Novel Therapies in Autoimmune Hepatitis
|
|
|
- Jeffery Clifton Walsh
- 6 years ago
- Views:
Transcription
1 Novel Therapies in Autoimmune Hepatitis Paul W. Rassam,MD Ass. Clinical Professor of Medicine Div. of Gastroenterology and Hepatology St George Hospital University Medical Center University of Balamand


2 Approaches to Treatment of AIH Need for Alternative Drugs
3 Background 40% of patients with untreated severe disease die within 6 mos of dx and if they survive the first 2 years of illness typically survive long term 10 yrs survival rate < 30% in mild untreated cases without treatment An acute onset of illness is seen in 40% patients Prednisone and azathioprine are mainstay of treatment
4
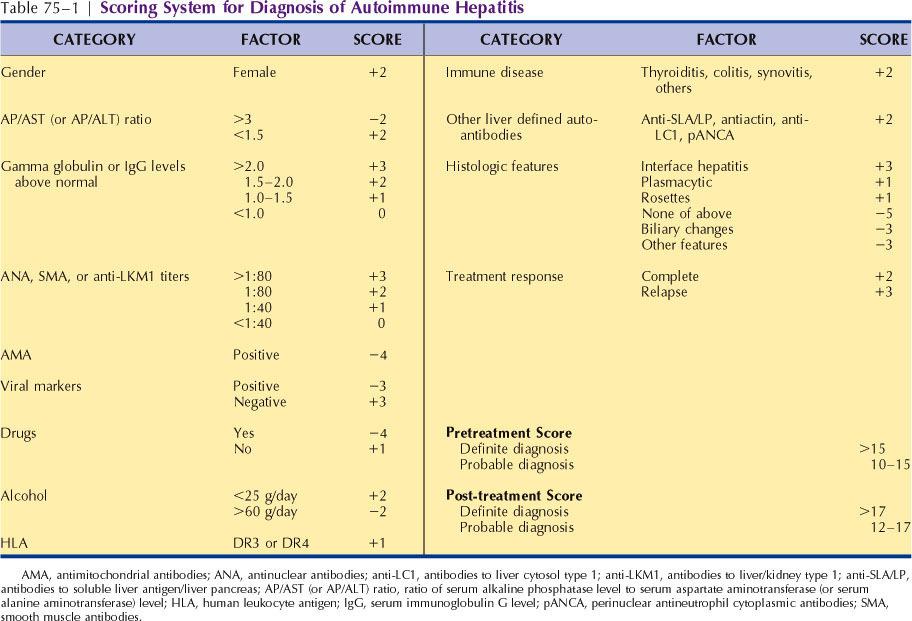
5 AIH simplified score Autoantibodies ANA or SMA ANA or SMA Antibodies to liver kidney microsome type 1 Antibodies to soluble liver antigen Absent autoantibodies +1:40 +1:80 +1:40 Positive None Immunoglobulin level Immunoglobulin G Histological Findings Morphological features of AIH Viral Disease Absence of viral hepatitis Score pre- treatment +=7 Dg certain +UNL +1.1 ULN Normal Compatible Typical Incompatible No viral markers Viral markers present Score pre- treatment 6 Dg probable Hennes EM, Zeniya M, Czaja AJ, Pares A, Dalekos GN, Krawitt EL, et al. Simplified diagnostic criteria for autoimmune hepatitis. HEPATOLOGY 2008;48:

6 HAI Comparaison of scores Simplified score not valid in overlap syndromes Both scores are equally sensitive but simplified score more specific
7 Indications for Treatment Absolute Serum AST>10x uln Serum AST>5x uln and globulin >2x nl Bridging necrosis or multiacinar necrosis Relative Symptoms (fatigue, arthralgia, jaundice) Serum AST and globulin less than absolute criteria Interface hepatitis No symptoms None Inactive cirrhosis Porta hepatitis
8 Pitfalls in therapy of AIH Inadequate initial therapy (histological remission lags behind biochemical remission) Failure to consider steroid sparing/free regimens Initiation of therapy without approriate indications (mild hepatitis, inactive cirrhosis) Persistent life long therapy in first complete remission with benign follow up liver biopsies Failure to recognize overalp syndromes
9 Prognostic Indices before Treatment Laboratory findings at presentation AST>10x nl: 50%, 3-year mortality AST>5x nl + GG>2x nl; 90%, 10-yr mortality AST<10x nl + GG<2x nl; 49%, cirrhosis at 15 yr; 10% 10-yr mortality Initial histolopathologic findings at presentation Interface hepatitis: 17% progression to cirrhosis in 5 yrs Bridging necrosis: 82% cirrhosis at 5 yrs; 45% 5-yr mortality Cirrhosis: 58%, 5 yr-mortality
10 Prognostic Indices after Treatment HLA B8, DR3 (onset at young age, severe disease at presentation, frequent relapse, need for OLT) HLA DR4 (onset in old age, women, response to steroids, concurrent immunological diseases) Multilobular necrosis with failure to respond, persistent hyperbilirubinemia after 2 weeks Failure to enter remission after 4 years and any occurrence of first sign of decompensation
11 Treatment Regimens Prednisone only Combination (Pred + AZA) Week 1 60 mg 30 mg+50 mg Week 2 40 mg 20 mg+50 mg Week 3 30 mg 15 mg+50 mg Week 4 30 mg 15 mg+50 mg Maintenance until endpoint 20 mg 10mg+50 mg
12 Therapy Autoimmune Hepatitis Remission following Prednisone +/-Azathioprine Absence of symptoms Absent or minimal piecemeal necrosis AST < twice normal value & normal bilirubin + gamma globulin % response to 6 months therapy symptoms biochemistry histology
13 Reasons for Preference Prednisone Severe cytopenia TPMT deficiency Pregnancy Malignancy Short course <6 mos Prior AZA intolerance Acute fulminant onset Prednisone and AZA Postmenopausal state Osteoporosis Brittle diabetes Obesity Acne Emotional lability Hypertension Prolonged therapy Elderly
14 Treatment Outcomes Remission (65-80%) Treatment Failure (9%) Incomplete Response (13%) Drug Toxicity/Intolerance (10%) Relapse off therapy Acute severe fulminant presentation
15 Remission Criteria Disappearance of symptoms for 2 yrs Normal bilirubin + globulin levels Transaminases normal or less than 2x Normal histology or minimal inflammation No interface hepatitis Histology lags 6 months Action Gradual withdrawal of prednisone over 6 wks Discontinuation of azathioprine Regular monitoring of AST/ALT/IgG at 3 wks intervals during and 3 months after drug withdrawal
16 Acute Severe Fulminant Prompt therapy with steroids monotherapy (?IV) AZA 50 mg/d added if therapy beyond 3 months OLT evaluation if: -worsening of condition with liver failure -worsening of biochemical parameters -progressive hyperbilirubinemia -no improvement in 2 weeks of intensive treatment -overall 5 yrs survival rates 50-80% Increased frequency of acute allograft rejection AIH recurrence 30-40% if inadequate immunosuppression
17 Incomplete Response Criteria Some or no improvement in clinical,and histology during therapy Failure to achieve remission after 3 years No worsening of condition Improvement in AST/ALT within twice ULN or normal AST/ALT without complete normalization IgG Action Reduction of pred dose 2.5 mg/month to lowest levels possible (< 10 mg/d) to prevent worsening AST/ALT Indefinite AZA 2 mg/kg if steroid intolerant Other immunosuppression (MMF/Cyclo/Tacrolimus) Check compliance Consider liver bx (exclude other diseases, HAI score)
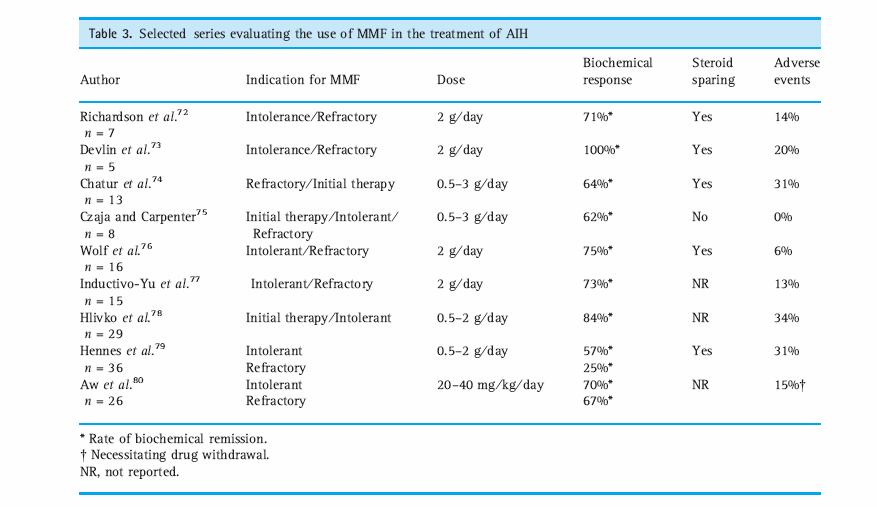
18 Drug Toxicity/Intolerance Reduce dose or stop offending agent Maintenance on tolerated drug in adjustred dose MMF? as an empiric option for AZ intolerance with a response rate around 70% Consider other immunosuppressives
19 Drug Toxicity
20 Treatment Failure Criteria Worsening clinical, labs and histology despite compliance Inc transaminasis by 67% Development of jaundice, ascites or hepatic encephalopathy Common in cirrhotics, disease onset at young age, long time before diagnosis, HLA B8 and/or HLA DR3 Action Pred 60 mg/d or pred 30 mg/d with AZA 150 mg/d x 1 mo (? 2mg/kg) Reduction of the dose each month of improvement until maintenance levels MMF 1 gm BID Prograf 4 mg BID Cyclosporin 2-3 mg/kg/d OLT as last option
21 Relapse Criteria: -Occurs in 20-80% who enter remission -Depends on histology at end point (presence of portal plasma cells, interface hepatitis, inactive cirrhosis)- -Increase AST>3folds -Increase IgG >2g/dl Action: (after 2 relapses) Retreat with same original regimen than taper Indefinite low dose prednisone (<10 mg/d) if AZA intolerant Indefinite low dose AZA 2 mg/kg/d Enforce compliance Does not need to be life-long? Role for combination
22 Maintenance Therapy Lowest effective dose for Prednisone 10mg/d or AZA mg/kg/d or Prednisosone 10 mg/d plus AZA 50 mg/d
23 Withdrawal of Therapy Withdrawal of therapy more successful if total duration of therapy at least 4 years Do not attempt in AIH type 2 (LKM+) Biopsy useful to assess histologic activity - wean prednisone by 2.5 mg q 3 months - wean AZA by 25 mg q 3 months - check ALT/AST/IgG monthly - if reactivation occurs, prednisone 0.5 mg/kg will suffice
24 Methotrexate Methotrexate Immunosuppressive effects due to inhibition of enzyme involved in the metabolism of folic acid MTX can be used as a second-line therapy in pediatric patients with AIH type I in whom traditional therapy with steroids and AZA/6-MP has failed or if the patient was to become intolerant to this regimen Relatively rapid onset of action (4-6 weeks) Side effects Stomatitis Oral ulcers GI upset Teratogenic in women of child bearing age
25 MMF Mycophenolate mofetil (MMF) is an alternative option for patients intolerant or incomplete responders to prior AZA therapy However a majority of patients fail MMF Patients with prior nonresponse to AZA have an even lower response rate to MMF as second line therapy with exceedingly SE (31%)
26
27 Cyclosporine Cyclosporine 3rd immunosuppressant identified Cyclic nonribosomal peptide Site of action- calcineurin (inhibits phosphatase activity) Side effects Interacts with a wide variety of other drugs and substances hyperplasia, convulsions, peptic ulcers, fever, vomiting, diarrhea, confusion, breathing difficulties, numbness and tingling, high blood pressure, kidney and liver dysfunction
28
29 Budesonide Corticosteroid with the highest affinity to glucocorticoid receptor and with a high 90% first pass in the liver (thus less steroid related SE ) Several controversial studies in the last decade as for it s role in inducing remission however it appears to be recommended in steroid dependant or steroid and AZA intolerant AIH patients Budesonide in combination with AZA induces and maintain remission in non cirrhotics patients with AIH
 or Prednisone (40 mg/d, tapered to 10 mg/d) PLUS")
30 compared the effects of budesonide and prednisone, both in combination with azathioprine. 6-month, prospective, double-blind multicenter RCT in patients with AIH without evidence of cirrhosis budesonide (3 mg, TID or BID) or Prednisone (40 mg/d, tapered to 10 mg/d) PLUS azathioprine (1 2 mg/kg/d) Primary end point: complete biochemical remission, (normalast and ALT,, at 6 months.
31 Results The primary end point was achieved in 47/100 patients given budesonide (47.0%) and in 19/103 patients given prednisone (18.4%). At 6 months, complete biochemical remission occurred in 60% of the patients given budesonide versus 38.8% of those given prednisone 72.0% of those in the budesonide group did not develop steroid-specific side effects versus 46.6% in the prednisone Among 87 patients who were initially given prednisone and then received budesonide after 6 months, steroid-specific side effects decreased from 44.8% to 26.4% at month 12
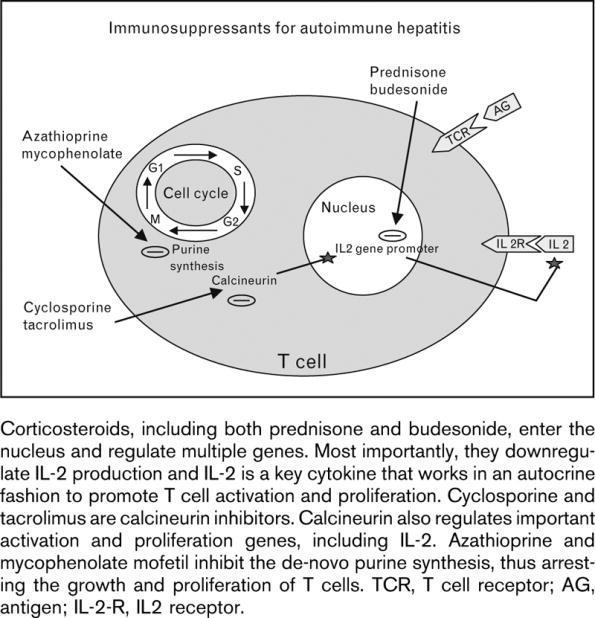
32 Immunosupressants in AIH


33 Algorithm for Treatment of AIH
34 Overlap Syndromes
35 AIH and Pregnancy If AIH in remission pregnancy tolerated unless evidence for PHTN Increased frequency of stillbirth and prematurity Many reports of AIH de novo or flares during pregnancy or post partum Consider increasing steroid dose shortly before the expected date of delivery Standard immunosuppression appears to be safe
36 Take Home Messages 1. The major factor of successful management of autoimmune hepatitis is the timely establishment of the correct diagnosis 2- Standard treatment is not ideal and characterized mainly by steroid side effects that affect compliance 3- Remisssion endpoints should aim at normalization of ALT/IgG and histology preferable with AZA monotherapy for 3-4 yrs 4- Steroids are drug of choice for remission induction and in noncirrhotic patients budesonide may offer an attractive alternative 5- Consider MMF (preferably), cyclosporin, or tacrolimus for treatment failures or when AZA not tolerated 6- OLT represents the ultimate treatment in true non responders with signs of pending liver failure with good survival rates but also a significant risk of graft loss because of disease recurrence
Serologic Markers CONVENTIONAL ANTIBODIES ANTIBODIES UNCONVENTIONAL. AIH Type I
 Autoimmune Hepatitis By Thomas Frazier Objective What we need to know about AIH Diagnosis Treatment Difficulties in both Liver transplantation concerns AASLD Guidelines: Hepatology. 2010 Jun;51(6):2193-213.
Autoimmune Hepatitis By Thomas Frazier Objective What we need to know about AIH Diagnosis Treatment Difficulties in both Liver transplantation concerns AASLD Guidelines: Hepatology. 2010 Jun;51(6):2193-213.
Autoimmune Hepatitis in Clinical Practice
 1 Autoimmune Hepatitis in Clinical Practice Atif Zaman, MD MPH Professor of Medicine Senior Associate Dean for Clinical and Faculty Affairs School of Medicine Oregon Health & Science University Disclosure
1 Autoimmune Hepatitis in Clinical Practice Atif Zaman, MD MPH Professor of Medicine Senior Associate Dean for Clinical and Faculty Affairs School of Medicine Oregon Health & Science University Disclosure
Autoimmune Hepatitis. What Drug and for How Long? Hepatology Day May 30 th, 2015
 Autoimmune Hepatitis What Drug and for How Long? Rajaa Chatila, MD Associate Professor of Medicine Director, Internal Medicine Residency Program Lebanese American University Hepatology Day May 30 th, 2015
Autoimmune Hepatitis What Drug and for How Long? Rajaa Chatila, MD Associate Professor of Medicine Director, Internal Medicine Residency Program Lebanese American University Hepatology Day May 30 th, 2015
Autoimmune Hepatitis. Dr. Stefania Casu Hepatology, UVCM, Inselspital Bern. November 14th, 2018
 Autoimmune Hepatitis Dr. Stefania Casu Hepatology, UVCM, Inselspital Bern November 14th, 2018 AIH - Definition Manns MP J Hepatol 2015, vol 62, P 100-111 AIH - Definition Autoimmune hepatitis (AIH) is
Autoimmune Hepatitis Dr. Stefania Casu Hepatology, UVCM, Inselspital Bern November 14th, 2018 AIH - Definition Manns MP J Hepatol 2015, vol 62, P 100-111 AIH - Definition Autoimmune hepatitis (AIH) is
budesonide, 3mg, gastro-resistant capsules (Budenofalk ) SMC No. (1043/15) Dr Falk Pharma UK Ltd
 SMC No. (1043/15) Dr Falk Pharma UK Ltd") budesonide, 3mg, gastro-resistant capsules (Budenofalk ) SMC No. (1043/15) Dr Falk Pharma UK Ltd 10 April 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
budesonide, 3mg, gastro-resistant capsules (Budenofalk ) SMC No. (1043/15) Dr Falk Pharma UK Ltd 10 April 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Difficult treatment decisions in autoimmune hepatitis
 Online Submissions: http://www.wjgnet.com/1007-9327office wjg@wjgnet.com doi:10.3748/wjg.v16.i8.934 World J Gastroenterol 2010 February 28; 16(8): 934-947 ISSN 1007-9327 (print) 2010 Baishideng. All rights
Online Submissions: http://www.wjgnet.com/1007-9327office wjg@wjgnet.com doi:10.3748/wjg.v16.i8.934 World J Gastroenterol 2010 February 28; 16(8): 934-947 ISSN 1007-9327 (print) 2010 Baishideng. All rights
Guideline Summary NGC-8005
 NGC banner Guideline Summary NGC-8005 Guideline Title Diagnosis and management of autoimmune hepatitis. Bibliographic Source(s) Manns MP, Czaja AJ, Gorham JD, Krawitt EL, Mieli-Vergani G, Vergani D, Vierling
NGC banner Guideline Summary NGC-8005 Guideline Title Diagnosis and management of autoimmune hepatitis. Bibliographic Source(s) Manns MP, Czaja AJ, Gorham JD, Krawitt EL, Mieli-Vergani G, Vergani D, Vierling
Hepatitis Autoinmune: Terapias Emergentes
 Hepatitis Autoinmune: Terapias Emergentes Jorge Rakela, MD, MACP, FAASLD Getz Family Research Professor Mayo Clinic Arizona Phoenix, AZ Santiago, 29 de septiembre, 2016 2013 MFMER slide-1 Objetivos: Describir
Hepatitis Autoinmune: Terapias Emergentes Jorge Rakela, MD, MACP, FAASLD Getz Family Research Professor Mayo Clinic Arizona Phoenix, AZ Santiago, 29 de septiembre, 2016 2013 MFMER slide-1 Objetivos: Describir
Diagnosis and Management of Autoimmune Hepatitis: Current Status and Future Directions
 Gut and Liver, Vol. 10, No. 2, March 2016, pp. 177-203 Review Diagnosis and Management of Autoimmune Hepatitis: Current Status and Future Directions Albert J. Czaja Division of Gastroenterology and Hepatology,
Gut and Liver, Vol. 10, No. 2, March 2016, pp. 177-203 Review Diagnosis and Management of Autoimmune Hepatitis: Current Status and Future Directions Albert J. Czaja Division of Gastroenterology and Hepatology,
Comparing Efficacy Between Regimens in the Initial Treatment of Autoimmune Hepatitis
 Elmer Original Article ress Comparing Efficacy Between Regimens in the Initial Treatment of Autoimmune Hepatitis Chijioke Enweluzo a, b, Fahad Aziz a, Amit Mori a Abstract Background: Autoimmune hepatitis
Elmer Original Article ress Comparing Efficacy Between Regimens in the Initial Treatment of Autoimmune Hepatitis Chijioke Enweluzo a, b, Fahad Aziz a, Amit Mori a Abstract Background: Autoimmune hepatitis
Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP
 Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP Autoimmune hepatobiliary diseases The liver is an important target for immunemediated injury. Three disease phenotypes are recognized:
Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP Autoimmune hepatobiliary diseases The liver is an important target for immunemediated injury. Three disease phenotypes are recognized:
Domenico ALVARO, MD Sapienza, University of Rome, Italy. Congresso Nazionale della Società Italiana di GastroReumatologia, Roma, 25 Giugno 2015.
 Epatite autoimmune e sindrome da "overlap Domenico ALVARO, MD Sapienza, University of Rome, Italy Congresso Nazionale della Società Italiana di GastroReumatologia, Roma, 25 Giugno 2015. AUTOIMMUNE HEPATITIS
Epatite autoimmune e sindrome da "overlap Domenico ALVARO, MD Sapienza, University of Rome, Italy Congresso Nazionale della Società Italiana di GastroReumatologia, Roma, 25 Giugno 2015. AUTOIMMUNE HEPATITIS
Management of autoimmune hepatitis. Pierre-Emmanuel RAUTOU Inserm U970, Paris Service d hépatologie, Hôpital Beaujon, Clichy, France
 Management of autoimmune hepatitis Pierre-Emmanuel RAUTOU Inserm U970, PARCC@HEGP, Paris Service d hépatologie, Hôpital Beaujon, Clichy, France Case 1 52 year-old woman, referred for liver blood tests
Management of autoimmune hepatitis Pierre-Emmanuel RAUTOU Inserm U970, PARCC@HEGP, Paris Service d hépatologie, Hôpital Beaujon, Clichy, France Case 1 52 year-old woman, referred for liver blood tests
Hépatopathies auto-immunes
 16 ème Journée d'automne Lausanne, le 19 octobre 2017 Hépatopathies auto-immunes Nurullah Aslan et Darius Moradpour Service de Gastroentérologie et d'hépatologie Centre Hospitalier Universitaire Vaudois
16 ème Journée d'automne Lausanne, le 19 octobre 2017 Hépatopathies auto-immunes Nurullah Aslan et Darius Moradpour Service de Gastroentérologie et d'hépatologie Centre Hospitalier Universitaire Vaudois
Clinical characteristics and response to therapy of autoimmune hepatitis in an urban Latino population
 Gastroenterology and Hepatology From Bed to Bench. 2016 RIGLD, Research Institute for Gastroenterology and Liver Diseases BRIEF REPORT Clinical characteristics and response to therapy of autoimmune hepatitis
Gastroenterology and Hepatology From Bed to Bench. 2016 RIGLD, Research Institute for Gastroenterology and Liver Diseases BRIEF REPORT Clinical characteristics and response to therapy of autoimmune hepatitis
Management of autoimmune hepatitis. Pierre-Emmanuel RAUTOU Inserm U970, Paris Service d hépatologie, Hôpital Beaujon, Clichy, France
 Management of autoimmune hepatitis Pierre-Emmanuel RAUTOU Inserm U970, PARCC@HEGP, Paris Service d hépatologie, Hôpital Beaujon, Clichy, France 41 year-old woman, coming to emergency department for fatigue
Management of autoimmune hepatitis Pierre-Emmanuel RAUTOU Inserm U970, PARCC@HEGP, Paris Service d hépatologie, Hôpital Beaujon, Clichy, France 41 year-old woman, coming to emergency department for fatigue
CASE 1 Plasma Cell Infiltrates: Significance in post liver transplantation and in chronic liver disease
 CASE 1 Plasma Cell Infiltrates: Significance in post liver transplantation and in chronic liver disease Maria Isabel Fiel, M.D. The Mount Sinai Medical Center New York, New York Case A 57 yo man, 7 months
CASE 1 Plasma Cell Infiltrates: Significance in post liver transplantation and in chronic liver disease Maria Isabel Fiel, M.D. The Mount Sinai Medical Center New York, New York Case A 57 yo man, 7 months
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
A Single Center Review of the Use of Mycophenolate Mofetil in the Treatment of Autoimmune Hepatitis
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:1036 1040 A Single Center Review of the Use of Mycophenolate Mofetil in the Treatment of Autoimmune Hepatitis JONATHAN T. HLIVKO, MITCHELL L. SHIFFMAN, R.
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:1036 1040 A Single Center Review of the Use of Mycophenolate Mofetil in the Treatment of Autoimmune Hepatitis JONATHAN T. HLIVKO, MITCHELL L. SHIFFMAN, R.
LIVER TRANSPLANTATION FOR OVERLAP SYNDROMES OF AUTOIMMUNE LIVER DISEASES
 LIVER TRANSPLANTATION FOR OVERLAP SYNDROMES OF AUTOIMMUNE LIVER DISEASES No conflict of interest Objectives Introduction Methods Results Conclusions Objectives Introduction Methods Results Conclusions
LIVER TRANSPLANTATION FOR OVERLAP SYNDROMES OF AUTOIMMUNE LIVER DISEASES No conflict of interest Objectives Introduction Methods Results Conclusions Objectives Introduction Methods Results Conclusions
TREATMENT OF PRIMARY BILIARY CIRRHOSIS (PBC)
") TREATMENT OF PRIMARY BILIARY CIRRHOSIS (PBC) URSO not indicated Therapy for PBC Difficulties Etiology is uncertain Therapies are based on ideas regarding pathogenesis Present medical therapies have a limited
TREATMENT OF PRIMARY BILIARY CIRRHOSIS (PBC) URSO not indicated Therapy for PBC Difficulties Etiology is uncertain Therapies are based on ideas regarding pathogenesis Present medical therapies have a limited
ACCME/Disclosures. The Overlap Syndromes: Do They Exist? Key Points and Questions 4/6/2016. Hans Popper Hepatopathology Society
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
Fat, ballooning, plasma cells and a +ANA. Yikes! USCAP 2016 Evening Specialty Conference Cynthia Guy
 Fat, ballooning, plasma cells and a +ANA. Yikes! USCAP 2016 Evening Specialty Conference Cynthia Guy Goals Share an interesting case Important because it highlights a common problem that we re likely to
Fat, ballooning, plasma cells and a +ANA. Yikes! USCAP 2016 Evening Specialty Conference Cynthia Guy Goals Share an interesting case Important because it highlights a common problem that we re likely to
Prototypes of autoimmune hepatitis and sclerosing cholangitis in childhood
 RIUNIONE MONOTEMATICA AISF 2013 Personalizzazione della Cura in Epatologia 17-19 ottobre 2013, PISA Prototypes of autoimmune hepatitis and sclerosing cholangitis in childhood La sottoscritta dichiara di
RIUNIONE MONOTEMATICA AISF 2013 Personalizzazione della Cura in Epatologia 17-19 ottobre 2013, PISA Prototypes of autoimmune hepatitis and sclerosing cholangitis in childhood La sottoscritta dichiara di
Autoimmune hepatitis
 Autoimmune hepatitis: Autoimmune hepatitis a spectrum within a spectrum Alastair Burt Professor of Pathology and Dean of Clinical Medicine Newcastle University Spectrum of autoimmune liver disease Autoimmune
Autoimmune hepatitis: Autoimmune hepatitis a spectrum within a spectrum Alastair Burt Professor of Pathology and Dean of Clinical Medicine Newcastle University Spectrum of autoimmune liver disease Autoimmune
Autoimmune Hepatitis in the Elderly: Diagnosis and Pharmacologic Management
 Drugs Aging https://doi.org/10.1007/s40266-018-0556-0 THERAPY IN PRACTICE Autoimmune Hepatitis in the Elderly: Diagnosis and Pharmacologic Management Syed Rizvi 1 Samer Gawrieh 2 Ó Springer International
Drugs Aging https://doi.org/10.1007/s40266-018-0556-0 THERAPY IN PRACTICE Autoimmune Hepatitis in the Elderly: Diagnosis and Pharmacologic Management Syed Rizvi 1 Samer Gawrieh 2 Ó Springer International
Kalliopi Azariadi, Pinelopi Arvaniti, Nikolaos Gatselis, George N. Dalekos, Kalliopi Zachou
 Severe acute non-a, non-b, non-c hepatitis with autoimmune features: Consider acute hepatitis E virus (HEV) infection not just autoimmune hepatitis (AIH) Kalliopi Azariadi, Pinelopi Arvaniti, Nikolaos
Severe acute non-a, non-b, non-c hepatitis with autoimmune features: Consider acute hepatitis E virus (HEV) infection not just autoimmune hepatitis (AIH) Kalliopi Azariadi, Pinelopi Arvaniti, Nikolaos
PBC features and management in the era of UDCA and Budesonide
 PBC features and management in the era of UDCA and Budesonide Raoul Poupon, MD Université P&M Curie, AP-Hôpitaux de Paris, Inserm, Paris, France The changing pattern of PBC Over the last 2 decades: More
PBC features and management in the era of UDCA and Budesonide Raoul Poupon, MD Université P&M Curie, AP-Hôpitaux de Paris, Inserm, Paris, France The changing pattern of PBC Over the last 2 decades: More
ORIGINAL ARTICLES LIVER, PANCREAS, AND BILIARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:98 103 ORIGINAL ARTICLES LIVER, PANCREAS, AND BILIARY TRACT Serologic Markers Do Not Predict Histologic Severity or Response to Treatment in Patients With
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:98 103 ORIGINAL ARTICLES LIVER, PANCREAS, AND BILIARY TRACT Serologic Markers Do Not Predict Histologic Severity or Response to Treatment in Patients With
Steroid Minimization: Great Idea or Silly Move?
 Steroid Minimization: Great Idea or Silly Move? Disclosures I have financial relationship(s) within the last 12 months relevant to my presentation with: Astellas Grants ** Bristol Myers Squibb Grants,
Steroid Minimization: Great Idea or Silly Move? Disclosures I have financial relationship(s) within the last 12 months relevant to my presentation with: Astellas Grants ** Bristol Myers Squibb Grants,
MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS
 MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS Wai K. Leung Li Shu Fan Medical Foundation Professor in Gastroenterology Associate Dean (Human Capital), LKS Faculty of Medicine, University
MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS Wai K. Leung Li Shu Fan Medical Foundation Professor in Gastroenterology Associate Dean (Human Capital), LKS Faculty of Medicine, University
Overview of PSC Jayant A. Talwalkar, MD, MPH Associate Professor of Medicine Mayo Clinic Rochester, MN
 Overview of PSC Jayant A. Talwalkar, MD, MPH Associate Professor of Medicine Mayo Clinic Rochester, MN 2012 Annual Conference PSC Partners Seeking a Cure May 5, 2012 Primary Sclerosing Cholangitis Multifocal
Overview of PSC Jayant A. Talwalkar, MD, MPH Associate Professor of Medicine Mayo Clinic Rochester, MN 2012 Annual Conference PSC Partners Seeking a Cure May 5, 2012 Primary Sclerosing Cholangitis Multifocal
ANCA+ VASCULITIDES CYCAZAREM,
 ANCA+ VASCULITIDES CYCAZAREM, q Comparison of 3 to 6 mo. oral CYC + CS then azathioprine or oral CYC for 12 mo.+ 10 mg/d CS. After 12 mo all the patients were treated with azathioprine q 150 patients followed
ANCA+ VASCULITIDES CYCAZAREM, q Comparison of 3 to 6 mo. oral CYC + CS then azathioprine or oral CYC for 12 mo.+ 10 mg/d CS. After 12 mo all the patients were treated with azathioprine q 150 patients followed
Transplant Hepatology
 Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant
 SDC, Patients and Methods Complement-dependent lymphocytotoxic crossmatch test () Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant donor-specific CXM was
SDC, Patients and Methods Complement-dependent lymphocytotoxic crossmatch test () Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant donor-specific CXM was
Autoimmune hepatitis: an approach to disease understanding and management
 British Medical Bulletin, 2015, 114:181 191 doi: 10.1093/bmb/ldv021 Advance Access Publication Date: 20 May 2015 Autoimmune hepatitis: an approach to disease understanding and management Margaret Corrigan,
British Medical Bulletin, 2015, 114:181 191 doi: 10.1093/bmb/ldv021 Advance Access Publication Date: 20 May 2015 Autoimmune hepatitis: an approach to disease understanding and management Margaret Corrigan,
1238 Autoimmune Hepatitis Mayo Clin Proc, December 2001, Vol 76 Table 1. Criteria for the Diagnosis of Autoimmune Hepatitis* Diagnostic criteria Diagn
 Mayo Clin Proc, December 2001, Vol 76 Autoimmune Hepatitis 1237 Review Current Concepts in the Diagnosis, Pathogenesis, and Treatment of Autoimmune Hepatitis JAMEELA ABDULLAH AL-KHALIDI, MD, AND ALBERT
Mayo Clin Proc, December 2001, Vol 76 Autoimmune Hepatitis 1237 Review Current Concepts in the Diagnosis, Pathogenesis, and Treatment of Autoimmune Hepatitis JAMEELA ABDULLAH AL-KHALIDI, MD, AND ALBERT
Key Points: Autoimmune Liver Disease: Update for Pathologists from the Hepatologist s Perspective. Jenny Heathcote, MD. University of Toronto
 Autoimmune Liver Disease: Update for Pathologists from the Hepatologist s Perspective Jenny Heathcote, MD University of Toronto Key Points: AILD comprise autoimmune hepatitis, primary biliary cirrhosis
Autoimmune Liver Disease: Update for Pathologists from the Hepatologist s Perspective Jenny Heathcote, MD University of Toronto Key Points: AILD comprise autoimmune hepatitis, primary biliary cirrhosis
A Case of Autoimmune Hepatitis with Antimitochondrial Antibody and No Detectable Antinuclear Antibody
 FFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFF St. Marianna Med. J. Case Report Vol. 32, pp. 33 38, 2004 FFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFF A Case
FFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFF St. Marianna Med. J. Case Report Vol. 32, pp. 33 38, 2004 FFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFFF A Case
Figure 1. Actuarial survival of patients with ABO I, ABO compatible, and ABO identical grafts.
 New Insights into Antibody Mediated Graft Injury after Pediatric Liver Transplantation S.V. McDiarmid MD Professor of Pediatrics and Surgery David Geffen School of Medicine University of California, Los
New Insights into Antibody Mediated Graft Injury after Pediatric Liver Transplantation S.V. McDiarmid MD Professor of Pediatrics and Surgery David Geffen School of Medicine University of California, Los
PBC/AIH variant/ overlap syndrome vs PBC with hepatitic features?
 22 November 2018 BD-IAP UK-LPG Liver Update PBC/AIH variant/ overlap syndrome vs PBC with hepatitic features? in a UDCA non-responder Dina G. Tiniakos Institute of Cellular Medicine, Faculty of Medical
22 November 2018 BD-IAP UK-LPG Liver Update PBC/AIH variant/ overlap syndrome vs PBC with hepatitic features? in a UDCA non-responder Dina G. Tiniakos Institute of Cellular Medicine, Faculty of Medical
Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids. Cholestasis
 Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids Cholestasis Biochemical hallmark Impaired bile flow from liver to small intestine Alkaline phosphatase is primary
Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids Cholestasis Biochemical hallmark Impaired bile flow from liver to small intestine Alkaline phosphatase is primary
Autoimmune hepatitis (AIH) is a rare disease, yet it. Fulminant Hepatic Failure as the Initial Presentation of Acute Autoimmune Hepatitis
 is a rare disease, yet it. Fulminant Hepatic Failure as the Initial Presentation of Acute Autoimmune Hepatitis") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:625 631 Fulminant Hepatic Failure as the Initial Presentation of Acute Autoimmune Hepatitis WILLIAM R. KESSLER,* OSCAR W. CUMMINGS, GEORGE ECKERT, NAGA CHALASANI,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:625 631 Fulminant Hepatic Failure as the Initial Presentation of Acute Autoimmune Hepatitis WILLIAM R. KESSLER,* OSCAR W. CUMMINGS, GEORGE ECKERT, NAGA CHALASANI,*
BK Virus (BKV) Management Guideline: July 2017
 Management Guideline: July 2017") BK Virus (BKV) Management Guideline: July 2017 BK virus has up to a 60-80% seroprevalence rate in adults due to a primary oral or respiratory exposure in childhood. In the immumocompromised renal transplant
BK Virus (BKV) Management Guideline: July 2017 BK virus has up to a 60-80% seroprevalence rate in adults due to a primary oral or respiratory exposure in childhood. In the immumocompromised renal transplant
Regulatory Status FDA-approved indication: Tysabri is an integrin receptor antagonist indicated for treatment of:
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.08.27 1 of 6 Last Review Date: December 5, 2014 Tysabri Description Tysabri (natalizumab) Background
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.08.27 1 of 6 Last Review Date: December 5, 2014 Tysabri Description Tysabri (natalizumab) Background
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture,
 To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
Regulatory Status FDA-approved indication: Tysabri is an integrin receptor antagonist indicated for treatment of (1):
:") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.60.13 Subject: Tysabri Page: 1 of 6 Last Review Date: June 22, 2017 Tysabri Description Tysabri (natalizumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.60.13 Subject: Tysabri Page: 1 of 6 Last Review Date: June 22, 2017 Tysabri Description Tysabri (natalizumab)
Overview of New Approaches to Immunosuppression in Renal Transplantation
 Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Investigations before OLT, Immunosuppression and rejection, Follow up after OLT.
 Investigations before OLT, Immunosuppression and rejection, Follow up after OLT andrea.degottardi@insel.ch When is liver transplantation indicated? When is liver transplantation indicated? Frequent: CIRRHOSIS
Investigations before OLT, Immunosuppression and rejection, Follow up after OLT andrea.degottardi@insel.ch When is liver transplantation indicated? When is liver transplantation indicated? Frequent: CIRRHOSIS
Autoimmune Liver Disease
 Autoimmune Liver Disease A Guide An explanation of what autoimmune liver diseases are including autoimmune hepatitis and autoimmune sclerosis cholangitis What are autoimmune diseases?... 4 What is autoimmune
Autoimmune Liver Disease A Guide An explanation of what autoimmune liver diseases are including autoimmune hepatitis and autoimmune sclerosis cholangitis What are autoimmune diseases?... 4 What is autoimmune
European Risk Management Plan. Measures impairment. Retreatment after Discontinuation
 European Risk Management Plan Table 6.1.4-1: Safety Concern 55024.1 Summary of Risk Minimization Measures Routine Risk Minimization Measures Additional Risk Minimization Measures impairment. Retreatment
European Risk Management Plan Table 6.1.4-1: Safety Concern 55024.1 Summary of Risk Minimization Measures Routine Risk Minimization Measures Additional Risk Minimization Measures impairment. Retreatment
Understanding Myositis Medications
 Understanding Myositis Medications 2015 TMA Annual Patient Conference Orlando, Florida Chester V. Oddis, MD University of Pittsburgh Director, Myositis Center Disclosures Mallinckrodt: Research Grant Genentech:
Understanding Myositis Medications 2015 TMA Annual Patient Conference Orlando, Florida Chester V. Oddis, MD University of Pittsburgh Director, Myositis Center Disclosures Mallinckrodt: Research Grant Genentech:
Immunosuppressants. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Immunosuppressants Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Immunosuppressive Agents Very useful in minimizing the occurrence of exaggerated or inappropriate
Immunosuppressants Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Immunosuppressive Agents Very useful in minimizing the occurrence of exaggerated or inappropriate
Drug Induced Liver Injury (DILI)
") Drug Induced Liver Injury (DILI) Aisling Considine- Consultant Hepatology Pharmacist. King s College Hospital NHS Foundation Trust aislingconsidine@nhs.net Drug Induced Liver Injury /Disease Acute Liver
Drug Induced Liver Injury (DILI) Aisling Considine- Consultant Hepatology Pharmacist. King s College Hospital NHS Foundation Trust aislingconsidine@nhs.net Drug Induced Liver Injury /Disease Acute Liver
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Tolerance Induction in Transplantation
 Tolerance Induction in Transplantation Reza F. Saidi, MD, FACS, FICS Assistant Professor of Surgery Division of Organ Transplantation Department of Surgery University of Massachusetts Medical School Percent
Tolerance Induction in Transplantation Reza F. Saidi, MD, FACS, FICS Assistant Professor of Surgery Division of Organ Transplantation Department of Surgery University of Massachusetts Medical School Percent
Hepatitis B Update. Jorge L. Herrera, M.D. University of South Alabama Mobile, AL. Gastroenterology
 Hepatitis B Update Jorge L. Herrera, M.D. University of South Alabama Mobile, AL Deciding Who to Treat Is hepatitis B a viral disease or a liver disease? Importance of HBV-DNA Levels in the Natural History
Hepatitis B Update Jorge L. Herrera, M.D. University of South Alabama Mobile, AL Deciding Who to Treat Is hepatitis B a viral disease or a liver disease? Importance of HBV-DNA Levels in the Natural History
Primary Sclerosing Cholangitis Medical Management
 Primary Sclerosing Cholangitis Medical Management Kapil Chopra M.D. Assistant Professor of Medicine Division of Transplant Medicine Mayo Clinic Arizona PSC Primary sclerosing cholangitis is a progressive
Primary Sclerosing Cholangitis Medical Management Kapil Chopra M.D. Assistant Professor of Medicine Division of Transplant Medicine Mayo Clinic Arizona PSC Primary sclerosing cholangitis is a progressive
Autoimmune and cholestatic liver diseases
 Autoimmune and cholestatic liver diseases Prof. Tom Hemming Karlsen Research Institute of Internal Medicine & Department of Transplantation Medicine University of Oslo & Oslo University Hospital, Norway
Autoimmune and cholestatic liver diseases Prof. Tom Hemming Karlsen Research Institute of Internal Medicine & Department of Transplantation Medicine University of Oslo & Oslo University Hospital, Norway
11 th Banff Conference on Allograft Pathology - An Update
 11 th Banff Conference on Allograft Pathology - An Update Stefan Hübscher, School of Cancer Sciences, University of Birmingham Dept of Cellular Pathology, Queen Elizabeth Hospital, Birmingham Enghien les
11 th Banff Conference on Allograft Pathology - An Update Stefan Hübscher, School of Cancer Sciences, University of Birmingham Dept of Cellular Pathology, Queen Elizabeth Hospital, Birmingham Enghien les
Recent advances in management of Pulmonary Vasculitis. Dr Nita MB
 Recent advances in management of Pulmonary Vasculitis Dr Nita MB 23-01-2015 Overview of the seminar Recent classification of Vasculitis What is new in present classification? Trials on remission induction
Recent advances in management of Pulmonary Vasculitis Dr Nita MB 23-01-2015 Overview of the seminar Recent classification of Vasculitis What is new in present classification? Trials on remission induction
CLINICAL ADVANCES IN LIVER, PANCREAS, AND BILIARY TRACT
 GASTROENTEROLOGY 2011;140:1472 1480 Comparability of Probable and Definite Autoimmune Hepatitis by International Diagnostic Scoring Criteria ALBERT J. CZAJA Division of Gastroenterology and Hepatology,
GASTROENTEROLOGY 2011;140:1472 1480 Comparability of Probable and Definite Autoimmune Hepatitis by International Diagnostic Scoring Criteria ALBERT J. CZAJA Division of Gastroenterology and Hepatology,
Autoimmune hepatitis: new paradigms in the pathogenesis, diagnosis, and management
 Hepatol Int (2010) 4:475 493 DOI 10.1007/s12072-010-9183-5 REVIEW ARTICLE Autoimmune hepatitis: new paradigms in the pathogenesis, diagnosis, and management Ye H. Oo Stefan G. Hubscher David H. Adams Received:
Hepatol Int (2010) 4:475 493 DOI 10.1007/s12072-010-9183-5 REVIEW ARTICLE Autoimmune hepatitis: new paradigms in the pathogenesis, diagnosis, and management Ye H. Oo Stefan G. Hubscher David H. Adams Received:
Chronic Hepatitis B Infection
 Chronic Hepatitis B Infection Mohssen Nassiri Toosi, MD Imam Khomeinin Hospital Tehran University of Medical Sciences Chronic Hepatitis B Infection Virus : HBs Ag Positive Host Liver Health Chronic Hepatitis
Chronic Hepatitis B Infection Mohssen Nassiri Toosi, MD Imam Khomeinin Hospital Tehran University of Medical Sciences Chronic Hepatitis B Infection Virus : HBs Ag Positive Host Liver Health Chronic Hepatitis
Hellenic Association for the Study of the Liver Clinical Practice Guidelines: Autoimmune hepatitis
 SPECIAL ARTICLE Annals of Gastroenterology (2019) 32, 1-24 Hellenic Association for the Study of the Liver Clinical Practice Guidelines: Autoimmune hepatitis George N. Dalekos a,b, John Koskinas c, George
SPECIAL ARTICLE Annals of Gastroenterology (2019) 32, 1-24 Hellenic Association for the Study of the Liver Clinical Practice Guidelines: Autoimmune hepatitis George N. Dalekos a,b, John Koskinas c, George
Diagnosis and Management of PBC
 Diagnosis and Management of PBC Cynthia Levy, MD, FAASLD University of Miami Miller School of Medicine Miami, Florida 1 Primary Biliary Cholangitis (PBC) Chronic cholestatic liver disease Autoimmune in
Diagnosis and Management of PBC Cynthia Levy, MD, FAASLD University of Miami Miller School of Medicine Miami, Florida 1 Primary Biliary Cholangitis (PBC) Chronic cholestatic liver disease Autoimmune in
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Ulcerative Colitis Therapy. Faculty Disclosure. Acknowledgements 28/11/2013. Amy Morse November 30/13
 Ulcerative Colitis Therapy Amy Morse November 30/13 GI for GP s Jasper AB Faculty Disclosure Faculty: Amy Morse Relationships with commercial interests: Grants/Research Support: Therapeutic Fellowship
Ulcerative Colitis Therapy Amy Morse November 30/13 GI for GP s Jasper AB Faculty Disclosure Faculty: Amy Morse Relationships with commercial interests: Grants/Research Support: Therapeutic Fellowship
Moderately to severely active ulcerative colitis
 Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Post Transplant Immunosuppression: Consideration for Primary Care. Sameh Abul-Ezz, M.D., Dr.P.H.
 Post Transplant Immunosuppression: Consideration for Primary Care Sameh Abul-Ezz, M.D., Dr.P.H. Objectives Discuss the commonly used immunosuppressive medications and what you need to know to care for
Post Transplant Immunosuppression: Consideration for Primary Care Sameh Abul-Ezz, M.D., Dr.P.H. Objectives Discuss the commonly used immunosuppressive medications and what you need to know to care for
Hangzhou, 15 March Ulrich Beuers Department of Gastroenterology and Hepatology Academic Medical Center University of Amsterdam
 Clinical Aspects of Primary Biliary Cirrhosis Hangzhou, 15 March 2008 Ulrich Beuers Department of Gastroenterology and Hepatology Academic Medical Center University of Amsterdam Epidemiology of Primary
Clinical Aspects of Primary Biliary Cirrhosis Hangzhou, 15 March 2008 Ulrich Beuers Department of Gastroenterology and Hepatology Academic Medical Center University of Amsterdam Epidemiology of Primary
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
In 1993, the International Autoimmune Hepatitis Group
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:417 421 Validation and Modification of Simplified Diagnostic Criteria for Autoimmune Hepatitis in Children ELIZABETH MILETI,* PHILIP ROSENTHAL,*, and MARION
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:417 421 Validation and Modification of Simplified Diagnostic Criteria for Autoimmune Hepatitis in Children ELIZABETH MILETI,* PHILIP ROSENTHAL,*, and MARION
K For patients who have never been tested for HCV, it is. K It is suggested that HCV-infected patients not previously
 http://www.kidney-international.org & 2008 DIGO Guideline 4: Management of HCV-infected patients before and after kidney transplantation idney International (2008) 73 (Suppl 109), S53 S68; doi:10.1038/ki.2008.87
http://www.kidney-international.org & 2008 DIGO Guideline 4: Management of HCV-infected patients before and after kidney transplantation idney International (2008) 73 (Suppl 109), S53 S68; doi:10.1038/ki.2008.87
Transplantation in Australia and New Zealand
 Transplantation in Australia and New Zealand Matthew D. Jose MBBS (Adel), FRACP, FASN, PhD (Monash), AFRACMA Professor of Medicine, UTAS Renal Physician, Royal Hobart Hospital Overview CKD in Australia
Transplantation in Australia and New Zealand Matthew D. Jose MBBS (Adel), FRACP, FASN, PhD (Monash), AFRACMA Professor of Medicine, UTAS Renal Physician, Royal Hobart Hospital Overview CKD in Australia
Treatment options for autoimmune hepatitis: A systematic review of randomized controlled trials
 Treatment options for autoimmune hepatitis: A systematic review of randomized controlled trials Mieke M.H. Lamers 1, Martijn G.H. van Oijen 1, Martine Pronk 2, Joost P.H. Drenth 1, * 1 Department of Gastroenterology
Treatment options for autoimmune hepatitis: A systematic review of randomized controlled trials Mieke M.H. Lamers 1, Martijn G.H. van Oijen 1, Martine Pronk 2, Joost P.H. Drenth 1, * 1 Department of Gastroenterology
Pharmacy Prior Authorization
 Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization
 Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Autoimmune Hepatitis
 Autoimmune Hepatitis Robert H. Squires, Jr., MD Professor of Pediatrics Children s Hospital of Pittsburgh Northwest Pediatric Liver Disease Symposium April 11,12, 2008 Seattle, Washington Common Liver
Autoimmune Hepatitis Robert H. Squires, Jr., MD Professor of Pediatrics Children s Hospital of Pittsburgh Northwest Pediatric Liver Disease Symposium April 11,12, 2008 Seattle, Washington Common Liver
Update on Autoimmune Liver Disease. Role of Liver Biopsy in Autoimmune Hepatitis, PBC and PSC
 Update on Autoimmune Liver Disease Role of Liver Biopsy in Autoimmune Hepatitis, PBC and PSC Stefan Hübscher, School of Cancer Sciences, University of Birmingham Dept of Cellular Pathology, Queen Elizabeth
Update on Autoimmune Liver Disease Role of Liver Biopsy in Autoimmune Hepatitis, PBC and PSC Stefan Hübscher, School of Cancer Sciences, University of Birmingham Dept of Cellular Pathology, Queen Elizabeth
Case #1. Digital Slides 11/6/ year old woman presented with abnormal liver function tests. Liver Biopsy to r/o autoimmune hepatitis
 45 year old woman presented with abnormal liver function tests Liver Biopsy to r/o autoimmune hepatitis Further down. ANA 1: 160; ASMA 1:80 ANA 1: 160; ASMA 1:80 IgG = 14.5 g/l (upper normal range: 16)
45 year old woman presented with abnormal liver function tests Liver Biopsy to r/o autoimmune hepatitis Further down. ANA 1: 160; ASMA 1:80 ANA 1: 160; ASMA 1:80 IgG = 14.5 g/l (upper normal range: 16)
LIVER SPECIALTY CONFERENCE USCAP Maha Guindi, M.D. Clinical Professor of Pathology Cedars-Sinai Medical Center Los Angeles, CA
 LIVER SPECIALTY CONFERENCE USCAP 2016 Maha Guindi, M.D. Clinical Professor of Pathology Cedars-Sinai Medical Center Los Angeles, CA Nothing to disclose Case History 47-year-old male, long standing ileal
LIVER SPECIALTY CONFERENCE USCAP 2016 Maha Guindi, M.D. Clinical Professor of Pathology Cedars-Sinai Medical Center Los Angeles, CA Nothing to disclose Case History 47-year-old male, long standing ileal
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report
 Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Not All Patients With Liver Disease Have HCV Diagnosis and Management of Some Common Non HCV Liver Diseases
 Not All Patients With Liver Disease Have HCV Diagnosis and Management of Some Common Non HCV Liver Diseases Prevalence of Chronic Liver Disorders in the United States Nonalcoholic Fatty Liver Disorder
Not All Patients With Liver Disease Have HCV Diagnosis and Management of Some Common Non HCV Liver Diseases Prevalence of Chronic Liver Disorders in the United States Nonalcoholic Fatty Liver Disorder
AASLD PRACTICE GUIDELINES. Diagnosis and Management of Autoimmune Hepatitis. 1. Preamble. 2. Introduction
 AASLD PRACTICE GUIDELINES Diagnosis and Management of Autoimmune Hepatitis Michael P. Manns, 1 Albert J. Czaja, 2 James D. Gorham, 3 Edward L. Krawitt, 4 Giorgina Mieli-Vergani, 5 Diego Vergani, 6 and
AASLD PRACTICE GUIDELINES Diagnosis and Management of Autoimmune Hepatitis Michael P. Manns, 1 Albert J. Czaja, 2 James D. Gorham, 3 Edward L. Krawitt, 4 Giorgina Mieli-Vergani, 5 Diego Vergani, 6 and
Acute Graft-versus-Host Disease (agvhd) Udomsak Bunworasate Chulalongkorn University
 Udomsak Bunworasate Chulalongkorn University") Acute Graft-versus-Host Disease (agvhd) Udomsak Bunworasate Chulalongkorn University Graft-versus-Host Disease (GVHD) Background GVHD is an immunologic reaction of the donor immune cells (Graft) against
Acute Graft-versus-Host Disease (agvhd) Udomsak Bunworasate Chulalongkorn University Graft-versus-Host Disease (GVHD) Background GVHD is an immunologic reaction of the donor immune cells (Graft) against
September 12, 2015 Millie D. Long MD, MPH, FACG
 Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
British Society of Gastroenterology (BSG) guidelines for management of autoimmune hepatitis
 guidelines for management of autoimmune hepatitis") 1 Liver Unit, Sheffield Teaching Hospitals Foundation Trust, Sheffield, UK 2 Institute of Liver Studies, King s College Hospital NHS Foundation Trust, London, UK Correspondence to Dr Dermot Gleeson, P
1 Liver Unit, Sheffield Teaching Hospitals Foundation Trust, Sheffield, UK 2 Institute of Liver Studies, King s College Hospital NHS Foundation Trust, London, UK Correspondence to Dr Dermot Gleeson, P
Long term liver transplant management
 Long term liver transplant management Dr Bill Griffiths Cambridge Liver Unit Royal College of Physicians 5.7.17 Success of Liver Transplantation Current survival, 1 st elective transplant: 1 yr survival
Long term liver transplant management Dr Bill Griffiths Cambridge Liver Unit Royal College of Physicians 5.7.17 Success of Liver Transplantation Current survival, 1 st elective transplant: 1 yr survival
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need?
 Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk Fatty liver disease Is there fatty
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk Fatty liver disease Is there fatty
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Sarcoidosis Case. Robert P. Baughman Interstitial Lung Disease and Sarcoidosis Clinic University of Cincinnati, USA. WASOG: educational material
 Sarcoidosis Case Robert P. Baughman Interstitial Lung Disease and Sarcoidosis Clinic University of Cincinnati, USA WASOG: educational material Sarcoidosis Case patient is a Caucasian male age 46 was diagnosed
Sarcoidosis Case Robert P. Baughman Interstitial Lung Disease and Sarcoidosis Clinic University of Cincinnati, USA WASOG: educational material Sarcoidosis Case patient is a Caucasian male age 46 was diagnosed
Drug-induced immune-mediated liver injury is. Drug-Induced Autoimmune Hepatitis: Clinical Characteristics and Prognosis
 Drug-Induced Autoimmune Hepatitis: Clinical Characteristics and Prognosis Einar Björnsson, 1,2 Jayant Talwalkar, 2 Sombat Treeprasertsuk, 2 Patrick S. Kamath, 2 Naoki Takahashi, 3 Schuyler Sanderson, 4
Drug-Induced Autoimmune Hepatitis: Clinical Characteristics and Prognosis Einar Björnsson, 1,2 Jayant Talwalkar, 2 Sombat Treeprasertsuk, 2 Patrick S. Kamath, 2 Naoki Takahashi, 3 Schuyler Sanderson, 4
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol
 Josep M. Campistol") Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Doncaster & Bassetlaw Medicines Formulary
 Doncaster & Bassetlaw Medicines Formulary Section 1.5 Chronic Bowel Disorders (including IBD) Aminosalicylates: Mesalazine 400mg and 800mg MR Tablets (Octasa) Mesalazine 1.2g MR Tablets (Mezavant XL) Mesalazine
Doncaster & Bassetlaw Medicines Formulary Section 1.5 Chronic Bowel Disorders (including IBD) Aminosalicylates: Mesalazine 400mg and 800mg MR Tablets (Octasa) Mesalazine 1.2g MR Tablets (Mezavant XL) Mesalazine
TREATMENT OF ANCA-ASSOCIATED VASCULITIS
 TREATMENT OF ANCA-ASSOCIATED VASCULITIS Loïc Guillevin Hôpital Cochin, Université Paris Descartes Cours DU, 11 mars 2016 1 Disclosure of interest regarding this presentation Roche has provided, in part,
TREATMENT OF ANCA-ASSOCIATED VASCULITIS Loïc Guillevin Hôpital Cochin, Université Paris Descartes Cours DU, 11 mars 2016 1 Disclosure of interest regarding this presentation Roche has provided, in part,
HCV care after cure. This program is supported by educational grants from
 HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Autoimmune liver diseases
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Autoimmune liver diseases Harrison s Principles of Internal Medicine 18-19 Ed. 2012 e seguenti Chronic hepatitis classification by cause
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Autoimmune liver diseases Harrison s Principles of Internal Medicine 18-19 Ed. 2012 e seguenti Chronic hepatitis classification by cause
Pediatric Primary Sclerosing Cholangitis and Potential Therapies
 Pediatric Primary Sclerosing Cholangitis and Potential Therapies Philip Rosenthal, M.D. Professor of Pediatrics & Surgery University of California, San Francisco DISCLOSURE I have the following financial
Pediatric Primary Sclerosing Cholangitis and Potential Therapies Philip Rosenthal, M.D. Professor of Pediatrics & Surgery University of California, San Francisco DISCLOSURE I have the following financial