2012 PENNSYLVANIA ASTHMA BURDEN REPORT
|
|
|
- Shannon Newton
- 6 years ago
- Views:
Transcription



1 2012 PENNSYLVANIA ASTHMA BURDEN REPORT
2
3 Table Of Contents Introduction Methodology Executive Summary Section 1: Pennsylvania Population and Economic Statistics Figure 1-1: Decennial Population Percent Change, PA Table 1-1: Demographic Profile by Age, PA Table 1-2: Demographic Profile by Race, PA Figure 1-2: Decennial Minority Population Percent Change, PA Table 1-3: Poverty Status in the Past 12 Months by Family Type and Presence of Related Children, PA counties: Section 2: Asthma Prevalence Asthma Prevalence in Pennsylvania vs. U.S. Figure 2-1: Adult Self-Reported Lifetime Asthma Prevalence Rate (Percent), PA vs. U.S., Figure 2-2: Adult Self-Reported Current Asthma Prevalence Rate (Percent) PA vs. U.S., Figure 2-3: Adult Self-Reported Lifetime Asthma Prevalence Rate (Percent) by Sex, PA vs. U.S., Table of Contents Figure 2-4: Adult Self-Reported Current Asthma Prevalence Rate (Percent) by Sex, PA vs. U.S., Figure 2-5: Adult Self-Reported Lifetime Asthma Prevalence Rate (Percent) by Race, PA vs. U.S., Figure 2-6: Adult Self-Reported Current Asthma Prevalence Rate (Percent) by Race, PA vs. U.S., Figure 2-7: Child Lifetime Asthma Prevalence Rate (Percent) by Sex, PA vs. U.S., Figure 2-8: Child Current Asthma Prevalence Rate (Percent) by Sex, PA vs. U.S., Figure 2-9: Child Lifetime Asthma Prevalence Rate (Percent) by Race, PA vs. U.S., Figure 2-10: Child Current Asthma Prevalence Rate (Percent) by Race, PA vs. U.S.,
4 Table Of Contents continued Asthma Prevalence in Pennsylvania Table 2-1: Lifetime Asthma Prevalence Among Pennsylvania Residents by Age Group, PA Table 2-2: Current Asthma Prevalence Among Pennsylvania Residents by Age Group, PA Table 2-3: Current Asthma Prevalence Among Adults by Education Attainment, PA Table 2-4: Self-Reported Current Asthma Prevalence Among Adults by Income, PA Table 2-5: Self-Reported Current Asthma Prevalence Among Adults by Selected Characteristics, PA Figure 2-11: Adult Self-Reported Current Asthma Prevalence Rate (Percent) by Health District, PA, Table of Contents Asthma Management and Quality of Life in Pennsylvania Figure 2-12: Percentage of Adults With Asthma Who Had Asthma Episode Attack in the Past Year, PA 2010 BRFSS Figure 2-13: Percentage of Adults With Asthma Attacks Who Visited an ER or Received Urgent Care For Asthma in Past Year, PA 2010 BRFSS Figure 2-14: Percentage of Adults With Asthma Attacks Who Visited Health Professional for Worsening Asthma Symptoms in Past Year, PA 2010 BRFSS Figure 2-15: Percentage of Adults With Asthma Who Visited Health Professional for Routine Treatment of Asthma in Past Year, PA 2010 BRFSS Figure 2-16: Percentage of Adults With Asthma Unable to work or Do Usual Activities Due to Asthma in Past Year, PA 2010 BRFSS Figure 2-17: Percentage of Adults With Asthma Who Had Asthma Symptoms Every day in the Past 30 Days, PA 2010 BRFSS Figure 2-18: Percentage of Adults With Asthma Symptoms Who Had 5+ Days Sleep Difficult Due to Asthma Symptoms in Past 30 Days, PA 2010 BRFSS Figure 2-19: Percentage of Adults With Asthma Who Used Prescription Asthma Meds to Prevent Attack 25+ days in Past 30 Days, PA 2010 BRFSS Figure 2-20: Percentage of Adults With Asthma Who Used Prescription Asthma Inhaler During Attack 5+ Times in Past 30 Days, PA 2010 BRFSS Figure 2-21: Percentage of Adults With Asthma Told Had Asthma At Age Less Than 10, PA 2010 BRFSS
5 Table Of Contents continued Section 3: Asthma Hospitalization in Pennsylvania Figure 3-1: Rates of Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis Among Children and Adults, PA Figure 3-2: Trends of Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis by Race and Ethnicity, PA Figure 3-3: Rates of Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis by Age Group and Gender, PA (Combined Data) Figure 3-4: Distribution of the Primary Payers for Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis, PA (Combined Data) Figure 3-5: Distribution of the Admission Types for Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis, PA (Combined Data) Figure 3-6: Average Charges per Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis among Children and Adults (does not include professional fees), PA Figure 3-7: Rates of Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis among Children and Adults admitted to the Hospital through the Emergency Room (ER) by Day of the Week, PA (Combined Data) Figure 3-8: Asthma Age-Adjusted Rates for Inpatient Hospitalizations with Asthma as the Primary Discharge Diagnosis by Health District, PA Table 3-1: Average Length of Stay (LOS) and Average Charges per Day in the Hospital for Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis Due To Asthma (does not include professional fees), PA Table of Contents Table 3-2: Number and Percentage of Inpatient Hospitalizations with Asthma as the Primary Discharge Diagnosis through the Emergency Room (ER), PA Table 3-3: Total Charges for Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis, including Total Charges for Admission through the Emergency Room (does not include professional fees), PA Table 3-4: Number of Admissions, Length of Stay (LOS) and Average Charges per Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis by Type of Asthma, PA Figure 3-9: Average Charges for Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis by Health District (does not include professional fees), PA Figure 3-10: Total Charges for Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis by Health District (does not include professional fees), PA
6 Table Of Contents continued Table 3-5: Number of Visits, Length of Stay (LOS) and Average Charge per Visit for Ambulatory/Outpatient Visits with Asthma as the Primary Discharge Diagnosis by Type of Asthma, PA Table 3-6: Number of Patient Readmissions, Length of Stay (LOS) and Average Charges per Hospitalization for Patients with Asthma as the Primary Discharge Diagnosis (does not include professional fees), PA Table 3-7: Number and Percentage of Inpatient Hospitalizations with Asthma as the Primary Discharge Diagnosis Entering the Hospital through the Emergency Room (ER) by Region, PA (Combined Data) Figure 3-11: Inpatient Hospitalization Rates with Asthma as the Primary Discharge Diagnosis among Adults, PA (Combined Data) Figure 3-12: Inpatient Hospitalization Rates with Asthma as the Primary Discharge Diagnosis among Children, PA (Combined Data) Table of Contents Figure 3-13: Inpatient Hospitalization Rates with Asthma as the Primary Discharge Diagnosis, PA (Overall) Table 3-8: Asthma Inpatient Hospitalization Rate per 10,000 Residents by Age Group Compared to the Healthy People (HP) 2010 Objectives, PA Section 4: Asthma Lifetime Prevalence among Pennsylvania School Students Figure 4-1: Lifetime Asthma Prevalence among School Students, Pennsylvania 1997/ / Table 4-1: Lifetime Asthma Prevalence among School Students Health District and County, Pennsylvania 2003/ / Table 4-1: (Continued): Lifetime Asthma Prevalence among School Students by Health District and County, Pennsylvania 2003/ / Figure 4-2: Lifetime Asthma Prevalence Among School Students by Health District, Pennsylvania 2003/ / Figure 4-3: Lifetime Asthma Prevalence Among School Students by County, Pennsylvania 2003/ /
7 Table Of Contents continued Section 5: Asthma Burden in Pennsylvania s Children s Health Insurance Program (CHIP) Figure 5-1: Emergency Room Visit Rates by Age Group, PA (Combined Data) Figure 5-2: Hospitalization Rates with Asthma as Primary Discharge Diagnosis by Age Group, PA Figure 5-3: Emergency Room Visit Rates by Health District and Year, PA Table 5-1: Emergency Room Visit Rates by Sex and Age Group, PA Table 5-2: Inpatient Hospitalization Rates with Asthma as Primary Discharge Diagnosis by Sex and Age Group, PA (Combined Data) Figure 5-4: Inpatient Hospitalization Rates with Asthma as Primary Discharge Diagnosis by Age Group and Health District, PA (Combined Data) Figure 5-5: Percentage of CHIP recipients with Asthma Receiving Appropriate Long-Term Control Medications by Sex and Age Group, PA Figure 5-6: Percentage of CHIP recipients with Asthma Receiving Appropriate Long-Term Control Medications by Health District, PA (Combined Data) Table 5-3: Number and Percentage of CHIP Recipients with Asthma Receiving Appropriate Long-Term Control Medications by Age Group and County, PA Table 5-3 (Continued): Number and Percentage of CHIP recipients with Asthma Receiving Appropriate Long-Term Control Medications by Age Group and County, PA Table of Contents Section 6: Asthma Mortality in Pennsylvania Figure 6-1: Age-Adjusted Asthma Death Rates Among Pennsylvania Residents, PA Figure 6-2: Age-Adjusted Asthma Death Rates by Race and Ethnicity, PA Figure 6-3: Age-Adjusted Asthma Death Rates by Sex, PA (Combined Data) Table 6-1: Age-Adjusted Asthma Death Rates by Age, PA Figure 6-4: Age-Adjusted Asthma Death Rates by County, PA (Combined Data) References Glossary of Terms Acknowledgements Disclaimers
8 Introduction Introduction Asthma remains a serious health concern in Pennsylvania. Asthma is the third leading cause of hospitalization among persons under 18 years of age. Asthma remains the most common chronic condition of childhood in the United States, exceeded only by pneumonia and injuries. The disease can be controlled by taking medicine and avoiding the triggers that can cause an attack, such as pollen, dust, animal dander, industrial chemicals, viral infections, changes in the weather, exercise, emotional stress, etc. If appropriate disease management is available and utilized, people with asthma can expect to prevent asthma symptoms during both day and night, reduce the number of missed school/work days, have minimal need for emergency room visits or hospitalizations, and maintain normal activity levels. The first Pennsylvania Asthma Burden Report was published in 2006, and updates have been developed every year to describe the burden of asthma in Pennsylvania in different areas of the state. In 2009, the Pennsylvania Department of Health (PA DOH) successfully competed for and was awarded a five-year cooperative agreement that allows continuance of implementations/ interventions to achieve positive health impacts, such as reduction in the number of deaths, hospitalizations and emergency room visits, thereby increasing the quality of life for Pennsylvania residents with asthma. The overall goal is to reduce the burden of asthma. The describes the burden of asthma among Pennsylvania residents by age, sex, race/ethnicity and geographical location. The report presents information on asthma prevalence in Pennsylvania vs. the U.S., asthma prevalence and asthma management in Pennsylvania, rates of asthma inpatient and outpatient hospitalization as the primary discharge diagnosis (according to ICD-9 code ), length of stay, hospital charges, sources of payment, admission type, and more. Analysis of lifetime asthma prevalence among school students is also represented in the report and describes the burden of asthma by year and geographical location. Analysis of asthma prevalence among children enrolled in Pennsylvania s Children s Health Insurance Program (CHIP), describes the burden of asthma among children (ages 0-18), including hospitalization and emergency room visits. Asthma death rates among Pennsylvania residents are represented in Section 6, Asthma Mortality in Pennsylvania, which also illustrates health disparities among different groups of residents. By utilizing asthma data from data providers, the asthma surveillance system is a critical component of the Pennsylvania Asthma Control Program (PA ACP). Data providers continuously provide materials for asthma surveillance system output/products/ publications to the public in an effort to reduce the burden of asthma in the Commonwealth of Pennsylvania. Analyses provided in this report can be useful for planning, prevention, education and evaluation of asthma control measures in areas with a high burden of asthma. 1
9 Methodology Data were analyzed using SAS software and Excel, with results presented in PowerPoint. Maps generated by Geographic Information System (GIS) tools are used for visual display of the data and for identification of areas with high burden. Both geographic (e.g., county, PA DOH health district) and demographic (e.g., age group) subpopulation analyses were conducted to identify disparities. However, due to the small size of some groups, descriptive information was limited, and estimated prevalence and hospitalizations rates of asthma for smaller geographical areas were not always available. Executive Summary Asthma is a chronic inflammatory disorder of the airways characterized by episodes of reversible breathing problems due to airway narrowing and obstruction. These episodes can range in severity from mild to life threatening. Symptoms of asthma include wheezing, coughing, chest tightness and shortness of breath. The increase in asthma seen among children in westernized countries may be the result of exposures to various factors in the fetal and early childhood period, which may, in turn, influence the development of the immune system. The exact cause of asthma is not known; asthma is a complex disease. However, risk factors for asthma currently being investigated include: Genetic predisposition such as atopy or an allergic reaction, which can be detected by specific serum IgE or skin-test reactivity to environmental allergens, is often associated with asthma; Sensitization to irritants and allergens such as cat and other animal dander, dust mites, cockroaches, diesel exhaust particles, mold, house dust, pollen, fungus, medicine, workplace contaminants, etc.; and Contributing factors, which may include respiratory infections such as influenza or common cold, indoor and outdoor air quality, and cigarette smoke. Parental smoking is very likely to be causally related to acute lower respiratory tract illnesses in infancy and to childhood asthma and wheezing. 1, 2 There is sufficient evidence to suggest that air pollutants, such as ozone and particulate matter, decrease lung function, trigger exacerbations of asthma and increase rates of hospitalization for asthma. Asthma is one of the most prevalent chronic conditions affecting Americans. Asthma affects the quality of life for people and their families. Asthma affects people of every race, sex and age. 3 However, significant disparities in asthma morbidity and mortality exist, in particular for low-income and minority populations. Populations with higher rates of asthma include: Children; Women (among adults) and boys (among children); African-Americans; Puerto Ricans; People living in the northeast United States; People living below the federal poverty level; and Employees with exposure to such irritants as paints; cleaning products; dusts from wood, grain and flour; latex gloves; certain molds; animals; and insects in the workplace. Methodology / Executive Summary 2
10 Daily preventive treatment can prevent symptoms and attacks and enable individuals who have asthma to lead active lives. The most current evidence-based guidelines for the diagnosis and management of asthma were developed by an expert panel commissioned by the National Asthma Education and Prevention Program (NAEPP), coordinated by the National Heart, Lung, and Blood Institute of the National Institutes of Health (NIH). 4 The NAEPP guidelines focus on four key components of asthma care to improve the quality of care and health outcomes of people with asthma: assessment and monitoring; patient education; control of factors contributing to asthma severity; and medical treatment. These guidelines indicated that, among other long-term control medications for asthma, inhaled corticosteroids were the most potent and consistently effective long-term control medication. 4 Key Findings: Executive Summary 3 in Asthma Prevalence in Pennsylvania vs. U.S. During the 10-year period of , the annual prevalence estimate of lifetime and current asthma among adults in both Pennsylvania and the U.S. has significantly increased [Figure 2-1 and Figure 2-2]. Between , in Pennsylvania and the U.S., the lifetime current asthma prevalence among adult females was consistently and significantly higher than adult males [Figure 2-3 and Figure 2-4]. Between , there were significant discrepancies in the lifetime and current asthma prevalence among adult blacks and whites in the U.S. for each year. In Pennsylvania, lifetime and current asthma prevalence among adult blacks was higher than among adult whites [Figure 2-5 and Figure 2-6]. During the five-year period of , in Pennsylvania, more boys had both lifetime and current asthma than girls. There was a significant difference in the estimated lifetime prevalence among boys in Pennsylvania compared to the U.S [Figure 2-7 and Figure 2-8]. Between , in Pennsylvania and the U.S., the child lifetime and current asthma prevalence among blacks was higher than among whites. There were no significant differences in the estimated annual child lifetime and current asthma prevalence among blacks and whites for Pennsylvania compared to the U.S. [Figure 2-9 and Figure 2-10]. Asthma Prevalence in Pennsylvania In 2008 and 2010, there were significant differences in the estimated child lifetime asthma prevalence in the age group compared to some other age groups. In 2006, 2007 and 2010, the estimated lifetime and current asthma prevalence among adults (18+) were significantly higher in age groups compared to some other adult age groups [Table 2-1 and Table 2-2]. During , there were some correlations between educational level and current asthma prevalence among adults [Table 2-3].
11 In 2006, 2008, 2009 and 2010, the current asthma prevalence among adults was significantly higher among people with an income level of less than $15,000, compared to an income level of $50,000 and higher. It seems that income level is related to current asthma prevalence among adults [Table 2-4]. In 2006, 2009 and 2010, the current asthma prevalence among adults with body mass index (BMI) greater than 30 was significantly higher compared to adults with BMI less than 30. It seems that the BMI level is related to current asthma prevalence among adults [Table 2-5]. In 2007 and 2009, the current asthma prevalence among adults who were Current Smokers was significantly higher than adults who were Former Smokers or Never Smoked. However, data are not sufficient to make concrete conclusions in terms of current asthma prevalence among adults according to their smoking status; more data are required to make an accurate analysis [Table 2-5]. In Pennsylvania, the highest current asthma prevalence in was observed in the Southeastern Health District, and the North central Health District had the highest prevalence in [Figure 2-11]. Asthma Management and Quality of Life in Pennsylvania Among adults with current asthma in Pennsylvania, 46 percent reported that they had one or more asthma attacks during the preceding 12 months. Females with current asthma were more likely to have had an asthma attack during the preceding 12 months than males (52 percent vs. 37 percent). Non-Hispanic whites with current asthma were more likely to have had an asthma attack during the preceding 12 months than non-hispanic blacks (48 percent vs. 40 percent) [Figure 2-12]. Among adults who experienced asthma attacks, only 27 percent reported that they visited an emergency room (ER) or urgent care facility because of their asthma during the past 12 months. Females were more likely to have visited the ER than males [Figure 2-13]. Among adults with asthma attacks, 39 percent reported that they visited a physician or nurse for urgent treatment of worsening asthma symptoms during the past 12 months [Figure 2-14]. Among adults with asthma, 56 percent reported that they were seen by their physician for a routine asthma checkup during the past 12 months [Figure 2-15]. Among adults with asthma, one out of five reported that, because of asthma, he or she was unable to work or carry out usual activities for at least one day during the past 12 months [Figure 2-16]. Among adults with asthma, 15 percent reported that they had asthma symptoms each day during the past 30 days [Figure 2-17]. Among adults with asthma, 34 percent reported that they used long-term control prescription medications to prevent an asthma attack for more than 25 days during the past 30 days. Of all adults with asthma, 38 percent of the females used long-term medications, as did 28 percent of the males. Of these same adults, 37 percent of the non-hispanic whites used long-term medications, as did 23 percent of the non-hispanic blacks [Figure 2-19]. Executive Summary 4
12 Among adults with asthma, 20 percent reported that they used asthma inhalers five or more times during the past 30 days. Of all adults with asthma, 23 percent of the females used inhalers five or more times in the past month, as did 15 percent of the males. Of these same adults, 20 percent of the non-hispanic whites used inhalers five or more times, as did 21 percent of the non-hispanic blacks [Figure 2-20]. Among adults with asthma, 26 percent were told they had asthma before age 10. Among females, 21 percent and 34 percent of the males were told they had asthma before age 10. Forty percent of non-hispanic blacks and 25 percent of the non-hispanic whites were told they had asthma before age 10 [Figure 2-21]. Executive Summary Asthma Hospitalization in Pennsylvania In 2010, the asthma hospitalization rate for age group 0-17 decreased approximately 9.6 percent from 2009 (22.4 per 10,000 vs. 24.8). For age group 18+, the rate decreased approximately 15.8 percent from 2009 (14.9 per 10,000 vs. 17.8) [Figure 3-1]. Between , the asthma hospitalization rates were consistently higher for black and Hispanic residents, compared to all other groups [Figure 3-2]. In , asthma hospitalization rates among males younger than 15 years of age were higher than females of the same age in Pennsylvania; however, females had higher rates than males in age groups 15 and older. The hospitalization rate for asthma decreased in age group and then increased until reaching age 65 and older [Figure 3-3]. In , Pennsylvania s largest hospital payer was Medicaid, which accounts for 42,749 asthma hospitalizations or almost 37 percent of all admissions [Figure 3-4]. During , about 74 percent of all admissions due to asthma as the primary discharge diagnosis entered hospitals through the ER [Figure 3-5]. In , the average charges for inpatient hospitalization with asthma as the primary discharge diagnosis were on the rise, with greater increases among adults than children [Figure 3-6]. Between , hospitalization charges were higher among males compared to females, among non-hispanic blacks compared to non-hispanic whites, and among Hispanics compared to non-hispanic groups [Table 3-1]. In 2010, total charges for inpatient hospitalization with asthma as the primary discharge diagnosis were less than they were in 2008 and 2009 [Table 3-3]. Between , rates of inpatient hospitalization for Pennsylvania residents with asthma as the primary discharge diagnosis through the ER were highest on Monday and lowest on Friday and Saturday [Figure 3-7]. Between , adults stayed in hospitals longer than children, females longer than males, non-hispanic whites longer than non-hispanic blacks, and non-hispanics longer than Hispanics [Table 3-1]. In 2010, the percentage of admissions to the hospital through the ER due to asthma as the primary discharge diagnosis decreased among children, males, females, non-hispanic blacks, Hispanics and non-hispanics compared to In 2010, the percentage of admissions was higher for adults and non-hispanic whites than in 2006 [Table 3-2]. 5
13 In , age-adjusted inpatient hospitalization rates with asthma as the primary discharge diagnosis were highest in the Southeast Health District, compared to other health districts [Figure 3-8]. The Southeast Health District also accounts for the highest total and average charges [Figure 3-9 and Figure 3-10]. In , the number of inpatient admissions due to asthma decreased for all types of asthma, with the exception of the Extrinsic and Intrinsic type [Table 3-4]. The number of outpatient/ambulatory visits due to asthma decreased as well; however, the number of visits of the Extrinsic and Intrinsic type of asthma increased [Table 3-5]. In , nearly 85 percent of all admissions occurred only one time, while about 15 percent of all admissions were readmitted two or more times [Table 3-6]. Between , Allegheny County accounts for the highest percentage of all hospital admissions through the ER, compared to Philadelphia County and the rest of the state. However, asthma hospitalization rates were highest in Philadelphia County, compared to Allegheny County and the rest of the state [Table 3-7]. Between , the asthma inpatient hospitalization rates remain higher than the 2010 HP Objectives for all age groups/characteristics, with two exceptions for white 0-4 and white 5-64 age groups. Pennsylvania exceeded the HP 2010 targets for each of the age groups [Table 3-8]. Asthma Lifetime Prevalence among Pennsylvania School Students Asthma prevalence among students in Pennsylvania almost doubled from 1997/98 to 2008/09 [Figure 4-1]. The highest asthma prevalence among students in the period between 2003/04 and 2008/09 took place in the Southeast Health District [Figure 4-2]. Philadelphia County, during the same period of time, had the highest asthma prevalence among students of all the counties in Pennsylvania [Figure 4-3]. Executive Summary Asthma Burden in Pennsylvania s Children s Health Insurance Program (CHIP) For the entire six-year period, ER visit rates among CHIP recipients younger than 13 was highest in ; in age group 13-18, the highest ER visits occurred in [Figure 5-1]. The inpatient hospitalization rates with asthma as the primary discharge diagnosis were highest in among ages However, in age group 0-5, the highest rates were observed in [Figure 5-3]. During , ER visit and inpatient hospitalization rates with asthma as the primary discharge diagnosis were highest among ages 0-5, followed by the 6-12 and age groups [Figure 5-1 and Figure 5-3]. For the entire six-year period, ER visit and inpatient hospitalization rates with asthma as the primary discharge diagnosis were higher in the Southeast Health District than in other districts [Figure 5-2 and Figure 5-4]. 6
14 In , among males aged 0-5, the percentage of those who received appropriate long-term control medications was higher than among females of the same age. In , in the same age group, the percentage of those who received appropriate long-term control medications was higher among females than among males. In , among children in age group 13-18, the percentage of those who received appropriate long-term control medications was higher among females than among males [Figure 5-5]. The Northcentral and Northeast Health Districts had the highest percentage of children taking long-term control medications. The southeast district accounts for the lowest rates [Figure 5-6]. Bradford, Lackawanna and Clearfield counties had the highest percentage of children taking long-term control medications. Montour, Greene and Perry counties had the lowest percent age of children taking long-term control medications [Table 5-3]. However, more data is required to make stronger conclusions. Executive Summary Asthma Mortality in Pennsylvania Overall, the age-adjusted mortality rates with asthma as the underlying cause of death dropped approximately 36 percent from 2000 to 2009 [Figure 6-1]. During , the age-adjusted mortality rates with asthma as the underlying cause of death were significantly higher among blacks, compared to whites. However, rates decreased among blacks by nearly 24 percent from 1998/2000 to 2007/2009 [Figure 6-2]. During , the age-adjusted asthma mortality rates with asthma as the underlying cause of death among females were significantly higher than among males. However, rates decreased among females and males from 1998/2000 to 2007/2009 (25 percent and 18 percent, respectively) [Figure 6-3]. Between , the highest age-specific asthma mortality rates with asthma as the underlying cause of death occurred among adults ages 70 years and older. The lowest age-specific asthma mortality rates occurred among adults ages [Table 6-1]. In , the age-adjusted mortality rate with asthma as the underlying cause of death was the highest in Monroe County (2.5 deaths per 100,000 population) and Philadelphia (2.5 per 100,000 population), compared to other counties [Figure 6-4]. Outdoor Air Quality In 2010, there were a number of unhealthy days at two Pennsylvania locations in particular, Pittsburgh and Philadelphia (10 days and 3 days, respectively). An elevated level of pollutants occurred most commonly near and downwind of major cities. 5 Unhealthy days mainly occur from May through September. The number of days when fine particle concentrations were unhealthy for sensitive groups, such as asthmatics, was greatest in the Pittsburgh area, less in smaller-sized cities of the state, and lowest in rural areas. The frequency of unhealthy fine particle days per year in Pittsburgh tended to decline over the period from 2000 to

15 Conclusions: The findings suggest the need for coordinated efforts at the local and state level, as well as support of preventive measures that can improve asthma health outcomes and access to health services. Effective preventive measures include promoting appropriate medical care, asthma self-management training, physical activity, appropriate use of inhaled corticosteroids to prevent symptoms and attacks, and avoidance of environmental allergens and irritants. To ensure access to appropriate health services, there must be recognition of specific needs associated with such factors as language, culture, age, gender, literacy, income and level of education. Section 1: Pennsylvania Population and Economic Statistics Pennsylvania ranks as the sixth largest state in United States, with an estimated population of 12,702,380 in There are 67 counties with 2,575 municipalities. Allegheny and Philadelphia Counties combined account for 21 percent of the population. There are 500 school districts in Pennsylvania. Pennsylvania also has one of the largest rural populations of any state in the United States of America. There are six community health districts, 10 local health departments, and a state health department located in Harrisburg, the capital city of Pennsylvania. Pennsylvania s population has increased in 2010 by approximately 420,000 people (3.4 percent) compared to Forest, Pike and Monroe are the counties with the biggest increases [Figure 1-1]. Figure 1-1: Decennial Population Percent Change, PA Section 1: Pennsylvania Population and Economic Statistics 8

 over the past 10 years, the percent of the elderly in comparison to the total Pennsylvania population actually declined slightly from 15.6 in 2000 to 15.4 in 2010.")
16 According to the 2010 U.S. Census Bureau, Pennsylvania s population continues to age. The population under 18 declined 4.5 percent, and the population 18 and older increased 5.9 percent from 2000 to The population age 62 and older has increased 7.7 percent since Pennsylvania s population has the 4th highest proportion of people 65 and older in the United States. While the size of the population age 65 and older increased by more than 40,000 Section 1: Pennsylvania Population and Economic Statistics (2.1 percent) over the past 10 years, the percent of the elderly in comparison to the total Pennsylvania population actually declined slightly from 15.6 in 2000 to 15.4 in There have been large increases in the population age 62 to 64 (43.2 percent) from 2000 to The median age rose from 38.0 years in 2000 to 40.1 years (5.5 percent) in 2010 [Table 1-1]. Table 1-1: Demographic Profile by Age, PA Data Source: U.S. Census Bureau, Pennsylvania State Data Center Pennsylvania s racial and ethnic composition is growing more diverse. In 2010, the Asian population had increased by 58.8 percent over the previous decade, while the American Indian and Alaska Native population had increased by 46.3 percent and the black or African-American population had increased by 12.5 percent. Pennsylvania s white population declined 0.7 percent during the decade [Table 1-2 and Figure 2-2]. Table 1-2: Demographic Profile by Race, PA Data Source: U.S. Census Bureau, Pennsylvania State Data Center 9
, followed by Cuban (73.0 percent) and Puerto Rican (60.2 percent).")
17 In 2010, Pennsylvania s Hispanic population had increased to 719,660 (almost 82.6 percent) compared to Each of the specific Hispanic origin groups in Pennsylvania increased from 2000 to The largest increase was in the population of Mexican origin (134.8 percent), followed by Cuban (73.0 percent) and Puerto Rican (60.2 percent). All of Pennsylvania s minority groups grew from 2000 to Figure 1-2: Decennial Minority Population Percent Change, PA According to the Census Bureau s 2010 American Community Survey (ACS), Pennsylvania residents of age 45 to 64 had a median household income of $61,185. That compares with $55,726 for ages 25 to 44 and $31,364 for ages 65 and older. Chester County had the highest median household income ($84,741), followed by Montgomery ($76,380) and Bucks ($74,828) counties. Cumberland County ($60,219) had the highest median household income outside of Southeastern Pennsylvania. Fayette County had the lowest median household income ($34,796), followed by Forest ($35,150) and Sullivan ($36,250) counties. All income estimates from the ACS have been inflation-adjusted to 2010 dollars. According to the Pennsylvania State Data Center, during the period , more than three times as many Pennsylvania children living below the federal poverty threshold resided in single parent families, as opposed to married-couple families. In , a total of 161,886 (33.5 percent) of single parent families with related children lived in poverty, compared to 49,307 (4.9 percent) of married-couple families with related children. Overall, during the period , a total of 211,193 (14.2 percent) of Pennsylvania families with related children had incomes below the federal poverty level. Section 1: Pennsylvania Population and Economic Statistics 10
 with 27.6 percent [Table 1-3].")
18 Philadelphia County had both the highest number and percent of families with related children living below the poverty level with 47,485 (29.0 percent). Fayette County followed (in terms of the highest proportion of families with children living in poverty) with 27.6 percent [Table 1-3]. Bucks County had the lowest percent of families with related children living in poverty (5.1 percent) followed by Chester (5.5 percent), Montgomery (5.6 percent) and Cumberland (6.4 percent) counties. Table 1-3: Poverty Status in the Past 12 Months by Family Type and Presence of Related Children, PA counties: (Top 10) Section 1: Pennsylvania Population and Economic Statistics Data Source: U.S. Census Bureau, Pennsylvania State Data Center According to U.S. Census Bureau, and the Pennsylvania State Data Center, in 2010, approximately 1,271,180 Pennsylvanians (10.2 percent) lacked health insurance. Nationwide, 15.5 percent of Americans were without health insurance coverage in
19 Section 2: Asthma Prevalence Asthma prevalence measures all individuals who are affected by asthma within a particular time period. It is the percentage of people who have asthma from the total group exposed. This section presents information on asthma prevalence in certain subpopulations. Lifetime asthma prevalence is the percentage of people who have had asthma at some point in their life. Current asthma prevalence is the percentage of people who currently have asthma. A 12-month time period is often used in conjunction with current asthma prevalence. Knowledge about asthma prevalence helps health professionals understand the probability of asthma and describes the asthma burden on a given population. The only available source for the Pennsylvania Asthma Control Program is the Pennsylvania Behavioral Risk Factor Surveillance System (PA BRFSS) which provides the PA ACP with lifetime and current asthma prevalence data. These data were provided by the Bureau of Health Statistics and Research, Pennsylvania Department of Health. PA BRFSS is a state-based system of health surveys that collects information on health risk behaviors, preventive health practices and health care access that are primarily related to chronic disease and injury. One of the surveys, the PA Asthma Call-back Survey, is unique to PA BRFSS and asthma. Data were collected by telephone interviews for adults (18+) and children (0-17). Data for children were based on information provided by an adult respondent about their children living at home. Information obtained from questions in the 2010 survey about adult and child asthma history, such as emergency room or urgent treatment and/or routine checkup visits, frequency of asthma attacks and asthma symptoms, activity limitations, sleep difficulties, and percentage of adults taking prescribed preventive asthma medications and prescribed asthma inhalers, all help the PA ACP to find the best ways to describe the burden of asthma and better understand health discrepancies in different groups of the population. Due to small sample size, descriptive information regarding children is limited. Analysis at a sub-state level and for some race/ethnicity groups is also limited due to sample size. For those indicators that regularly appear on the questionnaire, three years of data were combined to produce estimates for the Pennsylvania Health Districts and select regions. In 2010, the annual prevalence estimate of lifetime asthma among adults in Pennsylvania was 13.8 percent, or approximately 1,367,000 people; the annual prevalence estimate of current asthma among adults in Pennsylvania was 9.9 percent, or approximately 981,000 people. There are some limitations to the data: data are self-reported and subject to recall difficulties and misrepresentation. People excluded from the survey were those without telephones, those with only cell phones (through 2009), those living in nursing homes, prisons, other institutions or dormitories, and adults in the military service. Response rates for PA BRFSS and all telephone surveys have been declining in recent years, making non-response bias a possible concern. Section 2: Asthma Prevalence 12

20 Asthma Prevalence in Pennsylvania vs. U.S. Figure 2-1: Adult Self-Reported Lifetime Asthma Prevalence Rate (Percent), PA vs. U.S., BRFSS Section 2: Asthma Prevalence Data Source: The National Behavioral Risk Factor Surveillance System (BRFSS) Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. In general, during the 10-year period of , the annual prevalence estimate of lifetime asthma among adults in both Pennsylvania and the U.S. has significantly increased. Comparing 2001 to 2010, Pennsylvania rates increased 29 percent, while in the U.S., rates increased 23 percent. The prevalence of lifetime asthma among adults in Pennsylvania was lower than the U.S. until 2006, generally increasing to higher than U.S. rates from 2007 to However, between 2007 and 2010 there were no statistically significant differences in the prevalence of asthma among adults in Pennsylvania vs. adults in the U.S. 13
, PA vs. U.S.")
21 Figure 2-2: Adult Self-Reported Current Asthma Prevalence Rate (Percent), PA vs. U.S., BRFSS Data Source: The National Behavioral Risk Factor Surveillance System (BRFSS) Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. During the 10-year period of , the annual prevalence estimate of current asthma among adults in Pennsylvania was higher than the U.S. until 2009, becoming significantly higher compared to the U.S. in The annual prevalence estimate of current asthma among adults in Pennsylvania and the U.S. has significantly increased from 2001 to 2010 (approximately 35 percent in Pennsylvania and approximately 19 percent in the U.S.). Section 2: Asthma Prevalence 14
 Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval.")
22 Section 2: Asthma Prevalence Figure 2-3: Adult Self-Reported Lifetime Asthma Prevalence Rate (Percent) by Sex, PA vs. U.S., BRFSS Data Source: The National Behavioral Risk Factor Surveillance System (BRFSS) Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. Figure 2-4: Adult Self-Reported Current Asthma Prevalence Rate (Percent) by Sex, PA vs. U.S., BRFSS In Pennsylvania and the U.S. between 2006 and 2010, the lifetime prevalence among adult females was consistently and significantly higher than adult males. There were no statistically significant differences in the asthma prevalence estimate trend among females and males from year to year, either in Pennsylvania or in the U.S. The biggest gap in lifetime prevalence between females and males occurred in both Pennsylvania and in the U.S. in 2006 (almost 88 percent and 37 percent, respectively). In 2010, the lifetime prevalence for adult males in Pennsylvania and in the U.S. increased significantly compared to 2006 (11.7 percent vs. 8.4 percent in Pennsylvania and 11.7 percent vs percent in the U.S.). There was no significant increase of the lifetime prevalence among adult females in Pennsylvania or in the U.S. through In Pennsylvania and the U.S. between 2006 and 2010, the current prevalence among females was significantly and consistently higher compared to males. There was no significant increase of the current prevalence among adult females and adult males in Pennsylvania or in the U.S. through Data Source: The National Behavioral Risk Factor Surveillance System (BRFSS) Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval.
 by Race, PA vs. U.S.")

23 Figure 2-5: Adult Self-Reported Lifetime Asthma Prevalence Rate (Percent) by Race, PA vs. U.S., BRFSS Data Source: The National Behavioral Risk Factor Surveillance System (BRFSS) Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. Figure 2-6: Adult Self-Reported Current Asthma Prevalence Rate (Percent) by Race, PA vs. U.S., BRFSS From 2006 to 2010, the consistent trend over time showed significant discrepancies of the lifetime prevalence among adult whites and blacks in the U.S. for each year. In Pennsylvania, lifetime prevalence among adult blacks was higher in 2006, 2007, 2009 and 2010; and significantly higher in 2008 compared to adult whites. In 2010, the lifetime prevalence for adult blacks in Pennsylvania slightly decreased compared to 2006 (16.1 percent vs percent) and increased for adult whites (11.7 percent vs percent). Between , there were significant differences in the current prevalence among adult blacks and whites in the U.S. In Pennsylvania, current prevalence among adult blacks was significantly higher in 2008 and higher in 2006, 2007, 2009 and In 2010, the current prevalence for adult blacks in Pennsylvania decreased approximately 10 percent and increased for adult whites nearly 13 percent compared to Section 2: Asthma Prevalence Data Source: The National Behavioral Risk Factor Surveillance System (BRFSS) Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. 16
 Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval.")

24 Section 2: Asthma Prevalence 17 Figure 2-7: Child Lifetime Asthma Prevalence Rate (Percent) by Sex, PA vs. U.S., BRFSS Data Source: The National Behavioral Risk Factor Surveillance System (BRFSS) Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. Figure 2-8: Child Current Asthma Prevalence Rate (Percent)by Sex, PA vs. U.S., BRFSS Data Source: The National Behavioral Risk Factor Surveillance System (BRFSS) Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. During the five-year period of , in Pennsylvania, the child lifetime prevalence among males was significantly higher than females in 2008 and From 2006 to 2010 in the U.S., there were statistically significant differences in the asthma prevalence estimate among males and females. In Pennsylvania, the child lifetime prevalence among males was on the rise from 14.3 percent in 2006 to 18.6 percent in Among females, the percentage of children with lifetime prevalence varied from year to year. There is a significant difference in the estimated prevalence among males in Pennsylvania compared to the U.S. in During the five-year period of , in Pennsylvania, the child current asthma prevalence among males was higher than females every year and was significantly higher in Since 2007, the child current asthma prevalence has been higher among both males and females in Pennsylvania compared to the U.S. Generally, in Pennsylvania, the child current asthma prevalence among males increased from 2006 to 2010 by approximately 30 percent and decreased by almost 7 percent among females. In the U.S., a comparison of the rates between 2006 and 2010 shows a decrease among males of approximately 3 percent and of 4 percent among females.
 Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the")
 Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the Between 2006 and")
25 Figure 2-9: Child Lifetime Asthma Prevalence Rate (Percent) by Race, Pennsylvania vs. U.S., BRFSS Data Source: The National Behavioral Risk Factor Surveillance System (BRFSS) Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. Data Source: The National Behavioral Risk Factor Surveillance System (BRFSS) Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. Between 2006 and 2010 in Pennsylvania and the U.S., the child lifetime asthma prevalence among blacks was significantly higher than among whites, except in 2009 in Pennsylvania. In Pennsylvania, the child lifetime asthma prevalence among blacks increased from 2006 to 2007 approximately 33 percent and decreased by 2010 approximately 23 percent. In Pennsylvania, among whites, the percentage of children with lifetime asthma prevalence varied from year to year; there were no annual statistically significant differences in the asthma prevalence estimate. In addition, there were no significant differences in the estimated annual child lifetime asthma prevalence among blacks and whites for Pennsylvania compared to the U.S. Figure 2-10: Child Current Asthma Prevalence Rate (Percent) by Race, Pennsylvania vs. U.S., BRFSS In Pennsylvania and the U.S., the child current asthma prevalence among blacks was significantly higher than whites between 2006 and 2010, except for Pennsylvania in 2006 and In Pennsylvania, the child current asthma prevalence among blacks and whites increased in 2010 compared to 2006 (about 19 percent in blacks and 11 percent in whites). Generally, in the U.S., the child current asthma prevalence among blacks and whites decreased in 2010 compared to 2006 (approximately 4 percent in blacks and 11 percent in whites). There were no significant differences in the estimated annual child current asthma prevalence among blacks and whites in Pennsylvania compared to the U.S. Section 2: Asthma Prevalence 18
 CI denotes confidence interval.")

26 Asthma Prevalence in Pennsylvania Table 2-1: Lifetime Asthma Prevalence Among Pennsylvania Residents by Age Group: PA BRFSS Section 2: Asthma Prevalence Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) CI denotes confidence interval. Among children in Pennsylvania between 2006 and 2010, there were no significant differences in the estimated annual child lifetime asthma prevalence in age groups, except for the age group in 2008 compared to In 2008 and 2010, there were significant differences in the estimated child lifetime asthma prevalence in the age group compared to some other age groups. In 2006, 2007 and 2010, the estimated lifetime asthma prevalence among adults (18+) was significantly higher in age groups compared to other adult age groups. Table 2-2: Current Asthma Prevalence Among Pennsylvania Residents by Age Group: PA BRFSS Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) CI denotes confidence interval. Between 2006 and 2010, there were no significant differences in the estimated annual child current asthma prevalence in age groups among children (0-17) for Pennsylvania. In 2007, the current asthma prevalence among adults (18+) was significantly higher in the age group compared to other age groups. 19


27 Table 2-3: Current Asthma Prevalence Among Adults by Education Attainment, PA BRFSS Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) CI denotes confidence interval. In 2006 and 2010, the current asthma prevalence among adults with less than a high school education was significantly higher than among adults that graduated from high school. Between 2007 and 2009, the current asthma prevalence among adults was higher among people with less than a high school education, compared to people that graduated from high school and college. It seems that educational level is one of the contributing factors which may be related directly or indirectly to current asthma prevalence among adults. Table 2-4: Self-Reported Current Asthma Prevalence Among Adults by Income, PA BRFSS Section 2: Asthma Prevalence Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) CI denotes confidence interval. Between 2006 and 2010, the current asthma prevalence among adults was significantly higher among people with an income level of less than $15,000, compared to an income level of $50,000 and higher (except in 2007). It seems that income level is one of the contributing factors which may be related directly or indirectly to current asthma prevalence among adults. 20
 CI denotes confidence interval.")
28 Table 2-5: Self-Reported Current Asthma Prevalence Among Adults by Selected Characteristics, PA BRFSS Section 2: Asthma Prevalence Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) CI denotes confidence interval. The current asthma prevalence among adults with BMI GE 30 was significantly higher compared to adults with 25 LE BMI LT 30 and Neither Overweight nor Obese in 2006, 2009 and It seems that the BMI level is related to current asthma prevalence among adults. In 2007 and 2009, the current asthma prevalence among adults who were Current Smokers was significantly higher than adults who Never Smoked. However, data are not sufficient to make concrete conclusions in terms of current asthma prevalence among adults according to their smoking status; more data are required to make an accurate analysis. 21

29 Figure 2-11: Adult Self-Reported Current Asthma Prevalence Rate (Percent) by Health District, PA BRFSS Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. There were no significant differences in the estimated current asthma prevalence among people in Pennsylvania health districts in and , except in the northcentral. In Pennsylvania, the highest current asthma prevalence in was observed in the Southeast Health District, and the Northcentral Health District had the highest prevalence in However, data are not sufficient to make concrete conclusions in terms of current asthma prevalence among adults according to their smoking status; more data are required to make an accurate analysis. Section 2: Asthma Prevalence 22
 Vertical bars on the graph denote the 95% confidence interval.")

30 Asthma Management and Quality of Life in Pennsylvania Figure 2-12: Percentage of Adults With Asthma Who Had Asthma Episode or Attack in Past Year, 2010 BRFSS Section 2: Asthma Prevalence Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. The question asked of the respondent was: During the past 12 months, have you had an episode of asthma or an asthma attack? Figure 2-13: Percentage of Adults With Asthma Attacks Who Visited an ER or Urgent Care Facility For Asthma in Past Year, PA 2010 BRFSS Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. 23 The question asked of the respondent was: During the past 12 months, how many times did you visit an emergency room or urgent care center because of your asthma?
 Vertical bars on the graph denote the 95% confidence interval.")

31 Figure 2-14: Percentage of Adults With Asthma Attacks Who Visited Health Professional for Worsening Asthma Symptoms in Past Year, PA 2010 BRFSS Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. The question asked of the respondent was: During the past 12 months, how many times did you see your doctor, nurse or other health professional for urgent treatment of worsening asthma symptoms? Figure 2-15: Percentage of Adults With Asthma Who Visited Health Professional for Routine Treatment of Asthma in Past Year, PA 2010 BRFSS Section 2: Asthma Prevalence Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. The question asked of the respondent was: During the past 12 months, how many times did you see your doctor, nurse or other health professional for a routine checkup for your asthma? 24
 Vertical bars on the graph denote the 95% confidence interval.")
32 Figure 2-16: Percentage of Adults With Asthma Unable to Work or Do Usual Activities Due to Asthma in Past Year, PA 2010 BRFSS Section 2: Asthma Prevalence Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. The question asked of the respondent was: During the past 12 months, how many days were you unable to work or carry out your usual activities because of your asthma? Figure 2-17: Percentage of Adults With Asthma Who Had Asthma Symptoms Every Day in Past 30 Days, PA 2010 BRFSS Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. The question asked of the respondent was: During the past 30 days, how often did you have any symptoms of asthma? 25
 Vertical bars on the graph denote the 95% confidence interval.")

33 Figure 2-18: Percentage of Adults With Asthma Symptoms Who Had 5+ Days Sleep Difficulty Due to Asthma Symptoms in Past 30 Days, PA 2010 BRFSS Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. The question asked of the respondent was: During the past 30 days, how many days did symptoms of asthma make it difficult for you to stay asleep? Figure 2-19: Percentage of Adults With Asthma Who Used Prescription Asthma Meds to Prevent Attack 25+ Days in Past 30 Days, PA 2010 BRFSS Section 2: Asthma Prevalence Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. The question asked of the respondent was: During the past 30 days, how often did you take a prescription asthma medication to prevent an asthma attack from occurring? 26
 Vertical bars on the graph denote the 95% confidence interval.")
34 Figure 2-20: Percentage of Adults With Asthma Who Used Prescription Asthma Inhaler During Attack 5+ Times in Past 30 Days, PA 2010 BRFSS Section 2: Asthma Prevalence Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. The question asked of the respondent was: During the past 30 days, how often did you use a prescription asthma inhaler during an asthma attack to stop it? Figure 2-21: Percentage of Adults With Asthma Told Had Asthma At Age Less Than 10, PA 2010 BRFSS 27 Data Source: Pennsylvania Behavioral Risk Factor Surveillance System (BRFSS) Vertical bars on the graph denote the 95% confidence interval. The question asked of the respondent was: How old were you when you were first told by a doctor, nurse or other health professional that you had asthma?
35 Section 3: Asthma Hospitalization in Pennsylvania The Pennsylvania Health Care Cost Containment Council (PHC4) is the primary source of asthma hospitalization data in Pennsylvania. PHC4 collects data from Pennsylvania hospitals, including data concerning asthma as the primary discharge diagnosis (ICD-9 code ), such as inpatient and outpatient discharge data. The analysis in this report provides information about the number and rate of hospital admissions for people with asthma, trends over the last decade, length of stay, hospital charges, sources of payment, admission type, and more detailed data by patient age, gender and race/ethnicity. This section represents an analysis at the statewide and region/county levels and further represents the burden of asthma from The analysis is based on Pennsylvania residents who were admitted to any non-federal Pennsylvania hospital with asthma as the primary discharge diagnosis. Out-of-state residents hospitalized in Pennsylvania were excluded. Data was analyzed using SAS and Excel. Age-adjusted rates were adjusted to the 2000 US standard population via the direct method. Crude rates were calculated using PHC4 hospitalization data and U.S. Census population estimates for Pennsylvania, per 10,000 PA residents. Analyzing hospital admissions for asthma is critical for determining the efforts necessary to implement improvements in the quality of care for people with asthma. Reduction of Emergency Room (ER) visits, effective outpatient care and appropriate disease management can potentially decrease the need for asthma hospitalizations. To produce more reliable results the sample size and asthma hospitalization data were combined and aggregated for eight-year and five-year block periods. The number of inpatient hospitalizations with asthma as the primary discharge diagnosis declined from 24,959 in 2003 to 21,061 in In 2010, the asthma hospitalization rate for Pennsylvania s residents decreased approximately 14.4 percent from 2009 (16.6 per 10,000 vs. 19.4). Section 3: Asthma Hospitalization in Pennsylvania 28
 Vertical bars on the graph denote the 95% confidence interval.")
 In 2006-2010, inpatient hospitalization rates among children with asthma as the primary discharge diagnosis were significantly higher compared to adults (by approximately 20 percent to 50")
36 Figure 3-1: Rates of Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis among Children and Adults, PA Section 3: Asthma Hospitalization in Pennsylvania 29 Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) Vertical bars on the graph denote the 95% confidence interval. Figure 3-2: Trends of Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis by Race and Ethnicity, PA Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) In , inpatient hospitalization rates among children with asthma as the primary discharge diagnosis were significantly higher compared to adults (by approximately 20 percent to 50 percent depending on the year). Generally, the hospitalization rates for children decreased from 2006 (24.1 per 10,000) to 2010 (22.4). The highest rate for children, however, was in 2009 (24.8 per 10,000) and the lowest in 2008 (21.5). Among adults the highest rate was in 2008 (18.5 per 10,000) and the lowest in 2010 (14.9). During , the asthma hospitalization rates increased from 2001 to 2003 among whites, blacks, Hispanic and non-hispanic groups. Overall, from 2003 to 2010, asthma hospitalization rates significantly decreased. During , there were significant reductions in asthma hospitalization rates among black and Hispanic populations. During , the highest hospitalization rates with asthma as the primary discharge diagnosis among whites, blacks, Hispanic and non-hispanic groups were in 2003 (13.4; 61.8; 47.3; and 19.5 per 10,000, respectively) and lowest in 2010 (10.5; ; 27.7; and 16.0 per 10,000, respectively). During , the highest hospitalization rates with asthma as the primary discharge diagnosis were among blacks, and the lowest among whites.
 Vertical bars on the graph denote the 95% confidence interval.")
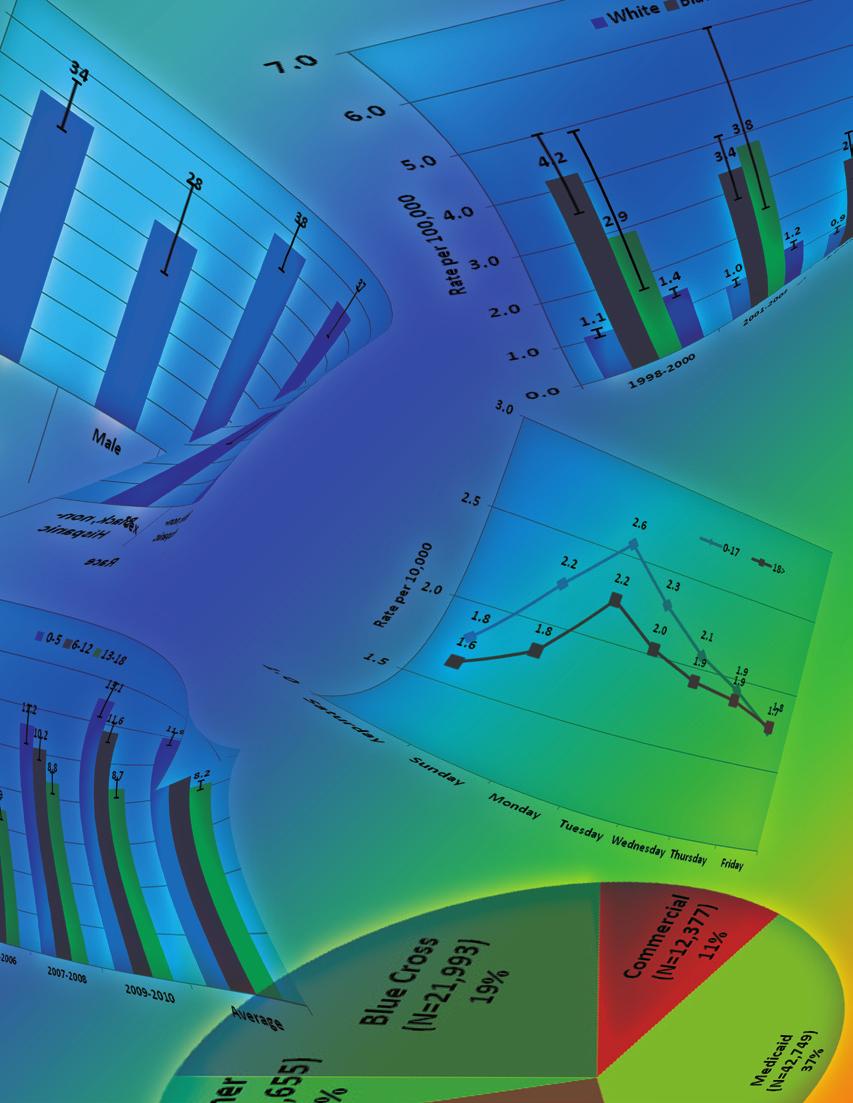
37 Figure 3-3: Rates of Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis by Age Group and Gender, PA (Combined Data) Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) Vertical bars on the graph denote the 95% confidence interval. In , age-adjusted inpatient hospitalization rates for asthma as the primary discharge diagnosis were significantly higher in children aged 0-4 (females 34.0 and males 56.5 per 10,000), while the lowest rates were among the age group (females 10.6 and males 5.3 per 10,000). Males younger than 15 years of age had significantly higher rates compared to females. For age groups 15 years and older, females had significantly higher rates compared to males. Generally, the highest rate for the five-year period was observed in age group 0-4, followed by the 65+ age group and (45.5, 27.2 and 18.3 per 10,000, respectively). Figure 3-4: Distribution of the Primary Payers for Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis, PA (Combined Data) During , Medicaid remained as the major payer in Pennsylvania and accounted for approximately 37 percent of the total hospitalization charges. Medicare accounted for roughly 29 percent of the total hospitalization charges. Nearly 34 percent of the total hospitalization charges were paid by Blue Cross, Commercial and other insurances. Section 3: Asthma Hospitalization in Pennsylvania Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) Note: Definitions of primary payers are in Section Glossary of Terms. 30


