Pulmonary Func-on Tes-ng. Chapter 8
|
|
|
- Moses Weaver
- 6 years ago
- Views:
Transcription
1 Pulmonary Func-on Tes-ng Chapter 8
2 Pulmonary Func-on Tes-ng Which of the following is the true pulmonary func-on test? Spirometry Lung volumes Diffusion capacity ABG
3 Pulmonary Func-on Tes-ng Process of having the pa-ent perform specific inspiratory and expiratory maneuvers Important to be familiar with these tests and values even if you do not work in a PFT lab Used for the following: Medical diagnosis Surgery related evalua-on Disability evalua-on Public Health/Research Studying the effects of exercise on the lungs
4 Contraindica-ons Recent abdominal, thoracic, or eye surgery Hemodynamic instability Symptoms of acute severe illness Chest pain, nausea, vomiting, high fever, dyspnea Recent hemoptysis Pneumothorax Recent history of abdominal, thoracic, or cerebral aneurysm
5 Normal Values Height Weight Age Gender Race Effort dependent
6 Pa-ent Instruc-ons Prior to Tes-ng Should not drink alcohol for four hours prior to test Should not smoke at least one hour before test Do not eat a large meal two hours prior to test No vigorous exercise 30 minutes before test Do not wear -ght form fiung clothes May need to remove loose dentures for test Should wait at least one month post MI, consider impact of problems that may affect results (chest/abdominal pain, oral or facial pain, stress incon-nence, demen-a, physical deformi-es or medical condi-ons) Bring a list of all medica-ons poten-ally withhold bronchodilators, cor-costeroids




7 Equipment Spirometer Respirometer Pneumotachometer Body Plethysmograph body box Diffusion System Gas Analysis
8 ATPS vs BTPS Ambient Temperature and Pressure Saturated Ambient temp is less than body temp Volume of air measured by spirometer is slightly less than the volume actually exhaled Measurements made by system must be converted Body Temperature and Pressure Saturated Requires knowing the ambient temperature, barometric pressure and humidity level ATPS is mul-plied by the correc-on factor to obtain the higher BTPS values
9 Conversion from ATPS to BTPS condi-ons Temp.ºC Corr.factor
10 Classifica-on of Lung Defects OBSTRUCTIVE Expiratory flow is below normal Anatomic site can be iden-fied Diseases: Cys-c fibrosis Bronchi-s Asthma Bronchiectasis Emphysema RESTRICTIVE Lung volumes are reduced Diseases: Neuromuscular Cardiovascular Pulmonary Trauma/chest wall dysfunc-on Obesity

11 NORMAL SPIROGRAM
12 Spirogram Volumes Tidal Volume Minute Volume Residual Volume Inspiratory Reserve Volume Expiratory Reserve Volume Capaci6es Vital Capacity Total Lung Capacity Func-on Residual Capacity Inspiratory Capacity
 Helps avoid air")
13 Vital Capacity Forced (FVC) Requires proper coaching Three dis-nct phases Decreased in both obstruc-ve and restric-ve diseases Slow (SVC) Helps avoid air trapping
14 Slow Vital Capacity
15 Total Lung Capacity Increased with obstruc-ve disease Decreased with restric-ve disorders Sum of the vital capacity and residual volume Obtain RV by: Body plethysmography Nitrogen washout Helium dilu-on

16 Body Plethysmography Uses the body box Boyles Law Unknown lung gas vol = Gas pressure of the box Known box gas vol Gas pressure of the lungs


17 In body plethysmography, the pa-ent sits inside an air-ght box, inhales or exhales to a par-cular volume (usually FRC), and then a shuber drops across their breathing valve. The subject makes respiratory efforts against the closed shuber causing their chest volume to expand and decompressing the air in their lungs. The increase in their chest volume slightly reduces the box volume and thus increases the pressure in the box. This method of measuring FRC actually measures all the conduc-ng pathways including abdominal gas; the actual measurement made is VTG (Volume of Thoracic gas).

18 Nitrogen Washout Open circuit method Pa-ent breathes 100% oxygen while the nitrogen washed out of the lungs is measured Assumes 79% of lung volume is nitrogen Several problems with this test

19 Helium Dilu-on Closed system Known volume and concentra-on of He added and it will be diluted in propor-on to the size of the lung volume

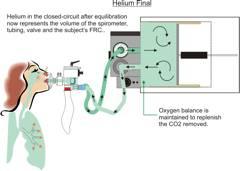
20 Helium Dilu-on
21 Flow Measurements FEV 1 FEV 3 FEF FEF 25 75% PEFR
22 FEV 1 Maximal volume exhaled during the first second of expira-on Best indicator of obstruc-ve lung disease Flow characteris-cs of the larger airways Best expressed as a percentage of the FVC (FEV 1 /FVC) Should be able to exhale 70% of the vital capacity in the first second Decreased in obstruc-ve disorders
23 FEV 3 Evaluates flow 3 seconds into expira-on Indicates flow in the smaller airways
24 Forced Expiratory Flow FEF 25 75% Examines the middle 50% of the exhaled curve Reflects degree of airway patency/condi-on of the medium to small airways Early indicator of obstruc-ve dysfunc-on Normal value is 4 5 L/sec
25 Forced Expiratory Flow FEF Average flow aner the first 200ml is exhaled Good indicator of the integrity of large airway fun-oning Decreased in obstruc-ve disorders Normal value is 6 7L/se
26 Peak Expiratory Flow Rate Maximum flow rate achieved during an FVC Used in asthma-cs to iden-fy the severity of airway obstruc-on and guide therapy Dependent on pa-ent effort Normal value is 10L/sec (600L/min), decreases with age and obstruc-on

27 Maximum Voluntary Ven-la-on MVV pa-ent breathes as fast and deep as possible for seconds Tests for overall lung func-on, ven-latory reserve capacity and air trapping Normal = 170L/min Decreased in obstruc-ve disorders

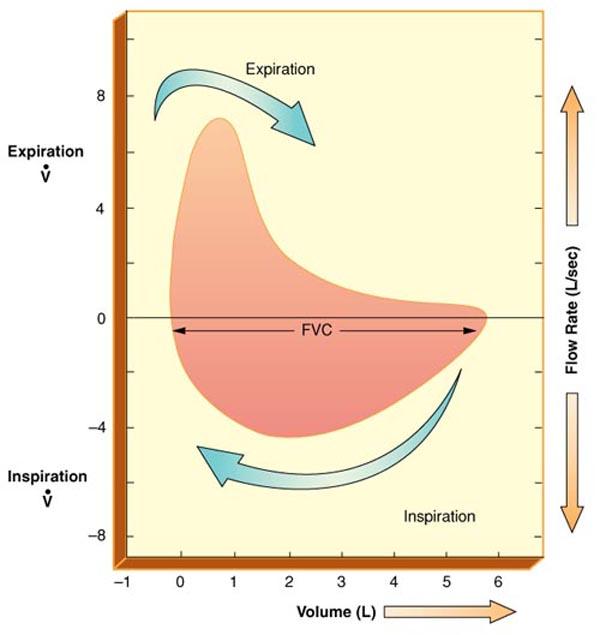
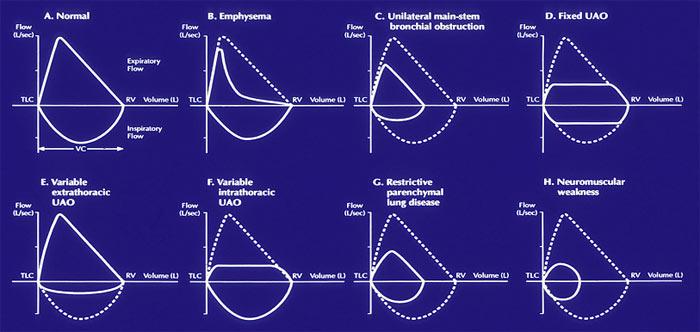
28 Flow Volume Loops Iden-fy inspiratory and expiratory components opposite from ven-lator waveforms! Reveals a pabern typical for certain diseases
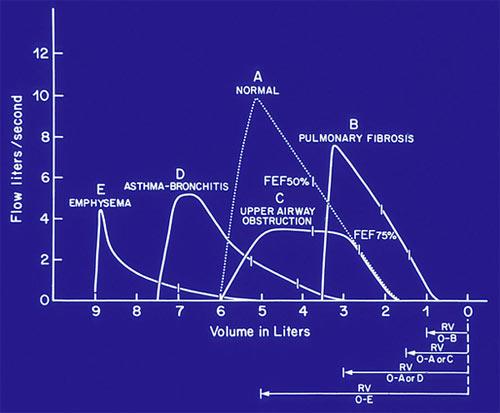
29 Graphic Representa-on of Values

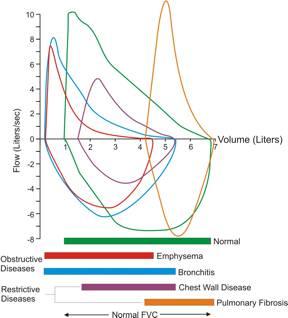
30 Flow Volume Loops Restric6ve Obstruc6ve
31 Figure Flow volume loop. These flow volume loops are typical paberns seen with (A) normal, (B) restric-ve lung diseases, (C) upper airway obstruc-on, and (D) severe chronic obstruc-ve lung disease
32
 variable intrathoracic upper")
33 Flow volume loops of (a) fixed upper airway obstruc-on, (b) variable extrathoracic upper airway obstruc-on, and (c) variable intrathoracic upper airway obstruc-on.
34

35 Iden-fy these loops!
36

37 Bronchodilators Test before and aner to assess the degree of reversibility of the airway obstruc-on Medica-on is not standardized A posi-ve response is demonstrated by: FVC increase >10% FEV 1 increase of 200ml or 15% over baseline FEF 25 75% 20% 30% increase Onen given a trial even if no response is seen

38 Diffusion Capacity (D L ) Represents the gas exchange capabili-es of the lungs Measures the ability of gas to diffuse across the alveolar capillary membrane using carbon monoxide: D L CO

39 D L CO Diseases that reduce surface area D L emphysema Inters--al altering of the membrane integrity D L " Pulmonary fibrosis, Asbestosis, Sarcoidosis
40 Other Studies Airway Resistance Quan-fying allows understanding of the severity of the disease Measured using plethysomograph Compliance Studies Iden-fies the rela-ve s-ffness of the lung Esophageal balloon catheter Nitrogen Washout Determines if there is gross maldistribu-on of ven-la-on Closing Volume Used for diagnosis of small airway obstruc-on Respiratory Quo-ent Determines the amount of carbon dioxide produced and oxygen consumed
41 Exercise Tes-ng 6 minute walk test Anaerobic threshold Exercise challenge Ven-latory Capacity
42 Bronchoprovoca-on Tes-ng Used to diagnose occult asthma Challenge the pa-ent with an inhaled bronchoconstrictor Methacholine (also can use cold air or exercise) Object is to determine the minimum level that elicits a 20% decrease in FEV1 Requires bronchodilator ready for use as well as resuscita-on equipment!
43 ATS Guidelines General Considera6ons for Lung Func6on Tes6ng Standardiza6on of Spirometry Standardiza6on of the Measurements of Lung Volumes Standardiza6on of the single breath determina6on of carbon monoxide uptake in the lung Interpre6ve Strategies for Lung Func6on Tests Cardiopulmonary Exercise Tes6ng Guidelines for the Six minute Walk Test Guidelines for Methacholine and Exercise Challenge Tes6ng
44 ATS (American Thoracic Society) STANDARDS 1. No coughing: especially during first second of FVC 2. Good start of test: <5% of FVC exhaled prior to a max expiratory effort. (<5% extrapola-on) 3. No early termina-on of expira-on: exhala-on -me of six seconds or a plateau of 2 seconds 4. No variable flows: flow rate should be consistent and as fast as possible throughout exhaled VC 5. Good reproducibility or consistency of efforts: 2 best FVC's and 2 best FEV1's should agree within 5% or 100 ml (whichever is greatest)
45 Evalua-on/Interpreta-on of PFT s INTERPRETATION CRITERIA TEST NORMAL MILD MODERATE SEVERE FVC >80% 61 80% 50 60% <50% Restric-on FEV1 >80% 61 80% 50 60% <50% Obstruc-on PEFR >80% 61 80% 50 60% <50% FEF25 75 >80% 61 80% 50 60% <50% Small Airway Disease FEV1/FVC 70 75% 60 69% 50 59% <50% Obstruc-on POSITIVE RESPONSE TO BRONCHODILATOR 1. FVC: increase greater than 10% 2. FEV1: increase of 200cc or 15% over baseline 3. FEF25 75: 20% increase 4. 2 out of 3 should improve to indicate a posi-ve response
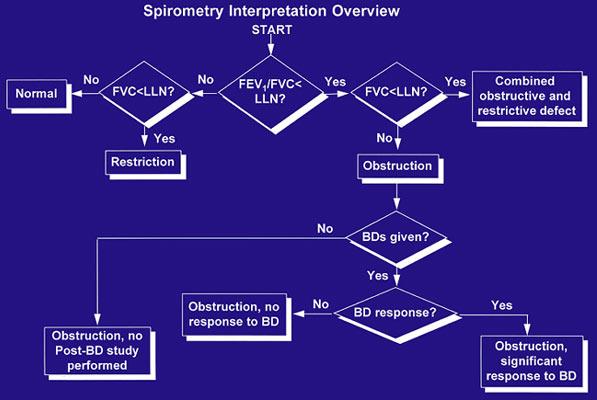
46 Evalua-on of Results Evalua-on of the Vital Capacity can be reduced in obstruc-ve and restric-ve disease if VC is reduced, evaluate the TLC if the TLC is increased = obstruc-on if the TLC is decreased = restric-on if VC is normal, evaluate the TLC if the FVC is greater than 90% of the SVC = normal if the FVC is less than 90% of the SVC = obstruc-on Evalua-on of the FEV1/ FVC if the FEV1/FVC is normal then the lungs are normal or restric-ve if the FEV1/FVC is reduced = obstruc-on
47 Evalua-on of Results Evalua-on of FEF 25 75% if normal then normal lungs or possible restric-on if reduced = peripheral obstruc-on Evalua-on of the Total Lung Capacity: % pred. increased =hyperinfla-on present evaluate the FEV1 Normal = normal lungs Decreased = obstruc-on Decreased evaluate the FEV1 Normal = restric-ve Decreased = obstruc-ve and restric-ve

48 Evalua-on of Results To differen-ate between obstruc-ve and restric-ve diseases u-lize the DLCO as well
49
50 Summary RESTRICTIVE PATTERN 1. Defined on the basis of a reduc-on in both the vital capacity and total lung capacity. 2. Residual volume and other volumes and capaci-es may be variably reduced. 3. Flow rates are normal unless restric-ve process is severe. 4. FEV1 is reduced, but the FEV1/FVC will be normal. OBSTRUCTIVE PATTERN 1. Defined on the basis of a reduc-on in one or more pulmonary flow tests. 2. Vital capacity tends to decrease and the residual volume tends to rise with increasing severity of the disease process causing the obstruc-ve pabern.
51 Cri-cal Thinking Both obstruc-ve and restric-ve diseases may exhibit decreased FVC and FEV1. How can the two kinds of paberns be differen-ated? FVC and FEV1 are reduced in both obstruc-ve and restric-ve disorders for different reasons. With restric-ve disease, lung expansion is reduced and all lung volumes are smaller than normal. With obstruc-ve disease there is airway obstruc-on which slows expiratory flow. FEV1 is reduced because of the increased airway resistance, which decreases expiratory flow rates. FVC is reduced because airway obstruc-on in the bronchioles causes air trapping in the lungs. To differen-ate between obstruc-ve and restric-ve paberns, compare the FEV1 with the FVC using the FEV1/FVC ra-o. Those with airway obstruc-ons will exhale less than 70% of their FVC in the 1st second. Those with restric-ve disease and/or healthy lungs will be able to exhale more than 70% of their FVC in one second.
52 Cri-cal Thinking A pa-ent has spirometry and lung volumes typical of the obstruc-ve pabern. The FEV1, FEV1/FVC and FEF's are significantly reduced and the FRC and TLC are increased. Two common obstruc-ve diseases are chronic bronchi-s and pulmonary emphysema. How can pulmonary func-on data differen-ate between these two diseases? THE DLCO! Chronic bronchi-s involves mostly airways and is characterized by chronic inflamma-on of the mucosa, excessive mucus, and bronchospasm; all of which narrow the airways. Pulmonary emphysema primarily involves alveolar structures and is characterized by destruc-on of alveolar architecture, elas-c fibers, and the alveolar capillary membrane. Emphysema decreases gas exchange surface area. Chronic bronchi-s does not involve alveoli and therefore does not change surface area for gas exchange. A decreased diffusion capacity is associated with emphysema
53 Cri-cal Thinking In the advanced stages of pulmonary emphysema, the FRC and the RV are increased; in addi-on the VC is onen decreased. Why do these changes occur? Emphysema is characterized by a destruc-on of elas-c -ssue in the lung, which causes a lower lung recoil force. When lung recoil forces decrease, as in emphysema, chest wall expansion forces predominate, the chest wall expands outward pulling the lung with it. A new equilibrium occurs at increased lung volume so the FRC is increased. The RV is increased in emphysema because the VC is decreased because of small airway obstruc-on. When a person with emphysema tries to exhale completely, his or her bronchioles collapse, trapping air in the lungs. Increased FRC = hyperinfla-on; Increased RV = air trapping
PULMONARY FUNCTION TESTING. Purposes of Pulmonary Tests. General Categories of Lung Diseases. Types of PF Tests
 PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
PULMONARY FUNCTION TESTS
 Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Chapter 3. Pulmonary Function Study Assessments. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 3 Pulmonary Function Study Assessments 1 Introduction Pulmonary function studies are used to: Evaluate pulmonary causes of dyspnea Differentiate between obstructive and restrictive pulmonary disorders
Chapter 3 Pulmonary Function Study Assessments 1 Introduction Pulmonary function studies are used to: Evaluate pulmonary causes of dyspnea Differentiate between obstructive and restrictive pulmonary disorders
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Coexistence of confirmed obstruction in spirometry and restriction in body plethysmography, e.g.: COPD + pulmonary fibrosis
 Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
6- Lung Volumes and Pulmonary Function Tests
 6- Lung Volumes and Pulmonary Function Tests s (PFTs) are noninvasive diagnostic tests that provide measurable feedback about the function of the lungs. By assessing lung volumes, capacities, rates of
6- Lung Volumes and Pulmonary Function Tests s (PFTs) are noninvasive diagnostic tests that provide measurable feedback about the function of the lungs. By assessing lung volumes, capacities, rates of
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Basic approach to PFT interpretation. Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic
 Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology
 Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
PFT Interpretation and Reference Values
 PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
Spirometry. Obstruction. By Helen Grim M.S. RRT. loop will have concave appearance. Flows decreased consistent with degree of obstruction.
 1 2 Spirometry By Helen Grim M.S. RRT 3 4 Obstruction loop will have concave appearance. Flows decreased consistent with degree of obstruction. Volumes may be normal, but can decrease with severity of
1 2 Spirometry By Helen Grim M.S. RRT 3 4 Obstruction loop will have concave appearance. Flows decreased consistent with degree of obstruction. Volumes may be normal, but can decrease with severity of
Pulmonary Function Testing. Ramez Sunna MD, FCCP
 Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
SPIROMETRY. Marijke Currie (CRFS) Care Medical Ltd Phone: Copyright CARE Medical ltd
 Care Medical Ltd Phone: Copyright CARE Medical ltd") SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual can
SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual can
Pulmonary Function Testing The Basics of Interpretation
 Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
S P I R O M E T R Y. Objectives. Objectives 2/5/2019
 S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
S P I R O M E T R Y. Objectives. Objectives 3/12/2018
 S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
PULMONARY FUNCTION TEST(PFT)
") PULMONARY FUNCTION TEST(PFT) Objectives: By the end of the present lab, students should be able to: 1. Record lung volumes and capacities and compare them with those of a typical person of the same gender,
PULMONARY FUNCTION TEST(PFT) Objectives: By the end of the present lab, students should be able to: 1. Record lung volumes and capacities and compare them with those of a typical person of the same gender,
Content Indica c tion Lung v olumes e & Lung Indica c tions i n c paci c ties
 Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
Respiratory System Mechanics
 M56_MARI0000_00_SE_EX07.qxd 8/22/11 3:02 PM Page 389 7 E X E R C I S E Respiratory System Mechanics Advance Preparation/Comments 1. Demonstrate the mechanics of the lungs during respiration if a bell jar
M56_MARI0000_00_SE_EX07.qxd 8/22/11 3:02 PM Page 389 7 E X E R C I S E Respiratory System Mechanics Advance Preparation/Comments 1. Demonstrate the mechanics of the lungs during respiration if a bell jar
PULMONARY FUNCTION TESTING. By: Gh. Pouryaghoub. MD Center for Research on Occupational Diseases (CROD) Tehran University of Medical Sciences (TUMS)
 Tehran University of Medical Sciences (TUMS)") PULMONARY FUNCTION TESTING By: Gh. Pouryaghoub. MD Center for Research on Occupational Diseases (CROD) Tehran University of Medical Sciences (TUMS) PULMONARY FUNCTION TESTS CATEGORIES Spirometry Lung volumes
PULMONARY FUNCTION TESTING By: Gh. Pouryaghoub. MD Center for Research on Occupational Diseases (CROD) Tehran University of Medical Sciences (TUMS) PULMONARY FUNCTION TESTS CATEGORIES Spirometry Lung volumes
Pulmonary Function Testing
 Pulmonary Function Testing Let s catch our breath Eddie Needham, MD, FAAFP Program Director Emory Family Medicine Residency Program Learning Objectives The Astute Learner will: Become familiar with indications
Pulmonary Function Testing Let s catch our breath Eddie Needham, MD, FAAFP Program Director Emory Family Medicine Residency Program Learning Objectives The Astute Learner will: Become familiar with indications
COMPREHENSIVE RESPIROMETRY
 INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
PULMONARY FUNCTION. VOLUMES AND CAPACITIES
 PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
Respiratory System. Chapter 9
 Respiratory System Chapter 9 Air Intake Air in the atmosphere is mostly Nitrogen (78%) Only ~21% oxygen Carbon dioxide is less than 0.04% Air Intake Oxygen is required for Aerobic Cellular Respiration
Respiratory System Chapter 9 Air Intake Air in the atmosphere is mostly Nitrogen (78%) Only ~21% oxygen Carbon dioxide is less than 0.04% Air Intake Oxygen is required for Aerobic Cellular Respiration
Pulmonary Function Tests. Mohammad Babai M.D Occupational Medicine Specialist
 Pulmonary Function Tests Mohammad Babai M.D Occupational Medicine Specialist www.drbabai.com Pulmonary Function Tests Pulmonary Function Tests: Spirometry Peak-Flow metry Bronchoprovocation Tests Body
Pulmonary Function Tests Mohammad Babai M.D Occupational Medicine Specialist www.drbabai.com Pulmonary Function Tests Pulmonary Function Tests: Spirometry Peak-Flow metry Bronchoprovocation Tests Body
A Primer on Reading Pulmonary Function Tests. Joshua Benditt, M.D.
 A Primer on Reading Pulmonary Function Tests Joshua Benditt, M.D. What Are Pulmonary Function Tests Used For? Pulmonary function testing provides a method for objectively assessing the function of the
A Primer on Reading Pulmonary Function Tests Joshua Benditt, M.D. What Are Pulmonary Function Tests Used For? Pulmonary function testing provides a method for objectively assessing the function of the
Lab 4: Respiratory Physiology and Pathophysiology
 Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
Pulmonary Function Testing
 In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
Breathing and pulmonary function
 EXPERIMENTAL PHYSIOLOGY EXPERIMENT 5 Breathing and pulmonary function Ying-ying Chen, PhD Dept. of Physiology, Zhejiang University School of Medicine bchenyy@zju.edu.cn Breathing Exercise 1: Tests of pulmonary
EXPERIMENTAL PHYSIOLOGY EXPERIMENT 5 Breathing and pulmonary function Ying-ying Chen, PhD Dept. of Physiology, Zhejiang University School of Medicine bchenyy@zju.edu.cn Breathing Exercise 1: Tests of pulmonary
Objectives. Pulmonary Assessment 12/13/2017
 Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
Respiratory Physiology In-Lab Guide
 Respiratory Physiology In-Lab Guide Read Me Study Guide Check Your Knowledge, before the Practical: 1. Understand the relationship between volume and pressure. Understand the three respiratory pressures
Respiratory Physiology In-Lab Guide Read Me Study Guide Check Your Knowledge, before the Practical: 1. Understand the relationship between volume and pressure. Understand the three respiratory pressures
Variation in lung with normal, quiet breathing. Minimal lung volume (residual volume) at maximum deflation. Total lung capacity at maximum inflation
 at maximum deflation. Total lung capacity at maximum inflation") r Total lung capacity at maximum inflation Variation in lung with normal, quiet breathing Volume of lungs at end of normal inspiration (average 2,200 ml) Minimal lung volume (residual volume) at maximum
r Total lung capacity at maximum inflation Variation in lung with normal, quiet breathing Volume of lungs at end of normal inspiration (average 2,200 ml) Minimal lung volume (residual volume) at maximum
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
Lung Pathophysiology & PFTs
 Interpretation of Pulmonary Function Tests (PFTs) Course # 1612 2:00 5:00pm Friday February 22, 2013 Lung Pathophysiology & PFTs Mark F. Sands MD, FCCP, FAAAAI Division of Allergy, Immunology & Rheumatology
Interpretation of Pulmonary Function Tests (PFTs) Course # 1612 2:00 5:00pm Friday February 22, 2013 Lung Pathophysiology & PFTs Mark F. Sands MD, FCCP, FAAAAI Division of Allergy, Immunology & Rheumatology
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Yesterday we spoke of the increased airway resistance and its two examples: 1) emphysema, where we have destruction of the alveolar wall and thus reducing the area available for
بسم هللا الرحمن الرحيم Yesterday we spoke of the increased airway resistance and its two examples: 1) emphysema, where we have destruction of the alveolar wall and thus reducing the area available for
Spirometry: FEVER DISEASE DIABETES HOW RELIABLE IS THIS? 9/2/2010 BUT WHAT WE PRACTICE: Spirometers are objective tools
 SPIROMETRY PRINCIPLES, PROCEDURE AND QA Spirometry: Dr. Rahul Kodgule CHEST RESEARCH FOUNDATION, PUNE FEVER ISCHAEMIC HEART DISEASE DIABETES BUT WHAT WE PRACTICE: Spirometers are objective tools to diagnose
SPIROMETRY PRINCIPLES, PROCEDURE AND QA Spirometry: Dr. Rahul Kodgule CHEST RESEARCH FOUNDATION, PUNE FEVER ISCHAEMIC HEART DISEASE DIABETES BUT WHAT WE PRACTICE: Spirometers are objective tools to diagnose
Spirometry in primary care
 Spirometry in primary care Wednesday 13 th July 2016 Dr Rukhsana Hussain What is spirometry? A method of assessing lung function Measures volume of air a patient can expel after a full inspiration Recorded
Spirometry in primary care Wednesday 13 th July 2016 Dr Rukhsana Hussain What is spirometry? A method of assessing lung function Measures volume of air a patient can expel after a full inspiration Recorded
Physiology lab (RS) First : Spirometry. ** Objectives :-
 First : Spirometry. ** Objectives :-") Physiology lab (RS) ** Objectives :- 1. Spirometry in general. 2. Spirogram (volumes and capacities). 3. The importance of vital capacity in diagnosis. 4. Flow volume loop. 5. Miss Arwa s part (the practical
Physiology lab (RS) ** Objectives :- 1. Spirometry in general. 2. Spirogram (volumes and capacities). 3. The importance of vital capacity in diagnosis. 4. Flow volume loop. 5. Miss Arwa s part (the practical
Assessment of the Lung in Primary Care
 Assessment of the Lung in Primary Care Andrew G Veale FRACP Auckland, New Zealand Presentation Cough (productive or dry) Haemoptysis Shortness of breath / dyspnea Wheeze (or noisy breathing) Chest pain
Assessment of the Lung in Primary Care Andrew G Veale FRACP Auckland, New Zealand Presentation Cough (productive or dry) Haemoptysis Shortness of breath / dyspnea Wheeze (or noisy breathing) Chest pain
Interpreting pulmonary function tests: Recognize the pattern, and the diagnosis will follow
 REVIEW FEYROUZ AL-ASHKAR, MD Department of General Internal Medicine, The Cleveland Clinic REENA MEHRA, MD Department of Pulmonary and Critical Care Medicine, University Hospitals, Cleveland PETER J. MAZZONE,
REVIEW FEYROUZ AL-ASHKAR, MD Department of General Internal Medicine, The Cleveland Clinic REENA MEHRA, MD Department of Pulmonary and Critical Care Medicine, University Hospitals, Cleveland PETER J. MAZZONE,
Spirometry: Introduction
 Spirometry: Introduction Dr. Badri Paudel 1 2 GMC Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.
Spirometry: Introduction Dr. Badri Paudel 1 2 GMC Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.
#8 - Respiratory System
 Page1 #8 - Objectives: Study the parts of the respiratory system Observe slides of the lung and trachea Equipment: Remember to bring photographic atlas. Figure 1. Structures of the respiratory system.
Page1 #8 - Objectives: Study the parts of the respiratory system Observe slides of the lung and trachea Equipment: Remember to bring photographic atlas. Figure 1. Structures of the respiratory system.
Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects
 Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC Benefits and Limitations of Pulmonary Function Testing Benefits
Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC Benefits and Limitations of Pulmonary Function Testing Benefits
Pulmonary Function Test
 Spirometry: Introduction Dr. Badri Paudel GMC Spirometry Pulmonary Function Test! Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after
Spirometry: Introduction Dr. Badri Paudel GMC Spirometry Pulmonary Function Test! Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
In order to diagnose lung diseases doctors
 You Take My Breath Away Activity 5C NOTE: This activity is designed to follow You Really Are Full of Hot Air! Activity Objectives: After completing You Really Are Full of Hot Air! Activity 5B, students
You Take My Breath Away Activity 5C NOTE: This activity is designed to follow You Really Are Full of Hot Air! Activity Objectives: After completing You Really Are Full of Hot Air! Activity 5B, students
Subject Index. Carbon monoxide (CO) disease effects on levels 197, 198 measurement in exhaled air 197 sources in exhaled air 197
 disease effects on levels 197, 198 measurement in exhaled air 197 sources in exhaled air 197") Subject Index Airway resistance airflow interruption measurement in preschoolers, see Forced oscillation technique; Interrupter technique plethysmography, see Plethysmography; Whole-body plethysmography
Subject Index Airway resistance airflow interruption measurement in preschoolers, see Forced oscillation technique; Interrupter technique plethysmography, see Plethysmography; Whole-body plethysmography
Chapter 10 The Respiratory System
 Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Essen%als of Spirometry and Assessment
 Essen%als of Spirometry and Assessment Objectives: 1. Review spirometric acceptability, reproducibility and reporting standards 2. Discuss lung volumes and capacities 3. Discuss Pre & Post bronchodilator
Essen%als of Spirometry and Assessment Objectives: 1. Review spirometric acceptability, reproducibility and reporting standards 2. Discuss lung volumes and capacities 3. Discuss Pre & Post bronchodilator
SPIROMETRY TECHNIQUE. Jim Reid New Zealand
 Jim Reid New Zealand The Basics Jim Reid Spirometry measures airflow and lung volumes, and is the preferred lung function test in COPD. By measuring reversibility of obstruction, it is also diagnostic
Jim Reid New Zealand The Basics Jim Reid Spirometry measures airflow and lung volumes, and is the preferred lung function test in COPD. By measuring reversibility of obstruction, it is also diagnostic
Understanding the Basics of Spirometry It s not just about yelling blow
 Understanding the Basics of Spirometry It s not just about yelling blow Carl D. Mottram, RRT RPFT FAARC Technical Director - Pulmonary Function Labs and Rehabilitation Associate Professor of Medicine -
Understanding the Basics of Spirometry It s not just about yelling blow Carl D. Mottram, RRT RPFT FAARC Technical Director - Pulmonary Function Labs and Rehabilitation Associate Professor of Medicine -
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE
 The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
Spirometry and Flow Volume Measurements
 Spirometry and Flow Volume Measurements Standards & Guidelines December 1998 To serve the public and guide the medical profession Revision Dates: December 1998 Approval Date: June 1998 Originating Committee:
Spirometry and Flow Volume Measurements Standards & Guidelines December 1998 To serve the public and guide the medical profession Revision Dates: December 1998 Approval Date: June 1998 Originating Committee:
The respiratory system
 The respiratory system Practical 1 Objectives Respiration, ventilation Intrapleural and intrapulmonary pressure Mechanism of inspiration and expiration Composition of the atmosphere and the expired air
The respiratory system Practical 1 Objectives Respiration, ventilation Intrapleural and intrapulmonary pressure Mechanism of inspiration and expiration Composition of the atmosphere and the expired air
SPIROMETRY METHOD. COR-MAN IN / EN Issue A, Rev INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark
 SPIROMETRY METHOD COR-MAN-0000-006-IN / EN Issue A, Rev. 2 2013-07 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
SPIROMETRY METHOD COR-MAN-0000-006-IN / EN Issue A, Rev. 2 2013-07 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
BETTER SPIROMETRY. Marijke Currie (CRFS) Care Medical Ltd Phone: Copyright CARE Medical ltd
 Care Medical Ltd Phone: Copyright CARE Medical ltd") BETTER SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual
BETTER SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C
 MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
Quality Assurance Mapping Your QC Program Equipment and Test Quality. Susan Blonshine RRT, RPFT, FAARC, AE-C
 Quality Assurance Mapping Your QC Program Equipment and Test Quality Susan Blonshine RRT, RPFT, FAARC, AE-C How to Begin Gather resources Define PF scope of service Procedures performed Equipment Describe
Quality Assurance Mapping Your QC Program Equipment and Test Quality Susan Blonshine RRT, RPFT, FAARC, AE-C How to Begin Gather resources Define PF scope of service Procedures performed Equipment Describe
How to Perform Spirometry
 Purpose How to Perform Spirometry This guideline provides recommendations regarding best practice to support high quality spirometry practice for KINNECT Pre-Employment Medicals. Scope This guideline provides
Purpose How to Perform Spirometry This guideline provides recommendations regarding best practice to support high quality spirometry practice for KINNECT Pre-Employment Medicals. Scope This guideline provides
UNIT TWO: OVERVIEW OF SPIROMETRY. A. Definition of Spirometry
 UNIT TWO: OVERVIEW OF SPIROMETRY A. Definition of Spirometry Spirometry is a medical screening test that measures various aspects of breathing and lung function. It is performed by using a spirometer,
UNIT TWO: OVERVIEW OF SPIROMETRY A. Definition of Spirometry Spirometry is a medical screening test that measures various aspects of breathing and lung function. It is performed by using a spirometer,
Spirometry Workshop for Primary Care Nurse Practitioners
 Spirometry Workshop for Primary Care Nurse Practitioners Catherine Casey S. Jones PhD, RN, AE-C, ANP-C Certified Adult Nurse Practitioner Texas Pulmonary & Critical Care Consultants P.A. and Adjunct Professor
Spirometry Workshop for Primary Care Nurse Practitioners Catherine Casey S. Jones PhD, RN, AE-C, ANP-C Certified Adult Nurse Practitioner Texas Pulmonary & Critical Care Consultants P.A. and Adjunct Professor
behaviour are out of scope of the present review.
 explained about the test, a trial may be done before recording the results. The maneuver consists initially of normal tidal breathing. The subject then inhales to maximally fill the lungs. This is followed
explained about the test, a trial may be done before recording the results. The maneuver consists initially of normal tidal breathing. The subject then inhales to maximally fill the lungs. This is followed
Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation. Susan Blonshine RRT, RPFT, AE-C, FAARC
 Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation Susan Blonshine RRT, RPFT, AE-C, FAARC Objectives Sample Title Recognize acceptable spirometry that meets the start
Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation Susan Blonshine RRT, RPFT, AE-C, FAARC Objectives Sample Title Recognize acceptable spirometry that meets the start
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
Accurately Measuring Airway Resistance in the PFT Lab
 Accurately Measuring Airway Resistance in the PFT Lab Angela Lorenzo, MS, RRT, RPFT Adjunct Faculty, Long Island University Respiratory Care Division Disclaimer The views in this lecture are those of the
Accurately Measuring Airway Resistance in the PFT Lab Angela Lorenzo, MS, RRT, RPFT Adjunct Faculty, Long Island University Respiratory Care Division Disclaimer The views in this lecture are those of the
Pulmonary Function Laboratory ATS Accreditation Are you prepared? Susan Blonshine RRT, RPFT, FAARC, AE-C
 Pulmonary Function Laboratory ATS Accreditation Are you prepared? Susan Blonshine RRT, RPFT, FAARC, AE-C Why Quality Consistent, accurate, reliable results Cost-effective Diagnosis Misclassification Reduce
Pulmonary Function Laboratory ATS Accreditation Are you prepared? Susan Blonshine RRT, RPFT, FAARC, AE-C Why Quality Consistent, accurate, reliable results Cost-effective Diagnosis Misclassification Reduce
Anatomy & Physiology 2 Canale. Respiratory System: Exchange of Gases
 Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
#7 - Respiratory System
 #7 - Respiratory System Objectives: Study the parts of the respiratory system Observe slides of the lung and trachea Perform spirometry to measure lung volumes Define and understand the lung volumes and
#7 - Respiratory System Objectives: Study the parts of the respiratory system Observe slides of the lung and trachea Perform spirometry to measure lung volumes Define and understand the lung volumes and
Clinical pulmonary physiology. How to report lung function tests
 Clinical pulmonary physiology or How to report lung function tests Lung function testing A brief history Why measure? What can you measure? Interpretation/ reporting Examples and case histories Exercise
Clinical pulmonary physiology or How to report lung function tests Lung function testing A brief history Why measure? What can you measure? Interpretation/ reporting Examples and case histories Exercise
BiomedicalInstrumentation
 University of Zagreb Faculty of Electrical Engineering and Computing BiomedicalInstrumentation Measurementofrespiration prof.dr.sc. Ratko Magjarević October 2013 Respiratorysystem Consistsofthelungs, airways
University of Zagreb Faculty of Electrical Engineering and Computing BiomedicalInstrumentation Measurementofrespiration prof.dr.sc. Ratko Magjarević October 2013 Respiratorysystem Consistsofthelungs, airways
The Aging Lung. Sidney S. Braman MD FACP FCCP Professor of Medicine Brown University Providence RI
 The Aging Lung Sidney S. Braman MD FACP FCCP Professor of Medicine Brown University Providence RI Is the respiratory system of the elderly different when compared to younger age groups? Respiratory Changes
The Aging Lung Sidney S. Braman MD FACP FCCP Professor of Medicine Brown University Providence RI Is the respiratory system of the elderly different when compared to younger age groups? Respiratory Changes
LUNGS. Requirements of a Respiratory System
 Respiratory System Requirements of a Respiratory System Gas exchange is the physical method that organisms use to obtain oxygen from their surroundings and remove carbon dioxide. Oxygen is needed for aerobic
Respiratory System Requirements of a Respiratory System Gas exchange is the physical method that organisms use to obtain oxygen from their surroundings and remove carbon dioxide. Oxygen is needed for aerobic
Respiratory Physiology
 Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
LUNG FUNCTION TESTING: SPIROMETRY AND MORE
 LUNG FUNCTION TESTING: SPIROMETRY AND MORE OBJECTIVES 1. To describe other lung function testing for toddlers and those who cannot perform spirometry 2. To describe a lung function test on infants 3. To
LUNG FUNCTION TESTING: SPIROMETRY AND MORE OBJECTIVES 1. To describe other lung function testing for toddlers and those who cannot perform spirometry 2. To describe a lung function test on infants 3. To
Chapter 11 The Respiratory System
 Biology 12 Name: Respiratory System Per: Date: Chapter 11 The Respiratory System Complete using BC Biology 12, page 342-371 11.1 The Respiratory System pages 346-350 1. Distinguish between A. ventilation:
Biology 12 Name: Respiratory System Per: Date: Chapter 11 The Respiratory System Complete using BC Biology 12, page 342-371 11.1 The Respiratory System pages 346-350 1. Distinguish between A. ventilation:
Spirometry: an essential clinical measurement
 Shortness of breath THEME Spirometry: an essential clinical measurement BACKGROUND Respiratory disease is common and amenable to early detection and management in the primary care setting. Spirometric
Shortness of breath THEME Spirometry: an essential clinical measurement BACKGROUND Respiratory disease is common and amenable to early detection and management in the primary care setting. Spirometric
-SQA-SCOTTISH QUALIFICATIONS AUTHORITY. Hanover House 24 Douglas Street GLASGOW G2 7NQ NATIONAL CERTIFICATE MODULE DESCRIPTOR
 -SQA-SCOTTISH QUALIFICATIONS AUTHORITY Hanover House 24 Douglas Street GLASGOW G2 7NQ NATIONAL CERTIFICATE MODULE DESCRIPTOR -Module Number- 0099111 -Session-1989-90 -Superclass- PB -Title- PRINCIPLES
-SQA-SCOTTISH QUALIFICATIONS AUTHORITY Hanover House 24 Douglas Street GLASGOW G2 7NQ NATIONAL CERTIFICATE MODULE DESCRIPTOR -Module Number- 0099111 -Session-1989-90 -Superclass- PB -Title- PRINCIPLES
Triennial Pulmonary Workshop 2012
 Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM
 CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
UNIVERSITY OF JORDAN DEPT. OF PHYSIOLOGY & BIOCHEMISTRY RESPIRATORY PHYSIOLOGY MEDICAL STUDENTS FALL 2014/2015 (lecture 1)
") UNIVERSITY OF JORDAN DEPT. OF PHYSIOLOGY & BIOCHEMISTRY RESPIRATORY PHYSIOLOGY MEDICAL STUDENTS FALL 2014/2015 (lecture 1) Textbook of medical physiology, by A.C. Guyton and John E, Hall, Twelfth Edition,
UNIVERSITY OF JORDAN DEPT. OF PHYSIOLOGY & BIOCHEMISTRY RESPIRATORY PHYSIOLOGY MEDICAL STUDENTS FALL 2014/2015 (lecture 1) Textbook of medical physiology, by A.C. Guyton and John E, Hall, Twelfth Edition,
Analysis of Lung Function
 Computer 21 Spirometry is a valuable tool for analyzing the flow rate of air passing into and out of the lungs. Flow rates vary over the course of a respiratory cycle (a single inspiration followed by
Computer 21 Spirometry is a valuable tool for analyzing the flow rate of air passing into and out of the lungs. Flow rates vary over the course of a respiratory cycle (a single inspiration followed by
Angela Lorenzo MS, RRT, RPFT Adjunct Faculty, Respiratory Care Long Island University, Brooklyn
 Angela Lorenzo MS, RRT, RPFT Adjunct Faculty, Respiratory Care Long Island University, Brooklyn Disclaimer The views in this lecture are those of the presenter and not those of the Department of Veterans
Angela Lorenzo MS, RRT, RPFT Adjunct Faculty, Respiratory Care Long Island University, Brooklyn Disclaimer The views in this lecture are those of the presenter and not those of the Department of Veterans
The role of Pulmonary function Testing In Interstitial lung disease in infants. [ ipft in child ]
![The role of Pulmonary function Testing In Interstitial lung disease in infants. [ ipft in child ]](/thumbs/77/74805557.jpg "The role of Pulmonary function Testing In Interstitial lung disease in infants. [ ipft in child ]") The role of Pulmonary function Testing In Interstitial lung disease in infants [ ipft in child ] Introduction Managing infants with diffuse lung disease (DLD) suspected to have interstitial lung disease
The role of Pulmonary function Testing In Interstitial lung disease in infants [ ipft in child ] Introduction Managing infants with diffuse lung disease (DLD) suspected to have interstitial lung disease
I LUNG FUNCTION ASSESSMENT AND THORACIC DIAGNOSTIC TECHNIQUES
 I LUNG FUNCTION ASSESSMENT AND THORACIC DIAGNOSTIC TECHNIQUES Roland H. Ingram, jr., m.d. Although the history and physical examination are essential to the diagnostic process, pulmonary signs and symptoms
I LUNG FUNCTION ASSESSMENT AND THORACIC DIAGNOSTIC TECHNIQUES Roland H. Ingram, jr., m.d. Although the history and physical examination are essential to the diagnostic process, pulmonary signs and symptoms
Ch 16 A and P Lecture Notes.notebook May 03, 2017
 Table of Contents # Date Title Page # 1. 01/30/17 Ch 8: Muscular System 1 2. 3. 4. 5. 6. 7. 02/14/17 Ch 9: Nervous System 12 03/13/17 Ch 10: Somatic and Special Senses 53 03/27/17 Ch 11: Endocrine System
Table of Contents # Date Title Page # 1. 01/30/17 Ch 8: Muscular System 1 2. 3. 4. 5. 6. 7. 02/14/17 Ch 9: Nervous System 12 03/13/17 Ch 10: Somatic and Special Senses 53 03/27/17 Ch 11: Endocrine System
DESIGN, ANALYSIS AND IMPLEMENTATION OF SPIROMETER
 DESIGN, ANALYSIS AND IMPLEMENTATION OF SPIROMETER Asmita Parve Mokal1, Dr. M.J. Sheikh2, Bipin D. Mokal3 1M Tech Student, Department of Mechanical Engg, B.D.C.O.E., Sevagram 442102 2Prof and HOD, Department
DESIGN, ANALYSIS AND IMPLEMENTATION OF SPIROMETER Asmita Parve Mokal1, Dr. M.J. Sheikh2, Bipin D. Mokal3 1M Tech Student, Department of Mechanical Engg, B.D.C.O.E., Sevagram 442102 2Prof and HOD, Department
Known Allergies: Shellfish. Symptoms: abdominal pain, nausea, diarrhea, or vomiting. congestion, trouble breathing, or wheezing.
 CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
DIAGNOSTIC ACCREDITATION PROGRAM. Spirometry Quality Control Plan
 DIAGNOSTIC ACCREDITATION PROGRAM Spirometry Quality Control Plan Table of Contents Introduction...1 Spirometry Definitions and Requirements...2 Spirometry Requirements... 2...4 Daily Quality Control (see
DIAGNOSTIC ACCREDITATION PROGRAM Spirometry Quality Control Plan Table of Contents Introduction...1 Spirometry Definitions and Requirements...2 Spirometry Requirements... 2...4 Daily Quality Control (see
Oxygenation. Chapter 45. Re'eda Almashagba 1
 Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
What lung function data are relevant concerning the assessment of COPD patients for out patient rehabilitation?
 What lung function data are relevant concerning the assessment of COPD patients for out patient rehabilitation? An information package on lung function tests and interpretation of test data in identifying
What lung function data are relevant concerning the assessment of COPD patients for out patient rehabilitation? An information package on lung function tests and interpretation of test data in identifying
Preoperative Workup for Pulmonary Resection. Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016
 Preoperative Workup for Pulmonary Resection Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016 Patient Presentation 50 yo male with 70 pack year smoking history Large R hilar lung
Preoperative Workup for Pulmonary Resection Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016 Patient Presentation 50 yo male with 70 pack year smoking history Large R hilar lung
Chapter 10. Respiratory System and Gas Exchange. Copyright 2005 Pearson Education, Inc. publishing as Benjamin Cummings
 Chapter 10 Respiratory System and Gas Exchange Function of the Respiratory System To obtain oxygen (O 2 ) for all cells in the body. To rid the cells of waste gas (CO 2 ). Oxygen (O 2 ) is vital chemical
Chapter 10 Respiratory System and Gas Exchange Function of the Respiratory System To obtain oxygen (O 2 ) for all cells in the body. To rid the cells of waste gas (CO 2 ). Oxygen (O 2 ) is vital chemical
Respiratory System. BSC 2086 A&P 2 Professor Tcherina Duncombe Palm Beach State College
 Respiratory System BSC 2086 A&P 2 Professor Tcherina Duncombe Palm Beach State College Respiration Ventilation of lungs Gas exchange between air/bld and bld/tissue Use of oxygen in cellular respiration
Respiratory System BSC 2086 A&P 2 Professor Tcherina Duncombe Palm Beach State College Respiration Ventilation of lungs Gas exchange between air/bld and bld/tissue Use of oxygen in cellular respiration
Office Spirometry Guide
 Office Spirometry Guide MD Spiro 803 Webster Street, Lewiston ME 04240 Telephone 207-786-7808 1-800-588-3381 Fax 207-786-7280 www.mdspiro.com e-mail: sales@mdspiro.com Why should you perform spirometry
Office Spirometry Guide MD Spiro 803 Webster Street, Lewiston ME 04240 Telephone 207-786-7808 1-800-588-3381 Fax 207-786-7280 www.mdspiro.com e-mail: sales@mdspiro.com Why should you perform spirometry
Credential Maintenance Program
 First Quarter of the Calendar 5 I. INSTRUMENTATION / EQUIPMENT 1 4 5 A. Set Up, Maintain, Calibrate 1 2 3 1. Blood gas analyzers 2. CO-oximeters / hemoximeters 3. Spirometers (for example, diagnostic,
First Quarter of the Calendar 5 I. INSTRUMENTATION / EQUIPMENT 1 4 5 A. Set Up, Maintain, Calibrate 1 2 3 1. Blood gas analyzers 2. CO-oximeters / hemoximeters 3. Spirometers (for example, diagnostic,
Spirometry Technique Maximizing Effort, Comprehension & Coordination
 Spirometry Technique Maximizing Effort, Comprehension & Coordination Carl Mottram, RRT RPFT FAARC Director - Pulmonary Function Labs & Rehabilitation Associate Professor of Medicine - Mayo Clinic College
Spirometry Technique Maximizing Effort, Comprehension & Coordination Carl Mottram, RRT RPFT FAARC Director - Pulmonary Function Labs & Rehabilitation Associate Professor of Medicine - Mayo Clinic College
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings