Dr Rob Young. General Physician Auckland City Hospital
|
|
|
- Sabina Cain
- 6 years ago
- Views:
Transcription

1 Dr Rob Young General Physician Auckland City Hospital
, FRACP, FRCP Department of Medicine,")
2 Managing COPD case studies. Associate Professor Robert Young BMedSc, MBChB, DPhil (Oxon), FRACP, FRCP Department of Medicine, Auckland City Hospital and University of Auckland, New Zealand GP CME 2013, Rotorua

3 3 COPD Management -?confused
4 4 COPD Management -?confused

5 COPD - simplified 5 But how do you define severity?
6 COPD Case Studies key messages 1. COPD is grossly under-diagnosed - spirometry is required to confirm the diagnosis 2. Patients with COPD under-report COPD-related symptoms that reduce their quality of life these should be screened for. 3. The natural history of COPD is highly variable and quite different to asthma know you patient s phenotype and beware of the their co-morbidities.
7 COPD is highly prevalent, underpercieved, underdiagnosed, and undertreated Bart Celli 2008
8 What is COPD and why diagnose it Affects 8% of adult population (1 in 10) Affects 20% of adult smokers (1 in 5) Affects 30% of adult general medical admissions Affects 50% of pneumonia over 65 yrs old COPD and asthma are very different diseases
9 Diagnosis, Assess & Management of COPD Diagnose - assess expiratory flow (spirometry, PEFR) Assess symptoms (CAT and MRC score) exacerbation risk (PHx of exacerbation, FEV 1 %pred) COPD co-morbidities (anxiety/depression, muscle wasting/fatigue) and COPD-related co-morbidities (CHD/CHF, lung cancer, osteoporosis) Manage reduce risk and reduce symptoms
10 Diagnosis, Assess & Management of COPD Diagnose - assess expiratory flow (spirometry, PEFR) Assess Diagnose symptoms (CAT and MRC score) Assess exacerbation risk (PHx of exacerbation, FEV 1 %pred) COPD co-morbidities (anxiety/depression, muscle wasting/fatigue) and COPD-related co-morbidities Manage (CHD/CHF, lung cancer, osteoporosis) Manage reduce risk and reduce symptoms
11 Diagnosis, Assess & Manage COPD Diagnose - assess expiratory flow(spirometry, PEFR) Diagnose Assess symptoms (CAT and MRC score) Assess risk of exacerbations (PHx of exacerbation) Assess COPD comorbidities (anxiety/depression, muscle Assess wasting/fatigue) Assess COPD-related comorbidities (CHD/CHF, lung Manage cancer, osteoporosis) Symptom score Expiratory flow Xacerbation risk Manage reduce risk and reduce symptoms
12 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) New GOLD-defined patient groups Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) but ET= manages hills ok 4 Good QOL CAT<10 (C) (D) Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10 2 or more 3 Poor Spirometry 2 Mildly reduced Spirometry (A) (B) Less than 2 1 Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) but ET=manages hills ok Good QOL CAT>10 mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10
13 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) New GOLD-defined patient groups Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) but ET= manages hills ok 4 Good QOL CAT<10 (C) (D) Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10 2 or more 3 2 Few symptoms Persisting symptoms (A) (B) Less than 2 1 Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) but ET=manages hills ok Good QOL CAT>10 mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10
14 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) New GOLD-defined patient groups Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) but ET= manages hills ok 4 Good QOL CAT<10 3 (C) Moderate (D) Severe Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10 2 or more 2 Mild (A) Moderate (B) Less than 2 1 Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) but ET=manages hills ok Good QOL CAT>10 mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10
15 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) New GOLD-defined patient groups Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) but ET= manages hills ok Good QOL CAT<10 4 Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10 Exacerbator (wet and wheezy) 3 (C) (D) 2 or more Severe (combined) 2 (A) (B) Less than 2 Mild (early) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) but ET=manages hills ok Good QOL CAT<10 1 mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Symptomatic (weak and wheezy) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10
16 Summary table of new recommendations Disease Severity Phenotypic features Treatment A. Mild (early) S E X B. Moderate symptomatic Weak and Wheezy S E X Low Sx score - mmrc 0-1, CAT<10 and Fair Spirometry - FEV 1 GOLD 1-2, and Low exacerbation rate - 0-1/yr High Sx score - mmrc 2+, CAT 10 and Fair Spirometry - FEV 1 GOLD 1-2, or Low exacerbation rate - 0-1/yr SABA or SAMA (prn) LABA or LAMA C. Moderate exacerbator Wet and Wheezy S E X Low Sx score - mmrc 0-1, CAT<10 and Poor Spirometry - FEV 1 GOLD 3-4, or High exacerbation rate - 2+/yr ICS/LABA or LAMA D. Severe (advanced) Wet, Weak and Wheezy S E X High Sx score - mmrc 2+, CAT 10 and Poor Spirometry - FEV 1 GOLD 3-4, and High exacerbation rate - 2+/yr ICS/LABA and LAMA Exacerbation = symptoms of increased cough, SOB ± sputum that required a course of ABs ± prednisone Spirometry FEV 1 /FVC<70% with FEV 1 50% predicted (GOLD1-2) or FEV 1 <50% predicted (GOLD3-4) 16
17 Case presentation Male 63 yo PC: HPc: 3 days of cough and sputum, mild shortness of breath Previously well
18 Case presentation Male 63 yo PC: HPc: PHx: 3 days of cough and sputum, mild shortness of breath Previously well Peptic ulcer 5 yrs ago 3 LRTI over the last 5 years Benign colon polyps
19 Case presentation Male 63 yo PC: HPc: PHx: SHx 3 days of cough and sputum, mild shortness of breath Previously well Peptic ulcer 5 yrs ago 3 LRTI over the last 5 years, last 3/12 ago Benign colon polyps Lives with his wife, retired builder, property developer, smoker with a 30 pk yr history
20 Case presentation Male 63 yo PC: HPc: PHx: SHx 3 days of cough and sputum, mild shortness of breath Previously well Peptic ulcer 5 yrs ago 3 LRTI over the last 5 years, last 3/12 ago Benign colon polyps Lives with his wife, retired builder, property developer, smoker with a 30 pk yr history
21 Case presentation Occ Hx: No dust/asbestos exposure Exam Afebrile and productive cough Chest scattered wheeze and crackles
22 Case presentation Occ Hx: No dust/asbestos exposure Exam Afebrile and productive cough Chest scattered wheeze and crackles Diagnosed with LRTI and treated with antibiotics
23 Role of Spirometry Symptom score Expiratory flow Xacerbation risk
24 Diagnosis, Assess & Management of COPD Diagnose - assess expiratory flow (spirometry, PEFR) Assess symptoms (CAT and MRC score) exacerbation risk (PHx of exacerbation, FEV 1 %pred) COPD co-morbidities (anxiety/depression, muscle wasting/fatigue) and COPD-related co-morbidities (CHD/CHF, lung cancer, osteoporosis) Manage reduce risk and reduce symptoms
25 Clinical cases at risk patients Patient >40 years old with respiratory symptoms of LRTI and/or Past smoking history or equivalent dust/occupational Hx Requires assessment to Identify the presence of COPD (spirometry) Identify other undisclosed symptoms relevant to QOL Quantify risk of disease progression/exacerbations Facilitate directed therapy and lifestyle changes

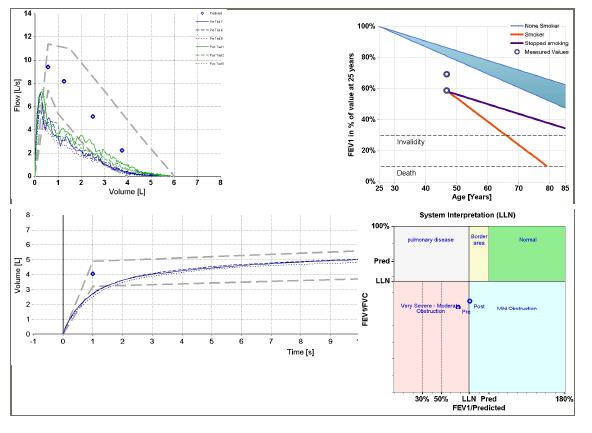
26 Spirometry and lung age
27 27 Decline of Lung Function: variable susceptibility
28 Decline in lung function with COPD severity Nonsmoker decline is ml/yr
29 Decline in lung function with COPD severity Diagnosed with screening spirometry of smokers/ex-smokers Diagnosed with recurrent episodes of SOB/cough/sputum/wheeze (AECOPD)
30 Case presentation Occ Hx: No dust/asbestos exposure Exam Invest Afebrile and productive cough Chest scattered wheeze and crackles Spirometry: FEV1=2.4 (60%), FEV/FVC=60% Diagnosed with asthma and treated with antibiotics and inhaler (SABA prn).
31 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) New GOLD-defined patient groups Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) but ET= manages hills ok Good QOL CAT<10 4 Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10 Exacerbator (wet and wheezy) 3 (C) (D) 2 or more Severe (combined) 2 (A) (B) Less than 2 Mild (early) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) but ET=manages hills ok Good QOL CAT<10 1 mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Symptomatic (weak and wheezy) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10
32 Summary table of new recommendations Disease Severity Phenotypic features Treatment A. Mild (early) S E X B. Moderate symptomatic Weak and Wheezy S E X Low Sx score - mmrc 0-1, CAT<10 and Fair Spirometry - FEV 1 GOLD 1-2, and Low exacerbation rate - 0-1/yr High Sx score - mmrc 2+, CAT 10 and Fair Spirometry - FEV 1 GOLD 1-2, or Low exacerbation rate - 0-1/yr SABA or SAMA (prn) LABA or LAMA C. Moderate exacerbator Wet and Wheezy S E X Low Sx score - mmrc 0-1, CAT<10 and Poor Spirometry - FEV 1 GOLD 3-4, or High exacerbation rate - 2+/yr ICS/LABA or LAMA D. Severe (advanced) Wet, Weak and Wheezy S E X High Sx score - mmrc 2+, CAT 10 and Poor Spirometry - FEV 1 GOLD 3-4, and High exacerbation rate - 2+/yr ICS/LABA and LAMA Exacerbation = symptoms of increased cough, SOB ± sputum that required a course of ABs ± prednisone Spirometry FEV 1 /FVC<70% with FEV 1 50% predicted (GOLD1-2) or FEV 1 <50% predicted (GOLD3-4) 32
33 Case Presentation Occ Hx: No dust/asbestos exposure Exam Afebrile and productive cough Chest scattered wheeze and crackles Invest Spirometry: FEV1=2.4 (60%), FEV/FVC=60% Diagnosed with asthma and treated with antibiotics and inhalers.. but breathlessness persisted for 6 weeks
34 Case Presentation Occ Hx: No dust/asbestos exposure Exam Afebrile and productive cough Chest scattered wheeze and crackles Invest Spirometry: FEV1=2.4 (60%), FEV/FVC=60% Diagnosed with asthma and treated with antibiotics and inhalers.. but breathlessness persisted for 6 weeks Repeat spirometry was unchanged, progressive SOBOE for 3 years and now diagnosed with COPD and put on LABA and ICS
35 Case Presentation Occ Hx: No dust/asbestos exposure Exam Afebrile and productive cough Chest scattered wheeze and crackles Invest Spirometry: FEV1=2.4 (60%), FEV/FVC=60% Diagnosed with asthma and treated with antibiotics and inhalers.. but breathlessness persisted for 6 weeks DAM Yes SEX - No
36 GOLD Strategy Document 2011 ( Management of COPD the aims Reduce symptoms Reduce risk Relieve symptoms Improve exercise tolerance Improve health status Prevent disease progression Prevent and treat exacerbations Reduce mortality
37 Role of Exacerbation History Symptom score Expiratory flow Xacerbation risk
38 Case presentation Male 63 yo PC: HPc: PHx: SHx 3 days of cough and sputum, mild shortness of breath Previously well Peptic ulcer 5 yrs ago 3 LRTI over the last 5 years, last 3/12 ago Benign colon polyps Lives with his wife, retired builder, property developer, smoker with a 30 pk yr history
39 Risk factors for future exacerbations Past history of exacerbations (<1 /yr and 1/yr) Poor lung function (GOLD 3 and 4) mmrc score >2 or CAT score >10 Low DLCO or emphysema on CT
40 Exacerbation of COPD = Lung Attack Hospitalisation for AECOPD Outcome same as for heart attack - 8% inpatient mortality - 25% mortality in the next 1 year Identifies a high risk group regardless of spirometry result (COPD severity)

41 Development and progression of COPD FEV 1 vs symptoms 41
42 % of patients The frequent exacerbator phenotype : Frequency/severity by GOLD Category (1) 50 p< GOLD II (N=945) GOLD III (N=900) GOLD IV (N=293) Hospitalised for exacerbation in yr 1 Frequent exacerbations (2 or more) ECLIPSE 1 year data Hurst et al. N Engl J Med 2010
43 Frequent exacerbators represent stable COPD phenotype - independent of severity Proportion of subjects experiencing 2 exacerbations/year increases year-on-year Stable population provides potential to understand the cause(s) of the phenotype 2 Exacerb./Yr 1 Exacerb./Yr 0 Exacerb./Yr 100% % % 40% % 492 0% ECLIPSE 3 year data Year 1 Year 2 Year 3 Hurst et al. N Engl J Med 2010
44 Consequences of COPD exacerbations Negative impact on quality of life Impact on symptoms and lung function Accelerated lung function decline EXACERBATIONS Increased Mortality Increased economic costs
45 When to add the steroids ICS are needed when patients suffer recurrent exacerbations characterised by productive cough and SOB. ICS with LABA are superior to ICS alone and shown to improve lung function, quality of life and survival as do LAMA (TORCH/UPLIFT study). Oral steroids for 3-10 days are useful for exacerbations characterised by SOB with productive cough. 45
46 Rate of moderate and severe exacerbations over three years Mean number of exacerbations/year NNT to prevent 1 exacerbation in 1 year = % reduction * 0.93* 0.85* Placebo SALM FP SFC Treatment *p < vs placebo; p = vs SALM; p = vs FP Calverley et al. NEJM 2007
47 Rate of exacerbations requiring systemic corticosteroids over three years Mean number of exacerbations/year % reduction * 0.52* 0.46* 0 Placebo SALM FP SFC Treatment *p < vs placebo; p < vs SALM; p = vs FP Calverley et al. NEJM 2007
48 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) New GOLD-defined patient groups Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) but ET= manages hills ok Good QOL CAT<10 4 Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10 Exacerbator (wet and wheezy) 3 (C) (D) 2 or more Severe (combined) 2 (A) (B) Less than 2 Mild (early) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) but ET=manages hills ok Good QOL CAT<10 1 mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Symptomatic (weak and wheezy) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10
49 Role of the Symptom Score Symptom score Expiratory flow Xacerbation risk

50 No correlation between QOL and FEV 1 severity 100 Stage 4 Stage 3 Stage 2 80 SGRQ score (CAT) Breathless walking on level ground 20 0 Upper limit of normal r = 0.23 P< FEV 1 (% predicted)
51 6MWD (Metres) Number of exacerbations mmrc score SGRQ-C Total score ECLIPSE showed weak correlation between disease outcome parameters & FEV Post-Dose FEV 1 (% Pred.) Rho=-0.36 p< Post-Dose FEV 1 (% Pred.) Rho=-0.38 p< Post-Dose FEV 1 (% Pred.) Rho=-0.34 p< Post-Dose FEV 1 (% Pred.) Rho=-0.21 p<0.001 Agusti et al. Resp Res 2010
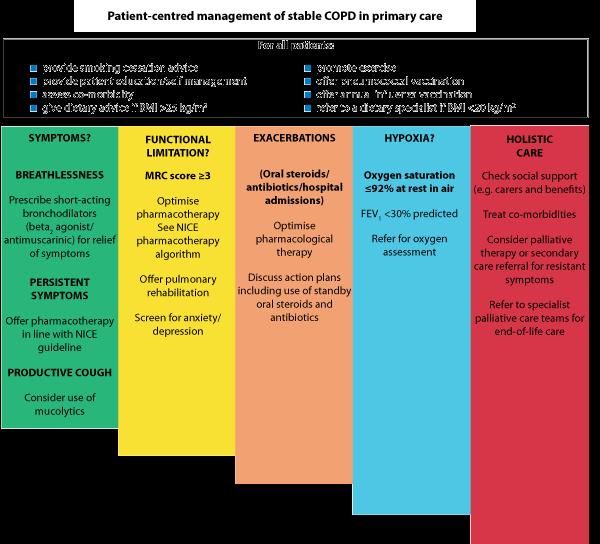
52 Treatment options in COPD a symptom based approach Spirometry document severity of airways obstruction (confirm diagnosis, end organ damage) Establish symptom profile (CAT) or mmrc breathlessness score (when well ) - tendency to LRTI, ABs course, prednisone course, AECOPD, hospitalisation for acute exacerbations. 52
53 Modified MRC Breathlessness Score Grade Description of Breathlessness 0 I only get breathless with strenuous exercise I get short of breath when hurrying on level ground or walking up a slight hill. On level ground, I walk slower than people of the same age because of breathlessness, or have to stop for breath when walking at my own pace. I stop for breath after walking about 100 yards or after a few minutes on level ground. I am too breathless to leave the house or I am breathless when dressing.
54 The CAT questionnaire (download from - Cough Phlegm Tight SOB Activity Confidence Sleep Energy A symptom based approach CAT COPD Self Assessment Test Score/40 - mild mod severe very severe Basis on which to establish - overall disability - specific disabilities and - response to treatments
 WET WHEEZY WEAK Cough Phlegm Tight SOB Activity Confidence Sleep Energy A symptom")

55 The CAT questionnaire (download from - WET WHEEZY WEAK Cough Phlegm Tight SOB Activity Confidence Sleep Energy A symptom based approach CAT COPD Self Assessment Test Score/40 - mild mod severe very severe Basis on which to establish - overall disability - specific disabilities and - response to treatments
56 Mr Smith s history CAT Score 1 Cough no morning or night-time cough, coughs with colds and chest infections only Phlegm - no morning or night-time phlegm, phlegm with colds and chest infections only Chest tightness feels chest tightness with walking up hills or one flight of stairs, or with colds or chest infections. Exertional breathlessness stops for breath after 200m and after climbing 8 steps at home
57 Mr Smith s history CAT Score 2 Limited with home activities can mow the lawn on the flat but takes longer, gardening with effort Confident leaving home hesitant to walk to the local shops now, can only walk 200 m on the flat Sleep sleeps on 2-3 pillows to help breathing, not generally woken by breathlessness or cough, up to toilet 2-3 times to pass urine Energy levels a bit frustrated as only leaves house for trips in the car, no longer playing golf, feels tired after outings to see friends or family.

58 CAT Score patient data X X X WHEEZY X 4 WEAK X X X CAT Score/40 - mild mod severe very severe Scoring range 0-40 X Total score 3 20 Severe
59 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) New GOLD-defined patient groups Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) but ET= manages hills ok Good QOL CAT<10 4 Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10 Exacerbator (wet and wheezy) 3 (C) (D) 2 or more Severe (combined) 2 (A) (B) Less than 2 Mild (early) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) but ET=manages hills ok Good QOL CAT<10 1 mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Symptomatic (weak and wheezy) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10
60 Diagnosis, Assess & Manage COPD Diagnose - assess expiratory flow(spirometry, PEFR) Diagnose Assess symptoms (CAT and MRC score) Assess risk of exacerbations (PHx of exacerbation) Assess COPD comorbidities (anxiety/depression, muscle Assess wasting/fatigue) Assess COPD-related comorbidities (CHD/CHF, lung Manage cancer, osteoporosis) Symptom score Expiratory flow Xacerbation risk Manage reduce risk and reduce symptoms
61 Management of COPD - summary At risk patients Spirometry Smoking cessation Reg LABA Mild Intermitant Sx Mild Persistant Sx CAT questionnaire Vaccinations Prn SABA Reg LABA Infective exacerbators LABA + ICS Mod Persisting Sx LABA + ICS ± LAMA Significant Disability Significant Co-morbidity ± LAMA LTOT Volume reduction/valve surgery CVS risk Lung cancer sx 61
62 A symptom based approach Smoking and aero-pollutant (dust) avoidance Yearly Flu vaccination, 5 yearly pneumococcal vaccination and regular exercise Exertional SOB- prn bronchodilators (SABA) Fatigue + poor ET reg bronchodilators (LABA and LAMA (*FEV1<60% predicted for Tiotropium)) LRTI/bronchitis/AECOPD Inhaled corticosteroids with LABA or LAMA (*FEV1<60% predicted) 2+ Hospitalisations/yr triple therapy
63 A symptom based approach HEED study Lung function alone is a poor predictor of symptoms Symptoms of COPD should be assessed regularly in patients with COPD (self administered CAT questionnaire, Reduced exercise tolerance was seen in 70% with mild disease (%predfev1>80%) and 74% with moderate disease (%predfev %). Jones P et al. Respir Med. 2010;105(1):57-66
64 Treatment options in COPD a symptom based approach Spirometry document severity of airways obstruction (confirm diagnosis, end organ damage) Establish symptom profile (CAT), tendency to LRTI, AECOPD, hospitalisation for acute exacerbations (direct inhaler treatment). Consider COPD a CVS risk factor Consider COPD a precursor to lung cancer 64
65 Summary table of new recommendations Disease Severity Phenotypic features Treatment A. Mild (early) S E X B. Moderate symptomatic Weak and Wheezy S E X Low Sx score - mmrc 0-1, CAT<10 and Fair Spirometry - FEV 1 GOLD 1-2, and Low exacerbation rate - 0-1/yr High Sx score - mmrc 2+, CAT 10 and Fair Spirometry - FEV 1 GOLD 1-2, or Low exacerbation rate - 0-1/yr SABA or SAMA (prn) LABA or LAMA C. Moderate exacerbator Wet and Wheezy S E X Low Sx score - mmrc 0-1, CAT<10 and Poor Spirometry - FEV 1 GOLD 3-4, or High exacerbation rate - 2+/yr ICS/LABA or LAMA D. Severe (advanced) Wet, Weak and Wheezy S E X High Sx score - mmrc 2+, CAT 10 and Poor Spirometry - FEV 1 GOLD 3-4, and High exacerbation rate - 2+/yr ICS/LABA and LAMA Exacerbation = symptoms of increased cough, SOB ± sputum that required a course of ABs ± prednisone Spirometry FEV 1 /FVC<70% with FEV 1 50% predicted (GOLD1-2) or FEV 1 <50% predicted (GOLD3-4) 65
66 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) X X X X 4 X X (C) (D) 2 or more X X (A) (B) Less than 2 Scoring range 0-40 Total score mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Questions?
67 Case Presentation Diagnosed with asthma and treated with antibiotics, inhalers and a short course of prednisone.. Symptoms of breathlessness improved
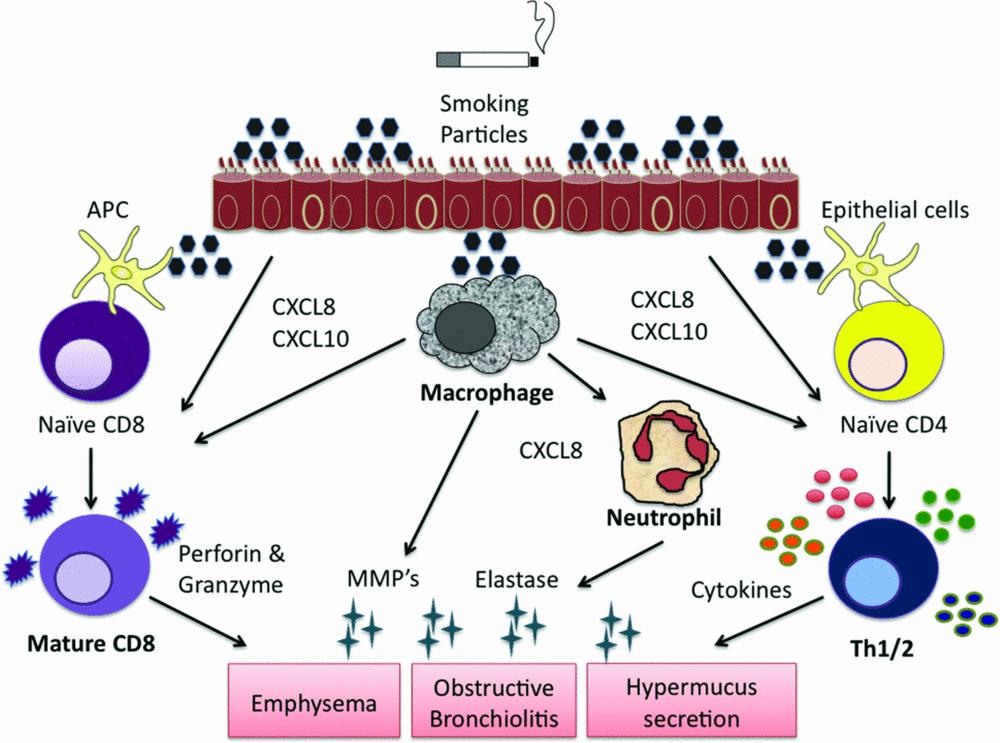
68 Case Presentation Diagnosed with asthma and treated with antibiotics, inhalers and a short course of prednisone. Symptoms of breathlessness improved.. But cough persisted for 6 months

69 Case Presentation CXR was normal but CT confirmed 2.5 cm LUL mass with +nodes Bronchoscopy confirmed squamous cell lung cancer
70 Diagnosed with asthma and treated with inhalers.. but cough persisted for 6 months CXR showed an opacity and CT confirmed 3 cm LUL mass with +nodes Bronchoscopy confirmed squamous cell LC

71 CXR Low sensitivity for detecting non-ca pulmonary nodules
72 COPD overlap with lung cancer Cigarettes Lung Cancer Emphysema/COPD 72
73 Progress: Patient underwent several courses of chemotherapy with small effect Died 18 months later Reflections: Patients express have feeling of guilt and regret acknowledge they should have given up sooner acceptance they are to blame although some identify other exposures that might have been relevant Recent studies report that over 50% of smokers and ex-smokers who get lung cancer did not think they were at risk!

74 Step 4 Eur Respir J 2009; 33: PJ Barnes and BR Celli 74

75 Decline of Lung Function: variable susceptibility FEV1: other morbidities apart from COPD - 5x Lung cancer -5x heart attack x stroke (Young et al. ERJ 2007)
 (B) Less than 2 Scoring range 0-40 Total score 22 76 mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Questions?")
76 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) X X X X 4 X X (C) (D) 2 or more X X (A) (B) Less than 2 Scoring range 0-40 Total score mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Questions?
77 What is COPD and why diagnose it Results from genetic susceptibility and aeropollutant (smoking) exposure Neutrophilic airway inflammation Presents with exertional breathlessness and LRTI (cough, sputum, wheeze and SOB) Fatigue and poor exercise tolerance Systemic inflammation and co-morbidities Precursor illness to 70-80% of all lung cancer

78 Step 1 Genetic susceptibility Combined effects of susceptibility and protective genetic effects
79 Step 2

80 Young RP, et al. (European Respir Review 2009) Step 3
81 A symptom based approach Eclipse study Frequent exacerbator* is a specific type of COPD that requires aggressive treatment with combination therapy (preferably fixed dose ICS and LABA) Frequent exacerbators may be found in those with moderate COPD (22%) and not just severe disease (30-50%). * 2+ exacerbations per year Hurst J et al. N Engl J Med. 2010;363:
82 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) New GOLD patient groups 4 (C) (D) 2 or more 3 2 (A) (B) Less than 2 1 mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Symptoms and Risk
83 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) New GOLD-defined patient groups Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) but ET= manages hills ok 4 Good QOL CAT<10 (C) (D) Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10 2 or more 3 2 (A) (B) Less than 2 1 Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) but ET=manages hills ok Good QOL CAT>10 mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10
84 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) New GOLD-defined patient groups Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) but ET= manages hills ok 4 Good QOL CAT<10 3 (C) Exacerbator (D) Severe (both) Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10 2 or more 2 Mild (early) (A) Symptomatic (B) Less than 2 1 Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) but ET=manages hills ok Good QOL CAT>10 mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10
 or 2+ exacerbations/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10 Exacerbator (wet and wheezy) 3 (C) (D) 2 or more Severe (combined) 2")
85 RISK* (GOLD Classification of Airflow Limitation) RISK* (Exacerbation history) New GOLD-defined patient groups Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) but ET= manages hills ok Good QOL CAT<10 4 Poor spirometry (FEV%pred 50%) or 2+ exacerbations/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10 Exacerbator (wet and wheezy) 3 (C) (D) 2 or more Severe (combined) 2 (A) (B) Less than 2 Mild (early) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) but ET=manages hills ok Good QOL CAT<10 1 mmrc 0-1 mmrc > 2 CAT <10 CAT >10 SYMPTOMS (mmrc or CAT score) Symptomatic (weak and wheezy) Reduced spirometry (FEV%pred>50%) or 0-1 exacerbation/yr (AB/pred/yr) and ET SOB up slight hills Poor QOL CAT 10
86 Beyond the airways Muscle fatigue, muscle weakness and cachexia (pulmonary rehab and optimised nutrition) Cardiovascular disease, stroke, CHF, pulmonary hypertension (aspirn, statin and β-blockers) Insulin resistance, metabolic syndrome, obesity (exercise, calorie restriction, wght loss) Osteoporosis (bisphosphonates)
87 Beyond the airways Future treatments will look to reduce [dynamic] hyperinflation measured as IC/TLC ratio rather than to use FEV 1 as a measure of outcome. Recent studies suggest that statins reduce hyperinflation by reducing inflammation, improving endothelial function and dilating small airways (clinical trial underway). Role of cardiovascular drugs in reducing CVS risk during COPD exacerbations
88 COPD and lung cancer COPD increases the risk of lung cancer by 4-6 fold compared to smokers with normal lung function % of lung cancer has pre-existing COPD 20-30% of deaths in COPD are from lung cancer

89 COPD overlap with lung cancer Cigarettes Lung Cancer Emphysema/COPD 89
Modern Management of COPD.
 Modern Management of COPD. Associate Professor Robert Young BMedSc, MBChB, DPhil (Oxon), FRACP, FRCP Department of Medicine, Auckland City Hospital and University of Auckland, New Zealand 2 Sponsor Disclaimer
Modern Management of COPD. Associate Professor Robert Young BMedSc, MBChB, DPhil (Oxon), FRACP, FRCP Department of Medicine, Auckland City Hospital and University of Auckland, New Zealand 2 Sponsor Disclaimer
Changing Landscapes in COPD New Zealand Respiratory Conference
 Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Dr Stephen Child. General Physician Auckland. 14:20-14:40 Secondary Care Perspective
 Dr Stephen Child General Physician Auckland 14:20-14:40 Secondary Care Perspective Wheeze Witchery Stephen Child MD, FRACP, FRCPC General Physician Respiratory Interest Director of Clinical Training Auckland
Dr Stephen Child General Physician Auckland 14:20-14:40 Secondary Care Perspective Wheeze Witchery Stephen Child MD, FRACP, FRCPC General Physician Respiratory Interest Director of Clinical Training Auckland
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Statins in lung disease
 Statins in lung disease Associate Professor Robert Young BMedSc, MBChB, DPhil (Oxon), FRACP, FRCP University of Auckland, New Zealand Smoking and its complications Respiratory COPD Cardiovascular CAD Smoking
Statins in lung disease Associate Professor Robert Young BMedSc, MBChB, DPhil (Oxon), FRACP, FRCP University of Auckland, New Zealand Smoking and its complications Respiratory COPD Cardiovascular CAD Smoking
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD GOLD Guidelines & Barnet inhaler choices. Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust
 COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university
 What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Curriculum Vitae. Head of Public Wing HCU - RSCM. Head of ICU Sari Asih Ciledug Hospital
 Curriculum Vitae Name : Dr. Ceva W. Pitoyo,SpPD,K-P,KIC,FINASIM POB / DOB : Jakarta, March 8th 1968 Education : o General Practitioner : FKUI 1993 o Internist : FKUI 2002 o Pulmonology Consultant : PAPDI-UI
Curriculum Vitae Name : Dr. Ceva W. Pitoyo,SpPD,K-P,KIC,FINASIM POB / DOB : Jakarta, March 8th 1968 Education : o General Practitioner : FKUI 1993 o Internist : FKUI 2002 o Pulmonology Consultant : PAPDI-UI
COPD in primary care: reminder and update
 COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013
 COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013 None Disclosures Definitions Asthma Asthma is a chronic inflammatory
COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013 None Disclosures Definitions Asthma Asthma is a chronic inflammatory
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Turning Science into Real Life Roflumilast in Clinical Practice. Roland Buhl Pulmonary Department Mainz University Hospital
 Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น
 รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
Life-long asthma and its relationship to COPD. Stephen T Holgate School of Medicine University of Southampton
 Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Common Pulmonary Problems. Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine
 Common Pulmonary Problems Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Obstructive
Common Pulmonary Problems Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Obstructive
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research
 Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
GOLD UPDATE on COPD and the Importance of Accurate Dyspnea Evaluation
 GOLD UPDATE on COPD and the Importance of Accurate Dyspnea Evaluation George Anderson, PhD Sr. Medical Science Liaison MA-AZAP ML-4006-US-0212 Approved 11/16 Glob al Strategy for the Diagnosis, Management,
GOLD UPDATE on COPD and the Importance of Accurate Dyspnea Evaluation George Anderson, PhD Sr. Medical Science Liaison MA-AZAP ML-4006-US-0212 Approved 11/16 Glob al Strategy for the Diagnosis, Management,
What is COPD? COPD Pharmacotherapy. COPD Mortality Is Increasing
 COPD Pharmacotherapy Chronic Bronchitis What is COPD? 75% 17.5% Emphysema Laura C. Feemster, MD, MS Assistant Professor University of Washington Division of Pulmonary & Critical Care April 23,2015 COPD
COPD Pharmacotherapy Chronic Bronchitis What is COPD? 75% 17.5% Emphysema Laura C. Feemster, MD, MS Assistant Professor University of Washington Division of Pulmonary & Critical Care April 23,2015 COPD
Objectives. Advances in Managing COPD Patients
 4:45 5:30pm Advances in Managing Patients SPEAKER Nicola Hanania, MD, FCCP, FRCP, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Nicola Hanania, MD,
4:45 5:30pm Advances in Managing Patients SPEAKER Nicola Hanania, MD, FCCP, FRCP, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Nicola Hanania, MD,
COPD in Korea. Division of Pulmonary, Allergy and Critical Care Medicine of Hallym University Medical Center Park Yong Bum
 COPD in Korea Division of Pulmonary, Allergy and Critical Care Medicine of Hallym University Medical Center Park Yong Bum Mortality Rate 1970-2002, USA JAMA,2005 Global Burden of Disease: COPD WHO & World
COPD in Korea Division of Pulmonary, Allergy and Critical Care Medicine of Hallym University Medical Center Park Yong Bum Mortality Rate 1970-2002, USA JAMA,2005 Global Burden of Disease: COPD WHO & World
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management. Colleen Sakon, PharmD BCPS September 27, 2018
 Management. Colleen Sakon, PharmD BCPS September 27, 2018") Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
PFT s / 2017 Pulmonary Update. Eric S. Papierniak, DO University of Florida NF/SG VHA
 PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
Current Approaches to Asthma & COPD
 10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Re-Screening Medical History Questionnaire
 Building Trades National Medical Screening Program Re-Screening Medical History Questionnaire Name: Address: _ City: _State: Zip Phone Number (include Area Code): Social Security # Date of Birth If female,
Building Trades National Medical Screening Program Re-Screening Medical History Questionnaire Name: Address: _ City: _State: Zip Phone Number (include Area Code): Social Security # Date of Birth If female,
Online Data Supplement. Prevalence of Chronic Obstructive Pulmonary Disease in Korea: Results of a Population-based Spirometry Survey
 Online Data Supplement Prevalence of Chronic Obstructive Pulmonary Disease in Korea: Results of a Population-based Spirometry Survey Dong Soon Kim, MD, Young Sam Kim MD, Kee Suk Chung MD, Jung Hyun Chang
Online Data Supplement Prevalence of Chronic Obstructive Pulmonary Disease in Korea: Results of a Population-based Spirometry Survey Dong Soon Kim, MD, Young Sam Kim MD, Kee Suk Chung MD, Jung Hyun Chang
SABA: VENTOLIN EVOHALER (SALBUTAMOL) SAMA: ATROVENT IPRATROPIUM. Offer LAMA (discontinue SAMA) OR LABA
 SAMA: ATROVENT IPRATROPIUM. Offer LAMA (discontinue SAMA) OR LABA") COPD GUIDELINES DIAGNOSIS >35 years of age Symptoms of cough, breathlessness, sputum, wheeze, Risk factor (SMOKING) Spirometry (post bronchodilator) FEV1/FVC = 0.7 ENCOURAGE PATIENTS TO BRING INHALERS
COPD GUIDELINES DIAGNOSIS >35 years of age Symptoms of cough, breathlessness, sputum, wheeze, Risk factor (SMOKING) Spirometry (post bronchodilator) FEV1/FVC = 0.7 ENCOURAGE PATIENTS TO BRING INHALERS
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
ASTHMA. Dr Liz Gamble BRI
 ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
Algorithm for the use of inhaled therapies in COPD Version 2 May 2017
 Algorithm for the use of inhaled therapies in COPD This document has been revised by the Berkshire West Respiratory Network to support clinicians in selecting the most appropriate, cost effective treatments
Algorithm for the use of inhaled therapies in COPD This document has been revised by the Berkshire West Respiratory Network to support clinicians in selecting the most appropriate, cost effective treatments
Potential risks of ICS use
 Potential risks of ICS use Randomised controlled trial Observational study Systematic review Pneumonia Tuberculosis Bone fracture Skin thinning/easy bruising Cataract Diabetes No effect on fracture risk
Potential risks of ICS use Randomised controlled trial Observational study Systematic review Pneumonia Tuberculosis Bone fracture Skin thinning/easy bruising Cataract Diabetes No effect on fracture risk
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD)
") Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) Zahava Picado, PharmD PGY1 Pharmacy Practice Resident Central Texas Veterans Healthcare System Temple, TX October
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) Zahava Picado, PharmD PGY1 Pharmacy Practice Resident Central Texas Veterans Healthcare System Temple, TX October
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
UNDERSTANDING COPD MEDIA BACKGROUNDER
 UNDERSTANDING COPD MEDIA BACKGROUNDER What is COPD? Chronic Obstructive Pulmonary Disease (COPD) also called emphysema and/or chronic obstructive bronchitis* is a preventable lung disease caused by the
UNDERSTANDING COPD MEDIA BACKGROUNDER What is COPD? Chronic Obstructive Pulmonary Disease (COPD) also called emphysema and/or chronic obstructive bronchitis* is a preventable lung disease caused by the
COPD. Salah Zeineldine, MD FACP Pulmonary & Critical Care Medicine American University of Beirut Lebanese Society of Family Medicine 2012
 COPD Salah Zeineldine, MD FACP Pulmonary & Critical Care Medicine American University of Beirut Lebanese Society of Family Medicine 2012 Attitude It is a disease on which a good deal of wholly, unmerited
COPD Salah Zeineldine, MD FACP Pulmonary & Critical Care Medicine American University of Beirut Lebanese Society of Family Medicine 2012 Attitude It is a disease on which a good deal of wholly, unmerited
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Known Allergies: Shellfish. Symptoms: abdominal pain, nausea, diarrhea, or vomiting. congestion, trouble breathing, or wheezing.
 CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
AECOPD: Management and Prevention
 Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
COPD: early detection, screening and case-finding: what is the evidence? Prof. Jan-Willem Lammers, Md PhD Department of Respiratory Diseases
 COPD: early detection, screening and case-finding: what is the evidence? Prof. Jan-Willem Lammers, Md PhD Department of Respiratory Diseases «If you test one smoker with cough every day You will diagnose
COPD: early detection, screening and case-finding: what is the evidence? Prof. Jan-Willem Lammers, Md PhD Department of Respiratory Diseases «If you test one smoker with cough every day You will diagnose
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX
 MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX") CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
A whistle stop tour of Respiratory Medicine and what the RUH & IMPACT offer
 A whistle stop tour of Respiratory Medicine and what the RUH & IMPACT offer Jay Suntharalingam, Respiratory Physician, RUH Claire Bullard, IMPACT Team Leader, Sirona Outline Respiratory 5 year strategy
A whistle stop tour of Respiratory Medicine and what the RUH & IMPACT offer Jay Suntharalingam, Respiratory Physician, RUH Claire Bullard, IMPACT Team Leader, Sirona Outline Respiratory 5 year strategy
Disclosures. Chronic Obstructive Pulmonary Disease. Chronic Obstructive Pulmonary Disease (COPD)
") Chronic Obstructive Pulmonary Disease May 14, 2016 Orlando, FL COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United States. Alarmingly, COPD recently became
Chronic Obstructive Pulmonary Disease May 14, 2016 Orlando, FL COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United States. Alarmingly, COPD recently became
Advancing COPD treatment strategies with evidencebased. 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy
 Advancing COPD treatment strategies with evidencebased approaches 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy Increasing understanding of COPD and the effect on guideline evolution. GOLD
Advancing COPD treatment strategies with evidencebased approaches 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy Increasing understanding of COPD and the effect on guideline evolution. GOLD
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC
 KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC") Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Comparisons of health status scores with MRC grades in COPD: implications for the GOLD 2011 classification
 ORIGINAL ARTICLE COPD Comparisons of health status scores with MRC grades in COPD: implications for the GOLD 2011 classification Paul W. Jones 1, Lukasz Adamek 2, Gilbert Nadeau 2 and Norbert Banik 3 Affiliations:
ORIGINAL ARTICLE COPD Comparisons of health status scores with MRC grades in COPD: implications for the GOLD 2011 classification Paul W. Jones 1, Lukasz Adamek 2, Gilbert Nadeau 2 and Norbert Banik 3 Affiliations:
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable
 THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
COPD: Applying New Guidelines to Optimizing Evaluation and Treatment
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
What is New in COPD: Times Are Changing! Meredith Chiasson, MD, FRCPC April 6, 2018
 What is New in COPD: Times Are Changing! Meredith Chiasson, MD, FRCPC April 6, 2018 No disclosures Disclosures objectives How to diagnose & Assess severity Treatment: Pharmacologic Non-Pharmacologic Maintenance
What is New in COPD: Times Are Changing! Meredith Chiasson, MD, FRCPC April 6, 2018 No disclosures Disclosures objectives How to diagnose & Assess severity Treatment: Pharmacologic Non-Pharmacologic Maintenance
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD UPDATE ıdr Shitrit David ıhead of the Pulmonary Department ımeir Medical Center
 COPD UPDATE 2012 ıdr Shitrit David ıhead of the Pulmonary Department ımeir Medical Center Definition of COPD COPD is a preventable and treatable disease with some significant extra pulmonary effects that
COPD UPDATE 2012 ıdr Shitrit David ıhead of the Pulmonary Department ımeir Medical Center Definition of COPD COPD is a preventable and treatable disease with some significant extra pulmonary effects that
Common Pulmonary Problems. Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine
 Common Pulmonary Problems Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Obstructive
Common Pulmonary Problems Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Obstructive
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Asthma ASTHMA. Current Strategies for Asthma and COPD
 Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017
 Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Self-management plan for COPD
 Sheffield Clinical Commissioning Group Sheffield Teaching Hospitals NHS Foundation Trust Self-management plan for COPD This is your personal management plan The aim of the plan is to help you have better
Sheffield Clinical Commissioning Group Sheffield Teaching Hospitals NHS Foundation Trust Self-management plan for COPD This is your personal management plan The aim of the plan is to help you have better
Pulmonary and Critical Care Year in Review
 Pulmonary and Critical Care Year in Review Heath E Latham, MD Assistant Professor University of Kansas Dept of Internal Medicine Division of Pulmonary and Critical Care None Disclosure Lung Cancer Screening
Pulmonary and Critical Care Year in Review Heath E Latham, MD Assistant Professor University of Kansas Dept of Internal Medicine Division of Pulmonary and Critical Care None Disclosure Lung Cancer Screening
Algorithm for the use of inhaled therapies in COPD
 Berkshire West Integrated Care System Representing Berkshire West Clinical Commisioning Group Royal Berkshire NHS Foundation Trust Berkshire Healthcare NHS Foundation Trust Berkshire West Primary Care
Berkshire West Integrated Care System Representing Berkshire West Clinical Commisioning Group Royal Berkshire NHS Foundation Trust Berkshire Healthcare NHS Foundation Trust Berkshire West Primary Care
Bronchial Provocation Results: What Does It Mean?
 Bronchial Provocation Results: What Does It Mean? Greg King 1 Department of Respiratory Medicine, Royal North Shore Hospital, St Leonards 2065 2 Woolcock Institute of Medical Research and Sydney Medical
Bronchial Provocation Results: What Does It Mean? Greg King 1 Department of Respiratory Medicine, Royal North Shore Hospital, St Leonards 2065 2 Woolcock Institute of Medical Research and Sydney Medical
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines
 Treatment Guidelines") Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Patient reported outcomes in respiratory diseases; How to assess clinical success in COPD
 Patient reported outcomes in respiratory diseases; How to assess clinical success in COPD Thys van der Molen, University of Groningen, Department of General Practice, The Netherlands Mr Valette Smoking
Patient reported outcomes in respiratory diseases; How to assess clinical success in COPD Thys van der Molen, University of Groningen, Department of General Practice, The Netherlands Mr Valette Smoking
Self-Management Plan for COPD
 Self-Management Plan for COPD This is your personal management plan. The aim of this plan is to help you have better control of your chronic obstructive pulmonary disease (COPD). It will enable you to
Self-Management Plan for COPD This is your personal management plan. The aim of this plan is to help you have better control of your chronic obstructive pulmonary disease (COPD). It will enable you to
TORCH: Salmeterol and Fluticasone Propionate and Survival in COPD
 TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic
 COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene
 Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
Reference Guide for Group Education
 A p l a n o f a c t i o n f o r l i f e Reference Guide for Group Education Session 5 Plan of Action: Part I Overview of the Plan of Action and Management of Respiratory Infections Plan of Action: Objectives
A p l a n o f a c t i o n f o r l i f e Reference Guide for Group Education Session 5 Plan of Action: Part I Overview of the Plan of Action and Management of Respiratory Infections Plan of Action: Objectives
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
 10:50-11:50am Case Studies in Pulmonary Medicine for the Primary Care Clinician SPEAKERS Timothy J. Scialla, MD Common Shortcuts/Common Misperceptions Smoking + Dyspnea = COPD Hospitalization for cough
10:50-11:50am Case Studies in Pulmonary Medicine for the Primary Care Clinician SPEAKERS Timothy J. Scialla, MD Common Shortcuts/Common Misperceptions Smoking + Dyspnea = COPD Hospitalization for cough
Disclosure Statement. Epidemiological Data
 EVALUATION OF THE MEDICATION UTILIZATION OF COPD PATIENTS AT THE MIAMI VA HEALTHCARE SYSTEM Simone Edgerton, PharmD. PGY 1 Pharmacy Resident Miami VA Healthcare System Miami, Florida Simone.edgerton2@va.gov
EVALUATION OF THE MEDICATION UTILIZATION OF COPD PATIENTS AT THE MIAMI VA HEALTHCARE SYSTEM Simone Edgerton, PharmD. PGY 1 Pharmacy Resident Miami VA Healthcare System Miami, Florida Simone.edgerton2@va.gov
Chronic Obstructive Pulmonary Disease (COPD).
.") Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
If you require this document in another format such as Braille, large print, audio or another language please contact the Trusts Communications Team
 MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
Blue, Pink and everything in between: an update on COPD. Tara Lohmann MD FRCPC Division of Respirology University of Calgary
 Blue, Pink and everything in between: an update on COPD Tara Lohmann MD FRCPC Division of Respirology University of Calgary Disclosures I have eaten lunches provided by many pharmaceutical companies (GSK,
Blue, Pink and everything in between: an update on COPD Tara Lohmann MD FRCPC Division of Respirology University of Calgary Disclosures I have eaten lunches provided by many pharmaceutical companies (GSK,
COPD exacerbation. Chiara Maruggi, PGY2
 COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
Chronic Obstructive Pulmonary Disease. Information about medication and an Action Plan to use if your condition gets worse due to an infection
 Chronic Obstructive Pulmonary Disease Information about medication and an Action Plan to use if your condition gets worse due to an infection Information about your medication Your usual treatment Inhalers
Chronic Obstructive Pulmonary Disease Information about medication and an Action Plan to use if your condition gets worse due to an infection Information about your medication Your usual treatment Inhalers
COPD: Treatment Update Property of Presenter. Not for Reproduction. Barry Make, MD Professor of Medicine National Jewish Health
 COPD: Treatment Update Barry Make, MD Professor of Medicine National Jewish Health Disclosures Advisory board, consultant, multi-center trial, research funding, Data Safety Monitoring Board (DSMB), or
COPD: Treatment Update Barry Make, MD Professor of Medicine National Jewish Health Disclosures Advisory board, consultant, multi-center trial, research funding, Data Safety Monitoring Board (DSMB), or
Three s Company - The role of triple therapy in chronic obstructive pulmonary
 Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) October 26 th, 2018 Zahava Picado, PharmD PGY1 Pharmacy Resident Central Texas Veterans Healthcare System Zahava.Picado@va.gov
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) October 26 th, 2018 Zahava Picado, PharmD PGY1 Pharmacy Resident Central Texas Veterans Healthcare System Zahava.Picado@va.gov