VENTILATING CHILDREN- a quick recap. Dr Despina Demopoulos Paediatric Intensivist
|
|
|
- Anna Norman
- 6 years ago
- Views:
Transcription

1 VENTILATING CHILDREN- a quick recap Dr Despina Demopoulos Paediatric Intensivist
2 Introduction Six Tricks Case Scenarios Goals of ventilation Modes of ventilation Different diseases Conclusion OVERVIEW
3 INTRODUCTION Children are not small adults Also not big neonates
4 INTRODUCTION Respiratory disorders main cause of respiratory failure Average PICU has about 30% (range 20% 64%) of its patients mechanically ventilated for a mean of 5 6 days

 Birth history: Prem @ 28 weeks gestation, BW 1050 grams.")
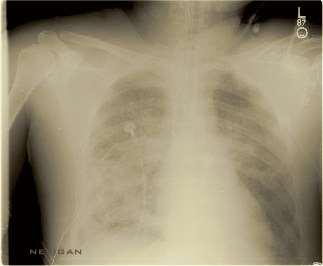
5 CASE 1 Baby Porky 10-month-old female infant 7-day history of cough, mild pyrexia, wheeze PMH: multiple episodes of cough and wheeze, some of which required admission to hospital (treated with inhaled bronchodilators and steroids) Birth history: 28 weeks gestation, BW 1050 grams. Required ncpap and suppl oxygen
6 CASE 1 Temperature 37.8 ºC Respiratory rate 48 breaths.min 1 Saturations 88% 92% R/A, 96% in 2 litres of oxygen Chest: Moderate subcostal/intercostal recession widespread expiratory wheeze and fine crackles Nasopharyngeal aspirate: Negative for respiratory viruses

7 CASE 1 Hyperexpanded with areas of atelectasis in both lung fields
8 CASE 1 Treatment: oxygen, a trial of salbutamol & ipratropium bromide inhalers as metered dose inhalers using a spacer device Next 24 hours episodes of increased respiratory distress & rising oxygen requirements Oral clarithromycin Feeds were given by nasogastric tube Blood gas: ph = 7.39, pco2 = 47 mhg, BE =3.1 Nasal Continuous Positive Airway Pressure (ncpap)

9 TRICK #1 Know which kids are sick and need ventilation Goals of ventilation
10 SICK KIDS Hypoxia Hypercarbia Airway protection (Decrease demand in cases of poor cardiac output)

11 SICK KIDS SIGNS OF DETERIORATION Increasing recession Increasing respiratory rate Increasing pulse rate Fatigue Altered mental status Cyanosis
12 CASE 1 Few hours later: deteriorated with a respiratory rate above 60 breaths min 1 Head-bobbing and severe recession Pale, sweaty, lethargic Blood gas: ph = 7.17 pco2 = 72 mmhg, BE = 3.4 No longer able to cope intubated


13 TRICK #2 Know your ventilator Terminology Different modes Ventilator settings

14 OXYGEN Alveolar gas equation PAO2 = FiO2 (PATM - PH2o) - PaCO2 Nasal Prongs 24%-30 % Face mask 28%-80 % NOT Double oxygen

15 CPAP and NIV 2 main effects Increase pressure in posterior pharynx => increase ΔP across conducting airways => improves airflow Increases PEEP, thus FRC > Closing capacity Nasal CPAP increasingly NB in neonates reduces need for ventilation in pre-term infants Also useful in small infants After infancy, before childhood difficult to achieve > 6-8years face mask


