For Those Who Lover Sputum: Bronchiectasis
|
|
|
- Myrtle Cook
- 6 years ago
- Views:
Transcription
1 For Those Who Lover Sputum: Bronchiectasis Douglas B. Hornick, MD Pulmonologist w/ an Infectious Attitude Division of Pulmonary/Critical Care & Occ Med Carver UI College of Medicine
2 Objectives Increase understanding of the general characteristics of non-cf Bronchiectasis Develop an approach to work-up & management Categorize & review heterogeneous causes Disclosure: No Conflicts of Interest
3 Key References McShane P, et al. Non CF Bronchiectasis Review. Am J Respir Crit Care Med 2013;188: Pasteur MC et al, BTS Guidelines for Non- CF Bronchiectasis Thorax 2010;65:i1-i58 Clinics in Chest Med, May 2013 Barker AF: NEJM 2003; 346: Ten Hacken NHT, et al: BMJ 2007;335:
4 Bronchiectasis Irreversible abnormal dilation of bronchial tree Inflamed, collapsible airways Bacterial Colonization (S. aureus, H. influenzae, P. aeruginosa) Chronic productive cough (wet vs. dry) Collected sputum 3 layers (foam, clear, purulent) cough 90%, sputum 76%, dyspnea 72%, hemoptysis 56% Exam: rales 70%, rhonchi 44%, wheeze 34%. Obstructive physiology Low FEV1, FVC preserved Decreased DLCO
5
6 Bronchiectasis Irreversible abnormal dilation of bronchial tree Inflamed, collapsible airways Bacterial Colonization (S. aureus, H. influenzae, P. aeruginosa) Chronic productive cough (wet vs. dry) Collected sputum 3 layers (foam, clear, purulent) cough 90%, sputum 76%, dyspnea 72%, hemoptysis 56% Exam: rales 70%, rhonchi 44%, wheeze 34%. Obstructive physiology Low FEV1, FVC preserved Decreased DLCO
7 US Prevalence of Non-CF Bronchiectasis Rate per 100, Total Prevalence: ~52/100,000 Men Women >=75 Prevalence may be increasing Sl F>M predominance Age, Years Weycker D et al: Clin Pulm Med 2005
8 Useless Morphology Classification Bronchiectasis can be: Focal (lobe/segment) Diffuse Cylindrical: creates tram track lines Varicose: beaded bronchi. Cystic: occ large cysts imitate cavity or give grape cluster pattern
9 Vicious Cycle Hypothesis Microbial colonization initiates & perpetuates airway inflammation PMNs infiltrate lungs & cause structural airway damage Impaired mucociliary clearance. Optimal for bacterial growth & certain spp. Selection (eg, S aureus, H flu, P aeruginosa)
10
11 Bronchiectasis Differential Diagnosis Idiopathic (50 10%...) Airway obstruction Primary Ciliary Dyskinesia Syndrome (PCD) Immunodeficiency (Ig Def, CLL/Rx, GVHD, HIV) Post-infectious Diffuse Panbronchiolitis Inflammatory Disease Alpha-1-Antitrypsin Syndrome Cystic Fibrosis
12 Airway Obstruction Foreign Body Aspiration Lower lobes, posterior segment upper lobe Obstruction broncholith, slow growing/b9 tumor Lymph nodes enlargement Middle Lobe Syndrome
13 Differential Diagnosis Idiopathic (50 10%...) Airway obstruction Primary Ciliary Dyskinesia Syndrome (PCD) Immunodeficiency (Ig Def, CLL/Rx, GVHD, HIV) Post-infectious Diffuse Panbronchiolitis Inflammatory Disease Alpha-1-Antitrypsin Syndrome Cystic Fibrosis
 = Kartagener s Classic ultrastructure")
14 Primary Ciliary Dyskinesia (PCD) Incidence ~ 1/ /60000 Autosomal recessive (some DNAH11) Classic triad Bronchiectasis Sinusitis Variable male sterility Situs inversus (50%) = Kartagener s Classic ultrastructure defect

15 Nasal NO for PCD Diagnosis Proper SOP, nno <77: Sensitivity 98%, Spec 99% 6 other centers: Identified correctly 70 out of 71 PCD Technology more user friendly nno for screening then confirm by EM, in vitro/vivo assess Leigh et al. Ann ATS 2013;10:574-81
16 Differential Diagnosis Idiopathic (50 10%...) Airway obstruction Primary Ciliary Dyskinesia Syndrome (PCD) Immunodeficiency (Ig Def, CLL/Rx, GVHD, HIV) Post-infectious Diffuse Panbronchiolitis Inflammatory Disease Alpha-1-Antitrypsin Syndrome Cystic Fibrosis
17 Immunodeficiency Hypogammaglobinemia presents in children Recurrent sinopulmonary infections (middle ear) Can be acquired in elderly Measure IgA, IgG, and IgG subclasses Measure response to protein, polysaccharide vaccine NB: D/t dysregulated T-cell function lung/ln bx may show granuloma misdx sarcoid/tb/ntm Treatment: IVIG infusion q mo. Heme-Malig: CLL, post rituximab, GVHD AIDS associated bronchiectasis (recurrent infection) Jobs Syndrome
18 Differential Diagnosis Idiopathic (50 10%...) Airway obstruction Primary Ciliary Dyskinesia Syndrome (PCD) Immunodeficiency (Ig Def, CLL/Rx, GVHD, HIV) Post-infectious Diffuse Panbronchiolitis Inflammatory Disease Alpha-1-Antitrypsin Syndrome Cystic Fibrosis
19 Post-Infectious Viral, Mycoplasma TB Pertussis Nontuberculous mycobacteria & Nodular Bronchiectasis Aspergillus Severe/recurrent bacterial pneumonia Post-op. nosocomial pneumonia Associated with kyphoscoliosis
20 What do you know about Nodular/Bronchiectasis Form of MAC Lung Infection? What about Rapid Growers? NTM Lung Infection a/w Pre-existing Bronchiectasis or CF? Fascinating Stuff???
