 Methacholine -ve Negative Predictive value 41.9% Positive predictive value 93.3%. 47 women & 41 men 14 to 75 yrs The clinical diagnosis of asthma was based on bronchodilator reversibility test.

24 COPENHAGEN STUDY was in yr olds in a general population with asthmatics identified by a respiratory physician Sverrild A et al, J Allergy Clin Immunol 2009;124:928-32


25 COPENHAGEN STUDY Subject Characteristics Sverrild A et al, J Allergy Clin Immunol 2009;124: One respiratory physician only made the diagnosis based on symptoms in last 1yr, in combination with an FeNO >30 ppb, a history of allergic rhino-conjunctivitis, dermatitis, a positive skin test response, a familial predisposition to atopic disease, non-allergic rhino-conjunctivitis or an FEV 1 /FVC ratio <75%.
26 COPENHAGEN STUDY Diagnostic properties of inhaled mannitol and methacholine in 238 subjects Asthma n=51 Non Asthma n=187 Positive Predictive value Negative Predictive value Mannitol 91% (78-97) 90% (88-91) Methacholine 49% (40-56) 90% (87-93) Sverrild A et al, J Allergy Clin Immunol 2009;124:928-32
27 What did we learn from the Copenhagen study? Mannitol PD 15 had a high positive predictive value compared with methacholine PC 20 i.e. 91% versus 49% That is there were many more false positive tests in nonasthmatics (n=37) using methacholine than there were using mannitol (n=3). The negative predictive value of mannitol was the same compared with methacholine (90% vs 90%). That is the same number of people had a false negative test result.
28 A 305 was a population of subjects with symptoms but without a definite diagnosis of asthma at study entry Anderson SD, Charlton B et al Respiratory Research 2009; 10:4
29 Patient demographics (enrolled subjects) Age Mean (SD) = 24.9 (10.6) yrs range = 6 50 yrs BMI Mean (SD) = 24.5 (4.7) Range = Gender 46.4% male 53.6% female Ethnicity Caucasian 74% Hispanic 9% Black 9% Asian 5% Other 2% A-305
30 Patient characteristics at baseline (enrolled) FEV 1 Mean (SD) = 91 (8.7)% of predicted at baseline Atopy 78% of subjects β 2 reversibility NAEPPII asthma severity rating 10.8% of all screened subjects 7.5% of PP subjects reversed Mean (SD) = 1.2 (0.6)* * 92.2% graded at Step 1 or 2 by clinician at Visit 1, on scale 0-4 This was a group of patients with normal spirometry, mild symptoms with an unclear diagnosis
31 A305 Study Design Visit 1 Visit 2 Visit 3 Visit 4 Visit 5 Medical history Physical exam Skin testing FEV 1 reversibility Clinician eval. - NAEPP - likelihood of having asthma Exercise challenge #1 Exercise challenge #2 Mannitol or methacholine challenge Mannitol or methacholine challenge Clinical diagnosis Randomization All visits separated from next visit by ~ 1 4 days Order for mannitol and methacholine challenges was randomized within the exercise negative and exercise positives arms Blinding Mannitol and methacholine challenges performed by staff different from those performing the rest of the procedures There was no access to results across groups Clinician doing diagnosis at Visit 5 had access to all data except mannitol and the methacholine challenge results
32 Methacholine and mannitol were equally sensitive for identifying bronchial hyperresponsiveness in the population Methacholine (5 breath dosimeter method) PC 20 <16 mg/ml (fall in FEV 1 of 20% from baseline) n= 156 were positive Mannitol PD 15 <635 mg (fall in FEV 1 of 15% from baseline) (or subject experienced a 10% between dose fall in FEV 1 ) 168 were positive Exercise (8 minute treadmill challenge) FEV 1 fall >10% from baseline on at least 1 of 2 exercise tests n=163 were positive
33 METHACHOLINE The positive predictive value was 78.2% The negative predictive value was 46.1% Thus a negative test was not useful to rule out asthma Methacholine +ve 122 Clin Dx +ve n=240 GM 2.14 mg/ml Methacholine -ve 118 > 16 mg/ml Clin Dx ve n= mg/ml 101 > 16 mg/ml Diagnosis by a Respiratory Physician on basis of comprehensive information only such as History,Examination,FEV 1 Reversibilty two exercise tests, Skin tests and Questionnaires Anderson SD et al Respir Res 2009: 10:4
34 MANNITOL The positive predictive value was 78.8% The negative predictive value was 48.2% A positive test was useful to rule in asthma Clin Dx +ve n=240 Mannitol +ve Clin Dx ve n=135 Mannitol -ve Diagnosis by a Respiratory Physician on basis of History,Examination, FEV 1 Reversibilty 2 exercise tests, Skin tests Questionnaires Anderson SD et al Respir Res 2009:10:4
35 What did we learn about methacholine from A 305? That Methacholine was no more sensitive for identifying AHR than mannitol or exercise and no more sensitive than mannitol for identifying a clinical diagnosis of asthma. There was a high rate of methacholine negative test results ( 49%) in those given a clinical diagnosis of asthma by a respiratory physician at the end of the study Based on comprehensive information that included History FEV 1 reversibility, two exercise tests,skin tests, questionnaire (the results of the methacholine or mannitol test results were withheld ) suggests that: a negative methacholine test result should not be relied upon to rule out a diagnosis of asthma in subjects with symptoms of asthma but without a definite diagnosis. The importance of these observations is that it is subjects with these characteristics who are most likely to be referred for testing.
36 What did we learn about Mannitol as a rule in test? Mannitol was as sensitive as methacholine for identifying BHR. Mannitol was never less sensitive than methacholine to identify a clinical Diagnosis of asthma when cut points of 8, 12 or 16 mg/ml were used. The clinical utility of a mannitol positive test result was upheld by the low number of false positive tests in A301 and Copenhagen studies & the high concordance (78.5%) between a clinical Dx at Visit 5 & a positive mannitol in A305.
37 Mannitol positive subjects compared with mannitol negative subjects In mannitol +ve subjects a PC 20 Methacholine was more frequent (66% vs 25%) and the PC 20 significantly lower 1.64 vs 3.54 mg/ml p<0.001 (Anderson SD et al Respir Res 2009) In mannitol +ve subjects EIB was more common (57% vs 33%) and more severe 21±10% vs 16±7% p<0.001) (Anderson SD et al Respir Res 2009;10:4) In mannitol +ve subjects FeNO was significantly higher 47 vs 19 ppb (Sverrild S et al JACI 2010) In those with eosinophilic asthma 82% are +ve to mannitol (Porsbjerg et al J Asthma 2009;46)

38 Athlete Study
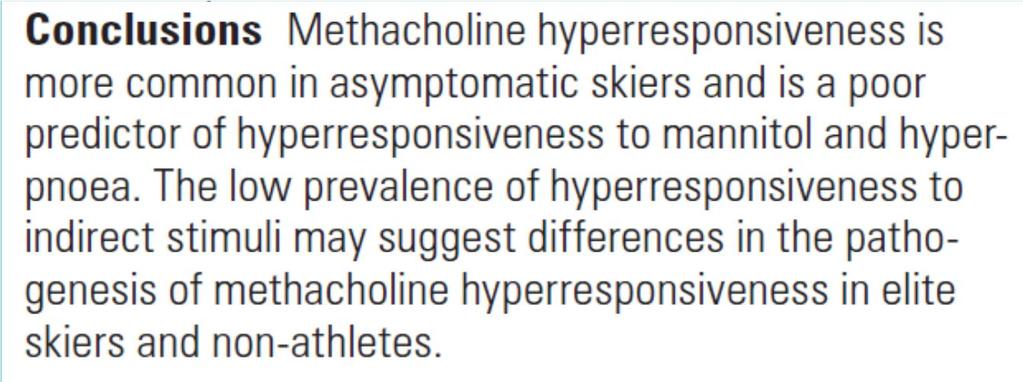
39 60 High Prevalence of airway hyperresponsiveness to methacholine, and low prevalence of response to AMP and Mannitol in Young skiers with and without symptoms of asthma Methacholine % AMP Mannitol Any kind of BHR Asthma-like symptoms (n=26) No asthma-like symptoms (n= 32) Sue Chu et al Brit J Sports Med 2010
40
41 What about methacholine as a Rule in test? Many clinicians use a positive methacholine test result as diagnostic of asthma at a PC 20 <16 mg/ml. Many factors however can contribute to AHR to methacholine. AHR at PC 20 <16 mg/ml can reflect airway injury from breathing large volumes of unconditioned air (e.g. cross country skiers or skaters) cigarette smoking or inhalation of pollutants (e.g. swimmers) or remodelling of the airways in response to childhood asthma. The findings of positive methacholine responses in elite athletes both with and without symptoms of asthma suggest that we should question if a positive methacholine test result is always consistent with a diagnosis of asthma.