38 Figure 3-5: Distribution of the Admission Types for Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis, PA (Combined Data) During , approximately 74 percent of all admissions due to asthma as the primary discharge diagnosis entered hospitals through the ER. Around 23 percent of all admissions entered hospitals urgently, and nearly 3 percent were admitted electively. It seems that reducing the number of ER visits may lead to improving the quality of life of people with asthma and save millions of dollars. Section 3: Asthma Hospitalization in Pennsylvania Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) Note: Definitions of types of asthma are in Section Glossary of Terms. Figure 3-6: Average Charges per Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis among Children and Adults (does not include professional fees), PA Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) In , the average charges for inpatient hospitalization with asthma as the primary discharge diagnosis were higher among adults compared to children (by approximately 50 to 90 percent). Overall, average charges were on the rise. In 2006, the average charge per stay in the hospital due to asthma was $18,765; the amount rose to $23,383 by 2010 (increasing approximately 24 percent). In , the charges for children rose from $11,863 to $16,757 (approximately 41 percent) and for adults from $21,591 to $26,184 (approximately a 21 percent rise). 31
 Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) Figure 3-8: Asthma Age-Adjusted Rates for Inpatient Hospitalizations with Asthma as the Primary")
. The lowest rates among children were on Fridays (1.")
39 Figure 3-7: Rates of Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis among Children and Adults admitted to the Hospital through the Emergency Room (ER) by Day of the Week, PA (Combined Data) Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) Figure 3-8: Asthma Age-Adjusted Rates for Inpatient Hospitalizations with Asthma as the Primary Discharge Diagnosis by Health District, PA Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) During , rates of inpatient hospitalization with asthma as the primary discharge diagnosis through the ER among children and adults were highest on Mondays (2.6 and 2.2 per 10,000, respectively). The lowest rates among children were on Fridays (1.7 per 10,000), and among adults, the lowest were on Saturdays (1.6 per 10,000). It seems that rates began to rise on Sunday for children and adults, reaching a peak on Monday, then decreasing through Friday or Saturday. Overall, during , the highest age-adjusted inpatient hospitalization rate for asthma as the primary discharge diagnosis was in the Southeast Health District (25.3 in 2008; 26.2 in 2009; and 22.1 in 2010 per 10,000), followed by the Southwest Health District (20.9; 19.5; and 18.1 per 10,000, respectively) and then the Northeast Health District (16.2, 16.0 and 13.7 per 10,000, respectively). Overall, ageadjusted inpatient hospitalization rates for asthma as the primary discharge diagnosis in 2010 have decreased 13.5 percent since 2008 (16.6 vs per 10,000, respectively). Section 3: Asthma Hospitalization in Pennsylvania 32
 In 2006-2010, the average LOS for inpatient hospitalization with asthma as the primary discharge diagnosis for all selected characteristics has not changed")

40 Table 3-1: Average Length of Stay (LOS) and Average Charges per Day in the Hospital Due To Asthma, PA Section 3: Asthma Hospitalization in Pennsylvania Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) In , the average LOS for inpatient hospitalization with asthma as the primary discharge diagnosis for all selected characteristics has not changed significantly from year to year. Children stayed in hospitals half the time that adults did. Males, non-hispanic blacks, and Hispanics spend much less time in hospitals compared to females, non-hispanic whites and non-hispanics. Average charges per day were higher among children compared to adults, among males compared to females, among non-hispanic blacks compared to non-hispanic whites, and among Hispanics compared to non-hispanic groups. Table 3-2: Number and Percentage of Inpatient Hospitalizations with Asthma as the Primary Discharge Diagnosis through the Emergency Room (ER), PA Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) 33 In , there was a significant decrease in the percentage of hospitalizations admitted through the ER from 2006 to 2010 (78.3 to 57.0 percent) among children. The same trend occurred among males (78.7 to 68.2 percent), females (77.2 to 74.8 percent), non-hispanics blacks (91.4 to 79.2 percent), Hispanics (85.5 to 43.6 percent) and non-hispanics (77.2 to 75.2 percent). However, the percentage of adults and non-hispanics whites who entered hospitals through the ER slightly increased in 2010, compared to 2006.
 Between 2008 and 2010, the total charges for inpatient hospitalization with asthma as the primary discharge diagnosis, including total charges for")

41 Table 3-3: Total Charges for Inpatient Hospitalization with Asthma as Primary Discharge Diagnosis, including Total Charges for Admission through Emergency Room, PA Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) Between 2008 and 2010, the total charges for inpatient hospitalization with asthma as the primary discharge diagnosis, including total charges for admission through the ER, decreased for all selected categories, except children and males. Overall in Pennsylvania, total charges in 2010 decreased approximately 6 percent compared to 2008 and nearly 12 percent compared to There is no significant percentage change in the total charges for admission through the ER that occurred in among selected groups, with the exception of the Hispanic population, for whom total charges for admission through the ER accounted for nearly 60 percent of total charges in 2008 and almost 50 percent in The amount of total charges varies; however, the percentage of the total charges for admission through the ER remains almost the same. Table 3-4: Number of Admissions, Length of Stay (LOS) and Average Charges per Inpatient Hospitalization with Asthma as Primary Discharge Diagnosis by Type of Asthma, PA Section 3: Asthma Hospitalization in Pennsylvania Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) Note: Definitions of types of asthma are in Section Glossary of Terms. In 2010, the average charge per hospitalization for patients with asthma as the primary discharge diagnosis increased compared to In , the highest charge per hospitalization was for chronic obstructive asthma, due to number of days spent in hospitals. In 2009 and 2010, time spent in hospitals compared to 2008 decreased for all types of asthma with one exception -- for Other and Unspecified. Overall, from 2008 to 2010, the number of admissions decreased for all types of asthma with the exception of Extrinsic and Intrinsic type of asthma. 34
 Figure 3-10: Total Charges for Inpatient Hospitalization with Asthma as the Primary Discharge")

42 Figure 3-9: Average Charges for Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis by Health District (does not include professional fees), PA Section 3: Asthma Hospitalization in Pennsylvania Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) Figure 3-10: Total Charges for Inpatient Hospitalization with Asthma as the Primary Discharge Diagnosis by Health District (does not include professional fees), PA Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) During , average charges for inpatient hospitalization for asthma as the primary discharge diagnosis were highest in the Southeast Health District, followed by the Northeast Health District. Overall, in Pennsylvania, the average charges for inpatient hospitalization in 2010 increased since 2006 by approximately 24 percent ($18,765 vs. $23,383). During , total charges were highest in the Southeast Health District. The Southeast Health District, representing approximately 40 percent of the Pennsylvania population, accounts for almost 70 percent of total charges in the state. In Pennsylvania, total charges decreased by about $63 million, from $555 million in 2009 to $492 million in
 Overall, between 2008 and 2010, total charges per hospitalization for patients with asthma as the primary discharge diagnosis")
 and Average Charges per Hospitalization for Patients with Asthma as the Primary Discharge Diagnosis (does not include professional")
43 Table 3-5: Number of Visits, Length of Stay (LOS) and Average Charge per Visit for Ambulatory/Outpatient Visits with Asthma as the Primary Discharge Diagnosis by Type of Asthma, PA Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) Overall, between 2008 and 2010, total charges per hospitalization for patients with asthma as the primary discharge diagnosis increased. In , the highest number of admissions and largest charge per asthma hospitalization were for Other and Unspecified type of asthma. Table 3-6: Number of Patient Readmissions, Length of Stay (LOS) and Average Charges per Hospitalization for Patients with Asthma as the Primary Discharge Diagnosis (does not include professional fees), PA Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) In , despite differences in number of patients, the percentage of patient admissions and readmissions to hospitals due to asthma remained the same. The length of stay (LOS) varies and was higher in second, third and fourth admissions compared to the rest. In general, in 2010, average charges per hospitalization for patients with asthma as the primary discharge diagnosis increased from 2008 levels in all categories but one, which was for people admitted a fourth time. Section 3: Asthma Hospitalization in Pennsylvania 36
 Section 3: Asthma Hospitalization in Pennsylvania Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) During 2006-2010, more than 95 percent of all admissions in Allegheny")
44 Table 3-7: Number and Percentage of Inpatient Hospitalizations with Asthma as the Primary Discharge Diagnosis Entering the Hospital through the Emergency Room (ER) by Region, PA (Combined Data) Section 3: Asthma Hospitalization in Pennsylvania Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) During , more than 95 percent of all admissions in Allegheny County among children with asthma as the primary discharge diagnosis were admitted into hospitals through the ER. The percentage was significantly higher compared to Philadelphia County and the rest of the state (59.6 vs. 61.8, respectively). However, the number of admissions among children in Philadelphia County (12.7 percent of the Pennsylvania child population ages 0-17) was almost equal to the total admissions of children in the rest of the Pennsylvania counties combined. Hospitalization rates among children were significantly higher in Philadelphia County compared to Allegheny County and the rest of the state (56.4 per 10,000 vs per 10,000 and 7.9 per 10,000, respectively). In Philadelphia County more than 94 percent of all admissions to the hospital among adults were admitted through the ER. The highest percentage of admissions and the highest asthma hospitalization rate (84 percent and 48.5 per 10,000) were among females who entered hospitals through the ER in Philadelphia County. Females in Allegheny County had a percentage of admission for asthma and hospitalization rate of 82.5 percent and 22.8, respectively, while the rest of the state was at 68.1 percent and 11.8 per 10,000, respectively. The highest percentage among males who entered hospitals through the ER was in Allegheny County (at 88.6 percent), compared to Philadelphia County and the rest of the state (71.6 percent vs percent, respectively). Overall, Allegheny County accounts for the highest percentage of all hospital admissions through the ER compared to Philadelphia County and the rest of the state (84.4 percent vs percent and 68.2 percent, respectively). However, asthma hospitalization rates were highest in Philadelphia County compared to Allegheny County and the rest of the state (41.0 per 10,000 vs per 10,000 and 9.2 per 10,000, respectively). 37

45 Figure 3-11: Inpatient Hospitalization Rates with Asthma as the Primary Discharge Diagnosis among Adults, PA Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) During , inpatient hospitalization rates for asthma as the primary discharge diagnosis were highest among adults in the following 10 out of 67 Pennsylvania counties: Cameron (72.0 per 10,000), Philadelphia (37.6), Lawrence (32.1), Westmoreland (25.0), Fayette (24.8), Beaver (21.7), Washington (21.6), Allegheny (21.4), Wyoming (20.6) and Carbon (20.2). Overall, for , inpatient hospitalization rates for asthma as the primary discharge diagnosis were 17.2 per 10,000 among adults. Section 3: Asthma Hospitalization in Pennsylvania 38
 Note: If numbers of admissions <60, the value does not count During 2003-2010, inpatient hospitalization rates for asthma as the primary discharge")
46 Figure 3-12: Inpatient Hospitalization Rates with Asthma as the Primary Discharge Diagnosis among Children, PA Section 3: Asthma Hospitalization in Pennsylvania Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) Note: If numbers of admissions <60, the value does not count During , inpatient hospitalization rates for asthma as the primary discharge diagnosis were highest among children in the following 10 out of 67 Pennsylvania counties: Philadelphia (92.5 per 10,000), Delaware (29.2), Susquehanna (22.8), Lawrence (21.7), Schuylkill (20.3), Allegheny (19.2), McKean (18.9), Indiana (18.7), Jefferson (17.2) and Monroe (16.8). Overall, for , inpatient hospitalization rates for asthma as the primary discharge diagnosis were 24.0 per 10,000 among children. 39

47 Figure 3-13: Inpatient Hospitalization Rates with Asthma as the Primary Discharge Diagnosis, PA (Overall) Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) During , overall inpatient hospitalization rates for asthma as the primary discharge diagnosis were highest among adults in the following 10 out of 67 Pennsylvania counties: Cameron (65.6 per 10,000), Philadelphia (51.1), Lawrence (29.8), Westmoreland (22.8), Fayette (22.3), Allegheny (21.0), Delaware (20.8), Beaver (19.6), Washington (19.2) and Indiana (19.0). Overall, for , inpatient hospitalization rates for asthma as the primary discharge diagnosis were 18.7 per 10,000. Section 3: Asthma Hospitalization in Pennsylvania 40
 Hispanics* can be any race During 2006-2010, the asthma inpatient hospitalization rates remain higher than the 2010 HP Objectives")
48 Table 3-8: Asthma Inpatient Hospitalization Rate per 10,000 Residents by Age Group Compared to the Healthy People (HP) 2010 Objectives, PA Section 3: Asthma Hospitalization in Pennsylvania Data Source: Pennsylvania Health Care Cost Containment Council (PHC4) Hispanics* can be any race During , the asthma inpatient hospitalization rates remain higher than the 2010 HP Objectives for all age groups/characteristics. Pennsylvania exceeded the HP 2010 targets for each of the age groups, except for white 0-4 and white 5-64 age groups. 41
49 Section 4: Asthma Lifetime Prevalence among Pennsylvania School Students Asthma is one of the leading causes of school absenteeism. Asthma is a leading chronic illness among children and youth in the United States. In 2007, it was reported that 5.6 million school-aged children and youth (5-17 years old) had asthma and that 2.9 million had experienced an asthma episode or attack within the previous year. 6 Data were obtained from the Pennsylvania Department of Health s Division of School Health database. All information in the database was submitted annually to the Department of Health by Pennsylvania s public school districts, comprehensive vocational-technical schools and charter schools. Data were not available by age, grade, sex or race. There are over 630 reporting school entities from all of the Pennsylvania s 67 counties and each of the state s six health districts. Students counted under this section have documentation (e.g., primary care provider notification, updated health history/physical exam form, medication order or formalized medically necessary plan of care) regarding the condition in his/her school health record within the past twelve months. A primary care provider is defined as a physician, physician assistant or certified registered nurse practitioner. The Department of Health s Division of School Health s report, entitled Students with Medical Diagnosis of Asthma by Health District and County, includes a count of the total number of students with a medical diagnosis of asthma, the average daily enrollment and the calculated percentage of students (K-12) with asthma. The data cover a 12-year period, beginning with the 1997/98 school year and extending through the 2008/09 school year. Due to problems with the validation process, school data for 2004/05 are missing. The data were aggregated by county, health district and specified school year, illustrating the asthma lifetime prevalence rates among school students in public and private/non-public schools. Section 4: Asthma Lifetime Prevalence among Pennsylvania School Students 42
, Division of School Health Note: the 2004-2005 School Year Data was not available from BCHS From the 1997/98 to the 2008/09 school year, the prevalence of asthma steadily increased")
50 Figure 4-1: Lifetime Asthma Prevalence among School Students, PA 1997/ /09 Section 4: Asthma Lifetime Prevalence among Pennsylvania School Students Data Source: Bureau of Community Health Systems (BCHS), Division of School Health Note: the School Year Data was not available from BCHS From the 1997/98 to the 2008/09 school year, the prevalence of asthma steadily increased every year (although 2004/05 school year data is not included). By the 2008/09 school year, lifetime asthma prevalence had increased almost 70 percent compared to 1997/98. In 1997/98 approximately 137,000 Pennsylvania school students in kindergarten through grade 12 were diagnosed with asthma; by 2008/09 that number had increased to more than 220,
, Division of School Health *Note: the 2004-2005 School Year Data is missing.")
51 Table 4-1: Lifetime Asthma Prevalence among School Students Health District and County, PA 2003/ /09 Data Source: Bureau of Community Health Systems (BCHS), Division of School Health *Note: the School Year Data is missing. Section 4: Asthma Lifetime Prevalence among Pennsylvania School Students 44
, Division of School Health *Note: the 2004-2005 School Year Data is missing. 45")
52 Table 4-1 (continued): Lifetime Asthma Prevalence among School Students by Health District and County, Pennsylvania 2003/ /09 Section 4: Asthma Lifetime Prevalence among Pennsylvania School Students Data Source: Bureau of Community Health Systems (BCHS), Division of School Health *Note: the School Year Data is missing. 45

53 Figure 4-2: Lifetime Asthma Prevalence Among School Students by Health District, Pennsylvania 2003/ /09 (Combined Data) Data Source: Bureau of Community Health Systems (BCHS), Division of School Health Note: the School Year Data is missing The data for school students diagnosed with asthma from school years 2003/04 to 2008/09 were combined by health district. The Southeast Health District had the highest percentage of children with asthma (11.7 percent), followed by the Southcentral Health District (10.2 percent). The lowest average rate was among children in the Northwest Health District (8.4 percent). Section 4: Asthma Lifetime Prevalence among Pennsylvania School Students 46
, Division of School Health Note: the 2004-2005 School Year Data is missing Overall, in the period between 2003/04-2008/09, the highest asthma")
54 Figure 4-3: Lifetime Asthma Prevalence Among School Students by County, Pennsylvania 2003/ /09 (Combined Data) Section 4: Asthma Lifetime Prevalence among Pennsylvania School Students Data Source: Bureau of Community Health Systems (BCHS), Division of School Health Note: the School Year Data is missing Overall, in the period between 2003/ /09, the highest asthma prevalence among school students was in Philadelphia County (14.0 percent), followed by Mifflin (13.0 percent) and Montour (12.9 percent). The lowest average rate was among children in Clinton, Sullivan and Cameron counties (5.1 percent, 3.9 percent and 3.2 percent, respectively). In the rural areas, the highest asthma prevalence rates were in Montour, Mifflin and McKean counties, and the lowest were in Sullivan, Clinton and Tioga counties. In the urban areas, the highest asthma prevalence rates among school students were in Philadelphia, Berks and Monroe counties, and the lowest were in Cameron, Elk and Luzerne counties. 47
55 Section 5: Asthma Burden in Pennsylvania s Children s Health Insurance Program (CHIP) Asthma is a very important part of the Children s Health Insurance Program (CHIP) population. This section of the Asthma Burden Report describes the burden of asthma among Pennsylvania children (ages 0-18) from 2005 to 2010 and provides hospitalization, emergency room visits and percentage of CHIP members taking appropriate control medications analyzed by age group and geographical location at county, health district and statewide levels. However, at this stage, data by sex is only shown statewide. The data, provided by PA CHIP is based on medical claims of Pennsylvania CHIP recipients from January 1, 2005 to December 31, In order to increase the sample size and produce more reliable results from analysis, data were combined in two-, three- and six-year sets. The following criteria were chosen in order to define an asthma claim/encounter: At least one emergency room visit with asthma as the principal diagnosis (ICD-9 code ) during a specified 12-month period. At least one acute inpatient discharge with asthma as principal diagnosis (ICD-9 code ) during a specified 12-month period. Only children 18 years and younger were included in the report. ER visit and inpatient hospitalization rates with asthma as the primary discharge diagnosis were calculated per 1,000 CHIP enrollees. These rates reflect the number of admissions, not the number of patients. Section 5: Asthma Burden in Pennsylvania s Children s Health Insurance Program (CHIP) 48
 Vertical bars on the graph denote the 95% confidence interval.")

56 Section 5: Asthma Burden in Pennsylvania s Children s Health Insurance Program (CHIP) Figure 5-1: Emergency Room Visit Rates by Age Group, PA (Combined Data) Data Source: Children s Health Insurance Program (CHIP) Vertical bars on the graph denote the 95% confidence interval. Figure 5-2: Annual Inpatient Hospitalization Rates with Asthma as Primary Discharge Diagnosis by Age Group, PA Data Source: Children s Health Insurance Program (CHIP) Vertical bars on the graph denote the 95% confidence interval. From 2005 through 2010, the rate of asthma ER visits per 1,000 CHIP recipients increased among children aged 13 and younger. In age group 13-18, the rate increased from to (6.9 to 8.8, respectively), and a rate decrease was observed from to (8.8 to 8.2, respectively). Overall, there was a significant difference between asthma ER visit rates for all age groups. The highest average rates were in age group 0-5 (11.9), and the lowest were in the age group (8.2). In , inpatient hospitalization rates for CHIP-enrolled children with asthma as the primary discharge diagnosis were significantly higher among age group 0-5 compared to other age groups. Generally, the hospitalization rates for the 0-5 age group decreased from (3.0 per 1,000) to (2.8). During the five-year period, the rates were significantly lower in age group compared to other age groups. The highest rates for all children in age group 0-5 were in (3.0 per 1,000), followed by age group 6-12 and age group in , with 1.9 and 1.1 admissions per 1,000, respectively. 49

57 Figure 5-3: Emergency Room Visit Rates by Health District and Year, PA (Combined Data) Data Source: Children s Health Insurance Program (CHIP) Between , the Southeast Health District had significantly higher ER visit rates than all other health districts in Pennsylvania (11.9 per 1,000), followed by the Northeast and Southwest Health Districts, with rates of ER admissions at 10.0 and 9.3, respectively. However, in spite of an increase in rates during the period in the Southwest Health District, rates in decreased to 9.2 per 1,000. Section 5: Asthma Burden in Pennsylvania s Children s Health Insurance Program (CHIP) 50
 During 2005-2010, among males younger than 13 years, ER visit rates were significantly higher than those of females by approximately 50 percent.")

58 Section 5: Asthma Burden in Pennsylvania s Children s Health Insurance Program (CHIP) Table 5-1: Emergency Room Visit Rates by Sex and Age Group, PA (Combined Data) Data Source: Children s Health Insurance Program (CHIP) During , among males younger than 13 years, ER visit rates were significantly higher than those of females by approximately 50 percent. The discrepancy in ER rates between males and females has increased through all available years of the current analysis. In contrast, for the same period of time, ER visits due to asthma attacks in age group were significantly more frequent among females than among males. The highest ER visit rates among females were observed in age group (9.1) and among males in age group 0-5 (15.9). Table 5-2: Inpatient Hospitalization Rates with Asthma as Primary Discharge Diagnosis by Sex and Age Group, PA (Combined Data) Data Source: Children s Health Insurance Program (CHIP) In , males aged 0-5 and 6-12 years had significantly higher asthma hospitalization rates than females: 3.4 vs. 2.1 per 1,000 in age group 0-5, 2.2 vs. 1.4 in age group For different years, the rates vary; however, males younger than 13 years of age had higher rates than females by approximately 35 percent to 70 percent. Males aged had almost the same hospitalization rates as females. Overall, for , males had significantly higher rates than females (1.4 vs. 1.9 per 1,000). The discrepancy in asthma hospitalization rates between males and females was greatest in and
 Between 2005-2010, among all children s age groups, the Southeast Health District had significantly higher hospitalization rates due to asthma (2.")
59 Figure 5-4: Inpatient Hospitalization Rates with Asthma as Primary Discharge Diagnosis by Age Group and Health District, PA (Combined Data) Data Source: Children s Health Insurance Program (CHIP) Between , among all children s age groups, the Southeast Health District had significantly higher hospitalization rates due to asthma (2.9 per 1,000), followed by the Northcentral Health District (1.1). The lowest average rate was among children in the Southcentral Health District (0.6). Children aged 0-5 years had a significantly higher average hospitalization rate per 1,000 compared to other age groups (2.7 vs. 1.8 in age group 6-12 and 1.0 in age group 13-18). Section 5: Asthma Burden in Pennsylvania s Children s Health Insurance Program (CHIP) 52
 Figure 5-6: Percentage of CHIP recipients with Asthma Receiving Appropriate Long-Term Control Medications by")

60 Section 5: Asthma Burden in Pennsylvania s Children s Health Insurance Program (CHIP) 53 Figure 5-5: Percentage of CHIP recipients with Asthma Receiving Appropriate Long-Term Control Medications by Sex and Age Group, PA Data Source: Children s Health Insurance Program (CHIP) Figure 5-6: Percentage of CHIP recipients with Asthma Receiving Appropriate Long-Term Control Medications by Health District, PA (Combined Data) Data Source: Children s Health Insurance Program (CHIP) In age group 0-5, the percentage of children who received appropriate long-term control medications has increased significantly from 73 percent in to 88 percent in Among children older than 5, there was an increase in the percentage that received appropriate medications in compared to However, among children of the 6-12 age group, the gap was not significantly different, and in age group 13-18, the percentage of those who received appropriate long-term control medications was higher among females than among males. Between , the percentage of Pennsylvania children who received appropriate medications in all age groups was the highest in the Northcentral Health District (95 percent), followed by the Northeast (92 percent) and Northwest with 90 percent. The southeast district accounts for the lowest rates among all age groups (81 percent). In Pennsylvania, the highest percentage of children with medicine compliance occurred in age group 6-12 (90 percent), and the lowest was observed in age group 0-5 (81 percent).
 N/D=Not displayed if count 10 Section 5: Asthma Burden in Pennsylvania s Children s Health Insurance Program (CHIP)")
61 Table 5-3: Number and Percentage of CHIP Recipients with Asthma Receiving Appropriate Long-Term Control Medications by Age Group and County, PA (Combined Data) Data Source: Children s Health Insurance Program (CHIP) N/D=Not displayed if count 10 Section 5: Asthma Burden in Pennsylvania s Children s Health Insurance Program (CHIP) 54
 Data Source: Children s Health Insurance Program (CHIP) N/D=Not displayed if")
62 Section 5: Asthma Burden in Pennsylvania s Children s Health Insurance Program (CHIP) Table 5-3 (continued): Number and Percentage of CHIP recipients with Asthma Receiving Appropriate Long-Term Control Medications by Age Group and County, PA (Combined Data) Data Source: Children s Health Insurance Program (CHIP) N/D=Not displayed if count 10 55
.")
63 Section 6: Asthma Mortality in Pennsylvania For the years , deaths with asthma as the underlying cause were classified according to ICD-9 ( ). Asthma deaths that occurred in 1999 and later are classified according to ICD-10 (J45-J46). This section describes mortality data of Pennsylvania residents who died of asthma from 1998 to 2009 as noted on their death certificates. To increase the sample size and produce more reliable results, asthma death data were combined for a three-year block period and aggregated by age, gender and race/ethnicity. Age-adjusted rates were calculated using the direct standardization method and presented per 100,000 population. In order to help explain the variability in each mortality rate, 95% Confidence Intervals were calculated and displayed. Mortality rates for demographic units with a small number of events (less than 10) were not calculated, because these rates were statistically unreliable. Figure 6-1: Age-Adjusted Asthma Death* Rates Among Pennsylvania Residents, PA Section 6: Asthma Mortality in Pennsylvania Data Source: Bureau of Health Statistics and Research, Pennsylvania Department of Health *Only includes death with asthma listed as the underlying cause Vertical bars on the graph denote the 95% confidence interval. Overall, the age-adjusted asthma mortality rate with asthma as the underlying cause of death significantly decreased in 2009 compared to 2000 (0.9 vs. 1.4 deaths per 100,000 population). The asthma age-adjusted asthma mortality rate decreased from 1.4 deaths per 100,000 population in 2000 to 1.1 in 2001, increased to 1.3 deaths per 100,000 population in 2003, decreased to 1.0 in 2005, increased to 1.3 in 2008, and significantly decreased to 0.9 in 2009, compared to 1.3 in

 than whites.")
64 Figure 6-2: Age-Adjusted Asthma Death* Rates by Race and Ethnicity, PA (Combined Data) Section 6: Asthma Mortality in Pennsylvania 57 Data Source: Bureau of Health Statistics and Research, Pennsylvania Department of Health *Only includes death with asthma listed as the underlying cause Vertical bars on the graph denote the 95% confidence interval. Figure 6-3: Age-Adjusted Asthma Death* Rates by Sex, PA (Combined Data) Data Source: Bureau of Health Statistics and Research, Pennsylvania Department of Health *Only includes death with asthma listed as the underlying cause Vertical bars on the graph denote the 95% confidence interval. During , the ageadjusted asthma mortality rate with asthma as the underlying cause of death was significantly higher among blacks (approximately two to four times higher) than whites. Generally, the rates among blacks decreased from 1998/2000 to 2004/2006 (4.2 vs. 2.7 deaths per 100,000 population). However, in 2007/2009, mortality rates among blacks increased to 3.2 deaths per 100,000 population. The age-adjusted asthma mortality rate with asthma as the underlying cause of death among whites has been steady. Mortality rates decreased among Hispanics from 2.9 in 1998/2000 to 1.5 in 2007/2009 with one exception: in 2001/2003, the rate increased to 3.8 deaths per 100,000 population. During , the ageadjusted asthma mortality rates with asthma as the underlying cause of death among females were significantly higher than among males. Overall, since 1998/2000 (1.4 deaths per 100,000 population), mortality rates among females decreased to 1.2 deaths per 100,000 population in 2004/2006 and 2007/2009. Among males, mortality rates decreased to 0.8 deaths per 100,000 population in 2004/2006, compared to 1.1 deaths per 100,000 population in 1998/2000. However, the rate increased to 0.9 deaths per 100,000 population in 2007/2009.

