Pediatric and Adult. Disclosure. Asthma. Learning Objectives. EPR-3: What s Changed? Asthma: Pediatric and Adult
|
|
|
- Abigayle O’Brien’
- 6 years ago
- Views:
Transcription

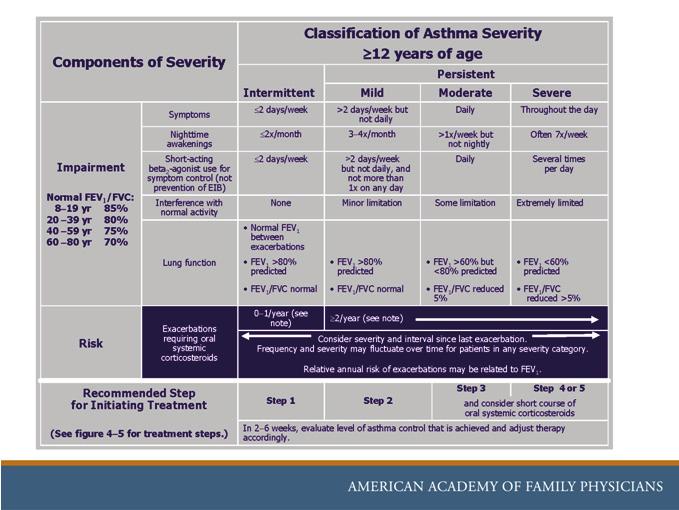
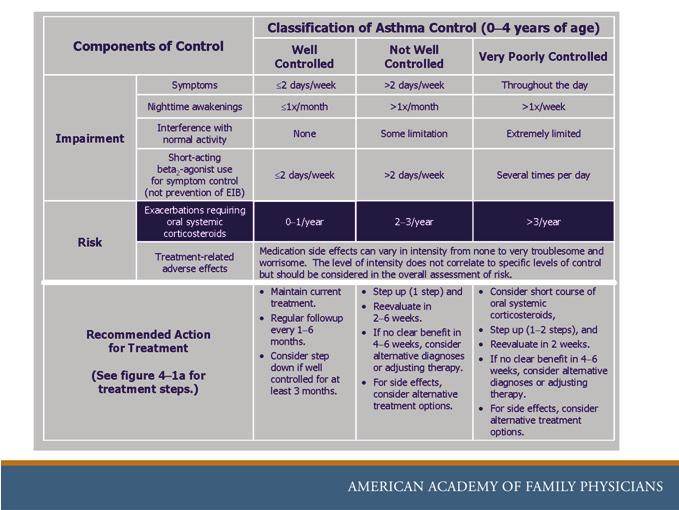
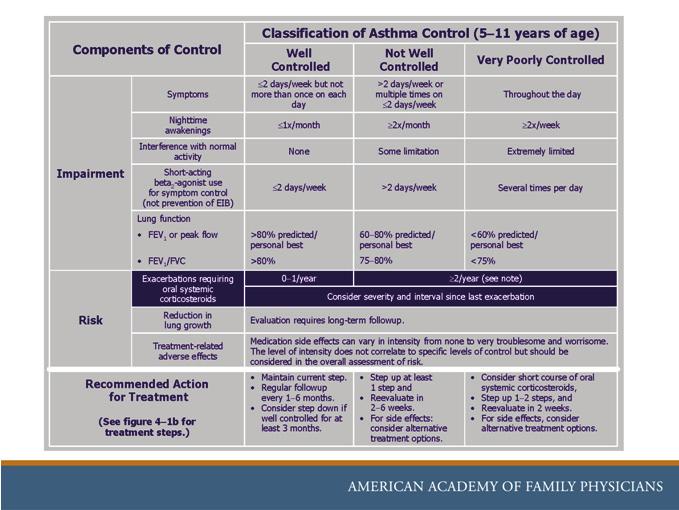
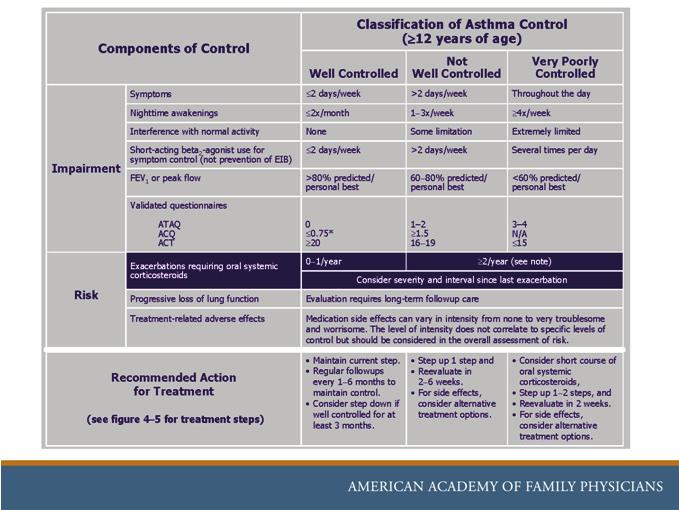
1 Asthma: Pediatric and Adult Americo D. Fraboni, MD, FAAFP Assistant Clinical Professor Department of Family Practice & Community Health University of Minnesota Medical School Minneapolis, Minnesota Disclosure The AAFP has selected all faculty appearing in this program. It is the policy of the AAFP that all CME planning committees, faculty, authors, editors, and staff disclose relationships with commercial entities upon nomination or invitation of participation. Disclosure documents are reviewed for potential conflicts of interest and, if identified, they are resolved prior to confirmation of participation. Only those participants who had no conflict of interest or who agreed to an identified resolution process prior to their participation were involved in this CME activity. Dr Americo Fraboni returned disclosures indicating that he has no affiliation or financial interest in any organization(s). Learning Objectives 1. Identify a treatment rationale for the patient who presents with status asthmaticus. 2. Describe the medical treatment of the allergic patient. 3. Recognize a pharmacologic therapy in the treatment of asthma. 4. State the current NIH guidelines for the treatment of chronic asthma. Asthma National Heart Lung and Blood Institute Practice guidelines (NHLBI) National Asthma Education and Prevention Program (NAEPP) Third Expert Panel Report (EPR-3) Initial report in 1991 Second report in 1997 Updated in 2002 Third report in 2007 Most comprehensive EB guidance for Dx and Rx to date EPR-3: What s Changed? The 2007 Guidelines: Recommend assessing asthma severity before starting Rx and assessing asthma control to guide adjustments in Rx (SOR B,C) Address both severity and control in terms of impairment and risk (SOR A) Feature 3 age breakdowns (0-4 yrs, 5-11 yrs, 12 yrs) and a 6-step approach to management (SOR C) Make it easier to individualize and adjust Rx (SOR B) 1. & 2. A 24-year-old female with no chronic illnesses arrives in your office relating a history of several episodes of shortness of breath associated with a hacky cough and chest tightness. She recently developed nasal congestion, sinus pressure, and muscle aches and thinks she has a cold. She has never before been short of breath, does not smoke, and has no family history of respiratory disease. She has taken over-the-counter decongestants with little relief of the coughing. She takes no prescription drugs. VS: BP 108/65, HR 80, RR 14, T 37.2 degrees C, O2 sats 95% on RA. PE: is remarkable for clear rhinorrhea, mild scattered expiratory wheezes, a normal cardiac exam, and non-tender maxillary and frontal sinuses.
2 1. What is the most likely trigger for her current symptoms? 1. What is the most likely trigger for her current symptoms? A. Viral upper respiratory tract infection B. Sinusitis C. Acute bacterial bronchitis D. Gastroesophageal reflux 92% 3% 3% 3% A. Viral upper respiratory tract infection B. Sinusitis C. Acute bacterial bronchitis D. Gastroesophageal reflux 2. What initial treatment would you prescribe for her at this time? 2. What initial treatment would you prescribe for her at this time? A. Codeine B. A steroid nasal spray C. Corticosteroid inhaler D. Albuterol inhaler 2% 16% 5% 79% A. Codeine B. A steroid nasal spray C. Corticosteroid inhaler D. Albuterol inhaler What Is Asthma? Clinical symptoms Intermittent Sxs Cough Wheeze SOB/Breathlessness Chest pain Rescue med use Diurnal variation Varying triggers Exacerbations Perennial/seasonal Episodic/continual Diurnal What Is Asthma? Biological indicators, pathophysiology Chronic airway inflammation Bronchial hyper-responsiveness (BHR) Airflow limitation Airway smooth muscle broncho-constriction Airway edema Mucus plug formation Bronchiolar obstruction Airway remodeling
3 Asthma Differential Dx Viral pneumonitis Pneumothorax Pulmonary embolism Vocal cord dysfunction syndrome COPD Pulmonary edema Endobronchial obstruction (tumor or FB) Acute hypersensitivity pneumonitis Epiglottitis COPD vs Asthma Symptom COPD Asthma Chronic cough common variable & sputum Breathless on exertion persistent, slowly variable, or poor lung fxn progressive intermittent, largely reversible Onset prior to 40 yrs less common common Tobacco use almost always sometimes Airway hyper- common always responsiveness Progression of Sxs slowly, little episodic and variability variable Identifiable triggers uncommon common Bronchodilator response modest often marked 3. Which of the following tests would you use to better categorize this patient s condition? 