21 Post-Infectious Viral, Mycoplasma TB Pertussis NTM and nodular bronchiectasis Aspergillus Severe/recurrent bacterial pneumonia Post-op. nosocomial pneumonia Associated with kyphoscoliosis
22 Allergic Bronchopulmonary Aspergillosis (ABPA) 1. Asthma 2. Skin test reactivity to Aspergillus fumigatus 3. Serum precipitins to Aspergillus fumigatus 4. IgE elevation (>1000 ng/ml or >500 IU/ml) 5. Specific IgE (IgG) antibodies to Aspergillus fumigatus 6. Proximal Bronchiectasis 7. Pulmonary Infiltrates (eg. fleeting, upper lobes, mucoid impaction) 8. Eosinophilia with pulmonary infiltrates Note: Positive sputum culture not essential for diagnosis Allergic Bronchopulmonary Mycosis (other Aspergillus spp, Candida, other fungi) Adapted from Patterson & Greenberger
23 Post-Infectious Viral, Mycoplasma TB Pertussis NTM and nodular bronchiectasis Aspergillus Severe/recurrent bacterial pneumonia Post-op. nosocomial pneumonia Associated with kyphoscoliosis
24 Idiopathic Differential Diagnosis Airway obstruction Dyskinetic Cilia Syndrome Immunodeficiency (Agammaglobulinemia) Post-infectious Diffuse Panbronchiolitis Inflammatory Disease α-1 Antitrypsin Syndrome Cystic Fibrosis
25
 Productive cough, dyspnea, wheezing, weight loss, clubbing uncommon Sputum: H. influenzae, S. aureus, P.")
26 Diffuse Panbronchiolitis (DPB) Japanese, Korean, M:F 2:1, onset y.o Clinical characteristics Chronic sinusitis 75%, precedes lung disease (yrs or decades) Productive cough, dyspnea, wheezing, weight loss, clubbing uncommon Sputum: H. influenzae, S. aureus, P. aeruginosa Acquisition of Psa poor survival 5 yr) PFTs: obstructive, mixed obstructive/restrictive Histopath: localized to resp bronch. transmural inflammation (lymphocytes, foamy macrophages) No: exocrine dysfunction, sweat Cl, CFTR abnormality

27 Survival Curves According to Year of Diagnosis WHY? Group A = , n= 190 B = , n= 221 C = , n= 87 Kudoh S. Curr Opin Pulm Med 1998
28 DPB and Macrolide Rx Serendipitous discovery 1982 Standard: E-mycin mg/day continuous No significant change in bacterial flora & serum levels (1 µg/ml) don t exceed MICs Clinical factors improved Randomized blinded trial (Yamamoto et al, 1991) 3 mos E-mycin vs. placebo Improved DOE, sputum volume, CRP, PFTs, CXR) PFTs P. aeruginosa infected group improves also Mortality rates decreased Other macrolides tested (clari-, roxi-, azithromycin) In vitro data: Macrolides modulate inflammatory response & Inhibit P. aeruginosa virulence factors (eg, biofilm)
29 Differential Diagnosis Idiopathic (50 10%...) Airway obstruction Primary Ciliary Dyskinesia Syndrome (PCD) Immunodeficiency (Ig Def, CLL/Rx, GVHD, HIV) Post-infectious Diffuse Panbronchiolitis Inflammatory Disease Alpha-1-Antitrypsin Syndrome Cystic Fibrosis
30 Young s Syndrome Similar to CF Sinusitis, bronchiectasis, azoospermia Nl Sweat Cl, NPD Nl pancreas function No genetic link yet found Infertile middle age males Decreasingly found (toxic exposure births/prior era?)
31 Inflammatory Diseases & Bronchiectasis Sjogren s Syndrome Rheumatoid Arthritis Ulcerative Colitis >> Crohn s disease
32 Alpha-1-Antitrypsin Deficiency Radiographic: Cystic bronchiectasis 10-20% Emphysema co-exists or overshadowed No other predisposing illness Uncertain clinical correlation (sputum production) No pathophysiologic association All causes bronchiectasis: no increase in AAT alleles (Cuvilier et al: Chest 2000)
33 Differential Diagnosis Idiopathic (50 10%...) Airway obstruction Primary Ciliary Dyskinesia Syndrome (PCD) Immunodeficiency (Ig Def, CLL/Rx, GVHD, HIV) Post-infectious Diffuse Panbronchiolitis Inflammatory Disease Alpha-1-Antitrypsin Syndrome Cystic Fibrosis
34 Differential Dx (Mnemonic: IA_SPICE) Idiopathic Airway Obstruction Sjogren s & other Inflammatory (RA, IBD) Post-Infectious (TB, non-tuberculosous mhycobacteria, Aspergillus, Pertussis, NP, virus) Immunodeficiency (Ig, AIDS) CF & other genetic/congenital (Primary Ciliary Dyskinesia, Sequestration, α-1 Anti-trypsin) Esoteric (Diffuse Panbronchiolitis, Yellow Nail Syn., Tracheobronchomegaly [Mounier-Kuhn], Cartilage deficiency [Williams-Campbell], Swyer James)
35 How do you evaluate a patient for bronchiectasis?
36 Evaluation for Bronchiectasis History Poorly resolving/recurrent pneumonia Purulent sputum (quantify) H/O of difficult asthma management Family history/gi problems/infertility Exam nasal polyps localized rales, wheezes, or rhonchi clubbing
37 Evaluation for Bronchiectasis Lab Data Spirometry Sputum Gram Stain & Culture (quantitative) S. aureus, H. influenzae P. aeruginosa (mucoid?) AFB smear/culture (AM x3 Mail Back) Consider: Immunoglobulin electrophoresis & quantification of IgG subclasses; pre/post PVX/DT titers Sweat Chloride, CF genetics (Ambry lab), NPD RF, CCP, ANA, SSA, SSB antibodies Exhaled nasal Nitric Oxide screen, then EM, genetics, Asthma?, Eos?, Aspergillus skin test, IgE (ARUP ABPA panel) Bronchoscopy for cultures (eg, elderly: NTM, other bacteria) Radiology Evaluation Chest x-ray & High Resolution Chest CT Sinus CT