65 Table 6-1: Age-Specific Asthma Death* Rates by Age, PA Data Source: Bureau of Health Statistics and Research, Pennsylvania Department of Health *Only includes death with asthma listed as the underlying cause ND =not displayed if count <10 L=the lower 95% confidence limit for the rate or percent that appears in the corresponding row U=the upper 95% confidence limit for the rate or percent that appears in the corresponding row **Age-Adjusted rates are standardized to 2000 U.S. Standard Million Population. During , the age-specific asthma mortality rates with asthma as the underlying cause were higher with age, with one exception, in the age group Mortality rates for people ages 85 and older were almost twice as high as it was for those ages under 80. Generally, for the age group 55 and older, asthma mortality rates decreased in 2007/2009 from those of 2001/2003. Section 6: Asthma Mortality in Pennsylvania 58
 or <3 (all other rates) NA* = Data not")
66 Figure 6-4: Age-Adjusted Asthma Death* Rates by County, PA (Combined Data) Section 6: Asthma Mortality in Pennsylvania Data Source: Bureau of Health Statistics and Research, Pennsylvania Department of Health *Only includes death with asthma listed as the underlying cause ND* = Not displayed if count <10 (age-adjusted/specific rates and SMRs) or <3 (all other rates) NA* = Data not available to calculate statistic Direct method per 100,000 US 2000 std million population used for an age-adjusted rates In , the age-adjusted mortality rate with asthma as the underlying cause of death varied by county. Among residents of Pennsylvania, the age-adjusted mortality rate was the highest in Monroe County (2.5 deaths per 100,000 population), Philadelphia (2.5 per 100,000 population), Lackawanna (1.4 per 100,000 population), Dauphin (1.4 per 100,000 population), Luzerne (1.3 per 100,000 population) and Allegheny (1.3 per 100,000 population). 59
67 References 1. Strachan DP, Cook DG. Health effects of passive smoking. Parental smoking and childhood asthma: longitudinal and case-control studies. Thorax 1998; 53: Tatum AJ, Shapiro GG. The effects of outdoor air pollution and tobacco smoke on asthma. Immunol Allergy Clin North Am 2005; 25: CDC. CDC health disparities and inequalities report---united States, MMWR 2011; 60 (Suppl). 4. National Institutes of Health, National Heart, Lung, and Blood Institute. Expert panel report 3: guidelines for the diagnosis and management of asthma. Bethesda, MD: US Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute; Available at gov/guidelines/asthma/asthgdln.pdf. Accessed April 7, U.S. Environmental Protection Agency. National air quality: status and trends through Air quality for W.Pa. hits 10-year best - Pittsburgh Tribune-Review html#ixzz1pmg5rffj References 7. American Lung Association, Epidemiology and Statistics Unit, Research and Program Services. Trends in Asthma Morbidity and Mortality January
68 Glossary of Terms Admission Types: Emergency the patient requires immediate medical intervention as a result of severe, life threatening asthma attack. Urgent the patient requires immediate attention for the care and treatment of asthma attack. Elective the patient s condition permits adequate time to schedule the availability of suitable accommodation. Age-Adjusted Rate: A rate calculated in a manner that allows areas with different age structures to be compared. Rates are standardized to a control population of 2000 U.S. Standard Million Population. Average Charges: The average sum of the hospital charges (excluding professional fees) for each hospitalization. Average Length of Stay (LOS): The average number of days per hospitalization that patient stayed in the facility. Body Mass Index (BMI): A mathematical method to determine obesity by dividing a person s metric weight by the square of the person s metric height. Glossary of Terms 61 Chronic obstructive asthma: Asthma with chronic obstructive pulmonary disease or chronic asthmatic bronchitis. Chronic obstructive pulmonary disease (COPD): Lung disease that can limit your airflow and may include chronic bronchitis, emphysema or both. Confidence Interval (CI): A way to measure sampling error and to define the range of values where percentages are estimated by multiple samples of the same population. Extrinsic asthma (allergic or atopic asthma): This type of asthma is due to an allergy to antigens; usually, the offending allergens are suspended in the air in the form of pollen, dust, smoke, automobile exhaust or animal dander. Hospital Readmission Rate: Represents the rate at which patients return to the hospital within 12 months of discharge following an inpatient stay due to asthma. Inhaled corticosteroid: Anti-inflammatory drugs taken on a daily ongoing basis to prevent asthma attacks. Inhaled short-acting beta2-agonist: Medications that quickly loosen the tightened muscles around swollen airways and often called rescue medications. Inpatient Hospitalization Rate: Inpatient hospitalizations with asthma as the primary discharge diagnosis reflecting the number of admissions (not the number of patients) per 10,000 residents. Intrinsic asthma: This type of asthma is usually secondary to chronic or recurrent infections of the bronchi, sinuses or tonsils and adenoids. Other and unspecified asthma: A respiratory condition that affects breathing that doesn t have an identified cause or the symptoms don t fit a specific type of asthma. Outpatient Visit Rate: Reflects the number of visits (not the number of patients) per 10,000 residents. Primary Payer: The main source from which hospitals expect to receive payment for hospitalization charges. Surveillance: The ongoing systematic collection, analysis and interpretation of health-related data essential to the planning, implementation and evaluation of public health practice. Total Charges: The sum of the hospital charges (excluding professional fees) for an entire year.
69 Acknowledgments This report was prepared by staff of the Asthma Control Program, Bureau of Health Promotion and Risk Reduction, Pennsylvania Department of Health. The Pennsylvania Asthma Control Program extends our appreciation to all members and organizations for their assistance in providing access to asthma data, as well as for reviewing and making recommendations for the publication of 2012 Asthma Burden Report. Centers for Disease Control and Prevention (CDC) Pennsylvania Department of Health, Bureau of Health Statistics and Research Pennsylvania Health Care Cost Containment Council (PHC4) Pennsylvania Department of Health s Division of School Health Children s Health Insurance Program (CHIP) Pennsylvania Department of Health, Bureau of Health Promotion and Risk Reduction Pennsylvania Department of Health, Bureau of Epidemiology For more information regarding data analysis and report compilation, please contact: Vadim Drobin, M.D., M.P.H., Asthma Epidemiologist Bureau of Epidemiology, Pennsylvania Department of Health 625 Forster St., Health and Welfare Building, Harrisburg, PA Phone: vdrobin@state.pa.us Acknowledgements The 2012 Asthma Burden Report can be downloaded from the Pennsylvania Asthma Partnership website: 62
70 Disclaimers This report was supported by Cooperative Agreement Number 5U59EH Addressing Asthma from a Public Health Perspective from the Centers for Disease Control and Prevention (CDC). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention. The Pennsylvania Department of Health, Bureau of Health Statistics and Research, Pennsylvania Department of Health s Division of School Health, and Children s Health Insurance Program specifically disclaim responsibility for any analyses, interpretations or conclusions made by the user of this report. The Pennsylvania Health Care Cost Containment Council is an independent state agency responsible for addressing the problem of escalating health costs, ensuring the quality of health care and increasing access to health care for all citizens. While PHC4 has provided data for this study, PHC4 specifically disclaims responsibility for any analyses, interpretations or conclusions. Disclaimers 63
71
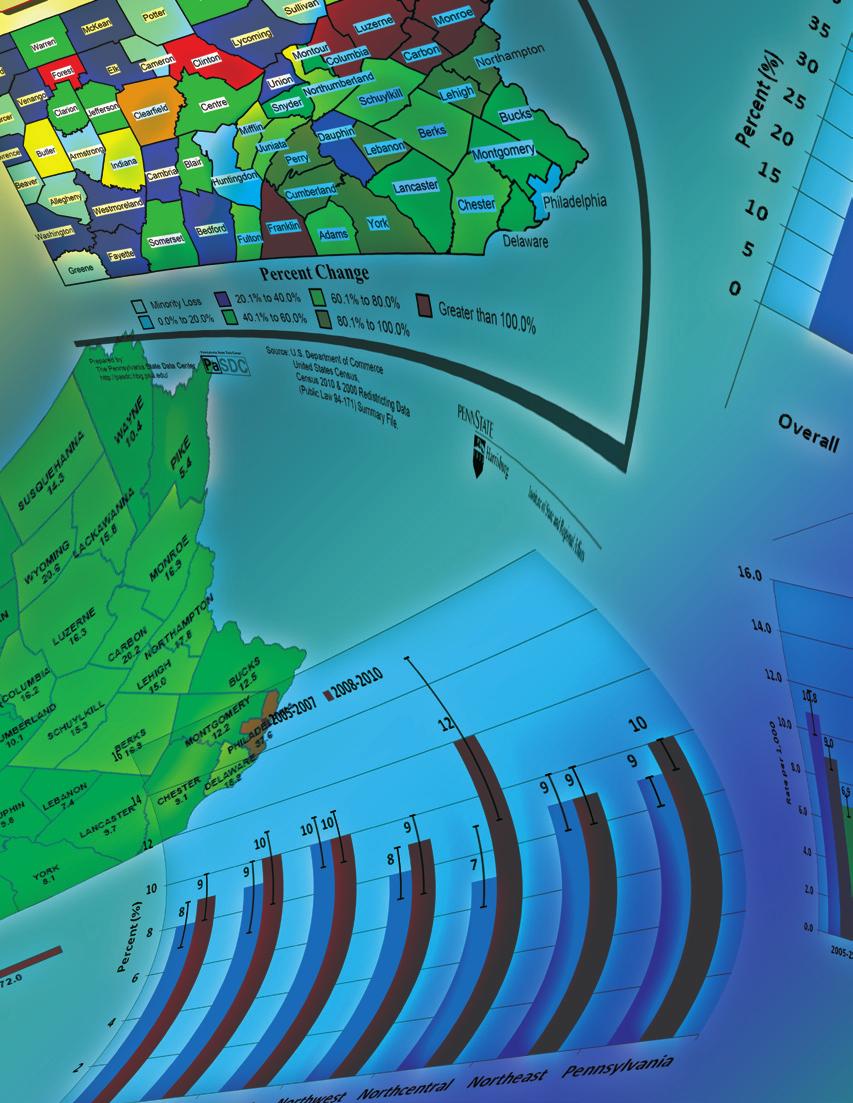
72 65
Asthma Burden. in the C HILDREN S H EALTH I NSURANCE PROGRAM Population. Asthma Control Program Pennsylvania Asthma Surveillance System
 Asthma Burden in the C HILDREN S H EALTH I NSURANCE PROGRAM Population Asthma Control Program Pennsylvania Asthma Surveillance System TABLE OF CONTENTS Introduction...1 Methodology...2 Summary...3 Figure
Asthma Burden in the C HILDREN S H EALTH I NSURANCE PROGRAM Population Asthma Control Program Pennsylvania Asthma Surveillance System TABLE OF CONTENTS Introduction...1 Methodology...2 Summary...3 Figure
Key Facts About. ASTHMA
 Key Facts About. ASTHMA Asthma is a serious lung disease that can be frightening and disabling. The public is becoming increasingly aware that more people, especially children, are suffering and dying
Key Facts About. ASTHMA Asthma is a serious lung disease that can be frightening and disabling. The public is becoming increasingly aware that more people, especially children, are suffering and dying
The 2013 Pennsylvania Asthma Disparities Report
 The 2013 Pennsylvania Asthma Disparities Report Asthma Control Program Pennsylvania Asthma Surveillance System Table of Contents: Introduction....1 Methodology...2 Success Stories...3 Executive Summary........5
The 2013 Pennsylvania Asthma Disparities Report Asthma Control Program Pennsylvania Asthma Surveillance System Table of Contents: Introduction....1 Methodology...2 Success Stories...3 Executive Summary........5
[Type text] Alabama. The Burden of Asthma. Alabama Department of Public Health 201 Monroe Street Montgomery, AL
![[Type text] Alabama. The Burden of Asthma. Alabama Department of Public Health 201 Monroe Street Montgomery, AL](/thumbs/77/76630993.jpg "[Type text] Alabama. The Burden of Asthma. Alabama Department of Public Health 201 Monroe Street Montgomery, AL") The Burden of Asthma Alabama 2013 [Type text] Alabama Department of Public Health 201 Monroe Street Montgomery, AL 36104 www.adph.org The Burden of Asthma in Alabama 2013 Alabama Department of Public
The Burden of Asthma Alabama 2013 [Type text] Alabama Department of Public Health 201 Monroe Street Montgomery, AL 36104 www.adph.org The Burden of Asthma in Alabama 2013 Alabama Department of Public
The Burden of Asthma in Mississippi:
 The Burden of Asthma in Mississippi: 2009 Asthma Surveillance Summary Report April 2009 The Burden of Asthma in Mississippi: 2009 Asthma Surveillance Summary Report Haley Barbour Governor F.E. Thompson,
The Burden of Asthma in Mississippi: 2009 Asthma Surveillance Summary Report April 2009 The Burden of Asthma in Mississippi: 2009 Asthma Surveillance Summary Report Haley Barbour Governor F.E. Thompson,
This page intentionally left blank THE BURDEN OF ASTHMA IN NEW MEXICO 2014 EPIDEMIOLOGY REPORT
 This page intentionally left blank THE BURDEN OF ASTHMA IN NEW MEXICO 214 EPIDEMIOLOGY REPORT This page intentionally left blank The Burden of Asthma in New Mexico: 214 New Mexico Asthma Program Environmental
This page intentionally left blank THE BURDEN OF ASTHMA IN NEW MEXICO 214 EPIDEMIOLOGY REPORT This page intentionally left blank The Burden of Asthma in New Mexico: 214 New Mexico Asthma Program Environmental
Asthma and Air Pollution
 Asthma and Air Pollution Health Effects Workshop Nov. 6, 2008 Joann Held with thanks to: Dave Brown Asthma and Airways Asthma Physiology A chronic disease that affects airways. The inside walls of airways
Asthma and Air Pollution Health Effects Workshop Nov. 6, 2008 Joann Held with thanks to: Dave Brown Asthma and Airways Asthma Physiology A chronic disease that affects airways. The inside walls of airways
Detroit: The Current Status of the Asthma Burden
 Detroit: The Current Status of the Asthma Burden Peter DeGuire, Binxin Cao, Lauren Wisnieski, Doug Strane, Robert Wahl, Sarah Lyon Callo, Erika Garcia, Michigan Department of Health and Human Services
Detroit: The Current Status of the Asthma Burden Peter DeGuire, Binxin Cao, Lauren Wisnieski, Doug Strane, Robert Wahl, Sarah Lyon Callo, Erika Garcia, Michigan Department of Health and Human Services
The Burden of Asthma in Indiana: Second Edition. March 2008
 The Burden of Asthma in Indiana: Second Edition March 28 March 28 Dear Reader: Asthma is a common chronic disease affecting more than half a million Hoosiers. The Indiana State Department of Health s Asthma
The Burden of Asthma in Indiana: Second Edition March 28 March 28 Dear Reader: Asthma is a common chronic disease affecting more than half a million Hoosiers. The Indiana State Department of Health s Asthma
Potentially Preventable Hospitalizations in Pennsylvania
 Potentially Preventable Hospitalizations in Pennsylvania Pennsylvania Health Care Cost Containment Council June 2012 About PHC4 The Pennsylvania Health Care Cost Containment Council (PHC4) is an independent
Potentially Preventable Hospitalizations in Pennsylvania Pennsylvania Health Care Cost Containment Council June 2012 About PHC4 The Pennsylvania Health Care Cost Containment Council (PHC4) is an independent
An Overview of Asthma - Diagnosis and Treatment
 An Overview of Asthma - Diagnosis and Treatment Definition of Asthma: Asthma is a common chronic disease of children and adults. Nationally, more than 1 in 14 Americans report having asthma and as many
An Overview of Asthma - Diagnosis and Treatment Definition of Asthma: Asthma is a common chronic disease of children and adults. Nationally, more than 1 in 14 Americans report having asthma and as many
New York State Department of Health Center for Environmental Health
 New York State Department of Health Center for Environmental Health March 2002 Evaluation of Asthma and Other Respiratory Hospital Admissions among Residents of ZIP Codes 14043 and 14227, Cheektowaga,
New York State Department of Health Center for Environmental Health March 2002 Evaluation of Asthma and Other Respiratory Hospital Admissions among Residents of ZIP Codes 14043 and 14227, Cheektowaga,
What is Asthma? Chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Night time or early morning coughing
 Asthma What is Asthma? Chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Night time or early morning coughing Episodes are usually associated with widespread, but
Asthma What is Asthma? Chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Night time or early morning coughing Episodes are usually associated with widespread, but
HealthPartners Care Coordination Clinical Care Planning and Resource Guide ASTHMA
 The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
Tennessee Department of Health in collaboration with Tennessee State University and University of Tennessee Health Science Center
 Tennessee Department of Health in collaboration with Tennessee State University and University of Tennessee Health Science Center 2006 Tennessee Department of Health 2006 ACKNOWLEDGEMENTS CONTRIBUTING
Tennessee Department of Health in collaboration with Tennessee State University and University of Tennessee Health Science Center 2006 Tennessee Department of Health 2006 ACKNOWLEDGEMENTS CONTRIBUTING
Avg PM10. Avg Low Temp
 Geography 532 Geography of Environmental Health Dr. Paul Marr Name: Ex 16- Seasonality, Time Delay, and Disease (10 pts) Below are asthma cases per month for the years 1992-1994. The table also includes
Geography 532 Geography of Environmental Health Dr. Paul Marr Name: Ex 16- Seasonality, Time Delay, and Disease (10 pts) Below are asthma cases per month for the years 1992-1994. The table also includes
THE BURDEN OF ASTHMA IN WEST VIRGINIA
 THE BURDEN OF ASTHMA IN WEST VIRGINIA Bob Wise Governor Paul L. Nusbaum, Secretary Department of Health and Human Resources Chris Curtis, M.P.H. Acting Commissioner, Bureau for Public Health Catherine
THE BURDEN OF ASTHMA IN WEST VIRGINIA Bob Wise Governor Paul L. Nusbaum, Secretary Department of Health and Human Resources Chris Curtis, M.P.H. Acting Commissioner, Bureau for Public Health Catherine
Asthma: A Growing Epidemic By Glen Andersen
 National Conference of State Legislatures ENVIRONMENTAL H EALTH SERIES May 2000 No. 4 Asthma: A Growing Epidemic By Glen Andersen OVERVIEW Rates for asthma have steadily increased over the past 20 years
National Conference of State Legislatures ENVIRONMENTAL H EALTH SERIES May 2000 No. 4 Asthma: A Growing Epidemic By Glen Andersen OVERVIEW Rates for asthma have steadily increased over the past 20 years
asthma Asthma in Minnesota 2005 Epidemiology Report
 Asthma in Minnesota 2005 Epidemiology Report ACCOMPLISHING STRATEGIES asthma HEALTHIER MINNESOTANS WITH ASTHMA Asthma Program Chronic Disease and Environmental Epidemiology Health Promotion and Chronic
Asthma in Minnesota 2005 Epidemiology Report ACCOMPLISHING STRATEGIES asthma HEALTHIER MINNESOTANS WITH ASTHMA Asthma Program Chronic Disease and Environmental Epidemiology Health Promotion and Chronic
Hospital Discharge Data
 Hospital Discharge Data West Virginia Health Care Authority Hospitalization data were obtained from the West Virginia Health Care Authority s (WVHCA) hospital discharge database. Data are submitted by
Hospital Discharge Data West Virginia Health Care Authority Hospitalization data were obtained from the West Virginia Health Care Authority s (WVHCA) hospital discharge database. Data are submitted by
Hospitalizations for Opioid Overdose Population Differences
 September 2018 Hospitalizations for Opioid Overdose Population Differences This research brief is part of a series produced by the PA Health Care Cost Containment Council (PHC4) that examines opioid-related
September 2018 Hospitalizations for Opioid Overdose Population Differences This research brief is part of a series produced by the PA Health Care Cost Containment Council (PHC4) that examines opioid-related
Demographics and Health Data
 Demographics and Health Data Information for Local Planners City of Lakewood, WA Demographic Characteristics Environmental Health Division 3629 South D Street, Tacoma, WA 98418 (253) 798-6470 Table 1 presents
Demographics and Health Data Information for Local Planners City of Lakewood, WA Demographic Characteristics Environmental Health Division 3629 South D Street, Tacoma, WA 98418 (253) 798-6470 Table 1 presents
1 in 37 Hospitalizations were Related to Opioids in (36,712 Opioid-Related Hospitalizations)
") October 2018 PA Health Care Cost Containment Council Research Briefs Hospital Admissions for Opioid Overdose and Opioid Use Disorder This research brief is part of a series produced by the PA Health Care
October 2018 PA Health Care Cost Containment Council Research Briefs Hospital Admissions for Opioid Overdose and Opioid Use Disorder This research brief is part of a series produced by the PA Health Care
Hospitalizations for Opioid Overdose 2016
 Opioid Overdose 2016 This research brief focuses on inpatient hospitalizations for patients whose principal reason for admission was overdose of heroin or pain medication. This brief follows one released
Opioid Overdose 2016 This research brief focuses on inpatient hospitalizations for patients whose principal reason for admission was overdose of heroin or pain medication. This brief follows one released
Asthma and IAQ. Lani Wheeler, MD, Medical Officer Sarah Merkle, MPH, Program Analyst
 Asthma and IAQ Lani Wheeler, MD, Medical Officer Sarah Merkle, MPH, Program Analyst Division of Adolescent and School Health Centers for Disease Control and Prevention Asthma is a Major Public Health Problem
Asthma and IAQ Lani Wheeler, MD, Medical Officer Sarah Merkle, MPH, Program Analyst Division of Adolescent and School Health Centers for Disease Control and Prevention Asthma is a Major Public Health Problem
Puerto Rico Asthma Surveillance Report 2009
 Puerto Rico Asthma Surveillance Report 29 Puerto Rico Asthma Project Puerto Rico Department of Health Puerto Rico Asthma Project Asthma Surveillance System Puerto Rico Department of Health Maternal, Child
Puerto Rico Asthma Surveillance Report 29 Puerto Rico Asthma Project Puerto Rico Department of Health Puerto Rico Asthma Project Asthma Surveillance System Puerto Rico Department of Health Maternal, Child
Asthma in Maryland 2004
 Asthma in Maryland 24 Prepared by the State of Maryland Department of Health and Mental Hygiene Family Health Administration Maryland Asthma Control Program MARYLAND ASTHMA SURVEILLANCE REPORT ACKNOWLEDGEMENTS
Asthma in Maryland 24 Prepared by the State of Maryland Department of Health and Mental Hygiene Family Health Administration Maryland Asthma Control Program MARYLAND ASTHMA SURVEILLANCE REPORT ACKNOWLEDGEMENTS
THE STATE OF ASTHMA IN INDIANA
 THE STATE OF ASTHMA IN INDIANA ASTHMA PROGRAM OCTOBER 2015 Jack Kinsey, MPH Asthma Epidemiologist Indiana State Department of Health A healthier and safer Indiana Today s Session Will Cover: Data from
THE STATE OF ASTHMA IN INDIANA ASTHMA PROGRAM OCTOBER 2015 Jack Kinsey, MPH Asthma Epidemiologist Indiana State Department of Health A healthier and safer Indiana Today s Session Will Cover: Data from
Pennsylvania Hospital Admissions for Diabetes
 November 2017 Pennsylvania Hospital Admissions for Examining hospital admissions for diabetes is one way to observe the quality of care provided to Pennsylvania residents with diabetes, especially as it
November 2017 Pennsylvania Hospital Admissions for Examining hospital admissions for diabetes is one way to observe the quality of care provided to Pennsylvania residents with diabetes, especially as it
Demographics and Health Data
 Demographics and Health Data Information for Local Planners City of Puyallup, WA Demographic Characteristics Environmental Health Division 3629 South D Street, Tacoma, WA 98418 (253) 798-6470 Table 1 presents
Demographics and Health Data Information for Local Planners City of Puyallup, WA Demographic Characteristics Environmental Health Division 3629 South D Street, Tacoma, WA 98418 (253) 798-6470 Table 1 presents
Pennsylvania s Super-Utilizers of Hospital Care
 Pennsylvania s of Hospital Care Super-utilizer has been used to describe patients who have repeated inpatient hospital stays or who make frequent trips to hospital emergency rooms often across different
Pennsylvania s of Hospital Care Super-utilizer has been used to describe patients who have repeated inpatient hospital stays or who make frequent trips to hospital emergency rooms often across different
Pathology of Asthma Epidemiology
 Asthma A Presentation on Asthma Management and Prevention What Is Asthma? A chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Pathology
Asthma A Presentation on Asthma Management and Prevention What Is Asthma? A chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Pathology
Trends in Pneumonia and Influenza Morbidity and Mortality
 Trends in Pneumonia and Influenza Morbidity and Mortality American Lung Association Epidemiology and Statistics Unit Research and Health Education Division November 2015 Page intentionally left blank Introduction
Trends in Pneumonia and Influenza Morbidity and Mortality American Lung Association Epidemiology and Statistics Unit Research and Health Education Division November 2015 Page intentionally left blank Introduction
ASTHMA IN THE PEDIATRIC POPULATION
 ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
HEALTH PROMOTION AND CHRONIC DISEASE PREVENTION PROGRAM OREGON STATE OF THE HEART AND STROKE REPORT 2001 PREPARED BY.
 OREGON STATE OF THE HEART AND STROKE REPORT 2001 PREPARED BY THE OREGON DEPARTMENT OF HUMAN SERVICES HEALTH SERVICES HEALTH PROMOTION AND CHRONIC DISEASE PREVENTION PROGRAM www.healthoregon.org/hpcdp Contents
OREGON STATE OF THE HEART AND STROKE REPORT 2001 PREPARED BY THE OREGON DEPARTMENT OF HUMAN SERVICES HEALTH SERVICES HEALTH PROMOTION AND CHRONIC DISEASE PREVENTION PROGRAM www.healthoregon.org/hpcdp Contents
Asthma. Guide to Good Health. Healthy Living Guide
 Asthma Guide to Good Health Healthy Living Guide Asthma Chronic Fatigue Syndrome (CFS) Chronic Obstructive Pulmonary Disease (COPD) Coronary Artery Disease (CAD) Depression Hyperlipidemia Hypertension
Asthma Guide to Good Health Healthy Living Guide Asthma Chronic Fatigue Syndrome (CFS) Chronic Obstructive Pulmonary Disease (COPD) Coronary Artery Disease (CAD) Depression Hyperlipidemia Hypertension
Prevalence of Mental Illness
 Section 1 Prevalence of Mental Illness The prevalence of mental health problems or mental illness appears to be quite stable over time. Full epidemiological surveys of prevalence, reported using complex
Section 1 Prevalence of Mental Illness The prevalence of mental health problems or mental illness appears to be quite stable over time. Full epidemiological surveys of prevalence, reported using complex
Asthma 101. Introduction
 TRIGGERS Introduction Asthma is a chronic disease of the lungs that makes it difficult for people to breathe. Asthma is extremely common. About 20 million Americans have asthma. About 5,000 die each year
TRIGGERS Introduction Asthma is a chronic disease of the lungs that makes it difficult for people to breathe. Asthma is extremely common. About 20 million Americans have asthma. About 5,000 die each year
HAMILTON COUNTY DATA PROFILE ADULT CIGARETTE SMOKING. North Country Population Health Improvement Program
 HAMILTON COUNTY DATA PROFILE ADULT CIGARETTE SMOKING North Country Population Health Improvement Program HAMILTON COUNTY DATA PROFILE: ADULT CIGARETTE SMOKING INTRODUCTION The Hamilton County Data Profile
HAMILTON COUNTY DATA PROFILE ADULT CIGARETTE SMOKING North Country Population Health Improvement Program HAMILTON COUNTY DATA PROFILE: ADULT CIGARETTE SMOKING INTRODUCTION The Hamilton County Data Profile
The State of Asthma in Arkansas
 2013 The State of Asthma in Arkansas Jennifer Maulden, MA Martha Phillips, PhD University of Arkansas for Medical Sciences Fay W. Boozman College of Public Health This project was supported by Award Number
2013 The State of Asthma in Arkansas Jennifer Maulden, MA Martha Phillips, PhD University of Arkansas for Medical Sciences Fay W. Boozman College of Public Health This project was supported by Award Number
Healthy Montgomery Obesity Work Group Montgomery County Obesity Profile July 19, 2012
 Healthy Montgomery Obesity Work Group Montgomery County Obesity Profile July 19, 2012 Prepared by: Rachel Simpson, BS Colleen Ryan Smith, MPH Ruth Martin, MPH, MBA Hawa Barry, BS Executive Summary Over
Healthy Montgomery Obesity Work Group Montgomery County Obesity Profile July 19, 2012 Prepared by: Rachel Simpson, BS Colleen Ryan Smith, MPH Ruth Martin, MPH, MBA Hawa Barry, BS Executive Summary Over
The Burden Report: Cardiovascular Disease & Stroke in Texas
 The Burden Report: Cardiovascular Disease & Stroke in Texas Texas Cardiovascular Health and Wellness Program www.dshs.state.tx.us/wellness Texas Council on Cardiovascular Disease and Stroke www.texascvdcouncil.org
The Burden Report: Cardiovascular Disease & Stroke in Texas Texas Cardiovascular Health and Wellness Program www.dshs.state.tx.us/wellness Texas Council on Cardiovascular Disease and Stroke www.texascvdcouncil.org
Speaker Disclosure. Identification and Diagnosis of Asthma. Definition of Asthma. Objectives 11/9/2017
 Speaker Disclosure Identification and Diagnosis of Asthma Isabel L. Virella Lowell, MD, Associate Professor, Pulmonology and Sleep Medicine, University of Alabama at Birmingham Isabel Virella-Lowell, MD
Speaker Disclosure Identification and Diagnosis of Asthma Isabel L. Virella Lowell, MD, Associate Professor, Pulmonology and Sleep Medicine, University of Alabama at Birmingham Isabel Virella-Lowell, MD
Epidemiology of Asthma. In Wayne County, Michigan
 Epidemiology of Asthma In Wayne County, Michigan Elizabeth Wasilevich, MPH Asthma Epidemiologist Bureau of Epidemiology Michigan Department of Community Health 517.335.8164 Publication Date: August 2005
Epidemiology of Asthma In Wayne County, Michigan Elizabeth Wasilevich, MPH Asthma Epidemiologist Bureau of Epidemiology Michigan Department of Community Health 517.335.8164 Publication Date: August 2005
The burden of asthma on the US Healthcare system and for the State of Texas is enormous. The causes of asthma are multifactorial and well known.
 The burden of asthma on the US Healthcare system and for the State of Texas is enormous. The causes of asthma are multifactorial and well known. There are also indications that rural counties have a higher
The burden of asthma on the US Healthcare system and for the State of Texas is enormous. The causes of asthma are multifactorial and well known. There are also indications that rural counties have a higher
Epidemiology of Asthma. In the Western Michigan Counties of. Kent, Montcalm, Muskegon, Newaygo, and Ottawa
 Epidemiology of Asthma In the Western Michigan Counties of Kent, Montcalm, Muskegon, Newaygo, and Ottawa Elizabeth Wasilevich, MPH Asthma Epidemiologist Bureau of Epidemiology Michigan Department of Community
Epidemiology of Asthma In the Western Michigan Counties of Kent, Montcalm, Muskegon, Newaygo, and Ottawa Elizabeth Wasilevich, MPH Asthma Epidemiologist Bureau of Epidemiology Michigan Department of Community
Connecting Health & Housing: Asthma and the Home. Presented by: The California-Nevada Public Health Training Center
 Connecting Health & Housing: Asthma and the Home Presented by: The California-Nevada Public Health Training Center Funded by Grant #UB6HP20202 from the Health Resources and Services Administration, U.S.
Connecting Health & Housing: Asthma and the Home Presented by: The California-Nevada Public Health Training Center Funded by Grant #UB6HP20202 from the Health Resources and Services Administration, U.S.
The Primary Prevention of Asthma
 The Primary Prevention of Asthma Risk Factors Associated with Asthma Onset Ted Schettler Science and Environmental Health Network Collaborative on Health and Environment June, 2013 Asthma: a complex disease(s)
The Primary Prevention of Asthma Risk Factors Associated with Asthma Onset Ted Schettler Science and Environmental Health Network Collaborative on Health and Environment June, 2013 Asthma: a complex disease(s)
Science in the News: Asthma
 Science in the News: Asthma Spring has returned to the United States. The sky is blue, the grass is green and many plants are flowering. Spring can be a beautiful time of year. But it is especially troublesome
Science in the News: Asthma Spring has returned to the United States. The sky is blue, the grass is green and many plants are flowering. Spring can be a beautiful time of year. But it is especially troublesome
Asthma Profile St. Louis County, Missouri
 Asthma Profile St. Louis County, Missouri Asthma is a chronic lung disease that inflames (swells) and narrows the airways (tubes that carry air into and out of your lungs).ff1 It affects people of all
Asthma Profile St. Louis County, Missouri Asthma is a chronic lung disease that inflames (swells) and narrows the airways (tubes that carry air into and out of your lungs).ff1 It affects people of all
Oregon Asthma Surveillance Summary Report August 2006
 Oregon Asthma Surveillance Summary Report August 26 Oregon Asthma Program Office of Disease Prevention and Epidemiology Public Health Services Oregon Department of Human Services Mel Kohn, MD, MPH, State
Oregon Asthma Surveillance Summary Report August 26 Oregon Asthma Program Office of Disease Prevention and Epidemiology Public Health Services Oregon Department of Human Services Mel Kohn, MD, MPH, State
CHRONIC DISEASE PREVALENCE AMONG ADULTS IN OHIO
 OHIO MEDICAID ASSESSMENT SURVEY 2012 Taking the pulse of health in Ohio CHRONIC DISEASE PREVALENCE AMONG ADULTS IN OHIO Amy Ferketich, PhD Ling Wang, MPH The Ohio State University College of Public Health
OHIO MEDICAID ASSESSMENT SURVEY 2012 Taking the pulse of health in Ohio CHRONIC DISEASE PREVALENCE AMONG ADULTS IN OHIO Amy Ferketich, PhD Ling Wang, MPH The Ohio State University College of Public Health
Presenter. Mona Sarfaty, MD, MPH, FAAFP Director, Program on Climate and Health Center for Climate Change Communication George Mason University
 Presenter Mona Sarfaty, MD, MPH, FAAFP Director, Program on Climate and Health Center for Climate Change Communication George Mason University Making the Connection: Climate Changes Allergies and Asthma
Presenter Mona Sarfaty, MD, MPH, FAAFP Director, Program on Climate and Health Center for Climate Change Communication George Mason University Making the Connection: Climate Changes Allergies and Asthma
Asthma. Jill Waldron Respiratory Specialist Nurse
 Asthma Jill Waldron Respiratory Specialist Nurse Asthma morbidity 15 20% of children In a class of c30 children likely to be 4-54 children with asthma In infancy more common in boys but becomes more common
Asthma Jill Waldron Respiratory Specialist Nurse Asthma morbidity 15 20% of children In a class of c30 children likely to be 4-54 children with asthma In infancy more common in boys but becomes more common
Asthma Disparities A National and Local Perspective
 Asthma Disparities A National and Local Perspective Tyra Bryant-Stephens, MD, Director and Founder of the Community Asthma Prevention Program of Philadelphia The Children s Hospital of Philadelphia Clinical
Asthma Disparities A National and Local Perspective Tyra Bryant-Stephens, MD, Director and Founder of the Community Asthma Prevention Program of Philadelphia The Children s Hospital of Philadelphia Clinical
ASTHMA TAKES OUR CHILDREN S BREATH AWAY DEMOGRAPHICS DEMOGRAPHICS NEHA AEC IAQ1101 Asthma: Takes Our Children s Breath Away
 ASTHMA TAKES OUR CHILDREN S BREATH AWAY DEMOGRAPHICS Duval County Located in North East Florida Comprised of the cities/towns of Jacksonville, Jacksonville Beach, Atlantic Beach, Neptune Beach, and Baldwin
ASTHMA TAKES OUR CHILDREN S BREATH AWAY DEMOGRAPHICS Duval County Located in North East Florida Comprised of the cities/towns of Jacksonville, Jacksonville Beach, Atlantic Beach, Neptune Beach, and Baldwin
The State of Asthma. Jeanne Moorman, NCEH Survey Statistician National Asthma Program
 The State of Asthma American College of Chest Physicians 14th Annual ACCP Community Asthma and COPD Coalitions Symposium October 24-25, 212 Atlanta, GA Jeanne Moorman, NCEH Survey Statistician National
The State of Asthma American College of Chest Physicians 14th Annual ACCP Community Asthma and COPD Coalitions Symposium October 24-25, 212 Atlanta, GA Jeanne Moorman, NCEH Survey Statistician National
LEARNING MODULE #17: ENVIRONMENTAL HEALTH: ISSUES AND IMPACT
 LEARNING MODULE #17: ENVIRONMENTAL HEALTH: ISSUES AND IMPACT Environmental Health: Issues and Impact Carol Ann Gross-Davis, PhD, MS Adjunct Assistant Professor Drexel University, School of Public Health
LEARNING MODULE #17: ENVIRONMENTAL HEALTH: ISSUES AND IMPACT Environmental Health: Issues and Impact Carol Ann Gross-Davis, PhD, MS Adjunct Assistant Professor Drexel University, School of Public Health
Outpatient Guideline for the Diagnosis and Management of Asthma
 Outpatient Guideline for the Diagnosis and Management of Asthma Initial Visit Follow-Up Visits See page 2 Asthma Diagnosis See page 3 Classifying Asthma Severity and Initiating Treatment See pages 2 and
Outpatient Guideline for the Diagnosis and Management of Asthma Initial Visit Follow-Up Visits See page 2 Asthma Diagnosis See page 3 Classifying Asthma Severity and Initiating Treatment See pages 2 and
Get Healthy Stay Healthy
 Asthma Management WHAT IS ASTHMA? Asthma causes swelling and inflammation in the breathing passages that lead to your lungs. When asthma flares up, the airways tighten and become narrower. This keeps the
Asthma Management WHAT IS ASTHMA? Asthma causes swelling and inflammation in the breathing passages that lead to your lungs. When asthma flares up, the airways tighten and become narrower. This keeps the
Pre-Conception & Pregnancy in Ohio
 Pre-Conception & Pregnancy in Ohio Elizabeth Conrey, PhD 1 January 217 1 State Maternal and Child Health Epidemiologist, Ohio Department of Health EXECUTIVE SUMMARY The primary objective of the analyses
Pre-Conception & Pregnancy in Ohio Elizabeth Conrey, PhD 1 January 217 1 State Maternal and Child Health Epidemiologist, Ohio Department of Health EXECUTIVE SUMMARY The primary objective of the analyses
Asthma and Travel to Beijing By Dr. Fiona Newton BMBS (Hons) Family Medicine Physician at Beijing United Family Hospital and Clinics
 Family Medicine Physician at Beijing United Family Hospital and Clinics") Asthma and Travel to Beijing By Dr. Fiona Newton BMBS (Hons) Family Medicine Physician at Beijing United Family Hospital and Clinics So you have asthma? Is travel to Beijing out of the question? Asthma
Asthma and Travel to Beijing By Dr. Fiona Newton BMBS (Hons) Family Medicine Physician at Beijing United Family Hospital and Clinics So you have asthma? Is travel to Beijing out of the question? Asthma
3.0 Asthma and Respiratory Disease
 3. Asthma and Respiratory Disease The air children breathe is an important source of exposure to substances that may potentially harm their health (US EPA 23).Exposures in early childhood when the lungs
3. Asthma and Respiratory Disease The air children breathe is an important source of exposure to substances that may potentially harm their health (US EPA 23).Exposures in early childhood when the lungs
Prince Edward Island Asthma Trends
 Prince Edward Island Asthma Trends 2001-2011 November 2014 Population Health Assessment and Surveillance Unit, Chief Public Health Office, Department of Health and Wellness Dr. Carol McClure, Chronic Disease
Prince Edward Island Asthma Trends 2001-2011 November 2014 Population Health Assessment and Surveillance Unit, Chief Public Health Office, Department of Health and Wellness Dr. Carol McClure, Chronic Disease
Asthma Among Minnesota Health Care Program Beneficiaries
 Asthma Among Minnesota Health Care Program Beneficiaries A JOINT REPORT FROM THE MINNESOTA DEPARTMENT OF HEALTH AND THE MINNESOTA DEPARTMENT OF HUMAN SERVICES November 2018 Asthma Among Minnesota Health
Asthma Among Minnesota Health Care Program Beneficiaries A JOINT REPORT FROM THE MINNESOTA DEPARTMENT OF HEALTH AND THE MINNESOTA DEPARTMENT OF HUMAN SERVICES November 2018 Asthma Among Minnesota Health
ASTHMA BY RACE AND ETHNICITY
 ASTHMA BY RACE AND ETHNICITY The following report depicts asthma rates for various races using data collected from the Michigan Behavioral Risk Factor Survey (MiBRFS), Minority Health Surveys, Michigan
ASTHMA BY RACE AND ETHNICITY The following report depicts asthma rates for various races using data collected from the Michigan Behavioral Risk Factor Survey (MiBRFS), Minority Health Surveys, Michigan
The Burden of Cardiovascular Disease in North Carolina June 2009 Update
 The Burden of Cardiovascular Disease in North Carolina June 2009 Update Sara L. Huston, Ph.D. Heart Disease & Stroke Prevention Branch Chronic Disease & Injury Section Division of Public Health North Carolina
The Burden of Cardiovascular Disease in North Carolina June 2009 Update Sara L. Huston, Ph.D. Heart Disease & Stroke Prevention Branch Chronic Disease & Injury Section Division of Public Health North Carolina
2010 Community Health Needs Assessment Final Report
 2010 Community Health Needs Assessment Final Report April 2011 TABLE OF CONTENTS A. BACKGROUND 3 B. DEMOGRAPHICS 4 C. GENERAL HEALTH STATUS 10 D. ACCESS TO CARE 11 E. DIABETES 12 F. HYPERTENSION AWARENESS
2010 Community Health Needs Assessment Final Report April 2011 TABLE OF CONTENTS A. BACKGROUND 3 B. DEMOGRAPHICS 4 C. GENERAL HEALTH STATUS 10 D. ACCESS TO CARE 11 E. DIABETES 12 F. HYPERTENSION AWARENESS
Some Facts About Asthma
 Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
Investing in Best Practices for Asthma: A Business Case
 Investing in Best Practices for Asthma: A Business Case A program of The Medical Foundation Produced by Dr. Polly Hoppin & Molly Jacobs/UMass Lowell Laurie Stillman, Asthma Regional Council Asthma Big
Investing in Best Practices for Asthma: A Business Case A program of The Medical Foundation Produced by Dr. Polly Hoppin & Molly Jacobs/UMass Lowell Laurie Stillman, Asthma Regional Council Asthma Big
Looking for Answers to Asthma
 01 May 2012 MP3 at voaspecialenglish.com Looking for Answers to Asthma AP Asthmatics feel like something heavy is on their chest during an attack, as demonstrated in Geneva for World Asthma Day in 2009
01 May 2012 MP3 at voaspecialenglish.com Looking for Answers to Asthma AP Asthmatics feel like something heavy is on their chest during an attack, as demonstrated in Geneva for World Asthma Day in 2009
Asthma and air pollution: health effects and prevention
 Asthma and air pollution: health effects and prevention FuyuenYip PhD, MPH Air Pollution and Respiratory Health Branch Division of Environmental Hazards and Health Effects National Center for Environmental
Asthma and air pollution: health effects and prevention FuyuenYip PhD, MPH Air Pollution and Respiratory Health Branch Division of Environmental Hazards and Health Effects National Center for Environmental
Financial Impact of Emergency Department Visits by Adults for Dental Conditions in Maryland
 Financial Impact of Emergency Department by Adults for Dental Conditions in Maryland Background Access to dental care remains challenging for many children and adults. Lack of preventive care services
Financial Impact of Emergency Department by Adults for Dental Conditions in Maryland Background Access to dental care remains challenging for many children and adults. Lack of preventive care services
Health Policy Research Brief
 Health Policy Research Brief February 2007 Pets and Smoking in the Home Associated with Asthma Symptoms and Asthma-Like Breathing Problems Theresa A. Hastert, Susan H. Babey, E. Richard Brown and Ying-Ying
Health Policy Research Brief February 2007 Pets and Smoking in the Home Associated with Asthma Symptoms and Asthma-Like Breathing Problems Theresa A. Hastert, Susan H. Babey, E. Richard Brown and Ying-Ying
Baseline Health Data Report: Cambria and Somerset Counties, Pennsylvania
 Baseline Health Data Report: Cambria and Somerset Counties, Pennsylvania 2017 2018 Page 1 Table of Contents Executive Summary.4 Demographic and Economic Characteristics 6 Race and Ethnicity (US Census,
Baseline Health Data Report: Cambria and Somerset Counties, Pennsylvania 2017 2018 Page 1 Table of Contents Executive Summary.4 Demographic and Economic Characteristics 6 Race and Ethnicity (US Census,
CENTRAL CALIFORNIA CHILDREN S INSTITUTE
 CENTRAL CALIFORNIA CHILDREN S INSTITUTE The Central California Children s Institute is dedicated to improving the well-being and quality of life for all children, youth, and their families in the Central
CENTRAL CALIFORNIA CHILDREN S INSTITUTE The Central California Children s Institute is dedicated to improving the well-being and quality of life for all children, youth, and their families in the Central
Millennium Collaborative Care PPS Community Profile
 Millennium Collaborative Care PPS Community Profile Counties served: Allegany, Cattaraugus, Chautauqua, Erie, Genesee, Niagara, Orleans, and Wyoming DEMOGRAPHICS 1 Millennium Collaborative Care (MCC) PPS
Millennium Collaborative Care PPS Community Profile Counties served: Allegany, Cattaraugus, Chautauqua, Erie, Genesee, Niagara, Orleans, and Wyoming DEMOGRAPHICS 1 Millennium Collaborative Care (MCC) PPS
Table of Contents. 2 P age. Susan G. Komen
 RHODE ISLAND Table of Contents Table of Contents... 2 Introduction... 3 About... 3 Susan G. Komen Affiliate Network... 3 Purpose of the State Community Profile Report... 4 Quantitative Data: Measuring
RHODE ISLAND Table of Contents Table of Contents... 2 Introduction... 3 About... 3 Susan G. Komen Affiliate Network... 3 Purpose of the State Community Profile Report... 4 Quantitative Data: Measuring
ASTHMA MANAGEMENT IN SCHOOL: WHAT ALL SCHOOL STAFF NEEDS TO KNOW! PROFESSIONAL IN-SERVICE Sunflower Co. Consolidated School District
 ASTHMA MANAGEMENT IN SCHOOL: WHAT ALL SCHOOL STAFF NEEDS TO KNOW! PROFESSIONAL IN-SERVICE Sunflower Co. Consolidated School District OVERVIEW AT THE END OF THIS IN-SERVICE, YOU WILL BE FAMILIAR WITH: Asthma
ASTHMA MANAGEMENT IN SCHOOL: WHAT ALL SCHOOL STAFF NEEDS TO KNOW! PROFESSIONAL IN-SERVICE Sunflower Co. Consolidated School District OVERVIEW AT THE END OF THIS IN-SERVICE, YOU WILL BE FAMILIAR WITH: Asthma
Texas Chronic Disease Burden Report. April Publication #E
 Texas Chronic Disease Burden Report April 2010 Publication #E81-11194 Direction and Support Lauri Kalanges, MD, MPH Medical Director Health Promotion and Chronic Disease Prevention Section, Texas Department
Texas Chronic Disease Burden Report April 2010 Publication #E81-11194 Direction and Support Lauri Kalanges, MD, MPH Medical Director Health Promotion and Chronic Disease Prevention Section, Texas Department
Community Health Needs Assessment
 Community Health Needs Assessment Gratiot County Community Health Assessment Community Health Assessment Data Sources Primary Data (new data collected first-hand) Community Opinion Survey Provider Opinion
Community Health Needs Assessment Gratiot County Community Health Assessment Community Health Assessment Data Sources Primary Data (new data collected first-hand) Community Opinion Survey Provider Opinion
ASTHMA AND CHILDCARE PART 1. Presented by: Robin Costley, CRT, AE-C Marion County Public Health Department Manager, Asthma Alliance of Indianapolis
 ASTHMA AND CHILDCARE PART 1 Presented by: Robin Costley, CRT, AE-C Marion County Public Health Department Manager, Asthma Alliance of Indianapolis OBJECTIVES By the end of training, participants will:
ASTHMA AND CHILDCARE PART 1 Presented by: Robin Costley, CRT, AE-C Marion County Public Health Department Manager, Asthma Alliance of Indianapolis OBJECTIVES By the end of training, participants will:
TRENDS IN PNEUMONIA AND INFLUENZA MORBIDITY AND MORTALITY
 TRENDS IN PNEUMONIA AND INFLUENZA MORBIDITY AND MORTALITY AMERICAN LUNG ASSOCIATION RESEARCH AND PROGRAM SERVICES EPIDEMIOLOGY AND STATISTICS UNIT February 2006 TABLE OF CONTENTS Trends in Pneumonia and
TRENDS IN PNEUMONIA AND INFLUENZA MORBIDITY AND MORTALITY AMERICAN LUNG ASSOCIATION RESEARCH AND PROGRAM SERVICES EPIDEMIOLOGY AND STATISTICS UNIT February 2006 TABLE OF CONTENTS Trends in Pneumonia and
Regional and Hispanic Subgroup Disparities in the Prevalence of Diabetes & Hypertension Among Older Adults
 Regional and Hispanic Subgroup Disparities in the Prevalence of Diabetes & Hypertension Among Older Adults Catherine Pérez Jennifer A. Ailshire Conference Series on Aging in the Americas September 21,
Regional and Hispanic Subgroup Disparities in the Prevalence of Diabetes & Hypertension Among Older Adults Catherine Pérez Jennifer A. Ailshire Conference Series on Aging in the Americas September 21,
July, Years α : 7.7 / 10, Years α : 11 / 10,000 < 5 Years: 80 / 10, Reduce emergency department visits for asthma.
 What are the Healthy People 1 objectives? July, 6 Sponsored by the U.S. Department of Health and Human Services, the Healthy People 1 initiative is a comprehensive set of disease prevention and health
What are the Healthy People 1 objectives? July, 6 Sponsored by the U.S. Department of Health and Human Services, the Healthy People 1 initiative is a comprehensive set of disease prevention and health
Racial disparities in health outcomes and factors that affect health: Findings from the 2011 County Health Rankings
 Racial disparities in health outcomes and factors that affect health: Findings from the 2011 County Health Rankings Author: Nathan R. Jones, PhD University of Wisconsin Carbone Cancer Center Introduction
Racial disparities in health outcomes and factors that affect health: Findings from the 2011 County Health Rankings Author: Nathan R. Jones, PhD University of Wisconsin Carbone Cancer Center Introduction
David V. McQueen. BRFSS Surveillance General Atlanta - Rome 2006
 David V. McQueen Associate Director for Global Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Atlanta BRFSS Surveillance General Atlanta - Rome 2006 Behavioral Risk
David V. McQueen Associate Director for Global Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Atlanta BRFSS Surveillance General Atlanta - Rome 2006 Behavioral Risk
The Health Effects of Air Pollution. Haim Bibi Carmel Medical Center
 The Health Effects of Air Pollution on Children Haim Bibi Carmel Medical Center Haifa Why are children at special risk? Physically, children are more vulnerable to air pollution than adults. Their respiratory
The Health Effects of Air Pollution on Children Haim Bibi Carmel Medical Center Haifa Why are children at special risk? Physically, children are more vulnerable to air pollution than adults. Their respiratory
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Central New York Care Collaborative, Inc. PPS Community Profile
 Central New York Care Collaborative, Inc. PPS Community Profile Counties served: Cayuga, Lewis, Madison, Oneida, Onondaga, and Oswego DEMOGRAPHICS 1 The total population of the Central New York Care Collaborative
Central New York Care Collaborative, Inc. PPS Community Profile Counties served: Cayuga, Lewis, Madison, Oneida, Onondaga, and Oswego DEMOGRAPHICS 1 The total population of the Central New York Care Collaborative
Table of Contents. 2 P a g e. Susan G. Komen
 NEW HAMPSHIRE Table of Contents Table of Contents... 2 Introduction... 3 About... 3 Susan G. Komen Affiliate Network... 3 Purpose of the State Community Profile Report... 4 Quantitative Data: Measuring
NEW HAMPSHIRE Table of Contents Table of Contents... 2 Introduction... 3 About... 3 Susan G. Komen Affiliate Network... 3 Purpose of the State Community Profile Report... 4 Quantitative Data: Measuring
Statewide Statistics and Key Findings 1
 % s, 30 Days PHC4 s for Same Condition Jan 03 through Aug 04 Data Statewide information about readmissions and the key findings of this report are presented in this section. The study examines hospitalizations
% s, 30 Days PHC4 s for Same Condition Jan 03 through Aug 04 Data Statewide information about readmissions and the key findings of this report are presented in this section. The study examines hospitalizations
About the Highmark Foundation
 About the Highmark Foundation The Highmark Foundation, created in 2000 as an affiliate of Highmark Inc., is a charitable organization and a private foundation that supports initiatives and programs aimed
About the Highmark Foundation The Highmark Foundation, created in 2000 as an affiliate of Highmark Inc., is a charitable organization and a private foundation that supports initiatives and programs aimed
Asthma Needs Assessment. Central Utah Public Health Department Including Juab, Millard, Piute, Sanpete, Sevier and Wayne County
 Asthma Needs Assessment Central Utah Public Health Department Including Juab, Millard, Piute, Sanpete, Sevier and Wayne County Bruce Costa, PhD, Health Officer Leslie Abraham, RN, Community Health Services
Asthma Needs Assessment Central Utah Public Health Department Including Juab, Millard, Piute, Sanpete, Sevier and Wayne County Bruce Costa, PhD, Health Officer Leslie Abraham, RN, Community Health Services
Measuring Equitable Care to Support Quality Improvement
 Measuring Equitable Care to Support Quality Improvement Berny Gould RN, MNA Sr. Director, Quality, Hospital Oversight, and Equitable Care Prepared by: Sharon Takeda Platt, PhD Center for Healthcare Analytics
Measuring Equitable Care to Support Quality Improvement Berny Gould RN, MNA Sr. Director, Quality, Hospital Oversight, and Equitable Care Prepared by: Sharon Takeda Platt, PhD Center for Healthcare Analytics
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Identifying Adult Mental Disorders with Existing Data Sources
 Identifying Adult Mental Disorders with Existing Data Sources Mark Olfson, M.D., M.P.H. New York State Psychiatric Institute Columbia University New York, New York Everything that can be counted does not
Identifying Adult Mental Disorders with Existing Data Sources Mark Olfson, M.D., M.P.H. New York State Psychiatric Institute Columbia University New York, New York Everything that can be counted does not
Trends in Pneumonia and Influenza Morbidity and Mortality
 Trends in Pneumonia and Influenza Morbidity and Mortality American Lung Association Research and Program Services Epidemiology and Statistics Unit September 2008 Table of Contents Trends in Pneumonia and
Trends in Pneumonia and Influenza Morbidity and Mortality American Lung Association Research and Program Services Epidemiology and Statistics Unit September 2008 Table of Contents Trends in Pneumonia and
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists