Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
|
|
|
- Britney Curtis
- 6 years ago
- Views:
Transcription
1 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital

2 Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
3 Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
4 Asthma prevalence Asthma affects 20% of children Asthma is the commonest chronic disease in South African children. South Africa is ranked 25th worldwide in the prevalence of asthma South Africa is ranked fifth for asthma case fatality rates
5 Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
6 What is asthma? Asthma is a disorder of the airways caused by reversible inflammation that leads to the air passages contracting in response to a wide range of stimuli with enhanced irritability of the airways and increased mucus secretion
7

8 Smooth muscle Spasm Swollen mucosa Secretions Set alight-ness Scarring
9 Allergic inflammation Inflammation is the most important aspect of asthma Inflammation causes the other features That s why asthma needs treatment with regular controller therapy given every day whether the patient is symptomatic or not to control the inflammation.
10 Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
11 How do we diagnose it?? recurrent wheeze and/or cough and/or dyspnoea responsive to bronchodilators
12 How do we diagnose it?? recurrent wheeze and/or cough and/or dyspnoea responsive to bronchodilators

13 Has the patient had recurrent wheezing? Do the patient s colds go to the chest or take >10 days to clear up? Does the patient have a cough at night? Are symptoms seasonal? Does the patient experience symptoms after exposure to allergens or pollutants? Does the patient wheeze or cough after exercise?
14 How do we diagnose it?? recurrent wheeze and/or cough and/or dyspnoea responsive to bronchodilators
15 Bronchodilator response Bedside test or < 5 Administer bronchodilator Reassess after 10 minutes Document respiratory rate respiratory distress auscultation Bronchodilator and diary card over 2 weeks Trial of oral corticosteroids for 7 14 days

 Diurnal")
16 Bronchodilator response Lung function tests 10 mins after bronchodilators > 5 yrs FEV1 increase by > 12 % (15 %) PEF increase by > 15 % (20%) Diurnal variability > 20 %
17 Exclude other conditions Respiratory infections worms foreign body lymph nodes cystic fibrosis Vocal cord dysfunction Cardiac pulmonary oedema myocarditis congenital abnormalities GIT G-O reflux disease Mimics other diseases. Asthma and atopy may coexist with other diseases.
18 Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
19 Select initial treatment according to severity Severity Days with Nights with PEFR / FEV1 (GINA Guide) symptoms symptoms 1) Mild intermittent 2) Mild persistent 3) Moderate persistent 4) Severe persistent < 2 / week < 2 / month > 80 % predicted < 20 % variability 3 6 / week 3 4 / month > 80 % predicted % variability daily > 5 / month % predicted > 30 % variability continual frequent < 60 % predicted > 30 % variability Assign patients to the most severe category in which any feature occurs.
20 Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
21 Step 1 Step 2 Step 3 Step 4 Step 5 No controller medication required Asthma education and environmental control As needed reliever medication e.g. rapid-acting β2-agonist
22 Education Goals of therapy Minimal or no chronic symptoms day or night Minimal or no exacerbations No limitation on activity; school or parent s work missed Minimal use of inhaled B2 agonists Minimal or no adverse effects from medication
23 Asthma medication Controllers (preventers) Inhaled steroid pumps Long acting B2 agonists Leukotriene receptor antagonists Theophylline Relievers SABA Ipratropium bromide
24 Step 1 Step 2 Step 3 Step 4 Step 5 Asthma education and environmental control As needed reliever medication e.g. rapid-acting β2-agonist No controller medication required Select one Low-dose inhaled steroid (ICS) Leukotriene modifier
25 Step 1 Step 2 Step 3 Step 4 Step 5 Asthma education and environmental control As needed reliever medication e.g. rapid-acting β2-agonist No controller medication required Select one Select one Low-dose inhaled steroid (ICS) Leukotriene modifier Medium-dose ICS Medium or Lowdose ICS plus long-acting β 2- agonist Low-dose ICS plus leukotriene modifier
26 Step 1 Step 2 Step 3 Step 4 Step 5 Asthma education and environmental control As needed reliever medication e.g. rapid-acting β2-agonist No controller medication required Select one Select one Select one Low-dose inhaled steroid (ICS) Leukotriene modifier Medium-dose ICS Medium or Lowdose ICS plus long-acting β 2- agonist Medium or highdose ICS plus long-acting β 2 - agonist Medium or highdose ICS plus Leukotriene modifier Low-dose ICS plus leukotriene modifier Medium or highdose ICS plus theophylline
27 Step 1 Step 2 Step 3 Step 4 Step 5 Asthma education and environmental control As needed reliever medication e.g. rapid-acting β2-agonist No controller medication required Select one Select one Select one add either Low-dose inhaled steroid (ICS) Medium-dose ICS Medium or highdose ICS plus long-acting β 2 - agonist Oral steroid (lowest dose) Leukotriene modifier Medium or Lowdose ICS plus long-acting β 2- agonist Medium or highdose ICS plus Leukotriene modifier Anti-IgE treatment Low-dose ICS plus leukotriene modifier Medium or highdose ICS plus theophylline
28 Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
29 Asthma Control Characteristic Assessing Daytime symptoms Limitation of activities Nocturnal symptoms/awakening Need for reliever/rescue medication Lung function (PEF or FEV 1 ) Monitoring Treating Follow up regularly. Assess and move up and down treatment algorithm according to control.
30 Asthma Control Characteristic Controlled (all of the following) Partly controlled (any measure present) Uncontrolled Daytime symptoms None (twice or less/week) Limitation of activities None Any Nocturnal symptoms/awakening None More than twice/week Any Three or more characteristics of partly controlled asthma Need for reliever/rescue medication Lung function (PEF or FEV 1 ) None (twice or less/week) Normal More than twice/week <80% predicted or personal best (if known)


31 Reasons for poor asthma control Incorrect diagnosis Individual variation in response to treatment Incorrect choice of inhaler and poor inhaler technique Smoking Patient belief and adherence Co-morbid rhinosinusitis


32 Before altering medication consider Is the diagnosis correct? Is there objective evidence of asthma? Other factors: Gastrooesophageal reflux, ABPA Is the patient adherent to their existing therapy? Does the patient have allergic rhinosinusitis? Treatment of this may improve asthma control Is the patient able to use their inhaler properly? Are there any correctable trigger factors, e.g. occupational sensitisers, does the patient smoke?
33 Step 1 Step 2 Step 3 Step 4 Step 5 No controller medication required Select one Select one Select one add either Low-dose inhaled steroid (ICS) Medium-dose ICS Medium or highdose ICS plus long-acting β 2 - agonist Oral steroid (lowest dose) Leukotriene modifier Medium or Lowdose ICS plus long-acting β 2- agonist Medium or highdose ICS plus Leukotriene modifier Anti-IgE treatment Low-dose ICS plus leukotriene modifier Medium or highdose ICS plus theophylline
34 Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
 Long-acting inhaled β 2 -agonists (LABA) (e.g. salmeterol, formoterol)")
35 Controller medications Inhaled glucocorticoids (e.g. budesonide, fluticasone propionate) Leukotriene modifiers (e.g. montelukast, zileuton) Long-acting inhaled β 2 -agonists (LABA) (e.g. salmeterol, formoterol)
36 Controller medications Inhaled glucocorticoids (e.g. budesonide, fluticasone propionate) The most effective controller medication, delivering drugs directly to the airways Leukotriene modifiers (e.g. montelukast, zileuton) Long-acting inhaled β 2 -agonists (LABA) (e.g. salmeterol, formoterol)


37

38 Inhaled corticosteroids Most asthmatics well controlled with low dose inhaled steroids. Side effects uncommon.
39 Steroid doses Low dose Medium High dose Budesonide (Budeflam, Pulmicort, Inflammide) Beclomethasone (Becotide, Beclate) Fluticasone (Flixotide) Document dose of MDIs accurately
40 Controller medications Inhaled glucocorticoids (e.g. budesonide, fluticasone propionate) The most effective controller medication, delivering drugs directly to the airways Leukotriene modifiers (e.g. montelukast, zileuton) Used as add on particularly in children < 5 Particularly appropriate for patients unwilling or unable to take ICS, or those that experience side effects with ICS Long-acting inhaled β 2 -agonists (LABA) (e.g. salmeterol, formoterol)


41
42 Uses for LTRA s Monotherapy for mild asthma Monotherapy if patient noncompliant or steroid phobic Mild asthma with exercise induced component Aspirin sensitive asthma. Add on therapy for moderate persistent asthma Potential for steroid sparing effects Add on therapy for severe uncontrolled asthma.
43 Controller medications Inhaled glucocorticoids (e.g. budesonide, fluticasone propionate) The most effective controller medication, delivering drugs directly to the airways Leukotriene modifiers (e.g. montelukast, zileuton) Used as add on particularly in children < 5 Particularly appropriate for patients unwilling or unable to take ICS, or those that experience side effects with ICS Long-acting inhaled β 2 -agonists (LABA) (e.g. salmeterol, formoterol) Synergistic effects Not monotherapy Not below 5
44 Long acting B 2 agonists Anti-inflammatory action is synergistic with steroids. Reduce bronchial hyperresponsiveness and inhibit release of inflammatory mediators and prevent plasma exudation. 12 hour bronchodilation. Receptor desensitisation and downregulation. This effect prevented by concomitant steroid administration.
45 Uses for LABAs Improves outcomes when added to medium or high dose inhaled steroids. Not first line agents Use only as combination, never mono-therapy Use as steroid sparing agents or as step up before increasing steroids Contraindicated below age of 5
46 SMART therapy LABAs are formoterol and salmeterol Both have long duration of action Salmeterol has delayed onset of action Formoterol is rapid acting Symbicord maintenance and reliever therapy To blunt attacks


47



48
49 Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
50 Drugs in acute asthma Adrenaline B2 receptors relaxation SABA s + relaxation Acetylcholine Cholinergic receptors spasm Anticholinergics - relaxation
51 Drugs in acute asthma Adrenaline B2 receptors relaxation SABA s + relaxation Acetylcholine Cholinergic receptors spasm Anticholinergics - relaxation
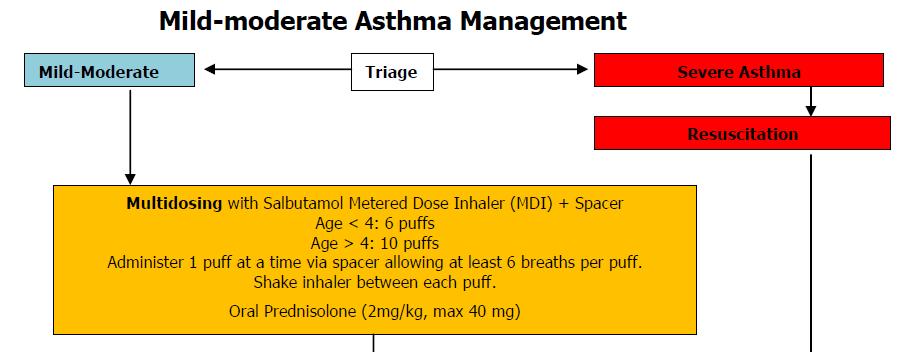
52 Acute exacerbations Oxygen therapy Monitor all patients Achieve O 2 saturation of 95%, >93% in children Inhaled rapid-acting β 2 -agonists MDI with spacer (unless hypoxic) Repeat (at least) 3 doses in first hour Oral glucocorticoids Early administration Oral
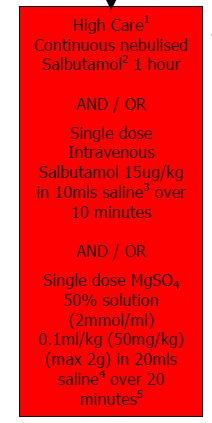
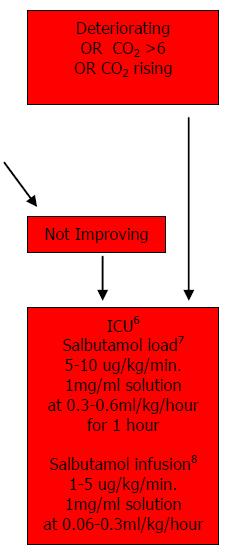
53 Acute asthma

54 Acute asthma
55
56 Administration of B2 agonists MDI/spacer 6-10 puffs Each puff separately Repeat every 20 minutes Drug (approved name) Dose Route Other directions Salbutamol 6 or 10 puffs INHAL via Spacer 100 microgram MDI How frequently should I prescribe multidoses? Multidose of bronchodilator gives an equivalent effect as a nebuliser and therefore does not require to be given more frequently than you would give nebulised medication

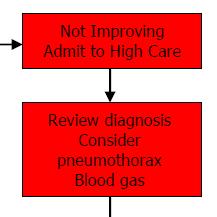
57 Severe exacerbations The attack is severe Cyanosis, sats < 94, prev ICU, drowsy, confused, silent chest, tachycardia, pulsus paradoxus, impaired speech / feeding breathless at rest, and/or PEF is <60% of predicted or personal best The response to the initial bronchodilator treatment is not prompt and sustained for at least three hours There is no improvement within 2 to 6 hours after oral glucocorticoid treatment is initiated There is further deterioration
58
59

60 Give adequate inhaled therapy before considering anything else
61
62 Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
63 Using a MDI is not easy Effective deposition of aerosols requires Slow inspiratory flow Deep inhalation and breath hold Quiet, non-distressed breathing
64 Using a MDI is not easy Timing is critical Actuation 1 second before inhalation reduces inhaled mass by 90% Late actuation results in the lung being filled with medication-free air and aerosol merely reaching the dead space and being exhaled Delivery of medication via a MDI without a spacer is highly ineffective

65 Spacers Problems with spacers Spacer is less portable than MDI alone Multiple actuations into spacer Need comfortable but well sealed mask Inspiratory flow to open holding valve with tidal breathing

66 Issues with nebulisers Flow rate of 6-8 l/min Driven by O2 or air Dead volume of 0.5-1ml When a nebuliser starts sputtering delivery is minimal Filling volume of 4-5 ml
67 Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
68 Inhaler technique Prepare the device Check the orientation Actuate the device Shake the device if it is an MDI
69 Inhaler technique Prepare the device Check the orientation Actuate the device Shake the device if it is an MDI Prepare the body Breathe out fully away from the mouthpiece Consider differences between MDI and DPI devices
70 Inhaler technique Prepare the device Check the orientation Actuate the device Shake the device if it is an MDI Prepare the body Breathe out fully away from the mouthpiece Consider differences between MDI and DPI devices mouthpiece in mouth Ensure a good seal and make sure the teeth are not in front of the device

71 Inhaler technique Prepare the device Prepare the body mouthpiece in mouth DPI MDI Check the orientation Actuate the device Shake the device if it is an MDI Breathe out fully away from the mouthpiece Consider differences between MDI and DPI devices Ensure a good seal and make sure the teeth are not in front of the device Breathe as fast and as hard as possible from the beginning OR Start breathing slowly and actuate. Breathe in over 5 seconds and hold breath for 5 seconds
72
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Stepping-down combination ICS/LABA asthma inhaler therapy: Adults 18yrs
 Step Down guidance Stepping-down combination ICS/LABA asthma inhaler therapy: Adults 18yrs Important Complete asthma control needs to be achieved for at least 12 weeks before attempting to step patients
Step Down guidance Stepping-down combination ICS/LABA asthma inhaler therapy: Adults 18yrs Important Complete asthma control needs to be achieved for at least 12 weeks before attempting to step patients
Adult Summary flowchart for Asthma Switch and Step Down to preferred inhaler choices
 HVCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to preferred
HVCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to preferred
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred inhaler choices
 ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred
ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred
MANAGING ASTHMA. Nancy Davis, RRT, AE-C
 MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
Respiratory Pharmacology
 Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
Bronchial asthma. E. Cserháti 1 st Department of Paediatrics. Lecture for english speaking students 5 February 2013
 Bronchial asthma E. Cserháti 1 st Department of Paediatrics Lecture for english speaking students 5 February 2013 Epidemiology of childhood bronchial asthma Worldwide prevalence of 7-8 and 13-14 years
Bronchial asthma E. Cserháti 1 st Department of Paediatrics Lecture for english speaking students 5 February 2013 Epidemiology of childhood bronchial asthma Worldwide prevalence of 7-8 and 13-14 years
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Position within the Organisation
 ASTHMA TREATMENT GUIDELINES Document Description Document Type Service Application Guidelines All healthcare professionals(hcps) caring for patients with asthma Version 4.0 Ratification date September
ASTHMA TREATMENT GUIDELINES Document Description Document Type Service Application Guidelines All healthcare professionals(hcps) caring for patients with asthma Version 4.0 Ratification date September
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma: Chronic Management. Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015
 Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL
 DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
Alberta Childhood Asthma Pathway for Primary Care
 Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Predicting, Preventing and Managing Asthma Exacerbations. Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa
 Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Respiratory Health. Asthma and COPD
 Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
Management of Acute Asthma Exacerbations in Children 2012 Update. Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch
 Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines
Management of Acute Asthma Exacerbations in Children 2012 Update Sharon Kling Dept Paediatrics & Child Health University of Stellenbosch Acknowledgements BTS/SIGN guidelines GINA guidelines NAEPP guidelines
Nancy Davis, RRT, AE-C
 Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Getting Asthma treatment right. Dr David Cremonesini Specialist Pediatrician American Hospital
 Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital cdavid@ahdubai.com } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate)
Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital cdavid@ahdubai.com } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate)
Prescribing guidelines: Management of COPD in Primary Care
 Prescribing guidelines: Management of COPD in Primary Care Establish diagnosis of COPD in patients 35 years with appropriate symptoms with history, examination and spirometry (FEV1/FVC ratio < 70%) Establish
Prescribing guidelines: Management of COPD in Primary Care Establish diagnosis of COPD in patients 35 years with appropriate symptoms with history, examination and spirometry (FEV1/FVC ratio < 70%) Establish
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma
 with asthma") Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Public Dissemination
 1. THE ASTHMA CONDITION 9 18 3 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
1. THE ASTHMA CONDITION 9 18 3 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
Medicine Dr. Kawa Lecture 4 - Treatment of asthma :
 Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
Medicine Dr. Kawa Lecture 4 - Treatment of asthma : Avoiding allergens. Hyposensitization :Subcutaneous injections of inially very small, but gradually increasing doses of allergens (desensitization or
ASTHMA PRESCRIBING GUIDELINES FOR ADULTS AND CHILDREN OVER 12
 North Hampshire CCG Asthma Prescribing Guidelines June 2015 ASTHMA PRESCRIBING GUIDELINES FOR ADULTS AND CHILDREN OVER 12 These guidelines are based on the British Thoracic Society (BTS) and Scottish Intercollegiate
North Hampshire CCG Asthma Prescribing Guidelines June 2015 ASTHMA PRESCRIBING GUIDELINES FOR ADULTS AND CHILDREN OVER 12 These guidelines are based on the British Thoracic Society (BTS) and Scottish Intercollegiate
I have no perceived conflicts of interest or commercial relationships to disclose.
 ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
ASTHMA TREATMENT GUIDE (ADULTS)
") ASTHMA TREATMENT GUIDE (ADULTS) The BTS/SIGN guideline provides a wide range of information and guidance on the treatment of patients with asthma. https://www.brit-thoracic.org.uk/document-library/clinical-information/asthma/btssign-asthma-guideline-2016/
ASTHMA TREATMENT GUIDE (ADULTS) The BTS/SIGN guideline provides a wide range of information and guidance on the treatment of patients with asthma. https://www.brit-thoracic.org.uk/document-library/clinical-information/asthma/btssign-asthma-guideline-2016/
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
DIFFICULT ASTHMA. Dr. Prathyusha Dr. S.Balasubramanian KKCTH
 DIFFICULT ASTHMA Dr. Prathyusha Dr. S.Balasubramanian KKCTH CASE SUMMARY 11 yr old girl, Neyveli Treated as moderate persistent asthma x 5 years On Seroflo [ LABA + steroid ] 250 2 puffs BD and intermittent
DIFFICULT ASTHMA Dr. Prathyusha Dr. S.Balasubramanian KKCTH CASE SUMMARY 11 yr old girl, Neyveli Treated as moderate persistent asthma x 5 years On Seroflo [ LABA + steroid ] 250 2 puffs BD and intermittent
Using an Inhaler and Nebulizer
 Using an Inhaler and Nebulizer Introduction An inhaler is a handheld device that is used to deliver medication directly to your airways. A nebulizer is an electric or battery powered machine that turns
Using an Inhaler and Nebulizer Introduction An inhaler is a handheld device that is used to deliver medication directly to your airways. A nebulizer is an electric or battery powered machine that turns
Asthma - An update BTS Asthma Guidelines 2016
 Asthma - An update BTS Asthma Guidelines 2016 Dr Ian Clifton Overview Diagnosis Supported self-management Non-pharmacological management Drugs / inhaled therapy Difficult asthma services Case discussions
Asthma - An update BTS Asthma Guidelines 2016 Dr Ian Clifton Overview Diagnosis Supported self-management Non-pharmacological management Drugs / inhaled therapy Difficult asthma services Case discussions
National Asthma Educator Certification Board Detailed Content Outline
 I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
beclometasone 100 MDI 2 puffs twice a day (recently changed to non CFC (Clenil Modulite))
)") Case 1 Mr Thomson, a 32 year old asthmatic who is well known to you comes into your pharmacy. He is known to have a best peak flow of 640 L/min. He tells you that over the last few weeks he has been wakening
Case 1 Mr Thomson, a 32 year old asthmatic who is well known to you comes into your pharmacy. He is known to have a best peak flow of 640 L/min. He tells you that over the last few weeks he has been wakening
Interventions to improve adherence to inhaled steroids for asthma. Respiratory department
 Interventions to improve adherence to inhaled steroids for asthma Respiratory department Content Overview Research References Overview Asthma is a chronic breathing condition that affects more than 300
Interventions to improve adherence to inhaled steroids for asthma Respiratory department Content Overview Research References Overview Asthma is a chronic breathing condition that affects more than 300
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Practical Approach to Managing Paediatric Asthma
 Practical Approach to Managing Paediatric Asthma Dr Andrew Tai FRACP, PhD Paediatric Respiratory and Sleep Specialist Women's and Children's Hospital, Adelaide Approaching the patient Check the diagnosis
Practical Approach to Managing Paediatric Asthma Dr Andrew Tai FRACP, PhD Paediatric Respiratory and Sleep Specialist Women's and Children's Hospital, Adelaide Approaching the patient Check the diagnosis
(Asthma) Diagnosis, monitoring and chronic asthma management
 Diagnosis, monitoring and chronic asthma management") Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Asthma Description. Asthma is a disease that affects the lungs defined as a chronic inflammatory disorder of the airways.
 Asthma Asthma Description Asthma is a disease that affects the lungs defined as a chronic inflammatory disorder of the airways. Symptoms of asthma In susceptible individuals, this inflammation causes recurrent
Asthma Asthma Description Asthma is a disease that affects the lungs defined as a chronic inflammatory disorder of the airways. Symptoms of asthma In susceptible individuals, this inflammation causes recurrent
Medications Affecting The Respiratory System
 Medications Affecting The Respiratory System Overview Asthma is a chronic inflammatory disorder of the airways. It is an intermittent and reversible airflow obstruction that affects the bronchioles. The
Medications Affecting The Respiratory System Overview Asthma is a chronic inflammatory disorder of the airways. It is an intermittent and reversible airflow obstruction that affects the bronchioles. The
Treatment. Assessing the outcome of interventions Traditionally, the effects of interventions have been assessed by measuring changes in the FEV 1
 58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
Management of acute asthma in children in emergency department. Moderate asthma
 152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
EXACERBATIONS IN ADULTS WHEN TO REFER
 06 Bronchial Asthma Contributors: Dr Chong Phui Nah Dr Tang Wern Ee PRESENTATION AND DIAGNOSIS CLASSIFICATION OF ASTHMA BY LEVEL OF CONTROL ASSESSMENT OF ASTHMA CONTROL USING THE ASTHMA CONTROL TEST ASTHMA
06 Bronchial Asthma Contributors: Dr Chong Phui Nah Dr Tang Wern Ee PRESENTATION AND DIAGNOSIS CLASSIFICATION OF ASTHMA BY LEVEL OF CONTROL ASSESSMENT OF ASTHMA CONTROL USING THE ASTHMA CONTROL TEST ASTHMA
II: Moderate Worsening airflow limitations Dyspnea on exertion, cough, and sputum production; patient usually seeks medical
 Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Asthma By Mayo Clinic staff
 MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
CHARM ASTHMA TREATMENT GUIDELINE
 NHS City and Hackney Prescribing Guidelines Adults ( 12 years of age) CHARM ASTHMA TREATMENT GUIDELINE Written by: Hetal Dhruve (Specialist Respiratory Pharmacist, City and Hackney CCG) Checked by: Prof
NHS City and Hackney Prescribing Guidelines Adults ( 12 years of age) CHARM ASTHMA TREATMENT GUIDELINE Written by: Hetal Dhruve (Specialist Respiratory Pharmacist, City and Hackney CCG) Checked by: Prof
Asthma Management. Photo from
 Asthma Management 1 Photo from www.nhlbi.nih.gov Course Overview 1. Recognition of the symptoms and signs Basic Knowledge of asthma Recognition of common symptoms Recognition of the signs of asthma including
Asthma Management 1 Photo from www.nhlbi.nih.gov Course Overview 1. Recognition of the symptoms and signs Basic Knowledge of asthma Recognition of common symptoms Recognition of the signs of asthma including
Asthma. chapter 7. Overview
 chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
chapter 7 Asthma Sinus Sinus Sinus Right lung Adenoids Tonsils Pharynx Epiglottis Oesophagus Right bronchus Nasal cavity Oral cavity Tongue Larynx Trachea Ribs Left bronchus Diaphragm Bronchiole Pleura
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Dose. Route. Units. Given. Dose. Route. Units. Given
 Chapter 4 Respiratory Andrew Stanton SALBUTAMOL (in acute asthma) 5 in acute asthma Nebulised (driven by oxygen not air) 4 6 hourly In acute severe asthma not responding to initial treatment or in life-threatening
Chapter 4 Respiratory Andrew Stanton SALBUTAMOL (in acute asthma) 5 in acute asthma Nebulised (driven by oxygen not air) 4 6 hourly In acute severe asthma not responding to initial treatment or in life-threatening
Asthma in Day to Day Practice
 Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Asthma. Definition. Symptoms
 Asthma Definition Asthma is a condition in which your airways narrow and swell and produce extra mucus. This can make breathing difficult and trigger coughing, wheezing and shortness of breath. For some
Asthma Definition Asthma is a condition in which your airways narrow and swell and produce extra mucus. This can make breathing difficult and trigger coughing, wheezing and shortness of breath. For some
Global Initiative for Asthma (GINA) What s new in GINA 2016?
 What s new in GINA 2016?") Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Asthma/wheeze management plan
 Asthma/wheeze management plan Name of Patient Date of Birth NHS Number GP surgery Telephone Next appointment Children s Assessment unit/ward telephone Out of hours call 111 Open access Y/N Until date Some
Asthma/wheeze management plan Name of Patient Date of Birth NHS Number GP surgery Telephone Next appointment Children s Assessment unit/ward telephone Out of hours call 111 Open access Y/N Until date Some
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
ASTHMA PROTOCOL CELLO
 ASTHMA PROTOCOL CELLO Leiden May 2011 1 Introduction This protocol includes an explanation of the clinical picture, diagnosis, objectives, non medical and medical therapy and a scheme for inhaler dosage.
ASTHMA PROTOCOL CELLO Leiden May 2011 1 Introduction This protocol includes an explanation of the clinical picture, diagnosis, objectives, non medical and medical therapy and a scheme for inhaler dosage.
Long Term Care Formulary RS -29
 RESTRICTED USE Asthma/COPD Management 1 of 6 PROTOCOL: Asthma Glossary of Medication Acronyms: SABA: short-acting beta agonist (e.g. salbutamol) SABD: short-acting bronchodilator (e.g. ipratropium or SABA)
RESTRICTED USE Asthma/COPD Management 1 of 6 PROTOCOL: Asthma Glossary of Medication Acronyms: SABA: short-acting beta agonist (e.g. salbutamol) SABD: short-acting bronchodilator (e.g. ipratropium or SABA)
ASTHMA IN THE PEDIATRIC POPULATION
 ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
Asthma and the competitive swimmer
 Asthma and the competitive swimmer Introduction: One in seven children and one in 25 adults in Great Britain have asthma and the number is growing. Thus every swim squad or club will have a number of asthmatics
Asthma and the competitive swimmer Introduction: One in seven children and one in 25 adults in Great Britain have asthma and the number is growing. Thus every swim squad or club will have a number of asthmatics
Dual-Controller Asthma Therapy: Rationale and Clinical Benefits
 B/1 Dual-Controller Asthma Therapy: Rationale and Clinical Benefits MODULE B The 1997 National Heart, Lung, and Blood Institute (NHLBI) Expert Panel guidelines on asthma management recommend a 4-step approach
B/1 Dual-Controller Asthma Therapy: Rationale and Clinical Benefits MODULE B The 1997 National Heart, Lung, and Blood Institute (NHLBI) Expert Panel guidelines on asthma management recommend a 4-step approach
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Guidelines and Pharmacological Treatment. Dr James Wilkinson
 Asthma Guidelines and Pharmacological Treatment Dr James Wilkinson Asthma is a common disease in the UK 5.4 million people in the UK are currently receiving treatment for asthma: 4.3 million adults (1
Asthma Guidelines and Pharmacological Treatment Dr James Wilkinson Asthma is a common disease in the UK 5.4 million people in the UK are currently receiving treatment for asthma: 4.3 million adults (1
Bronchial asthma. MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL
 Bronchial asthma MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL DEFINITION ASTHMA BRONCHIALE = Asthma is a chronic inflammatory disorder of the airways in which
Bronchial asthma MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL DEFINITION ASTHMA BRONCHIALE = Asthma is a chronic inflammatory disorder of the airways in which
Asthma. If an Ambulance is required - call immediately - do not delay. H & A Training PL RTO No:90871
 Asthma is a reversible breathing problem caused from sudden or progressive narrowing and spasming of the smaller airways and includes mucus production, which interferes with oxygen exchange. People who
Asthma is a reversible breathing problem caused from sudden or progressive narrowing and spasming of the smaller airways and includes mucus production, which interferes with oxygen exchange. People who
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma Action Plan and Education
 Acute Services Division Asthma Action Plan and Education Name: Date: Index What is Asthma? Page 4 Asthma Triggers Page 5 Peak Expiratory Flow Rate (Peak Flow) Page 6 Asthma Treatments Page 7 Asthma Action
Acute Services Division Asthma Action Plan and Education Name: Date: Index What is Asthma? Page 4 Asthma Triggers Page 5 Peak Expiratory Flow Rate (Peak Flow) Page 6 Asthma Treatments Page 7 Asthma Action
COPD RESOURCE PACK Section 5. Drug Treatment & Inhalers in Stable COPD
 COPD RESOURCE PACK Section 5 Drug Treatment & Inhalers in Stable COPD In this section: 1. Links to Fife Formulary 2. Pharmacological Management of Stable COPD 3. How to use a Metered Dose Inhaler 4. How
COPD RESOURCE PACK Section 5 Drug Treatment & Inhalers in Stable COPD In this section: 1. Links to Fife Formulary 2. Pharmacological Management of Stable COPD 3. How to use a Metered Dose Inhaler 4. How
It is recommended that a mask and protective eyewear be worn when providing care to a patient with a cough
 UNIVERSITY HEALTH NETWORK POLICY #: PAGE 1 OF 7 POLICY AND PROCEDURE MANUAL: RESPIRATORY THERAPY DEPT PATIENT CARE SECTION ORIGINAL DATE: 04/03 ISSUED BY: SITE LEADER APPROVED BY: Infection Prevention
UNIVERSITY HEALTH NETWORK POLICY #: PAGE 1 OF 7 POLICY AND PROCEDURE MANUAL: RESPIRATORY THERAPY DEPT PATIENT CARE SECTION ORIGINAL DATE: 04/03 ISSUED BY: SITE LEADER APPROVED BY: Infection Prevention
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Asthma and Vocal Cord Dysfunction
 Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Meeting the Challenges of Asthma
 Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Minimum Competencies for Asthma Care in Schools: School Nurse
 Minimum Competencies for Asthma Care in Schools: School Nurse Area I. Pathophysiology 1. Explain using simple language and appropriate educational aids the following concepts: a. Normal lung anatomy and
Minimum Competencies for Asthma Care in Schools: School Nurse Area I. Pathophysiology 1. Explain using simple language and appropriate educational aids the following concepts: a. Normal lung anatomy and
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
The Acute & Maintenance Treatment of Asthma via Aerosolized Medications
 The Acute & Maintenance Treatment of Asthma via Aerosolized Medications Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Associate Professor and Chairman Department of Respiratory Therapy Objectives Define Asthma.
The Acute & Maintenance Treatment of Asthma via Aerosolized Medications Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Associate Professor and Chairman Department of Respiratory Therapy Objectives Define Asthma.
In the name of God. Asthma
 In the name of God Asthma Objectives- at the end of this 2 sessions you should be able to: Discriminate between obstructive and restrictive airway disease. Define pathophysiology and symptoms of asthma.
In the name of God Asthma Objectives- at the end of this 2 sessions you should be able to: Discriminate between obstructive and restrictive airway disease. Define pathophysiology and symptoms of asthma.
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University
 Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University Asthma-related Comorbidities Comorbid conditions of the upper airways Rhinitis and Sinusitis
Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University Asthma-related Comorbidities Comorbid conditions of the upper airways Rhinitis and Sinusitis
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2018 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2018 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
in children Diagnosing and managing Asthma is chronically common amongst New Zealand children Diagnosing asthma in children
 Diagnosing and managing in children New Zealand has one of the highest rates of childhood asthma in the developed world. 1 It is the leading cause of sleep disturbance, missed school days and hospital
Diagnosing and managing in children New Zealand has one of the highest rates of childhood asthma in the developed world. 1 It is the leading cause of sleep disturbance, missed school days and hospital
Medicines Management of Asthma
 Wandsworth Borough Team Medicines Management of Guidelines for Primary Care September 2011 Version 1 Guideline Authors: Shaneez Dhanji (Wandsworth borough) Reena Rabheru-Dodhy (Sutton & Merton borough)
Wandsworth Borough Team Medicines Management of Guidelines for Primary Care September 2011 Version 1 Guideline Authors: Shaneez Dhanji (Wandsworth borough) Reena Rabheru-Dodhy (Sutton & Merton borough)
ASTHMA. Dr Liz Gamble BRI
 ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
Emily DiMango, MD Asthma II
 Emily DiMango, MD Asthma II Director John Edsall/John Wood Asthma Center Columbia University Medical Center HP 2000 Goal: 2.25/1,000 Comparison of Asthma Hospitalization Rates in Children Aged 0-14 in
Emily DiMango, MD Asthma II Director John Edsall/John Wood Asthma Center Columbia University Medical Center HP 2000 Goal: 2.25/1,000 Comparison of Asthma Hospitalization Rates in Children Aged 0-14 in
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCIDENCE UP TO 380,000 PEOPLE IN IRELAND HSE FIGURES 110,000 DIAGNOSED AND 200,000 UNDIAGNOSED. AFFECTS MORE MEN THAN WOMEN BUT RATES ARE RISING 1500 DEATHS PER YEAR
CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCIDENCE UP TO 380,000 PEOPLE IN IRELAND HSE FIGURES 110,000 DIAGNOSED AND 200,000 UNDIAGNOSED. AFFECTS MORE MEN THAN WOMEN BUT RATES ARE RISING 1500 DEATHS PER YEAR
Asthma/COPD. Asthma synopsis. chronic inflammation of bronchial airways bronchi lining bronchi muscles mucus
 1 Asthma & COPD Asthma synopsis chronic inflammation of bronchial airways bronchi lining bronchi muscles mucus 2 Asthma synopsis chest tightness tachypnea wheezing acute broncho-constriction cough shortness
1 Asthma & COPD Asthma synopsis chronic inflammation of bronchial airways bronchi lining bronchi muscles mucus 2 Asthma synopsis chest tightness tachypnea wheezing acute broncho-constriction cough shortness