16 NIV Key Features of Airvo Humidifier: Humidifier with integrated flow generator Oxygen delivery without a blender Variety of interfaces Easy to set up and use Validated high-level disinfection process
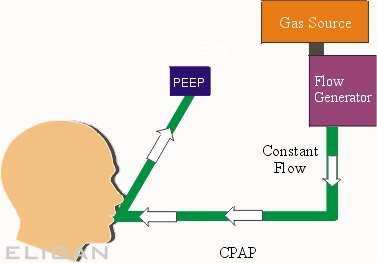
17 VENTILATORS-schematic
18 VENTILATORS-terminology TIME I - Time: amount of time spent in inspiration E - Time: amount of time spent in expiration Volume Amount of tidal volume that a patient receives Pressure Measure of impedance to gas flow rate Flow Measure of rate at which gas is delivered
19 VENTILATORS-terminology PEEP = positive end expiratory pressure Pressure maintained in the airways at the end of exhalation Keeps Alveoli from collapsing PIP = peak inspiratory pressure Point of maximal airway pressure Delta P = the difference between PIP PEEP MAP = mean airway pressure
20 MODES OF VENTILATION Controlled Mechanical Ventilation (CMV) Assist Control (AC) Continuous Positive Airway Pressure (CPAP) Intermittent Mandatory Ventilation (IMV) Synchronized Intermittent Mandatory Ventilation (SIMV) Pressure Support Volume Support Pressure Regulated Volume Control (PRVC)
21 VOLUME VENTILATION Preset Volume PEEP Rate I-time FiO2 Ventilator Determines Pressure required Advantages Guaranteed minute ventilation More comfortable for patient Draw-backs Large ETT leak Not optimal for poorly compliant lungs
22 PRESSURE VENTILATION Preset PIP PEEP Rate I-time Advantages Provides more support at lower PIP for poorly compliant lungs Draw back Minute ventilation not guaranteed FiO2 Vent determines Tidal volume given
23 MODES OF VENTILATION Control Modes: every breath is fully supported by ventilator in classic control modes, patients unable to breathe except at the controlled set rate in newer control modes, machines may act in assist-control, with a minimum set rate and all triggered breaths above that rate also fully supported. IMV Modes: intermittent mandatory ventilation modes - breaths above set rate not supported SIMV: vent synchronizes IMV breath with patient s effort
24 MODES OF VENTILATION Assist/Control Mode Ventilation Combined mode of ventilation Ventilator delivers positive pressure breath of predetermined TV in response to each inspiratory effort (assisted ventilation) If pt fails to initiate breath within a specific time period, ventilator automatically delivers a mechanical breath to maintain minimum or backup respiratory rate (controlled ventilation) To trigger assisted breath must lower airway pressure by preset amount- the trigger sensitivity.
25 MODES OF VENTILATION Advantages: Ensures the security of controlled ventilation and allows synchronization of the breathing rhythm of patient and ventilator. Ensures ventilatory support during every breath. Disadvantages: Excessive patient work may occur if inadequate peak flow or sensitivity setting, especially for pts with increased ventilatory drive May be poorly tolerated in awake, non-sedated subjects and can require sedation to ensure synchrony; May be associated with respiratory alkalosis due to excessive triggering of ventilator by anxious patient May potentially worsen air trapping
26 MODES OF VENTILATION Synchronized Intermittent Mandatory Ventilation Mandatory number of positive pressure breaths per minute, each synchronized to patient effort. Ventilator detects initiation of spontaneous breath and does not deliver machine breath during a spontaneous breath. Between mechanical breaths may breathe an indefinite number of times from reservoir Spontaneous breaths produce no response from the ventilator.
27 MODES OF VENTILATION Advantages: Pt able to perform variable amount of respiratory work with security of preset mandatory level of ventilation; Allows for variation in support-full support to spontaneous breathing Useful weaning mode. Disadvantages: Dysynchrony between pt effort and machine-delivered volume can occur especially with inadequate flow rates; Hyperventilation and respiratory alkalosis possible, similar to A/C; Excessive work of breathing during spontaneous breaths can occur due to presence of poorly responsive demand valve or inappropriate flow delivery; May potentially worsen air trapping with asthma.
28 MODES OF VENTILATION Pressure-Support Ventilation When inspiratory flow rate falls below preset threshold, flow of gas terminates. Patient controls respiratory rate and inspiratory time and flow. TV + minute ventilation partly determined by patient + partly by ventilator. Advantages: Most spontaneously breathing pts comfortable with little dys-synchrony. Useful as weaning tool Disadvantages: Tidal volume dependent on respiratory mechanics, cycling frequency, and patient-ventilator synchrony. Need careful monitoring for unstable patients and back-up minute ventilation needed for safety.
29 MODES OF VENTILATION Pressure Control Ventilation (PCV) Minimises static airway pressures in ARDS patients. Involves setting target airway pressure on ventilator which then delivers rapid flow to that set pressure with a square pressure wave form. Advantages: Airway pressures uniformly controlled by set pressure limit thus minimizing overdistension Decelerating flow curve? allows improved oxygenation by optimizing alveolar recruitment Disadvantages: Can be an uncomfortable mode of ventilation and thus require significant sedation TV varies with compliance close monitoring avoid excessive/inadequate ventilation
30 MODES OF VENTILATION Pressure regulated volume control (PRVC) Good alternative to PCV if rapidly changing compliance -Remains a pressure regulated approach but pressure varies to maintain given tidal volume. Tidal volume, PEEP, rate, inspiratory time is set Advantage of having a guaranteed tidal volume with a flow pattern that doesn t harm the lungs Agitated patients may hyperventilate
31 MODES OF VENTILATION Airway Pressure Release Ventilation (APRV) Spontaneous breathing with CPAP interrupted by short (1-1.5s) releases of pressure to augment expiration. Moderately high airway pressure (20-30 cm H2O) most of the time, thereby keeping alveoli open. Unique in that ventilation is enhanced by reduction rather than increase in lung volume. During short expiratory release PEEP remains present to keep alveoli with slow time constants open as well
32 MODES OF VENTILATION Advantages: Preservation of spontaneous breathing -may improve comfort + decrease sedation need CPAP useful in keeping alveoli open A short expiratory time which favours ventilation of fast compartments Reduced barotrauma risk Relatively low airway pressures - volutrauma, improve pulmonary circulation + O2 delivery
33 MODES OF VENTILATION Disadvantages: Very short expiration times can lead to incomplete exhalation of slow compartments of the lung which can lead to the development of auto-peep secondary to breath stacking Requires spontaneous respiratory drive? associated with work of breathing Dead space ventilation may be relatively increased due to lower tidal volumes Potential for de-recruitment and atelectrauma during intermittent pressure releases
34 Conventional (Positive Pressure) Ventilation Trigger Limits Cycle Controlled Ventilator Ventilator Ventilator (time) Assisted Patient Ventilator Ventilator (time) Supported Patient Ventilator Patient (flow)
35 CASE 1 SIMV 27 cmh2o PIP and 6 cmh2o PEEP, to generate a tidal volume of 6 7ml kg 1 Central venous and arterial access Nebulized salbutamol was administered. Intravenous cefotaxime was added to her antibiotic regime
36 CASE 1 Deteriorated: HFOV Oxygenation index was 19.0 Alveolar Arterial Difference in Oxygen (AaDO2) 520 mmhg. Prone position Therapeutic options reconsidered nitric oxide, steroids, surfactant, and ECMO discussed
37
38 HFOV Adjustable Parameters Mean Airway Pressure: usually set 2-4 higher than MAP on conventional ventilator Amplitude: monitor chest rise Hertz: number of cycles per second FiO2 I-time: usually set at 33%
39 HFOV Advantages: Decreased barotrauma / volutrauma: reduced swings in pressure and volume Improve V/Q matching: secondary to different flow delivery characteristics Disadvantages: Greater potential of air trapping Hemodynamic compromise Physical airway damage: necrotizing tracheobronchitis Difficult to suction Often require sedation