3. Which of the following tests would you use to better categorize this patient s condition? A. Spirometry B. CXR C. ABG D. Methacholine challenge 84% 1% 1% 15% A. Spirometry B. CXR C. ABG D. Methacholine challenge Establishing a Diagnosis Clinical Testing Based on a patient s Medical history Physical exam Pulmonary function tests (PFTs) Laboratory tests Spirometry is recommended in order to make the Dx Level of severity based on Impairment Risk Spirometry Recommended for every pt 5 yrs of age If pt <5 yrs of age, a therapeutic trial of medication is recommended Studies specific to individual patients Allergy testing CXR Bronchial provocation testing Sinus x-rays or CT scan GERD evaluation CBC with eosinophils, total IgE, sputum exam
4 4. Which of the following PFT results is most likely to be below the normal predicted range in this patient with asthma? 4. Which of the following PFT results is most likely to be below the normal predicted range in this patient with asthma? A. FVC (Forced Vital Capacity) B. FEV1 (Forced Expiratory Volume in 1 second) C. TLC (Total Lung Capacity) D. FRC (Functional Residual Capacity) 11% 86% 2% 3% A. FVC (Forced Vital Capacity) B. FEV1 (Forced Expiratory Volume in 1 second) C. TLC (Total Lung Capacity) D. FRC (Functional Residual Capacity) 5. At least what percentage of airway reversibility do you need in order to confirm the diagnosis of asthma? 5. At least what percentage of airway reversibility do you need in order to confirm the diagnosis of asthma? A. 10% B. 25% C. 12% D. 18% 15% 38% 36% 12% A. 10% B. 25% C. 12% D. 18% Spirometry Spirometry Measurements pre and post a short-acting beta2-agonist (SABA) FEV1 FVC FEV1/FVC Airflow obstruction Reduced FEV1 and FEV1/FVC values relative to predicted values (FEV1 <80% predicted) Significant reversibility after inhaling a SABA Increase by 12% and 200 ml in FEV1 Mild asthmatics Repeat every 1-2 yrs Confirms dx and objectifies serial change and level of control Moderate and severe asthmatics More frequently depending on their response to therapy
5 Pulmonary Function Tests Asthmatic patient FEV1 is decreased FVC may fall, but FEV1 is much more common to be below predicted TLC is normal to elevated FRC is usually elevated Asthma Triggers URI Environmental Occupational or Recreational Viral Allergens Allergens ASA Cardiac Asthma Irritants -Perfume -Tobacco smoke -Wood burning stoves Temperature Humidity Exercise Drug CHF GERD Trigger for bronchospasm Irritants NSAIDS Consider in both peds and adult patients Beta Blockers Sulfites (food) 6. In considering the atopic patient and asthma. Which of the following is true? 6. In considering the atopic patient and asthma. Which of the following is true? A. Atopy is one of the strongest predisposing factors for the patient with asthma B. A peripheral eosinophil count is sufficiently sensitive to be used alone in the diagnosis of asthma C. The CXR is usually abnormal in asthma D. Skin allergy tests are rarely positive in the atopic patient 92% 3% 0% 6% A. Atopy is one of the strongest predisposing factors for the patient with asthma B. A peripheral eosinophil count is sufficiently sensitive to be used alone in the diagnosis of asthma C. The CXR is usually abnormal in asthma D. Skin allergy tests are rarely positive in the atopic patient The Atopic Patient The Atopic Patient Atopy is one of the strongest predisposing factors for the patient with asthma Genetic predisposition for the development of an IgE mediated response Investigation into the role of allergy Complete history in every patient is indicated Given the high prevalence of positive skin tests among individuals with asthma And the benefits of limiting exposure to known allergens History may help to distinguish seasonal allergies but may be inadequate for perennial allergies Eosinophil count and IgE may be elevated in asthma Neither test has sufficient specificity or sensitivity to be used alone in a diagnosis The chest x-ray and electrocardiogram are usually normal in asthma May be useful to exclude other pulmonary or cardiac conditions Sputum examination may be helpful if sputum eosinophilia or infection are suspected

6 Allergy Treatment Can Improve Asthma Sxs Key to Control Avoidance of allergens or environmental control Intranasal corticosteroids Reduce both allergic rhinitis and asthma sxs in pts with mild asthma Antihistamines alone or combined with a decongestant May reduce asthma and rhinitis sxs Leukotriene modulators Treat sxs of asthma and allergic rhinitis at the same time Immunotherapy May reduce development of asthma in pts with seasonal rhinoconjunctivitis Control of House Mites Essential actions Encase the mattress in an allergen impermeable cover Encase the pillow in an allergen impermeable cover or wash it weekly Wash the sheets and blankets on the patient's bed weekly in hot water A temperature of 130ºF is necessary for killing house-dust mites Severity and Control Severity A measure of the intrinsic intensity of the disease process established ideally before initiating treatment Control Monitored over time to guide adjustments to therapy Assess Severity and Control Within the Domains of: Impairment - Based on Asthma symptoms (identified by patient or caregiver recall of the past 2-4 weeks), Quality of life Functional limitations Risk -of Asthma exacerbations Progressive decline in pulmonary function (or reduced lung growth in children) Adverse events Assess Severity and Control Predictors of increased risk for exacerbations or death: Persistent and/or severe airflow obstruction At least 2 visits to the ED or hospitalizations for asthma within the past year And a history of intubation or admission to the ICU, especially within the past 5 years

7 Asthma: Pediatric and Adult


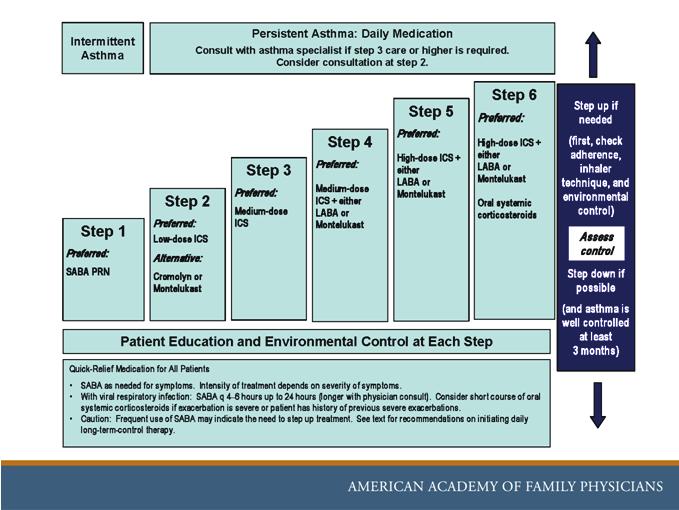
8 7. In classifying the asthmatic patient, an individual with symptoms greater than two times per week, but less than one time per day OR with nocturnal symptoms greater than two times per month would be classified as: A. Mild Intermittent B. Mild Persistent C. Moderate Persistent D. Severe Persistent 7. In classifying the asthmatic patient, an individual with symptoms greater than two times per week, but less than one time per day OR with nocturnal symptoms greater than two times per month would be classified as: 8% A. Mild Intermittent 58% B. Mild Persistent 36% C. Moderate Persistent 0% D. Severe Persistent Asthma Classification Mild Intermittent Mild Persistent Moderate Persistent Severe Persistent Sxs <2x/wk Sxs >2x/wk, but <1x/d exacerbations may affect activity Daily sxs, daily use of inhaled SABA, exacerbations affect activity, exacerbations >2x/wk; may last days Continual sxs, limited physical activity, frequent exacerbations Nocturnal sxs <2x/mo FEV1 or PEF >80% predicted Nocturnal sxs >2x/mo FEV1 or PEF >80% predicted Nocturnal sxs >1x/wk FEV1 or PEF 60%- 80% predicted Frequent nocturnal sxs FEV1 or PEF <60% predicted 6 Steps of Care Step 1-Intermittent Step 2-Mild persistent Step 3-Moderate persistent Step 4-Moderate persistent Step 5-Severe persistent Step 6-Severe persistent PEF variability 20%-30% PEF variability >30% PEF variability >30% Am Fam Physician Jul 1;84(1):40-47 *See the Stepwise approach for managing asthma chart (figure 3) at the end of these slides for more details*
9 Stepwise Preferred Treatment 0-4 Years of Age Most recommendations are based on limited data. Step 1: SABA PRN Step 2: Low dose ICS Step 3: Medium dose ICS Step 4: Medium dose ICS and LABA or montelukast (Singulair) Step 5: High dose ICS and LABA or Singulair Step 6: High dose ICS and oral corticosteroid and LABA or Singulair Stepwise Preferred Treatment 5-11 Years of Age Step 1: SABA PRN Step 2: Low dose ICS Step 3: Low dose ICS and LABA, LTRA or theophylline, OR medium dose ICS Step 4: Medium dose ICS and LABA Step 5: High dose ICS and LABA Step 6: High dose ICS and LABA and oral corticosteroids Stepwise Preferred Treatment 12 Years of Age Step 1: SABA prn Step 2: Low dose ICS Step 3: Low dose ICS and LABA OR medium dose ICS Step 4: Medium dose ICS and LABA Step 5: High dose ICS and LABA; consider omalizumab (Xolair) if allergies Step 6: High dose ICS and LABA and oral corticosteroid; consider Xolair if allergies 8. Which of the following is NOT true? A. Long acting beta agonists like salmeterol can increase mortality if used alone B. ICS use is indicated if PRN use of albuterol exceeds >2 times/wk C. Oral corticosteroids are as effective as IV D. Cromolyn is a first line drug to control acute asthma symptoms 8. Which of the following is NOT true? 4% 7% 3% 89% A. Long acting beta agonists like salmeterol can increase mortality if used alone B. ICS use is indicated if PRN use of albuterol exceeds >2 times/wk C. Oral corticosteroids are as effective as IV D. Cromolyn is a first line drug to control acute asthma symptoms Treatment Albuterol The most appropriate treatment for acute bronchospasm is an inhaled SABA Use a spacer. Codeine or other cough suppressants are basically ineffective. Nasal and inhaled steroids have an onset that is too slow.
10 Treatment Inhaled corticosteroids (ICS) Most potent and effective long-term controller therapy Foundation of therapy for patients of all ages who have persistent asthma (SOR A) ICS improve long-term outcomes in children with mild to moderate persistent asthma (SOR A) Studies are limited comparing them to other alternative treatments The Expert Panel Recommends For patients 5 years of age with mild or moderate persistent asthma, the preferred therapy is inhaled corticosteroids (low dose) (SOR A) Alternative therapies (listed alphabetically due to insufficient data to rank) Cromolyn LTRAs (Leukotriene Receptor Antagonists) Nedocromil (Alocril) (production ceased in 2008) Sustained-release theophylline Strong Evidence From Clinical Trials Following Children for Up to 6 Years Suggests that the use of inhaled corticosteroids at recommended doses Does not have long-term, clinically significant, or irreversible effects on any of the outcomes reviewed, (Vertical growth, Bone mineral density (BMD), Ocular toxicity, Suppression of adrenal/pituitary axis) Inhaled corticosteroids do improve health outcomes (SOR A, B) For children with mild or moderate persistent asthma The potential but small risk of delayed growth is well balanced by their effectiveness Patients With Moderate Persistent Asthma The addition of another long-term control agent to inhaled corticosteroids improves outcomes LABA added to low-medium-dose inhaled corticosteroids (SOR A) Preventing Progression of Asthma? Does Early Intervention of Long-Term Control Therapy (Inhaled Corticosteroids) Prevent Progression of Asthma? Evidence is insufficient to draw conclusions Early intervention with inhaled steroids likely will improve overall asthma management, but its effect on preventing irreversible airway injury remains to be determined (SOR A, B) Treatment - Key Points Long-acting inhaled Beta2-agonists (LABA): Used concomitantly with inhaled corticosteroids are the preferred combination therapy for long-term control and prevention of symptoms in moderate and severe persistent asthma (SOR A, B)
11 Treatment - Key Points Cromolyn and nedocromil Used as alternative (not preferred) medications for the treatment of mild persistent asthma (SOR A, B) Leukotriene modifiers Again as an alternative (not preferred) medication for the treatment of mild persistent asthma (SOR B) Treatment - Key Points Safety is a key consideration Weigh the benefits and risks of therapy Systemic effects of higher doses of ICS Rare but potential risk of life-threatening or fatal exacerbations with daily LABA Rx Oral corticosteroid use regardless of age Reassessment Follow-up Every 2-6 wk intervals for starting Rx or those that require a step up to regain control Once controlled, reassess at least every 1-6 mo Measures of control are the same as those to assess severity plus use of, Validated multidimensional questionnaires like the asthma control test (ACT) A step down is recommended for patients whose asthma is well controlled for 3 months or more. Decrease dose of ICS gradually 25% to 50% q3mo deterioration in asthma control is highly variable 9. In considering the use of an asthma action plan, which of the following are true? A. Data is sufficient to support the benefits of written action plans. B. A PEF of 80% or more defines the Yellow Zone. C. The use of written action plans is recommended. D. It is recommended that Home Peak Expiratory Monitoring be used in patients with mild intermittent asthma. 9. In considering the use of an asthma action plan, which of the following are true? 20% 4% 60% 17% A. Data is sufficient to support the benefits of written action plans. B. A PEF of 80% or more defines the Yellow Zone. C. The use of written action plans is recommended. D. It is recommended that Home Peak Expiratory Monitoring be used in patients with mild intermittent asthma. Asthma Action Plans Data are insufficient to support or refute the benefits of written action plans (SOR B) Expert Panel opinion Use of written action plans is recommended (SOR B, C) Especially for patients with moderate or severe persistent asthma Patients with a history of severe exacerbations Action plans should Address individual sxs, and/or PEF measurements Self-management instructions
12 Asthma Action Plan Green Zone: Usual activity PEF 80% or more of personal best Yellow Zone: Some of usual activity PEF 50%-80% of personal best Red Zone: Cannot do usual activities PEF less than 50% of personal best Home Peak Expiratory Flow (PEF) Monitoring Evidence neither supports nor refutes the benefits of peak flow monitoring Expert Panel opinion (SOR B) PEF monitoring should be considered for Patients with moderate or severe persistent asthma Difficulty recognizing signs of exacerbations History of severe exacerbations It may enhance clinician-patient communication It may increase patient and caregiver awareness of the disease status and control Patient Education Control is enhanced Ensuring access to education about asthma Skills necessary to manage it Self-monitoring Correct use of inhalers Following a plan for managing asthma longterm Promptly handling signs of worsening asthma 10. A patient who comes to the Emergency Department in acute respiratory distress caused by a severe attack of asthma should be treated with all of the following EXCEPT: A. IV fluids B. Humidified, high-flow-rate oxygen C. IV corticosteroids D. IV antibiotics 10. A patient who comes to the Emergency Department in acute respiratory distress caused by a severe attack of asthma should be treated with all of the following EXCEPT: 8% 4% 2% 86% A. IV fluids B. Humidified, high-flow-rate oxygen C. IV corticosteroids D. IV antibiotics Acute Asthma Exacerbation Symptoms Progressive breathlessness Cough Wheezing Chest tightness Severity assessment is critical Using objective measures Focused H&P Measurement of airflow FEV1 PEF

13 Acute Asthma Exacerbation Acute Asthma Exacerbation Characterized by Decreased PEF (<50% predicted normal) FEV1 may be more useful in predicting exacerbations Failure to respond to a beta 2 -agonist Extreme anxiety due to breathlessness Gasping for air, sweaty, or cyanotic Rapid deterioration over a few hours Severe retractions and nasal flaring Hunched forward Am Fam Physician Jul 1;84(1):40-47 Acute Asthma Exacerbation Risk factors for death from asthma History of sudden severe exacerbations Prior intubation for asthma Prior admission for asthma to ICU 3 emergency care visits for asthma in the past year Hospitalization or an emergency care visit for asthma within past month >2 canisters per month of inhaled shortacting beta 2 -agonist Acute Asthma Exacerbation Risk factors for death from asthma (cont) Current use or recent withdrawal from systemic corticosteroids Difficulty perceiving airflow obstruction or its severity Serious psychiatric disease or psychosocial problems Low SES and urban residence Illicit drug use Sensitivity to Alternaria Exacerbation Management SABA by MDI or nebulizer Corticosteroids Oral or IV Strongly consider systemic use Aids symptom resolution Prevents asthma relapse Exacerbation Management Alternatives Epinephrine (1:1000) Ipratropium added to nebulized SABA Improves lung function and decreases hospitalizations in children 1-18 yrs of age with mild moderate or severe exacerbations Levalbuterol Corticosteroids Initiate or increase anti-inflammatory medication ICS Cromolyn Consider leukotriene modifiers
14 Exacerbation Management ED or inpatient management Most children who require hospitalization can be identified by a repeat assessment 1 hr after initial treatment. If a patient meets - Criteria for severe exacerbation, >86% chance require hospitalization Criteria for moderate exacerbation, 84% chance require hospitalization Criteria dropped to the mild level, 18% chance of hospitalization Exacerbation Management Poor response to treatment - Early intervention with Bi-PAP may prevent mechanical intubations Heliox may be a secondary therapy if no response to first-line Rx Ketamine - Consider for use only in severe exacerbations Magnesium sulfate IV for severe exacerbations Decreases hospitalization in children 1-18 yrs of age, not adults Reassess pt shortly after inpatient admission Decision when to D/C from ED or admit must be individualized and depends on response to treatment, pulmonary function, and socioeconomic factors Exacerbation Management Intermittent nebs vs continuous nebs? Data suggests they are equally efficacious FEV1 <50% predicted Statistically significant improvement in FEV1 with continuous nebs in one study, not in another PEF <200 Statistically significant improvement in PEF and decrease in hospitalizations with continuous nebs Antibiotics? Does routinely adding antibiotics to a patient s regimen without signs and symptoms of bacterial infection improve the outcomes of treatment for acute exacerbation of asthma? No! Benefit from antibiotic therapy for asthma exacerbations has not been demonstrated: Whether administered routinely Or when suspicion of bacterial infection is low (SOR B) Exercise-Induced Bronchospasm (EIB) Occurs in 90% of pts with asthma >10% of general population Often indicates poorly controlled asthma Use long-term control therapy if appropriate Pretreatment prior to exercise SABAs, LABAs are effective in up to 80% of pts LTRAs are effective in up to 50% of pts Encourage pts to warm up prior to exercise and consider wearing a mask or scarf in cold weather Goals of Therapy Asthma Control Summary Minimal or no chronic symptoms day or night Minimal or no exacerbations No limitations on activities; no school or work missed Maintain (near) normal pulmonary function Minimal use of short-acting inhaled beta 2 agonist Minimal or no adverse effects from medications
15 Answers 1. A 2. D 3. A 4. B 5. C 6. A 7. B 8. D 9. C 10.D Websites Expert Panel Report 3 (EPR3): Guidelines for the Diagnosis and Management of Asthma (440 pgs) ICSI Heath Care Guidelines: Diagnosis and Management of Asthma (70 pgs) The Journal of Family Practice: Help patients gain better asthma control (10 pgs)
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Improving the Management of Asthma to Improve Patient Adherence and Outcomes
 Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
I have no perceived conflicts of interest or commercial relationships to disclose.
 ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Clinical Implications of Asthma Phenotypes. Michael Schatz, MD, MS Department of Allergy
 Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Exercise-Induced Bronchospasm. Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute
 Exercise-Induced Bronchospasm Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute EIB Episodic bronchoconstriction with exercise May be an exacerbation
Exercise-Induced Bronchospasm Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute EIB Episodic bronchoconstriction with exercise May be an exacerbation
Asthma in the Athlete
 Asthma in the Athlete Jorge E. Gomez, MD Associate Professor Texas Children s Hospital Baylor College of Medicine Assist Team Physician UH Understand how we diagnose asthma Objectives Be familiar with
Asthma in the Athlete Jorge E. Gomez, MD Associate Professor Texas Children s Hospital Baylor College of Medicine Assist Team Physician UH Understand how we diagnose asthma Objectives Be familiar with
Asthma and Vocal Cord Dysfunction
 Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Objectives. Asthma in Primary Care. Definition. Epidemiology. Pathophysiology
 Objectives Asthma in Primary Care Jed Grant, PA-C Program Director, SJVC PA Program Staff PA, AMCH Emergency Department Apply the NAEPP guideline measures of severity and control including current impairment
Objectives Asthma in Primary Care Jed Grant, PA-C Program Director, SJVC PA Program Staff PA, AMCH Emergency Department Apply the NAEPP guideline measures of severity and control including current impairment
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
In 2002, it was reported that 72 of 1000
 REPORTS Aligning Patient Care and Asthma Treatment Guidelines Eric Cannon, PharmD Abstract This article describes how the National Asthma Education and Prevention Program Guidelines for the Diagnosis and
REPORTS Aligning Patient Care and Asthma Treatment Guidelines Eric Cannon, PharmD Abstract This article describes how the National Asthma Education and Prevention Program Guidelines for the Diagnosis and
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Presented by the California Academy of Family Physicians 2013/California Academy of Family Physicians
 Family Medicine and Patient-Centered Asthma Care Presented by the California Academy of Family Physicians Faculty: Hobart Lee, MD Disclosures: Jeffrey Luther, MD, Program Director, Memorial Family Medicine
Family Medicine and Patient-Centered Asthma Care Presented by the California Academy of Family Physicians Faculty: Hobart Lee, MD Disclosures: Jeffrey Luther, MD, Program Director, Memorial Family Medicine
MANAGING ASTHMA. Nancy Davis, RRT, AE-C
 MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
Asthma for Primary Care: Assessment, Control, and Long-Term Management
 Asthma for Primary Care: Assessment, Control, and Long-Term Management Learning Objectives After participating in this educational activity, participants should be better able to: 1. Choose the optimal
Asthma for Primary Care: Assessment, Control, and Long-Term Management Learning Objectives After participating in this educational activity, participants should be better able to: 1. Choose the optimal
Learning Objective. Asthma. Discuss the pathophysiology, clinical presentation, diagnosis, and treatment of Asthma 2/22/2017
 Marianne Curran, PA C 3/1/17 Learning Objective Discuss the pathophysiology, clinical presentation, diagnosis, and treatment of Definition many variations Chronic Disorder with Reversible (Intermittent
Marianne Curran, PA C 3/1/17 Learning Objective Discuss the pathophysiology, clinical presentation, diagnosis, and treatment of Definition many variations Chronic Disorder with Reversible (Intermittent
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS
 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
Adult asthma management: focus on control
 Adult asthma management: focus on control Jennifer W. McCallister, MD Associate Professor Pulmonary, Allergy, Critical Care & Sleep Medicine The Ohio State University Wexner Medical Center Objectives Apply
Adult asthma management: focus on control Jennifer W. McCallister, MD Associate Professor Pulmonary, Allergy, Critical Care & Sleep Medicine The Ohio State University Wexner Medical Center Objectives Apply
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Learning the Asthma Guidelines by Case Studies
 Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Asthma in Pediatric Patients. DanThuy Dao, D.O., FAAP. Disclosures. None
 Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Public Dissemination
 1. THE ASTHMA CONDITION 9 18 3 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
1. THE ASTHMA CONDITION 9 18 3 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
National Asthma Educator Certification Board Detailed Content Outline
 I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma Pathophysiology and Treatment. John R. Holcomb, M.D.
 Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Nancy Davis, RRT, AE-C
 Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Asthma ASTHMA. Current Strategies for Asthma and COPD
 Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
10/6/2014. Tommy s Story: An Overview of Asthma Mangement. Disclosure. Objectives for this talk.
 Tommy s Story: An Overview of Asthma Mangement Clifton C. Lee, MD, FAAP, FHM Associate Professor of Pediatrics Chief, Pediatric Hospital Medicine Children s Hospital of Richmond at VCU Disclosure Obviously,
Tommy s Story: An Overview of Asthma Mangement Clifton C. Lee, MD, FAAP, FHM Associate Professor of Pediatrics Chief, Pediatric Hospital Medicine Children s Hospital of Richmond at VCU Disclosure Obviously,
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION
 Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
+ Asthma and Athletics
 + Asthma and Athletics Shaylon Rettig, MD, MBA Champion Sports Medicine + Financial Disclosure Dr. Shaylon Rettig has no relevant financial relationships with commercial interests to disclose. + Asthma
+ Asthma and Athletics Shaylon Rettig, MD, MBA Champion Sports Medicine + Financial Disclosure Dr. Shaylon Rettig has no relevant financial relationships with commercial interests to disclose. + Asthma
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Symptoms are worse at night and in the morning and includes cough, whz, chest tightness.
 Asthma Review ETIOLOGY Airflow limitation is caused by the following: - bronchoconstriction - mucous pluggin - airway inflammation Sudden death - heavy mucous plugging is common - typically occurs between
Asthma Review ETIOLOGY Airflow limitation is caused by the following: - bronchoconstriction - mucous pluggin - airway inflammation Sudden death - heavy mucous plugging is common - typically occurs between
Pathology of Asthma Epidemiology
 Asthma A Presentation on Asthma Management and Prevention What Is Asthma? A chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Pathology
Asthma A Presentation on Asthma Management and Prevention What Is Asthma? A chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Pathology
ASTHMA IN THE PEDIATRIC POPULATION
 ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD
 Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Impact of Asthma in the U.S. per Year. Asthma Epidemiology and Pathophysiology. Risk Factors for Asthma. Childhood Asthma Costs of Asthma
 American Association for Respiratory Care Asthma Educator Certification Prep Course Asthma Epidemiology and Pathophysiology Robert C. Cohn, MD, FAARC MetroHealth Medical Center Cleveland, OH Impact of
American Association for Respiratory Care Asthma Educator Certification Prep Course Asthma Epidemiology and Pathophysiology Robert C. Cohn, MD, FAARC MetroHealth Medical Center Cleveland, OH Impact of
II: Moderate Worsening airflow limitations Dyspnea on exertion, cough, and sputum production; patient usually seeks medical
 Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network
 Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Joint Session ACOFP and AOASM: Exercise Induced Asthma. Bruce Dubin, DO, JD, FCLM, FACOI
 Joint Session ACOFP and AOASM: Exercise Induced Asthma Bruce Dubin, DO, JD, FCLM, FACOI ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please check where applicable and sign below. Provide additional pages as
Joint Session ACOFP and AOASM: Exercise Induced Asthma Bruce Dubin, DO, JD, FCLM, FACOI ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please check where applicable and sign below. Provide additional pages as
Get Healthy Stay Healthy
 Asthma Management WHAT IS ASTHMA? Asthma causes swelling and inflammation in the breathing passages that lead to your lungs. When asthma flares up, the airways tighten and become narrower. This keeps the
Asthma Management WHAT IS ASTHMA? Asthma causes swelling and inflammation in the breathing passages that lead to your lungs. When asthma flares up, the airways tighten and become narrower. This keeps the
National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline UPDATE. Susan K. Ross RN, AE-C MDH Asthma Program.
 NAEPP 2007 Asthma Guideline UPDATE. Susan K. Ross RN, AE-C MDH Asthma Program.") National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline UPDATE Susan K. Ross RN, AE-C MDH Asthma Program 651-201 201-5629 Susan.Ross@health.state.mn.us 1 National Institutes of Health National
National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline UPDATE Susan K. Ross RN, AE-C MDH Asthma Program 651-201 201-5629 Susan.Ross@health.state.mn.us 1 National Institutes of Health National
Adult Asthma Clinical Practice Guideline Summary
 Adult Asthma Clinical Practice Guideline Summary The following evidence-based guideline was developed to assist Primary Care physicians and other clinicians in the management of asthma in adults. It was
Adult Asthma Clinical Practice Guideline Summary The following evidence-based guideline was developed to assist Primary Care physicians and other clinicians in the management of asthma in adults. It was
Asthma. UVM. University of Vermont. Alicia Jacobs MD Fletcher Allen Health Care and the University of Vermont
 University of Vermont ScholarWorks @ UVM Family Medicine Scholarly Works 6-14-2013 Asthma Alicia Jacobs MD Fletcher Allen Health Care and the University of Vermont Follow this and additional works at:
University of Vermont ScholarWorks @ UVM Family Medicine Scholarly Works 6-14-2013 Asthma Alicia Jacobs MD Fletcher Allen Health Care and the University of Vermont Follow this and additional works at:
Some Facts About Asthma
 Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
(Asthma) Diagnosis, monitoring and chronic asthma management
 Diagnosis, monitoring and chronic asthma management") Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Global Initiative for Asthma (GINA) What s new in GINA 2016?
 What s new in GINA 2016?") Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Inhaler Confusion. Today s Speaker Dr. Randall Brown. Director of Asthma Programs 6/7/2016. Dr. Randall Brown March 31, 2016
 + Inhaler Confusion Dr. Randall Brown March 31, 2016 + Today s Speaker Dr. Randall Brown Director of Asthma Programs Center for Managing Chronic Disease University of Michigan 1 ASTHMA ESSENTIALS IN PRIMARY
+ Inhaler Confusion Dr. Randall Brown March 31, 2016 + Today s Speaker Dr. Randall Brown Director of Asthma Programs Center for Managing Chronic Disease University of Michigan 1 ASTHMA ESSENTIALS IN PRIMARY
The Asthma Guidelines: Diagnosis and Assessment of Asthma
 The Asthma Guidelines: Diagnosis and Assessment of Asthma Christopher H. Fanta, M.D. Partners Asthma Center Brigham and Women s Hospital Harvard Medical School Objectives Know how the diagnosis of asthma
The Asthma Guidelines: Diagnosis and Assessment of Asthma Christopher H. Fanta, M.D. Partners Asthma Center Brigham and Women s Hospital Harvard Medical School Objectives Know how the diagnosis of asthma
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
ASTHMA BEST PRACTICES FOR SCHOOL NURSES. School Nurses November 2015
 ASTHMA BEST PRACTICES FOR SCHOOL NURSES School Nurses November 2015 1 BACKGROUND AND CURRENT STATS General definitions and explanations 2 Incidence of Asthma Centers for Disease Control (CDC) - 1 in 12
ASTHMA BEST PRACTICES FOR SCHOOL NURSES School Nurses November 2015 1 BACKGROUND AND CURRENT STATS General definitions and explanations 2 Incidence of Asthma Centers for Disease Control (CDC) - 1 in 12
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies
 Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
Asthma By Mayo Clinic staff
 MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
Current Approaches to Asthma & COPD
 10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
ASTHMA CARE FOR CHILDREN BASKET OF CARE SUBCOMMITTEE Report to: Minnesota Department of Health. June 22, 2009
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp ASTHMA CARE FOR CHILDREN
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp ASTHMA CARE FOR CHILDREN
Asthma. Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital. Figure 1 Asthma Prevalence,
 Asthma Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital Figure 1 Asthma Prevalence, 1980-2000 * Gap between 1995-1996 and 1997 indicates a break in trend due to
Asthma Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital Figure 1 Asthma Prevalence, 1980-2000 * Gap between 1995-1996 and 1997 indicates a break in trend due to
Allwin Mercer Dr Andrew Zurek
 Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
31 - Respiratory System
 31 - Respiratory System Asthma 1. Asthma has two components. Name the two components. 2. What are the common triggers of asthma? (LP p319) (e.g., pets) Upper respiratory infections ( ) 3. Describe a normal
31 - Respiratory System Asthma 1. Asthma has two components. Name the two components. 2. What are the common triggers of asthma? (LP p319) (e.g., pets) Upper respiratory infections ( ) 3. Describe a normal
Asthma. chapter 7. Overview
 chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Work Group on the Algorithm for the Diagnosis and Management of Asthma: a Practice Parameter update:
 Página 1 de 10 MD Consult information may not be reproduced, retransmitted, stored, distributed, disseminated, sold, published, broadcast or circulated in any medium to anyone, including but not limited
Página 1 de 10 MD Consult information may not be reproduced, retransmitted, stored, distributed, disseminated, sold, published, broadcast or circulated in any medium to anyone, including but not limited
1. ASTHMA 1. Eve A. Kerr, MD, MPH and Kenneth A. Clark, MD, MPH
 1. ASTHMA 1 Eve A. Kerr, MD, MPH and Kenneth A. Clark, MD, MPH The general approach to developing quality indicators for asthma diagnosis and treatment was based on Guidelines for the Diagnosis and Management
1. ASTHMA 1 Eve A. Kerr, MD, MPH and Kenneth A. Clark, MD, MPH The general approach to developing quality indicators for asthma diagnosis and treatment was based on Guidelines for the Diagnosis and Management
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL
 DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
Known Allergies: Shellfish. Symptoms: abdominal pain, nausea, diarrhea, or vomiting. congestion, trouble breathing, or wheezing.
 CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al.
 Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
How to distinguish between uncontrolled and severe asthma
 How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
THE PLANNED ASTHMA VISIT
 THE PLANNED ASTHMA VISIT Rhonique Shields-Harris, MD Molly Savitz, MSN, FNP, AE-C CNHN Childhood Asthma QI MOC Learning Collaborative October 30, 2012 Childhood Asthma QI Collaborative CME Learning Objectives
THE PLANNED ASTHMA VISIT Rhonique Shields-Harris, MD Molly Savitz, MSN, FNP, AE-C CNHN Childhood Asthma QI MOC Learning Collaborative October 30, 2012 Childhood Asthma QI Collaborative CME Learning Objectives
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
COPD COPD. Update on COPD and Asthma
 Update on COPD and Asthma Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco, CA COPD COPD
Update on COPD and Asthma Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco, CA COPD COPD
Allergies and Asthma 5/21/2013. Objectives. Allergic Rhinitis (AR): Risk Factor for ASTHMA. Rhinitis and Asthma
: Risk Factor for ASTHMA. Rhinitis and Asthma") Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Life-long asthma and its relationship to COPD. Stephen T Holgate School of Medicine University of Southampton
 Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Asthma in Day to Day Practice
 Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
HealthPartners Care Coordination Clinical Care Planning and Resource Guide ASTHMA
 The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University
 Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University Asthma-related Comorbidities Comorbid conditions of the upper airways Rhinitis and Sinusitis
Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University Asthma-related Comorbidities Comorbid conditions of the upper airways Rhinitis and Sinusitis
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
Meeting the Challenges of Asthma
 Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 Page 1 of 9 PURPOSE To assure that DOP inmates with Pulmonary Diseases are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers and Chronic Disease Nurses are
Page 1 of 9 PURPOSE To assure that DOP inmates with Pulmonary Diseases are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers and Chronic Disease Nurses are
A review of the current guidelines for allergic rhinitis and asthma
 A review of the current guidelines for allergic rhinitis and asthma Robert F. Lemanske, Jr., MD Madison, Wis. Allergic rhinitis and asthma are common chronic respiratory tract disorders. These disorders
A review of the current guidelines for allergic rhinitis and asthma Robert F. Lemanske, Jr., MD Madison, Wis. Allergic rhinitis and asthma are common chronic respiratory tract disorders. These disorders