EOSINOPHLIC LUNG DISEASES
|
|
|
- Augustus Maurice Perry
- 6 years ago
- Views:
Transcription
1 EOSINOPHLIC LUNG DISEASES
2 A wide spectrum of infiltrative lung diseases characterized by infiltration of lung parenchyma with eosinophils and/or peripheral blood eosinophilia.
3 How is the diagnosis made? Clinical and radiological features along with laboratory investigations : BAL and peripheral blood eosinophilia. BAL <2% eosinophils - normal 2-25% - non specific conditions >25% - IAEP >40% - ICEP Peripheral blood eosinophilia > 1000/mm 3 (>1500/mm 3 )
4 Classification Eosinophilic Lung Diseases of Undetermined Cause : - ICES, IAES - Chrug-strauss syndrome, IHES. Eosinophilic Lung Diseases of Determined Cause : - TPE, Loffler s syndrome, other parasites. - ABPA, Bronchocentric Granulomaosis, other fungi. - Drugs/ Toxins/ Radiation. Miscellaneous : - Asthma, Eosinophilic bronchiis, IPF, Sarcoidosis, Lung transplantation, Prarneoplastic eosinophilic pneumonia.
5 ICEP -F > M years. - H/o of asthma / atopy / chronic rhinitis or sinusitis. - Non smokers.
6 Clinical Features Mean interval between onset of symptoms and diagnosis is 4 months - Cough ( dry, later on productive ). - Dyspnoea. - Chest pain. - Fatigue, malaise, fever, night sweats, weight loss. - Wheeze / Crackles.
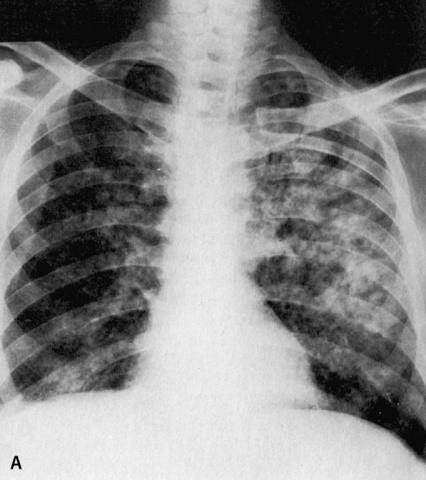
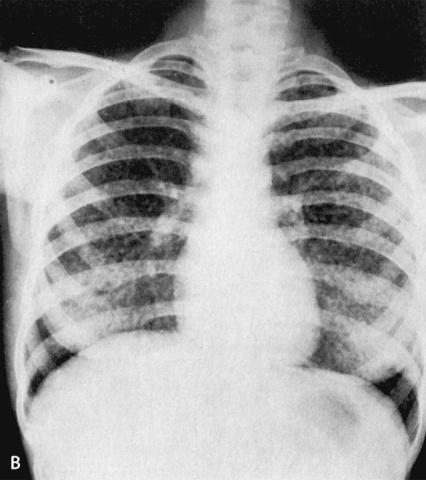
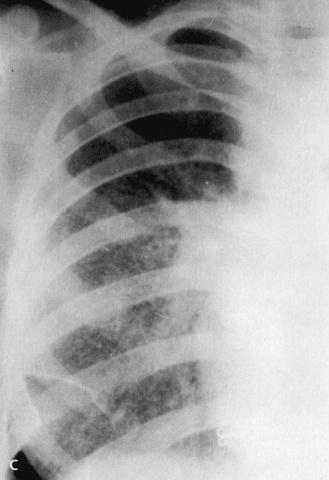
7 Laboratory Investigations CXR - B/l non migratory peripheral opacities. - Photographic negative of pulmonary edema (25%). - Ground glass to consolidation. HRCT - B/l peripheral alveolar opacities. - Septal thickening/ atelectasis / small pleural effusions / mediastinal lymphadenopathy
8 BLOOD TLC, ESR. Total IGE >1000 IU/ml. AEC >5500/mm 3. BAL >40% eosinophils. PFT obstructive / restrictive.
9 Treatment Mainstay of treatment is Corticosteroids. 1 mg/kg/d for 2 weeks, then tapering over 4 6 weeks. Symptoms improve in 2 weeks and CXR clear in 2 months. Relapse rate is 80% after stopping of treatment. Relapse respond well to Corticosteroids resumption.
10 IAEP - M > F years. - H/o of respiratory exposure to dust, initiation of tobacco smoke
11 Clinical Features - Acute onset ( <7 days or 7 31 days ). - Cough. - Dyspnoea. - Chest pain, myalgia, fever. - Tachypnoea. - Tachycardia. - Crackles.
12 Laboratory Investigations 1.BLOOD - Lack of pulmonary blood eosinophilia. TLC, ESR. IgE > 1000 IU/ml. 2.BAL - 25% EOSINOPHILS ( %). 3.PFT Restrictive. Severe hypoxemia ( PaO2/FiO2 < 300 mmhg)/( PaO2/FiO2 < 200 mmhg ).
13 CXR - B/l alveolar and interstitial peripheral opacities. - Ground glass and micronodular. CECT - B/l alveolar and interstitial opacities. - Poorly defined nodules along bronchovascular. prominence - Septal thickening.
14 Treatment Role of corticosteroids is unconfirmed, may recover spontaneously. Initial bolus dose of Methyl Predinosolone mg 6 hrly then oral Predinosolone mg/d for 2 4 weeks, tapering over few weeks. Complete recovery, no relapse
15 Diagnostic criteria for IAEP 1. Acute onset. 2. B/l diffuse infiltrates on CXR. 3. PaO2 < 60 mmhg or SpO2 < 90% or PaO2/FiO2 < 300 mmhg. 4. BAL > 25% Eosinophils. 5. Absence of any determined cause.
16 Chrug - Strauss Syndrome Eosinophilic granulomatous inflammation involving the respiratory tract and necrotizing vasculitis of medium and small sized vessels along with asthmas and peripheral blood eosinophilia. -M > F years. - H/o of asthma (severe and corticosteroid dependant ) / rhinitis / relapsing paranasal sinusitis / polyps.
17 Clinical Features - Cough, dyspnoea, wheezing - Weight loss, myalgia, arthralgia - Extra pulmonary manifestations Cardiac M.C. cause of death CNS, GIT, Renal, Skin
18 Laboratory Investigations 1. BLOOD TLC, ESR. IGE > 1000 IU /ml. AEC > 1500/mm 3. p-anca. 2. BAL > 60 % eosinophils. 3. PFT early stage - obstructive. later stages - restrictive.
19 CXR - Normal or b/l peripheral migratory and transient pulmonary infiltrates. - B/l non- cavitating nodular opacities. HRCT - B/l peripheral migratory & transient pulmonary infiltrates. - Septal thickening. - Hilar or mediastinal lymphadenopathy. - Bronchial wall dilation.

20 B/l pulmonary infiltrates

21 B/l ground glass opacities
22 Diagnostic Criteria 1. H/o Asthma. 2. PBE > 1500 / mm Systemic vasculitis > 2 extra pulmonary organs. 4. p-anca. 5. Skin, nerve, muscle biopsy ( Lung biopsy is not recommended )
23 Treatment Corticosteroids - Initial bolus dose of methyl Prednisolone - 15 mg/kg/d for 3 days. - Than 1 mg/kg/d for several weeks with tapering over 1 year. FIVE FACTOR SCORE ( poor prognosis ) - Renal, cardiac, CNS, GIT, mild to moderate relapses Use of following drugs is recommended - Cyclophosphamide, Azathioprine, s.c. IFN- gamma, CyclosporineA
24 IHS Heterogeneous group of disorder characterized by multiorgan eosinophilic infiltration an end organ damage without any underlying cause. -M > F years.
25 Clinical Features - Cough, dyspnoea, fever, malaise, fatigue. - Extra pulmonary manifestations Cardiac, CNS, Skin.
26 Laboratory Investigations 1. BLOOD - TLC, ESR, IgE. 2. BAL - Mild. 3. PFT - Restrictive. AEC > 1500/mm3 for at least 6 months or death before 6 months. LAP, Serum vit B 12, Hypergammaglobinemia, ILK.
27 CXR - B/l transient pulmonary infiltrates. CECT - B/l transient pulmonary infiltrates. - Small nodules.
28 Diagnostic Criteria 1. Severe PBE (> 1500/mm 3 ) for at least 6 months or death before 6 months. 2. Absence of any other cause. 3. Multi organ dysfunction.
29 Treatment 1. Eosinophilia without endorgan dysfunction observation. 2. With organ damage - Prednisolone( 1 mg/kg/d ) for weeks than tapering over 1 year 3. If diseases progresses - Add Hydroxyurea ( g/d ) 4 Refractory causes : IFN alpha, Imatinib, Vincristine, Anti-IL5monoclonal Ab.
30 Tropical Pulmonary Eosinophilia - Caused by filarial parasites - Wucheria Bronchofti and Brugia Malayi. - Hypersensitivity reaction to Microfilarial antigens. -M > F years.
31 Clinical Features - Dry cough without dyspnoea (90%). - Dry cough with dyspnoea (45%). - Mucopurulent sputum (40%). - Fever, anorexia, weight loss. - Wheeze.
32 Laboratory Investigations 1.BLOOD - TLC, ESR,IGE. - AEC > 3000/mm 3. - Absence of microfilaria in blood and sputum. - Specific filarial IgE, IgG. 2.BAL - Eosinophils. 3. PFT - Obstructive ( when presents in < 1 month ). -Mixed.
33 CXR - Normal ( 20% ). - B/l disseminated reticulonodular opacities in MZ / LZ. - Hilar prominence, miliary mottling. CECT - B/l reticulonodular opacities. - Bronchiectasis, air trapping, calcification.
34 B/l diffuse bronchopneumonia B/l diffuse miliary nodules
35 Reticulonodular Pattern
36 Diagnosis 1. H/o residing or visit to an endemic area. 2. Eosinophilia > 3000/mm Elevated IgE. 4. Specific IgE, IgG Ab. 5. Absence of microfilaria in blood and sputum. 6. Response to DEC.
37 Treatment -Diethylcarbazine mg/kg/day for 3 weeks. - Corticosteroids and Ivermectin are tried in chronic variant of disease. - If untreated, disease may resolve spontaneously or may lead to development of interstitial lung disease
38 Loffler s Syndrome - Immune response to Ascaris larva during migration of larva through lungs. - Other parasites and drugs are also responsible. - No cause in 1/3 patients. - All age groups. -M = F.
39 Clinical Features - Cough, mostly non-productive. - Dyspnoea. - Low grade fever. - Anorexia, malaise, weight loss. - Crackles.
40 Laboratory Investigations 1. BLOOD - TLC, ESR, IgE. - AEC > 3000 mm/ SPUTUM - Eosinophils, larva during pneumonic stage, charcot - leyden crystals. 3. STOOL - Ova, parasites ( not seen up to 8 weeks after onset of respiratory symptoms. 4. PFT - Restrictive.
41 CXR - B/L transient migratory peripheral infiltrates. - May coalesce to form areas of consolidation. CECT - B/l transient migratory peripheral infiltrates.
42 Treatment - Search for the etiological cause - parasites / drugs. - Mild cases resolve spontaneously in 1 2 weeks. - Severe cases Corticosteroids 1 mg/kg/day. - To prevent late GIT symptoms : - Albendazole 400 mg single oral dose. - Mebendazole 500 mg single oral dose. - Follow up after 3 months is needed.
43 ABPA - Immune response of the bronchi and lung parenchyma in response to Ag of Aspergillus colonizing the airways. -M = F years ( any age may be affected ). - H/o of asthma / atopy. - Family occurrence of ABPA is a rarity.
44 Clinical Features - Cough with sputum. - Dyspnoea. - Fever, lethargy, malaise. - Expectoration of golden brown plugs. - Wheeze / Crackles. - Signs of clubbing, cyanosis, cor-pulmonale, RF.
45 Major Criteria 1. H/o asthma. 2. Immediate skin reaction to Ag ( type 1). 3. AEC > 2000/mm IgE > 1000 IU/ ml. 5. Serum precipitins against Aspergillus fumigatus. 6. Specific IgE and IgG against Aspergillus fumigatus. 7. Transient pulmonary infiltrates on CXR. 8. Central bronchiectasis with normal tapering of distal bronchi.
46 Minor Criteria 1. Delayed skin reaction to Ag ( type 3 ). 2. Brownish plugs in sputum. 3. Sputum culture positive for Aspergillus fumigatus.
47 Minimum Essential Criteria 1. H/o asthma. 2. Immediate skin reaction to Aspergillus fumigatus. 3. IgE. 4. Central bronchiectasis. 5. Specifis IgE and IgG against Aspergillus fumigatus.
48 STAGING 1. Acute. 2. Remission. 3. Exacerbation. 4. Steroid dependant. 5. Fibrotic lung disease.
49 Laboratory Investigations 1. BLOOD - TLC, ESR, IgE. - AEC > 1000/mm 3. - Serum precipitins against A.F. 2. SPUTUM - Eosinophils. - Positive culture for A.F. 3. SKIN TESTS - Positive immediate test. 4. PFT - Restrictive / obstructive / mixed.
50 CXR -. TRANSIENT CHANGES - Fleeting shadows, Tram-line shadows. - Tooth-paste and Gloved finger shadows. - Lobar/segmental collapse, consolidation. PERMANENT CHANGES - Central bronchiectasis. - Parallel line shadows, Ring shadows. - Fibrosis, honeycombing, cavities. CECT- Central bronchiectasis.

51 Large lobulated perihilar shadows.


52 Lobulated masses contained in the cystic cavities extending to the central hilum.
53 Treatment Corticosteroids Acute / Exacerbation mg/kg/day for 2 weeks, then 0.5 mg/kg alternate day for 2-3 months with gradual tapering. Steroid dependant mg alternate day. Fibrotic - low dose daily or alternate day. Itraconazole Reduces dose of CS, decrease rate of exacerbations but long term effect is not known.
54 Drugs / Radaition - Develop progressively. - Cough, dyspnoea, fever, cutaneous rashes ( drugs ). - B/L pulmonary infiltrates in CXR. - AEC > 1000/mm 3 ; BAL > 40%. - Resolution of infiltrates after stopping of drug, steroid hasten recovery in severely ill. - Corticosteroids are mainstay if treatment in radiation induced disease.
55 All the best..
Disease spectrum. IPA Invasive pulmonary aspergillosis
 Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Eosinophilic lung diseases
 Eosinophilic lung diseases Chai Gin Tsen Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital The eyes do not see what the mind does not know Not very common A high index of suspicion
Eosinophilic lung diseases Chai Gin Tsen Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital The eyes do not see what the mind does not know Not very common A high index of suspicion
Atopic Pulmonary Disease: Findings on Thoracic Imaging
 July 2003 Atopic Pulmonary Disease: Findings on Thoracic Imaging Rebecca G. Breslow Harvard Medical School Year IV Churg-Strauss Syndrome Hypersensitivity Pneumonitis Asthma Atopic Pulmonary Disease Allergic
July 2003 Atopic Pulmonary Disease: Findings on Thoracic Imaging Rebecca G. Breslow Harvard Medical School Year IV Churg-Strauss Syndrome Hypersensitivity Pneumonitis Asthma Atopic Pulmonary Disease Allergic
Imaging Spectrum of Allergic Lung Disease: Hypersensitivity Reactions on the Lung Parenchyma
 Imaging Spectrum of Allergic Lung Disease: Hypersensitivity Reactions on the Lung Parenchyma Moon Sung Kim 1, Ki-Nam Lee 1, Won Jin Choi 1, Bo Ra Kim 1, Eun-Ju Kang 1 1 Department of Radiology, Dong-A
Imaging Spectrum of Allergic Lung Disease: Hypersensitivity Reactions on the Lung Parenchyma Moon Sung Kim 1, Ki-Nam Lee 1, Won Jin Choi 1, Bo Ra Kim 1, Eun-Ju Kang 1 1 Department of Radiology, Dong-A
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
HYPERSENSITIVITY PNEUMONITIS
 HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
INTERSTITIAL LUNG DISEASE Dr. Zulqarnain Ashraf
 Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Professor Rob Miller
 BHIVA AUTUMN CONFERENCE 2013 Including CHIVA Parallel Sessions Professor Rob Miller University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Prof Rob Miller
BHIVA AUTUMN CONFERENCE 2013 Including CHIVA Parallel Sessions Professor Rob Miller University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Prof Rob Miller
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
Dr.kassim.m.sultan F.R.C.P
 Dr.kassim.m.sultan F.R.C.P inflammatory disorder of the lung, involving alveolar walls and terminal airways, that is induced, in a susceptible host, by repeated inhalation of a variety of organic agents.
Dr.kassim.m.sultan F.R.C.P inflammatory disorder of the lung, involving alveolar walls and terminal airways, that is induced, in a susceptible host, by repeated inhalation of a variety of organic agents.
4/17/2010 C ini n ca c l a Ev E a v l a ua u t a ion o n of o ILD U dat a e t e i n I LDs
 Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Manish Powari Regional Training Day 10/12/2014
 Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Interesting cases in fungal asthma
 Interesting cases in fungal asthma Ritesh Agarwal MD, DM Professor of Pulmonary Medicine Postgraduate Institute of Medical Education and Research Chandigarh, India Fungal asthma Broadly defined as the
Interesting cases in fungal asthma Ritesh Agarwal MD, DM Professor of Pulmonary Medicine Postgraduate Institute of Medical Education and Research Chandigarh, India Fungal asthma Broadly defined as the
The Ghost in the Closet. Allergic Sino-Bronchopulmonary Aspergillosis Without Bronchial Asthma: A Case Report & Review of the Subject
 Proceeding S.Z.P.G.M.I. Vol: 24(1): pp. 55-59 2010. The Ghost in the Closet. Allergic Sino-Bronchopulmonary Aspergillosis Without Bronchial Asthma: A Case Report & Review of the Subject Department of Pulmonology,
Proceeding S.Z.P.G.M.I. Vol: 24(1): pp. 55-59 2010. The Ghost in the Closet. Allergic Sino-Bronchopulmonary Aspergillosis Without Bronchial Asthma: A Case Report & Review of the Subject Department of Pulmonology,
Recent advances in diagnosis and management of ABPA. Arindam SR(Pulmonary Medicine)
") Recent advances in diagnosis and management of ABPA Arindam SR(Pulmonary Medicine) Conventional diagnostic criteria for ABPA Primary Episodic bronchial obstruction (asthma) Peripheral blood eosinophilia
Recent advances in diagnosis and management of ABPA Arindam SR(Pulmonary Medicine) Conventional diagnostic criteria for ABPA Primary Episodic bronchial obstruction (asthma) Peripheral blood eosinophilia
Imaging Small Airways Diseases: Not Just Air trapping. Eric J. Stern MD University of Washington
 Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Interstitial Lung Disease. SS Visser, Lung Unit, UP.
 Interstitial Lung Disease SS Visser, Lung Unit, UP. ILD - Definition Heterogenous group of diseases with involvement of alveolar walls and peri- alveolar tissue -nonmalignant, non-infective. ± 180 diseases
Interstitial Lung Disease SS Visser, Lung Unit, UP. ILD - Definition Heterogenous group of diseases with involvement of alveolar walls and peri- alveolar tissue -nonmalignant, non-infective. ± 180 diseases
Eosinophilic lung diseases - what the radiologist needs to know
 Eosinophilic lung diseases - what the radiologist needs to know Poster No.: C-0803 Congress: ECR 2014 Type: Authors: Keywords: DOI: Educational Exhibit E.-M. Heursen, R. Reina Cubero, F. Japon Sola; Cádiz/ES
Eosinophilic lung diseases - what the radiologist needs to know Poster No.: C-0803 Congress: ECR 2014 Type: Authors: Keywords: DOI: Educational Exhibit E.-M. Heursen, R. Reina Cubero, F. Japon Sola; Cádiz/ES
Allergic Bronchopulmonary Aspergillosis: An Unusual Complication of Bronchial Asthma
 Allergic Bronchopulmonary Aspergillosis: An Unusual Complication of Bronchial Asthma Pages with reference to book, From 329 To 331 S. Fayyaz Hussain, Javaid A. Khan ( Department of Medicine, The Aga Khan
Allergic Bronchopulmonary Aspergillosis: An Unusual Complication of Bronchial Asthma Pages with reference to book, From 329 To 331 S. Fayyaz Hussain, Javaid A. Khan ( Department of Medicine, The Aga Khan
Differential diagnosis
 Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
The Pathologic Manifestations of Small Airway Disease. Samuel A. Yousem, MD. Small Airway Disease (SAD) SAD
 SAD") The Pathologic Manifestations of Small Airway Disease Samuel A. Yousem, MD Small Airway Disease (SAD) A clinicopathologic syndrome reflecting a CHRONIC inflammatory and cicatricial process primarily affecting
The Pathologic Manifestations of Small Airway Disease Samuel A. Yousem, MD Small Airway Disease (SAD) A clinicopathologic syndrome reflecting a CHRONIC inflammatory and cicatricial process primarily affecting
Outline Definition of Terms: Lexicon. Traction Bronchiectasis
 HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
Eosinophilia Associated Lung Diseases
 Eosinophilia Associated Lung Diseases Stephen P. Peters, MD, PhD, FAAAAI, FACP, FCCP, FCPP Thomas H. Davis Chair in Pulmonary Medicine Chief, Section on Pulmonary Critical Care, Allergy & Immunologic Diseases
Eosinophilia Associated Lung Diseases Stephen P. Peters, MD, PhD, FAAAAI, FACP, FCCP, FCPP Thomas H. Davis Chair in Pulmonary Medicine Chief, Section on Pulmonary Critical Care, Allergy & Immunologic Diseases
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
HRCT in Diffuse Interstitial Lung Disease Steps in High Resolution CT Diagnosis. Where are the lymphatics? Anatomic distribution
 Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c)
 Diffuse bronchiectasis b) Cystic fibrosis c)") Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
The Respiratory System
 The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
Eosinophils and effusion: a clinical conundrum
 Ruth Sobala, Kevin Conroy, Hilary Tedd, Salem Elarbi kevin.peter.conroy@gmail.com Respiratory Dept, Queen Elizabeth Hospital, Gateshead, UK. Eosinophils and effusion: a clinical conundrum Case report A
Ruth Sobala, Kevin Conroy, Hilary Tedd, Salem Elarbi kevin.peter.conroy@gmail.com Respiratory Dept, Queen Elizabeth Hospital, Gateshead, UK. Eosinophils and effusion: a clinical conundrum Case report A
SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW
 SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW Lung disease can be a serious complication of scleroderma. The two most common types of lung disease in patients with scleroderma are interstitial
SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW Lung disease can be a serious complication of scleroderma. The two most common types of lung disease in patients with scleroderma are interstitial
Radiological Imaging of Drug-Induced Pulmonary Lesions
 Review Article imedpub Journals www.imedpub.com Journal of Clinical Radiology and Case Reports Radiological Imaging of Drug-Induced Pulmonary Lesions D souza M *, Rajiah P, Khan A and Irion K Department
Review Article imedpub Journals www.imedpub.com Journal of Clinical Radiology and Case Reports Radiological Imaging of Drug-Induced Pulmonary Lesions D souza M *, Rajiah P, Khan A and Irion K Department
Case 1: Question. 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule
 HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
Diseases of the Lung and Respiratory Tract, Part I. William Bligh-Glover M.D. Department of Anatomy, CWRU
 Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
LUNG DISEASES DUE TO ORGANIC&INORGANIC DUSTS. Dr.kassim.m.sultan F.R.C.P
 LUNG DISEASES DUE TO ORGANIC&INORGANIC DUSTS Dr.kassim.m.sultan F.R.C.P efinition of hypersensitivity pneumonitis(extrinsic allergic alveolitis): Inflammatory disorder of the lung, involving alveolar walls
LUNG DISEASES DUE TO ORGANIC&INORGANIC DUSTS Dr.kassim.m.sultan F.R.C.P efinition of hypersensitivity pneumonitis(extrinsic allergic alveolitis): Inflammatory disorder of the lung, involving alveolar walls
ASTHMATIC PULMONARY EOSINOPHILIA
 ASTHMATIC PULMONARY EOSINOPHILIA Pages with reference to book, From 300 To 302 Mohammad Zaman ( Department of Pulmonary Medicine, Pakistan Institute of Medical Sciences, Islamabad. ) Asthmatic pulmonary
ASTHMATIC PULMONARY EOSINOPHILIA Pages with reference to book, From 300 To 302 Mohammad Zaman ( Department of Pulmonary Medicine, Pakistan Institute of Medical Sciences, Islamabad. ) Asthmatic pulmonary
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Idiopathic Chronic Eosinophilic Pneumonia, a Rare Differential Diagnosis
 Human Journals Case Report June 2018 Vol.:9, Issue: 4 All rights are reserved by Vladimir Macavei et al. Idiopathic Chronic Eosinophilic Pneumonia, a Rare Differential Diagnosis Keywords: Airway diseases;
Human Journals Case Report June 2018 Vol.:9, Issue: 4 All rights are reserved by Vladimir Macavei et al. Idiopathic Chronic Eosinophilic Pneumonia, a Rare Differential Diagnosis Keywords: Airway diseases;
Pulmonary Aspergillosis
 May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
Bronchiectasis: An Imaging Approach
 Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Allergic aspergillosis of the respiratory tract
 EUROPEAN RESPIRATORY UPDATE ALLERGIC RESPIRATORY ASPERGILLOSIS Allergic aspergillosis of the respiratory tract Ashok Shah 1 and Chandramani Panjabi 2 Affiliations: 1 Dept of Respiratory Medicine, Vallabhbhai
EUROPEAN RESPIRATORY UPDATE ALLERGIC RESPIRATORY ASPERGILLOSIS Allergic aspergillosis of the respiratory tract Ashok Shah 1 and Chandramani Panjabi 2 Affiliations: 1 Dept of Respiratory Medicine, Vallabhbhai
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis
 Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
and localized ground glass opacities, or bronchiolar focal or multifocal micronodules;
 E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
When to suspect Wegener Granulomatosis: A radiologic review
 When to suspect Wegener Granulomatosis: A radiologic review Poster No.: P-0038 Congress: ESTI 2015 Type: Educational Poster Authors: A. Tilve Gómez, R. Díez Bandera, P. Rodríguez Fernández, M. Garcia Vazquez-Noguerol,
When to suspect Wegener Granulomatosis: A radiologic review Poster No.: P-0038 Congress: ESTI 2015 Type: Educational Poster Authors: A. Tilve Gómez, R. Díez Bandera, P. Rodríguez Fernández, M. Garcia Vazquez-Noguerol,
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Case Presentations in ILD. Harold R. Collard, MD Department of Medicine University of California San Francisco
 Case Presentations in ILD Harold R. Collard, MD Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Definition/Classification High-resolution CT scan Multidisciplinary
Case Presentations in ILD Harold R. Collard, MD Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Definition/Classification High-resolution CT scan Multidisciplinary
RESPIRATORY BLOCK. Bronchial Asthma. Dr. Maha Arafah Department of Pathology KSU
 RESPIRATORY BLOCK Bronchial Asthma Dr. Maha Arafah Department of Pathology KSU marafah@ksu.edu.sa Jan 2018 Objectives Define asthma (BA) Know the two types of asthma 1. Extrinsic or atopic allergic 2.
RESPIRATORY BLOCK Bronchial Asthma Dr. Maha Arafah Department of Pathology KSU marafah@ksu.edu.sa Jan 2018 Objectives Define asthma (BA) Know the two types of asthma 1. Extrinsic or atopic allergic 2.
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
5/9/2015. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. No, I am not a pulmonologist! Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates
 and Updates") Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates Maria Elena Vega, M.D Assistant Professor of Medicine Lewis Katz School of Medicine at Temple University Nothing to
Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates Maria Elena Vega, M.D Assistant Professor of Medicine Lewis Katz School of Medicine at Temple University Nothing to
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia. Nitra and the Gangs.
 Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
DIAGNOSTIC APPROACH MILIARY OPACITIES.
 DIAGNOSTIC APPROACH TO MILIARY OPACITIES. 1 INTRODUCTION The term miliary derives from the radiographic picture of diffuse, discrete, nodular shadows about the size of a millet seed (~2mm). 2 CHEST X-RAY
DIAGNOSTIC APPROACH TO MILIARY OPACITIES. 1 INTRODUCTION The term miliary derives from the radiographic picture of diffuse, discrete, nodular shadows about the size of a millet seed (~2mm). 2 CHEST X-RAY
Restrictive lung diseases
 Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Eosinophilic Lung Disease
 COMMENTARY Eosinophilic Lung Disease Bhupinder Mann Respiratory department, West Middlesex University Hospital, Middlesex, London, England. Abstract: Eosinophilic lung diseases represent a group of disorders
COMMENTARY Eosinophilic Lung Disease Bhupinder Mann Respiratory department, West Middlesex University Hospital, Middlesex, London, England. Abstract: Eosinophilic lung diseases represent a group of disorders
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Update on Biologicals for ABPA and Asthma
 Update on Biologicals for ABPA and Asthma 5 th Advances Against Aspergillosis Istanbul 27 Jan 2012 Richard B. Moss MD Professor of Pediatrics Stanford University Palo Alto CA USA Disease of chronic airway
Update on Biologicals for ABPA and Asthma 5 th Advances Against Aspergillosis Istanbul 27 Jan 2012 Richard B. Moss MD Professor of Pediatrics Stanford University Palo Alto CA USA Disease of chronic airway
UIP OR NOT UIP PATTERN: THAT IS NOT THE ONLY QUESTION!
 UIP OR NOT UIP PATTERN: THAT IS NOT THE ONLY QUESTION! STÉPHANE JOUNEAU 11 JULY 2014 Respiratory Medicine Department, Pontchaillou Hospital, Rennes, France CASE OVERVIEW This case highlights how a usual
UIP OR NOT UIP PATTERN: THAT IS NOT THE ONLY QUESTION! STÉPHANE JOUNEAU 11 JULY 2014 Respiratory Medicine Department, Pontchaillou Hospital, Rennes, France CASE OVERVIEW This case highlights how a usual
Respiratory diseases in Ostrołęka County
 Respiratory diseases in Ostrołęka County 4400 persons underwent examination 950 persons were given referrals to more detailed investigation 600 persons were examined so far The results of more detailed
Respiratory diseases in Ostrołęka County 4400 persons underwent examination 950 persons were given referrals to more detailed investigation 600 persons were examined so far The results of more detailed
Prof Neil Barnes. Respiratory and General Medicine London Chest Hospital and The Royal London Hospital
 Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Diagnostic challenges in IPF
 Medicine, Nursing and Health Sciences Diagnostic challenges in IPF Dr Ian Glaspole Central and Eastern Clinical School, Alfred Hospital and Monash University March 2015 Disclosures Consultancy fees from
Medicine, Nursing and Health Sciences Diagnostic challenges in IPF Dr Ian Glaspole Central and Eastern Clinical School, Alfred Hospital and Monash University March 2015 Disclosures Consultancy fees from
Bronkhorst colloquium Interstitiële longziekten. Katrien Grünberg, klinisch patholoog
 Bronkhorst colloquium 2013-2014 Interstitiële longziekten De pathologie achter de CT Katrien Grünberg, klinisch patholoog K.grunberg@vumc.nl Preparing: introduction and 3 cases The introduction on microscopic
Bronkhorst colloquium 2013-2014 Interstitiële longziekten De pathologie achter de CT Katrien Grünberg, klinisch patholoog K.grunberg@vumc.nl Preparing: introduction and 3 cases The introduction on microscopic
REFERRAL GUIDELINES RESPIRATORY
 REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
REFERRAL GUIDELINES RESPIRATORY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Bronchiolar disorders: Current perspective on diagnosis & management. Puneet Malhotra Senior Resident, Dept. of Pulmonary Medicine, PGIMER
 Bronchiolar disorders: Current perspective on diagnosis & management Puneet Malhotra Senior Resident, Dept. of Pulmonary Medicine, PGIMER Anatomic considerations Classification Diagnostic approach Specific
Bronchiolar disorders: Current perspective on diagnosis & management Puneet Malhotra Senior Resident, Dept. of Pulmonary Medicine, PGIMER Anatomic considerations Classification Diagnostic approach Specific
Radiation Pneumonitis Joseph Junewick, MD FACR
 Radiation Pneumonitis Joseph Junewick, MD FACR 03/19/2010 History 16 year old with history of relapsed stage IV-A Hodgkin disease. Prior pulmonary involvement was irradiated. Diagnosis Radiation Pneumonitis
Radiation Pneumonitis Joseph Junewick, MD FACR 03/19/2010 History 16 year old with history of relapsed stage IV-A Hodgkin disease. Prior pulmonary involvement was irradiated. Diagnosis Radiation Pneumonitis
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Idiopathic Pulmonary Fibrosis Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Idiopathic Pulmonary Fibrosis (Esbriet /pirfenidone, Ofev /nintedanib)
Idiopathic Pulmonary Fibrosis Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Idiopathic Pulmonary Fibrosis (Esbriet /pirfenidone, Ofev /nintedanib)
September 2014 Imaging Case of the Month. Michael B. Gotway, MD. Department of Radiology Mayo Clinic Arizona Scottsdale, AZ
 September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School, University of Crete Prague, June 2014
 Hypersensitivity pneumonitis: Causes, clinical course, diagnosis and differential diagnosis, treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
Hypersensitivity pneumonitis: Causes, clinical course, diagnosis and differential diagnosis, treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
CT Diagnosis of Pulmonary Wegener s Granulomatosis: A Case Report and Review of Literature
 CASE REPORT JIACM 2008; 9(4): 321-5 CT Diagnosis of Pulmonary Wegener s Granulomatosis: A Case Report and Review of Literature Shibani Mehra*, Shailendra Aggarwal Abstract The diagnosis of Wegener s granulomatosis
CASE REPORT JIACM 2008; 9(4): 321-5 CT Diagnosis of Pulmonary Wegener s Granulomatosis: A Case Report and Review of Literature Shibani Mehra*, Shailendra Aggarwal Abstract The diagnosis of Wegener s granulomatosis
David E. Griffith, MD has the following disclosures to make:
 Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
An Image Repository for Chest CT
 An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
A Review of Interstitial Lung Diseases. Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco
 A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
HOSPITAL RECORD ABSTRACTION FORM
 HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: VERSION: A 10/23/2015 0a. Form Completion Date... / / 0b. Staff Code... 0c. Event ID: 0d. Event Date: / / Instructions: Answers are derived from the medical
HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: VERSION: A 10/23/2015 0a. Form Completion Date... / / 0b. Staff Code... 0c. Event ID: 0d. Event Date: / / Instructions: Answers are derived from the medical
Role of Computed Tomography in Diagnosis of Diffuse Lung Diseases Chauhan Jayant 1*, Panchal Pankaj 2, Faruqui Tehzeeb 3
 ORIGINAL ARTICLE Role of Computed Tomography in Diagnosis of Diffuse Lung Diseases Chauhan Jayant 1*, Panchal Pankaj 2, Faruqui Tehzeeb 3 1 MD,DTCD,Additional Professor& HOD, 2,3 MBBS, 3 rd year resident
ORIGINAL ARTICLE Role of Computed Tomography in Diagnosis of Diffuse Lung Diseases Chauhan Jayant 1*, Panchal Pankaj 2, Faruqui Tehzeeb 3 1 MD,DTCD,Additional Professor& HOD, 2,3 MBBS, 3 rd year resident
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Chapter 16. Lung Abscess. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Liebow and Carrington's original classification of IIP
 Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Langerhans Cell Histiocytosis with Anterior Mediastinum, Pulmonary and Liver Involvement: CT Demonstration
 Chin J Radiol 2002; 27: 191-195 191 Langerhans Cell Histiocytosis with Anterior Mediastinum, Pulmonary and Liver Involvement: CT Demonstration SIU-CHEUNG CHAN 1 MUN-CHING WONG 1 SHIU-FENG HUANG 2 WAN-CHAK
Chin J Radiol 2002; 27: 191-195 191 Langerhans Cell Histiocytosis with Anterior Mediastinum, Pulmonary and Liver Involvement: CT Demonstration SIU-CHEUNG CHAN 1 MUN-CHING WONG 1 SHIU-FENG HUANG 2 WAN-CHAK
The Imaging Analysis of Pulmonary Sarcodiosis
 www.cancercellresearch.org ISSN: 2161-2609 Article The Imaging Analysis of Pulmonary Sarcodiosis Xin He, Chuanyu Zhang* Department of Radiology, Affiliated Hospital of Qingdao University, Qingdao, China
www.cancercellresearch.org ISSN: 2161-2609 Article The Imaging Analysis of Pulmonary Sarcodiosis Xin He, Chuanyu Zhang* Department of Radiology, Affiliated Hospital of Qingdao University, Qingdao, China
Pulmonary Sarcoidosis - Radiological Evaluation
 Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Allergic bronchopulmonary Aspergillosis mimicking as bilateral cavitatory pulmonary tuberculosis.
 INTERNATIONAL JOURNAL OF CURRENT RESEARCH IN BIOLOGY AND MEDICINE ISSN: 2455-944X www.darshanpublishers.com DOI:10.22192/ijcrbm Volume 3, Issue 3-2018 Original Research Article DOI: http://dx.doi.org/10.22192/ijcrbm.2018.03.03.004
INTERNATIONAL JOURNAL OF CURRENT RESEARCH IN BIOLOGY AND MEDICINE ISSN: 2455-944X www.darshanpublishers.com DOI:10.22192/ijcrbm Volume 3, Issue 3-2018 Original Research Article DOI: http://dx.doi.org/10.22192/ijcrbm.2018.03.03.004