40 SETTING THE VENTILATOR
41 Ventilator Settings- FiO 2 Dangerous drug Lowest setting to keep Sats >88-92 % Closed loop Auto-weaning Trigger α Patient comfort Flow vs Pressure Beware Auto-triggering Beware increased work of breathing New Neurally Adjusted Ventilatory Assist
42 Ventilator Settings- PEEP Role in Paediatrics? Improve FRC > Closing capacity Normal healthy lung has PEEP +/- 3-5 cmh 2 O Intubation removes natural PEEP augmentation bypassing post pharynx Generally 8-10 cmh 2 O Higher for recruitment Contra-indications Isolated head injury Asthma
43 Ventilator settings- Driving Pressure PIP vs ΔP Generates MAP oxygenation Generates TV Alveolar ventilation Should not exceed 30 cm H 2 O
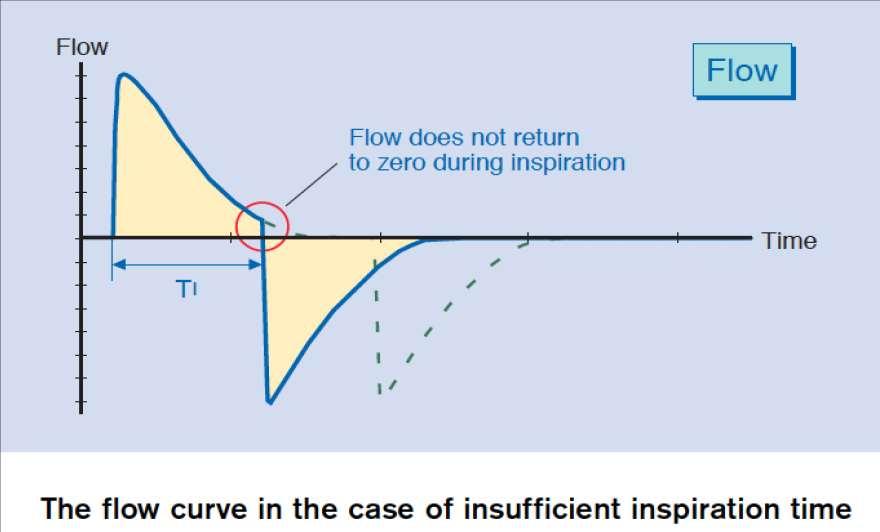
44 Ventilator settings I:E I-time / I:E ratios Dependent on age of patient Dependent on time constant relationship to compliance and resistance of the lung Neonate 0.4sec, Child sec, Big Child 1 sec Guided by Flow-time curve
45
46


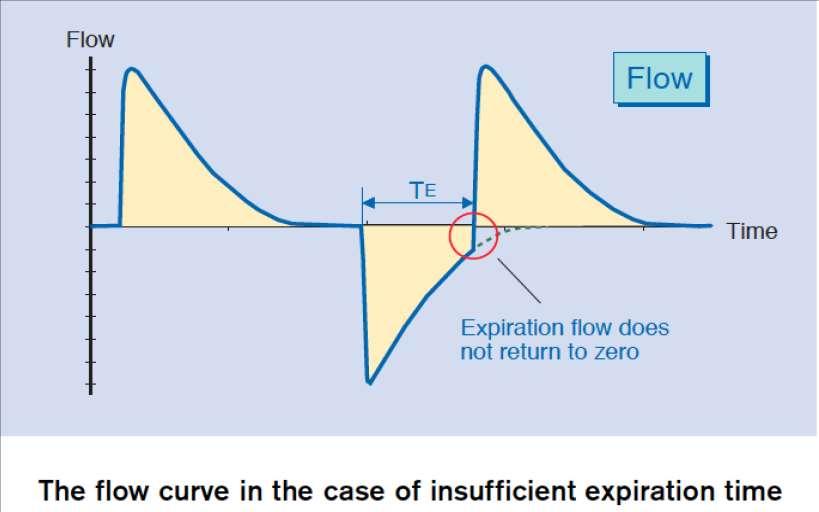
47 Too short Ti will reduce delivered Vt unneccessary high PIP will be applied unnecessary high intrathoracic pressures Too short Te will not allow to deliver max. possible Vt at given P will induce PEEPi increases the risk for hemodynamic instability The patient respiratory mechanics dictate the maximal respiratory frequency
48 Ventilator Settings- Rate In Assist control back-up rate Set to allow spontaneous breaths Air drawn to lower regions Avoid high rates to blow off CO 2 Can cause drop in TV; dead space ventilation Be guided by flow-time curve
49 TRICK #3 Know how to manage different diseases Know the pathophysiology Lung protective strategies
50 HYPOXIA Hypoventilation: decreased alveolar ventilation, i.e. CNS depression Diffusion impairment: abnormality at pulmonary capillary bed Shunt: blood flow without gas exchange Intra-pulmonary Intra-cardiac Ventilation-perfusion mismatch: Both dead space and shunt abnormalities


51 TREATING HYPOXIA Increase FiO 2 : >60% toxic to lung parenchyma Increase mean airway pressure PEEP : not too much, not too little PIP I-time
52 HYPERCARBIA Decreased minute ventilation Respiratory rate Tidal volume Treatment: Increase respiratory rate: assure I-time not too short as rate increased Increase tidal volume Allow permissive hypercarbia

53 LUNG PROTECTIVE STRATEGIES High PEEP Pressure limiting PIP: <30 cmh2o Low tidal volume: 4-6 ml/kg FiO2 <60% Permissive hypercarbia Permissive hypoxia
54 ALI/ARDS Disorders marked by a significant inflammatory response to a local (pulmonary) or remote (systemic) insult resulting in injury to alveolar epithelial and endothelial barriers of the lung, acute inflammation and protein rich pulmonary oedema. ARDS is the more severe form of ALI.
55
56
57 ARDS Management Mechanisms implicated in VILI Oxygen toxicity from use of high FiO2 Over distension of alveoli leading to volutrauma and barotrauma Repetitive opening and closing of alveoli causing shear stress and triggering further inflammation (atelectrauma)
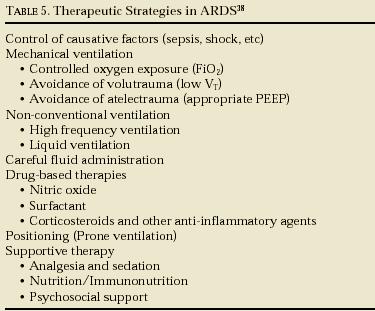
58 ARDS Management Key features of lung protective ventilation Controlled oxygen exposure Permissive hypercapnia Low tidal volumes 4-6 ml/kg Adequate PEEP Peak pressure < 30 cm H2O
59 ARDS Management- PEEP PEEP improves oxygenation by providing movement of fluid from the alveolar to interstitial space, recruitment of small airways and collapsed alveoli and an increase in functional residual capacity. PEEP is adjusted between 8 cm H2O and 20 cm H2O; PEEP is progressively increased by 2-3 cm H2O increments to maintain saturation between 90 and 95% with FiO2 < 0.5. The child should be monitored for any evidence of cardiovascular compromise and hyperinflation
60 ARDS- HFOV The advantages of HFOV are use of low VT and avoidance of barotrauma maintenance of near normal PaCO2 with improved minute ventilation. Some studies in paediatric population have shown that early initiation of HFOV is associated with better oxygenation but none have demonstrated clearly improved outcome.
61 ARDS- NITRIC OXIDE (NO) Causes pulmonary vasodilation and decrease in pulmonary hypertension. Maximal improvement in oxygenation is usually achieved with <10 ppm in most patients. The effect can be frequently seen in less than ten minutes or may take several hours. Paediatric studies suggest that ino improves short-term oxygenation in children with ARDS but little change is seen in long-term oxygenation indices.
 in these patients Dose: 2ml/kg")
62 ARDS- SURFACTANT THERAPY Metanalysis (Crit Care 2007) & systemic review of surfactant use in critically ill children with acute respiratory failure significant reduction in mortality, as well as a significant reduction of ventilator days and less need for rescue therapy (nitric oxide, High frequency ventilation and ECMO) in these patients Dose: 2ml/kg (50mg/kg/dose)
63 Acute hypoxaemic respiratory failure with no improvement within 48 hrs of starting ventilation using a lung protective strategy.(wilson, 2005) With OI >7 (Wilson 2005, Wilson 1999) With PF<150 (Luchetti 1998, 2002) Diffuse bilateral infiltrates on CXR (Wilson 1999, 2005, Moller 2003) Aspiration of hydrocarbons. ( Horoz OO 2010, Mastropietro 2011) Bronchiolitis Ventilated >24 hrs without improvement (Luchetti 1998) PF <160 (Luchetti 2002, 1998) CXR showing air trapping (Luchetti 2002)
64 ARDS- CORTICOSTEROIDS Prospective, randomized controlled trial prolonged administration of methylprednisolone in adult patients with unresolving ARDS (ARDS>7 days) improvement in lung injury and MODS scores and reduced mortality. Larger more recent RCTs have shown improved ventilatory parameters but increased late mortality in the group given steroids

65 PRONE POSITIONING Changes in regional lung perfusion, regional pleural pressures & recruitment of dorsal lung improve oxygenation during prone positioning Few risks & costs involved

66 CASE 2 Child Amy 13-year-old girl History of recurrent exacerbations of asthma Now sudden onset of severe respiratory distress 2 hours earlier. She had not improved, despite repeated doses of aerosolised salbutamol
67 CASE 2 Conscious patient, agitated Increasing respiratory effort, RR 55 Intercostal and suprasternal retraction and nasal flaring. Wheezing, poor air entry and poor chest movement, the heart rate had increased 165 min 1, whilst her skin was still warm and well perfused.
68 CASE 2 Deteriorated inability to speak, a decrease in chest movement, air entry, sats 85% Non-invasive assisted ventilation using triggered full-face mask biphasic positive airway pressure (BiPAP) at 5 and 20 cmh20 ABG: ph of 7.1, pco2 65mmHg, po2 75mmHg, BE 8, lactate 8mmol l 1, and a potassium of 2.3mmol l 1. Over the next hour, fluctuating conscious state and markedly decreased peripheral perfusion. INTUBATED
69 PULMONARY DISEASE- RESTRICTIVE Compromised lung volume: Intrinsic lung disease External compression of lung Recruit alveoli, optimize V/Q matching Lung protective strategies
70 PULMONARY DISEASE- OBSTRUCTIVE Airway obstruction causing increase resistance to airflow: e.g. asthma Optimize expiratory time by minimizing minute ventilation Bag slowly after intubation Don t increase ventilator rate for increased CO 2
71 ASTHMA Pressure controlled ventilation (keep PIP <30) or volume controlled ventilation (Tv 5-8 ml/kg) may be used A long expiratory time (with a optimum inspiratory time) with an I/E ratio of >1:2 and a slow rate allow emptying of the lungs and avoid air trapping and progressive hyperinflation Manual decompression of chest may help to deflate overinflated lungs and improves ventilation.
.")
72 ASTHMA Sedation important to avoid the complications of air-leak Preferred drugs for these patients are ketamine (has a bronchodilator effect) & fentanyl (as morphine causes histamine release which might aggravate bronchospasm).? Suction and physiotherapy clear mucus plugging and prevent atelectasis Specific treatments for asthma nebulised and intravenous salbutamol, intravenous aminophylline, systemic steroids and magnesium sulphate
73 CASE 2 Initially, the ventilator was set at a rate of 30 min 1, I:E ratio 1:4, PIP 40 cmh2o, and PEEP 0cmH2O. Considering a rise in arterial pco2 from 110 to 130mmHg, the PEEP was increased to 8 cmh2o. Infusions of ketamine, midazolam, and paralysis with a vecuronium infusion Magnesium sulphate at a dose of 30 mg kg 1per h was added to the continuous intravenous treatment with salbutamol and aminophylline.
")
74 BRONCHIOLITIS Apnoeas (relatively normal lungs) Minimise VILI with low Tv Air trapping Manage like asthma ARDS Manage like ARDS (including HFOV, ino, ECMO)
 Minimise atelectrauma (adequate PEEP) Minimise volutrauma (low Tv 4-6 ml/kg)")
75 PNEUMONIA/LUNG COLLAPSE Minimise oxygen toxicity (FiO2 <0.60) Minimise atelectrauma (adequate PEEP) Minimise volutrauma (low Tv 4-6 ml/kg) Permissive hypercapnia
 Neurogenic")
76 PULMONARY OEDEMA/HAEMORRHAGE Cardiogenic Negative pressure (post-obstructive) Neurogenic Non-cardiogenic
77 PULMONARY OEDEMA/HAEMORRHAGE Conventional ventilation Minimise oxygen toxicity (FiO2 <0.60) Minimise atelectrauma (adequate PEEP) Minimise volutrauma (low Tv 4-6 ml/kg) Permissive hypercapnia High frequency ventilation Constant MAP Recruitment of lung

78 TRICK #4 Be safe Safety bundle
79 VENTILATOR-ASSOCIATED PNEUMONIA (VAP)BUNDLE: DVT prophylaxis GI prophylaxis Head of bed (HOB) elevated to Daily Sedation Vacation Daily Spontaneous Breathing Trial
80 TRICK #5 Daily assessment trial of readiness to extubate Adjuncts to extubation eg decr airway oedema in UAO (steroids >6 hrs) Sedation holiday Conservative fluid regime
81
82 Daily sedation vacation/ Spontaneous Breathing Trials Implement a protocol to lighten sedation daily at an appropriate time to assess for neurological readiness to extubate. Include precautions to prevent self-extubation such as increased monitoring and vigilance during the trial. Include a sedation vacation strategy in your overall plan to wean the patient from the ventilator if you have a weaning protocol, add "sedation vacation" to that strategy.

83 VENTILATOR MODES IN WEANING

84 CRITERIA FOR EXTUBATION READINESS TEST FAILURE Pediatr Crit Care Med 2009 Vol. 10, No. 1

85 TRICK #6 Know how to read problems on your vent

86 Air Leak

87 Autocycling
88 Secretions
89 Auto PEEP If the respiratory rate is set high or the expiratory time is not long enough there is a risk for auto PEEP. The patient does not have enough time to exhale and it is evident on the flow curve that flow will not return to zero before the next breath starts.
90 Considerations aimed at alleviating this condition could be: 1. Decreasing the set respiratory rate; 2. Decreasing the inspiratory time to give more expiratory time; 3. If the patient is triggering the respiratory rate, consider that : the tidal volume is not appropriate (too small) and the patient may be experiencing hypoventilation, or the patient may be hypoxemic and attempt to increase mean airway pressure by creating a higher PEEP. In this case, an increase in the PEEP level may be appropriate.
91 Pressure volume loop If an imaginary line is drawn to connect the origin of the loop with the PIP, it can estimate the dynamic compliance of the lung. Compliance is mathematically determined by Δ volume/ Δ pressure Is graphically displayed on the LOOP screen.
92 Pressure volume loop A loop indicating good compliance will be described as upright (compliance axis>45 ) A loop indicating poor compliance is described as flat, or lying on its side.
93 OVERDISTENTION

94 Pressure volume loop Inadequate hysteresis, producing a narrow loop, may be indicative of inadequate flow


95 Flow volume loop The effect of altering resistance by use of a bronchodilator. After treatment, resistance improves, and there is a demonstrable difference in the appearance of the loop.
96 FLOW SYNCHRONY Defined as the ideal matching of inspiratory flow of a ventilator breath to the patient's inspiratory demand during assisted or supported ventilation. Asynchrony: Inadequate inspiratory flow at any point during inspiration causing an increased or irregular patient effort. leads to increased WOB fighting the ventilator
97 FLOW ASYNCHRONY
98 TRIGGER INSENSITIVITY
99 INSPIRATORY SYNCHRONY Optimal inspiratory patient - ventilator synchrony is a function of: inspiratory flow pattern adequate inspiratory flow appropriate trigger sensitivity ETT effects appropriate lung inflation
100 PATIENT- VENTILATOR INTERACTIONS Expiratory synchrony end-expiratory lung volume premature termination of exhalation & intrinsic PEEP expiratory resistance
101 INSPIRATORY RISE TIME Inspiratory rise time is the time taken to reach peak inspiratory flow or pressure at the start of each breath, expressed either as a percentage of the respiratory cycle time or in seconds.
102 INSPIRATORY RISE TIME The flow and pressure rise time can be adapted in accordance with the patient. The Inspiratory rise time has to be set to a comfortable value for the patient and can be evaluated by the shape of the flow and pressure curves
103 CONCLUSION Children have natural propensity to have lung collapse Ventilation aims to restore oxygenation, lung volumes, decrease work of breathing Set Ventilator to cause least harm, most benefit and comfort to the patient
104 CONCLUSION Rare for a child to fight ventilation Hypoxia Blocked tube Inadequate settings DO NOT SEDATE/PARALYSE WITHOUT CAUSE Sedation Protocols keep patient comfortable, not agitated allow spontaneous breathing
105 CONCLUSION Tricks of the Trade: Recognise sick kids and goals of ventilation Know your ventilator & settings Learn how to manage different diseases Lung protective strategies Be safe Daily assessment trial of readiness to extubate Know how to read problems on the vent
106 Available on request Acknowledgements: Dr Mary Morgan Dr Harshad Ranchod Dr Susan Murphy Dr Linda Doedens Prof A Argent REFERENCES

107 Thank you
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Potential Conflicts of Interest
 Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION
 DEFINITION") CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
VENTILATOR GRAPHICS ver.2.0. Charles S. Williams RRT, AE-C
 VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
Lung Wit and Wisdom. Understanding Oxygenation and Ventilation in the Neonate. Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital
 Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Monitor the patients disease pathology and response to therapy Estimate respiratory mechanics
 Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Effects of PPV on the Pulmonary System. Chapter 17
 Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL
 PROTOCOL") AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL A. Definition of Therapy: 1. Cough machine: 4 sets of 5 breaths with a goal of I:E pressures approximately the same of 30-40. Inhale time = 1 second, exhale
AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL A. Definition of Therapy: 1. Cough machine: 4 sets of 5 breaths with a goal of I:E pressures approximately the same of 30-40. Inhale time = 1 second, exhale
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Dr. AM MAALIM KPA 2018
 Dr. AM MAALIM KPA 2018 Journey Towards Lung protection Goals of lung protection Strategies Summary Conclusion Before 1960: Oxygen; impact assessed clinically. The 1960s:President JFK, Ventilators mortality;
Dr. AM MAALIM KPA 2018 Journey Towards Lung protection Goals of lung protection Strategies Summary Conclusion Before 1960: Oxygen; impact assessed clinically. The 1960s:President JFK, Ventilators mortality;
TO THE OPERATOR AND PERSON IN CHARGE OF MAINTENANCE AND CARE OF THE UNIT:
 fabian HFO Quick guide TO THE OPERATOR AND PERSON IN CHARGE OF MAINTENANCE AND CARE OF THE UNIT: This Quick Guide is not a substitute for the Operation Manual. Read the Operation Manual carefully before
fabian HFO Quick guide TO THE OPERATOR AND PERSON IN CHARGE OF MAINTENANCE AND CARE OF THE UNIT: This Quick Guide is not a substitute for the Operation Manual. Read the Operation Manual carefully before
Ventilator Waveforms: Interpretation
 Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
and Noninvasive Ventilatory Support
 Chapter 2 Mechanical Ventilation and Noninvasive Ventilatory Support Megan L. Anderson and John G. Younger PERSPECTIVE Invasive and noninvasive ventilation are essential tools for treatment of critically
Chapter 2 Mechanical Ventilation and Noninvasive Ventilatory Support Megan L. Anderson and John G. Younger PERSPECTIVE Invasive and noninvasive ventilation are essential tools for treatment of critically
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study
 D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Asthma Management in ICU. by DrGary Au From KWH
 Asthma Management in ICU by DrGary Au From KWH Overview of Asthma Pathophysiology Therapeutic options Medical treatment NPPV Mechanical ventilation Salvage therapy ~ 235 million people worldwide were affected
Asthma Management in ICU by DrGary Au From KWH Overview of Asthma Pathophysiology Therapeutic options Medical treatment NPPV Mechanical ventilation Salvage therapy ~ 235 million people worldwide were affected
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
You are caring for a patient who is intubated and. pressure control ventilation. The ventilator. up to see these scalars
 Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Slide 1. Slide 2. Slide 3 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Objectives: I have nothing to disclose.
 Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Basics of NIV. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Respiratory Failure in the Pediatric Patient
 Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Diagnosis and Management of Acute Respiratory Failure
 Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
CLINICAL VIGNETTE 2016; 2:3
 CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
Respiratory Distress During RSV Season
 Respiratory Distress During RSV Season Carroll King, MD, FAAP Disclosure : Carroll King, MD, FAAP has nothing to disclose. 1 Objectives At the end of this educational activity, participants should be able
Respiratory Distress During RSV Season Carroll King, MD, FAAP Disclosure : Carroll King, MD, FAAP has nothing to disclose. 1 Objectives At the end of this educational activity, participants should be able
Proportional Assist Ventilation (PAV) (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure
 (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure") Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล
 Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
C h a p t e r 1 4 Ventilator Support
 C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Module 4: Understanding MechanicalVentilation Jennifer Zanni, PT, DScPT Johns Hopkins Hospital
 Module 4: Understanding MechanicalVentilation Jennifer Zanni, PT, DScPT Johns Hopkins Hospital Objectives Upon completion of this module, the learner will be able to: Identify types of airways and indications
Module 4: Understanding MechanicalVentilation Jennifer Zanni, PT, DScPT Johns Hopkins Hospital Objectives Upon completion of this module, the learner will be able to: Identify types of airways and indications
CONVENTIONAL VENTILATION Part II
 CONVENTIONAL VENTILATION Part II Conventional Ventilation Part II Objective of Presentation Review disease specific ventilator strategies Discuss non-invasive approaches to improving gas exchange Review
CONVENTIONAL VENTILATION Part II Conventional Ventilation Part II Objective of Presentation Review disease specific ventilator strategies Discuss non-invasive approaches to improving gas exchange Review
NAVA. In Neonates. Howard Stein, M.D. Director Neonatology. Neurally Adjusted Ventilatory Assist. Toledo Children s Hospital Toledo, Ohio
 NAVA Neurally Adjusted Ventilatory Assist In Neonates Howard Stein, M.D. Director Neonatology Toledo Children s Hospital Toledo, Ohio Disclaimers Dr Stein: Is discussing products made by Maquet Has no
NAVA Neurally Adjusted Ventilatory Assist In Neonates Howard Stein, M.D. Director Neonatology Toledo Children s Hospital Toledo, Ohio Disclaimers Dr Stein: Is discussing products made by Maquet Has no
Mechanical ventilation in the emergency department
 Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
COBIS Management of airway burns and inhalation injury PAEDIATRIC
 COBIS Management of airway burns and inhalation injury PAEDIATRIC 1 A multidisciplinary team should provide the management of the child with inhalation injury. Childhood inhalation injury mandates transfer
COBIS Management of airway burns and inhalation injury PAEDIATRIC 1 A multidisciplinary team should provide the management of the child with inhalation injury. Childhood inhalation injury mandates transfer
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
MECHANICAL VENTILATION PROTOCOLS
 GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
An introduction to mechanical ventilation. Fran O Higgins, Adrian Clarke Correspondence
 Update in Anaesthesia An introduction to mechanical ventilation Respiratory Summary Mechanical ventilation is the major invasive intervention offered in the ICU. In low income countries, where the facilities
Update in Anaesthesia An introduction to mechanical ventilation Respiratory Summary Mechanical ventilation is the major invasive intervention offered in the ICU. In low income countries, where the facilities
Non Invasive Ventilation In Preterm Infants. Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid
 Non Invasive Ventilation In Preterm Infants Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid Summary Noninvasive ventilation begings in the delivery room
Non Invasive Ventilation In Preterm Infants Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid Summary Noninvasive ventilation begings in the delivery room
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
7 Initial Ventilator Settings, ~05
 Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
CHAPTER 2 Mechanical Ventilation and Noninvasive Ventilatory Support
 CHAPTER 2 Mechanical Ventilation and Noninvasive Ventilatory Support Todd A. Seigel PERSPECTIVE Invasive and noninvasive ventilation are essential components in the management of critically ill patients.
CHAPTER 2 Mechanical Ventilation and Noninvasive Ventilatory Support Todd A. Seigel PERSPECTIVE Invasive and noninvasive ventilation are essential components in the management of critically ill patients.
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
New Modes and New Concepts In Mechanical Ventilation
 New Modes and New Concepts In Mechanical Ventilation Prof Department of Anesthesia and Surgical Intensive Care Cairo University 1 2 New Ventilation Modes Dual Control Within-a-breath switches from PC to
New Modes and New Concepts In Mechanical Ventilation Prof Department of Anesthesia and Surgical Intensive Care Cairo University 1 2 New Ventilation Modes Dual Control Within-a-breath switches from PC to
Recurrent wheezing illnesses 24.9% Similar to Australia Above global averages
 Prof Mike South Department of General Medicine Royal Children s Hospital Melbourne Australia www.mikesouth.org.au Asthma is very common in Australia Approx 25% children have recurrent wheezing illnesses
Prof Mike South Department of General Medicine Royal Children s Hospital Melbourne Australia www.mikesouth.org.au Asthma is very common in Australia Approx 25% children have recurrent wheezing illnesses
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
GE Healthcare. Non Invasive Ventilation (NIV) For the Engström Ventilator. Relief, Relax, Recovery
 For the Engström Ventilator. Relief, Relax, Recovery") GE Healthcare Non Invasive Ventilation (NIV) For the Engström Ventilator Relief, Relax, Recovery COPD is currently the fourth leading cause of death in the world, and further increases in the prevalence
GE Healthcare Non Invasive Ventilation (NIV) For the Engström Ventilator Relief, Relax, Recovery COPD is currently the fourth leading cause of death in the world, and further increases in the prevalence
Practical Application of CPAP
 CHAPTER 3 Practical Application of CPAP Dr. Srinivas Murki Neonatologist Fernadez Hospital, Hyderabad. A.P. Practical Application of CPAP Continuous positive airway pressure (CPAP) applied to premature
CHAPTER 3 Practical Application of CPAP Dr. Srinivas Murki Neonatologist Fernadez Hospital, Hyderabad. A.P. Practical Application of CPAP Continuous positive airway pressure (CPAP) applied to premature
Emergency Department Protocol Initiative
 Emergency Department Protocol Initiative ACUTE ASTHMA MANAGEMENT TOOLKIT March 2006 Provincial Emergency Services Project PHYSICIAN ORDER TEMPLATE FOR CTAS LEVEL 1 ASTHMA ADULT PEDIATRIC Date: Site: Arrival
Emergency Department Protocol Initiative ACUTE ASTHMA MANAGEMENT TOOLKIT March 2006 Provincial Emergency Services Project PHYSICIAN ORDER TEMPLATE FOR CTAS LEVEL 1 ASTHMA ADULT PEDIATRIC Date: Site: Arrival
Ventilating the paediatric patient. Lizzie Barrett Nurse Educator November 2016
 Ventilating the paediatric patient Lizzie Barrett Nurse Educator November 2016 Acknowledgements Kate Leutert NE PICU Children's Hospital Westmead Dr. Chloe Tetlow VMO Anaesthetist and Careflight Overview
Ventilating the paediatric patient Lizzie Barrett Nurse Educator November 2016 Acknowledgements Kate Leutert NE PICU Children's Hospital Westmead Dr. Chloe Tetlow VMO Anaesthetist and Careflight Overview
Web Appendix 1: Literature search strategy. BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up. Sources to be searched for the guidelines;
 write-up. Sources to be searched for the guidelines;") Web Appendix 1: Literature search strategy BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up Sources to be searched for the guidelines; Cochrane Database of Systematic Reviews (CDSR) Database of
Web Appendix 1: Literature search strategy BTS Acute Hypercapnic Respiratory Failure (AHRF) write-up Sources to be searched for the guidelines; Cochrane Database of Systematic Reviews (CDSR) Database of
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
SESSION 3 OXYGEN THERAPY
 SESSION 3 OXYGEN THERAPY Harith Eranga Yapa Department of Nursing Faculty of Health Sciences The Open University of Sri Lanka 1 Outline Methods of delivery Complications of oxygen therapy Artificial airways
SESSION 3 OXYGEN THERAPY Harith Eranga Yapa Department of Nursing Faculty of Health Sciences The Open University of Sri Lanka 1 Outline Methods of delivery Complications of oxygen therapy Artificial airways
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015
: Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015") Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
CURRENT TRENDS IN NON-INVASIVE VENTILATION. Disclosures. Why not invasive ventilation? Objectives. Currently available modes
 CURRENT TRENDS IN NON-INVASIVE VENTILATION ----------------------------------------------------------- Karen Drinkard, RRT-NPS Neonatal Respiratory Clinical Specialist University of Washington Medical
CURRENT TRENDS IN NON-INVASIVE VENTILATION ----------------------------------------------------------- Karen Drinkard, RRT-NPS Neonatal Respiratory Clinical Specialist University of Washington Medical
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,