38 What are the radiographic features of bronchiectasis?
39 Radiography Bonchograms (history of medicine) CXR and High Resolution CT Signet Ring Engagement Ring Tram Tracks Railroad tracks

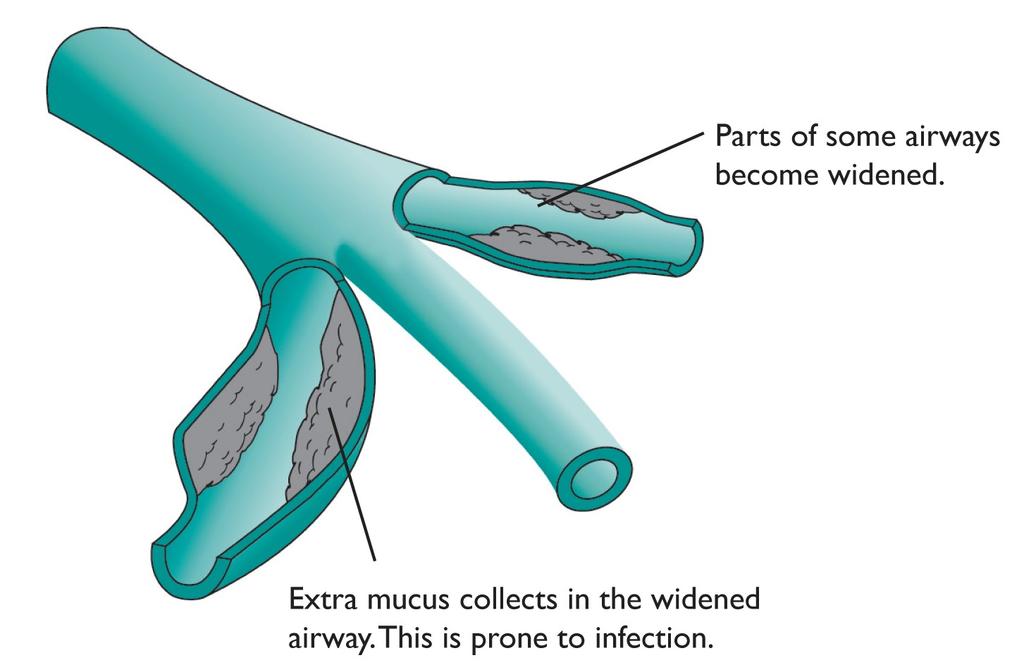
40 Normal Airway Air in dilated airway Swollen airway wall
 Normal: Bronchus Vessel Engagement (Signet) ring: Bronchus")
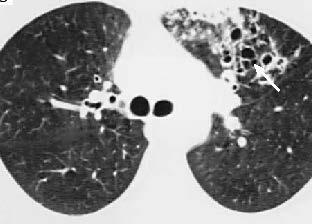
41 CT Characteristics: High resolution= Thin sections (1.5-3 mm) Normal: Bronchus Vessel Engagement (Signet) ring: Bronchus Vessel Railroad tracks
42 HRCT: Other Characteristics Lack of tapering bronchi Clusters = Grape-like appearance Enlarged bronchi can appear cystic vs. Blebs of emphysema (thinner walls)

43 Lack of Tapering Bronchi
44 Grape-like Clusters

45 Cystic Bronchi
46 HRCT bronchiectasis Dx Central ABPA Upper lobe CF Lobar Post-infectious; obstructive (eg, LN, FB) Correlation: # abnormal airways and severity

47 Traction Bronchiectasis Radiographic finding w/o clinical features of bronchiectasis Pulmonary Fibrosis Radiation injury
48 How do you identify acute exacerbation of bronchiectasis?
49 Sypmtoms of Acute Exacerbation of Bronchiectasis Change in sputum production Increased dyspnea Increased cough Increased wheezing Malaise, fatigue, lethargy, decreased exercise tolerance ± Fever (T>38) Changes in chest exam Reduced pulmonary function Radiographic changes (subtle vs. new infiltrate) Adapted from Odonnell et al: Chest 1998
50 How do you treat bronchiectasis?
51 Rx Extrapolated from CF Antibiotics generally effective for chronic Rx Suppress bacteria burden: bacteria = evil cytokines Nebulized tob, gent, colistin effective, small trials Nebulized aztreonam (Cayston) not effective Eradication Rx for P aeruginosa likely effective Cycling antibiotics: no supportive data, but often done Exacerbation: IV antibiotics aimed at predom spp little supportive data Pulmozyme trial not good, maybe harmful Anti-inflammatory Rx Avoid long term steriods except ABPA ICS weak data; ICS/LABA no supportive data (ex. Asthma too) Macrolide randomized control trial data supportive Azithro MWF (EMBRACE, BAT trials) & E-mycin 250 bid (BLISS) Brodt et al. Eur Resp J 2014;44:382-93; Barker AF et al. Lancet Resp Med Aug 2014; O Donnell AE et al Chest 1998 Wong C et al. Lancet 2012;380:660-67; Altenburg J et al. JAMA 2013;309: ; Serisier JD et al. JAMA 2013;309:
52 Bronchiectasis Treatment Overview Manage/alter underlying cause Antibiotics Acute exacerbation, parenteral abx based on culture & susceptibilities Preventive strategies-uncertain benefit Cycling Abx (no real data to support) Inhaled Abx (tobramycin [gent], colistin, not aztreonam) 7% saline neb bid Bronchodilators (widely used no good data) Chest physiotherapy (various modalities) & Aerobic exercise Pulmozyme No ICS (minimal if any benefit) Macrolides (must r/o NTM) Nutrition Surgery
53 Comprehensive Overview McShane P et al. Am J Respir Crit Care Med 2013;188:647-56
Bronchiectasis: An Imaging Approach
 Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
NON-CYSTIC FIBROSIS BRONCHIECTASIS
 NON-CYSTIC FIBROSIS BRONCHIECTASIS MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the
NON-CYSTIC FIBROSIS BRONCHIECTASIS MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the
Evaluation of Patients with Diffuse Bronchiectasis
 Evaluation of Patients with Diffuse Bronchiectasis Dr. Patricia Eshaghian, MD Assistant Clinical Professor of Medicine Director, UCLA Adult Cystic Fibrosis Affiliate Program UCLA Division of Pulmonary
Evaluation of Patients with Diffuse Bronchiectasis Dr. Patricia Eshaghian, MD Assistant Clinical Professor of Medicine Director, UCLA Adult Cystic Fibrosis Affiliate Program UCLA Division of Pulmonary
Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX
 Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX Pioneer of Respiratory Medicine 2016 marked 200th anniversary of his
Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX Pioneer of Respiratory Medicine 2016 marked 200th anniversary of his
Disease spectrum. IPA Invasive pulmonary aspergillosis
 Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
CCLI. Bronchiectasis Treatment Antibiotics. Charles Haworth. Physician / Patient Conference, Georgetown University, May 2017
 Physician / Patient Conference, Georgetown University, May 2017 Bronchiectasis Treatment Antibiotics Charles Haworth CCLI Cambridge Centre for Lung Infection Disclosures Educational talks and / or consultancy
Physician / Patient Conference, Georgetown University, May 2017 Bronchiectasis Treatment Antibiotics Charles Haworth CCLI Cambridge Centre for Lung Infection Disclosures Educational talks and / or consultancy
A Place For Airway Clearance Therapy In Today s Healthcare Environment
 A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
NON-CF BRONCHIECTASIS IN ADULTS
 Séminaire de Pathologie Infectieuse Jeudi 25 juin 2008 Cliniques Universitaires UCL de Mont-Godinne, Yvoir NON-CF BRONCHIECTASIS IN ADULTS Dr Robert Wilson Royal Brompton Hospital, London, UK Aetiology
Séminaire de Pathologie Infectieuse Jeudi 25 juin 2008 Cliniques Universitaires UCL de Mont-Godinne, Yvoir NON-CF BRONCHIECTASIS IN ADULTS Dr Robert Wilson Royal Brompton Hospital, London, UK Aetiology
Bronchiectasis. What is bronchiectasis? What causes bronchiectasis?
 This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
What is Cystic Fibrosis? CYSTIC FIBROSIS. Genetics of CF
 What is Cystic Fibrosis? CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Chronic, progressive and life limiting autosomal recessive genetic disease characterized by chronic
What is Cystic Fibrosis? CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Chronic, progressive and life limiting autosomal recessive genetic disease characterized by chronic
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c)
 Diffuse bronchiectasis b) Cystic fibrosis c)") Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
Chronic lung diseases in children Simple choice 1. Finger clubbing is not characteristic for: a) Diffuse bronchiectasis b) Cystic fibrosis c) Bronchiolitis obliterans d) Complicated acute pneumonia e)
Bronchiectasis. Grant Waterer. Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago
 Bronchiectasis Grant Waterer MBBS PhD MBA FRACP FCCP Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago Conflicts of Interest I have
Bronchiectasis Grant Waterer MBBS PhD MBA FRACP FCCP Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago Conflicts of Interest I have
How To Assess Severity and Prognosis
 How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
Bronchiectasis. Introduction. Key points
 15 Bronchiectasis Introduction i Key points Patients with bronchiectasis typically have chronic airway infection, punctuated by acute exacerbations and accompanied by progressive airflow obstruction. Bronchiectasis
15 Bronchiectasis Introduction i Key points Patients with bronchiectasis typically have chronic airway infection, punctuated by acute exacerbations and accompanied by progressive airflow obstruction. Bronchiectasis
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Non Cystic Fibrosis Bronchiectasis: How to Proceed?
 Non Cystic Fibrosis Bronchiectasis: How to Proceed? Dr Ankit Parakh MD, DNB, MNAMS, RCPCH Fellow (UK), European Diplomate of Pediatric Respiratory Medicine ERS Fellowship Pediatric Medicine & NIV (GOSH,
Non Cystic Fibrosis Bronchiectasis: How to Proceed? Dr Ankit Parakh MD, DNB, MNAMS, RCPCH Fellow (UK), European Diplomate of Pediatric Respiratory Medicine ERS Fellowship Pediatric Medicine & NIV (GOSH,
Chronic suppurative lung disease in adults
 Case Report Chronic suppurative lung disease in adults Mark L. Metersky 1, Antranik Mangardich 2 1 Division of Pulmonary and Critical Care Medicine, University of Connecticut School of Medicine, Farmington,
Case Report Chronic suppurative lung disease in adults Mark L. Metersky 1, Antranik Mangardich 2 1 Division of Pulmonary and Critical Care Medicine, University of Connecticut School of Medicine, Farmington,
Interesting cases in fungal asthma
 Interesting cases in fungal asthma Ritesh Agarwal MD, DM Professor of Pulmonary Medicine Postgraduate Institute of Medical Education and Research Chandigarh, India Fungal asthma Broadly defined as the
Interesting cases in fungal asthma Ritesh Agarwal MD, DM Professor of Pulmonary Medicine Postgraduate Institute of Medical Education and Research Chandigarh, India Fungal asthma Broadly defined as the
Historical perspective
 Bronchiectasis Dilated airways with frequently thickened walls Faculty/Presenter Disclosure Faculty: Dr. Alan Kaplan Relationships with commercial interests (12 months) Grants/research support: N/A Speakers
Bronchiectasis Dilated airways with frequently thickened walls Faculty/Presenter Disclosure Faculty: Dr. Alan Kaplan Relationships with commercial interests (12 months) Grants/research support: N/A Speakers
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
C.S. HAWORTH 1, A. WANNER 2, J. FROEHLICH 3, T. O'NEAL 3, A. DAVIS 4, I. GONDA 3, A. O'DONNELL 5
 Inhaled Liposomal Ciprofloxacin in Patients With Non-Cystic Fibrosis Bronchiectasis and Chronic Pseudomonas aeruginosa: Results From Two Parallel Phase III Trials (ORBIT-3 and -4) C.S. HAWORTH 1, A. WANNER
Inhaled Liposomal Ciprofloxacin in Patients With Non-Cystic Fibrosis Bronchiectasis and Chronic Pseudomonas aeruginosa: Results From Two Parallel Phase III Trials (ORBIT-3 and -4) C.S. HAWORTH 1, A. WANNER
Bronchiectasis Domiciliary treatment. Prof. Adam Hill Royal Infirmary and University of Edinburgh
 Bronchiectasis Domiciliary treatment Prof. Adam Hill Royal Infirmary and University of Edinburgh Plan of talk Background of bronchiectasis Who requires IV antibiotics Domiciliary treatment Results to date.
Bronchiectasis Domiciliary treatment Prof. Adam Hill Royal Infirmary and University of Edinburgh Plan of talk Background of bronchiectasis Who requires IV antibiotics Domiciliary treatment Results to date.
INHALED ANTIBIOTICS THERAPY IN NON-CF LUNG DISEASE
 INHALED ANTIBIOTICS THERAPY IN NON-CF LUNG DISEASE Hannah Blau MBBS Pulmonary Institute and Graub CF Center SCHNEIDER CHILDREN S MEDICAL CENTER OF ISRAEL Chipap 18 th February 2015 Inhaled antibiotic therapy:
INHALED ANTIBIOTICS THERAPY IN NON-CF LUNG DISEASE Hannah Blau MBBS Pulmonary Institute and Graub CF Center SCHNEIDER CHILDREN S MEDICAL CENTER OF ISRAEL Chipap 18 th February 2015 Inhaled antibiotic therapy:
Starship Paediatric Respiratory and Sleep Medicine Department Outpatient Referral Criteria General Principles
 Starship Paediatric Respiratory and Sleep Medicine Department Outpatient Referral Criteria General Principles This document provides guidance for elective outpatient referrals to the Starship Tertiary
Starship Paediatric Respiratory and Sleep Medicine Department Outpatient Referral Criteria General Principles This document provides guidance for elective outpatient referrals to the Starship Tertiary
Diagnostic Evaluation of NTM and Bronchiectasis
 Division of Pulmonary, Critical Care and Sleep Medicine Diagnostic Evaluation of NTM and Bronchiectasis Ashwin Basavaraj, MD, FCCP NTM patient education program November 9, 2016 Involves a combination
Division of Pulmonary, Critical Care and Sleep Medicine Diagnostic Evaluation of NTM and Bronchiectasis Ashwin Basavaraj, MD, FCCP NTM patient education program November 9, 2016 Involves a combination
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
CYSTIC FIBROSIS OBJECTIVES NO CONFLICT OF INTEREST TO DISCLOSE
 CYSTIC FIBROSIS Madhu Pendurthi MD MPH Staff Physician, Mercy Hospital Springfield, MO NO CONFLICT OF INTEREST TO DISCLOSE OBJECTIVES Epidemiology of Cystic Fibrosis (CF) Genetic basis and pathophysiology
CYSTIC FIBROSIS Madhu Pendurthi MD MPH Staff Physician, Mercy Hospital Springfield, MO NO CONFLICT OF INTEREST TO DISCLOSE OBJECTIVES Epidemiology of Cystic Fibrosis (CF) Genetic basis and pathophysiology
Bronchiectasis. Examples include: Viral infections (measles, adenovirus, influenza)
") Bronchiectasis What is Bronchiectasis? Bronchiectasis (pronounced bron-kee-ek'-tas-is) is a condition of the airways in the lungs. These airways (bronchial tubes) are tubelike structures that branch from
Bronchiectasis What is Bronchiectasis? Bronchiectasis (pronounced bron-kee-ek'-tas-is) is a condition of the airways in the lungs. These airways (bronchial tubes) are tubelike structures that branch from
Lung Disease in Pediatrics: is it all in the Genes?
 Lung Disease in Pediatrics: is it all in the Genes? Jay K. Kolls, M.D. Chair, Department of Genetics LSU Health Sciences Center New Orleans, LA Children s s Hospital of Pittsburgh Severe combined immunodeficiency
Lung Disease in Pediatrics: is it all in the Genes? Jay K. Kolls, M.D. Chair, Department of Genetics LSU Health Sciences Center New Orleans, LA Children s s Hospital of Pittsburgh Severe combined immunodeficiency
Inhalational antibacterial regimens in non-cystic fibrosis patients. Jeff Alder Bayer HealthCare
 Inhalational antibacterial regimens in non-cystic fibrosis patients Jeff Alder Bayer HealthCare Alder - Inhaled therapy for non-cf - EMA 25-26 Oct 2012 1 Inhalational antibacterials: two approaches 1.
Inhalational antibacterial regimens in non-cystic fibrosis patients Jeff Alder Bayer HealthCare Alder - Inhaled therapy for non-cf - EMA 25-26 Oct 2012 1 Inhalational antibacterials: two approaches 1.
Swyer-James Syndrome: An Infrequent Cause Of Bronchiectasis?
 ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 12 Number 1 Swyer-James Syndrome: An Infrequent Cause Of Bronchiectasis? A Huaringa, S Malek, M Haro, L Tapia Citation A Huaringa, S Malek, M
ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 12 Number 1 Swyer-James Syndrome: An Infrequent Cause Of Bronchiectasis? A Huaringa, S Malek, M Haro, L Tapia Citation A Huaringa, S Malek, M
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
NTM AND BRONCHIECTASIS (BXSIS): THE CHICKEN AND THE EGG
: THE CHICKEN AND THE EGG") REMINGTON WINTER COURSE IN ID VAIL, CO FEBRUARY, 2010 NONTUBERCULOSIS MYCOBACTERIA AND BRONCHIECTASIS: Revised 1/28/10 10:31 AM- CQ MICHAEL D. ISEMAN, MD OR In some cases NTMs invade pre-existing BXSIS
REMINGTON WINTER COURSE IN ID VAIL, CO FEBRUARY, 2010 NONTUBERCULOSIS MYCOBACTERIA AND BRONCHIECTASIS: Revised 1/28/10 10:31 AM- CQ MICHAEL D. ISEMAN, MD OR In some cases NTMs invade pre-existing BXSIS
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB Case Presentations Doug Hornick, MD; Iowa U Medical School December 1, 2010 Pulmonary Fascinomas with a Tuberculous Attitude Douglas B. Hornick, MD
TB Intensive San Antonio, Texas December 1-3, 2010 TB Case Presentations Doug Hornick, MD; Iowa U Medical School December 1, 2010 Pulmonary Fascinomas with a Tuberculous Attitude Douglas B. Hornick, MD
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
"Management and Treatment of Patients with Cystic fibrosis (CF)
") "Management and Treatment of Patients with Cystic fibrosis (CF) Dr. Malena Cohen-Cymberknoh Pediatric Pulmonology and CF Center Hadassah Hebrew-University Medical Center Jerusalem, Israel Afula, March
"Management and Treatment of Patients with Cystic fibrosis (CF) Dr. Malena Cohen-Cymberknoh Pediatric Pulmonology and CF Center Hadassah Hebrew-University Medical Center Jerusalem, Israel Afula, March
5/5/2013. The Respiratory System. Chapter 16 Notes. The Respiratory System. Nasal Cavity. Sinuses
 The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
Overview of Cystic fibrosis in children. Apeksha Sathyaprasad, MD Pediatric pulmonologist
 Overview of Cystic fibrosis in children Apeksha Sathyaprasad, MD Pediatric pulmonologist No conflicts of interest OBJECTIVES Review pathophysiology of pulmonary disease in cystic fibrosis Review diagnostic
Overview of Cystic fibrosis in children Apeksha Sathyaprasad, MD Pediatric pulmonologist No conflicts of interest OBJECTIVES Review pathophysiology of pulmonary disease in cystic fibrosis Review diagnostic
BTS Guideline for non-cf Bronchiectasis
 ISSN 2040-2023 July 2010 BTS Guideline for non-cf Bronchiectasis A Quick Reference Guide British Thoracic Society www.brit-thoracic.org.uk BTS GUIDELINE FOR NON-CF BRONCHIECTASIS A QUICK REFERENCE GUIDE
ISSN 2040-2023 July 2010 BTS Guideline for non-cf Bronchiectasis A Quick Reference Guide British Thoracic Society www.brit-thoracic.org.uk BTS GUIDELINE FOR NON-CF BRONCHIECTASIS A QUICK REFERENCE GUIDE
Goals Basic defect Pathophysiology Clinical i l signs and symptoms Therapy
 CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Goals Basic defect Pathophysiology Clinical i l signs and symptoms Therapy What is Cystic Fibrosis? Chronic, progressive
CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Goals Basic defect Pathophysiology Clinical i l signs and symptoms Therapy What is Cystic Fibrosis? Chronic, progressive
Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis
 Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Bronchiectasis exacerbations; differences and management. Michael Loebinger Royal Brompton Imperial College
 Bronchiectasis exacerbations; differences and management Michael Loebinger Royal Brompton Imperial College Plan Bronchiectasis background and burden Exacerbation and Management Longer term Management Cases
Bronchiectasis exacerbations; differences and management Michael Loebinger Royal Brompton Imperial College Plan Bronchiectasis background and burden Exacerbation and Management Longer term Management Cases
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Recent advances in diagnosis and management of ABPA. Arindam SR(Pulmonary Medicine)
") Recent advances in diagnosis and management of ABPA Arindam SR(Pulmonary Medicine) Conventional diagnostic criteria for ABPA Primary Episodic bronchial obstruction (asthma) Peripheral blood eosinophilia
Recent advances in diagnosis and management of ABPA Arindam SR(Pulmonary Medicine) Conventional diagnostic criteria for ABPA Primary Episodic bronchial obstruction (asthma) Peripheral blood eosinophilia
Cystic Fibrosis. Jennifer McDaniel, BS, RRT-NPS
 Cystic Fibrosis Jennifer McDaniel, BS, RRT-NPS Overview Cystic fibrosis is the most common fatal, inherited disease in the U. S. CF results from a defective autosomal recessive gene One copy of gene =
Cystic Fibrosis Jennifer McDaniel, BS, RRT-NPS Overview Cystic fibrosis is the most common fatal, inherited disease in the U. S. CF results from a defective autosomal recessive gene One copy of gene =
Importance of fractional exhaled nitric oxide in diagnosis of bronchiectasis accompanied with bronchial asthma
 Original Article Importance of fractional exhaled nitric oxide in diagnosis of bronchiectasis accompanied with bronchial asthma Feng-Jia Chen, Huai Liao, Xin-Yan Huang, Can-Mao Xie Department of Respiratory
Original Article Importance of fractional exhaled nitric oxide in diagnosis of bronchiectasis accompanied with bronchial asthma Feng-Jia Chen, Huai Liao, Xin-Yan Huang, Can-Mao Xie Department of Respiratory
Update on bronchiectasis guidelines. James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK
 Update on bronchiectasis guidelines James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK University of Dundee Bronchiectasis guidelines 2017 2010 2006 2008 2015 2015 Currently valid guidelines
Update on bronchiectasis guidelines James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK University of Dundee Bronchiectasis guidelines 2017 2010 2006 2008 2015 2015 Currently valid guidelines
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Cystic fibrosis: From the gene to the disease
 Cystic fibrosis: From the gene to the disease Christiane Knoop, MD, PhD Institut de Mucoviscidose de l ULB Hôpital Erasme christiane.knoop@erasme.ulb.ac.be Cystic fibrosis «The infant that tastes of salt
Cystic fibrosis: From the gene to the disease Christiane Knoop, MD, PhD Institut de Mucoviscidose de l ULB Hôpital Erasme christiane.knoop@erasme.ulb.ac.be Cystic fibrosis «The infant that tastes of salt
Immune-mediated lung disease. Ian Sabroe
 Immune-mediated lung disease Ian Sabroe It s all immune? Diseases that doesn t have immune involvement? The processes of response to injury and tissue repair are key homeostatic pathways involved in all
Immune-mediated lung disease Ian Sabroe It s all immune? Diseases that doesn t have immune involvement? The processes of response to injury and tissue repair are key homeostatic pathways involved in all
Dr.Sivaramakrishnan PICU KKCTH
 Dr.Sivaramakrishnan PICU KKCTH CASE 1 11/2 year old female child Known wheezer on intermittent bronchodilators Admitted with h/o cough for 2 days Increased work of breathing for 1 day Afebrile/sick looking
Dr.Sivaramakrishnan PICU KKCTH CASE 1 11/2 year old female child Known wheezer on intermittent bronchodilators Admitted with h/o cough for 2 days Increased work of breathing for 1 day Afebrile/sick looking
Eosinophilic lung diseases
 Eosinophilic lung diseases Chai Gin Tsen Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital The eyes do not see what the mind does not know Not very common A high index of suspicion
Eosinophilic lung diseases Chai Gin Tsen Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital The eyes do not see what the mind does not know Not very common A high index of suspicion
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
DIAGNOSIS OF PRIMARY CILIARY DYSKINESIA
 DIAGNOSIS OF PRIMARY CILIARY DYSKINESIA Kris De Boeck, MD PHD Pediatric Pulmonology, University of Leuven, Belgium Introduction Cause Congenital dysfunction of motile cilia Absence/dysfunction of one of
DIAGNOSIS OF PRIMARY CILIARY DYSKINESIA Kris De Boeck, MD PHD Pediatric Pulmonology, University of Leuven, Belgium Introduction Cause Congenital dysfunction of motile cilia Absence/dysfunction of one of
CASE REPORT. 1. Assistant Professor. Department of Paediatrics, Vinayaka Missions Medical College, Karaikal
 A CASE OF KARTAGENER SYNDROME Pagadpally Srinivas 1. Assistant Professor. Department of Paediatrics, Vinayaka Missions Medical College, Karaikal CORRESPONDING AUTHOR: Pagadpally Srinivas, 72, Vellai Pillaiyar
A CASE OF KARTAGENER SYNDROME Pagadpally Srinivas 1. Assistant Professor. Department of Paediatrics, Vinayaka Missions Medical College, Karaikal CORRESPONDING AUTHOR: Pagadpally Srinivas, 72, Vellai Pillaiyar
Update on Biologicals for ABPA and Asthma
 Update on Biologicals for ABPA and Asthma 5 th Advances Against Aspergillosis Istanbul 27 Jan 2012 Richard B. Moss MD Professor of Pediatrics Stanford University Palo Alto CA USA Disease of chronic airway
Update on Biologicals for ABPA and Asthma 5 th Advances Against Aspergillosis Istanbul 27 Jan 2012 Richard B. Moss MD Professor of Pediatrics Stanford University Palo Alto CA USA Disease of chronic airway
Ciliary structure and function. Respiratory tract defense mechanisms. Mechanical lung host defenses
 Respiratory tract defense mechanisms Ciliary structure and function Upper airway Mechanical barriers Nasal turbinates Glottis Reflexes Cough, sneeze Maintenance of oropharyngeal flora Saliva Bacterial
Respiratory tract defense mechanisms Ciliary structure and function Upper airway Mechanical barriers Nasal turbinates Glottis Reflexes Cough, sneeze Maintenance of oropharyngeal flora Saliva Bacterial
Journal Club The ELITE Trial. Sandra Katalinic, Pharmacy Resident University Hospital of Northern British Columbia April 28, 2010
 Journal Club The ELITE Trial Sandra Katalinic, Pharmacy Resident University Hospital of Northern British Columbia April 28, 2010 Overview Journal article Title, journal, authors, funding Abstract Introduction
Journal Club The ELITE Trial Sandra Katalinic, Pharmacy Resident University Hospital of Northern British Columbia April 28, 2010 Overview Journal article Title, journal, authors, funding Abstract Introduction
PNEUMONIA. I. Background 6 th most common cause of death in U.S. Most common cause of infection related mortality
 Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Cystic Fibrosis Care Guidelines for Challenging Cystic Fibrosis
 Cystic Fibrosis Care Guidelines for Challenging Cystic Fibrosis APRIL 2018 Authors Steve Kent MD, CF Clinic Director, Victoria General Hospital (VGH), Victoria Mark Chilvers MD, CF Clinic Director, B.C.
Cystic Fibrosis Care Guidelines for Challenging Cystic Fibrosis APRIL 2018 Authors Steve Kent MD, CF Clinic Director, Victoria General Hospital (VGH), Victoria Mark Chilvers MD, CF Clinic Director, B.C.
Fungal (Aspergillus and Candida) infections in Cystic fibrosis
 infections in Cystic fibrosis") Fungal (Aspergillus and Candida) infections in Cystic fibrosis Malena Cohen-Cymberknoh, MD CF Center Hadassah-Hebrew University Medical Center Jerusalem, Israel Israeli Annual CF Conference, Herzlyia,
Fungal (Aspergillus and Candida) infections in Cystic fibrosis Malena Cohen-Cymberknoh, MD CF Center Hadassah-Hebrew University Medical Center Jerusalem, Israel Israeli Annual CF Conference, Herzlyia,
Nontuberculous Mycobacteria (NTM)
") Nontuberculous Mycobacteria (NTM) Bacteria, like plants and animals, have been classified into similar groups. The groups are called "families." One such family of bacteria is known as the Mycobacteriaceae.
Nontuberculous Mycobacteria (NTM) Bacteria, like plants and animals, have been classified into similar groups. The groups are called "families." One such family of bacteria is known as the Mycobacteriaceae.
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Total collapse of the lung in aspergillosis
 Thorax (1965), 20, 118. Total collapse of the lung in aspergillosis R. H. ELLIS From the Gloucestershire Royal Hospital, Pulmonary aspergillosis can be divided conveniently into two main types, allergic
Thorax (1965), 20, 118. Total collapse of the lung in aspergillosis R. H. ELLIS From the Gloucestershire Royal Hospital, Pulmonary aspergillosis can be divided conveniently into two main types, allergic
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
PATHOLOGY & PATHOPHYSIOLOGY
 PATHOLOGY & PATHOPHYSIOLOGY DISORDERS OF THE RESPIRATORY SYSTEM DISORDERS OF THE RESPIRATORY SYSTEM Disorders of the Respiratory System Infections Degenerative Tumours Immune Trauma Congenital Upper respiratory
PATHOLOGY & PATHOPHYSIOLOGY DISORDERS OF THE RESPIRATORY SYSTEM DISORDERS OF THE RESPIRATORY SYSTEM Disorders of the Respiratory System Infections Degenerative Tumours Immune Trauma Congenital Upper respiratory
Imaging Small Airways Diseases: Not Just Air trapping. Eric J. Stern MD University of Washington
 Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Pulmonary Exacerbations:
 Pulmonary Exacerbations: Better Understanding Needed Michael Tracy, MD Clinical Assistant Professor Pediatric Pulmonary CF Pulmonary Exacerbations Definition Importance Causes Treatment Research opportunities
Pulmonary Exacerbations: Better Understanding Needed Michael Tracy, MD Clinical Assistant Professor Pediatric Pulmonary CF Pulmonary Exacerbations Definition Importance Causes Treatment Research opportunities
Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University
 Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University Asthma-related Comorbidities Comorbid conditions of the upper airways Rhinitis and Sinusitis
Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University Asthma-related Comorbidities Comorbid conditions of the upper airways Rhinitis and Sinusitis
10/05/2017. Learning Objectives. Etiology and Prevalence. Diagnosis of Cystic Fibrosis. Disease of Childhood? Survival in Cystic Fibrosis
 Management of the Cystic Fibrosis Patient Jessica Goggin, MAS, RN Nurse Manager UC San Diego Adult Cystic Fibrosis Program Learning Objectives 1. Describe the symptoms associated with Cystic Fibrosis (CF).
Management of the Cystic Fibrosis Patient Jessica Goggin, MAS, RN Nurse Manager UC San Diego Adult Cystic Fibrosis Program Learning Objectives 1. Describe the symptoms associated with Cystic Fibrosis (CF).
COMMON VARIABLE IMMUNODEFICIENCY
 COMMON VARIABLE IMMUNODEFICIENCY This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 COMMON VARIABLE IMMUNODEFICIENCY Also available
COMMON VARIABLE IMMUNODEFICIENCY This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 COMMON VARIABLE IMMUNODEFICIENCY Also available
Asthma. - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness.
 Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Clinical Commissioning Policy: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages)
") Clinical Commissioning Policy: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages) Reference: NHS England: 16029/P NHS England INFORMATION READER BOX Directorate Medical Operations and
Clinical Commissioning Policy: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages) Reference: NHS England: 16029/P NHS England INFORMATION READER BOX Directorate Medical Operations and
Vascular Lung Diseases
 Vascular Lung Diseases SESSION SPECIFIC OBJECTIVES List the major types of vascular lung disease Recognize and describe the pathology of vascular lung disease: Pulmonary embolism, thrombosis, hypertension,
Vascular Lung Diseases SESSION SPECIFIC OBJECTIVES List the major types of vascular lung disease Recognize and describe the pathology of vascular lung disease: Pulmonary embolism, thrombosis, hypertension,
Allergic Bronchopulmonary Aspergillosis: An Unusual Complication of Bronchial Asthma
 Allergic Bronchopulmonary Aspergillosis: An Unusual Complication of Bronchial Asthma Pages with reference to book, From 329 To 331 S. Fayyaz Hussain, Javaid A. Khan ( Department of Medicine, The Aga Khan
Allergic Bronchopulmonary Aspergillosis: An Unusual Complication of Bronchial Asthma Pages with reference to book, From 329 To 331 S. Fayyaz Hussain, Javaid A. Khan ( Department of Medicine, The Aga Khan
Cystic fibrosis: From childhood to adulthood. Eitan Kerem Department of Pediatrics and CF Center Hadassah University Hospital Jerusalem Israel
 Cystic fibrosis: From childhood to adulthood Eitan Kerem Department of Pediatrics and CF Center Hadassah University Hospital Jerusalem Israel Vas deference H 2 O Cl - Na + H 2 O Na + Cl - Cl - Cl -
Cystic fibrosis: From childhood to adulthood Eitan Kerem Department of Pediatrics and CF Center Hadassah University Hospital Jerusalem Israel Vas deference H 2 O Cl - Na + H 2 O Na + Cl - Cl - Cl -
Conference Bronchiectasis A Growing Problem
 Conference 2015 Bronchiectasis A Growing Problem Bronchiectasis (in Children) What is it? Why such a concern in NZ? What to look out for? Management Positives? Just a note that the bar for diagnosis, referral
Conference 2015 Bronchiectasis A Growing Problem Bronchiectasis (in Children) What is it? Why such a concern in NZ? What to look out for? Management Positives? Just a note that the bar for diagnosis, referral
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012
 Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
2018 Vindico Medical Education. Non-tuberculous Mycobacteria: Circumventing Difficulties in Diagnosis and Treatment
 Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Chronic Cough An Unusual Presentation. Dr Sourabh Jain Department of Respiratory Medicine
 Chronic Cough An Unusual Presentation Dr Sourabh Jain Department of Respiratory Medicine A 72 years old male from Pune, non smoker, with no co-morbidities Chief Complaints : Chronic cough with scanty mucoid
Chronic Cough An Unusual Presentation Dr Sourabh Jain Department of Respiratory Medicine A 72 years old male from Pune, non smoker, with no co-morbidities Chief Complaints : Chronic cough with scanty mucoid
Nontuberculous Mycobacteria (NTM) in Patients with Cystic Fibrosis
 in Patients with Cystic Fibrosis") Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/cystic-fibrosis-in-focus/nontuberculous-mycobacteria-ntm-in-patientswith-cystic-fibrosis/8337/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/cystic-fibrosis-in-focus/nontuberculous-mycobacteria-ntm-in-patientswith-cystic-fibrosis/8337/
4.6 Small airways disease
 4.6 Small airways disease Author: Jean-Marc Fellrath 1. INTRODUCTION Small airways are defined as any non alveolated and noncartilaginous airway that has an internal diameter of 2 mm. Several observations
4.6 Small airways disease Author: Jean-Marc Fellrath 1. INTRODUCTION Small airways are defined as any non alveolated and noncartilaginous airway that has an internal diameter of 2 mm. Several observations
Cystic Fibrosis the future
 Cystic Fibrosis the future Pathophysiologic cascade Abnormal Gene Abnormal CFTR Therapy Gene replacement Protein replacement Gene read through therapy Abnormal sodium chloride & water movement through
Cystic Fibrosis the future Pathophysiologic cascade Abnormal Gene Abnormal CFTR Therapy Gene replacement Protein replacement Gene read through therapy Abnormal sodium chloride & water movement through
4/17/2010 C ini n ca c l a Ev E a v l a ua u t a ion o n of o ILD U dat a e t e i n I LDs
 Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
The Ghost in the Closet. Allergic Sino-Bronchopulmonary Aspergillosis Without Bronchial Asthma: A Case Report & Review of the Subject
 Proceeding S.Z.P.G.M.I. Vol: 24(1): pp. 55-59 2010. The Ghost in the Closet. Allergic Sino-Bronchopulmonary Aspergillosis Without Bronchial Asthma: A Case Report & Review of the Subject Department of Pulmonology,
Proceeding S.Z.P.G.M.I. Vol: 24(1): pp. 55-59 2010. The Ghost in the Closet. Allergic Sino-Bronchopulmonary Aspergillosis Without Bronchial Asthma: A Case Report & Review of the Subject Department of Pulmonology,