Taking the harm out of Polypharmacy Step by step. Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian
|
|
|
- Sharon Bradley
- 6 years ago
- Views:
Transcription
1 Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian
2 Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application of the guidelines in the care home setting Workshop: Polypharmacy case Feedback and comparison with pharmacist s review
3 Appropriate polypharmacy? All medicines are prescribed for the purpose of achieving specific therapeutic objectives Therapeutic objectives are being achieved Therapy has been optimised to minimise the risk of adverse drug reactions The patient is motivated and able to take all medicines as intended
4 Inappropriate polypharmacy? No evidence based indication, the indication has expired or the dose is unnecessarily high One or more medicines fail to achieve the therapeutic objective One or the combination of medicines cause unacceptable ADR s The patient is not willing or able to take the medicines as intended

5

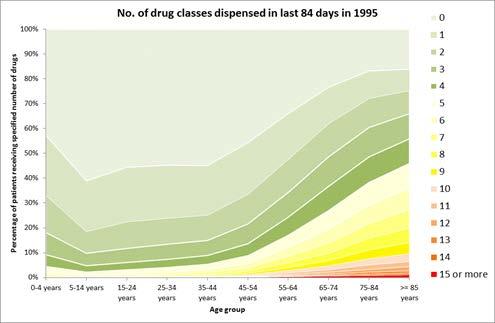
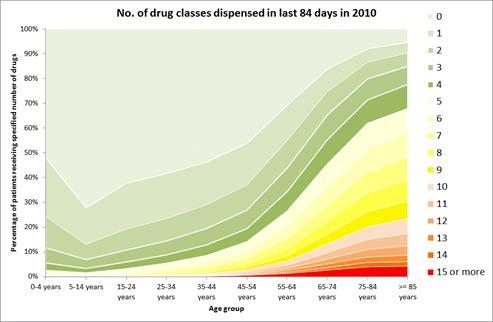
6 Multimorbidity in Scotland Mercer, Guthrie, Wyke: Scottish School of Primary Care
7
8
9 Contributory Factors Patient expectation Limited patient engagement? Prescriber attitude (it s easier to start prescription...) Original indication unclear Consultations with several prescribers Guidelines unipathology Primary care Quality Outcome Framework (QOF) targets? Hospitalisation, especially repeat episodes of care Poor communication across the interfaces
10
11
12 The Polypharmacy Guidance macy_guidance.pdf The Knowledge Network Mobile App Library at ome/tools-and-apps/mobileknowledge/search.aspx?device=non e&q=polypharmacy&p=1&rpp=20 itunes and Google Play app stores.
13
14
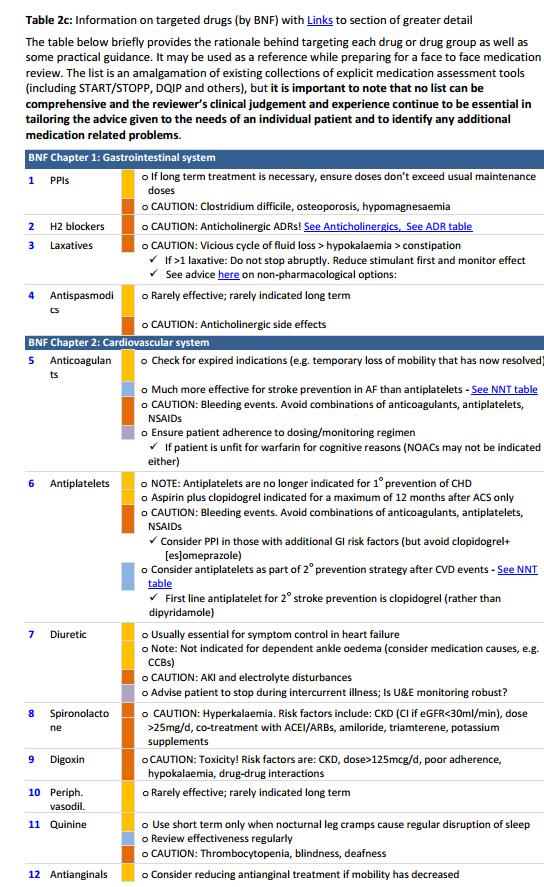
15 How does the guideline aim to help? Clear structure for a drug review Empower the patient and the clinician to make decisions on what to take and why Case studies Medication safety Drug efficacy and applicability table
16
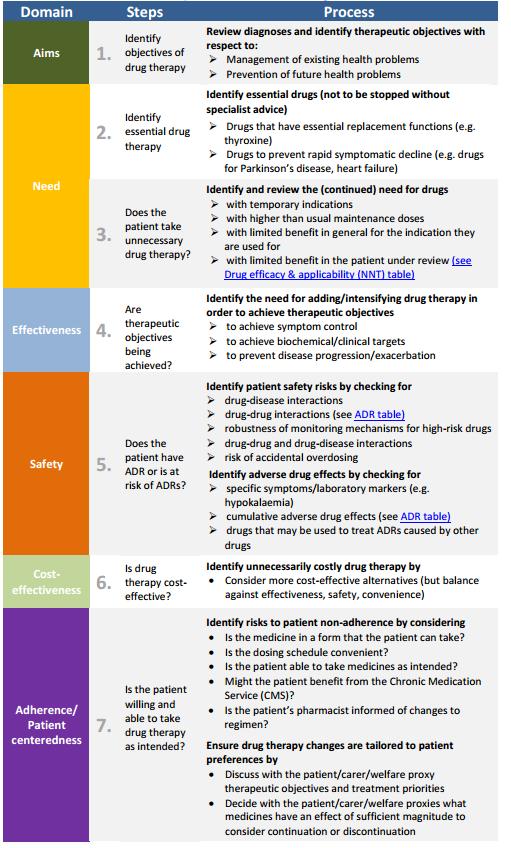
17 Step 1 Aim What are you trying to achieve? Is the priority: Prevention/risk reduction? Symptom management? What does the patient want?
18 Step 2 and 3 need... essential versus non essential If a drug doesn t have a clear ongoing reason stop it Consider duration was long term treatment intended? Has the evidence base changed? If there are multiple drugs for 1 indication? Do you need them all? Is there an indication without a drug?
19 Step 4 Effectiveness Diabetic with neuropathic pain on Gabapentin seems reasonable but is it helping? Elderly lady with urinary incontinence on Solifenacin seems reasonable but is it helping? 80 year old man with a history of gout on allopurinol 100mg once daily for > 20 years and no urate level on file are we achieving our treatment goal?
20 Step 5 Safety Ask the patient Open question - any side effects? Can specific/closed questioning tease them out? High risk combinations Additive effects e.g. Anticholinergic burden Consider pro-active monitoring to avoid harm Consider the therapeutic cascade
21 Step 6 Cost-effective? Pharmacy reviews 109 patient Identifying non compliance and stopping medicines the patient is not taking Stopping unnecessary medicines Reducing unnecessarily high doses consider cost-effective formulations/formulary choices/scriptswitch
22 Step 7 Adherence/Patient centredness Is the patient willing and able to take the medicine as intended Identify risks to patient non-adherence by considering Is the prescription in a form the patient can take? Is dosing convenient?
23
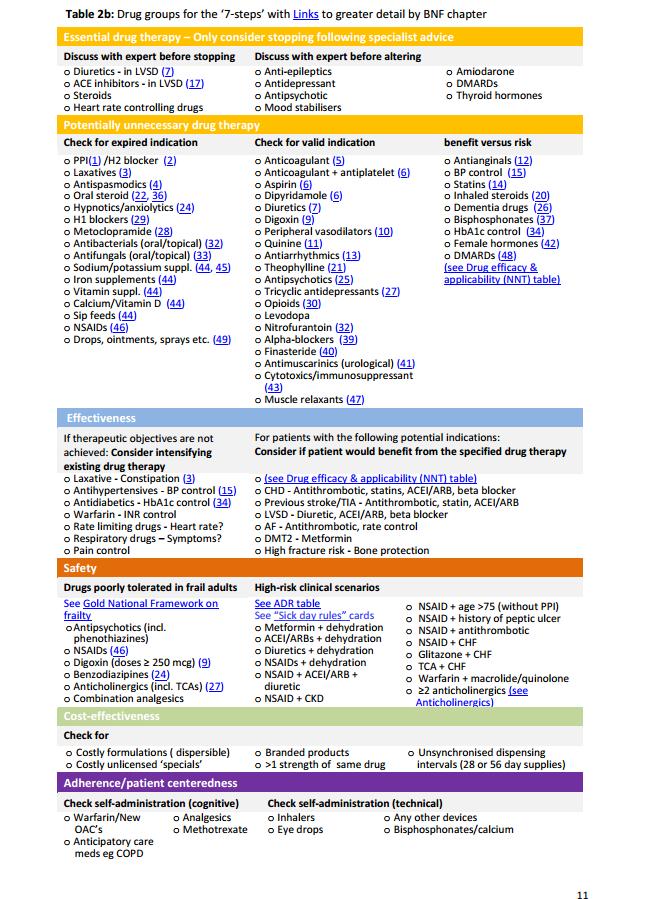
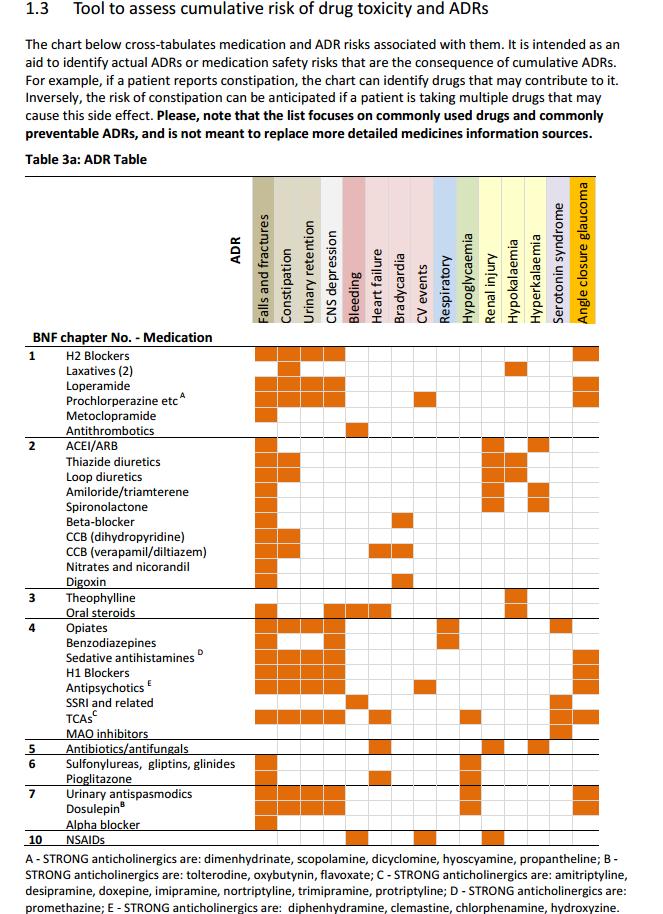
24 Safety Drugs poorly tolerated in frail adults See Gold National Framework on frailty o Antipsychotics (incl. phenothiazines) o NSAIDs (46) o Digoxin (doses? 250 mcg) (9) o Benzodiazipines (24) o Anticholinergics (incl. TCAs) (27) o Combination analgesics High-risk clinical scenarios See ADR table o Metformin + dehydration o ACEI/ARBs + dehydration o Diuretics + dehydration o NSAIDs + dehydration o NSAID + ACEI/ARB + diuretic o NSAID + CKD o NSAID + age >75 (without PPI) o NSAID + history of peptic ulcer o NSAID + antithrombotic o NSAID + CHF o Glitazone + CHF o TCA + CHF o Warfarin + macrolide/quinolone o?2 anticholinergics (see Anticholinergics)
25
26 Safety Drugs poorly tolerated in frail adults See Gold National Framework on frailty o Antipsychotics (incl. phenothiazines) o NSAIDs (46) o Digoxin (doses? 250 mcg) (9) o Benzodiazipines (24) o Anticholinergics (incl. TCAs) (27) o Combination analgesics High-risk clinical scenarios See ADR table o Metformin + dehydration o ACEI/ARBs + dehydration o Diuretics + dehydration o NSAIDs + dehydration o NSAID + ACEI/ARB + diuretic o NSAID + CKD o NSAID + age >75 (without PPI) o NSAID + history of peptic ulcer o NSAID + antithrombotic o NSAID + CHF o Glitazone + CHF o TCA + CHF o Warfarin + macrolide/quinolone o?2 anticholinergics (see Anticholinergics)
27
28 Hot topics Anticholinergics Medication and risk of falls in the older person Antipsychotics in patients with dementia Benzodiazepines and z drugs Management of constipation Management of blood glucose control
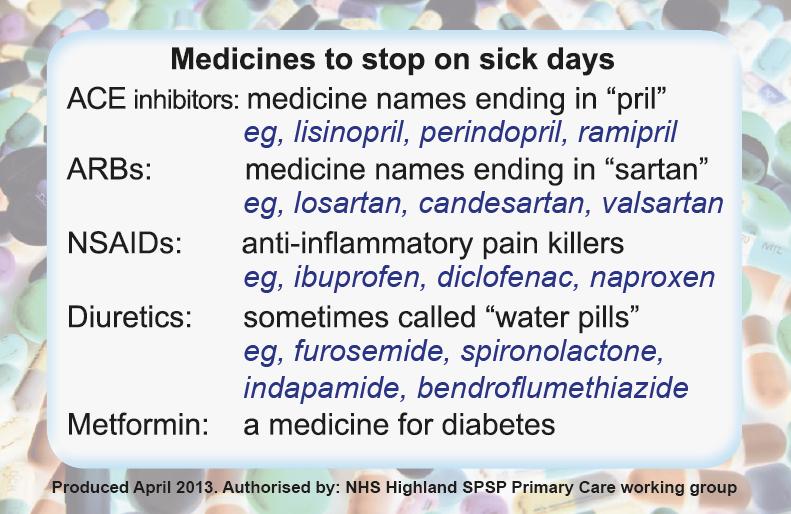
29 Appendices Patient information leaflet on medicines and dehydration Medicine sick day rule cards NNT explained Health economics and analysis of polypharmacy review Indicators and monitoring


30
31 Life expectancy and NNTs Some older, frail people are likely to die within a few months Continuing secondary prevention medication in this group is probably not useful Use of NNT data from trials has been proposed as a way of identifying medications that are unlikely to benefit those with limited life expectancy
32
33 NHS Lothian Polypharmacy Review Jan 2012 onwards All 126 GP practices in NHS Lothian invited to participate in Service Level Agreements (SLA) Aims To target priority patient groups - those most at risk of ADRs: care home residents, frail housebound, those on high-risk medications (either alone or in combination). To carry out systematic medication reviews to optimise medicines minimise medicines which may be harmful (particularly in those experiencing ADRs) or no longer appropriate, maximise benefit in line with NHS Lothian Polypharmacy Guidance for prescribing in frail adults (based on NHS Highland guidance, later Scottish guidance 1 st ed Oct 2012) To undertake joint review discussions GP/patient/pharmacist and implement changes
34 SUMMARY 2012/ / /15 to date patient cohort care home residents plus 24 patients per practice aged >75yrs on >10 repeat meds at least one of which high risk 24 patients per practice aged >75yrs with SPARRA score 40-60% having received meds from >10 BNF sections one of which high risk care home residents plus 24 patients per practice aged >75yrs with SPARRA score 40-60% having received meds from >10 BNF sections one of which high risk no. practices signed up to SLA/126 practices NHS Lothian no. patient medication reviews /4858 no. medicines stopped of which high risk medicines no. medicines with dose reduced no. medicines with dose increased no. medicines started no. medicines switched estimated medicines cost/patient/year saved ( )

35 Multidisciplinary team working key to success
36 Polypharmacy Case Patient characteristics Age: 88 Sex: Male Weight:63kg Relevant Medical History COPD Hypertension T2DM Eczema LVF moderate Drug allergies No known drug allergies Current Medication Metformin 500mg daily Ferrous Sulphate 200mg three times a day Macrogol 3350 sachets One sachet as required Simvastatin 20mg nocte Furosemide 40mg daily Tamsulosin MR 400micrograms daily Amlodipine 5mg daily Quinine 300mg nocte Omeprazole 20mg daily Paracetamol 1g 4 to 6hourly as required Salbutamol 100micrograms 2 puffs when required Symbicort 400/12 1 puff twice daily Aqueous cream to be used as directed Calmurid cream to be applied as directed twice daily Available Results BP 120/65 HbA1c 36 Hb 108 MCV 91 platelets 167 Cr Cl 20mls/min e GFR 30mls/min/1.73m2 Cholesterol 3.6 Suggested medication changes (Please mark with a cross in the appropriate column whether you would continue/modify or stop e listed medication. Where possible, please list your rationale for change)
37 Current Medication Dose Suggested change Metformin Ferrous Sulphate Macrogol 3350 sachets Simvastatin Furosemide Tamsulosin MR Amlodipine Quinine Omeprazole Paracetamol Salbutamol 100micrograms Symbicort 400/12 Aqueous cream Calmurid cream 500mg daily 200mg three times a day One sachet as required 20mg nocte 40mg daily 400micrograms daily 5mg daily 300mg nocte 20mg daily 1g 4 to 6hourly as required 2 puffs when required 1 puff twice daily use as directed applied as directed twice daily Continue Modify Dose Stop (please specify to what) Rationale for suggested change (or no change)
38 Care Home Polypharmacy Review PMH MH COPD Hypertension T2DM Eczema LVF moderate Metformin 500mg daily Ferrous Sulphate 200mg three times a day Macrogol 3350 sachets One sachet as required Simvastatin 20mg daily Furosemide 40mg daily Tamsulosin MR 400micrograms daily Amlodipine 5mg daily Quinine 300mg nocte Omeprazole 20mg daily Paracetamol 1g 4 to 6hourly as required Salbutamol 100micrograms 2 puffs when required Symbicort 400/12 1 puff twice daily Aqueous cream to be used as directed Calmurid cream to be applied as directed twice daily
39 Most recent Investigations BP 120/65 HbA1c 36 Hb 108 MCV 91 platelets 167 Cr Cl 20mls/min e GFR 30mls/min/1.73m2 Cholesterol 3.6 Other points of note Long term urinary catheter No known drug allergies
40 Past Medical History Medicine History Pharmaceutical Care Issues COPD Salbutamol 100micrograms 2 puffs when required Symbicort 400/12 1 puff twice daily Spirometry did not support diagnosis of COPD. Not known to respiratory. If asthma trial of stepping down. Check inhaler technique Hypertension Amlodipine 5mg daily Last BP 120/65 recheck BP and review need T2DM Metformin 500mg daily egfr 30ml/min/1.73m2 CrCl 20mls/min HbA1c 36
41 Past Medical History Medicine History Pharmaceutical Care Issues Eczema Aqueous cream to be used as directed Calmurid cream to be applied as directed BD Calmurid last ordered 18 months ago. Review eczema symptoms and treatment. LVF Furosemide 40mg daily Monitor symptoms of LVF balance between optimising treatment without deteriorating renal function.?anaemia Ferrous sulphate 200mg three times a day Hb chronically low despite long term treatment. Bloods do not reflect an iron deficient picture. Metformin can cause Vitamin B12 deficiency? Fe/Vitamin B12/folate not measured.?anaemia of chronic disease?investigate cause
42 Past Medical History Medicine History Pharmaceutical Care Issues?Primary prevention Simvastatin 20mg daily Cholesterol 3.6 review risk/benefit?urinary retention Tamsulosin MR 400micrograms daily Long term catheter in situ review need?gastroprotection Omeprazole 20mg daily Review need. Reduce to 10mg with a view to stopping
43 Past Medical History Medicine History Pharmaceutical Care Issues Constipation Macrogol 3350 sachets 1 sachet as required Review use. Constipation may be caused by Ferrous sulphate?night cramps Quinine 300mg nocte Review effectiveness. Routine treatment not recommended?pain Paracetamol 1g 4 to 6hourly as required Review use.
44
45 Care Home Polypharmacy Review PMH MH COPD Hypertension T2DM Eczema LVF moderate Metformin 500mg daily Ferrous Sulphate 200mg three times a day Macrogol 3350 sachets 1 sachet as required Simvastatin 20mg daily Furosemide 40mg daily Tamsulosin MR 400micrograms daily Amlodipine 5mg daily Quinine 300mg nocte Omeprazole 20mg daily Paracetamol 1g 4 to 6hourly as required Salbutamol 100micrograms 2 puffs when required Symbicort 400/12 1 puff twice daily Aqueous cream to be used as directed Calmurid cream to be applied as directed twice daily
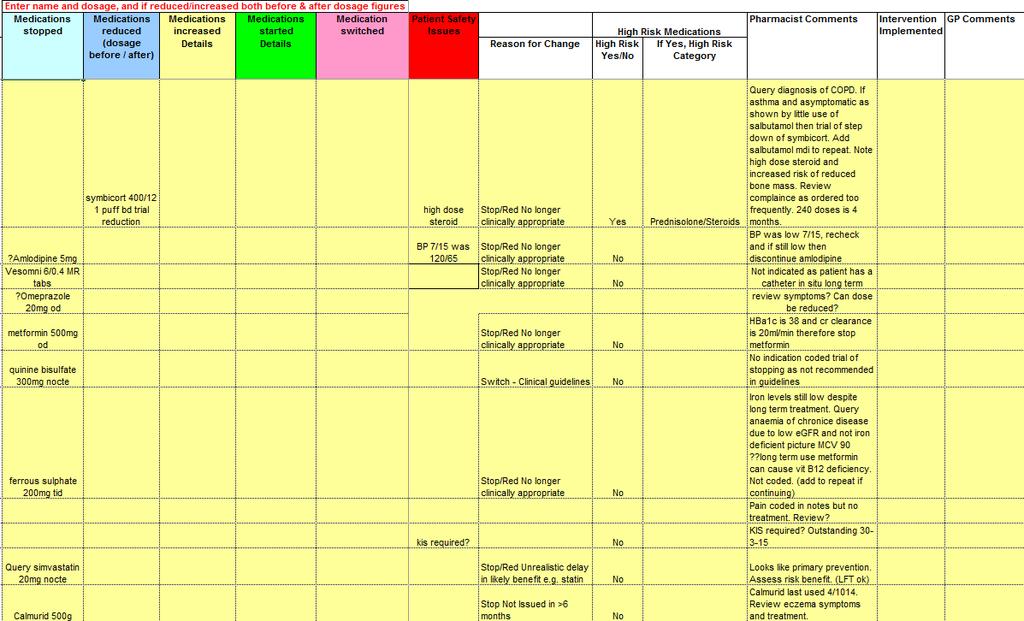
46 Current Medication Dose Suggested change Rationale for suggested change (or no change) Continue Modify Dose Stop (please specify to what) Metformin 500mg daily egfr 30ml/min/1.73m2 CrCl 20mls/min HbA1c 36 Ferrous Sulphate 200mg three times a day Hb chronically low despite long term treatment. Bloods do not reflect an iron deficient picture. Metformin can cause Vitamin B12 deficiency Fe/Vitamin B12/folate not measured.?anaemia of chronic disease?investigate cause Macrogol 3350 sachets One sachet as required Review use. Constipation may be caused by Ferrous sulphate Simvastatin 20mg nocte? Cholesterol 3.6 review risk/benefit Furosemide 40mg daily Monitor symptoms of LVF balance between optimising treatment without deteriorating renal function. Tamsulosin MR 400micrograms daily Long term catheter in situ review need Amlodipine 5mg daily Last BP 120/65; recheck BP and review need Quinine 300mg nocte Review effectiveness. Routine treatment not recommended Omeprazole 20mg daily Review need. Reduce to 10mg with a view to stopping Paracetamol 1g 4 to 6hrly as required Review use. Salbutamol 100micrograms 2 puffs when required Review use. Symbicort 400/12 1 puff twice daily Spirometry did not support diagnosis of COPD. Not known to respiratory. If asthma trial of stepping down. Check inhaler technique Aqueous cream use as directed Review use Calmurid cream applied as directed twice Calmurid last ordered 18 months ago. Review daily eczema symptoms and treatment.
47 Care Home Polypharmacy Review PMH COPD Hypertension T2DM Eczema LVF moderate MH Macrogol 3350 sachets 1 sachet as required Furosemide 40mg daily Omeprazole 10mg daily Paracetamol 1g 4 to 6hourly as required Salbutamol 100micrograms 2 puffs when required Symbicort 200/6 1 puff twice daily Aqueous cream to be used as directed
48 Many medicines are necessary Some are harmful Some are of variable benefit Understand the patient s perspective Taking the harm out of polypharmacy is everyone s responsibility
49 Right medicine Right dose Right reason Right time Right follow up in place





50 ...improve quality of life

51
Tackling inappropriate polypharmacy in NHS Scotland
 Tackling inappropriate polypharmacy in NHS Scotland Francesca Aaen Lead Care Homes Pharmacist - NHS Lanarkshire Heather Harrison - Senior Prescribing Advisor/ Chronic Pain Primary Care Service Development
Tackling inappropriate polypharmacy in NHS Scotland Francesca Aaen Lead Care Homes Pharmacist - NHS Lanarkshire Heather Harrison - Senior Prescribing Advisor/ Chronic Pain Primary Care Service Development
Cover images courtesy of jk1991 at FreeDigitalPhotos.net Infographics courtesy of SIMPATHY consortium
 If using any content from this document, please acknowledge the Scottish Government Polypharmacy Model of Care Group, 2018. When referencing this document, please use the following format: Scottish Government
If using any content from this document, please acknowledge the Scottish Government Polypharmacy Model of Care Group, 2018. When referencing this document, please use the following format: Scottish Government
Optimising prescribing in primary care in the face of multimorbidity and polypharmacy
 University of Dundee School of Medicine Optimising prescribing in primary care in the face of multimorbidity and polypharmacy Bruce Guthrie Professor of Primary Care Medicine, University of Dundee NICE
University of Dundee School of Medicine Optimising prescribing in primary care in the face of multimorbidity and polypharmacy Bruce Guthrie Professor of Primary Care Medicine, University of Dundee NICE
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Polypharmacy: Guidance for Prescribing in Frail Adults
 Polypharmacy: Guidance for Prescribing in Frail Adults Why is reviewing polypharmacy important? Medication is by far the most common form of medical intervention. Four out of five people aged over 75 years
Polypharmacy: Guidance for Prescribing in Frail Adults Why is reviewing polypharmacy important? Medication is by far the most common form of medical intervention. Four out of five people aged over 75 years
POLYPHARMACY. A practical approach to deprescribing in care homes. Care Home Pharmacy Team. Herts Valleys Clinical Commissioning Group
 POLYPHARMACY A practical approach to deprescribing in care homes. Care Home Pharmacy Team Herts Valleys Clinical Commissioning Group Neeta Gulhane Specialist Pharmaceutical Advisor Care Homes The Care
POLYPHARMACY A practical approach to deprescribing in care homes. Care Home Pharmacy Team Herts Valleys Clinical Commissioning Group Neeta Gulhane Specialist Pharmaceutical Advisor Care Homes The Care
PRESCRIBING IN THE ELDERLY. CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas
 PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
Reviewing Medicines in at risk patients care homes
 Reviewing Medicines in at risk patients care homes Clinical Medication Reviews by Pharmacists in Collaboration with GP Surgeries across Brighton and Hove CCG Liz Butterfield FRPharmS 19th April 2016 NICE:
Reviewing Medicines in at risk patients care homes Clinical Medication Reviews by Pharmacists in Collaboration with GP Surgeries across Brighton and Hove CCG Liz Butterfield FRPharmS 19th April 2016 NICE:
DEPRESCRIBING IN THE ELDERLY
 DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
Managing Polypharmacy: Thinking outside the box
 Managing Polypharmacy: Thinking outside the box Martin Wilson Consultant Physician Care of the Elderly NHS Highland Clare Morrison Lead Pharmacist (North) Senior Quality Clinical Lead NHS Highland Disclosure
Managing Polypharmacy: Thinking outside the box Martin Wilson Consultant Physician Care of the Elderly NHS Highland Clare Morrison Lead Pharmacist (North) Senior Quality Clinical Lead NHS Highland Disclosure
Polypharmacy Strategy for NHS Fife
 Polypharmacy Strategy for NHS Fife 2016-19 1 Introduction The purpose of this document is to describe the factors contributing to the issue of inappropriate polypharmacy as it relates to NHS Fife and proposes
Polypharmacy Strategy for NHS Fife 2016-19 1 Introduction The purpose of this document is to describe the factors contributing to the issue of inappropriate polypharmacy as it relates to NHS Fife and proposes
Alpana Mair, Deputy Chief Pharmaceutical Officer, Scottish Government (Chair)
") Acknowledgements It has been a pleasure to chair the development of this Polypharmacy Guidance 2015 and work with a team that are committed to improving outcomes for patients. This document has been produced
Acknowledgements It has been a pleasure to chair the development of this Polypharmacy Guidance 2015 and work with a team that are committed to improving outcomes for patients. This document has been produced
Deprescribing with Confidence Dr Sanjay Suman MD FRCP
 Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas
Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas
STOPP and START criteria October 2011
 # START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
# START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
Frailty: what s it all about?
 Frailty: what s it all about? What is frailty? 1. an inevitable consequence of aging 2. A state due to multiple long term conditions 3. A condition in which the person becomes fragile 4. A state associated
Frailty: what s it all about? What is frailty? 1. an inevitable consequence of aging 2. A state due to multiple long term conditions 3. A condition in which the person becomes fragile 4. A state associated
STOPP START Toolkit Supporting Medication Review in the Older Person
 STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
Medication Reviews within Care Homes. Catherine Armstrong
 Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
NSAIDs Change Package 2017/2018
 NSAIDs Change Package 2017/2018 Aim: To Reduce harm to patients from Non-Steroidal Anti-inflammatory Drugs (NSAIDs) in primary care Background A key aim of the Safety in Practice programme is to reduce
NSAIDs Change Package 2017/2018 Aim: To Reduce harm to patients from Non-Steroidal Anti-inflammatory Drugs (NSAIDs) in primary care Background A key aim of the Safety in Practice programme is to reduce
< = > less is more. De-diagnosing De-prescribing Non-testing
 < = > less is more De-diagnosing De-prescribing Non-testing Who says? Overdiagnosis Polypharmacy False positives Too much medicine Risk aversion $$$ Sources Prof David Le Couteur, Clin Pharm and Aged Care
< = > less is more De-diagnosing De-prescribing Non-testing Who says? Overdiagnosis Polypharmacy False positives Too much medicine Risk aversion $$$ Sources Prof David Le Couteur, Clin Pharm and Aged Care
Prescribing in the Elderly. Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry
 Prescribing in the Elderly Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry 24 th September 2014 Objectives Understand the significance of polypharmacy in the elderly Become familiar with the
Prescribing in the Elderly Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry 24 th September 2014 Objectives Understand the significance of polypharmacy in the elderly Become familiar with the
Doctors, Nurses... and pharmacists - why this threesome works. Vanessa Brown Brendan Duck RNZCGP GPCME 2014
 Doctors, Nurses... and pharmacists - why this threesome works. Vanessa Brown Brendan Duck RNZCGP GPCME 2014 What is a clinical pharmacist? Specialist Pharmacist Practitioner Post Graduate education and/or
Doctors, Nurses... and pharmacists - why this threesome works. Vanessa Brown Brendan Duck RNZCGP GPCME 2014 What is a clinical pharmacist? Specialist Pharmacist Practitioner Post Graduate education and/or
Mucky Meds: A (practical) approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP
 approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP") Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Intelligent Polypharmacy. Professor Colin P Bradley Department of General Practice University College Cork
 Intelligent Polypharmacy Professor Colin P Bradley Department of General Practice University College Cork Polypharmacy No standard definition 2005 review the use of medications that are not clinically
Intelligent Polypharmacy Professor Colin P Bradley Department of General Practice University College Cork Polypharmacy No standard definition 2005 review the use of medications that are not clinically
Frailty & Polypharmacy
 Frailty & Polypharmacy Elderly with LUTS Recognition and Management Dr Sanjay Suman MD FRCP Clinical Director Elderly Care Medway Maritime Hospital Kent Declaration of interests Honoraria and Advisory
Frailty & Polypharmacy Elderly with LUTS Recognition and Management Dr Sanjay Suman MD FRCP Clinical Director Elderly Care Medway Maritime Hospital Kent Declaration of interests Honoraria and Advisory
Care homes: Good practice guide to prescribing and medication reviews
 B112i. October 2015 Care homes: Good practice guide to prescribing and medication reviews The effective management of medicines in care homes requires robust systems to be in place as well as good communication
B112i. October 2015 Care homes: Good practice guide to prescribing and medication reviews The effective management of medicines in care homes requires robust systems to be in place as well as good communication
Identifying and Managing Chronic Kidney Disease: A Practical Approach
 Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Proactive Care Pharmacy Services
 Proactive Care Pharmacy Services Achieving excellence and efficiency in holistic domiciliary care Kayt Blythin Senior Clinical pharmacist Proactive Care Coastal 20 Jan 2015; update June 2015 Proactive
Proactive Care Pharmacy Services Achieving excellence and efficiency in holistic domiciliary care Kayt Blythin Senior Clinical pharmacist Proactive Care Coastal 20 Jan 2015; update June 2015 Proactive
If using any content from this document, please acknowledge the Scottish Government Polypharmacy Model of Care Group, 2018.
 3 rd Edition, 2018 If using any content from this document, please acknowledge the Scottish Government Polypharmacy Model of Care Group, 2018. When referencing this document, please use the following format:
3 rd Edition, 2018 If using any content from this document, please acknowledge the Scottish Government Polypharmacy Model of Care Group, 2018. When referencing this document, please use the following format:
Asthma: Room for improvement in management. Hasanin Khachi Lead Respiratory Medicine Pharmacist Barts Health NHS Trust July 2014
 Asthma: Room for improvement in management Hasanin Khachi Lead Respiratory Medicine Pharmacist Barts Health NHS Trust July 2014 Challenges that the NHS faces are well documented What are the challenges?
Asthma: Room for improvement in management Hasanin Khachi Lead Respiratory Medicine Pharmacist Barts Health NHS Trust July 2014 Challenges that the NHS faces are well documented What are the challenges?
Guidelines for the Management of Chronic Non-Malignant Pain (CNMP) in Primary Care (not including neuropathic pain (NeP).
 in Primary Care (not including neuropathic pain (NeP).") Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex CCG Guidelines for the
Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex CCG Guidelines for the
Polypharmacy and the Older Adult. Leslie Baker, PharmD, BCGP Umanga Sharma, MD
 Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
Appropriate prescribing and deprescribing for older people getting it right. Alan Davis Northland District Health Board
 Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Optimising Safe & Appropriate Medicines Use and Deprescribing. Katie Smith, Director, East Anglia Medicines Information Service February 2014
 Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
Patient Profile. Patient s details Initials: IF Age: 40 Gender: Male. Weight: 139.7kg Height: 510 metres BMI: >47
 Patient Profile Patient background and medication list Reason for selecting profile Interesting depression case whereby there were several opportunities for intervention as a pharmacist to ensure drug-related
Patient Profile Patient background and medication list Reason for selecting profile Interesting depression case whereby there were several opportunities for intervention as a pharmacist to ensure drug-related
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
beclometasone 100 MDI 2 puffs twice a day (recently changed to non CFC (Clenil Modulite))
)") Case 1 Mr Thomson, a 32 year old asthmatic who is well known to you comes into your pharmacy. He is known to have a best peak flow of 640 L/min. He tells you that over the last few weeks he has been wakening
Case 1 Mr Thomson, a 32 year old asthmatic who is well known to you comes into your pharmacy. He is known to have a best peak flow of 640 L/min. He tells you that over the last few weeks he has been wakening
If a bad thing is happening to a patient, a drug did it until proven otherwise
 Dr Vicki s First Rule of Geriatrics Deprescribing in the Elderly Victoria Braund MD, FACP, CMD Director, Division of Geriatrics NorthShore University HealthSystem Medical Director, Brandel Health & Rehab
Dr Vicki s First Rule of Geriatrics Deprescribing in the Elderly Victoria Braund MD, FACP, CMD Director, Division of Geriatrics NorthShore University HealthSystem Medical Director, Brandel Health & Rehab
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy
 START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
Pharmaceutical Care for Geriatrics
 Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Medicines Optimisation Annual Report Dr Emma Harris and Neil Hardy on behalf of the Medicines Management Team June 2016
 Medicines Optimisation Annual Report 2015-2016 Dr Emma Harris and Neil Hardy on behalf of the Medicines Management Team June 2016 1 Clinical Objectives Improve the effective use of medicines Maximise health
Medicines Optimisation Annual Report 2015-2016 Dr Emma Harris and Neil Hardy on behalf of the Medicines Management Team June 2016 1 Clinical Objectives Improve the effective use of medicines Maximise health
MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES. MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) KEY ISSUES
 KEY ISSUES") MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) Medicines Management Services aim to ensure that (i) Service users receive their medicines
MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) Medicines Management Services aim to ensure that (i) Service users receive their medicines
Polypharmacy. A CPPE distance learning programme
 A CPPE distance learning programme DLP 177 January 2016 Contents About CPPE distance learning programmes About this learning programme Glossary of key terms v vii ix Contents Section 1 The problem with
A CPPE distance learning programme DLP 177 January 2016 Contents About CPPE distance learning programmes About this learning programme Glossary of key terms v vii ix Contents Section 1 The problem with
Polypharmacy, whose problem, whose responsibility? Catherine Gerard & Les Toop
 Polypharmacy, whose problem, whose responsibility? Catherine Gerard & Les Toop Health Quality and Safety Commission University of Otago, Christchurch Pegasus Health Canterbury Clinical Network RNZCGP QS
Polypharmacy, whose problem, whose responsibility? Catherine Gerard & Les Toop Health Quality and Safety Commission University of Otago, Christchurch Pegasus Health Canterbury Clinical Network RNZCGP QS
Screening tools for elderly patients in primary care
 Screening tools for elderly patients in primary care Cristín Ryan 1 Prof. Julia Kennedy 1 Dr. Denis O Mahony 2 Dr. Stephen Byrne 1 Co-Investigator: Dr. Paul Gallagher 2 1 Pharmaceutical Care Research Group,
Screening tools for elderly patients in primary care Cristín Ryan 1 Prof. Julia Kennedy 1 Dr. Denis O Mahony 2 Dr. Stephen Byrne 1 Co-Investigator: Dr. Paul Gallagher 2 1 Pharmaceutical Care Research Group,
Medicines Optimisation the opportunities and challenges. Christina Short Medicines Optimisation Project Manager
 Medicines Optimisation the opportunities and challenges Christina Short Medicines Optimisation Project Manager The remit:- Clinical Pharmacy input into the Locality Model Proposal: To contract a senior
Medicines Optimisation the opportunities and challenges Christina Short Medicines Optimisation Project Manager The remit:- Clinical Pharmacy input into the Locality Model Proposal: To contract a senior
Prescribing Dilemmas. Sue Mulvenna Head of Pharmacy and CD Accountable Officer South Region SW 19 th May
 Prescribing Dilemmas Sue Mulvenna Head of Pharmacy and CD Accountable Officer South Region SW 19 th May 2016 The four principles of medicines optimisation Aim to understand the patient s experience Evidence
Prescribing Dilemmas Sue Mulvenna Head of Pharmacy and CD Accountable Officer South Region SW 19 th May 2016 The four principles of medicines optimisation Aim to understand the patient s experience Evidence
Berkshire West Area Prescribing Committee Guidance
 Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Reshaping Care Pathways for Older People. Anne Hendry National Clinical Lead for Quality
 Reshaping Care Pathways for Older People Anne Hendry National Clinical Lead for Quality Reshaping Care for Older People 10 Year Programme to 2021 300 million Change Fund to 2015 32 Partnerships between
Reshaping Care Pathways for Older People Anne Hendry National Clinical Lead for Quality Reshaping Care for Older People 10 Year Programme to 2021 300 million Change Fund to 2015 32 Partnerships between
1/21/2016 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE OBJECTIVES AGING GOALS BEERS CRITERIA
 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
Home MURs for vulnerable older people
 8 This module is also online at pharmacymagazine.co.uk CPD MODULE module 258 Home MURs for vulnerable older people Contributing author: Lelly Oboh, consultant pharmacist, care of older people WORKING IN
8 This module is also online at pharmacymagazine.co.uk CPD MODULE module 258 Home MURs for vulnerable older people Contributing author: Lelly Oboh, consultant pharmacist, care of older people WORKING IN
Palliative care in long-term conditions Scottish Palliative Care Pharmacists Association
 Palliative care in long-term conditions 2011 2012 Scottish Palliative Care Pharmacists Association Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment
Palliative care in long-term conditions 2011 2012 Scottish Palliative Care Pharmacists Association Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE
 POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
A Process for Performing Medication Assessments
 A Process for Performing Medication Assessments Derek Jorgenson, BSP, PharmD, FCSHP College of Pharmacy and Nutrition University of Saskatchewan Objectives 1. Learn an overview of a medication assessment
A Process for Performing Medication Assessments Derek Jorgenson, BSP, PharmD, FCSHP College of Pharmacy and Nutrition University of Saskatchewan Objectives 1. Learn an overview of a medication assessment
ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS
 ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS Philip J. Schneider, MS, FASHP The University of Arizona College of Pharmacy Learning Objectives: Describe the medication-use system and all interdependent
ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS Philip J. Schneider, MS, FASHP The University of Arizona College of Pharmacy Learning Objectives: Describe the medication-use system and all interdependent
Disclosures. Use caution in the elderly: review of safe and effective medication use in older patients. Institute of Medicine. Learning Objectives
 Use caution in the elderly: review of safe and effective medication use in older patients Disclosures I have no disclosures or conflicts of interest related to this presentation John T. Holmes, PharmD,
Use caution in the elderly: review of safe and effective medication use in older patients Disclosures I have no disclosures or conflicts of interest related to this presentation John T. Holmes, PharmD,
Deprescribing: A Practical Guide
 Deprescribing: A Practical Guide The information in this booklet should be used as a pragmatic decision aid, in conjunction with other relevant patient specific data. Useful resource links http://www.derbyshiremedicinesmanagement.nhs.uk/assets/clinical_guidelines/clinical_guidelines_fr
Deprescribing: A Practical Guide The information in this booklet should be used as a pragmatic decision aid, in conjunction with other relevant patient specific data. Useful resource links http://www.derbyshiremedicinesmanagement.nhs.uk/assets/clinical_guidelines/clinical_guidelines_fr
Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma. Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree
 and egfr: Decision and Dilemma. Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree") Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree Topics CKD background egfr background Patient with egfr Referral Guidelines
Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree Topics CKD background egfr background Patient with egfr Referral Guidelines
Pharmacology in the Elderly
 Pharmacology in the Elderly James Hardy Geriatrician, Royal North Shore Hospital A recent consultation Aspirin Clopidogrel Warfarin Coloxyl with senna Clearlax Methotrexate Paracetamol Pantoprazole Cholecalciferol
Pharmacology in the Elderly James Hardy Geriatrician, Royal North Shore Hospital A recent consultation Aspirin Clopidogrel Warfarin Coloxyl with senna Clearlax Methotrexate Paracetamol Pantoprazole Cholecalciferol
MEDICINE OPTIMISATION IN BERKSHIRE EAST CCGS
 MEDICINE OPTIMISATION IN BERKSHIRE EAST CCGS Melody Chapman, Lead CCG Prescribing Support Pharmacist 23 rd July 2015 MEDICINES OPTIMISATION TEAM Team of pharmacists who work to get the best out of medicines
MEDICINE OPTIMISATION IN BERKSHIRE EAST CCGS Melody Chapman, Lead CCG Prescribing Support Pharmacist 23 rd July 2015 MEDICINES OPTIMISATION TEAM Team of pharmacists who work to get the best out of medicines
Polypharmacy in the Elderly
 Polypharmacy in the Elderly Or How Scotland invented the Modern World Sir William Ferguson Anderson 1914-2001 Became the first Professor of Geriatrics in the world when he was appointed to the David Cargill
Polypharmacy in the Elderly Or How Scotland invented the Modern World Sir William Ferguson Anderson 1914-2001 Became the first Professor of Geriatrics in the world when he was appointed to the David Cargill
Southern Derbyshire Shared Care Pathology Guidelines. AKI guidelines for primary care
 Southern Derbyshire Shared Care Pathology Guidelines AKI guidelines for primary care Contents: Flow Diagram: Recommended response time to AKI warning stage test results for adults in primary care 2 Table
Southern Derbyshire Shared Care Pathology Guidelines AKI guidelines for primary care Contents: Flow Diagram: Recommended response time to AKI warning stage test results for adults in primary care 2 Table
Found in practice. Joint Formulary. Joint Formulary. Embedded into practice. Embedded into practice. As above. As above.
 IPSWICH HOSPITAL ADULT THERAPEUTIC SUBSTITUTION REGISTER FOR PHARMACISTS What s New? New Substitutions Added exclusion criteria of Recommended by psychiatry to escitalopram switch Enoxaparin 40mg to 20mg
IPSWICH HOSPITAL ADULT THERAPEUTIC SUBSTITUTION REGISTER FOR PHARMACISTS What s New? New Substitutions Added exclusion criteria of Recommended by psychiatry to escitalopram switch Enoxaparin 40mg to 20mg
Managing medicines in older people. Jane Noble and Caroline Ralph
 Managing medicines in older people Jane Noble and Caroline Ralph Where? Community Hospital Care Home What? Prescribing Dispensing Administering Case 1 84 year old lady Admitted with reduced mobility Recurrent
Managing medicines in older people Jane Noble and Caroline Ralph Where? Community Hospital Care Home What? Prescribing Dispensing Administering Case 1 84 year old lady Admitted with reduced mobility Recurrent
Rational prescribing in the older adult. Assoc Prof Craig Whitehead
 Rational prescribing in the older adult Assoc Prof Craig Whitehead Introduction Physioloical ageing and frailty Medication risks in older adults Drug Burden Anticholinergic and sedative drug burden Cascade
Rational prescribing in the older adult Assoc Prof Craig Whitehead Introduction Physioloical ageing and frailty Medication risks in older adults Drug Burden Anticholinergic and sedative drug burden Cascade
How to prescribe The elderly. Andi Shirtcliffe Pharmacist
 How to prescribe The elderly Andi Shirtcliffe Pharmacist Psycho geriatric long stay hospital Rest home Generalist in a specialist setting Workshop outline Step through how I perform a medicine review Cases
How to prescribe The elderly Andi Shirtcliffe Pharmacist Psycho geriatric long stay hospital Rest home Generalist in a specialist setting Workshop outline Step through how I perform a medicine review Cases
Iatrogenesis in the frail elderly
 Iatrogenesis in the frail elderly Professor Michael Dooley Director of Pharmacy Alfred Health Professor of Clinical Pharmacy Centre for Medicine Use and Safety Monash University Iatrogenesis in the frail
Iatrogenesis in the frail elderly Professor Michael Dooley Director of Pharmacy Alfred Health Professor of Clinical Pharmacy Centre for Medicine Use and Safety Monash University Iatrogenesis in the frail
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY
 TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
Guidance for cost-sensitive HIV therapy prescribing in NHS Scotland 2017
 Guidance for cost-sensitive HIV therapy prescribing in NHS Scotland 2017 Scottish Health Protection Network HIV Clinical Leads FINAL Approved for circulation 17 May 2017 Version No. 6.2 (04/05/17) Date
Guidance for cost-sensitive HIV therapy prescribing in NHS Scotland 2017 Scottish Health Protection Network HIV Clinical Leads FINAL Approved for circulation 17 May 2017 Version No. 6.2 (04/05/17) Date
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Medication History. Case 1. Case 1. Case 2. Case 1. Four components of prescribing. Charles Mitchell
 Medication History Charles Mitchell Director CSEP, University of Queensland Four components of prescribing Information gathering Clinical decision making Monitor and review Communicate decision - prescribe
Medication History Charles Mitchell Director CSEP, University of Queensland Four components of prescribing Information gathering Clinical decision making Monitor and review Communicate decision - prescribe
HA CONVENTION Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward
 Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward HA CONVENTION 2017 Candis Chang Pharmacist Department of Pharmacy Ruttonjee and Tang Shiu Kin Hospitals Background
Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward HA CONVENTION 2017 Candis Chang Pharmacist Department of Pharmacy Ruttonjee and Tang Shiu Kin Hospitals Background
Medicines Management Team Update
 Medicines Management Team Update Medicines Optimisation in 2017 Deprescribing/reducing variation Care homes Dietetics Improving Clinical outcomes e.g. reducing stroke, Antibiotics Joint Formulary Responses
Medicines Management Team Update Medicines Optimisation in 2017 Deprescribing/reducing variation Care homes Dietetics Improving Clinical outcomes e.g. reducing stroke, Antibiotics Joint Formulary Responses
Wednesday September 20 th CMT Regional Study Day. Dr Colin Mason, Consultant DME, Addenbrooke s Hospital
 Wednesday September 20 th CMT Regional Study Day Dr Colin Mason, Consultant DME, Addenbrooke s Hospital Develop a structured approach to a patient presenting with a fall Risk stratify who can go home and
Wednesday September 20 th CMT Regional Study Day Dr Colin Mason, Consultant DME, Addenbrooke s Hospital Develop a structured approach to a patient presenting with a fall Risk stratify who can go home and
Amal AL-Anazi, BSc.(Pharm) Medication Safety Officer In Eastern Region
 Medication Safety Officer In Eastern Region") Risks Of Polypharmacy Amal AL-Anazi, BSc.(Pharm) Medication Safety Officer In Eastern Region What is Polypharmacy? Polypharmacy means many drugs. In practice, polypharmacy refers to the use of more medication
Risks Of Polypharmacy Amal AL-Anazi, BSc.(Pharm) Medication Safety Officer In Eastern Region What is Polypharmacy? Polypharmacy means many drugs. In practice, polypharmacy refers to the use of more medication
Use caution in the elderly: review of safe and effective medication use in older patients
 Use caution in the elderly: review of safe and effective medication use in older patients John T. Holmes, PharmD, BCPS Assistant Professor of Family Medicine and Pharmacy Practice In support of improving
Use caution in the elderly: review of safe and effective medication use in older patients John T. Holmes, PharmD, BCPS Assistant Professor of Family Medicine and Pharmacy Practice In support of improving
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
NHS DUMFRIES & GALLOWAY Guidance for Prescribing for Frail Adults
 NHS DUMFRIES & GALLOWAY Guidance for Prescribing for Frail Adults Guidance for Prescribing in Frail Adults Prescribing for frail adults should prioritise their comfort and quality of life. Unnecessary
NHS DUMFRIES & GALLOWAY Guidance for Prescribing for Frail Adults Guidance for Prescribing in Frail Adults Prescribing for frail adults should prioritise their comfort and quality of life. Unnecessary
Medication Use in Older Adults
 Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
National Therapeutic Indicators and Additional Prescribing Measures 2017/18 - Early Release Document
 National Therapeutic Indicators and Additional Prescribing Measures 2017/18 - Early Release Document 1 National Therapeutic Indicators 2017-18 National Therapeutic Indicators (NTIs) and Additional Prescribing
National Therapeutic Indicators and Additional Prescribing Measures 2017/18 - Early Release Document 1 National Therapeutic Indicators 2017-18 National Therapeutic Indicators (NTIs) and Additional Prescribing
Title of Project: NHS Dumfries & Galloway Respiratory Bundle Asthma: Bronchodilator Overuse Review April 2015
 Title of Project: NHS Dumfries & Galloway Respiratory Bundle Asthma: Bronchodilator Overuse Review April 2015 1 Reason for the review Respiratory prescribing is long term and can be costly. Appropriate
Title of Project: NHS Dumfries & Galloway Respiratory Bundle Asthma: Bronchodilator Overuse Review April 2015 1 Reason for the review Respiratory prescribing is long term and can be costly. Appropriate
Chronic Kidney Disease in Primary Care
 Clinical Stream Chronic Kidney Disease in Primary Care Dr Gerald Waters Dr Gerald Waters Renal Physician Chronic Kidney Disease Chronic Kidney Disease Normal functions of Kidneys Management of CKD Drugs
Clinical Stream Chronic Kidney Disease in Primary Care Dr Gerald Waters Dr Gerald Waters Renal Physician Chronic Kidney Disease Chronic Kidney Disease Normal functions of Kidneys Management of CKD Drugs
NES Asthma Hospital Medication Care Plan 7
 NES Asthma Hospital Medication Care Plan 7 PATIENT DETAILS Name Liz Duncan Address Consultant Gender Female Weight 60kg Height 1.6m General Practitioner Dr Jones Community Pharmacist Date of Birth (Age)
NES Asthma Hospital Medication Care Plan 7 PATIENT DETAILS Name Liz Duncan Address Consultant Gender Female Weight 60kg Height 1.6m General Practitioner Dr Jones Community Pharmacist Date of Birth (Age)
Deprescribing Unnecessary Medications: A Four-Part Process
 Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks
 Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Swindon PCT/CCG - Cost based ASTRO-PU variance to the England average prescribing spend by month
 Appendix x Swindon CCG Primary Care Prescribing Costs and Patient Outcomes Variance to the England average 105.00% Swindon PCT/CCG - Cost based ASTRO-PU variance to the England average prescribing spend
Appendix x Swindon CCG Primary Care Prescribing Costs and Patient Outcomes Variance to the England average 105.00% Swindon PCT/CCG - Cost based ASTRO-PU variance to the England average prescribing spend
Pharmaceutical Care of People with Atrial Fibrillation. Course activities
 Pharmaceutical Care of People with Atrial Fibrillation Course activities Pharmaceutical Care of People with Atrial Fibrillation Course activities page 3 Case Study 1 5 Case Study 2 7 Case Study 3 9 Case
Pharmaceutical Care of People with Atrial Fibrillation Course activities Pharmaceutical Care of People with Atrial Fibrillation Course activities page 3 Case Study 1 5 Case Study 2 7 Case Study 3 9 Case
Gateshead Pain Guidelines for Chronic Conditions
 Gateshead Pain Guidelines for Chronic Conditions Effective Date: 13.2.2013 Review Date: 13.2.2015 Gateshead Pain Guidelines: Contents PAIN GUIDELINES Chronic Non-Malignant Pain 5 Musculoskeletal Pain 6
Gateshead Pain Guidelines for Chronic Conditions Effective Date: 13.2.2013 Review Date: 13.2.2015 Gateshead Pain Guidelines: Contents PAIN GUIDELINES Chronic Non-Malignant Pain 5 Musculoskeletal Pain 6
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care
 SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
Medicines save lives
 Optimizing Aging Collaborative Disclosures Too much of a good thing: No financial interests to disclose John Newman, MD, PhD Assistant Professor Division of Geriatrics, UCSF Kirby Lee, PharmD, MAS Associate
Optimizing Aging Collaborative Disclosures Too much of a good thing: No financial interests to disclose John Newman, MD, PhD Assistant Professor Division of Geriatrics, UCSF Kirby Lee, PharmD, MAS Associate
Summary of 2012/13 QOF Changes
 Summary of QOF Changes Retirements 2011/12 CHD13 AF4 QP1 QP2 QP3 QP4 QP5 2011/12 Indicator Wording Threshold For patients with newly diagnosed angina (diagnosed after 1 April 2011), the percentage who
Summary of QOF Changes Retirements 2011/12 CHD13 AF4 QP1 QP2 QP3 QP4 QP5 2011/12 Indicator Wording Threshold For patients with newly diagnosed angina (diagnosed after 1 April 2011), the percentage who
Rivaroxaban film coated tablets are available in 2 strengths for this indication: 15mg and 20mg.
 Primary Care Prescriber Information RIVAROXABAN (XARELTO ) Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism INDICATION Rivaroxaban is a non-vitamin K antagonist
Primary Care Prescriber Information RIVAROXABAN (XARELTO ) Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism INDICATION Rivaroxaban is a non-vitamin K antagonist
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018
 From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
De-Prescribing in relation to Polypharmacy. Liz Corteville Locality Lead Pharmacist West Hampshire CCG July 2018
 De-Prescribing in relation to Polypharmacy Liz Corteville Locality Lead Pharmacist West Hampshire CCG July 2018 WHO Global Patient Safety Challenges 1 st handwashing 2 nd safe surgery checklist 3 rd medication
De-Prescribing in relation to Polypharmacy Liz Corteville Locality Lead Pharmacist West Hampshire CCG July 2018 WHO Global Patient Safety Challenges 1 st handwashing 2 nd safe surgery checklist 3 rd medication
Polypharmacy Guidance
 Polypharmacy Guidance October 2012 Developed by The Model of Care Polypharmacy Working Group Quality and Efficiency Support Team Scottish Government Health and Social Care Directorates - 2 - Acknowledgements
Polypharmacy Guidance October 2012 Developed by The Model of Care Polypharmacy Working Group Quality and Efficiency Support Team Scottish Government Health and Social Care Directorates - 2 - Acknowledgements
Monitoring polypharmacy and reducing problematic prescribing
 CLINICAL AUDIT Monitoring polypharmacy and reducing problematic prescribing Valid to November 2020 bpac nz better medicin e Audit Focus Patients taking ten or more medicines are at an increased risk of
CLINICAL AUDIT Monitoring polypharmacy and reducing problematic prescribing Valid to November 2020 bpac nz better medicin e Audit Focus Patients taking ten or more medicines are at an increased risk of
Dear Colleagues, NATIONAL STANDARD FOR MONITORING THE PHYSICAL HEALTH OF PEOPLE BEING TREATED WITH LITHIUM
 Directorate of Chief Medical Officer T: 0131-244 6930 E: john.mitchell4@gov.scot Dear Colleagues, NATIONAL STANDARD FOR MONITORING THE PHYSICAL HEALTH OF PEOPLE BEING TREATED WITH LITHIUM Lithium is a
Directorate of Chief Medical Officer T: 0131-244 6930 E: john.mitchell4@gov.scot Dear Colleagues, NATIONAL STANDARD FOR MONITORING THE PHYSICAL HEALTH OF PEOPLE BEING TREATED WITH LITHIUM Lithium is a
Frailty and Type 2 Diabetes Guidelines for clinicians
 H.G. WELLS PROJECT Frailty and Type 2 Diabetes Guidelines for clinicians Victoria Ruszala victoria.ruszala@nhs.net H.G. Wells Project team Dugal T, Partington E. Kernow CCG Diabetes and Frailty Guideline
H.G. WELLS PROJECT Frailty and Type 2 Diabetes Guidelines for clinicians Victoria Ruszala victoria.ruszala@nhs.net H.G. Wells Project team Dugal T, Partington E. Kernow CCG Diabetes and Frailty Guideline
Rebecca Rottman-Sagebiel, Pharm.D., BCPS Sharon Jung Tschirhart, Pharm.D., BCPS Geriatric Clinical Pharmacy Specialists STVHCS, Audie L.
 Rebecca Rottman-Sagebiel, Pharm.D., BCPS Sharon Jung Tschirhart, Pharm.D., BCPS Geriatric Clinical Pharmacy Specialists STVHCS, Audie L. Murphy Division Clinical Assistant Professors, University of Texas/UTHSCSA
Rebecca Rottman-Sagebiel, Pharm.D., BCPS Sharon Jung Tschirhart, Pharm.D., BCPS Geriatric Clinical Pharmacy Specialists STVHCS, Audie L. Murphy Division Clinical Assistant Professors, University of Texas/UTHSCSA