42 LEARNING OBJECTIVE Evaluate methacholine and mannitol as potential test for monitoring asthma treatment
43 Monitoring Response to ICS treatment measuring AHR with DIRECT STIMULI Airway hyperresponsiveness (AHR) to direct stimuli e.g. methacholine and histamine may reflect a fixed component such as a change in airway calibre from airway remodelling or a variable component due to inflammation or both. Thus AHR to methacholine can be documented either in the presence of currently active airway inflammation or in its absence as may be the case in those with airway remodelling from past asthma or from environmental injury as occurs in elite skaters, skiers and swimmers. While daily treatment with adequate doses of inhaled corticosteroids (ICS) reduces AHR to methacholine the PC 20 remains well below 8 mg/ml even after many weeks or months of treatment presumably because a component of AHR is due to airway remodelling and injury.
44 Change in direct AHR to inhaled corticosteroids PD 20 PC 20 µg mg/ml 0 0 Dose (mcg) Duration (wks) Reddel du Toit Jenkins Foresi Lim Sont Modified from Brannan et. al. Clin Respir J 2007; 1
45 Monitoring Response to ICS treatment measuring AHR with INDIRECT STIMULI Most attacks of asthma that occur in daily life are due to stimuli that act indirectly, by release of mediators from inflammatory cells, and these mediators cause smooth muscle contraction and airway narrowing. Airway hyperresponsiveness (AHR) to indirect stimuli e.g. exercise and mannitol indicates currently active airway inflammation i.e. the inflammatory cells are present in sufficient numbers and the mediators in a sufficiently high concentration for a responsive bronchial smooth muscle to contract. Treatment daily with adequate doses of inhaled corticosteroids (ICS) would be expected to resolve or significantly reduce AHR due to inflammation such that an exercise or mannitol test would become negative within the time a patient would be expected to comply with ICS treatment e.g weeks. For example the majority of children & adults with exercise-induced bronchoconstriction (EIB), or AHR to mannitol treated daily with ICS for 3 to 8 weeks are likely to have a significant reduction or even complete resolution of their EIB or AHR to mannitol.
46 Treatment goal with steroids is clear for an indirect test, i.e. until response is within the normal range (usually takes 8 12 weeks) % Fall in FEV % Fall in FEV /14 (71%) 0 9/14 (64%) Pre Post Pre Post 100 µg/day for 12 weeks 200 µg/day for 12 weeks FEV ± 12% predicted FEV ± 10% predicted Budesonide Jonasson G. Pediatr Allergy Immunol 2000;11:120 5; personal communication
47 Exercise response after 3 weeks of Rx Group 1 FEV 1 91% ± % ± 3 % Fall in FEV µg % Fall in FEV µg FEV 1 93% ± % ± Group mcg mcg 80 µg 320 µg FEV % ± % ± 4.6 % Fall in FEV % Fall in FEV FEV % ± % ± mcg mcg Baseline 3 weeks CIC Baseline 3 weeks CIC Subbarao PJ, et al. J Allergy Clin Immunol 2006;117:
 and")

48 Exercise response following ciclesonide low (40, 80 µg/day) & high doses (160, 320 µg/day) in those with >5% and <5% eosinophils >5% Eosinophils <5% Eosinophils Changes from baseline were compared within a group (*) and between groups ( ) for each dose level at p<0.05 ANOVA. The >5% sputum eosinophil group showed a significantly greater change from baseline for high-dose versus low-dose ( ) ciclesonide. Duong M, et al. Chest 2008;133:404 11,
49
50 AHR to mannitol resolved or reduced after 6-9 wk of ICS SENSITIVITY REACTIVITY PD 15 to Mannitol (mg) n = 18 Before R x After R x No PD 15 p < Response Dose Ratio to Mannitol Before Rx RDR = Response (%) Dose (mg) Non-asthmatic, healthy After Rx 78 (51, 117) mg 289 (202, 414) mg 95% CI in healthy subjects % fall/mg Brannan et al. Respirology 2002; 7: 37-44
51
52 AHR to mannitol resolved or reduced after weeks of treatment with 1000 mcg of budesonide 2D Graph 2 Mannnitol PD15 mg Mannitol PD Months MONTHS 7/17 (41%) unresponsive after 3 m Rx & 82% were unresponsive at one visit Koskela H et al. CHEST 2003;124:1341-9
53 The frequency of symptoms, daily doses of relief medication, and sum symptom score before and at 3 m and 6 m of Rx with budesonide daily symptoms (5) Several times/week (4) Symptom Frequency Approx once/week (3) 1-5 times/month (2) < once/month (1) No symptoms (0) Koskela H et al. CHEST 2003;124:1341-9
54
55 Back titration of steroid dose The airway response to both an indirect (mannitol) and a direct (histamine) stimulus was measured at baseline in people well controlled on ICS. 24 subjects had AHR (PD 15 ) to mannitol and 15 a (PC 20 ) to histamine at baseline. The ICS dose was halved every 2 m & response to mannitol measured On the initial visit 23 had no AHR or response to mannitol and at the final visit 9 were still unresponsive with 7 still off ICS 2 m later. A PD 15 mannitol at baseline did not predict failure of dose reduction A PD 15 mannitol <635 mg during the dose reduction had 90% sensitivity and a specificity 42% to predict failure of dose reduction. Neither FEV 1 nor PEF % predicted nor FeNO ppb were markers for failed reduction although sputum eosinophils >6% had a 90% sensitivity and 58% specificity to predict failure and an exacerbation.
56 Comparison of values before the last successful ICS reduction and the values before the failed ICS reduction in the same 26 subjects Mean values (95% confidence interval) Successful reduction Exacerbation p-value RDR mannitol 0.05 ( ) 0.09 ( ) Exhaled NO (ppb) 18.4 ( ) 18.5 ( ) 0.95 FEV 1 predicted (%) 87.4 ( ) 86.9 ( ) 0.84 FVC predicted (%) 88.7 ( ) 87.5 ( ) 0.73 PEF predicted (%) 84.3 ( ) 82.6 ( ) 0.65 PEF (lowest % best) 85.5 ( ) 82.9 ( ) 0.57 Sputum neutrophils (%) 26 ( ) 18.6 ( ) 0.23 Sputum eosinophils (%) 7.9 ( ) 22.5 ( ) 0.03 Sputum macrophages (%) 56.8 ( ) 58.6 ( ) 0.62 Sputum lymphocytes (%) 3.2 ( ) 0.53 ( ) 0.13 Sputum mast cells (%) 0.09 ( ) 0.4 ( ) 0.42 RDR: %fall FEV 1 at the last dose/cumulative dose mg; FEV 1 : forced expiratory volume in one second; FVC: forced expiratory volume; PEFR: peak expiratory flow rate Leuppi et al., AJRCCM 2001; 163:
57 PD 15 <635mg 90% sensitivity
58
59 Return of the PD 15 to mannitol in previously well controlled subjects after stepwise dose reduction of ICS and is not reflected in a change in FEV n = 9 (No PD15 recorded after 635 mg) PD15 to mannitol (mg) n = 14 FEV 1 % pred n = n = 23 No PD 15 With PD 15 Initial Visit Final Visit (median time = 125 days) Initial Visit Final Visit (median time = 125 days) Redrawn from Leuppi JD et al, AJRCCM 2001;163:
60 Earlier studies by Sont J et al AJRCCM 1999 used methacholine and guidelines and Green R et al Lancet 2002 used or eosinophils and guidelines

61
62 STAMINA Trial using a treatment strategy aimed at reducing AHR to mannitol versus treatment using BTS guidelines. The AHR strategy involved adjusting ICS dose every 2 months until mannitol PD 10 <635 mg and measuring outcome by a number of inflammatory indices including FeNO, eosinophilic cationic protein (ECP) AHR to methacholine, symptom and reliever use. LABAs or LT antagonists not permitted. When the dose of ICS was adjusted in accordance with AHR to mannnitol there was a significant reduction in FeNO (p<0.05) and ECP (p<0.05) AHR to mannitol (p<0.0001) methacholine (p<0.05) symptoms (p<0.005) & reliever use (p<0.001) When the treatment strategy involved adjusting ICS dose based on changes in PEF, FEV 1, reliever use or symptom scores there were no significant changes in indices of inflammation There was no change in FEV 1 or PEF or AQLQ in response to ICS (Lipworth BJ et al Chest 2012:141;607-15)
63 Methods Ciclesonide dosing regimen in both groups : step #1 80 ug/day step #2 160 ug/day step #3 320 ug/day step #4 480 ug/day step #5 640 ug/day
64 Control group AHR group p n = 58 n = 61 value Age (yr) 53.7 (1.7) 53.2 (1.6) ns FEV 1 % 85.1 (1.9) 84.0 (2) ns PEF% 87.0 (2.6) 91.2 (2.2) ns Mannitol PD 10 (mg) Baseline Demographics 114.7( ) ( ) ns Methacholine PC 20 (mg/ml) 0.85 ( ) 0.84 ( ) ns FeNO (pbb) 24.9 ( ) 25.7 ( ) ns ICS (ug/day) (9.98) (14.8) ns Data shown as mean (SEM) or geo mean (95%CI) Lipworth BJ et al Chest 2012;141:
65 Improvements in Symptoms and reliever use & morning peak flow in group whose dose guided by airway response to mannitol AHR Group n=58 Baseline End Study Change p value PEF am Night Symptoms Day Symptoms Reliever use Control Group n=61 Baseline End Study Change p value PEF am Night Symptoms Day Symptoms Reliever use Lipworth BJ et al Chest 2012;141: *
66 No significant change in spirometry peak flow or quality of life in either Control or AHR group AHR Group n=58 Baseline End Study Change p value FEV 1 % 83.6(1.9) 85.6% (2.0) 2.0( ) 0.48 PEF% 89.2 (2.0) 92.3(2.7) 3.1( ) 0.34 FVC% 91.5(1.9) 92.7(1.9) 1.2( ) 0.66 AQLQ 5.9(0.10) 6.0(0.11) Control Group n=61 Baseline End Study Change p value FEV 1 % 86.3% (1.9) 88.0 (2.8) 1.7( ) 0.59 PEF% 88.5 (2.6) 94.3(3.3) 5.8 ( ) 0.17 FVC% 93.0(2.4) 94.0(2.6) 1.0 ( ) 0.77 AQLQ 6.5(0.13) 6.2(0.16) Lipworth BJ et al Chest 2012;141:
67 Significant improvement in Methacholine responsiveness, FeNO and ECP in the group whose dose of steroids was guided by AHR to mannitol AHR Group Baseline End of Study Change p value Methacholine PC 20 (mg/ml)* 0.84( ) 2.43( ) 1.54( ) Mannitol PD 10 (mg)* 108.9( ) 482( ) 2.1( ) <0.001 FeNO (pbb) 25.7( ) 18.8( ) 1.37( ) 0.02 ECP (ug/l) 16.8( ) 11.1(8-15.5) 1.51( ) 0.04 OUCortisol/C (mmol/10h) 4.00( ) 4.21( ) 0.95( ) 0.76 Lipworth BJ et al Chest 2012;141:
68 NO Significant improvement in Methacholine responsiveness, FeNO and ECP in the control group whose dose of steroids was guided by BTS Clinical Guidelines Control Group BTS Baseline End of Study Change p value Methacholine PC 20 (mg/ml)* 0.85( ) 1.59( ) 0.9( ) 0.07 Mannitol PD 10 (mg)* 114.7( ) 168.5( ) 0.7( ) 0.10 FeNO (pbb) 24.9( ) 23.7( ) 1.05( ) 0.81 ECP (ug/l) 11.8( ) 9.8( ) 1.2( ) 0.42 OUCortisol/C (mmol/10h) 3.62( ) 3.62( ) 1.00( ) 0.99 Lipworth BJ et al Chest 2012;141:
69 Dose of inhaled steroid (Ciclesonide) 306ug (95%CI ) difference between AHR vs Control (P<0.0001) Lipworth BJ et al Chest 2012;141:
70 What are the clinical implications? In a primary care setting repeated mannitol challenge (as PD 10 ) is safe to use in mild to moderate asthmatics to assess AHR Further long-term studies are required in more severe patients to fully define its clinical role as an asthma inflammometer
71 A 301 Phase 3 study for Registration December 9 th :144 Study in well defined populations of asthmatic and healthy subjects
72 A 301 Phase 3 study showed mannitol has a high specificity i.e. a positive response in a healthy subject is unlikely Gold Standard Clinicians Diagnosis Clin Dx Clin Dx Adjusted For ICS Mannitol n = 492 Sensitivity Specificity Mannitol n =333 Sensitivity Specificity Sensitivity increased from 60 to 89% when data adjusted for the confounding effect of benefit from treatment with inhaled corticosteroids (ICS) and mannitol negative subjects taking ICS are removed. Age 6-83 yrs ( Mean 34.8 yr) Brannan JD Anderson SD et al 2005 Respiratory Research 6: 144
73 Caucasian Adults Asthmatic taking ICS A301 Study Positive (PD 15 ) Negative (No PD 15 ) p Non-Asthmatic No ICS N (% Females) 129 (69%) 123 (56.9%) NS 80 (45%) % taking ICS with LABA 60.4% 66.6% NS 0% Age (yr) 40.4± ±13.9 NS 40.2±13.1 Ht (cm) 166.7± ±10.4 NS 171.8± 10.2 BMI 27.2± ±6.0 NS 25± 3.9 FEV 1 % Predicted screening 91.3± ±14.8 < %± 11.7 Mannitol PD 15 (Geomean) (110,165) - n =2 + ve 58 & 207 mg Geomean RDR (%fall FEV 1 /mg) 95% Confidence interval , , < , Percent with > 10% fall FEV 1 100% 21.1% 11.3% Atopic 94.5% 80.5% < % Coughed in last week 53% 66% < % Brannan JD et al J Allergy Clin Immunol 2012 Letter
74 Advice relating to mannitol test outcome Mannitol Positive* Mannitol Negative Not on ICS Using ICS Not on ICS Using ICS Clinical diagnosis of asthma Asthmatic with active airway inflammation that will respond to ICS Check technique & Adherence & Maintain or increase ICS dosage Consider alternative diagnosis Well controlled asthmatic Consider reducing dosage of ICS If fall <10% or RDR 95% CI * PD15 = 15% fall in FEV1 to a dose 635 mg
75 Why challenge with Mannitol? Advantages : High positive predictive value for Clinical Dx of asthma Dose-response curve obtained Median time taken for + ve test 17 min, - ve test 26 min More than one mediator involved LT s, Hist, PGD 2 Positive test predicts potential for EIB Negative test in asthmatic = good control of asthma Response dose ratio can guide back titration of steroid Positive test = currently active airway inflammation Identifies those who would benefit from Rx with ICS Disadvantage : Some cough during challenge 55% of those taking ICS will have a negative test
Mechanisms of action of bronchial provocation testing
 Mechanisms of action of bronchial provocation testing TSANZ / ANZSRS Masterclass: April 3rd, 2016 13:00 13:30 John D. Brannan PhD Scientific Director - Dept. Respiratory & Sleep Medicine John Hunter Hospital,
Mechanisms of action of bronchial provocation testing TSANZ / ANZSRS Masterclass: April 3rd, 2016 13:00 13:30 John D. Brannan PhD Scientific Director - Dept. Respiratory & Sleep Medicine John Hunter Hospital,
Methacholine versus Mannitol Challenge in the Evaluation of Asthma Clinical applications of methacholine and mannitol challenges
 Methacholine versus Mannitol Challenge in the Evaluation of Asthma Clinical applications of methacholine and mannitol challenges AAAAI San Antonio Tx February 2013 Catherine Lemière MD, MSc Hôpital du
Methacholine versus Mannitol Challenge in the Evaluation of Asthma Clinical applications of methacholine and mannitol challenges AAAAI San Antonio Tx February 2013 Catherine Lemière MD, MSc Hôpital du
NON-SPECIFIC BRONCHIAL HYPERESPONSIVENESS. J. Sastre. Allergy Service
 NON-SPECIFIC BRONCHIAL HYPERESPONSIVENESS J. Sastre. Allergy Service Asthma: definition Asthma is a syndrome defined on basis of three main aspects: 1- Symptoms due to variable and reversible airway obstruction
NON-SPECIFIC BRONCHIAL HYPERESPONSIVENESS J. Sastre. Allergy Service Asthma: definition Asthma is a syndrome defined on basis of three main aspects: 1- Symptoms due to variable and reversible airway obstruction
Optimal Assessment of Asthma Control in Clinical Practice: Is there a role for biomarkers?
 Disclosures: Optimal Assessment of Asthma Control in Clinical Practice: Is there a role for biomarkers? Stanley Fineman, MD Past-President, American College of Allergy, Asthma & Immunology Adjunct Associate
Disclosures: Optimal Assessment of Asthma Control in Clinical Practice: Is there a role for biomarkers? Stanley Fineman, MD Past-President, American College of Allergy, Asthma & Immunology Adjunct Associate
NG80. Asthma: diagnosis, monitoring and chronic asthma management (NG80)
") Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Searching for Targets to Control Asthma
 Searching for Targets to Control Asthma Timothy Craig Distinguished Educator Professor Medicine and Pediatrics Penn State University Hershey, PA, USA Inflammation and Remodeling in Asthma The most important
Searching for Targets to Control Asthma Timothy Craig Distinguished Educator Professor Medicine and Pediatrics Penn State University Hershey, PA, USA Inflammation and Remodeling in Asthma The most important
Bronchial Provocation Results: What Does It Mean?
 Bronchial Provocation Results: What Does It Mean? Greg King 1 Department of Respiratory Medicine, Royal North Shore Hospital, St Leonards 2065 2 Woolcock Institute of Medical Research and Sydney Medical
Bronchial Provocation Results: What Does It Mean? Greg King 1 Department of Respiratory Medicine, Royal North Shore Hospital, St Leonards 2065 2 Woolcock Institute of Medical Research and Sydney Medical
GETTING STARTED WITH MANNITOL CHALLENGE TESTING. Rick Ballard, RRT, RPFT Applications/Education Specialist MGC Diagnostics
 GETTING STARTED WITH MANNITOL CHALLENGE TESTING Rick Ballard, RRT, RPFT Applications/Education Specialist MGC Diagnostics OBJECTIVES Indications for provocation testing Identify candidates for testing
GETTING STARTED WITH MANNITOL CHALLENGE TESTING Rick Ballard, RRT, RPFT Applications/Education Specialist MGC Diagnostics OBJECTIVES Indications for provocation testing Identify candidates for testing
Exhaled Nitric Oxide: An Adjunctive Tool in the Diagnosis and Management of Asthma
 Exhaled Nitric Oxide: An Adjunctive Tool in the Diagnosis and Management of Asthma Jason Debley, MD, MPH Assistant Professor, Pediatrics Division of Pulmonary Medicine University of Washington School of
Exhaled Nitric Oxide: An Adjunctive Tool in the Diagnosis and Management of Asthma Jason Debley, MD, MPH Assistant Professor, Pediatrics Division of Pulmonary Medicine University of Washington School of
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
(Asthma) Diagnosis, monitoring and chronic asthma management
 Diagnosis, monitoring and chronic asthma management") Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Using Patient Characteristics to Individualize and Improve Asthma Care
 Using Patient Characteristics to Individualize and Improve Asthma Care Leonard B. Bacharier, M.D. Associate Professor of Pediatrics Clinical Director, Division of Allergy, Immunology, & Pulmonary Medicine
Using Patient Characteristics to Individualize and Improve Asthma Care Leonard B. Bacharier, M.D. Associate Professor of Pediatrics Clinical Director, Division of Allergy, Immunology, & Pulmonary Medicine
Bronchial challenge tests: usefulness, availability and limitations
 This article is based on a postgraduate course from the Barcelona 2010 ERS Annual Congress S.D. Anderson Bronchial challenge tests: usefulness, availability and limitations Introduction Indirect challenges
This article is based on a postgraduate course from the Barcelona 2010 ERS Annual Congress S.D. Anderson Bronchial challenge tests: usefulness, availability and limitations Introduction Indirect challenges
Ass. Prof. Pulmonary and Crit.Care Medical School,University of Athens
 Diagnosis i of Exercise Induced Asthma Ch. Gratziou Ass. Prof. Pulmonary and Crit.Care Medical School,University of Athens Other Diagnostic Challenges for Exercise Induced Asthma Do we need other tests
Diagnosis i of Exercise Induced Asthma Ch. Gratziou Ass. Prof. Pulmonary and Crit.Care Medical School,University of Athens Other Diagnostic Challenges for Exercise Induced Asthma Do we need other tests
Life-long asthma and its relationship to COPD. Stephen T Holgate School of Medicine University of Southampton
 Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Exercise-Induced Bronchospasm. Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute
 Exercise-Induced Bronchospasm Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute EIB Episodic bronchoconstriction with exercise May be an exacerbation
Exercise-Induced Bronchospasm Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute EIB Episodic bronchoconstriction with exercise May be an exacerbation
COPD and Asthma: Similarities and differences Prof. Peter Barnes
 and Asthma: Similarities and Differences and Asthma: 1 Imperial College Peter Barnes FRS, FMedSci, National Heart & Lung Institute Imperial College, London, UK p.j.barnes@imperial.ac.uk Royal Brompton
and Asthma: Similarities and Differences and Asthma: 1 Imperial College Peter Barnes FRS, FMedSci, National Heart & Lung Institute Imperial College, London, UK p.j.barnes@imperial.ac.uk Royal Brompton
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al.
 Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
FeNO-based asthma management results in faster improvement of airway hyperresponsiveness
 ORIGINAL ARTICLE ASTHMA FeNO-based asthma management results in faster improvement of airway hyperresponsiveness Katrine Feldballe Bernholm 1, Anne-Sophie Homøe 1, Howraman Meteran 1, Camilla Bjørn Jensen
ORIGINAL ARTICLE ASTHMA FeNO-based asthma management results in faster improvement of airway hyperresponsiveness Katrine Feldballe Bernholm 1, Anne-Sophie Homøe 1, Howraman Meteran 1, Camilla Bjørn Jensen
Airway hyperresponsiveness to mannitol and methacholine and exhaled nitric oxide: A random-sample population study
 Airway hyperresponsiveness to mannitol and methacholine and exhaled nitric oxide: A random-sample population study Asger Sverrild, MD, Celeste Porsbjerg, MD, PhD, Simon Francis Thomsen, MD, PhD, and Vibeke
Airway hyperresponsiveness to mannitol and methacholine and exhaled nitric oxide: A random-sample population study Asger Sverrild, MD, Celeste Porsbjerg, MD, PhD, Simon Francis Thomsen, MD, PhD, and Vibeke
Sergio Bonini. Professor of Internal Medicine, Second University of Naples INMM-CNR, Rome, Italy.
 Assessment of EIA in the community and in athletes: the role of standardized questionnaires Sergio Bonini Professor of Internal Medicine, Second University of Naples INMM-CNR, Rome, Italy se.bonini@gmail.com
Assessment of EIA in the community and in athletes: the role of standardized questionnaires Sergio Bonini Professor of Internal Medicine, Second University of Naples INMM-CNR, Rome, Italy se.bonini@gmail.com
Asthma: diagnosis and monitoring
 Asthma: diagnosis and monitoring NICE guideline: short version Draft for second consultation, July 01 This guideline covers assessing, diagnosing and monitoring suspected or confirmed asthma in adults,
Asthma: diagnosis and monitoring NICE guideline: short version Draft for second consultation, July 01 This guideline covers assessing, diagnosing and monitoring suspected or confirmed asthma in adults,
Asthma and obesity, implications for airway inflammation and Bronchial Hyperresponsiveness
 Asthma and obesity, implications for airway inflammation and Bronchial Hyperresponsiveness Fernando Holguin MD MPH Asthma Institute University of Pittsburgh Obesity Trends* Among U.S. Adults BRFSS, 1990,
Asthma and obesity, implications for airway inflammation and Bronchial Hyperresponsiveness Fernando Holguin MD MPH Asthma Institute University of Pittsburgh Obesity Trends* Among U.S. Adults BRFSS, 1990,
Asthma Pathophysiology and Treatment. John R. Holcomb, M.D.
 Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Research Article Exercise-Induced Asthma Symptoms and Nighttime Asthma: Are They Similar to AHR?
 Allergy Volume 2009, Article ID 378245, 6 pages doi:10.1155/2009/378245 Research Article Exercise-Induced Asthma Symptoms and Nighttime Asthma: Are They Similar to AHR? V. Backer and L. M. Rasmussen Department
Allergy Volume 2009, Article ID 378245, 6 pages doi:10.1155/2009/378245 Research Article Exercise-Induced Asthma Symptoms and Nighttime Asthma: Are They Similar to AHR? V. Backer and L. M. Rasmussen Department
Airways hyperresponsiveness to different inhaled combination therapies in adolescent asthmatics
 Airways hyperresponsiveness to different inhaled combination therapies in adolescent asthmatics Daniel Machado 1, MD Celso Pereira 1,2, MD, PhD Beatriz Tavares 1, MD Graça Loureiro 1, MD António Segorbe-Luís
Airways hyperresponsiveness to different inhaled combination therapies in adolescent asthmatics Daniel Machado 1, MD Celso Pereira 1,2, MD, PhD Beatriz Tavares 1, MD Graça Loureiro 1, MD António Segorbe-Luís
Asthma Phenotypes, Heterogeneity and Severity: The Basis of Asthma Management
 Asthma Phenotypes, Heterogeneity and Severity: The Basis of Asthma Management Eugene R. Bleecker, MD Professor and Director, Center for Genomics & Personalized Medicine Research Professor, Translational
Asthma Phenotypes, Heterogeneity and Severity: The Basis of Asthma Management Eugene R. Bleecker, MD Professor and Director, Center for Genomics & Personalized Medicine Research Professor, Translational
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Abnormal Spirometry Medical Risk in Aviation Conference Royal Aeronautical Society, Dec 2017
 Abnormal Spirometry Medical Risk in Aviation Conference Royal Aeronautical Society, Dec 2017 Professor Howard Branley MBChB MSc MD FCCP FRCP FRAeS Consultant in Respiratory Medicine What I want to cover
Abnormal Spirometry Medical Risk in Aviation Conference Royal Aeronautical Society, Dec 2017 Professor Howard Branley MBChB MSc MD FCCP FRCP FRAeS Consultant in Respiratory Medicine What I want to cover
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Role of bronchoprovocation tests in identifying exercise-induced bronchoconstriction in a non-athletic population: a pilot study
 Original Article Role of bronchoprovocation tests in identifying exercise-induced bronchoconstriction in a non-athletic population: a pilot study Jessica H. Y. Tan 1 *, Wui Mei Chew 1 *, Therese S. Lapperre
Original Article Role of bronchoprovocation tests in identifying exercise-induced bronchoconstriction in a non-athletic population: a pilot study Jessica H. Y. Tan 1 *, Wui Mei Chew 1 *, Therese S. Lapperre
Sponsor. Generic drug name. Trial indication(s) Protocol number. Protocol title. Clinical trial phase. Study Start/End Dates.
 Protocol number. Protocol title. Clinical trial phase. Study Start/End Dates.") Sponsor Novartis Generic drug name Fluticasone propionate Trial indication(s) Moderate-severe bronchial asthma Protocol number CQAE397A2202 Protocol title A randomized open label study to assess the utility
Sponsor Novartis Generic drug name Fluticasone propionate Trial indication(s) Moderate-severe bronchial asthma Protocol number CQAE397A2202 Protocol title A randomized open label study to assess the utility
NICE guideline Published: 29 November 2017 nice.org.uk/guidance/ng80
 Asthma: diagnosis, monitoring and chronic asthma management NICE guideline Published: 29 November 2017 nice.org.uk/guidance/ng80 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Asthma: diagnosis, monitoring and chronic asthma management NICE guideline Published: 29 November 2017 nice.org.uk/guidance/ng80 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Török et al. BMC Pediatrics 2014, 14:196
 Török et al. BMC Pediatrics 2014, 14:196 RESEARCH ARTICLE Open Access An open-label study examining the effect of pharmacological treatment on mannitol- and exercise-induced airway hyperresponsiveness
Török et al. BMC Pediatrics 2014, 14:196 RESEARCH ARTICLE Open Access An open-label study examining the effect of pharmacological treatment on mannitol- and exercise-induced airway hyperresponsiveness
#1 cause of school absenteeism in children 13 million missed days annually
 Asthma Update 2013 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Pulmonary & Critical Care Medicine The Ohio State University Wexner Medical Center Disclosures None 2 Objectives Review burden
Asthma Update 2013 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Pulmonary & Critical Care Medicine The Ohio State University Wexner Medical Center Disclosures None 2 Objectives Review burden
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Bronchial asthma. MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL
 Bronchial asthma MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL DEFINITION ASTHMA BRONCHIALE = Asthma is a chronic inflammatory disorder of the airways in which
Bronchial asthma MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL DEFINITION ASTHMA BRONCHIALE = Asthma is a chronic inflammatory disorder of the airways in which
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL
 DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Beta 2 adrenoceptor agonists and the Olympic Games in Athens
 Beta 2 adrenoceptor agonists and the Olympic Games in Athens 1 Appendix A of the Olympic Movement Anti-Doping Code, the List of Prohibited Substances and Prohibited Methods dated 1 st January 2003 states
Beta 2 adrenoceptor agonists and the Olympic Games in Athens 1 Appendix A of the Olympic Movement Anti-Doping Code, the List of Prohibited Substances and Prohibited Methods dated 1 st January 2003 states
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Impact of Asthma in the U.S. per Year. Asthma Epidemiology and Pathophysiology. Risk Factors for Asthma. Childhood Asthma Costs of Asthma
 American Association for Respiratory Care Asthma Educator Certification Prep Course Asthma Epidemiology and Pathophysiology Robert C. Cohn, MD, FAARC MetroHealth Medical Center Cleveland, OH Impact of
American Association for Respiratory Care Asthma Educator Certification Prep Course Asthma Epidemiology and Pathophysiology Robert C. Cohn, MD, FAARC MetroHealth Medical Center Cleveland, OH Impact of
Prof Neil Barnes. Respiratory and General Medicine London Chest Hospital and The Royal London Hospital
 Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Current Asthma Therapy: Little Need to Phenotype. Phenotypes of Severe Asthma. Cellular Phenotypes 12/7/2012
 Subbasement Membrane Thickness(µm) 12/7/212 Current Asthma Therapy: Little Need to Phenotype Phenotypes of Severe Asthma Most mild and to some degree moderate asthmatics respond well to currently available
Subbasement Membrane Thickness(µm) 12/7/212 Current Asthma Therapy: Little Need to Phenotype Phenotypes of Severe Asthma Most mild and to some degree moderate asthmatics respond well to currently available
Scottish Medicines Consortium
 Scottish Medicines Consortium budesonide/formoterol 100/6, 200/6 turbohaler (Symbicort SMART ) No. (362/07) Astra Zeneca UK Limited 9 March 2007 (Issued May 2007) The Scottish Medicines Consortium (SMC)
Scottish Medicines Consortium budesonide/formoterol 100/6, 200/6 turbohaler (Symbicort SMART ) No. (362/07) Astra Zeneca UK Limited 9 March 2007 (Issued May 2007) The Scottish Medicines Consortium (SMC)
Phenotypes of asthma; implications for treatment. Medical Grand Rounds Feb 2018 Jim Martin MD DSc
 Phenotypes of asthma; implications for treatment Medical Grand Rounds Feb 2018 Jim Martin MD DSc No conflicts to declare Objectives To understand the varied clinical forms of asthma To understand the pathobiologic
Phenotypes of asthma; implications for treatment Medical Grand Rounds Feb 2018 Jim Martin MD DSc No conflicts to declare Objectives To understand the varied clinical forms of asthma To understand the pathobiologic
Financial Disclosure. Exercise Induced Bronchospasm BHR. Exercise Induced Asthma
 Financial Disclosure Exercise Induced Bronchospasm Elizabeth Bailey MSN, CRNP Allergy & Asthma Specialists BREATHE II March, 23, 2012 I have no commercial conflicts of interest and no financial relationships
Financial Disclosure Exercise Induced Bronchospasm Elizabeth Bailey MSN, CRNP Allergy & Asthma Specialists BREATHE II March, 23, 2012 I have no commercial conflicts of interest and no financial relationships
TORCH: Salmeterol and Fluticasone Propionate and Survival in COPD
 TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Action plans, and asthma self-management, 47 51 education on, 48 49 health literacy-based education on, 49 50 Airway hyperresponsiveness, assessment
Note: Page numbers of article titles are in boldface type. A Action plans, and asthma self-management, 47 51 education on, 48 49 health literacy-based education on, 49 50 Airway hyperresponsiveness, assessment
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Alternatives to exercise challenge for the objective assessment of exerciseinduced
 Alternatives to exercise challenge for the objective assessment of exerciseinduced bronchospasm: eucapnic voluntary hyperpnoea and the osmotic challenge tests Educational aims To describe alternative tests
Alternatives to exercise challenge for the objective assessment of exerciseinduced bronchospasm: eucapnic voluntary hyperpnoea and the osmotic challenge tests Educational aims To describe alternative tests
Outline FEF Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications?
 Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
KEY WORDS airflow limitation, airway hyperresponsiveness, airway inflammation, airway lability, peak expiratory flow rate
 Allergology International. 2013;62:343-349 DOI: 10.2332 allergolint.13-oa-0543 ORIGINAL ARTICLE Stratifying a Risk for an Increased Variation of Airway Caliber among the Clinically Stable Asthma Atsushi
Allergology International. 2013;62:343-349 DOI: 10.2332 allergolint.13-oa-0543 ORIGINAL ARTICLE Stratifying a Risk for an Increased Variation of Airway Caliber among the Clinically Stable Asthma Atsushi
Meeting the Challenges of Asthma
 Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
**This form MUST accompany a TUE Application for a Beta-2 Agonist if submitted to USADA**
 **This form MUST accompany a TUE Application for a Beta-2 Agonist if submitted to USADA** PHYSICIAN- You must select one of the Objective Tests in the Table below and report the result. Please take note
**This form MUST accompany a TUE Application for a Beta-2 Agonist if submitted to USADA** PHYSICIAN- You must select one of the Objective Tests in the Table below and report the result. Please take note
Joint Session ACOFP and AOASM: Exercise Induced Asthma. Bruce Dubin, DO, JD, FCLM, FACOI
 Joint Session ACOFP and AOASM: Exercise Induced Asthma Bruce Dubin, DO, JD, FCLM, FACOI ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please check where applicable and sign below. Provide additional pages as
Joint Session ACOFP and AOASM: Exercise Induced Asthma Bruce Dubin, DO, JD, FCLM, FACOI ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please check where applicable and sign below. Provide additional pages as
This is a cross-sectional analysis of the National Health and Nutrition Examination
 SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
The Clinical Phenotype of Asthma in Obesity. Anne Dixon, MA, BM, BCh
 The Clinical Phenotype of Asthma in Obesity Anne Dixon, MA, BM, BCh Outline Epidemiology How obesity effects clinical phenotype Phenotypes of asthma in the obese Obesity Trends* Among U.S. Adults BRFSS,
The Clinical Phenotype of Asthma in Obesity Anne Dixon, MA, BM, BCh Outline Epidemiology How obesity effects clinical phenotype Phenotypes of asthma in the obese Obesity Trends* Among U.S. Adults BRFSS,
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Clinical efficacy of montelukast in anti-inflammatory treatment of asthma and allergic rhinitis
 Clinical efficacy of montelukast in anti-inflammatory treatment of asthma and allergic rhinitis Kim Hyun Hee, MD, PhD. Dept. of Pediatrics The Catholic University of Korea College of Medicine Achieving
Clinical efficacy of montelukast in anti-inflammatory treatment of asthma and allergic rhinitis Kim Hyun Hee, MD, PhD. Dept. of Pediatrics The Catholic University of Korea College of Medicine Achieving
Outcome, classification and management of wheezing in preschool children Paul L.P. Brand
 Outcome, classification and management of wheezing in preschool children Paul L.P. Brand Princess Amalia Children s Clinic Isala klinieken, Zwolle the Netherlands p.l.p.brand@isala.nl Valle de la Luna,
Outcome, classification and management of wheezing in preschool children Paul L.P. Brand Princess Amalia Children s Clinic Isala klinieken, Zwolle the Netherlands p.l.p.brand@isala.nl Valle de la Luna,
Asthma in Pediatric Patients. DanThuy Dao, D.O., FAAP. Disclosures. None
 Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Evolution of asthma from childhood. Carlos Nunes Center of Allergy and Immunology of Algarve, PT
 Evolution of asthma from childhood Carlos Nunes Center of Allergy and Immunology of Algarve, PT allergy@mail.telepac.pt Questionnaire data Symptoms occurring once or several times at follow-up (wheeze,
Evolution of asthma from childhood Carlos Nunes Center of Allergy and Immunology of Algarve, PT allergy@mail.telepac.pt Questionnaire data Symptoms occurring once or several times at follow-up (wheeze,
Importance of fractional exhaled nitric oxide in diagnosis of bronchiectasis accompanied with bronchial asthma
 Original Article Importance of fractional exhaled nitric oxide in diagnosis of bronchiectasis accompanied with bronchial asthma Feng-Jia Chen, Huai Liao, Xin-Yan Huang, Can-Mao Xie Department of Respiratory
Original Article Importance of fractional exhaled nitric oxide in diagnosis of bronchiectasis accompanied with bronchial asthma Feng-Jia Chen, Huai Liao, Xin-Yan Huang, Can-Mao Xie Department of Respiratory
HCT Medical Policy. Bronchial Thermoplasty. Policy # HCT113 Current Effective Date: 05/24/2016. Policy Statement. Overview
 HCT Medical Policy Bronchial Thermoplasty Policy # HCT113 Current Effective Date: 05/24/2016 Medical Policies are developed by HealthyCT to assist in administering plan benefits and constitute neither
HCT Medical Policy Bronchial Thermoplasty Policy # HCT113 Current Effective Date: 05/24/2016 Medical Policies are developed by HealthyCT to assist in administering plan benefits and constitute neither
Allergic Rhinitis and Its Impact on Ast. Rhinitis: A Risk Factor for Asthma? Ronald Dahl, Aarhus University Hospital, Denmark
 Allergic Rhinitis and Its Impact on Ast Rhinitis: A Risk Factor for Asthma? Ronald Dahl, Aarhus University Hospital, Denmark Rhinitis and asthma SIT-SLIT Evidence A SIT-SLIT Evidence A? SIT Evidence? Rhinitis
Allergic Rhinitis and Its Impact on Ast Rhinitis: A Risk Factor for Asthma? Ronald Dahl, Aarhus University Hospital, Denmark Rhinitis and asthma SIT-SLIT Evidence A SIT-SLIT Evidence A? SIT Evidence? Rhinitis
Current Asthma Management: Opportunities for a Nutrition-Based Intervention
 Current Asthma Management: Opportunities for a Nutrition-Based Intervention Stanley J. Szefler, MD Approximately 22 million Americans, including 6 million children, have asthma. It is one of the most prevalent
Current Asthma Management: Opportunities for a Nutrition-Based Intervention Stanley J. Szefler, MD Approximately 22 million Americans, including 6 million children, have asthma. It is one of the most prevalent
Asthma: Chronic Management. Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015
 Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
CME/CE POSTTEST CME/CE QUESTIONS
 CME/CE POSTTEST CME/CE QUESTIONS Controlling Asthma Severity: Identifying Unmet Needs and Optimizing Therapeutic Options There are no fees for participating in and receiving continuing medical education
CME/CE POSTTEST CME/CE QUESTIONS Controlling Asthma Severity: Identifying Unmet Needs and Optimizing Therapeutic Options There are no fees for participating in and receiving continuing medical education
Biologic Therapy in the Management of Asthma. Nabeel Farooqui, MD
 Biologic Therapy in the Management of Asthma Nabeel Farooqui, MD None Disclosures Objectives Define severe asthma phenotypes and endotypes Describe the role of biologics in asthma management Review pivotal
Biologic Therapy in the Management of Asthma Nabeel Farooqui, MD None Disclosures Objectives Define severe asthma phenotypes and endotypes Describe the role of biologics in asthma management Review pivotal
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Medicine Dr. Kawa Lecture 1 Asthma Obstructive & Restrictive Pulmonary Diseases Obstructive Pulmonary Disease Indicate obstruction to flow of air
 Medicine Dr. Kawa Lecture 1 Asthma Obstructive & Restrictive Pulmonary Diseases Obstructive Pulmonary Disease Indicate obstruction to flow of air through the airways. As asthma, COPD ( chronic bronchitis
Medicine Dr. Kawa Lecture 1 Asthma Obstructive & Restrictive Pulmonary Diseases Obstructive Pulmonary Disease Indicate obstruction to flow of air through the airways. As asthma, COPD ( chronic bronchitis
Dual-Controller Asthma Therapy: Rationale and Clinical Benefits
 B/1 Dual-Controller Asthma Therapy: Rationale and Clinical Benefits MODULE B The 1997 National Heart, Lung, and Blood Institute (NHLBI) Expert Panel guidelines on asthma management recommend a 4-step approach
B/1 Dual-Controller Asthma Therapy: Rationale and Clinical Benefits MODULE B The 1997 National Heart, Lung, and Blood Institute (NHLBI) Expert Panel guidelines on asthma management recommend a 4-step approach
Putting NICE guidance into practice. Resource impact report: Asthma: diagnosis, monitoring and chronic asthma management (NG80)
") Putting NICE guidance into practice Resource impact report: Asthma: diagnosis, monitoring and chronic asthma management (NG80) Published: November 2017 Summary This report focuses on the recommendations
Putting NICE guidance into practice Resource impact report: Asthma: diagnosis, monitoring and chronic asthma management (NG80) Published: November 2017 Summary This report focuses on the recommendations
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Exercise-Induced Bronchoconstriction EIB
 Exercise-Induced Bronchoconstriction EIB Case 1 14 yo boy, freshman in high school Complains of shortness of breath 2 minutes into a mile-run in his first gym class Same complains in his 2 nd gym class
Exercise-Induced Bronchoconstriction EIB Case 1 14 yo boy, freshman in high school Complains of shortness of breath 2 minutes into a mile-run in his first gym class Same complains in his 2 nd gym class
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies
 Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
THE PROMISE OF NEW AND NOVEL DRUGS. Pyng Lee Respiratory & Critical Care Medicine National University Hospital
 THE PROMISE OF NEW AND NOVEL DRUGS Pyng Lee Respiratory & Critical Care Medicine National University Hospital Pyng_lee@nuhs.edu.sg Asthma Prevalence, Morbidity, Mortality 235 million suffer from asthma
THE PROMISE OF NEW AND NOVEL DRUGS Pyng Lee Respiratory & Critical Care Medicine National University Hospital Pyng_lee@nuhs.edu.sg Asthma Prevalence, Morbidity, Mortality 235 million suffer from asthma
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Is it Under Diagnosed?
 Asthma in Icehockey Is it Under Diagnosed? Dr. med. B. Villiger CEO, Schweizer Paraplegiker Zentrum Nottwil Asthma bronchiale Mechanism Inflammation Remodelling Bronchial Hyperreactivity Airway - obstruction
Asthma in Icehockey Is it Under Diagnosed? Dr. med. B. Villiger CEO, Schweizer Paraplegiker Zentrum Nottwil Asthma bronchiale Mechanism Inflammation Remodelling Bronchial Hyperreactivity Airway - obstruction
AHEAD OF PRINT - ARTICLE IN PRESS
 Prim Care Respir J 2011; 20(x): - RESEARCH PAPER Feasibility and acceptability of using bronchial hyperresponsiveness to manage asthma in primary care: a pilot study *James A Turton a, Nicholas J Glasgow
Prim Care Respir J 2011; 20(x): - RESEARCH PAPER Feasibility and acceptability of using bronchial hyperresponsiveness to manage asthma in primary care: a pilot study *James A Turton a, Nicholas J Glasgow
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network
 Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Content Indica c tion Lung v olumes e & Lung Indica c tions i n c paci c ties
 Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
Do We Need Biologics in Pediatric Asthma Management?
 Do We Need Biologics in Pediatric Asthma Management? Ting Fan LEUNG, MBChB, MD, FRCPCH, FAAAAI Professor and Chairman Department of Paediatrics The Chinese University of Hong Kong Asthma and Allergy by
Do We Need Biologics in Pediatric Asthma Management? Ting Fan LEUNG, MBChB, MD, FRCPCH, FAAAAI Professor and Chairman Department of Paediatrics The Chinese University of Hong Kong Asthma and Allergy by
Diet, Obesity and Asthma: evidence based advice on healthy eating for asthma A/Prof Lisa Wood
 Diet, Obesity and Asthma: evidence based advice on healthy eating for asthma A/Prof Lisa Wood Centre for Asthma and Respiratory Disease University of Newcastle and Hunter Medical Research Institute NSW
Diet, Obesity and Asthma: evidence based advice on healthy eating for asthma A/Prof Lisa Wood Centre for Asthma and Respiratory Disease University of Newcastle and Hunter Medical Research Institute NSW
University of Groningen. Indirect bronchial provocation tests in childhood asthma Kersten, Elin
 University of Groningen Indirect bronchial provocation tests in childhood asthma Kersten, Elin IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from
University of Groningen Indirect bronchial provocation tests in childhood asthma Kersten, Elin IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from
Diagnosis and Management of Fungal Allergy Monday, 9-139
 Diagnosis and Management of Fungal Allergy Monday, 9-139 13-2010 Alan P. Knutsen,, MD Director, Pediatric Allergy & Immunology Director, Jeffrey Modell Diagnostic Center for Primary Immunodeficiencies
Diagnosis and Management of Fungal Allergy Monday, 9-139 13-2010 Alan P. Knutsen,, MD Director, Pediatric Allergy & Immunology Director, Jeffrey Modell Diagnostic Center for Primary Immunodeficiencies
ALLERGEN-INDUCED CHANGE IN AIRWAY RESPONSIVENESS TO DIRECT AND INDIRECT STIMULI IN MILD ATOPIC ASTHMATICS.
 ALLERGEN-INDUCED CHANGE IN AIRWAY RESPONSIVENESS TO DIRECT AND INDIRECT STIMULI IN MILD ATOPIC ASTHMATICS. A Thesis Submitted to the College of Graduate Studies and Research In Partial Fulfillment of the
ALLERGEN-INDUCED CHANGE IN AIRWAY RESPONSIVENESS TO DIRECT AND INDIRECT STIMULI IN MILD ATOPIC ASTHMATICS. A Thesis Submitted to the College of Graduate Studies and Research In Partial Fulfillment of the
Clinical trial efficacy: What does it really tell you?
 Clinical trial efficacy: What does it really tell you? Joseph Spahn, MD Denver, Colo The primary goal of most clinical trials is an evaluation of the efficacy of the drug being evaluated. Therefore, it
Clinical trial efficacy: What does it really tell you? Joseph Spahn, MD Denver, Colo The primary goal of most clinical trials is an evaluation of the efficacy of the drug being evaluated. Therefore, it
COPD or not COPD, that is the question.
 COPD or not COPD, that is the question. Asthma-COPD Overlap Syndrome: ACOS Do we really need this? Michelle Harkins Disclosure Slide Slide help - William Busse, MD Organizational Interests ATS, ACCP, ACP
COPD or not COPD, that is the question. Asthma-COPD Overlap Syndrome: ACOS Do we really need this? Michelle Harkins Disclosure Slide Slide help - William Busse, MD Organizational Interests ATS, ACCP, ACP
Pediatric Asthma: Pharmacotherapy. Joseph Spahn, MD Children s Hospital Colorado & University of Colorado Medical School Aurora, Colorado
 Pediatric Asthma: Pharmacotherapy Joseph Spahn, MD Children s Hospital Colorado & University of Colorado Medical School Aurora, Colorado Pediatric Asthma: Pharmacotherapy Disclosures/Conflicts of Interest:
Pediatric Asthma: Pharmacotherapy Joseph Spahn, MD Children s Hospital Colorado & University of Colorado Medical School Aurora, Colorado Pediatric Asthma: Pharmacotherapy Disclosures/Conflicts of Interest:
Potent and Selective CRTh2 Antagonists are Efficacious in Models of Asthma, Allergic Rhinitis and Atopic Dermatitis
 Potent and Selective CRTh2 Antagonists are Efficacious in Models of Asthma, Allergic Rhinitis and Atopic Dermatitis Laura L. Carter, Yoshi Shiraishi, Yooseob Shin, Laurence Burgess, Christine Eberhardt,
Potent and Selective CRTh2 Antagonists are Efficacious in Models of Asthma, Allergic Rhinitis and Atopic Dermatitis Laura L. Carter, Yoshi Shiraishi, Yooseob Shin, Laurence Burgess, Christine Eberhardt,
C ough variant asthma, gastro-oesophageal reflux associated
 14 ASTHMA Comparison of atopic cough with cough variant asthma: is atopic cough a precursor of asthma? M Fujimura, H Ogawa, Y Nishizawa, K Nishi... See end of article for authors affiliations... Correspondence
14 ASTHMA Comparison of atopic cough with cough variant asthma: is atopic cough a precursor of asthma? M Fujimura, H Ogawa, Y Nishizawa, K Nishi... See end of article for authors affiliations... Correspondence
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting